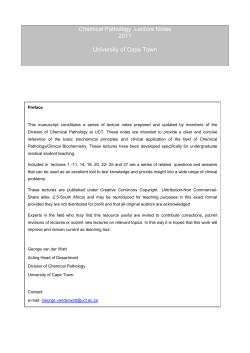
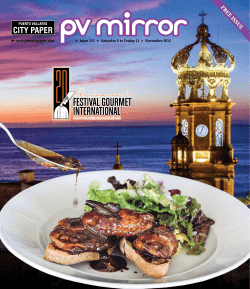
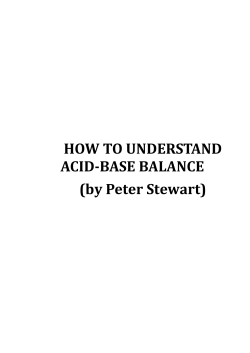
RAPID COMMUNICATION Activated Protein C Resistance: Molecular Mechanisms Based on Studies Using Purified G1n5O6-FactorV By Mary J. Heeb, Yumi Kojima, Judith S. Greengard, and John H. Griffin Gln=-factor V (W) was purified from plasma of an individual homozygous for an Arg506Gln mutation in FV that is associated with activatedproteinC (APC)resistance.Purified GlnW-FV, aswell as Glnm-FVa generated by either thrombin or FXa, conveyed APC resistance to FV-deficient plasma in coagulation assays. Clotting assay studies also suggested that APC resistance doesnot involve any abnormalityin FVAPC-cofactor activity. In purified reaction mixtures,GlnmFVa in comparison to normal N a showed reduced susceptibility to APC,because it was inactivated -10-fold slower It was previously reported that inacthan normal ArgW-FVa. tivation of normal FVa by APC involves an initial cleavage at Argm followed by phospholipid-dependent cleavage at Argaos.lmmunoblotandaminoacid sequenceanalyses of Glnm-FVa was showed that the 102-kDheavychain cleaved at Argaos duringinactivation byAPC in a phospholipid-dependent reaction. This reducedbut measurable susceptibilityof Glnm-FVa to APC inactivation may help explain why APC resistance is a mild risk factor for thrombosis becauseAPCcan inactivatebothnormalFVa andvariant Glnm-FVa. In summary, this study shows that purified Gln--FV can account for APC resistanceof plasma because Gln=-FVa, whether generated by thrombin or M a , is relatively resistant to APC. 0 7995 by The AmericanSociety of Hematology. T with 2.6 for pooled nomal plasma using APTT assays as previously described.' The father (age 63 years), mother (age 63 years), and sister (age 26 years) of the individual were determined to be heterozygous for the mutation Arg506Gln in FV and to be A X resistant (AP'IT ratios of 1.5, 1.7, and 1.65, respectively). A brother (age 29 years) was determined to have only normal FV and plasma that was not APC resistant. The only notable thrombosis episode occurring before the age of 60 years in this family was a documented incident of thrombophlebitis and pulmonary embolism presented by the father of the propositus at 49 years of age. The fraternal grandparents and the fraternal uncle of the propositus were reported to have experienced deep vein thrombosis, stroke, and myocardial infarction after 60 years of age, respectively. Free protein S antigen (Asserachrom free protein S ; Diagnostica Stago, Asnieres, France) and protein C amidolytic activityx7were within the normal ranges for the propositus, his parents, and two siblings. FVpurifcation. Blood (450 mL) from the individual homozygous for the mutation Arg506Gln in FV was collected after informed consent into 50 mL of 0.11 m o a trisodium citrate. Plasma was prepared by centrifugation at room temperature and made 50 pg/ mL in soybean trypsin inhibitor, 10 mmoIL in benzamidine, and 1 0 0 U/mL in aprotinin and frozen at -70°C. A second unit (450 mL) of blood was similarly obtained 8 weeks later, and the plasma was treated with inhibitors and combined with thawed plasma from HE PROTEIN C anticoagulant pathway provides a major physiologic mechanism that regulates thrombosis, and defects in this pathway account for most currently known genetic risk factors for venous thrombosis. Hereditary heterozygous deficiency of protein C or of protein S is associated with increased risk for venous thrombosis in young adults,'-3 whereas severe deficiency (< 1%) of protein C or protein S is associated with purpura fulminans or massive venous thrombosis in the neonatal peri0d.4.~Another hereditary abnormality of the protein C pathway involves a laboratory finding of a poor anticoagulant response to activated protein C (APC), termed APC re~istance.~.' APC resistance is detected in 20% to 50% of venous thrombosis patients, depending on criteria for patient population selection.'.'' The genetic and molecular basis for APC resistance involves a mutation in the coagulation factor V (W)gene at nucleotide 1691 that causes the mutation, Arg506Gln.I3-l5Two reports of functional activity studies suggested that the variant GlnSM-FVais resistant to cleavage by APC.'3*'6One report, using FV purified from two individuals heterozygous for the ArgSO6Gln-W mutation, concluded that thrombin-activated GlnsM-FVais APC resistantI6;however, another report, using unpurified adsorbed plasma from an individual homozygous for the Arg506Gln mutation, concluded that Gln5M-FVagenerated by Factor Xa ( m a ) activation is APC resistant, whereas Gln5"-FVa generated by thrombin activation is not APC resi~tant.'~ Todate, no studies comparing purified Gln5"FV activated by FXa or by thrombin have been reported. To address this controversy and to assess the hypothesis that purified Glns"-FV indeed accounts for APC resistance in plasma, the present study based on purification of GlnSM-FVfrom homozygous plasma was undertaken. MATERIALS AND METHODS Patient material. During testing of normal laboratory worker volunteers for APC resistance, a 32-year-old man was identified as homozygous for the DNA mutation predicted to give Gln5"-FV using DNA analysis performed as previously described.14Clotting assays of the proband's plasma showed it to be markedly APC resistant with a ratio of (activated partial thromboplastin time [AFTTI + APC)/(AFIT) of 1.1 to 1.3 on different dates, compared Blood, Vol 85, No 12 (June 15). 1995: pp 3405-3411 From the Departments of Molecular and Experimental Medicine and of Vascular Biology, The Scripps Research Institute, La Jolla, CA. Submitted February 16, 1995: accepted March 21, 1995. Supported in part by National Institutes of Health Grants No. ROI-HW2246, ROl-HL21544, and MOIRR00833 and by the Stein Endowment Fund. A preliminary report of this study was presented at the American Heart Association Meeting, Dallas, l X , November, 1994, and at the American Society of Hematology Meeiing, Nashville, TN, December, 1994. Address reprint requests to SBRS, The Scripps Research Institute, I0666 N Torrey Pines Rd. La Jolla, CA 92037. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordnnce with 18 U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8512-0.00/0 3405 3406 the first collection. Diisopropylfluorophosphateand phenylmethylsulfonic acid were each added to a concentration of 1 mmoVL and the plasma was barium adsorbed as described." The supernatant solution was sequentially treated with 7% and then 13% polyethylene glycol-6000 (PEG); the precipitate from 13%PEG containing FV was further purified as described." FV was similarly prepared from 500 mL of plasma from an individual determined not to be APC resistant by APTT and from 1.5 L of pooled plasma from 6 individuals of undetermined APC resistance status. In experiments described below, normal FV from the single donor was used unless otherwise stated. FV characterization and activation. FV was characterized by absorbance at 280 nm using Ala, = 8.9, by sodium dodecyl sulfatepolyacrylamide gel electrophoresis (SDS-PAGE), by enzyme-linked immunosorbent assay (ELISA) for FV antigen, and by functional assay. The sandwich ELISA was performed as described for protein S antigen" using immobilized rabbit anti-FV IgG (Dako, Carpenteria, CA) at 7.5 pg/mL as the capturing antibody and monoclonal anti-FVa light chain antibody at 5 pg/mL (Hematologic Technologies, Essex Jct, VT) as the detecting antibody. Dilutions of normal plasma were simultaneously assayed and the data were used to construct a standard curve, assuming a plasma concentration of 30 nmol/ L FV antigen. FV activity was determined in a FXa-l-stage assay in which 60 pL of FV-deficient plasma (George King Biomedical, Overland Park, KS) was mixed with 20 pL of HEPES-buffered saline, pH 7.4 (HBS), and 50 pL of cephalin (prepared as recommended by the manufacturer, Sigma, St Louis, MO). After 2 minutes of preincubation of this reaction mixture at 37"C, IO pL containing 20 nmoVL FXa (Enzyme Research Laboratories, South Bend, IN) and IO pL of a dilution of normal plasma or of a test sample as a source ofFV or FVa were added. Finally, 50 pL of 33 mmol/L CaCI,inHBS containing 1% bovine serum albumin (BSA) was added and clot time was measured at 37°C using an ST4 coagulometer (American Bioproducts, Parsippany, NJ). FV activity in the test samples was calculated by reference to a standard curve constructed with dilutions of normal plasma. Activity was expressed in units, in which 1 U equals the FV coagulant activity in I mL of normal plasma. FV (1 00 nmoUL) was activated at room temperature in HBS containing 0.5% BSA and 5 mmoUL CaCI2 using either I nmol/L thrombin (Enzyme Research Laboratories) or IO nmol/L FXa and 25 MmoVL phospholipid vesicles (20% phosphatidylserine and 80% phosphatidylcholine). Maximal activation time for FV was about 1 hour in each case, after which thrombin was neutralized2' and the sample was diluted in HBS-0.5% BSA for immediate further use. APC resistance assays. APTT assays were performed as follows. FV-deficient plasma (45 pL) wasmixed with 5 pL of test sample (consisting of plasma, 1 nmoUL final FV, or 22 pmol/L final FVa) and 50 pL of Platelin LS (Organon Teknika, Durham, NC). After 200 seconds of preincubation at 37°C the mixture was recalcified with 30 mmol/L CaCI, in HBS, 0.5% BSA at 37°C in the presence or absence of 16 nmoVLAPC in this solution. The ratio of ( A m + APC)/(A€TT) was calculated. An FXa-l-stage assay was performed as indicated above, except that CaCl' was added in the presence or absence of 48 nmol/L final concentration of APC. The ratio of (clotting time + APC)/(clotting time) was calculated. APC inactivation of FVa. FVa or Gln5"-FVa was reacted with APC at various concentrations at room temperature in the presence of 25 pmol/L phospholipid vesicles, HBS, 0.5% BSA, and 5 mmol/ L CaC1,. Aliquots were removed at suitable times and immediately assayed for residual FVa activity in prothrombinase assays or boiled for 1 minute in SDS-PAGE sample buffer for immunoblotting analysis. Ofher analyses. Prothrombinase assays were as described else- HEEB ET AL Table 1. APC Resistance of W-Deficient Plasma Containing Aliquots of Plasma, F V ,or FVa Normal ArgWB-FV Test Sample Plasma Purified FV 1.9 Thrombin-activated3.0 FVa FXa-activated FVa 2.8 Xa-l- APT Stage Assay 2.1 3.1 4.6 3.2 Variant Gln50B-FV APTT Stage Assay 1.8 1.2 1.4 1.3 1.2 1.6 1.5 Xa-l- 1.4 1.4 where2' and used 20 pmoVL FVa or GlnSLm-FVa, 1 nmoVL FXa, 25 p m o K phospholipid vesicles, 5 mmoK CaCI,, 0.1 mmol/L " l , , and 0.3 pmollL prothrombin in HBS-0.5% BSA. The rate of thrombin formation was assessed using the chromogenic substrate S-2238 in a Biotek (Winooski, VT) microplate reader using Kineticalc software. SDS-PAGE was performed with 4% to 15% gradient gels in a mini-gel apparatus (Hoeffer, San Francisco, CA). For immunoblotting, gels were transferred to Immobilon membranes (Millipore, Bedford, MA), blocked, and reacted as described:' except that detection used rabbit anti-FVa heavy chain antiserum (1:500), followed by biotinylated antirabbit IgG diluted 1:1,000 (Pierce Chemical CO, Rockford, IL), streptavidin-alkaline phosphatase 1 :500 (Pierce), and phosphatase substrate kit (Bio-Rad, Hercules, CA). Antiserum to FV heavy chain was provided by Drs Jan Rosing, Guido Tans, and Harry Bakker (University of Limburg, Maastricht, The Netherlands). NH,-terminal amino acid sequences were obtained from bands on an Immobilon membrane using an Applied Biosystems (Foster City, CA) model 470A gas phase sequencer under the supervision of Dr Lisa Bibbs in The Scripps Research Institute Core Laboratory. Each experiment presented in Table 1 or in Figs I through 3 was performed on at least three separate occasions, with good agreement of results. RESULTS Variant GlnS"-FV waspurified from plasma obtained from an APC-resistant subject who was homozygous for the DNA mutation of G to A at nucleotide 1691 that predicts the mutation Arg506Gln. Normal FV and GlnSo6-FV were 2 5 0 % pure as judged byfinal antigedprotein ratio and 270% pure as judged by SDS-PAGE (data not shown). A purification of greater than 2,880-fold was achieved based on initial versus final antigedprotein ratio, with a recovery of 10% antigen. To define the APC resistance of the variant Gln5"-FV in comparison to normal F V , APTT assays were performed using FV-deficient plasma reconstituted with samples containing normal or variant forms of FV or FVa. Test samples including normal plasma, homozygous Gldo6-FV plasma, purified normal FV or FVa, or purified GlnSoh-FVor Gin'"'FVa were analyzed (Table 1). The APTT values for each test sample were determined in duplicate in the presence and in the absence of APC. The ratio of APTT in the presence ofAPC to the APTT valuein the absence of APCwas calculated in each case and the mean value for this APC resistance ratio is given in Table 1. When purified normal FV was used to reconstitute FV-deficient plasma, the APC resistance ratio was 3.1, similar to that seen for normal plasma, whereas the APC resistance ratio for the addition of APC RESISTANCE AND PURIFIED GLN~-FACTORV purified Gln'"-FV was 1.2, similar to that for whole plasma from the same subject homozygous for the Arg506Gln mutation. This finding shows that purified Glns"-FV indeed conveysAPC resistance to plasma, as predi~ted.'~"~ Subsequently, experiments were performed to determine whether normal and variant FVa generated by either thrombin or FXa activation conveyed APC resistance in AP?T assays. FVdeficient plasma was reconstituted with the various FVa species, as described under experimental procedures, and the APC resistance ratios were determined (Table 1). Normal FVa, whether generated by thrombin or by FXa activation, was quite susceptible to APC as indicated by APC resistance ratios of 4.6 and 3.2, respectively (Table 1). The data in Table 1 indicate that the variant Glns"-FVa, whether activated by thrombin or by FXa, was relatively resistant to APC, giving ratios of 1.6 and 1.5, respectively. These results indicate that, in comparison to normal FVa, the purified variant Glns"-FVa is relatively resistant to APC independent of whether it is activated by thrombin or FXa. If the variant Glns"-FVa were insusceptible, ie, completely resistant, to AFT, one would predict that the APC resistance ratio should be 1.00. However, values for APC resistance ratios of Glns"-FVa in APTT assays were 1.05 to 1.6 (Table 1 and data not shown). Ratios greater than 1.0 could conceivably reflect inactivation of FVIIIa byAPC during coagulation as monitored in APTT assays. To exclude any contribution of inactivation of FVIIIa by APC, FXa-1stage assays were also used for APC resistance tests because these are independent of FVIIIa. The APC resistance ratios from the ma-l-stage assays were also greater than 1.0, ie, 1.2 to 1.4 for Gln5"-FV and Gln5"-FVa (Table l), suggesting that Gln5"-FV and/or G1n'"-FVa are not completely insusceptible to APC. Interestingly, in the FXa-l-stage assays, the APC resistance ratio of normal FV was 1.9, whereas for normal FVa activated by FXa or thrombin the ratios were 2.8 and 3.0, respectively (Table 1). Similarly, when the APC resistance ratios were determined using APTT assays, the ratios for normal and variant FVa were greater than those for normal or variant FV (Table 1). Studies were made to define the influence on APC resistance ratios of the concentration of purified normal and variant FV that was added to FV-deficient plasma. When [FV] was varied from 0.9 to 4.5 nmol/L, the APC resistance ratios in FXa-l-stage assays for either normal FV or Gln'"-FV were essentially constant (1.90 2 0.05 or 1.15 -I- 0.05, respectively). Similarly, the APC resistance ratios in APTT assays were constant, ie, independent of [FV] between 0.9 and 4.5 nmoVL (3.35 +. 0.35 or 1.03 ? 0.05; data not shown). In the absence of APC, the FXa-l-stage clotting times for the mixture of FV-deficient plasma with normal FV varied from 55 to 35 seconds, and the clotting time for the FVdeficient plasma containing Glns"-FV varied from 51 to 34 seconds depending on the [FV] (0.9 to 4.5 nmol/L). The preparations of normal and variant FV used for these studies were mostly single-chain FV. Thus, the APC resistance ratio in FXa-l-stage and in APTT assays was independent of FV final concentration between 0.9 and 4.5 nmol/L, equivalent to an initial plasma FV level of 9% to 45%. 3407 Studies were performed to compare the sensitivity of purified Gln5"-FVa with that of normal FVa to inactivation by APC and to determine if these sensitivities were markedly different for thrombin-activated versus FXa-activated FVa species. For these experiments, normal and variant purified FV were separately activated either by FXa or by thrombin. The time courses for maximal activation were similar in each case (data not shown). Each of the various species of FVa was mixed withvarying amounts of APC (0 to 1.33 nmol/L). Inactivation of normal and Gln5%-FVa thatoccurred during 3 minutes of incubation was quantitated by measuring the residual FVa activity using a purified prothrombinase assay (Fig 1). Under the conditions used, thrombin-activated normal FVa was inactivated by APC with the same dose response as FXa-activated normal FVa (Fig 1, lower curves). In comparison to normal ArgS"-FVa,both thrombin-activated and FXa-activated Gln5"-FVa were relatively resistant to APC, with the apparent sensitivity to APC of the variant FVa species approximately 10-fold less than the normal FVa species (Fig 1). Moreover, Gln5%-FVaactivated by thrombin was indistinguishable from Gln'"-FVa activated by FXa in its relative resistance to APC.To compare further the relative sensitivities of each FVa to APC, the time course of APC inactivation was examined at two doses of APC (Fig 2). At 100 pmol/L APC, 20% to 25% inactivation of Gln5"-FVa was observed within 30 minutes of incubation, whereas a similar extent of inactivation of normal FVa was observed within approximately 2 to 3 minutes (Fig 2, left panel). The time for 50% inactivation of normal FVa by 100 pmoVL APC was 4 to 7 minutes, whereas for 50% inactivation of Gln'"-FVa it was 8 minutes for 800 pmol/L APC (Fig 2, right panel). These comparisons suggest that, under the conditions of these experiments, GlnSo6-FVais approximately 8- to 10-fold less susceptible than normal FVato APC inactivation. At 800 p m o m APC, 80% inactivation of Gln5%-FVa was observed within 30 minutes, with a similar extent of inactivation of normalFVa within about 5 minutes (Fig 2, right panel). These results were independent of whether the Gln5"FVa or normal FVa had been generated by thrombin or by FXa. In other experiments with longer times and higher APC concentrations, greater than 90% inactivation of Glns"-FVa was observed. To compare the proteolytic fragments of normal and variant FVa produced by APC during inactivation, cleavage of the heavy chains of Glns"-FVa and normal FVa was monitored by immunoblotting using a polyclonal antibody against the human FVa heavy chain (Fig 3). The first heavy chain fragments observed during incubation of normal FVa with APC were of apparent molecular mass 76 and 30 kD (Fig 3 and data not shown), suggesting initial cleavage at Arg'" as reported by Kalafatis et al.23 Subsequent appearance of a fragment of approximately 44 k D , the size of a polypeptide containing residues 1-306, was consistent with a secondary cleavage at Arg3%in normal FVa, in agreement with previous work.23Generation of the fragment containing residues 1-306 would also be associated with release of a 30-kD fragment corresponding to residues 307-506, and indeed a HEEB ET AL 3408 110 - .? I' Gln50B-FVa(FIla-activated) \ -0 \ \ "Q.. . .. .... . \ 90 ~ .. 70 "" Gln50B-FVa(FXa-activated) 50 FVa(Flla-activated) 30 FVa( FXa-act ivat ed) 10 0 0.33 0.67 APC, nM 1 .o 1.33 Fig 1. Inactivation of thrombin-activated and FXa-activated FVa and Glnm-Na as a function of APC concentration. Various APC concentrations as indicated were incubated with phospholipids and normal or variant N a (200 pmollLl for 3 minutes. The mixtures were then assayed for residual FVa activity using prothrombinase assays as described in Materials and Methods. tion was shown to cosegregate withriskof thrombosis in 30-kD doublet was observed on this and other blots (data familial APC re~istance.'""'.'~ Toshow that this DNA defect not shown). Because the 30-kD banddid not increase in is indeed the direct biochemical cause ofAPC resistance, intensity after 3 minutes, it is possible that the original 30we purified FV from plasma of a subject homozygous for kD fragment probably corresponding to residues 507-709 was further cleaved by APC at residue 679, as reported.'.' Gln'"-FV. Coagulation studies (Table I ) show that purified However, no fragments smaller than 30 kD were observed GldDh-FVimparts to plasma resistance to APC. We previously reported experiments suggesting that with the particular anti-heavy chain antibodies used in this thrombin-activated Glns"-FVa is relatively resistant to study. APC";in contrast. others suggested that FXa-activated In contrast to the results for normal FVa, the fragments Gld"-FVa, but not thrombin-activated Glns"-FVa, is resisthat appeared upon incubation of Gln"'"-FVa with APC were tant to APC." Studies described here show that Gln'"-FVa at approximately 44 and 58 kD, consistent with a single cleavage at Arg"" (Fig 3). To identify the site of phosphoconveys APC resistance to plasma and that Glns'K-FVa is relatively resistant toAPC independent of whetherthe lipid-dependent cleavage of Gld"-FVa by APC, the heavy chain fragments of 44 kD and 58 kD were sequenced. The Glns"-FVa is generated by thrombin or by FXa, thusclarifying this important conceptual conflict. 44-kD fragment had the expected NH,-terminal sequence of residues 1-9 of FV, Lys-Gln-Leu-Thr-Gln-Phe-Tyr-Val- The molecular defect responsible for APC resistance was Ala-. The 58-kD fragment had the sequence X-Leu-Lysinitially hypothesized to involve a new APC cofactor I1 defiLys-He-X-Arg-, corresponding to the expected sequence of cit"; subsequently, it was suggested to involvedefective APC residues 307-3 13, Asn-Leu-Lys-Lys-Ile-Thr-Arg-. Because cofactor activity of FV in APC-resistant patients.2sThe incleavage at Arg'" of normal FVa is known to be phosphofluence of the concentration of normal or variant FV added to lipid dependent? Gln"-FVa was treated with 700 pmol/L FV-deficient plasma onthe response to APC wasdetermined APC in the absence of phospholipid for 90 minutes.No using APTT and FXa-I -stage assays, and the results showed inactivation (S10%) was observed and no heavy chain fragthat the APC resistance ratios are insensitive to FV concenmentation was observed on immunoblots. In contrast, in the tration. Because increasing the amounts of FV does not imabsence of phospholipids, -25% inactivation of normal FVa prove the APC resistance ratio, ie, apparently does not enwas observed in 3 minutes, with no further loss of activity hance APC activity, these findings do not support the observed in 90 minutes (data not shown). These observations hypothesis that single-chain normal FV or GlnsM-FV can act are consistent with inactivation of Glns"-FVa via phosphoas a significant cofactor for APC anticoagulant activity in lipid-dependent cleavage at Arg'". plasma under typical conditions of the clotting assays used. Studies in which purified Gln'"-FVa was added to FVDISCUSSION deficient plasma consistently gave APC resistance ratios suggesting that GlnsOh-FVawas not insusgreater than 1 .W, APC resistance has been associated with a DNA mutation ceptible toAPC. In studies usingpurified proteins, dosecausing replacement of Arg'"" by Gln in F V , and this muta- APCRESISTANCE AND PURIFIED GLN~-FACTOR V 3409 [APC] =800pM [APC] =l OOpM 100 I ................................................... , A * 3 A\ Ita-activated Arg-FVa .;. ................ .9.t!a-activated GIMV~ . . . . . 80 *Xa-activated Arg-FVa \\ 'p\ Q:\ A-Xa-activated Gln-FVa ......,\ ........................................... 60 *. 40 20 0 0 10 20 30 0 10 20 30 TIME, min TIME, min Fig 2. Time course of inactivation of thrombin-activated andFXa-activated normal FVa and Gin*-FVa. Normal or variantFVa (200 pmol/ L) was incubatedwith APC and phospholipids. At various timesas indicated, aliquots were removed and assayed for residual FVa prothrombinase activity as described in Materials and Methods. For the left panel, APC concentration was100 pmol/L. For the rightpanel, APC concentration was800 pmol/L. ( 0 )Thrombin-activated normalFVa, [A)FXa-activated normal FVa, ( 0 )thrombin-activated Glnm-FVa, (A) FXa-activated GlnmFVa. response studies and time course studies at different concentrations of APC (Figs 1 and 2 ) confirmed that purified Gln'"FVa is not completely resistant to APC and suggested that the variant Glr?"-FVa is approximately IO-fold less sensitive to APC than is normal FVa. These findings imply that the inactivation of Glns"-FVa by APC can occur in vivo, albeit at a reduced rate compared withnormalFVa. This implication may help explain why APC resistance appears tobe a rather mildrisk factor for venous thrombosis and why a combination of genetic risk factors for venous thrombosis is found in a significant fraction of symptomatic patients.7.~n.?4.?~.~9 The APC-dependent cleavage patterns for the FVa heavy chains of normal FVa and GlnS"-FVa were compared using immunoblotting. The observed time-dependent cleavage patterns for normal FVa were consistent with a report showing that inactivation of normal FVa involves an initial cleavage at Arg'" followed by a phospholipid-dependent cleavage at FVa Gln506=FVa I Std. I1 t = 60 3 60 126 '60 3 30 60 Fig 3. lmmunoblot of FVa and Gln=-FVa heavy chains after APC inactivation. Normal RI or GlnSOBFV were each activated with thrombin and then incubated at 5 nmol/L with APC (350 pmol/L) and phospholipidslCa". Atthetimes indicated, aliquots containing 60 n g of FVa wereremovedand subjected t o boiling, SDS-PAGE, and immunoblotting for FVa heavy chain epitopes as indicated in Materials and Methods. FVa activity assays performed in parallel indicated thatGln5w-FVawas greater than 80% inactivated at 120 minutes and that normal FVa was greater than 90% inactivated at 60 minutes. min. -200 Mr x 103 765844- 30APC- I + + + - + + + HEEB ET AL 3410 Arg306.23 Incontrast to the pattern for normal FVa, inactivation of Gln506-FVaby AFT was associated with appearance of polypeptide fragments of approximately 44 and 58 kD (Fig 3 ) because of cleavage at Arg306,as confirmed by NH2terminal amino acid sequencing. These results show that cleavage by APC at Arg306in FVa is sufficient to inactivate FVa, but that this cleavage is inefficient, approximately 10 times slower, unless prior cleavage at kgso6occurs. Baboon studies suggest that FVa rather than FV is the physiologic substrate for APC. APC at antithrombotic levels of 6 and 30 nmoYL circulating in vivo for up to 1 hour in baboons did not significantly decrease FV or FVIII levels even though the AFTT was very markedly prolonged, eg, 36 to 169 seconds at 30 nmoYL In contrast, when thrombin was infused at 2 U/kg/min into baboons for 1 hour, levels of FV and FVIII decreased significantly (40% to 60%).31Infused thrombin activates FV and FVIII to FVa and FVIIIa, increases the level of circulating APC to -7 nmol/L, and prolongs the APlT (eg, 32 to 158 seconds at 2 U thr~mbin/kg/h).~~ Compared with normal FVa, GlnSMFVa has a relatively reduced rate of inactivation by APC in the presence of phospholipids. The fact that Arg506Gln mutation is clearly associated with increased risk of thrombosis6-12.24 and that cleavage of GlnSM-FVby APC is similar to that of normal F V 3 ’ (Heeb, Kojima, and Griffin, unpublished data) further supports the concept that FVa rather than FV is the physiologic target of A P C . After this report was submitted, Kalafatis et a13’ reported biochemical studies that are related to this study and that complement the coagulation experiments presented here. Using purified component prothrombinase assays with the fluorescent thrombin inhibitor DAPA, it was shown3’ that purified thrombin-activated Gln5”-FVa was inactivated by APC by cleavage at ,g3% at a rate slower than that of normal FVa that was cleaved at ArgM, and Arg306. ACKNOWLEDGMENT We are very grateful for skilled technical assistance of Marissa Maley and Yolanda Montejano and for DNA analyses for the FT Arg506Gln mutation performed by Xiao Xu. We appreciate the ELISA data provided by Dr JosC Fernhdez and the gift of anti-FT antibodies provided byDrs Jan Rosing, Guido Tans, andHarry Bakker. REFERENCES 1. Griffin JH, Evatt B, Zimmerman TS, Kleiss AJ, Wideman C: Deficiency of protein C in congenital thrombotic disease. J Clin Invest 68:1370, 1981 2. Schwarz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH: Plasma protein S deficiency in familial thrombotic disease. Blood 64:1297, 1984 3. Comp PC, Nixon R R , Esmon C T Determination of functional levels of protein C, an antithrombotic protein, using thrombin-thrombomodulin complex. Blood 63:15, 1984 4. Branson HE, Katz J, Marble R, Griffin JH: Inherited protein C deficiency and a coumarin-responsive chronic relapsing purpura fulminans syndrome in a neonate. Lancet 2:1165, 1983 5. Mahasanha C, Suvatte V, Marlar RA, Manco-Johnson MJ, Jacobson LJ, Hathaway WE: Neonatal purpura fulminans associated with homozygous protein S deficiency (letter). Lancet 335:61, 1990 6. Dahlback B, Carlsson M, Svensson PJ: Familial thrombophilia due to a previously unrecognized mechanism characterized by poor anticoagulant response to activated protein C: Prediction of a cofactor to activated protein C. Proc Natl Acad Sci USA 90:1004, 1993 7. Dahlback B: Inherited thrombophilia: Resistance of activated protein C as a pathogenic factor of venous thromboembolism. Blood 85:607, 1995 8. Griffin JH, Evatt B, Wideman C, Fernbdez JA: Anticoagulant protein C pathway defective in majority of thrornbophilic patients. Blood 821989, 1993 9. Koster T, Rosendaal FR, deRonde H, Briet E, Vandenbroucke JP, Bertina R: Venous thrombosis due topoor anticoagulant response to activated protein C: Leiden thrombophilia study. Lancet 342: 1503, 1993 10. Svensson PJ, Dahlback B: Resistance to activated protein C as a basis for venous thrombosis. N Engl J Med 330:517, 1994 11. Halbmayer W-M, Haushofer A, Schon R, Fischer M: The prevalence of poor anticoagulant response to activated proteinC (APC resistance) among patients suffering from stroke or venous thrombosis and among healthy subjects. Blood Coag Fibrinol 551, 1994 12. Cadroy Y, Sie P, Boneu B: Frequency of a defective response to activated protein C inpatients with a history of venous thrombosis. Blood 83:2008, 1994 13. Bertina R M , Koeleman BPC, Koster T, Rosendaal FR, Dirven RJ, de Ronde H, van der Velden PA, Reitsma PH: Mutation in blood coagulation factor V associated with resistance to activated protein C. Nature 36964, 1994 14. Greengard JS, Sun X, Xu X, Fernbdez JA, Griffin JH, Evatt B: Activated protein C resistance caused by Arg506Gln mutation in factor Va. Lancet 343:1361, 1994 15. Voorberg 3, Roelse J, Koopman R, Buller H, Berends F, ten Cate JW, Mertens K, van Mourik JA: Association of idiopathic venous thromboembolism with single point-mutation at A$” of factor V. Lancet 343:1535, 1994 16. Sun X, Evatt B, Griffin JH: Blood coagulation factor Va abnormality associated with resistance to activated protein C in venous thrombophilia. Blood 83:3120, 1994 17. Francis RT, Seyfert U: Rapid amidolytic assay of protein C in whole plasma using an activator from the venom of Agkistrodon contrortrix. Am J Clin Pathol 87:619, 1987 18. Stenflo J: A new vitamin K-dependent protein. J Biol Chem 251:355, 1976 19. Tans G, Rosing J, Thomassen MC, Heeb MJ, Zwaal RFA, Griffin JH: Comparison of anticoagulant and procoagulant activities of stimulated platelets and platelet-derived rnicroparticles. Blood 77:2641, 1991 20. Griffin JH, Gruber A, Fernandez JA: Reevaluation of total, free, and bound protein S and C4b-binding protein levels in plasma anticoagulated with citrate or hirudin. Blood 79:3203, 1992 21. Heeb MJ, Mesters RM, Tans G, Rosing J, Griffin JH: Binding of protein S to factor Va associated with inhibition of prothrombinase that is independent of activated protein C. J Biol Chem 268:2872, 1993 22. Heeb MJ, Espaila F, Griffin JH: Inhibition and complexation of activated protein Cby two major inhibitors in plasma. Blood 73:446, 1989 23. Kalafatis M, Rand MD, Mann KG: The mechanism of inactivation of human factor V and human factor Va by activated protein C. J Biol Chem 269:31869, 1994 24. a l l e r B, Svensson PJ, He X, Dahlback B: Identification of the same factor V gene mutation in 47 out of 50 thrombosis-prone families with inherited resistance to activated protein C. J Clin Invest 942521, 1994 APC RESISTANCE AND PURIFIED GLN~-FACTORV 25. DahlWck B, Hildebrand B: Inherited resistance to activated protein C is corrected by anticoagulant cofactor activity found be to a property of factor V. Proc Natl Acad Sci USA 91:13%, 1994 26. Greengard JS, Eichinger S , Griffin JH, Bauer KA: Brief report: Variability ofthrombosisamonghomozygous siblings with resistance to activated protein C duean toArg-Gln mutation in the gene for factor V. N Engl J Med 331:1559, 1994 27. Koeleman BPC, Reitsma PH, Allaart CF, Bertina RM: Activated protein C resistance as an additional risk factorfor thrombosis in protein C-deficient families. Blood 84:1031, 1994 28. Vandenbroucke JP, Koster T, Briet E, Reitsma PH, Bertina R M , Rosendaal FR: Increased risk of venous thrombosis in oralcontraceptive users who are caniers of factor V Leiden mutation. Lancet 3M1453, 1994 29. Gandrille S , Greengard JS,Alhenc-Gelas M, Juhan-Vague I, 341 1 Abgrall JF, Jude B, Griffin JH, Aiach M, and the French Network on the behalf of INSERM: Molecular abnormalities responsible for protein C and protein S deficiencies: Incidence of activated protein C resistance dueto the ARG 405 GLN mutation in factor V in 1 13 unrelated symptomatic protein C deficient patients. Blood (in press) 30. Gruber A, Hanson SR, Kelly AB, Yan BS, Bang N, Griffin JH, Harker LA: Inhibition of thrombus formation by activated recombinant protein C in a primate model of arterial thrombosis. Circulation 82578, 1990 31. Hanson SR. Griffin JH, Harker LA, Kelly AB, Esmon C T , Gruber A: Antithrombotic effects of thrombin-induced activation of endogenous protein C in primates. J Clin Invest 92:2003, 1993 32. Kalafatis M, BertinaRM, Rand MD, Mann K G Characterization of the molecular defectin factor V-. J Biol Chem2704053, 1995
© Copyright 2024 Paperzz