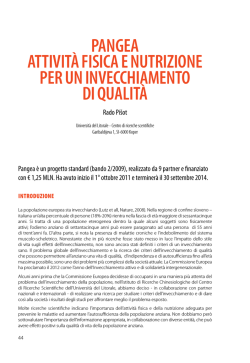
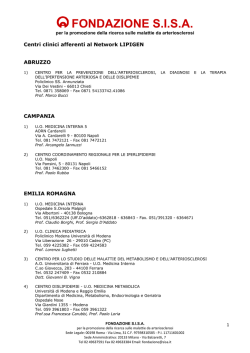
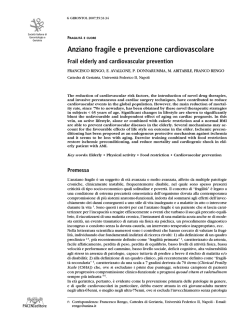
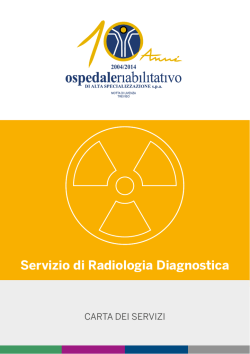
Intern Emerg Med DOI 10.1007/s11739-014-1124-1 IM - REVIEW Multimorbidity and polypharmacy in the elderly: lessons from REPOSI Pier Mannuccio Mannucci • Alessandro Nobili REPOSI Investigators • Received: 1 July 2014 / Accepted: 20 August 2014 Ó SIMI 2014 Abstract The dramatic demographic changes that are occurring in the third millennium are modifying the mission of generalist professionals such as primary care physicians and internists. Multiple chronic diseases and the related prescription of multiple medications are becoming typical problems and present many challenges. Unfortunately, the available evidence regarding the efficacy of medications has been generated by clinical trials involving patients completely different from those currently admitted to internal medicine: much younger, affected by a single disease and managed in a highly controlled research environment. Because only registries can provide information on drug effectiveness in real-life conditions, REPOSI started in 2008 with the goal of acquiring data on elderly people acutely admitted to medical or geriatric hospital wards in Italy. The main goals of the registry were to evaluate drug prescription appropriateness, the relationship between multimorbidity/polypharmacy and such cogent outcomes as hospital mortality and re-hospitalization, and the identification of disease clusters that most often concomitantly occur in the elderly. The findings of 3-yearly REPOSI runs (2008, 2010, 2012) suggest the following pertinent tasks for the internist in order to REPOSI denotes the REgistro POliterapie SIMI, Societa` Italiana di Medicina Interna. The participating units and co-authors are listed in the Appendix. P. M. Mannucci (&) Scientific Direction, IRCCS Foundation Maggiore Hospital Policlinico, Via Francesco Sforza 28, 20122 Milan, Italy e-mail: [email protected] A. Nobili Department of Neuroscience, IRCCS Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy optimally handle their elderly patients: the management of multiple medications, the need to become acquainted with geriatric multidimensional tools, the promotion and implementation of a multidisciplinary team approach to patient health and care and the corresponding involvement of patients and their relatives and caregivers. There is also a need for more research, tailored to the peculiar features of the multimorbid elderly patient. Keywords Multimorbidity Polypharmacy Aging Drug prescription Multidimensional evaluation Adverse drug effects Introduction Elderly people with multimorbidity will number around 75 million people in 2050 in Europe, representing more than 10 % of the entire population [1, 2]. The president of the Italian Society of Internal Medicine (SIMI) [3] has recently emphasized a new mission for the internist of the third millennium, triggered by the shift from the care of diseases occurring in relatively young people, and mainly affecting a single organ or system to that of multiple chronic diseases in the elderly, with the related need for polypharmacy. Because of this evolving epidemiological picture, SIMI chose to initiate in 2007 a collaboration with the IRCCS Mario Negri Institute for Pharmacological Research of Milan and IRCCS Ca’ Granda Foundation of Milan, with the broad goal of collecting information on the clinical characteristics and patterns of drug prescription in people older than 65 years of age admitted to internal medicine and geriatric hospital wards run by SIMI constituents. The strategy chosen to achieve this goal was a prospective, non-interventional, multicenter 123 Intern Emerg Med Background and issues Fig. 1 Organization of REPOSI. Asterisk means available form 2010; double asterisk available from 2012 registry (REPOSI, i.e., REgistro POliterapie SIMI), designed to collect a set of clinical and laboratory data on elderly patients consecutively hospitalized during 4 index weeks (one for each season) in 3 years (2008, 2010 and 2012). The data set contained sociodemographic features, diagnosis on hospital admission and at discharge, comorbidities and intercurrent clinical and pharmacological adverse events. Moreover, the number and types of drugs prescribed on admission and discharge were recorded. After discharge, additional follow-up data were collected via telephone calls at 3 and 12 months (Fig. 1 shows the main steps of REPOSI). Figure 2 shows the flowchart of the 4,035 cases included so far (2008–2010–2012) by 95 medical or geriatric wards from all over Italy, while Table 1 shows the main characteristics of enrolled patients, who are an accurate and actual picture of the ill people admitted to hospital wards of internal medicine and geriatrics. Their average age was close to 80 years; nearly half of them had some degree of dependence and a prolonged hospital stay after resolution of the cause for acute admission. Not unexpectedly, they took multiple medications. In the next sections of this article we shall outline again the main issues related to the management of the oldest adult which led SIMI, Mario Negri and Maggiore Hospital to conceive and implement REPOSI, the main data so far obtained in the frame of this registry, what we have learned, and why the findings prompt some challenges and changes pertaining to research and clinical practice for the internist. 123 In Europe, people aged 80 years or more are the fastest growing group, so that by 2060 they will be nearly 20 % of the population [2]. This dramatic increase in life expectancy is a monument to the progress of medical sciences, improvement in life styles, availability of innovative drugs and implementation of the welfare state. However, successful aging is a formidable challenge for those responsible for healthcare strategies and the implementation of the welfare state, with implications on labor markets, social programs and family dynamics. For instance, a source of great concern is the growing unbalance between the oldest old and the still active citizens who must sustain the societal burden of the latter. This unbalance is epitomized by the progressive decrease of an index such as the ratio of the number of active people between 40 and 60 years of age to those aged 85 years or older. This ratio, as high as 31 in 1974, decreased to 14 in 2010, and is expected to be as low as 5 in 2030 [4], also owing to the lowering birth rate, particularly in high-income countries. Aging is inevitably characterized by a multiplicity of apparently independent chronic diseases in the same person. Multimorbidity must be distinguished from comorbidity, which defines clinical manifestations stemming as complications of the clinical course of a clearly identified index disease. In Italy, the prevalence of chronic diseases has reached in 2012 the impressive rate of 38 % in those aged more than 65 years, with values of 50 % at ages 75–85 and 64 % beyond 85 years [5]. Multimorbidity is almost always accompanied by polypharmacy, the most widely accepted definition of this situation pertaining to the daily intake of five or more drugs [6]. According to the Geriatrics Working Group of AIFA (Agenzia Italiana del Farmaco), 1.3 million elderly Italians take more than 10 daily drugs, with the age group between 75 and 84 years recording the highest intake: 55 % take between five and nine drugs per day, 14 % take ten or more [7]. In terms of expenditures, the older citizens absorb 60 % (15.7 billion Euros) of the total cost of drugs (26.3 billions) [8]. Why is polypharmacy so widespread? Because physicians tend to follow the guidelines available for each of the multiple diseases that affect the elderly, and hence prescribe all the drugs recommended for each disease. Unfortunately, guidelines hardly take into account multimorbidity and polypharmacy, and clinical trials, i.e., the basis for drug prescription according to evidence-based medicine, usually enroll patients completely different from the elderly: relative young, and highly selected for having only the disease that is expected to benefit from the drug under investigation [9]. Clinical trials do investigate a disease, not the individual patient. Hence, they provide evidence on efficacy, i.e., the extent to which a drug Intern Emerg Med Fig. 2 Flow-chart of the cohort of 4,035 patients enrolled in REPOSI. 1 Low quality of data, 2 follow-up not requested, 3 only for REPOSI 2012, 4 ten wards were unavailable for 12-month follow-up produces a beneficial effect under ideal conditions, but fail to provide evidence on effectiveness under real-life circumstances [9, 10]. Polypharmacy is a formidable problem, with a number of negative implications that are listed in Table 2. Because 20–65 % of the oldest adults take potentially inappropriate medications, they are at an increased risk of adverse reactions and hence of repeated visits to the hospital emergency department (ED), admissions and readmissions and deaths [11–13]. Some of these drugs may adversely affect the course of a coexisting disease: a situation called therapeutic competition, which occurs in at least one-fifth of the older patients receiving multiple medications [14]. Commonly, complications and symptoms due to inappropriate drug intake are interpreted as the onset of new conditions or diseases, that are often tackled adding more drugs to the already existing burden (the so-called prescribing cascade) [15]. Moreover, prescribing errors, an important cause of harm to patients, are much more likely to occur when a greater total number of drugs are prescribed [16, 17]. A crucial aspect of appropriate drug prescription is the need to bolster a patient-centered instead of the current disease-focused approach, because the latter inevitably leads to fragmentation in the management of the multimorbidity of the elderly by various specialists, and to the inappropriate use of healthcare facilities. Centeredness implies the engagement of older people, their relatives and caregivers about options and values of treatments. Patients’ feelings and beliefs about their health, medical conditions and treatment options are key determinants of whether or not they will comply with the recommended medications. The issue of adherence clearly highlights the importance of consideration and in-depth discussion of preferences, in general and particularly pertaining to the multimorbid elderly people who use multiple drugs [18]. Many studies 123 Intern Emerg Med Table 1 Main characteristics of 4,035 patients enrolled in the REPOSI Registry Cohort characteristics REPOSI 2008 REPOSI 2010 REPOSI 2012 Number (N) of patients enrolled 1,332 1,380 1,323 Females, N (%) 721 (54.1) 696 (50.4) 672 (50.8) Age (years), mean (SD) 79.3 (7.5) 79.0 (7.3) 79.3 (7.4) 65–74 409 (30.7) 430 (31.2) 403 (30.5) 75–84 607 (45.6) 650 (47.1) 583 (44.1) C85 316 (23.7) 300 (21.7) 337 (25.5) Need of caregivers, N (%) – 772 (56.5) 689 (52.1) Number of diagnoses at admission, mean (SD) 4.3 (2.3) 5.8 (2.8) 5.7 (2.8) Patients at admission with five or more diagnoses, N (%) 571 (42.9) 884 (64.1) 839 (63.4) Number of drugs at admission, mean (SD) Patients at admission taking five or more drugs, N (%) 4.9 (2.8) 689 (51.7) 5.3 (2.8) 805 (58.3) 5.4 (3.1) 778 (58.8) Severity index at admissiona, mean (SD) – 1.6 (0.3) 1.7 (0.3) Age class, N (%) a Comorbidity index at admission , mean (SD) – 2.9 (1.7) 3.1 (1.9) Patients with Barthel index at admissionab – – 1,289 (94.4) Barthel index at admission, mean (SD) – – 78.5 (29.2) Complete dependence (0–24) – – 124 (9.6) Severe dependence (25–49) – – 86 (6.7) Moderate dependence (50–74) – – 167 (13.0 Mild dependence (75–90) – – 200 (15.5) Groups according to Barthel index at admission, N (%) – – 712 (55.2) Patients with Barthel index at hospital staya, N (%) No or negligible dependence (90–100) – 1,362 (98.7) 1,264 (95.5) Barthel index at hospital stay, mean (SD) – 76.8 (30.7) 72.6 (32.4) Complete dependence (0–24) – 155 (11.4) 169 (13.4) Severe dependence (25–49) Moderate dependence (50–74) – – 111 (8.2) 150 (11.0) 126 (10.0) 175 (13.8) Mild dependence (75–90) – 211 (15.5) 200 (15.8) Groups according to Barthel index at hospital stay, N (%) No or negligible dependence (90–100) – 735 (54.0) 594 (47.0) Patients with Short Blessed Testa, N (%) – 1,339 (97.0) 1,217 (92.0) Short Blessed Test, mean (SD) – 9.9 (8.2) 9.2 (7.8) Short Blessed Test, severe (10–28), N (%) – 637 (47.6) 541 (44.5) Patients with Geriatric Depression Scalea, N (%) – 1,295 (93.8) 1,121 (84.7) Geriatric Depression Scale, mean (SD) – 1.4 (1.2) 1.4 (1.2) Dead, N (%) 66 (5.0) 50 (3.6) 42 (3.0) 1,159 (87.6) Patients discharged, N (%) 1,155 (86.7) 1,159 (84.0) Number of diagnosis at discharge, mean (SD) 5.9 (2.5) 6.5 (3.0) 6.3 (2.8) Patients at discharge with five or more diagnosis, N (%) 796 (68.9) 857 (73.94) 834 (72.0) Number of drugs at discharge mean (SD) 6.0 (2.9) 6.3 (2.8) 6.4 (3.1) Patients at discharge taking five or more drugs, N (%) 770 (66.7) 838 (72.3) 838 (72.3) Severity index at discharge, mean (SD) Comorbidity index at discharge, mean (SD) – – 1.7 (0.3) 3.0 (1.8) 1.7 (0.3) 3.2 (2.0) Hospital stay days, mean (SD) 11.1 (8.5) 10.9 (8.2) 11.4 (8.5) Pts patients a Data not collected in 2008 b Data not collected in 2010 123 Intern Emerg Med Table 2 Main risks related to polypharmacy Adverse drug reactions and interactions Exposure to potentially inappropriate medications Under-prescribing of recommended drugs (‘‘treatment risk paradox’’) Medication errors Poor adherence Cognitive and functional decline Occurrence of geriatric syndromes (delirium, falls, incontinence, behavioral disturbances, malnutrition, etc.) More institutionalization various stakeholders (family doctors, pharmacists, relatives, caregivers, and, most importantly, the patients themselves). A simple approach to drug review is that of asking some questions, listed as examples in Table 3. Furthermore, one can choose among several available tools that help to improve drug prescription, after having chosen the most suitable for the actual patient [23, 24]. All in all, prescription criteria based upon guidelines and evidence-based medicine are likely to often be inadequate in the complex patient admitted to internal medicine wards in the third millennium, as we shall see in the next sections. Higher mortality Greater costs Main REPOSI findings and their clinical relevance Table 3 Basic questions for medication review 1. Has a full medication history been collected? 2. How long ago has the latter been reviewed? 3. Are all drugs taken by the patient indicated and likely to be effective? 4. Is the patient taking any inappropriate or incompatible medication? 5. Are there actual drug(s) that could be discontinued? Are there essential drugs that are not actually prescribed? 6. Are the dosage, dose frequency and formulation appropriate? 7. Is the patient at high risk of therapeutic competition? 8. Are drug interactions present? 9. Is the patient compliant with medications? have demonstrated that patients’ values related to their healthcare vary enormously, and differ significantly from those of their physicians, relatives and caregivers [19]. Elderly people are often over-treated, because many drugs provide at best a marginal effect in clinical outcomes that truly matter. For example, anti-hypertension drugs are perhaps used too widely, because after the age of 80 years high blood pressure is not a prominent risk factor for stroke [20]. On the other hand, anti-hypertension drugs may cause hypotension, with the associated risk of falls in the frail elderly. By the same token, statins have a modest role in cardiovascular prevention, but may cause musculoskeletal pain that facilitates falls [20] and reduces physical activity in elderly people [21]. Hence, an important task for the internist and other generalist medical professionals who take care of the elderly (geriatricians, primary care physicians) is to critically review at regular intervals which drugs are really needed for optimal patient benefit, and to consider the option of deprescribing some drugs. On the other hand, in some instances polypharmacy may lead to lack of prescription of essential medications (the so-called treatment risk paradox) [22]. Medication revision should involve the The pattern of results obtained in the frame of the first 3-yearly runs of the registry (2008, 2010, 2012) can be broadly divided into those pertaining to the appropriateness of drug prescription; and those on the relationship between multimorbidity/polypharmacy and such outcomes as mortality in hospital, and soon after discharge, as well as rates of hospital readmission. Other results pertain to the identification of the disease clusters that more often concomitantly occur in the elderly, their consistency over different REPOSI runs, as well as the relationship between disease clusters and clinical outcomes. Appropriateness of drug prescription Polypharmacy is inherently associated with a high risk of inappropriate prescription. For instance, in 6 different European countries inappropriate drug prescriptions ranged from 22 to 77 % of hospitalized cases [25]. Pertaining to the consequences of inadequate prescription, drug-related adverse events are among the first five causes of in-hospital death, admission to emergency departments and hospitalization [26, 27]. With this background, prescription appropriateness was first tackled in REPOSI with reference to the following frequently used medications: antithrombotic prophylaxis in atrial fibrillation and bedridden medical patients [28–30], proton pump inhibitors [31], antidepressants [32] and drugs with anticholinergic effects [33]. Collectively, these studies did show a high degree of inappropriate prescription, not only at the time of hospital admission (reflecting the prescriptions of general practitioners as well as patient adherence), but also at discharge (reflecting the actual prescription of such specialists as hospital internists and geriatricians). For instance, among elderly patients with chronic atrial fibrillation, as many as 26 % at admission and 32 % at discharge were taking no antithrombotic drug despite their high risk of cardioembolism, and 44 and 41 % were on inappropriate thromboprophylaxis according to the risk of embolism dictated by 123 Intern Emerg Med the CHADS2 and related scores [28]. Even though in these patients the cardioembolic risk was higher than the bleeding risk, results of the bleeding scores led to the preferential use of aspirin rather than warfarin [30]. In the oldest old with atrial fibrillation, aspirin is not only ineffective in the prevention of thromboembolic stroke, it carries a risk of bleeding no smaller than that of warfarin [34]. By the same token, only 15 % of patients received pharmacological thromboprophylaxis with low molecular weight heparins or fondaparinux, because the risk of bleeding was deemed to be more alarming than that of venous thromboembolism, notwithstanding that these patients were multimorbid and often bedridden [30]. Furthermore, inappropriate prescription of proton pump inhibitors, very high at admission (62 %), remained equally high at discharge (63 %). The main reason for inappropriate prescription was that many other drugs were concomitantly prescribed [31], in spite of the fact that the prophylactic efficacy of proton pump inhibitors is not proven in the absence of gastrointestinal ailments. Proton pump inhibitors are not free of side effects particularly relevant for the elderly, such as osteoporosis, Clostridium difficile infections, hypomagnesaemia and pneumonia [35]. Overprescription was also observed for drugs used to manage depression, because at hospital discharge, 24 % of patients were recommended to use them in spite of the fact that there was little evidence of depression [32]. It is known that drugs with anticholinergic effects are associated in the elderly with a high risk of such adverse events as cognitive and psychomotor impairment, delirium, falls, unintentional injuries and loss of independence. In the frame of REPOSI, the use of these drugs was indeed associated with worse cognitive and functional performance [33]. Antidepressant and antipsychotic drugs, often inappropriately prescribed in the elderly, are endowed with strong anticholinergic effects. decreased the rate of inappropriateness, perhaps because both versions deal with several drugs not widely used in Europe [39]. Another important clinical outcome tackled in REPOSI was early re-hospitalization (the so-called phenomenon of the revolving door), which occurred in 19 % of patients within 3 months after discharge, and was most frequently associated with previous hospital admissions, adverse events causing hospitalization, and diagnoses of vascular and liver disease [40]. Finally, the search for simple prognostic markers of clinical significance did show that a severely reduced glomerular filtration rate was associated with a threefold increased risk of in-hospital mortality and a 2.6-fold increased risk of dying within 3 months after discharge [41]. Cluster analysis There is still poor knowledge on how and why multiple diseases concomitantly occur in the elderly. Cluster analysis is a statistical technique that allows the identification of groups of diseases (clusters) that concomitantly occur apparently by chance [42]. In REPOSI, the hypothesis underlying the use of this analysis was that knowledge about the more frequent clusters of diseases may help in the development of strategies to design cluster-randomized drug trials. The main clusters were those including heart failure and either chronic renal failure or chronic obstructive pulmonary disease, which are associated with a 3- to 4-fold increased risk of in-hospital death and adverse clinical events during hospitalization [42]. Heart failure in various combinations with other ailments is also associated with the highest utilization of multiple drugs [43]. A comparison of the main disease clusters in the 2008 REPOSI run with those in 2010 did show that the pattern of co-occurring diseases was broadly similar [44], strengthening the views of disease associations other than by chance. Polypharmacy and clinical outcomes The expected high rate of polypharmacy at the time of admission (52 %), rather than decreasing due to the critical drug review made by expert hospital internists, dramatically increased at discharge (67 %) [36]. In terms of compatibility between the multiple drugs prescribed, 60 % of patients were exposed to at least one potential drug–drug interaction, of which at least one-fourth were potentially severe [37]. Elderly patients with more severe cognitive impairment were more likely to die during hospitalization and in the early post-discharge period [38]. REPOSI also evaluated whether or not the rate of appropriateness improved by applying the 2003 and 2012 updated versions of the Beers criteria for safer drug prescription in the elderly. There was no evidence that their applications 123 The role of REPOSI for research in internal medicine Research is vital to establish the best strategies of care, and is an important task for each clinician, because it helps to critically evaluate and improve clinical practice. In this context, REPOSI must be understood as a research tool that can be used by the internist to explore many aspects, questions and problems of their daily practice through a structured and standardized approach. The current publications stemming from REPOSI describe how this opportunity has been exploited so far. However, in the next few years, REPOSI should be able to propose new lines of research in patients with multimorbidity and polypharmacy. Some ideas might be summarized as follows: Intern Emerg Med – – – – – The implementation of REPOSI in a larger number of internal and geriatric wards, at national as well as international level, should help to better understand the characteristics, complexity and effects on relevant clinical outcomes of the current pattern of care provided to the hospitalized elderly. In the conclusive statements of the AIFA Geriatric Working Group, Bernabei et al. [7] emphasize the need to establish networks involving elderly patients studied with common assessment instruments and codified information on medication use. Wider adoption of REPOSI would help to meet this need, and to design pragmatic clinical trials in which, for instance, patients are randomized in relation to disease clusters to receive or not receive a specific treatment. There is an urgent need to start a new era of patientoriented trials, in which the clinical complexity of the elderly with multiple chronic diseases and polypharmacy is the paradigm, and clinical outcomes of intervention are shared with the patients taking into account their health priorities. In this context, risk stratification approaches may be useful methodological tools to individualize and prioritize treatments [45]. Comparing data of the REPOSI Registry to other data sets pertaining to the oldest adult could be used to set up studies of comparative effectiveness research [45], involving for instance patients selected according to clusters of the most representative combinations of chronic diseases, in order to evaluate benefits and harms of specific interventions, or innovative models of care on clinical outcomes truly patient relevant (such as, symptom burden, cognitive impairment, disability and active life expectancy). Availability of large patient samples is a prerequisite in order to be able to implement new approaches of data analysis meant to assess the complex connections of multiple chronic diseases. Network analysis represents a methodology applicable to different fields of research, ranging from molecular medicine to human, social and clinical setting [46]. Network analysis could also be applied to investigate the rationale of multiple drug prescription, thereby allowing the collection of information on the relationship between drugs and their coprescriptions, and how these patterns differ in different age and gender groups. N-of-1 trials [47, 48] are within-patient randomized multi-period crossover trials that compare, in a doubleblind fashion, therapeutic strategies (e.g., an active drug versus no treatments, or two different active therapies) using the actual patient as a control [49]. The ultimate aim of N-of-1 trials is to objectively and empirically determine the best therapeutic choice for a single patient. – Narrative medicine [50, 51] might be an additional tool in order to study a patient’s experience with cumulative illnesses, diagnostic and therapeutic burden and their real-life clinical encounters with different medical specialists. Narrative medicine bridges the gap between patients and providers, and teaches that the mode of care delivery (the process) is just as important as which type of care is delivered (the content). After having acquired narrative competence, physicians can join their patients, recognize their own personal journeys through medicine and illness, acknowledge kinship with and duties towards other health care providers, and inaugurate an interaction with the community at large on health care. A narrative medicine approach might also help to elucidate the rationale of therapeutic choices that have driven the current management of different illnesses in the absence of evidence-based information. What the internist has learnt from REPOSI In the third millennium, internists and geriatricians must acquire a leading role, together with primary care physicians, in order to make health care systems fit for the management of an aging population. Are we ready for this formidable task? Until now, medical schools and postgraduate education have trained physicians to manage single diseases in relatively young people. The success of modern medicine and the resulting increase of an aging population have utterly transformed this picture, but medical education and the resulting healthcare services have hardly succeeded in coping culturally and practically with this huge shift. Medical subspecialties (cardiology, pneumology, endocrinology, gastroenterology et alia), which were much fostered in the last part of the second millennium owing to the dramatic development of specialized technologies and procedures, are not suited to handle multiple concomitant diseases. The hospital internist, with an holistic approach to disease management, should in principle find it easier to tackle this challenge. 1. 2. A first most important goal is to critically review all prescribed drugs, both at the time of hospital admission and discharge. Setting therapeutic priorities and stopping inappropriate or useless medications favor compliance and quality of life in the elderly. Another important task is to become acquainted with the use of multidimensional evaluation tools that mainly belong to the clinical expertise of geriatricians. In the elderly, an impaired cognitive status and the decreased ability to perform the basic activities of 123 Intern Emerg Med 3. 4. 5. daily living are accompanied by a reduction of functional and physical reserves, that ultimately lead to frailty and a high risk of death. A prompt and timely recognition of this impairment is potentially able to improve prognosis, because the sequence of adverse outcomes is sometimes reversible. The traditional approach based upon clinical history and physical examination may be inadequate to pick up subtle impairments of cognitive and functional status, unless some instruments of the multidimensional evaluation are routinely used (such as the Mini-Mental State Examination [52], the Short Blessed Test [53] and the Barthel index on the basal activities of daily living [54]). A multidisciplinary team approach is essential to avoid care fragmentation, to provide a comprehensive evaluation of problems and needs, and to practice a combination of problem-based and patient-oriented medicine, i.e., a realistic personalized medicine. To this end, the internist needs to orchestrate a team involving nurses, pharmacists, social workers and clinical pharmacologists, the latter unfortunately often being lacking in the healthcare settings that handle the multimorbid and polytreated elderly. Communication and transparency between hospital and community care providers is essential in order to promote continuity and integration of care and reduce patient’s stress, redundancy, fragmentation and costs. Coordination, integration and continuity of care means a realistic assessment of available resources and social/ health services, with inevitable compromises and negotiations between all involved parties. Closer involvement of the elderly in the choice of priorities and aims of clinical and therapeutic decisions is another important task. While awaiting the greater availability of electronic health records, which may help to share the patient’s information between different nodes of the hospital and community services, the internist must promote and facilitate a close relationship with the patient’s family, primary care physicians and social workers, both on hospital admission and at discharge. Conclusive remarks All in all, there are still many gaps in the knowledge necessary for the internist to optimally and effectively tackle the many issues related to the health care of the elderly with multimorbidity and associated polypharmacy. There is a dramatic need for more focused research in this field. A registry such as REPOSI, which from 2014 is going 123 to be a joint effort of Italian and Spanish internists, should become a permanent observatory on the complexity of health and care in the elderly. In the near future, we hope to develop research protocols able to lead to more evidencebased prescription of multiple drugs. Conflict of interest None. Appendix Investigators and co-authors of the REPOSI (REgistro POliterapie SIMI, Societa` Italiana di Medicina Interna) Study Group are as follows: Steering Committee Pier Mannuccio Mannucci (Chair, Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano), Alessandro Nobili (co-chair, IRCCS-Istituto di Ricerche Farmacologiche ‘‘Mario Negri’’, Milano), Mauro Tettamanti, Luca Pasina, Carlotta Franchi (IRCCS-Istituto di Ricerche Farmacologiche ‘‘Mario Negri’’, Milano), Francesco Salerno (IRCCS Policlinico San Donato Milanese, Milano), Salvatore Corrao (ARNAS Civico, Di Cristina, Benfratelli, DiBiMIS, Universita` di Palermo, Palermo), Alessandra Marengoni (Spedali Civili di Brescia, Brescia), Maura Marcucci (Geriatric Unit, Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano). Clincal data monitoring and revision: Eleonora Sparacio, Stefania Alborghetti, Rosa Di Costanzo, Tarek Kamal Eldin (IRCCS-Istituto di Ricerche Farmacologiche ‘‘Mario Negri’’, Milano). Database Management and Statistics: Mauro Tettamanti, Codjo Djignefa Djade (IRCCS-Istituto di Ricerche Farmacologiche ‘‘Mario Negri’’, Milano). Investigators: Domenico Prisco, Elena Silvestri, Caterina Cenci, Tommaso Barnini (Azienda Ospedaliero Universitaria Careggi Firenze, SOD Patologia Medica); Giuseppe Delitala, Stefano Carta, Sebastiana Atzori (Azienda Mista Ospedaliera Universitaria, Sassari, Clinica Medica); Gianfranco Guarnieri, Michela Zanetti, Annalisa Spalluti (Azienda Ospedaliera Universitaria Ospedali Riuniti di Trieste, Trieste, Clinica Medica Generale e Terapia Medica); Maria Grazia Serra, Maria Antonietta Bleve (Azienda Ospedaliera ‘‘Cardinale Panico’’ di Tricase, Lecce, Unita` Operativa Complessa Medicina); Massimo Vanoli, Giulia Grignani, Gianluca Casella (Azienda Ospedaliera della Provincia di Lecco, Ospedale di Merate, Lecco, Medicina Interna); Laura Gasbarrone (Azienda Ospedaliera Ospedale San Camillo Forlanini, Roma, Medicina Interna 1); Giorgio Maniscalco, Massimo Gunelli, Daniela Tirotta (Azienda Ospedaliera Ospedale San Salvatore, Pesaro, Soc Medicina Interna); Antonio Brucato, Silvia Ghidoni, Paola Intern Emerg Med Di Corato (Azienda Ospedaliera Papa Giovanni XXIII, Bergamo, Medicina 1); Mauro Bernardi, Silvia Li Bassi, Luca Santi (Azienda Ospedaliera Policlinico Sant’OrsolaMalpighi, Bologna, Semeiotica Medica Bernardi); Giancarlo Agnelli, Alfonso Iorio, Maura Marcucci, Emanuela Marchesini (Azienda Ospedaliera Santa Maria della Misericordia, Perugia, Medicina Interna e Cardiovascolare); Elmo Mannarino, Graziana Lupattelli, Pamela Rondelli, Francesco Paciullo (Azienda Ospedaliera Santa Maria della Misericordia, Perugia, Medicina Interna, Angiologia, Malattie da Arteriosclerosi); Fabrizio Fabris, Michela Carlon, Francesca Turatto (Azienda Ospedaliera Universita` di Padova, Padova, Clinica Medica I); Maria Cristina Baroni, Marianna Zardo (Azienda Ospedaliera Universita` di Parma, Parma, Clinica e Terapia Medica); Roberto Manfredini, Christian Molino, Marco Pala, Fabio Fabbian (Azienda Ospedaliera - Universitaria Sant’Anna, Ferrara, Unita` Operativa Clinica Medica); Ranuccio Nuti, Roberto Valenti, Martina Ruvio, Silvia Cappelli (Azienda Ospedaliera Universita` Senese, Siena, Medicina Interna I); Giuseppe Paolisso, Maria Rosaria Rizzo, Maria Teresa Laieta (Azienda Ospedaliera Universitaria della Seconda Universita` degli Studi di Napoli, Napoli, VI Divisione di Medicina Interna e Malattie Nutrizionali dell’Invecchiamento); Teresa Salvatore, Ferdinando Carlo Sasso (Azienda Ospedaliera Universitaria della Seconda Universita` degli Studi di Napoli, Napoli, Medicina Interna e Malattie Epato-Bilio Metaboliche Avanzate); Riccardo Utili, Emanuele Durante Mangoni, Daniela Pinto (Azienda Ospedaliera Universitaria della Seconda Universita` degli Studi di Napoli, Napoli, Medicina Infettivologica e dei trapianti); Oliviero Olivieri, Anna Maria Stanzial (Azienda Ospedaliera Universitaria Integrata di Verona, Verona, Unita` Operativa di Medicina Interna B); Renato Fellin, Stefano Volpato, Sioulis Fotini (Azienda Ospedaliera Universitaria Ospedale Sant’Anna, Ferrara, Unita` Operativa di Medicina Interna Gerontologia e Geriatria); Mario Barbagallo, Ligia Dominguez, Lidia Plances, Daniela D’Angelo (Azienda Ospedaliera Universitaria Policlinico Giaccone Policlinico di Palermo, Palermo, Unita` Operativa di Geriatria e Lungodegenza); Giovanbattista Rini, Pasquale Mansueto, Ilenia Pepe (Azienda Ospedaliera Universitaria Policlinico P. Giaccone di Palermo, Palermo, Medicina Interna e Malattie Metaboliche); Giuseppe Licata, Luigi Calvo, Maria Valenti (Azienda Ospedaliera Universitaria Policlinico P. Giaccone di Palermo, Palermo, Medicina Interna e Cardioangiologia); Claudio Borghi, Enrico Strocchi, Elisa Rebecca Rinaldi (Azienda Ospedaliera Universitaria Policlinico S. OrsolaMalpighi, Bologna, Unita` Operativa di Medicina Interna Borghi); Marco Zoli, Elisa Fabbri, Donatella Magalotti (Azienda Ospedaliera Universitaria Policlinico S. OrsolaMalpighi, Bologna, Unita` Operativa di Medicina Interna Zoli); Alberto Auteri, Anna Laura Pasqui, Luca Puccetti (Azienda Ospedaliera Universitaria Senese, Siena, Medicina 3); Franco Laghi Pasini, Pier Leopoldo Capecchi, Maurizio Bicchi (Azienda Ospedaliera Universitaria Senese, Siena, Unita` Operativa Complessa Medicina 2); Carlo Sabba`, Francesco Saverio Vella, Alessandro Marseglia, Chiara Valentina Luglio (Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari, Bari, Medicina Interna Universitaria C. Frugoni); Giuseppe Palasciano, Maria Ester Modeo, Annamaria Aquilino, Pallante Raffaele (Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari, Bari, Medicina Interna Ospedale ‘‘PendeFerrannini’’); Stefania Pugliese, Caterina Capobianco (Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari, Bari, Clinica Medica I Augusto Murri); Alfredo Postiglione, Maria Rosaria Barbella, Francesco De Stefano (Azienda Ospedaliera Universitaria Policlinico Federico II di Napoli, Medicina Geriatrica Dipartimento di Clinica Medica); Luigi Fenoglio, Chiara Brignone, Christian Bracco, Alessia Giraudo (Azienda Sanitaria Ospedaliera Santa Croce e Carle di Cuneo, Cuneo, S. C. Medicina Interna); Giuseppe Musca, Olga Cuccurullo (Azienda Sanitaria Provinciale di Cosenza Presidio Ospedaliero di Cetraro, Cosenza, Unita` Operativa Complessa Medicina Interna); Luigi Cricco, Alessandra Fiorentini (COB Stabilimento Montefiascone, Viterbo, Unita` Operativa Complessa di Geriatria e Medicina); Maria Domenica Cappellini, Giovanna Fabio, Sonia Seghezzi, Margherita Migone De Amicis (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Unita` Operativa Medicina Interna IA); Silvia Fargion, Paola Bonara, Mara Bulgheroni, Rosa Lombardi (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna 1B); Fabio Magrini, Ferdinando Massari, Tatiana Tonella (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Unita` Operativa Medicina Cardiovascolare); Flora Peyvandi, Alberto Tedeschi, Raffaella Rossio (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna 2); Guido Moreo, Barbara Ferrari, Luisa Roncari (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna 3); Valter Monzani, Valeria Savojardo, Christian Folli, Maria Magnini (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Medicina d’Urgenza); Daniela Mari, Paolo Dionigi Rossi, Sarah Damanti, Silvia Prolo (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Geriatria); Maria Sole Lilleri (Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Milano, Medicina Generale ad Indirizzo Geriatrico); Luigi Cricco, Alessandra Fiorentini (COB Viterbo, Stabilimento Montefiascone, Viterbo, UOC Geriatria e Medicina); Giuliana Micale (IRCCS Istituto Auxologico Italiano, Milano, Medicina 123 Intern Emerg Med Generale ad indirizzo Geriatrico); Mauro Podda, Carlo Selmi, Francesca Meda (IRCCS Istituto Clinico Humanitas, Milano, Clinica Medica); Francesco Salerno, Silvia Accordino, Alessio Conca, Valentina Monti (IRCCS Policlinico San Donato e Universita` di Milano, San Donato Milanese, Medicina Interna); Gino Roberto Corazza, Emanuela Miceli, Marco Vincenzo Lenti, Donatella Padula (IRCCS Policlinico San Matteo di Pavia, Pavia, Clinica Medica I, Reparto 11); Carlo L. Balduini, Giampiera Bertolino, Stella Provini, Federica Quaglia (IRCCS Policlinico San Matteo di Pavia, Pavia, Clinica Medica III); Giovanni Murialdo, Marta Bovio (IRCS Azienda Ospedaliera Universitaria San Martino-IST di Genova, Genova, Clinica di Medicina Interna 2); Franco Dallegri, Luciano Ottonello, Alessandra Quercioli, Alessandra Barreca (Universita` di Genova, Genova, Medicina Interna 1); Maria Beatrice Secchi, Davide Ghelfi (Ospedale Bassini di Cinisello Balsamo, Milano, Divisione Medicina); Wu Sheng Chin, Laura Carassale, Silvia Caporotundo (Ospedale Bassini, Cinisello Balsamo, Milano, Unita` Operativa di Geriatria); Luigi Anastasio, Lucia Sofia, Maria Carbone (Ospedale Civile Jazzolino di Vibo Valentia, Vibo Valentia, Medicina interna); Giancarlo Traisci, Lucrezia De Feudis, Silvia Di Carlo (Ospedale Civile Santo Spirito di Pescara, Pescara, Medicina Interna 2); Giovanni Davı`, Maria Teresa Guagnano, Simona Sestili (Ospedale Clinicizzato SS. Annunziata, Chieti, Clinica Medica); Elisabetta Bergami, Emanuela Rizzioli (Ospedale del Delta, Lagosanto, Ferrara, Medicina Interna); Carlo Cagnoni, Luca Bertone, Antonio Manucra (Ospedale di Bobbio, Piacenza, Unita` Operativa Medicina e Primo Soccorso); Alberto Buratti, Tiziana Tognin, Nicola Lucio Liberato (Azienda Ospedaliera della Provincia di Pavia, Ospedale di Casorate Primo, Pavia, Medicina Interna); Giordano Bernasconi, Barbara Nardo (Ospedale di Circolo di Busto Arsizio, Varese, Medicina I); Giovanni Battista Bianchi, Sabrina Giaquinto Ospedale ‘‘SS Gerosa e Capitanio’’ di Lovere, Bergamo, Unita` Operativa Complessa di Medicina Generale, Azienda Ospedaliera ‘‘Bolognini’’ di Seriate, Bergamo; Giampiero Benetti, Michela Quagliolo, Giuseppe Riccardo Centenaro (Ospedale di Melegnano, Vizzolo Predabissi, Melegnano, Medicina 1); Francesco Purrello, Antonino Di Pino, Salvatore Piro (Ospedale Garibaldi Nesima, Catania, Unita` Operativa Complessa di Medicina Interna); Gerardo Mancuso, Daniela Calipari, Mose` Bartone, Francesco Gullo (Ospedale Giovanni Paolo II Lamezia Terme, Catanzaro, Unita` Operativa Complessa Medicina Interna); Michele Cortellaro, Marina Magenta, Francesca Perego; Maria Rachele Meroni (Ospedale Luigi Sacco, Milano, Medicina 3°); Marco Cicardi, Antonio Gidaro Marina Magenta (Ospedale Luigi Sacco, Milano, Medicina II); Andrea Sacco, Antonio Bonelli, Gaetano Dentamaro (Ospedale Madonna delle Grazie, Matera, Medicina); 123 Renzo Rozzini, Lina Falanga, Alessandro Giordano (Ospedale Poliambulanza, Brescia, Medicina Interna e Geriatria); Paolo Cavallo Perin, Bartolomeo Lorenzati, Gabriella Gruden, Graziella Bruno (Dipartimento di Scienze Mediche, Universita` di Torino, Citta` della Scienza e della Salute, Torino, Medicina 3); Giuseppe Montrucchio, Elisabetta Greco, Pietro Tizzani (Dipartimento di Scienze Mediche, Universita` di Torino, Citta` della Scienza e della Salute, Torino, Medicina Interna 5); Giacomo Fera, Maria Loreta Di Luca, Donatella Renna (Ospedale San Giacomo di Monopoli, Bari, Unita` Operativa Medicina Interna); Antonio Perciccante, Alessia Coralli (Ospedale San Giovanni-Decollato-Andisilla, Civita Castellana Medicina); Rodolfo Tassara, Deborah Melis, Lara Rebella (Ospedale San Paolo, Savona, Medicina I); Giorgio Menardo, Stefania Bottone, Elsa Sferrazzo (Ospedale San Paolo, Savona, Medicina Interna e Gastroenterologia); Claudio Ferri, Rinaldo Striuli, Rosa Scipioni (Ospedale San Salvatore, L’Aquila, Medicina Interna Universitaria); Raffaella Salmi, Piergiorgio Gaudenzi, Susanna Gamberini, Franco Ricci (Azienda Ospedaliera-Universitaria S. Anna, Ferrara, Unita` Operativa di Medicina Ospedaliera II); Cosimo Morabito, Roberto Fava (Ospedale Scillesi d’America, Scilla Medicina); Andrea Semplicini, Lucia Gottardo (Ospedale SS. Giovanni e Paolo, Venezia, Medicina Interna 1); Giuseppe Delitala, Stefano Carta, Sebastiana Atzori (Ospedale Universitario Policlinico di Sassari, Sassari, Clinica Medica); Gianluigi Vendemiale, Gaetano Serviddio, Roberta Forlano (Ospedali Riuniti di Foggia, Foggia, Medicina Interna Universitaria); Luigi Bolondi, Leonardo Rasciti, Ilaria Serio (Policlinico Sant’OrsolaMalpighi, Bologna, Unita` Operativa Complessa Medicina Interna); Cesare Masala, Antonio Mammarella, Valeria Raparelli (Policlinico Umberto I, Roma, Medicina Interna D); Filippo Rossi Fanelli, Massimo Delfino, Antonio Amoroso (Policlinico Umberto I, Roma, Medicina Interna H); Francesco Violi, Stefania Basili, Ludovica Perri (Policlinico Umberto I, Roma, Prima Clinica Medica); Pietro Serra, Vincenzo Fontana, Marco Falcone (Policlinico Umberto I, Roma, Terza Clinica Medica); Raffaele Landolfi, Antonio Grieco, Antonella Gallo (Policlinico Universitario A. Gemelli, Roma, Clinica Medica); Giuseppe Zuccala`, Francesco Franceschi, Guido De Marco, Cordischi Chiara, Sabbatini Marta (Policlinico Universitario A. Gemelli, Roma, Roma, Unita` Operativa Complessa Medicina d’Urgenza e Pronto Soccorso); Martino Bellusci, Donatella Setti, Filippo Pedrazzoli (Presidio Ospedaliero Alto Garda e Ledro, Ospedale di Arco, Trento, Unita` Operativa di Medicina Interna Urgenza/Emergenza); Giuseppe Romanelli, Caterina Pirali, Claudia Amolini (Spedali Civili di Brescia, Brescia, Geriatria); Enrico Agabiti Rosei, Damiano Rizzoni, Luana Castoldi (Spedali Civili di Brescia, Brescia, Seconda Medicina); Antonio Intern Emerg Med Picardi, Umberto Vespasiani Gentilucci, Chiara Mazzarelli, Paolo Gallo (Universita` Campus Bio-Medico, Roma, Medicina Clinica-Epatologia); Luigina Guasti, Luana Castiglioni, Andrea Maresca, Alessandro Squizzato, Sara Contini, Marta Molaro (Universita` degli Studi dell’Insubria, Ospedale di Circolo e Fondazione Macchi, Varese, Medicina Interna I); Giorgio Annoni, Maurizio Corsi, Sara Zazzetta (Universita` degli studi di Milano-Bicocca Ospedale S. Gerardo, Monza, Unita` Operativa di Geriatria); Marco Bertolotti, Chiara Mussi, Roberto Scotto, Maria Alice Ferri, Francesca Veltri (Universita` di Modena e Reggio Emilia, AUSL di Modena, Modena, Nuovo Ospedale Civile, Unita` Operativa di Geriatria); Franco Arturi, Elena Succurro, Giorgio Sesti, Umberto Gualtieri (Universita` degli Studi Magna Grecia, Policlinico Mater Domini, Catanzaro, Unita` Operativa Complessa di Medicina Interna); Francesco Perticone, Angela Sciacqua, Michele Quero, Chiara Bagnato (Universita` Magna Grecia Policlinico Mater Domini, Catanzaro, Unita` Operativa Malattie Cardiovascolari Geriatriche); Paola Loria, Maria Angela Becchi, Gianfranco Martucci, Alessandra Fantuzzi, Mauro Maurantonio (Universita` di Modena e Reggio Emilia, Medicina Metabolica-NOCSAE, Baggiovara, Modena); Roberto Corinaldesi, Roberto De Giorgio, Mauro Serra, Valentina Grasso, Eugenio Ruggeri, Lorenzo Mauro Carozza, Fabio Pignatti (Dipartimento di Scienze Mediche e Chirurgiche, Unita` Operativa di Medicina Interna, Universita` degli Studi di Bologna/Azienda OspedalieroUniversitaria S.Orsola-Malpighi, Bologna). 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. References 1. Cohen JE (2003) Human population: the next half century. Science 302:1172–1175 2. Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, Meinow B, Fratiglioni L (2011) Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev 10:430–439 3. Corazza GR, Lenti MV, Di Sabatino A (2014) Trusting internal medicine in hard times. Intern Emerg Med 9:121–122 4. Robine JM, Michel JP, Herrmann FR (2007) Who will care for the oldest people in our ageing society? BMJ 334:570–571 5. http://www.sciencemag.org. Accessed 12 May 2014 6. Veehof LJG, Meyboom-de Jong B, Haaijer-Rasamp FM (2000) Polypharmacy in the elderly—a literature review. Eur J Gen Pract 6:98–106 7. Bernabei R, Caputi A, Di Cioccio L, Fini M, Gallo PF, Marchionni N, Marrocco W, Melchiorri D, Mugelli A, Pilotto A, Rasi G, Zuccaro SM (2011) Need for redesigning pharmacologic research in older individuals. A position statement of the Geriatric Working Group of the Agenzia Italiana del Farmaco (AIFA). J Gerontol A Biol Sci Med Sci 66:66–67 8. L’uso dei farmaci in Italia. http://www.agenziafarmaco.it. Accessed 12 May 2014 9. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW (2005) Clinical practive guidelines and quality of care for older patients 20. 21. 22. 23. 24. 25. with multiple comorbid diseases: implications for pay for performance. JAMA 294:716–724 Onder G, Landi F, Fusco D, Corsonello A, Tosato M, Battaglia M, Mastropaolo S, Settanni S, Antocicco M, Lattanzio F (2014) Recommendations to prescribe in complex older adults: results of the CRIteria to assess appropriate Medication use among Elderly complex patients (CRIME) project. Drugs Aging 31:33–45 Liu GG, Christensen DB (2002) The continuing challenge of inappropriate prescribing in the elderly: an update of the evidence. J Am Pharm Assoc (Wash) 42:847–857 Opondo D, Eslami S, Visscher S, de Rooij SE, Verheij R, Korevaar JC, Abu-Hanna A (2012) Inappropriateness of medication prescriptions to elderly patients in the primary care setting: a systematic review. PLoS One 7:e43617 Lau DT, Kasper JD, Potter DE, Lyles A, Bennett RG (2005) Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med 165:68–74 Lorgunpai SJ, Grammas M, Lee DS, McAvay G, Charpentier P, Tinetti ME (2014) Potential therapeutic competition in community-living older adults in the US: use of medications that may adversely affect a coexisting condition. PLoS One 9(2):e89447 Rochon PA, Gurwitz JH (1997) Optimising drug treatment for elderly people: the prescribing cascade. BMJ 315:1096–1099 Dean B, Schachter M, Vincent C, Barber N (2002) Causes of prescribing errors in hospital inpatients: a prospective study. Lancet 359:1373–1378 Ryan C, Ross S, Davey P, Duncan EM, Francis JJ, Fielding S, Johnston M, Ker J, Lee AJ, MacLeod MJ, Maxwell S, McKay GA, McLay JS, Webb DJ, Bond C (2014) Prevalence and causes of prescribing errors: the PRescribing Outcomes for Trainee Doctors Engaged in Clinical Training (PROTECT) study. PLoS One 9:e79802 Osterberg L, Blaschke T (2005) Adherence to medication. N Engl J Med 353:487–497 MacLean S, Mulla S, Akl EA, Jankowski M, Vandvik PO, Ebrahim S, McLeod S, Bhatnagar N, Guyatt GH (2012) Patient values and preferences in decision making for antithrombotic therapy: a systematic review: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141(suppl. 2):e1S–e23S Byatt K (2014) Polypharmacy: thoughtful or random? BMJ 348:g17 Lee DS, Markwardt S, Goeres L, Lee CG, Eckstrom E, Williams C et al (2014) Statins and physical activity in older men: the osteoporotic fractures in men study. JAMA Intern Med. doi:10. 1001/jamainternmed.2014.2266 [Epub ahead of print] Steinman MA, Landefeld CS, Rosenthal GE, Berthenthal D, Sen S, Kaboli PJ (2006) Polypharmacy and prescribing quality in older people. J Am Geriatr Soc 54:1516–1523 Dimitrow MS, Airaksinen MS, Kivela SL, Lyles A, Leikola SN (2011) Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: a systematic review. J Am Geriatr Soc 59:1521–1530 O’Connor MN, Gallagher P, O’Mahony D (2012) Inappropriate prescribing: criteria, detection and prevention. Drugs Aging 29:437–452 Gallagher P, Lang PO, Cherubini A, Topinkova´ E, Cruz-Jentoft A, Montero Errasquı´n B, Ma´dlova´ P, Gasperini B, Baeyens H, Baeyens JP, Michel JP, O’Mahony D (2011) Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol 67:1175–1188 123 Intern Emerg Med 26. Lazarou J, Pomeranz BH, Corey PN (1998) Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 279:1200–1205 27. Budnitz DS, Lovegrove MC, Shehab N, Richards CL (2011) Emergency hospitalization for adverse drug events in older Americans. N Engl J Med 365:2002–2012 28. Marcucci M, Iorio A, Nobili A, Tettamanti M, Pasina L, Marengoni A, Salerno F, Corrao S, Mannucci PM, REPOSI Investigators (2010) Factors affecting adherence to guidelines for antithrombotic therapy in elderly patients with atrial fibrillation admitted to internal medicine wards. Eur J Intern Med 21:516–523 29. Marcucci M, Iorio A, Nobili A, Tettamanti M, Pasina L, Djade CD, Marengoni A, Salerno F, Corrao S, Mannucci PM, REPOSI (REgistro POliterapie Societa` Italiana di Medicina Interna) Investigators (2013) Prophylaxis of venous thromboembolism in elderly patients with multimorbidity. Intern Emerg Med 8:509–520 30. Marcucci M, Nobili A, Tettamanti M, Iorio A, Pasina L, Djade CD, Franchi C, Marengoni A, Salerno F, Corrao S, Violi F, Mannucci PM, REPOSI Investigators (2013) Joint use of cardioembolic and bleeding risk scores in elderly patients with atrial fibrillation. Eur J Intern Med 24:800–806 31. Pasina L, Nobili A, Tettamanti M, Salerno F, Corrao S, Marengoni A, Iorio A, Marcucci M, Mannucci PM, REPOSI Investigators (2011) Prevalence and appropriateness of drug prescriptions for peptic ulcer and gastro-esophageal reflux disease in a cohort of hospitalized elderly. Eur J Intern Med 22:205–210 32. Marengoni A, Bianchi G, Nobili A, Tettamanti M, Pasina L, Corrao S, Salerno F, Iorio A, Marcucci M, Mannucci PM, SIMI Investigators (2012) Prevalence and characteristics of antidepressant drug prescriptions in older Italian patients. Int Psychogeriatr 24:606–613 33. Pasina L, Djade CD, Lucca U, Nobili A, Tettamanti M, Franchi C, Salerno F, Corrao S, Marengoni A, Iorio A, Marcucci M, Violi F, Mannucci PM (2013) Association of anticholinergic burden with cognitive and functional status in a cohort of hospitalized elderly: comparison of the anticholinergic cognitive burden scale and anticholinergic risk scale: results from the REPOSI study. Drugs Aging 30:103–112 34. Yang YX, Metz DC (2010) Safety of proton pump inhibitor exposure. Gastroenterology 139:1115–1127 35. van Walraven C, Hart RG, Connolly S, Austin PC, Mant J, Hobbs FD, Koudstaal PJ, Petersen P, Perez-Gomez F, Knottnerus JA, Boode B, Ezekowitz MD, Singer DE (2009) Effect of age on stroke prevention therapy in patients with atrial fibrillation: the atrial fibrillation investigators. Stroke 40:1410–1416 36. Nobili A, Licata G, Salerno F et al (2011) Polypharmacy, length of hospital stay, and in-hospital mortality among elderly patients in internal medicine wards. The REPOSI study. Eur J Clin Pharmacol 67:507–519 37. Pasina L, Djade CD, Nobili A, Tettamanti M, Franchi C, Salerno F, Corrao S, Marengoni A, Iorio A, Marcucci M, Mannucci PM (2013) Drug-drug interactions in a cohort of hospitalized elderly patients. Pharmacoepidemiol Drug Saf 22:1054–1060 38. Marengoni A, Nobili A, Romano V, Tettamanti M, Pasina L, Djade S, Corrao S, Salerno F, Iorio A, Marcucci M, Mannucci PM, SIMI Investigators (2013) Adverse clinical events and mortality during hospitalization and 3 months after discharge in cognitively impaired elderly patients. J Gerontol A Biol Sci Med Sci 68:419–425 123 39. Pasina L, Djade CD, Tettamanti M, Franchi C, Salerno F, Corrao S, Marengoni A, Marcucci M, Mannucci PM, Nobili A, REPOSI Investigators (2014) Prevalence of potentially inappropriate medications and risk of adverse clinical outcome in a cohort of hospitalized elderly patients: results from the REPOSI Study. J Clin Pharm Ther. doi:10.1111/jcpt.12178 40. Franchi C, Nobili A, Mari D, Tettamanti M, Djade CD, Pasina L, Salerno F, Corrao S, Marengoni A, Iorio A, Marcucci M, Mannucci PM, REPOSI Investigators (2013) Risk factors for hospital readmission of elderly patients. Eur J Intern Med 24:45–51 41. De La Higuera L, Riva E, Djade CD, Mandelli S, Franchi C, Marengoni A, Salerno F, Corrao S, Pasina L, Tettamanti M, Marcucci M, Mannucci PM, Nobili A (2013) Prognostic value of estimated glomerular filtration rate in hospitalized elderly patients. Intern Emerg Med. doi:10.1007/s11739-013-1028-5 42. Marengoni A, Bonometti F, Nobili A, Tettamanti M, Salerno F, Corrao S, Iorio A, Marcucci M, Mannucci PM, Italian Society of Internal Medicine (SIMI) Investigators (2010) In-hospital death and adverse clinical events in elderly patients according to disease clustering: the REPOSI study. Rejuvenation Res 13:469–477 43. Nobili A, Marengoni A, Tettamanti M, Salerno F, Pasina L, Franchi C, Iorio A, Marcucci M, Corrao S, Licata G, Mannucci PM (2011) Association between clusters of diseases and polypharmacy in hospitalized elderly patients: results from the REPOSI study. Eur J Intern Med 22:597–602 44. Marengoni A, Nobili A, Pirali C, Tettamanti M, Pasina L, Salerno F, Corrao S, Iorio A, Marcucci M, Franchi C, Mannucci PM, REPOSI Investigators (2013) Comparison of disease clusters in two elderly populations hospitalized in 2008 and 2010. Gerontology 59:307–315 45. Tinetti ME, Studenski SA (2011) Comparative effectiveness research and patients with multiple chronic conditions. N Engl J Med 364:2478–2481 46. Baraba´si AL, Gulbahce N, Loscalzo J (2011) Network medicine: a network-based approach to human disease. Nat Rev Genet 12:56–68 47. Sackett DL (2011) Clinician-trialist rounds: 4. why not do an N-of-1 RCT? Clin Trials 8:350–352 48. Gabler NB, Duan N, Vohra S, Kravitz RL (2011) N-of-1 trials in the medical literature: a systematic review. Med Care 49:761–768 49. Tinetti ME, Bogardus ST Jr, Agostini JV (2004) Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 351:2870–2874 50. Charon R (2001) Narrative medicine: a model for empathy, reflection, profession, and trust. JAMA 286:1897–1902 51. Kalitzkus V, Matthiessen PF (2009) Narrative-based medicine: potential, pitfalls, and practice. Perm J 13:80–86 52. Folstein MF, Folstein SE, Mc Hugh PR (1975) Mini-Mental State. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198 53. Katzman R, Brown T, Fuld P, Peck A, Schechter R, Schimmel H (1983) Validation of a short orientation-memory-concentration test of cognitive impairment. Am J Psychiatry 140:734–739 54. Shah S, Vanclay F, Cooper B (1989) Improving the sensitivity of the Barthel index for stroke rehabilitation. J Clin Epidemiol 42:703–709
© Copyright 2026 Paperzz