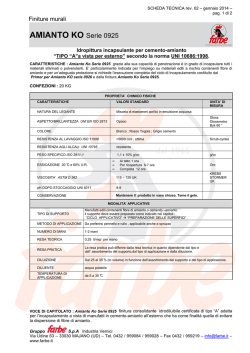
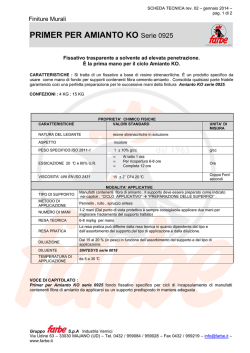
Fusione e demolizione molecolare: i due principi chimico-fisici impiegati nel processo di "inertizzazione" dell'amianto Prof. Renato Sinno Prof. Dott. Renato Sinno già docente di Mineralogia Università di Napoli Federico II AMIANTO, STATO DELL’ARTE: IN ATTESA DI UNA SOLUZIONE DEFINITIVA ROMA - Camera dei Deputati Convegno O.N.A. 20 marzo 2014 È a tutti noto che lo stato di salute dell’economia viene considerato come l’elemento essenziale per definire lo stato di prosperità di un paese. Per questo motivo grandi attenzione viene perciò riservata al costo della vita, allo sviluppo industriale, al potere di acquisto della moneta, al prezzo del petrolio e via discorrendo, al punto tale da rappresentare gli argomenti chiave che vengono dibattuti con grande frequenza, con l’ausilio di tutti i mezzi di informazione che vanno dalla carta stampate alla radio, alla televisione, che si impegnano ad aumentarne tali conoscenze e quindi la cultura di questo settore anche se le metodologie scelte per l’incremento dell’economia non trovano tutti d’accordo. Vi è da notare, e non con grande meraviglia, che un’attenzione certamente altrettanto rilevante non è stata mai attribuita al progressivo ed incalzante mutamento delle condizioni fisiche della terra non solo in tema di cambiamenti climatici, ma soprattutto in virtù dei più svariati interventi non sempre incoraggianti del fattore antropico che ritenendosi il padrone assoluto della natura, con comportamenti molto spesso sconsiderati finisce per rendere sempre più difficile l’esistenza degli equilibri naturali creando condizioni di vita poco accettabili. Foto 1: microscopio elettronico: ingrandimento 100 X Struttura fibrosa amianto di serpentino (crisotilo con crocidolite) AMIANTO O ASBESTO di Serpentino di Anfibolo 1 – Crisotilo (serpentino fibroso) Mg6(OH)6Si4O11.H2O 2 – Lizardite Mg6(OH)6Si4O11 3 – Antigorite (serpentino lamellare) Mg6(OH)8Si4O10 4 – Amesite (asbesto bruno) Mg6Al2OH8[Al3Si2O10] 1 – Antofillite (Mg,Fe)7(OH)2Si8O22 2 – Tremolite Ca”2Mg5(OH)2Si8O22 3 – Actinolite Na2Ca3Mg10(OH)4Si16O44 4 – Riebeckite Na3Fe”3Fe”’2(OH)2Si8O22 5 – Crocidolite (asbesto blu) Na2(Mg,Fe”)3(OH)2Si8O22 Foto 2: microscopio elettronico: ingrandimento 1.000 X Struttura fibrosa amianto di serpentino (crisotilo con crocidolite) I materiali contenenti amianto (MCA) Metodologie impiegate nei processi di inertizzazione dell’amianto: 1) torce al plasma (Francia): temperature di fusione dei componenti dell’amianto 2000°C temperature impiegate per la messa a regime dell’impianto temperature molto al di sopra; 2) prodotti ottenuti dopo l’inertizzazione (analisi spettrofotometrica di un tipo di plasma provenienza francese: silicato doppio di calcio e cobalto - akermanite, silicato doppio di calcio e magnesio – merwinite, silicato di ferro – fayalite; 3) demolizione della molecola di crisotilo mediante temperatura e additivi “bassofondenti”; 4) svolgimento della reazione: Mg6(OH)8Si4O10 → 3Mg2SiO4 + SiO2 + 4H2O Silicato basico di Magnesio (900°C- 950°C) → silicato di magnesio + silice + acqua 5) l’analisi spettrofotometrica conferma la presenza di fosterite (silicato di magnesio + silice Foto microscopio elettronico: ingrandimento 100 X e 1000 X Silice amorfa (dopo la trasformazione) Foto microscopio elettronico: ingrandimento 1000 X Dal convegno di Casale Monferrato (Al) 18 sett. 2012 dalle relazione dei Ministri Forneri (lavoro), Balduzzi (salute), e Clini (ambiente) Siti di interesse nazionale per presenza di amianto 12 Luoghi censiti come “pericolosi” 34.000 Luoghi di “prima pericolosità” 373 Quantità di amianto smaltito al 2009 379.000 ton. Quantità di amianto ancora da smaltire 32.000.000 ton. Quantità ancora da smaltire calcolata in % 99% Tempo occorrente stimato per lo smaltimento totale (calcolato al ritmo di 379.000 ton/anno) 85 anni COMUNICATO DELL'U.E. SEGUENTE ALLA RIUNIONE DI GENNAIO 2013. RECENTE “RISOLUZIONE” DELL'U.E. PROPOSTE PER LA SICUREZZA DELLO SMALTIMENTO DEFINITIVO DELL'AMIANTO SULLA SCORTA DELLE STATISTICHE CHE ANCORA LO VEDONO PRESENTE IN GRAN NUMERO NELLE TUBATURE DELL' ACQUA, NEI TRENI, NELLE NAVI, NEI MACCHINARI E SOPRATTUTTO IN MOLTI EDIFICI, NONCHÉ SULL'ONDA DEL TIMORE SUSCITATO DALLA FUGA DI AMIANTO CHE HA PORTATO ALLA CHIUSURA RECENTE DI ALCUNI EDIFICI COMUNITARI A STRASBURGO, (dalla relazione dell'europarlamentare STEPHEN HUGHES approvata con 558 voti a favore e 51 contrari) • • • • • • • • 1) Scadenza definitiva per il completamento della strategia: anno 2028; 2) Introduzione di un registro pubblico degli edifici contenenti amianto negli Stati membri dell'Unione; 3) Sostegno alle Associazioni delle vittime; 4) Definizione di una tabella di marcia degli interventi; S) Definizione di un piano che imponga la garanzia che gli ispettori che operano sul campo siano protetti da attrezzature adeguate; 6) Gli addetti alla rimozione siano sufficientemente qualificati; 7) Assoluto divieto del conferimento in discarica di qualunque tipo di materiale contenente amianto a causa della eventuale azione delle acque di falda; 8) Invito a tutti i paesi dell'unione alla realizzazione di centri di trattamento e di “inertizzazione” dei rifiuti contenenti amianto, prevedendo la graduale cessazione del conferimento in discarica degli stessi. Ultima dichiarazione ufficiale del ministro Balduzzi: il piano previsto non sarà caratterizzato da altre 200 pagine di analisi e prospettive ma sarà un piano di proposte di grande innovazione. Due gli elementi e gli aspetti che caratterizzeranno la lotta all'amianto che richiedono particolare attenzione, la ricerca e la bonifica. Infatti la battaglia contro l'asbesto non è ancora vinta, perché occorre fare molto su questi due fronti, sui quali si concentra una parte importante del piano nazionale in dirittura di arrivo. Tre sono le macroaree di azione del piano: la tutela della salute, la tutela dell’ambiente e gli aspetti previdenziali e di sicurezza del lavoro. Ministero della Salute: Presentato il Piano Nazionale Amianto – marzo 2013 …”È una risposta operativa ad una vicenda sulla quale a livello Nazionale era sceso l’oblio. Il Governo Monti ha riportato una triste vicenda a livello Nazionale ma anche Internazionale in Europa. L’Italia è diventata punto di riferimento dell’Unione per l’organizzazione di una rete europea per la lotta alle malattie correlate all’amianto” (relazione al Consiglio dei Ministri del Ministro Balduzzi). Voglio concludere con un monito umile ed affettuoso rivolto a quanti sottovalutano certi problemi ecologici e, sorridendo, si adagiano non senza saccenteria, sulla comoda piattaforma del potere che per fortuna e per legge naturale ha un processo vitale ben definito. Ricordo un’espressione del grande William Shakespeare che ritengo molto profonda; “il saggio sa di essere stupido, è lo stupido che crede di essere saggio”. ROMANO BATTAGLIA • Rimanere se stessi in un mondo che giorno e notte si adopera per trasformare ognuno di noi in un essere qualsiasi, vuol dire combattere la battaglia più dura della vita. Aggiungo con molta modestia: essere betulla è facile, restare quercia è molto più difficile, ma è soprattutto doloroso! Integrazione di tecniche e dati per lo studio della presenza di cemento amianto sul territorio Dott.ssa Lorenza Fiumi Integrazione di tecniche e dati per lo studio della presenza di cemento amianto sul territorio Lorenza Fiumi Gruppo di ricerca: Lorenza Fiumi (resp.) Stefano Tocci e Carlo Meoni Seconda Conferenza Internazionale ”Lotta all’amianto: il diritto incontra la scienza” Camera dei Deputati – Auletta dei Gruppi Parlamentari - 20 marzo 2014 Il sensore MIVIS (Multispectral Infrared Visible Imaging Spectrometer) per la mappatura delle coperture in c-a Il CNR possiede e gestisce il MIVIS un sensore aeroportato con 102 canali e con una risoluzione spaziale fino a 3m x 3m, ne fanno uno strumento innovativo ed unico nelle applicazioni dirette sul territorio e delle relative risorse. Sviluppi della ricerca: caratterizzazione dello stato di alterazione del c.-a. Cemento-amianto chiaro: il colore chiaro è un buon indicatore dell’ottimo stato di conservazione del materiale che risulta integro in tutte le sue componenti. Cemento-amianto scuro: il materiale è soggetto a complesse degradazioni che portano ad una minore consistenza del prodotto e all’affioramento di fibre di amianto in superficie. -OBIETTIVI: -migliorare l’accuratezza e di valutare con estremo rigore il grado di attendibilità delle mappe; - realizzare mappe di rischio in cui siano evidenziate lo stato di alterazione del materiale in modo da fornire un sistema di supporto essenziale per monitorare aree a rischio ambientale. Sviluppi della ricerca: migliorare l’accuratezza di classificazione - finalizzata a ridefinirne la geometria dei poligoni eliminando quindi le discontinuità, ad esempio i vuoti, da ogni copertura. Copertura a volta falda + 51% volta + 40% Intersezione Spaziale è stata eseguita con i dati classificati MIVIS e la CTR a scala 1:5000, entrambi vettoriali quest’ultima relativa al solo tematismo dell’edificato. Integrazione di tecniche e dati in ambiente GIS GEOGRAPHIC INFORMATION SYSTEM (GIS) DATI TELERILEVATI e + DATI ISTAT Integrazione di tecniche e dati per: stima di c-a sul territorio del comune di Pomezia Ripartizione delle coperture in c-a in base alla superficie 2,78% 8,83% (mq) 0,48% 3,39% 100-500 25,76% 9,92% 0-100 500-1000 1000-2000 48,85% 2000-3000 3000-5000 >5000 Amianto (mq) 460.350 Numero coperture (amianto min) 827 Amianto /Superficie coperta (mq/kmq) 2.788 Peso (kg) 5.984.550 Popolazione (ISTAT 2010) 60.167 Amianto / Popolazione (mq/ab) 7,65 La ricerca sul mesotelioma pleurico: dal laboratorio alla pratica clinica Prof. Luciano Mutti Are there new Evidences Changing our Approach to Mesothelioma ? MPM: hindsight and perspectives Luciano Mutti M.D. PhD on behalf of Buzzi Foundation and G.I.M.e Expecting the Worldwide Epidemics ERS/ESTS TASK FORCE Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma A. Scherpereel, P. Astoul, P. Baas, T. Berghmans, H. Clayson, P. de Vuyst,H. Dienemann, F. GalateauSalle, C. Hennequin, G. Hillerdal, C. Le Pe´choux, L. Mutti, J-C. Pairon, R. Stahel, P. van Houtte, J. van Meerbeeck, D. Waller and W. Weder R1a. Every patient should receive best supportive care. R1b. When a decision is made to treat patients with chemotherapy alone, patients in a good performance status (PS; > 60 on the Karnofsky scale or < 3 on the ECOG scale) should be treated with first line combination chemotherapy consisting of platinum and pemetrexed or raltitrexed (1B). Alternatively, patients could be included in first and second-line clinical trials. R1c. In the light of limited evidence of efficacy of chemotherapy, the decision to administer chemotherapy should be discussed with the patients and his relatives on a case by case basis . Hence what should we do to conduct fruitful pre-clinical and clinical research on asbestos-related tumours and to cope with this unsettled scenario ? Awaiting Genetic Based Medicine grows up (1) OncoTargets and Therapy Drugs for solid cancer: the productivity crisis prompts a rethink Science does not proceed linearly but by paradigmatic shifts driven by translational productivity // Awaiting Genetic Based Medicine grows up (2) Preclinical Knowledge Cancer Research is Translational Cancer Research aimed at changing the clinical practice via clinical research based on strong rationale •ASCO Blueprints, Nov 2011 (pats stratification) •Clinical Trials Directives-Regulations •GCP Biomarkers validation on proper animal models and IHC from human tumours tissues aimed at Novel Therapies, Diagnosis, Prognosis Susceptibility Tests Early Phases Clinical Trials with Appropriate End Points Tests validation in humans Therapies currently in Phase II trials for malignant pleural Mesothelioma Pinton G. et al. Expert Opin Investig Drugs, 2013 5. Expert opinion Back in 2005 in their review of theirs, Kumar and Kratzke had foreseen that targeted therapy addressed to growth factor receptors and cell cycle proteins would change the prognosis of patients with MPM [57]. Eight years later, unfortunately, such a result has not been achieved and looks like being still rather far away. To get ahead, first, we should ask ourselves: ‘Why?’. An obvious stallmate that requires a swift U-turn paradigmatic shift . New scenarios should be explored “A change is better than a rest” Irish Proverb Clinical Focus: The Evolving Role of Systemic Therapy for Mesothelioma clinicaloptions.com/oncology Inhibition of PDGFR Increases Uptake of Drug in Tumor Cells by Decreasing IFP Imatinib inhibition of stromal PDGF-Rβ decreases tumor IFP Drug uptake increases in tumors Tumor Uptake of [3H]Taxol Tumor IFP (mm Hg) 8 6 4 2 0 PBS STI571 Taxol Taxol + STI-571 16. Pietras K, et al. Cancer Res. 2002;62:5476-5484. 8 6 4 2 0 Control STI-571 Control STI-571 8 24 Hrs After Injection [3H]Taxol -14379 Toward the shift: genetic hints Validaton of Data Mining: 119 gene deregulated in at least two refs High expression OS 20.8 vs 40 months (NME1\2 and THBS2 are hypoxia-regulated genes) Toward the shift: Hypoxia Examples of diffuse immunostaining of CA IX and CA XII proteins in normal and neoplastic tissues and MPM is an extremely hypoxic tumour related to (GRP78) PAKT and low apoptosis rate. Hypoxia induces NOTCH 1 and its downregulation in MPM (obtained either through RNA interference or chemical inhibition) leads to cell death via AKT deactivation Ivanov S et al Am J Pathology, 2001 Graziani I et al Cancer Res, 2008 Enhancement of in vitro cell motility and invasiveness of MPM cells under hypoxia via HIF1/MUC1 Pathway . Morover high IHC MUC1 expression in the tumor are indicators of poor prognosis in MPM Goudarzi H et al. Cancer Letter, 2013 Pillai K et al. J Biol Markers 2013 Is Hypoxia and its effects a new direction to take ? Overview Hypoxia and Translational control in cancer and in MPM Hypoxia and MPM Metabolism Therapeutic Translational implications and “Take home message” Have we any findings suggesting Hypoxia-dep Translational abnormalities in MPM cells ? Toward the shift: Hypoxia and Translation (1) In all human tumours IF-4E//4E-BP1 is critical : 4E-BP1 loss or P- reduces pts survival Hypoxic Tumours show increased P- eIF-4E and/or reduced 4E-BP1 Toward the shift: Hypoxia and Translation (2) All major pathways regulating translation PNAS, 2002; 22 (99): 14374-14379 are constitutively “ON” in MPM cells… Toward the shift: Hypoxia and Translation (3) …however their inhibition does not reduce translation and suggests PNAS, 2002; 22 (99): 14374-14379 the presence of specific modulators Toward the shift: Hypoxia and Translation (4) …moreover, even more importantly, MPM cells have abnormal, constitutive active translation that is not stimulated by Growth Factors Toward the shift: Hypoxia and Translation (5) Translation in MPM cells is insensitive to mTORc1/2 dual inhibition by PP42 in spite of constitutive mTORc activity Toward the shift: Hypoxia and Translation (6) Eventually in MPM cells both 4E-BP1 overexpression and eIF-4E downregulation restore sensitivity to mTOR inhibition PNAS, 2002; 22 (99): 14374-14379 according to translation on hypoxia Toward the shift: Hypoxia and Translation (7) MPM cells show unique massive eIF6 expression and eIF6 is induced by hypoxia Have we any findings suggesting Hypoxia-dep Metabolic abnormalities in MPM cells ? Warburg effect Glutamine catabolism Glucose Piruvate Lactate Hypoxic tumours differently but largely rely on Glucose/Lactate metabolism and promote EMT and “Stemcellness” Toward the shift : Hypoxia and metabolism Hypoxic conditions sensitize MPM cells to glycolysis inhibitors and to interferences with lactate cycle Toward the shift : Hypoxia and EMT miR200 Family members and miR149 are related to Hypoxia and EMT miR200 Family members and miR149 are uniquely expressed in MPM -related to hypoxia levels- but not not in HMC (personal communicaton) and unleash EMT gene expression (SNAIL, SNUG, Zeb1, Twist, AKT). Ongoing project amid EU, US, AU, CN Snail expression is associated with poor prognosis in MPM Kobayashi M. et al Ann Thora Surg, 2013 Highlights and implications of MPM cells translation: the shift (1) • Translation is abnormally regulated by constitutive ativation of regulatory pathways regardless Growht Factor activation • MPM with high 4E-BP1 and low eIF-4E become sensitive to mTOR inhibition • IHC analysis of MPM tissue revealed a striking increased expressions of eIF6 in MPM tissue Morevor Enzaustarin (PKC inhibitors) inhibits eIF6 with in vitro/vivo anti-neoplastic effects on MPM cells This is a Scenario that Complies with the Hypoxic Hypothesis Highlights on implications of MPM cells Metabolism and EMT: the shift (2) Hypoxia-dep responders inhibitors (not TKR that in vivo are strongly expressed only in a small fraction of hypoxic, mesenchimal MPM and without biological relevance) •Glicogenolysis inhibitors •LDH and Lactate excretion inhibitors Pathways involved in miRs-dep hypoxixc EMT •Direct miRs antagonists/agonists (Phase I Au and …Europe) Is this the MPM Achille’s Heel ? Is this below the ultimate paradigmatic shift ? EMT MET + - Hypoxia Immunotherapy: a Master Key against Tumours and MPM ? B7H3 Immunotherapy: a Master Key against Tumours and MPM (1) ? Original Research Articles Int J Cancer. Dec 1998 Primary human mesothelioma cells express class II MHC, ICAM-1 and B7-2 and can present recall antigens to autologous blood lymphocytes. Int J Mol Med. Feb 2003 Transforming growth factor-beta released by PPD-presenting malignant mesothelioma cells inhibits interferon-gamma synthesis by an anti-PPD CD4+ T-cell clone.Article first published online: 22 JUL 2011 Journal of Cellular Physiology October 2011 Expression and regulation of B7-H3 immunoregulatory receptor, in HMCandMPM: Immunotherapeutic implications PlosOne, March 2013 Synergistic Effect of CTLA-4 Blockade and Cancer Chemotherapy in the Induction of Anti-Tumor Immunity A Master Key ? A second-line phase II clinical study with Int J Cancer. 1998; Int J Mol Med. 2003. a fully humanized anti-CTLA-4 monoclonal antibody as monotherapy in patients with unresectable MMe (Pfeizer) MMe cells act as APC of recall antigens Study extended Expression og B7-H3 on human MMe cells and tissue J Cell Physiol. 2011 160 HLA-DR 140 p<0.04 cell count/microL 120 MMe cell 100 p<0.02 80 p<0.03 40 20 AG PPD TT 0 Baseline d14 d30 1st cycle The Translational Research Cycle: Bench/Bedside/Bench d60 NR R 60 d1 d14 d30 2nd cycle d60 October, 2013 Analysis of overall survival for 29 patients Baseline PD 2 dose PR 3 dose PR 4 dose with MPM treated with tremelimumab Median OS: 10·7 months Changes in circulating CD4+ICOS+ T cell counts by response 160 140 p<0.04 Time points 6 months 12 months 18 months % Pts alive Pts at risk 79.3 23 48.3 14 36.7 9 24 months 36.7 8 cell count/microL 120 100 p<0.02 80 p<0.03 NR R 60 40 20 0 Baseline d14 d30 1st cycle d60 d1 d14 d30 d60 2nd cycle The Translational Research Cycle: Bench/Bedside/Bench Immunotherapy: a Master Key against Tumours and MPM (2) ? RCT vs Placebo (sic) on course. If/When phase II was confirmed: •Very selected pats with very good PS and life expectancy, •Relatively low extensive disesase TAKE -HOME MESSAGE MPM cells show a combined unique pattern of deranged cell machinery with potential “bespoke” translational implications This combined abnormality discloses novel approaches to the treatment of this tumour aimed at increasing its sensitivity to medical treatments The evidences seem to bring us away from most of the current innovative treatment for human cancers (TKRI) We are achieving a much better understanding of how to breach MMP cells metabolic and environmental shield and of the differences among the subtypes and this seems to be a crucial step forward Taking advantage of the capability of MPM cells to elicit an immune response and the results obtained from the first early clinical trials of immunotherapy are disclosing new scenarios “Here is Edward Bear, coming downstairs now, bump, bump, bump, on the back of his head, behind Christopher Robin. It is, as far as he knows, the only way of coming downstairs, but sometimes he feels that there really is another way, if only he could stop bumping for a moment and think of it” A.A. Milne 1926 Illustration E.H.Shepard 192614 “If you always do what you always did, you always get what you always got” Mark Twain We are not «Waiting for Godot» Let’s booggie to take action now “BREAKTHROUGH”, “ FAST TRACK” TRIALS TO SPEED UP THE NEXT CLINICAL RESARCH FOR MPM Contributors Metabolism. Arcangela G. Manente, Giulia Pinton, Laura Moro Dept. Pharmaceutical Sciences, University of Piemonte Orientale “A. Avogadro”, Novara, Italy Daniela Valenti, Rosa A. Vacca CNR-IBBE, Bari, Italy Puthen V. Jithesh, Liverpool Cancer Research UK Centre, University of Liverpool, UK Antonio Daga, IRCCS San Martino-IST, Genova, Italy Leonardo Rossi, Dept. of Human Morphology and Applied Biology, University of Pisa, Pisa, Italy Steven G. Gray, Kenneth J. O'Byrne, Institute of Molecular Medicine, St James's Hospital, Dublin 8, Ireland Dean Fennell, Thoracic Medical Oncology, University of Leicester & Leicester University Hospitals, Leicester, UK Translation. Stefano Biffo S. Raffaele Sci Inst, Milan, Italy Stefano Grosso MRC Toxicology Unit, University of Leicester, UK Genetics. Carlo Croce, Pierluigi Gasparini Columbus University. OH, USA Immunotherapy . M Maio, L Calabro’ Immmunotherapy Unit , Siena Hospital, Italy Ruolo della chirurgia nel mesotelioma pleurico Prof. Vittore Pagan Vittore Pagan RUOLO DELLA CHIRURGIA NEL MESOTELIOMA PLEURICO CH TORACICA IST TUMORI AVIANO •DIAGNOSI E STADIAZIONE VIDEOTORACOSCOPIA MICROTORACOTOMIA VIDEOMED/LAPARO •TERAPIA PALLIAZIONE CURA: ERADICAZIONE DI TUMORE SOLIDO CH TORACICA IST TUMORI AVIANO TUMORE SIEROSO • CONFINI IMPERCETTIBILI • PROGRESSIONE ? polifocale contiguità diffusione • DIAGNOSI TARDIVA • SOTTOSTADIAZIONE CH TORACICA IST TUMORI AVIANO MARGINS TO BE RESECTED IN REALLY R0 MPM RESECTION REMOVED BY EPP: • • • • • • PLEURA LUNG PERICARDIUM DIAPHRAGM LYMPH NODES PHRENIC NERVE UNREMOVABLE: • CONTRALAT PLEURA INTERFACE ADHESION • • RIBS + CHEST WALL NERVES (PLEXUS, • • • • • • TRACHEA ESOPHAGUS THORACIC DUCT SVC, AORTA, AZYGOS V SUBCLAVIAN VESSELS MEDIASTINAL TISSUE SYMPATHETIC, VAGUS T-ROOTS + INTERCOSTAL) CH TORACICA IST TUMORI AVIANO LIMITI CH CURATIVA • R 1 DI FATTO INELUDIBILE RIPRESA POST-CHIR PREVAL LOCO-CONFINARIA CITORIDUZIONE MASSIMALE CT/RT ADIUV • LIMITATA OPERABILITA’ CANDIDABILE 60% RESEZ COMPLETA 70% dei dei 572 OSSERVATI 280 ESPLORATI • MORBI-MORTALITA’ POSTOP CH TORACICA IST TUMORI AVIANO OUTCOME CHIRURGIA • DA SOLA SOPRAVV MEDIA SOVRAPPONIBILE NON OPERATI • IN MULTIMODALE SOPRAVV 13% 5 ANNI CH TORACICA IST TUMORI AVIANO OBIETTIVI REALISTICI CHIRURGIA • IN CONTESTO MULTIMOD ALTERARE STORIA NATURALE MPM (CT NEOAD?) • MASSIMA COMPLETEZZA MACRO E MINIMI R1 E COMPLICANZE • CON MIGLIORI PALLIAZIONE E QUALITA’ DI VITA POSSIBILI CH TORACICA IST TUMORI AVIANO CANDIDABILI CHIRURGIA • ISTOTIPO EPIT SARC E M+ MISTO SI’ NO DIBATTUTO • CONDIZIONI GENERALI ETA’ ≤ 70 a ≤ 75 a ? RISERVE C-R IK CO-PATOL • ERADICABILITA’MACROSCOPICA E NO LINFONODI CH TORACICA IST TUMORI AVIANO INTERVENTI CURATIVI (PPE e PTE) • PLEURO-PNEUMONECTOMIA • PLEURECTOMIA TOTALE o P/D ± ESTESE DIAFR/PERIC CH TORACICA IST TUMORI AVIANO MORTALITA’ 30gg = 4% COMPLICANZE MAGGIORI PPE-RELATE 6m = 1,5-2 VOLTE VS. 30gg PTE PLEURECTOMIA TOTALE ESTESA CH TORACICA IST TUMORI AVIANO VANTAGGI PTE • INCREMENTO CANDIDABILITA’ • MINORE MORBI-MORTALITA’ • MIGLIORE Q d V E RISERVA C-R • COALESCENZA POLM-PARETE FACILITA PERFUS CT ADIUV SU R1-2 CH TORACICA IST TUMORI AVIANO Autori vari PPEVS.PTE MORTALITA’ 4-15% 1-4% MORBILITA’ 50% 50% REINTERV 16% 2% SOPRAVV 5a 15% 15% ns sopravv 3a 22% 33% (EARLY+LATE) ARRUOLATI AD OGGI 101 CASI MPM CH TORACICA IST TUMORI AVIANO CONCLUSIONE POICHE’ SCOPO PRAGMATICO ATTUALE CHIRURGIA E’ ALTERARE CORSO MPM, PREVEDENDO R1 E TER ADIUVANTE, OFFRENDO QV, COMPLICANZE, SOPRAVVIVENZA MIGLIORI POSSIBILI, PTE PROPONIBILE COME PRIMA SCELTA VS. PPE SE COMPROVATA PARI COMPLETEZZA EXERESI CH TORACICA IST TUMORI AVIANO
© Copyright 2026 Paperzz