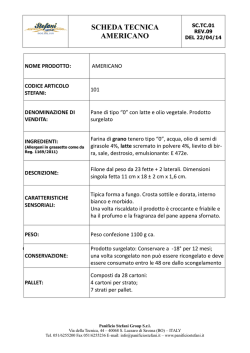
Allergia al latte In 20 minuti dirò dei 2 aspetti dell’ APLV che, in questi ultimi anni, mi hanno interessato di più In discussione, potremo affrontare altri aspetti che, magari, interessano di più a voi, per es. le domande “anticipate” SMS Ciro, 9 anni - 1 Ambulatorio, 18 Marzo 2014 • Intorno ai 6 mesi di vita, assume per la sua prima (?) volta il latte vaccino sotto forma di latte formulato e presenta immediatamente difficoltà respiratorie – Prova anche il parmigiano e presenta orticaria e angioedema – Effettua prick test che risultano positivi – Da allora non assume latte vaccino, né derivati – In questi anni, assunzioni accidentali di latte e derivati hanno portato alla comparsa di reazioni orticarioidi e respiratorie (asma) – A Giugno 2013 ha eseguito un TPO con latte vaccino fresco e ha presentato una reazione anafilattica, gli è stata somministrata adrenalina per via intramuscolare – Ciro è anche affetto da asma e dermatite atopica SMS Ciro, 9 anni - 2 Ambulatorio, 18 Marzo 2014 Prick test • Latte vaccino fresco = positivo (diametro medio del pomfo 13 mm) • Caseina = positivo (diametro medio del pomfo 5 mm) • Beta-lattoglobulina = positivo (diametro medio del pomfo 12 mm) • Lattoalbumina = positivo (diametro medio del pomfo 11 mm) • Controllo negativo = negativo • Istamina = positivo (diametro medio del pomfo 6 mm) SMS Ciro, 9 anni - 3 Ambulatorio, 18 Marzo 2014 • Vuol sapere se può iniziare la procedura di desensibilizzazione – Dove ha fatto il TPO, la DOPA gli è stata sconsigliata In quella occasione i medici sono stati conformi alle LG ? SMS Le ultime LG sulla AA (in genere) LG NIAID, JACI 2010 • Pag. S27. Guideline 19: The EP recommends that individuals with documented IgE-mediated FA should avoid ingesting their specific allergen or allergens – Rationale: The EP recognizes that allergen avoidance is a strategy that is unproven in RCTs. However, allergen avoidance is currently the safest strategy for managing FA • Pag. S29. Guideline 28: The EP does not recommend using allergenspecific immunotherapy to treat IgE-mediated FA – Rationale: Allergen-specific immunotherapy improves clinical symptoms of FA while on treatment. However, it is currently difficult to draw conclusions on the safety of such an approach and whether clinical tolerance (ie, improvement in clinical symptoms that persists even after allergen-specific immunotherapy is discontinued) will develop with long-term treatment. – Because of the risk of severe reactions, the approach should only be used in highly controlled settings SMS Le penultime LG proprio sulla APLV LG DRACMA, JACI 2010 • …. it is shown that standard OIT can increase the threshold of reactivity in about 80% of patients with CMA • However, mild adverse reactions are very common, and occasionally more severe reactions occur (approximately 1 in 100 doses resulted in multisystem reactions) • Taken together, these studies leave an important question unanswered: Are we dealing with desensitization or induced tolerance? Only prospective studies will tell. SMS Le ultime LG proprio sulla APLV LG BSACI, CEA 2014 • There are risks of adverse reactions associated with OTI – These predominantly affect the skin and gastrointestinal tract and are thus mild to moderate in severity – Anaphylactic reactions that require treatment with adrenaline have, however, been reported • Although OTI in cow’s milk allergy has been more widely studied than in allergy to hen’s egg and peanut, there are still a number of unanswered questions requiring further research – to establish which subjects to treat – what protocol to use – whether the treatment actually achieves true tolerance with a longlasting effect or just temporary desensitization – and data on long-term safety • Most authors thus do not currently recommend OTI for routine clinical practice SMS UN PASSO INDIETRO SMS La Desensibilizzazione agli alimenti Processo d'appello L'accusa Stefano Miceli Sopo [email protected] SMS DOPA o Dieta ? Stefano Miceli Sopo, Congresso SIAIP 2006 • Un bilancio che riguardi – La sicurezza per il paziente – Le problematiche logistiche e organizzative SMS Miceli Sopo et al, PAI 2009 Our answer to the starting question is that SOTI is still an experimental therapy SMS …. other studies are needed to clarify which is the best treatment and protocol to follow in order to reduce the adverse events and to increase the percentage of success, before thinking that SOTI might be part of the clinical practice. SMS Oral immunotherapy for milk allergy Yeung et al, Cochrane Database Syst Rev. 2012 Nov 14 • Five randomized trials were included. In general, the studies were small and had inconsistent methodological rigor. Each study used a different MOIT protocol. A total of 196 patients were studied (106 MOIT, 90 control) and all were children. Three studies were blinded and two used an avoidance diet control. • Sixty-six patients (62%) in the MOIT group were able to tolerate a full serving of milk (about 200 mL) compared to seven (8%) of the control group (RR 6.61, 95% CI 3.51 to 12.44). • In addition, 27 (25%) in the MOIT group could ingest a partial serving of milk (10 to 184 mL) while none could in the control group (RR 9.34, 95% CI 2.72 to 32.09). • None of the studies assessed the patients following a period off immunotherapy. Adverse reactions were common (97 of 106 MOIT patients had at least one symptom), although most were local and mild. Because of variability in reporting methods, adverse effects could not be combined quantitatively. For every 11 patients receiving MOIT, one required intramuscular epinephrine. • AUTHORS' CONCLUSIONS:A major drawback of MOIT is the frequency of adverse effects, although most are mild and self-limited. The use of parenteral epinephrine is not infrequent. Because there are no standardized protocols, guidelines would be required prior to incorporating desensitization into clinical practice. SMS La mia DOPA si chiama Julie Julie Wang e Hugh Sampson, Asian Pac J Aller Imm 2013 • Current evidence indicates that desensitization is possible for the majority of subjects who undergo oral immunotherapy • Adverse reactions are common, however, and thus safety concerns remain. Although the symptoms were often localized, systemic reactions requiring epinephrine were seen not only during the escalation phase, but also in association with home doses • Another unanswered question is whether tolerance induction is achievable. Studies showed that 21-65% of children were not able to maintain the clinical effects of OIT when treatment was discontinued • Optimization and standardization of protocols, along with additional assessments of safety are still needed before OIT, SLIT or EPIT can be approved for the routine management of individuals with food allergies SMS Dalla Teoria alla Pratica (italiana) Indagine Commissioni AA e ITS SIAIP, RIAP 2013 • La DOPA viene effettuata in 55 (!) centri di allergologia (nei prossimi anni avremo un sacco di pubblicazioni sulla DOPA Italiana) – Il 50% ha gestito meno di 20 pazienti, il 20% meno di 10 • Il 68% DOPA chiunque, anafilattici e non – Il 16% solo gli anafilattici – Il 16% solo i non anafilattici e che già tollerano piccole quantità di cibo – Il 33% esclude chi ha asma non controllato • Il 44% fa incrementare la dose solamente in ospedale • Il 52% utilizza l’ alimento cotto • Il 55% è disponibile, tramite telefono mobile, 24/24 ore • Il 35% ha chiesto l’ approvazione da parte del CE per effettuare la DOPA • L’ 83% fa firmare un consenso informato SMS «Comunicazione mio malgrado» Email di Iride Dello Iacono all’ APAL – 23 Feb 14 • «Cari Apalliani, mio malgrado debbo comunicare di aver chiuso la lista d'attesa per la DOPA del mio Centro. • Come molti di voi sanno, perchè mi conoscono, io sono già avanti negli anni di attività ed ho in attesa più bambini-ragazzi di quanti non ne riuscirò a smaltire nei prossimi 5-6 anni. • Inoltre, purtroppo, nessuno dei miei giovani collaboratori si è voluto interessare di questa pratica, non per incapacità, ma per mancata volontà di assunzione di rischi in tempi già durissimi per noi medici, dal punto di vista medico-legale.» Come dare loro torto? SMS Tanto per quantificare un po’ - 1 Marta Vazquez-Ortiz et al, CEA 2013 • 81 CM-allergic children aged 5–18 underwent a CM-OIT – 60 children (75%) had occasional symptoms which ceased over time. 86% of them reached complete desensitization (200 mL) – 20 children (25%) suffered frequent (78% of total reactions), more severe and unpredictable reactions, which persisted during follow-up or led to withdrawal (6 cases) • Cox proportional hazards multivariate regression model identified 3 variables (CM-sIgE >50 kU/l, CM-SPT >9 mm and Sampson’s severity grades 2, 3 and 4 at baseline food challenge) as independent risk factors of reactions persistence – The combination of 2 or 3 of these factors involved hazard ratios to develop persistent reactions of 2.26 (95% CI: 1.14–4.46; p = 0.019) and 6.06 (95% CI: 2.7–13.7; p < 0.001), respectively. SMS Tanto per quantificare un po’ - 2 Marta Vazquez-Ortiz et al, CEA 2013 • • Thirty-two per cent of reactions during IP coincided with dose increases, and 12% of reactions occurred in the setting of cofactors, affecting 47 children (58%) Cofactors identified (and number of children affected) were – – – – – – – – – • post-intake lying down (12) exercise (12) infection (11) emotional stress (8) asthma exacerbation (6) fasting (6) tiredness (5) using straw (1) and NSAID intake (1) Pertanto, il 56% delle reazioni non sono prevenibili Fifty-five patients (67.9%) had had NSAIDs 6 hours before or after CM dose without incidences SMS Tanto per quantificare un po’ - 3 Marta Vazquez-Ortiz et al, CEA 2013 • Group 1 included 60 patients (75% of all treated patients), who developed reactions only occasionally, mainly triggered by known cofactors and which ended to resolve over time. In them, our protocol could be considered safe and efficacious • On the other extreme, group 2 included 20 patients (25% of all treated children) and their reactions were frequent, more severe and mainly unpredictable, persisting over time or leading to withdrawal. In them, CM-OIT was insufficiently safe Tuttavia SMS La DOPA normalizza … Desensibilizzazione Orale Per Alimenti • Un grazie speciale per avermi reso «normale» SMS … non del tutto Desensibilizzazione Orale Per Alimenti • Severe anaphylaxis to sheep's milk cheese in a child desensitized to cow's milk through specific oral tolerance induction Tripodi et al, EAACI 2013 • Our paper reports a case of a 5-year-old girl with cow's milk allergy, who developed severe anaphylaxis after the ingestion of a croissant containing sheep's milk ricotta cheese, even though she had been previously desensitized to cow's milk through SOTI • We conclude that SOTI is a species-specific procedure and the induced tolerance to cow's milk doesn't necessarily provide protection against milk of other mammals • Therefore, children desensitized to cow's milk through SOTI should strictly avoid the intake of milk of other mammals, until tolerance to those kinds of milk is documented by an oral food challenge Episodio simile è capitato anche ad Andrea SMS Giusto una settimana fa DH di Allergologia Pediatrica, 16 Aprile 2014 • La Nonna di Annelie: – “Ieri Annelie ha preso la dose da 3 ml (solita da 4 settimane) e poco dopo ha presentato eritema periorale, prurito alle mani, poi asma. Ha assunto cetirizina e Ventolin, la situazione si è normalizzata. Nelle ultime 4 settimane le reazioni avverse si sono presentate 2 altre volte. Annelie aveva giocato e saltato con un’ amica fino a 2 ore prima di assumere la dose di latte. • Il Padre di Gennaro: – “Dopo circa un ora dalla somministrazione dei 15 ml di latte, ha cominciato a tossire (tosse da crisi d'asma) sempre con maggiore insistenza, per poi cominciare a lamentarsi di un restringimento alla gola e di avere difficoltà a respirare, e subito dopo un fortissimo prurito su tutto il corpo ed in particolar modo alla gola. Contemporaneamente al prurito sono comparsi 2 pomfi sul collo ed 1 sulla pancia, di piccola dimensione (pochi mm).” – Nei giorni successivi, Gennaro ha presentato episodi più lievi, ha sospeso la DOPA per 3 giorni e dopo 5 giorni dal primo episodio è stata fatta diagnosi di 5^ malattia da parte del pediatra curante SMS Ciro, 9 anni - 4 Ambulatorio, 18 Marzo 2014 • “Si consiglia di eseguire test di provocazione orale con un prodotto da forno contenente latte vaccino” – – – – – – • 100 ml di latte intero (3 gr di proteine) 60 grammi di farina 40 grammi di zucchero 1 cucchiaino di lievito per dolci ½ fialetta di aroma vaniglia (facoltativa) Cuocere in forno preriscaldato ventilato a 180° per 30 minuti L’ ha fatto e passato il 9 Aprile scorso SMS La svolta del Muffin Ania Nowak-Wegrzyn et al, JACI Agosto 2008 23/91 (25%) NON tollerano muffin e wafle 8/91 (9%) Æ Anafilassi con necessità di adrenalina 91 individui con età media di 6.6 anni (range 2.1 – 17.3) SMS I Magnifici 6 Obiettivi dell’ AIDS Alimenti Ipoallergenici Domestici Study 1. Valutare l’ effettiva importanza e necessità dell’ effetto matrice nella riduzione della allergenicità del latte vaccino e dell’ uovo baked, sperimentando la tollerabilità di latte e uovo al forno privi di grano 2. Valutare l’ esistenza di un fenotipo “tollerante” di bambino con APLV o APUG IgE-mediata in grado di tollerare sia il latte al forno che il parmigiano e il latte solo parzialmente idrolisato (per quanto riguarda l’ APLV), oppure l’ uovo al forno e l’ uovo bollito per 10 minuti (quindi una via di mezzo tra l’ uovo al forno e l’ uovo crudo) 3. Valutare il Valore Predittivo Negativo (VPN) del prick test con gli AIDs (100%?) 4. Valutare la possibilità di identificare valori cut off con Valore Predittivo Positivo (VPP) > 95% nei confronti dell’ AID con cui si esegue il prick test 5. Valutare il mantenimento nel tempo della tolleranza agli AIDs nel tempo e nelle varie situazioni che la vita può offrire (malattie, sforzi fisici, differenze di cottura occasionali) 6. Valutare se la tolleranza agli AIDs possa essere considerato un marker di precoce acquisizione della tolleranza all’ alimento “crudo” SMS AIDS al Latte – Feb 2014 Alimenti Ipoallergenici Domestici Study Parametro Positivi Negativi N°. Bambini = 24 n.a. n.a. Prick test con latte vaccino 24 n.a. Prick test con LFMG 17/23 6/23 Prick test con parmigiano 17/20 3/20 Prick test con latte HA 12/20 8/20 Prick test con LFSMG 7/10 3/10 17 7 n.a. TPO con LFMG 5/22 17/22 (77%) TPO con parmigiano 3/14 11 /14 (79%) TPO con latte HA 2/13 11/13 (85%) 6/8 2/8 (25%) TPO con latte vaccino Anafilassi entro 12 mesi TPO con LFSMG SMS Prick negativo = TPO negativo ? latte Prick test negativo TPO negativo/TPO effettuati LFMG (6) 5/5 Parmigiano (3) 3/3 Latte HA 1 (8) 6/6 LFSMG (3) 2/2 SMS Non va sempre così, almeno con l’ uovo Faraj et al, Allergy Asthma Clin Immunol. 2012 RESULTS • Fifty-eight patients had negative SPT to the heated milk or egg in a muffin. All of these children underwent OFC to the appropriate heated food in the outpatient clinic • Fifty-five of these patients tolerated the OFC. The negative predictive for the SPT with the extensively heated food product was 94.8% value Prick effettuato con una goccia di sospensione L’ heated food era uovo in questi 3 casi SMS La Grande Bugia …. la sua assunzione prolungata favorisce la successiva tolleranza al latte intero Kim et al Dietary baked milk accelerates the resolution of cow's milk allergy in children JACI 2011 SMS Disegno di studio originale ARRUOLATI (6 mesi-21 anni; diagnosi di APLV) Cortesia di ESCLUSI (malattia allergica non stabilizzata; GE Eosinofila; recente reazione al latte cotto) Marcello Bergamini CHALLENGE CON LATTE MOLTO COTTO (muffin) NEGATIVO POSITIVO DIETA DI ESCLUSIONE NUOVO CHALLENGE CON LATTE MOLTO COTTO DOPO 6 MESI … recruitment was unsuccessful, failing to enroll a single subject over 1 year RANDOMIZZAZIONE DIETA DI ESCLUSIONE NUOVI CHALLENGE CON LATTE MENO COTTO, POI CRUDO 1-3 pasti/die (prodotti commerciali a basso contenuto di latte) NUOVI CHALLENGE CON LATTE MENO COTTO POI CRUDO SMS Disegno di studio modificato (quadro d’insieme) ARRUOLATI (6 mesi-21 anni; diagnosi di APLV) ESCLUSI (malattia allergica non stabilizzata; GE Eosinofila; recente reazione al latte cotto) CHALLENGE CON LATTE MOLTO COTTO POSITIVO (BMR) DIETA DI ESCLUSIONE NUOVO CHALLENGE CON LATTE MOLTO COTTO DOPO 6 MESI TRANSIZIONE AL GRUPPO “BMT” NEGATIVO (BMT) 1-3 pasti/die (prodotti commerciali a basso contenuto di latte) Cortesia di Marcello Bergamini GRUPPO DI CONTROLLO “STORICO” (STESSI CRITERI DI INCLUSIONE) DIETA DI ESCLUSIONE CHALLENGE CON PIZZA AL FORMAGGIO DOPO 6 MESI >>> se tollera >>> CHALLENGE CON LATTE CRUDO CHALLENGE ESEGUITI SECONDO IL NORMALE “STANDARD OF CARE” SMS Chi s’ accontenta gode Kim et al, JACI 2011 SMS Errare è umano, perseverare … Dietary baked egg accelerates resolution of egg allergy in children - Leonard et al, JACI 2012 • Subjects in the active group were categorized as baked egg–tolerant or baked egg–reactive • Subjects tolerant to baked egg were advised to consume 1 to 3 servings of baked egg per day and avoid regular egg • Subjects ingesting baked egg were reevaluated every 3 to 12 months, and after 6 months or more were offered challenges to regular egg • Subjects reactive to baked egg were offered repeat challenges to baked egg after 12 months or more NEANCHE QUI C’E’ UN GRUPPO DI BAMBINI TOLLERANTI AL BAKED EGG A CUI SIA STATO DETTO DI NON MANGIARLO SMS Uno dei molti Avallamenti Julie Wang e Hugh Sampson, Asian Pac J Aller Imm 2013 • Oral immunotherapy with heatdenatured proteins is an option for the majority of children with milk and egg allergy • In a longitudinal study of milk-allergic and egg-allergic children who were including baked milk or egg products in their diet, many of these children experienced accelerated tolerance induction SMS Insistono, proprio facce toste LG BSACI su APLV, CEA 2014 • The addition of baked milk to the diet may accelerate the further development of tolerance, including to fresh milk • Consequently, once tolerance is established, greater exposure through ingestion of less processed cow’s milk according to the ‘milk ladder’ limited by the individual’s tolerance, can be encouraged (D) SMS Barbara e la DOPAIDS Una Idea Viterbese L’ ingestione dell’ alimento al forno velocizza l’ efficacia della DOPA ? • Bambini con tolleranza all' alimento al forno randomizzati a – DOPA più alimento al forno vs – DOPA senza alimento al forno • Ogni 3 mesi TPO con alimento crudo SMS Le Domande “Anticipate” Una Ottima Idea 1. prima, anni fa, ogni sintomo o quasi era suggestivo di allergia al latte...oggi, forse, siamo passati a non pensarci quasi più... ma qual è la reale stima dei veri allergici al latte oggi ?? – A seconda della nazione e del tipo di studio da 0.34% a 2.2% (Sicherer et al. JACI 2013) – Dal 2% al 3% nel 1° anno di vita secondo le LG BSACI sulla APLV (CEA, 2014) 2. quali sintomi sono assolutamente suggestivi e quali quelli per nulla ? – Anafilassi per la prima categoria e obesità per la seconda sono due esempi 3. quali gli step x la diagnosi? – Anamnesi, prick test, tpo 4. indagini? se si, quali? e in che sequenza? – Vedi domanda n. 3 5. sintomi fortemente suggestivi di allergia al latte: quando, avendo certi sintomi, devo pensare all’ allergia e quando mai (es stipsi...) – Vedi domanda n. 2 – Nb: l’ esempio circa il “mai” riportato nella domanda non è in linea con le migliori evidenze scientifiche pubblicate disponibili ad oggi SMS Tutti i pensieri intelligenti sono già stati pensati Occorre soltanto tentare di ripensarli Johann Wolfgang Goethe SMS Tanto per quantificare un po’ - 2 Marta Vazquez-Ortiz et al, CEA 2013 • Grading of Food-Induced Anaphylaxis According to Severity of Clinical Symptoms (Hugh Sampson, Pediatrics 2003 – grade 1 for localized skin symptoms – grade 2 for mild rhinoconjunctivitis, nausea or isolated vomiting – grade 3 for intense rhinoconjunctivitis, repetitive vomiting or anxiety – grade 4 for asthma symptoms, hoarseness, diarrhoea, mild hypotension or dysrhythmia – grade 5 for loss of bowel control, respiratory/cardiac arrest, loss of consciousness, severe bradycardia or hypotension SMS Tanto per quantificare un po’ - 3 Marta Vazquez-Ortiz et al, CEA 2013 • Most patients had a relative low number of reactions – Thus, the majority of reactions corresponded to a minority of patients, especially in MP • 91.3% of reactions affected a single organ – Multisystemic reactions occurred in 37 patients, being generally not severe – No relevant changes occurred in reactions severity between IP and MP • Grade 4 reactions were the most frequent, followed by grades 1 and 2 – Isolated mild asthma, the symptom most frequently detected, gathered 76% of reactions classified as grade 4 – One grade 5 reaction was recorded SMS
© Copyright 2026 Paperzz