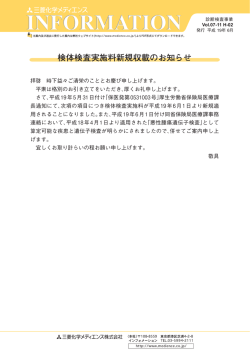
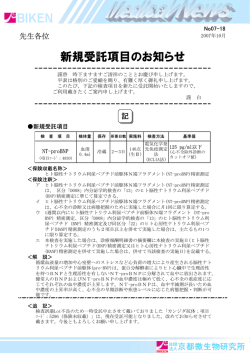
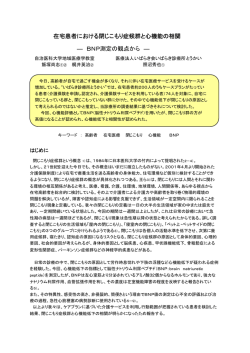
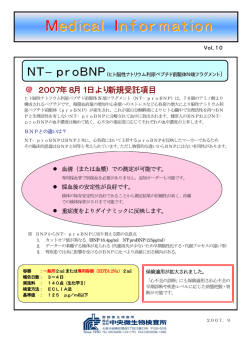
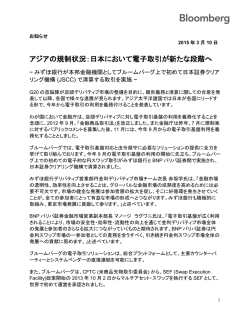
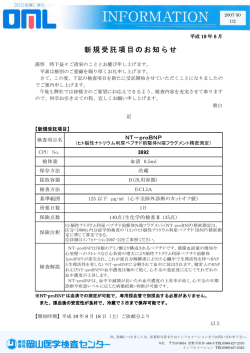
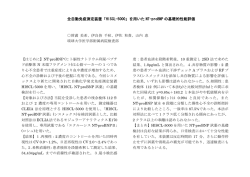
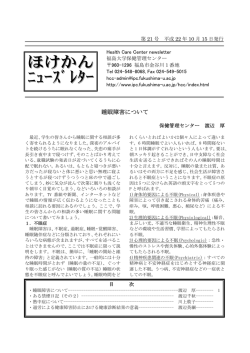
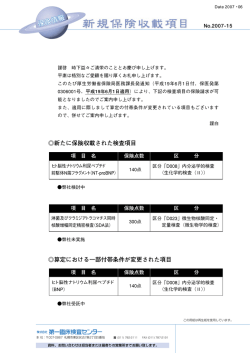
総 説 循環器疾患における血中BNP,NT-proBNP 測定 の意義 B-type natriuretic peptide (BNP) and N terminal -proBNP in cardiovascular disease 佐藤 幸人 * 藤原 久義 鷹津 良樹 Yukihito SATO, MD, FJCC *, Hisayoshi FUJIWARA, MD, FJCC, Yoshiki TAKATSU 兵庫県立尼崎病院循環器内科 要 約 「心不全に関する生化学指標のガイドライン」が,National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelineとして2007年に発表された.ガイドライン中では数ある心不全のバイオマーカーの候補の中から,心負荷 の指標としての血中 B-type natriuretic peptide(BNP) ,N terminal(NT) -proBNP 測定の有用性と,心筋障害の指標とし ての血中心筋トロポニン測定の可能性が論じられ,Class 分類とエビデンスレベル分類が試みられた.BNP,NT-proBNPが, 他の心不全のバイオマーカーと比較して圧倒的に論文数の多いバイオマーカーである理由としては,1)心不全の診断に有用, 2)心不全の予後予測指標として有用であること以外に,3)臓器,疾患特異的な指標であること,4)心不全の治療指標とし ての可能性が高いことなどが挙げられる.さらに救急疾患の多い循環器領域では迅速測定系が開発されたことによる影響も 大きい.NT-proBNPは,わが国では2007年7月より測定可能となったばかりであるが,欧米ではInternational NT-proBNP Concensus Panelとして,国際化統一を得ようとする動きもある.本稿ではこれら最新のガイドライン,コンセンサスパネル を基本としてBNP,NT-proBNPについて基礎知識,心不全患者での意義,冠動脈疾患患者での意義,一般住民での意義, さらには診察時検査(point of care test)について概説する. <Keywords> ナトリウム利尿ペプチド 心不全 狭心症 トロポニン 高血圧 はじめに J Cardiol Jpn Ed 2008; 2: 163 – 177 BNP,NT-proBNP が,他の心不全のバイオマーカーと比較 バイオマーカーは専門的技術がなくても客観的に疾患の して圧倒的に論文数の多いバイオマーカーである理由として 評価が可能な検査法のひとつであるが,循環器領域におけ は,1)心不全の診断に有用,2)心不全の予後予測指標と るバイオマーカーの検討は比較的新しい.昨年,急性冠症 して有用であること以外に,3)臓器,疾患特異的な指標で 候群と心不全領域におけるバイオマーカー測定についてのガ あること,4)心不全の治療指標としての可能性が高いこと イドラインが,National Academy of Clinical Biochemistry などがあげられる 2,3).さらに救急疾患の多い循環器領域で Laboratory Medicine Practice Guidelineとして初めて発表 は迅速測定系が開発されたことによる影響も大きい.NT- 1,2) された .「心不全に関する生化学指標のガイドライン」で proBNPは,わが国では昨年 7月より測定可能となったばか は,数あるバイオマーカーの候補の中から(表 1),心負荷 りであるが,欧米では International NT-proBNP Concen- の指標としての血中 B-type natriuretic peptide(BNP), sus Panelとして,その臨床意義にコンセンサスが得られつ N terminal(NT)-proBNP 測定の有用性と,心筋障害の指 つある 4).本稿ではこれら最新のガイドライン,コンセンサス 標としての血中心筋トロポニン測定の可能性が 論じられ, パネルを基本として BNP,NT-proBNPについて現在までの Class 分類とエビデンスレベル分類が 試みられた(表 2). 知見を述べる. * 兵庫県立尼崎病院循環器内科 1.BNP,NT-proBNP の基礎知識 660-0828 尼崎市東大物町 1-1-1 E-mail: [email protected] 2008年 5月20日受付,2008年7月4日改訂,2008年7月8日受理 BNP は 1988 年にブタの脳から分離され5),その後直ちに 主として心臓から分泌されることが判明した 6).BNP は通 Vol. 2 No. 3 2008 J Cardiol Jpn Ed 163 表 1 慢性心 不全のリスク評 価に検討されたバイオマーカー(文 献 2 より改変). 一般検査 Na,BUN,クレアチニン,ヘモグロビン,白血球数, アルブミン,ビリルビン,尿酸 れらの分子がどのような形で存在するのか詳しいことは不 明である10). BNP は血管拡張作用,ナトリウム利尿作用を持つペプ チドであるが交感神経系,レニンアンジオテンシン系に拮 抗する作用を有し,繊維化抑制作用もあわせ持つ 11).ナトリ 神経体液因子 ウム利尿ペプチド系には細胞内情報伝達に関わる2 つの受 カテコラミン(ノルエピネフリン,エピネフリン) レニン,ACE 活性,アンギオテンシン II,アルドステロン ナトリウム利尿ペプチド(ANP,BNP,CNP, N-terminal proANP,N-terminal proBNP) エンドテリン –1 バソプレッシン カルジオトロフィン –1 アドレノメデュリン,ウロテンシン –II 容体(natriuretic peptide receptor(NPR) -A,NPR-B)と ひとつのクリアランス受容体(C 受容体)がある11-13) (図 2). これらの受容体は主として血管平滑筋,心筋,腎尿細管上 皮細胞に存在し,BNP の作用は NPR-A受容体を介して細 胞内 cGMPを上昇させることにより発揮される.また BNP の血中からのクリアランスは,C 受容体を介して行われるほ か,腎近位尿細管,血管内皮にも認められる中性エンドペ 炎症性マーカー プチダーゼで分解を受ける. 高感度 CRP 可溶性 ST2 レセプター TNF– α,TNF– αレセプター IL–6 体内での生物学的半減期は BNP 約 20 分,NT-proBNP 約120 分であるが,採血後室温保存にて BNPは EDTA 添 加試験管内で数時間ほどは 90%安定しており,NT-proBNP は 72 時間安定である14).また BNP 測定の絶対値に関する 代謝マーカー 注意点として,測定系により使用している抗体が認識するエ レプチン アディポネクチン グレリン アペリン IGF–1 ピトープが異なるため 15),Biosite やAbbott の数値よりShionogiは 50%ほど低い数値が出る.このため,欧米の試験の 絶対値の解釈には注意を要する. BNP,NT-proBNP 値の修飾因子 心筋細胞構成蛋白 心筋トロポニン I,心筋トロポニン T BNP,NT-proBNPは基本的には心筋への壁応力を反映 するが,様々な因子により修飾を受ける.肥満は BNP,NTproBNP 値を低下させ 16,17) (ただし日本人で BMI30 以上の肥 常の状 態では 70%が心室由来で残りは心房由来とされ 7), 満はまれ 18)),心房細動 19),加齢 20),女性 20),腎機能悪 心房では顆粒として貯蔵されているが 8),心室に圧負荷が 化 21,22)は値を上昇させる.なかでも腎機能が与える影響に かかるとpre-proBNP1-134 の合成が直ちに開始される.pre- ついては従来,NT-proBNP は腎クリアランスなので腎機 proBNP1-134 は,切断されてproBNP1-108 となった後に,血中 能の影響を受けるが,BNP のクリアランスは C 受容体と中 に流出する際 BNP1-32 とNT-proBNP1-76 とに分かれるが,血 性エンドペプチダーゼの分 解によるので腎機能の影響は 中にはproBNP1-108 自体も存在する.さらに BNP1-32 は,B - 弱いとされてきた.しかし,BNP 値を説明する因子として, NP3-32 と一部は BNP 7-32 になる (図 1).生物学的活性は 心機能と腎機能を同時に解析した検討では,BNP 値は心 NT-proBNP1-76 には認めないが,BNP1-32 とBNP3-32 には認 臓への負荷と同様,腎機能の影響も受けており,NT-pro- める.BNP 測定値,NT-proBNP 測定値は以上の分子のい BNPよりは腎機能の影響は少ないものの,腎機能低下症例 くつかの総和を計測していると考えられており,BNP 測定 では少なからず腎機能に影響を受けることが判明した(図 系は BNP1-32 ,BNP3-32 ,proBNP1-108 を測定し,NT-proBNP 21,23,24) 3) .以上の修飾因子はそれぞれの疾患の診断,予後 測定系は,NT-proBNP1-76 とproBNP1-108 を測定しているとさ 推定においてカットオフ値に影響することが予想されるが, 7) 7) れている .しかし重症心不全患者の血中では BNP1-32 は検 すべての病態のカットオフ値について年齢,性 別,腎機 9) 能,心房細動の有無など別に値を設定することは現実的で 出されないという報告もあり ,それぞれの患者の状態でこ 164 J Cardiol Jpn Ed Vol. 2 No. 3 2008 循環器疾患における血中 BNP,NT-proBNP 測定の意義 表 2 心不全におけるバイオマーカー測定のガイドライン(文献 2 より改変). 心不全の初期評価 A.心不全診断 Class I 1. BNP,NT-proBNP を,急性心不全を疑う症状の患者に対し,診断,除外診断のために測定する(エビデンスレベル A) Calss IIa 1. BNP,NT-proBNP を,慢性心不全を疑う症状の患者に対し,除外診断のために測定する(エビデンスレベル C) Class III 1. 明らかに心不全の診断で間違いない患者に BNP,NT-proBNP を測定する(エビデンスレベル C) 2. 心不全の診断において BNP,NT-proBNP 測定は,臨床症状や他の心エコー,血行動態検査にとってかわるものではない(エ ビデンスレベル C) B.リスク評価 Martinez-Rumayor et al/ Biology of the Natriuretic Peptides 5A Table 1 IIa Class Important regulators of the B-type natriuretic peptide (BNP) gene* 1. BNP,NT-proBNP 測定は従来よりも詳細なリスク評価が求められるときに有用である(エビデンスレベル A) Stimulus Potential Effectors cis Elements 2. BNP,NT-proBNP を経過を追って採血し,その変化によりさらなるリスク評価する(エビデンスレベル B) -Adrenergic cAMP, Src, Rac, GSK3, CaMKII, PI3K GATA (85), MCAT (97 and 124) Class IIb agonist Interleukin-1 Ras, Rac, p38 MAPK, PKC MCAT (97) 1. 心筋トロポニン測定を心不全患者のリスク評価に用いる(エビデンスレベル B) Endothelin-1 Rac, Src GATA; region between 1818 and 408; TRE at 1000 Class III Stress Activators of MKK6 and p38 MAPK AP-1–like site at 111 Ischemic injury Unknown Region between 1. バイオマーカーを心不全患者のリスク評価のためだけに測定する(エビデンスレベル B) 408 and 100 Phenylephrine Calcineurin NF-AT at 927 Thyroid receptor TRE at 1000 Thyroid hormone (T3) 心不全の治療指標 Mechanical stretch p38 MAPK SSREs (652 to 633 and 162) Class AP-1 III activating protein–1; cAMP cyclic adenosine monophosphate; CaMKII calcium/calmodulin-dependent protein kinase-II; GSK3 glycogen synthase kinase–3; MAPK mitogen activated protein kinase; MCAT muscle-CAT binding site; MKK6 mitogen-activated protein kinase kinase 6; 1. BNP,NT-proBNP は intra,inter variation が大きい指標であるため,治療効果判定に使用するにはデータが不十分である(エ NF-AT nuclear factor of activated T cells; PI3K phosphatidylinositol 3-kinase; PKC protein kinase C; SSREs shear stress response elements; TRE ビデンスレベル B) TPA-response element. * The wide variety of factors with significant effects on BNP gene activity is reflected clinically in the broad array of disease states known to affect concentrations of BNP and N-terminal pro-BNP in patients. Figure 1. A paradigm for natriuretic peptide synthesis and release. BNP B-type natriuretic peptide; DPP-IV dipeptidyl peptidase–IV; NT-proBNP amino-terminal pro–B-type natriuretic peptide. から,BNP1-32,NT-proBNP1-76 までのプロセッシング 7). 図 1 Pre-proBNP1-134 were similar to recombinant proBNP1-108.59 These results were subsequently further confirmed in population testing, which demonstrated that a great percentage of circulating “NTproBNP” or “BNP” is, in fact, proBNP1-10860 (Figure 1). At present, it is hard to know exactly what forms of NP cent study has demonstrated that the peptidase meprin A, which is highly expressed in the kidney, also processes BNP1-32 to BNP7-32Vol. .63 2 No. 3 2008 J Cardiol Jpn Ed 165 There is mounting evidence that these different molecular forms of BNP have differential biologic activity in HF. nical Chemistry 52, No. 8, 2006 ntly associNT-proBNP rgely comthe use of bitors and was indesitive relasuch assowith the logy, presnd internal GTP Neutral endopeptidase cGMP Biological effects CNP nd bnp found ber filtration 0.34, P elationship NP or BNP NT-proBNP renal funcwith eGFR 59, 1.5% 1531 NPR–B S Institute, ion of NTn 3916). L (41–242). seline conP 0.0001). NP accordesented in y higher in mptomatic ysfunction, erial blood rillation at es was also y markers es (plasma e protein). univariate except for ma aldoste). NP concenDd, with r2 as continp between es, categoboth natri- ANP/BNP Guanylyl cyclase-A GTP cGMP NPR–C ANP>CNP>BNP Clearance receptor . hormone binding and clearance 図 2 BNP Figure 1:の受容体とクリアランス Natriuretic peptide 11) 1400 B-type natriuretic peptide (ng/L) NPR–A 1200 1000 800 600 400 200 0 No con BNP のクリアランスはクリアランスレセプター NPR-C を介する経路と,中性エンドペプチダーゼ GTP=guanosine triphosphate. GMP=guanosine monophosphate. Atrial heart による分解とがある.BNP は natriuretic peptide receptor(NPR)A に結合し,生物学的効 1532 (ANP) and brain natriuretic Massonpeptide et al.: B-Type Natriuretic Peptides in Heart Failure natriuretic peptide (BNP) bind to (n=7 果を発揮する. 1532 Masson et al.: B-Type Natriuretic Peptide natriuretic peptide receptor (NPR) A, a guanylyl cyclase receptor that GTP = guanosine triphosphate, GMP = guanosine monophosphate. mediates the biological effects of these peptides. The peptide is cleared via two mechanisms: binding to NPR-C and degradation by neutral The independent prognostic values o endopeptidase. Figure 2: BNP Thecon in NT-proBNP were tested separately in C dyspnoea NT-proBN and en models that included the demographic, c models th Data are median (IQ Natriuretic peptides relax vascular smooth muscle, causing cardiographic variables with a statist cardiogra with permission from at univariate a arterial and venous dilation and leading to reduced association blood with outcome associatio First, the natriuretic peptides and the 30,31 First, the pressure and ventricular preload. ANP and BNP also were entered as categorical variables, dic were ente have important central and peripheral sympathoinhibitory elderly havemoc or below the median value. or In these or below was the first predictor of outcome with h effects. Both hormones block cardiac sympathetic nervous such as pulmon was the fi CI) of32,33 2.07 (1.76 –2.46) for mortality, 2.2 CI) of 2.0 system activity, even when cardiac filling pressures fall. raised concentr M&M, and of 2.66 (2.19 –3.22) for hospi M&M, an (Fig. 4). Similarly,from BNP resulted as the st other These hormones also inhibit the renin-angiotensin(Fig.cau 4). S dent predictor of mortality [1.87 (1.59 –2 left-ventricular aldosterone axis: ANP infusion directly blocks secretion of dent pred (180 –2.34)], and hospitalization for HF [ (180 –2.34 ANP, with sen renin and aldosterone and further inhibits the stimulatory When the natriuretic peptides andaappro When 30,34,35 42,43the were considered as continuous variables of 80–90%. effect of angiotensin II on release of aldosterone. BNP were conT Fig. 2. Median plasma concentrations of NT-proBNP and BNP according value was consistent with the analysis Fig. 2. Median plasma concentrations of NT-proBNP and BNP according value has direct lusitropic (relaxing) properties in the of a series of wa sm Ventricular Ejection Fraction (LVEF),estimated glomerular filtration rate (eGFR) と B図 3 慢性心不全患者における Left to eGFR. cutoff values. For instance, an incremen to eGFR. cutoff va 36 NP,NT-proBNP 値 24). eGFR categories are based on the National Kidney Foundation classification of myocardium, commercially av and might have antiproliferative andNT-proBNP baseline concentration cor eGFR categories are based on the National Kidney Foundation classification of BNP,NT-proBNP 値ともに LVEF,eGFR の影響を受けている. baseline renal function. Vertical scale is different for NT-proBNP (black bars) and BNP 37,38 renal function. Vertical scale is different for NT-proBNP (black bars) and BNP increase of risk of 3.8% for mortality (P (white bars). The number of patients in each category is shown By above bars. recently been antifibrotic effects in vascular tissues. contrast with increase v o (white bars). The number of patients in each category is shown above bars. an increment of 50 ng/L of baseline BN an increm patients present ANP andprognostic BNP, CNP does not function as a circulating corresponded to an increase of risk of 5 value of bnp and nt-probnp correspon 39 prognostic value of bnp andas nt-probnp hormone, but acts locally in the vasculature a In this Similarly, increases of risk for study, M&M wer The adjusted hazard ratios for 急現場における急性心不全の診断についてであり,Nationdeath, M&M, or hospitalはない.特に緊急を要する急性心不全の診断におけるカッ Similarly The adjusted hazard ratios for death, M&M, or hospital40 3.0% and 5.7% for hospitalization for and ization HF according baseline deciles ofproliferation, NT-proBNP vasodilator andforinhibitor oftovascular cellHF patients with de and 3.0% ization for according to baselineand deciles of NT-proBNP トオフ値について,NT-proBNP 値では腎機能を考慮せず, al Academy of Clinical Biochemistry Laboratory Medi(P 0.0001 for all). Finally, the like and BNP are presented in Fig. 3. There was a similar (P 0.00 and BNP are presented in Fig. 3. There was a similar with know in the central nervous system, where it has several 25) showed that BNPthose or NT-proBNP pro progression in the probability of death withGuidelineでもClass increasing 年齢のみ考慮した値が提唱されている . cine Practice I,エビデンスレベルA showed progression in the probability of death with increasing 41 incremental prognostic value for the p heart failure exa functions.plasma concentration of NT-proBNP or BNP, with hazard 2) incremen plasma concentration.救急室における急性心不全の早期 of NT-proBNP or BNP, with hazard の扱いとなっている cause mortality, M&M, andor hospitaliza ratios in the tenth decile of 4.02 (2.63– 6.11) and 4.02 failure left-v cause mo ratios in the tenth decile of 4.02 (2.63– 6.11) and 4.02 2.急性心不全を対象とした測定(診断, 診断,リスク評価は,緊急を要する疾患であるという意味 with P 0.0001) compared with a mode (2.70 –5.99),リスク評価) respectively. Corresponding values for M&M withgrea P (2.70 –5.99), respectively. Corresponding values for M&M threshold graphic, echocardiographic, andof clinical were 4.74 (3.36 – 6.70) and 3.67で大変重要であり,実際に (2.70 – 4.98). An apparent BNP,NT-proBNPを救急の現 1)急性心不全の診断 graphic, e were 4.74 (3.36 – 6.70) and 3.67 (2.70 – 4.98). An apparent The predictiveBNP values of NT-proBNP superiorityto ofbe NT-proBNP over BNP for predicting the For a biomarker valuable in clinical should The pr superiority of practice, NT-proBNP it over BNP for predicting thedid better BNP,NT-proBNP の研究の中で最も確立した領域は救 場で臨床応用するためには迅速測定系の開発が必須であ compared by means of ROC curves (Ta risk of hospitalization for patients with HF was observed compared risk of hospitalization for patientsat withaHF was clinical observed judgmen be able across to be measured rapidly and accurately (SE) for NT-proBNP (0.679 [0.011]) was m the whole range of concentrations. For instance, the (SE) for N across the whole range information of concentrations. For instance, the Fig. 1. Median concentrations of baseline NT-proBNP and BNP by reasonable cost; add diagnostic or prognostic contributed exp than for BNP (0.665 [0.001]; P 0.073 relative risk of hospitalization for HF was higher in the quartiles of age, LVEF, and LVIDd. than for relative risk of hospitalization for HF was higher in the all-cause mortality. For M&M, NT-proBN tenth decile NT-proBNP [7.51 help (4.30 –13.11)] compared to Vol.available methods; guide [7.51 patient that incorporat Differences of median concentrations among quartiles wereof evaluated by theand all-cause tenth decile to of NT-proBNP (4.30 –13.11)] compared J Cardiol Jpn Ed 2 No. 3with 2008 166 [0.009]) had a statistically significant h Kruskal–Wallis test and were significant for age, that LVEF,of andBNP LVIDd[3.86 for both (2.56 –5.84)], although 95% confi[0.009]) h with that of BNP [3.86 (2.56most –5.84)], although 95% confimanagement. BNP and N-terminal BNP fulfil of history, examin peptides (all with P 0.00001). Vertical scale is different for NT-proBNP (black dence intervals (CIs) always overlapped. value than BNP [0.674 (0.009); P 0.033 bars) and BNP (white bars). The number of patients in each category is shown dence intervals (CIs) always overlapped. value tha Natriuretic peptides as cardiac biomarkers above bars. these criteria in patients with suspected heart failure. BNP especially usefu 循環器疾患における血中 BNP,NT-proBNP 測定の意義 NT-proBNP NT-proBNP NT-proBNP > < 300 pg/ml rule out NT-proBNP Gray zone rule in ** 図 4 急性の呼吸困難症状示す患者の診断アルゴリズム 29). < 50 歳:450 pg/ml,50-75 歳:900 pg/ml,> 75 歳:1,800 pg/ml. * 急性心不全の年齢補正 rule in 値. る.Breathing Not Properly試験において Maiselらは1,586 NT-proBNP(ICON)試験にて詳しく検討され,年齢により 例の急性の呼吸困難を主訴に救急受診した患者を対象に, カットオフ値を50 才以下450 pg/ml,50-75 歳 900 pg/ml, 臨床症状のみで診断するよりもTriage BNP(Biosite)を 75 歳以上 1,800 pg/mlとすることにより,positive predic- 組み合わせたほうがより正確に急性心不全の診断が可能な tive value を 90%近くまで上げることが可能なことが示さ ことを報告したが,BNPの急性心不全の診断におけるarea れた 28).図 4 に呼吸困難症状を呈する患者を対象にした, under the receiver-operating characteristic curve(AUC) 急性心不全の診断におけるNT-proBNP 測定のアルゴリズ 26) は 0.91とかなりよい数字であった .NT-proBNP(エクルー ムを示 す 29). 救 急 現 場での急性心 不 全の診 断における シスproBNP,Roche Diagnostics)についても同様の検討が BNP,NT-proBNP 値 の 解 釈 で 注 意 を 要 する点として, Januzziらによって行われ,ProBNP Investigation of Dysp- Flash pulmonary edemaでは発症が 1 時間前後と急激なた nea in the ED(PRIDE)試験における599 例の検討では, めに値が充分上昇しないことがある 30). NT-proBNP の急性心不全の診断におけるAUC は 0.94であ 2) “Gray zone”の解釈 り,臨床指標よりもより正確な急性心不全の診断が可能で “Gray zone”とは呼吸苦を主訴として救急室を受診した 27) あった .また,NT-proBNP の急性心不全の診断における 患者の,急性心不全 診断におけるrule inカットオフ値と rule out 値として,PRIDE 試験では NT-proBNP 値 300 pg/ rule out カットオフ値の間のことを言い,NT-proBNP 値で ml 以下では急性心不全の negative predictive valueは 99 は 300-900 pg/ml(50-75 歳)である 31).この間の数値の %と報告された.NT-proBNP の急性心不全の診断における 患者は明らかな急性心不全の可能性は低いが,急性心不全 rule in 値についてはさらに International Collaborative of の可能性を念頭において続いて検査を進めるべきであり, Vol. 2 No. 3 2008 J Cardiol Jpn Ed 167 NT-proBNP の数値自体も予後予測指標という情報を持った 慢性心不全の予後予測におけるBNP,NT-proBNP 測定の 29) 重要な数値である . 有用性については下記の薬剤多施設試験も含めて多くの報 3)急性心不全患者における予後予測能 告があり 38,39),ガイドラインでの扱いは Class IIa,エビデ ガイドラインでの扱いは Class IIa,エビデンスレベルAで ンスレベルAである 2). ある 2).BNP,NT-proBNP の予後予測能については,救急 慢性心不全,高血圧の薬剤多施設試験におけるBNP,NT- 室におけるBNP 値が 90日後の予後予測因子であることが proBNP Rapid Emergency Department Heart Failure Outpatient 近年の高血圧,慢性心不全の薬剤多施設試験ではサブ 32) Trial(REDHOT)により報告された .PRIDE 試験から 解析として BNP,NT-proBNPを測定している試験が増えつ は心エコーのEFと比較してもNT-proBNP 値が強い予後予 つある.これらの研究の内容は,小規模研究で既に証明さ 33) 測指標であることが示された .欧米では急性心不全の代 れていることの確認であることもあるが,新しい結果が出る 表的なレジストリーとして 15 万症例規模のAcute Decom- こともある.代表的なものを下記に示す. pensated Heart Failure National Registry(ADHERE) a)慢性心不全の薬剤多施設試験 があるが,このデータベースでもBNP 値は院内死亡の強い 現在までバイオマーカーについて検討している最も多い症 予後予測因子であった 34). 例数の慢性心不全薬剤多施設試験は,ARB バルサルタン 4)BNP,NT-proBNP 測定が入院日数に及ぼす影響 を用いたVal-HeFT(Valsartan Heart Failure Trial)であ B-type Natriuretic Peptide for Acute Shortness of る.約 4,000 例の慢性心不全患者についてBNP(Shiono- breath EvaLuation(BASEL)試験において Muellerらは gi),NT-proBNP(Roche)などのバイオマーカーが測定さ 呼吸困難にて救急室を受診した452 例の患者を対象に,救 れ,慢性心不全患者において観察開始時のBNP,NT-pro- 急室で迅速に BNPを測定することにより心不全の的確な評 BNPは強い予後予測指標であることが改めて確認された 価が可能になり,死亡率を増加させることなく入院日数と医 (観察開始時 BNP 中央 値 99 pg /ml ,NT-proBNP 中央 値 35) 療費を軽減できたと報告した .NT-proBNPについても同 24,40) 895 pg/ml) .重要なことは観察期間中のBNP 値の変化 様の検討が IMPROVE-CHF(Improved Management of 率が 慢 性心不全のハードエンドポイントであるall cause Patients With Congestive Heart Failure)試験にて行わ mortality and morbidityと相関したことである 38,40).このよ れ,60日間の医療コストが有意に減少した 36).しかし,こ うに臨床経過とバイオマーカーの変動が並行することは, れらの試験にも記載されているように,欧米の急性心不全 理想的なバイオマーカーの必須条件であるが 3),証明は意 の入院期間は 1 週間ほどと極端に短く,医療保険制度,社 外と困難で BNP以外のバイオマーカーでは証明されていな 会背景により医療コストの結果はかなり左右されると思われ い.Val-HeFT 試験ではランダム化前,ランダム化後 4,12 る. カ月後に心エコーも行われており,経過中のBNP の低下が 心エコーでのEF 改善と相関することも報告された 41).同様 3.慢性心不全の診断,リスク評価における測定 に BNP 値の変化と心エコー所見の改善が相関することを報 慢性心不全の診断におけるBNP,NT-proBNP 測定の有 告した他の試験としては,カンデサルタンとエナラプリルを 用性は Class IIa,エビデンスレベル Cとなっており,慢性 用いた Randomized Evaluation of Strategies for Left Ven- 2) 心不全の診断ではなく,除外に用いると表現されている . tricular Dysfunction(RESOLVD)がある 42).さらに血中 慢性心不全の場合,急性心不全と比較すると,患者の基礎 ノルエピネフリンや,血中レニン活性,血中アルドステロン 疾患や状態によって BNP,NT-proBNP 値が大きく異なる. 値などは古典的生化学指標として,慢性心不全患者の予後 そのため診断においてコンセンサスの得られる単一のカット 予測指標であることが報告されていたが,Val-HeFT 試験 オフ値を決定することは困難であるが,International NT- ではこれら古典的生化学指標と比較してもBNP 値が圧倒 proBNP Concensus Panelでは,慢性心不全症状を疑う外 的に強い予後予測指標であることが確認された 43). 来患者を対象にした場合,125 pg/mlのカットオフ値で neg- Carvedilol Prospective Randomized Cumulative Sur- 37) vival(COPERNICUS)は,慢性心不全患者におけるNT- ative predictive valueは約 97%であると報告している . 168 J Cardiol Jpn Ed Vol. 2 No. 3 2008 rt et al rt et al 循環器疾患における血中 BNP,NT-proBNP 測定の意義 NT-proBNP in Decompensated Heart Failure NT-proBNP in Decompensated Heart Failure 2171 2171 ication ication harge harge た.Carvedilol Or Metoprolol European Trial(COMET) 試験では1,559 例の患者で NT-proBNP が測定されたが(中 央値 1,242 pg/ml),β遮断薬投与後の観察期において NT- 95% CI 95% CI 42–1.12 42–1.12 99–1.04 99–1.04 66–1.72 66–1.72 47–1.22 47–1.22 86–2.24 86–2.24 proBNP 値が持続高値である患者の予後は悪く,NT-proBNP 値が低下した患者の予後はよいことが報告され,COPERNICUS で得られた知見が再確認された 46). b)高血圧の薬剤多施設試験 高血圧の多施設試験では心不全薬ほど詳細な検討はさ 65–2.70 65–2.70 67–3.03 67–3.03 80–3.88 80–3.88 81–1.009 81–1.009 79–1.018 79–1.018 09–1.051 09–1.051 95–1.006 95–1.006 75–1.28 75–1.28 37–1.077 37–1.077 00–1.05 00–1.05 16–8.35 16–8.35 23–0.74 23–0.74 52–1.42 52–1.42 62–1.68 62–1.68 23–3.71 23–3.71 29–3.82 29–3.82 05–1.020 05–1.020 12–1.024 12–1.024 れていないが,ARBロサルタンとβ遮断薬アテノロールを比 23–3.91 23–3.91 60–12.23 60–12.23 心不全患者では観察開始時の BNP,NT-proBNP 値よ ed in 25 d in 25 mission mission her than er than lization lization pg/mL; pg/mL; end of endwas of nts nts was 384.3 384.3 during during patients patients lization lization 432.7 432.7 較した Losartan Intervention For Endpoint Reduction in Hypertension(LIFE)試験のサブ解析では,NT-proBNP が,心肥大を伴った高血圧患者において心血管イベントの予 後予測因子であることが示され 47),治療効果判定について ロサルタン投与群で NT-proBNP 値が低下した 48).また高 血圧の試験ではないが,心不全を除いた心血管病変のハイ リスク患者を対象として,ACE 阻害薬ラミプリルを用いた Heart Outcomes Prevention Evaluation(HOPE)試験に おいてもNT-proBNP は心血管イベントの予後予測指標で あった 49).しかし,高血圧症例におけるBNP,NT-proBNP 測定の意義については心不全症例での測定と比較すると未 解決の部分が多く,今後の検討を待たねばならない 50). 4.慢性心不全,急性心不全治療指標としての可能性 について りも治療にて安定後の数値のほうが,予後予測能が高いこ Figure 1. Cumulative hospitalization-free survival according to ,退 図 5 心不全にて入院した患者の予後は入院時よりも(上段) Figure 1. Cumulative hospitalization-free survival6778.5 according to NT-proBNP plasma level at admission (median, pg/mL) NT-proBNP plasma level4137.0 at admission pg/mL) and discharge (median, pg/mL).(median, 6778.5 51) 院時の NT-proBNP 値(下段) のほうが予後と相関する . and discharge (median, 4137.0 pg/mL). とが知られている 51,52).特に急性心不全患者を対象にした proBNP の予後予測能が,多人数 (1,011例)で確認された 2 presents the Kaplan-Meier cumulative hospitalization最初の大規模試験である (NT-proBNP 値は平均 3,235 pg/ 2free presents Kaplan-Meier survivalthe curve according tocumulative the change hospitalizationin NT-proBNP. ml,中央値 1,767 pgaccording /ml) free survival curve to the change in NT-proBNP. Table 4 shows the final .多変量解析の結果,NT-promultivariate Cox regression model Table 4 shows the final multivariate Cox regression model performed by a stepwise method starting with all variables BNP 高値,カルベジロール投薬の有無,低血圧,心不全 performed by a stepwise starting with all variables that in univariate analysis method were significantly associated with 入院の既往は独立した予後予測因子であり,なかでもNTthat in univariate were significantly associated with a higher hazard ofanalysis dying or being readmitted. 44) proBNP .さらに観察期間 a higher hazard dying being Whenの予後予測能は強力であった death asofthe onlyor end pointreadmitted. was analyzed, the results When death as the only end point was analyzed, the results 3,6カ月後においてカルベジロールが の経時的 were very similar, except that age andNT-proBNP atrial fibrillation were were very similar, except that age and atrial fibrillation were 45) significant predictors of death in univariate analysis. The な数値を抑制することが確認された .本試験の結果によ significant in univariate analysis. The multivariatepredictors model forofthedeath explanation of death is shown in り,従来β遮断薬投与後数週間は BNP,NT-proBNP の上 multivariate model for the explanation of death is shown in Table 4. Table 4. 昇がみられることが報告されていたが,長期的な予後改善 のNT-proBNP値のほうが著明に予後予測因子として強い Discussion に伴って数カ月後にはこれらの指標も低下すると解釈され These results stronglyDiscussion suggest that variations in NTThese suggest that variations in NTproBNPresults levelsstrongly during hospitalization and predischarge proBNP levels during hospitalization and predischarge NT-proBNP levels are predictors of hospital readmission NT-proBNP levels are predictors of hospital readmission and death within 6 months of discharge of hospitalized HF and death within 6 months of discharge of hospitalized HF patients. Thus, measurement of NT-proBNP is potentially patients. Thus, measurement of NT-proBNP is potentially als.org by TADASHI MIYAMOTO on October 6, 2008 ls were ls were scharge scharge adverse adverse levels, levels, ization, ization, Figure Figure 場合その傾向が強く,Bettencourtらの急性心不全患者を 対象にした報告でも入院時のNT-proBNP 値よりも退院時 51) (図 5) .この事実は BNP,NT-proBNP が治療効果と平 行して変動しており,治療効果判定に使用可能な指標であ ることを強く示唆している.しかしBNP,NT-proBNP 測定 が心不全領域において診断,予後推定に有用であるという ことはガイドラインレベルでも異論のないところであるが, 治療効果判定としての使用法については,1)絶対値の持つ 意味が個人により異なる,2)生物学的変動(Biologic variability)が NT-proBNP で 20%,BNP で 30%と大きい 53),3) 使用する測定系により絶対値が異なる,4)β遮断薬導入直 後は数値が上昇することがある 54),5)BNP,NT-proBNP Vol. 2 No. 3 2008 J Cardiol Jpn Ed 169 の変動を 「前値との差」で治療効果を評価するのか,「前 当初より母集団の患者の重症度により結果が異なることが 値との比」で評価するのか定まっていない,6)biochemical 予想されていた.多施設試験 STARS-BNP(Systolic Heart responder,non responderと予後との直接の相関をみた報 Failure Treatment Supported by BNP)では EF < 45%の 告数がまだ十分でないなどの理由により,National Acade- 慢性心不全患者 220 例が,標準治療群とBNP 値ガイド群 my of Clinical Biochemistry Laboratory Medicine Prac- (Biocite Triage BNP < 100 pg/ml が目標)に振り分けら tice GuidelineでもClass III,エビデンスレベルB の扱いと れ,BNP ガイド群では心不全死と心不全入院の減少がみら 2) なっている . れた 61).BNP ガイド群では ACE 阻害薬,β遮断薬が有意 Chengらは退院時,自覚症状が改善していてもBNP 値に に多く処方されていたが,観察終了時に両群に体重差は認 改善がみられない乖離現象を示す患者の予後は不良である められなかった.また,BNP ガイド群では観察開始時 352 55) と述べた .Millerらは急性心不全患者を対象にNT-pro- ±260 pg/mlであった BNP 値 は 3カ月後 284 ±180 pg/ml BNPを経時測定したが,全例治療により自覚症状の改善が まで減少したが,実際に BNP < 100 pg/mlまで低下した患 得られた患者群であったにもかかわらず, biochemical res- 者の割合は,観察開始時16%,3カ月後で 33%であった. ponder(確立された定義はないが,彼らの検討では前値よ Strategies for Tailoring Advanced Heart Failure Regi- り20%以上の数値の低下をbiochemical responderとしてい mens in the Outpatient Setting: Brain Natriuretic Pep- る)の割合は 30%と著明に低かったことを報告し,その考 tide Versus the Clinical Conges Tion Score(STAR- 察の中でも「自覚症状の改善とbiochemical responder の BRITE)試験では BNP ガイド群に有用な結果は得られな 56) 驚くべき乖離」と表現している .Bettensourt,Januzziら かったが(2006 年AHAシカゴでの口頭発表より),EF < は NT-proBNPコンセンサスパネルの中で,急性心不全で 35%という重症患者が対象であったことが,良い結果が得 は前値の 30%以上のNT-proBNP の低下を目標とすると述 られなかった原因の可能性もある 62).NT-proBNP ガイド べている 57).今後,慢性心不全,急性心不全の治療指標と 治 療 の 多施 設 試 験としては NT-proBNP-Assisted Treat- して BNP,NT-proBNPを測定するためには,生物学的変 ment to Lessen Serial Cardiac Readmission and Death 動以上の数値の変化をbiochemical responderとする形で, (BATTLESCARRED)が進行中である 63). 学会レベルでのコンセンサスが必要と考えられる. 5.急性冠症候群,狭心症における測定 心不全関連イベントの予防を目的とした外来での BNP,NT- 心筋梗塞患者で血中 BNP が早期より検出されるという proBNP ガイド治療の可能性について 報告は古く,Moritaらは心筋梗塞患者で血中 BNP が数時 慢性心不全患者は経過中に入退院を繰り返して状態が 間後より上昇し,重症患者では 2 峰性になることを報告し 58) 悪化してゆく .従って入院回避のためのシステム構築が た 64).その後,心筋梗塞後 3,4 週間後のBNP 値が平均約 必要であるが,学問的というよりは社会的な要素も強くなり, 5 年の観察期間という長期予後予測因子であることも報告さ 59) 論文として発表が困難な領域である .Throughtonは 69 れ 65),第 1ピークは虚血に対する急性反 応を反映して IL- 例のLVEF < 40%の慢性心不全患者について,外来におい 1β,エンドテリン-1,アンジオテンシンII が BNP 産生の刺 て NT-proBNP < 200 pmol/ℓ(約1,680 pg/ml)を目標とし 激因子であり,第 2ピークは心筋リモデリングによる心負 て治療した NT-proBNP ガイド群と従来の臨床評価のみで 荷を反映すると考察された.Omlandらの急性冠症候群に 治療した群の経過を観察し,NT-proBNP ガイド群のほう おける検討では,NT-proBNP の上昇は心不全を認めない が,心血管イベントの有意な減少が得られたと報告した. 患者においてもみられ,Killip 分類とは独立した予後予測 NT-proBNP ガイド群では ACE 阻害薬,ループ利尿薬,ス 指標であった 66). ピロノラクトンの処方が多かったが,LVEFの改善は両群と 欧米の多施設試験では非 ST上昇型心筋梗塞を中心に検 60) も同程度であった .しかし,実際の臨床では予後不良患 討され,Orbofiban in Patients with Unstable coronary Syn- 者の場合,低血圧や腎機能の悪化によりBNP,NT-proB- dromes-Thrombolysis In Myocardial Infarction(OPUS- NP 値の目標数値にまで到達不可能なことも多い.従って, 67) TIMI)16(BNP 測定) ,Treat Angina with Aggrastat 170 J Cardiol Jpn Ed Vol. 2 No. 3 2008 循環器疾患における血中 BNP,NT-proBNP 測定の意義 and determine Cost of Therapy with an Invasive or CommitteeによるとBNP,NT-proBNP の正常値は年齢, Conservative Strategy-Thrombolysis In Myocardial In- 性別に健常者の 97.5th パーセンタイル値を用い,各測定系の 68) farction(TACTICS-TIMI)18(BNP測定) ,Fragmin and ばらつきを示す% coefficient variation(CV)は 15%以下と Fast Revascularization During Instability in Coronary なっている 78).日本でのNT-proBNP の 2007年 6月からの 69) Artery Disease(FRISC)II(NT-proBNP 測定) ,Global 改定添付文書では正常値について,35.1±12.5 歳で男女と Utilization of Strategies to Open occluded arteries(GU- も55 pg/mlと記載されている 79).一方,正常値に近い数値 70) STO)IV(NT-proBNP 測定) ,Platelet Receptor Inhibi- の差でもBNP,NT-proBNP 値は将来の心血管イベントの tion in Ischemic Syndrome Management(PRISM) (NT- 予測因子であることが最近報告された.フラミンガムオフス 71) proBNP 測定) 試験などのサブ解析として BNP,NT-pro- プリング研究の第 6サイクル目の調査に参加した 3,346 例の BNP が測定された.いずれも急性冠症候群において BNP, 被験者において,BNP が高値であるに従い将来の死亡,初 NT-proBNPは心筋トロポニンとは独立した予後予測指標で 回の重篤な心血管イベント,心不全,心房細動,脳卒中発 あるとの結果が多い.FRISC-II では 2日,6 週間,3カ月, 作または一過性脳虚血発作は有意に増加した 80).NT-pro- 6カ月後の採血も行われ,NT-proBNP 値は慢性期の値ほど BNP についても同様の報告があるが 81),いずれも心不全 強い予後予測指標であることが示されている 69).また GU- の診断,予後予測,治療効果判定における値とは異なり, STO IVなどでは NT-proBNP 値が高値であれば侵襲的冠 BNP 値で 20 pg/ml 前後以下,NT-proBNP 値で100 pg/ml 動脈インターベンションの効果が高いことが示された 72,73) . 急性 冠症候群の病態には炎症も含まれるが,血中 CR P 前後以下の低い値での検討である.これらの結果からも, 真の基準値は健常人より算出すべきと考えられる. も急性 冠症候群において予後予測因子である.Morrow, Braunwaldらは急性冠症候群において,心筋障害の指標 7.左室拡張機能障害とBNP,NT-proBNP (トロポニン),心筋負荷の指標(BNP,NT-proBNP),炎 左室拡張機能障害による心不全は,心不全患者の約半 症の指標(hs-CRP,CD40L),動脈硬化促進の指標(Hb- 数にみられ,高齢の女性に多く高血圧の合併も多い 82).予 A1c,血糖),血管損傷の指標(クレアチニンクリアランス, 後は不良で,心不全入院や死亡率は左室収縮機能障害より 微量アルブミン尿)などを組み合わせてマルチマーカースト わずかによい程度であり,左室収縮機能障害の患者の予後 ラテジーとしてリスク評価することを提唱している 74).急性 は年代を追って少し改善しているが,拡張機能障害の患者 冠症候群におけるバイオマーカーガイドラインにおいて,ト ではあまり改善していない 83). ロポニンの他に BNP,NT-proBNPを測定しリスク評価に用 拡張機能障害におけるBNP,NT-proBNP 値は収縮機能 いることは Class IIa,エビデンスレベルAとなっているが, 障害と比較してはやや低値であるが 84),壁応力を反映してお 測定のタイミング,リスク評価におけるカットオフ値について り 85),収 縮機能障害時と同様に予後規定因子である 86,87). は今後の検討を要する1). しかし,実際の臨床で拡張機能障害におけるBNP,NT- 安定狭心症患者については運動負荷による虚血により, 75) proBNP 値をどのように使用するかは,収縮機能障害におけ BNP が一過性に上昇するとの報告もあるが .Kragelund るBNP,NT-proBNP 測定ほど明確になっていない.また らは安定狭心症患者において左室機能とは無関係に NT- Redfieldらの一般住民を対象とした報告では BNP の拡張機 76) proBNP が将来の総死亡の予測指標であることを述べ , 能障害の検出感度,特異度はそれぞれ 75%,69%と大変低 Bibbins-Domingoらは 左 室収 縮 機 能, 拡 張 機 能,CRP, く,BNP 測定単独で拡張機能障害の検出は不可能と推測 心筋トロポニン T などを補正しても,NT-proBNP が安定狭 できる 88). 心症患者において心血管イベントの予測指標であることを報 現状では BNP,NT-proBNP 値自身は左室収縮機能障害, 77) 告した . 拡張機能障害を区別できないが,心エコー所見にて左室収 縮機能が保たれているにもかかわらず BNP,NT-proBNP 6.一般住民における測定と,正常値 値が高い場合は,拡張機能障害を疑う根拠になると思わ National Academy of Clinical Biochemistry and IFCC れる 89).また,カンデサルタンを用いた心不全の大規模試 Vol. 2 No. 3 2008 J Cardiol Jpn Ed 171 験であるCHARM(Candesartan in Heart Failure: Assess- は全血で BNP 測定が可能な機器である102).また Cardiac ment of Reduction in Mortality and morbidity)試験の Reader NT-proBNP(Roche Diagnostics) は全 血を専用 preservedアームの心エコーサブ解析では,心エコーにて のキットに滴下して 15 分後に実数が表示される小型機器で mitral inflow pattern が 正 常 の 場 合,pseudnormal pat- ある.従来のエクルーシスNT-proBNP(電気化学発光免疫 ternと鑑別するために NT-proBNPを測定している 90). 測定法,測定 範囲 5-35,000 pg/ml,total interassay CV は 217 pg/mlで4.8%,4,261 pg/mlで 2.1%)と比較すると 8.心 不全患者のリスク評価における心筋トロポニン との同時採血について Cardiac Reader NT-proBNPは(イムノクロマトグラフィー 臨床において心筋トロポニン T(cTnT),心筋トロポニ pg/mlで12.8%,1,166 pg/mlで 8.6%)とやや表示範囲が狭 ンI(cTnI)測定の最も重要な使用方法は急性心筋梗塞の く精度が悪いものの,実際の臨床現場でのエクルーシス 1) 法,測定範囲 60-3,000 pg/ml,total interassay CV は 163 早期診断,リスク層別化であるが ,近年その測定感度の NT-proBNP 値とCardiac Reader NT-proBNP 値の相関は 高さから心不全患者においても微小心筋傷害を検出できる r=0.96と非常に良好であった 103).日本では NT-proBNP 測 ことが 報 告されている 2,91,92) .慢性心不全患者において, 定についてCardiac Readerをさらに小型化させたハンディ cTnT,cTnI は心不全の原因に関係なく,BNP,NT-pro- タイプのコバス h 232(重量 650 g 充電可能)が,BNP 測 BNPとは独立した予後予測因子であることが報告されてお 定についてはシオノスポット(塩野義製薬株式会社,重量 り 93-95) ,最近慢性心不全治療薬の多施設試験であるVal- sartan Heart Failure Trial(Val-HeFT)のサブ解析でも, 96) 同様の結果が報告された (この解析には従来の cTnTの ほか,precommercial assayであるhigh sensitive(hs) -TnT も測定されており,非常に低濃度のhs-TnT でも予後予測指 標であることが示されている).また急性心不全においても 同様に cTnT が BNP,NT-proBNPとは独立した予後予測 因子であることが,急性心不全のレジストリーであるADHERE 97)やPRIDE 試験のサブ解析のデータ 98)から示され ている.現在のところガイドラインでは心不全患者のリス ク評価に cTnT,cTnIを測定することは Class IIb,エビデ ンスレベルBとなっているが 2),将来は Peacock やBraunwaldらが最近 New England Journal of Medicineで述べて いるように心不全の一般検査となる可能性もあると思われ る 99,100). 9.迅速小型測定機器の開発 他疾患における生化学指標と異なり,循環器領域では急 性心筋梗塞,急性心不全など急性期に直ちに病態を評価 し,治療を開始する必要があるため,迅速測定機器の開発 が必須であった 101).Biosite Triage BNP(日本では使用で きない)やエクルーシスNT-proBNPはその迅速さから多く の臨床研究で用いられてきたが,最新機器に求められる機 能として重要なものに「迅速性」に加えて,「簡便性」「携 帯性」などがある.PATHFAST(三菱化学メディエンス) 172 J Cardiol Jpn Ed Vol. 2 No. 3 2008 2.1 Kg,BNP 測定,充電可能)が発売されており,救急現 場や一般外来での診察時検査(point of care test)として の使用が期待される. 文 献 1) Morrow DA, Cannon CP, Jesse RL, Newby LK, Ravkilde J, Storrow AB, Wu AH, Christenson RH. National Academy of Clinical Biochemistry. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: Clinical characteristics and utilization of biochemical markers in acute coronary syndromes. Circulation 2007; 115: e356-e375. 2) Tang WH, Francis GS, Morrow DA, Newby LK, Cannon CP, Jesse RL, Storrow AB, Christenson RH, Apple FS, Ravkilde J, Wu AH. National Academy of Clinical Biochemistry Laboratory Medicine. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: Clinical utilization of cardiac biomarker testing in heart failure. Circulation 2007; 116: e99-e109. 3) Anand IS, Florea VG, Fisher L. Surrogate end points in heart failure. J Am Coll Cardiol 2002; 39: 1414-1421. 4) Januzzi JL, Richards AM, for the International NT-proBNP Consensus Panel. Introduction. Am J Cardiol 2008; 101: 1A-2A. 5) Sudoh H, Kangawa K, Minamino N, Matsuo H. A new natriuretic peptide in porcine brain. Nature 1988; 332: 78-81. 6) Saito Y, Nakao K, Itoh H, Yamada T, Mukoyama M, Arai H, Hosoda K, Shirakami G, Suga S, Minamino N, Brain natriuretic peptide is a novel cardiac hormone. Biochem Biophys Res Commun 1989; 158: 360-368. 7) Martinez-Rumayor A, Richards AM, Burnett JC, Januzzi JL Jr. Biology of the natriuretic peptides. Am J Cardiol 循環器疾患における血中 BNP,NT-proBNP 測定の意義 2008; 101: 3A-8A. 8) Hasegawa K, Fujiwara H, Itoh H, Nakao K, Fujiwara T, Imura H, Kawai C. Light and electron microscopic localization of brain natriuretic peptide in relation to atrial natriuretic peptide in porcine atrium. Immunohistocytochemical study using specific monoclonal antibodies. Circulation 1991; 84: 1203-1209. 9) Hawkridge AM, Heublein DM, Bergen HR 3rd, Cataliotti A, Burnett JC Jr, Muddiman DC. Quantitative mass spectral evidence for the absence of circulating brain natriuretic peptide (BNP -32) in severe human heart failure. Proc Natl Acad Sci U S A 2005; 102: 17442-17447. 10) Hammerer-Lercher A, Halfinger B, Sarg B, Mair J, Puschendorf B, Griesmacher A, Guzman NA, Lindner HH. Analysis of Circulating Forms of proBNP and NTproBNP in Patients with Severe Heart Failure. Clin Chem 2008; 54: 858-865. 11) De Lemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet 2003; 362: 316-322. 12) Suga S, Nakao K, Hosoda K, Mukoyama M, Ogawa Y, Shirakami G, Arai H, Saito Y, Kambayashi Y, Inouye K, Imura H. Receptor selectivity of natriuretic peptide family, atrial natriuretic peptide, brain natriuretic peptide, and C-type natriuretic peptide. Endocrinology 1992; 130: 229-239. 13) Mukoyama M, Nakao K, Hosoda K, Suga S, Saito Y, Ogawa Y, Shirakami G, Jougasaki M, Obata K, Yasue H. Brain natriuretic peptide as a novel cardiac hormone in humans. Evidence for an exquisite dual natriuretic peptide system, atrial natriuretic peptide and brain natriuretic peptide. J Clin Invest 1991; 87: 1402-1412. 14) Yeo KT, Wu AH, Apple FS, Kroll MH, Christenson RH, Lewandrowski KB, Sedor FA, Butch AW. Multicenter evaluation of the Roche NT-proBNP assay and comparison to the Biosite Triage BNP assay. Clin Chim Acta 2003; 338: 107-115. 15) Apple FS, Panteghini M, Ravkilde J, Mair J, Wu AH, Tate J, Pagani F, Christenson RH, Jaffe AS; Committee on Standardization of Markers of Cardiac Damage of the IFCC. Quality specifications for B-type natriuretic peptide assays. Clin Chem 2005; 51: 486-493. 16) Daniels LB, Clopton P, Bhalla V, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu AH, Steg PG, Westheim A, Knudsen CW, Perez A, Kazanegra R, Herrmann HC, McCullough PA, Maisel AS. How obesity affects the cutpoints for B-type natriuretic peptide in the diagnosis of acute heart failure. Results from the Breathing Not Properly Multinational Study. Am Heart J 2006; 151: 999-1005. 17) Horwich TB, Hamilton MA, Fonarow GC. B-type natriuretic peptide levels in obese patients with advanced heart failure. J Am Coll Cardiol 2006; 47: 85-90. 18) Iwanaga Y, Kihara Y, Niizuma S, Noguchi T, Nonogi H, Kita T, Goto Y. BNP in overweight and obese patients with heart failure: an analysis based on the BNP-LV diastolic wall stress relationship. J Card Fail 2007; 13: 663-667. 19) Knudsen CW, Omland T, Clopton P, Westheim A, Wu AHB, Duc P, McCord J, Nowak RM, Hollander JE, Storrow AB, Abraham WT, McCullough PA, Maisel A. Impact of atrial fibrillation on the diagnostic performance of B-type natriuretic peptide concentration in dyspneic patients. An analysis from the Beathing Not Properly Multinational Study. J Am Coll Cardiol 2005; 46: 838-844. 20) Redfield MM, Rodeheffer RJ, Jacobsen SJ, Mahoney DW, Bailey KR, Burnett JC. Plasma brain natriuretic peptide concentration: Impact of age and gender. J Am Coll Cardiol 2002; 40: 976-982. 21) Forfia PR, Watkins SP, Rame JE, Stewart KJ, Shapiro EP. Relationship between B-type natriuretic peptides and pulmonary capillary wedge pressure in the intensive care unit. J Am Coll Cardiol 2005; 45: 1667-1671. 22) McCullough PA, Duc P, Omland T, McCord J, Nowak RM, Hollander JE, Herrmann HC, Steg PG, Westheim A, Knudsen CW, Storrow AB, Abraham WT, Lamba S, Wu AH, Perez A, Clopton P, Krishnaswamy P, Kazanegra R, Maisel AS; Breathing Not Properly Multinational Study Investigators. B-type natriuretic peptide and renal function in the diagnosis of heart failure: an analysis from the Breathing Not Properly Multinational Study. Am J Kidney Dis 2003; 41: 571-579. 23) Tsutamoto T, Wada A, Sasaki H, Ishikawa C, Tanaka T, Hayashi M, Fuijii M, Yamamoto T, Dohke T, Ohnishi M, Takashima H, Kinoshita M, Horie M. Relationship between renal function and plasma brain natriuretic peptide in patients with heart failure. J Am Coll Cardiol 2006; 47: 582-586. 24) Masson S, Latini R, Anand IS, Vago T, Angelici L, Barlera S, Missov ED, Clerico A, Tognoni G, Cohn JN; Val-HeFT Investigators. Direct comparison of B-type natriuretic peptide (BNP) and amino-terminal proBNP in a large population of patients with chronic and symptomatic heart failure: The Valsartan Heart Failure (Val-HeFT) data. Clin Chem 2006; 52: 1528-1538. 25) DeFilippi C, van Kimmenade RR, Pinto YM. Amino-terminal pro-B-type natriuretic peptide testing in renal disease. Am J Cardiol 2008; 101: 82A-88A. 26) Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu AH, Clopton P, Steg PG, Westheim A, Knudsen CW, Perez A, Kazanegra R, Herrmann HC, McCullough PA; Breathing Not Properly Multinational Study Investigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002; 347: 161-167. 27) Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, Tung R, Cameron R, Nagurney JT, Chae CU, Lloyd-Jones DM, Brown DF, Foran-Melanson S, Sluss PM, Lee-Lewandrowski E, Lewandrowski KB. The N-terminal Pro-BNP investigation of dyspnea in Vol. 2 No. 3 2008 J Cardiol Jpn Ed 173 the emergency department (PRIDE) study. Am J Cardiol 2005; 95: 948-954. 28) Januzzi JL, van Kimmenade R, Lainchbury J, Bayes-Genis A, Ordonez-Llanos J, Santalo-Bel M, Pinto YM, Richards M. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: the International Collaborative of NT-proBNP Study. Eur Heart J 2006; 27: 330-337. 29) Januzzi JL Jr, Chen-Tournoux AA, Moe G. Amino-terminal pro-B-type natriuretic peptide testing for the diagnosis or exclusion of heart failure in patients with acute symptoms. Am J Cardiol 2008; 101: 29A-38A. 30) Daniels LB, Maisel AS. Natriuretic peptides. J Am Coll Cardiol 2007; 50: 2357-2368. 31) Van Kimmenade RR, Pinto YM, Januzzi JL Jr. Importance and interpretation of intermediate (gray zone) amino-terminal pro-B-type natriuretic peptide concentrations. Am J Cardiol 2008; 101: 39A-42A. 32) Maisel A, Hollander JE, Guss D, McCullough P, Nowak R, Green G, Saltzberg M, Ellison SR, Bhalla MA, Bhalla V, Clopton P, Jesse R; Rapid Emergency Department Heart Failure Outpatient Trial investigators. Primary results of the Rapid Emergency Department Heart Failure Outpatient Trial (REDHOT). J Am Coll Cardiol 2004; 44: 1328-1333. 33) Chen AA, Wood MJ, Krauser DG, Baggish AL, Tung R, Anwaruddin S, Picard MH, Januzzi JL. NT-proBNP levels, echocardiographic findings, and outcomes in breathless patients: results from the ProBNP Investigation of Dyspnoea in the Emergency Department (PRIDE) echocardiographic substudy. Eur Heart J 2006; 27: 839-845. 34) Fonarow GC, Peacock WF, Phillips CO, Givertz MM, Lopatin M; ADHERE Scientific Advisory Committee and Investigators.Admission B-type natriuretic peptide levels and in-hospital mortality in acute decompensated heart failure. J Am Coll Cardiol 2007; 49: 1943-1950. 35) Mueller C, Scholer A, Laule-Kilian K, Martina B, Schindler C, Buser P, Pfisterer M, Perruchoud AP. Use of B-type natriuretic peptide in the evaluation and management of acute dyspnea. N Engl J Med 2004; 350: 647-654. 36) Moe GW, Howlett J, Januzzi JL, Zowall H; Canadian Multicenter Improved Management of Patients With Congestive Heart Failure (IMPROVE-CHF) Study Investigators. N-terminal pro-B-type natriuretic peptide testing improves the management of patients with suspected acute heart failure: primary results of the Canadian prospective randomized multicenter IMPROVE-CHF study. Corculation 2007; 115: 3103-3110. 37) Hildebrandt P, Collinson PO. Amino-terminal pro-B-type natriuretic peptide testing to assist the diagnostic evaluation of heart failure in symptomatic primary care patients. Am J Cardiol 2008; 101: 25A-28A. 38) Masson S, Latini R. Amino-terminal pro-B-type natriuretic peptides and prognosis in chronic heart failure. Am J 174 J Cardiol Jpn Ed Vol. 2 No. 3 2008 Cardiol 2008; 101: 56A-60A. 39) Nishii M, Inomata T, Takehana H, Naruke T, Yanagisawa T, Moriguchi M, Takeda S, Izumi T. Prognostic utility of B-type natriuretic peptide assessment in stable low-risk outpatients with nonischemic cardiomyopathy after decompensated heart failure. J Am Coll Cardiol 2008; 51: 2329-2335. 40) Anand IS, Fisher LD, Chiang YT, Latini R, Masson S, Maggioni AP, Glazer RD, Tognoni G, Cohn JN. Changes in brain natriuretic peptide and norepinephrine over time and mortality and morbidity in the Valsartan Heart Failure Trial. Circulation 2003; 107: 1278-1283. 41) Latini R, Masson S, Wong M, Barlera S, Carretta E, Staszewsky L, Vago T, Maggioni AP, Anand IS, Tan LB, Tognoni G, Cohn JN; Val-HeFT Investigators. Incremental prognostic value of changes in B-type natriuretic peptide in heart failure. Am J Med 2006; 119: e23-e30. 42) Yan RT, White M, Yan AT, Yusuf S, Rouleau JL, Maggioni AP, Hall C, Latini R, Afzal R, Floras J, Masson S, McKelvie RS; Randomized Evaluation of Strategies for Left Ventricular Dysfunction (RESOLVD) Investigators. Usefulness of temporal changes in neurohormones as markers of ventricular remodeling and prognosis in patients with left ventricular systolic dysfunction and heart failure receiving either candesartan or enalapril or both. Am J Cardiol 2005; 96: 698-704. 43) Latini R, Masson S, Anand I, Salio M, Hester A, Judd D, Barlera S, Maggioni AP, Tognoni G, Cohn JN; For the Val-HeFT Investigators. The comparative prognostic value of plasma neurohormones at baseline in patients with heart failure enrolled in Val-HeFT. Eur Heart J 2004; 25: 292-299. 44) Hartmann F, Packer M, Coats AJ, Fowler MB, Krum H, Mohacsi P, Rouleau JL, Tendera M, Castaigne A, Anker SD, Amann-Zalan I, Hoersch S, Katus HA. Prognostic impact of plasma N-terminal pro-brain natriuretic peptide in severe chronic congestive heart failure. A substudy of the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) trial. Circulation 2004; 110: 1780-1786. 45) Hartmann F, Packer M, Coats AJ, Fowler MB, Krum H, Mohacsi P, Rouleau JL, Tendera M, Castaigne A, Trawinski J, Amann-Zalan I, Hoersch S, Katus HA. NT-proBNP in severe chronic heart failure: rationale, design and preliminary results of the COPERNICUS NT-proBNP substudy. Eur J Heart Fail 2004; 6: 343-350. 46) Olsson LG, Swedberg K, Cleland JG, Spark PA, Komajda M, Metra M, Torp-Pedersen C, Remme WJ, Scherhag A, Poole-Wilson P; COMET Investigators. Prognostic importance of plasma NT-proBNP in chronic heart failure in patients treated with a β-blocker: Results from the Carvedilol Or Metoprolol European Trial (COMET) trial. Eur J Heart Fail 2007; 9: 795-801. 47) Olsen MH, Wachtell K, Tuxen C, Fossum E, Bang LE, Hall C, Ibsen H, Rokkedal J, Devereux RB, Hildebrandt P. N-terminal pro-brain natriuretic peptide predicts car- 循環器疾患における血中 BNP,NT-proBNP 測定の意義 diovascular events in patients with hypertension and left ventricular hypertrophy: a LIFE study. J Hypertens 2004; 22: 1597-1604. 48) Olsen MH, Wachtell K, Tuxen C, Fossum E, Bang LE, Hall C, Ibsen H, Rokkedal J, Devereux RB, Hildebrandt PR. Opposite effects of losartan and atenolol on natriuretic peptides in patients with hypertension and left ventricular hypertrophy: a LIFE substudy. J Hypertens 2005; 23: 1083-1090. 49) Blankenberg S, McQueen MJ, Smieja M, Pogue J, Balion C, Lonn E, Rupprecht HJ, Bickel C, Tiret L, Cambien F, Gerstein H, M-nzel T, Yusuf S; HOPE Study Investigators. Comparative impact of multiple biomarkers and N-Terminal pro-brain natriuretic peptide in the context of conventional risk factors for the prediction of recurrent cardiovascular events in the Heart Outcomes Prevention Evaluation (HOPE) Study. Circulation 2006; 114: 201-208. 50) Hildebrandt P, Richards AM. Amino-terminal pro-B-type natriuretic peptide testing in patients with diabetes mellitus and with systemic hypertension. Am J Cardiol 2008; 101: 21A-24A. 51) Bettencourt P, Azevedo A, Pimenta J, Frioes F, Ferreira S, Ferreira A. N-terminal-pro-brain natriuretic peptide predicts outcome after hospital discharge in heart failure patients. Circulation 2004; 110: 2168-2174. 52) Maeda K, Tsutamoto T, Wada A, Mabuchi N, Hayashi M, Tsutsui T, Ohnishi M, Sawaki M, Fujii M, Matsumoto T, Kinoshita M. High levels of plasma brain natriuretic peptide and interleukin-6 after optimized treatment for heart failure are independent risk factors for morbidity and mortality in patients with congestive heart failure. J Am Coll Cardiol 2000; 36: 1587-1593. 53) Ordonez-Llanos J, Collinson PO, Christenson RH. Amino-terminal pro-B-type natriuretic peptide: analytic considerations. Am J Cardiol 2008; 101: 9A-15A. 54) Davis ME, Richards AM, Nicholls MG, Yandle TG, Frampton CM, Troughton RW. Introduction of metoprolol increases plasma B-type cardiac natriuretic peptides in mild, stable heart failure. Circulation 2006; 113: 977-985. 55) Cheng V, Kazanagra R, Garcia A, Lenert L, Krishnaswamy P, Gardetto N, Clopton P, Maisel A. A rapid bedside test for B-type peptide predicts treatment outcomes in patients admitted for decompensated heart failure: a pilot study. J Am Coll Cardiol 2001; 37: 386-391. 56) Miller WL, Hartman KA, Burritt MF, Borgeson DD, Burnett JC Jr, Jaffe AS. Biomarker responses during and after treatment with nesiritide infusion in patients with decompensated chronic heart failure. Clin Chem 2005; 51: 569-577. 57) Bettencourt P, Januzzi JL Jr. Amino-terminal pro-B-type natriuretic peptide testing for inpatient monitoring and treatment guidance of acute destabilized heart failure. Am J Cardiol 2008; 101: 67A-71A. 58) Gheorghiade M, De Luca L, Fonarow GC, Filippatos G, Metra M, Francis GS. Pathophysiologic targets in the ear- ly phase of acute heart failure syndromes. Am J Cardiol 2005; 96: 11G-17G. 59) Wolfel EE. Can we predict and prevent the onset of acute decompensated heart failure- Circulation 2007; 116: 1526-1529. 60) Troughton RW, Frampton CM, Yandle TG, Espiner EA, Nicholls MG, Richards AM. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) concentrations. Lancet 2000; 355: 1126-1130. 61) Jourdain P, Jondeau G, Funck F, Gueffet P, Le Helloco A, Donal E, Aupetit JF, Aumont MC, Galinier M, Eicher JC, Cohen-Solal A, Juilli-re Y. Plasma brain natriuretic peptide-guided therapy to improve outcome in heart failure: the STARS-BNP Multicenter Study. J Am Coll Cardiol 2007 Apr 24; 49: 1733-1739. 62) Shah MR, Claise KA, Bowers MT, Bhapkar M, Little J, Nohria A, Gaulden LH, McKee VK, Cozart KL, Mancinelli KL, Daniels H, Kinard T, Stevenson LW, Mancini DM, O'Connor CM, Califf RM. Testing new targets of therapy in advanced heart failure: the design and rationale of the Strategies for Tailoring Advanced Heart Failure Regimens in the Outpatient Setting: BRain NatrIuretic Peptide Versus the Clinical CongesTion ScorE (STARBRITE) trial. Am Heart J 2005; 150: 893-898. 63) Lainchbury JG, Troughton RW, Frampton CM, Yandle TG, Hamid A, Nicholls MG, Richards AM. NTproBNPguided drug treatment for chronic heart failure: design and methods in the "BATTLESCARRED" trial. Eur J Heart Fail 2006; 8: 532-538. 64) Morita E, Yasue H, Yoshimura M, Ogawa H, Jougasaki M, Matsumura T, Mukoyama M, Nakao K. Increased plasma levels of brain natriuretic peptide in patients with acute myocardial infarction. Circulation 1993; 88: 82-91. 65) Suzuki S, Yoshimura M, Nakayama M, Mizuno Y, Harada E, Ito T, Nakamura S, Abe K, Yamamuro M, Sakamoto T, Saito Y, Nakao K, Yasue H, Ogawa H. Plasma level of B-type natriuretic peptide as a prognostic marker after acute myocardial infarction. A long-term follow-up analysis. Circulation 2004; 110: 1387-1391. 66) Omland T, Persson A, Ng L, O'Brien R, Karlsson T, Herlitz J, Hartford M, Caidahl K. N-terminal pro-B-type natriuretic peptide and long-term mortality in acute coronary syndromes. Circulation 2003; 106: 2913-2918. 67) De Lemos JA, Morrow DA, Bentley JH, Omland T, Sabatine MS, McCabe CH, Hall C, Cannon CP, Braunwald E. The prognostic value of B-type natriuretic peptide in patients with acute coronary syndromes. N Engl J Med 2001; 345: 1014-1021. 68) Morrow DA, de Lemos JA, Sabatine MS, Murphy SA, Demopoulos LA, DiBattiste PM, McCabe CH, Gibson CM, Cannon CP, Braunwald E. Evaluation of B-type natriuretic peptide for risk assessment in unstable angina/ non-ST-elevation myocardial infarction: B-type natriuretic peptide and prognosis in TACTICS-TIMI 18. J Am Coll Cardiol 2003; 41: 1264-1274. 69) Lindahl B, Lindback J, Jernberg T, Johnston N, Stridsberg Vol. 2 No. 3 2008 J Cardiol Jpn Ed 175 M, Venge P, Wallentin L. Serial analysis of N-terminal pro-B-type natriuretic peptide in patients with non-STsegment elevation acute coronary syndrome. A Fragmin and Fast Revascularization During Instability in Coronary Artery Disease (FRISC)-II substudy. J Am Coll Cardiol 2005; 45: 533-541. 70) James SK, LIndahl B, Siegbahn A, Stridsberg M, Venge P, Armstrong P, Barnathan ES, Callif R, Topol EJ, Simoons ML, Wallentin L. N-terminal pro-brain natriuretic peptide and other risk markers for the separate prediction of mortality and subsequent myocardial infarction in patients with unstable coronary artery disease. A Global Utilization of Strategies to Open occluded arteries (GUSTO)IV substudy. Circulation 2003; 108: 275-281. 71) Heeschen C, Hamm CW, Mitrovic V, Lantelme NH, White HD, for the Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) Investigators. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation 2004; 110: 3206-3212. 72) James SK, Lindb-ck J, Tilly J, Siegbahn A, Venge P, Armstrong P, Califf R, Simoons ML, Wallentin L, Lindahl B. Troponin-T and N-terminal pro-B-type natriuretic peptide predict mortality benefit from coronary revascularization in acute coronary syndromes: a GUSTO-IV substudy. J Am Coll Cardiol 2006; 48: 1146-1154. 73) Jernberg T, Lindahl B, Siegbahn A, Andren B, Frostfeldt G, Lagerqvist Bo, Stridsberg M, Venge P, Wallentin L. N-terminal pro-brain natriuretic peptide in relation to inflammation, myocardial necrosis, and the effect of an invasive strategy in unstable coronary artery disease. J Am Coll Cardiol 2003; 42: 1909-1016. 74) Morrow DA, Braunwald E. Future of biomarkers in acute coronary syndromes: moving toward a multimarker strategy. Circulation 2003; 108: 250-252. 75) Sabatine MS, Morrow DA, de Lemos JA, Omland T, Desai MY, Tanasijevic M, Hall C, McCabe CH, Braunwald E. Acute changes in circulating natriuretic peptide levels in relation to myocardial ischemia. J Am Coll Cardiol 2004; 44: 1988-1995. 76) Kragelund C, Cronning B, Kober L, Hildebrandt P, Steffensen R. N-terminal pro-B-type natriuretic peptide and long-term mortality in stable coronary heart disease. N Engl J Med 2005; 352: 666-675. 77) Bibbins-Domingo K, Gupta R, Na B, Wu AH, Schiller NB, Whooley MA. N-terminal fragment of the prohormone brain-type natriuretic peptide (NT-proBNP), cardiovascular events, and mortality in patients with stable coronary heart disease. JAMA 2007; 297: 169-176. 78) Apple FS, Wu AH, Jaffe AS, Panteghini M, Christenson RH, Cannon CP, Francis G, Jesse RL, Morrow DA, Newby LK, Storrow AB, Tang WH, Pagani F, Tate J, OrdonezLlanos J, Mair J; National Academy of Clinical Biochemistry; IFCC Committee for Standardization of Markers of Cardiac Damage Laboratory Medicine. National Academy of Clinical Biochemistry and IFCC Com- 176 J Cardiol Jpn Ed Vol. 2 No. 3 2008 mittee for Standardization of Markers of Cardiac Damage Laboratory Medicine practice guidelines: Analytical issues for biomarkers of heart failure. Circulation 2007; 116: e95-e98. 79) Seino Y, Ogawa A, Yamashita T, Fukushima M, Ogata K, Fukumoto H, Takano T. Application of NT-proBNP and BNP measurements in cardiac care: a more discerning marker for the detection and evaluation of heart failure. Eur J Heart Fail 2004; 6: 295-300. 80) Wang TJ, Larson MG, Levy D, Benjamin EJ, Leip EP, Omland T, Wolf PA, Vasan RS. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N Engl J Med 2004; 350: 655-663. 81) McKie PM, Rodeheffer RJ, Cataliotti A, Martin FL, Urban LH, Mahoney DW, Jacobsen SJ, Redfield MM, Burnett JC. Amino-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide. Biomarkers for mortality in a large community-based cohort free of heart failure. Hypertension 2006; 47: 874-880. 82) Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu P. Outcome of heart failure with preserved ejection fraction in apopulation-based study. N Engl J Med 2006; 355: 260-269. 83) Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355: 251-259. 84) Maisel AS, McCord J, Nowak RM, Hollander JE, Wu AH, Duc P, Omland T, Storrow AB, Krishnaswamy P, Abraham WT, Clopton P, Steg G, Aumont MC, Westheim A, Knudsen CW, Perez A, Kamin R, Kazanegra R, Herrmann HC, McCullough PA; Breathing Not Properly Multinational Study Investigators. Bedside B-Type natriuretic peptide in the emergency diagnosis of heart failure with reduced or preserved ejection fraction. Results from the Breathing Not Properly Multinational Study. J Am Coll Cardiol 2003; 41: 2010-2017. 85) Iwanaga Y, Nishi I, Furuichi S, Noguchi T, Sase K, Kihara Y, Goto Y, Nonogi H. B-type natriuretic peptide strongly reflects diastolic wall stress in patients with chronic heart failure: comparison between systolic and diastolic heart failure. J Am Coll Cardiol 2006; 47: 742-748. 86) Kirk V, Bay M, Parner J, Krogsgaard K, Herzog TM, Boesgaard S, Hassager C, Nielsen OW, Aldershvile J, Nielsen H. N-terminal proBNP and mortality in hospitalized patients with heart failure and preserved vs. reduced systolic function: data from the proapective Copenhagen Hospital Heart Failure Study (CHHF). Eur J Heart Fail 2004; 6: 335-341. 87) Valle R, Aspromonte N, Feola M, Milli M, Canali C, Giovinazzo P, Carbonieri E, Ceci V, Cerisano S, Barro S, Milani L. B-type natriuretic peptide can predict the medium-term risk in patients with acute heart failure and preserved systolic function. J Card Fail 2005; 11: 498-503. 88) Redfield MM, Rodeheffer RJ, Jacobsen SJ, Mahoney 循環器疾患における血中 BNP,NT-proBNP 測定の意義 DW, Bailey KR, Burnett JC. Plasma brain natriuretic peptide to detect preclinical ventricular systolic or diastolic dysfunction. A community-based study. Circulation 2004; 109: 3176-3181. 89) Lubien E, DeMaria A, Krishnaswamy P, Clopton P, Koon J, Kazanegra R, Gardetto N, Wanner E, Maisel AS. Utility of B-natriuretic peptide in detecting diastolic dysfunction: comparison with Doppler velocity recordings. Circulation 2002; 105: 595-601. 90) Persson H, Lonn E, Edner M, Baruch L, Lang CC, Morton JJ, Ostergren J, McKelvie RS; Investigators of the CHARM Echocardiographic Substudy-CHARMES. Diastolic dysfunction in heart failure with preserved systolic function: need for objective evidence: results from the CHARM Echocardiographic Substudy-CHARMES. J Am Coll Cardiol 2007; 49: 687-694. 91) Sato Y, Yamada T, Taniguchi R, Nagai K, Makiyama T, Okada H, Kataoka K, Ito H, Matsumori A, Sasayama S, Takatsu Y. Persistently increased serum concentrations of cardiac troponin T in patients with idiopathic dilated cardiomyopathy are predictive of adverse outcomes. Circulation 2001; 103: 369-374. 92) Sato Y, Kita T, Takatsu Y, Kimura T. Biochemical markers of myocyte injury in heart failure. Heart 2004; 90: 1110-1113. 93) Horwich TB, Patel J, MacLellan WR, Fonarow GC. Cardiac troponin I is associated with impaired hemodynamics, progressive left ventricular dysfunction, and increased mortality rates in advanced heart failure. Circulation 2003; 108: 833-838. 94) Miller WL, Hartman KA, Burritt MF, Grill DE, Rodeheffer RJ, Burnett JC Jr, Jaffe AS. Serial biomarker measurements in ambulatory patients with chronic heart failure: the importance of change over time. Circulation 2007; 116: 249-257. 95) Ishii J, Ozaki Y, Lu J, Kitagawa F, Kuno T, Nakano T, Nakamura Y, Naruse H, Mori Y, Matsui S, Oshima H, Nomura M, Ezaki K, Hishida H. Prognostic value of serum concentration of heart-type fatty acid-binding protein rel- ative to cardiac troponin T on admission in the early hours of acute coronary syndrome. Clin Chem 2005; 51: 1397-1404. 96) Latini R, Masson S, Anand IS, Missov E, Carlson M, Vago T, Angelici L, Barlera S, Parrinello G, Maggioni AP, Tognoni G, Cohn JN; Val-HeFT Investigators. Prognostic value of very low plasma concentrations of troponin T in patients with stable chronic heart failure. Circulation 2007; 116: 1242-1249. 97) Fonarow GC, Peacock WF, Horwich TB, Phillips CO, Givertz MM, Lopatin M, Wynne J; ADHERE Scientific Advisory Committee and Investigators. Usefulness of B-type natriuretic peptide and cardiac troponin levels to predict in-hospital mortality from ADHERE Am J Cardiol 2008; 101: 231-237. 98) Sakhuja R, Green S, Oestreicher EM, Sluss PM, Lee-Lewandrowski E, Lewandrowski KB, Januzzi JL Jr. Aminoterminal pro-brain natriuretic peptide, brain natriuretic peptide, and troponin T for prediction of mortality in acute heart failure. Clin Chem 2007; 53: 412-420. 99) Peacock WF 4th, De Marco T, Fonarow GC, Diercks D, Wynne J, Apple FS, Wu AH; ADHERE Investigators. Cardiac troponin and outcome in acute heart failure. N Engl J Med 2008; 358: 2117-2126. 100)Braunwald E. Biomarkers in heart failure. N Engl J Med 2008; 358: 2148-2159. 101)Prontera C, Storti S, Emdin M, Passino C, Zyw L, Zucchelli GC, Clerico A. Comparison of a fully automated immunoassay with a point-of-care testing method for B-type natriuretic peptide. Clin Chem 2005; 51: 1274-1276. 102)Kurihara T, Yanagida A, Yokoi H, Koyata A, Matsuya T, Ogawa J, Okamura Y, Miyamoto D. Evaluation of cardiac assays on a benchtop chemiluminescent enzyme immunoassay analyzer, PATHFAST. Anal Biochem 2008; 375: 144-146. 103)Alehagen U, Janzon M. A clinician's experience of using the Cardiac Reader NT-proBNP point-of-care assay in a clinical setting. Eur J Heart Fail 2008; 10: 260-266. Vol. 2 No. 3 2008 J Cardiol Jpn Ed 177
© Copyright 2026 Paperzz