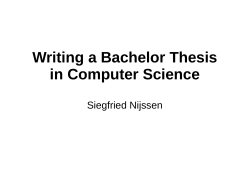
MASTER IN DE ERGOTHERAPEUTISCHE WETENSCHAP Interuniversitaire master in samenwerking met: UGent, KU Leuven, UHasselt, UAntwerpen, Vives, HoGent, Arteveldehogeschool, AP Hogeschool Antwerpen, HoWest, Odisee, PXL, Thomas More Faculteit Geneeskunde en Gezondheidswetenschappen Conversion to the ICF and psychometric properties of the Housekeeping Damage Scale (HODA- Scale) Annelies VANOOTEGHEM Masterproef ingediend tot het verkrijgen van de graad van Master of science in de ergotherapeutische wetenschap Promotor: Dr. Dominique Van de Velde Co- promotor: Lode Sabbe Academiejaar 2015-2016 MASTER IN DE ERGOTHERAPEUTISCHE WETENSCHAP Interuniversitaire master in samenwerking met: UGent, KU Leuven, UHasselt, UAntwerpen, Vives, HoGent, Arteveldehogeschool, AP Hogeschool Antwerpen, HoWest, Odisee, PXL, Thomas More Faculteit Geneeskunde en Gezondheidswetenschappen Conversion to the ICF and psychometric properties of the Housekeeping Damage Scale (HODA- Scale) Annelies VANOOTEGHEM Masterproef ingediend tot het verkrijgen van de graad van Master of science in de ergotherapeutische wetenschap Promotor: Dr. Dominique Van de Velde Co- promotor: Lode Sabbe Academiejaar 2015-2016 Nederlandstalig abstract Titel: Converteren naar de International Classification of Functioning, disability and health en de psychometrische kenmerken van de Housekeeping Damage Scale (HODAschaal) Achtergrond: Core sets zijn een set van categorieën gebaseerd op het ICF. Ze representeren het minimum aantal nodige categorieën voor metingen, overdracht en communicatie omtrent factoren voor een bepaalde doelgroep. Doel: (1) het converteren van de HODA-schaal naar de ICF categorieën om de core set voor personen met een traumatisch hersenletsel te coveren. (2) een evaluatie van de psychometrische kenmerken van het meetinstrument. Methode: Aan de hand van de linking rules en de expertise van een expertenpanel werden de items van de HODA-schaal geconverteerd naar het ICF. Dataverzameling voor de evaluatie van de psychometrische kenmerken vond plaats in het UZ Gent, bij 34 patiënten met een NAH. De interne consistentie en de test-hertest betrouwbaarheid werd nagegaan. Er werd gebruik gemaakt van twee meetinstrument, de ELIDA-schaal en de JAMAR. Hiermee werd de construct- en discriminatieve validiteit te bepalen. Resultaten: Drie items uit de HODA-schaal coveren de core set TBI. De interne consistentie is zeer sterk blijkt uit de item- total correlatie van 0.592 tot 0.910. De testhertest betrouwbaarheid is zeer sterk op schaalniveau (ICC van 0.98) en matig op itemniveau (Kappa van 0.56). de constructvaliditeit is sterk op schaalniveau (r=0.82), op itemniveau varieert de correlatie tussen 0.15 en 0.83. De discriminatieve validiteit gaf een correlatie van -0.558 met de JAMAR. Conclusie: De HODA-schaal is een valide en betrouwbaar instrument en is succesvol geconverteerd naar het ICF. Trefwoorden: NAH, core set, ICF, psychometrische kenmerken, Housekeeping Damage Scale. Aantal woorden in deze masterproef: 8009 English abstract Title: Conversion to the International Classification of Functioning, disability and health and psychometric properties of the Housekeeping Damage Scale (HODA- Scale) Background: Core sets are a set of categories based on the ICF. It represents the minimum categories necessary for measurement, transmission and communication of factors related to a patient population. Aim: (1) convert the items of the HODA-scale to ICF-categories for covering the coreset of Traumatic Brain Injury (TBI). (2) evaluate the psychometric properties of the HODA-scale. Method: The linking rules and the expertise of an expert panel were used to convert the items to the ICF. The data collection for the evaluation of the psychometric properties was conducted at the University Hospital Ghent with 34 people with an Acquired Brain Injury (ABI). The reliability and internal consistency were conducted. There were two outcome scales used, ELIDA-scale and JAMAR to conduct the construct- and discriminative validity. Results: Three items of the HODA-scale covered the core set TBI. The internal consistency was very strong appears out the item total correlation from 0.592 to 0.910. The test-retest reliability is strong on scale level (ICC: 0.98) and moderate on item- level (Kappa: 0.56). the construct validity is strong on scale level (r=0.82) and variates on itemlevel with a correlation between 0.15 and 0.83. The discriminative validity gave a correlation of -0.558 with the JAMAR. Conclusion: The HODA-scale is a valid and reliable instrument and is successfully converted to the ICF. Keywords: ABI, core- set, ICF, psychometric properties, Housekeeping Damage scale. Amount of words in this master thesis: 8009 Inhoud Woord vooraf.................................................................................................................... 1 Introduction ...................................................................................................................... 2 Qualitative part ................................................................................................................. 7 1. Method ............................................................................................................... 7 Linking rules .............................................................................................................. 7 Expert panels.............................................................................................................. 8 Process of conversion ................................................................................................ 8 2. Results ................................................................................................................ 9 Quantitative part ............................................................................................................. 12 1. Sampling .......................................................................................................... 12 2. Method ............................................................................................................. 12 2.1. Assessment instruments ................................................................................... 12 2.2. Protocol ............................................................................................................ 14 2.3. Construct validity ............................................................................................. 15 2.4. Discriminative validity .................................................................................... 17 2.5. Factorial Validity ............................................................................................. 17 2.6. Internal consistence .......................................................................................... 18 2.7. Test- retest reliability ....................................................................................... 18 3. Results .............................................................................................................. 19 3.1. Study population .............................................................................................. 19 3.2. Construct validity ............................................................................................. 19 3.3. Discriminative validity .................................................................................... 21 3.4. Factorial validity .............................................................................................. 22 3.5. Internal consistence .......................................................................................... 24 3.6. Reliability......................................................................................................... 24 Discussion....................................................................................................................... 25 Conclusion ...................................................................................................................... 27 References ...................................................................................................................... 28 Appendix ........................................................................................................................ 33 Appendix A: Occupational therapy in core set TBI .................................................... 33 Appendix B: HODA-scale .......................................................................................... 35 List of figures ................................................................................................................. 37 List of tables ................................................................................................................... 38 Woord vooraf Deze masterproef is tot stand gekomen dankzij de hulp en steun van enkele personen. Graag wil ik mijn promotor Dr. Dominique Van de Velde bedanken voor de nodige steun, tips en advies dat hij mij gaf doorheen dit proces. Daarnaast wil ik ook graag Lode Sabbe bedanken voor zijn tips en ondersteuning bij deze masterproef. Ook bedankt aan Sofie Slos. Zonder haar medewerking en hulp had het veldwerk dat nodig was voor deze masterproef niet kunnen plaatsvinden. Bedankt aan alle patiënten die bereidt waren deel te nemen aan de afnames van het assessment, de ergotherapeuten van het CLNR die tijd voor mij vrij maakte en alle leden van het expertenpanel dat nodig was voor de conversie van de HODA-schaal. Zonder de medewerking van deze mensen was het niet mogelijk geweest om deze masterproef tot stand te brengen. Een speciale bedanking aan mijn mama die mij niet alleen de mogelijkheid geboden heeft om deze opleiding te volgen maar mij ook altijd gesteund heeft en vertrouwen in mij had. Tenslotte ook bedankt aan de rest van mijn familie en mijn vrienden die mij gesteund hebben doorheen deze opleiding. 1 Introduction An acquired brain injury or an ABI can be defined as an injury caused after birth and that can’t be associated with a degenerative disease or a congenital disorder (Cochrane et al. 2000). It is used as an collective term and can be a result of a traumatic or non- traumatic cause (O’Reilly & Pryor, 2002). A traumatic brain injury or TBI can be defined as a change in the functioning of the brain or other proof of brain pathology such as seen on visual, laboratory or neuroradiology validation of depravation of the brain, caused by an external force (Menon, Schwab, Wright & Maas, 2010). A non- traumatic brain injury is created by an internal event like an infection, stroke or hypoxia (O’Reilly & Pryor, 2002). In Flanders there is a prevalence of 183/100000 people and an incidence of 28/100000 people for ABI. TBI has in Flanders an incidence of 11/100000 people with permanent limitations. Brain injury of a non- traumatic cause more specifically people with stroke, has an incidence of 35-57/100000 by people younger than 70 years (Lannoo et al., 2007). A brain injury can have long term consequences on physical, social and health terms. People indicate that one year after the injury they still need support for their cognitive and physical ADL, that there is no social re-integration, that they experience problems in fulfilling domestic roles and there is a sense of restrictions in productivity (Andelic et al., 2010). Assessment instruments can be used to make an evaluation and to get an idea of the impact of the injury. (Goljar et al., 2010). As a caregiver it is important to measure outcomes objectively in various areas and to ensure that those instruments show significant and meaningful functional improvement (Watanabe, Miller, Jacinta & McElligott, 2003). Outcome measures are necessary for supporting communication between caregivers and for clinical learning and research (Turners- Stokes et al., 2012). Using standardised assessment instruments for measuring the effectiveness of clinical interventions is accepted as a central point in good clinical practice (Van der Putten, Hobart, Freeman & Thompson, 1998). Yet there are still restrictions caregivers experience. A big problem is the number of different available instruments for mapping the performance and limitations by people with a brain injury (Bernabeu et al., 2009). A major concern in using outcome measures is their psychometric properties. A good 2 instrument should be reliable and valid, reproducible and must have good scale properties, preferable on interval level. In addition to these features a scale should also be clinical sensitive and easy to apply in practice. It also should be interpretable, relevant and responsive to chance that is clinical important (Turner- Stokes et al. 2012). Thereby an ideal assessment instrument of human functioning or aspects of human functioning is based on a universal and common shared classification. This can serve standards for reporting aspects of functioning over a large amount of outcome measures and it can also be used as a building block for the development of these instrument (Stucki, Kostanjsek, Üstün & Cieza, 2008). A general accepted framework is The International Classification of Functioning, disability and health (ICF) developed by the World Health Organisation (WHO) in 2001. The ICF gives a biopsychosocial approach to the different perspectives of health and related aspects. It has the aim to help with understanding and studying health and related states, determinants and outcomes related to health and this on a scientific basis. Thereby it wants to improve communication between different persons by establishing a common language, to give the opportunity to compare data across different care givers and services and to classify health information in a systematic coding scheme (WHO, 2001). The ICF can be divided in two main parts, ‘functioning and disability’ and ‘ contextual factors’. These parts exist of two components, for ‘functioning and disability’ these are ‘body functions and structures’ and ‘activities’ and ‘participation’. For the ‘contextual factors’ the components are ‘environmental factors’ and ‘personal factors’. The components are indicated on a base of an alphanumeric system. ‘Body functions’ are assigned to the letter ‘b’, ‘body structures’ to the letter ‘s’, ‘activity and participation’ is assigned to the letter ‘d’ and ‘environmental factors’ are assigned to the letter ‘e’. The ‘personal factors’ do not have an assignment to a letter and is not further divided because of the variation in the contextual factor which it’s based on (eg. sex and age). Because of the hierarchical approach of the ICF each component is further divided in domains, these domains are divided in categories and categories are divided in levels. An example of the different levels: b1: mental functions b114 orientation functions 3 b1142 orientation to person b11421 orientation to others (WHO,2001). Figure 1: The ICF- framework (WHO, 2001) When someone wants to use the codes one must take into account that the use of the codes requires the use of one or more qualifiers. These are displayed in a code behind the point (eg. xxx.0). If one does not place these qualifiers behind the codes, they lose their meaning. There are seven possible qualifiers. The same generic scale is found in all the components. Encountering a problem can refer to a limitation, impairment of restriction (WHO, 2001). Figure 2: ICF- qualifiers (WHO, 2001) An issue in using the ICF in clinical practice is the size of this framework. Therefore a practical tool is needed, like core sets (Stucki et al., 2008). Core sets are a set of categories of the International Classification of Functioning, disability and health that represent the 4 minimum requirements for measurement, transmission and communication of factors who are related to functioning and health of patients. Each core set should be goaloriented, compact and useful in daily clinical practice (Yen et al., 2012). These sets ensure that professionals in clinical settings and researches can describe functioning of an individual in a generally accepted universal language. In addition, it can also contribute to the content validity of measurement scales and give professionals the possibility to select the most appropriate scale for the specific needs of a given population patients (Bernabeu et al. 2009). Research by Ptyushki, Vidmar, Burger & Marincek (2012) confirmed the valuable contribution of the ICF in traumatic brain injury rehabilitation. It states that the ICF can help caregivers to take the different interactions and relationships between the components of the framework into account. Semlyen, Summers & Barnes (1998) investigated the multidisciplinary approach in rehabilitation. Such an approach seems to be efficient in gaining functional improvement, reduce caregiver distress and to increase the level of independence. An occupational therapist was part of such a multidisciplinary team. An occupational therapist focuses in the rehabilitation process in patients with a brain injury such as stroke, mainly on issues experienced by the patient in activities of daily life, domestic tasks, leisure and cognition (De Wit et al., 2006). A recently developed instrument that measures domestic tasks is the Housekeeping Damage Scale or the HODA- Scale. The aim of the outcome measure is to indicate the damage after injury in these tasks. The HODA-scale represents a total score of 100 which shows the damage in terms of a percentage (Brusselmans, Thomas, Cook & Vermeulen, 2014). Aim of the study: This study consist of two main parts. First there is a qualitative part which involves the conversion of the scale to the ICF. In this part the meaningful concepts of each item of the HODA-scale was identified and linked to the most appropriate ICF-category. To link the concepts the linking rules by Cieza et al. (2005) were implied and the input from a number of experts all with years of clinical experience were used. The aim of the 5 conversion is to cover the ICF categories specifically for occupational therapists in the core set for patients with TBI. The second part is a quantitative part where the psychometric properties of the HODAscale are evaluated. Data was collected at the University Hospital Ghent by patients with an acquired brain injury. The total sample consisted of 34 people. The overall aim of this part is to examine the construct-, discriminative- and factorial validity, the internal consistency and the test- retest reliability of the HODA- Scale by patients with ABI. 6 Qualitative part This part of the study includes a conversion of the HODA-scale to the ICF categories. The overall aim of the conversion is to identify the possibility of the outcome measure to cover items in the core set for people with a traumatic brain injury. 1. Method Linking rules To convert an assessment it is important to implement the Linking Rules of Cieza et al. (2005). The aim of the linking rules are to provide guidelines to link systematic and standardized measures to the ICF (Cieza et al. 2002). There are eight distinct linking rules which has the intention to link technical and clinical measures, interventions and health status measures to the ICF. When linking outcome measures to the ICF with these rules it is important to take into account that all important meaningful concepts of the outcome measure are linked to the ICF. When one is linking, it can be the case that an ICF category may occur more than one time (Cieza et al. 2005). An overview of the linking rules is listed in table 1. Table 1: ICF linking rules (Cieza et al. 2005) Linking rule 1. Good knowledge of the taxonomical and conceptual fundaments of the ICF is necessary before starting to link meaningful concepts to the ICF. Also knowledge of chapters, domains and categories of the ICF is important, as are knowledge of the definitions. 2. The meaningful concept must be linked to the most exact ICF category. 3. The categories ‘other specified’ with code 8 may not be used. When the meaningful concept is not named in an ICF category one has to state that the information is not explicit named in the ICF. 4. The categories ‘unspecified’ with code nine may not be used. It has to be named with the lower level category 5. Use ‘not definable’ when there can’t be a decision for the most appropriate ICF category. This rule includes special cases: when meaningful concepts refer to health, mental of physical health they are assigned as “not definable general health, not definable psychical health, not definable mental health”. The same has to been done with concepts who refer to quality of life, they are assigned as “not definable quality of life”. 6. When the ICF does not include the meaningful concept but it’s a personal factor like it is defined in the ICF, one has to give the concept the assignment of personal factor 7. When the concept is not include in the ICF and it is not a personal factor give it the assignment of not covered by the ICF 8. When the concept is a diagnosis or a health state give the concept the assignment of health condition 7 Expert panels In order to contain a reliable conversion an expert panel was assembled. This method was also used in previous research concerning the conversion of outcome measures, eg. the MMSE (De Vriendt, Gorus, Bautmans & Mets, 2012). The systematic review of Fayed, Cieza & Bickenbach (2011) indicates that the persons who are involved in conversing outcome measures have a lot of expertise in clinical practice, the ICF or have professional or research experience. The experts that were involved in this research included three occupational therapists, two psychologists, one physical therapist and a doctor in health science. All of these people had clinical experience, expertise in the ICF or in scientifically research. The experts were divided in two independent panels who conversed the assessment separately. Process of conversion At first the items of the assessment were converted by myself and another student who was involved in the research around the TBI-core set. In each item of the assessment the meaningful concept was identified and we went true all the codes and selected the one we thought was the most suitable. Later, when all concepts were linked to a category, we invited the two independent expert panels. At the start of the meeting we explained the goal of the research and elucidated the linking rules which were a major concern for the reliability of the conversion. The independent expert panels converted the assessment to the ICF, I was present the whole meeting but I had no input because of the interests of the reliability of the conversion. The third step that was taken included a comparison of the codes that were granted to the items. There is made a comparison between the codes the other student and I gave to the items, the codes of the first expert panel and the codes of the second expert panel. When there were three codes the same there was an overall consensus, when two codes were the same the other one was excluded and when not one code was the same there was asked for a second opinion of the expert panel. This was done by an online survey, which was sent to all participants. When the conversion was complete the categories assigned to the HODA-scale were compared with the core-set. 8 2. Results After the expert panel, 23 items were converted in consensus. Two items remained in which no full consensus was reached. After sending the online survey to the experts one expert did not complete the online survey. Beside the experts the other student and I also answered on the survey. Because of the missing vote of one expert the total size for the online survey was reduced from nine to eight. After the online survey there wasn’t a full consensus over the two items. Therefore, it was decided to choose the items with the largest number of votes. The results of the online survey can be seen in the figures 3 and 4. Figure 3: item 1 online survey Figure 4: item 2 online survey 9 After the survey each item of the HODA-scale was assigned to an ICF- category. An overview of the conversion is shown in table 2. Table 2 : conversion of the HODA- scale Item HODA- Scale 1. ICF code Kitchen activities 1. Kitchen activities - Heating a meal for example in the microwave - d6300 Preparing simple meals - Independent peeling and cutting potatoes - d6300 Preparing simple meals - Preparing a full meal, cooking process and - d6301 Preparing complex meals timing preparation - d6401 Cleaning cooking area and utensils setting and clearing of the table, inclusive hot - d6401 Cleaning cooking area and utensils - and fragile material - Cleaning the kitchen and the dining room, washing the dishes 2. 3. Cleaning 2. - dust off furniture - vacuum one or multiple rooms - mopping/wet cleaning Cleaning - (handle cleaning d6402 Cleaning living area - d6403 Using household appliances - d6402 Cleaning living area convenience and bucket filled with water) - d6402 Cleaning living area - cleaning windows (maximum three steps high) - d6402 Cleaning living area - making the beds and change linens clothing and maintenance of the house 3. clothing and maintenance of the house - perform hand wash (wash, rinse out, hang to - d6400 Washing and drying clothes and garments dry) - d6403 Using household appliances filling, emptying and operating washing - d6403 Using household appliances machine and dryer - d6402 Cleaning living area ironing and folds of several linen (inclusive - d6404 Storing daily necessities - opening and closing the ironing board) - cleaning the house (loose scattered clothing, various objects, lecture, etc.) - storage in closets or racks and take out various household products and food. 4. jobs and managing household 4. jobs and managing household - performing repairs and replacements in the house - d6501 Maintaining dwelling and furnishings (replacing lamps, replacing batteries, etc.) - d6405 Disposing of garbage collect and sort garbage and placing it on the - d6200 Shopping streetside. - d5700 Ensuring one's physical comfort Management of the required reserves of household - d860 Basic economic transactions - equipment and making a shopping list - Keep supervision of the house and react appropriate (heating, open and close doors and windows, breakdowns, etc.) - Financial management housekeeping. 5. transport and groceries 5. transport and groceries 10 - shopping in a corner shop (butchery, bakery, - d6200 Shopping newsagent) - d6200 Shopping shopping in a supermarket (inclusive displacement, - d6200 Shopping loading and unloading goods) - d3600 Using telecommunication devices - shopping in a shopping district or shopping centre - d4602 Moving around outside the home and other - shopping online - use and transfer to several services (post office, - buildings bank, administrative services, etc.) The HODA-scale covered d620 acquisition of goods and services, d640 doing housework and d860 basic economic transactions in the TBI core set. An overview of the ICF categories in the core set for TBI specifically for occupational therapy and which ones are covered by the HODA-scale can be seen in appendix A. 11 Quantitative part This part of the study includes an evaluation of the psychometric properties of the HODA-scale in a ABI patient population. 1. Sampling The collection of the data took place in the University Hospital Ghent, Centre of Locomotor and Neurological Rehabilitation (CLNR). Inclusion criteria were people with the different forms of an acquired brain injury. The exclusion criteria were people with an aphasia and people who didn’t speak or understand the Dutch language. 2. Method It is the goal of this part of the study to define the construct validity of the HODA. Therefore, the ELIDA will be used. To determine the discriminative validity the Jamar will be used. Factorial validity and internal consistency will be evaluated as is the testretest reliability. 2.1. Assessment instruments The Housekeeping Damage Scale The Housekeeping Damage Scale or the HODA- scale is an assessment instrument developed to indicate the damage after injury. Housekeeping damage is defined as the damage of the energetic and functional potential of a victim with an economically assessable impact on the ability of performing domestic chores. This manifests itself in a partial or complete impossibility to perform this tasks or an increased effort. When judging, one has to take the actual family situation and foreseeable evolution into account. The HODA- scale has the aim to make a contribution to the determination of housekeeping damage in accordance with the indicative table 2012. This table represents a list of financial compensations after injury. The scale takes functional limitations when performing household chores with the assignment of more effort and increased time of performing. Domestic tasks can be defined as the activities with a general nature and who are a part of the essence of the household. Damage can be displayed by comparing the actual and potential functioning before and after the accident. For the development of the HODA-scale the items of the assessment are based on chapter six of the ICF- 12 classification. Also the scoring system is based on the ICF criteria. The HODA-scale has a five-point scale ranging from zero to four (Brusselmans et al., 2014). Table 3: score system HODA-scale based on the ICF score criteria (Brusselmans et al. 2014) Score Definition 0 Normal or almost normal functioning 1 Mild obstruction of performance, the activity can be performed independent but requires a bit more effort and increased time. 2 Moderate obstruction of performance, the activity can be performed independent but requires clearly more effort and increased time. 3 Severe obstruction of performance, there is clearly increased effort and time needed, the activity can only be performed with partial assistance from others. 4 Activity can’t be performed autonomic, full assistance of third is necessary The HODA-scale consists of 25 items divided over five sections. Each item in the scale can get a score between zero and four. The total score will variate between 0 and 100 and gives a percentage of housekeeping damage. The assessor has to mention in each of the five sections whether the patient uses tools and when this is the case, describe which tools. The procedure for the completion of the assessment is questioning the patient, conducting a case study and observation. (Brusselmans et al., 2014). A score sheet of the HODAscale can be seen in appendix B. Estimate of Loss of Independence in Daily Activities Scale The Estimate of Loss of Independence in Daily Activities or the ELIDA-scale is an assessment scale designed to determine the need of assistance by patients with a work related accident. It is independent of the nature of the injury and can as result be used by various patients. It shows wider aspects of self-reliance such as instrumental activities of daily life and social self- reliance. The instrument consists of 50 items that are located into ten subscales. These subscale include: toilet, body hygiene, care: dress and undress, food, food preparation, take care of clothes, daily domestic tasks, not- daily domestic tasks, regulation of the environment and sleep, activities outside the house and communication and basic skills. Within these subscale are five items that can be scored with a positive (+) or a negative sign (-). A positive sign includes the ability to perform the activities independent and a negative sign represents dependence. When the assessment is completed the negative signs in each subscale are summed and multiplied 13 by two. As result one gets a score between 0-100. How lower the score on the scale how more independent the functioning of the patient. The procedure for the completion of the assessment is questioning the patient (Brusselmans, 1992). JAMAR The Jamar is an instrument that measures grip strength on the basis of a closed hydraulic system. It represents the measured values in kilogram (kg) and is applicable in different pathologic conditions such as stroke, neuromuscular diseases and rheumatoid arthritis (Bellace, Healy, Besser, Byron & Hohman, 2000). Measuring the grip strength has to be done bilateral (affected and non-affected hand) (Lafayette Instrument Company, 2004). The reference values for males vary between 47,4 kg and 29,8 kg for the left hand and 53,3 kg and 28,0 kg on the right hand. For females the reference values for the left hand range between 27,9 kg and 16,4 kg and for the right hand between 30,6kg and 18,0 kg. These reference values are depending on the age of the patient (Boannon, Peolsson, Massy- Westropp, Desrosiers & Bear- Lehman, 2006). The validity of the Jamar was tested with the Dexter dynamometer and had an ICC of 0.99 at the dominant hand and an ICC of 0.98 at the non-dominant hand (Bellace et al., 2000). The inter-instrument reliability with the Rolyan Dynamometers gave as result an ICC that ranged from 0.90 to 0.97 (Mathiowetz, 2002). 2.2. Protocol Data was collected for the three different outcome measures, the HODA-scale, the ELIDA-scale and the Jamar. Between the evaluation of the patients with these scale there was a time interval of one week maximum, there is scientific proof that a test- retest evaluation between two days and two weeks is adequate (Marx, Menezes, Horovitz, Jones & Warren, 2003). In order to make the collection of data practically feasible and to limit the change in functioning the same time interval was applied for the two other scales. 14 Figure 5: test protocol 2.3. Construct validity Construct validity can be defined as “the extent to which scores on a particular instrument relate to other measures in a manner that is consistent with theoretically derived hypotheses concerning the concepts that are being measured” (Terwee et al., 2007, p. 36). To assess the construct validity predefined hypotheses should be tested. How more specific the hypotheses the better for the results, otherwise there would be a higher risk for biases. This because afterwards one can for the low correlation attempt to provide an alternative explanation , instead of accepting that the instrument is not valid (Terwee et al., 2007). For the evaluation of the construct validity the HODA-scale is compared with the ELIDAscale. The construct validity is calculated by a correlation on one hand between the total score of the HODA- scale and the total score of the ELIDA- scale and on the other hand there are correlations calculated between the different items (cfr. hypotheses.) . Before processing the date a Shapiro- Wilk normality test is conducted to determinate the distribution of the data. When this test is significant (p< .05), a non- parametric test will be applied. When this test is not significant (p>.05) a parametric test will be applied. 15 Hypotheses On scale level there is hypothesized that the total score of the HODA-scale would correlate good with the total score of the ELIDA-scale because of the similarity in the construct displayed by both scales. On item- level there is hypothesized that (1) ‘Heating a meal for example in the microwave’ would correlate with ‘can independently prepare a simple meal’, (2) ‘Independent peeling and cutting potatoes’ would correlate with ‘can independently prepare a simple meal’, (3) ‘preparing a full meal, cooking process and timing preparation’ would correlate with ‘Can safely and independently operate a stove and monitor heating and cooking (taking a pot or pan on and off included)’, (4) ‘setting and clearing of the table, inclusive hot and fragile material’ would correlate with ‘Can independently set and clear the table (including hot and brittle materials)’, (5) ‘vacuum one or multiple rooms’ would correlate with ‘Can independently sweep the floor/ handle the vacuum cleaner’, (6) ‘mopping/wet cleaning (handle cleaning convenience and bucket filled with water)’ would correlate with ‘Can independently scrub the floor’, (7) ‘cleaning windows (maximum three steps high)’ would correlate with ‘Can independently wash the windows’, (8) ‘making the beds and change linens’ would correlate with ‘Can independently prepare and chance the bed’, (9) ‘perform hand wash (wash, rinse out, hang to dry)’ would correlate with ‘Can make a small hand wash by himself’, (10) ‘filling, emptying and operating washing machine and dryer’ would correlate with ‘Can control, fill and empty a washing machine/dryer’, (11) ‘ironing and folds of several linen (inclusive opening and closing the ironing board)’ would correlate with ‘Can safely use an iron and folds clothes’, (12) ‘storage in closets or racks and take out various household products and food’ would correlate with ‘Can take autonomous objects and store it properly in closets and storage spaces (eg. Clothing, household equipment)’, (13) ‘performing repairs and replacements in the house (replacing lamps, replacing batteries, etc.)’ would correlate with ‘can independently do minor repairs or replacements in the house (eg. Replacement of a lamp)’, (14) ‘Keep supervision of the house and react appropriate (heating, open and close doors and windows, breakdowns, etc.)’ would correlate with ‘Independently have control over the state of the house and functioning of devices (eg. Leaks, observing damage and respond appropriately)’, ‘Can independently 16 guarantee the necessary lighting, ventilation and shielding of the house (windows and (role)shutters, switches)’ and ‘Can be independently responsible for opening and closing the doors of the house’, (15) ‘shopping in a corner shop (butchery, bakery, newsagent)’ would correlate with ‘Can shop safely and completely independent in a known environment (moving on varied terrain included)’, (16) ‘shopping in a supermarket (inclusive displacement, loading and unloading goods)’ would correlate with ‘‘Can shop safely and completely independent in a known environment (moving on varied terrain included)’, (17) ‘Shopping in a shopping district or shopping centre’ would correlate with ‘Can move safely and independently in an unknown environment, for wheelchair use, including riding on and off pavements and small obstacles (moving on varied terrain included)’, (18) ‘use and transfer to several services (post office, bank, administrative services, etc.)’ would correlate with ‘Can independently carry out activities in or not in a wheelchair at an accessible public building (eg. Station, bank,…)’. 2.4. Discriminative validity Discriminative validity is an indication about the different results researches would expect between two measures who assess different constructs (Portney & Watkins, 2014). The discriminative validity is calculated by a correlation between the total score of the HODA- scale and the mean score of the Jamar. Before processing the date a ShapiroWilk normality test is conducted to determinate the distribution of the data. When this test is significant (p< .05), a non- parametric test will be applied. When this test is not significant (p>.05) a parametric test will be applied. Hypotheses Because the HODA-scale and the Jamar measure two different constructs, there is hypothesized that they will show a lower correlation than the correlation with the ELIDAscale. 2.5. Factorial Validity The factorial validity gives an indication about the factorial composition of a measurement. It is based on the correlation between the identified factors that determine the score on a test (Fawcett, 2009). 17 To conduct the factorial validity of the HODA-scale a confirmatory factor analyses was conducted to the data. The goal was to confirm on an empirically way the factor structure of the scale and identify possible additional underlying dimensions. There was a principal component used as the extraction method and in function to maximize the factor simplicity oblique rotation was used for the rotation method (Lorenzo- Seva, 1999). In order to check whether the data was suitable for a confirmative factor analysis the KaiserMeyer-Olkin was applied. This had to have a value greater than 0.70 (Tabachnick, 2007). Additionally a Bartlett’s test of sphericity was performed to check whether there were correlations in the data set who were suitable for a factor analysis and was defined as significant before processing the data (Tabachnick, 2007). 2.6. Internal consistence Internal consistency represents the extent to which items in an assessments scale are correlated. It is important to examine in scales who have the intention to identify one construct on basis of various items (Terwee et al., 2007). It is “the degree of interrelatedness among the items” (Mokkink et al., p. 743, 2010). The internal consistence of the HODA-scale was assessed using the Cronbach’s Alpha coefficient. The internal consistence is considered to be good when the results of the Cronbach’s Alpha range between 0.70 and 0.95 (Terwee et al., 2007). 2.7. Test- retest reliability Reliability can be defined as the coherence of scores when they are obtained by the same person and are measured again on a different time or with different sets or similar sets of items. When an assessment has a good test- retest reliability the test will give the same results (Marx et al. 2003). To examine the test- retest reliability of the HODA-scale the assessment instrument was conducted twice with a time interval of up to one week. On scale level an Intraclass Correlation Coefficient (ICC) was applied to the collected data with a confidence interval (CI) of 95% (two way random model – absolute agreement) . On item level a weighted kappa was applied. The reliability is rated as good if the ICC and the weighted kappa are greater or equal to 0.70 (Terwee et al., 2007). 18 3. Results 3.1. Study population The total study sample included 34 people diagnosed with a form of acquired brain injury. The response rate for testing construct validity was for the HODA- scale and the ELIDAscale 100% (n=34). All the patients who were assessed with the HODA- scale were also assessed by the ELIDA-scale. For the discriminant validity with the Jamar the response rate was lower, 47% (n= 16). For factorial validity and internal consistence the response rate was also 100% (n= 34) for the HODA- scale. For the test- retest reliability there was a response rate of 47% (n=16). Table 4: Characteristics of the participants (n=34) Age: mean (SD) 42,9 (11,7) Gender: male/female 21/13 Diagnosis: n (%) - Non- traumatic: other than stroke 7 (20,6) - TBI 8 (23,5) - Stroke 19 (55,9) Highest level of education: n (%) - General secondary education (12 to 18 years) 1 (2,9) - Technical and vocational secondary education (12 to 18 years) 14 (41,2) - Special secondary education (13 to 21 years) 1 (2,9) - Associate degree (18+) 2 (5,9) - University college (18+) 7 (20,6) - University (18+) 7 (20,6) - Unknown 2 (5,9) Family situation: n (%) 3.2. - Married with children 16 (47,0) - Married 0 - Couples living in a consensual union/registered partnership with children 2 (5,9) - Couples living in a consensual union /registered partnership 2 (5,9) - Single with children 4 (11,8) - Single 10 (29,4) Construct validity The Shapiro- Wilk normality test was significant (p<0.05), therefore a non-parametric test was performed, the Spearman-rank correlation coefficient. The Spearman correlation coefficient between the total score of the HODA-scale and the total score of the ELIDA-scale was .819 (significant at the 0.01 level, 2-tailed). 19 Figure 6: scatterplot correlation total HODA-scale – total ELIDA-scale An overview of the correlation between the congruent items of both assessment scales can be seen in table 5. Table 5: correlation HODA-scale items and ELIDA-scale items Item HODA-scale Item ELIDA-scale Spearman correlation coefficient (1) Heating a meal for example in the microwave Can independently prepare a simple meal .154 (2) Independent peeling and cutting potatoes Can independently prepare a simple meal .557** (3) Preparing a full meal, cooking process and timing Can safely and independently operate a stove and .634** preparation monitor heating and cooking (taking a pot or pan on and off included) (4) Setting and clearing of the table, inclusive hot and Can independently set and clear the table (including fragile material hot and brittle materials) Cleaning the kitchen and the dining room, washing Can independently wash and dry the dishes (including the dishes pots and pans) (6) Vacuum one or multiple rooms Can independently sweep the floor/ handle the vacuum (7) Mopping/wet (5) .632** .615** .643** cleaner cleaning (handle cleaning Can independently scrub the floor .761** convenience and bucket filled with water) (8) Cleaning windows (maximum three steps high) Can independently wash the windows .676** (9) Making the beds and change linens Can independently prepare and chance the bed .829** Can make a small hand wash by himself .315 (10) Perform hand wash (wash, rinse out, hang to dry) 20 (11) Filling, emptying and operating washing machine Can control, fill and empty a washing machine/dryer .431* Can safely use an iron and folds clothes .507** Can take autonomous objects and store it properly in .591** and dryer (12) Ironing and fold several linen (inclusive opening and closing the ironing board) (13) Storage in closets or racks and take out various household products and food. closets and storage spaces (eg. Clothing, household equipment) (14) Performing repairs and replacements in the house (replacing lamps, replacing batteries, etc.) (15) Keep supervision of the house and react Can independently do minor repairs or replacements in .584** the house (eg. Replacement of a lamp) - Independently have control over the state of the .419* appropriate (heating, open and close doors and house and functioning of devices (eg. Leaks, .429* windows, breakdowns, etc.) observing damage and respond appropriately) .429* - Can independently guarantee the necessary lighting, ventilation and shielding of the house (windows and (role)shutters, switches) - Can be independently responsible for opening and closing the doors of the house (16) Shopping in a corner shop (butchery, bakery, newsagent) Can shop safely and completely independent in a .679** known environment (moving on varied terrain included) (17) Shopping in a supermarket (inclusive displacement, loading and unloading goods) Can shop safely and completely independent in a .569** known environment (moving on varied terrain included) (18) Shopping in a shopping district or shopping centre Can move safely and independently in an unknown .562** environment, for wheelchair use, including riding on and off pavements and small obstacles (moving on varied terrain included) (19) Use and transfer to several services (post office, bank, administrative services, etc.) Can independently carry out activities in or not in a .528** wheelchair at an accessible public building (eg. Station, bank,…) **: Significant at 0.01; 2 tailed *: Signiant at 0.05; 2 tailed 3.3. Discriminative validity The Shapiro- Wilk normality test was not significant (p>0.05), therefore a parametric test should be performed, the Pearson correlation coefficient. De Pearson correlation coefficient between the total score of the HODA-scale and the mean score of the JAMAR was -.558 (significant at the 0.05 level, 2 tailed). 21 Figure 7: scatterplot correlation HODA-scale- Jamar 3.4. Factorial validity The Kaiser-Meyer- Olkin measure had a result of .634, the Bartlett’s test of sphericity was significant (X²= 1128.5, df=300, p<0.01). Communalities after extraction varied between .760 and .935. Two factors were identified. Factor one accounted for 63,54% of the total variance and factor two accounted 9,11% of the total variance. Table 6: factorial validity HODA-scale Item HODA-scale Factor 1 Factor 2 Total variance 63,54% 1. Heating a meal for example in the microwave .682 2. Independent peeling and cutting potatoes .817 3. Preparing a full meal, cooking process and timing preparation .817 4. setting and clearing of the table, inclusive hot and fragil material .865 5. Cleaning the kitchen and the dining room, washing the dishes .865 6. dust off furniture .820 7. vacuum one or multiple rooms .894 8. mopping/wet cleaning (handle cleaning convenience and bucket .865 9,11% filled with water) 9. cleaning windows (maximum three steps high) .850 22 10. making the beds and change linens .929 11. perform hand wash (wash, rinse out, hang to dry) .805 12. filling, emptying and operating washing machine and dryer .835 13. ironing and fold several linen (inclusive opening and closing the .909 ironing board) 14. cleaning the house (loose scattered clothing, various objects, .833 lecture, etc.) 15. storage in closets or racks and take out various household .819 products and food. 16. performing repairs and replacements in the house (replacing .883 lamps, replacing batteries, etc.) 17. collect and sort garbage and placing it on the streetside. .896 18. Management of the required reserves of household equipment .692 and making a shopping list 19. Keep supervision of the house and react appropriate (heating, .659 .406 20. Financial management household. .605 .305 21. shopping in a corner shop (butchery, bakery, newsagent) .657 .560 22. shopping in a supermarket (inclusive displacement, loading and .603 .537 23. Shopping in a shopping district or shopping centre .709 .453 24. shopping online .766 .249 25. use and transfer to several services (post office, bank, .709 .516 open and close doors and windows, breakdowns, etc.) unloading goods) administrative services, etc.) 23 3.5. Internal consistence The Cronbach’s Alfa for internal consistence is .975. The item- total correlation ranged between .592 to .910. An overview can be seen in table 7. Table 7: item- total correlation HODA-scale Item HODA-scale Item- total correlation 1. Heating a meal for example in the microwave .661 2. Independent peeling and cutting potatoes .785 3. Preparing a full meal, cooking process and timing preparation .796 4. setting and clearing of the table, inclusive hot and fragile material .845 5. Cleaning the kitchen and the dining room, washing the dishes .843 6. dust off furniture .793 7. vacuum one or multiple rooms .877 8. mopping/wet cleaning (handle cleaning convenience and bucket filled with water) .838 9. cleaning windows (maximum three steps high) .821 10. making the beds and change linens .910 11. perform hand wash (wash, rinse out, hang to dry) .783 12. filling, emptying and operating washing machine and dryer .812 13. ironing and fold several linen (inclusive opening and closing the ironing board) .889 14. cleaning the house (loose scattered clothing, various objects, lecture, etc.) .808 15. storage in closets or racks and take out various household products and food. .789 16. performing repairs and replacements in the house (replacing lamps, replacing batteries, etc.) .872 17. collect and sort garbage and placing it on the streetside. .879 18. Management of the required reserves of household equipment and making a shopping list .674 19. Keep supervision of the house and react appropriate (heating, open and close doors and windows, .643 breakdowns, etc.) 20. Financial management household. .592 21. shopping in a corner shop (butchery, bakery, newsagent) .642 22. shopping in a supermarket (inclusive displacement, loading and unloading goods) .596 23. Shopping in a shopping district or shopping centre .701 24. shopping online .756 25. use and transfer to several services (post office, bank, administrative services, etc.) .705 3.6. Reliability The reliability statistics gave the result of a Cronbach’s alfa of .978. The ICC single measures is .957 with a CI between .957 and .964. The kappa resulted in .560. 24 Discussion Before discussing the results of this study a few limitations should be explained. First completing the assessments was done only by questioning the patients. The manual of the assessments states that the assessor has to question and observe the patients and should consult the patient his file. In this study it was not possible to observe all the activities which were represented by the HODA-scale. Therefore after questioning the patient, we went through the assessment with the occupational therapist that worked with that specific patient. Second, for the evaluation of the test-retest reliability the assessment was only filled in based on the answers of the patient. It is import when using this approach to take into account that a lot of patients with a brain injury haven an impaired self- awareness what makes that the patient minimizes limitations and difficulties caused by the injury (Caldwell et al., 2014). Therefore the psychometric properties should be evaluated in other pathology groups to provide a complete and accurate picture of the psychometric properties. Lastly, the overall sample size is small and for reliability and discriminative validity they are even smaller which can have an influence on the results. The overall aim of this master thesis was to conduct the possibility of the HODA-scale to be converted to ICF categories and to contribute in this way to the covering of the TBI core set. In addition to this an evaluation of the psychometric properties of the scale was conducted. The conversion included two expert panels who came together once. Previous investigation showed that it is the intention to keep the discussion about the most appropriate category of the ICF until consensus is reached (De Vriendt et al. 2012). This was not done in this study, instead an online survey was send to the different experts. A negative aspect of this approach was that one expert did not answered the online survey and therefore the HODA-scale was converted with a reduced number of experts for these two items. The converted HODA-scale covered only a few items from the core set. Besides the conversion, five psychometric properties of the HODA-scale were examined. The construct validity with the ELIDA scale on scale level indicated a good significant result of .819 which was above the limit of .70 as given by Terwee et al. (2007). However on item-level the correlations were lower than was hypothesised for most of the items. Only for hypothesis six ‘mopping/wet cleaning (handle cleaning convenience and bucket 25 filled with water)’ which was assumed to correlate with ‘Can independently scrub the floor’ and hypothesis eight ‘making the beds and change linens’ which was assumed to correlate with ‘Can independently prepare and chance the bed’ the limit of .70 was reached with .761 for hypothesis six and .829 for hypothesis eight, both significant. The lower correlations are remarkable because at first side there is an agreement between the items, they handle about the same concept. The discriminative validity was obtained by a correlation with the Jamar. As hypothesized this correlation would be lower because of the different constructs. The result was a negative and a moderate correlation. The negative sign of the correlation can indicate that it is possible to have a good score on the Jamar but a low score on the HODA-scale or when one has a high score on the HODA-scale one will have a low score on the Jamar. In other words a patient with a high score on the HODA-scale will have a lower grip strength and one with a good grip strength will have a lower HODA-scale score and less problems with fulfilling domestic tasks. The factorial validity of the HODA-scale was performed by a confirmatatory factor analysis. The Kaiser-Meyer-Olkin was .634 which is lower than .70. This can be explained by the small sample size. But because the Bartlett’s test of sphericity was significant and the score of the Kaiser-Meyer-Olkin was moderate a factor analyse could be performed. All items of the assessment were mostly loaded on the first factor. A small part of them were loaded on the second one. The HODA-scale originally consists of five components and 25 items. The result of this factor analysis does not confirm these five factors, but shows only two. This result offers opportunities to reduce the number of items in two subscales to obtain the same results. However, when all items are relevant to obtain a detailed view of the patients’ functioning, one can decide to keep the items instead of removing them from the scale. The internal consistency of the HODA-scale gave an Cronbach’s Alfa of .975, which falls outside the limits of .70 and .90 reported by Terwee et al. (2007). A high Cronbach’s Alfa could point to an excess of items in the scale (Terwee et al. 2007). It may refer to an unnecessary duplication of items and to redundancy of items instead of homogeneity (Streiner, 2003). The item-total correlation varied .592 to .910. The literature states that 26 a strong internal consistency includes a moderate correlation between the items that vary between .70 and .90. Some items of the HODA-scale are under or above this limit which can indicate that when they are too low they measure possibly different characteristics and when it is too high the items can be redundant which may have an influence on the content validity (Portney & Watkins, 2014). The test-retest reliability gave an ICC of .957 and a weighted kappa of .560. The ICC gives an idea about the reliability on scale level and is indicated as good (above .70). The weighted kappa was too low and indicates there is only for 56% an agreement on the different items for the test and the retest. An explanation for this can be due to the three different scores one gets on the HODA-scale. All items who get a score from zero to two are separately added from the items with the scores from three to four. These are named as more effort and time to perform (score zero to two) and help from others (score three to four). When these two scores are counted together a patient can have the same total score but these both can vary. Conclusion The HODA-scale is an assessment instrument to indicate the total damage in domestic tasks after injury. It is based on the scoring-system of the ICF and also the items are based on chapter six of the ICF. It is successfully converted to ICF categories and it covers some items in the core set for TBI. The psychometric properties of the HODA-scale evaluated with people with an ABI are moderate (take the small sample size into account), but there is more research needed to conduct these properties in other patient populations. 27 References 1. Andelic, N., Sigurdardottir, S., Schanke, A.K., Sandvik, L., Sveen U. & Roe, C. (2010). Disability, physical health and mental health 1 year after traumatic brain injury. Disability and Rehabilitation, 32(13), 1122-1131. 2. Barnabeu, M., Laxe, S., Lopez, R., Stucki, G., Ward, A., Barnes, M., Kostanjek, N., Reed, G., Tate, R., Whyte, J., Zasler, N. & Cieza, A. (2009). Developing core sets for persons with traumatic brain injury based on the International Classification of Functioning, disability and health. Neurorehabilitation and Neural Repair, 26(5), 464-467. 3. Bellace, J.V., Healy, D., Besser, M.P., Byron T. & Hohman, L. (2002). Validity of the Dexter Evaluation system’s Jamar Dynamometer attachment for assessment of hand grip strength in a normal population. Journal of Hand Therapy, 13, 46-51. 4. Bohannon, R.W., Peolsson, A., Massy-Wesropp, N., Desrosiers J. & Bear-Lehman, J. (2006). Reference values for adult grip strength measured with a Jamar dynamometer: a descriptive meta-analysis. Physiotherapy, 92, 11-15. 5. Brusselmans, W., Thomas, T., Cook C. & Vermeulen, K. (2014). Housekeeping Damage scale. Ongepubliceerd manuscript, Universitair Ziekenhuis Gent, Gent, België. 6. Brusselmans, W. (1992). Estimate of Loss of Independence in Daily Activities Scale. Geraadpleegd op 12 november 2015 via http://ergos.deds.nl/arbd/file/elida_nl.pdf 7. Caldwell, S.B., Wilson, F.C., McBrinn, J., Carton, S., Delargy, M., McCann, J.P, Walsh J. & McGuire, B.E. (2014). Self- awareness following acquired brain injury: measurement and relationship to executive functioning. The Irish Journal of Psychology, 35, 53-68. 28 8. Cieza, A., Brockow, T., Ewert, T., Amman, E., Kollerits, B.,B., Chatterji, S., Üstün, T.B. & Stucki, G. (2002). Linking healt-status measurements to the International Classification of Functioning, disability and health. Journal of Rehabilitation Medicine, 34, 205-2010. 9. Cieza, A., Geyh, S., Chatterji, S., Kostanjsek, N., Üstün, B. & Stucki, G. (2005). ICF-Linking rules: an update based on lessons learned. Journal of Rehabilitation Medicine, 37, 212-218. 10. Cochrane, J., Goering, P., Durbin, J., Butterill, D., Dumas, J.& Wasylenki, D. (2000). Tertiary mental health services: II. Subpopulations and best practices for service delivery. The Canadian Journal of Psychiatry, 45(2), 185- 190. 11. De Vriendt, P., Gorus, E., Bautmans I. & Mets, T. (2012). Conversion of the MiniMental State Examination to the International Classification of Functioning, disability and health terminology and scoring system. Gerontology, 58, 112-119. 12. De Wit, L., Putman, K., Lincoln, N., Baert, I., Berman, P., Beyens, H., Bogaerts, K., Brinkmann, N., Conell, L., Dejaeger, E., De Weerdt, W., Jenni, W., Lesaffre, E., Leys, M., Louckx, F., Schuack, B., Schupp, W., Smith B. & Feys, H. (2006). What do physiotherapists and occupational therapist actually do? Stroke, 37, 1483-1489. 13. Fawcett, A.L. (2007). Principles of assessment and outcome measurement for occupational therapists and physiotherapists: theory, skills and application. WestSussex: John Wiley & Sons. 14. Fayed, N., Cieza A. & Bickenbach, J.E. (2011). Linking health and health-related information to the ICF: a systematic review of literature from 2001 to 2008. Disability and Rehabilitation, 33(21-22), 1941-1951. 29 15. Goljar, N., Burger, H., Vidmar, G., Marincek, C., Krizaj, J., Chatterji, S., Raggi,, A., Leonardi, M. & Bickenbach, J.E. (2010). Fuctioning and disability in stroke. Disability and Rehabilitation, 32, S50-S58. 16. Lafayette Instrument. (2004). Jamar hydrolic hand dynamometer user instructions. Geraadpleegd op 18 maart 2016 via https://henrotech.be/sites/default/files/product/manual/Instruction%20Jamar%20Han d%20Dynamometer%20NL%20%20-%20%20Henrotech.pdf 17. Lannoo, E., Larmuseau, D., Van Hoorde, W., Ackaert, K., Lona, M., Leys, M., De Barsy T. & Eyssen, M. (2007). Chronische zorgbehoeften bij personen met een nietaangeboren hersenletsel (NAH) tussen 18 en 65 jaar: KCE reports 51A. Brussel: Federaal Kenniscentrum voor de Gezondheidszorg (KCE). 18. Laxe, S., Zasler, N., Robles, V., López- Blázquez, R., Tormos, J.M. & Bernabeu, M. (2014). ICF-profiling of patients with traumatic brain injury: an international professional survey. Disability and Rehabilitation, 36(1), 82-88. 19. Lorenzo-Seva, U. (1999). Promin: A method for oblique factor rotation. Multivariate Behavioural Research, 34, 347-365. 20. Marx, R.G., Menezes, A., Horovitz, L. Jones, E.C. & Warren, R.F. (2003). A comparison of two time intervals for test- retest reliability of health status instruments. Journal of Clinical Epidemiology, 50, 730-735. 21. Mathiowetz, V. (2002). Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occupational Therapy International, 9(3), 201-209. 22. Menon, D.K., Schwab, K., Wright D.W. & Maas, A.I. (2010). Position statement: definition of Traumatic Brain Injury. Archive Physical and Medical Rehabilitation, 91, 1637-1640. 30 23. Mokkink, L.B., Terwee, C.B., Patrick, D.L., Alonso, J., Stratford, P.W., Knol, D.L., Bouter L.M. & De Vet, H.C.W. (2010). The COSMIN study reached international consensus on taxonomy, terminology and definitions of measurement properties for health-related patient-reported ouctomes. Journal of Clinical Epidemiology, 63, 737745. 24. O’Reilly, K. & Pryor, J. (2002). Young people with brain injury in nursing homes: not the best option! Australian Health Review, 25(3), 46-51. 25. Portney L.G. & Watkins, M.P. (2014). Foundations of Clinical Research: applications to practice. Essex: Pearson Education Limited. 26. Ptyushin, P., Vidmar, G., Burger H. & Marincek, C. (2012). Use of the International Classification of Functioning, disability and health in traumatic brain injury rehabilitation. American Journal of Physical and Medical Rehabilitation, 91(suppl), S48-S54. 27. Semlyen, J.K., Summers S.J. & Barnes, M.P. (1998). Traumatic Brain Injury: Efficacy of multidisciplinary rehabilitation. Archives of Physical Medicine and Rehabilitation, 79(6), 678-683. 28. Streiner, D.L. (2003) Starting at the beginning: an introduction to coefficient alpha and internal consistency. Journal of Personality Assessment, 80(1), 99-103. 29. Stucki, G;, Kostanjsek, N., Üstün, B. & Cieza, A. (2008). ICF-based classification and measurement of functioning. Journal of Physical and Rehabilitation Medicine, 44(3), 315-328. 30. Svestkova, O., Angerova, Y., Sladkova, P., Bickenbach J.E. & Raggi, A. (2010). Functioning and disability in traumatic brain injury. Disability and Rehabilitation, 32, S68-S77. 31 31. Tabachnik, C.B. (2007). Using multivariate statistics. Bosten: Pearson Education Inc. 32. Terwee, C.B., Bot, S.D.M. De Boer, M.R. Van Der Windt, D.A.W.M., Knol, D.L., Dekker, J., Bouter L.M. & De Vet, H.C.W. (2007). Quality criteria were proposed for measurement properties of health status questionnaires. Journal of Clinical Epidemiology, 60, 34-42. 33. Turner-Stokes, L., Williams, H., Sephton, K., Rose, H., Harris S. & Thu, A. (2012). Engaging the hearts and minds of clinicians in outcome measurement – the UK rehabilitation outcomes collaborative approach. Disability and Rehabilitation, 34(22), 1871-1879. 34. Van der Putten, J.J.M.F., Hobart, J.C. & Thompson, A.J. (1998). Measuring change in disability after inpatient rehabilitation: comparison of the responsiveness of the Barthel Index and the Functional Independence Measure. Journal of Neurology, Neurosurgery and Psychiatry, 66, 480-484. 35. Watanabe, T.K., Miller M.A. & Mc Elligott, J.M. (2003). Congenital and acquired brain injury. 5. Outcomes after acquired brain injury. Archive of Physical and Medical Rehabilitation, 84, s23-27. 36. World Health Organization. (2001). International Classification of Functioning, Disability and Health. Geneva: World Health Organization. 37. Yen, T.H., Liou, T.H., Chang, K.H., Wu, N.N., Chou L.C., & Chen, H.C. (2014). Systematic review of ICF core set from 2001- 2012. Disability and Rehabilitation, 36(3), 177-184. 32 Appendix Appendix A: Occupational therapy in core set TBI ICF-categories core set TBI for occupational therapy ICF- categories core set TBI covered by HODAscale d155 Ontwikkelen van vaardigheden d175 Oplossen van problemen d177 Besluiten nemen d210 Ondernemen van enkelvoudige taak d220 Ondernemen van meervoudige taken d230 Uitvoeren van dagelijkse routinehandelingen d430 Optillen en meenemen d440 Nauwkeurig gebruiken van hand d445 Gebruiken van hand en arm d470 Gebruiken van vervoermiddel d510 Zich wassen d620 Verwerven van goederen en diensten x d640 Huishouden doen x d825 Beroepsopleiding d840 Werkend leren d850 Betaald werk 33 d860 Basale financiële transacties x d865 Complexe financiële transacties d870 Economische zelfstandigheid e115 Producten en technologie voor persoonlijk gebruik in het dagelijks leven e135 Producten en technologie voor werkdoeleinden e165 Activa e590 Voorzieningen, systemen en beleid met betrekking tot werkgelegenheid 34 Appendix B: HODA-scale 35 Appendix C “De auteur en de promotor geven de toelating deze masterproef voor consultatie beschikbaar te stellen en delen ervan te kopiëren voor persoonlijk gebruik. Elk ander gebruik valt onder de beperkingen van het auteursrecht, in het bijzonder met betrekking tot de verplichting uitdrukkelijk de bron te vermelden bij het aanhalen van resultaten uit deze masterproef.” Datum: (handtekening student) (handtekening promotor) (Naam student) (Naam promotor) 36 List of figures - Figure 1: The ICF-framework - Figure 2: ICF- qualifiers - Figure 3: item 1 online survey - Figure 4: item 2 online survey - Figure 5: test protocol - Figure 6: scatterplot correlation total HODA-scale and total ELIDA-scale - Figure 7: scatterplot correlation total HODA-scale and mean Jamar 37 List of tables - Table 1: ICF-linking rules - Table 2: Conversion of the HODA-scale - Table 3: Scoresystem HODA-scale based on the ICF score criteria - Table 4: characteristics of the participants - Table 5: correlation HODA-scale items and ELIDA-scale items - Table 6: factorial validity of the HODA-scale - Table 7: item-total correlation HODA-scale 38
© Copyright 2026 Paperzz