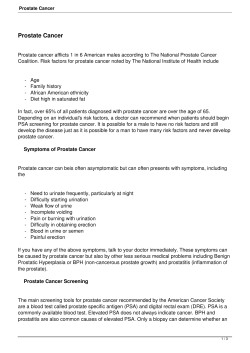
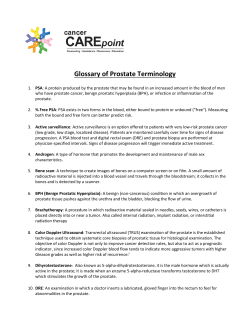
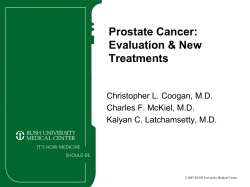
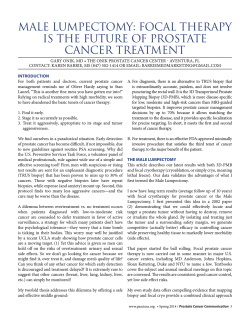
PCRI Patient & Physician in Co-Partnership nsights New Developments in Prostate Cancer Treatment MAY 2005 VOL 8: NO 2 The PCRI Today: A Repor t f rom the Execut ive D irector As PCRI approaches its tenth anniversary, it is useful to look back briefly at the early days of the organization in contrast with the PCRI today. PCRI was founded by two prostate cancer oncologists, Drs. Stephen Strum and Mark Scholz. Drs. Strum and Scholz were hopeful that an organization combining insightful clinical research with high-level educational activities, PCRI Executive Director, directed to both the patient and the Glenn D. Weaver physician, would greatly enhance outcomes for prostate cancer patients everywhere. Over the years, the PCRI has changed from a founder-driven clinical research-based organization to a mission-based organization, and as such the mission of the PCRI has evolved into the vital role of disseminating information and prostate cancer education and patient awareness: The Prostate Cancer Research Institute’s mission is to improve the quality of men’s lives by supporting research and disseminating information that educates and empowers patients, families and the medical community. The evolution of the PCRI has reflected the changes that have taken place in the prostate cancer community as a whole. There are a number of leading organizations that are The goal of education is the committed to the fight advancement of knowledge against prostate cancer. and the dissemination of truth. Among them are –John F. Kennedy (alphabetically listed) the American Cancer Society, the American Society of Clinical Oncology, the American Urological Association, the Foundation for Cancer Research & Education, Patient Advocates for Advanced Cancer Treatment, the Prostate Cancer Foundation, and Us TOO International – as well as the PCRI. continued on page 11 A B O U T T H E M E D I C A L A RT I C L E S I N T H I S I S S U E What Every Doctor Who Treats Male Newer Concepts in the Treatment of HRPC with Bone Metastases Patients Should Know By Oliver Sartor,MD By Stephen B.Strum,MD,FACP and Donna Pogliano Bone metastases with pain represent a common and significant problem for patients with advanced prostate cancer. Data from prospective randomized clinical trails now support the use of Samarium-153-EDTMP in patients with Hormone-Refractory PC and painful bone metastases. Pain relief and decreases in analgesic consumption can be expected in the majority of patients treated. Side effects are limited to transient and relatively mild platelet and white blood cell suppression. Combination therapies that incorporate cytotoxic agents such as Taxotere in combination with Strontium-89 or Samarium-153-EDTMP regimens are now being actively explored in clinical trials. This approach has the potential of promoting synergy between active agents. Preliminary data suggest that this might be of considerable interest. This article is directed at General Practitioners and other medical professionals who are not familiar with modern prostate cancer clinical practice. The article covers screening tools such as PSA and uPM3, describes how to differentiate benign prostate conditions from prostate cancer, and explains the role of such PSA derivatives as free-PSA percentage, PSA velocity, and PSA doubling time.The article goes on to discuss slow-growing versus aggressive prostate cancer as diagnosed by PSA level, PSA doubling time, Gleason score and other biomarkers, and how this information affects the decision between active objectified observation and immediate local therapy. Dr. Strum concludes that with this information we can detect prostate cancer at a time when currently available therapies are most likely to cure the disease. Who’s Really at Risk for What? By Mark C.Scholz,MD and Ralph Blum Dr. Scholz is struck by the prodigious efforts men make to understand and get appropriate treatment for prostate cancer while ignoring the fact that they are at greater risk of dying from other causes unrelated to prostate cancer. Therefore, he has written this article to provide advice to prostate cancer patients about health issues unrelated to prostate cancer. The goal of the article is to bring the risks associated with prostate cancer into perspective with the risks of other potentially serious illness, including heart attacks, osteoporosis, colon cancer, sarcopenia, lung cancer, and melanoma. For each of these diseases, he suggests preventive and/or early detection steps men can and should take. The article is accompanied by a useful description of laboratory blood tests and what they may reveal. Newer Concepts in the Treatment of Hormone-Refractory Prostate Cancer with Bone Metastases: Combinations of Bone-Seeking Radiopharmaceuticals and Chemotherapy Oliver Sartor, MD Chief, Hematology-Oncology Section; Director, Stanley S. Scott Cancer Center, LSU Health Sciences Center, New Orleans, LA PAIN FROM BONE METASTASIS IS ONE OF THE MOST DIFFICULT CLINICAL PROBLEMS IN PATIENTS WITH HORMONE-REFRACTORY PROSTATE CANCER (HRPC). Radiographic evidence of distant metastatic spread to bone occurs in the vast majority of cases of latestage disease, and in most patients these lesions are osteoblastic (bone-forming) in nature. The most reliable method of detecting bone metastases in a prostate cancer patient is a conventional bone scan.However,even in a patient with prostate cancer, not all areas of enhanced uptake on bone scan are associated with metastatic disease, particularly in the case of solitary lesions or uptake in joints. Confirmation of metastases by additional imaging modalities such as plain radiographs or MRI scans may be needed prior to making a clear diagnosis. Bone metastases may or may not be associated with painful symptoms when initially detected.1 In patients initially diagnosed with bone metastases and then subsequently treated with hormonal therapy, Newling and colleagues have determined that increases in serum PSA occur approximately six months 99m Tc-MDP Anterior 153 prior to changes in bone scan which in turn occur approximately four months prior to patient reports of pain.2 The timing of this sequence of events in patients treated with hormonal therapy before the onset of bone metastases (most patients today) has not been well studied, but the interval between PSA rise and the onset of a positive bone scan is suspected to be much longer (more than two years on average). Even in patients with a positive bone scan who report painful symptoms, a comprehensive examination may be needed to establish the cause of the pain and evaluate any possible complicating factors such as spinal cord compression, neuropathic conditions, and pathologic fractures. Patients with bone metastases may also have non-malignant sources of bone pain, and the causes of such pain need to be evaluated on a case by case basis.It is not uncommon for arthritis or other benign problems to cause pain in a patient with cancer. A number of therapies for advanced prostate cancer are available, including secondary hormonal manipulations, external beam radiation, bone-seeking radiopharma- Sm-EDTMP 99m Tc-MDP Posterior Conventional bone scan (99mTc-MDP) versus 153Sm-EDTMP demonstrating identical uptake. 153 Sm-EDTMP emits an imageable 103 keV gamma photon that can be viewed up to 3-5 days after the initial injection by either planar or single photon emission computed tomography (SPECT). Uptake and distribution of 153Sm-EDTMP are similar to those of 99mTc-MDP used in bone scans. Comparison of the two images produced by gamma radiation emitted by gamma radiation emitted from 153Sm-EDTMP and 99mTc-MDP in the same patient illustrates how similar the radiographs produced by 153Sm-EDTMP are. Thus, 153Sm-EDTMP may also be used for diagnostic imaging. Images courtesy of Todd Hoover. 2 PCRI INSIGHTS ceuticals, and systemic chemotherapy (see Table 1). External beam radiation provides excellent palliation for focal painful lesions, but in patients with systemic disease, repeated courses are typically required for effective treatment. The approach to decreasing the intensity of pain from bone metastases varies depending on a number of factors including degree of symptoms, extent of disease and prior treatments. Analgesics, anti-tumor agents, hormones, chemotherapy, steroids, local surgery, bisphosphonates, anesthesia, and radiation therapy (local and systemic) are all appropriate treatments under selected circumstances. In general, a combination of systemic and local modalities is required, and no single treatment regimen is effective for an extended period of time. Of the many options available for HRPC, one treatment option that I will focus upon in this brief discussion involves the newer concept of combining intravenous radiopharmaceuticals with chemotherapy for possible synergy. Three radionuclides are currently approved for the treatment of metastatic bone pain: phosphorous-32 (32P), strontium-89 (89Sr or Metastron), and samarium-153 (153Sm-EDTMP or Quadamet). These radionuclides all localize to regions of enhanced bone turnover and deliver high local doses of radiation through the emission of beta particles.The mechanism of bone targeting varies for each of them. Phosphorous32 is targeted to bone through inorganic phosphate pathways while strontium-89 is taken up as a calcium analog. Samarium-153 is targeted to bone via its chemical conjugation to EDTMP (ethylenediaminetetramethylenephosphonic acid). The relevant nuclear decay properties of these radionuclides are shown in Table 2. Decay properties such as half-life and particle energy play significant roles in such important clinical characteristics of these agents as onset and duration of palliative effects and degree of and time to recovery from bone marrow suppression. The particle emission energies of 32P and 89Sr and the corresponding ranges in bone and soft tissue are NEWER CONCEPTS IN THE TREATMENT OF HRPC FROM PAGE 2 radionuclides in combination with chemomuch greater than those of 153Sm.Higher enerTable 1. Therapies for therapeutics.The first of these trials was pubgy particles are associated with greater marHormone-Refractory Prostate Cancer lished by Tu and colleagues5,who used a comrow toxicity as the result of the larger volumes bination of 89Sr and doxorubicin.Patients were of marrow exposed to radiation. The shorter 1. Anti-androgen (bicalutamide, 153 randomized to receive either doxorubicin physical half-life of Sm (1.9 days) results in a nilutamide, flutamide) withdrawal alone or in combination therapy after first more rapid delivery of radiation than either 32P 2. Anti-androgen (bicaluitamide, being treated with a combination therapy of (14.3 days) or 89Sr (50.5 days). For example, flutamide, nilutamide) ketoconazole, doxorubicin, estramustine, and delivery of 90% of the total dose of radiation administration vinblastine. Of note, this combination of requires approximately 3.5 half-lives of decay, 3. Adrenal suppressives such as agents is no longer used. Only patients with a time interval of approximately one week for ketoconazole 153 32 89 stable disease or responding disease after the Sm,seven weeks for P and 25 weeks for Sr. 4. Estrogens such as DES plus warfarin preliminary therapy were eligible for the ranThe current relative indications and con5. Glucocorticoids such as prednisone domization. Patients randomized to the comtraindications for the use of bone-targeted or dexamethasone bination of 89Sr and doxorubicin had a longer radiopharmaceuticals are presented in Table 6. Bisphosphonates (zolendronate in survival compared to those patients who were 3. Baseline complete blood counts are necesbone scan positive patients) treated with doxorubicin alone.This trial supsary to establish adequate pretreatment levels 7. External beam radiation therapy ports the concept that targeting bone and of platelets and white blood cells since all of using a radiosensitizing chemotherapy (in 8. Bone-seeking radiopharmaceuticals these agents result in some suppression of combination) might be an effective therapeu(bone scan positive patients) bone marrow function. Severe renal dysfunctic approach. 9. Chemotherapy (docetaxel, tion is a contraindication to the use of bonemitoxantrone, etc.) Preliminary data is available regarding the targeted radionuclides because currently combination of 153Sm-EDTMP and docetaxel available agents are predominantly excreted 10. Experimental Therapies in patients with hormone refractory prostate by the kidney. cancer. In a phase I study conducted in Several prospective randomized Table 2. Nuclear Decay Properties and 3,4 Sweden by Widmark and colleagues6 controlled studies have been perBone Penetration Depth of Radionuclides that examined preliminary efficacy, six formed to evaluate the effectiveness of Approved for Treatment of Metastatic Bone Pain patients were treated with weekly docusing bone-seeking radiopharmaceutiHalf-life β-Emission Penetration Radionuclide etaxel at a dose of 30 mg/m2, in combicals to relieve the pain of bone metas(days) (Avg, MeV) (mm) nation with a dose of 1.0 mCi/kg given in tases in HRPC patients. One of the Phosphorous-32 14.3 0.7 2.7 week four, 24 hours prior to treatment largest of these trials was published by Strontium-89 50.5 0.58 2.4 4 with docetaxel.38 Optimal uptake by Sartor and colleagues in 2004 evaluatSamarium-153 1.9 0.22 0.55 tumor sites was seen 8-24 hours after ing 153Sm-EDTMP. In this prospective, injection. Five of the six patients had a multi-center, randomized, double-blind, decrease in PSA of >50% and four of the six placebo-controlled study in patients with Table 3. Indications and had a decrease in PSA of >80% which persistbone metastases from hormone-refractory Contraindications to the use of Bone ed for more than six months.Toxicity was not prostate cancer,152 patients were randomized Targeted Radiophamaceuticals for dose limiting; only one episode of neuin a 1:2 ratio to placebo (n=51) or a 1.0 Treatment of Metastatic Bone Pain tropenic fever was reported.This study clearly mCi/kg dose of the active drug (n=101) and deserves additional follow up and expanded Indications were followed for up to 16 weeks.Pain intensipatient numbers. ty was measured twice daily (by patients) ❍ Bone Scan Positive In another preliminary study (by Arnsusing validated linear and non-linear scales. • Osteoblastic Lesions meier and colleagues)7, six patients with Daily opioid analgesic use was also recorded. ❍ Bone Pain Due to Cancer metastatic prostate cancer were treated with Patients who received the active drug exhibit❍ Multi-focal Disease paclitaxel 200 mg/m2 q for three weeks with ed significant improvements (as compared to Relative Contraindications estramustine and of 153Sm-EDTMP. Subsethe placebo group) in pain scores at each of quent groups of six patients were each treated ❍ Predominant Soft-tissue Pain the first four weeks following administration. with paclitaxel 90 mg/m2 q for three weeks. This decrease in pain occurred while pain ❍ Unifocal Bone Lesions 153 Sm-EDTMP was administered with chemomedications were decreased.These data clear❍ “Osteolytic”Lesions 153 therapy, starting with a dose of 1 mCi/kg and ly demonstrate that Sm-EDTMP can reduce • Poor Uptake on Bone Scan escalating in 0.5 mCi/kg dose increments. pain from bone metastases in patients with Absolute Contraindications Moderate decreases in white cells were seen in HRPC. Toxicity was mild and was limited to ❍ Severe Marrow Suppression one of the six patients at the 1.5 mCi/kg dosetransient decreases in white cells and platelets. level, but no significant toxicity had been ❍ Severe Renal Dysfunction Recently, considerable interest has emerged in the use of skeletal targeted continued on page 10 PCRI INSIGHTS 3 What Every Doctor Who Treats Male Patients Should Know Stephen B. Strum, MD, FACP Medical Oncologist Specializing in Prostate Cancer and Donna Pogliano Prostate Cancer Advocate Clinical Practice Prostate Cancer Diagnosis Guidelines Starting at forty years of age, every man should have an annual PSA (prostate-specific antigen) test and a DRE (digital rectal examination).Men at risk due to a family history of prostate cancer (brothers,fathers)1-3,men with a family history of breast cancer (mothers, sisters, aunts)1,4-6 and African-American men should begin annual screening at age 35. A PSA of 2.0 and over at any age should be investigated to rule out prostate cancer. A first step in investigation of a PSA elevated at 2.0 or above should be a free-PSA percentage test. • A free-PSA percentage of more than 25% is associated with a low risk of prostate cancer. • A free-PSA percentage of less than 15% is associated with a higher risk of prostate cancer7. An elevated PSA and a correspondingly low free PSA percentage can be caused by prostatitis, which is a benign rather than a malignant condition.If prostatitis symptoms are noted and/or if expressed prostatic secretions are consistent with prostatitis, four to six weeks of Cipro or similar antibiotic should be prescribed prior to recommending a biopsy. At the end of the Cipro therapy, a repeat PSA determination should be made.If there is significant lowering of the PSA, an element of prostatitis is likely to be present. The PSA value after antibiotic therapy will more aptly reflect the status of the patient in the situation where a diagnosis of prostate cancer is subsequently established. BPH (benign prostate hyperplasia) does not cause a low free PSA percentage. It may cause an elevated PSA, however. Therefore, in the case of an elevated PSA but a high free PSA percentage (equal to or greater than 25%),an estimate of gland volume by DRE or via transrectal ultrasound of the prostate may reveal findings consistent with a diagnosis of BPH.A general rule of thumb is that an accurate gland volume (best determined by transrectal ultrasound of the prostate) x 0.066 will equal the amount of benign-related PSA. Therefore, assuming only the presence of 4 PCRI INSIGHTS BPH, a 60-gram or 60 cubic centimeter prostate is entitled to secrete approximately 3.96 ng of PSA into the blood. PSA velocity (PSAV) and PSA doubling time (PSADT) are important markers that can indicate the existence of prostate cancer. Blood sampling for PSA determinations,done at least three months apart, and by the same laboratory using the same testing procedure, are necessary to establish PSAV and PSADT. The validity of such determinations is increased if such testing involves at least three determinations over an 18-month span of time. However, a progressive and serial increase in PSA values should raise concern that prostate cancer is present and that a greater degree of vigilance is mandatory. • A PSAV that exceeds 0.75 ng/ml/yr is associated with a higher probability of PC.8 • A PSADT of less than 12 years is associated with a higher probability of PC. PSA readings that bounce up and down are more indicative of a benign process than a malignant process. A PSA that shows a persistent rise over time, particularly three consecutive rises three months apart,is suspicious for prostate cancer regardless of the PSA level. Any amount of PSA in excess of the measured benign-related PSA should be considered to have been produced by a malignant process until proven otherwise. Recently,an additional new screening tool has become available. Bostwick Laboratories now offers the uPM3 test, the first urinebased genetic test for prostate cancer.uPM3 is based on PCA3, a specific gene that is profusely expressed in prostate cancer tissue. On average, the amount of PCA3 is 34 times greater in malignant prostate tissue than it is in benign prostate tissue.No other human tissues have ever been shown to produce PCA3. The uPM3 test predicts cancer as confirmed by prostate biopsy with 81% accuracy, compared to 47% accuracy for PSA. Therefore, after an elevated PSA, further investigations might reasonably include uPM3 testing to enhance the accuracy of diagnosis. Systematic biopsy of the prostate under ultrasound guidance, however, remains the definitive diagnostic procedure when clinical and/or laboratory findings indicate the possibility of prostate cancer. An approach using biological detection techniques such as those described above would eliminate advanced presentations of PC. Annual screening in this manner presents us with an opportunity to detect localized PC in over 95% of men.9 Such statistics offer an outstanding chance for a curative approach to this disease. An approach involving these profiling techniques allows the patient-physician team to discern the three major types of PC manifestation using the analogy of the tortoise,the hare and the raven (see Figure 1). The tortoise represents the very slow growing presentation of prostate cancer that may be monitored using active objectified surveillance (so-called watchful waiting) as opposed to the garden variety prostate cancer case (the hare),for which local treatment typically results in long-term biological eradication of disease.Most importantly, attention to PSA kinetics accomplished by monitoring the PSA and PSA derivatives such as free-PSA percentage, PSADT, PSAV and other calculations, should result in an almost total disappearance of the highly aggressive presentation of prostate cancer (the raven). This latter presentation is most commonly associated with rapidly progressive disease and fatality. However, the more typical presentations of prostate cancer (the hare) would be diagnosed years earlier if attention was directed to PSA kinetics, along with confirmatory tests such as free PSA, uPM3 and other new diagnostic advances. Such earlier diagnosis of prostate cancer, and for that matter any type of cancer,is associated with a lesser volume of cancer, a decrease in the risk of spread of the disease and thus a greater likelihood of cure with local therapy. These opposite extremes in the clinicopathological nature of prostate cancer, i.e., the very slow growing variants versus the aggressive ones, are important to differentiate due to the highly different evaluation and management recommendations advised for each circumstance. CONTINUED FROM PAGE 4 Slow-Growing versus Aggressive Prostate Cancer Slow-growing variants in general, have low PSA values (under 10) and long doubling times (greater than 24 months and often 48 months or longer), as well as low PSA velocities (<0.75 ng/ml/yr ± 10%). If a biopsy is done on a patient with a PSA that is under 10, the Gleason score often turns out to be (3,3). Depending on the calculated tumor volume, clinical stage, PSA doubling time, and other factors, these objectified biologic parameters may allow many such patients to be candidates for active objectified surveillance (also called watchful waiting).10 Patients who choose to monitor their illness rather than seek immediate local therapy must be cognizant of the significance of change in biology over time, or biologic trend. They need to be aware that if manifestations of disease progression become evident, their situation should be reevaluated.In such circumstances, consideration must be made for some form of local treatment – before the window of opportunity for successful local therapy is lost. Aggressive variants, in general, have high PSAs (over 10) OR very low PSAs associated with very aggressive, high Gleason score [(4,3), (4,4), (4,5), (5,4), (5,5)] cancers. These variants are very dangerous, often escaping investigation for long periods of time because the PSAs appear to be in the so-called normal range. Investigating all PSAs of 2.0 and over will help to catch these aggressive prostate cancers while they are still organ-confined and treatable with local therapies such as surgery and radiation. The probability of detecting these low PSA/high Gleasonscore cancers is enhanced if patients and doctors monitor even very low PSA levels over time to note any persistent increases. High Gleason score cancers often have reverted to an embryonic state in which PSA secretion into the blood is markedly reduced. Checking the serum for abnormal elevations in markers such as CGA (Chromogranin A), NSE (Neuron Specific Enolase), CEA (Carcino-Embryonic Antigen) and PAP (Prostatic Acid Phosphatase) is important to discern PC activity secondary to these de-differentiated tumor cell populations. Therefore, in cases Figure 1.PC Biology Made Simple.Prostate cancer can be thought of as being indolent,intermediate or aggressive.The indolent subtype (the tortoise) is slow moving and slow growing and rarely leaves the prostate gland.It can be rationally managed by active objectified surveillance.10 The intermediate subtype (the hare), without proper attention and treatment can escape the confines of the prostate and result in morbidity and mortality.The aggressive,sinister and often lethal subtype (the raven) is fortunately uncommon and is associated with high mortality but perhaps with more aggressive monitoring and preventive strategy we can minimize this biologic presentation. such as this, the normal guidelines for PSA velocity and doubling time may not be applicable. HOWEVER, the concept of slope or trend in a biomarker of disease activity remains valid, and any biomarker elevation should be tracked at regular intervals to determine the presence of abnormal growth of primitive (embryonic) tumor cell clones. connection when it comes to men with PC?11 Aren’t the 300,000 American lives lost each decade too great a price to pay? Working together and listening attentively to the biology of cancer, we will achieve vast inroads into the diagnosis, evaluation and treatment of this illness and alter the course of human lives. ■Conclusion References If we scientifically observe the biological manifestations of prostate health or disease, we can detect PC at a time when currently available therapies are most likely to cure the most common malignancy facing man. If we ignore the biological communications that can alert us to the presence of a life-threatening condition, we will miss a vital opportunity to change the course of the illness. The loss of life, productivity, and the extreme costs to the health care system—all of which result from a late-stage diagnosis of this disease—should provide impetus for all of us to be proactive when it comes to an early diagnosis of a malignant condition. This fundamental concept has been heralded for many malignances, such as cancer of the cervix,lung cancer,colorectal malignancy and breast cancer. When will we make the same 1. Cerhan JR, Parker AS, Putnam SD, et al: Family history and prostate cancer risk in a population-based cohort of Iowa men. Cancer Epidemiol Biomarkers Prev 8:53-60, 1999. 2.Hayes RB,Liff JM,Pottern LM,et al: Prostate cancer risk in U.S.blacks and whites with a family history of cancer. Int J Cancer 60:361-4, 1995. 3. Isaacs SD, Kiemeney LA, Baffoe-Bonnie A, et al: Risk of cancer in relatives of prostate cancer probands.J Natl Cancer Inst 87:991-6,1995. 4.Bennett KE,Howell A,Evans DG,et al:A follow-up study of breast and other cancers in families of an unselected series of breast cancer patients. Br J Cancer 86:718-22, 2002. 5. Ford D, Easton DF, Bishop DT, et al: Risks of cancer in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Lancet 343:692-5, 1994. 6. Goldgar DE, Easton DF, Cannon-Albright LA, et al: Systematic population-based assessment of cancer risk in first-degree relatives of cancer probands. J Natl Cancer Inst 86:1600-8, 1994. 7.Ito K,Yamamoto T,Ohi M,et al: Free/total PSA ratio is a powerful predictor of future prostate cancer morbidity in men with initial PSA levels of 4.1 to 10.0 ng/mL. Urology 61:760-4, 2003. 8. Ito K,Yamamoto T, Ohi M, et al: Usefulness of prostate-specific antigen velocity in screening for prostate cancer. Int J Urol 9:316-21, 2002. 9. Labrie F, Candas B, Cusan L, et al: Diagnosis of advanced or noncurable prostate cancer can be practically eliminated by prostate-specific antigen. Urology 47:212-7, 1996. 10.Hardie C,Parker C,Norman A,et al: Early outcomes of active surveillance for localized prostate cancer. BJU Int 95:956-60, 2005. 11. Labrie F, Candas B, Dupont A, et al: Screening decreases prostate cancer death: first analysis of the 1988 Quebec prospective randomized controlled trial. Prostate 38:83-91,1999. PCRI INSIGHTS 5 Who’s Really at Risk for What? By Mark C. Scholz, MD Director, Prostate Oncology Specialists, Marina del Rey, CA, and Ralph Blum PC Survivor Editor’s Note: This is an article by Dr. Scholz providing advice to prostate cancer patients about health issues unrelated to prostate cancer. The goal of the article is to bring the risks associated with prostate cancer into perspective with the risks of other potentially serious illness, including heart attacks, osteoporosis, colon cancer sarcopenia, lung cancer, and melanoma. Cancer is the Spur Like many doctors, I am often struck by the prodigious efforts men make to understand and get appropriate treatment for prostate cancer (PC) while ignoring the fact that they are at greater risk of dying from other causes unrelated to PC. I’ll never forget the unexpected phone call I received from the distraught wife of a 55year-old patient who had consulted me for the first time only a week previously. “How did you know?”she cried.“How did you know that my husband had heart disease?”At first I didn’t even understand what she was referring to. Then she told me that her husband had died in his sleep from a massive heart attack four days after our initial consultation. During our initial consultation, I had only recommended that he undergo screening to see if any heart disease was present. There had been no indication whatsoever that he had an underlying heart problem during the initial evaluation. One thing I did know, however, is that silent heart disease is very common among men in this age group. Deeply sorry for her loss, I explained to her that men come to my office because of their concern about dying of PC. When I see them, they are often found to have low-risk variants of PC,a form of the disease that pracTable 1. Annual U.S. Male Death Rates Heart Disease Lung Cancer Stroke Accidents Emphysema Diabetes Prostate Cancer Flu/Pneumonia Colon Cancer Suicide 6 PCRI INSIGHTS 350,000 89,000 65,000 63,000 62,000 31,000 28,000 27,000 25,000 23,000 tically never leads to death. I point out to them that that they are 10 times more likely to die of a heart attack or a stroke than from their early stage PC.See Table 1 for the annual death rates for men in the United States each year. For this reason, I routinely recommend cardiac screening to our newly diagnosed PC patients, even though they usually try to tell me what good shape they are in, how low their cholesterol is, and generally how good they feel. For the past decade,my focus has been on treating PC exclusively.Some forms of PC can be quite dangerous. Fortunately, these more aggressive forms are not as common as the lower-grade, less dangerous forms. These days, when men are commonly being diagnosed at an early stage,we can confidently tell them that their risk of dying of PC within 10 years is less than 1%. However, their risk of dying from other diseases can be far greater, so I customarily advise my patients that they at least undergo screening for certain common, preventable, and potentially dangerous diseases. The place to start is with a simple baseline physical examination that includes some common blood tests looking for any irregularities that might indicate the presence of underlying illness. (The accompanying article on page 10 describes these laboratory blood tests, discusses what they test for,and projects what the results may indicate.) Screening for unexpected latent medical problems is not always a popular pursuit. It can be inconvenient, uncomfortable, and on occasion, expensive, since sometimes insurance does not pay for screening tests. Also troubling is the fact that the screening process can occasionally produce a false positive or a false negative. So it might take additional studies to validate a finding, causing additional stress and cost for the patient. Despite all these drawbacks, screening is our best defense, and is the best tool available for early detection of certain common and preventable heath problems. The Scanning Revolution Fortunately, times are changing and rapid progress is occurring in the field of medical technology. One of the most significant advances has been the refinement of a body scanning technique called computerized tomography, popularly referred to as CT scans.Body scans have been around for some years now, but older technology could not accurately image moving organs.If we use the analogy of a camera,the older scans could not take pictures of the moving parts of the body because they had “excessively slow exposure times.” “Pictures” of moving organs like the heart, the lungs, and the colon always came out blurred.Today,however,newer technology renders excellent image quality. I am not advocating that total body scans should be undertaken randomly or without explicit reason such as those procedures that are being widely advertised on the radio in major population centers. The value of this sort of global scanning is highly debatable because random scanning frequently uncovers what we term “incidental findings” that subsequent tests show to be completely benign. The disadvantage of global body scanning is that when any slight abnormality is seen, it becomes necessary to embark on a stressful, time-consuming, and expensive process to determine that a suspicious area found in the scan does or does not indicate the beginning of some malignant process. This then can require further scans, blood tests,consultations with medical experts and, in some cases,biopsies or even surgery. However, there are selective ways that these scans can be used to image certain critical areas of the body, especially in groups of patients known to be at high risk. One of the areas where fast CT scans are beneficial is in detecting the presence of cholesterol plaque in the coronary arteries. Patients in our practice (who are usually older than 50) belong to the population most at risk for atherosclerosis, otherwise known as hardening of the arteries. Simply described,hardening of the arteries occurs when cholesterol builds up in the arteries.In extreme degrees the buildup reaches the point where the artery is totally blocked off. When an artery to the heart is completely blocked, it results in a heart attack. When an artery to the brain is completely blocked off, it results in a stroke. Over 400,000 men die of either heart attack or stroke every year. Perhaps twice that many men have non-fatal strokes and heart attacks each and every year. Clearly, we have an epidemic on our hands. In WHO’S REALLY AT RISK FOR WHAT? comparison, the annual death rate from PC is 28,000, only 9% of the rate that men are dying from heart attacks and strokes. Much of the mortality from heart disease is preventable. The problem is that atherosclerosis is a silent disease until suddenly a disaster occurs. There are indirect means (e.g. cholesterol testing) to estimate the likelihood of impending serious atherosclerosis,yet these tests are too imprecise. Elevated blood cholesterol provides a warning by telling how much cholesterol is floating in the blood,but we want more. We really want to know how much cholesterol is sticking to the wall of the artery. This varies widely from individual to individual even in men with really high or low levels of cholesterol floating in the blood. Fast CT scanning can accurately evaluate the status of the coronary arteries. Population studies indicate that a lucky minority of men have absolutely no calcified plaque at all. The rest of us have small amounts, average amounts, or extensive amounts of disease. In the United States, having an “average”amount of plaque is a serious situation. With heart attacks and strokes at epidemic levels,is seems foolish to be unwilling to have a simple 10 minute $300 test to determine the status of one’s arteries. This does not require annual testing; reevaluations can probably be done every three to five years. FROM PAGE 6 porosis. Osteoporosis is defined as bone that has been weakened from calcium loss over time. Calcium loss is a silent phenomenon until a bone fracture occurs.Common fracture sites from osteoporosis are the spine,rib,wrist, and hip.Osteoporotic fractures often have dire consequences. Bone fractures are associated with shortened survival in men with PC.1 Compression fractures of the spine can be extremely painful, result in loss of height and, when advanced, result in a forward curvature of the spine known as the “dowager’s hump.” Osteoporosis is mistakenly thought to occur only in women,but fully a third of all hip fractures occur in men. There are many causes of osteoporosis. Men who are slender have less bone reserve and are more predisposed to osteoporosis.Thyroid or parathyroid hyperactivity can contribute to osteoporosis. Other contributing causes of osteoporosis are excessive use of alcohol, caffeine, or tobacco. Cortisone, used to treat asthma or arthritis, is another common culprit. Excess vitamin A has also been associated with osteoporosis and fractures.2 Lack of exercise, lack of sunlight exposure (low vitamin D),and low calcium intake are additional potential causes. Osteoporosis-induced bone fractures are even more frequent in men treated for PC with testosterone inactivating pharmaceuticals (TIP).3,4 Testosterone deprivation therapy reduces estrogen levels. Normal levels of both these hormones inhibit excess calcium loss from bone. Osteoporosis needs to be identified by scanning before a fracture occurs, but not all scans are equally effective. It is important to choose the right scanning technique to diagnosis osteoporosis because the most popular equipment available, DEXA scans, grossly underestimate the incidence of osteoporosis in men.5 The problem with DEXA scans is that men over age fifty usually have some degenercontinued on page 9 EBCT “positive” for coronary calcium Check List for Plaque Management What should you as a PC patient do if you learn that there is a lot of cholesterol plaque in your coronary arteries? 1. See a qualified cardiologist; 2. Obtain a cardiac stress treadmill annually; 3. Obtain an ultrasound of your carotid arteries; 4. Start Lipitor to diminish your LDL cholesterol to 60; 5. Start aspirin 81 mg a day (if there are no contraindications to aspirin); 6. Check homocysteine.If it is elevated,start taking folic acid 1 mg daily; 7. Reduce blood pressure to 125 over 75 or less; 8. Diet and exercise; 9. Perform a repeat scan in three years to make sure what you are doing is working. Atherosclerosis (Above) Figure 1. Progressive development of plaque over time. This process, in various stages of development, can be seen in many areas of the coronary artery system, consistent with the “diffuse” nature of coronary artery disease. (Left) Figure 2. The calcium impregnation of the plaque as would be visualized by the scanner. The Specter of Osteoporosis We must also consider the problem of osteoPCRI INSIGHTS 7 WHO’S REALLY AT RISK FOR WHAT? FROM PAGE 7 ative arthritis of the lower back which results in excess calcium in the tissues surrounding the spine.When the DEXA scan sends x-rays through this area to measure spine density, the excess calcium surrounding the spine results in an artificially high bone density reading, a situation that masks the presence of osteoporosis in the spine. Fortunately,another more accurate technique of measuring bone mineral density is available: the quantitative CAT scan,or QCT.This scan measures the calcium density in the center of the vertebral column thereby bypassing the problem of the excess calcium surrounding the spine. Many health care providers are unaware of the DEXA scan’s limitations,although these limitations have been well documented in a study from Massachusetts General Hospital.6 The study compared DEXA and QCT in 41 men with PC who had never previously been treated with TIP.QCT detected osteoporosis in 63% of the men but DEXA only found osteoporosis in 5%! On the basis of this study, which was done in men whose average age was 68, we can conclude that osteoporosis is common even in men who have never had previous exposure to testosterone-lowering drugs. What do you do if you find out that you have osteoporosis? In these QCT scans, the yellow lines demark the area of bone being analyzed. Courtesy of Parkview Imaging. 1. Start calcium citrate 500 mg twice a day; 2. Start prescription Vitamin D (Calcitriol); LABORATORY TESTS DEFINED An important first step in the screening procedure is, of course, the physical examination taken at the first visit of a patient to our practice and scheduled to be repeated each year thereafter.In addition to the tactile examination,a complete physical will include a number of blood tests which, when analyzed, can provide an early indication of disease or incipient disease. The results of the laboratory results are written in a shorthand code that your physician can readily interpret, but that might just bewilder you as a patient.For each blood test result,the report includes (1) an entry in a column for your quantitative results and (2) an entry in a column presenting the reference range for males. In addition, if one of your results is outside of this range,that result is flagged so you can quickly see anomalous results. But what are these tests? What do they measure? What is the possible significance of an anomalous result? The following will answer these questions for you. BMP: BASIC METABOLIC PANEL The GLU test measures blood glucose levels that vary before and after meals. Patients with diabetes have blood sugar levels that remain persistently elevated. Low levels of glucose occur in patients on macrobiotic diets and are desirable in prostate cancer patients because less sugar is available to the growing tumor cells.Low levels of glucose in diabetic patients can be indicative of excess medication or insulin. Since blood glucose varies, a better way to diagnose diabetes is the glycohemoglobin blood test.An abnormal GLU result may cause your doctor to prescribe this additional blood test. Elevation of Blood Urea Nitrogen (BUN) can result from dehydration or from a high protein diet but it can also be a result of a kidney malfunction (but when this is the case there is almost always simultaneous elevation of the creatinine level as well).BUN is very sensitive, and a modest elevation of BUN does not necessarily indicate a need for intervention. Low BUN levels have no implications of consequence. Creatinine (CREAT) is a fairly accurate indication of kidney efficiency. Elevated levels of creatinine are indicative of kidney impairment.The development of creatinine elevation above previous baseline signals the need for further tests. Minor elevation of creatinine can be seen from aging and is usually not significant if the minor elevation remains stable.Low creatinine levels have no implications of consequence. The concentration of Sodium (Na) in the blood is regulated by the kidneys and adrenal glands.Drinking too much water can cause abnormally low amounts in the blood, but so does heart failure or kidney malfunction. Hence, levels of sodium outside the normal range represent a significant problem that needs evaluation and correction. Small amounts of Potassium (K) can be measured in the blood.Blood levels outside the normal range are of critical significance.Low blood levels of potassium result from diuretics (water pills) when there is an inadequate amount of potassium replacement. High blood levels can result from kidney disease or from excess potassium replacement. Occasionally, potassium can be elevated in the breakdown process of the red blood cells (hemolysis), which occurs when the blood is being drawn.When hemolysis is suspected, the blood draw is repeated to determine if the potas- sium elevation is artifactual.Levels of potassium outside the normal range represent a significant problem that needs evaluation and correction. Abnormal Chloride (CL) levels usually accompany abnormalities of sodium or potassium. Borderline low or high levels of chloride generally have no significance. Calcium (Ca) blood levels are tightly regulated by parathyroid hormone and vitamin D. Over-active parathyroid glands can also cause excess blood levels of calcium.Grossly elevated calcium levels are dangerous and can cause sleepiness and heart arrhythmias. Low levels of calcium can cause muscle spasms,typically in the hands. Low levels of calcium can also be observed in patients with low albumin levels (protein levels) in the blood. Elevated levels of calcium can occur by taking excess amounts of vitamin D. The accuracy of the blood calcium can be confirmed with a more accurate test called ionized calcium. HEPATIC PANEL (Liver function tests) Transaminases (AST/ALT) are the most sensitive indicators of liver cell irritation or damage. AST and ALT (also known as SGOT and SGPT) can occasionally elevate to minor degrees from viral infections or from excess alcohol. Larger degrees of elevation can occur as a result of toxicity from medications or from cancer spread.AST/ALT elevation can also occur after a heart attack.Low levels of AST/ALT are of no significance. Blood bilirubin (TBIL) levels are reflective of the rate that the body recycles the red cells in the blood; bilirubin is a breakdown product of old, used up red cells. Elevations of bilirubin can occur with bile duct blockage if the red cell breakdown process is acceler- 3. Start a bisphosphonate such a Fosamax, Actonel,Aredia or Zometa; 4. Exercise (preferably some form of weight lifting); 5. Repeat bone density testing every year to ensure that the treatment is working; 6. While on treatment,consider checking the urine for signs of excess bone breakdown products with tests such as Pyrilinks D and N Telopeptide to make sure that the treatment is working. Colon Cancer This cancer kills about the same number of men in the United States each year as PC does. Early diagnosis with colon screening can detect the disease long before it spreads.Generally,it is recommended that colon screening occur every five years with either a colonoscopy (a scope performed by a physician called a gastroenterologist), or with a fast CT scan,which is termed a virtual colonoscopy. ated by disease.A mild chronic elevation of bilirubin may be a benign genetic condition that does not cause illness. (DBIL) is a sub fraction of bilirubin. Relative changes of the two forms can help distinguish the different causes of bilirubin elevation. Alkaline Phosphatase (ALP) is another indicator of liver health and function.ALP is also a produced in the bones so elevations of ALP can occur either from problems originating from the liver or bone or both. Liver cell function problems can cause an elevation of ALP in a manner similar to AST/ALT.ALP is also sensitive to blockage of the bile ducts,so elevations ofALP in conjunction with elevations of Bilirubin indicate bile duct blockage.Low ALP levels are not of concern. Total Protein (TP) is a simple measure of the amount of protein in the blood including albumin. The non-albumin portion of the blood includes antibodies,that function as a portion of the immune system. Elevated levels of TP can be seen in immune derangements where antibodies are over-produced. Albumin is the most common protein circulating in the blood. Albumin fulfills a number of functions such as maintaining vascular blood volume, binding hormones,and acting as a storage reserve for protein. Low albumin levels are reflective of malnutrition,liver disease,or kidney disease.Elevation of albumin levels is usually minor and of no consequence. CBC: COMPLETE BLOOD COUNT The CBC contains several different measures of importance though for PC patients the real issue is the presence or absence of anemia.Anemia is the relative reduction of red cells in the blood resulting in a decrease in oxygen carrying capacity. Severe anemia can be felt as tiredness and shortness of breath.Ane- Advantages of Virtual Colonoscopy Disadvantages of Virtual Colonoscopy ✔ Minimal if any risk of colon perforation ✔ No need for sedation � May not be quite as accurate � Regular colonoscopy will be required Advantages of Colonoscopy ✔ Effectiveness is more established ✔ If any polyps are visualized,they can be removed during the procedure Beware of Sarcopenia Sarcopenia is the official word describing loss of muscle mass. Muscle loss is a normal part of aging. Some men age gracefully, but others don’t. Men who allow themselves to get weak are the ones who look and act old. Strength is what we associate with heath and youthfulness. Weakness is associated with advanced age and decrepitude. Muscle loss can have a dramatic effect on health.Studies indicate that poor fitness in the elderly is more dangerous than smoking.Table 2 shows the predicted 10year survival of normal healthy individuals at mia is measured by three factors in the CBC: Hematocrit (HCT),Hemoglobin (HGB), and Red Blood Count (RBC).An HCT level less than 40 in men constitutes a low level.Symptoms of tiredness and shortness of breath do not usually occur until the HCT declines to around 32 though there are occasional exceptions. A low HCT is treatable with a non-toxic substance called Erythropoietin. The other important measures in the CBC take on more significance in patients receiving chemotherapy. Chemotherapy can cause reductions in Platelet count (PLT) and White blood count (WBC). Platelets help the blood clot normally. White blood cells are part of the immune system.The WBC is broken down into Granulocytes (GRAN) and Lymphocytes (LYM).An elevated level of granulocytes is indicative of an underlying bacterial infection. Viral infections can cause low lymphocyte counts. MCV, MCH, and MCHC are measures of red cell dimensions.MCV is the most commonly utilized.Low MCV can be seen in iron deficiency and in a congenital anemia called thallassemia.High MCV can be seen in liver disease and B12 deficiency. RDW is a measure of red cell size variability. Elevation of RDW can occur early in the development of iron deficiency. LIPID PANEL Triglyceride (TRIG) is simply another name for fat. Elevated fasting triglyceride levels indicate a higher risk for coronary arteriosclerosis. However, transient declines in the White Blood Count (WBC) and the triglyceride levels are not as accurate predictors of arteriosclerosis as cholesterol. Previously, total cholesterol (CHOL) levels of over 200 were thought to be indicative of an increased risk for arteriosclerosis. This is true if anything is detected Disadvantages of Colonoscopy � Sedation is often required � A small risk of colon perforation an average age of 65. In this study, subjects were divided into three groups: the strong,the average,and the weak.Despite having no specific illnesses at the time,only 60% of the weak individuals were still alive ten years later. continued on page 10 Table 2. Fitness Predicts Survival Degree of Fitness Superior Average Inferior Ten-year survival 90% 75% 60% but better indicators have been developed. Low Density Lipoprotein (LDL) cholesterol or “bad cholesterol”is an indicator for the risk of developing arteriosclerosis. The American Heart Association recommends that LDL cholesterol should be less than 100 to prevent deposition of cholesterol on the arterial wall.Modern statin drugs such as Lipitor dramatically lower LDL levels in the blood and can lead to reversal of blood vessel clogging. High Density Lipoprotein (HDL) cholesterol is called “good cholesterol” because higher levels of HDL protect against the development of arteriosclerosis by scavenging excess cholesterol from the walls of the blood vessels. The HDL level can be increased with exercise and niacin. Studies show that the higher the level of HDL the lower the risk for heart disease. Levels of HDL that are under 40 represent a particular concern. OTHER TESTS Ultra-sensitive Thyroid Stimulating Hormone (TSH) is the hormone that stimulates thyroid hormone production. Elevated levels of TSH indicate blood levels of thyroid hormone are inadequate. Low levels of TSH indicate that the thyroid may be overactive. If patients are already taking thyroid hormone, TSH can be used to ensure that the correct amount of hormone is being administered. C-Reactive Protein (CRP) is a protein marker for inflammation. Elevated levels are usually caused by infections and arthritic conditions.More recent studies have shown that abnormal levels are also associated with an increased risk of heart attacks and colon cancer, soPCRI CRP results are9 now INSIGHTS given equal weight to CHOL results. WHO’S REALLY AT RISK FOR WHAT? Ninety percent of the people in the strong group were still alive 10 years later. Loss of strength is correctable to a large degree with appropriate exercise. Exercise is unpleasant for most of us. My approach has been to purchase discipline and expertise by hiring a trainer. I spend one hour twice a week taking orders from a ruthless individual who has a mandate to make me stronger. This process is accomplished exclusively with weight machines.Aerobic exercise is great, but optimally it should be done for 40 minutes a day.I just don’t have that kind of time to spare.I have been doing this one-hour,twiceweekly regimen for five years. It has been expensive and mostly unpleasant, but the results are rather remarkable. I used to have to eat selectively to avoid gaining weight. Now I eat pretty much whatever I want without any concern for my weight. I am about twice as strong as I was five years ago. I have put on at least 15-20 pounds of muscle and lost 20-30 pounds of fat.In my professional life I can work longer hours at a faster pace, but at the end of the day I still have energy to interact with my family. For our patients, this issue of muscle loss is even more critical.Men with PC who are being treated with testosterone-inactivating pharmaceuticals loose muscle mass very, very quickly.The muscle loss is preventable but only with a consistent weight training program performed for an hour twice a week.7 Lung Cancer Early diagnosis of lung cancer is vital,since it is almost universally fatal in men who are not diagnosed until after they have a symptom of the disease such as cough,chest pain,or weight loss. The average survival is only nine months in men diagnosed after they have symptoms. Fortunately,fast CT scans can detect small early stage lung cancers when they are only a quarter of an inch in diameter.When a lung cancer is found at such an early stage, it can often be removed with a telescopic device in a process called thoracoscopy. (This is very similar to laparoscopy for operations in the abdominal area.) Cure rates for men with small lung cancers are high (about 80%).Any life-long smoker would be crazy not to spring for $300 each year to have a lung scan done. Less Common Cancers Bladder cancer Bladder cancer kills about six thousand men each year, five times less than PC. The pres10 PCRI INSIGHTS FROM PAGE 9 ence of bladder cancer is often signaled by microscopic amounts of blood in the urine which can be detected by performing a simple urine analysis. So obviously a urine analysis should be done as part of the general annual physical examination. Melanoma Three thousand men die each year from melanoma,a pigmented cancer that can look like a new mole in its early stages.There is no effective treatment for melanoma after it has spread, but if it is detected early, it is usually curable with surgical excision. An annual visit to the dermatologist (the doctor with the trained eye for spotting melanoma in its earliest stages) can save your life. Other Causes I can’t resist making a common sense statement in an area where I have no specific expertise. Consider that just as many men are dying in car accidents each year as are dying each year from PC. If that is the case, what are some simple precautions? Consider keeping a robust grid of steel around you while you are doing battle on the highways; stay away from sub-compact cars. Drive a heavy car that has front and side air bags. And of course wear a seat belt. Harkening back to my Internal Medicine training leads me to also mention that the next most common killer after PC is pneumonia and flu. While most men have heard of flu vaccines, many are unaware that there are now FDA approved antibiotics to treat flu: Tamiflu, and Flumadine. These are very effective against influenza if they are started promptly after the onset of symptoms. They can also be helpful in the situation where one family member is sick; in that case, the drugs can be taken before the flu develops and thereby may preclude the development of illness. I have also found that many men are unaware that there is now an effective vaccine against pneumonia available called pneumovax.The pneumovax is administered every five years and is recommended for men over age 65 or for men with chronic illnesses. Conclusion Many of these illnesses can be prevented by an annual visit to the doctor’s office.But it takes a lot to get us guys to go to the doctor. Prostate cancer seems to do the trick.A diagnosis of PC shatters the illusion of immortality.Men finally sit up and take notice that good health is not a guaranteed right.Therefore,the diagnosis of PC may actually turn out to be beneficial if being diagnosed can lead to an increased awareness of health-related issues that have been previously neglected. Common sense dictates that if it is worth expending considerable time, energy, and resources to minimize the chance of death from PC, it certainly makes sense to expend time and energy to minimize the risks of these other preventable causes of death.■References 1. Skeletal fractures negatively correlate with overall survival in men with prostate cancer.Oefelein,M,Ricchiuti,V,et al Journal of Urology Vol.168: 1005-1007,2002. 2. Excess dietary intake of vitamin A is associated with reduced bone mineral density and increased risk of hip fracture. Ann Intern Med Vol.129: 770-778,1998. 3. Osteoporosis after orchiectomy for prostate cancer.Daniell,H,Journal of Urology Vol.157,439-444 ,1997. 4. Osteoporosis in men treated with androgen deprivation therapy for prostate cancer. Ross, R, Small, E, Journal of Urology Vol. 167: 19521956,2002. 5. Low bone mineral density in hormone-naïve men with prostate cancer.Smith,M,McGovern,F,et al Cancer Vol.91: 2238-2245,2001. 6. Exercise capacity and mortality among men referred for exercise testing. Myers, J. New England Journal of Medicine Vol. 346 page 793 2002. 7. Resistance exercise in men receiving androgen deprivation therapy for prostate cancer.Segal RJ: J Clin Oncol 21:1653-9,2003. NEWER CONCEPTS IN THE TREATMENT OF HRPC FROM PAGE 3 reached at the time of the report. Chemotherapy, particularly with nonbone marrow suppressing agents such as weekly taxanes, 5-FU infusion, or capecitabine, clearly has the potential to augment activity of bone-seeking radiopharmaceuticals and additional studies are warranted to determine best dosing, best agents, and optimal timing of such therapies. Summary and Conclusion Bone metastases with pain represent a common and significant problem for patients with advanced prostate cancer. Data from prospective randomized clinical trails now support the use of 153Sm-EDTMP in patients with HRPC and painful bone metastases. Pain relief and decreases in analgesic consumption can be expected in the majority of patients treated. Side effects are limited to transient and relatively mild platelet and white blood cell suppression. Combination therapies that incorporate continued at right THE PCRI TODAY: FROM THE EXECUTIVE DIRECTOR There are three basic functions that the prostate cancer community performs: 1. Research 2. Support 3. Patient Education & Awareness In the past, there has been functional overlap in the services that these and other organizations provide. But I believe that today the lines of demarcation are becoming much sharper. Ultimately, it would be in the best interest of the PC community if the primary functions of the PC organizations were more in line with their missions. In this way, the pooled efforts would be greater as a whole, rather than fragmented among individual organizations spending resources on activities, however useful, that are outside the scope of their primary mission. The PCRI, in pursuing its primary goal of fostering public awareness of prostate cancer and educating prostate cancer patients, their families, and their family doctors to the disease, its prevention, and its treatment options, has expanded its programs to take advantage of additional media. In the past year, for example, we have augmented our unique Insights newsletter/journal and our national NEWER CONCEPTS IN THE TREATMENT OF HRPC FROM PAGE 10 cytotoxic agents in combination with 89Sr or 153Sm-EDTMP regimens are now being actively explored in clinical trials. This approach has the potential of promoting synergy between active agents.Preliminary data suggest that this might be of considerable interest, although additional trials are needed to optimize this approach. ■FROM PAGE 1 Helpline programs with educational programs that have appeared on PBS and cable TV; we have produced a DVD explaining prostate cancer issues and the PCRI’s role in dealing with them; and we have produced educational mailers on these subjects for groups such as Blue Cross/Blue Shield of Florida members, general practitioners, and the general public. All of these expanded activities are important to our mission, but they do cost money. Therefore, the PCRI is embarking upon an educational campaign to find a national sponsor willing to support the fight against prostate cancer with funds and mass media exposure.We feel that this support, plus a continuation of generous contributions from people like you, our subscribers, will enable us to pursue the ambitious program that is so important to the fulfillment of our mission. And we hope that you will continue to rely on the PCRI for the most accurate, timely, and useful information about prostate cancer. We further hope that you will join with us in our campaign to reach other men at risk from prostate cancer by directing them to the PCRI cost-free information conduits: (800) 641-PCRI, www.pcri.org, and of course, Insights. How to Contribute Please help PCRI continue its mission of providing information and education about prostate cancer through its programs, such as this newsletter, in the following ways: • Direct Donation: Cash, check, or credit card; stock or real estate • Memorial and Honorarium Contributions: Honoring someone you care about with a memorial or commemorative gift • Payroll Deduction: Federal employees can contribute to the Combined Federal Campaign in their workplace.To find PCRI’s CFC number, look in the HEALTH section of the CFC directory or call PCRI. • Planned Giving: Naming PCRI in your will or as beneficiary of a life insurance policy. Your tax-deductible gift in the form of cash, stocks or real estate should be made payable to ”PCRI” and mailed to PCRI at: 5777 W. Century Blvd., Suite 800 Los Angeles, CA 90045 Federal Tax ID Number: 95-4617875 PCRI Helpline 800-641-7274 [email protected] www.pcri.org Credit card donations can be made online at: www.pcri.org or by calling (310) 743-2116. For further information, contact PCRI at [email protected]. Prostate Cancer Research Institute is a non-profit corporation, exempt from federal income taxes under section 501(c)(3) of the Internal Revenue Code. It has been classified as an organization that is not a private foundation as defined in section 509(a) of the Code, and qualifies for a maximum charitable contribution by individual donors. References 1. Gandhok N and Sartor O. Bone-targeted therapy for prostate cancer. In: Klein EA, ed. Current clinical urology: Management of prostate cancer, second edition. Totowa: Humana Press, 2004:589-606. 2. Newling DW, Denis L,Vermeylen K. Orchiectomy versus goserelin and flutamide in the treatment of newly diagnosed metastatic prostate cancer. Analysis of the criteria of evaluation used in the European Organization for Research and Treatment of Cancer-Genitourinary Group Study 30853. Cancer 1993;72(12 suppl):3793-3798 . 3. Serafini AN, Houston SJ, Resche I, et al, Palliation of pain associated with metastatic bone cancer using samarium-153 lexidronam: A double-blind placebo-controlled study. J Clin Oncol 1998;16:1574-1581. 4. Sartor O, Reid RH, Hoskin PJ, et al, Samarium-153-lexidronam complex for the treatment of painful bone metastases in hormone refractory prostate cancer. Urology 2004;63:940-945. 5. Tu SM, Millikan RE, Mengistu B, et al.Bone-targeted therapy for advanced androgen-independent carcinoma of the prostate: a randomised phase II trial. Lancet. 2001; 357(9253):336-41. 6. Widmark A, Linne T, Modig H, Johansson L. Optimizing the time of co-administration of docetaxel and samarium-153 for advanced androgen independent carcinoma of the prostate [abstract]. Proc Am Soc Clin Oncol 2003;22:433. 7. Arnsmeier SL, Spies S, Shervin D, et al. Phase I/II study of taxane and estramustine with samarium in patients with hormone refractory prostate cancer [abstract]. Proc Am Soc Clin Oncol 2004;23:438. The Prostate Cancer Research Institute’s mission is to improve the quality of men’s lives by supporting research and disseminating information that educates and empowers patients, families and the medical community. PCRI INSIGHTS 11 The Ostrich Seven years ago, poet Ric Masten was diagnosed as having the deadly neuroendocrine prostate cancer,also known as non-secreting-PSA prostate cancer. This diagnosis came as a complete surprise. As he now recalls,“Like most older men I had avoided the annual checkup for years.The proverbial ostrich with his head stuck deeply into the sand of the workaday world.I felt fine so why bother? Of course,what really kept me out of the doctor’s office was the thought that he just might find something wrong.” Over the years, he has developed a close relationship with the PCRI’s Program Director, Harry Pinchot, and he now is an active advocate for annual checkups (www.ric-masten.net). For the past six years, CONTINUED HEADER FROM PAGEhe 1 has been sending poems and updates on his fight with cancer (www.ric-masten.org).He is no longer an ostrich. THIS ISSUE The PCRI Today Newer Concepts in the Treatment of HRPC with Bone Metastases What Every Doctor Who Treats Male Patients Should Know Who’s Really at Risk for What? The Ostrich PCRI Published By nsights Prostate Cancer Research Institute 5777 W. Century Blvd., Suite 800 Los Angeles, CA 90045 PROSTATE CANCER HELPLINE 800-641-PCRI or 310-743-2110 PCRI ONLINE www.pcri.org EMAIL [email protected] 1 2 4 6 12 after the original diagnosis and treatment I became the classic “ostrich” head thrust deep in the sand of denial. I did my best to keep myself in the dark and during that blind unattended time my disease sneaks up on me morphing into the very aggressive dedifferentiated neuroendocrine carcinoma the label alone being a head’s up eye opener! at long last I faced the fact that the ostrich cannot fly time to take an active role in my fight for survival time to look the monster in the eye so I go on line where dumb luck and a benevolent “search engine” find the Prostate Cancer Research Institute. I dial the “helpline” and for more than an hour an anonymous Good Samaritan calmly slowed me down until my philosophy of life could catch up and begin to see me through. once again I’m able to recall that only where the path of difficulty crosses the easy way can growth and change occur, that the height of my highest high is in direct proportion to the depth of my “deepest down” lessons I’d lost sight of when my butt was in the sky and my brains were under ground. PCRI nsights Editor: Review Board: Design & Production: Charles Bader Duke K. Bahn, MD Stanley A. Brosman, MD Arthur N. Lurvey, MD Mark C. Scholz, MD Diana Garnand Prostate Cancer Research Institute 5777 W. Century Boulevard, Suite 800 Los Angeles, CA 90045 Phone (310) 743-2116 | Fax (310) 743-2113 Helpline (310) 743-2110 E-mail: [email protected] www.pcri.org and www.prostate-cancer.org Executive Director: Glenn D. Weaver E-mail: [email protected] Board of Directors Chester A. Swenson, President Chairman,Marketing & Financial Services Enterprises Jerome Seliger, PhD, Vice President Professor of Health Administration, California State University, Northridge Barry L. Friedman, JD, Secretary Attorney at Law T. Kent Graham, Treasurer Financial Consultant, T. Kent Graham & Associates Duke K. Bahn, MD Director, Prostate Institute of America Stanley A. Brosman, MD Pacific Urology Institute, Pacific Clinical Research Brian L. Gauthier, MBA Gauthier Management Company Arthur N. Lurvey, MD Medicare Contractor Medical Director Jerry Peters MCG Records Claudia B. Sangster, Esq. Director of Philanthropy Services, myCFO, Inc. Mark C. Scholz, MD, PCRI Co-founder Director, Prostate Oncology Specialists The cost of printing and mailing this newsletter is made possible through a generous grant from The Life Extension Foundation P.O. Box 229120, Hollywood, FL 33022 800-544-4440 www.lef.org/prostate The opinions expressed in the by-lined articles are those of the authors and should not be considered opinions of the PCRI. © Copyright 2005.
© Copyright 2026 Paperzz