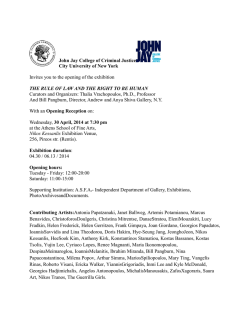
Under the Auspices of The Minister of Health 22nd Final Program Pancyprian Accredited with 12 CME points. Ankle Orthopaedic & ot Conference Fo In Association: with the Hellenic Association of 26-28 Orthopaedic Surgery and Traumatology and the Greek College of Orthopaedic Surgeons. October 2012 The official language of the conference is English Sponsors: Hilton Cyprus Hotel Organizer: Accredited as: EFORT FORA MSE Congress Plus tel. +35722466400 | fax.+35722767680 | email. [email protected] | www.mse.com.cy 2 26-28 Aγαπητοί Φίλοι, October 2012 Σας καλωσορίζω στο 22ο Παγκύπριο Ορθοπαιδικό Συνέδριο, η θεματολογία του οποίου αφορά στο πόδι και στην ποδοκνημική άρθρωση. Η ΚΕΧΟΤ τα τελευταία 15-20 χρόνια έχει καταβάλει μεγάλες προσπάθειες για την εκπαίδευση των ορθοπαιδικών ιατρών στη Κύπρο. Το φετεινό συνέδριο εντάσσεται μέσα σε αυτά τα πλαίσια αλλά φέτος για πρώτη φορά κυπριακή επιστημονική εταιρεία εκδίδει και δίνει στα μέλη της κατευθυντήριες γραμμές για την αντιμετώπιση και θεραπεία συγκεκριμένων προβλημάτων. Γι αυτό πρέπει να ευχαριστήσω θερμά το συνάδελφο Χριστόφορο Σολομωνίδη ο οποίος είχε την ιδέα και δούλεψε σκληρά προς την ολοκλήρωση των συγκεκριμένων οδηγιών. Φέτος η εναρκτήρια τελετή του συνεδρίου θα γίνει στην αίθουσα τελετών του Πανεπιστημίου Κύπρου και θα είναι αφιερωμένη στην έναρξη της λειτουργίας της πρώτης ιατρικής σχολής σε κρατικό Πανεπιστήμιο της Κύπρου, το οποίο ευελπιστούμε να προσδώσει βαρύτητα στην άσκηση της ιατρικής στη Κύπρο. Tέλος θα ήθελα να εκφράσω τις θερμές μου ευχαριστίες στην EFORT (Εuropean Federation of National Associations of Orthopaedics and Traumatology) για την πολύτιμη βοήθεια που μας παρέχει, στην ΕΕΧΟΤ (Ελληνική Εταιρεία Χειρουργικής Ορθοπαιδικής και Τραυματολογίας) και στο ΚΕΟΧ (Κολλέγιο Ελλήνων Ορθοπαιδικών Χειρουργών) για τη συνεργασία και συμπαράσταση όλα αυτά τα χρόνια. Το κοινωνικό πρόγραμμα συμπληρώνεται με το επίσημο δείπνο του συνεδρίου που θα δοθεί στην Πύλη Αμμοχώστου και θα είναι μεγάλη μας χαρά να σας δούμε εκεί. Με συναδελφικούς χαιρετισμούς, Νικόλαος Π. Μαρουδιάς Πρόεδρος ΚΕΧΟΤ Dear Friends, Welcome to the 22nd Pancyprian Orthopaedic Conference! In the past 15-20 years CAOST (Cyprus Association of Orthopaedic Surgery and Traumatology) has endeavour to promote orthopaedic training and education in Cyprus and this year’s conference is part of this ongoing effort. Also this year we have managed to issue and distribute to our members a set of guidelines for the treatment of certain conditions. For their help and continues support through the years we would like to thank EFORT and the Hellenic Association of Orthopaedic Surgery and Traumatology as well as the Greek College of Orthopaedic Surgeons for their SUPPORT. The opening ceremony of the conference will be held at the University of Cyprus celebrating the opening of the first public medical school in Cyprus. We welcome you over and wishing you a pleasant stay. Yours Sincerely, Nicolaos P. Maroudias President of CAOST 3 final program 22nd PancyprianOrthopaedic Conference THE BOARD OF DIRECTORS 2011-2013 Chairman Nicolaos P. Maroudias Vice President Tanos Andreas Secretary Georgiou Constantinos Treasurer Efstathiades Yiannis Members Sergiou Sergios Shiamishis Georgios Papaloukas Nicos Spastris Petros Athanatos Odysseas Constantinou Vasos Schizas Akis Christou Andreas Garpozis Demetris 4 5 Βέλτιστη ανάμιξη για οστικά τσιμέντα: Εύκολο – ασφαλές – αποτελεσματικό* Σύστ η ού ανάμιξης κεν μα AEUS ο σ τ ι κά τ σ ι μ έ ντ για α ΑΠΟ ΤΗ HER PALAMIX® – εύκολος χειρισμός για όλες τις εφαρμογές ομοιογενές και έτοιμο για εφαρμογή οστικό τσιμέντο σε λίγα μόνο βήματα * ασφαλές αξιόπιστος έλεγχος κενού μέσω δείκτη κενού στο σωλήνα αέρα * αποτελεσματικό ένα σύστημα για όλες τις εφαρμογές στην προσθετική τσιμεντοποίησης χάρη σε μία ποικιλία διαφορετικών μεγεθών φυσίγγων και ειδικών παρελκομένων * εύκολο Heraeus Hellas EPE · ΛΕΩΦ.ΚΗΦΙΣΙΑΣ 124 · 11526 ΑΘΗΝΑ · ΕΛΛΑΔΑ · Τηλ: 210 6995 666 · Φαξ: 210 6995 664 · www.heraeus-medical.com 6 www.pitsilidis.gr Π Ρ Ο Σ ΤΑ Σ Ι Α Α Π Ο Φ Θ Ε * DC000718 12/2009 Ισορροπημένη Αποτελεσματικότητα και Ασφάλεια1,2 *ΦΘΕ: Φλεβική Θρομβοεμβολή ΟΙ ΟΥΣΙΩΔΕΙΣ ΠΛΗΡΟΦΟΡΙΕΣ ΤΗΣ ΠΕΡΙΛΗΨΗΣ ΧΑΡΑΚΤΗΡΙΣΤΙΚΩΝ ΠΡΟΪΟΝΤΟΣ ΕΜΦΑΝΙΖΟΝΤΑΙ ΣΕ ΕΠΟΜΕΝΗ ΣΕΛΙΔΑ ΤΟΥ ΕΝΤΥΠΟΥ BOEHRINGER INGELHEIM EΛΛAΣ Α.Ε. ΕΛΛΗΝΙΚΟY 2, 167 77 ΕΛΛΗΝΙΚO, ΑΘHΝΑ, ΤΗΛ.: 210 8906 300, ΓΡΑΦΕIΟ ΜΑΚΕΔΟΝIΑΣ ΘΡAΚΗΣ: ΑΝΤΩΝΗ ΤΡIΤΣΗ 15-17 & ΜΑΡIΑΣ ΚAΛΛΑΣ 6, 57001,ΘEΡΜΗ, ΘΕΣΣΑΛΟΝIΚΗ, ΤΗΛ. 2310 424618 7 Αλλάζει την αντιπηκτική αγωγή 22nd PancyprianOrthopaedic Conference FRIDAY 26/10/2012 14:30-15:00 REGISTRATIONS 15:00-16:15 SESSION A. BASIC SCIENCES FOOT & ANKLE Chairmen: Andreas Tanos and Yiannis Vasiliou 15:00-15:15 Clinical Examination Speaker: Andreas Christou The function of the foot - Biomechanics Speaker: Vlatis Georgios The foot and ankle - Radiology Speaker: Demos Michaelides The use of foot pressure platform in designing of orthotic-orthopaedic insoles Speaker: Diamanto Malliotou Papasavvas Discussion 15:15-15:30 15:30-15:45 15:45-16:00 16:00-16:15 16:15-17:10 SESSION B. METATARSALGIA Chairman: Akis Schizas 16:15-16:35 Etiology Speaker: Yves Tourné Operative treatment when & how-metatarsal osteotomies Speaker: Fernando Alvarez Discussion 16:35-16:55 16:55-17:10 17:10-17:30 Lecture: Historic Findings & Symbolisms of footprints Speaker: Eleftherios E. Dounis 17:30-18:00 COMMERCIAL EXHIBITION OPENING 18:30-20:30 Opening Ceremony / Welcome Reception Dedicated at the opening of the medical school of the University of Cyprus. Venue: University of Cyprus (The language of the opening ceremony is Greek. Written translation in English will be given to all foreign participants) 18:30-18:50 ADRESSES: 1. Rector of the University of Cyprus, Mr. Christofides Constantinos 2. President of the Cyprus Association of Orthopaedic Surgery and Traumatology, Dr. Nicolaos P. Maroudias 8 8 3. Representative of the Ministry of Education and Culture, Dr. Eleni Meli 4. President of the Hellenic Association of Orthopaedic Surgery and Traumatology, Dr. Dionisios-Alexandros Verettas 5. Vice President of the Hellenic Association of Orthopaedic Surgery and Traumatology, Professor at the University of Thessalia, Dr. Malizos N. Konstantinos 18:50-19:05 LECTURE: Τhe Medical School at the University of Cyprus: who needs it? Prof. Andreas Adam, Chairman of the Interim IT Medical School Board Committee, Professor of Interventional Radiology at King’s Col lege London, and Clinical Director of Radiology, Nuclear Medicine and Medical Physics, at Guy’s and St Thomas’ Hospital. 19:05-20:30 COCKTAIL PARTY 08:00 - 10:00 SATURDAY 27/10/2012 08:30-10:00 REGISTRATIONS 09:00-10:00 FREE PAPER PRESENTATIONS Chairmen: Lanitis Venetoklis and Petros Spastris PARALLEL SESSION Room: Ahera PHYSIOTHERAPY SESSION Physiotherapy Session programme at page 13 Aποκλεισμός του κνημιαίου και του περονιαίου νεύρου για επεμβάσεις άκρου ποδός και ποδοκνημικής. Λέκκα Ν., Κορδαλής Ν., Μανουλίδου Ρ. outcome measure. Lambros Athanatos, Mathew Nixon, Gill Holmes, Leroy James, Alf Bass Management strategy for ankle impingement in athletes: a ten-year experience. George D. Tsikouris, Panagiotis I. Intzirtis, Emmanouil V. Zambiakis, Lucas Tamprantzis, Demetrios Tsikouris, Eleftherios Tsikouris, Panagiotis Kourougenis, Sotirios K. Plessas 9 Fixation of Mitchell osteotomy with bioabsorbable pins for treatment of hallux valgus deformity. N. Efstathopoulos, S. Lallos, J. Lazarettos, D. Korres, L. Roumeliotis, VS Nikolaou 22nd PancyprianOrthopaedic Conference The scarf osteotomy in hallux valgus surgery. Malizos K.N, Samaras D, Dailiana Z, Gougoulias N, Varitimidis S, Hantes Mr The LCP distal ulna hook plate for the fixation of distal ulna fractures. Constantinos Kritiotis, Claire Simpson, Manish Gupta, Dominic Power The medial femoral condyle vascularised bone graft for the treatment of non union of the clavicle. A report of two cases. Constantinos Kritiotis, Claire Simpson, Simon Tan, Dominic Power 10:00-10:30 BREAK / COMMERCIAL EXHIBITION VISITING TIME 10:30-12:30 SESSION C. EFORT FORUM - FIRST RAY PATHOLOGY (H.V= Hallux Valgus) Chairmen: Eleftherios E. Dounis, Louis Loizou 10:30-10:45 12:15-12:30 Opening of the EFORT forum Speaker: Nicolaos P. Maroudias & Thierry Begue (EFORT) Etiology - Natural History of Hallux Valgus Speaker: Eleftheriou Kyriacos How do you treat Algorithm + Conservative treatment Speaker: Don Mc Bride Distal osteotomies, when & how Speaker: Yves Tourne Proximal osteotomies, when & how Speaker: Fernando Alvarez Tarsometatarsal arthrodesis for the treatment of Hallux Valgus Speaker: Thanos Badekas Hallux Rigidus Speaker: Don Mc Bride Discussion & Summary of the EFORT Forum 12:30-15:30 LUNCH BREAK 12:30-14:00 Industrial symposium by AstraZeneca/Alector Pharmaceuticals Room: Kantara “Γαστροπροστασία από Μη Στεροειδή Αντιφλεγμονώδη: ο ρόλος των PPIs“ (Gastroprotection from NSAIDs: The role of PPIs) Ομιλητής / Speaker: Σπήλιος Μανωλακόπουλος Επίκουρος Καθηγητής Παθολογίας-Γαστρεντερολογίας, Ιατρική Σχολή Πανεπιστημίου Αθηνών, 2η Πανεπιστημιακή Παθολογική Κλινική, Γενικό Νοσοκομείο Αθηνών ¨ΙΠΠΟΚΡΑΤΕΙΟ¨ 10:45-11:00 11:00-11:15 11:15-11:30 11:30-11:45 11:45-12:00 12:00-12:15 Light lunch will follow for all symposium participants 10 13:45-15:30 26-28 Workshop by Orthofix Srl Room: Ahera “In a world of trauma a Galaxy of solutions” October 2012 15:30-16:00 Keynote Lecture: Chairman: Nicolaos P.Maroudias Interventional Radiology: It’s Surgery, but not as surgeons know it Speaker: Andreas Adam 16:00-16:30 BREAK / COMMERCIAL EXHIBITION VISITING TIME 16:30-19:30 SESSION D. TRAUMA Chairmen: Malizos N. Konstantinos and Stathis Tourvas 16:30-16:50 19:10-19:30 Pilon Fractures Speaker: Antoniou Constantinos Calcaneal fractures open or minimal invasive Reconstruction Speaker: Peter Rosenfeld Calcaneal fracture management with circular frames below the ankle joint. An innovative approach. Speaker: Malizos N. Konstantinos Talus fractures Speaker: Dionysios - Alexandros Verettas Lisfranc fracture dislocation Speaker: Thierry Begue Achilles tendon acute ruptures Speaker: Antoniou Constantinos Ankle instability acute and chronic Speaker: Peter Rosenfeld Diabetic Ankle Fractures Speaker: Thanos Badekas Discussion 20:30 Gala Dinner 16:50-17:10 17:10-17:30 17:30-17:50 17:50-18:10 18:10-18:30 18:30-18:50 18:50-19:10 SUNDAY 28/10/2012 09:00-11:00 SESSION E. ARTHROSCOPY IN THE ANKLE AND FOOT Chairmen: Odysseas Athanatos and Nicos Papaloukas 09:00-09:15 Basic Principles and practical aspects of the Foot and Ankle Arthroscopy Speaker: Peter Rosenfeld 11 final program 22nd PancyprianOrthopaedic 09:15-09:30 Conference 10:30-11:00 Arthroscopic treatment of ankle impingement Speaker: Prof Kang-lai Tang Subtalar joint arthroscopy Speaker: Prof Kang-lai Tang Small joints arthroscopy of the Foot Speaker: Kyriacos Eleftheriou Endoscopy of the non joint disease of foot Speaker: Prof Kang-lai Tang Arthroscopic treatment of ankle osteochondral lesions Speaker: Kyriacos Eleftheriou Discussion 11:00-11:30 BREAK / COMMERCIAL EXHIBITION VISITING TIME 11:30-11:50 Lecture: Chairman: Andreas Tanos Problems of the lumbar spine associated to the kinematics of the lower limbs Speaker: George S. Sapkas 11:50-13:35 SESSION F. ANKLE ARTHRITIS DEFORMITIES AND CONDITIONS Chairmen: Yiannis Papayiannis and Sergios Sergiou 11:50-12:05 Adult acquired flatfoot deformity Speaker: Vlatis Georgios The Diabetic foot general principles of treatment Speaker: Eleftherios E. Dounis Open & Arthroscopic ankle arthrodesis Speaker: Prof. Kang-lai Tang Ankle arthritis ankle arthroplasty treatment Speaker: Thanos Badekas Triple arthrodesis and isolated fusions Speaker: Vlatis Georgios Cavovarus foot reconstruction Speaker: Thanos Badekas Discussion 09:30-09:45 09:45-10:00 10:00-10:15 10:15-10:30 11:05-12:20 12:20-12:35 12:35-12:50 12:50-13:05 13:05-13:20 13:20-13:35 END OF CONFERENCE 12 26-28 ΠΡΟΓΡΑΜΜΑ ΦΥΣΙΚΟΘΕΡΑΠΕΥΤΙΚΗΣ ΕΝΟΤΗΤΑΣ October 2012 ROOM: Ahera προεδρείο: Δρ Γιάννης Ευσταθιάδης - Λάκης Δρουσιώτης Θεματολογία Α 08:00 - 08:15 Α1. Δρ Άκης Ελευθερίου - Αντιμετώπιση των ασθενών με κατάγματα ποδοκνημικής στην ορθοπεδική. Προτεινόμενοι τρόποι αξιολόγησης και αποκατάστασης ασθενών με την συγκεκριμένη παθολογία. 08:15 - 08:30 Α2. Χρίστος Καραγιάννης - Φυσιοθεραπευτική αντιμετώπιση των ασθενών με κατάγματα ποδοκνημικής. Προτεινόμενοι τρόποι αξιολόγησης και αποκατάστασης ασθενών με την συγκεκριμένη παθολογία 08:30 - 08:40 Συζήτηση Θεματολογία Β 08:40-08:55 Β1. Δρ Γιάννης Ευσταθιάδης - Αντιμετώπιση των ασθενών με τενοντοπάθεια αχίλλειου στην ορθοπεδική. Προτεινόμενοι τρόποι αξιολόγησης και αποκατάστασης των ασθενών με τη συγκεκριμένη παθολογία. 08:55-09:10 Β2. Μιχάλης Ευσταθίου - Φυσιοθεραπευτική αντιμετώπιση των ασθενών με τενοντοπάθεια αχίλλειου. Προτεινόμενοι τρόποι αξιολόγησης και αποκατάστασης ασθενών με την συγκεκριμένη παθολογία 09:10-09:20 Συζήτηση Θεματολογία Γ 13 09:20-09:35 Γ1. Δρ Φοίβος Κυνηγός - Αντιμετώπιση ασθενών με χρόνια αστάθεια ποδοκνημικής άρθρωσης στην ορθοπεδική. Προτεινόμενοι τρόποι αξιολόγησης και αποκατάστασης ασθενών με την συγκεκριμένη παθολογία. 09:35-09:50 Γ2. Χρίστος Σάββα - Φυσιοθεραπευτική αντιμετώπιση των ασθενών με χρόνια αστάθεια ποδοκνημικής άρθρωσης. Προτεινόμενοι τρόποι αξιολόγησης και αποκατάστασης ασθενών με την συγκεκριμένη παθολογία 09:50-10:00 Συζήτηση final program Invited Speakers: Andreas Adam Professor of Interventional Radiology at King’s College London Clinical Director of Radiology Nuclear Medicine and Medical Physics at Guy’s and Thomas’ Hospital Andreas Christou Orthopaedic Surgeon Antoniou Constantinos MD,MSc Orthopaedic Surgeon - Traumatologist Demos Michaelides Radiologist A Evresis Diagnostic Centre Nicosia - Cyprus Diamanto Malliotou-Papasavvas Podologist Nicosia - Cyprus Dionysios - Alexandros Verettas MD, PhD, MSc (Orth) Democritus University of Thrace, Greece President of Hellenic Association of Orthopaedic Surgery and Traumatology (HAOST) Don Mc Bride Consultant Orthopaedic Foot and Ankle Surgeon University Hospital North Staffordshire Past President British Orthopaedic Foot and Ankle Society Council Member European Foot and Ankle Society Council Member British Orthopaedic Association Eleftherios E. Dounis M.D F.A.C.S Consultant Foot Surgeon (emeritus) Athens Fernando Alvarez Head of Foot and Ankle Unit Hospital Sant Rafael, Barcelona, Spain George S. Sapkas Associate Professor in Orthopaedics Medical School Athens University Greece President of the Greek College of Orthopaedic Surgeons Kang-lai Tang, MD, PhD, Professor Chief, Division of Foot and Ankle Surgery Chief, Division of Shoulder and Elbow Surgery Department of Orthopaedic Surgery Southwest Hospital The Third Military Medical University Kyriacos Eleftheriou MD, FRCS(Orth) Foot & Ankle Fellow Chelsea and Westminster Hospital London Malizos N. Konstantinos, MD, PhD Professor & Chairman, Dpt of Orthopaedic Surgery & Musculoskeletal Trauma, University of Thessalia, Greece Peter Rosenfeld Consultant Foot & Ankle Surgeon Imperial Hospital, Fortius Clinic U.K Thanos Badekas M.D Director Foot & Ankle Clinic Metropolitan Hospital Athens Hon Treasurer European Foot & Ankle Society Past President Greek Foot & Ankle Society Thierry Begue (EFORT) M.D., Ph.D. Senior orthopedic Surgeon Professor of Orthopedic and Trauma Surgery Chairman Department of Orthopaedic and Trauma Surgery, Antoine Beclere Hospital, University Paris-Sud XI, Clamart, France. Professor of Orthopaedic Surgery, Bicetre Medical School, University Paris-Sud XI. Vlatis Georgios Orthopaedic Surgeon Athens - Greece Yves Tourne Orthopaedic Surgery, Foot & Ankle Surgery Past-President of the Association Francaise de Chirurgie du Pied Chairman Education Committee of EFAS Groupe Chirurgical République-Grenoble-France [email protected] 14 Orthofix redesigns External Fixation, again! Orthopedics | Spine | Sport Medicine DWXUGD\ Live at the Orthofix booth… VKRSRQ6 WKHZRUN 7U\LWDW Cyprus Pharmaceutical Organization Ltd ORGANIZATION wCOSTAS w w. o r t hPAPAELLINAS ofix.com 15 ABSTRACT BOOK 17 FREE PAPER ABSTRACTS 18 26-28 October 2012 ΑΠΟΚΛΕΙΣΜΟΣ ΤΟΥ ΚΝΗΜΙΑΙΟΥ ΚΑΙ ΤΟΥ ΠΕΡΟΝΙΑΙΟΥ ΝΕΥΡΟΥ ΓΙΑ ΕΠΕΜΒΑΣΕΙΣ ΑΚΡΟΥ ΠΟΔΟΣ ΚΑΙ ΠΟΔΟΚΝΗΜΙΚΗΣ Λέκκα Ν., Κορδαλής Ν., Μανουλίδου Ρ. Γενικό Νοσοκομείο Αμμοχώστου Σκοπός αυτής της εργασίας είναι να τονισθεί η αποτελεσματικότητα και η ασφάλεια του αποκλεισμού του ισχιακού νεύρου στο επίπεδο του ιγνυακού βόθρου ως τεχνική επιλογής για χειρουργική αναισθησία άκρου ποδός με τη χρήση και μη της ίσχαιμης περίδεσης. Ο αποκλεισμός αυτός αφορά τεχνική επιλογής για ασθενείς μιας μέρας νοσηλείας, για επιβεβαρυμμένους ασθενείς, για ασθενείς με αντένδειξη χορήγησης γενικής αναισθησίας και όταν δεν είναι εφικτοί οι κεντρικοί αποκλεισμοί. Μελετήσαμε 13 ασθενείς, όπου οι 7 αφορούσαν κατάγματα έσω/έξω σφυρού, οι 3 κατάγματα μεταταρσίων και οι 3 διόρθωση βλαισού μεγάλου δαχτύλου. Οι ασθενείς έλαβαν 30cc όγκου διαλύματος Ropivacaine 0,5 %. Τοποθετήθηκαν σε πρηνή θέση, με υποστήριξη του άκρου. Αναγνωρίστηκε η πτυχή με τα όρια του τένοντα του δικεφάλου του μηριαίου και του τένοντα του ημιυμενώδους μυός. Στο μέσον τους σε απόσταση 7 εκατοστών από την πτυχή του γόνατος γίνεται η έγχυση του τοπικού αναισθητικού μετά από ανίχνευση μυϊκής διέγερσης με τη χρήση νευροδιεγέρτη ( 2Hz, 100μsec) στα 0.4-0.6 mA σε βάθος 3- 5 εκατοστών. Ίσχαιμη περίδεση .τοποθετήθηκε κάτω από το γόνατο σε 10 ασθενείς. Σημειώσαμε το χρόνο ανάγκης της πρώτης μετεγχειρητικής αναλγησίας, την εμφάνιση τυχόν επιπλοκών και την ικανοποίηση των ασθενών. Ο συγκεκριμένος αποκλεισμός αποτελεί εξαιρετική τεχνική για επεμβάσεις άκρου ποδός και ποδοκνημικής . Παρατηρήσαμε δε ότι η μέση διάρκεια της μετεγχειρητικής αναλγησίας ήταν 280λεπτά. Δεν παρουσιάστηκε καμία επιπλοκή (παραισθησίες, ενδαγγειακή έγχυση) και οι ασθενείς δήλωσαν ικανοποιημένοι από την τεχνική αυτή. Ο α π ο κ λ ε ι σ μ ό ς α υ τό ς α π ο τ ε λ ε ί μ έ θ ο δ ο ε π ι λ ο γ ή ς σ ε ε π ε μ β ά σ ε ι ς ά κ ρ ο υ π ο δ ό ς και ποδοκνημικής , ιδιαιτέρως σε επεμβάσεις με νοσηλεία μιας ημέρας. 19 final program 22nd PancyprianOrthopaedic Conference THE ROLE OF PEDOBRAPRAPHIC ASSESSMENT OF FLATFOOT AND IT’S PLACE AS AN OUTCOME MEASURE Lambros Athanatos 1, Mathew Nixon1, Gill Holmes2, Leroy James1 and Alf Bass1 1 Alder Hey Children’s Hospital, Trauma & Orthopaedics, Liverpool, UK 2 Alder Hey Children’s Hospital, North West Movement Analysis Centre, Liverpool, UK Author correspondence: [email protected] This paper is submitted as a free paper. SCOPE OF THE PAPER Flexible flat foot is considered one of the commonest normal variants in children’s orthopaedic practice. The weight-bearing foot is usually regarded as flexible on the basis of results from clinical and radiographic examination as well as measured foot-ground pressure pattern. Our aim was to compare the pedobarographic and radiographic findings of normal arched and symptomatic flexible flat feet and investigate if there were sensitive markers that could be used in selecting patients for surgical correction. PATIENTS/MATERIALS and METHODS We retrospectively collected data from eighteen patients (ten to sixteen year old). Our control group consisted of ten patients (twenty feet) with normal arched feet and the study group of eight patients (fifteen feet) with symptomatic flat feet who were awaiting surgical correction. The mean and standard deviations of three radiographic markers (Calcaneal pitch, Naviculocuboid overlap and lateral Talo-1st metatarsal angle) in addition to foot pressures measured at the hindfoot, medial/ lateral/total midfoot (MMF, LMF, TMF), forefoot and the percentage of weight going through the MMF over the TMF (medial midfoot ratio (MMFR) during the mid-stance gait phase are reported. In addition, the sensitivity, specificity, positive predictive value and negative predictive value of the pedobarographic parameters were estimated. RESULTS There was a significant difference in the Naviculocuboid overlap (P<0.001 T test) and Calcaneal pitch (P<0.05 T test) between both groups. The flat feet group had significantly higher MMF, LMF, TMF and MMFR (P < 0.001 Mann-Whitney). LMF had the highest sensitivity and negative predictive value (94%) whereas MMF, TMF and MMFR had the highest specificity and positive predictive value (100%). CONCLUSIONS Compared to our control group, patients with symptomatic flexible flat feet had significantly higher pressures distributed in the midfoot, in particular in the medial midfoot. Pedobarography appears to be a sensitive and specific tool that can be used, in conjunction with clinical and radiographic findings, in diagnosing flat feet. Our study suggests that pedobarography could be used to measure the degree of deformity before and after surgical intervention. 20 26-28 October 2012 MANAGEMENT STRATEGY FOR ANKLE IMPINGEMENT IN AHTLETES: A TEN – YEAR EXPERIENCE George D. Tsikouris1, Panagiotis I. Intzirtzis1, Emmanouil V. Zampiakis1, Lucas Tamprantzis1, Demetrios P. Tsikouris1, Eleftherios P. Tsikouris1, Panagiotis T. Kourougenis1, Sotirios K. Plessas1 1Athens Kolonaki Orthopaedics & Sports Medicine Center BACKGROUND: Soft-tissue and osseous anterior impingement syndromes of the ankle can be an important cause of painful limitation of ankle movement, particularly in athletes. These conditions arise from initial ankle injuries which, in a subacute or chronic basis, lead to development of abnormal osseous and soft-tissue thickening within the ankle joint. AIM: To present the outcome of arthroscopic excision of restrictors in ankle movement with concomitant anatomic ankle ligament reconstruction in athletes. PATIENTS and METHODS : Eighteen athletes, 12 males and 6 females, (of which, 9 basketball-players, 4 football-players, 2 dancers) were treated over the last 10 years. The mean age was 22 years. The sports activities of all patients were dramatically deteriorated due to chronic ankle pain and/or a “giving way” feeling. The thorough clinical examination included reproduction of impingement pain (anterior, anterolateral, anteromedial, or posterior) and stability testing in comparison to the contralateral ankle. Radiographs included anteroposterior, lateral and oblique views in a weightbearing position. Ultrasound and plain MRI testing was performed without exception. Each patient underwent arthroscopic evaluation. Arthroscopic debridement of hypertrophic tissue arising from AITFL, ATFL or deltoid was performed in 16 patients. Arthroscopic decompression of bony impingement (excision of tibial or talar osteophyte) was needed in 10 patients. Ankle ligament reconstruction was performed in 13 cases (modified Brostrom in 11 athletes, deltoid reconstruction in 2 others). Excision of osseous and soft-tissue components of posterior impingement via open posterolateral approach was performed in 2 dancers. In addition, debridement and microfractures were indicated in 4 patients with osteochondral lesions and to 2 patients was applied Autologus Chondrocyte Implantation. A custom rehabilitation program was utilized for each individual. RESULTS: Patients were followed up at 1, 3, 6, 9, and 12 months postoperatively using the FADI score. The results at 12 months were ranged above 90 for 13 athletes, between 85 – 90 for 4 athletes and between 80 – 85 for 1 athlete. Poorer results are correlated with concomitant osteochondral lesions. The highest scores were achieved when ligament reconstruction had been performed. DISCUSSION: Inadequately and inappropriately healed ligaments do not regain the mechanical integrity that is necessary to stabilize the ankle against physiologic stresses. Chronic ankle instability should always be suspected in an athlete with chronic ankle pain and findings of ankle impingement. A clinical exam and an ultrasound exam contribute in a more accurate diagnosis for an ankle instability. The appearance of an injured ligament on plain MRI varies and is not reliable to estimate the functional sufficiency of the ligament. Ankle arthroscopy provides great visualization of joint pathology in impingement syndromes that is amenable to repair. Open ligament repair is reliable and optimizes the functional results. CONCLUSION: Arthroscopic treatment of anterior ankle impingement together with ankle ligament reconstruction, when indicated, is essential for obtaining a stable and functionally efficient ankle. 21 final program 22nd PancyprianOrthopaedic Conference Fixation of Mitchell Osteotomy With Bioabsorbable Pins For Treatment Of Hallux Valgus Deformity. N. Efstathopoulos, S. Lallos, J. Lazarettos, D. Korres, L. Roumeliotis, VS Nikolaou, 2nd Department of Orthopaedics, Athens University, Konstantopoulio Hospital, Greece ORAL PRESENTATION Objective: We hypothesised that the use of bioabsorbable pins in Mitchell΄s osteotomy would improve the outcome of patients treated for Hallux Valgus deformity. Patients and methods: 68 patients underwent Mitchell osteotomy to correct hallux valgus deformity. 33 patients(Group A) had Mitchell osteotomy augmented with bioabsorbable pins. 35 patients were treated with the classical operative procedure(Group B). Hallux valgus angle(HVA), intermetatarsal angle(IMA), the AOFAS’ hallux–metatarsophalangeal–interphalangeal scale and the pain visual analog score(VAS) were measured preoperatively and postoperatively. Results: There was no statistical significant difference between the two groups as far as the improvement of the IMA , HVA and the AOFAS’ scale concerns. Patients of group A had significantly less postoperative pain and returned to the previous activities earlier than patients of group B. Conclusions: The usage of the pins didn’t improve the final outcome of the osteotomy. However, allowed for faster rehabilitation due to less postoperative pain. 22 26-28 October 2012 THE SCARF OSTEOTOMY IN HALLUX VALGUS SURGERY Samaras D., Dailiana Z., Gougoulias N., Varitimidis S., Hantes M., Malizos K.N. Department of Orthopaedic Surgery, University of Thessalia, Larissa, Greece Aim: To evaluate the long-term results and present our experience with Scarf osteotomy. Patients & Methods: Between 2001 and 2011, 84 patients (79 women and five men with mean age of 53,7 years) underwent 96 scarf osteotomies. All operations (except 4 cases with spinal anesthesia) were performed under peripheral nerve block. Akin osteotomy was performed in four cases and 44 lesser metatarsal osteotomies in 33 feet (38 Helal, 6 Weil). Toe deformities were corrected in 18 cases. Excision of Morton’s neuroma was done in one patient. Postoperatively a heel weight-bearing shoe was worn for six weeks. Prophylaxis for thromboembolism was administered for 3 weeks. Mean follow-up was 60 months (12-123). Results: There was decrease of Hallux Valgus Ankle (HVA) from 37o (26-62) preoperatively to 17o (5-28) postoperatively and of IMA from 16º (10-27) to 10º (5-16) respectively. The forefoot AOFAS score improved from 45 (35-60) preoperatively to 87 (65-98) postoperatively. Nine early complications: intraoperative fractures (2), confirmed DVT (1), CRPS- type I (4), superficial infection (2) were encountered successfully. There were 3 cases of failure of fixation – one required new ORIF with plate. In two patients removal of prominent screws was necessary. In 3 cases with recurrence of the deformity revision of lateral release was performed, but in one case an arthrodesis of 1st metatarsophalangeal joint was performed 5 years after initial procedure. In 9 of 96 operated feet the patients were not satisfied. Conclusions: Although the procedure is technically demanding with extending learning curve, it is effective with acceptable rate of complications. 23 final program 22nd PancyprianOrthopaedic Conference THE LCP DISTAL ULNA HOOK PLATE FOR THE FIXATION OF DISTAL ULNA FRACTURES Constantinos KRITIOTIS, Claire SIMPSON, Manish GUPTA, Dominic POWER Birmingham Hand Centre Queen Elizabeth Hospital Birmingham University Hospital Birmingham NHS Trust Birmingham UK Purpose : To report our early results with the use of an anatomical locking hook plate for the fixation of distal ulna fractures. Methods : We performed a retrospective review of all cases of distal radius fractures requiring simultaneous ulna fixation at the Birmingham Hand Centre between May 2010 and September 2012. The distal ulna fractures were classified using the Fernandez classification. The mean follow up period was 28 months. Patients were assessed measuring both radiological and clinical outcomes. Results : 436 patients had operative stabilization of distal radius fractures during the study period. 15 of the patients who required stabilization of the associated distal ulna fracture were treated with a 2mm anatomical fixed angle locking plate. The age range of patients was 17 to 81 years (mean 47 years). All fractures united. There were no infections. One patients had a subsequent Darrach’s procedure for DRUJ arthritis due to screw penetration. Three other patients had the plates removed due to hardware giving them symptoms, which completely resolved after the removal of plates. One patient had a malunion of the distal ulna due to inappropriate implant selection. Conclusions : The LCP distal ulna hook plate provides reliable union of distal ulna fractures. Type of Study/Level of Evidence : Therapeutic IV 24 26-28 October 2012 THE MEDIAL FEMORAL CONDYLE VASCULARISED BONE GRAFT FOR THE TREATMENT OF NON UNION OF THE CLAVICLE. A REPORT OF TWO CASES Constantinos KRITIOTIS, Claire SIMPSON, Simon TAN, Dominic POWER Birmingham Hand Centre Queen Elizabeth Hospital Birmingham University Hospital Birmingham NHS Trust Birmingham UK Purpose : To report our results from the use of medial femoral condyle vascularized bone graft in two cases with clavicle non union. Methods : In 28/02/12 and in 08/05/12 we performed in two patients medial femoral condyle vascularized bone grafting for clavicle non unions. The first case was an infected non union of the left clavicle in a 46-year old female patient with concomitant iatrogenic brachial plexus damage and the second case was a non union in a 46-year old patient following a corrective osteotomy of the clavicle for brachial plexus entrapment in the callus after a malunion of the clavicle. Results : The patients were assessed with radiological and clinical criteria. Both patients recovered completely from their neurological problems due to the fact that there was not significant plexus injury. The first patient progressed into complete union seven months after the operation and has returned to her everyday activities (including working as a bus driver). The second patient is also making a very good recovery and is able to perform his everyday activities without pain. His x-rays reveal that his fracture is progressing to full union as well. Conclusion : The vascularized medial femoral condyle bone graft proves to be a versatile tool in the hands of the surgeon. It can help reconstruct small to medium size bone defects anywhere in the body and certainly can be a very good alternative for the reconstruction of bone defects in the clavicle. 25 final program POSTER ABSTRACTS 26 26-28 October 2012 TRANSCALCANEAL TALONAVICULAR DISLICATION ASSOCIATED WITH AN OPEN COMMINUTED CALCANEAL FRACTURE: A CASE REPORT. Vassilios Papathanasiou, Spyridon P. Galanakos, Stamatis Kyriakopoulos Helias Kotoulas, Ioannis P. Sofianos Orthopaedic Department General Hospital of Levadia Greece. Patients and methods: A 27-year-old injured his left hindfoot after a fall from height while at work. He was found to have a deformity of his hindfoot and a wound measuring approximately 15 cm long extended from the medial malleolus to the plantar aspect of his heel with small bone fragments exposed in the wound. There was no neurovascular compromise in his injured left foot. Anteroposterior, lateral, and oblique radiographs of the foot and ankle were obtained and revealed a multifragmentary fracture of the calcaneum associated with a talonavicular dislocation. The talus was planterflexed with its head portion displaced plantarwards through the calcaneal fracture. The talonavicular joint was stabilized with 2-mm Kirschner wires (K-wires) introduced from the dorsal and medial aspect of the foot transfixing the talonavicular joint. Furthermore, the calcaneal fracture was manipulated through the open wound to obtain better alignment and using a hybrid Ace-Fisher External Fixation System (DePuy Ace, Warsaw, IN, USA). Results: Three weeks later, the wound was healed completely without any further complications and after that it was managed with normal dry sterile dressing changes At 6 weeks postoperatively, the K-wires from the talonavicular joint were removed, but the hybrid fixator remained for an additional 10 weeks. At the end of the first postoperative year, range of motion of his left ankle was dorsiflexion 5_, plantarflexion 40°, inversion 20° and eversion 10°. The American Orthopaedic Foot and Ankle Society hindfoot score6 at 18 months was 63. Discussion Association of dorsal dislocation of the navicular from the talus with an open fracture of the calcaneus is an uncommon but severe injury. It is known that the goals of open calcaneal fracture management include timely healing of the soft tissue without infection and maintenance of bony alignment Besides the good results of the case patient, the prognosis for most of these types of injuries varies from severe functional limitations and/or chronic pain to even amputation. 27 final program 22nd PancyprianOrthopaedic Conference ΧΡΗΣΗ ΕΙΔΙΚΗΣ ΔΙΑΜΟΡΦΩΣΗΣ ΚΛΕΙΔΟΥΜΕΝΩΝ ΠΛΑΚΩΝ ΣΤΗ ΧΕΙΡΟΥΡΓΙΚΗ ΤΟΥ ΑΚΡΟΥ ΠΟΔΑ Στ. Κυριακόπουλος, Η. Κωτούλας , Δ. Σκουτέρης , Η. Τσολής, Ι.Π Σοφιανός Ορθοπαιδική κλινική Γενικού Νοσοκομείου Λιβαδειάς Σκοπός: Σκοπός της εργασίας είναι η παρουσίαση της εμπειρίας της κλινικής μας στη χειρουργική του άκρου πόδα με την εφαρμογή ειδικών κλειδούμενων πλακών τύπου DARKΟ Υλικό και Μέθοδος: Πρόκειται για 15 ασθενείς 10 γυναίκες και 5 άνδρες ηλικίας από 25 ως 82 ετών οι οποίοι έπασχαν από βλαισό μέγα δάκτυλο (12 περιπτώσεις) και χρόνιο υπεξάρθρημα της 1ης Μεταταρσιοφαλαγγικής άρθρωσης (3 περιπτώσεις συνεπεία Ρευματοειδούς Αρθρίτιδας). Η αντιμετώπιση του βλαισού μεγάλου δακτύλου έγινε με ανοικτή έσω οστεοτομία βάσης, συγκράτηση της οστεοτομίας με ειδική τετράπλευρη πλάκα η οποία στο κέντρο έχει κατάλληλη διαμόρφωσησφήνα η οποία εισχωρεί ανάμεσα στην οστεοτομία και χρήση 4 κλειδούμενων κοχλιών. Στις περιπτώσεις του υπεξαρθρήματος έγινε αρθρόδεση της μεταταρσιοφαλαγγικής άρθρωσης ύστερα από κατάλληλη διαμόρφωση των επιφανειών με ειδικά ανατομικά γλύφανα Αποτελέσματα: Η πόρωση των οστεοτομιών και η επίτευξη της αρθρόδεσης επετεύχθη σε όλες τις περιπτώσεις. Η βάδιση έγινε άμεσα με τη χρήση ειδικού υποδήματος αποφόρτισης του προσθίου ποδός για διάρκεια 20 ημερών. Συμπεράσματα: Η χρήση των κλειδούμενων πλακών ανατομικών πλακών τύπου DARKO αποτελούν μια αξιόπιστη λύση στη χειρουργική του άκρου πόδα. Το χαμηλό τους προφίλ και το υλικό κατασκευής (τιτάνιο) την καθιστούν εύκολη στη χρήση ακόμα και στον μη πεπειραμένο χειρουργό. Προσφέρουν εξαιρετική σταθερότητα η οποία επιτρέπει την άμεση κινητοποίηση του ασθενή περιορίζοντας πολύ το ποσοστό αστοχιών και επιπλοκών. 28 26-28 October 2012 Long term follow-up, of an Inflammatory leiomyosarcoma of the Ankle Joint. VS Nikolaou, S. Lallos, J. Lazarettos, D. Korres, N. Efstathopoulos 2nd Department of Orthopaedics, Athens University, Konstantopoulio Hospital, Greece POSTER Abstract Inflammatory leiomyosarcoma is a rare variant of smooth muscle cell tumor more often found in the trunk, extremities and retroperitoneoum. We present a case of inflammatory leiomyosarcoma arising in the ankle joint of a 55 year old white male. Immunohistochemistry, electron microscopy, and cytogenetics is useful in the differentiation of this rare variant of leiomyosarcoma from other tumors. Ten years after surgical excision of the lesion, patient is disease-free, with no symptoms and good limb function. Prognosis of this variant seems to be favourable when treated with wide excision of the tumor. 29 final program 22nd PancyprianOrthopaedic Conference RECURRENT INTRA-ARTICULAR OSTEOID OSTEOMA OF THE HIP AFTER RADIOFREQUENCY ABLATION. LONG TERM FOLLOW UP. N. Efstathopoulos , L. Roumeiotis, E. Brilakis, VS Nikolaou, 2nd Department of Orthopaedics, Athens University, Konstantopoulio Hospital, Greece POSTER Abstract We present a case of a 53-year-old woman with recurrent intra-articular osteoid osteoma of the hip 6 months after initial treatment with percutaneous radiofrequency ablation. En bloc surgical excision of the osteoid osteoma and prophylactic internal fixation for impending stress fracture was performed. The patient is pain free, has returned to normal function and there is no sign of recurrence at the 9-year follow-up. Intra – articular osteoid osteoma, present a diagnostic challenge and often they are misdiagnosed. Minimally invasive ablation techniques can fail in significant percentage and then surgical excision with histological confirmation remains the definitive treatment of choice. 30 26-28 October 2012 Morton’s Neuroma: A clinical versus radiological diagnosis Philip Pastides, Sameh El-Sallakh, Charalambos Charalambides The Whittington Hospital, London, UK Aims: The aim of our study was to compare the clinical versus radiological diagnosis of patients suffering from a Morton’s neuroma. Methods: Clinical assessments and pre-operative radiological imaging of patients who had excision of a Morton’s neuromas were retrospectively compared. Results: 43 neuromas were excised from 36 patients over 68 months. The commonest clinical symptoms were tenderness on direct palpation (100%), pain on weight bearing (91%) which was relieved by rest (81%). The most sensitive clinical sign was a Mulder’s click. Clinical assessment had a sensitivity of 98% (42/43). Ultrasonography had a sensitivity of 90% (28/31) and magnetic resonance imaging had a sensitivity of 88% (14/16). Conclusion: There is no absolute requirement for imaging patients who clinically have a Morton’s neuroma. The two main indications for imaging are (a) an unclear clinical assessment and (b) cases when more than one web space is affected. Ultrasonography should be the investigation of choice. 31 final program 22nd PancyprianOrthopaedic Conference SUTURE FIXATION OF AKIN OSTEOTOMY: CLINICAL RESULTS AND COST ANALYSIS OF A PROSPECTIVE STUDY Philip Pastides, Ahmad K Malik, Bhupinder Mann, Charalambos Charalambides , Charalambos Charalambides The Whittington Hospital, London, UK Aims: In his original work, Akins did not describe the use of any metal work for his osteotomy. Today the osteotomy is most commonly held and fixed with either a staple or screw, however we describe the results obtained with a simple suture technique. Methods: Data was prospectively collected on 125 consecutive patients undergoing an Akin osteotomy. The hallux valgus (HV) and intermetatarsal (IM) angles pre and postoperatively were recorded. Patients were reviewed at 6 week follow up to assess their function and alignment. A cost analysis was also performed comparing different fixation methods. Results: 111 of the patients were female and the average age at time of surgery was 49 years. 104 cases were in conjunction with hallux valgus correction while 21 cases were for hallux interphalangeus. The mean preoperative HV angle was 33.3 degrees (range 22 to 53), and the IM angle 13.3 degrees (range 9 to 25). At the 6 week follow up all patients had shown signs of radiological union. The postoperative HV angle was 12.4 degrees (range 7 to 17) and the IM angle 6.4 degrees (range 5 to 11) Conclusion: This method is a quick, easy, implant free method of fixing the Akin osteotomy, with no need for removal of metalwork. In addition it is a cost effective method which is clinically just as effective as methods requiring a staple or screw 32 26-28 October 2012 MINIMALLY INVASIVE CHEILECTOMY FOR THE TREATMENT OF LOW GRADE HALLUX RIGIDUS: A PROSPECTIVE STUDY REPORTING ON PATIENT OUTCOME Philip Pastides, Sameh El-Sallakh, Charalambos Charalambides The Whittington Hospital, London, UK Introduction: Hallux rigidus is a benign condition that can cause significant restriction of everyday function and activities. It can lead to significant restriction of everyday function and recreational activities. Methods: 41 patients (54 feet) with grade I to III hallux rigidus underwent minimally invasive cheilectomy over a twenty month period. The mean age was 43 years. Outcomes were quantified using the American Orthopaedic Foot and Ankle Society Hallux Metatarso-Interphalangeal scoring system. Results: At six weeks, AOFAS-HMI scores improved from 88.2 to 71.2 (p<0.001). Improvements were noted in pain, function, footwear and range of movement (p<0.002). Most of the patients returned to clinic in their own shoes at two weeks and all of them at six weeks. Thirty patients (73%) had returned to sporting activities by six weeks. Isolated cases of painful scars and altered sensation completely resolved by three to six months. Conclusion: Minimally invasive cheilectomy is a joint preserving procedure that produces good short to mid term results, with minimal disruption to the soft tissues around the hallux. We advocate the use of this procedure in patients with grade I to III hallux rigidus and no pain during mid range of movement. 33 final program 22nd PancyprianOrthopaedic Conference DEBRIDEMENT AND MICROFRACTURE IN THE TREATMENT OF LATE STAGE FREIBERG’S DISEASE Philip Pastides, Sameh El-Sallakh, Charalambos Charalambides The Whittington Hospital, London, UK Background: Freiberg’s disease is an uncommon condition of anterior metatarsalgia that involves the head of metatarsals. Several operative techniques have been described to treat late stage disease. Methods: We retrospectively reviewed a consecutive series of patients who presented to our institution who did not respond to conservative methods. These patients were treated surgically with an operative technique involving microfracture of the metatarsal head and reattachment of the cartilage flap. Results: Mean follow up was 49 post operative months (18-96). At six months, mean visual analogue pain score at rest and on mobilising was 2.1 (0-3) and 3.1 (0-5) respectively (p<0.05). All 11 patients had reported a satisfactory outcome and return to acceptable activity levels. Conclusion: This operative technique is a safe and feasible treatment option for patients suffering from late stage Freiberg’s disease. It is advantageous as is not causing shortening or other anatomical abnormalities in the area. All of our patients reported a significant reduction of pain in their feet and all were able to walk and run almost pain free. There were no reported cases of severe restriction of movement or fixed deformity of the toe. We conclude that our technique is a successful alternative operative technique for late stage Freiberg’s disease. 34 35 35 36 26-28 October 2012 The Organizing Commitee would like to thank the following companies for their contribution: Main Sponsors: AstraZeneca / Alector Pharmaceuticals Eurobank EFG Cyprus Orthofix Srl Sponsors: Bayer Health Care / Novagem Marios Theocharides Ltd Pfizer Hellas (Cyprus Branch) Unimed (Cyprus) Ltd Vouros Healthcare Ltd Supporters: A. Constantinides Pharmaceuticals Aegis Ltd Anatomic Help Boehringer Ingelheim / CPO George Petrou Ltd Heraeus Hellas Lifepharma Ltd - Member of MSJ Group of Companies MSD Mundipharma Pharmaceuticals Ltd Remedica The Star Medicines Importers Co Ltd Traumatonic Ltd 37 final program 38 19 18 17 LIFT EXHIBITION PLAN 20 16 15 14 13 1 2 3 4 5 12 11 10 9 8 7 6 26-28 October 2012 Booths: 1 Aegis Ltd 3 Mundipharma Pharmaceuticals Ltd 4 MSD 5 Traumatonic Ltd 6 AstraZeneca/Alector Pharmaceuticals 7 Remedica Ltd 9&10 Anatomic Help 11 The Star Medicines Importers Co Ltd 13 George Petrou Ltd 14 Orthofix Srl 15&16 Bayer Health Care/Novagem. 17 Unimed (Cyprus) Ltd 18 Marios Theocharides Ltd 19 Pfizer Hellas (Cyprus Branch) 20 Vouros Healthcare Ltd 39 final program
© Copyright 2026 Paperzz