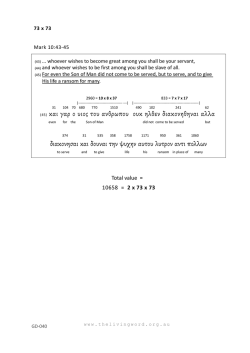
Μπαλατσούρας Δ Φασόλης Α Μπουκόνης Κ Κουκούτσης Γ Παπαλιάκος Ε Καμπέρος Α Ωτορινολαρυγγολογική Κλινική, Τζάνειο Γενικό Νοσοκομείο Πειραιά, Πειραιάς Βλεννογόνιος πλασματοκύττωση: Παρουσίαση περιστατικού Ελληνική Ωτορινολαρυγγολογία Χειρουργική Κεφαλής & Τραχήλου Τόμος 33 - Τεύχος 1 Περίληψη Abstract Eισαγωγή. Η βλεννογόνιος πλασματοκύττωση αποτελεί Introduction. Mucous membrane plasmacytosis is a rare σπάνια ιδιοπαθή βλάβη που συνίσταται από πυκνό idiopathic condition consisting of dense polyclonal Balatsouras D Fassolis A Boukonis C Koukoutsis G Papaliakos E Kaberos A ENT Department, Tzanion General Hospital of Piraeus, Piraeus, Greece Hellenic Otorhinolaryngology Head and Neck Surgery Volume 33 - Issue 1 Corresponding author: Mr. Dimitrios G. Balatsouras, M.D., 23 Achaion Street – Ag. Paraskevi, GR-15343 Athens (Greece), Tel. +30 210 600 4683, Fax +30 210 4592 671 E-Mail: [email protected] Mucous membrane plasmacytosis: Α case report του plasma cell infiltration of the mucous membrane. A case βλεννογόνου. Παρουσιάζουμε μια σπάνια περίπτωση report of mucous membrane plasmacytosis is presented. βλεννογονίου πλασματοκύττωσης. Case report. An 83-year-old man was followed up in our πολυκλωνικό πλασματοκυτταρικό διήθημα Περιγραφή περιστατικού. Άνδρας 83 ετών παρακολου- department for 2 years with increasing hoarseness and θήθηκε στην Κλινική μας επί 2 έτη με βράγχος φωνής και breathlessness. Microlaryngoscopy and pharyngo-oe- δύσπνοια. Η μικρολαρυγγοσκόπηση και η φαρυγγο- sophagoscopy under general anaesthesia revealed a very οισοφαγοσκόπηση υπό γενική αναισθησία αποκάλυψαν την swollen thickened epiglottis. Postoperatively a tra- παρουσία λίαν οιδηματώδους, παχυσμένης επιγλωττίδος. cheostomy was performed. Biopsies and immunocyto- Μετεγχειρητικά πραγματοποιήθηκε τραχειοστομία. Η chemistry from the epiglottis, posterior pharyngeal wall βιοψία και η ανοσοϊστοχη μική μελέτη δειγμάτων εκ της and tracheal ring showed dense subepithelial polyclonal επιγλωττίδος, εκ του οπισθίου φαρυγγικού τοιχώματος και plasmacytosis and squamous metaplasia with focal εκ του τραχειακού δακτυλίου έδειξαν πυκνή υποεπιθηλιακή dyskeratosis and hyperkeratosis, suggesting a diagnosis πολυκλωνική πλασματοκύττωση και πλακώδη μεταπλασία of mucous membrane plasmacytosis. Differential diagno- με εστιακή δυσκεράτωση και υπερκεράτωση, θέτοντας την sis and treatment of this disorder are further discussed. διάγνωση της βλεννογονίου πλασματοκύττωσης. Στη Conclusion. Mucous membrane plasmacytosis of the συνέχεια συζητούνται η διαφορική διάγνωση και η θεραπεία upper aerodigestive tract is a rare condition of unknown της παθήσεως. aetiology. There is no established treatment that is in- Συμπέρασμα. Η βλεννογόνιος πλασματοκύττωση της variably effective. ανωτέρας αεροπεπτικής οδού αποτελεί σπάνια νόσο Key words: Plasmacytoma, plasma cells, epiglottis, la- άγνωστης αιτιολογίας. Δεν υπάρχει ομόφωνα αποδεκτή ryngeal neoplasms, mucous membrane θεραπεία, η οποία να είναι πάντοτε αποτελεσματική. Λέξεις κλειδιά: Πλασματοκύττωμα, πλασματοκύτταρα, επιγλωττίς, λαρυγγικά νεοπλάσματα, βλεννογόνος Mucous membrane plasmacytosis is a rare idiopathic condition consisting of dense polyclonal plasma cell infiltration of the mucous membrane1. Plasma cell infiltrates have been found in the buccal mucosa, palate, nasal aperture, gingival lips, tongue, epiglottis and larynx2. We present a rare case of mucous membrane plasmacytosis of the larynx. throat. He was an ex smoker. He had ischemic heart disease, congestive cardiac failure, diabetes mellitus and cerebro¬vascular disease. On clinical examination, the vocal cords appeared red and slightly oedematous. There was a lot of sticky mucous in the supraglottis and glottis. Suspicious feature for malignancy were absent. Chest x-ray was normal. The patient’s symptoms and appearance of his larynx did not improve after a 2-week course of antibiotics, but afterwards spontaneous improvement occurred and he was discharged after 2 months, with a normal appearance of his larynx. Case Report An 83-year-old man was referred by his general practitioner with 5-week history of hoarse voice and sore 49 The patient was referred back, after one month, because of recurrence of the symptoms. He had 2 recent transient ischaemic attacks and angina, on walking a small distance. Flexible laryngoscopy showed thick yellow mucous in the supraglottis. The vocal cords appeared normal. There was swelling and redness at the supraglottis, and in particular, on the right side of the epiglottis. The appearance failed to improve with amoxycillin-clavulanic acid, and a course of ciprofloxacin. Biopsy under local anaesthesia was decided upon, because general anesthesia was considered too dangerous for the patient’s general condition. Flexible bronchoscopy showed the epiglottis to be diffusely swollen and thickened. The supraglottis was diffusely pale and swollen symmetrically. The true vocal cords appeared normal. Small white nodules were seen on the posterior wall of the hypopharynx, giving a cobblestone appearance. Biopsies from the epiglottis and one of the pharyngeal nodules showed non specific acute and chronic inflammation only. The patient’s condition did not improve and he developed increasing hoarseness and breathlessness. The epiglottis remained swollen and thickened. An examination under general anaesthetic was considered justified in order to obtain more reliable biopsy specimens. Microlaryngoscopy and pharyngo-oesophagoscopy under general anaesthesia revealed a very swollen thickened epiglottis (Fig. 1). The tip and the vallecular surface were smooth, but the laryngeal surface was irregular. The false and true vocal cords were symmetrically oedematous. There was a slight oedema of the subglottis. Multiple small round lesions, measuring a few millimetres in diameter, were found on the mucosa of the posterior wall of the hypopharynx. Otherwise, the remainder of the hypopharynx was normal. Large specimens for biopsy from the epiglottis and posterior pharyngeal wall were obtained. Since intubation had been extremely difficult and because of the fact that some swelling and bleeding were anticipated postoperatively, a tracheostomy was performed. Part of the third tracheal ring was removed to insert the tracheostomy tube, which was sent for histological examination as well. Biopsies from the epiglottis, posterior pharyngeal wall and tracheal ring all showed similar changes. There was a squamous metaplasia of the overlying epithelium. Beneath the epithelium, there was a dense plasmatocytic infiltrate (Fig. 2). Occasional large and binucleate cells were seen, but overall there was no significant atypia. Immunocytochemistry confirmed that the plasmatocytes expressed CD79a, and the plasmatocyte specific marker V38 and CD138. They showed an approximate normal proportion of kappa and lambda light chains. The combination of dense subepithelial polyclonal plasmacytosis and squamous metaplasia with focal dyskeratosis and hyperkeratosis suggested the diagnosis of mucous membrane plasmacytosis. From the laboratory evaluation, full blood count was normal and erythrocyte sediment rate was 30. Urea, electrolytes, calcium, liver function test, uric acid, and lactic acid dehydrogenase were within normal limits, apart from a slightly elevated gamma gluteryl transpeptidase. Immunoglobuline levels were normal, but pro- Fig. 1. Endoscopic view of the larynx (epiglottis) of the patient. Fig. 2. Microscopic appearance of the lesion (specimen of the epiglottis). 50 tissue surgically or with CO2 laser and systematic chemotherapy and radiotherapy7,11. A few patients require tracheostomy, because of airway obstruction. There appears to be no treatment that guarantees a favourable response. One case has been reported where the disease responded favorably to a prolonged course of beclamethasone oral spray6. Our patient responded favorably to oral steroids, allowing decannulation of the trachea. Improvement was maintained by the continuous use of beclamethasone inhaler. Although the epiglottis looked similar as before treatment, inflammation and oedema in the supraglottis, glottis and subglottis improved. None of the previously reported cases has shown a disease regression, but long term survival is good. The longest known survivor has a 16-year duration of the disease. There are not reports of the disease progressing to malignancy. It may be concluded that mucous membrane plasmacytosis of the upper aerodigestive tract is a rare condition of unknown aetiology. There is no established treatment that is invariably effective. Our case responded favourably to oral and inhaled steroids. tein electrophoresis showed a slight increase in gamma globulin. Urine protein electro¬phoresis showed a slight non specific proteinuria. Bone marrow was normal. The patient was treated with prednisolone 30mg daily, for 10 days, with a gradual taper off, for another 10 days. A steroid inhaler was initiated. The tracheostomy tube was removed 10 days after treatment was started and the patient was discharged 5 days later. On re-examination, 1-month, 5-month and 1-year later, he remained well, with normal breathing, voice and swallowing. Epiglottis is still mildly swollen but the remainder of the supraglottis, glottis, and subglottis appear normal. Treatment by steroid inhaler is continued. Discussion Zoon was the first to describe a plasma cell infiltrate of the glans penis, in 19523, and White et al.1 were the first to describe mucous membrane plasmacytosis of the upper aerodigestive tract in 1986, followed by Timms et al4. Ferreiro et al.2 reported 9 cases of this rare condition, in 1996. Since then, several more cases have been reported5-10. The aetiology of the disease is unknown. Interestingly, 2 of the 9 cases reported by Fereiro et al.2, and 1 case reported by Imbing et al.5 occurred in patients with diabetes mellitus. Our patient was diabetic too. This condition affects the mucosa of the upper aerodigestive tract, with multiple cobblestone lesions7,10. Mucosa between these foci is normal. Occasionally, lesions may be ulcerative. When occurring on the lips and gums, these areas are sore. Lesions are well circumscribed, slightly elevated, soft oedematous masses, with red glistening surface but no ulceration. Lesions occurring on the buccal mucosa, palate, pharynx, epiglottis, and larynx, tend to be wart-like or cobblestone. Patients complain of sore mouth, sore throat, dysphonia, and difficulty in breathing, depending on the distribution of the lesion. Clinical differential diagnosis consists of extra medullary plasmacytoma, plasma cell granuloma, sarcoidosis, fungal infection, lichen planus, rhinoscleroma, RosaiDorfman disease, and Melkerson- Rosenthal syndrome2,7. Diagnosis may be obtained by finding the typical histological features, the polyclonal nature of the plasmatocyte infiltrate, and the elimination of infective agents as a cause, by the absence of fungal hyphae, absence of spirochetes on silver staining (and negative serology) and negative Warthins Starry silver stain. Plasma cell granulomas tend to be solitary and are usually located in the oral cavity or periodontal tissue. Several treatment options have been tried, including systemic, topical and intralesional steroids, removal of REFERENCES 1. WhiteJWJr,OlsenKD,BanksPM.Plasmacellorificialmucositis.Reportofacase andreviewoftheliterature.ArchDermatol1986;122:1321-4. 2. FerreiroJA,EgorshinEV,OlsenKD.Mucousmembraneplasmacytosisoftheupper aerodigestivetract.Aclinicopathologicstudy.AmJSurgPathol1994;18:1048-53. 3. ZoonJJ.Chronicbenigncircumscriptplasmocyticbalanoposthitis.Dermatologica 1952;105:1-7. 4. TimmsMS,SloanP,BalzanAP.Idiopathicplasmacytosisoftheoralandsupraglottic mucosa.JLaryngolOtol1988;102:646-8. 5. ImbingFD,AdesokanA,AdegboyegaPA.Pathologicquizcase2.Mucousmembrane plasmacytosisoftheupperaerodigestivetract.ArchOtolaryngolHeadNeckSurg 1996;122:1413-5. 6. KhanNA,MckerrowWS,PalmerTJ.Mucousmembraneplasmacytosisoftheupper aerodigestivetract.Acasereportwitheffectivetreatment.JLaryngolOtology1997; 111:293-5. 7. BhartiR,SmithDR.Mucousmembraneplasmacytosis:acasereportandreviewof theliterature.DermatolOnlineJ2003;9:15. 8. TongDC,LeaperMR,ColquhounAN,RichAM.Anunusualpresentationoforopharyngealmucosalplasmacytosisrelatedtotoothpaste.JLaryngolOtol2008;122:112-4. 9. GarzaroM,PecorariG,PezzoliM,ArrondiniM,NoveroD,NadalinJ,GiordanoC.MucousmembraneplasmacytosisofthenoseinapatientaffectedbyB-cellchronic lymphocyticleukemia.EurArchOtorhinolaryngol2009;266:16514. 10. PepperT,ShekarK,SinghM,BrennanPA.Squamouscellcarcinomaarisinginmucosalplasmacytosis.BrJOralMaxillofacSurg2010;48:208-10. 11. Δανιηλίδης Ι, Γεωργόπουλος Χ, Κωστόπουλος Ι, Σφήκας Θ. Εξωμυελικό πλασματοκύττωμα λάρυγγα-τραχείας. Παρουσίαση περισατικού. Ωτορινολαρυγγολογία-ΧειρουργικήΚεφαλής&Τραχήλου2009;35:52-4. 51
© Copyright 2026 Paperzz