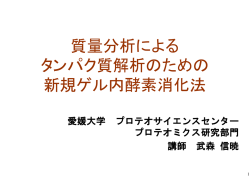
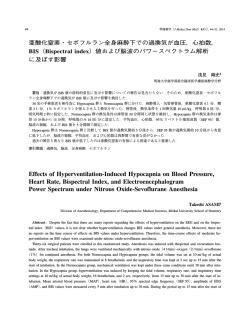
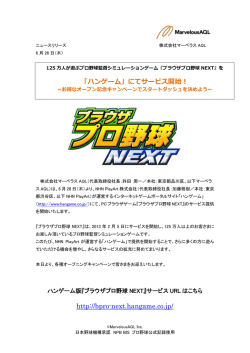
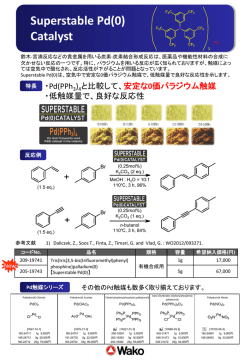
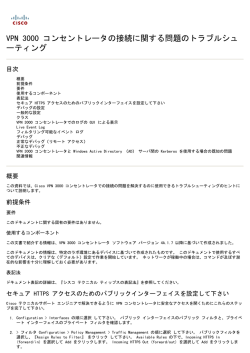
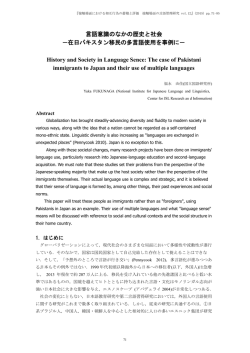
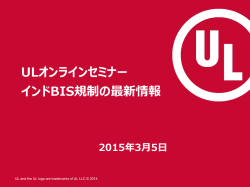
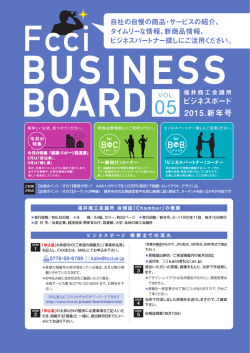
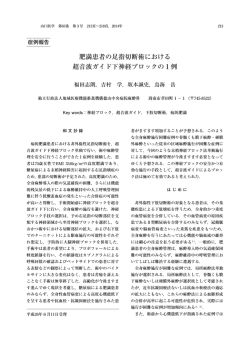
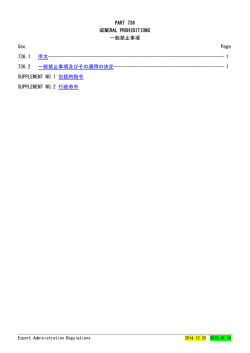
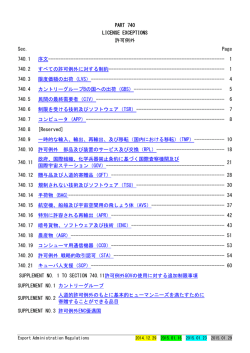
28 明海歯学(J Meikai Dent Med )43(1) , 28−33, 2014 全身麻酔下ペンタゾシン投与後の BIS(bispectral index)値変動に 及ぼすセボフルラン濃度の影響 長尾 泰好§ 明海大学歯学部総合臨床医学講座麻酔学分野 要旨:1% セボフルラン(SEV)全身麻酔下にペンタゾシン(PENT)0.6 mg/kg を静脈内投与すると BIS 値は上昇する ことが知られている.しかし,PENT 投与後の BIS 値上昇に及ぼす SEV 濃度の影響は不明である.本研究では 1% SEV もしくは 2% SEV 全身麻酔下に PENT 0.6 mg/kg を静脈内投与して BIS 値の変動を観察した. 全身麻酔で施行予定の歯科口腔外科手術症例を対象とし,1% SEV 吸入群(41 名)と 2% SEV 吸入群(24 名)の 2 群 に無作為に分けた.BIS 値は挿管 5 分後から,平均血圧と心拍数は導入前から挿管後 30 分まで 5 分間隔で測定した. 吸入 SEV 濃度と男女比を除き,2 群間で患者背景に有意差はなかった.挿管 15 分後と比較して,1% SEV 吸入群では PENT 投与後 5 分から,2% SEV 吸入群では PENT 投与後 15 分から,有意に BIS 値が上昇した. 血圧と心拍数で 2 群間に有意差がなかったため BIS 値に有意差が生じたことは循環動態の変動に起因するものでない といえる.全身麻酔下での PENT の併用は BIS を用いた麻酔深度の判定を困難にする場合があることが明らかとなった. 索引用語:BIS 値,セボフルラン,ペンタゾシン Effects of Sevoflurane Concentration on Bispectral Index after Intravenous Administration of Pentazocine Yasuyoshi NAGAO§ Division of Anesthesiology, Department of Comprehensive Medical Sciences, Meikai University School of Dentistry Abstract : It is known that intravenous administration of pentazocine at 0.6 mg/kg increases bispectral index(BIS)values under 1% sevoflurane- nitrous oxide-induced anesthesia. This mechanism is speculated to involve direct excitatory action on EEG activity in the frontal lobe. In general, it is appreciated that sevoflurane has concentration-dependent suppressive actions on the central nervous system. In contrast, sevoflurane has also been reported to have an abnormal excitatory action on EEG activity in the frontal lobe, such as epileptogenic action. Clinically, anesthesiologists can control the concentration of sevoflurane to afford theappropriate depth of anesthesia desired. However, there are no reports on the concentration-dependent effects of sevoflurane regarding the pentazocine-induced increase in BIS values. Therefore, we examined the effects of 1% and 2% sevoflurane on BIS values under general anesthesia. Patients, scheduled for elective oral surgery, were randomly assigned to one of 2 groups : 1% sevoflurane group(n=41)or 2 % sevoflurane group(n=24) . Pentazocine(0.6 mg/kg)was administered intravenously at 15 min after the intubation. Mean blood pressure(BP) , heart rate(HR) , and BIS values were recorded as baseline values under general anesthesia. These values were measured every 5 min after the intubation up to 30 min. In part of the present study, the raw EEG signal was recorded on a personal computer using Bispectrum Analyzer BIS A 2000 version software. In the 1% sevoflurane group, BIS values were significantly increased from 5 to 15 min after administration of pentazocine(p <0.01). In the 2% sevoflurane group, these values were significantly increased 15 min after administration of pentazocine(p <0.05) . On the other hand, BP and HR were not significantly changed after administration of pentazocine. BP and HR showed no significant differences between the 2 groups during the study. ペンタゾシン投与による BIS 値変動 29 The mechanism of this pentazocine-induced increase in BIS values was not due to cardiovascular suppression, because BP and HR showed no significant differences between the 2 groups during the study. Therefore, determinination of the depth of anesthesia should be assessed carefully when pentazocine is also administered, even under 2% sevoflurane anesthesia. Key words : bispectral index values, sevoflurane, pentazocine 緒 数に影響せずに BIS 値を上昇させる1−3).PENT による 言 BIS 値上昇の機序は,PENT 自身の薬理作用による大脳 脳波解析をもとに BIS(bispectral index)モニタのパ ラメータとして算出される BIS 値は麻酔深度判定に有 皮質脳波の低振幅速波化を反映したものであると考えら れる1−3). 用な指標として本邦では広く普及している.しかし,BIS SEV は一般的に濃度依存性に中枢神経系を抑制する 値の評価について不明な点が多い1−3).全身麻酔中,執 が,てんかん誘発作用もあり脳波上大脳皮質が異常な興 刀の刺激によって上昇した BIS 値はオピオイドの投与 奮を示す場合がある6, 7).臨床的には適切な SEV 濃度を によって刺激前の BIS 値に回復するが,手術刺激が加 得るために,必要に応じて濃度調節を行うが,PENT 投 わらない状態では一般にオピオイドの投与は BIS 値に 与後の BIS 値上昇に及ぼす SEV 濃度の影響は不明であ 影響を与えないと報告されている4).しかし,近年,亜 る.そこで 1%,もしくは 2% SEV 全身麻酔下に PENT 酸化窒素 SEV 全身麻酔時に PENT を静脈内投与すると 0.6 mg/kg を静脈内投与して BIS 値の変動を観察した. BIS 値は上昇することが報告されている1−3). さらに一部の症例で脳波解析を行った. 全身麻酔下にオピオイドを投与して BIS 値が変動す 方 る報告は散見される.プロポフォール麻酔下でのレミフ 法 ェンタニル投与は本研究と同様に無刺激状態で観察した 本研究は明海大学歯学部倫理委員会において承認され 場合,投与量依存性に血圧低下と心拍数減少,および BIS た(A 0906).研究内容と麻酔方法について術前患者に 値低下をきたすと報告5)されている.この機序としてレ 説明し文書で同意を得た.明海大学歯学部付属明海大学 ミフェンタニルに鎮静作用が存在する可能性があるこ 病院において予定された歯科口腔外科手術症例 65 例 と,もしくは,循環抑制に伴ってプロポフォールの鎮静 (ASA クラスⅠ)を対象とし,1% SEV 吸入群(n=41) 作用が増強されることが考えられている5).しかし,レ と 2% SEV 吸入群(n=24)の 2 群に無作為に分けた. 5) ミフェンタニルの報告 と異なり,PENT は血圧と心拍 Table 1 全症例で前投薬を施行しなかった.手術室入室後,生 Patient demographics Age(years) Weight(kg) Height(cm) Gender(M : F) Rectal temperature(℃) Expired CO2(mmHg) Pre general anesthetic HR(bpm) Pre general anesthetic mean blood pressure(mmHg) Expired nitrous oxide(%) 2% Sevoflurane group 1% Sevoflurane group p values 43.4±17.9 65.8±16.2 161.8±10.8 19 : 05 36.8±0.4 29.4±3.0 72.8±15.5 98.8±17.1 64.5±1.2 38.2±15.9 58.5±13.1 164.5±7.8 19 : 22 36.7±0.4 29.4±2.9 73.4±17.1 92.5±14.7 64.0±1.0 0.22 0.06 0.28 0.01 0.27 0.98 0.88 0.1 0.08 Data are shown as means±standard deviation. There are no significant differences between the 2 groups except of the gender ratio. M=male, F=female, HR=heart rate, bpm=beat per minutes ───────────────────────────── §別刷請求先:長尾泰好,〒350-0283 埼玉県坂戸市けやき台 1-1 明海大学歯学部臨床医学講座麻酔学分野 30 長尾泰好 明海歯学 43 体モニタ(BP-608 EvolutionII,オムロンコーリン,東 Ⓡ 2014 SEF 95 値(Fig 2) 京),BIS モニタ(model A-2000 ,Aspect Medical Sys- Bispectrum Analyzer によって 1% SEV 吸入群では 23 tems, Natick, MA, USA, an electrode BIS QuattroⓇ,Aspect 例で,2% SEV 吸入群では 13 例で 95% 端スペクトラ周 Medical Systems, Newton, MA, USA)を装着した.また, 波数(SEF 95)値を解析できた.1% SEV 吸入群では base- Bispectrum Analyzer(BSA Ver 3.22B2)を BIS モニタに line の SEF 95 値が 15.5±2.4 Hz であったのに対して,2 8) 接続し,脳波を解析した .麻酔の導入はチオペンター %SEV 吸入群では baseline の SEF 95 値が 11.4±2.4 Hz ル 6 mg/kg,ベクロニウム 0.1 mg/kg を静脈内投与して で有意に 1% SEV 吸入群の方が高かった(p<0.01) (Fig 気管挿管(挿管)を行った.全身麻酔は,1% SEV もし 2). くは 2% SEV に亜酸化窒素 4 l /分,および酸素 2 l /分 1% SEV 吸入群では,baseline(15.5±2.4 Hz)と比較 を併用して維持し,換気条件を 1 回換気量 10 ml /kg,換 して PENT 投与後 5 分から有意に SEF 95 値(18.5±3.0 気回数 12 回/分とした.体温測定は直腸温を用いて挿管 Hz)が上昇した(p<0.01).2% SEV 吸入群では,baseline 15 分後に計測した.PENT を挿管 15 分後に投与し base- (11.4±2.4 Hz)と比較して PENT 投与後 15 分で有意に line とした.データについて BIS 値は挿管 5 分後から, SEF 95 値(14.0±2.0 Hz)が上昇した(p<0.05). また平均血圧(BP)と心拍数(HR)は導入前から挿管 1% SEV 吸入群と 2% SEV 吸入群を比較すると,1% 30 分後まで 5 分間隔で測定した.その後手術を開始し SEV 吸入群の方が PENT 投与後 5, 10, 15 分で有意に た. SEF 95 値が高かった(p<0.01). データは男女比以外平均値±標準偏差で示した.統計 処理は男女比については χ 2 検定をおこなった.その他 BP および HR(Figs 3, 4) 3 群間以上は一元配置分散分析を行い,有意差があった BP および HR に関して baseline(挿管後 15 分)値は 場合 post-hoc テストとして Tukey 法を用いた.危険率 2 群間で有意差がなかった.また,2 群とも BP および 5% 未満を有意差ありとした. HR の baseline と比較して PENT 投与後有意の変動はな 結 果 男女比を除いて年齢,体重,身長,挿管 15 分後の体 温,挿管 15 分後の呼気 CO2 分圧,入室時 HR,入室時 BP,挿管 15 分後の呼気亜酸化窒素濃度に 2 群間で有意 差がなかった(Table 1).SpO2 値は酸素吸入開始から 挿管 30 分後まで 65 例とも 100% を示した. BIS 値(Fig 1) 1% SEV 吸入群では,baseline の BIS 値が 42.8±7.0 であったのに対して,2% SEV 吸入群では,baseline の BIS 値が 34.7±11.3 で有意に 1% SEV 吸入群の方が高 かった(p<0.01). 1% SEV 吸入群では,baseline(42.8±7.0)と比較し て PENT 投与 5 分後から有意に BIS 値(56.8±8.9)が 上 昇 し た (p <0.01 ). 2% SEV 吸 入 群 で は , baseline (34.7±11.3)と比較して PENT 投与 15 分後で有意に BIS 値(42.1±8.3)が上昇した(p<0.05). 1% SEV 吸入群と 2% SEV 吸入群を比較すると,1% SEV 吸入群の方が PENT 投与 5, 10, 15 分後で有意に BIS 値が高かった(p<0.01). Fig 1 Changes in bispectral index(BIS)values after intravenous administration of pentazocine(0.6 mg/kg)in patients anesthetized with(1% or 2%)sevoflurane and nitrous oxide. Fifteen minutes after the intubation, BIS was recorded as a baseline (time 0) . Pentazocine was administered at baseline on the scale. Data are presented as the means±standard deviation. **P<0.01 versus baseline values. *P<0.05 versus baseline values. ++ P<0.01 versus 2% sevoflurane group. ペンタゾシン投与による BIS 値変動 Fig 2 Changes in 95% spectral edge frequency(SEF 95)values after intravenous administration of pentazocine(0.6 mg/kg)in patients anesthetized with(1% or 2%)sevoflurane and nitrous oxide. Fifteen minutes after the intubation, SEF 95 was recorded as a baseline(time 0) . Pentazocine was administered at baseline on the scale. Data are presented as the means±standard deviation. **P<0.01 versus baseline values. *P<0.05 versus baseline values. ++ P<0.01 versus 2% sevoflurane group. 31 Fig 4 Changes in heart rate after intravenous administration of pentazocine(0.6 mg/kg)in patients anesthetized with(1% or 2 %)sevoflurane and nitrous oxide. Fifteen minutes after the intubation, heart rate was recorded as a baseline(time 0) . Pentazocine was administered at baseline on the scale. Data are presented as the means±standard deviation. bpm=beat per minutes かった.また 2 群間で BP と HR に有意差がなかった. 考 察 本研究で 1% SEV 全身麻酔下に PENT 0.6 mg/kg を静 脈内投与すると BIS 値が上昇した.このことは過去の 報告と一致する1−3).また,新しい知見として 2% SEV 全身麻酔下に PENT 0.6 mg/kg 静脈内投与すると 1% SEV 全身麻酔下と比べて程度は低いものの BIS 値は上 昇することが明らかとなった.BP と HR で 2 群間に有 意差がなかったので両群間で BIS 値に有意差が生じた ことは循環動態の変動に起因するものでないと考えられ る. 患者背景では 2% SEV 吸入群で有意に女性の割合が 低かった.過去の報告では,男女間で吸入麻酔薬の感受 性に差がある報告がある9).しかし,吸入麻酔薬の感受 性に男女差が存在する報告9)は,麻酔方法や麻酔薬使用 Fig 3 Changes in mean blood pressure after intravenous administration of pentazocine(0.6 mg/kg)in patients anesthetized with (1% or 2%)sevoflurane and nitrous oxide. Fifteen minutes after the intubation, mean blood pressure was recorded as a baseline(time 0) . Pentazocine was administered at baseline on the scale. Data are presented as the means±standard deviation. が男女で同一ではなかった.しかも著者らの過去におけ る報告では全身麻酔下 PENT 静脈内投与の BIS 値に及 ぼす影響や SEV の感受性に男女に差がなかった1).し たがって,被験者の男女比に有意差が生じても本研究の 結果に影響を与えるものとは考え難い. 32 長尾泰好 明海歯学 43 ヒトにおいて SEV は濃度依存性に BIS 値を低下させ 10, 11) 2014 値が 42.8±7.0 で,2% SEV 吸入群で BIS 値は baseline .しかし,濃度依存性の効果は 1.4% 値が 34.7±11.3 であった.BIS 値を指標にした適切な麻 以下の吸入濃度で示されるが,それ以上の高濃度では必 酔深度は 40 から 60 の範囲といわれるので,麻酔深度を る報告がある 10) ずしも濃度依存性を示さない .一方,高濃度の SEV 得るためには 1% SEV 吸入群の方が推奨される17).しか を吸入させると中枢神経系の興奮をきたし,てんかん様 し,手術侵襲による BP と HR の上昇をブロックするた 6) 脳波を呈し,BIS 値上昇を示した報告がある .また, めの SEV 濃度である MAC-BAR(minimum alveolar con- 緩徐導入法を用いて SEV を吸入させると,てんかん様 centration of an anesthetic that blocks adrenergic response to 脳波は吸入濃度依存性に出現頻度を増し,2% SEV 吸入 incision)値は,本研究で用いた亜酸化窒素濃度とほぼ でもてんかん様脳波を呈する症例がある12).本研究では 同様の 0.7 MAC 亜酸化窒素併用では 2.6 MAC である18). 1% SEV 吸 入 群 と 比 較 し て 2% SEV 吸 入 群 は 有 意 に したがって手術侵襲による BP と HR を抑制するために BIS 値が低下した.また,baseline の SEF 95 値を両群 必要とされる吸入麻酔濃度は,2% SEV 吸入群(約 1.8 間で比較すると有意に 2% SEV 吸入群の方が低く脳波 MAC)よりも高濃度の SEV 濃度が推奨される.この相 上徐波化を示した.したがって,本研究の結果によると 違について BIS 値は大脳皮質脳波を観察しているもの SEV 濃度を 1% から 2% へと上昇させても循環抑制は であり,MAC-BAR は大脳皮質より下位中枢が関与して なく,大脳皮質脳波の興奮作用も出現せず,むしろ抑制 いる脊髄反射や自律神経反射を観察したもので,それぞ 作用が発揮されていることが明らかとなった.本研究で れ機序と指標が異なるためであると考えられる.臨床的 2% SEV 濃度吸入によって大脳皮質脳波の興奮作用が出 に吸入麻酔薬のみで BIS 値や MAC-BAR 値の両者を適 現しなかった理由はおそらく麻酔導入法の違い,および 切な値にするためには無理があり19),やはり局所麻酔法 亜酸化窒素併用の有無などによるものと推測している. やオピオイド投与の併用が必要であると考えられる. 無麻酔状態や亜酸化窒素麻酔中ヒトにおいて PENT 結 (15∼30 mg でほぼ 0.3 ないし 0.6 mg/kg に相当)を静脈 内投与すると,脳波は低振幅速波化をきたすと報告13)さ れている.PENT は鎮痛作用を有し,中枢神経系の侵害 14) 論 1 )1% SEV 吸入群と 2% SEV 吸入群の間で BP と HR に有意差はなかった. 受容機構を抑制する .一方,中枢神経系に対してオピ 2 )1% SEV 吸入群と 2% SEV 吸入群の間で BIS 値と オイドは興奮作用も有する15).本研究では 1% SEV 吸入 SEF 95 値は baseline から PENT 0.6 mg/kg 静脈内投与 群 で は PENT 投 与 後 5 分 か ら ,2% SEV 吸 入 群 で は 後 15 分まで有意に 1% SEV 吸入群の方が高かった PENT 投与後 15 分で有意に baseline より SEF 95 が上昇 (p<0.01). した.すなわち PENT の大脳皮質脳波に対する興奮作 3 )1% SEV 吸入群で PENT 0.6 mg/kg 静脈内投与する 用は,2% SEV 吸入群では完全ではないもののマスクさ れることが明らかとなった. SEV の循環系への影響は被験者が 20 歳台であるが, と投与 5 分後より BIS 値は上昇する(p<0.01) . 4 )2% SEV 吸入群で PENT 0.6 mg/kg 静脈内投与する と投与 15 分後の BIS 値は上昇する(p<0.05). 覚醒時と比べて 1 minimum alveolar concentration(MAC) 5 )1% SEV 吸入群で PENT 0.6 mg/kg 静脈内投与する の SEV 濃度は HR に影響を与えないと報告されてい と投与 5 分後より SEF 95 値は上昇する(p<0.01). 16) る .本研究でも麻酔導 入 前 と baseline の HR で 1% 6 )2% SEV 吸入群で PENT 0.6 mg/kg 静脈内投与する SEV,および 2% SEV においても有意差はなかった.BP と投与 15 分後の SEF 95 値は上昇する(p<0.05). に関しては覚醒時と比べて 1 MAC の SEV 濃度吸入は 7 )1% SEV 吸入群と 2% SEV 吸入群の間で PENT 0.6 有意に低下するものの,1 MAC から 1.5 MAC に濃度を mg/kg 静脈内投与後の BIS 値と SEF 95 値は 1% SEV 上昇させても有意な低下はないと報告されている16).本 吸入群の方が有意に高かった(p<0.01). 研究でも麻酔導入前と比べて baseline は有意に BP が低 8 )上記の結果から 1% SEV 吸入群と比較すると 2% 下するものの,1% SEV 吸入群と 2% SEV 吸入群の間 SEV 吸入群は PENT 0.6 mg/kg 静脈内投与後の BIS 値 で有意差はなかった.本研究の被験者は平均 40 歳前後 の変動を抑えることが明らかとなった.また,BP と であったが,BP と HR に関してほぼ過去の報告16)と同 HR は 2 群間に有意差がなかったので両群間で BIS 値 様の結果を得た. 本研究条件では 1% SEV 吸入群で BIS 値は baseline と SEF 95 値に有意差が生じたことは循環動態の変動 に起因するものでないと考えられる. ペンタゾシン投与による BIS 値変動 9 )本研究の臨床的意義として 2% SEV 全身麻酔下で の PENT の併用は麻酔深度の判定を困難にする場合 があることが判明した. 稿を終えるに当たり,終始ご懇切なるご指導とご高閲を 賜りました総合臨床医学講座麻酔学分野教授 長坂 浩先 生に深謝いたします.また,種々の御懇切なる御教示と御 高閲を賜りました病態診断治療学講座口腔顎顔面外科学分 野教授 嶋田 淳先生に深謝いたします.さらに,御指導 と御高閲を賜りました総合臨床医学講座内科学分野教授 長谷川 彰彦先生,ならびに形態機能成育学講座生理学分 野教授 村本和世先生に深甚なる謝意を表します.さら に,脳波の解析にご指導賜りました大阪大学大学院医学系 研究科麻酔・集中治療医学講座講師 萩平 哲先生,研究 資料の収集のご協力いただきました総合臨床医学講座麻酔 学分野および埼玉医科大学病院麻酔科の諸先生に御礼申し 上げます. 引用文献 1)小貫典子,小貫和之,長尾泰好,長坂 浩,長谷川彰彦, 嶋田 淳:亜酸化窒素−セボフルラン麻酔下ペンタゾシン静 脈内投与前後の BIS 値に及ぼす性差の影響.臨床麻酔 36, 1011−1015, 2012 2)小宅宏史,小貫和之,山西優一郎,浅見剛史,小貫典子, 吉川秀明,嶋田 淳,長坂 浩:セボフルラン全身麻酔下ペ ンタゾシン静脈内投与の BIS 値に及ぼす影響について.麻 酔 60, 1128−1134, 2011 3)小貫和之,小宅宏史,山西優一郎,内田茂則,今村敏克, 塚本真規,吉川秀明,田島 徹,嶋田 淳,長谷川彰彦,長 坂 浩:亜酸化窒素・セボフルラン全身麻酔下でのペンタゾ シンが auditory evoked potential と bispectral index に及ぼす影 響.日歯麻誌 39, 628−632, 2011 4)Hagihira S, Takashima M, Mori T, Ueyama H, and Mashimo T : Electroencephalographic bicoherence is sensitive to noxious stimuli during isoflurane or sevoflurane anesthesia. Anesthesiology 100, 818−825, 2004 5)Koitabashi T, Johansen JW, and Sebel PS : Remifentanil dose/ electroencephalogram bispectral response during combined propofol/regional anesthesia. Anesth Analg 94, 1530−1533, 2002 6)Kaisti KK, Jääskeläinen SK, Rinne JO, Metsähonkala L, and Scheinin H : Epileptiform discharges during 2 MAC sevoflurane anesthesia in two healthy volunteers. Anesthesiology 91, 1952− 1955, 1999 7)Särkelä MO, Ermes MJ, van Gils MJ, Yli-Hankala AM, Jäntti VH, and Vakkuri AP : Quantification of epileptiform electroen- 33 cephalographic activity during sevoflurane mask induction. Anesthesiology 107, 928−38, 2007 8)Hagihira S, Takashima M, Mori T, Mashimo T, and Yoshiya I : Practical issues in bispectral analysis of electroencephalographic signals. Anesth Analg 93, 966−70, 2001 9)Buchanan FF, Myles PS, and Cicuttini F : Effect of patient sex on general anaesthesia and recovery. Br J Anaesth 106, 832−9, 2011 10)Katoh T, Suzuki A, and Ikeda K : Electroencephalographic derivatives as a tool for predicting the depth of sedation and anesthesia induced by sevoflurane. Anesthesiology 88, 642−650, 1998 11)Katoh T, Bito H, and Sato S : Influence of age on hypnotic requirement, bispectral index, and 95% spectral edge frequency associated with sedation induced by sevoflurane. Anesthesiology 92, 55−61, 2000 12)Julliac B, Guehl D, Chopin F, Arne P, Burbaud P, Sztark F, and Cros AM : Risk factors for the occurrence of electroencephalogram abnormalities during induction of anesthesia with sevoflurane in nonepileptic patients. Anesthesiology 106, 243−251, 2007 13)Yanagida H and Yamamura H : The electroencephalogram and the site of action of pentazocine on the brain. Can Anaesth Soc J 18, 621−630, 1971 14)長坂 浩,中村信一,松本 勲,佐藤 勲:侵害刺激とし てフォルマリンを用いての脊髄後角第五型細胞活動に及ぼす ペンタゾシンの影響−術後疼痛に関連しての考察.ペインク リニック 20, 643−649, 1999 15)Manninen PH : Opioids and seizures. Can J Anaesth 44, 463− 466, 1997 16)Malan TP, DiNardo JA, Isner RJ, Frink EJ Jr, Goldberg M, Fenster PE, Brown EA, Depa R, Hammond LC, and Mata H : Cardiovascular effects of sevoflurane compared with those of isoflurane in volunteers. Anesthesiology 83, 918−928, 1995 17)萩平 哲:脳波からみた麻酔深度.臨床麻酔 31, 325− 338, 2007 18)Nakata Y, Goto T, Ishiguro Y, Terui K, Niimi Y, and Morita S : Anesthetic doses of sevoflurane to block cardiovascular responses to incision when administered with xenon or nitrous oxide. Anesthesiology 91, 369−373, 1999 19)Daniel M, Weiskopf RB, Noorani M, and Eger EI 2nd : Fentanyl augments the blockade of the sympathetic response to incision(MAC-BAR)produced by desflurane and isoflurane : desflurane and isoflurane MAC-BAR without and with fentanyl. Anesthesiology 88, 43−49, 1998 (受付日:2013 年 10 月 23 日 受理日:2013 年 11 月 27 日)
© Copyright 2026 Paperzz