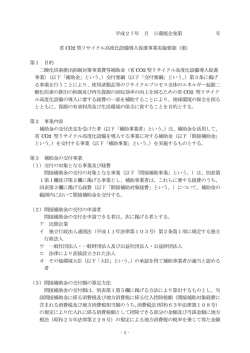
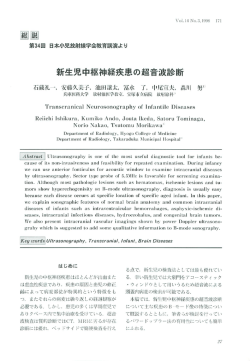
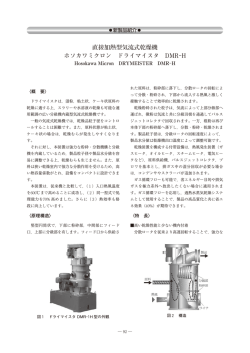
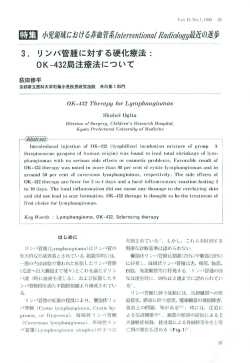
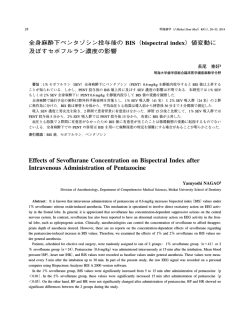
44 明海歯学(J Meikai Dent Med )43(1) , 44−51, 2014 亜酸化窒素・セボフルラン全身麻酔下での過換気が血圧,心拍数, BIS(Bispectral index)値および脳波のパワースペクトラム解析 に及ぼす影響 浅見 剛史§ 明海大学歯学部総合臨床医学講座麻酔学分野 要旨:過換気が BIS 値の経時的変化に及ぼす影響についての報告は見当たらない.そのため,亜酸化窒素・セボフル ラン全身麻酔下での過換気が BIS 値に及ぼす影響を検討した. 36 名の手術患者を無作為に Hypocapnia 群と Normocapnia 群に分けた.麻酔導入・気管挿管後,亜酸化窒素 4 l /分,酸 素 2 l /分,1% セボフルランを吸入させ人工換気を行った.挿管後,換気条件を 1 回換気量 10 ml /kg,呼吸数 8 回/分, 吸気時間 2 秒に設定した.Normocapnia 群の換気条件は挿管後 30 分間同じ状態を維持し,Hypocapnia 群の換気条件は挿 管 15 分後から 15 分間,呼吸数のみ 16 回/分に設定した.平均血圧,心拍数,95% スペクトル端周波数(SEF 95)値, 脳波の振幅,および BIS 値を 5 分間隔で測定した. Hypocapnia 群は Normocapnia 群と比較して BIS 値が過換気開始 5 分後から,SEF 95 値が過換気開始 10 分後から有意 に低下したが,脳波の振幅,平均血圧,および心拍数は両群間で有意な差がなかった. 過去の報告と異なり BIS 値が低下したのは亜酸化窒素の有無による相違であると推測した. 索引用語:過換気,脳波,全身麻酔,セボフルラン Effects of Hyperventilation-Induced Hypocapnia on Blood Pressure, Heart Rate, Bispectral Index, and Electroencephalogram Power Spectrum under Nitrous Oxide-Sevoflurane Anesthesia Takeshi ASAMI§ Division of Anesthesiology, Department of Comprehensive Medical Sciences, Meikai University School of Dentistry Abstract : Despite the fact that there are many reports regarding the effects of hyperventilation on the EEG and on the bispectral index(BIS)values, it is not clear whether hyperventilation changes BIS values under general anesthesia. Moreover, there are no reports on the time course of effects on BIS values under hyperventilation. Therefore, the time-course effects of moderate hyperventilation on BIS values were examined under nitrous oxide-sevoflurane anesthesia. Thirty-six surgical patients were enrolled in this randomized study. Anesthesia was induced with thiopental and vecuronium bromide. After tracheal intubation, the lungs were ventilated mechanically with nitrous oxide(4 l /min) -oxygen(2 l /min) -sevoflurane (1%)for continued anesthesia. For both Normocapnia and Hypocapnea groups, the tidal volume was set at 10 ml /kg of actual body weight, the respiratory rate was maintained at 8 breaths/min, and the inspiratory time was kept at 2 sec up to 15 min after the start of intubation. In the Normocapnia group, mechanical ventilation was kept under these same conditions until 30 min after intubation. In the Hypocapnia group, hyperventilation was induced by keeping the tidal volume, respiratory rate, and inspiratory time settings at 10 ml /kg of actual body weight, 16 breaths/min, and 2 sec, respectively, from 15 min up to 30 min after the start of intubation. Mean arterial blood pressure(MAP), heart rate(HR), 95% spectral edge frequency(SEF 95), amplitude of EEG (AMP) , and BIS values were measured every 5 min after intubation up to 30 min. During the period up to 15 min after the start of 全身麻酔下の過換気が BIS 値に及ぼす影響 45 intubation, the data were recorded as baseline values. In our present results, the mean Pa CO2 value with hyperventilation was 28.5 mmHg at 15 min of intubation in contrast to the value of 38.1 mmHg for the normocapnia group. BIS values in the Hypocapnia group were significantly lower than those in the Normocapnia group at 5 to 15 min after baseline. SEF 95 in the Hypocapnia group was significantly lower compared with that for the Normocapnia group at 10 and 15 min after baseline. In the former group BIS and SEF 95 values decreased and AMP increased, but not significantly, with hyperventilation compared with those values for the Normocapnia group. However, hyperventilation-induced hypocapnia did not affect either the MAP or HR. We speculate that the presence or absence of nitrous oxide may account for the difference in findings among previous reports. Key words : hyperventilation, EEG, general anesthesia, sevoflurane 緒 多く,過換気の BIS 値と循環動態に及ぼす影響を同時 言 に観察し,しかも時間経過の検討はなされてない.その 周術期の過換気は脳圧の軽減を目的として脳神経外科 ため,本研究は 1% セボフルラン全身麻酔下歯科口腔外 手術でしばしば行われる1).また,過換気症候群は歯科 科症例患者における過換気の血圧と心拍数,および BIS 2) 診療時の偶発症として周知のとおりである . 値に及ぼす影響を時間経過とともに観察し検討した. 全身麻酔中の過換気が脳波に影響を与えることはよく 対象と方法 知られている1, 3).また,脳波解析をもとに BIS(Bispectral Index)モニターのパラメータとして算出された BIS 値 は麻酔深度判定に有用な指標として本邦では広く普及し 本研究は明海大学歯学部倫理委員会において承認され た「A 0906」. ている4−6).しかし,過換気の脳波に及ぼす影響につい ての研究は比較的多いにもかかわらず全身麻酔中の過換 対象 気が BIS 値に及ぼす影響は不明な点が多い.過換気は 研究内容と麻酔方法について術前患者に説明し書面で 分時換気量が増すとともに動脈血 CO2 分圧(Pa CO2 )低 承諾を得た歯科口腔外科患者 36 名(ASA クラスⅠ)を 下をきたす7)が,セボフルラン全身麻酔では過換気によ 対象とした. って Pa CO2 が 24 mmHg 前後になると Normocapnia の状 態と比べて BIS 値が有意に低下する報告がある3).一 方,セボフルラン全身麻酔下でも過換気によって呼気終 投与方法 前投薬を施行せず,手術当日 0 時から絶飲食とした. 末 CO2 分圧(PETCO2)が 28 mmHg 前後の Hypocapnia の 手術室入室後,自動血圧計,心電計,パルスオキシメー 状態では BIS 値が有意に低下しない報告もある1).さら タ(BP-608 EvolutionⅡⓇ ,オムロンコーリン,愛知), に,プロポフォール全身麻酔下では PETCO2 が 22.5−30 および BIS モニター(model A-2000Ⓡ ,Aspect Medical mmHg の過換気で有意に BIS 値の低下が観察されない Systems, Natick, MA, USA, an electrode BIS QuatroTM, 報告もある.したがって,換気条件や麻酔薬によって BIS Aspect Medical Systems, Newton, MA, USA)を装着し 値の変動が異なることが推測される. た.また,Bispectrum Analyzer5)を BIS モニターに接続 過換気の血圧および心拍数に及ぼす影響は Pa CO2 低 7) し,脳波を解析した.血圧を連続 3 回測定後,ベクロニ 下 の程度もしくは胸腔内圧上昇の程度にかかわらず有 ウム臭化物 0.1 mg/ kg と チ オ ペ ン タ ー ル ナ ト リ ウ ム 意の血圧および心拍数の変動はないとの報告がある8). (Thi)6 mg/kg を静脈内投与して気管挿管を行った.全 一方,過換気は血圧低下をきたすとする報告があり,全 身麻酔は呼気 CO2 濃度をモニターし,1% セボフルラ 身麻酔導入後の過換気ではしばしば重篤な血圧低下をき ン,亜酸化窒素 4 l /分,酸素 2 l /分で維持し,以下に述 たす恐れがある7, 9). べる換気モードで調節呼吸(アコマ人工呼吸器 PRO-55 や過換気 VⓇ,アコマ医科工業,東京)を行った.平均血圧,心 は散見されるが不明な点が 拍数,BIS 値,脳波の振幅,および 95% スペクトル端 1, 3) このように過換気の BIS 値に関する研究 7−10) の循環動態に及ぼす研究 ───────────────────────────── §別刷請求先:浅見剛史,〒350-0283 埼玉県坂戸市けやき台 1-1 明海大学歯学部臨床医学講座麻酔学分野 周波数(SEF 95)値測定は 5 分間隔で行った.体温は直 腸温から得た.輸液は乳酸リンゲル液を 10 ml /kg/時の 46 浅見剛史 明海歯学 43 速度で投与した. Table 1 Patients demographics. 測定方法 患者は 1% セボフルラン濃度で Normocapnia 群と Hypocapnia 群の 2 群に無作為に分けた.baseline は気管挿 管後 15 分とし,Hypocapnia 群では過換気を開始した. Normocapnia 群は換気条件を 1 回換気量 10 ml /kg,換 2014 Number Male : Female Age(yr) Height(cm) Weight(kg) Hypocapnia group Normocapnia group 18 8 : 10 40.3±21.9 161.8±12.9 53.6±14.6 18 7 : 11 40.1±17.9 158.3±7.1 59.3±15.3 気回数 8 回/分の呼気終末ゼロ圧(Zero End Expiratory Pressure ; ZEEP)を気管挿管後 30 分まで行なった. Data are presented as the means ± standard deviation, or as actual numbers, where appropriate. Hypocapnia 群は,換気条件を気管挿管後 15 分まで 1 回換気量 10 ml /kg,換気回数 8 回/分の ZEEP で行い, 気管挿管 15 分後以降は換気条件を 1 回換気量 10 ml /kg, 換気回数 16 回/分の ZEEP とした. Table 2 Body temperature, blood gas analysis, and expired gas analysis during hypocapnia and normocapnia at baseline. I/E 比は,2 群とも 1/2 とした. 血液ガス分析は Normocapnia 群で気管挿管 30 分後 に,Hypocapnia 群で気管挿管 15 分後と気管挿管 30 分 後に足背動脈から採血を行った. データは,気管挿管後 30 分までを採用し,その後, 術野の消毒を行って外科手術を開始した. 統計処理 データを男女比以外平均値±標準偏差(SD)で示し た.2 群間の比較では unpaired t test を行った.3 群間以 Rectal temperature(℃) Pa CO2(mmHg) pH Sevoflurane concentration(%) N2O concentration(%) Expired CO2 tension(mmHg) Hypocapnia group Normocapnia group 36.6±0.5 39.1±4.2 7.42±0.03 0.91±0.04 62.6±2.3 35.8±3.5 36.9±0.3 no sample no sample 0.89±0.04 65.0±1.8 37.9±3.7 Data are presented as the means±standard deviation, where appropriate. N2O=nitrous oxide 上の比較は二元分散分析を行い,有意差があった場合 F-PLSD( Fisher’s Protected Least Significant Difference) 法を用いた.危険率 5% 未満を有意差ありとした. 結 果 Hypocapnia 群と Normocapnia 群間の患者背景の比較 男女比,年齢,身長,体重は 2 群間で有意差がなかっ た(Table 1). 気管挿管 15 分後(baseline)の Hypocapnia 群と Normocapnia 群間の比較 気管挿管 15 分後(baseline)の体温,呼気セボフルラ ン濃度,呼気亜酸化窒素濃度,呼気 CO2 分圧は 2 群間 で有意差がなかった(Table 2). BIS 値(Fig 1),SEF 95 値(Fig 2),脳波の振幅(Fig 3),血圧(Fig 4),および心拍数(Fig 5)に両群間で有 意差がなかった. Baseline 15 分後の Hypocapnia 群と Normocapnia 群間 の比較 呼気セボフルラン濃度,呼気亜酸化窒素濃度は 2 群間 Fig 1 Changes in the bispectral index with hyperventilation in patients anesthetized with sevoflurane and nitrous oxide. Fifteen minutes after the intubation, the data was recorded as a baseline. The time at start of hyperventilation was indicated as a baseline on the scale. *P<0.05 versus the Normocapnia group. 全身麻酔下の過換気が BIS 値に及ぼす影響 47 Fig 2 Changes in the SEF 95 with hyperventilation in patients anesthetized with sevoflurane and nitrous oxide. Fifteen minutes after the intubation, the data was recorded as a baseline. The time at start of hyperventilation was indicated as a baseline on the scale. *P<0.05 versus the Normocapnia group. Fig 4 Changes in mean blood pressure with hyperventilation in patients anesthetized with sevoflurane and nitrous oxide. Pregeneral anesth, before induction of general anesthesia ; bpm, beats per minutes. Fifteen minutes after the intubation, the data was recorded as a baseline. The time at start of hyperventilation was indicated as a baseline on the scale. Fig 3 Changes in the amplitude of EEG with hyperventilation in patients anesthetized with sevoflurane and nitrous oxide. Fifteen minutes after the intubation, the data was recorded as a baseline. The time at start of hyperventilation was indicated as a baseline on the scale. Fig 5 Changes in heart rate with hyperventilation in patients anesthetized with sevoflurane and nitrous oxide. Pre-general anesth, before induction of general anesthesia ; bpm, beats per minutes. Fifteen minutes after the intubation, the data was recorded as a baseline. The time at start of hyperventilation was indicated as a baseline on the scale. で有意差はなかった.Hypocapnia 群では baseline 15 分 は 7.53±0.04 を示し,Normocapnia 群より有意に上昇し 後(過換気開始 15 分後)に Pa CO2 28.5±4.1 mmHg,呼 た(Table 3). 気 CO2 分圧 24.8±3.4 mmHg を示し,Normocapnia 群よ BIS 値(Fig 1)と SEF 95 値(Fig 2)は Normocapnia りも有意に低下した.pH に関しては Hypocapnia 群で 群よりも Hypocapnia 群の方が有意に低かった.脳波の 48 浅見剛史 明海歯学 43 2014 Table 3 Blood gas analysis and expired gas analysis during hypocapnia and normocapnia at 15 min from baseline. Pa CO2(mmHg) pH Sevoflurane concentration(%) N2O concentration(%) Expired CO2 tension(mmHg) Hypocapnia group Normocapnia group 28.5±4.1* 7.53±0.04* 0.92±0.04 64.1±1.4 24.8±3.4* 38.1±3.4 7.43±0.03 0.90±0.01 65.5±1.6 37.6±3.7 Data are presented as the means±standard deviation, where appropriate. N2O=nitrous oxide *P<0.05 compared to normocapnia group 振幅(Fig 3),血圧(Fig 4),および心拍数(Fig 5)に 両群間で有意差がなかった(Figs 3, 4, 5). また,SpO2 値は酸素吸入開始から挿管 30 分後まで 36 例とも 100% を示した. BIS 値(Fig 1) Normocapnia 群は baseline 値と比較して baseline 15 分 後(過換気開始 15 分後)の値まで有意の変動がなく,45 前後の BIS 値を保った.Hypocapnia 群は baseline 5 分後 (過換気開始 5 分後)から 15 分後(過換気開始 15 分後) まで 36 前後と有意に Normocapnia 群よりも低かった. SEF 95 値(Fig 2) Normocapnia 群は baseline 値と比較して baseline 15 分 後(過換気開始 15 分後)の値まで有意の変動がなく,15 Fig 6 Representative raw EEG wave and corresponding power spectra before and after hyperventilation-induced hypocapnia in a patient anesthetized with sevoflurane and nitrous oxide. (A)Raw EEG wave before hyperventilation-induced hypocapnia at baseline : BIS, 48.6 ; amplitude, 14.0 μ V ; 95% spectral edge frequency, 15.2 Hz. (B)Raw EEG wave 5 min after hyperventilation-induced hypocapnia : BIS, 33.8 ; amplitude, 14.3 μ V, 95% spectral edge frequency, 12.8 Hz. (C)Representative corresponding power spectra from normocapnia and hypocapnia. Hyperventilation-induced hypocapnia causes a prominent increase in the lower frequency area of the power spectrum. Hz 前後の SEF 95 値を保った.Hypocapnia 群は baseline 10 分後(過換気開始 10 分後)に 14 Hz, 15 分後(過換 気開始 15 分後)に 13 Hz と有意に Normocapnia 群より 気開始 15 分後)の値まで有意の変動を血圧(Fig 4)お も低かった. よび心拍数(Fig 5)共示さず,両群間で差がなかった. 脳波の振幅(Fig 3) 脳波の波形およびパワースペクトラムの 1 例(Fig 6) Normocapnia 群は baseline 値と比較して baseline 15 分 Fig 6 での A は気管挿管後 15 分(baseline)の脳波で 後(過換気開始 15 分後)の値まで有意の変動がなく,13 BIS 値 48.6,脳波の振幅 14.0 幅 n, SEF 95 値は 15.2 Hz μ V 前後を保った.Hypocapnia 群は baseline 10 分後(過 換気開始 10 分後)に 14 μ V まで増加したが,共に統計 的に有意な変動を示さなかった. であり,B は baseline 5 分後(過換気開始 5 分後)の脳 波で BIS 値 33.8 ,脳波の振幅 14.3 幅 n, SEF 95 値 は 12.8 Hz であった. 過換気による Hypocapnia によって,低周波領域のパ 平均血圧および心拍数(Figs 4, 5) Normocapnia 群と Hypocapnia 群は麻酔前値と比較し て baseline 値が血圧および心拍数共に有意に低下した (p<0.05).baseline 値と比較して baseline 15 分後(過換 ワーは増加し,また 35 Hz 以上の高周波領域のパワー の増加も見られた. 全身麻酔下の過換気が BIS 値に及ぼす影響 考 49 数を示し,脳波の徐波化の指標となる.さらに Hayashi 察 ら3)の報告では過換気による血圧および心拍数について 呼気終末二酸化炭素分圧(PETCO2)と Pa CO2 の計測値に 検討していないが,本研究で得た結果から過換気によっ 与える影響について て血圧および心拍数は変動しないので BIS 値の変動や 本研究ではカプノメータで呼気 CO2 分圧を測定した. PETCO2 は非侵襲的非観血的,および持続的に測定した Pa CO2 値として臨床では用いられるが,PETCO2 と Pa CO2 11) 脳波の徐波化は血圧および心拍数の変動によるものでな いことが明らかとなった. 全身麻酔下で脳波の徐波化は baseline 10 分後(過換 は必ずしも一致しない .PETCO2 は呼気終末 CO2 分圧で 気開始 10 分後)から,また BIS 値の低下は baseline 5 あり,Pa CO2 は動脈血 CO2 分圧である.PETCO2 と Pa CO2 分後(過換気開始 5 分後)から観察された.無麻酔のヒ の差は Pa-ETCO2 と言われ,高齢者,喫煙者,ASA 分類 トでは 3 分間の過換気で脳波の変化が観察される15, 16). 11) のリスクが大きい患者で Pa-ETCO2 の値が大きくなる . 過換気による脳波の変化の機序は過換気によって脳血流 また,換気は可能であるが,ガス交換のための血流が乏 が低下し脳の低酸素をきたすこと,もしくは pH 上昇に しい状態である死腔効果や換気が血流に対して小さくな よる脳代謝の変化などそれ以外の因子による2, 17)可能性 るシャント効果によって Pa-ETCO2 の値が大きくなる.一 が報告されている.無麻酔下と比べて全身麻酔下で脳波 方,換気回数が一定で一回換気量を増すと Pa-ETCO2 の値 の変化の発現が遅くなる理由は不明であるがおそらく全 11) は小さくなる .Pa-ETCO2 の値に関する報告は術中仰臥 身麻酔薬によって上記の因子の発現が遅延すると推測し 位 7.2 mmHg12),術中仰臥位で 6 mmHg13),全身麻酔下の ている. 14) 健康な仰臥位被験者で 6 mmHg 程度 である.本研究で Schlünzen ら1)は 1 MAC(最小肺胞内濃度;Minimum は,呼気二酸化炭素曲線でプラトーが形成されて測定し Alveolar Concentration)セボフルラン全身麻酔下で PETCO2 ているので PETCO2 と置き換えることもできる.しかし, が 28 mmHg では Normocapnia と比べて有意の BIS 値変 上記の報告と比較して本研究で得た Pa-ETCO2 値は 4 ない 動がなかったことを報告している.Schlünzen ら1)の麻酔 し 1 mmHg と小さかった.これは本研究での症例の場 方法と比較して Hayashi ら3)は 1.5% セボフルランでほ 合,手術侵襲がなく,患者の全身状態が良好なためであ ぼ 同 様 の 全 身 麻 酔 薬 で 維 持 し て い る が , Pa CO2 が 24 11) mmHg で Schlünzen ら1)よりも過換気の程度が大きい状 ると考えられる . 態で BIS 値の低下を報告している.本研究の結果は亜 全身麻酔下における過換気による脳波および BIS 値の 酸化窒素・1% セボフルラン全身麻酔下で PETCO2 が 25 変動 mmHg で有意の BIS 値の低下を観察した(Fig 1).BIS 本研究から Pa CO2 が 39.1 mmHg から 28.5 mmHg に低 値の結果について Schlünzen ら1)の報告と本研究で得た 下する程度の過換気において全身麻酔下で baseline 10 結果の違いは,麻酔条件の違いと推測している.すなわ 分後(過換気開始後 10 分後)から脳波は SEF 95 値が ち,亜酸化窒素,セボフルラン濃度,および PETCO2 の 低下し,有意に徐波化を示すことがわかった.しかし, 影響の有無が考えられる.亜酸化窒素を併用した全身麻 脳波の振幅については有意の低下が観察されなかった. 酔下に過換気を加えると麻酔深度が深くなることは古く また,BIS 値は baseline の 5 分後(過換気開始後 5 分 からよく知られている18, 19).過換気の脳波に及ぼす影響 後)から有意の低下を示した.Schlünzen ら1)の報告では を見てみる2)と,ヒト無麻酔下でも PETCO2 が 22.5 mmHg PETCO2 が 28 mmHg 前後で BIS 値は有意の低下を示さな から 15 mmHg では脳波は徐波化し α 波が減少すると 3) かったが,Hayashi ら の報告では Pa CO2 が 24 mmHg 前 報告されている. 後で BIS 値の低下を示したとしている.本研究で得た また,PETCO2 は 30 mmHg ないし 22.5 mmHg の過換気 結果は Hayashi らの3)結果を支持するものである.しか でも程度は軽減されるが同様の脳波変化の見られる報告 し,Hayashi ら3),および Schlünzen ら1)の報告では過換 がある.しかし,ハロタン単独の全身麻酔下では Normo- 気の時間経過に関して検討していない.また,Hayashi capnia か ら 過 換 気 に よ っ て Pa CO2 が 15 mmHg の Hy- 3) ら の報告では SEF 95 値が本研究で得た結果と同様に pocapnia に低下しても麻酔薬の強さの指標である MAC 有意に低下するが,脳波の振幅は本研究と異なり有意に に変化がないと報告されている20).また,ネコの研究で 増加したと報告している.SEF 95 値とは,0 から 30 Hz は亜酸化窒素・全身麻酔下で過換気により脊髄後角細胞 までのパワースペクトラムの面積を 95 : 5 に分ける周波 活動の抑制が促進される報告がある21).さらに,無麻酔 50 浅見剛史 明海歯学 43 2014 下過換気で末梢神経への電気刺激を用いて体性感覚刺激 究と同程度の過換気は有意の血圧変動をきたさないこと による脳波誘発反応に関して亜酸化窒素を併用すると誘 を報告した.従って,本研究の結果は過去の報告29)を支 1) 発反応の抑制は増強される.従って,Schlünzen ら の研 究と異なり本研究条件では亜酸化窒素を併用したため, 過換気によって脳波が徐波化して BIS 値が低下した可 持する結果である. 結 論 能性がある.本研究開始にあたっての予備研究で亜酸化 本研究において,亜酸化窒素・セボフルラン全身麻酔 窒素を除いて 1% セボフルラン麻酔のみで過換気を行っ 下での過換気の及ぼす脳波への影響に関する経時的変化 たところ PETCO2 が 24 mmHg の条件で BIS 値は 47 から について以下のことが示唆された. 49 と変動が観察されなかった結果を得ている.Schlünzen 1 )過換気における BIS 値や脳波パワースペクトラム 1) ら の BIS 値が 40 前後であったのは,セボフルラン濃 解析の経時的変化として Normocapnia 群に比べ Hy- 度の違いと考えられる.また,プロポフォール全身麻酔 pocapnia 群では BIS 値,SEF 95 が低下した.脳波は 下では PETCO2 が 22.5−30 mmHg の過換気で有意の BIS 高振幅化を示したが有意差はなかった. 値低下が観察されない報告もある.したがって,麻酔薬 2 )本研究において過換気による循環動態の変動はな によって,BIS 値の変動の程度が異なることがわかる. く,亜酸化窒素・セボフルラン全身麻酔下での過換気 Fig 6 に示すように過換気によって δ や θ 波のよう による BIS 値の変動や脳波の変化は血圧および心拍 な低周波数領域のパワーの増加のみならず β 波のよう 数の影響によるものでないことが明らかとなった. な高周波領域のパワーも増加した.Hayashi ら3)の報告 以上の結果は,全身麻酔中の過換気によっておこる引 ではセボフルラン全身麻酔では低周波数領域のパワーの き起こされる深麻酔や覚醒遅延などのリスク増大にも関 増加のみで高周波領域のパワーは増加していない.Hay- 与すると考えられ,臨床的にも意義深い結果となる. 3) ashi ら の報告は 1.5% セボフルラン全身麻酔下での過 換気であるが,本研究での麻酔条件は 1% セボフルラン に亜酸化窒素の併用のもとでの過換気である. 亜酸化窒素全身麻酔の存在下での過換気の脳波に及ぼ す影響に関する研究では過換気によって δ 波, θ 波, α 波,および β 波の周波数領域のパワーの増加が報告 されている22).また,Yamamura ら23)の研究では 50 ない し 70% 亜酸化窒素吸入により脳波のパワースペクトラ ムで 35 Hz 付近のパワーの増加が報告されている.した がって,Hayashi ら3)の報告と若干異なった理由は,亜 酸化窒素の有無による違いと推測している. 亜酸化窒素の BIS 値に及ぼす影響は,Normocapnia の 状態で BIS 値に影響を与えない24),もしくは BIS 値を 低下する25)との報告があり意見の一致が見られていな い.今回の研究では全症例に亜酸化窒素を併用している ので亜酸化窒素の BIS 値に及ぼす影響は不明である. 全身麻酔下における過換気による血圧および心拍数の変 動 本研究の麻酔条件では過換気によって血圧および心拍 数は有意に変動しないことが明らかとなった.無麻酔状 態のヒトで過換気は末梢の血管を拡張させ低血圧をきた すが26),全身麻酔下での過換気は,心拍出量を減少さ せ,高頻度に血圧を低下させる27, 28)との報告がある.一 方,著者ら29)は 2% セボフルランであるが,過去に本研 稿を終えるに当たり,終始ご懇切なるご指導とご高閲を 賜りました本学大学院歯学研究科機能系薬理研究群 長坂 浩教授に深謝いたします.また,種々の御懇切なる御教 示と御高閲を賜りました本学大学院歯学研究科形態系病態 形態研究群 嶋田 淳教授に深謝いたします.さらに,御 指導と御高閲を賜りました本学大学院歯学研究科機能系正 常機能研究群 村本和世教授,ならびに本学大学院歯学研 究科機能系病態機能研究群 町野 守教授に深甚なる謝意 を表します.さらに,脳波の解析にご指導賜りました大阪 大学大学院医学系研究科麻酔・集中治療医学講座 萩平 哲講師,研究資料の収集のご協力いただきました総合臨床 医学講座麻酔学分野および埼玉医科大学病院麻酔科の諸先 生に御礼申し上げます. 引用文献 1)Schlünzen L, Vafaee MS, Juul N and Cold GE : Regional cerebral blood flow responses to hyperventilation during sevoflurane anaesthesia studied with PET. Acta Anaesthesiol Scand 54, 610−615, 2010 2)Van der Worp HB, Kraaier V, Wieneke GH and Van Huffelen AC : Quantitative EEG during progressive hypocarbia and hypoxia. Hyperventilation-induced EEG changes reconsidered. Electroencephalogr Clin Neurophysiol 79, 335−341, 1991 3) Hayashi K, Fujikawa M and Sawa T : Hyperventilationinduced hypocapnia changes the pattern of electroencephalographic bicoherence growth during sevoflurane anaesthesia. Br J Anaesth 101, 666−672, 2008 4)Guignard B, Menigaux C, Dupont X, Fletcher D and Chauvin M : The effect of remifentanil on the bispectral index changes and hemodynamic responses after orotracheal intubation. Anesth 全身麻酔下の過換気が BIS 値に及ぼす影響 Analg 90, 161−167, 2000 5)Hagihira S, Takashima M, Mori T, Ueyama H and Mashimo T : Electroencephalographic bicoherence is sensitive to noxious stimuli during isoflurane or sevoflurane anesthesia. Anesthesiology 100, 818−825, 2004 6)Lefoll-Masson C, Fermanian C, Aime I, Verroust N, Taylor G, Laloe P-A, Liu N, Aegerter P and Fischler M : The comparability of bispectral index and state entropy index during maintenance of sufentanil-sevoflurane-nitrous oxide anesthesia. Anesth Analg 105, 1319−1325, 2007 7)Prys-Roberts C, Kelman G R, Greenbaum R and Robinson R H : Circulatory influences of artificial ventilation during nitrous oxide anaesthesia in man II results : the relative influence of mean intrathoracic pressure and arterial carbon dioxide tension. Br J Anaesth 39, 533−548, 1967 8) Theye RA, Milde JH and Michenfelder JD : Effect of hypocapnia on cardiac output during anesthesia. Anesthesiology 27, 778−782, 1966 9)Stoddart JC : Electroencephalographic activity during voluntarily controlled alveolar hyperventilation. Br J Anaesth 39, 2−10, 1967 10)Ketty SS and Schmidt CF : The effects of active and passive hyperventilation on cerebral blood flow, cerebral oxygen consumption, cardiac output, and blood pressure of normal young men. J Clin Invest 25, 107−119, 1946 11)Wahba RW and Tessler MJ : Misleading end-tidal CO2 tensions. Can J Anaesth 43, 862−866, 1996 12)Russel GB and Graybeal JM : The arterial to end-tidal carbon dioxide difference in neurosurgical patients during craniotomy. Anesth Analg 81, 806−810, 1995 13)Grenier B, Verchère E, Mesli A, Dubreuil M, Siao D, Vandendriessche M, Calès J and Maurette P : Capnography monitoring during neurosurgery : reliability in relation to various intraoperative positions, Anesth Analg 88, 43−48, 1999 14)Askrog V : Changes in(a−A)CO2 difference and pulmonary artery pressure in anesthetized man. J Appl Physiol 21, 1299− 1305, 1966 15)Kennealy JA, Penovich PE and Moore-Nease SE : EEG and spectral analysis in acute hyperventilation. Electroencephalogr Clin Neurophysiol 63, 98−106, 1986 16)Burykh EA : Interaction of hypocapnia, hypoxia, brain blood flow, and brain electrical activity in voluntary hyperventilation in humans. Neurosci Behav Physiol 38, 647−659, 2008 17)Patel VM and Maulsby RL : How hyperventilation alters the 51 electroencephalogram : a review of controversial viewpoints emphasizing neurophysiological mechanisms. J Clinical Neuropysiology 4, 101−120, 1987 18)Geddes Ic and Gray Tc : Hyperventilation for the maintenance of anaesthesia. Lancet 2, 4−6, 1959 19)Matsuda I, Tachibana N and Yamamura H : Effect of nitrous oxide and hyperventilation on the cerebral evoked response. Masui 22, 50−58, 1973 20)Eisele JH, Eger EI 2nd and Muallem M : Narcotic properties of carbon dioxide in the dog. Anesthesiology 28, 856−865, 1967 21)Kitahata LM, Taub A and Sato I : Lamina-specific suppression of dorsal horn unit activity by nitrous oxide and by hyperventilation. J Pharmacol Exp Ther 176, 101−108, 1971 22)Kalkman CJ, Boezeman EH, Ribberink AA, Oosting J, Deen L and Bovill JG : Influence of changes in arterial carbon dioxide tension on the electroencephalogram and posterior tibial nerve somatosensory cortical evoked potentials during alfentanil / nitrous oxide anesthesia. Anesthesiology 75, 68−74, 1991 23)Yamamura T, Fukuda M, Takeya H, Goto Y and Furukawa K : Fast oscillatory EEG activity induced by analgesic concentrations of nitrous oxide in man. Anesth Analg. 60, 283−291, 1981 24)Rampil IJ, Kim JS, Lenhardt R, Negishi C and Sessler DI : Bispectral EEG index during nitrous oxide administration. Anesthesiology 89, 671−677, 1998 25) Hans P, Bonhomme V, Benmansour H, Dewandre PY, Brichant JF and Lamy M : Effect of nitrous oxide on the bispectral index and the 95% spectral edge frequency of the electroencephalogram during surgery. Anaesthesia 56, 999−1002, 2001 26)Burnum JF, Hickam JB and McIntosh HD : The effect of hypocapnia on arterial blood pressure. Circulation 9, 89−95, 1954 27) Theye RA, Milde JH and Michenfelder JD : Effect of hypocapnia on cardiac output during anesthesia. Anesthesiology 27, 778−782, 1966 28)Prys-Roberts C, Kelman GR, Greenbaum R and Robinson RH : Circulatory influences of artificial ventilation during nitrous oxide anaesthesia in man. II. Results : the relative influence of mean intrathoracic pressure and arterial carbon dioxide tension. Br J Anaesth 39, 533−548, 1967 29)浅見剛史,大木良蔵,宮澤有美子,小貫和之,内田茂則, 竹内菊子,小宅宏史,長谷川彰彦,長坂 浩:セボフルラン 全身麻酔下での間欠的陽圧換気条件が血圧・動脈血ガス分析 に及ぼす影響について.明海歯科医学 38, 128−132, 2009 (受付日:2013 年 10 月 28 日 受理日:2013 年 11 月 27 日)
© Copyright 2026 Paperzz