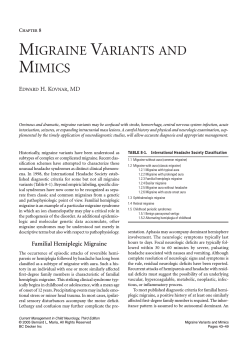
01_News_PM_0414_rt.qxp:01_PM_0414 14/04/2014 10:59 Page 1 £7.50 www.pharmacymag.co.uk Volume 20 – No 4 April 2014 The Big Debate Headache & migraine Animal health Sport & fitness Should pharmacy be stocking e-cigarettes? Page 26 Giving migraine sufferers the right therapy and advice Page 29 What to do when bunny gets the bugs... Page 33 Avoiding, managing and treating injuries Page 36 Promoting physical activity and exercise See page 17 Winner: Best Monthly Title 2013 Avicenna Media Awards Give us a better system Good community pharmacy practice is breaking through despite the system – not because of it, delegates heard at a recent Westminster Health Forum event. Ailsa Colquhoun reports the strategy to enable and empower community pharmacists to work in this way. A priority is to change the commissioning of primary care. He told policy chiefs that the NHS has “over-medicalised” the primary care response. “If we don’t develop community pharmacy we will lose people – and that puts pressure on the wrong bit of the system. We will spend more money than we should to support people as they use the NHS,” he said. GP money better spent in pharmacy? The elephant in the room... DISCUSSING the topic of �Next steps for pharmacy services in England’, Mike Farrar, former NHS Confederation chief executive turned independent consultant, told the conference that pharmacies could become a community authority “at the centre of preventative care”. Addressing senior officials from the Department of Health and NHS England in the audience, he told them that community pharmacy needed enablers to be put in place if it was to develop at scale and pace. It was “frustrating”, he said, that NHS England lacked Different contracts “Commissioners of community pharmacy [services] need to understand where [the sector] fits and should empower that resource,” Farrar continued. This would mean increasing the level of resource and integrating budgets. It should also mean thinking innovatively – for example, having different contracts for different community pharmacy contractor types, and entering into “prime contracts”, where one organisation subcontracts services to providers, including pharmacy. “We need to have different ways of working in different environments. Providers have different estates, and different models and they need different solutions.” However he admitted that GP funding could be a major obstacle in achieving these aims. “The elephant in the room is the issue of whether [GP and pharmacy services] are competitive,” he said. “We need to ask questions about value: is the GMS contract offering the value that it should? Is there money trapped in GMS that might be better directed at community pharmacy?” Discussing self-care, Farrar said: “We need to see it not as a weak �we can’t do anything, so do it yourself’ response, but as a way to respond to a growing consumer appetite for supported self-care.” This could include moving traditional services online, he ventured. any unplanned admission amounts to a system failure. We need to see medicines not as a cost but as a value proposition – and if we don’t see that happening, patients will end up in hospital.” New General Pharmaceutical Council chair Nigel Clarke said that services such as MURs had to be evaluated in terms of outcomes and not just outputs. “Counting heads” is not P sufficient enough for MURs and does not equate to good patient care, he suggested. He also made clear the regulator’s interest in achieving pharmacy access to the summary care record. “This is crucial. Patients are at risk if there is no sharing of information. We need [pharmacy access to] a single patient record. Harm is being done because this doesn’t exist. We see this as a regulatory issue and one we can’t run away from.” IN THIS ISSUE: Sleep advice Value proposition Ash Soni, vice-chairman of the RPS English Pharmacy Board, called for pharmacists to become NHS England’s “coordinators of medicines” and said that pharmacists work more effectively in a multidisciplinary care environment. Pharmacist prescribing was crucial to ensuring patients got the best out of their medicines. He urged the NHS in England to “move to a position where Omega Pharma is dedicated to making a difference by equipping pharmacy teams with the highest standard of training so that they can provide expert advice and service to customers. www.omegapharma.co.uk 2 Editor’s Comment 4 Insight 6 Opinion 8 Script Sense 14 PM Questions 16 CPPE Focus 25 NPA View 25 Society 28 Practice 39 Business Briefing 02_News_PM_0414_rt.qxp:02_PM_0414 14/04/2014 15:01 Page 2 VIEWPOINT NEWS Trusted care providers twitter: @PharMag_Richard Richard Thomas, editor email: [email protected] COMMUNICATIONS INTERNATIONAL GROUP, Linen Hall, 162-168 Regent Street, London W1B 5TB. Tel: 020 7434 1530 Fax: 020 7437 0915 Email: [email protected] EDITOR: Richard Thomas, BSc, FRPharmS. ASSISTANT EDITOR: Charlotte Rixon. EDITORIAL CONSULTANT: Liz Platts. CLINICAL DIRECTOR: Professor Alison Blenkinsopp OBE PhD, FRPharmS. FEATURES: Sasa Jankovic, Charlotte Rixon, Francesca Robinson. DESIGN: Peter Lawrence; Tony Gummer, Truprint Media. COMMERCIAL DIRECTOR: Martin Calder-Smith. ADVERTISEMENT MANAGER: Mark Walley. SALES EXECUTIVE: Abigail Tee. PUBLISHING ASSISTANT: Karen McClean. SPECIAL PROJECTS, KEY ACCOUNTS: Frances Shortland. EDITORIAL DIRECTOR, CIG HEALTHCARE PARTNERSHIP: Rosanne Please. PUBLISHING DIRECTOR: Felim O’Brien. EDITORIAL PANEL: Professor Alison Blenkinsopp OBE PhD, FRPharmS, Professor of the Practice of Pharmacy, University of Bradford; Dr David Temple PhD, FRPharmS, Welsh School of Pharmacy; Dr Colin Adair MPSNI, director NICPLD; Dr Gillian Hawksworth, PhD, FRPharmS; Mr Peter Curphey FRPharmS; Mr Alan Nathan FRPharmS, lecturer King’s College, London; Mr Hemant Patel FRPharmS, past-president RPSGB; Mr Mark Koziol MRPharmS, chairman PDA; Mr Liam Stapleton MRPharmS, consultant, Metaphor Development; Mr Steve Howard MRPharmS, pharmacy superintendent, Celesio UK; Ms Sue Sharpe OBE, chief executive PSNC. Published under licence by Communications International Group Ltd. © Groupe Eurocom Ltd. McCaul – first impressions count independent pharmacies as a whole suffer from an image problem, the research found. The pharmacist was considered a key element in an independent pharmacy’s service offering. Pharmacy assistants were recognised for their product knowledge but less so for their health and wellbeing expertise. Three areas were identified with the potential to grow independents’ business: • Introduce/promote services currently offered by GPs. Raise awareness of supplementary and emergency prescription services • Get closer to customers. Demonstrate professionalism combined with friendly service CIRCULATION/SUBSCRIPTION ENQUIRIES: The National Pharmacy Database, Precision Marketing Group, Precision House, Bury Road, Beyton, Bury St Edmunds IP30 9PP. Tel: 01284 718912; email: [email protected] PHARMACY MAGAZINE/TRAINING MATTERS COMPETITION RULES 1. Competitions are only open to pharmacists/pharmacy assistants currently employed at registered UK premises. 2. Only one entry is allowed per pharmacist/assistant. 3. The names of competition winners can be obtained by sending a SAE to the address above. 4. Any personal information we collect from competitions will be used in accordance with the Data Protection Act 1998 and other applicable laws. A Communications International Group publication 2 APRIL 2014 PHARMACY MAGAZINE RESEARCH BITES Customer perceptions… of the multiples: “Greedy, faceless organisations” “Lacking in privacy” “Greater focus on personal care” Customer perceptions… of independents: “The first thing I noticed was the smell” “Loads of random stuff in the window – it just looks messy” “It’s a shop you have to go to, rather than want to go to” 16:11 Page 5 Unannounced inspections to stay The GPhC says its new inspection model is currently taking on average around three to four hours per pharmacy visit, longer than the two hours initially envisaged. However, despite criticism from pharmacists and other professional bodies that the current system of unannounced visits leaves little time for pharmacy teams to prepare, the regulator is “unlikely” to move away from this approach as it is considered important for public credibility, head of inspection Mark Voce told the IPF spring conference. Training had been held for inspectors on making the visits more streamlined, he said. “We are working hard to make the process as efficient as possible.” Independents could help things along by doing as much preparation in advance as possible, including thoroughly briefing their support staff. “It’s not about catching people out. We are taking a Are you... Undervalued? Overworked? Underrepresented? FOUNDING EDITOR: Anne Anstice • Improve the retail proposition with a relevant product range for the local community and a clean, uncluttered store. The research was discussed at last month’s IPF spring conference in Hatfield. Chairman Fin McCaul told delegates to look at their pharmacies through the eyes of their patients. “Get your friends, husbands and wives to come into the pharmacy and look at it from the patient perspective. Make it the right environment so that patients want to come back.” Do independent pharmacies have an image problem? According to some new market research, this could well be the case (see story opposite). Pharmacists themselves and, on the whole, their support staff, came out well in the research. Lauded for their expertise, local convenience and personal service, independents were considered to be trusted healthcare providers. But consumers’ overall experience of independent pharmacy was less positive. Words used to describe the appearance of independents’ premises, for instance, included �messy’, �old school’, �chaotic’, �disorganised’ and �dark’. Some even objected to the smell… Many of our readers won’t recognise these adjectives as applying to them. And there has certainly been some significant investment by independent owners in recent years in modernising their premises. But there are also plenty of pharmacies that simply aren’t attractive places to visit. This is not a problem exclusively confined to the independent sector, either. Pop into any medium-sized multiple in a typical market town or city centre, and you’re often greeted by half-empty shelves, with fixtures and fittings that have seen better days. Could it be that the hundreds of millions of pounds sucked out of pharmacy funding since 2005 is beginning to have an effect? If large parts of the network are looking tired and down-at-heel, this does not help pharmacy’s efforts to provide a modern, inviting healthcare and retail experience. Independent pharmacies have more credibility offering advice and information services than large chains and supermarket pharmacies. They are seen as trusted healthcare providers, according to new customer research from Reckitt Benckiser. Customer service was the key driver of pharmacy choice among users of independents, who were more likely to place value on staff, prescription services and relationships. Frequent users strongly associated independents with medical expertise, locality, personal service and easy access to trusted advice. Multiple pharmacy shoppers, on the other hand, were influenced more by the look and feel of the store, with convenience and price the key drivers in supermarket pharmacies in particular. However it was felt that staff lacked knowledge and experience. Independents were seen to offer the least retail expertise and the quality of the retail proposition “varied hugely” from pharmacy to pharmacy. As a result of those pharmacies with �bad’ retail propositions, Then help for you could be at hand… The INDEPENDENT PHARMACY FEDERATION is here to support independent contractors like you. Membership is only £10 per month – join us at www.theipf.co.uk human approach,” he said. No reports of pharmacy visits will be made available to the public during the prototype phase of the scheme, he reassured delegates. Comments received so far from inspected pharmacies had been positive, according to Mr Voce. Pharmacists valued the instant feedback from inspectors and welcomed the new �show and tell’ approach. Visits were seen as a learning and development opportunity for all the pharmacy team, he added. Mr Voce urged pharmacists to “get on the front foot” with the inspections. “Don’t wait to be asked: tell the inspector the three or four things you are most proud of and why patients love your pharmacy and how you keep them safe. Don’t be afraid to proactively identify areas for improvement and say what you are doing to make the changes.” It is up to pharmacies to provide the evidence and examples required in whatever way they choose, he said. 03_News_PM_0414_rt.qxp:03_PM_0414 14/04/2014 15:04 Page 3 NEWS Both pharmacists and pharmacy technicians are considerably less likely to be unemployed when compared to the economically active population as a whole, a survey conducted by the General Pharmaceutical Council has revealed (reports Asha Fowells). The census provides a good illustration of the diversity and adaptability of the profession, with over a tenth of registrants having more than one job. Just 2 per cent of pharmacy professionals reported being out of work, a figure that is considerably lower than the 7.6 per cent for the general population over the same period of time. While some 10 per cent of pharmacists and 5 per cent of pharmacy technicians said that they were not working in a job relating to pharmacy, the vast majority said this was because they were caring for a family. However the working hours clocked up by pharmacy professionals fell short of what many would consider to be a full working week, at 35.7 hours for pharmacists and 32.5 hours for pharmacy technicians. This compares to 37.6 hours per week for the economically active population as a whole. Appraisals Community is the setting where most pharmacists and pharmacy technicians work (72 per cent and 53 per cent respectively), with hospital the second largest sector (23 per cent of pharmacists and 39 per cent of pharmacy technicians). Those working in hospital were considerably more likely than their community colleagues to have had a performance appraisal in the last year – something that may be relevant as continuing fitness to practise draws closer. The GPhC commissioned the survey as a way of finding out where pharmacy professionals work and the type of responsibilities they have, in order to develop effective and appropriate regulatory approaches. All 21,672 pharmacy technicians and 30,040 of the pharmacists on the register in autumn 2013 were invited to take part, with just under 30,000 (55 per cent) choosing to participate. PHARMACY PROFESSIONALS IN THE COMMUNITY SETTING Community settings worked in* Hours worked** 65% 40% Large multiple community pharmacy Employment status** 27% 73% Employee Part time Full time 21% 24% Locum/self-employed/ Community pharmacy with 4 or fewer stores 11% Another multiple community pharmacy 35.3 Hours worked per week on average 11% Business owner Key components roundup E-CIGS: ENSURE INFORMED CHOICE Pharmacies selling e-cigarettes must ensure that they provide sufficient information and advice so that customers can make an informed choice as to whether to use them or not, a legal expert has advised. Noel Wardle, a partner at Charles Russell, told delegates at his firm’s spring conference that procedures and training for pharmacy assistants must be in place to avoid the prospect of more undercover media investigations into pharmacy. PEOPLE MISSING OUT ON HEALTH CHECKS INSPECTION SUPPORT FROM IPF Barely half the people who are supposed to get an NHS Health Check in England are actually getting one, according to a new report from Diabetes UK. The report, called NHS Health Checks in Local Authorities, shows that just over 6 per cent of people aged 40 to 74 years got one of the checks in the first nine months since the programme switched from NHS to local government control – significantly less than the 11.25 per cent of people in this age range Diabetes UK says should be getting the check. The IPF has teamed up with Xact, a company specialising in human resources, employment law and regulatory advice, to support members through the new GPhC inspection regime. Members can access services at a discounted rate. learners, as well as for those who want to deliver learning, such as employers and local training organisations • An assessment framework, which encourages pharmacy professionals to work through a self-assessment process to identify their learning needs. There is also an online assessment, which uses videoed consultations that pharmacy professionals can access to check their learning and development. The resources can be accessed at www.consultationskillsfor pharmacy.com. • See also the CPPE Focus column on p16. Check out the PM app – news, views, analysis and CPD on your tablet or mobile The answers to the OTC Treatment Clinic are on p4 of Pharmacy Magazine New consultation skills framework launched The main components of the framework are: • A set of practice standards for consultation skills in pharmacy that outline the competencies that pharmacy professionals need to achieve in order to conduct consultations and public health interventions effectively • A learning pathway, which individual pharmacy professionals can follow to develop the consultation skills they need. To coincide with the launch, a CPPE distance learning pack will be mailed to all pharmacists and pharmacy technicians in England • A range of training formats (e.g. face-to-face learning, e-learning and printed workbooks). A variety of resources is available for email: [email protected] freelancer/contractor *All respondents currently working in a paid pharmacy-related job **All respondents with main job in community setting only Source: GPhC A major new initiative to help pharmacists and pharmacy technicians enhance their communication and consultation skills has been launched by the Centre for Pharmacy Postgraduate Education (CPPE) and Health Education England (HEE). The consultation skills framework represents the beginning of a national programme of change in pharmacy, says CPPE director, Professor Christopher Cutts. “The framework will apply to more than 60,000 pharmacy professionals across England. This includes pharmacists, pharmacy technicians and preregistration pharmacy trainees. It also affects those who are training the next generation of pharmacists and pharmacy technicians.” GPhC census shows pharmacy still a solid career choice COMMENTARY: WHY FRAMEWORK IS NEEDED By CPPE tutor Reena Barai: I can imagine many of you are rolling your eyes and thinking – why do I need to be taught how to do the obvious? While there are many pharmacy professionals with great consultation skills, I am pretty sure every one of us can remember a consultation with a patient that hasn’t gone as well as we would have liked. It is also fair to say that most of us have never had any formal training on consultation skills and have relied wholly on our innate communication skills to get our message across to patients. Our role and the services we provide are becoming increasingly patient-facing, be it over the counter or in our consulting rooms. We have to adopt a patient-centred approach if we are to rise to the challenge of supporting patients to optimise their medication and self-care. Unfortunately time constraints are a potential barrier to adopting this approach. I would argue that by perfecting our consultation skills, especially some of the skills needed to close a consultation, we might actually become more effective and save time. Historically many pharmacy professionals may have even avoided conducting consultations due to a fear of needing to be the perceived �expert’. A patient-centred consultation is possibly less daunting as you actually have to listen more and talk less. Above all there is the immense sense of job satisfaction you get from actually delivering patient-centred care and supporting a patient to achieve a better health outcome. PHARMACY MAGAZINE APRIL 2014 3 04_Insight_PM_0414_rt.qxp:04_PM_031411/04/201412:07Page4 TEAM TRAINING VIEWPOINT subject: ovulation and pregnancy testing pharmacist training support by Alexander Humphries* I’m tired of people who have never risked anything in their lives telling me how to run my business. It’s time we held this civil service bureaucracy to account... Ivory tower thinking I’VE SPENT the last few weeks getting annoyed about the hypocrisy of unelected and unaccountable civil servants. They lecture me about the need to be efficient and to look for new models of service. Well, it’s time we held them to account, starting with England’s chief pharmaceutical officer (CPO). Take the Pharmacy Call to Action. This began with a wave of enthusiasm from pharmacy bodies with an interest in how the community pharmacy contract develops, but when I saw the questions I was less enthusiastic. Was this an excuse to wield the axe? The CPO says there are some areas where there are too many pharmacies. In part I share his view, but I wasn’t the person in post at the DH in the aftermath of the disastrous relaxation of market entry rules, which let many new pharmacies in through the back door in places they weren’t actually needed or even wanted. He says that his view “can be quite disturbing to people who have invested a lot of time, energy and money into their business”. Well, we can certainly agree on that. The problem is, the DH and NHSE seem to want us to move towards a hub-and-spoke model, where prescription �factories’ ship finished prescriptions out to those pesky community collection points. Great news if you happen to be a wholesaler or a large chain that can quickly move towards this new world, where economies of scale and efficiencies exist. Not such good news for small businesses. The Government should care about small pharmacy businesses because they perform a unique public duty with respect to their competitive purchasing of medicines on behalf of the NHS. You see, it is in wholesalers’ interests to keep prices high, because this keeps their owners happy. It is only because independents drive the market price down through competitive purchasing that the taxpayer reaps the benefit through category M clawbacks. Reduce the number of independents (and therefore competition) and you sustain fewer independent wholesalers, leading to less competition on price. The ultimate result is higher medicine costs. “ Dr Ridge is playing with long-term economic fire ” Governments cannot perform this function efficiently, but the market can. Dr Ridge is playing with long-term economic fire if he thinks otherwise. It is really easy for civil servants who are paid every month, regardless of performance, with the prospect of a nice pension at the end, to lecture us about the need for efficiencies. And just as easy to gamble with the sector’s future when you don’t have a direct stake in it. Savings before safety With regard to technology, it appears as though the bureaucrats have made their mind up that they want wider use of technology, almost certainly because they think it will save them money, not because it is necessarily safer or better for patients. A great example of the hypocrisy of Government is its stance on the Falsified Medicines Directive, an EU diktat which says that the public needs to be safeguarded from fake medicines. This could be done in pharmacies and tied in with software to remove the danger of most dispensing errors. But the Government’s stance is, we’re reasonably happy for it to happen – we just don’t want to pay for it. A bad deal A final example of out-of-touch bureaucrats meddling with no thought for the long-term consequences is the Modernising Pharmacy Careers programme, which would present a huge windfall for universities as it would largely give them total control of pharmacist training up to registration, and the money to go with it. The trade-off was supposed to be a cap on student numbers to make the profession sustainable, but that does not seem to be coming any time soon. Make no mistake, this is an historic and irrevocably bad deal for employers, students and for pharmacy. So, returning to the Call to Action, those bureaucrats who have already demonstrated a naive and reckless attitude towards market entry, technology and training will be able to cherry pick from the 800 responses... or decide to do exactly what they wanted to do in the first place, hiding behind a thin veneer of legitimacy. The world must look very different from those Whitehall ivory towers, but officials must be honest – are they trying to make the pharmacy service cheaper or better? * Pen name of a practising community pharmacist. Alexander Humphries’ views are not necessarily those of Pharmacy Magazine. Does pharmacy policy disadvantage small businesses? Email [email protected] 4 APRIL 2014 PHARMACY MAGAZINE Activities such as training your support staff are important CPD triggers. This Pharmacist Training Support column runs in conjunction with this month’s OTC Treatment Clinic in Training Matters and can be used as a Team Tuesday exercise. Supporting Training Initiatives educat ion the otc treatm ent clinic Common condition s and the ir treatment options This module has as part of their been endorsed with the NPA’ ongoing learn ing. Complete s Training Seal as suita the questions ble for use by medicine at the end s to include in your self- counter assistants development portfolio module 20 Ovulati 4n and pregnanocy testing Welcome to Treatment TM’s OTC Clinic series handy, four-p . This age sectio specially n is designed so that you can detach it from the magazine and future refere keep it for nce. Each mont h, TM different OTC treatmcovers a to help you ent for this mod keep up-to area with the ule latest produ -date developme ct OBJECTIVES we focus nts. In this issue, : • Understan After studying on this modu pregnancy ovulation and d the diffe le, assist • Be awar rent stage ants will: end of the testing. At the e of the s of the statistics • Be awar female multiple module there are related e of the monthly to infer choice quest importanc cycle • Be able tility for you to e of good to complete, ions • Be famil advise on the progress use of ovula pre-conception so iar with the can be moni your care and tion tests • Have early signs by your a healthy an unde pharmacist. tored and symp rstanding lifestyle toms of of home You can pregnancy pregnancy the Coun find out more in tests and It is much ter Intelligence when they more comm training Plus can be on for wome having a guide. used. baby. author: Jane Fee ly, PhD The last six topic s we have covered are: ing cessa tion care l Smok l Oral l Daily fatigue and stress hs Sore throa ts l Colds and flu l Coug l You can download previous modules from www.tm-m odules.co.u k n today to Indeed, it number delay has been of babies ovulation born to wome reported that the and pregn has more ancy tests, n over the than doubl may visit concerned the pharm age of 50 ed in four number couples acy to ask years and of wome purchase n over 40 for advice the a test to by 13 per having childre and help pinpo cent – from a woman’s int the best n has risen monthly 26,419 in 2012 – with time during cycle to try 2008 to one in 25 Failure to 29,994 in and conce births being 40. And fall pregn ive. in 2012, ant within expected to wome nearly half time frame a couple n over to mothe of all babies ’s own can cause rs aged 30 it’s impor were disappointm tant to be and over. born While many sensitive advice. It’s women in when custom ent, so also a good can expec their mid-3 ers seek t to have leaflets – idea to displa 0s and healthy pregn as some older that a woma y information people may advice from ancies, it n’s prefer to is a fact biggest decrea fertility decreases the privac read the y of their with age. It’s also impor se in fertilit The 30s and y begins tant to know own home. couples who pharmacist. during the when to opt to wait midThis includ their family refer to the before startin date with es wome may feel n who are vaccinations under pressu successful g not up to ; are taking as soon as diabetes, re if they epilep are not they had medication; With recent anticipated. couples who sy, asthma or a thyroi have advances have a history d condition in the techn have previo and ology of of gene usly had home a pregnancy abnormalities or tube defect affected s. by neura l TM APRIL SUBJECT: 2014 PULL OUT AND KEEP OVULATION AND PREGNANCY TESTING This module provides pharmacists with a useful training resource for pharmacy assistants. Refer to this month’s OTC Treatment Clinic on ovulation and pregnancy testing in Training Matters. The materials are accredited by the NPA. REFLECTION • Do we give the best possible advice on the use of ovulation test kits? • Do we know how they work and when they should be used? • Am I aware of the latest statistics on infertility in this country? • Am I aware of the latest NICE guidelines on fertility? (Clinical guidelines, CG156; February 2013) • Do we give appropriate, evidence-based lifestyle advice to couples trying to conceive? TRAINING CHECKLIST Ensure support staff understand the following key points: • Trying to conceive is a sensitive subject • Conceiving a baby does not necessarily happen quickly • How the different stages of the female monthly cycle link in with the way in which ovulation test kits work • The differences between the newest and older ovulation test kits • The importance of healthy eating and lifestyle while trying to conceive and during pregnancy • The importance and timing of folic acid supplementation • How home pregnancy testing kits work. I WILL ENSURE: • My knowledge of ovulation test kits is up to date • My staff know when customers with problems trying to conceive should see the GP • My staff understand the importance of sensitivity and privacy in communication with customers who are trying to conceive • My pharmacy assistants can meet the points in the training checklist. PRACTICE ACTIVITY • What support is available to couples having fertility problems? See: www.nhs.uk/conditions/pregnancy-andbaby/pages/help-infertility.aspx; www.infertility networkuk.com; and www.fertilityfriends.co.uk Answers to OTC Treatment Clinic no. 204 on ovulation and pregnancy testing: 1.c 2.a 3.d 4.d 5.d 6.a 05_PM_0414:05_PM_0414 09/04/2014 13:23 Page 1 Are you up-to-date with emergency hormonal contraception? The tolerability of emergency hormonal contraception (EHC) hasn’t changed.. ... ...but the efficacy has. ellaOne has a tolerability profile comparable to levonorgestrel1 ellaOne prevents significantly more unplanned pregnancies than levonorgestrel Two comparative non-inferiority studies showed ellaOne is at least as Most frequent adverse events in the intention-to-treat population1 effective in preventing pregnancy as levonorgestrel.1,2 When these data 25 significantly reduced compared with levonorgestrel.1 15 When ellaOne is taken within 24 hours of UPSI, a woman’s risk of pregnancy drops by almost two-thirds vs. levonorgestrel1 10 5 Risk of pregnancy with ellaOne vs. levonorgestrel:1 0.9% vs. 2.5% (odds ratio 0.35; 95% CI 0.11–0.93; p=0.035) ellaOne (n=1104) in pa k Ba c Which means 16 fewer unplanned pregnancies per 1000 women1 ab do m al in m do Ab levonorgestrel (n=1117) U p in per al pa in in pa es s Di zz in ue tig Fa se a N au a oe or en Dy sm ea da rh ch e 0 H Proportion of women (%) were pooled in a meta-analysis the risk of pregnancy with ellaOne was 20 Adapted from Glasier AF et al., Lancet 2010.1 With ellaOne – 9 unplanned pregnancies per thousand 9 With levonorgestrel – 25 unplanned pregnancies per thousand 25 Adapted from Glasier AF et al., a 2010 Lancet meta-analysis.1 ABBREVIATED PRESCRIBING INFORMATION (UK) ellaOne®(ulipristal acetate). Please refer to the SmPC before prescribing ellaOne® Presentation: White/off-white, round curved tablet engraved“ella” on both faces Indications: Emergency contraception within 120 hours (5 days) of unprotected sexual intercourse or contraceptive failure. Dosage: One 30mg tablet to be taken orally as soon as possible, but no later than 120 hours after unprotected intercourse or contraceptive failure, with or without food. Another tablet should be taken if vomiting within 3 hours of intake. Can be taken at any point in menstrual cycle. Pregnancy should be excluded. Renal or hepatic impairment: no specific dose recommendations. Severe hepatic impairment: not recommended. Children and adolescents: Limited safety and efficacy data in women under 18 years. Contraindications: Hypersensitivity to active substance or excipients. Pregnancy. Special warnings and precautions for use: Concomitant use with an emergency contraceptive containing levonorgestrel is not recommended. Use in severe asthma insufficiently controlled by oral glucocorticoid not recommended. Emergency contraception only; women should be advised to adopt a regular method of contraception. May reduce contraceptive action of regular hormonal contraception, when continued or initiated immediately after ellaOne use; subsequent acts of intercourse should be protected by reliable barrier method until next menstrual period. Repeated administration within the same menstrual cycle is not advisable. No data for unprotected intercourse more than 120 hours before intake. Does not prevent pregnancy in every case; delay of >7 days in next menstrual period, abnormal bleeding at menses, or symptoms of pregnancy, exclude pregnancy. If pregnancy occurs, consider possibility of ectopic pregnancy. Menstrual periods can sometimes occur earlier or later than expected by a few days. In ~ 7%, menstrual periods occurred > 7 days early. In ~ 18.5% a delay of > 7 days occurred, and in 4% the delay was > 20 days. Contains lactose monohydrate; patients with galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should avoid. CYP3A4 inducers (e.g. rifampicin, phenytoin, phenobarbital, carbamazepine, efavirenz, fosphenytoine, nevirapine, oxcarbazepine, primidone, rifabutine, St John’s wort/Hypericum perforatum, long term use of ritonavir) may reduce plasma concentrations of ulipristal acetate and decrease efficacy, even if stopped enzyme inducer within last 2-3 weeks. Concomitant use not recommended. Potential for other medicinal products to affect ulipristal acetate: CYP3A4 inducers - In vivo results using potent inducer show marked decreases of Cmax and AUC (>90%) and reduced half life (2.2-fold) corresponding to 10-fold decrease in exposure. CYP3A4 Inhibitors - In vivo results show administration of ulipristal acetate with a potent and a moderate CYP3A4 inhibitor increased Cmax and AUC of ulipristal acetate 2- and 5.9-fold, (max) respectively; clinical consequences unlikely. Medicinal products affecting gastric pH - Administration of ulipristal acetate (10 mg) together with esomeprazole (20 mg daily for 6 days) resulted in approx 65% lower mean Cmax, delayed tmax and 13% higher mean AUC; clinical relevance unknown. Potential for ulipristal acetate to affect other medicinal products: P-gp substrates - In vitro data indicate that ulipristal acetate may inhibit P-gp; in vivo results with fexofenadine inconclusive. Hormonal contraceptives - Ulipristal acetate binds to the progesterone receptor with high affinity and may interfere with contraceptive action of progestogencontaining products. Fertility, pregnancy and lactation: contra-indicated during existing or suspected pregnancy. Extremely limited data available on health of the foetus/new-born in pregnancy exposed to ulipristal acetate. No teratogenic potential was observed; animal data insufficient with regard to reproduction toxicity. Marketing Authorisation Holder maintains a pregnancy registry to monitor outcomes of pregnancy in women exposed to ellaOne®. Patients and health care providers are encouraged to report any exposure. Ulipristal acetate is excreted in human breast milk; breastfeeding is not recommended for one week after intake. Breast milk should be expressed and discarded. A rapid return of fertility is likely following ellaOne use; regular contraception should be continued or initiated as soon as possible; subsequent acts of intercourse should be protected by reliable barrier method until next menstrual period. Undesirable effects: Always consult the SmPC before prescribing. Most commonly reported adverse reactions: headache, nausea, abdominal pain and dysmenorrhea. Common (ш1/100 to <1/10): mood disorders, dizziness, abdominal pain upper, vomiting, abdominal discomfort, myalgia, back pain, dysmenorrhea, pelvic pain, breast tenderness and faitigue. Uncommon (ш1/1,000 to <1/100): vaginitis, nasopharyngitis, influenza, UTI, appetite disorders, emotional disorder, anxiety, insomnia, hyperactivity disorder, libido changes, somnolence, migraine, visual disturbance, hot flush, abdominal pain lower, diarrhoea, dry mouth, dyspepsia, constipation, flatulence, acne, skin lesion, pruritus, menorrhagia, vaginal discharge, menstrual disorder, metorrhagia, vaginal haemorrhage, hot flush, premenstrual syndrome, pain, irritability, chills, malaise, pyrexia. Rare (ш1/10,000 to <1/1,000): conjunctivitis, hordeolum, pelvic inflammatory disease, dehydration, disorientation, tremor, disturbance in attention, dysguesia, poor quality of sleep, parosmia, syncope, abnormal sensation in eye, ocular hyperaemia, photophobia, vertigo, haemorrhage, upper respiratory tract congestion, cough, dry throat, epistaxis, gastro-oesophageal reflux disease, toothache, urticaria, general pruritus, pain in extremity, arthralgia, urinary tract disorder, chromaturia nephrolithiasis, renal pain, bladder pain, genital pruritus, dysfunctional uterine bleeding, dyspareunia, ruptured ovarian cyst, vulvovaginal pain, menstrual discomfort, hypomenorrhea, chest discomfort, inflammation, and thirst. Package quantities and basic NHS price: ellaOne® 30 mg Tablet Oral use 1 tablet blister pack: £16.95. Marketing authorisation holder: Laboratoire HRA Pharma, 15, rue Béranger, F-75003 Paris, France. Marketed in the UK by: HRA Pharma UK & Ireland Limited, Unit 7, RB Building, 557 Harrow Rd Kensal Green London W10 4RH. Additional information is available on request, contact medical information on 0800 917 9548 or e mail [email protected]. Marketing authorisation number(s) EU/1/09/522/001 Legal category: POM. Date of last revision of the API text: July 2013. Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to HRA Pharma UK & Ireland Ltd on 0800 917 9548 or email [email protected] Date of preparation: March 2014 Any case of pregnancy exposed to ellaOne should be reported on www.hra-pregnancy-registry.com References: 1. Glasier AF et al., Lancet 2010; 375: 555–62. 2. Creinin MD et al., Obstet Gynecol 2006; 108: 1089–97. Item code: UK/ELLA/0314/0022 06_Opinion_PM_0414_rt.qxp:06_PM_0414 10/04/2014 11:31 Page 6 VIEWPOINT KEY POINTS: FOOT PROBLEMS IN DIABETES • 1 million people in the UK with diabetes are at high risk of developing foot problems • 15 per cent of people with diabetes still do not receive a foot check • Delaying a referral can mean the difference between keeping a foot and losing it Help us stay one step ahead of foot disease Barbara Young, chief executive of Diabetes UK, wants pharmacists to be on the look-out for diabetic patients at high risk of a �foot attack’ IT’S OFTEN THE CASE that people with diabetes engage far more regularly with their pharmacist than they do with their GP – and this puts pharmacists in a unique position to help ensure they get the care they deserve. We want pharmacists to make sure people who are at high or increased risk of a foot attack to: • Know their risk status • Understand the importance of good foot care • Understand the urgent need to see a doctor if they have any signs of a foot attack. When you consider that 1m people with diabetes are at high risk of a foot attack, it is really worrying that many of these people are being left in the dark about what to look for and when they need to seek urgent medical help. This means that, all too often, people are seeing the signs of foot disease but are not then acting on it and potentially losing their foot as a result. The NHS needs to shift its approach to diabetic foot disease so that people understand the importance of addressing foot problems quickly. Even a matter of hours in delaying referral can mean the difference between keeping a foot and losing it. Many hundreds of amputations a year could be prevented “ ” There is an important role for pharmacists to play. They should urgently signpost people to their GP if they mention they have any of the symptoms of a foot attack. These include: • A red, warm or swollen foot • A break in the skin • Oozing onto socks or stockings. This is particularly urgent if any of these symptoms are accompanied by feeling unwell. It is also important to routinely remind people with diabetes that having their feet checked is an important part of their annual review and that they, or someone else, need to be keeping an eye on their feet for the other 364 days of the year. National Diabetes Audit data shows that 15 per cent of people with diabetes are still not receiving this check. Well placed Pharmacists are well placed to have a meaningful conversation with people to ask if they are aware of their risk status of having a foot attack and find out if they know what to do in the event of having any of the symptoms. To help with this conversation we have a new booklet, �How To Spot A Foot Attack’, which is available to order free from our online store. We would encourage pharmacists to display the booklet and give it to anyone in the �at risk’ categories. It really is a question of communication and pharmacists can be invaluable because they have an opportunity to listen to what people with diabetes are saying and respond accordingly. For example, many people with diabetes experience loss of feeling in their feet, so it is crucial that they understand the importance of regularly checking their own feet for changes or getting a carer to do so, as they may be having a foot attack but not be experiencing any pain or discomfort. By getting better at providing foot checks and raising awareness, many hundreds of amputations a year could be prevented. This would mean huge cost savings for the NHS but also that those people would avoid the devastation of having an amputation that could have been prevented. The free booklet can be ordered from www.shop. diabetes.org.uk/go/red-cardfoot-booklet. DEDICATED Whatever the weather, Kevin’s customers get their deliveries on-time, every time. The winter tyres help, but with more than 900 on-time deliveries every month, it’s his dedication that gets him through. We can deliver so much more to support your business – giving you back time to focus on improving patient services. Find out at www.aah.co.uk/competence or call 0844 561 8899 6 APRIL 2014 PHARMACY MAGAZINE 07_PM_0414:07_PM_0414 09/04/2014 14:39 Page 1 08-13_Script_PM_0414_rt.qxp:08-13_PM_0414 09/04/2014 16:26 Page 8 CLINICAL NEWS clinical roundup & news reView scriptsense edited by Mark Greener Call to help boost diabetic foot care Community pharmacists should do more to help people with diabetic foot problems avoid amputation, experts have told Pharmacy Magazine. Over a year, researchers from University Hospitals of Leicester identified 20 patients with active foot disease who were �delayed new referrals’. In 16 patients, the median time from first symptom to referral was 25 weeks, resulting from their reluctance to attend the clinic or lack of understanding of the significance of their foot disease. Three patients presented with gangrene and the researchers identified one case of Charcot’s arthropathy. Five patients needed �minor’ amputations due to foot sepsis or osteomyelitis. One patient needed an above-knee amputation for a non-revascularisable limb that presented with toe gangrene and rest pain. “Diabetic foot problems can deteriorate very quickly. As a result, they require rapid treatment and assessment,” Nikki Joule, Diabetes UK policy manager, told PM. “Community pharmacists can contribute directly to the prevention of foot problems by encouraging people with diabetes to get their annual foot checks, and making sure they are aware of their risk of developing foot problems and what they need to look out for.” “Community pharmacists should signpost patients with possible diabetes-related foot ACEIs reduce mortality in diabetes Angiotensin-converting enzyme inhibitors (ACEIs) reduce allcause mortality, cardiovascular (CV) deaths and major CV events in patients with diabetes, a new meta-analysis reports. The meta-analysis included 23 studies comparing ACEIs with placebo or active drugs (32,827 patients) and 13 comparing angiotensin II receptor blockers (ARBs) with no therapy (23,867 patients). Compared with controls, ACEIs significantly reduced the risk of all-cause mortality by 13 per cent, CV deaths by 17 per cent and major CV events by 14 per cent. Specifically, ACEIs reduced the risk of myocardial infarction by 21 per cent and heart failure by 19 per cent. ARBs did not significantly influence all-cause mortality, CV death or major CV events – except for a 30 per cent reduction in heart failure. Neither ACEIs nor ARBs reduced stroke risk. ACEI benefits on all-cause and CV mortality did not depend on baseline blood pressure and proteinuria or the type of ACEI. The authors concluded that “ACEIs should be considered as first-line therapy to limit excess mortality and morbidity” in people with diabetes. (JAMA Intern Med doi:10.1001/ jamainternmed.2014.348). Oseltamivir saves lives Best foot forward for people with diabetes problems to appropriate services,” adds Dr Kath Higgins, diabetes consultant at University Hospitals of Leicester and one of the study authors. “They should be aware of the referral pathways in the Diabetes UK �Putting Feet First’ literature and their local pathways to ensure that they are signposting appropriately. Pharmacists should also understand which foot problems require urgent attention. It is vital that patients with diabetes and foot problems obtain specialist advice at the earliest opportunity.” (See also Opinion on p6.) Rapid treatment with a neuraminidase inhibitor, such as oseltamivir, reduced mortality among adults admitted to hospital with suspected or proven pandemic influenza, reports a Rochesponsored meta-analysis in Lancet Respir Med. Based on an analysis of 29,234 patients from 78 studies performed during the 2009-10 H1N1 pandemic, neuraminidase inhibitors reduced mortality by 19 per cent compared to no treatment. Starting neuraminidase inhibitors within two days of the onset of influenza symptoms reduced mortality by 52 per cent compared to later treatment and by 50 per cent compared to no treatment. Neuraminidase inhibitors did not significantly reduce mortality in children. (doi:10.1016/S2213-2600(14) 70041-4) AED prevents head and neck cancer? Valproic acid reduces head and neck cancer risk by 34 per cent with a dose-response relationship, without affecting lung, bladder, colon or prostate cancer (Cancer doi:10.1002/ cncr.28479). PASSIONATE Whatever your retail space, Vicki’s there to make it profitable. The displays and branding help, but its Vicki’s passion for creating the best retail experiences that drives her to make over 50 pharmacy visits every month. We can deliver so much more to support your business – giving you back time to focus on improving patient services. Find out at www.aah.co.uk/commitment or call 0844 561 8899 8 APRIL 2014 PHARMACY MAGAZINE 09_PM_0414:09_PM_0414 10/04/2014 10:23 Page 1 What do your customers with eczema use for washing? • FR NCE • R AG A FR EE NICE and BAD guidelines are clear: eczema sufferers should avoid using soap and detergent-containing products to avoid exacerbating their condition.1,2 That means offering your customers effective emollient wash products, like the Oilatum wash range. Less than 15% of GP patients are prescribed both bath and cream emollients.3 There’s a huge opportunity to help improve the lives of your customers with eczema – simply recommend them a wash emollient alongside their cream prescription, in line with clinical guidelines.1,2 Oilatum wash products protect the skin from drying, and provide a barrier against allergens and irritants. Recommend a product from the No.1 prescribed emollient wash range4 as an addition to your customers’ emollient creams, for soothed skin and satisfied customers. Light liquid paraffin Product Information Oilatum Junior (light liquid paraffin) Bath Additive. Oilatum Shower Gel Fragrance-Free (light liquid paraffin). References: Indications Contact dermatitis, atopic dermatitis, senile pruritus, ichthyosis and related dry skin conditions. Dosage and method of use All ages: Apply to wet skin or add to water. $GXOWEDWK 1-3 capfuls in an 8 inch bath of water, soak for 10-20 minutes, pat dry. ,QIDQWEDWK ½-2 capfuls in a basin of water, apply gently over entire body with a sponge, pat dry. Precautions Hypersensitivity to any ingredient. Stop use if rash or irritation occurs. Side effects Application site reactions including erythema, rash, pruritus, dermatitis. GSL . Pack sizes and RSP (excl. VAT): 150 ml £4.21, 250 ml £4.88, 300 ml £7.62, 600 ml £8.83. PL 00079/0708. PL holder Stiefel, 980 Great West Road, Brentford, Middlesex, TW8 9GS. Date of revision March 2014. Indications Contact dermatitis, atopic dermatitis, senile pruritus, ichthyosis and related dry skin conditions. Dosage and method of use All ages: Use as often as necessary. Apply to wet skin, normally as a shower gel. Precautions Hypersensitivity to any ingredient. Not for use on greasy skin. Side effects Application site reactions including erythema, rash, pruritus, dermatitis. GSL . Pack size and RSP (excl. VAT) 150 g £7.73. PL 00079/0704. PL holder Stiefel, 980 Great West Road, Brentford, Middlesex, TW8 9GS. Date of revision March 2014. 1. NICE Clinical Guideline 57. Atopic eczema in children. Management of atopic eczema in children from birth up to the age of 12 years. December 2007. Available at: http://guidance.nice.org.uk/CG57. Accessed 03/03/14. 2. Primary Care Dermatology Society & British Association of Dermatologists. Guidelines for the management of atopic eczema. Available at http://www.eguidelines.co.uk. Accessed 09/04/14. 3. GSK data on file, GP prescription data 2013. 4. IMS unit performance data, MAT to Jan 2014. OILATUM and TAKE COMFORT IN OUR SCIENCE are registered trade marks of the GSK group of companies. 08-13_Script_PM_0414_rt.qxp:08-13_PM_0414 09/04/2014 16:27 Page 10 CLINICAL NEWS Cholesterol rises in the winter Cholesterol levels rise in the winter, according to research presented during the American College of Cardiology’s annual meeting. Previous studies showed that heart attacks and cardiac mortality peak during the winter, so researchers at Johns Hopkins University, Baltimore, looked at changes in seasonable lipids in 2.8m adults. LDL and non-HDL cholesterol levels were 3.5 and 1.7 per cent higher in men and women respectively during the colder compared to warmer months. Triglycerides were 2.5 per cent higher in men during the winter. HDL did not vary much between seasons. “In this very large sample, we found that people tend to have worse cholesterol numbers on average during the Seasonal lipid variation colder months than in the warmer months – not by a very large amount, but the variation is significant,” said lead investigator Parag Joshi, cardiology fellow, Johns Hopkins Hospital. “It confirms findings from smaller studies and raises a lot of interesting questions” – not least the cause of the fluctuations. Behavioural changes seem to be partly responsible. “In the summer, we tend to get outside, we are more active and have healthier behaviours overall,” Dr Joshi said. “In the colder months, we tend to crawl into our caves, eat comfort foods and get less exercise, so what we see is that LDL and non-HDL are slightly worse.” In addition, the limited time spent outside means less sun exposure. The resulting lower concentration of vitamin D worsens lipid profiles. However, researchers still need to identify the causes of these seasonal variations. Interactions �a significant cause’ of hospitalisations Drug-drug interactions (DDIs) are “a significant cause” of hospital admissions and visits, according to a meta-analysis of 13 studies. Overall, DDIs accounted for a median of 1.1 per cent of hospital admissions and 0.1 per cent of hospital visits (e.g. to accident and emergency). In people hospitalised for adverse drug reactions, DDIs accounted for a median of 22.2 per cent of hospital admissions and 8.9 per cent of hospital visits. Aspirin was the drug most commonly involved in interactions with other medicines, contributing to 23.5 per cent of DDIs that needed hospital admissions. Other NSAIDs accounted for 12.9 per cent of DDIs that lead to hospital admissions. Gastrointestinal tract bleeding (40.4 per cent) and cardiac arrhythmias (29.8 per cent) were the most frequent adverse events resulting from DDIs. (Pharmacoepidemiology and Drug Safety doi:10.1002/ pds.3592) Flu usually asymptomatic … Recent seasonal influenza outbreaks and the 2009 pandemic were asymptomatic in about three-quarters of those infected, a new study reports. The analysis, which covered seasonal and pandemic influenza in England between 2006 and 2011, accrued 5,448 person-seasons’ of follow-up. On average, influenza infected 18 per cent of unvaccinated people each winter. There were 69 respiratory illnesses per 100 person-seasons among those infected with influenza compared with 44 per 100 in those not infected with influ- enza, the authors say. The age-adjusted attributable rate among infected people was 23 illnesses per 100 personseasons, so up to threequarters of influenza infections were asymptomatic. The authors hope the findings will inform seasonal disease control and pandemic planning by, for example, increasing the validity of models examining the efficacy and cost-effectiveness of countermeasures, including antivirals, vaccines and behavioural interventions. (Lancet Respir Med dx.doi.org/ 10.1016/S2213-2600(14)70034-7) … but flu jabs save lives Influenza vaccination significantly reduces hospitalisations for major cardiovascular and respiratory conditions as well as lowering all-cause mortality in type 2 diabetes, according to research from Imperial College, London, presented at the Diabetes UK Professional Conference. The retrospective study collected data from the Clinical Practice Research Database for 124,503 patients with type 2 diabetes between 2003/4 and 2009/10. After adjustment, vaccination reduced hospitalisations for: • Stroke by 30 per cent • Acute myocardial infarction by 21 per cent • Heart failure by 20 per cent • Pneumonia or influenza by 15 per cent. All-cause mortality was 28 per cent lower in vaccinated compared with non-immunised people. The authors conclude that “efforts should be focused on improvements in vaccine uptake in this important target group”. New natural eczema treatment Drug interactions warning Reczema is a new natural treatment that the manufacturer Secuvie says is “clinically proven to significantly improve the symptoms of eczema and irritated skin”. According to Secuvie, Reczema calms and moisturises dry and irritated skin, forms a barrier layer and encourages “intense cellular repair” due to CHD-FA, a “pure and concentrated form of fulvic acid” that “helps cells … absorb the vital nutrients they need to heal”. PROMISE When you make one to a patient, we’ll help you keep it. That’s why every one of our 180,000 monthly telephone orders is processed in lightning-quick time. And why every one of our 500,000 deliveries is guaranteed to arrive at the same time each day. Twice if you need us. To make sure patients get their prescriptions on time, every time. We promise. We can deliver so much more to support your business – giving you back time to focus on improving patient services. Brian Deal Pharmacist, Ashwell Pharmacy 10 APRIL 2014 PHARMACY MAGAZINE Find out at www.aah.co.uk/promise or call 0844 561 8899 11_PM_0414:11_PM_0414 08/04/2014 10:17 Page 1 PROMOTION THE TERMS heartburn and indigestion are often used interchangeably. They both occur soon after eating or drinking, yet these are two different digestive symptoms. Nearly three-quarters of people in the UK suffer from both heartburn and indigestion, and nearly one in five cases suffer from both symptoms at the same time.1 Many people get confused about which symptoms they are suffering from, leading them to misdiagnose themselves. This can make it difficult for pharmacy teams to give appropriate advice and make product recommendations. Identifying the cause of the symptoms is important, as indigestion and heartburn treatments have different modes of action. indigestion can ease their symptoms by adapting their lifestyle and taking suitable OTC remedies such as antacids and alginates.5 Antacids provide immediate relief from indigestion.8 They work by neutralising excess stomach acid so that it no longer causes irritation.8 Alginates relieve heartburn and acid reflux.8 They form a protective barrier that floats on the surface of the stomach contents, keeping acid in the stomach and away from the oesophagus.8 Some medicines, such as Gaviscon Double Action, contain an alginate and antacids to tackle the symptoms of heartburn and indigestion at the same time. Heartburn versus indigestion Gaviscon Double Action is ideal for customers suffering from both heartburn and indigestion. Its powerful formula has two modes of action, offering dual relief in one product. 1. Sodium alginate forms a strong raft over the stomach contents to soothe the burning pain of heartburn.8 2. The two antacids, sodium bicarbonate and calcium carbonate, neutralise excess stomach acid to relieve the pain and discomfort of indigestion.8 In most people, heartburn and indigestion are mild and occur only occasionally.2 Sometimes they are associated with gastrooesophageal reflux disease (GORD).2,3 Heartburn is a burning pain or a feeling of discomfort behind the breastbone and at the back of the throat.4 It may be accompanied by an acid taste in the mouth.4 Symptoms occur when acid, pepsin and bile, which normally sit within the protective lining of the stomach, escape back up into the oesophagus (called reflux). The acid damages the lining of the oesophagus.5 Indigestion, also known as dyspepsia, is often used to describe a range of different symptoms.6 It tends to cause an uncomfortable or painful feeling in the upper chest or stomach, usually associated with sickness, bloating and nausea.7 Indigestion is caused by stomach acid coming into contact with the sensitive lining of the digestive system, causing irritation and inflammation.2 product champion For customers suffering from heartburn and indigestion, Gaviscon Double Action offers effective dual-action relief13,14 Gaviscon Double Action about the management of heartburn and indigestion.11 As well as making appropriate product recommendations, they can suggest lifestyle measures to relieve the symptoms, such as losing weight, stopping smoking and avoiding any trigger foods.11 Pharmacists are also ideally placed to refer customers to their GP if the symptoms are frequent or severe or don’t respond to OTC medicines. Customers can learn more about heartburn and indigestion by visiting www.gaviscon.co.uk. A definite Product Champion! Management options Heartburn and indigestion are more common in people who smoke or are overweight, and in pregnant women.5 They tend to have similar triggers, including eating rich or fatty foods, wearing tight clothes and stooping or bending forwards.5 Most people with mild to moderate heartburn and Research shows that 50 per cent more consumers enjoy fast relief with Gaviscon Liquid versus an antacid gel9 containing magnesium and aluminium hydroxide. Around 90 per cent say they would use Gaviscon Double Action Liquid again.10* Pharmacy recommendation Pharmacists play an important role in advising customers Gaviscon Double Action Key benefits to customers: • Provides dual relief from heartburn and indigestion • Liquids soothe in three minutes10 • Lasts for up to four hours, up to twice as long as antacids12 • Contains double the concentration of calcium carbonate (antacid) compared to Gaviscon Original products. • Suitable for use in pregnancy13,14 • Suitable for adults and children 12 years and over • Available in mint liquid, tablets and liquid sachets formats. Sodium alginate, Sodium bicarbonate, Calcium carbonate REFERENCES 1. Winkle, global segmentation research, 2010 2. Indigestion: Introduction. NHS Choices. 2012. www.nhs.uk/conditions/Indigestion/Pages/Introduction.aspx [accessed February 2014] 3. Heartburn and gastro-oesophageal reflux disease – causes. NHS Choices. 2012. www.nhs.uk/Conditions/Gastroesophageal-reflux-disease/Pages/Causes.aspx [accessed February 2014] 4. Heartburn and gastro-oesophageal reflux disease – symptoms. NHS Choices. 2012. www.nhs.uk/Conditions/Gastroesophageal-reflux-disease/Pages/Symptoms.aspx [accessed February 2014] 5. Information about heartburn and gastro-oesophageal reflux. Core charity. February 2011. www.corecharity.org.uk/files/files/A1213_Heartburn%20A5_AW.pdf [accessed February 2014] 6. Indigestion. British Society of Gastroenterologists. www.bsg.org.uk/patients/general/indigestion.html [accessed February 2014] 7. Indigestion: Symptoms. NHS Choices. 2012. www.nhs.uk/Conditions/Indigestion/Pages/Symptoms.aspx [accessed February 2014] 8. Indigestion – treatments. NHS Choices 2012. www.nhs.uk/Conditions/Indigestion/Pages/Treatment.aspx [accessed February 2014] 9. Chevrel B. J Int Med Res 1980; 8(4):300-2 10. Strugala V, et al. J Int Med Res 2010; 38:449-57 11. Indigestion (dyspepsia) in adults. Information for the Public. NICE 2004. www.nice.org.uk/nicemedia/live/10950/29462/29462.pdf [accessed February 2014] 12. Dector DL, Malcolm R, Maton PN, Lanza FL and Gottlieb S. Effects of aluminium/ magnesium hydroxide and calcium carbonate on esophageal and gastric pH in subjects with heartburn. American Journal of Therapeutics 2, 546-552 (1995) 13. Gaviscon Double Action Mint Tablets Summary of Product Characteristics. Date of last revision 27/1/11. Available at: www.medicines.org.uk. [Last accessed 15/11/12] 14. Gaviscon Double Action Mint Summary of Product Characteristics. Date of last revision 28/1/11. www.medicines.org.uk [last accessed 15/11/12] * based on 45 sufferers UK/G-OTC/0214/0019 Prescribing information can be found on the page overleaf This article is supported by an educational grant from Reckitt Benckiser Healthcare (UK) Limited and has been developed in partnership with Pharmacy Magazine PHARMACY MAGAZINE APRIL 2014 11 08-13_Script_PM_0414_rt.qxp:08-13_PM_0414 09/04/2014 16:27 Page 12 CLINICAL NEWS Essential information: Essential Information for Gaviscon Double Action Mint and Gaviscon Double Action Tablets Active Ingredients: Gaviscon Double Action Mint: Each 10ml dose contains sodium alginate 500mg, sodium bicarbonate 213mg and calcium carbonate 325mg. Also contains methyl and propyl hydroxybenzoates and sodium saccharin. Gaviscon Double Action Tablets: Each tablet contains sodium alginate 250 mg, sodium bicarbonate 106.5mg and calcium carbonate 187.5mg. Also contains mannitol, aspartame and xylitol. Indications: Treatment of symptoms of gastro-oesophageal reflux such as acid regurgitation, heartburn and indigestion, for example, following meals or during pregnancy, and for symptoms of excess stomach acid (hyperacidity). Dosage Instructions: Gaviscon Double Action Mint For oral administration. Adults and children 12 years and over: 10-20ml after meals and at bedtime, up to four times per day. Gaviscon Double Action Tablets: For oral administration, after being thoroughly chewed. Adults and children 12 years and over: Two to four tablets after meals and at bedtime, up to four times per day. Contraindications: Hypersensitivity to any of the ingredients, including the esters of hydroxybenzoates (parabens). Precautions and Warnings: Care needs to be taken in treating patients with hypercalcaemia, ephrocalcinosis and recurrent calcium containing renal calculi. Treatment of children younger than 12 years of age is not generally recommended, except on medical advice. If symptoms do not improve after seven days, the clinical situation should be reviewed. Due to the presence of calcium carbonate which acts as an antacid, a time-interval of 2 hours should be considered between Gaviscon intake and the administration of other medicinal products, especially H2-antihistaminics tetracyclines, digoxin, fluoroquinolone, iron salt, ketoconazole, neuroleptics, thyroxine, penicill amine, beta-blockers (atenolol, metoprolol, propranolol), glucocorticoid, chloroquine, and diphosphonates. Gaviscon Double Action Mint: Each 10ml dose has a sodium content of 127.25mg (5.53mmol). This should be taken into account when a highly restricted salt diet is recommended, e.g. in some cases of congestive cardiac failure and renal impairment. Each 10ml dose contains 130mg (3.25mmol) of calcium. Care needs to be taken in treating patients with hypercalcaemia, nephrocalcinosis and recurrent calcium containing renal calculi. Gaviscon Double Action Tablets: The sodium content of a twotablet dose is 110.75 mg (4.82 mmol). This should be taken into account when a highly restricted salt diet is recommended, e.g. in some cases of congestive cardiac failure and renal impairment. Each two-tablet dose contains 150 mg (3.75 mmol) of calcium. Due to its aspartame content this product should not be given to patients with phenylketonuria. Pregnancy and Lactation: Open controlled studies in 281 pregnant women did not demonstrate any significant adverse effects of Gaviscon on the course of pregnancy or on the health of the foetus/new-born child. Based on this and previous experience the medicinal product may be used during pregnancy and lactation. Care should be taken when recommending medicines for use in pregnancy as medicines can cross the placenta and may affect the fetus. Side-effects: Very rarely (<1/10,000) patients sensitive to the ingredients may develop allergic manifestations such as urticaria or bronchospasm, anaphylactic or anaphylactoid reactions. Ingestion of large quantities of calcium carbonate may cause alkalosis, hypercalcaemia, acid rebound, milk alkali syndrome or constipation. These usually occur following larger than recommended dosages. Retail Price: Gaviscon Double Action Mint 150ml £4.79, 300ml £7.89, 600ml £11.99, Liquid Sachets £4.99, Gaviscon Double Action Tablets: 8s £2.17; 16s £3.39, 32s £5.49. Marketing Authorisation: Gaviscon Double Action Mint PL00063/0552 Gaviscon Double Action Tablets PL 00063/0157. Supply Classification: GSL Holder of Marketing Authorisation: Reckitt Benckiser Healthcare (UK) Limited, Dansom Lane, Hull HU8 7DS. Date of Preparation Liquids: February, 2011. Date of Preparation Tablets: March, 2014. 12 APRIL 2014 PHARMACY MAGAZINE VIEWPOINT FROM UKCPA Pharmacists can help improve the suboptimal management of patients with CHD, says Rani Khatib, senior cardiology pharmacist and lecturer at Leeds Teaching Hospitals NHS Trust Supporting GTN use Coronary heart disease (CHD) is the UK’s biggest killer with an estimated 2.6m people living with the condition. NICE emphasises the importance of prescribing the appropriate secondary prevention medicines in patients with CHD and the up-titration of beta-blockers and ACE inhibitors to evidencebased target doses or maximum tolerated doses. Despite an improvement in prescribing secondary prevention medicines, up-titration of doses post-discharge is still poor. Of 37 post-myocardial infarction patients in a recent study who were followed up to six months post-discharge, 85 per cent did not have any up-titration of their beta- The team has developed a GTN advice card “ ” blocker doses, nor 47 per cent of their ACE inhibitor doses. The symptom most commonly experienced by patients with CHD is chest pain. Sublingual glyceryl trinitrate (GTN) is often prescribed to alleviate anginal chest pain but various studies have shown that not all angina patients are prescribed it – and many do not seem to know how to use it. Failure to use An evaluation of 35 patients with established CHD who were admitted to our cardiology wards revealed that 12 did not use their GTN when they had experienced chest pain, with five citing fear of side-effects as a reason. When knowledge of how to use GTN was assessed, only six patients showed full knowledge, despite being providing with various booklets and educational sessions about their CHD medicines. Advice on how to use GTN was not retained (possibly due to its infrequent use) and patients reported a lack of satisfaction with the GTN written information, which was not readily accessible, nor simple and practical. The pharmacy teams should include assessment of GTN use as part of their medicines optimisation strategy to ensure that patients who have angina are prescribed GTN, provided with correct advice on how to use it and offered a refresher on its use, possibly once a year or whenever a new GTN supply is dispensed. Verbal advice should be supported with appropriate written material. GTN advice card. To further reinforce this message the cardiac team, in collaboration with CHD patients, has developed a GTN advice card. NICE has quality assured the development of the card and made the full project available as “shared-learning” at www.nice.org.uk/shared learning. The UKCPA has also endorsed the card, which is now available for use by all healthcare professionals in primary and secondary care. Orders can be placed with the Leeds Teaching Hospitals NHS Trust Print Unit ([email protected]). For more information about the UKCPA, access www.ukcpa.org or tel: 0116 2776999 COPD linked to mild cognitive impairment COPD increases the risk of non-amnesic mild cognitive impairment (MCI), JAMA Neurology reports. Researchers followed 1,425 people aged 70-89 years with normal cognition at baseline for a median of 5.1 years. Of these, 171 had COPD at baseline, while 370 developed MCI during follow-up. COPD significantly increased the risk of non-amnesic-MCI by 83 per cent but did not significantly increase the risk of MCI or amnesic-MCI. People diagnosed with COPD for longer than five years at baseline were 58 and 158 per cent more likely to develop MCI and non-amnesic-MCI respectively. The authors suggest that inflammation, vascular disease and hypoxia could explain the link between COPD and MCI. The findings may suggest targets for “early intervention to prevent or delay the onset and progression of MCI,” especially non-amnesic impairment, they say. (doi:10.1001/jamaneurol. 2014.94) Women with AF have a high stroke risk Atrial fibrillation (AF) increases stroke risk by about five-fold. However numerous factors influence each AF patient’s risk of stroke, including a history of congestive heart failure, hypertension, diabetes, previous stroke or transient ischaemic attack; being at least 75 years of age; and, according to a new study, being female. A meta-analysis of 17 studies revealed that women with AF were 31 per cent more likely to have a stroke than men with arrhythmia. Women aged 75 years and over accounted for most of the increased risk – they were 28 per cent more likely to have a stroke than men of the same age with AF. The increased risk of stroke in women emerged in those receiving (29 per cent) and not taking (49 per cent) oral anticoagulation. The results underscore the importance of identifying and treating AF patients at the highest stroke risk, say the authors. (QJM doi:10.1093/ qjmed/hcu054) Research: pre-hypertension and stroke WHAT IS THE BACKGROUND? Previous studies assessing whether pre-hypertension – blood pressure that is just above normal – increases stroke risk have produced inconsistent results. WHAT WAS THE METHOD? A meta-analysis involving 762,393 people from 19 studies. Researchers defined low- and high-range pre-hypertension as 120-129/80-84 and 130-139/85-89mmHg respectively. WHAT WERE THE RESULTS? Pre-hypertension increased stroke risk by 66 per cent compared with blood pressure below 120/80mmHg. After controlling for other cardiovascular risk factors, low- and high-range prehypertension increased stroke risk by 44 and 95 per cent respectively. The population attributable risk – essentially the number of strokes caused by pre-hypertension – was 19.6 per cent. Results were consistent across stroke type, stroke endpoint, age, study characteristics, follow-up duration and ethnicity. WHAT ARE THE CONCLUSIONS? Even low-range pre-hypertension increases stroke risk compared with optimal blood pressure. REFERENCE This column is produced in association with the UKCPA. The views expressed are those of the author and are not necessarily those of either Pharmacy Magazine or the UKCPA Huang Y, Cai X, Li Y et al. (2014) Pre-hypertension and the risk of stroke: A meta-analysis. Neurology 08-13_Script_PM_0414_rt.qxp:08-13_PM_0414 09/04/2014 16:28 Page 13 CLINICAL NEWS Saving a minute saves almost two days “Realistically achievable small reductions” in the time between the start of symptoms and tissue-type plasminogen activator (tPA) therapy can produce “significant and robust” improvements in outcomes, says a report in Stroke. For example, a 15-minute decrease in onset-to-treatment time translated into, on average, an additional month of disability-free life. Researchers applied evidence from major tPA trials to 2,258 consecutive stroke patients from Australia and Finland. Each minute of onsetto-treatment time saved translated into, on average, 1.8 days of “extra healthy life”. The benefit of reducing onsetto-treatment time emerged in all groups assessed. For example, each minute reduction provided: • 0.6 days in old people (80 years) with severe strokes • 0.9 days in old people with mild strokes • 2.7 days in young people (50 years) with mild stokes • 3.5 days in young people with severe strokes. “�Save a minute, save a day’ is the message from our study,” says lead author Atte Meretoja associate professor of neurology, University of Melbourne, Australia. Each reduction of a minute between symptom onset and treatment may save around two million neurones. Dr Meretoja hopes that the “concrete easy-to-relate-to figures will inspire medical services to measure and improve their game for the benefit of our stroke patients. Patients should never wait a single minute for stroke signs, such as face droop, arm weakness or speech disturbance, to go away. They should call for help immediately.” Intravenous thrombolysis with tissue-type plasminogen activator (tPA) is described as “the only medical therapy shown to improve patient outcomes in acute ischaemic stroke”. (10.1161/STROKEAHA. 113.002910) No wonder patients with chronic anal fissure avoid the toilet… Heart of the matter... How old is your heart? A new website helps patients prevent cardiovascular disease (CVD) by estimating their heart’s age. The recently published Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease (JBS3) extends the focus from targeting people at high risk of a heart attack or stroke within the next 10 years to also include those whose familial and lifestyle factors indicate a low short-term risk, but a high lifetime risk. The JBS based the recommendations on growing evidence that a long pre-clinical phase precedes CVD and that most heart attacks and strokes occur in people at �intermediate’ risk. So the recommendations include a risk calculator (www.jbs3risk.com) to help healthcare professionals and patients understand and tackle cumulative lifetime CVD risk. For example, the calculator estimates the heart’s age based on current familial and lifestyle risk factors, and predicts how many more years the person can expect to live before a heart attack or stroke if they don’t take action. CHMP approval The CHMP recently approved combining insulin degludec (Tresiba), a once-daily basal insulin, and the GLP-1 receptor agonist liraglutide (Victoza). Further information is available on request from: ProStrakan Limited, Galabank Business Park, Galashiels TD1 1QH, UK. Legal Category: POM. Please consult Summary of Product Characteristics before prescribing, particularly in relation to side effects, precautions and contraindications. Information about this product, including adverse reactions, precautions, contraindications and method of use can be found at http://www.medicines.org.uk/emc/. Rectogesic® 4mg/g Rectal Ointment is indicated for relief of pain associated with chronic anal fissure. Marketing Authorization Holder: ProStrakan Ltd, Galabank Business Park, Galashiels, Scotland TD1 1QH. Date of preparation: March 2014. M011/1207. glyceryl trinitrate 4mg/g Rectal Ointment Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to ProStrakan Ltd. on 01896 664000 PHARMACY MAGAZINE APRIL 2014 13 14_pm0414_PM Questions_rt.qxp:14_PM_0413 11/04/2014 11:58 Page 18 INTERVIEW THIS MONTH: CLARE HOWARD pmquestions Talking to the personalities on pharmacy’s front line PEOPLE PROFILE Clare Howard has been involved in pharmacy since the age of 16 and studied for her degree at Aston University. She became deputy chief pharmaceutical officer for NHS England in 2013 and is married with two children. NHS England’s deputy chief pharmacist Clare Howard is leading on the medicines optimisation agenda but has strong views on a variety of issues currently affecting community pharmacy. Interview by Asha Fowells Not another buzzword There has been criticism from some quarters that medicines optimisation is simply the latest in a long line of DH catchphrases. Ms Howard is adamant that this isn’t the case. “Is it another buzzword? Absolutely not. The project recognises that we have over the last few years focused on the cost of medicines at the expense of fundamental areas that we now recognise have led to the use of medicines in this country being sub-optimal.” Medicines optimisation aims 14 APRIL 2014 PHARMACY MAGAZINE to shift the emphasis away from drug costs and towards achieving better value by supporting patients to get more out of their medicines, she explains. “Patients are clearly telling us they want more information, better consultation and to understand what services are available, particularly from community pharmacy, to help them [with their medicines],” says Ms Howard. The work will also filter through to local level, she adds. “We are in the process of developing a sort of prototype �dashboard’ with measures that aim to help CCGs think about what they need to be looking at locally, to make sure that patients in their area get the most out of their medicines.” This is clearly a huge programme of work with a broad remit. Ms Howard describes a couple of examples, such as how the programme is looking to improve services for patients with long-term conditions and support those recently discharged from IN SOME WAYS it feels like NHS England has always been around. Every month the body is in the news because of a new initiative, campaign, event or policy, and a quick glance at NHSE’s website confirms a constant stream of news stories and announcements. Certainly there has been a lot going on – yet NHS England is only one year old. A former community pharmacist and pharmaceutical adviser, Ms Howard was seconded to the Department of Health in 2012 to lead the national medicines use and procurement QIPP work stream. She was announced as chief pharmaceutical officer Keith Ridge’s deputy just ahead of the NHS reforms coming into force in April 2013. While some deputies prefer to work in the background and leave someone else to be the public face of an organisation, this has certainly not been the case for the NHS England pharmacy team. Ms Howard has been vocal on a whole range of topics affecting the profession and is also leading the work on the medicines optimisation agenda. Clare Howard on: The possibility of a new pharmacy contract One of the benefits of Call to Action was the spotlight that it shone on collaborative working. “There are some incredible examples of community pharmacy and general practice working well together for the good of their patients,” Ms Howard says. The success of repeat dispensing in the North East is a prime illustration. “It has worked really well because pharmacists and GPs have sat down together at training events to work out how this could work for their patients… The benefits are there and you see it in action in their figures.” In some instances, the differences between community pharmacy and general practice are worth exploiting, she suggests. “Look at the vaccination programmes that have been run where community pharmacy has been able to demonstrate that it can get access to patients who don’t necessarily see their GP.” Another example is the South Central respiratory project, which demonstrated a reduction in admissions and also an improvement in quality of life for patients. However the flip side is that sometimes the gap between general practice and community pharmacy feels more like a chasm, with concerns voiced in some quarters about how well the two professions can work together when their contracts are so disparate. But there may be light at the end of the tunnel. “We are exploring how the [pharmacy] contract could be better organised to support patients in primary care,” she says. With NHS England now responsible for the national contracts for both pharmacy and general practice, might we finally see some formal alignment between the two? It would be long overdue. Something no doubt for Ms Howard’s overflowing in-tray... that medication use is as safe as possible,” she says. Call to Action A national contract is often quite a blunt instrument to resolve all the issues “ ” hospital, and is clear that it sits comfortably with other NHSE priorities. “Things like the better use of EPS and electronic patient records will make sure Talk to anyone prominent in pharmacy – or even primary care – and the NHS Call to Action consultation soon crops up. It’s the major topic of the moment. And quite right too. As Ms Howard puts it: “It is the opportunity for pharmacy to help the NHS and shape the way that primary care services are organised in the future.” NHS England has been delighted with how the profession has risen to the challenge, she adds, explaining, “I am really encouraged by the sorts of things that pharmacists have put forward and have been thinking about”. What is also reassuring is the fact that the views of healthcare professionals seem aligned with what patients want, she says. “I think that some of what we are hearing chimes with what we have already heard through the medicines optimisation work, which is that patients want more support around their medicines taking.” However what is increasingly evident is the lack of public awareness of what community pharmacy can offer in addition to dispensing. Campaigns such as NHS England’s �The earlier, the better’ and Pharmacy Voice’s �Dispensing health’ clearly have an important role to play here, she says. The “conversation” phase of the community pharmacy Call to Action ended on March 18 but Ms Howard is keen to emphasise that this wasn’t a paper-pushing exercise with an already decided outcome. “We don’t want to pre-empt things… we’ll need a period of time to reflect on what’s come in.” The responses will also be considered with the Calls to Action for other areas of primary care, such as general practice and dentistry, and the review of emergency care services, she points out. Although NHS England will take its time to sift through the ideas and suggestions that have stemmed from events and online replies, Ms Howard stresses that the process is about more than just deciding overall NHS strategy. “Call to Action isn’t just about what happens nationally. It is there for [NHSE’s] area teams, who over the next few months will be developing their five-year plans around community pharmacy, primary care and out-of-hospital care in general. My sense is that area teams will be using what they have heard at their events to shape their strategies.” The trick will always be about achieving a balance between the national need for consistency while at the same time making sure that local areas have the ability to innovate and develop services, she says. “A national contract is often quite a blunt instrument to resolve all the issues.” “If we hadn’t had that local flexibility, then some of the amazing services and great innovative work that has come out of community pharmacy in recent times wouldn’t have happened. At a local level, things can happen quite quickly.” THIS INTERVIEW FIRST APPEARED IN THE APP VERSION OF THE MARCH ISSUE 15_PM_0414:15_PM_0414 11/04/2014 12:17 Page 1 17:29 16_CPPE_PM_0414_rt.qxp:16_PM_0314 10/04/2014 12:07 Page 16 LEARNING ZONE Consultation skills for pharmacy practice Effective consultations lie at the heart of delivering patientcentred care. To help you assess and develop your consultation skills, a new website (www.consultationskills forpharmacy.com) has been developed to provide easy access to a range of resources, including guidance, practice standards, learning options and assessment tools. The website, which also offers advice to employers and trainers, supports users through a six-step learning pathway: 1. Why are consultation skills important for all pharmacy professionals? Using effective consultation skills will enable you to enhance patient care, and promote the respect and recognition of pharmacy professionals among patients and other healthcare professionals. 2. How do I know what standard is expected of me? A new set of national practice standards has been prepared to define the competencies that all pharmacy professionals should aspire to. 3. How do I know how effective my consultation skills are now? There is a range of options available for you to establish how effective your current practice is when conducting medicines and public health consultations. Health Education England (HEE) and CPPE have launched new national practice standards and a Consultation Skills for Pharmacy Practice learning and development programme 4. How do I improve my performance? People learn in different ways, so a set of learning steps are recommended to enable you to achieve your development goal. 5. How can I check my learning and development? Once you have worked through your chosen learning pathway, you will be able to complete an online assessment to evaluate your knowledge and ability to identify good practice in delivering effective consultations. 6. How do I continue to develop my performance? At this stage of your learning pathway, you can access the options available for you to regularly reassess your performance and identify opportunities for further improvement. Core learning • The new distance learning programme, Consultation Skills for Pharmacy Practice: Taking a Patient-Centred Approach, has been developed to support you to assess and develop your skills. • A face-to-face workshop, Consultation Skills: Meeting the New Practice Standards for Pharmacy, is also being run by the CPPE to help you apply your knowledge and skills to practice. More information at www.consultationskillsfor pharmacy.com Contact CPPE Website: www.cppe.ac.uk Email: [email protected] General enquiries: 0161 778 4000 You can follow us on: Facebook: www.facebook.com/cppeengland Twitter: www.twitter.com/cppeengland LinkedIn: www.linkedin.com/company/centre-for-pharmacypostgraduate-education YouTube: www.cppe.ac.uk/youtube 16 APRIL 2014 PHARMACY MAGAZINE PRACTICE SCENARIO intermittent fasting Technician Lucy returns to the pharmacy after her lunch break with a magazine in her hand and a puzzled look on her face... “Can you help me get my head round this please?” Lucy asks pharmacist Parveen. “I’ve been reading in this magazine about something called 16:8 eating. Is it the same as the 5:2 diet? But that would mean that you eat for 16 days then fast for eight. It’s so confusing!” ANSWER The 16:8 diet involves restricting eating to an eighthour window each day and rose to fame when a book entitled �The 8 Hour Diet’ was published last year. The author makes many claims about this way of eating, but there is little evidence supporting such an approach to weight loss. One study in mice suggested that feeding times influenced metabolism, and while another paper pointed towards a combination of calorie restriction, exercise and intermittent fasting as a way of reversing some of the changes caused by ageing, the research team agreed that more work needed to be done to explore exactly what regimen of eating and fasting works best. The truth of the matter is that restricting the time during which someone can eat to just eight hours a day tends to limit the amount of calories that they consume. By only eating between the hours of, say 210pm each day, the individual will miss breakfast, and have a late lunch meaning they are more likely to eat a smaller dinner. Ultimately, if the number of calories being taken in is exceeded by the calories being used up, weight loss will result. email:[email protected] NPA HITS THE ROAD The NPA is running another event in Wales to help members prepare for the new GPhC inspection and ratings model. It takes place on Wednesday May 14, 7.20-9.30pm, at the Kinmel Manor Hotel in Conwy and includes a presentation from the GPhC on understanding the premises standards and inspection process and what pharmacists can expect from a visit by the inspector. PHARMA CHALLENGES The bigger picture Intermittent fasting hit the headlines when the BBC screened a Horizon documentary on the topic in 2012. The 5:2 diet quickly became popular because it is much more straightforward than many weight loss plans: eat normally for five days a week, and fast for the other two days, which must not run consecutively. The fasting days involve restricting calorie intake to just 500 per day for women and 600 for men. There is evidence supporting the health benefits of the 5:2 model. A 2010 study found that this way of eating achieved similar levels of weight loss as a more general calorie controlled diet, and there was a decrease in a number of biomarkers, which point towards a possible reduction in the risk of developing conditions such as type 2 diabetes. A 2012 study found that there may also be a reduction in the risk of developing breast cancer. However, much of the success of the 5:2 diet has been attributed to the simple fact that fasting helps people relearn what it feels like to both be hungry and full. This, in turn, makes people more aware of what they are eating on nonfasting days. Most people who follow the 5:2 diet experience a net decrease in calorie intake over the week. Extend your learning • Find out more about intermittent fasting at www.nhs.uk/ news/2013/01January/Pages/ Does-the-5-2-intermittentfasting-diet-work.aspx and www.bbc.co.uk/news/health19112549. Over half of the active products in the global industry research pipeline are personalised medicines – but the UK healthcare system is at risk of failing to adapt to this new challenge, a new report from the ABPI has revealed. The discussion paper, �Securing a Future for Innovative Medicines’, highlights further challenges including rising drug development costs and difficulty with patient recruitment for clinical trials. The UK needs to improve trial performance by enabling faster patient enrolment, encouraging the use of electronic health records and streamlining the research governance process, the ABPI says. TURBO-CHARGED NHS The NHS must achieve “turbocharged” change in the way health is delivered in England if it is to significantly improve care for patients, says Monitor. Setting out its corporate strategy for 2014-17, the regulator adds there is a growing consensus about the fundamental changes required to achieve “nothing short of a complete redesign of how care is delivered in England.” This includes integrating access to care around the needs of patients, breaking down traditional barriers between providers, doing less in hospitals and more in the community, and inventing new models of hospital care. CPD MODULE This month’s CPD module in Pharmacy Magazine is on promoting physical activity and exercise. It can be found on the centre pages of this issue. Remember to complete the pre-test, learning scenarios and post-test at www.pharmacy mag.co.uk. 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:48 Page 17 CPD MODULE the continuing professional development module 222 programme www.pharmacymag.co.uk THIS IS the two hundred and twenty second module in the Pharmacy Magazine Continuing Professional Development Programme. This module looks at promoting physical activity and exercise. Continuing professional development (CPD) is a statutory requirement for pharmacists. Journal-based educational programmes are an important means of keeping up-to-date with clinical and professional developments and can form a significant element of your CPD. Completion of this module will contribute to the nine pieces of CPD that must be recorded a year, as stipulated by the GPhC. Before reading this module, test your existing understanding of the topic by completing the pre-test at www.pharmacymag.co.uk. Then, after studying the module in the magazine, work through the six learning scenarios and post-test. Record your learning and how you applied it in your practice using the CPD report form available online and on pviii of this module. Self-assess your learning needs: • What are the recommended amounts of physical activity for adults and young people? • What is meant by �active living’? • Are you familiar with the �Let’s Get Moving’ screening questions? forthismodule GOAL To update pharmacists on the latest thinking regarding physical activity and exercise. OBJECTIVES: After completing this module you should be able to: • Provide brief interventions to help people to exercise • Explain the amount and type of physical activity needed to produce health benefit • Advise individual patients on an appropriate physical activity programme. pharmacy First in professional development Promoting physical activity and exercise Contributing authors: Professor Claire Anderson, University of Nottingham, and Professor Alison Blenkinsopp, University of Bradford Background There is strong evidence that a sedentary lifestyle is detrimental to health and that undertaking regular physical activity can improve health and prolong life. Regular activity is related to reduced incidence of many chronic conditions such as diabetes, CHD, cancer, joint disease and mental health. Regular physical activity can improve health outcomes irrespective of whether individuals achieve weight loss. Physical activity encompasses, but is not restricted to, exercise (see Table 1). The chief medical officer for England recommends that adults should achieve at least 30 minutes of moderate activity on five or more days of the week. NICE has issued guidance on four common methods used to increase the population’s physical activity levels: • Brief interventions in primary care • Exercise referral schemes • Pedometers and community-based walking • Cycling programmes. Guidance has also been issued on promoting physical activity in children and young people. magazine PULL OUT AND KEEP This module is suitable for use by pharmacists as part of their continuing professional development. After reading this module, complete the learning scenarios and post-test at www.pharmacymag.co.uk and include in your CPD portfolio. Previous modules in the Pharmacy Magazine CPD Programme are available to download from the website. LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PHARMACY MAGAZINE APRIL 2014 CPD i 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:49 Page 18 www.pharmacymag.co.uk Physical activity: any bodily movement produced by skeletal muscles resulting in energy expenditure Exercise: anything that is planned, structured, involves repetitive bodily movements and is usually undertaken during leisure time for the purpose of maintaining physical fitness Physical fitness: a set of attributes that people have or can acquire that relates to their ability to perform physical activity. These are: • Aerobic fitness: the ability of the heart and lungs to supply fuel during sustained physical activity and to eliminate waste products • Strength: the amount of external force that a muscle can exert • Flexibility: the range of motion at a joint. Intensity: the intensity of physical activity is important: • Light activities require little exertion, not causing a noticeable change in breathing • Moderate activities require sustained, rhythmic, muscular movements and leave someone warm and slightly out of breath • Vigorous activity requires sustained, rhythmic, large muscle movements at a minimum of 60-70 per cent of maximum heart rate and leaves someone sweating and out of breath. In a 2008 national survey only 39 per cent of adult men and 29 per cent of adult women met the chief medical officer’s recommendations for physical activity (encouragingly, up slightly from 35 per cent of men and 24 per cent of women in the previous survey conducted in 2004). The proportion meeting the guideline recommendations decreased steadily with age. Research has also shown that people in higher income quintiles are more likely to have participated in at least one occasion of physical activity of at least moderate intensity in the previous four weeks. Physical activity levels are strongly related to body mass index (BMI) and activity levels fall from 30 per cent among those who have a desirable BMI, to 18 per cent among those who are obese or morbidly obese (BMI over 40). Men and women with low activity levels are more likely to have a raised waist circumference compared to those with high activity levels. Within minority ethnic groups, Irish and Black Caribbean men have the highest percentage Why get involved? Table 1: Definitions Table 2: Health benefits of regular physical activity • Lower mortality from all causes • Reduced risk of developing coronary heart disease • Reduced mortality after a heart attack • Reduced risk of a heart attack in obese patients • Possible reduced risk of stroke • Prevention or delay in development of high blood pressure • Reduction of high blood pressure in people with hypertension • Greater weight loss than by dieting alone, and a better conservation of fat-free body tissue during dieting • Decreased risk of cancer of the colon • Lower risk of developing non-insulin dependent diabetes • Higher bone mass density and fewer osteoporotic fractures • Reduction in mild anxiety and depression • Sleep patterns improve meeting the current physical activity recommendations (39 and 37 per cent respectively) but were also more likely to be obese. Bangladeshis were the least active and almost twice as likely as the general population to be classified as sedentary. Only 11 per cent of Bangladeshi and 14 per cent of Pakistani women reported achieving the recommended amounts of physical activity in the previous four weeks. Among women, Bangladeshi females reported low levels of physical activity but they were also among the groups least likely to be obese. With community pharmacies increasingly involved in supporting healthy lifestyles, pharmacy teams are well placed to advise on physical activity in association with services such as cardiovascular risk assessment and weight management, as well as through signposting to support self-care and public health. Physical activity and improved health: the evidence Recent years have seen a large increase in research on physical activity and health. Table 2 contains a summary of health benefits. Physical activity has been definitively shown to play a Regular physical activity will reduce the incidence of many long-term health conditions ii CPD APRIL 2014 PHARMACY MAGAZINE Reflection exercise 1 Think about the profile of the customers and patients who use your pharmacy. How might you make use of the data on physical activity to inform your practice? new medicine service extended – again The NMS has been extended until 2014-15 pending the results of an evaluation study LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PULL OUT AND KEEP 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:50 Page 19 CPD MODULE Starting a conversation about physical activity Most members of the public do not know how much and what sort of physical activity they should be aiming for. A third of people surveyed had not heard about the recommended levels of physical activity. The majority of adults perceived themselves as fairly active, with only one in 20 considering themselves to be not at all physically active. Encouragingly, more than twothirds of adults said they would like to do more physical activity. Work commitments and lack of leisure time were the most commonly reported barriers. Improvements in health and fitness depend on the intensity (see Table 1), duration and frequency of the activity. The key questions are: • How much is good for you? • How often and how hard? • How long should each session last? The �Let’s Get Moving’ primary care screening questions can be useful (see Table 4 below). People are asked which statement most applies to them. Using these simple statements gives both you and the customer a starting point for any discussion. part in the prevention and treatment of hypertension, non-insulin dependent diabetes, osteoporosis, stroke, some cancers and depression. It can help to keep older people independent and active and reduce the incidence of falls. The key messages to convey are: • Becoming even moderately active on a regular basis can improve the health of people who are usually inactive • Physical activity does not need to be strenuous to improve health • There is no need to join a gym – �active living’ and home-based activities are just as beneficial for health. Table 3: Specific benefits of physical activity for older people • Improved muscle strength and flexibility leading to reduced risk of falls (muscle strengthening exercises) • Reduction in bone fractures (muscle strengthening exercises) • Improved memory • Improved self-esteem and confidence in performing daily tasks • Enhanced ability to live independently For people who are in the preparation or contemplation stage, find out more and make some suggestions that will fit that person’s lifestyle and preferences. Where someone is at the pre-contemplation stage, encourage further discussion in the future. Make a note on your PMR to remind you that you have had the conversation and record a suggested date for a future one. The NHS recommendations for adults aged 19-64 years and for people aged 65 years and over who are generally fit and have no health conditions that limit their mobility are the same (see Table 5). No one is too old to benefit from regular physical activity and most people can start a gentle programme without any problems. To make sure that all local health professionals are giving the same messages, it would be helpful to discuss advice on physical activity with local GP practices to agree who might need medical advice. Guidelines in the US suggest that men over 40 years and women over 50 who are planning to start a programme of vigorous activity should check with their doctor first. Exercise sessions should be postponed during illness, such as colds and flu, and care should be taken when the weather is very hot or humid. Moderate activity slightly raises the heart rate (see Table 6 for examples). Musclestrengthening activities include lifting weights, Table 4: The �Let’s Get Moving’ screening questions You do some physical activity but not enough to meet the description of regular physical activity Preparation You are not regularly physically active but are thinking about becoming more active in the next six months Contemplation You are not regularly physically active and do not intend to be in the next six months Pre-contemplation PULL OUT AND KEEP working with resistance bands, doing exercises that use body weight for resistance (e.g. pushups and sit-ups), heavy gardening (e.g. digging and shovelling) and yoga. It was thought in the past that vigorous aerobic exercise was the only sort that could have health benefits. Research has shown that this is not the case and the emphasis is now on �active living’ – the integration of moderate physical activity into daily living. Younger people are likely to need activity of higher intensity (e.g. cycling) than older people to raise the heart rate in order to gain benefit. In older age groups, brisk walking will provide sufficient intensity, likely to raise the heart rate to �training level’ in the over 50s. A further benefit of regular walking for older people is that it helps other daily activities – for example, a regular daily 30-minute walk is associated with maintaining the ability to climb stairs. Some activities can be performed at different intensities – table 6 offers a guide to using daily living activities in a programme of physical activity. The aim should be a feeling of mild fatigue after moderate activity, not exhaustion. Older people who are doing walking as their main form of activity can take the �talk test’ – if they cannot carry on a conversation while walking, they should slow down. Physical activity for children and young people When thinking about encouraging physical activity among children it is important to bear in mind that parental physical activity levels are associated with children’s activity levels. In households where both parents report high levels of physical activity, children in all age and gender groups are also more likely to report higher levels than in those households where only one parent has high activity levels. The NHS recommends that children and young people between five and 18 years of age should do at least 60 minutes (one hour) of physical activity every day, which should range between moderate-intensity activity (e.g. cycling and playground activities) and vigorousintensity activity (e.g. fast running and tennis). On three days a week, these activities should involve muscle-strengthening activities (e.g. push-ups) and bone-strengthening activities �More than two-thirds of adults said they would like to do more physical activity’ LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PHARMACY MAGAZINE APRIL 2014 CPD iii 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:51 Page 20 www.pharmacymag.co.uk Table 5: NHS recommendations for adults aged 19 years and over • At least 150 minutes (two hours and 30 minutes) of moderate-intensity aerobic activity, such as cycling or fast walking, every week, and musclestrengthening activities on two or more days a week that work all major muscle groups (legs, hips, back, abdomen, chest, shoulders and arms) OR • 75 minutes (one hour and 15 minutes) of vigorousintensity aerobic activity, such as running or a game of singles tennis every week, and musclestrengthening activities on two or more days a week that work all major muscle groups (legs, hips, back, abdomen, chest, shoulders and arms) OR • An equivalent mix of moderate- and vigorousintensity aerobic activity every week (e.g. two 30minute runs plus 30 minutes of fast walking), and muscle-strengthening activities on two or more days a week that work all major muscle groups (legs, hips, back, abdomen, chest, shoulders and arms). (e.g. running). Many vigorous-intensity activities can help meet weekly muscle- and bonestrengthening requirements (e.g. running, skipping, gymnastics, martial arts and football). Coronary heart disease People who undertake regular physical activity are less likely to die from heart disease and more likely to live longer. While the mechanism of protection is not completely understood, physical activity is likely to modify other risk factors such as body weight, decreasing blood clotting, lowering blood pressure, improving lipid profile and increasing insulin sensitivity. Obese people who take regular exercise can reduce their risk of heart disease to the same as that of exercisers of normal weight. After a heart attack the risk of death is reduced by about 20 per cent by regular physical activity. Diabetes Physical activity/exercise is now widely considered to be an integral element of diabetes management and evidence demonstrates that it can produce a clinically important improvement in glucose control in people with type 2 diabetes (in the absence of weight loss), producing an average improvement in HbA1c of between -0.4 and -0.6 per cent. Type 2 diabetes NICE gives general advice about physical activity in type 2 diabetes saying that people with diabetes should be assessed regarding: • Activity at work, and in getting to and from the workplace • Activity in domestic activities and hobbies • The possibility of formal physical exercise on a regular basis; for example: • Brisk walking for 30 minutes a day • Active swimming for one hour, three times a week. People with diabetes should be advised that physical exercise can benefit insulin sensitivity, blood pressure and blood lipid control, and should be taken at least every two to three days for optimum effect. They also need to be aware that exercise may increase the risk of acute and delayed hypoglycaemia. Pharmacists should check what the patient has been told already about appropriate blood glucose self-monitoring, additional carbohydrate and dose adjustment of glucoselowering therapy for those using insulin. Alcohol may exacerbate the risk of hypoglycaemia after exercise. There are also risks from foot damage for people with diabetes, so low impact exercise is best if this is a problem. Cancer Increased physical activity may protect against various cancers and much research has focused on colon cancer. A significant, inverse association between physical activity level and risk of colon cancer has been reported. Studies show that exercise could reduce colon cancer risk by about a quarter. By maintaining a healthy weight as well, the studies estimate that colon cancer risk could be as much as halved, compared to people who are overweight and don’t exercise. Physical activity doesn’t appear to have an effect on rectal cancer risk. Studies in breast cancer have shown a protective effect ranging from 20 to 40 per cent, so being active may lower women’s risk of developing breast cancer by between a fifth and just over a third. Womb cancer risk is also lowered by exercise, by between one-fifth to a third. There is also some evidence that exercise helps to lower the risk of prostate cancer. Moderate exercise enhances the immune system and this may be linked to a reduced cancer risk. Exercise fitness may also reduce reactivity to stress (psychosocial) and mitigate Specific health conditions and physical activity Type 1 diabetes In type 1 diabetes, NICE offers the following guidance to healthcare professionals: • Advise that physical activity can reduce enhanced arterial risk in the medium and longer term • If the person chooses to increase physical activity he/she should be advised on: • Appropriate intensity and frequency of physical activity • Self-monitoring of changed insulin and/or nutritional needs • Effect of exercise on blood glucose levels when insulin levels are adequate (risk of hypoglycaemia) or when hypoinsulinaemic (risk of exacerbation of hyperglycaemia) • Appropriate adjustments of insulin dosage and/or nutritional intake for exercise and for 24 hours afterwards • Alcohol may exacerbate the risk of hypoglycaemia after exercise. Table 6: Examples of moderate amounts of �daily living’ physical activity* Less vigorous (more time) • Cleaning windows or floors for 45-60 minutes • Decorating (painting, wallpapering) for 45-60 minutes • Gardening for 45-60 minutes • Walking a mile-and-three-quarters in 35 minutes (20 minutes per mile) – walking up a 5 per cent gradient increases energy expenditure by 50 per cent “Mall walking”, a popular group activity in the US, is becoming common in the UK with groups running at shopping centres such as the Bullring in Birmingham, The Trafford Centre in Manchester and the White Rose in Leeds • Cycling five miles in 30 minutes (10 miles per hour) • Pushing a pushchair one-and-a-half miles in 30 minutes (20 minutes per mile) More vigorous (less time) • Walking two miles in 30 minutes (15 minutes per mile) • Aqua aerobics for 30 minutes • Cycling four miles in 15 minutes (16 miles per hour) • Skipping for 15 minutes • Running one-and-a-half miles in 15 minutes (10 minutes per mile) • Stair walking for 15 minutes • “Green gyms”, where experienced leaders guide volunteers through a range of practical projects, giving them the opportunity to tackle physical jobs in the outdoors. * Roughly equivalent to 150 calories per activity iv CPD APRIL 2014 PHARMACY MAGAZINE LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PULL OUT AND KEEP 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:52 Page 21 CPD MODULE Pharmacists should seek every opportunity to promote exercise and physical activity to customers exercise programme and can be prevented by gradually increasing the level of activity to the desired level over a period of weeks. Injuries also occur when people undertake excessive amounts of physical activity, sometimes when they know they are becoming tired but want to make a last effort. Pharmacists are well placed to offer both preventive advice and treatment when minor musculoskeletal problems occur. The use of ice or heat packs (depending on the time since the injury occurred) and support aids (e.g. for knees and wrists) can help. Concerns have been expressed about the adverse cardiovascular effects of vigorous exertion and there have been well publicised cases of joggers dying from heart attacks while out exercising. However these cases of sudden death are extremely rare and they are more likely in someone who was previously sedentary and has quickly moved to vigorous exercise. The net effect of physical activity is a lower risk of mortality from cardiovascular disease. How community pharmacy can help amount recommended for �active living’ do not cause arthritis or make existing disease worse. Reflection exercise 2 How might you target those people at risk from osteoporosis with health promotion messages about physical activity? What would your message for them be? against the effects of biochemical changes associated with the stress response. This may also be linked to a reduced cancer risk but the evidence is not yet definitive. Osteoporosis Weight-bearing exercise helps to maintain bone mass. Active men and women have a higher bone density and fewer osteoporotic fractures than those who are sedentary. The mechanism is not yet fully clear because exercise, in addition to its effects on bone density, also improves muscle strength, co-ordination and balance. Physical activity thus has an important role in preventing falls as well as reducing the harm caused when they occur. PULL OUT AND KEEP Adverse effects of physical activity Musculoskeletal injuries related to physical activity often occur in the early stages of an Arthritis Regular physical activity can help to control joint swelling and pain. Activities of the type and Mental health Evidence is emerging indicating the benefits of exercise on psychological wellbeing as well as on physical health. Studies show that exercise increases self-esteem and self-efficacy (the belief that one can influence one’s own life in a positive way). Physical activity has been shown to improve mood and to enhance cognitive functioning and quality of life. Patients suffering from anxiety, stress and depression are less likely to be exercising regularly and can benefit from doing so. In depression aerobic exercise e.g. jogging and cycling, and weight training, are most likely to be beneficial but needs to be sustained over several months. Reflection exercise 3 Think about what your pharmacy is already doing to promote physical activity. How could you extend this? Which people might you target and how? If everyone adopted the recommended levels of physical activity the overall gain in health would be: • Nearly one-third of all CHD incidence avoided • One-quarter of stroke avoided • Nearly one-quarter of non-insulin dependent diabetes in over 45s avoided • Just over half the hip fractures in over 45s avoided. The informal atmosphere of a community pharmacy, together with the regular contact with the public and provision of services like vascular and diabetes screening, make it an excellent setting for this sort of health promotion advice. NICE guidance states that commissioners need to pay attention to the needs of hardto-reach and disadvantaged communities, including minority ethnic groups, when developing service infrastructures to promote physical activity. Pharmacists come into contact with many people who could benefit from increased physical activity and can also target specific groups of patients from their PMRs. Local campaigns encouraging the public to get advice on physical activity from community LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PHARMACY MAGAZINE APRIL 2014 CPD v 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:53 Page 22 www.pharmacymag.co.uk Table 7: Department of Health’s general practice physical activity questionnaire General Practice Physical Activity Questionnaire Brief interventions Brief interventions involve opportunistic advice, discussion, negotiation or encouragement. They are commonly used by pharmacists in many areas of health promotion. Interventions vary from basic advice to more extended, individually-focused attempts to identify and change factors that influence activity levels. There is sufficient evidence to recommend the use of brief interventions in primary care. Physical activity – NICE recommendations 1. Primary care practitioners should take the opportunity, whenever possible, to identify inactive adults and advise them to aim for 30 minutes of moderate activity on five days of the week (or more). They should use their judgement to determine when this would be inappropriate (e.g. because of medical conditions or personal circumstances). They should use a validated tool, such as the Department of Health’s general practice physical activity questionnaire (see Table 7), to identify inactive individuals. 2. When providing physical activity advice, primary care practitioners should take into account the individual’s needs, preferences and circumstances. They should agree goals with them. They should also provide written information about the benefits of activity and local opportunities to be active. They should follow them up at appropriate intervals over a three- to six-month period. Date……………………… Name…………………….. 1. Most people who currently are sedentary say that lack of time, lack of facilities and costs are Reflection exercise 4 Check the signposting list in your pharmacy. What does it contain regarding physical activity opportunities? Look up local authority and primary care organisation websites to find out what is available (e.g. free swimming, green gyms, walking groups, chair-based exercise). Please tell us the type and amount of physical activity involved in your work. Please mark one box only a I am not in employment (e.g. retired, retired for health reasons, unemployed, fulltime carer etc.) b I spend most of my time at work sitting (such as in an office) c I spend most of my time at work standing or walking. However, my work does not require much intense physical effort (e.g. shop assistant, hairdresser, security guard, childminder, etc.) d My work involves definite physical effort including handling of heavy objects and use of tools (e.g. plumber, electrician, carpenter, cleaner, hospital nurse, gardener, postal delivery workers etc.) e My work involves vigorous physical activity including handling of very heavy objects (e.g. scaffolder, construction worker, refuse collector, etc.) 2. During the last week , how many hours did you spend on each of the following activities? Please answer whether you are in employment or not Please mark one box only on each row None Some but 1 hour but 3 hours or less than less than more 1 hour 3 hours d Physical exercise such as swimming, jogging, aerobics, football, tennis, gym workout etc. Cycling, including cycling to work and during leisure time Walking, including walking to work, shopping, for pleasure etc. Housework/Childcare e Gardening/DIY 3. How would you describe your usual walking pace? Please mark one box only. a b c Advice on getting started vi CPD APRIL 2014 PHARMACY MAGAZINE pharmacies raise awareness of pharmacists’ role and increase customer loyalty. Pharmacies can also make sure their lists of local facilities and services for signposting include those involving physical activity. Slow pace (i.e. less than 3 mph) Steady average pace Brisk pace Fast pace (i.e. over 4mph) LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PULL OUT AND KEEP 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:54 Page 23 CPD MODULE the main barriers. Community pharmacists are well-placed to advise on types of physical activity to fit with the person’s lifestyle and existing commitments. It should be borne in mind that while some people prefer exercise as a solitary activity, others may welcome a social component. Find out what activities are available locally. Examples might be walking schemes, cycling programmes, outdoor gyms or gentle exercise classes for older people. Should pharmacists wait to be asked for advice on physical activity? Helping people to keep going with physical activity Many people drop out of physical activity programmes, even when they started with enthusiasm and the best of intentions. As with medicines, non-compliance or non-adherence to physical activity routines is widely recognised to be a problem. People need physical and/or psychological goals to motivate them to continue with a physical activity programme. Getting someone Planning pharmacy-based support for physical activity Rather than seeing physical activity as a �campaign’, it should be thought of as a longterm input. Targeting patients from PMRs (e.g. those with angina, hypertension, osteoporosis) can be done gradually over a long period of time to control the rate and numbers of people offered advice. To help ensure that the same messages are given throughout the healthcare team: • Find out what your local primary care organisation’s policy is concerning physical activity • Use leaflets (e.g. patients targeted from PMRs) • Respond to requests for advice about exercise • Suggest that the person keeps an exercise diary to monitor his/her progress • Encourage follow-up by visits to the pharmacy so progress can be monitored. Pharmacy teams can use the “4 A’s” to individualise advice: Assess – what is the current level and type of physical activity? Does the patient need to do more? Advise – might they prefer an �active living’ approach or organised exercise sessions? Assist – have leaflets available with simple guidelines on increasing physical activity; also have details on-hand of local facilities Arrange follow-up – invite the person to come back to tell you how they are doing. Pharmacists are sometimes concerned that a customer might object if they are offered advice without having asked for it. However research has shown that the vast majority of people offered health advice in community pharmacies welcomed it and many would never have thought to ask for it. This lack of awareness that pharmacists have a lot to offer in terms of general health advice can only be changed if pharmacists and their staff become more proactive. The way in which advice is offered is also important, and introducing the subject by saying that your pharmacy is taking part in local initiatives to improve health can break the ice. who was previously sedentary to take up and maintain simple lifestyle activities is more likely to produce a sustained change than starting a vigorous exercise programme that requires attendance at exercise classes. The costs of an �active living’ approach are also considerably less. People who take up a home-based physical activity programme are more likely to stick to it than those required to attend a health club or leisure centre. To avoid possible injuries and muscle soreness, activity should be increased gradually. For older people, for example, increasing walking distance by an additional two minutes every other week has been suggested. Careful stretching of key muscles before and after unaccustomed activity, such as gardening or decorating, can help. Wearing well-fitting and comfortable shoes with good arch support is important for walking. Keeping a diary to record the activity undertaken and progress towards goals (e.g. weight loss) has been shown to increase adherence. Pharmacists can help by asking about progress and encouraging continued participation. Flagging the PMRs of patients to whom you give advice about physical activity will provide a reminder to ask them how they are doing when they next come into the pharmacy for a prescription. Norfolk folk get fit... In Norfolk community pharmacies have been working with national and local sports organisations to develop a series of community walking groups and activities to encourage physical activity for people aged 50 years and over. The programme is promoted through community pharmacies in conjunction with lifestyle advice and health services such as cholesterol testing, health checks and MURs. Over 2,700 people have registered with the programme and more than 1,100 events have taken place. In September 2013 a referral scheme was launched in the Broadlands area of Norfolk. Pharmacists in this area are able to refer patients directly to an �Active Broadlands’ co-ordinator for assessment and a fully funded and supervised exercise programme. Pharmacy Magazine’s CPD modules are available on Cegedim Rx’s PMR systems, Pharmacy Manager and Nexphase. Just click on the �Professional Information & Articles’ button within Pharmacy KnowledgeBase and search by therapy area. Please call the Cegedim Rx helpdesk on 0844 630 2002 for further information. Note: the content of this module remains the copyright of Pharmacy Magazine and cannot be reproduced without permission in the form of a valid licence granted after July 1, 2011. PULL OUT AND KEEP LEARNING SCENARIOS FOR THIS MODULE AT WWW.PHARMACYMAG.CO.UK PHARMACY MAGAZINE APRIL 2014 CPD vii 17-24_CPD Module_PM_0414_rt.qxp:00-00_PM_0414 07/04/2014 11:54 Page 24 www.pharmacymag.co.uk Pharmacy Magazine CPD record PROMOTING PHYSICAL ACTIVITY & EXERCISE April 2014 Use this form to record your learning and action points from this module on Promoting physical activity & exercise and include it in your CPD portfolio and record online at www.uptodate.org.uk 1. There is good evidence that physical activity can prevent death or prolong survival in which of the following? a. Osteoporosis b. Stroke c. People who have had a myocardial infarction d. Breast cancer 2. Which is NOT one of the 4A’s of health promotion advice? a. Address the agenda b. Assess the person’s level c. Advise on an approach d. Arrange follow-up 3. Which is the FALSE statement regarding regular physical activity? a. The risk of death from stroke is reduced b. The relative risk of death from heart disease is reduced c. Blood pressure is reduced in hypertensive individuals d. Half of all CHD incidence would be avoided if people adopted recommended levels of exercise 4. Which is TRUE? Current NHS guideline-based recommendations on physical activity for adults recommend: a. The same amount and type of physical activity for adults aged over 19 years b. 150 minutes each week of moderate or vigorous intensity activity dependent on age c. 90 minutes of vigorous activity d. Muscle-strengthening activities that work all major muscle groups once a week Activity completed. (Describe what you did to increase your learning. Be specific) (ACT) 5. Identify the TRUE statement: a. Physical activity should not be advised for people over 80 b. Older people undertaking regular physical activity are less likely to have a fall c. Aerobic exercise is more beneficial than other types of exercise in preventing falls in older people d. Most hip fractures would be avoided if people adopted recommended levels of physical activity Date: Time taken to complete activity: What did I learn that was new in terms of developing my skills, knowledge and behaviours? Have my learning objectives been met?* (EVALUATE) 6. Which statement about brief interventions is FALSE? a. There is sufficient evidence to recommend the use of brief interventions in primary care b. Pharmacists should use a validated tool to identify inactive individuals c. Pharmacists should provide written information about the benefits of activity and the local opportunities to be active d. Pharmacists should follow up people annually How have I put this into practice? (Give an example of how you applied your learning) Why did it benefit my practice? (How did your learning affect outcomes?) (EVALUATE) 7. Which is an example of moderate physical activity? a. Cleaning windows or floors for two hours b. Painting/wallpapering for a day c. Gardening for an afternoon d. Walking a mile-and-threequarters in 35 minutes Do I need to learn anything else in this area? (List your learning action points. How do you intend to meet these action points?) (REFLECT & PLAN) 8. Which cancer risk does physical activity NOT appear to have an effect on? a. Colon cancer b. Breast cancer c. Rectal cancer d. None of the above * If as a result of completing your evaluation you have identified another new learning objective, start a new cycle. This will enable you to start at Reflect and then go on to Plan, Act and Evaluate. This form can be photocopied to avoid having to cut this page out of the module. Complete the learning scenarios at www.pharmacymag.co.uk ENTER YOUR ANSWERS HERE Please mark your answers on the sheet below by placing a cross in the box next to the correct answer. Only mark one box for each question. Once you have completed the answer sheet in ink, return it to the address below together with your payment of £3.75. Clear photocopies are acceptable. You may need to consult other information sources to answer the questions. 1. a. b. c. d. 2. a. b. c. d. 3. a. b. c. d. 4. a. b. c. d. 5. a. b. c. d. 6. a. b. c. d. 7. a. b. c. d. Name (Mr, Mrs, Ms) Business/home address Town Postcode Tel GPhC/PSNI Reg no. I confirm the form submitted is my own work (signature) Please charge my card the sum of £3.75 Name on card Card No. Date viii CPD APRIL 2014 PHARMACY MAGAZINE Visa Start date Switch/Maestro Issue Number Mastercard Expiry date Switch/Maestro 8. a. b. c. d. Processing of answers Completed answer sheets should be sent to Precision Marketing Group, Precision House, Bury Road, Beyton, Bury St Edmunds IP30 9PP (tel: 01284 718918; fax: 01284 718920; email: cpd@precisionmarketing group.co.uk), together with credit/debit card/cheque details to cover administration costs. This assessment will be marked and you will be notified of your result and sent a copy of the correct answers. The assessors’ decision is final and no correspondence will be entered into. 222 PULL OUT AND KEEP 25_NPA-RPS_PM_0414_rt.qxp:25_PM_0514 11/04/2014 16:32 Page 25 OPINION SOCIETY SPOTLIGHT OTCPRODUCTNEWS NPA VIEW NPA launches consultation on wholesalers regional matters What do you think of your wholesalers’ service standards, asks Gareth Jones, NPA public affairs manager THE NPA HAS LAUNCHED a member consultation on pharmaceutical wholesaler service standards. The purpose is to: • Gather data about wholesaler service standards generally, against the backdrop of limited distribution and direct-topharmacy supply arrangements • Create tools with which NPA members can measure and benchmark the performance of their wholesaler/s. NPA members will then be in a better position to challenge poor service or acknowledge good service – and to make informed choices, where choice exists • Inform wholesalers about how their service is viewed by NPA members. Our starting point is to ask members to endorse or modify the performance framework laid out in our consultation document. We suggest the following as service principles against which to assess performance: • Fairness (e.g. any surcharges should be proportionate and linked to the value of service provided) • Responsiveness (e.g. responding promptly to queries or complaints) • Timely communication (e.g. proactively notifying a pharmacy at the point of ordering if the wholesaler is unable to supply a product) • Efficiency (e.g. reliable, regular and frequent supply) • Transparency (e.g. describing in detail why a quota has been set at a certain level). NPA members can answer consultation questions online at: npa.co.uk/independents-voice/consultations/wholesalers. Positive developments Members can also access a medicines supply chain toolkit (see last month’s column), which includes a branded product availability chart (showing which wholesalers supply the product of those manufacturers that use direct-to-pharmacy or restricted wholesaler schemes), a list of the medicines currently subject to supply problems and a patient leaflet explaining the background to medicines shortages, in the event of difficulties supplying to a patient in a timely fashion. The wholesaler consultation and the toolkit both result from recommendations of the Manifesto for Independent Community Pharmacy task groups. A manifesto progress report will be presented at the NPA conference in London on Sunday June 8. NPA members can register at npa.co.uk/conference2014. The NPA is now consulting on wholesaler service standards “ ” FEVER’S RISING BIG DEBATE: SHOULD YOU STOCK E-CIGARETTES? SEE P26 Including a community pharmacy pilot in the Scottish Patient Safety Programme (SPSP) is great news, says Professor John Cromarty, Scottish Pharmacy Board chair PHARMACY IS OFTEN described as a risk averse profession, contrasted, for example, with the medical profession’s approach to dealing with uncertainty. However there are strengths in pharmacists’ ability to detect errors in their scrutiny of prescriptions and in their advice on drug interactions that provide important protection for patients. With the Public Bodies (Joint Working) (Scotland) Bill now approved by the Scottish Parliament, it will become even more crucial that pharmacists’ contribution to medicines safety is integrated within the wider health and social care system. Access and input into a shared patient record is clearly important in enabling effective collaboration and partnership working between health and social care professionals in order to improve patient care. Positive impact Within community-based care, there is a particular opportunity for pharmacists to become more fully involved in the relevant parts of the Scottish Patient Safety Programme (SPSP). This was launched in 2008 to reduce adult mortality and adverse events in acute hospitals by the end of 2012. In that time mortality was reduced by 12.4 per cent across Scotland. However, while that was the programme’s key aim, it also demonstrated a real positive impact for patients, such as reduced infection rates and reliability in the completion of surgical checklists that are a key part of the care of patients receiving any surgical procedure. The programme was recently awarded funding from the Health Foundation to test the expansion further into community pharmacy. Mortality was reduced by 12.4 per cent “ ” Great news The inclusion of the community pharmacy pilot in the SPSP is great news. Full inclusion of community pharmacy in medicines reconciliation, particularly when patients enter and return from other care settings (e.g. hospital or care home), will provide more clear information for all professionals involved. This will improve safety and overall patient care. The Scottish Government’s increased focus and acknowledgement of the clinical and patient-facing role of pharmacists can only be welcomed, but it will be crucial that we get patients’ buy-in and understanding of the expert input on medicines that pharmacists can provide. The number of hay fever sufferers is set to more than double to 31.8 million by 2030, leading pollen expert Dr Jean Emberlin has warned in a new report sponsored by Opticrom Hayfever Eye Drops. The report claims that as a result of pollution and climate change, up to 45 per cent of people in big cities like London are expected to suffer from hay fever in the next two decades. In a survey of 2,000 UK adults by Opticrom, nearly a third reported worsening symptoms over the past few years. GOT THE ITCH? New emollient range XeraCalm A.D from Eau Thermale Avene by Pierre Fabre has been found to reduce itching by up to 97 per cent in a study of 32 children with eczema. A survey of eczema sufferers and parents of children with eczema commissioned by the company revealed that itching was the most troublesome symptom (81 per cent), followed by dryness (60 per cent) and redness (43 per cent). One in ten adult sufferers had never found an effective treatment and 61 per cent of parents had applied aqueous cream to their child’s eczema. XeraCalm A.D contains I-modulia, which has been shown through in-pharmacological testing to reduce inflammation and increase the skin’s innate immunity, says Pierre Fabre. BE HAIR AWARE Hair loss supplement Nourkrin is sponsoring the National Hair Aware Campaign throughout 2014. The brand will be reaching over 35 million people through a £1 million investment, including TV, radio and print advertising. POS material and educational materials will be mailed to community pharmacies. In a consumer trial of 3,000 Nourkrin users, 90 per cent noticed a visible improvement in their hair after six months. Approved by EFSA, Nourkrin contains a drug-free formulation called Marilex, which contains substances similar to those found naturally in the scalp. . More product news on p39 PHARMACY MAGAZINE APRIL 2014 25 26-27_Debate_PM_0414_liz_rt.qxp:26-27_PM_0414 10/04/2014 16:25 Page 26 FORUM THE BIG DEBATE YOUR COMMENTS Where do you stand on pharmacies selling e-cigarettes? Email [email protected] Should we be stocking e-cigarettes? E-cigarettes are one of the most controversial products ever to hit pharmacy shelves – but do they belong there? Chris Chapman investigates BACKGROUNDER Regardless of where you stand on the e-cigarette issue – and it’s certainly a hugely controversial issue that has divided pharmacy – there’s little doubt that they’ve taken the UK by storm. E-cigarettes have hit the shelves in Boots, LloydsPharmacy, Tesco, Superdrug and Asda and, increasingly, independent pharmacies are getting in on the act too. According to market research company IRI, the e-cig market in the UK is worth a staggering £100m in just traditional pharmacy and grocery outlets alone. And, with pop-up shops, market stalls and other, less traditional operators grabbing a slice of the action, it’s likely the market value is far higher. “They are a godsend for independent grocers,” remarks IRI’s retail head of strategic insight Martin Wood, “but e- cigarettes are still a pin-prick in the tobacco market.” The market Context is key. The £100m seen in community pharmacy and grocery outlets is almost a match for traditional stopsmoking products (worth around £125m in the UK) but only about 5 per cent of the total e-cigarette market. However, that is nothing compared with the tobacco market, worth anywhere between £15bn and £25bn a year. This growth area is attracting major players who may be unwelcome bedfellows on pharmacy shelves; for example, Phillips, pharmacist and contractor, Hertfordshire YES Graham I believe community pharmacy has a bright future based upon our core safe-supply role, combined with medicines optimisation and public health. Key to the last of these is smoking cessation – a passion of mine since NRT first went OTC in the 1980s, at a time when the NHS abdicated any responsibility for cessation. My local primary care group (PCG) established smokingcessation services more than 10 years ago, and I was the smoking lead, training local GPs. So it may surprise you that I believe pharmacies should stock e-cigarettes. I want pharmacy to be the �go to’ place for quitting. And while I’m entirely in favour of licensing e-cigarettes, if we 26 APRIL 2014 PHARMACY MAGAZINE wait for licences to be granted we will have missed the boat. Consumers – they don’t see themselves as patients because they are not ill – will simply go elsewhere for the products and we will lose out, just as we have in the vitamins and health food markets. Let’s have a nationallycommissioned pharmacy smoking cessation service. That said, we must remember not to take a paternalistic attitude to the public’s health, or we render ourselves irrelevant as healthcare providers. We don’t just lose the sales; we lose the opportunity to help people make healthy choices. Pharmacy has a wider tendency to be over-cautious. We sometimes seem so worried about not doing If we wait for licences to be granted we will have missed the boat “ ” Why do we need 100 variations of what is essentially the same service? And let’s have a national NHS PGD for varenicline. harm that we risk not doing good. This is the same riskaverse psychology that allowed nurses to be NHS prescribers years before Vype is owned by British American Tobacco. “You have to set the e-cigarette market’s [growth and] size against the lack of growth in the OTC market, and the contracting but enormous tobacco market,” Wood explains. “Now the big boys are muscling in.” With such heavy hitters – with heavy advertising budgets – ready to enter the market, pharmacists will need to ask themselves whether they are comfortable about where their money goes when they stock e-cigarettes. Effectiveness pharmacists; we lacked confidence. Many of us will remember when NRT could not be supplied to pregnant women due to the concern about risk to the unborn child. This was looking through the wrong end of the telescope. The question we should have asked then was: “Which is safer in pregnancy: continuing to smoke or using NRT?” Today’s question should be: “Which is safer – smoking or e-cigarettes?” It’s a nobrainer. Another thorny issue is that of effectiveness. Currently e-cigarettes are not health products regulated by the MHRA and make no claims about helping smokers to quit. Yet advocates are clear that they consider e-cigarettes a reduced-harm option that can help people quit smoking for good. This is a situation only likely to be compounded by the EU’s Tobacco Products Directive, which will see e-cigarettes not sold and regulated as medicines classed as tobacco products. The problem is that, as yet, the evidence doesn’t support 26-27_Debate_PM_0414_liz_rt.qxp:26-27_PM_0414 10/04/2014 16:26 Page 27 FORUM “ This growth area is attracting major players who may be unwelcome bedfellows on pharmacy shelves Johnson, senior medicines information pharmacist, Newcastle-upon-Tyne NO Hayley Selling cigarettes for the treatment of asthma was not, with hindsight, pharmacy’s greatest moment. But sell them we did, and they were, staggeringly, a pharmacy staple until 1985. Of course, we know now that smoking cigarettes is more likely to significantly worsen asthma than treat it, thanks to the emergence of robust, scientific research and consensus. Asthma cigarettes are now an interesting – if embarrassing – part of pharmacy history. Could e-cigarettes be leading the profession down a similarly dangerous path? At the moment, we just don’t have enough research to know for certain. We can reasonably theorise that they are probably safer than cigarettes, but without good, robust safety and efficacy data, we simply don’t know. ” this concept. Last month a longitudinal analysis of 949 smokers, of whom 88 were using e-cigarettes, was published in JAMA Internal Medicine. It found that although 85 per cent of smokers using ecigarettes reported using them to quit, they were no more successful in their quit attempts than non-users a year later. The dilemma The question facing the profession is whether they have any place in community glycol and other excipients known to be harmful through inhalation are present in many e-cigarette products, and their longterm safety is unknown. Under what circumstances can we sell these products in a pharmacy? They aren’t regulated as medicines, so we can’t make any claims that they act as nicotine replacement therapies. We are therefore selling them for recreational use. Is this a suitable precedent to set for pharmacy? It leaves us The more we know about e-cigarettes, the less rosy the picture is looking “ medical literature. Poisons centres worldwide are dealing with cases of accidental nicotine poisoning due to ingestion of nicotine refills. Propylene pharmacies today – or whether we wait to see what the MHRA, and the evidence, says. ” in an awkward ethical situation. While e-cigarettes are undoubtedly a useful product for many – there is a vociferous, passionate Effectiveness and concerns about their safety aside, there is a clear consumer demand for the products that shows absolutely no signs of lessening. And while major tobacco companies are taking over the market, this is ultimately a side issue: there is little doubt e-cigarettes are less harmful than traditional tobacco cigarettes themselves. Are all the cries of “probably safer” and “maybe more effective” enough for us as a profession to hang our hats on? The more we know about e-cigarettes, the less rosy the picture is looking. Several studies have suggested that they often contain different levels of nicotine to that claimed. A small German study suggests they may cause indoor air pollution. Cases of fatal ingestion of e-cigarette refill liquid have been emerging in the community supporting their use – their unregulated nature is limiting their promise. As healthcare professionals, we should be vocally supporting the need for research before encouraging their wider adoption by the public. At the moment, the e-cigarette situation leaves us with more questions than answers. We should be demanding the evidence before we throw ourselves headlong into another potential asthma cigarette situation. COMMENTARY The ultimate NRT? By Darush Attar-Zadeh, smoking cessation trainer and clinical leader for the respiratory pathway redesign project at Barnet CCG TABLE 1. E-CIGARETTES – THE CURRENT STATE OF PLAY Company/organisation Policy When? Asda Boots British Medical Association Co-operative Pharmacy LloydsPharmacy NPA NICE Stocks Stocks Regulate Stocks Stocks Regulate Against MHRA Morrisons Rowlands RPS Sainsbury’s Superdrug Tesco Regulate Stocks Stocks Regulate Stocks Stocks Stocks Introduced April 2013, now in 90 per cent of stores Introduced February 2014 – Puritane only Supports regulation and ban in public spaces Introducing products April 2014 Introduced December 2013, initially in 20 per cent of stores Supports regulation Recommends NRT due to lack of evidence on safety and effectiveness as a stop-smoking aid Supports regulation; will licence from 2016 Introduced April 2012, now in 99 per cent of stores Vype only Supports regulation; seeking a consensus Introduced July 2012, now in 99 per cent of stores Introduced, first as trial, 2012, now in 98 per cent of stores Introduced end of 2012, now in 99 per cent of stores Data: IRI UK Are e-cigarettes the ultimate NRT? They certainly could tick a lot of boxes that help smokers to stop or reduce their cigarette usage since they have the capacity to raise the blood level of nicotine quickly (by at least 10ng/ml in 10 minutes), they come in a formulation that avoids local side-effects and they incorporate sensory properties and behavioural rituals of the kind that help to make cigarette smoking so attractive. Sales of e-cigarettes are growing at an exceptional rate. If, ultimately, this leads to more people quitting smoking or reducing harm, then it has to be a positive outcome. But there are a few things that concern me about e-cigarettes: • They could be seen as undermining the smoke-free policy by confusing the issue of what is and isn’t allowed indoors • They could normalise vaping (especially among the young) and may be a precursor to smoking • Selling e-cigarettes in pharmacies may give the public the impression that they are safe and tested. If we are selling these items, then it’s very important we are able to discuss the technique, dose, side-effects, cautions, contra-indications and duration of course. We can do this with licensed treatments because they have gone through rigorous clinical trials. So I look forward to a day when we can start recommending licensed e-cigarettes that don’t undermine our smoke-free legislation. PHARMACY MAGAZINE APRIL 2014 27 28_Therapeutic Update_PM_0414_rt.qxp:28_PM_0414 07/04/2014 15:07 Page 28 CLINICAL PRACTICE THERAPEUTIC UPDATE LEARNING OBJECTIVE After reading this article you should be able to: • Appreciate the important role pharmacy teams can play in ensuring patients are able to use their asthma and COPD inhalers correctly Is your technique letting you down? What chance do patients have to manage their asthma and COPD properly when most healthcare professionals are unable to demonstrate how to use inhalers correctly? Mark Greener reports EFFECTIVE MANAGEMENT of asthma and chronic obstructive pulmonary disease (COPD) depends on good inhaler technique. Yet despite a proliferation of devices – most recently the dry powder inhaler (DPI) Relvar Ellipta – patients often experience problems that undermine the effectiveness of these potentially lifesaving therapies. To add to their woes, most healthcare professionals don’t get the technique right either. Now a new initiative aims to tackle this pervasive problem. Numerous studies highlight the scale of the problem posed by poor inhaler technique. One review reported that only between 23 and 43 per cent of patients got all the steps right when using a metered dose inhaler (MDI). Just 55-57 per cent of those using a spacer with a MDI and 53-59 per cent of those using a DPI performed all the steps correctly1. Moreover, 10-15 per cent of people aged 20 to 40 years made a mistake using their DPI that affected the amount of drug they inhaled. This proportion increased to 40 and 60 per cent among people aged more than 60 and 80 years respectively2. They are not alone. According to Rita Bali, a pharmacist and executive development officer for Cambridgeshire and Peterborough LPC, 90 per cent of healthcare professionals (HCPs) cannot demonstrate inhaler technique correctly to their asthma and COPD patients. A recent study revealed that just 7 per cent of 150 HCPs in primary and secondary care – including doctors, nurses and community pharmacy staff – got all seven steps needed for correct MDI technique right and showed appropriate, objectively 28 APRIL 2014 PHARMACY MAGAZINE Rita Bali measured, inspiratory flow. Only 9 per cent of the 113 HCPs who said they taught inhaler technique could demonstrate all seven steps3. “Time and time again, poor inhaler technique emerges as an GPs, respiratory nurses and community matrons – on the Isle of Wight received training in inhaler technique. Community pharmacists who received MUR payments trained patients. After training, emergency admissions for asthma fell by 50 per cent (41 to 20 over three months) and deaths by 75 per cent, from eight to two over the same time. (To put these figures into context, the Isle of Wight’s population is around 142,000.) Initial results also suggested that prescriptions for selective beta-agonist and corticosteroids declined by 25 and 5 per cent respectively – trends that seem to be continuing4. 90 per cent of HCPs cannot demonstrate correct inhaler technique to their patients “ issue in the sub-optimal care of people with asthma or COPD,” says Monica Fletcher, chief executive of the charity Education for Health. “Inhaler technique often gets forgotten, particularly when time is limited. Indeed, with so many people typically involved with the care of patients, many HCPs think that someone else has trained the patient. So community pharmacists and their staff have a vital role in improving inhaler technique.” ” Against this background, a new programme developed by Napp Pharmaceuticals and Education for Health aims to both train HCPs in correct inhaler use and work with CCGs to audit outcomes. During the training programme, Education for Health “concentrates on what’s happening at a local level” and Training to make a difference Effectively and efficiently training patients and professionals is essential to enhance inhaler technique and improve outcomes. Recently, for example, multidisciplinary teams – including Monica Fletcher INTEGRATED APPROACH IN PETERBOROUGH An ongoing project in Peterborough is developing an integrated approach to asthma management between hospital and community. After patients are discharged from hospital following a severe asthma attack, community pharmacists perform regular MURs to check inhaler technique. Initial results should be available later this year. “I really hope we’ll see that we prevent readmissions due to poor inhaler technique,” says Rita Bali. “I also hope the project will help hospital and community teams to work more closely together to help people with asthma and COPD.” prioritises teaching on inhalers that are in local formularies, says Monica Fletcher. Teaching sessions cover all the devices on the market, not just those sold by Napp. The meetings also look at ways to optimise the effectiveness of local primary healthcare teams, such as the interaction between practice nurses and pharmacists. That said, there’s a lot of ground to cover. There are currently around 15 inhaler devices available and still more to come to market, says Monica Fletcher. “I believe we need innovation,” she says, “but with so many available, it will get more and more confusing for HCPs and patients alike. The hope is, one day, a company will develop the perfect device but it seems we’re not there yet. So pharmacists and other HCPs need to understand and be able to teach how to use a range of inhalers.” Rita Bali agrees that community pharmacists need to keep up to date about the various inhaler devices. “Pharmacists should be the experts on new medicines. They should understand the subtle nuances of the different devices.” Community pharmacists should use this expertise to aid the development of local formularies, she adds. Piloting a new course in inhaler training Pilot programmes with community pharmacists started last December in Gateshead, and Cambridgeshire and Peterborough CCG (see panel). “Community pharmacists generally have more contacts with patients than any other HCP,” Rita Bali told Pharmacy Magazine, “so they are ideally placed to demonstrate inhaler technique to their patients. We received very good feedback from the participants. “The meeting was oversubscribed and we plan to run further training sessions. There is definitely an interest in improving knowledge about inhaler technique and a recognition that intervention by community pharmacists can make a difference.” Monica Fletcher adds that a pharmacist or other HCP should sign off on the patient’s management plan that he or she has received inhaler technique training – something pharmacists could do during MURs or when counselling patients when they receive a new device. “Checking inhaler technique improves the quality of the intervention without adding a burden to community pharmacists,” says Rita Bali. Patients’ ability to use an inhaler correctly gradually declines, so community pharmacists should check patients’ technique “as often as possible, and certainly at least annually”, she says. Monica Fletcher believes companies should offer more placebo inhalers and says HCPs also need anatomical teaching aids (e.g. images of lung deposition) to show the importance of the correct inhaler technique. She also believes there is a growing role for technology, such as an iPhone app that ensures people use the inhaler correctly by recording the breathing sound. “Patients often don’t realise why good inhaler technique is so important,” she comments. “It is essential to ensure that asthma and COPD patients get the most benefit from drugs. A HCP wouldn’t start a patient on insulin without explaining how to use a pen device. GPs, nurses and pharmacists need to take inhaler use much more seriously.” REFERENCES 1. Health Technology Assessment 2001; 5:26 2. Lancet 2010; 376:803-13 3. Thorax 2010; 65:A117 4. Pharmacy management 2009; 25(3):15-19 29-32_Headache_PM_0414_rt.qxp:29-32_PM_0414 08/04/2014 13:29 Page 29 HEADACHE & MIGRAINE Key facts • Migraine affects 8m people in the UK • Some pharmacy staff lack confidence when it comes to recommending sumatriptan • People who take painkillers on a regular basis are at risk of developing medication overuse headache “ Migraine is under-diagnosed and under-treated in at least half of patients By Francesca Robinson Head hunter Which? showed that pharmacy staff are not offering migraine sufferers adequate advice. So how can they get ahead? MOST HEADACHES, including migraine, although debilitating for the sufferer, aren’t serious and can be treated with OTC remedies and self-care. However the recent Which? report found that nearly a quarter of pharmacy staff, in particular medicine counter assistants, were unsure about the sales procedure for OTC sumatriptan (Imigran Recovery) and the advice they should be offering migraine sufferers. In some cases the mystery shoppers, posing as ideal candidates for the medication, were unnecessarily referred to their GP. Other research shows that migraine is under-diagnosed and under-treated in at least half of patients and that one-third of sufferers will experience significant disability as a result of their migraines at some stage of their lives. Such research demonstrates how crucial it is that pharmacy staff understand the type of headache a customer has and the best treatment to recommend. “The pharmacy team needs to be able to feel confident about recommending migraine treatments based on what is best for the patient,” says community pharmacist Sultan Dajani. “If they are unsure, then this is something they should do as a CPD point. Having Imigran Recovery as an OTC medication and not using it is a waste for patients in terms of their quality of life – and it is also a waste of a POM to P switch.” LEARNING OBJECTIVES After reading this feature you should be able to: • Recognise the different types of common headache • Accurately identify migraine • Recommend the most appropriate treatments and offer self-care advice for migraine and headache While there are around 200 distinct types of headache, 95 per cent are due to four types of treatable disorders: • Tension-type headache • Migraine • Cluster headache • Medication overuse headache. These types of headaches are known as primary headaches (i.e. they are based on symptoms and are not due to an underlying health problem). Another category is secondary headaches (i.e. those headaches that have a distinct cause). This category includes headaches associated with a head injury, stroke, substance misuse and/or its withdrawal (including alcohol), infection and disorders of the neck, eyes, nose, sinuses or teeth. Dr Mark Weatherall, consultant neurologist at Charing Cross and Ealing Hospitals and a trustee of the Migraine Trust, says: “Primary headache disorders are by far the commonest type of headache. If you start from the basis that patients are sufficiently troubled to actually seek advice about their headache rather than just take tablets at home, then the most likely reason that they are seeking advice in the pharmacy is that they have a migraine.” Migraine affects 8 million people in the UK, mostly adults aged 35-45 years, but it can affect all ages including children. Migraine is commoner in women – affecting 18 per cent of women compared to just 8 per cent of men. How to identify migraine Migraines are experienced as a headache of at least moderate severity, usually on one side of the head, accompanied by other symptoms such as nausea, vomiting, and sensitivity to light and noise. The headache is usually made worse by physical activity. Migraines usually last from four to 72 hours and in most cases there is complete freedom from symptoms between attacks. PHARMACY MAGAZINE APRIL 2014 29 29-32_Headache_PM_0414_rt.qxp:29-32_PM_0414 08/04/2014 13:30 Page 30 THE PRINCESS MARGARET MIGRAINE CLINIC CHARING CROSS HOSPITAL/SPL HEADACHE & MIGRAINE Certain factors are involved in triggering an attack in those predisposed to migraine. These can include lifestyle and hormonal changes. There are several types of migraine: • Migraine with aura is when there is a warning sign before the migraine begins. About a third of people with migraine have this. Warning signs may include visual problems (such as flashing lights) and stiffness in the neck, shoulders or limbs • Migraine without aura • Migraine without headache, also known as silent migraine. This is when an aura or other migraine symptoms are experienced, but a headache does not develop. Episodic migraine (defined as fewer than 15 headache days a month) is the commonest migrainous condition and can occur at any time. Frequency can vary between one attack a year to one a week. Chronic migraine is defined as more than 15 headache days a month over a three-month period, of which more than eight are migrainous. Those afflicted are classified as chronic sufferers. This type of migraine affects less than 1 per cent of the population. The most basic way to diagnose migraine is to identify a recurrent headache with certain features. Migraine should comprise: • At least two of the following symptoms: unilateral pain, throbbing pain, aggravation by movement, moderate or severe intensity • At least one of the following symptoms: nausea/vomiting or photophobia and phonophobia. A pharmacist can make a migraine diagnosis if the patient has an established pattern of migraine. Migraine treatments The main non-prescription migraine treatment options are analgesics and sumatriptan. Analgesics Analgesics, such as paracetamol, NSAIDs (aspirin, ibuprofen and diclofenac) and combined analgesics containing paracetamol or an NSAID with codeine, can be used as first-line treatment to relieve the pain of the migraine headache. There are also treatments that can be combined with paracetamol, such as buclizine and prochlorperazine to treat the nausea as well as the headache. If the patient is nauseous a soluble painkiller may be recommended as these are absorbed quicker from the stomach. When to recommend analgesics Analgesics can be recommended: • For the first three attacks of migraine unless the initial attacks are very severe and disabling • If the customer has previously used analgesics and is happy with the relief they provide • For customers who have not been diagnosed with migraine. When not to recommend analgesics Analgesics should not be recommended: • If the treatment has failed on three occasions • If a woman is pregnant (refer to doctor) 30 APRIL 2014 PHARMACY MAGAZINE About a third of people who suffer with migraine have aura “ • Refer to doctor and do not give NSAIDs to a customer who has ulcers or a history of bleeding in the stomach or intestines, anaemia, high blood pressure, or kidney, liver or heart disease • Be cautious when recommending NSAIDs to asthmatics • Be alert to a patient who might be chronically overusing analgesics or addicted to their properties and consequently suffering from medication overuse headache. “The first general principle for migraine is to recommend that patients take an [appropriate] dose of whatever painkiller they are going to take as early as possible when they feel an attack coming on,” says Mark Weatherall. “People sometimes have a tendency to take, say, 500mg of paracetamol two hours into an attack and will then get only a mild or partial response. “With simple analgesics, that means taking paracetamol 1g or [the maximum dose of] ibuprofen. People should not take more than 1,200mg ibuprofen in a day or 900-1,200mg of aspirin a day. As well as advising on an adequate dosage of analgesics, the pharmacist should also ask questions about nausea and, if needed, recommend an anti-emetic. “Although medication containing codeine is widely advertised and available for treating migraine I would always advise pharmacists to be cautious about recommending opiates because there is quite a high chance of people becoming dependent on them or developing medication overuse headache. I spend a lot of my working life getting people off codeine.” Triptans Triptans (e.g. sumatriptan) are generally recommended to sufferers if ordinary painkillers are not helping to relieve their migraine. They relieve pain by narrowing blood vessels in the head and blocking the transmission of pain in the sensory nerves that supply the skin and structures of the face. As well as relieving the pain associated with migraine, sumatriptan also relieves nausea and sensitivity to light. The OTC triptan Imigran Recovery (sumatriptan) has replaced its pre-sale two-page questionnaire with a simpler sales protocol that can be used as a reference for pharmacy staff. When to recommend sumatriptan Sumatriptan can be recommended: • For customers with an established and stable pattern of migraine • For customers who have failed to obtain relief from OTC analgesics on three occasions • If the initial attacks are very severe and disabling. When not to recommend sumatriptan Sumatriptan should not be recommended to: • Those under 18 or over 65 years of age • Pregnant or breastfeeding women (refer to doctor) • Customers with heart problems or with a family history of heart problems • Customers who have had a stroke • Customers with high blood pressure • Customers with kidney, peripheral vascular or liver disease • Customers with epilepsy or who are prone to fits • Women taking combined oral contraceptives (refer to GP). When to refer... Red flag symptoms associated with headache include: • Frequent or severe headaches that come on suddenly • Anyone complaining of the following symptoms: unilateral muscle weakness, double vision, tinnitus, clumsy and uncoordinated movement and reduced level of consciousness, weakness of muscles controlling eye movement, along with a headache lasting a week or more • A headache following an accident, in particular a head or neck injury • Anyone experiencing blackouts • Headaches brought on with every cough, sneeze, bend or by standing up • Weakness, numbness or slurred speech • Anyone with a headache lasting longer than 24 hours • Additional features such as seizure-like movements, a rash or a headache confined to the back of the head • Headaches that frequently wake someone from sleep • Anyone whose migraine attack occurs for the first time after 50 years of age • Anyone diagnosed with high blood pressure • Recent marked deterioration in migraine (duration, severity or frequency) • Women with migraine using the combined oral contraceptive pill. 31_PM_0414:31_PM_0414 14/04/2014 10:25 Page 1 A Be wise when you advertise Test a publisher ’s circulation claims Ask to see a current ABC certificate See it, trust it, believe it Our ABC certificate provides accurate, honest, independently verified circulation figures ensuring you get the exposure you have been promised All the latest ABC data is available free of charge at www.abc.org.uk Look for the ABC stamp of trust 29-32_Headache_PM_0414_rt.qxp:29-32_PM_0414 08/04/2014 13:31 Page 32 HEADACHE & MIGRAINE “If a customer has been previously diagnosed with migraine and in the absence of any other neuro symptoms or injury I would have no qualms about recommending sumatriptan as a first-line treatment because taking other painkillers might just be delaying the inevitable,” says Sultan Dajani. “It is a perfectly safe medication, the side-effects are very rare and the worst case scenario is that it won’t work. If that is the case, then it’s a sign the patient needs to see their GP.” With cluster headaches the pain is always unilateral and, although for some people the side can vary from time to time, it is usually centred over one eye, one temple or the forehead. It can spread to a larger area making diagnosis harder. Cluster headaches occur in clusters for four to 12 weeks around the same time of year. The pain is often experienced at a similar time each day. Such patients should be referred to the GP. Migraine and self-care Medication-induced headache, the third commonest cause of headache, is the result of taking painkillers too often. Up to one in 50 people experience headaches caused by medication overuse and women are five times more likely to get them than men. NICE guidance advises pharmacists to be alert to the possibility of medication overuse headaches in people whose headache developed or worsened while they were taking the following drugs for three months or more: • Triptans, opioids, ergots or combination analgesic medications on 10 days a month or more • Paracetamol, aspirin and a NSAID, either alone or any combination, on 15 days a month or more. Such patients should be referred to the GP. Martin Underwood, a GP and professor of primary care research at Warwick Medical School, who chaired the NICE guideline on the diagnosis and management of headache, says: “Treatment involves stopping medication abruptly with the headache getting much worse for several weeks before it will improve. When talking to people about a headache it is important to warn them to prevent medication overuse.” Medication overuse headache Pharmacists have a key role to play in educating migraine sufferers on how to bring their condition under control and take preventive action between attacks to help avoid migraine altogether. Triggers for migraine attacks can vary from one person to another and sufferers should be advised to keep a migraine diary to try to identify the causes. It is likely a combination of triggers will cause a migraine attack. Triggers can include: • Certain foods (e.g. cheese and chocolate) and drinks containing caffeine and alcohol • Emotional stress • Menstrual periods • Changes in normal sleep pattern • Extreme fatigue • Skipping meals and fasting • Sudden changing weather conditions • Exercise • Smoking • Bright and flickering lights • Odours • Medicines such as the combined oral contraceptive pill, hormone replacement therapies and sleeping tablets. The misery of migraine... • Image on p30 shows a single photon emission tomography image of the brain in a patient during an attack of classical migraine. Migraine diary headache & migraine 4HEAD Described as a completely different way to treat headaches, 4head is applied directly to the forehead targeting the pain relief just where it is needed, says DDD. Containing levomenthol as its active ingredient, 4head works to block headache pain signals and relax the muscles in the head associated with tension headaches, says the company. (Tel: 01923 205704) Commonest types of recurring headache Tension headache Tension-type headaches are the most commonly occurring. The pain is often described as feeling like a tight band around the head or a weight on top of it. The neck or shoulder muscles may also hurt and the pain can last from 30 minutes to several days, or may be continuous. Stress is one cause, but others may include drinking too much alcohol, not getting enough sleep, depression, skipping meals and becoming dehydrated. Whereas migraine can be identified as a headache with associated features, such as nausea and sensitivity to light, people experiencing headaches without features are likely to be suffering from the tension variety. These headaches can be treated with OTC painkillers such as ibuprofen and paracetamol. Self-care advice could include learning relaxation techniques, avoiding stressful situations where possible, using hot and cold packs to relax the muscles in the head and neck, or massaging the affected areas. cpd resources • NICE guidance on diagnosis and management of headache in young people and adults (http://publications.nice.org.uk/headaches-cg150) • Imigran Recovery support package for pharmacy staff: www.imigranrecovery.co.uk A migraine diary should record: • When the migraine started and ended • The symptoms • Whether it’s a throbbing or piercing pain • Where the pain is • Any other medication taken prior to the attack • Amount of sleep prior to the attack • Food eaten recently • Any recent exercise. “Migraine is a complex disorder with very individual symptoms and triggers,” says Dr Nicholas Silver, consultant neurologist at the Walton Centre, Liverpool. “That’s why it is important for sufferers to understand their condition and what triggers attacks so they can get the best out of their healthcare professional. The most successful migraine management plans rely on a foundation of good lifestyle and effective treatment.” KOOL�N’SOOTHE SOLPADEINE Many migraine sufferers find cooling relief to be of benefit during a migraine attack. Kool�n’Soothe Migraine are soft gel sheets that need no refrigeration and are ready to use straight from the pack. Each gel sheet will stay in place on the forehead delivering eight continuous hours of cooling relief. (Tel: 0208 987 9976) The Solpadeine line-up includes a wide range of pain solutions to address different customer needs. Pharmacy training for the brand includes on and off-line training tools aimed at refreshing pharmacy knowledge on the pain management category. The Omega Pharma online training portal can be found at www.omegapharmatraining.co.uk. Face-to-face training and in-store POS materials to support customer selection are also available. ([email protected]) Cluster headache IMIGRAN Cluster headaches are one of the most painful conditions an individual can experience and are even more debilitating than migraine. They are excruciatingly painful headaches, which cause an intense pain around one eye. A relatively rare condition affecting one or two people in every 1,000, cluster headaches are often misdiagnosed as migraine or sinus headache and subsequently mistreated. Imigran Recovery has replaced its pre-sale two-page questionnaire with a simpler sales protocol reminder as part of a new and improved support package for pharmacy staff. The support pack also features an A5 flowchart which can be used as a reference tool, a treatment pathway tool, a pharmacy training module and a consumer information booklet. (Tel: 0844 243 6661) 32 APRIL 2014 PHARMACY MAGAZINE 33-35_Animal Health_PM_0414_CR_rt.qxp:33-35_PM_0414 08/04/2014 16:05 Page 33 ANIMAL HEALTH Pet peeves Key facts • The number of pets in the UK increased by 4 million from 2012 to 2013 • Lyme disease and lungworm infections are on the rise • Vets are treating more pets for accidental poisoning By Charlotte Rixon Britain may be a nation of animal lovers, but pet health awareness could be higher. This ought to give pharmacists pause for thought... Animal welfare According to the latest PDSA Animal Wellbeing (PAW) report, there are 7.8 million pet dogs, 9.5 million pet cats and 1 million pet rabbits in the UK, with nearly half of households having a pet. Figures from the Pet Food Manufacturers’ Association (PFMA) show that the total pet population (excluding fish) increased by 4 million in just one year, from 67 million in 2012 to almost 71 million in 2013. Under the Animal Welfare Act 2006, pet owners have a �duty of care’ to ensure that they meet their pets’ five welfare needs: • A suitable environment • A suitable diet • The need to express normal behaviour • The need to live with or apart from other animals • Protection from pain, suffering, injury and disease. However the PAW report found that just 38 per cent of people who keep a pet are aware of this legislation, while over a quarter undertook no research into the costs and obligations of pet ownership before acquiring a pet. “People should do their research before getting a pet,” advises PDSA senior vet, Elaine Pendlebury. “Find out how much exercise a dog needs and make sure you are not allergic to pet dander. It is not fair on the animal if you take it on and discover you can’t provide for its needs.” Preventative healthcare Practising preventative healthcare, including regularly checking for and treating parasitic infestations, is an essential part of animal welfare, yet only 63 per cent of owners surveyed in the PAW report thought that preventative healthcare could extend an animal’s life – and 6 per cent had reduced spending on it since the start of the recession, potentially affecting nearly 1 million animals. So what is the current advice for preventing and managing parasitic infestations in pets? LEARNING OBJECTIVES After reading this feature you should be able to: • Help pet owners minimise the risks of zoonosis • Remind owners to correctly treat pets for infestations • Raise awareness of the risks of poisoning in pets PET OWNERSHIP in the UK continues to rise despite the recent recession, with most pet owners agreeing that ours is a nation of animal lovers. Yet due to misinformed choices and lack of awareness of preventative healthcare, vets and animal charities are concerned that the welfare needs of many pets are being compromised. For example, preventative treatments, such as regular defleaing and worming, are not only essential for animal welfare but also reduce the risk of potentially serious zoonoses – infections that are transmitted between vertebrate animals and people. With an estimated 500,000 pet owners visiting community pharmacies every day, pharmacists have a responsibility to raise awareness of the importance of preventative healthcare in pets, as well as providing sensible, but not alarmist, advice on reducing the risk of zoonotic diseases. UNHAPPY BUNNIES ... The PDSA (People’s Dispensary for Sick Animals) is concerned that many rabbits are at risk of serious conditions like myxomatosis and flystrike, because they are often bought for young children, on a whim or as a result of �pester power’, without considering the responsibility involved. Myxomatosis The myxoma virus is transmitted to rabbits via fleas and other biting insects, including mites and mosquitoes, and can also pass directly between rabbits. The first sign of myxomatosis in unvaccinated rabbits is runny eyes and swollen genitals. The disease rapidly progresses, causing severe conjunctivitis, blindness, lumpy swellings on the head and body, and death after around two weeks. Treatment is usually futile and serves only to prolong the animal’s suffering, so euthanasia is usually recommended. Vaccinated rabbits usually develop a milder, treatable form of the disease but the PDSA is concerned that less than half of all pet rabbits may be vaccinated against myxomatosis and viral haemorrhagic disease – another preventable, deadly disease. Rabbits in households where there is also a cat or a dog, or in rural areas with wild rabbit populations, are most at risk. Besides ensuring that their pets are vaccinated, rabbit owners are advised to fit insect screens to outdoor hutches and runs and eliminate standing water from gardens. Flystrike During the summer months rabbits are vulnerable to flystrike. This is caused by flies laying eggs on the rabbit’s fur, which hatch into maggots that eat the animal’s flesh. The problem is associated with dirty living conditions, so regularly cleaning hutches and runs is essential. It’s also important to check under the tail for signs of flystrike at least twice a day in summer. PHARMACY MAGAZINE APRIL 2014 33 33-35_Animal Health_PM_0414_CR_rt.qxp:33-35_PM_0414 08/04/2014 16:07 Page 34 ANIMAL HEALTH Fleas According to Stephen Goddard, Frontline veterinary surgeon, one in five cats and one in 10 dogs have fleas at any given time – yet around half of owners are unaware that their pet has an infestation. “Unprotected pets can pick up fleas from the garden, park or an infested home – wherever wild animals, stray cats or unprotected pets have been,” he says. Flea infestations can result in intense itching and scratching, leading to inflammation, fur loss and secondary bacterial infections. Animals with flea allergy dermatitis (FAD), due to an allergic reaction to antigens in flea saliva, can develop severe irritation and inflammation from a single bite, while heavy infestations can lead to lifethreatening anaemia in puppies and kittens. Furthermore, fleas carry the risk of tapeworm infestations because tapeworms spend part of their lifecycle inside fleas. Symptoms and treatment Signs of a flea infestation include scratching, biting and grooming more than usual, and inflamed skin. Fleas or flea dirt may also be visible on the coat, while owners may notice insect bites on their own skin. However cats and dogs should be treated for fleas throughout the year, even if they have no signs of infestation. “Any gap in treatment can allow fleas and ticks to survive and breed on your pet, which may also allow a home infestation to develop,” says Goddard. NFA-VPS licensed flea treatments include �spot-on’ products containing fipronil, which spreads around the body, killing fleas within 24 hours and ticks within 48 hours, and is suitable for use on cats and dogs, but not rabbits. Imidacloprid offers an alternative to fipronil that is suitable for rabbits, but does not kill ticks. Animals should be defleaed at least once every three months, at the same time as worming although, for optimum flea control, Goddard advises using fipronil every four to five weeks on cats, and every one to two months on dogs. It is vital to administer the correct product and dosage according to the animal’s species, age, weight and health status. All pets in the same household should be treated together, while animals with FAD require specialist veterinary treatment. Frequent vacuuming, washing pet bedding above 60 degrees and using a household spray containing an insect growth regulator will help reduce the problem. TOXIC HAZARDS The PDSA has reported an increase in accidental pet poisoning cases in recent years, with vet referrals to the Veterinary Poisons Information Service (VPIS) rising by 73 per cent between 2002 and 2009. The charity lists the top five commonest causes of accidental poisoning in pets as: • Incorrect use of flea treatments in cats (using too much or using treatments intended for dogs) • Rat and mouse poisons • Human medication such as paracetamol • Slug and snail killer • Antifreeze. On a daily basis vets see cases where owners have inadvertently poisoned their cats with permethrinbased flea treatments intended for dogs. “The margin of toxicity with permethrin in cats is very small,” says PDSA senior vet, Elaine Pendlebury. “Even coming into contact with a dog that has been treated with permethrin can be dangerous.” The wrong medicine Most human medicine poisoning cases occur when owners give paracetamol or ibuprofen to their pets in a misguided attempt to relieve their pain, or when pets consume human medicines that have not been safely put out of reach. In particular, paracetamol is highly toxic to cats because they lack the enzymes to break it down. While vets do prescribe human medicines to pets when there is no specific animal equivalent, it is important to stress to pet owners that all medicines they use on their pets should either be licensed for use in that specific animal or given in accordance with their vet’s instructions. Poisonous perils Ticks Ticks are small parasitic mites that commonly live in damp shaded areas like woodland and rough grassland, but can also be found in urban parks and gardens. A recent study in the journal Medical and Veterinary Entomology found that at any one time nearly 15 per cent of dogs are infested with ticks. A single tick may go unnoticed, but a heavy infestation can cause pain and anaemia. Elaine Pendlebury advises dog owners to check their dog’s fur carefully all over with rubber gloves after walking in wooded areas, as well as checking their own skin and clothing. Ticks can be difficult to remove, as their mouthparts can remain embedded in the skin, which may lead to irritation and infection. The PDSA recommends seeking a vet’s advice initially regarding the correct removal technique. Special devices for removing ticks are available. Lyme disease Ticks carry the threat of infectious diseases, including Lyme disease, the commonest vector-borne disease in Europe. The Health Protection Agency (HPA) says there has been a 300 per cent increase in the number of reported human cases in the UK since 2001. The first symptom is usually a circular rash (erythema migrans), which expands over several days or weeks. Infected individuals may also experience flu-like symptoms, such as headaches, tiredness and Rat and mouse poisons and slug and snail killer pose obvious hazards, while antifreeze contains ethylene glycol, which tastes pleasant to dogs and cats but causes kidney damage. In addition, chocolate can poison dogs due to the toxic effects of theobromine, with vets seeing an increase in cases around Easter, while all parts of the lily plant can cause kidney failure in cats. Pet owners should contact their vet immediately if they suspect their pet has been poisoned and should never �watch and wait’. “ The welfare of many pets is being compromised joint pain and, without treatment, may develop neurological symptoms and heart problems. According to Elaine Pendlebury, the reasons behind the rise are unclear. “It could be due to climate change, increasing deer populations or the rise in popularity of outdoor activity holidays, or it could be simply that diagnosis has improved,” she says. Being �tick aware’ by sticking to footpaths and covering up with long clothing in wooded areas, as well as regularly treating pets for external parasites, can reduce the risk of infectious diseases. Worms Two types of parasitic worm (helminth) affect cats and dogs – roundworm (nematodes) and tapeworm (cestodes). Animals pick up the former by consuming dead animals or sniffing faeces containing their larvae, while they become infested with the latter through swallowing infected fleas during grooming. y c a m r a h P E E R F Get your ! w o n p p A e in z a g a M specially azine early along with ag m e th of es su is ss Acce s. nced CPD learning tool ha en d an t en nt co d te crea 34 APRIL 2014 PHARMACY MAGAZINE Available to download via Apple App Store and Google Play for all devices. 33-35_Animal Health_PM_0414_CR_rt.qxp:33-35_PM_0414 09/04/2014 16:00 Page 35 ANIMAL HEALTH Worm infestations can cause diarrhoea and vomiting, poor condition and weight loss. Infested puppies and kittens can become malnourished, and in some cases, worms may be present in vomit or faeces, but there are often no obvious signs in adult animals. The commonst roundworm, Toxocara canis, presents a zoonotic risk (toxocariasis), which in rare cases can cause blindness. “Worm eggs can survive in the soil for up to three years; they are very resilient and can endure cold temperatures, so it’s important to be sensible, always pick up after your dog, and don’t let your dog lick your face,” urges Elaine Pendlebury. “Children should be encouraged to wash their hands thoroughly before eating and after playing outdoors.” Lungworm Another type of nematode that is becoming increasingly common in the UK, and which can cause life-threatening health problems in dogs, is the lungworm Angiostrongylus vasorum. Dogs become infected by ingesting slugs, snails or frogs (intermediate hosts to the lungworm larvae) or from contact with soil contaminated with fox faeces. Infestation signs include coughing, tiring easily, excessive bleeding from even minor wounds, anaemia, appetite loss, vomiting and diarrhoea. If dog owners suspect that their dog has been infected with lungworms, they should seek urgent help from their vet. Regularly washing food and water bowls and bringing in dog toys from the garden may help to reduce the risk. Pet care in pharmacy: opportunity knocks Pet healthcare continues to provide a significant opportunity to community pharmacy. The total UK animal medicines market is estimated to be worth £530m, with companion animals making up 56 per cent of the share. “Appropriate training for registered SQPs (suitably qualified persons) can reduce any apprehension regarding selling animal medicines over the counter, and pharmacists can then provide a knowledgeable pet advice service that will gain new and repeat business,” says Frontline veterinary surgeon Stephen Goddard. Most of the leading animal health manufacturers provide training materials for pharmacy staff, such as the �Pharmacy Pet Healthcare’ training series from Merial Animal Health, as well as posters and leaflets for pet owners. Treatment The British Small Animal Veterinary Association (BSAVA) recommends that dogs and cats be wormed at least every three months, while young puppies and kittens require more frequent treatment under the supervision of a vet. As with flea treatments, owners should ensure they follow the manufacturer’s instructions carefully to ensure they administer the correct dose for the animal’s species, age, size and weight. Toxoplasmosis Another parasitic infection, which is common in cats and presents a zoonotic risk, is toxoplasmosis. The infection is caused by the protozoa Toxoplasma gondii, which can be picked up from food or soil contaminated with cat faeces, undercooked meat and unpasteurised goat’s milk. There is also a small risk of infection during the lambing season. The infection rarely causes any symptoms in cats or people; however it can have serious complications in immunocompromised individuals and pregnant women who have not previously been infected. Nevertheless the risks are low and can be minimised by good hand hygiene and avoiding cat litter. PHARMACY MAGAZINE APRIL 2014 35 36-38_Sport_PM_0414_rt.qxp:36-38_PM_0414 09/04/2014 11:29 Page 36 SPORT & FITNESS Pull the other o Knowing how to advise customers to avoid, treat and manage a range of sports injuries correctly can help them steer clear of long-term muscular pain and joint damage A WORRYINGLY HIGH percentage of people simply ignore niggling sports injuries or treat them incorrectly, according to a new survey carried out by Lanes Health. The survey found that men are three times more likely to injure themselves playing sport than women (27 per cent versus 9 per cent), and that a fifth of UK adults injure themselves playing sport and leave the injury untreated. According to the survey, the commonest injuries that put people out of action for a fortnight or more are: • Backache (15 per cent) • Muscle strains (9 per cent) • Muscle inflammation (7 per cent) • Neck ache (6 per cent). So how are these injuries caused in the first place? “Sprains and strains happen when muscles or ligaments are overstretched, when competing for the ball, making a sudden stop or changing direction sharply,” says Matthew Jamieson, senior product manager at Mentholatum, “while injuries such as tennis elbow, shin splints, stress fractures or runners’ knee problems are typical of injuries that occur when too much is done too soon. They may happen when someone starts exercising or playing sport after doing little or nothing for some time.” Most sprains and strains can usually be treated with self-care such as the PRICE technique (protection, rest, ice, compression and elevation), and should improve within six to eight weeks – although severe muscle strains may take longer. However leaving an injury untreated can lead to “a once fixable problem having long-term, serious implications,” warns GP and medical broadcaster Dr Sarah Jarvis. While painkillers can be used to help ease any discomfort, advise customers to see their GP if they are in severe pain or if their injury is either not improving or getting worse. LEARNING OBJECTIVES After reading this feature you should be able to: • Explain the causes of the commonest sports injuries • Advise customers on how to prevent them in the first place • Identify which therapies and OTC remedies might help relieve symptoms Jogger’s nipple Another common condition – not just experienced by runners – is the obviously named jogger’s nipple. This is caused when the nipples are irritated by chafing against clothing during physical activity. Again, taking a break from running will give the nipple time to heal and an antiseptic cream can help treat the irritation and prevent infection. Shin splints Anyone taking part in strenuous exercise that involves impact or a lot of stopping and starting (e.g. long-distance running, tennis and basketball) can suffer from shin splints – the general term for exercise-induced pain at the front of the shins. The commonest cause is medial tibial stress syndrome (MTSS), which is the result of frequent and intense periods of exercise when the body is not used to it. According to NHS advice, it is important that sufferers don’t continue to exercise in case the pain is a sign of an injury to the bone and surrounding tissues. Customers should be advised to take a break from load-bearing exercise for at least a fortnight and to speak to their GP if the problem persists. Tennis elbow Tennis elbow (lateral epicondylitis) is a self-limiting condition usually caused by overuse of the muscles attached to the elbow that straighten the wrist, leading to pain around the outside of the elbow when bending, extending or lifting the arm. If these muscles and tendons are strained, tiny tears and inflammation can develop near the bony lump (the lateral epicondyle) on the outside of the elbow. Despite its name, tennis elbow is caused by any activity that places repetitive stress on the elbow, such as playing the violin or decorating, as well as racquet sport. Avoiding the activity should help the symptoms to improve, as will applying a cold or gel compress to the area. Running obstacles With April the start of marathon season, it’s important that runners look after their joints as well as their muscles. Acute knee injuries include runner’s knee (patellofemoral pain syndrome), which is caused by the impact of running irritating the site where the patella rests against the femur, resulting in sharp or dull pain and swelling. “Knee injury can increase the chances of developing and aggravating osteoarthritis in many people,” warns fitness expert and personal trainer Kristoph Thompson, so anyone experiencing knee pain should “allow enough time for full recovery and seek advice [from their GP] if symptoms persist.” “ A fifth of UK adults injure themselves playing sport and leave the injury untreated ” 36-38_Sport_PM_0414_rt.qxp:36-38_PM_0414 09/04/2014 11:30 Page 37 SPORT & FITNESS r one Warming up and cooling down By Sasa Jankovic Paracetamol can help with the pain and ibuprofen will reduce any swelling, but customers should consult their GP if the condition persists. Feet first All kinds of activities can lead to blisters, which are the skin’s way of protecting itself from excessive heat, moisture and friction. Although painful, most blisters will heal on their own unless they become infected, but they can be easily prevented in the first place by covering tender spots with a friction-resistant dressing or plaster. If they do occur, then specialist blister plasters, which claim to aid rapid healing by absorbing the fluid, protecting skin from bacteria and helping relieve the pain of friction and pressure, can be used. Remind customers who have diabetes to be particularly vigilant when checking for blisters, as their foot injuries take longer to heal due to poorer blood circulation. Key facts • Many UK adults do not know how to deal with sports injuries • Leaving an injury untreated can lead to long-term problems • Prevention and self-care are important in maintaining sports health and fitness Swimmer’s ear Another painful condition afflicting swimmers is swimmer’s ear, or otitis externa, which causes inflammation of the external ear canal between the outer ear and eardrum. Most cases are caused by a bacterial infection, although swimmer’s ear can also be caused by irritation, fungal infections and allergies. Repeated exposure to water can make the ear canal more vulnerable to inflammation. Symptoms include ear pain, itchiness in the ear canal, discharge of liquid or pus from the ear, and some degree of temporary hearing loss. Customers should see their GP, who will prescribe ear drops or even antibiotics. Remind them to avoid inserting cotton wool buds and other objects into their ears as this can damage the sensitive skin in the ear canal. They should also avoid getting water, soap or shampoo into their ears during bathing while the infection clears up. Regular swimmers should take a break from the pool until the symptoms pass and then consider using ear plugs or wearing a swimming cap to cover their ears when swimming to avoid further infections. Verruca assault Staying on the subject of feet, don’t forget verrucas – often caught from the wet floors in changing rooms and swimming pools – which manifest as warts growing up into the soles of the feet with a black dot in the centre surrounded by a harder, white area. It is common to have more than one verruca at a time, and they can become more painful the longer they are left. Up to 80 per cent resolve themselves within about two years, but OTC treatments can treat verrucas much faster. Advise customers to use such treatments with care as they are generally tissue destructive. Many contain salicylic acid, which breaks down the verruca, so they should not be applied to healthy skin, which can be shielded with petroleum jelly or surgical tape. Cryotherapy treatments that freeze the verruca are also available over the counter, but again all surrounding healthy tissue must be protected. If your customers would rather not tackle verrucas themselves, recommend they see a podiatrist. Joint action Joints can also benefit from a bit of ongoing care and attention, as Kristoph Thompson explains. “Injury can occur when a joint is taken outside of its comfortable range of motion, so stronger stabiliser muscles and increased flexibility lessen the likelihood or severity of an injury. “Maintaining a healthy weight can also be beneficial on joints. One study claimed that losing about a pound of weight delivers almost a four-pound reduction in knee joint load for each step.” Managing pain Athlete’s foot Regular exercisers and gym-goers also increase their risk of another common foot condition – athlete’s foot (tinea pedis). Athlete’s foot is caused by the Trichophyton fungus, which thrives in warm, moist environments (e.g. sweaty trainers) and can be picked up from changing room floors. Symptoms include itching or burning and flaking skin, particularly between the toes, although the whole foot can be affected. The condition can be treated with products containing fungicidal or fungistatic ingredients. Making sure the feet are completely dry after washing; regularly changing footwear and wearing cotton socks can help ensure feet are less fungus-friendly. Just as a Formula One driver warms up his tyres before he begins racing, so sports players at every level should not expect their body to perform as well as it can when �starting from cold’, says Matthew Jamieson. “It is essential to make time to get the blood circulating in your muscles and to stretch those ligaments that you will soon be putting under stress.” Ideally, you should spend 15 or 20 minutes warming up and stretching before the game or training session starts, he says. “It is also important to be sensible and, especially if you have not taken much exercise for a while, to build up slowly to more strenuous activity.” DID YOU KNOW? Ankle sprains account for an estimated 1.5 million visits to UK hospital accident and emergency departments each year, according to nhs.uk. “Topical analgesics are a popular and effective treatment for the sprains, strains and knocks that are part and parcel of playing sport – but it is crucial that the appropriate product is chosen for the needs of each individual,” says Matthew Jamieson. “For example, when someone has suffered a sprain or strain, it should be treated with a cold or freeze product for the first 72 hours to help reduce swelling and inflammation and only when this period is over should heat be used to help increase blood flow to the affected area bringing oxygen, proteins and other nutrients to help promote healing.” Cold and heat therapies can be as simple as using a pack of frozen peas in a damp cloth or a hot water bottle on the affected area but these are not always practical, adds Matthew, “which is why many turn to topical analgesics as a convenient option, with a choice of rubs, sprays and patches that combine ease of use with effectiveness. “Topical NSAID products that offer an anti-inflammatory action together with pain relief are another option to help with muscle and joint aches and pains arising from sports injuries.” An independent charity for pharmacists and their families, former pharmacists and pharmacy students. Our free and confidential services include Financial Assistance stress helpline Information and enquiry line Health Support Programme Listening Friends addiction support and counselling Specialist Advice Services debt, benefits and employment General enquiry line: 0808 168 [email protected] Listening Friends Helpline: 0808 168 5133 Health Support Helpline: 0808 168 5132 www.pharmacistsuppor t.org Pharmacist Support is a registered charity, No. 221438, and is funded by donations from pharmacists. PHARMACY MAGAZINE APRIL 2014 37 36-38_Sport_PM_0414_rt.qxp:36-38_PM_0414 09/04/2014 11:31 Page 38 SPORT & FITNESS Gyms and health clubs are not everyone’s cup of tea, but there are many other exercise alternatives that people can do by themselves, or with friends, that don’t need expensive equipment or lots of training to take part in. The key to getting active – and sticking at it – is finding something that a person enjoys and can easily build into their lifestyle. Joining up with a �fitness buddy’ to keep them company can also help maintain motivation. Diet and movement specialist Joanna Hall, one of the UK’s leading fitness and walking experts and co-founder of the Walkactive initiative that encourages people to incorporate more walking into their day, is an advocate of simply putting one foot in front of the other. “Walking is simple, easy, and just about anyone can do it,” she says. “Some people are sceptical about many of its benefits, but there is no disputing the research. Walking at the right pace and with the right technique can reduce the risk of many diseases and painful conditions. Whether someone is completely new to fitness, wants to firm up, lose excess pounds, or just get fitter and healthier, walking is perfect, has few side-effects and can be done by almost anyone, anywhere.” Cycling is another effective way to burn calories and increase cardiovascular fitness, as well as being an environmentally-friendly mode of travel that can save time and money. “Cycling has many more health benefits than you think,” says Claire Beaumont, Evans Cycles’ fitness expert. “We all think of it as an alternative mode of transport but the workout you get from cycling helps keep you fit without realising it and is so much better for your wellbeing.” THROW AWAY THE GYM MEMBERSHIP... SPORT & FITNESS DEEP FREEZE GOPO Results of a study published in the British Journal of Sports Science show that the natural anti-inflammatory, painkilling effects of GOPO could benefit active people, says Lanes Health. Researchers found that just 12 weeks’ supplementation with GOPO decreased joint pain, improved the quality of joint movement, and could prevent the degeneration of joint tissue and cartilage. (Tel: 01452 507458) Mentholatum is running a 10-week campaign of adverts, promotions and sponsorship on XFM, The Rock, indie and alternative music radio stations. Research shows listeners are more likely to participate in sport. Sports bulletins on the weekday breakfast and drive shows will be sponsored by Deep Freeze and there will be core messages delivered at the weekend when listeners, who are likely to be playing or getting ready to play sport, have the chance to win sport-related prizes. (Tel: 01202 780558) ARNICARE Many injuries can be avoided by warming up and doing stretches immediately before and after physical activity. Nelsons Arnicare arnica cooling gel combines the benefits of arnica with the refreshing sensation of natural grapefruit oil and menthol. The gel is perfect to massage into muscles following physical exertion or to revive tired, heavy legs, says Nelsons. (Tel: 0208 780 1290) Sports supplements While it remains important to follow a varied and balanced diet and healthy lifestyle, some people believe that sports supplements have a role to play in boosting their performance and recovery, and helping them avoid injury. “Exercise puts added strain on the body, such as the immune system, muscles and heart,” says Dr Carrie Ruxton from the Health Supplements Information Service. “While a balanced, high carbohydrate diet with plenty of fluid should be the cornerstone of any advice, dietary supplements can also help those taking part in regular exercise.” According to Dr Ruxton, examples include: • Multinutrient supplements, which deliver recommended amounts of vitamins and minerals. These are useful as research shows that intakes of vitamin D, iron, calcium, selenium and magnesium are low in the general population, especially women • Omega-3 fatty acids and antioxidant nutrients (e.g. vitamins C and E, selenium) help to reduce inflammation and may help muscle soreness • Vitamin C, vitamin D and zinc are proven to support immune function and may reduce the duration of respiratory illnesses • Products high in nitrates, such as beetroot and spinach, have been shown to boost endurance performance • Products containing caffeine which, if taken before endurance sports such as marathons or long cycle races, can reduce fatigue and improve alertness • Creatine supplements can help build muscle and improve high intensity exercise (e.g. weight lifting, sprinting). “The Self Care Forum factsheets suggest that patients should visit their pharmacy for help in treating minor problems,” adds Matthew Jamieson, “and pharmacists and counter staff should be ready with advice to help them make the appropriate choices [and] have a selection of lines from trusted manufacturers to give customers a good choice of market-leading products.” With self-care being strongly promoted to the general public at the moment, now is the ideal time to not only encourage your customers to find a form of exercise that they enjoy, but also to remind them there is much they can do to look after themselves while they do it. (See also this month’s CPD module on promoting physical activity and exercise, starting on p17.) FURTHER INFORMATION • Self Care Forum factsheets: www.selfcareforum.org/fact-sheets • Health Supplements Information Service: www.hsis.org • Walkactive: www.joannahall.com/index.php 38 APRIL 2014 PHARMACY MAGAZINE BAZUKA Bazuka offers a range of treatments for verrucas and warts including Bazuka Gel (P) and Bazuka Treatment Gel (GSL) – both with the original formulation. Also available are Bazuka Extra Strength (P) and Bazuka Extra Strength Treatment Gel (GSL), which contain twice the amount of salicylic acid as the original formulation. For those looking for a freeze treatment, there’s Bazuka Sub-Zero. (Tel: 01923 205704) MENTHOLATUM As many as 22m sporting injuries are suffered in the UK each year, most commonly sprains and pulled muscles, says senior product manager Matthew Jamieson. “Mentholatum is the expert in muscle and joint care and the Deep Freeze and Deep Heat ranges allow sports injury sufferers to treat their minor injuries effectively with products that can take them from the moments after a sprain or strain through the healing and recovery period and right back onto the pitch or track.” (Tel: 01202 780558) TENA One in four women experience light bladder weakness while exercising and playing sport, according to a recent survey for lights by TENA. The range of liners is specifically designed to ensure women experiencing light bladder weakness feel fresh and confident, even when exercising, says the company. At 3.5mm thick, each liner offers discreet protection, locking moisture away from the body for all-day comfort. (Tel: 0870 333 0874) MAXINUTRITION #FeedYourMuscles is a new £5m advertising campaign from GlaxoSmithKline to promote the benefits of its protein-based sports nutrition range, Maxinutrition. The TV advert uses real people training across a range of sports to demonstrate how Maxinutrition products improve performance and recovery and includes the tagline: �You, Stronger’. It is supported by experiential, print and online advertising. The Maxinutrition range includes products suitable for every level of exercise. Tel: 0870 240 8602 39_Stock_PM_0314_rt.qxp:39_PM_0414 11/04/2014 14:45 Page 39 TEAM TRAINING pharmacist support column Team Tuesday is a chance for your pharmacy team to learn together. On the first Tuesday of the month after Pharmacy Magazine and Training Matters arrive in-store, get together for a training session based on selected content in the magazines. This support column is designed to help pharmacists structure and lead a Team Tuesday training session. SUBJECT: HAY FEVER This column provides pharmacists with a training resource for support staff. REFLECTION • Can the pharmacy team explain the advantages and disadvantages of the different types of hay fever product for a customer’s specific symptoms (e.g. blocked nose, itchy eyes)? • Do I know which hay fever remedies are suitable for pregnant women? • Is the pharmacy team confident to advise on how to use hay fever remedies effectively (e.g. timing, dose, frequency)? • Is the team confident in its ability to pass on tips on hay fever symptom reduction/prevention? • Are we confident in our advice on how to use nasal sprays and eye drops? • Do we stress the importance of compliance? TRAINING CHECKLIST Ensure your support staff understand the following key points: • The incidence of hay fever and other allergies is increasing • Which oral antihistamines are most or less likely to cause drowsiness • The importance of the pollen count • Which products suitable for hay fever are licensed for customers under the age of 18 years • Specific lifestyle tips for customers with hay fever • Hay fever can develop in people with asthma • Hay fever can result in complications such as sinusitis • When to refer customers with hay fever to the pharmacist. ACTION. I WILL: • Consider how we can raise awareness of starting hay fever prevention before symptoms start • Ensure that the pharmacy team is up to date on the role of drug-free treatments for hay fever • Train my pharmacy assistants to ensure that they can meet the points in the training checklist. PRACTICE POINTS • Do a Google search for phone and tablet apps for pollen forecasts and allergy. Discuss their quality and usability with the pharmacist. Which one(s) might you recommend? • What is non-allergic rhinitis, what causes it and what can be recommended to treat it? TEAM TUESDAY: LEARNING TOGETHER STOCKCHECK Juvela improves its cookies Dioralyte back on TV screens Juvela has reformulated and improved its range of low protein cookies. While the cookies are still available in choc-chip, cinnamon and orange flavours, the flower-design has been replaced with a more traditional shape. The new-look cookies are chunkier, have a lighter crisper texture and an improved flavour, says Juvela. ACBS approved, the low protein cookies come in boxes of 12 (125g), containing two individual trays of six. A box retails for £7.62. Dioralyte is back on TV during April and May with 10- and 20second ads appearing on a range of mainstream TV channels, such as ITV1 and Channel 4. “We are excited to be relaunching our TV ad campaign this spring,” says consumer brand manager Eleonore Baco, “and we hope this support will continue to generate increased sales…by communicating the brand’s key messages and increasing awareness among non-users.” The ad campaign follows a couple through common life stages and highlights product usage in different scenarios. Juvela 0800 783 1992 Refer to this month’s Team Tuesday focus feature in Training Matters on hay fever and work through the training exercises and quiz questions together with your team. The answers to the MCQs are: 1.d 2.a 3.d 4.b 5.c 6.a PRODUCTS Ceuta Healthcare: 01202 780558 BUSINESS BRIEFING Avoiding pension pitfalls The pension landscape is changing and employers can be fined if they fail to comply, warns Heather Chandler The Government has for some time been concerned that people are not saving enough for their retirement and has moved from the concept of employees being able to choose to join a pension scheme to one of automatic enrolment. Since October 2012, larger businesses have been required to automatically enrol eligible employees into a pension scheme and pay a minimum level of pension contributions for each employee. By February 2018, every employer, no matter how small the company, will be subject to the same obligations. Generally speaking, employers with between 50 and 249 employees will have staging dates (to join auto-enrolment) between April 2014 and April 2015. Employers with fewer than 50 employees will be subject to the requirements between April 2015 and April 2017. New businesses have staging dates at the end of the timetable. The pensions regulator will notify every business of its staging dates. Following their staging date, they must register with the regulator. There are penalties for non-compliance. Who is covered? Those covered by the auto-enrolment rules include permanent, fixed-term and temporary employees, as well as agency workers. The self-employed will not be subject to the requirements. Employees already enrolled into a qualifying scheme through their workplace will remain in that scheme and the duty of auto-enrolment will not apply in respect of them. A sole trader who does not employ anybody else is not affected. Workers fall into different categories depending on age and earnings, and the obligations on employers differ accordingly. Employees between the age of 22 and state pension age, who earn over the income tax threshold, are �eligible jobholders’ who must be automatically enrolled into a scheme at the staging date (or on later joining the business). The employer is required to pay contributions into the pension scheme in respect of these employees. Those earning below the income tax threshold but above the lower earnings limit, and those earning above the lower earnings limit but who do not meet the age criteria, will be able to opt into the scheme should they wish. If they do opt in, the employer must also pay contributions for them. What if employees do not want to be enrolled? For those employees who do not want to be enrolled, the process demands that they must first be automatically enrolled into the scheme before being allowed to opt out. They must then be automatically re-enrolled every three years. Finding a scheme to join To implement the new system, a firm can use an existing occupational or personal pension scheme if it meets certain statutory requirements; set up a new scheme; or enrol employees in the National Employment Savings Trust (NEST), a new central scheme set up by the Government. The pensions regulator suggests businesses allow 12-18 months to prepare for auto-enrolment. There is a fixed penalty of £400 for noncompliance and there are other financial penalties, including escalating penalty notices of £50 to £10,000 a day, depending on employee numbers. Information www.nestpensions.org.uk www.thepensionsregulator.gov.uk Heather Chandler is a partner in the pensions team at Shoosmiths LLP No part of this publication may be reproduced without the written permission of the publishers. Published under license by Communications International Group Ltd. Some of the editorial photographs in this issue are courtesy of the companies whose products they feature. Unbranded pictures copyright Photodisc/Digital Stock/iStockphoto. Certain articles in this issue are supported by educational grants from manufacturers. The publisher accepts no responsibility for any statements made in signed contributions or in those reproduced from any other source, nor for claims made in advertisements, or information on products or ranges featured in editorial stories. © Groupe Eurocom Ltd. Colour Repro by Truprint Media, Margate. Printed by Grange Press, Brighton. Pharmacy Magazine is published monthly, copies are available on subscription to individuals who do not qualify within the terms of the controlled circulation. UK £95, $155, €120 Overseas £170, $275, €210. ABC figure for January to December 2013 is 17,692. PHARMACY MAGAZINE APRIL 2014 39 40_PM_0414:40_PM_0414 14/04/2014 14:31 Page 1
© Copyright 2026 Paperzz