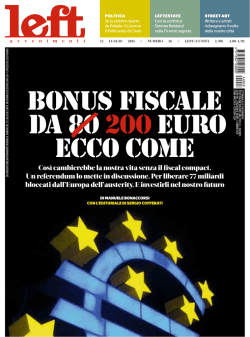
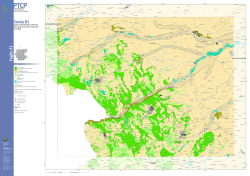
Rare extra-adrenal paraganglioma mimicking a painful Schwannoma Ann. Ital. Chir. Published online (EP) 26 September 2014 pii: S2239253X14022907 www.annitalchir.com Case report PR RE IN AD TI -O N G NL PR Y O CO H P IB Y IT ED Andrea Picchetto, Alessandro M. Paganini, Andrea Balla, Silvia Quaresima, Vito Cantisani, Giancarlo D’Ambrosio, Emanuele Lezoche Department of General Surgery, Surgical Specialties and Organ Transplantation “Paride Stefanini” (Direttore Prof. Emanuele Lezoche) “Sapienza” University of Rome U.O.C. Clinica Chirurgica e Tecnologie Avanzate Rare extra-adrenal paraganglioma mimicking a painful Schwannoma. Case report INTRODUCTION: Paragangliomas originate from chromaffin tissue primarily found in the Zuckerkandl body. A 53 years old man, was investigated with abdominal MRI for chronic backache, that had lasted for 2 years. CASE REPORT: MRI revealed an incidental mass in para-aortic region, at the adrenal lodge, with characteristics of a solid nodular mass, which did not seem to arise from the adrenal gland. An abdominal CT showed a mass localized prior to left adrenal gland; the radiologist reported this mass as a malignant peripheral nerve sheath tumor (Schwannoma). During his stay in hospital, tumoral markers chromogranin and neuron-specific enolase were dosed, with a concentration of 187.00 ng/mL and 7.7 ng/mL. Patient’s back pain was treated first with ketorolac, without any resolution of the problem, then with ketorolac plus tramadol in elastomeric pump, again with no relief, and finally with a continuous infusion of morphine. Since the exact nature of the neoplasm was not known and a CT guided biopsy was not technically feasible to do, a laparoscopic excision of the mass, with transperitoneal anterior submesocolic approach, as well as for the left adrenalectomy, was planned. After surgery, the patient no longer needed morphine. The postoperative course was uneventful. RESULTS: Histopathological findings consisted of periadrenal paraganglioma. Extra-adrenal paragangliomas are rarely recognized during preoperative study. This is often due to its capacity of mimicking other type of tumors. CONCLUSIONS: Paragangliomas could be successfully resected by laparoscopy, they are difficult to distinguish from other tumor and they should be investigated even if preoperative findings argue for something else. KEY WORDS: Laparoscopic adrenalectomy, Paraganglioma, Schwannoma Introduction The incidence of paragangliomas is 1/100.000, and are approximately ten percent of catecholamine secreting tumors 1. Paragangliomas originate from chromaffin tissue primarily found in the Zuckerkandl body, the kidneys, the sympathetic plexus of the urinary bladder, and the heart or in the sympathetic ganglia of the head or neck 1. Due to the possibility of catecholamine’s secretion, patients with paragangliomas may present with signs and symptoms including hypertension, palpitations, tremor, pallor, headache and tachyarrhythmia 2,10. Catecholamine-secreting paragangliomas are only 25%. The remainder present with an abdominal mass only and no evidence of hypertension 3,10. Case report Pervenuto in Redazione Aprile 2014. Accettato per la pubblicazione Maggio 2014 Correspondence to: Dott. Andrea Picchetto, Clinica Chirurgica e Tecnologie Avanzate, Dept. “Paride Stefanini”, Policlinico “Umberto I”, Viale del Policlinico 155, 00161 Roma (E-mail: [email protected]) A 53 years old man, followed up for a previously treated Hodgkin’s lymphoma in 1993 and with hypercholesterolemia/hypertriglyceridemia, was investigated with Published online (EP) 26 September 2014 - Ann. Ital. Chir 1 A. Picchetto, et al. abdominal MRI for chronic backache that had lasted for two years. The patient tried to relieve the back pain (VAS Score 8), unsuccessfully, with several types of nonsteroideal anti-inflammatory drugs (NSAID). MRI revealed an incidental para-aortic solid nodular mass (29x25mm) located within the left adrenal lodge, which did not seem to arise from the left adrenal gland. CT scan (Fig. 2) showed the mass to be localized anteriorly to the left adrenal gland and was reported as a malignant peripheral nerve sheath tumor (Schwannoma) or, alternatively, as a partially colliquated lymph node. Biopsy, due to its difficult location, was not performed. The patient did not report headaches, excessive sweating, palpitations, hypertension, or any other systemic symptom. During his stay in hospital, tumor markers chromogranin and neuron-specific enolase (NSE) were 187.00 ng/mL (n.v. <90.00 ng/mL) and 7.7 ng/mL (n.v. <12 ng/mL), respectively. The patient’s back pain was treated with ketorolac first, with no relief, then with ketorolac plus tramadol in elastomeric pump, again with no relief, and finally with a continuous infusion of morphine, which was successfully. Treatment Fig. 1: Trocar positions during left transperitoneal adrenalectomy. The surgeon and first assistant stand on the left of the patient while the second assistant stands on the right. Fig. 2: Axial CT scan showed the presence of round shaped, well marginated, hypodense lesions of....mm x mm. The lesion was strictly adjacent to adrenal gland. PR RE IN AD TI -O N G NL PR Y O CO H P IB Y IT ED Since the exact nature of the neoplasm was not known and a CT guided biopsy was not technically feasible, a laparoscopic excision of the mass was planned, with a transperitoneal anterior submesocolic approach, as commonly performed by the authors for left adrenalectomy 4-5. Surgery was performed under general anesthesia. A nasogastric tube and a urinary catheter were positioned. The patients was monitored with an intra-arterial radial artery catheter for blood pressure measurement and a central venous catheter (internal jugular access) to monitor changes in central venous pressure and for rapid introduction of liquids, if necessary. Pneumoperitoneum was established with a Veress needle at the umbilicus. Pneumoperitoneum at 13 mmHg pressure was obtained with carbon dioxide insufflator adjusted at 30 l/minute. Four 12mm trocars (Fig. 1) and a 45° optic were used. This approach was performed with the patient supine, in anti-Trendelenburg position and with the operating table rotated 30° towards the opposite side of the lesion, to facilitate exposure of the surgical field. The surgeon stands on the side ipsilateral to the lesion. The first trocar was inserted to the left of the midline above the umbilicus (Fig. 1). A second trocar was inserted on the right midclavicular line below the right costal arch. A third and fourth trocar were placed one on the left midclavicular line above the transverse umbilical line and one on the left anterior axillary line, respectively. The transverse mesocolon was raised by the assistant with atraumatic forceps introduced through the right midclavicular trocar to expose the first jejunal loop at the ligament of Treitz and to identify the inferior mesenteric vein. The posterior peritoneum was opened at the insertion of the transverse mesocolon on the lower edge of 2 Ann. Ital. Chir - Published online (EP) 26 September 2014 Rare extra-adrenal paraganglioma mimicking a painful Schwannoma. Case report icked a malignant peripheral nerve sheath tumor, a MIBG scintigraphy, however, was not performed. Paragangliomas are difficult to distinguish from other tumors. Any extra-adrenal mass should be investigated even if the preoperative findings argue for something else. In this patient, the paraganglioma mimicked an adrenal mass and it was treated with the same laparoscopic approach that is commonly employed by the authors to treat adrenal masses, with good results. The submesocolic approach was found to be safe and feasible to treat this peri-adrenal mass. PR RE IN AD TI -O N G NL PR Y O CO H P IB Y IT ED the pancreas, between the first jejunal loop and the inferior mesenteric vein. After Toldt’s fascia identification, the dissection proceeded posteriorly along the retro-pancreatic plane, elevating the body of the pancreas. Then Gerota’s fascia was opened to identify the superior margin of the left renal vein. This was prepared latero-medially until its junction with the inferior adrenal vein, which was adferent the mass. The left adrenal vein was prepared and divided between clips (AcuClip, Tyco / Healthcare, Norwalk, Connecticut, USA) to allow access to the mass. After adrenal gland division, the medial subdiaphragmatic connections of the mass with the surrounding anatomical structures were divided with a radiofrequency vessel sealing device (LigaSure ™ tissue fusion, Covidien, Mansfield, Massachusetts, USA). Monopolar electrocautery was selectively used for hemostasis. Once released, the mass was removed inside an extraction bag. The residual space was filled with hemostatic material (Floseal, Baxter Healthcare Corporation, Deerfield, Illinois, USA) and a drainage was left in place. After surgery, the patient no longer needed morphine and the pain was easily controlled with paracetamol, suspended on POD 3. The postoperative course was uneventful. The resected specimen consisted of a brownish tissue of 5x3x2 cm, with an area of central colliquation. Histological examination revealed a polygonal cells’ nests mass, which presented a round- to oval-cell predominant smear with occasional striking anisonucleosis, free of histological anomalies. Mitosis or necrotic areas were not seen. Immunohistochemical stainings have reported diffuse positivity with chromogranin, synaptophysin and S100 protein; CKAE1-AE3 and melan-A were negative. The proliferation index was found to be 2-3%. Histopathological findings were consistent with the diagnosis of periadrenal paraganglioma. Follow-up The patient is alive, free of symptoms and has been followed up for 15 months. Follow up abdominal CT and MRI scans were repeated, both of them were unremarkable. Discussion/Conclusion Extra-adrenal paragangliomas are rarely recognized preoperatively. This is often due to its capacity of mimicking other types of tumors 6-15. Magnetic resonance imaging (MRI and computerized tomography (CT) are highly sensitive in detection of small tumors but are not specific for paragangliomas 16-17. MIBG scintigraphy is specific for paraganglioma but is less sensitive than MRI and CT 18. Due to normal plasma and urine catecholamine levels and to CT and MRI findings that mim- Riassunto I paragangliomi hanno un’incidenza annuale di circa 1/100000; essi originano dai tessuti cromaffini dei corpi di Zurckerkandl. In questo case report riportiamo il caso di un uomo di 53 anni, già trattato e seguito per un precedente limfoma di Hodkin che è stato sottoposta a RMN dell’addome per una lombalgia cronica che durava da due anni e che non riusciva ad alleviare con i FANS. La RMN ha rivelato un’incidentaloma: una massa in regione para-aortica, a livello della loggia surrenalica sinistra con le caratteristiche di una massa nodulare solida (29*25mm), che non sembrava originare direttamente dal surrene. Il pz ha inoltre eseguito un TC dell’addome che ha mostrato una massa localizzata di fronte al surrene di sinistra; il collega radiologo ha definito questa massa come un tumore maligno delle guaine nervose periferiche (Schwannoma) o come un linfonodo colliquato (essendo nota la patologia linfomatosa già descritta in anamnesi). Il paziente non riferiva cefalea, palpitazioni, picchi ipertensivi ne’ altri sintomi sistemici. Durante il suo ricovero, sono stati dosati i marker tumorali cromogranina e l’enolasi neurono-specifica che sono risultati essere rispettivamente 187.00 ng/mL and 7.7 ng/mL. La lombalgia è stata trattata inizialmente con Ketorolac, senza beneficio alcuno, quindi con Ketorolac più Tramadolo in pompa elastomerica, nuovamente senza beneficio per il paziente, infine con infusione continua di Morfina. Dato che l’esatta natura della neoformazione non era nota e che l’esecuzione di una biopsia TC guidata non era tecnicamente possibile, è stata eseguita un’escissione per via laparoscopica della massa, con approccio anteriore submesocolico trans peritoneale, così come gli Autori sono soliti eseguire per la surrenalectomia sinistra. Sin dai primi giorni postoperatori il paziente non ha più necessitato della morfina. Il decorso postoperatorio è stato del tutto regolare. L’esame istologico è risultato essere paraganglioma. I paragangliomi extra-surrenalici sono raramente riconosciuti duranti gli esami preoperatori. Questo errore è spesso dovuto alla sua capacità di simulare vari altri tipi di tumore. Published online (EP) 26 September 2014 - Ann. Ital. Chir 3 A. Picchetto, et al. Gli Autori credono che i paragangliomi possano essere resecati con successo tramite approccio laparoscopico, che essi sono difficili da distinguere altri tipi di tumore e che debbano essere sospettati anche se i risultati preoperatori depongono per qualcos’altro. References 1. Plouin PF, Gimenez-Roqueplo AP: Pheochromocytomas and secreting paragangliomas. Orphanet J Rare Dis, 2006; 1:49. 10. Giangrande DL, Paliogiannis P, Denti S, Attene F, Scognamillo F, Serventi F, Trignano M: Surgical management of a voluminous abdominal paraganglioma and review of the literature. Ann Ital Chir, www.annitalchir.com, 2011; 82(3):211-15. 11. Capel I, Gil MP, Marqués G, Barcons S, Rigla M: Cervical paraganglioma mimicking a thyroid nodule with recurrent nerve involvement. Endocrinol Nutr, 2012; 59(4):274-5. doi: 10.1016/j.endonu.2011.09.011. Epub 2011 Dec 11. Spanish. 12. Durai R, Husain F, Oke T, Siddiqui M: Paraganglioma mimicking adrenal incidentaloma. Br J Hosp Med (Lond), 2011; 72(10):593. PR RE IN AD TI -O N G NL PR Y O CO H P IB Y IT ED 2. Young WF Jr.: Paragangliomas: clinical overview. Ann NY Acad Sci, 2006; 1073:21-9. 9. Bartolacci ML, Bartolacci S, Leombruni E, Annunziata A, Di Rienzo M, Picardi N: Adrenal incidentaloma: a dopamine-secreting pheochromocytoma with an atypical clinical picture. A case report and review of the literature. Ann Ital Chir, www.annitalchir.com, 1998; 69(6):805-14. 3. Muzaffar S, Fatima S, Siddiqui MS, Kayani N, Pervez S Raja AJ: Mesenteric paraganglioma. Can J Surg, 2002; 45(6):459-60. 4. Scoglio D, Balla A, Paci M, Guerrieri M, Lezoche G, D’Ambrosio G, Fabiani B, Ursi P, Paganini AM: Laparoscopic transperitoneal anterior adrenalectomy. Ann Ital Chir, 2013; 84:411-16. 5. Perretta S, Campagnacci R, Guerrieri M, Paganini AM, De Sanctis A, Sarnari J, Rimini M, Lezoche E: Sub-mesocolic access in laparoscopic left adrenalectomy. Surg Endosc, 2005; 19(7):977-80. 6. Amin MF, EL Ameen NF: Diagnostic efficiency of multidetector computed tomography versus magnetic resonance imaging in differentiation of head and neck paragangliomas from other mimicking vascular lesions: Comparison with histopathologic examination. Eur Arch Otorhinolaryngol, 2013; 270(3):1045-53. doi: 10.1007/s00405-0122084-6. Epub 2012 Jun 27. 7. Lee HM, Jeong DS, Park PW, Kim WS, Sung K, Lee YT: Anterior mediastinal paraganglioma mimicking thymoma. Heart Surg Forum, 2012; 15(3):E170-1. doi: 10.1532/HSF98.20111173. 8. Napolitano L, Francomano F, Angelucci D, Napolitano AM: Thyroid paraganglioma: Report of a case and review of the literature. Ann Ital Chir, www.annitalchir.com, 2000; 71(4):511-13. 4 Ann. Ital. Chir - Published online (EP) 26 September 2014 13. Singhi AD, Hruban RH, Fabre M, Imura J, Schulick R, Wolfgang C, Ali SZ: Peripancreatic paraganglioma: a potential diagnostic challenge in cytopathology and surgical pathology. Am J Surg Pathol, 2011; 35(10):1498-504. 14. Tuncel A, Aslan Y, Han O, Horasanli E, Seckin S, Atan A: Laparoscopic resection of periadrenal paraganglioma mimicking an isolated adrenal hydatid cyst. JSLS, 2010; 14(4):579-82. 15. Lightfoot N, Santos P, Nikfarjam M: Paraganglioma mimicking a pancreatic neoplasm. JOP, 2011; 12(3):259-61. 16. Sahdev, Sohaib A, Monson JP, Grossman AB, Chew SL, Reznek RH: CT and MR imaging of unusual locations of extra-adrenal paragangliomas (pheochromocytomas). Eur Radiol, 2005; 15:85-92. 17. Chen H, Sippel RS, O’Dorisio MS, Vinik AI, Lloyd RV, Pacak K: The NANETS consensus guideline for the diagnosis and management of neuroendocrine tumors: Pheochromocytoma, paraganglioma, and medullary thyroid cancer. Pancreas, 2010; 39(6):775-83. 18. Whitson BA, Tuttle TM: Laparoscopic resection of periaortic paragangliomas. Am Surg, 2005; 71:450-454. Pancreas. 2010; 39(6):775-83.
© Copyright 2026 Paperzz