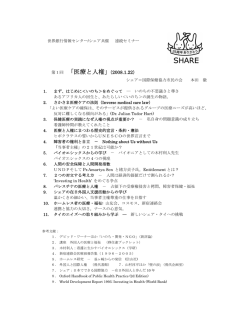
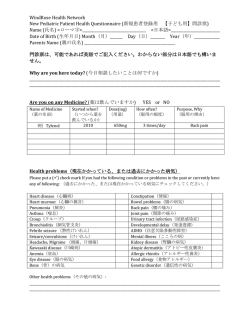
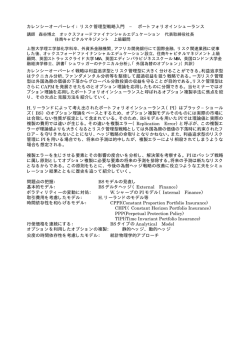
国民健康保険公団のホームページ http://www.nhic.or.kr/ より 国民健康保険公団の紹介 1.理事長挨拶 近年、韓国のヘルスケアシステムはいくつかの画期的な変化を経験している。2000 年 7 月、韓国政府は多数の保険 者の単一保険者と、医薬分業である。この統合改革によって、国民健康保険公団(NHIC)は 2000 年 7 月に設立された。 NHIC は、人々の健康および NHI プログラムにより韓国における社会保障制度の継続的改善を目指す。 韓国で唯一の公衆衛生保険者としての NHIC の最終ゴールは、国民健康保険プログラムによる病気の危険からの適 切な保護と、人々の高度な生活の達成である。 2.国民健康保険公団に関して 2-1.Propose and Vision 国民健康保険公団(NHIC)は、国民健康保険法の第 12 条によって設立された公共団体である。NHIC は、韓国社会保 障領域の重要な組織の 1 つとして、人々の健康および NHI プログラムによって韓国における社会保障制度を継続的に 改良する。 2-2.Major Activities NHIC はその管理法則として 3 つの基本方針をセットした。①科学的管理、②効率的なオペレーション、③社会指向の 管理上のサービスである。2000 年 7 月以来、NHIC はその既存の機能を豊かにし、さらに、統合公衆衛生保険者が韓 国人のヘルスケアの必要性に対応するために活動の範囲を拡張している。 2-3.Organization 2-3-2.幹事会 NHIC の基本方針を決定します。毎年の事業計画、財産のオペレーション、財務計画、予算ドラフトおよび決算の準備、 規則の修正、財産を購入し配置する決定、金銭と弁済の借用、また NHIC のオペレーションその他の重要事項を総括 する。 幹事会は 18 人のメンバーで構成されている。取締役会長は NHIC の理事長で、保健福祉部長は労働組合、雇用者 協会、農民と漁師の協会および消費者の保護団体から 17 人の管理者を任命する。 2-3-3 健康保険財政委員会 健康保険財政委員会は、健康保険金融に関する問題および医療費給付経費の契約を調査する。委員会の主な目 的は、重要な財政問題に関する NHI プログラムの利害関係者の間の意志決定であり、委員会は 30 人のメンバー、10 人は雇被保険者、10 人は自営被保険者、そして 10 人は公益代表からである。 2-3-4 Headquarter 本部には 10 の事業部門、監査と検査のオフィス、研究センターおよび事務局を運営する。 ①計画・調整部、②広報活動部、③総務部、④人的資源管理部、⑤金融管理部、⑥健康保険部、⑦登録&貢献管理 部、⑧情報処理部、⑨健康増進管理部、⑩消費者支援保護部、⑪監査および検査室、⑫健康保険研究センター 1 健康保険公団の組織図 2-3-5 Regional Headquarters and Branch Offices 6 つの地方本部と 227 の支店 全国の 6 つの地方本部および 227 の支店と、被保険者およびその扶養家族は、それらが必要とする日々のサービス に容易にアクセスすることができる。 2 これらのオフィスは、直接の健康保険サービスの提供により NHIC の中核フィールド役割を引き受ける。本部と支店 の間の仲介人として、6 つの地方本部は支店を支援し監督する。個々の地方本部は、支店のフィールド・ビジネスの調 整および支援を管理する。 各支店は、登録管理、貢献賦課および収集のような NHI プログラムの毎日のフィールド・ビジネス、寄付の調節、現 金給付に対する報酬、様々な健康増進活動および供給者の詐欺のヘルスケア・サービスのモニタリングを行なう。 2-3-6 イルサン病院 2000 年 2 月に開院された HNIC イルサン病院は NHIC が所有する唯一の医療機関で、NHI プログラムのためのモデ ル病院として役立ち、ヘルスケア・セクターの公の役割を促進するとともにイルサン市の地元住民のヘルスケア需要を 満たすために設立された。 公衆衛生保険プログラム用のモデル医療施設として、イルサン病院は、供給者の現在の払い戻しスケジュールを評 価し、かつ将来の払い戻しのより合理的な準備を深めるのを支援する重要な役割をとる。 さらに、病院は、最先端技術の設備および技術、およびその美しい環境で有名。保険業者の病院として、病院の使 命の中心となるのは、患者指向の質注意によって患者に役立つ際に優越性に対するその関与である。 新しく建設された 13 階の病院は 744 床を備え 24 の臨床の部を持っている。それは京義道 Baeksuk-dong、Koyang 市に位置する。 イルサン病院年報 年患者数、( )は 1 日患者数 2000 2001 2002 2003 435,012 743,963 833,809 918,285 (1,722) (2,506) (2,817) (3,109) 入院患者 123,766 222,220 237,465 242,331 外来患者 311,246 526,743 596,344 675,954 病床利用率 81.4% 84.4% 87.4% 89.8% 計 2-4.Management Innovation NHI プログラムは、画期的なリストラクチャリングを含む多くの経営革新および改革で構築されている。 常に変わる環境に対処するため、NHIC は様々な管理イニシアチブをとりました。イニシアチブの主な目的は、その経 営過程を改善し、organizational な構造を合理化し、その財政状態を安定させることを支援し、可能な最高品質のサー ビスを安全にすることである。 マンパワーは、1998 年(第 1 の統合改革)時の 15,653 が 5,199(33.2%) にまで縮小された。現在は、10,454 人で合理 的なレベルに管理上のコストを維持し、将来の NHIC の経営効率に貢献している.。 NHIC は、できるだけ保険資金を増大させるため、特にその収集活動の強化および自動銀行口座振替およびクレジッ トカードのような新しい収集方法を導入した。最近、NHIC が既にインプリメントしている政府の手段に加え、多くの収入 を得るための努力によって、NHIC は、財政状態が徐々によくなっているサインが見られる。 さらに、NHI 資金を保護し、 かつ金融を安全化するため、不正行為、および供給者によって提供する不適当なサービスを検知し防止に努力してい る。供給者の詐欺・乱用の慣習を効率的に検知するために、NHIC は、医療を含む一連のモニタリングシステムを導入 した。 3 2-5-1 Health Promotion and Prevention 健康増進と予防 健康増進は NHIC 活動において重要性を増大している。NHIC は、病気を防ぎ、かつ人口の健康を増進するために、 健康教育、無喫煙キャンペーン、禁酒運動などのような健康増進活動に大きな重点を置いている。例えば、毎年、健 康情報と知識に関する小冊子を数十万作成して学校、workplaces、健康機関および軍部隊などを含む様々な組織に それらを配布している。また、健康指向のライフスタイルヘ導く、徒歩の会、走る会およびハイキングする会のような健 康増進を精力的に対応している。 2-5-2 Support for Appropriate Uses of Health Services ヘルス・サービスの適切な用途の支援 NHIC の別の重要な活動は、ヘルスケア・サービスの合理的・博識の用途に保険付きのものをガイドするその新しい 努力である。2002 年以来、NHIC はその主要機関エリアのリストにケース・マネジメント・プログラムを置きました。プロ グラムは、患者を、高血圧症、糖尿病、卒中、腎臓失敗および小児喘息のような慢性の条件と同一視し、かつヘルス・ サービスを賢明に利用し、かつヘルスケア・コストの縮小に従って帰着して、健康なライフスタイルを実行するようにそ れらに活動的に勧めることを目指しています。約束する結果を示す最初のプログラム、およびプログラムで満足な、参 加する患者で、NHIC は、より多くの目標母集団グループをカバーするケース・マネジメント・プログラムを拡張すること を計画します。 また、NHIC は、健康に関連する個々の振る舞いおよびアクションに対する肯定的な影響を及ぼすためにヘルス・サ ービスの過剰ユーザあるいは口汚いユーザがコンサルテーション、推薦およびガイドラインのような保険業者からの特 に教養のある人員による支持物を識別され与えられる別の新しいプログラムを実行しています。この活動は、さらに信 頼できて信頼できる公衆衛生保険の確立に向けての新しいステップのうちの 1 つを表わします。 2-5-3 Active Provision of Health Services ヘルス・サービスの活発な準備 最近、ちょうど高度に産業化された西方の国々でのように、認識されている健康消費者の権利として、consumerism の概念は韓国のヘルスケアの中で出現しています。そこの情況の中で、成長している、製作における活発な役割がそ れらの健康に関して決定に通知したと遊ぶようにそれらを促進するためにヘルス・サービスのユーザに適切な健康情 報を提供する必要があること ニーズを満たすために、NHIC は、人口に、情報準備に関するその役割を強くするために HRA(健康危険度評価)サー ビス、医療施設情報サービスのようないくつかの新しいイニシアチブ、様々な疾病情報サービスなどを導入しています。 情報準備に注目するイニシアチブは、さらに消費者を最初に置いた消費者指向のサービスへの NHIC のオン現にある 努力を表わします。 2-6.Public relations 設立以来、広報活動はその努力を集中させる重要な領域のうちの 1 つでした。NHIC は、活発に適格性と医療費給付 に関する詳細な情報を含む国民健康保険プログラムの内容および手続きの保険付きのものに通知しています。 ラジオ、テレビおよび新聞上の様々な説明的広告によって、公団は公からの好意的な周知を増強し、かつプログラム に参加するようにさらに公を激励するために知識および国民健康保険プログラムに関する情報を流布しています。 さらに、「健康保険」、消費者のための自由なマガジンおよび専門家の公表によって、NHIC は、プログラム上の最新 情報を提供しており、公についてのよりよい理解を促進するためにエキスパートからの主な問題について逐条的に述 4 べます。 また、特に、インターネットの時代に、容易なアクセスのやり方でできるだけ情報と周知の材料を記入して、NHIC は、 連続的に、よりユーザー・フレンドリーで、興味引き起こすものであるためにそのウェブサイトを改良しようとしています。 その結果、顧客は、より多くの興味をもって、それらが必要とするものに容易にアクセスすることができます。 2-7 Research Activities NHIC は、さらに、国民健康保険プログラムの経営陣の中で戦略の、証拠に基づいた意志決定を支援する活動を研 究するその最善の努力を当てています。 研究の重要な義務を始めるために、健康保険研究センターは 2000 年 7 月 1 日に NHIC の内にセット・アップされまし た。研究センターの権限は、健康保険分野での高品質の適用可能な研究結果の生産によって NHI プログラムに関係 のあることを作る政策用の証拠ベースを提供することです。 その権限を完了するために、研究センターは、貢献を徴収し、医療費給付配置、コスト封じ込め手段、供給者の払い 戻しおよび管理などの革新的対処法適切な方法を含む健康保険 affaires の様相をすべて調査します。今日の知識に 基づいた経済で国際的にさえより競争率の高いこと、研究センターモニター、また社会保障を分析する、韓国のよりよ い健康保険制度の開発に他の国々からの価値のある経験および結果をもたらすために世界的に向かいます。 研究センターは、さらに、ヘルスケア研究ニーズをより十分に満たし、かつこれらの考えと発見物を政策とプログラム に翻訳するために学術的なセクターのエキスパートと同様に他の研究機関との協力に活動的に従事しようとしていま す。 NHIC の研究努力は、国の健康保険制度の改良に非常に寄与しています。完全にこれらの活動の重要性を認識して、 NHIC は、詳細な研究活動を促進するその努力を継続するでしょう。 2-8.Electronic Date Processing System スーパーハイウェーコミュニケーション・ネットワークによる、本部および 6 つの地方本部を接続するために、国民健 康保険の電子データ処理システム(EDPS)を利用することによって、健康保険サービス情報は国のどこにおいても情報 を提示することができる。 本部では、データ・ベース・システムは、ヘルスケア・コストに対する報酬の領域をカバーします、組織の経営陣は人 間ドック登ります、適格性インデックス、健康治療レコードなど 地方本部では、それは適格性管理、寄付の収集および健康利点記録をカバーします。 NHIC は、本部および 6 つの地方本部で 6 種類のデータ・ベースを持っています。 データ・ウェアハウス・システムは、情報アクセスのための時間を短くし、「OLAP」分析ツールを使用して、データを直 接探索し分類することにより情報準備プロセスを増強します。データ・ウェアハウス・システムは、多次元の分析および データ・サンプリングを通じて意志決定に寄与する種々の情報の提供により、統計分析機能を強くします。 Electronic data interchange EDI system NHI ビジネスのために導入されたEDIシステムには 2 つのタイプがある。ひとつは NHIC と workplcaces の間にオンライ ン EDI で、他のひとつは医療機関と健康保険審査評価院を介する医療機関用の EDI システムである。EDI システムは、 1997 年 7 月から導入されている。 5 EDI システムを採用している事業所数 年 2001 2002 2003 全事業所数 363,210 416,607 489,384 EDI 採用事業所数 28,478 69,682 108,970 7.8% 16.7% 22.3% EDI 比率 EDI を採用する workplces の数は、2001 年の 7.8%から、2003 年の 22.3%まで、確実に増加しています。20 人を越える workplaces においては、2003 年に 66.7%までになっています。 2.EDI システムを採用している事業所数(2003 年) 全事業所 事業所数 被保険者数 3 被保険者数が 20 人 被保険者が 20 人 未満の事業所 以上の事業所 対象 EDI 採用 対象 EDI 採用 対象 EDI 採用 事業所数 事業所数 事業所数 事業所数 事業所数 事業所数 489,384 108,970 428,775 (22.3) 8,804,906 5,388,773 (61.2) 68,522 60,609 (16.0) 2480,877 602,661 (24.3) 40,448 (66.7) 6,324,029 4,786,112 (75.7) SOCIAL SECURITY OF KOREA 3-1 SOCIAL SECURITY SYSTEM 韓国で社会保障制度を導入する努力は、社会保障と保護関連の法整備を行った 1960 年代から初まった。1960 年代 の高度経済成長は、韓国の政府が韓国で社会保障のフレームワークとして主な社会保険プログラムを導入することを 可能にした。 この分野での著しい進歩は、政府が医療保険プログラムを始めた 1970 年代に得られました。1977 年には、民間会 社の従業員のための医療保険プログラムが導入されました。1979 年には、別の同様の保険プログラムが公務員およ び私立学校従業員のためにインプリメントされた。しかしながら、それは、1988 年まで、田園地帯の、および 1989 年ま で自営業の(都市のエリアの自営業のすべてのもののためのプログラムがインプリメントされたという)すべてのものま で医療保険プログラムが延長されたということではない。人々の社会的保護の増加で、韓国の健康保険制度は急速 に発展した。 6 近年、韓国経済は厳しい困難を経験しているが、韓国の社会保障制度はより高いレベルに改善されている。 人々のニーズの増大に応じて最近の 30 年間、政府は国民健康保険、失業の保険、国民年金保険および業務災害 補償保険と、様々な社会保障制度を導入し、それを強化することによってクオリティー・オブ・ライフを改善するために 努力している。韓国の社会保障制度は広くあります、社会保険プログラム、公の援助計画および社会福祉事業プログ ラムから構成された談話。図は、韓国の全面的な社会保障制度を示します。 3-2 HEALTH SECURITY SYSTEM 韓国の健康安全保障制度は、人々の健康を促進し、かつ、疾病、傷、誕生および死に必要なヘルスケア・サービス などを提供することにより、社会保障を改善するために追求します。韓国で、健康安全保障制度として普通の人々の ための国民健康保険プログラムおよび低収入の世帯のための医療扶助プログラムがあります。 韓国の NHI プログラムは強制的社会保険方式として全住民をカバーしている。その主な財源は保険と国庫補助であ る。 ヘルスケアの給付は現物給付と現金給付とがあり、ヘルスケアのタイプごとに複雑な自己負担が設けられている。 患者は供給者が自由に選択できる。西洋医学か東洋医学かを選ぶこともできる。 NHI プログラムの管理は NHIC が行い、健康保険審査評価院(HIRA)は供給者の請求の調査を担当し、保健福祉部は 全体としてそのオペレーションを監督します。 医療扶助プログラムは、低収入の世帯の最小の生計を安全とし、医療サービスの提供によってその自助を支援する ために公の援助制度として設けられている。一般所得者と低所得者の間の溝によって生じる健康不平等の社会問題 に直面する政府は、1977 年に医療扶助行為を 1979 に低所得者に本質的な医療サービスを供給するためにこのプロ グラムを開始した。 4 NATIONAL HEALTH INSURANCE PROGRAM 4-1 BRIEF HISTRY OF NHI 出来ず 4-2 関連法規 大韓民国の国民健康保険プログラムは 2 つの法規で規制されている。 1 つは 1999 年 2 月 8 日に公布された国民 健康保険法で、他のひとつは期限を設けた法として、2002 年 1 月 19 日に発布された国民健康保険の金融安定化のた めの特別法である。 国民健康保険法の主な目的は、単一の保険者に多数の社会保険を統合し、調達資金の管理上の効率および公正 を増強し、人々のための健康予防および促進を含む総合保健を提供することである。 安定化のための特別法は、健康保険制度を持続させるため、収入と消費の間のバランスを維持し、NHI を金融危機 から保護するために立法化され、有効期限は 2006 年 12 月 31 日までとなっている。 特別法は国庫補助によってあるレベルの資金を安全にするために政府の金融責任を規定したものである。 4-3 POPULATION COVERAGE 4-3-1 Mandatory coverage 人口のすべてをカバーする韓国の健康保険制度は、韓国の社会保険方式の主たるものであり、僅かの医療扶助受 益者を除き、韓国在住韓国人の義務となっている。 国民健康保険プログラムには、雇用被保険者と自営被保険者の 2 つのカテゴリーに分類される。 7 4-3-2 Covered population 2004 年 10 月に、NHI によってカバーされた人数は 4700 万で人口の 96.9%に達しており、残りの 3.1%にあたる 150 万 の極貧または低所得層は医療扶助プログラムによって援助計画でカバーされる。 対象人口 (単位 1000 人) 保険者 被保険者 人 数 全人口 48,199 小 計 健康保険制度 健康保険制度 医療扶助制度 4-3-3 比 率 地方政府 47,322 96.9% 雇用被保険者 25,676 52.6% 自営被保険者 21,646 44.3% 低所得者 1,496 3.1% Category of the Insured 保険付きのもののカテゴリー 健康保険プログラムによってカバーされる従業員は、民間企業の従業員、軍人を含む政府従業員および私立学校 従業員を含み、それらの扶養家族も同様にカバーする。 しかし、雇用が 1 か月当たり 80 時間未満の日雇い賃金労働者は、保険に入った従業員のカテゴリーからは除外され る。 雇用被保険者数 (単位:1000 人) 1998 1999 2000 2001 2002 2003 企業数 182.3 199.8 222.9 363.2 405.7 477.5 従業員数 6,536 6,803 7,268 7,885 8,323 8,712 扶養家族数 14,268 14,914 15,136 15,281 15,429 15,886 2.18 2.19 2.08 1.94 1.85 1.82 扶養比 自営被保険者 企業の従業員のカテゴリーから除外された個人、自営業者はカテゴリーに含まれる。さらに、外国駐在の韓国人およ び韓国に滞在する登録外国人は、自由意志によって国民健康保険プログラムに加入できる。 8 自営被保険者数 (単位:1000 人) 世帯数 被保険者数 被保険者/世帯 1998 1999 2000 2001 2002 2003 7,900 8,005 8,215 8,564 8,7701 8,761 23,665 23,467 23,492 23,213 22,908 22,465 3.00 2.93 2.86 2.71 2.63 2.56 4-3-4 外国人 外国人は諸条件を満たせば NHI プログラムが適用される。 2005 年時点で、204,319 人の外国人が NHI プログラム によってカバーされている。 4-4 HEALTH INSURANCE FINANCIAL 国民健康保険は払われた寄付を通じて融資されます、保険がつけられた、そしてそれらの雇用者、また国庫補助。 国民健康保険プログラムが社会保険プログラムとして実行されたとともに、保険付きのものからの寄付、プログラムの その収入の主な源を構成します。 4-4-1 Contribution 保険者の組織的な統合は、2000 年 7 月に完全に実現されたが、雇用保険者と自営業者の保険財源の共同化は 2003 年 7 月 1 日に実現され、それまでは別々に管理されてきた。保険金を計算する定式は、2 つのカテゴリーの保険 者の間で異なったものであった。 国民健康保険行為によれば、NHIC で設立された健康保険財政委員会には、月給または給料の 8%未満の範囲内に保 険に入った従業員のために貢献割合を設定する能力があります。しかしながら、国民健康保険の金融安定化のため のスペシャル法の下では、貢献割合を設定する機能は厚生省で設立された健康保険政策批評委員会に上方へ渡さ れました。 Contribution Rates ( )は年伸び率 雇用被保険者 Contribution Rates 自営被保険者 Value per Point 2001 2002 2003 2004 2005 3.4% 3.63% 3.94% 4.21% 4.31% 100 ウォン 106.7 ウォン 115.8 ウォン 123.6 ウォン 126.5 ウォン (6.7%) (8.5%) (6.75%) (2.35%) 寄付に対する報酬は世帯の雇用者およびすべてのメンバーの責任です。それらは翌月の 10 日目までに毎月の貢献 を払うために要求されます。支払いの任意の失敗の場合には、保険業者(NHIC)が、法則の適切な条件に従って高圧 的な収集を実行することができました。 The Employee Insured The contribution of employee insured is based on the gross salary or wage of the insured.And the contribution rate of the employee insured is 4.31% for employees in private sector and for government and private school employees as well. 保険に入った従業員の貢献は、保険付きのものの総体の給料か賃金に基づきます。また、保険に入った従業員の 貢献割合は、民間部門の従業員のために、および政府と私立学校の従業員のために同様に 4.31%です。 The contribution of the employee insured is borne by both employee and employer.For employees in private sector, the employer pays 50% of the contribution and the employee pays the other 50%.For government employees, the government, as their legal employer, pays 50% of the contribution, and the public servant pays the other 50%.For private 9 school employees, however, the owner of the private school pays only 30%, the government subsidizes 20% of the contribution and the employee pays the remaining 50%. 保険に入った従業員の貢献は従業員と雇用者の両方によって生まれます。民間部門の従業員のために、雇用者は、 貢献の 50%を払います。また、従業員は他方に 50%を払います。政府従業員のために、政府は、彼らの法的な雇用者 として、貢献の 50%を払います。また、官吏は他方に 50%を払います。私立学校従業員のために、しかしながら、私立学 校の所有者はわずか 30%しか払いません。政府は、貢献の 20%に補助金を交付します。また、従業員は残りの 50%を払 います。 保険料の割当額と徴収額 (単位:10 億ウォン) 年 合 計 自営被保険者 雇用被保険者 割当額 徴収額 % 割当額 徴収額 % 割当額 徴収額 % 2003 13,740.8 13,427.7 97.7 4,572.5 4314.5 94.4 9,168.3 9,113.2 99.4 2002 10,860.1 10,840.9 99.8 4,055.8 4,049.3 99.8 6,804.3 6,791.6 99.8 2001 8,856.2 8,779.8 99.1 3,615.4 3,562.2 98.5 5,240.8 5,216.6 99.5 2000 7,228.8 6,891.3 95.3 3,099.9 2,776.1 89.6 4,128.9 4,115.2 99.7 1999 6,305.6 6,097.2 96.7 2,726.7 2,526.6 92.7 3,578.9 3,570.6 99.8 1998 5,255.0 4,991.6 95.0 2,403.5 2,154.1 89.6 2,851.5 2,837.5 99.5 The Self employeed Insurance For the self-employed insured, contributions are basically calculated on the basis of income.The contributions are calculated by using a formula in which the insured persons' properties, income, motor vehicles, age, and gender are taken into consideration. 自営業のために、保証した、寄付は、収入に基づいて基本的に計算されます。その寄付は、保険に入った人の特性、 10 収入、モータ乗り物、時代およびジェンダーが考慮に入れられる定式の使用により計算されます。 However, there are two types of formula for the calculation of the self-employed insured's contributions.Two different formulas apply to two different income groups :the one group for individuals whose income is less than 5 million won each year, and the other for individuals whose income is 5 million won or more each year. しかしながら、自営業の insured の寄付の計算の 2 つのタイプの定式があります。異なる 2 つの定式が 2 つの異なる 所得階層とは当てはまります:その収入が 500 万未満である個人のための 1 つのグループは、その収入が毎年 500 万 ウォン以上である個人のために毎年および他方を勝ち取りました。 The total contribution amount of the self-employed insured is set by their total contribution points and value of each point.Currently, the value per point is set at 126.5 won.The calculated contribution is paid by the insured.And the government subsidizes about 50% of total expenditures for both the payment of benefits for the self-employed insured and its administrative costs. 合計の貢献量、自営業、保険がつけられた、それらの完全な貢献ポイントおよび各ポイントの値によってセットされま す。現在、1 つのポイント当たりの値は 126.5 ウォンでセットされます。計算された貢献は、保険がつけられたことによっ て払われます。また、政府は、自営業のもののための利点に対する両方の報酬に対する費用の合計の約 50%に補助 金を交付します、保証した、またその管理上のコスト。 Reduction and Exemption of Contributions For the employee insured, persons who are working in an underserved area like islands or remote rural areas, or working in a foreign country with any dependent living in Korea have 50% reduction in monthly contributions.Also for the self-employed insured, some portion of contribution can be reduced for the insured who resides in underserved areas, who has a family member aged 65 or over, or who has the disabled insured registered pursuant to the Welfare Act for the Disabled. 保険に入った従業員のために、島あるいは遠隔の田園地帯のように不当なエリアで働いているか働いている、韓国 で任意の依存する生活を持った外国の人は、毎月の寄付の 50%の縮小を持っています。さらに自営業のために、保証 した、貢献のある部分は、不当なエリアに駐在するか、この人は 65 歳以上の家族を持っているか、この人は不具のも のを持っている、人(保険に入った)のために縮小することができます、不具のもののためのウェルフェア法に準ずるよ うに登録されて保証しました。 Insured persons who are working in a foreign country with no dependents in Korea, military personnel serving military obligations, or insured persons detained in correctional institutions are exempted from paying contributions. 韓国(軍事の義務に役立つ軍人)で扶養家族なしで外国で働いているか、刑務所で拘留された人を保証した、保険に 入った人は、寄付を払うのを免除されます。 4-4-2 国庫補助 金融安定化のための特別法による国庫補助は、タバコ販売の総合課税と付加料金によってまかなわれる。 政府援助 単位:100 万ウォン 年 政府援助 一般税 計 タバコ収益 2001 2,625.0 - 2,625.0 2000 2,574.7 439.2 3,013.9 11 4-4-3 MAGER HEALTH INSURANCE DATA The National Health Insurance is financed through the contributions paid by the insured and their employers, and government subsidies.As the National Health Insurance program has been run as a social insurance program, the contributions from the insured constitutes the major source of its revenue of the program. 国民健康保険は払われた寄付を通じて融資されます、保険がつけられた、そしてそれらの雇用者、また国庫補助。 国民健康保険プログラムが社会保険プログラムとして実行されたとともに、保険付きのものからの寄付、プログラムの その収入の主な源を構成します。 Major Health Insurance Data メージャー健康保険データ xpenditure against revenue ratio has been increased until 2001 since the separation of prescribing and dispensing lead a steep increase of medical fees while the modest increase of contribution rate has not kept with medical fees increase. 貢献割合の適度の増加が医療費増加で続いていない間に、2001 が分離以来規定と分配に医療費の急激な増加を リードするまで、収入比率に対する消費が増加させられました。 From 2002, however, balance between expenditure and revenue has been improved thanks to government subsidy, collection ratio on contribution, and all concerned parties' efforts to achieve sound finance of NHI. 2002 年から、しかしながら、消費と収入の間のバランスは、国庫補助、貢献中の代金回収率および NHI の健全財政 を達成するすべておるパーティーの努力への改善された感謝でした。 Major Health Insurance by Year 1999 2000 2001 2002 2003 保険加入者 4,5184 45,896 46,,379 46,659 46,963 Total 8,8925 9,827,717 11,928,330 14,305,319 17,466,651 revenue Total Contributions 1000 人 100 万ウォ ン 9,610,122 10,744,194 14,105,819 14,798,463 15,972,379 expenditures Ratio 単 位 100 万ウォ ン 108.1 109.3 118.3 103.4 91.4 7,291,118 8,609,783 11,322,718 13,811,740 17,028,319 % 100 万ウォ ン e Insurance 7,947,963 9,285,605 13,195,616 13,823,665 14,893,489 benefits Net ratio Annual 100 万ウォ ン 109.0 107.8 116.5 100.1 87.5 % 162,925 187,432 245,659 297,005 362,593 ウォン 177,602 202,144 285,294 297,261 317,135 ウォン contribution per person Annual benefits costs 12 4-5 INSURANCE BENEFIT 4-5-1 INSURANCE BENEFIT 国民健康保険行為の第 39 条によるヘルスケアの処置の範囲やその上限などの健康保険給付の標準は、保健福祉 部規則によって決められる。 保険給付の内容 Health Insurance Benefits 便益の受領者 医療給付 被保険者および扶養者 健康診断 被保険者および扶養者 一部負担の払い戻し 被保険者および扶養者 葬祭費 葬祭実施者 一部負担の補償 被保険者および扶養者 機材の損耗 被保険者および扶養者 現物給付 現金給付 保険の支出 単位:100 万ウォン 年 1998 1999 2000 2001 2002 2003 計 現物給付 現金給付 6,687,188 6,584,518 102,670 7,780,440 7,652,875 127,565 (16.3) (16.9) (24.2) 8,928,518 8,789,329 139,189 (14.8) (14.9) (9.1) 13,059,994 12,940,603 119,391 (46.3) (47.2) (-14.2) 13,539,386 13,424,536 114,850 (3.7) (3.7) (-3.8) 14,864,830 14,755,199 109,631 (9.8) (9.9) (-4.5) 第 1 次積算 第 2 次積算 分配、配分の変更 8 診断群に DRG 導入 医療費給付は診断、検査、投薬、医用材料、治療、手術、予防のケア、リハビリテーション、入院、看護および輸送を 含んでいる。健康保険で治療を受ける場合、保険者および扶養家族は、予定原価に共通のパーセンテージまたは一 定額を支払う。日常生活に必要とは考えられないサービス、例えば、形成外科などは NHI プログラムによってはカバー されない。 高血圧症、糖尿病、肝臓病および肺結核のような慢性の退廃的な疾病の早期発見および治療を保証するために、 NHIC は健康診査サービスを提供しており、2 年に一度は 40 歳以上の被保険者および扶養家族は、健康診断を無料で 受けることができる。 受益者は、毎年胃癌、結腸癌および直腸癌のための検査を申し込むことができる。乳癌検査の費用も NHI によって 賄われる。また、肝臓癌検査費用は肝臓疾病と関連したと診断された人の場合は賄われる。 Refunding Allowance for Health care 13 The Refunding Allowance for Health Care is payable when a beneficiary receives health care treatments in an emergency situation at a health care institution which has been excluded from the health care providers under the National Health Insurance system.In this case, the NHIC pays back the beneficiary the expenses amounting to the applicable health care costs as a refunding allowance.Documentations proving in details the provision of the health care treatments must be submitted to NHIC for the compensation of the health care costs. 受益者が国民健康保険システムの下のヘルスケア供給者から除外されたヘルスケア機関の非常時局のヘルスケア 治療を受ける場合、ヘルスケアのための払い戻す費用は払うべきです。この場合、NHIC は、払い戻す手当てとして適 用可能なヘルスケア・コストになる経費を受益者に後ろに払います。ヘルスケア処理の準備がそうでなければならない 詳細の中で証明するドキュメンテーションは、ヘルスケア・コストの補償用の NHIC に従いました。??? 葬式費用は受益者が死亡した場合、葬式を担当している人に 250,000 ウォンを支払う。 Compensation for Excessive Co-payment The Compensation for Excessive Co-payment is payable when the insured or dependents received treatments at health care institutions and made co-payments exceeding 1,200,000 won within 30 days;the insured will be compensated 50% of the exceeding amount by NHIC.This compensation mechanism has been introduced to alleviate excessive financial burden of beneficiaries arising from high co-payments. エクセッシブの共同支払いに対する賠償金は払うべきです、いつ、保険がつけられた、あるいは、扶養家族はヘルス ケア機関で治療を受けて、30 日以内に共同支払いの過度の 1,200,000 ウォンを作りました; 保険付きのものは NHIC による過度の量の償われた 50%になるでしょう。この補償メカニズムは高い定額自己負担から発生する受益者の過度 の財政負担を緩和するために導入されました。 Appliance Expenses for the Disabled 不具者のための器具経費は、経済的支援として支払われる。給付は杖、支え、車椅子、視界不良、義眼、虫眼鏡用 の補足的な眼鏡、補聴器などの医療器具は相当する。 4-5-2 保険適用外 単純な疲労および違和感、斑点、にきび、いぼの除去、単純ないびき対策、疾病でない包茎手術、二重まぶた成形、 隆鼻術、豊胸手術/胸縮小、脂肪吸引のようなプラスチック(化粧品)手術およびその副作用の治療、斜視修正。 眼鏡とコンタクトレンズのための代案としての視覚的な修正、任意の健康診断、予防免疫接種。 歯科衛生のための規則的なスケーリング。 運動病気予防および非喫煙のための処理。 遺伝疾病など胎児の細胞分析。 予防医療。 正常なベッドに代わるアメニティー・ベッドの入院用追加費用 、入院中の食事チャージ。 援助者、補聴器、眼鏡およびコンタクトレンズのような器具など。 補助生殖技術、父性テスト。 歯の回復の器具(prosthetic な資料および歯の専門家料金を含んで) Additional cost according to the Regulation of Selective Cares where a patient receives selective cares in accordance with the article 37(2) of Medical Service Act 14 患者が、個 37 の医療サービス行為(2)に従って選択的な注意を受け取るところで、選択的な注意の規則による追加費 用 新しい医学の技術など、厚生大臣&ウェルフェアはそれを決定していません/この施行規則による、保険給付あるい は非利益として気づいた、新しい医学の技術などを除いて、11(1)あるいは 13(1)それは遡及して記事 11(4)、およびこ の施行規則の記事 13(1)の後の部分の準備による保険給付に含むことができる。 Diagnosis?treatment?operation and other medical care, drug or medical material which is decided and noticed by the Minister of Health&Welfare owing to obscurity of economic efficiency in suppling health care benefits such as cost effectiveness, etc. Diagnosis?treatment?operation、および他の医療(コスト有効性などのような医療費給付をしなやかにする際に経済 効率の不明瞭に起因する Health&Welfare の大臣によって決定され気づかれる薬か医用素材)。 In the case that the relevant medical services, drugs, or medical materials, etc. impose a heavy burden on National Health Insurance Finance 適切な医療サービス、薬または医用材料が国民健康保険財政に重い負担を課するもの (a) 超音波イメージング (2006 年 12 月 31 日まで) コスト、有用性が他の医療サービス、薬または医用材料に置き換えができる比較的高価なもの(2004 年 12 月 31 日ま で) 保健福祉部大臣が規定しないすべての医療サービスおよび医用素材 DRG との関係なしで投与されるすべての薬 東洋の理学療法(空気・水治療法、電気療法、温熱療法などを含む) 漢方の医学書の処方に基づいた漢方のパック薬および漢方生薬 4-5-3 RESTRICTION OF BENEFIT Even though any ensured person keeps enrollment, the insured can not get health insurance benefits if the insured comes under one of the following cases:when injury was deliberately caused or due to criminal actions;when the insured person intentionally violated the instructions or regulations of the NHIC or health care institutions;when the insured person intentionally disregarded the inquiry or diagnosis of the NHIC or health care institutions;or when the insured person has already been compensated for the injuries or diseases that happened at work or during on public duty from other social security programs like Industrial Accidents Compensation Insurance. たとえいずれかの保証された人が登録を維持しても、保険付きのものが次の場合のうちの 1 つの下に入る場合、保 険付きのものは健康保険利点を得ることができません: 傷はいつ慎重に引き起こされたか。あるいは、刑事訴訟に予定されていたか;保険に入った人は、いつ故意に NHIC ま たはヘルスケアの機関の指示か規則を破ったか;保険に入った人は、いつ故意に NHIC またはヘルスケアの機関の質 問か分析を無視したか;あるいは、保険に入った人が働いて起こった傷あるいは疾病のために既に償われた場合、あ るいはに、業務災害補償保険のような他の社会保障制度からの公の義務上で。 In addition, any medical care that has nothing to do with the treatments required to get rid of hinderance in working or daily living activities are not covered by the National Health Insurance program.So the costs of drugs or medical materials for simple fatigue, hair loss, freckles, warts, hirsutism, acne, impotence, hereditary deformity of genitals, simple snoring, plastic surgery, and operations to correct eyesight are not covered by the NHI program. さらに、全く働くことで hinderance を取り除くのに必要な処理と関係がないどんな医療あるいは日常生活活動も、国民 健康保険プログラムによってカバーされません。したがって、単純な疲労、脱毛、斑点、いぼ、hirsutism、にきび、無力、 15 genitals の遺伝的不具、視力を修正するために単純にいびきをかくこと、形成外科および手術のための薬か医用素材 のコストは、NHI プログラムによって賄われません。 4-5-4 DURATION OF BENEFIT 1 年当たりの健康保険用の利益時期は 1998 年までは 300 日、1999年にからは 330330日に延長された。その場 合でも 65 歳以上に対しては制限なくカバーされた。 2000 年 7 月 1 日から、利益時期は 365 日に延長された。 4-6 COP-PAYMENT SYSTEM ヘルスケア治療を受ける人は、国民健康保険法の第 41 条による定額自己負担として、ヘルスケア・コストのある部 分を、ヘルスケア機関に直接支払う。 Co-payment Ceiling System The Co-payment Ceiling System has been introduced since July 1, 2004 as a health insurance safety net.The system is designed to protect people who pay high co-payments.When an insured individual pays for co-payments exceeding the co-payment ceiling threshold currently set at 3 million won within a period of 6 consecutive months, he or she is exempted from any further co-payments occurred.This is to alleviate financial burden of households against catastrophic or high-cost diseases helping to prevent them from falling into bankruptcy.This ceiling system is applicable for inpatient, outpatient, and pharmaceutical services. 定額自己負担の上限は、健康保険の安全ネットとして 2004 年 7 月 1 日以来導入された。このシステムは、高額の自 己負担を払う人々を保護することを目指しています。自己負担金が上限値を越えて支払う場合、6 か月連続の期間内 の 300 万ウォン以上の支払いが免除されます。このシーリングは入院、外来および調剤に対して適用される。 ○入院診療 患者が、クリニック、病院あるいは総合病院で受診する場合、チャージの 20%の支払いが求められる。 ○外来診療 外来ケアのための自己負担は、医療施設のレベルあるいは合計金額によって変化する。 医院で提供される外来診療については、完全なチャージが 15,000 ウォン(歯科医院での; 3,500 ウォン)を超過しない 場合、患者は 3,000 ウォンを払わなければなりません。しかしながら、完全なチャージが 15,000 ウォンを超過しない場 合、初老の患者はわずか 1,500 ウォンしか払いません;患者は、完全なチャージが 15,000 ウォンを超過する場合に診断 料金を含む完全な料金の 30%を払います。 For outpatient services provided at a hospital or a general hospital, 40% or 50%, respectively, of the total charges is paid for co-payment.And, when a patient visits a hospital or a general hospital in remote and rural areas for outpatient services, the patient, if the total cost does not exceed 15,000 won, pays 4,100 won or 4,600 won, respectively, if exceeding 15,000 won, pays 35% or 45% of total costs, respectively.However, at a specialized general hospital the patient has to pay 50% of the total charges, excluding the diagnosis and consultation fee. 病院または総合病院で提供される外来診療については、40%あるいは 50%がそれぞれ、完全なチャージに定額自己 負担に払われます。そして、患者が外来診療用の遠隔・田園地帯の中の病院あるいは総合病院を訪れる場合、患者、 全コストは 15,000 ウォンを超過しない、4,100 ウォンあるいは 4,600 ウォンを払う、それぞれ、15,000 ウォンを超過する 場合、全コストの 35%あるいは 45%を払う、それぞれ。しかしながら、専門の総合病院では、患者は、診断と相談料以外 に、完全なチャージの 50%を払わなければなりません。 16 患者の一部負担金 入院 医療機関の 医療機関の所在 一部負担金 種別 地 全種 全地域 20% 総合専門病 全地域 (診察料+相談料)+(全費用の 50%) 都市エリア 全医療費の 50% 院 総合病院 病院 田園地帯 都市エリア 歯科病院 漢方病院 田園地帯 外来 漢方診療所 15,000 ウォン未満の場合:4,600 ウォン 全医療費の 40% 15,000 ウォンを超えた場合:全費用の 35% 15,000 ウォン未満の場合:4,600 ウォン 15,000(歯科は 3500)ウォンを超えた場合 診療所 歯科医院 15,000 ウォンを超えた場合:50% 全費用の 30% 全地域 15,000(歯科は 3500)ウォン未満の場合 -3,000 ウォン(65 歳未満) 保健所 -1,500 ウォン(65 歳以上) 10,000 ウォンを超えた場合:全費用の 30% 処方せんありの場 合 10,000 ウォン以下の場合 -3,000 ウォン(65 歳未満) -1,500 ウォン(65 歳以上) 薬 局 4,000 ウォンを超えた場合:全費用 40% 処方せんなしの場 合 4,000 ウォン以下の場合 -1,400 ウォン(薬剤が 1 日分の場合) -1,600 ウォン(薬剤が 2 日分の場合) -2,000 ウォン(薬剤が 3 日分以上の場合) 4-7 HEALTH CARE DERIVAERY SYSTEM 4-7-1 PROCEDURE n principle, all the medical facilities in Korea are by law required to provide medical services covered by the NHI to the insured patients. 韓国で医療施設はすべて、保険に入った患者への NHI によってカバーされた医療サービスを提供するのに必要な法 則に原則としてよります。 手続き Beneficiaries are required to receive the first-stage health care treatments and then are allowed to receive the second-stage health care treatments (supplied by specialized general hospitals) in due sequence except in such cases as:emergency situations, giving birth to a child;receiving dental treatments;in addition, when disabled persons who are registered according to the Disabled and Welfare Act or when persons acknowledged as needing treatment in specialized rehabilitative care receive health care treatments in rehabilitative care departments. 17 受益者は、初期ヘルスケア治療を受けることを要求され、次に、次のような場合以外においては正当のシーケンスで 第 2 の段階ヘルスケア治療(専門の総合病院によって供給された)を受けることを認められます:子供を生む非常時局; 歯の治療を受けること;さらに、無効になった時、不具でとウェルフェア行為によって登録される人、あるいは、専門の rehabilitative なケア中の治療を必要とするように定評ある人が rehabilitative なケア部の中のヘルスケア治療を受ける 場合。 The first-stage health care treatments refer to the cases when beneficiaries receive health care treatments at health care facilities other than specialized general hospitals. 受益者が、専門の総合病院以外の医療施設でヘルスケア治療を受ける場合、初期ヘルスケア治療はその場合に言 及します。 The second-stage health care treatments refer to the cases when beneficiaries receive health care treatments at specialized general hospitals.When receiving the second-stage health care treatments, beneficiaries should carry a referral issued by the doctor who provided the first-stage health care treatments or the results of a health checkup showing the doctor's opinion that the patient is diagnosed as needing further medical treatments. 受益者が専門の総合病院でヘルスケア治療を受ける場合、第 2 の段階ヘルスケア治療はその場合に言及します。 第 2 の段階ヘルスケア治療を受ける場合、受益者は、初期ヘルスケア治療を提供した医者あるいは患者がさらに医療 を必要とすると診断されるという医者の見解を示す健康診査の結果によって出された referral を運ぶべきです。 In accordance with Article 7 of the Regulation on Health Care Treatment Standards, health care institutions have to issue receipts for health care costs to beneficiaries who have received health care treatments.Furthermore, if a beneficiary demands a detailed explanation of health care costs, health care institutions have to issue the relevant specifications. ヘルスケア治療基準に関する規則の第 7 条に従って、ヘルスケア機関は、ヘルスケア治療を受けた受益者へのヘル スケア・コストの領収書を出さなければなりません。更に、受益者がヘルスケア・コストの詳細な説明を要求すれば、ヘ ルスケア機関は適切な仕様書を出さなければなりません。 4-7-2 HEALTH CARE INSTITUTION In principle, all the medical facilities in Korea are by law required to provide medical services covered by the NHI to the insured patients. 韓国で医療施設はすべて、保険に入った患者への NHI によってカバーされた医療サービスを提供するのに必要な法 則に原則としてはよります。 韓国で医療施設のベッドの 90%以上は、民間部門によって経営されています。薬局はすべて個々の薬剤師によって 所有され経営されています。 4-8 PAYMENT OF MEDICAL FEE 4-8-1 FEE SCADULE AND PAYMENT Basically, the health care benefit costs are reimbursed by fee-for-service.For setting the fee-schedule, the Minister of Health & Welfare first determines the point value of each medical service unit based on the RBRVS (Resources-based relative-value scale) after receiving the decision on the matters from the National Health Insurance Deliberation and Coordination Committee (currently, Health Insurance Policy Review Committee under the Special Act for the Financial Stability of Health Insurance) which is composed of representatives from the insurer, the insured,the employer, the professional associations and the public.And then, the president of the NHIC and the chairman of the Medical Care Fee Contract Committee, which is established in the providers's circle, negotiate to set the monetary value per unit of medical services annually. 18 医療機関の施設数 2000 2001 2002 2003 61,836 62,744 65,471 67,801 総合病院 288 278 283 284 病 院 680 706 780 852 19,690 21,340 22,728 23,554 60 71 90 102 10,607 10,790 11,145 11,522 140 139 149 151 7,249 7,558 8,119 8,650 助産所 127 87 82 70 保健所 3433 3403 3390 3403 薬 局 19,562 18,372 18,705 19,213 合 計 医科診療所 歯科病院 歯科診療所 漢方病院 漢方診療所 基本的に、医療費給付コストはサービスに対する料金によって償われます。料金スケジュールを決めるために、厚生 大臣&ウェルフェアは、最初に保険業者からの代表から構成される国民健康保険熟慮および調整委員会(現在健康保 険の金融安定性のためのスペシャル法の下の健康保険政策批評委員会)からその問題に関する決定を受け取った後 に RBRVS(資源に基づいた相対価値基準)に基づいた各医療サービスユニットのポイント価値を決定します、保険がつ けられた、雇用者、専門職協会および公。また、その後、NHIC の社長および医療料金契約委員会の議長(それは providers の円に身を落ち着ける)は医療サービスの 1 ユニット当たりの金銭価値を毎年セットするために交渉します。 新しい支払い方式の試行として、7 つの診断のグループ用の DRG システムが 2002 年 1 月に入院患者治療サービス に限って導入されました。7 つの診断グループは、レンズ挿入、扁桃腺またはアデノイド摘出、肛門手術、鼠蹊部また は大腿ヘルニア手術、虫垂炎手術、子宮手術ならびに帝王切開で、現在、約 2000 の医療機関が、DRG 支払いに自由 意思で参加しています。 薬および医療材料のコストの償還の上限は保健福祉部長官が設定します。 サービス形態別の医療費経費 (単位:100 万ウォン、%) 年 合計 1998 1999 2000 2001 2002 2003 医 療 薬剤 小計 入院 外来 6,584,518 6,422,392 2,692,914 3,729,478 162,126 7,652,875 7,452,126 3,059,082 4,393,044 200,749 (16.9) (16.0) (13.6) (17.8) (23.8) 8,789,329 7,941,467 3,144,118 4,797,349 847,862 (14.9) (6.6) (2.8) (9.2) (322.3) 12,940,603 9,531,674 3,533,114 5,998,560 3,408,929 (47.2) (20.0) (12.4) (25.0) (302.1) 13,424,536 9,795,667 3,653,241 6,142,426 3,628,869 (3.7) (2.8) (3.4) (2.4) (6.5) 14,755,199 10,798,375 4,354,138 6,444,237 3,956,824 (9.9) (10.2) (19.2) (4.9) (9.0) ( ):年伸び率 19 次のテーブルは、医療費給付の傾向はコストがかかることを示します。薬屋のための経費が 1609%に急騰して 3200 億ウォンから 5 兆 4760 億ウォンになっている一方、全コストは 2003 年に 1999 年に 11 兆 5220 億ウォンから 80%20 兆 7420 億ウォンに増加されました。この傾斜は、1999 年からの市場価格に基づいた高いコストの薬を主として使用する ことによります。また、これは 2002 年から安定しています。 施設ごとの医療費用 単位 100 万ウォン,( 合 計 総合病院 病 院 診療所 歯 科 漢 方 保健所 薬 局 ) は年増加率% 1999 2000 2001 2002 2003 11,521,631 12,912,221 17,843,321 18,831,672 20,741,997 (12.1) (38.2) (5.5) (10.1) 4,699,416 4,569,175 4,907,199 5,940.539 (-3.9) (-2.8) (7.4) (21.1) 976,159 1,070,108 1,172,069 1,407,615 (4.1) (9.6) (9.5) (20.1) 4,589,396 5,866,077 5,914,414 5,960,076 (10.5) (27.8) (0.8) (0.8) 776,198 933,790 918,768 949,490 (16.5) (20.3) (-1.6) (3.3) 529,606 678,008 782,929 889,047 (39.5) 28.0) (15.5) 7(13.6) 150,861 119,268 111,323 119,683 (-12.1) (-20.9) (-6.7) (7.5) 1190,585 4606,901 5024,970 5475,547 (271.5) (286.9) (9.1) (9.0) 4,892,398 937,679 4,153,553 666,385 379,526 171,617 320,473 医療費の支払いは NHIC が行ないます。健康保険審査評価院(HIRA)は、医療機関から提出された請求を調査して評 価し、NHIC に結果を報告します。 4-8-2 REV IEW AND EVALUATION OF MEDICAL SERVICES Medical providers can summit payment claims in three different ways;'paper claims', 'diskette claims' and 'Electronic Data Interchange(EDI) claims'.They are encouraged to adopt EDI and diskette claims in order to reduce costs and time for reviewing processing.The number of provider adopting E-claims has continuously increased and reached nearly 95 percent of total institutions currently. 3 つの異なる方法でメディカル供給者缶頂上支払いクレーム; 「紙クレームの、「diskette クレームの「そして電子デー タ交換(EDI)クレームの。それらは、EDI を採用するように促進されます。また、diskette は処理を調査するためのコスト および時間を縮小するために要求します。 E-クレームを採用する供給者の数は、機関の合計のほぼ 95 パーセントを 連続的に現在増加させて到着しました 20 EDI 請求を採用している医療機関 分類 計 施設数 歯科 漢方 漢方 診療所 病院 診療所 103 11,558 153 8,704 16288 92 8,715 45 (69.1) (89.3) (75.4) (29.4) 総合病院 病院 診療所 歯科病院 67,993 283 870 23,573 EDI 54,020 200 465 採用 (79.5) (70.7) (53.5) 助産所 保健所 薬局 70 3,407 19,272 7,815 2,560 17,840 (89.8) (75.1) (92.6) 施設 Review of Claim By the National Health Insurance Act, the HIRA undertakes responsibilities to review claims of medical providers supplying health services to patients.Providers submit claims for review to the HIRA.The submission of claims to the HIRA is regarded as submission to the insurer, the NHIC, by the Act. 国民健康保険行為によって、HIRA は、患者にヘルス・サービスを供給する医学の供給者のクレームを調査するため に責任を試みます。供給者は、HIRA に再考のためのクレームを提出します。HIRA へのクレームのサブミッションは行 為によって、保険業者(NHIC)へのサブミッションと見なされます。 HIRA reviews health care services to determine whether services are furnished at the optimum level and in cost effective methods provided on the basis of the review standards, regulations or guidelines of the Act. HIRA は、最適のレベルに、および行為の調査基準、規則あるいはガイドラインに基づいて有効な方法が提供したコ ストの中でサービスが供給されるかどうか決めるヘルスケア・サービスを調査します。 Health Care Review and Evaluation Committee has been established within the HIRA to secure fair and efficient review activities.The Committee consists of 30 full-time members and 600 part-time members who are doctors, dentists, herb-doctors and pharmacists.It has a Central Review Committee, a Central Evaluation Committee, and seven Local Review and Evaluation Committees.In order to support reviews requiring highly professional expertise, the Central Review Committee has 30 Subcommittees by medical specialty and the Local Review and Evaluation Committee has 10 Subcommittees by medical specialty. 公平で効率的な検閲機関を安全にするために、ヘルスケア調査および評価委員会は HIRA の内に確立されました。 委員会は、30 人の常勤のメンバー、および医者、歯科医、薬草医者および薬剤師である、600 人のパート・タイムのメ ンバーから成ります。それは中央の調査委員会、中央の評価委員会、および 7 つのローカルの調査および評価委員 会を持っています。高度に専門的知識を要求する調査を支援するために、中央の調査委員会は医学の専門およびロ ーカルの調査によって 30 の小委員会を持っています。また、評価委員会は医学の専門によって 10 の小委員会を持っ ています。 Medical institutions should report all relevant information such as their manpower, equipment, and other facilities to the HIRA, which compiles the reported information in data base and uses in the review process.Review standards determined by the committee are open to the public on a monthly basis for medical institutions to make their claims more accurate. 医療機関は、それらの人材、設備および HIRA への他の設備のような関連情報をすべて報告するべきです。それは、 データ・ベース中の報告された情報をコンパイルし、調査プロセスの中で使用します。委員会によって決定された調査 基準は、それらのクレームをより正確にする医療機関のために、月単位で一般に開放されています。 21 The review results should be sent to the NHIC and concerned health care institutions, respectively.Based on the results, the NHIC reimburses to providers. 調査結果は、NHIC および関係のあるヘルスケア機関にそれぞれ送られるべきです。結果に基づいて、NHIC は償い ます、供給者に。 The review procedures have been continuously improved and decentralized.The headquarter of HIRA handle the claims from tertiary care hospitals, general hospitals, dental teaching hospitals and herb-doctor hospitals, which its 7 branch agencies review and evaluate the claims from clinics and hospitals. 調査手続きは連続的に改善され地方分散されました。 HIRA の headquarter、専門治療病院、総合病院、歯の教える 病院および薬草医者病院(その 7 つの枝機関はそれらを調査する)からのクレームを扱い、クリニックと病院からのクレ ームを評価する。 Evaluation of Appropriateenness of Health Care Services The HIRA is also in charge of evaluating the appropriateness of health care services provided to patients.This activity is to guarantee the quality, effectiveness, and appropriateness of health care services.It induces providers to enhance performance and responsibility of supplying medical services, consequently contributing to protecting and improving patients' health and satisfaction, and responding to the specific health needs of individuals. HIRA は患者に提供されるヘルスケア・サービスの適切な性質を評価することを担当しています。この活動は、ヘルス ケア・サービスの質、有効性および適切な性質を保証することです。それは、医療サービスを供給し、患者の健康およ び充足の保護および増進に従って寄与し、個人の特定のヘルス・ニードに応答する実行と責任を増強するように供給 者に勧めます。 The evaluation of appropriateness of medical benefits is designed to secure the appropriateness of overall medical care services by involving physicians, medical care institutions, and other interested parties in collaborative efforts instead of solely focusing on individual clinical errors and rare instances of substandard cares. 医療給付の適切な性質の評価は、単独で、標準以下の注意の個々の臨床のエラーおよびまれな実例に注目する代 わりに共同努力に内科医、医療機関および他の利害関係者を巻き込むことにより、全面的な医療サービスの適切な 性質を安全にすることを目指しています。 4-9 OPERATION STRUCTURE OF HEALTH INSURANCE PROGRAM 4-9-1 MOHW The Ministry of Health & Welfare(MOHW) provides general supervision about the operation of the NHI program through the formulation and implementation of policies.The MOHW carries out the supervisory intervention mainly by enacting the regulations of the health insurance system, supervising the implementation of these regulations and approving the annual activities and budgets of the NHIC and the HIRA. 厚生省&ウェルフェア(MOHW)は、政策の公式化およびインプリメンテーションを通じて NHI プログラムのオペレーショ ンに関する総監督を提供します。MOHW は、主として健康保険制度の規則を実行し、これらの規則のインプリメンテー ションの監督 NHIC と HIRA の毎年の活動および予算の承認により、監視介在を行ないます。 Under the Ministry are two standing committees which are established by law to make final decisions or recommendations on important matters concerning the health insurance program. 省の下では、健康保険プログラムに関する重要事項上の最終決定あるいは推薦をするために法則によって設立さ れる 2 つの常任委員会がいます。 22 One is the Health Insurance Policy Review and Coordination Committee which deals with health care benefits standards, health care benefits costs, and other matters closely related to health insurance.The committee consists of 20 members, eight of them representing the insurer, beneficiaries and employers, six representing medical and pharmaceutical sectors, and six representing public interests, respectively.The members, whose tenure is two years, are appointed or assigned by the Minister of Health & Welfare. 1 つは、医療費給付基準、医療費給付コストおよび他の問題を備えた取り引きが、健康保険に、密接に関連づけた 健康保険政策批評および調整委員会です。委員会は、20 人のメンバー、それらが保険業者、受益者および雇用者を 表わすことのうちの 8、6 つの表わす医学・製薬のセクターおよび 6 つの表わす公衆の利益からそれぞれ成ります。メ ンバー(その保有は 2 年である)は厚生大臣&ウェルフェアによって指定されるか割り当てられます。 The other committee is the Dispute Mediation Committee which deals with appeals filed by insured persons or medical care institutions when they are not satisfied with the decisions made by the NHIC or the HIRA.The committee consists of fifteen members with considerable knowledge and experience in the fields of law, health and medicine.The committee members are appointed or assigned by the Minister of Health & Welfare. 別の委員会は、NHIC または HIRA によって下された決定に満足でないときに、保険に入った人か医療機関によって ファイルされた訴えに対処する論争仲裁委員会です。委員会は、法則、健康および医学の分野での相当な知識およ び経験を備えた 15 人のメンバーから成ります。委員は厚生大臣&ウェルフェアによって指定されるか割り当てられま す。 If the insured, dependents or medical care institutions are not satisfied with the decision made by the NHIC or the HIRA, they can submit appeals for formal objection first to the Formal Objection Committee.After receiving the decision from the Committee of the NHIC or the HIRA, any person who is not satisfied with the decision can file a further appeal to the Dispute Mediation Committee. 保険付きか扶養家族あるいは医療機関ものが、NHIC または HIRA によって下された決定に満足でない場合、それら は形式上の反対委員会に形式上の反対を求める訴えを最初に提出することができます。NHIC または HIRA の委員会 から決定を受け取った後に、決定に満足でないどんな人も、論争仲裁委員会への一層の訴えを提出することができま す。 According to the Article 2 of the Special Act for Financial Stabilization, the Health Insurance Policy Review Committee was established under the MOHW.This temporary Committee consists of 25 members including the vice minister of MOHW, eight of them representing the insured, eight representing provider sectors, eight representing public interests groups.And it handles important matters related to the standards of health insurance benefits, health care benefit costs(reimbursements), monthly contributions, and other important matters assigned by the Presidential Ordinance. 金融安定化のためのスペシャル法の記事 2 によれば、健康保険政策批評委員会は MOHW の下で設立されました。 この一時的委員会は、MOHW、それらが保険付きのものを表わす 8、8 つの表わす供給者セクター、8 つの表わす公の 利益グループの副大臣を含む 25 人のメンバーから成ります。また、それは、健康保険給付、医療費給付コスト(払い戻 し)、毎月の寄付、およびプレジデンシャル法令によって割り当てられた他の重要事項の標準と関係する重要事項を扱 います。 4-9-2 NHIC The National Health Insurance Corporation is a public insurer for the public health insurance program in Korea.The 23 NHIC is responsible for administering the national health insurance, including management of the qualifications of the insured and their dependents, the collection of contributions, the setting of medical fees schedule through negotiation with providers, the provision of health insurance benefits through payments for medical services rendered to the insured, and the operation of other related projects such as health promotion and prevention activities. 国民健康保険公団は韓国で公衆衛生保険プログラムのための公の保険業者です。 NHIC は国民健康保険の処理 原因です、資格の管理を含んでいること、保険がつけられた、またそれらの扶養家族、寄付の収集、供給者との交渉 による医療費スケジュールのセッティング、保険がつけられたことに与えられた医療サービスに対する報酬による健康 保険利点の準備、および健康増進と予防の活動のような他の関連するプロジェクトのオペレーション。 4-9-3 HIRA To improve people's health and strengthen social security through performing fair and efficient review and evaluation of health care services, Health Insurance Review Agency(HIRA) is established in accordance with the Article 55 of the National Health Insurance Act as a statutory public organization. 人々の健康を増進し、かつヘルスケア・サービスの公平で効率的な調査および評価を行なうことによって社会保障を 強くするために、健康保険審査評価院(HIRA)は、法令による公共団体として、国民健康保険行為の記事 55 に従って 設立されます。 Mission The HIRA, succeeding to the medical claims review section of National Federation of Medical Insurance, was established to conduct claims review and health care assessment as an independent agency.The HIRA is responsible for reviewing claims and evaluating the clinical appropriateness of health care services provided to patients. HIRA、医学のものに続くことは、医療保険の国立連合の調査セクションを要求します、クレームを導くために確立され た、調査する、また独立機関としてのヘルスケア評価。HIRA は、クレームの調査および患者に提供されるヘルスケア・ サービスの臨床の適切な性質の評価原因です。 健康保険審査評価院は、ヘルスケア・サービスの調査および評価に加え、さらにヘルスケアの標準および料金スケ ジュールを確立し改訂するために支援し、医療機関に関する情報を管理し、ヘルスケア・サービスのための品質改良 イニシアチブをインプリメントし、様々な研究を行なうなど、多くの活動を行ないます。 健康保険審査評価院は、理事長と製薬協会(5)、NHIC(3)、HIRA(3)、労働組合(1)、雇用者協会(1)、農民漁師協会(1)、 消費者協会(1)および政府(1)からの 16 人の代表によって理事会を構成します。 理事長は保健福祉部長官によって任 命されます。 5 MAJOR REFORM 5-1 INTEGRATION REFORM 5-1-1 GOAL AND PROCEDURE The Korean government implemented two major reforms in July 2000, which could have big impacts on the overall Korean health care system as well as the National Health Insurance Program.The first one was, so called, the Integration Reform in which existing multiple insurance societies were integrated into a single insurer.And the second one was the Separation Reform in which the functions of prescribing and dispensing drugs between doctors and pharmacists were separated and specialized. 24 韓国の政府は 2 をインプリメントしました、主、2000 年 7 月に改良する、それは、国民健康保険プログラムと同様に全 面的な韓国のヘルスケアシステムに大きな影響を及ぼすことができました。第 1 のものはそうでした、したがって、呼ば 25 れた、既存の多数の保険社会が一人の保険業者へ統合された統合改革。また、第 2 のものは、医者と薬剤師の間の 薬を処方するおよび分配する機能が分離され特定化された分離改革でした。 Goal and Procedure ゴールと手続き There are two main reasons why the government decided to merge all the insurance societies into a single insurer. 一人の保険業者へ保険社会をすべて合併することを政府が決定した、2 つの主な理由があります。 The first reason is to increase equity in health financing.Although the insurance benefits each insurance society offered were all the same, individual insurance society had widely different methods in assessing contributions of the insured.So, individuals with similar income paid different contributions for the same benefits across different insurers. 第 1 の理由は健康調達資金で公正を増加させることです。各保険社会が提示した保険給付はすべて同じでしたが、 個人保険社会は保険付きのものの寄付を評価する際に広く異なる方法を持っていました。したがって、同様の収入を 持った個人は異なる保険業者を横切って同じ利点に異なる寄付を払いました。 The second reason is to improve efficiency of the NHI administrative system.Actually the policy of gradual establishment of many insurance societies enabled the government to achieve universal coverage relatively in a short period of time, but it gave rise to the inefficient financing and administrative structure of the overall NHI system. 第 2 の理由は NHI 行政機関の効率を改善することです。現実に、政府は、時間の短期の中で、多くの保険社会の 徐々の確立の政策によって比較的普遍的な報道を達成することができました。しかし、それは、非能率的な調達資金 および全面的な NHI システムの運営機構を生じさせました。 And many insurance societies were not big enough to guarantee an efficient pooling of revenues, many small societies, therefore, could not sufficiently disperse the risk across a large number of enrollees .Because the multiple insurers system could not take advantage of economies of scale in management, administrative costs tended to be high. Also, the NHI could not act as a single purchaser and prudent buyer of health care services before the reform. また、多くの保険社会が収入の効率的に共同出資することを保証するほどは大きくありませんでした、多くの小さな 社会が、十分にしたがって、多くの enrollees を横切って危険を分散させることができませんでした。複合の保険業者シ ステムが管理で規模の経済性を利用することができなかったので、管理上のコストは高い傾向がありました。さらに、 26 NHI は、改革の前にヘルスケア・サービスの一人の購入者および思慮深い買い手の役割をすることができませんでし た。 The Figure below explains the organizational changes according to the phased amendments of the relevant laws.With the first integration completed in October 1998, the National Medical Insurance Corporation (NMIC) was established, integrating 227 regional insurance societies covering all the self-employed insured with KMIC covering government employees and private school employees.And then subsequently, through the second integration initiative which integrated NMIC with 139 employee insurance societies covering employees of companies in the private sector, the National Health Insurance Corporation (NHIC) was established on July 1, 2000. 下記の図は、適切な法則の段階的な修正によって組織変更について説明します。1998 年 10 月に完成した第 1 の統 合で、国立医療保険株式会社(NMIC)は確立している統合する 227 の地方保険社会でした、カバー、すべての、自営業、 政府従業員および私立学校従業員をカバーする KMIC で保険がつけられました。そして民間部門の会社の従業員をカ バーする、139 の従業員保険社会に NMIC を統合した第 2 の統合イニシアチブによって、そのとき続いて、国民健康保 険株式会社(NHIC)は 2000 年 7 月 1 日に設立されました。 But even at this stage, the insurance funds of the self-employed were managed separately from that of the employed.The employed and self-employed accounts were finally combined on 1 July 2003, which meant the NHI had completed the integration reforms.Now, the NHIC is the only insurer of the national health insurance program covering the total population in a uniform way both administratively and financially. しかし、この段階でさえ、自営業のものの保険資金は、使用されたもののそれから別々に管理されました。使用され 自営業のアカウントは 2003 年 7 月 1 日に最後に組み合わせられました。それは、NHI が統合改革を終えたことを意味 しました。さて、NHIC は、一定の方法で人口の合計を管理上財政的にの両方カバーする国民健康保険プログラムの ただ一人の保険業者です。 5-1-2 OUTCOME OF THE REFORM The Korean government implemented two major reforms in July 2000, which could have big impacts on the overall Korean health care system as well as the National Health Insurance Program.The first one was, so called, the Integration Reform in which existing multiple insurance societies were integrated into a single insurer.And the second one was the Separation Reform in which the functions of prescribing and dispensing drugs between doctors and pharmacists were separated and specialized. 韓国の政府は 2 をインプリメントしました、主、2000 年 7 月に改良する、それは、国民健康保険プログラムと同様に全 面的な韓国のヘルスケアシステムに大きな影響を及ぼすことができました。第 1 のものはそうでした、したがって、呼ば れた、既存の多数の保険社会が一人の保険業者へ統合された統合改革。また、第 2 のものは、医者と薬剤師の間の 薬を処方するおよび分配する機能が分離され特定化された分離改革でした。 財政の改革 The equity of contributions payment has improved in both employees and self-employed realms.A uniform standard for assessing contributions is now applied nationwide.The Integration Reform, moreover, has stimulated redistribution of wealth because the contributions of the rich rose after the reform, while poor individuals mostly saw a fall. 寄付支払いの公正は従業員および自営業の領域の両方の中で改善しました。寄付の評価のための一定の基準は 今全国的に適用されます。統合改革は、さらに、富の再配送を刺激しました、ので、改革の後の豊富なバラの寄付、貧 27 しい個人がほとんど落下を見た一方。 Efficency in Administration Increased economies of scale in management seem to have brought out lower expenditures in administration costs.The organizational structure, including its geographical configuration, has been rationalized.Early evidence indicates that administrative costs have dropped from 8.85 of total NHI expenditures in 1999 to 7.3% in 2000, 4.5% in 2001 and 4.0% in 2002.235 insurance branches and six regional head offices replaced 389 insurance societies by July 2000, and manpower was also reduced by 5,199 persons(-33.2%) by 2002. 管理での増加した規模の経済性は、管理コスト中の外により低い消費をもたらしたように見えます。その地理的な配 置を含む organizational な構造が合理化されました。初期の証拠は、1999 年の NHI 消費の合計のうちの 8.85 から 7.3% まで 2002 年に 2000 年、2001 年の 4.5%および 4.0%に管理上のコストが落ちたことを示します。 235 本の保険枝および 6 社の地域本部会社が 2000 年 7 月までに 389 の保険社会に取って代わりました。また、人材も 2002 年までに 5,199 人(-33.2%)縮小されました。 5-2 SEPARATION REFORM 5-2-1 GOAL AND PROCEDURE One of the goals the separation reform pursues is to reduce the over-use of drugs.The reform aimed at advancing the rationality of prescription and reducing consumption of drugs.Doctors had incentives to dispense high-margin drugs but not sufficient incentives to dispense the most clinically appropriate ones.The reform intended to remove providers' margin on drugs and thus their economic incentives to encourage the over-use of pharmaceuticals.It also intended to remove commercial incentives, which could influence what types of drug to prescribe.There was especially a concern about the rate of injections and the use of antibiotics.Before the Reform, there was a report that physician consultations included an injection in 57% of cases, and antibiotics accounted for 59% of drugs dispensed, too high a proportion to be justified on clinical ground. 分離改革が追求するゴールのうちの 1 つは薬の過剰使用を縮小することです。その改革は規定の合理性を進めて 薬の消費を縮小することを目指しました。医者には、最も臨床的に適切なものを分配する十分な誘因ではなく高いマ ージンの薬を分配する誘因がありました。その改革は、供給者の薬の上のマージンおよびしたがって調合薬の過剰使 用を促進するそれらの経済的誘因を削除するつもりでした。さらに、それは商用誘因(それらは影響を及ぼすかもしれ ない)を削除するつもりでした、どんなタイプ、処方するべき薬の。特に注入の割合および抗生物質の使用に対する懸 念がありました。改革の前に、内科医コンサルテーションが事例の 57%に注入を含んでいたという報告書がありました。 また、抗生物質は、分配された薬の 59%(あまりにも高い割合)で臨床の地上で正当化することができないことを説明し ました。 The other goal is to improve patient rights for information.Doctors did not explain about the type, quantity and treatment period of medication to the patient.This lack of disclosure increased the asymmetry of information between doctors and patients.The reform intended to increase patients' awareness and ability to check upon doctors' behaviors by opening the prescription to patients and pharmacists. 別のゴールは情報のための忍耐強い権利を改善することです。医者は患者に、薬物治療のタイプ、量および治療期 間に関して説明しませんでした。開示のこの不足は、医者と患者の間の情報の不調和を増加させました。その改革は 患者の意識および、患者と薬剤師に処方を公開することにより医者の振る舞いでチェックする能力を高めるつもりでし た。 28 5-2-2 OUTCOME OF THE REFORM Some evidence shows that the use of antibiotics and injections has been decreasing.This decrease must be a positive results because antibiotics were highly overused before the reform. ある証拠は、抗生物質と注入の使用が減少していることを示します。この減少はそうであるに違いありません、1 つの、 肯定的な結果、ので、抗生物質、改革の前に高度に過剰使用された。 People who used to receive medical advice, treatment and pills directly from a doctor, now have to make two visits, first to the doctor and then to the pharmacist.Similarly, people who used to buy drugs, including antibiotics, directly over the counter, are now obliged to see a physician before getting drugs.Nonetheless, the reform will increase the appropriateness and the quality of prescribing.It assigns the central functions of diagnosis and prescription to doctors.On the other hand, it expands patient right to know about prescribed drugs by opening the prescription papers to the patients.It encourages doctors to prescribe drugs more attentively.It gives the pharmacist a function of scrutiny over the optimality of the quantity and type of drugs prescribed by the doctors.Prescriptions can be checked both by the doctor and pharmacist, a guarantee for improved drug services for the patients, eventually resulting in quality care through the specialization among the professionals. かつては医者から医学の助言、治療および錠剤を直接受けた人々は、今、医者に、その後薬剤師に最初に 2 つの訪 問を行わなければなりません。同様に、かつては店頭で、抗生物質を含む薬を直接買った人々は今、薬を得る前に内 科医に診てもらわなければなりません。それにもかかわらず、その改革は適切な性質および規定する質を増加させる でしょう。それは、医者に分析と処方の中央の機能を譲渡します。他方では、それは、患者に規定紙を公開することに より処方された薬のことを知る忍耐強い権利を拡張します。それは、薬をより注意して処方するように医者を激励しま す。それは、薬剤師に医者によって処方された薬の量およびタイプの optimality の上の調査の機能を与えます。医者 および薬剤師(患者のための改善された薬サービスの保証)の両方は処方を専門家の間の特殊化によって質注意に 帰着して、結局チェックすることができます。 5-3 CHARENGE AND TASK 5-3-1 STRENGTHENING HEALTHCARE PROCEDURE Stronger protection against catastrophic illnesses could improve affordability of care and income security for low-income households and the chronically ill.Health insurance is a risk transfer mechanism in which the risk of a large unexpected loss is transferred from the individual, by paying a small certain contributions, to the insurer.This mechanism is certainly very effective for protecting individuals against high-cost risks. 破滅的な病気からのより強い保護は、注意および低収入の世帯のための収入セキュリティのアフォーダビリティを改 善するかもしれません、そしてその、慢性的に悪く。健康保険は、大規模な予期しないロスの危険が個人から転送され る危険トランスファー・メカニズムです、によって、払う、1 つの、保険業者への小さなある寄付。このメカニズムは、高い コストの危険から個人を保護することには確かに非常に有効です。 Due to relatively weak service coverage of NHI, the population, however, has been exposed to high level of risks. NHI の比較的弱いサービス報道により、しかしながら、人口は危険のハイ・レベルに露出されました。 So since the Integration Reform, the government policy focuses have been placed on expanding benefit coverage to secure the adequate protection of health insurance, while many efforts to stabilize insurance finance have also been taken through various drastic measures.For example, high-cost services such as CT and MRI have come under health insurance benefit umbrella.And for the same purpose many new measures and cost relief actions have been taken ;applying inpatient co-payment rate of 20% to outpatient cancer treatments, co-payment exemption for virginal 29 delivery(natural childbirth), reducing outpatient co-payment rates for severe psychiatric patients, covering motorized wheelchairs, scooter as insured items for the disabled, benefit day extension for osteoporosis drugs, etc. したがって、統合改革以来、政府政策焦点は、保険金融を安定させる多くの努力も様々な徹底的な手段によって得 られている一方、健康保険の適切な保護を安全にするために利益報道を拡張することに置かれました。例えば、CT と MRI のような高いコストのサービスは健康保険利益傘の下に入りました。また、同じ目的のために、多くの新しい手段 およびコスト軽減処置が取られました;外来患者癌治療への 20%の入院患者共同支払い料金の適用、モーターつき車 椅子をカバーする厳しい精神病患者のための外来患者共同支払い料金を縮小する処女の配達(自然な出産)のため の共同支払い免除、不具のもののための保険付きのアイテムとしてのスクーター、骨粗鬆症薬などのための利益日拡 張 And in order to further protect the insured against catastrophic risks, the NHI program has a mechanism, which covers 50% of the co-payment for bills exceeding 1.2 million won during the period of consecutive 30 days.Yet, the mechanism alleviate the burden of payment for patients with high bills only marginally.Taking the case of in-patient services, it is likely that even 50% of the average out-of-pocket expenditure on bills above 1.2 million won is too high a financial burden for low-income individuals. また、さらに破滅的な危険から保険付きのものを保護するために、NHI プログラムはメカニズムを持っています。それ は、連続する 30 日の期間に 120 万ウォンを超過する紙幣のための定額自己負担の 50%をカバーします。まだ、メカニ ズム、高い紙幣を持った患者にとって支払いの負担を単にわずかに緩和します。イン忍耐強いサービスの場合をとっ て、120 万ウォン以上の紙幣上の平均ポケット外消費の 50%さえ、低収入の個人にとって高すぎる財政負担でしょう。 So the government and NHIC have introduced the Co-payment Ceiling system in 2005.The Ceiling system will serve as a safety net against patients' excessive co-payments under which the patient is exempted from paying further co-payments if his or her co-payments exceed a certain threshold, say, 3 million won within 6 months. したがって、政府と NHIC は 2005 年に定額自己負担シーリング方式を導入しました。シーリング方式は、6 か月以内 に、患者が彼または彼女の定額自己負担があるしきい値を越える場合に例えばさらに定額自己負担を払うのを免除 される、患者の過度の定額自己負担に対する安全ネットとして 300 万ウォン役立つでしょう。 5-3-2 Securing Financial Stability of NHI System The government has been taking several drastic measures to improve the financial status which deteriorated seriously after the Separation Reform. 政府は、分離改革の後にひどく下がった財政状態を改善するためにいくつかの徹底的な手段を取っています。 Facing unprecedented financial crisis of NHI, the government approved two sets of measures to deal with the crisis.A plan of action to reduce deficits in the system was issued in May 2001, and a Special Act for Stabilizing the NHI fund was enacted in Jan. 2002 with validity until the end of 2006. NHI の先例がない金融危機に面して、政府は、危機に対処する 2 セットの法案を承認しました。システムでの赤字を 縮小するアクションの計画は 2001 年 5 月に出されました。また、NHI 資金を安定させるためのスペシャル法は 2006 年 の終わりまで有効性で 2002 年 1 月に実行されました。 The government plan of action to tackle the financial crisis aims at achieving fiscal stability by 2006.The plan includes a variety of measures such as an increase in the government subsidy, a rise in co-payment, more through detection mechanisms for providers frauds, improvements in income assessment for the self-employed, and a 9% annual raise of the current contribution rate until 2006. 30 金融危機に取り組むアクションの政府計画は 2006 年までに会計の安定を達成することを目指します。計画は、2006 年まで、供給者不正行為、自営業のもののための収入評価における改良および現在の貢献割合の 9%の毎年の賃上 げのための検知メカニズムによって国庫補助(定額自己負担の上昇)の増加のような様々な手段をもっと含んでいま す。 And by the Special Act, more government committment to financial responsibilities was guaranteed ;40% of the administrative and benefits costs of the self-employed pool and 10% of the funds raised through the Health Promotion Fund(revised to 35% and 15%, respectively, effective from 2005). また、スペシャル法によって、金融責任へのより多くの政府 committment が保証されました;40%の、管理上、また自 営業のプールの利点コスト、および健康増進資金(2005 年から有効で、35%および 15%までそれぞれ改訂された)によっ て調達された資金の 10%。 Due to the government measures taken in accordance with the plan and reduced demands on health care services apparently caused by recent years' economic recession, the NHI financial status has been rapidly and dramatically improved covering up completely the previous huge deficits by the end of 2004. 計画に従って取られた政府案により、および見たところでは、最近の年の景気後退によって引き起こされたヘルスケ ア・サービスに関する縮小された要求、NHI 財政状態は、2004 年の終わりまでに完全に前の巨大な損失を補填して、 急速に劇的に改善されました。 Even though the NHI is overcoming its financial crisis a bit successfully, the financial status can be unstable at any time because the revenue side actions are not sufficient to guarantee the longer-term stability of NHI fund. たとえ NHI がその金融危機を少し成功裡に克服していても、収入副作用が NHI 資金のより長期的な安定性を保証す るのには十分でないので、財政状態はいつでも不安定になりえます。 So besides the revenue side measures, expenditure control is also needed.But it has been pointed out that reliance on containing cost via tight controlling of fee schedule and co-payments are likely to be inadequate.While certain increases in co-payments can be considered as possible measures to stabilize the NHI finances, many experts agree that these cannot be further increased without weakening equity of financing and of access, and giving patients awareness of cost has not been sufficient to control costs. したがって、収入側手段に加えて、消費コントロールも必要です。しかし、料金スケジュールの厳しくコントロールする ことによってコストを含んでいることに対する信頼および定額自己負担が不適当だろうことは指摘されました。共同支 払いのある増加を NHI 財源を安定させる可能な手段と見なすことができますが、多くのエキスパートが、これらがさら にありえないことに合意します、調達資金の、およびアクセスの公正を弱めず、かつ、コストの意識がそうでなかった患 者を与えて、増加した、コストを調整するのに十分。 Both theoretically and empirically, the institutional features of the supply side in the Korean health care system, private profit-oriented providers and fee-for-service payments, have encouraged providers to increase volumes, supply more intensive and specialist cares, and duplicate technology. 両方、理論上経験的に、韓国のヘルスケアシステム、私的利益指向の供給者およびサービスに対する料金の支払 い中の供給側の制度上の特徴、ボリュームを増加させるように供給者を激励した、集中的な専門家ケアおよび複製の 技術をもっと供給します。 31 In order to maintain sustainable expenditure growth, while not damaging patents' access to health care, we need to consider adopting additional cost containment measures including a new mechanism of providers' payments. 持続可能な消費成長を維持するために、特許のヘルスケアへのアクセスを破損していない間、私たちは供給者の支 払いの新しいメカニズムを含む追加費用封じ込め手段を採用することを考慮する必要があります。 5-3-3 PREPARATION FOR INTRODUCING LONG-TERM CARE INSURANCE SCHEME The demand for long-term care is expected to increase as a result of a rapidly ageing population, growing female participation into labor markets, and a decreasing proportion of elderly living with their children.As the informal family network, which used to provide strong social and health care support to the elderly, is weakening, there is a growing need for public forms of care. It is indisputable that the hospitalization of the elderly in need of nursery could excercise heavy financial burden on the NHI expenditures. 長期的な介護の需要が増加すると予想されます、の結果、1 つの、急速に、彼らの子供たちと一緒に住んで、初老の ことに労働市場の中への女性の参加および減少する割合を育てる老齢人口。非公式の家族ネットワーク(それは高齢 者に強い社会とヘルスケア支援をするために使用される)が弱まっているとともに、ケアの公の形式の成長している必 要があります。はがの(育児室を必要とする高齢者の入院、できる)確実です、NHI 消費上の重い財政負担を excercise します。 Currently, no distinction exists between chronic beds and acute care beds in hospitals. It would create an undue burden on the already strained NHI system in terms of longer stays and higher cost of treatment in hospitals, compared to nursing care in specialized institutions such as residential homes or at home. But to avoid it, adequate and affordable care services need to be available. 現在、区別は病院に慢性のベッドおよび鋭い注意ベッドの間に存在しません。それは、住宅のような専門の機関の、 あるいはホームで介護と比較して、病院での治療のより長期滞在およびより高いコストの点から既に緊張した NHI シス テム上の不適当な負担を作成するでしょう。しかし、それを回避するために、適切で手頃な注意サービスは利用可能 である必要があります。 So, while expanding long-term care facilities for the elderly and chronically ill in the Korean health care system, we also need to introduce another financing mechanism, like long-term health insurance, for the population groups. そのように、長期ケア設備を拡張している間、のために、韓国のヘルスケアシステムにおいて初老で・慢性病、さらに、 私たちは人口グループのために、長期的な健康保険のように、別の融資メカニズムを導入する必要があります。 To cope with the situation, the government has been running a special task force to map out a comprehensive measure to expand the availability of long-term care services for the elderly, tentatively aiming at introducing the long-term care insurance program in 2007. 状況に対処するために、政府は、2007 年に長期注意保険プログラムを導入することを一時的に目指して、高齢者の ための長期的な注意サービスの有効性を拡張する包括的な手段の計画を立てるために特別対策委員会を運営して います。 完 国民健康保険公団のホームページより、2005-7-12 ダウンロード西山孝之 32
© Copyright 2026 Paperzz