Paper
zz
Explore Categories
Log in
Create new account
No category
Malabsorption syndromes Dr. Abonyi Margit
Download
Report
M l b ti ti l Malabsorption: etiology, pathogenesis and pathogenesis
Recent Study Reveals Growth Prospects of Lactose Intolerance Treatment Market During 2017 - 2025
Food Allergy and Intolerance Products Market
Celiac Disease Drugs Market
Hydrogen Breath Test Analyzer Market Global Trends, Market Share, Industry Size, Growth, Opportunities, and Market Forecast 2019 to 2029
TDS: Manganous DI Oxide (MnO2) – 78-80%
disaccharidase activities in small intestinal mucosa of alloxan
Early Diagnosis of Pancreatic Cancer
Lecture 2
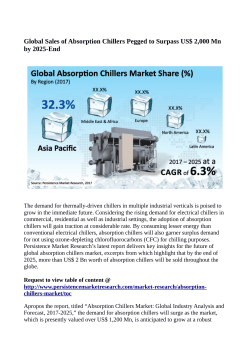
Absorption Chillers Market Expected to Reach US$ 2 Billion By 2025
© Copyright 2026 Paperzz
About Paperzz
DMCA / GDPR
Report