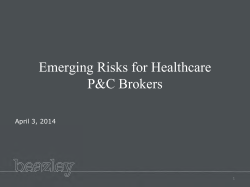
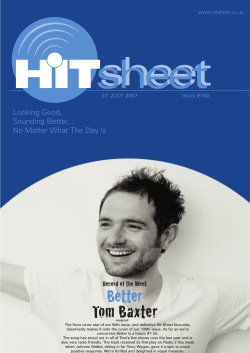
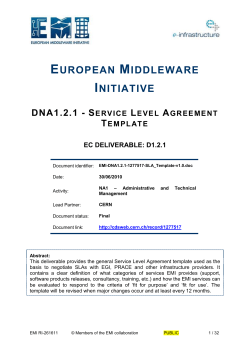
PORTFOLIO TABLE OF CONTENTS Sample: My Resume ............................................................................. 3 Sample: College Entrance Essay .............................................................. 4 Sample: Healthcare Informatics in the News Short Paper ............................... 7 Sample: Health Information Technology Short Paper .................................... 11 Sample: Website Review ...................................................................... 15 Sample: Annotated Bibliography ............................................................. 19 Sample: Relational Database System Design ............................................... 23 Sample: Personas ............................................................................... 55 Sample: Heuristic Evaluation ................................................................. 58 Sample: Term Paper - EMI in Wireless Networks in Hospitals ........................ 115 Sample: Final Paper - Significant Influential Factors Affecting Health Information Technology Diffusion and Infusion......................................................... 146 Sample: PowerPoint Presentation ......................................................... 166 Sample: Use Case ............................................................................. 172 Sample: UML Class Diagram and Domain Model ......................................... 180 Sample: Press Release ....................................................................... 184 Sample: Instructions.......................................................................... 187 Sample: Feasibility Study ................................................................... 190 Sample: Process Description ................................................................ 202 Sample: Documentation Plan for an SOP ................................................. 205 Sample: Standard Operating Procedure .................................................. 208 Sample: Documentation Plan for Tutorial ................................................ 221 Sample: Usability Test Plan and Results .................................................. 224 Sample: Tutorial .............................................................................. 229 Sample: Request for Proposal .............................................................. 248 Sample: Healthcare Informatics Evaluation Proposal .................................. 256 Sample: My Resume Lisa Romanoski 1040 Mason Street, Apt. 102, San Francisco, CA 94108 • 415-264-4401 • [email protected] HEALTH INFORMATICS PROFESSIONAL Health informatics graduate student with excellent ability to multitask and work collaboratively on mulitiple projects and communicate across disciplines in a fast-paced, deadline-oriented, environment, with attention to detail, schedules, budgets, and stakeholder satisfaction. EDUCATION MS, Drexel University, Health Informatics, 9/2011 – Present (Graduation Date: June 2013): Foundations of Information Systems Human-Computer Interaction  Concepts/applications of IS/IT  User-oriented approach to design/evaluation Introduction to Database Management  Database design, data manipulation and integrity maintenance, SQL queries IS Analysis & Design  Object-oriented analysis and design techniques based on UML Distributed Computing and Networking  Networking planning, design principles, network protocols, internetworking, and distributed computing topics Healthcare Informatics  Intro to IS applications in healthcare  Sociotechnical aspects  Planning and evaluation Coursework in Technical and Professional Writing, San Francisco State University, 2009 MS, University of Hawaii at Manoa, Ocean Resources Engineering, 2000 BSE, Purdue University, Interdisciplinary Engineering, 1999 EXPERIENCE Project Support/ Management  Conducted design development and contract document work sessions in conjunction with project managers, appropriate technical professionals, and other disciplines.  Prepared scopes of work for procurement of subcontracts.  Prepared cost estimates and project schedules.  Managed $750K to 5M projects, including review of contractor submittals and requests for information. Applied fast problem-solving techniques to address issues/avoid change orders.  Managed multiple contracts with clients and subconsultants simultaneously.  Prepared meeting minutes for team members and clients.  Identified and performed trouble-shooting of schedules and cost conflicts.  Consulted with and adhered to regulatory agencies and associated laws and guidelines. Technical Writing  Prepared: feasibility studies, proposals, technical specifications, memos.  Synthesis of technical information and interpretations.  Excellent ability to explain complicated projects in layman’s terms: writing or presentations. Certifications  Collaborative Institutional Training Initiative (CITI), Human Subjects Research Training, 8/12  HIPPA and Medical Research and HIPPA Security (Parts I and II), 9/12  Des Moines University, Medical Terminology, 9/12 WORK HISTORY Staff Engineer, Water Resources Engineering, Inc., San Francisco, CA, 9/2010 – 9/2011 Engineering Consulting Firm Contractor, Civil Engineer, Innovative Technical Solutions, Walnut Creek, CA, 7/2009 – 11/2009 Engineering / Environmental Consulting Firm Civil Engineer, Mactec Engineering and Consulting, Inc., Oakland, 2008 – 2009 National Engineering / Environmental Consulting Firm Civil Engineer, Project Manager, TranSystems Corporation, Oakland, 2006 – 2008 National Transportation Engineering Consulting Firm Water Resources Engineer, U.S. Army Corps of Engineers, San Francisco, 2002 – 2006 AFFILIATIONS Member, American Medical Informatics Association (AMIA) Member, Healthcare Information and Management Systems Society (HIMSS) Portfolio of writing samples and references available. 4 Sample: College Entrance Essay The following sample is my master’s program entrance essay. I’ve decided to showcase it here because it exemplifies my writing style and provides insight to why I’ve decided to change my career. Ten years of civil engineering experience in the San Francisco Bay Area is the background I bring to the Drexel University iSchool Master of Science in Health Informatics Program. While civil engineering is different from health informatics, both fields involve data compilation, analysis, and trend identification. I envision building upon this type of work in the graduate program and then in a new career in a research setting or perhaps assisting on a clinical trial. My relevant experience and enthusiasm for continual learning and personal achievement is outlined with a project example from my career, as detailed in the following paragraphs. The Berkeley Marina Rehabilitation Project is my favorite project that I have worked on during my career. I joined the project team mid-way through the design phase and brought myself up to speed on project status and needs. As a construction manager, I watched plans become reality, addressed unanticipated construction issues stemming from an oil spill, and focused team efforts on providing the best possible project. Similarly, as I transition into a new career, I see myself working in a challenging environment that allows me to apply investigative strategies and problem-solving in an effort to develop new solutions. The Berkeley project taught me some valuable lessons. The first thing I learned is that people like to see a tangible product for the money they spend. For example, it was not enough to say your construction permit is on the way. The City engineer wanted his permit despite a regulatory agency request for additional environmental testing because of the oil spill, a random occurrence placing a burden on the client in tough economic times. After negotiating with the agency, we agreed to a realistic and financially appropriate course of action. I succeeded in getting the permit with minimal delays to the project schedule. The second lesson I learned is that if something does not work, it is best to try something new in an effort to find a solution. During the project, the contractor was unable to drive a concrete pile in a specified location. Instead of risking damage to an expensive project component, I worked with our geotechnical engineer and the contractor to determine an alternative location. We also had to adjust how the rest of our project pieces fit with this new pile position. From this experience, I learned to be more flexible and adaptable to changing situations. While I did not know the answer to the problem, a combined team work effort resulted in a solution with minimal charges to my client. The third lesson I learned is that once the project ends, it is time to apply knowledge gained to new, exciting endeavors. While most companies have multiple projects on-going in various stages of development, sometimes they never receive funding, experience delays, or are canceled. This leads to instability, employee layoffs, and overwhelming competition among a lot of experienced engineers. After being laid off due to lack of work at three companies, I have decided to pursue a career change to health informatics, an area that I anticipate will be challenging, rewarding, and have a greater hiring and job retention capacity. I hope to build upon the skills and lessons learned from past experience and bring a different perspective to the program and health care field. 7 Sample: Healthcare Informatics in the News Short Paper This sample was prepared for Drexel INFO 648, Healthcare Informatics. Details for this course are as follows: Description The course presents an overview of all aspects of healthcare informatics, including medical, nursing and bioinformatics. It provides an introduction to the applications of information systems in a variety of healthcare environments, including education, research and clinical settings. It includes extensive reading and critical discussion of relevant professional research literature. Course Objectives        Describe how standards and structures affect the expression, collection, manipulation and representation of data and information in biomedicine and public health Describe the role of decision support in healthcare Articulate and give examples of sociotechnical issues in healthcare informatics Demonstrate the ability to evaluate informatics tools, systems and applications used in healthcare Discuss the effect of privacy and security regulations on the development and implementation of informatics applications in healthcare Describe recent developments in bioinformatics and be able to conduct a basic search in a bioinformatics database Critically discuss current research literature in healthcare informatics EHR INFLUENCE ON MEDICAL MALPRACTICE LIABILITY 1 Do Electronic Health Records Increase or Decrease Medical Malpractice Liability? According to InformationWeek’s Paul Cerrato, electronic health records (EHR) have advantages and disadvantages for clinicians, including fast access to patient health data but also increased malpractice risk (2011). This discussion summarizes a clinician’s malpractice risk from EHRs and briefly analyzes whether that risk is elevated or lowered from their use. One of the most frequently cited studies for the case that EHRs may lower malpractice risks is a 2005 Harvard Medical School study of 1,140 Massachusetts clinicians, of which 6.1% with EHRs and 10.8% without EHRs had paid malpractice settlements in the preceding 10 years, according to Managed Care Weekly Digest (2008). In terms of decreasing malpractice risk, Dembrow (2009) and Terry (2007) report that EHRs provide:  Easier, instantaneous, and remote access to records, which may reduce errors  More comprehensive records  Automatic alerts for things like allergies and drug interactions  Improved follow-up capability  Better adherence to clinical guidelines provided by decision-support systems In comparison, Carter (2011), Goldberg (2011), and Terry (2007) report that malpractice risk can be increased because EHRs:  Can go missing due to system crashes, resulting in limited or no access to data  Divert attention away from a patient’s signs and symptoms  If not consulted, can fail to alert clinicians to all steps required by decision-support systems  May not include all aspects of a patient’s medical history  May not be used by clinicians These lists show that EHRs can pose both a benefit and threat to healthcare practices. One of the reasons for this depends on the stage in which an EHR is in, which can affect its ability to be useful. According to Mangalmurti et al. (2010), medical malpractice liability exists throughout the lifetime of an EHR, from initial setup, to regular system use, and to widespread use as a mature system. For instance, during initial EHR setup, a patient’s health record may still be a combination of hard copy records and new electronic records. This dual paper and electronic recording system can cause problems such as failing to alert a physician to the need to notify a patient, an issue that is more commonplace with dual systems as compared to those that use EHR INFLUENCE ON MEDICAL MALPRACTICE LIABILITY 2 either hard copy or EHRs (Goldberg, 2011). Documentation gaps or errors caused by inadequate EHR training can exacerbate the problem (Mangalmurti et al., 2010). Regardless of an EHR’s evolution within a healthcare practice, using clinical decisionsupport functions can be crucial when it comes to medical liability. Benefits are achieved if a clinician adheres to decision support reminders and recommendations (Waxman, 2010). Ignoring them can lead to liability. Because clinicians have these guidelines available to them, they may be held to a higher standard than those who don’t have access to them (Cerrato, 2011). Not having an EHR may constitute deviation from the standard of care, which Goldberg (2011) defines as “what is customary among physicians in the same specialty in similar settings.” Medical malpractice stems from proving that a defendant caused injuring by not adhering to an established standard of care (Mangalmurti et al., 2010). In sum, existing case studies and examples show that EHRs can both increase and lower a clinician’s malpractice risk. To help bolster support for positive EHR outcomes and eliminate some of the negative risks of EHR implementation, Carter (2011) recommends funding for a federal mandate for the nationwide adoption of EHRs and state-by-state statutory protections to reduce a clinician’s exposure to unreasonable liability. According to Carter (2011) and Dougherty et al. (2010), multiple stakeholders will need to be involved in the process, including but not limited to:  The clinicians who use the system  Health Information Management (HIM) professionals charged with ensuring an official record of care is compliant, credible, and disclosable for secondary uses  Policy makers seeking to improve healthcare  Lawmakers who can help address some of the current legal implications of EHRs Most experts acknowledge the fears associated with EHRs but remain confident that because they are still in an early stage of development, EHRs will have benefits that overshadow their risks (Mangalmurti et al., 2010; Terry, 2007). EHR INFLUENCE ON MEDICAL MALPRACTICE LIABILITY 3 References Carter, B. (2011). Electronic Medical Records: A Prescription for Increased Medical Liability? Vanderbilt Journal of Entertainment and Technical Law, 13(2), 385-406. Cerrato, P. (2011, September 29). Will Your EHR Land You in Court? Retrieved from: http://www.informationweek.com/news/healthcare/EMR/231602442?queryText=health+ care+informatics Dembrow, M. (2009, February). Electronic Records Linked to Fewer Malpractice Payouts. Renal & Urology News, 26. Dougherty, M., & Washington, L. Still Seeking the Legal HER. Journal of the American Health Information Management Association, 81(2), 42-45. Goldberg, D. (2011, February). EHR Expectations. Dermatology Times, 32(2), 8. Managed Care Weekly Digest (2008, December 8). Harvard Medical School: Electronic Health Records May Lower Malpractice Settlements, 37. Mangalmurti, S.S., Murtagh, L., & Mello, M.M. Medical Malpractice Liability in the Age of Electronic Health Records. The New England Journal of Medicine, 363(21), 2060-2067. Terry, K. (2007, July 6). Will an HER Affect Your Malpractice Risk? Medical Economics, 5558. Waxman, S. (2010, June). EHRs Offer Significant Medicolegal Benefits – and Risks: Thorough Documentation Remains Vital to Avoiding Malpractice Lawsuits. Urology Times, 37(7), 36. 11 Sample: Health Information Technology Short Paper This sample was prepared for Drexel INFO 648. Course description and goals are here. HIT OFFERS BENEFITS; STUDY ASSUMPTIONS UNCERTAIN 1 HIT Offers Improvement to Healthcare Despite Dubious Underlying Study Assumptions Healthcare information technology (HIT) has been the subject of much debate and study since the President earmarked $22.6 billion for it in 2009, anticipating it will modernize U.S. healthcare (U.S. Department of Health and Human Services (HHS), 2011). This discussion looks at the benefits of HIT as a means to solve several healthcare issues, beginning with an introduction to the subject based on a Radio Times talk show interview with Dr. Ashish Jah, and concludes with my opinions on the subject. In his interview, Dr. Ashish Jah of Harvard’s School of Public Health informs listeners about the switch from paper-based medical records to EHRs, citing these benefits: financial incentives from the government to make the switch; information presentation in an easy-to ready format; lower costs; the capacity to build an information exchange across locations; treatment and medication alerts; reduction and/or elimination of duplicate testing; and decision support based on recent advances in medicine (Moss-Coane, 2009). While I appreciate Dr. Jah’s discussion points on the HIT benefits, I was more impressed by callers’ comments and personal experience with EHRs, expressing skepticism about having enough technological tools available for multiple patient care, concern about privacy, and appreciation for existing systems that identified crucial information that might have otherwise gone missing in paper records (Moss-Coane, 2009). It’s easy to research benefits of EHRs in various publications, but being able to comment from personal experience or highlight other aspects rarely touched on in the articles I’ve reviewed was more enlightening, realistic, and practical. New aspects of HIT unfamiliar to me prior to listening to the show include debate on privatizing or nationalizing the HIT effort and building upon the already existing, “free” Veterans Administration system (Moss-Coane, 2009). After listening to this broadcast, I remain convinced that HIT is beneficial and can help solve some healthcare problems. Additional research findings that support my optimistic feelings about the benefits of HIT include two studies, one carried out with 72 Texas hospitals and the other focused on analyzing data from 27 studies conducted throughout the U.S. The Texas study linked reduced mortality, complications, and costs to greater automation in a hospital (Amarasingham et al., 2009). The second study showed that electronic prescribing can reduce the risk for medication errors and adverse drug events (ADE)” (Ammenwerth et al., 2008, p. 585). HIT OFFERS BENEFITS; STUDY ASSUMPTIONS UNCERTAIN 2 While I remain convinced of the benefits of HIT, I’m slightly more skeptical now than before I read the articles and listened to Radio Times. My skepticism stems from how people relate their findings and collectively use them to support their beliefs in support of HIT. At issue is the fact that people use different study methods to arrive at the same conclusion. The Texas study used a questionnaire to measure a hospital’s level of automation based on physician interactions with the system (Amarasingham et al., 2009, p. 108). In the ADE study, the authors performed a systematic and quantitative review of 27 previously-published studies (Ammenwerth et al, 2008, p. 590-591). The Texas study could be construed as a qualitative study: one that gathers information not in a numerical form, such as unstructured interviews and open-ended questionnaires. In contrast, a quantitative study gathers data in numerical form for categorization, ranking, and unitbased measurement (Mcleod, 2008). The ADE study seems more like a quantitative study to me. The Texas study appears to have used a questionnaire and then quantified the answers. The “danger” of using qualitative and quantitative studies together is that both approaches do not study the same phenomena and therefore probably shouldn’t be combined for other purposes (Sale et al., 2002, p. 43). According to Sale et al. (2002), a quantitative approach is based on positivism, the state or quality of being positive. An investigator can study something without influencing or being influenced by it (Sale et al., 2002, p. 44). In comparison, a qualitative approach is based on interpretivism – “there are multiple realities or truths based on one’s construction of reality” (Sale et al., 2002, p. 45). Sale et al. (2002) state that a “researcher and the study object are linked so that findings are created within the context of the situation that shapes the inquiry” (p. 45). Sale et al. (2002) go on to say that “samples are not meant to represent large populations” so much as they are used to “provide important information” (p. 45). In light of this information, I’d be apt to do away with Dr. Jah’s interview and the two journal articles in support of HIT. However, I’m going to set aside my engineer’s intuition and continue to look at HIT as a layperson looking in on a series of debates and research studies that say HIT has many benefits. For now I’m in favor of an argument included by Sale et al. in their quantitative-qualitative debate: “forge ahead with what works” (2002, p. 47); and HIT seems to be working to solve some serious healthcare issues like medical errors and ADEs. HIT OFFERS BENEFITS; STUDY ASSUMPTIONS UNCERTAIN References Amarasingham, R., Plantinga, L. Diener-West, M., Gaskin, D.J., & Power, N.R. (2009, January 26). Clinical Information Technologies and Inpatient Outcomes: A Multiple Hospital Study. Archives of Internal Medicine, 169(2), 108-114. Ammenwerth, E., Schnell-Inderst, P., Machan, C., & Siebert. U. (October 2008). The Effect of Electronic Prescribing on Medication Errors and Adverse Drug Events: A Systematic Review. Journal of the American Medical Informatics Association, 15(5), 585-600. Mcleod, S. (2008). Qualitative Quantitative. Retrieved from: http://www.simplypsychology.org/qualitative-quantitative.html Moss-Coane, M. (Producer). (2009, May 11). Ashish Jah on Electronic Health Records. Philadelphia: WHYY, Inc. Positivism. (2011). In Dictionary.com online. Retrieved from: http://dictionary.reference.com/browse/positivism Sale, J.E.M., Lohfeld, L.H., & Brazil, K. Revisiting the Quantitative-Qualitative Debate: Implications for Mixed-Methods Research. Quality & Quantity, 36, 43-53. U.S. Department of Health and Human Services. (2011). Recovery Act-Funded Programs. Retrieved from: http://www.hhs.gov/recovery/programs/index.html#Health 3 15 Sample: Website Review This sample was prepared for Drexel INFO 648. Course description and goals are here. REVIEW OF TWO WEIGHT LOSS MEDICATION WEBSITES 1 Credibility Review of Two Weight Loss Medication Websites Using the Internet to research health information is common practice for millions of Americans, but organizations like the National Library of Medicine (NLM) urge caution when it comes to reviewing and accepting content for fact (Medical Library Association (MLA), 2011; NLM, 2011). Using the NLM’s guidelines, a non-credible and credible weight loss medication website was reviewed, and results based on publicly available content as of November 13, 2011, are presented herein. According to the NLM (2011), a non-credible website may have unknown authors and references, sponsorship bias, unclear purpose, unlabeled advertisements, outdated information, or “miracle cure” promises. In contrast, a credible website typically: provides contact information for its authors, references professionally-accepted medical sources and current research, and discloses its privacy policy (NLM, 2011). To highlight these differences, an example of a noncredible and credible website on the subject of weight loss medication is presented as follows. When using search engine Google to look for information on “fast weight loss,” fast-weight-losstips.com is an example of one of the resulting websites. I was looking for information on weight loss medication, so I selected the Diet Pills tab, which presents the page shown in Figure 1. No author is cited for the Figure 1. The Diet Pills page on fast-weight-loss-tips.com (http://www.fast-weight-loss-tips.com/category/diet-pills/2011). Lipovox article shown in Figure 1 or any of the other commentary present on the page. It’s not evident who runs, maintains, and writes content, as there is no “About Us” informational section or similar identifying criteria. All articles were written in January 2009. There are no references to medical or other reputable resources. Hyperlinks appear to be functional (fast-weight-loss-tips.com, 2009). REVIEW OF TWO WEIGHT LOSS MEDICATION WEBSITES There are five unlabeled advertisements on the “Diet Pills” tab (fast-weight-losstips.com, 2009). The “As Seen on TV” advertisement in Figure 1 takes a consumer to another website that attempts to explain why people are fat and offers for a sale a “pro” and “hardcore elite” version of a fat loss plan (Gudakunst, n.d.). Based on the defining criteria previously presented, fast-weightloss-tips.com does not appear to be credible. In search of greater credibility, I visited the website Drugs.com and reviewed the webpage Weight Loss Medications. Drugs.com (2011) “provides free, peer-reviewed, accurate and independent data on more than 24,000 prescription drugs, over-the-counter medicines and natural products.” The purpose of the Figure 2. The Weight Loss Medication page on Drugs.com (http://www.drugs.com/condition/weight-loss.html, 2011). Weight Loss Medications page, its references, and how its information should and should not be used is clearly stated. The page provides active hyperlinks to additional information and to the website’s certificate of compliance with the Health on the Net (HON) Code of Conduct, a nonfee certification provided by independently-operated HON Foundation (Drugs.com, 2011; HON 2011). HON reviews websites to verify that they attempt to publish objective, transparent, quality medical information (HON, 2011). In conclusion, I’d use Drugs.com because it clearly states its sources and limitations. While HON certification is reassuring, it’s not going to persuade me to use one website over another. I rely on multiple information sources, so Drugs.com would be one of several sources I’d consult. I consider fast-weight-loss-tips.com less credible because it does not cite sources or references. Its advertisements are shoddy in appearance and content, indicating a lack of professionalism and misuse of a desktop illustration program to present misleading before and after results. Quality and professionalism matter, and Drugs.com achieves these standards by choosing to use clear language and provide full disclosure of all information presented. 2 REVIEW OF TWO WEIGHT LOSS MEDICATION WEBSITES References Drugs.com. (2011). Weight Loss Medications. Retrieved from: http://www.drugs.com/condition/weight-loss.html Fast-weight-loss-tips.com. (2009). Articles in the Diet Pills Category. Retrieved from: http://www.fast-weight-loss-tips.com/category/diet-pills/ Gudakunst, S.( n.d.). Shocking Proof: Here’s the Real Reason You’re Fat. Retrieved from: http://topsecretfatlosssecret.com/?hop=zakura Health on the Net Foundation. (2011). Certificate of Compliance with the Code of Conduct HONcode. Retrieved from: http://www.hon.ch/HONcode/Conduct.html?HONConduct756274 Health on the Net Foundation. (2011). What is It? The Commitment to Reliable Health and Medical Information on the Internet. Retrieved from: http://www.hon.ch/HONcode/Patients/Visitor/visitor.html Medical Library Association (MLA). (2011). A User's Guide to Finding and Evaluating Health Information on the Web. Retrieved from: http://www.mlanet.org/resources/userguide.html National Library of Medicine. (2011). Evaluating Internet Health Information. [Adobe Flash Tutorial]. Retrieved from http://www.nlm.nih.gov/medlineplus/webeval/webeval.html 3 19 Sample: Annotated Bibliography This sample was prepared for Drexel INFO 648. Course description and goals are here. ANNOTATED BIBLIOGRAPHY: SURVEILLANCE 1 Annotated Bibliography for Public Health Surveillance Andresen, E. M., Diehr, P. H., & Luke, D. A. (2004). Public Health Surveillance of LowFrequency Populations. Annual Review of Public Health, 25(1), 25-52. Problems and approaches for situations with insufficient surveillance data using examples of race and ethnic minority groups are presented. The need for this work is established from the authors’ experience of achieving confidence in data, which is difficult to attain because small ethnic group numbers can cause margins of error. The intended audience includes those involved in health surveillance activities. Advantages and disadvantages of using traditional data sources and surveillance methods are discussed. Data collection improvements are recommended for sampling strategies, field methods, and survey logistics. Also included are data analysis recommendations: spatial smoothing with Geographic Information Systems (GIS), small area estimation, exact statistical methods, and/or provider profiling methods. This article is valuable because it’s comprehensive and provides insight into the advantages and disadvantage of surveillance strategies. It’s a great go-to article for help on determining how to enhance existing surveillance methods and how to make the most of existing data sets. A specific set of steps for definitive corrective action is not included, but the authors say this is not the intended purpose. The article is meant to encourage steps for revising existing methods or incorporating new strategies to better results. Lazarus, R., Yih, K., & Platt, R. (2006, September 19). Distributed Data Processing for Public Health Surveillance. Biomed Central Public Health, 25(1), 235-246. Advantages and disadvantages of using a distributed processing model for routine, automated syndromic surveillance are presented. In the authors’ system, which supports the National Bioterrorism Syndromic Surveillance Demonstration Program (NDP), data processing is distributed to data collection sites rather than being performed at one central location, allowing personal health information (PHI) to be pre-processed remotely under the security and control of the data provider. The intended audience of this article includes those who need information on how to develop syndromic surveillance systems, regardless of worldwide location. This article is valuable because it demonstrates a feasible system in which PHI is protected concurrently with on-going syndromic surveillance activities. While this is the second publication on this specific topic, the authors feel strongly that their system is a valuable alternative surveillance system option that warrants more in-depth explanation and debate. The article is straightforward and honest in terms of presenting the system’s advantages and disadvantages. It presents a good case study of a system that addresses PHI privacy concerns and should be one of several consulted on the topic of syndromic surveillance. ANNOTATED BIBLIOGRAPHY: SURVEILLANCE McNabb, S. J. N. (2010). Comprehensive Effective and Efficient Global Public Health Surveillance. Biomed Central Public Health, 10(Supplement 1), 3-7. A global forum used to develop an interoperable, global public health grid that can provide information when and where it’s needed is proposed. The intended audience is anyone doing work on or in support of global public health surveillance. The author cites three global movements that can set in motion joint, global surveillance efforts, including the adoption of revised International Health Regulations (IHR) by all World Health Organization (WHO) Member States, advances in health informatics and information technology, and consensus between global security and public health groups that it is mutually beneficial to achieve public health surveillance. Interdependent prerequisites are needed for development to occur: demand and mutual interest; respect for human rights and data ownership; a shared vision; regional, national, and global perspectives; standard operating procedures and lines of authority; assessment of existing workflow; training and transparency; and funding. This article is a great starting point for discussions on global public health surveillance. It is valuable because it specifically lists challenges and requirements necessary for making progress in this area. This article should be one of several articles consulted on the subject of global public health surveillance. Nordin, J. D., Kasimow, S., Levitt, M. J., & Goodman, M. J. (2008, May). Bioterrorism Surveillance and Privacy: Intersection of HIPPA, the Common Rule, and Public Health Law. American Journal of Public Health, 98(5), 802-807. In response to a lack of privacy safeguards, this article proposes three health surveillance ethical review processes that can be implemented independently or combined prior to surveillance being carried out, including a systems solution involving data agreements, a structural solution such as a public health information privacy board, and/or expansion of an institutional review board. The authors contend that such review is necessary to prevent accidental or intentional data releases and misunderstandings or misinterpretations associated with privacy and public health laws. The intended audience is health policymakers, legislative authorities, and those interested in learning about health privacy issues. This article is an editorial piece. It does a good job of explaining in layman’s terms the three main privacy laws: the Health Insurance Portability and Accountability Act, the Common Rule and protection of human study participants, and public health law. However, the specific idea proposed is confusing and not intuitively obvious until the last paragraph. Even then, readers 2 ANNOTATED BIBLIOGRAPHY: SURVEILLANCE may be left wondering if they’ve understood the article correctly. This article should be one of several reviewed on the subject of health surveillance and policy. Wartenberg, D. Thompson, W. D., Fitzgerald, E. F., Gross, H. J., Condon, S. K., Kim, N., Goun, B. D., Opiekun, R. E., & the University of Medicine and Dentistry of New Jersey (UMDNJ) Collaborative Project Working Group on Northeast United States (U.S.) Ambient Air Quality and Adverse Birth Outcomes Surveillance. (2008, November). Developing Integrated Multistate Environmental Public Health Surveillance. Journal of Public Health Management Practice, 14(6), 552-561. Preliminary steps are summarized for the University of Medicine and Dentistry of New Jersey (UMDNJ) Collaborative Project on Northeast U.S. Ambient Air Quality and Adverse Birth Outcomes, conducted under the Centers for Disease Control’s (CDC) Environmental Public Health Tracking (EPHT) Program. The intended audience for this article is any local, national, or international agency working on public health issues and/or surveillance. Study participants and methodology are presented, along with the study’s goals: to demonstrate states’ abilities to identify a common environmental health issue, establish and share consistent data, and collaboratively analyze data to develop observations and conclusions of local and regional significance for intervention. Administrative and scientific issues likely to arise in a nationwide assessment are identified and discussed in order to demonstrate feasibility. The value of this article is in the presentation of a multi-state, collaborative study framework as compared to an individual-scale surveillance study. A multi-state framework can be difficult to establish because of the need for consensus, confidence that data will remain private, and data analysis protocol development that is mutually acceptable to all parties. There are no weaknesses in this article other than the proposed use of computer model-generated air quality data. The limitations of using this data are clearly acknowledged by the authors, so one can presume that study results will be interpreted appropriately. This is one of several articles that should be consulted on the subject of multi-state collaborative frameworks for public health surveillance. 3 23 Sample: Relational Database System Design Logical Design and Implementation This sample was prepared for Drexel INFO 605, Introduction to Database Management. Details for this course are as follows: Description INFO 605 emphasizes the basic concepts and methods employed in the theory and practice of modern database systems. We will focus on database design, data manipulation, and data integrity maintenance. Topics include database design techniques using the entity-relationship approach, techniques of translating entityrelationship diagrams into relational schema, integrity constraints, relational algebra, commercial query languages and normalization techniques.. Course Objectives        Explain the fundamental concepts associated with database management systems Analyze data management problems (e.g., assess the information needs of a business) Design databases that address those problems using industry-standard methodologies Implement those designs using popular commercial-grade database software packages Develop applications that interact with databases using SQL Search in a bioinformatics database Critically discuss current research literature in healthcare informatics Database Design for Meals on Wheels Jinyan Chen Kurt Esposito Tracy Lamb Lisa Romanoski Drexel University Author Note This paper has been prepared in accordance with the requirements of INFO 605, Course Project Milestone 2. Certification I certify that:  This paper/project/exam is entirely my own work.  I have not quoted the words of any other person from a printed source or a website without indicating what has been quoted and providing an appropriate citation.  I have not submitted this paper/project to satisfy the requirements of any other course. Signatures: Jinyan Chen Kurt Esposito Tracy Lamb Lisa Romanoski Date: March 23, 2012. DATABASE DESIGN: MEALS ON WHEELS Table of Contents Project Description.......................................................................................................................... 1 Chestnut Hill Meals on Wheels ................................................................................................ 1 Current Operations .................................................................................................................... 2 Data Management Problem....................................................................................................... 3 Opportunities............................................................................................................................. 4 Requirements Specification ............................................................................................................ 5 Information That Needs to Be Captured ................................................................................... 5 Associated Business Rules ........................................................................................................ 6 Conceptual Design .......................................................................................................................... 8 EER Diagram ............................................................................................................................ 8 Relational Schema .......................................................................................................................... 9 Database Implementation.............................................................................................................. 11 Data Queries.................................................................................................................................. 13 Data Manipulation ........................................................................................................................ 15 INSERT examples .................................................................................................................. 15 UPDATE examples ................................................................................................................. 16 DELETE examples ................................................................................................................. 18 Summary ....................................................................................................................................... 19 References ..................................................................................................................................... 21 i DATABASE DESIGN: MEALS ON WHEELS List of Figures Figure 1. CHMOW delivery area (www.mapquest.com). .............................................................. 1 Figure 2. CHMOW’s labels in MS Word. ..................................................................................... 3 Figure 3. Extended Entity Relationship Diagram (EERD) for the CHMOW database. ................ 8 Figure 4. CHMOW Relational Schema ....................................................................................... 10 List of Appendices Appendix A: Kitchen Spreadsheet ............................................................................................... 22 Appendix B: Driver Packet .......................................................................................................... 25 ii DATABASE DESIGN: MEALS ON WHEELS 1 Project Description The steps following conceptual database design are logical design and implementation (Whitten and Bentley, 2005, p. 202). These steps were carried out using a requirements analysis and conceptual design for the Meals on Wheels Chestnut Hill, Pennsylvania, chapter (CHMOW). This paper is part two of a two-part project report and includes the following:  Requirements specification  Conceptual design  Relational schema  Database implementation  Example data queries  Example data manipulation tasks We conclude with a summation of our project and discuss how it can facilitate data management at CHMOW. Chestnut Hill Meals on Wheels As we mentioned in project report one, Chestnut Hill Meals on Wheels (CHMOW) is a community-based, nonprofit organization providing fresh, nutritious meals to physically and/or mentally incapacitated seniors aged 60 years or older via volunteer-based delivery Figure 3. CHMOW delivery area (www.mapquest.com). to the Chestnut Hill, Erdenheim, Mt. Airy, Flourtown, Oreland, and Wyndmoor communities north of Philadelphia, PA, as shown in Figure 1 (CHMOW, 2012). Up to two meals a day at a cost of $7 a day or $35 a week may be delivered on a schedule that has any combination of days DATABASE DESIGN: MEALS ON WHEELS during the entire week (CHMOW, 2012). With the exception of its executive and administrative staff, CHMOW relies on volunteers to assist in one of five areas: meal packing, meal delivery, congregate center assistance, special events, and fund raising (CHMOW, 2012). Current Operations As mentioned previously, CHMOW is comprised of executive and administrative staff and volunteers. All CHMOW operations requiring a computer are carried out using Microsoft (MS) Office software on Apple computers. No databases are used. Typical, daily CHMOW operations are as follows: 1. In preparation for the next day’s meals, the executive director opens an Excel spreadsheet to the “Route Totals” sheet. Column A lists all clients, organized by route. Subsequent columns indicate food and dietary preferences, including but not limited to portion size, bread choice (wheat, white, etc.), and vegetarian or meat options. For each client, subsequent cell values are “toggled” on or off: “0” indicates no value and “1” indicates a chosen preference. For example, if a client will not receive a meal the next day, “client” is changed to “0.” Cell values are either “0” or “1,” but there are circumstances that warrant a larger number entry. For example, a client may request one sandwich but two low-fat milks daily. The entry under “milk” would read “2.” 2. After updating the columns, the executive director navigates to and prints the “Kitchen List” sheet which calls total values from the “Route Totals” sheet. Changes are saved if they are permanent changes. For example, a client’s dietary needs may change such that pork is no longer acceptable in a dinner entrée but beef and chicken are. Changes are not saved if the desired action is temporary. For example, a client will be out of town and miss a daily delivery but will still require annual meal delivery. 2 DATABASE DESIGN: MEALS ON WHEELS 3. Next, meal labels are printed for the kitchen staff using MS Word, as shown in Figure 2. Of a twopage document, page 1 labels are attached to cold meals (lunch sack) and page 2 labels are attached to hot meal (aluminum trays with lids). The labels and the spreadsheet’s kitchen totals output are then Figure 4. CHMOW’s labels in MS Word. provided to staff. 4. A separate Excel spreadsheet is used each day to track client billing. Clients’ entries are updated as needed and then information is extracted with which to make invoices. Invoices are generated using MS Office software and then mailed once a month to clients. Fees paid, unpaid, and other miscellaneous notes are kept on file in the same spreadsheet. 5. The next morning, the kitchen staff assembles lunch sacks and hot trays, attaching the correct labels to each, and place the meals into two coolers per client route for one of six routes. Coolers and route-specific information packets are stacked outside for pick up. The packet contains a route’s client list, including addresses and special instructions, and driving directions for house-to-house navigation. 6. Lastly, the drivers arrive, pick up meals, and make deliveries. Following deliveries, coolers and informational packets are returned to CHMOW headquarters (see Appendices A and B for kitchen and driver packet examples). Data Management Problem The problem with CHMOW’s data management practices is that the organization is limited to using a combination of MS Office products that do not interact with one another, resulting in operational inefficiency and increased likelihood for errors. For example, if a client 3 DATABASE DESIGN: MEALS ON WHEELS requests a temporary meal delivery cessation, the labels for the next day must be manipulated in Word based on information in one master Excel spreadsheet. In addition, invoice practices are time consuming, requiring staff to open the master Excel spreadsheet and cut and paste information into a separate Word document for invoicing. Another Word document is then used to print labels for envelopes. In summary, CHMOW’s administrative tasks tend to be disjointed from all the opening and closing of separate documents and can be susceptible to errors due to slow update times depending on user operations. Opportunities for improvement are discussed in the next section. Opportunities Opportunities for improving CHMOW’s business needs include creating one central database with which to link and regularly update multiple functional areas, including but not limited to kitchen preparation, delivery label-making, production of daily delivery information, invoicing, and donor activities. Database representations of CHMOW’s activities can be conceptualized as miniworlds. For CHMOW, there are two miniworlds: 1. Correct execution of daily operations based on current information, and 2. On-going community outreach efforts as related to fund-raising and volunteer drives. Although the miniworlds have different data and business processes, they are related by the people involved in the processes. The database design will focus on daily operations only. Future database expansion for community outreach operations and invoicing will be considered in the design process but not incorporated in the first database iteration. 4 DATABASE DESIGN: MEALS ON WHEELS 5 Requirements Specification Information That Needs to Be Captured Having determined the need for a database, data that needs to be captured about CHMOW’s operations includes information about staff, volunteers, and donor, as summarized in Table 1. Our project is limited in scope to creating a database that can produce reports daily for the kitchen and drivers. Financial reporting and invoicing are not included in our project scope. Table 1. CHMOW Database Needs Category Data Needed Staff Taxpayer identification First, last name Address Phone Email Volunteers Driver’s license First, last name Address Phone Email Completed application Signed release form Insurance card copy Orientation program completion status Training status Availability Primary driving schedule (with map) Alternate driving schedule (with map) Miscellaneous notes (other) Clients First, last name Billing address Delivery address Primary phone Alternative phone Emergency contact number Email Meal preferences Delivery schedule (any combination of days) Route Invoice preparation status DATABASE DESIGN: MEALS ON WHEELS 6 Category Data Needed Invoice delivery status Invoice payment status Miscellaneous notes (other) Donors Taxpayer identification First, last name Address Phone Email Donation amount Donation date (month/day/year) Thank you note composition status Thank you note delivery status Documents Daily kitchen report Address label template Thank you note template Associated Business Rules In addition to identifying informational needs for the database, business rules need to be incorporated as well. Business rules are constraints in that they dictate and/or limit database activities and functions. Table 2 lists CHMOW’s business rules. Table 2. CHMOW’s Business Rules Business Rules Meals are delivered Monday through Friday and holidays. Each client and volunteer is entered into the database once. a) b) c) d) e) f) (1) g) h) i) Meal preferences: Meal type: regular or double Soup: yes or no Salad: yes or no Bread: yes or no Bread preference: white, whole wheat, or rye Sandwich: yes or no Preference: white, whole wheat, or rye Fruit cup: yes or no Fresh fruit: yes or no Dessert: yes or no DATABASE DESIGN: MEALS ON WHEELS j) (1) k) (1) Business Rules Milk: yes or no Preference: Lactaid, low fat, skim, whole Juice: yes or not Preference: apple, cranberry, or orange Client dietary restrictions are variable and include: a) b) c) d) e) f) g) h) i) j) k) l) m) n) o) p) q) ADA (indicates diabetic) Bananas (indicates client needs banana for potassium) No Beef No Cilantro No Chicken Legs Vegetarian No corn, beans, seeds or nuts No fish No fried foods No leafy foods No meat loaf No mushrooms No pasta No pork No shrimp No tomato sauce Soft foods and chopped a) b) c) d) Routes: Have a number that is variable Have names Are created and removed as the number of clients changes May have zero or more clients a) b) c) d) Drivers may or may not have scheduling preferences, which include: Day of week Frequency (weekly, monthly, etc.) Availability (for example, June, July and Aug only) Ability to be on-call to drive as needed When scheduling drivers, each route can have one or two drivers on any given day. 7 DATABASE DESIGN: MEALS ON WHEELS 8 Conceptual Design EER Diagram Following identification of business needs and constraints, an EER diagram of CHMOW’s database was completed and is shown below. Included in the EER diagram are primary and foreign keys, relationship cardinality, and participation numbers. Person Assumptions:       Only active clients receive meals Only 1 meal is delivered to a client on any given day A single driver will only drive 1 route on any one day. All meals, regardless of preferences and restrictions, are charged a single fee for each meal. (Currently, $7.00) There are several more categories of Volunteers; they are not shown here as it is outside the scope of this project. Billing and invoicing are not included, as that is handled by a separate accounting software package. personID {PK} name fname lname title address street1 street2 city state zip primaryPhone alternatePhone email notes Donation Gives4 1..1 donationID {PK} donationDate donationAmount thankyouSent 1..* {Optional, And} Client MealComponent 1..* mcID {PK} mcDescription sortOrder Prefe rs 0..* ClientMeal personID {PPK} mcID {PPK} quantity 0..* H DietaryRestriction as 0..* 0..* ClientRestriction Figure personID {PPK} includes some drID {PPK} changes from the first EERD that was presented part one of this two-part project report: personID {PK} active completedApp signedRelease orientationStatus trainingStatus preferredDays mon tues wed thurs fri availability startDate endDate 1..1 Assigned To drID {PK} drDescription sortOrder Volunteer personID {PK} active dateAdded schedule mon tues wed thurs fri emergencyContact fname lname phoneNbr billingAddress street1 street2 city state zip 0..1 1..1 Route 1..1 Delivers 1..2 routeNum {PK} /nbrOfClients direction MealDelivery date {PPK} driverID {PPK} clientID {PPK} routeNum Figure 5. Extended Entity Relationship Diagram (EERD) for the CHMOW database. Driver 3 personID {PK} onCall driversLicense insurance backgroundCheck notes in DATABASE DESIGN: MEALS ON WHEELS  Staff, Donor, and Donation entities were removed because the scope effort was re-focused to address only clients and volunteers who are drivers.  Meal Delivery is included as a new entity to replace the previous Meal entity: it allows for tracking of meals and delivery dates by client.  Preference and Dietary Restriction entities were removed to accommodate Meal Component with Client Meal preference and Dietary Restriction linked to a Client Restriction. This allows for making both meal preferences and dietary restrictions attribute values. The roles of the Meal Component and Dietary Restrictions entities become that of a lookup entity in which the identifying attribute appears as a field within the parent entity (Microsoft, 2012). Lookup entities are helpful when there is really only one attribute of interest for people creating reports or obtaining information (Microsoft, 2012). Since lookup entities can only have one attribute specified as an Identifying Attribute property (Microsoft, 2012), the identifying attributes are mcID (meal component identification) and drID (dietary restriction ID). Relational Schema The next step in the logical design process involved translating the EERD into a relational schema, as shown in Figure 4. Primary keys and foreign keys are listed to the right of the figure. 9 DATABASE DESIGN: MEALS ON WHEELS 10 MealDelivery date (PPK) Person (personID, fname, lname, title, street1, street2, city, state, zip, primaryPhone, alternatePhone, email, notes) driverID (PPK) clientID (PPK) routeNum Person title lname fname personID(PK) alternatePhone primaryPhone zip state city street street1 Donation email notes Client (personID, active, Monday, Tuesday, Wednesday, Thursday, Friday, emergencyFName, emergencyLName, emergencyPhone, billingStreet1, billingStreet2, billingCity, billingState, zip, routeNum) Foreign key personID references Person(personID) Route donationDate personID donationID (PK) routeNum (PK) thankyouSent donationAmount direction Volunteer(personID, active, completedApp, signedRelease, orientationStatus, mon, tues, wed, thurs, fri, startDate, endDate) Foreign key personID references Person(personID) Client personID (PK) active monday tuesday wednesday thursday friday emergency emergency billingStreet1 billingStreet2 Phone LName billingCity billingState zip routeNum drID (PPK) drID (PK) drDescription Donation (donationID, personID donationDate, donationAmount, thankyouSent) Foreign key personID references Person(personID) sortOrder MealComponent mcID (PK) mcDescription Driver (personID, onCall, driverLicense, insurance, backgroundcheck, notes) Foreign key personID references Person(personID) DietaryRestriction ClientRestriction personID (PPK) emgergency FName Route (routeNum, description) sortOrder MealComponent (mcID, mcDescription, sortOrder) DietaryRestriction (drID, drDescription, sortOrder) ClientMeal personID (PPK) mcID (PPK) ClientMeal (personID, mcID, quantity) Foreign key personID references Person(personID) Foreign key mcID references MealComponent(mcID) quantity Volunteer personID (PK) active completedApp signedRelease orientationStatus trainingStatus Driver personID (PK) onCall driversLicense Figure 6. CHMOW Relational Schema insurance backgroundCheck notes mon tues wed thurs fri startDate endDate ClientRestriction (personID, drID) Foreign key personID references Person(personID) Foreign key drID references DietaryRestriction( drID) MealDelivery (date, driverID, clientID, routeNum) Foreign key driverID references Person(personID) Foreign key clientID references Person(personID) Foreign key routeNum references Route(routeNum) DATABASE DESIGN: MEALS ON WHEELS Database Implementation Following the creation of the relational schema, DDL statements were composed as follows for each table: CREATE TABLE Person (personID NUMBER(5) NOT NULL, taxpayerID NUMBER(9) UNIQUE, fname VARCHAR2(20), lname VARCHAR2(20), title VARCHAR2(30), street1 VARCHAR2(30), street2 VARCHAR2(30), city VARCHAR2(30) state NUMBER(2), zip VARCHAR2(9), primaryPhone NUMBER(10), alternatePhone NUMBER(10), email VARCHAR2(50), notes LONG, CONSTRAINT PersonID_PK PRIMARY KEY (personID)); CREATE TABLE Donation (personID NUMBER(5) NOT NULL, donationID NUMBER(9) NOT NULL, donationDate DATE, donationAmount NUMBER(6,2), thankyouSent DATE, CONSTRAINT DonationID_PK PRIMARY KEY (donationID) CONSTRAINT Donation_FK FOREIGN KEY (personID) REFERENCES Person(personID) ON DELETE CASCADE; CREATE TABLE Volunteer (personID NUMBER(5) NOT NULL, active CHAR(1) completedApp DATE NOT NULL, signedRelease DATE NOT NULL, orientationStatus DATE NOT NULL, trainingStatus DATE NOT NULL, mon CHAR(1), tues CHAR(1), wed CHAR(1), thurs CHAR(1), fri CHAR(1), startDate DATE, 11 DATABASE DESIGN: MEALS ON WHEELS endDate DATE, CONSTRAINT Volunteer_PK PRIMARY KEY(personID), CONSTRAINT Volunteer_FK FOREIGN KEY (personID) REFERENCES Person(personID) ON DELETE SET NULL) ON DELETE CASCADE; CREATE TABLE Driver (personID NUMBER(5) NOT NULL, onCall CHAR(1), driversLicense VARCHAR2(10), insurance VARCHAR2(20), insuranceNo VARCHAR2(16), backgroundCheck DATE, notes LONG, CONSTRAINT Driver_PK PRIMARY KEY(personID) , CONSTRAINT Driver_FK FOREIGN KEY (personID) REFERENCES Person(personID) ON DELETE SET NULL) ON DELETE CASCADE; CREATE TABLE Client (personID NUMBER(5) NOT NULL, active CHAR(1), dateADDED DATE, mon CHAR(1), tues CHAR(1), wed CHAR(1), thurs CHAR(1), fri CHAR(1), emergencyfname VARCHAR2(20), emergencylname VARCHAR2(20), emergencyPhone NUMBER(10), billingStreet1 VARCHAR2(30), billingStreet2 VARCHAR2(30), billingCity VARCHAR2(30) billingState CHAR(2), zip VARCHAR2(9), routeNUM VARCHAR2(10), CONSTRAINT Client_PK PRIMARY KEY(personID), CONSTRAINT Client_FK FOREIGN KEY (personID) REFERENCES Person(personID) ON DELETE SET NULL) ON DELETE CASCADE; CREATE TABLE Route (routeNum NUMBER(4) NOT NULL, direction LONG, CONSTRAINT routeNum_PK PRIMARY KEY (routeNum)); CREATE TABLE MealDelivery (date DATE NOT NULL, 12 DATABASE DESIGN: MEALS ON WHEELS driverID NUMBER(5) NOT NULL, clientID NUMBER(5) NOT NULL, routeNum NUMBER(4), CONSTRAINT date_PK1 PRIMARY KEY(date), CONSTRAINT driverID_PK2 PRIMARY KEY(driverID), CONSTRATIN clientID_PK3 PRIMARY KEY(clientID), CONSTRAINT MealDelivery_FK1 FOREIGN KEY (driverID) REFERENCES Person(personID) ON DELETE CASCADE, CONSTRAINT MealDelivery_FK2 FOREIGN KEY (clientID) REFERENCES Person(personID) ON DELETE CASCADE), CONSTRAINT routeNUM_FK3 FOREIGN KEY (routeNum) REFERENCES Route(routeNum)); CREATE TABLE MealComponent (mcID NUMBER(4) NOT NULL, mcDescription VARCHAR2(50), sortOrder NUMBER(4), CONSTRAINT MealComponent_PK PRIMARY KEY(mcID)); CREATE TABLE ClientMeal (personID NUMBER(5) NOT NULL, mcID NUMBER(4) NOT NULL, quantity NUMBER(2), CONSTRAINT ClientMeal_PK PRIMARY KEY (personID, mcID) CONSTRAINT personID_FK1 FOREIGN KEY references Person(personID) ON DELETE CASCADE, CONSTRAINT mcID_FK1 FOREIGN KEY references MealComponent(mcID) ON DELETE CASCADE); CREATE TABLE DietaryRestriction (drID NUMBER(4) NOT NULL, drDescription VARCHAR2(50), sortOrder NUMBER(4), CONSTRAINT DietaryRestriction_PK PRIMARY KEY (drID)); CREATE TABLE ClientRestriction (personID NUMBER(5) NOT NULL, drID NUMBER(4) NOT NULL, CONSTRAINT ClientRestriction_PK PRIMARY KEY (personID, drID) CONSTRAINT personID_FK1 FOREIGN KEY references Person(personID), CONSTRAINT drID_FK2 FOREIGN KEY references DietaryRestriction( drID)); Data Queries The following statements are examples of data queries for the new database: 13 DATABASE DESIGN: MEALS ON WHEELS  Find the number of clients who deliveries on Mondays, Wednesday, and Fridays. Include personID and list by routeNum in ascending order. SELECT personID FROM Client c, MealDelivery md WHERE c.personID = md.clientID AND c.mon = �Y’ AND c.wed = �Y’ AND c.fri = �Y’ ORDERBY routeNum;  Determine which clients received meals on Thursday, February 16. SELECT clientID FROM MealDelivery WHERE date = ’16-Feb-12’; Or SELECT fname, lname FROM Person WHERE personID IN (SELECT personID FROM MealDelivery WHERE date= ’16-Feb-12’);  Find the donors who donated more than $5,000 to CHMOW in each donation. SELECT * FROM Person WHERE personID IN (SELECT DISTINCT personID FROM Donation WHERE donationAmount=5000);  Determine which clients have no-dairy dietary restrictions. SELECT personID FROM ClientRestriction WHERE drID = 1100;  Which drivers delivered food for which clients on March 12, 2012? SELECT driverID, clientID FROM MealDelivery WHERE date = ’12-Mar-12’ GROUPBY routeNum;  Print phone number, emergency contact phone number and address of a client whose ID is 12345. 14 DATABASE DESIGN: MEALS ON WHEELS SELECT p.phoneNum, c.phoneNbr, p.street1, p.street2, p.city, p.state FROM Person p, Client c WHERE p.personID =c.personID AND p.personID=12345; Data Manipulation The following statements are examples using the Insert, Update, and Delete commands: INSERT examples INSERT INTO Person VALUES (12345, �Eric’, �Blair’, �Mr.’ �1984 Oceania Dr.’, NULL, �Chestnuthill’, �PA’, �02556’, �6105551701’, �6105551948’, �[email protected]’, NULL); INSERT INTO Person VALUES (12346, �Peter’, �Lake’, �Mr.’, �345 Winter Rd.’ �Apt.3D’, �Chestnuthill’, �PA’, �02556’, �6105554830’, NULL, �[email protected]’, NULL); INSERT INTO Person VALUES (12347, �Beverly’, �Penn’, �Miss’, �200 Coheeries Ln.’, NULL, �Chestnuthill’, �PA’, �02556’, �610555007’, �6105551901’, �[email protected]’, NULL); INSERT INTO Volunteer VALUES (12346, �Y’, ’06-Jun-11’, ’13-Jun-11’, ’13-Jun-11’, ’13-Jun-11’, �Y’, �N’, �Y’, �N’, �Y’, ’22-Jun-11’, NULL) INSERT INTO Driver (12346, �N’, �E140258834’, �Geico’, �104484848337’, ’18-Jun-11’, NULL) INSERT INTO Client VALUES (12347, �Y’, ’10-OCT-08’, �Y’, �Y’, �Y’, �Y’, �Y’, �Isaac’, �Penn’, �6105556767’, �200 Coheeries Ln.’, NULL, �Chestnuthill’, �PA’, �02556’) INSERT INTO Donation VALUES (12345, 122533432, ’22-Ded-11’, 5000.00, NULL); INSERT INTO Donation VALUES (12345, 122533671, ’18-Mar-12’, 150.00, NULL); INSERT INTO Donation VALUES (12346, 122533419, ’19-Dec-11’, 100.00, NULL); INSERT INTO Route VALUES (8812, 5, �SW along Harrison until Vine’); INSERT INTO Route VALUES (8814, 7, �NW Mitchell through Evergreen’); INSERT INTO Route VALUES (8816, 3, �N White Horse through Blue Ridge Apartments’); 15 DATABASE DESIGN: MEALS ON WHEELS INSERT INTO MealDelivery VALUES (’19-Mar-12’, 12346, 12347, 8812); INSERT INTO MealDelivery VALUES (’21-Mar-12’, 12346, 12347, 8812); INSERT INTO MealDelivery VALUES (’23-Mar-12’, 12346, 12347, 8812); INSERT INTO MealComponent VALUES (3155, �sandwich, NULL); INSERT INTO MealComponent VALUES (3167, �fruitcup, NULL); INSERT INTO MealComponent VALUES (3124, �milk’, NULL); INSERT INTO ClientMeal VALUES (12347, 3155, 1); INSERT INTO ClientMeal VALUES (12347, 3167, 1); INSERT INTO ClientMeal VALUES (12347, 3124, 1); INSERT INTO DietaryRestriction VALUES (1122, �no cilantro’, NULL); INSERT INTO DietaryRestriction VALUES (1339, �soft foods’, NULL); INSERT INTO DietaryRestriction VALUES (1123, �vegetarian’, NULL); INSERT INTO DietaryRestriction VALUES (1100, �no dairy’, NULL); INSERT INTO ClientRestriction VALUES (12347, 1122); INSERT INTO ClientRestriction VALUES (12347, 1339); INSERT INTO ClientRestriction VALUES (12347, 1123); UPDATE examples Person UPDATE Volunteer SET wed = �N’ WHERE personID = 12346; UPDATE Person 16 DATABASE DESIGN: MEALS ON WHEELS SET primaryPhone = 6105551111 WHERE personID = 12346; Update Client Set fri = �N’ WHERE personID = 12347; Donation UPDATE Donation SET thankyouSent = �22-Mar-12’ WHERE personID = 12345 AND donationID = 122533671; UPDATE Donation SET thankyouSent = �2-Feb-12 WHERE personID = 12345 AND donationID = 122533432; UPDATE Donation SET thankyouSent = �2-Feb-12’ WHERE personID = 12346 and donationID = 122533419; Route UPDATE Route SET numberofClients = 4 WHERE routeNum = 8812; UPDATE Route SET direction = �NW Mitchell through Evergreen including Hempstead’ WHERE routeNum = 8814; UPDATE Route SET direction =’SW along Harrison until Vine including Lake and Valley’ WHERE routeNum = 8812; ClientMeal UPDATE ClientMeal SET quantity = 2 WHERE personID = 12347 AND mcID = 3155; UPDATE ClientMeal SET quantity = 2 WHERE personID = 12347 AND mcID = 3167; UPDATE ClientMeal SET quantity = 2 WHERE personID = 12346 AND mcID = 3124; 17 DATABASE DESIGN: MEALS ON WHEELS DELETE examples Person DELETE FROM Person WHERE personID = 12347; DELETE FROM Driver WHERE personID = 12346; DELETE FROM Person WHERE person ID = 12345; Donation DELETE FROM Donation WHERE personID = 12345 AND donationID = 122533432; DELETE FROM Donation WHERE personID = 12345 AND donationID = 122533671; DELETE FROM Donation WHERE personID = 12346 AND donationID = 122533419; Route DELETE FROM Route WHERE routeNum = 8812; DELETE FROM Route WHERE routeNum = 8814; DELETE FROM Route WHERE routeNum = 8816; MealDelivery DELETE FROM MealDelivery WHERE date = ’19-Mar-12’ AND driverID = 12346 AND clientID = 12347; DELETE FROM MealDelivery WHERE date = ’21-Mar-12’ AND driverID = 12346 AND clientID = 12347; DELETE FROM MealDelivery WHERE date = ’23-Mar-12’ AND driverID = 12346 AND clientID =12347; MealComponent DELETE FROM MealComponent WHERE mcID = 3155; 18 DATABASE DESIGN: MEALS ON WHEELS DELETE FROM MealComponent WHERE mcID = 3167; DELETE FROM MealComponent WHERE mcID = 3124; ClientMeal DELETE FROM ClientMeal WHERE personID = 12347 AND mcID = 3155; DELETE FROM ClientMeal WHERE personID = 12347 AND mcID = 3167; DELETE FROM ClientMeal WHERE personID = 12347 AND mcID = 3124; DietaryRestriction DELETE FROM DietaryRestriction WHERE drID = 1122; DietaryRestriction DELETE FROM DietaryRestriction WHERE drID = 1339; DietaryRestriction DELETE FROM DietaryRestriction WHERE drID = 1123; ClientRestriction DELETE FROM ClientRestriction WHERE personID = 12347 AND drID = 1122; DELETE FROM ClientRestriction WHERE personID = 12347 AND drID = 1339; DELETE FROM ClientRestriction WHERE personID = 12347 AND drID = 1123; Summary In summary, CHMOW’s operational activities depend on data that is manipulated using MS Office software. This method is inefficient in that various documents need to be manually opened and updated in order to view, enter, delete, or copy and paste data into other documents 19 DATABASE DESIGN: MEALS ON WHEELS to successfully execute tasks. Due to the fact that the software programs can’t interact with each other, the length of time to execute activities and the likelihood for errors can be substantial. Developing a central database that automatically updates data used by several functions, such as the kitchen preparation lists and daily delivery route information for drivers, would increase efficiency and decrease likelihood for errors. This paper, part two of a two-part project report, presents how to begin the process of transforming CHMOW’s operational practices from one that relies on MS Office software to one that relies on a database. We expect to see increased operational efficiency, sharing of data, reduction in data redundancy, data consistency, program-data independence, and improved data accessibility (Li, 2012). 20 DATABASE DESIGN: MEALS ON WHEELS References Chestnut Hill Meals on Wheels. (2012). Chestnut Hill Meals on Wheels. Retrieved from: http://www.chestnuthillmow.com/ Li, J. (2012). Introduction to Database Management [Powerpoint Slides]. Retrieved from: http://drexel.blackboard.com/webapps/portal/frameset.jsp?tab_id=_2_1&url=%2fwebapp s%2fblackboard%2fexecute%2flauncher%3ftype%3dCourse%26id%3d_464820_1%26ur l%3d Microsoft. (2012). Lesson 9: Specifying a Lookup Entity. Retrieved from: http://msdn.microsoft.com/en-us/library/ms345302.aspx Whitten, J., & Bentley, L. (2005). System Analysis and Design Methods. New York, NY: McGraw Hill. 21 DATABASE DESIGN: MEALS ON WHEELS Appendix A: Kitchen Spreadsheet 22 DATABASE DESIGN: MEALS ON WHEELS Figure A-1. Route Totals worksheet. Figure A-2. Kitchen List worksheet. This worksheet is provided daily to kitchen staff. 23 DATABASE DESIGN: MEALS ON WHEELS Figure A-3. Invoicing Worksheet 24 DATABASE DESIGN: MEALS ON WHEELS Appendix B: Driver Packet 25 DATABASE DESIGN: MEALS ON WHEELS Figure B-2. An example of directions provided to volunteers. 26 DATABASE DESIGN: MEALS ON WHEELS Figure B-1. An example of a daily delivery client list. 27 55 Sample: Personas This sample was prepared for Drexel INFO 608, HumanComputer Interaction. Details for this course are as follows: Description This course focuses on the design and evaluation of human-computer interfaces covering such topics as task analysis techniques for gathering design information, iterative design through prototyping, and formative and summative usability testing; theoretical foundations of HCI and cognitive modeling of user interactions; the integration of HCI techniques into the software development life cycle and the use of user constraints to generate new interaction designs. Course Objectives     Describe the general areas of study within the field of human-computer interaction Describe the interaction between people, the work they do, the information systems they use, and the environments in which they work Apply a user-oriented approach to the design of interactive computer systems Apply a user-oriented approach to the evaluation of interactive computer systems Persona: Sally Sally is 35 years old, works full time, and is pursuing a master’s degree in information sciences in order to advance her career. Her bachelor’s degree was obtained at a four-year college with traditional, in-person class attendance. Sally is proficient in using PCs and Macs, Microsoft Office software, workspecific software, and is eager to learn new things and develop new skills. Although Sally accesses Blackboard while at work when she has a spare moment or is on a lunch break, most of her Blackboard activity is conducted from home. At work, Sally uses a PC running Windows XP. Internet access is provided via a LAN. At home, Sally has both a PC and a Mac but prefers the Mac. For internet service, she subscribes to her local cable provider for basic service that has a download speed of 1.5 Mbps. She has a wireless router and connects to the internet using Google Chrome on both her PC and MAC. After experiencing connection difficulties with Blackboard due to an incompatible internet browser running on her Mac, Sally now accesses Blackboard with her PC. She estimates that she logs on one to three times a day, six days a week. The length of time she stays logged in depends on what she needs to log in for. Sometimes she downloads course materials, closes Blackboard, and carries on with her activities outside of Blackboard. She estimates that her lengthier Blackboard log-ins are associated with writing Discussion Board posts, varying from 10 to 30 minutes. Prior to enrolling in Drexel, Sally had never used Blackboard or any other e-learning medium. Sally completed Drexel’s iSchool Blackboard orientation, which introduced her to Blackboard. She found the orientation helpful but really needed to do an exploration of Blackboard on her own to really gain a comfort level with the program and its capabilities. Sally is now well into her second quarter at Drexel. The features she typically accesses during a quarter include Discussion Board, Group Workspace, My Grades, Wiki, Blogs, course material folders, and Digital Dropbox. She finds the features easy to use and has generally positive experiences with Blackboard, but she experienced some difficulties with submitting assignments through Digital Dropbox. Sally would like to see a more reliable Digital Dropbox and be able to access her Drexel webmail from within Blackboard. She’d also find it helpful if Blackboard could notify her when her professor has added content. Sally occasionally uses other tools for working with teams instead of those provided within Blackboard. She’s used Skype for collaboration and Dropbox for file sharing. Decisions to use these tools are made based on either negative experiences with Blackboard features or the personal request of other students working on her team. She also prefers to email her professor using her personal email interface instead of the email access provided by Blackboard. In summary, Sally considers herself to be fairly adept at navigating and using Blackboard after her first quarter at Drexel. She appreciates having 24-7 access to technical support, which she has used several times for Blackboard issues. All issues were successfully addressed. Scenario: Bob The following scenario describes how a student might access and use Blackboard for team collaboration. Bob has just been assigned a project and four teammates to work with for his Drexel information technology class. Bob’s team needs to have a few meetings to talk about their project approach, tasks, and schedule. Bob’s not sure how this is going to work because he and his teammates are spread out across the U.S. in different time zones. Bob’s also unsure of what form of communication to use because he doesn’t have the means to host or participate in a video or phone conference. While large corporations have these capabilities, Bob is a full time student and doesn’t have a job with an employer that could provide such things. Bob figures that since Drexel is allowing him to complete his entire study program through online learning, the university must provide him and his teammates with some kind of free collaboration tool. Bob turns on his computer and accesses the Drexel Blackboard to see what’s available. He navigates to Communication, Group Pages, and his team’s group page. He clicks on Collaboration and sees that there is a means by which to talk live online with his teammates. He experiments by selecting “Collaboration Session” and sets up a dummy meeting to see how it works. He sets a date and time two minutes from his Blackboard log in and selects “Chat” and “Submit.” He waits two minutes and accesses his session to see what comes up on the screen. He types in some dummy phrases and finds that if other users were logged into the session, they could also type in words or questions. Bob decides this will be an effective means by which to communicate in real time with his teammates. He exits Blackboard and opens his personal email account to send a message to his teammates about what he’s found. 58 Sample: Heuristic Evaluation This sample was prepared for Drexel INFO 608. Course description and goals are here. Heuristic Evaluation of the IPL Lina Bertinelli Tiffany Chow Jackie Ortanez Lisa Romanoski Heather Sherman Drexel University Author Note This paper has been prepared in accordance with the requirements of INFO 608, Final Report. REPORT: IPL HEURISTIC EVALUATION I certify that:  This paper/project/exam is entirely my own work.  I have not quoted the words of any other person from a printed source or a website without indicating what has been quoted and providing an appropriate citation.  I have not submitted this paper/project to satisfy the requirements of any other course. Signatures: Lina Bertinelli Tiffany Chow Jackie Ortanez Lisa Romanoski Heather Sherman Date: March 18, 2012 REPORT: IPL HEURISTIC EVALUATION Table of Contents Executive Summary ........................................................................................................................ 1 Introduction ..................................................................................................................................... 2 Digital libraries ............................................................................................................................... 2 The Internet Public Library............................................................................................................. 2 Human Computer Interaction ......................................................................................................... 3 Study Limitations ............................................................................................................................ 5 Summary and Prioritization of Test Results ................................................................................... 6 Recommendations for Design ....................................................................................................... 10 Conclusion .................................................................................................................................... 15 References ..................................................................................................................................... 17 List of Tables Table 1. Prioritization of Test Results ........................................................................................... 7 List of Figures Figure 1. Visibility and System Status ......................................................................................... 10 Figure 2. Match Between System and the Real World ................................................................ 11 Figure 3. Match Between System and the Real World, Example 2 ............................................. 11 Figure 4. User Control and Freedom. .......................................................................................... 12 Figure 5. Recognition Rather than Recall. ................................................................................... 13 Figure 6. Recognition Rather than Recall, Example 2................................................................. 13 Figure 7. Recovering from Errors ................................................................................................ 14 i REPORT: IPL HEURISTIC EVALUATION List of Appendices Appendix A: Team Interview Instrument .................................................................................... 19 Appendix B: Individual Interview Notes ..................................................................................... 22 Appendix C: Personas and Scenarios .......................................................................................... 35 Appendix D: Heuristic Evaluations ............................................................................................. 46 ii REPORT: IPL HEURISTIC EVALUATION Executive Summary The result of the merger between the Internet Public Library (IPL) and the Librarian’s Internet Index (LII), ipl2 is self-described as a “public service organization and learning/teaching environment” (The ipl2 Consortium, n.d.a). The website hosts several collections of reliable Internet resources and provides users with an online reference service run by volunteers and graduate students. This report serves to introduce the findings of a usability evaluation of ipl2. For this study, we interviewed four K-12 current or former educators and one K-12 student to represent ipl2’s intended audience. We gathered information through the interview to create personas and scenarios based on our interviewees and conducted a heuristic evaluation through the perspective of each user. By examining our evaluations, we found three areas that were both cited frequently and rated as a major or catastrophic problem: • Website features, especially search and navigation, did not correspond with user expectations, based on their experience with other information websites. • Website features, especially search and navigation, were found to be inflexible or inefficient. • Inadequate help features were provided, including a lack of a website tutorial or an extensive help page. In this report, we detail these problems and others further and provide recommendations based on Jakob Nielsen’s principles for user interface design and Donald Norman’s fundamentals for everyday design. 1 REPORT: IPL HEURISTIC EVALUATION Introduction Heuristic evaluations were conducted using personas and scenarios of anticipated users on the Internet Public Library 2 (ipl2) website to determine usability problems in March 2012. The purpose was formative and summative in that it gave information related to the worth or merit of what is being evaluated (Reeves et al, 2005, p. 14). Individuals from different states such as California, Florida, New Jersey, and South Carolina were interviewed to develop the personas and scenarios. This project was conducted by five graduate students in the iSchool at Drexel, College of Information Science and Technology, for Info 608, Human-Computer Interactions. Digital libraries Digital libraries first began to develop in the 1990s (Jeng, 2005, p. 47). In simple terms, Jeng explains that digital libraries are collections of information on a digital format, are available through networks (i.e. Internet), and at times may include service such as reference (p. 47). This project focuses on the ipl2, a digital library mainly geared towards K-12 affiliates (i.e. teachers, students, parents). Since digital libraries hold digital information, these affiliates may use it in order to search for reliable and valid information. The Internet Public Library The creation of IPL began in January 1995 in a graduate seminar at the School of Information and Library Studies at the University of Michigan 2012 (The ipl2 Consortium, n.d.b). It officially opened on March 17, 1995. The course instructor of the seminar, Dr. Joe Janes, wanted to create the IPL in order to allow individuals to ask questions related to libraries and librarianship. A section for children called “KidSpace” was also created to allow younger audiences to become familiar with the IPL. After 17 years, the IPL has been revamped several 2 REPORT: IPL HEURISTIC EVALUATION times and new sections like “TeenSpace” were added. In April 2009, IPL merged with the Librarian’s Internet Index (LII) (The ipl2 Consortium, n.d.b). Together, they created the ipl2 which allows individuals to find “Information You Can Trust.” Today, ipl2 allows patrons to search for their own information or ask an ipl2 librarian for help. Response time from an ipl2 librarian typically takes less than three business days. The ipl2 states that their mission is to provide “in-service learning and volunteer opportunities for library and information science students and professionals, offers a collaborative research forum, and supports and enhances library services” (The ipl2 Consortium, n.d.c). However, that is not to say that the ipl2 strives to take the place of a traditional in-person library. The ipl2 strives to “explore what the rich history and intellectual traditions of librarianship have to offer the dynamic but chaotic world of the Internet” (The ipl2 Consortium, n.d.d). IPL2 has been designed to cater to patrons of the digital world: it offers resources for kids and teenagers and on a plethora of subjects. Ipl2 has created its own original content such as “Special Collections Created by ipl2” but also allow patrons to search for reliable information from other Internet resources. Human Computer Interaction Human computer interaction (HCI) is the “study of how people use technological artifacts and their design” and the study of “how these artifacts can be designed to facilitate this use” (May, 2002, p. 7031). In order to fully understand ipl2’s capabilities, three steps were followed: • Five interviews were conducted with individuals with no ties to this particular course. • Personas and scenarios were created after reviewing interview results. • Heuristic evaluations were carried out based on interview scenarios to evaluate ipl2. 3 REPORT: IPL HEURISTIC EVALUATION As stated previously, five interviews were conducted with people outside of Info 608 who have involvement in K-12 education. Participants were recruited based on personal connections to the authors or from inquiries through a work or friendship-based network. Participants included a student in junior high school, a retired school librarian, teachers, and a retired teacher who now tutors at a community center. A persona and scenario was created for every person who was interviewed for this particular project. A persona is a description “of typical users of the product under development that the designers can focus on and design the product for” (Preece et. al, 2011, p. 481). It is because of this statement that individuals with some sort of affiliation to K-12 education were selected. A persona includes an individual’s “skills, attitudes, tasks, and environment” and each individual persona has different goals and aspirations (Preece et. al, 2011, p. 484). For example, one person who was interviewed wishes to “direct teachers/educators to teach resources in a specific subject area” while another interviewee has the goal of playing his guitar often. A scenario “describes human activities or tasks in a story that allows exploration and discussion of contexts, needs, and requirements” (Preece et. al, 2011, p. 505). These stories explain what the individual was trying to achieve. Scenarios are often unique just as personas are. For example, although educators were interviewed, they each used ipl2 for different reasons: • A retired educator used the site to search for information on United States presidents • A different educator performed searches on the solar system • A third educator searched Spanish materials she could use in her classroom • A high school librarian assists a student in finding information on Amerigo Vespucci • A high school student searches independently for foosball information 4 REPORT: IPL HEURISTIC EVALUATION 5 Together, a persona and scenario gives individuals an idea of who exactly the users are and what they do in order to fulfill their goals. Each persona and scenario that was created by our individual group members can be found at the end of this report. A heuristic evaluation attempts “to find the usability problems in the design so that they can be attended to as part of an iterative design process” (Nielsen, 2005). In order to conduct a heuristic evaluation, a small group of individuals test out the website to see if there is anything wrong with the heuristics. It is a “method for quick, cheap, and easy evaluation of the user interface” (Danino, 2001). Essentially, one will select evaluators who have experience with the site and those who do not have experience with the site. After browsing the site for some time, each user will assess the site based on the ten main principles (Nielsen, 2005): • Visibility of system status • Recognition rather than recall • Match between the system and the real world • Flexibility and ease of use • • Aesthetic and minimalist design User control and freedom • Helping users recognize, diagnose, and recover from errors • Help and documentation • Consistency and standards • Error prevention A summary of the findings will be further discussed in this report. Study Limitations As in any other study, limitations do exist. Questionnaires were used as a basis for interviewing typical users for the use in developing personas and scenarios. Reeves et al. (2005) explain that although questionnaires are a common evaluation tool, they tend to have limited utility in usability evaluations (p. 34). That is, our interview was able to find some of the problems with ipl2’s usability but did not give us a comprehensive list of every problem. Another limitation was due to time constraints: the user only used the incredibly large site for a REPORT: IPL HEURISTIC EVALUATION certain amount of time and then was asked about their opinions. With being exposed to the site for such little time, it was extremely difficult to evaluate every aspect of the site. Although ipl2 is directed more towards those in K-12, individuals not affiliated with this type of education may also use the site. Therefore, it may be helpful for future investigators to also get the opinion of those individuals. Although we were unable to find every problem, our team did evaluate heuristics that seemed to be common problems that were brought up by the interviewees. Our findings can be used to determine usability problems with those who are somehow affiliated with K-12 education. Summary and Prioritization of Test Results Heuristic evaluations of the Internet Public Library (ipl2) were completed utilizing the personas and scenario/tasks developed by each team member. The persona and scenario/task gives us a user’s perspective of the IPL whereby we can evaluate and assess usability issues/comments pertaining to IPL (Reeves et al., 2005, p. 33). The heuristic evaluation is based on ten usability heuristics and the degree and/or severity of the selected heuristic (Reeves et al., 2005, p. 33). The results have been compiled into an attached Excel spreadsheet (Table 1) which lists the test results by the most chosen heuristic number (in descending order) and severity (in ascending order). The most frequently chosen usability finding was heuristic #2, Match Between System and the Real World - with a highest severity of 4 (major). Most of the usability problems/comments were related to how effective the results are based on the type of search information being used. The common properties are search and navigation features. 6 REPORT: IPL HEURISTIC EVALUATION 7 The most frequent usability findings include heuristic #10, Help and Documentation ,which has a severity of 3 (major), and heuristic #7, Flexibility and Efficiency of Use, which has a severity of 4 (catastrophe). Problematic areas include “Search Help” and “Ask a Librarian.” Heuristics #1 and #9 were the least chosen with a severity of 2 and 3, respectively. Common findings pertain to the search engine. Opinions differed on heuristic severity, ranging from “no problem” to “catastrophe.” Evaluations for heuristic #6 were similar in that severity ratings were either 2 or 3. Based on the description of problems/comments from the heuristic evaluation, the most commonly identified issues of ipl2 include usability, reliability, availability, and functionality. Table 1. Prioritization of Test Results Description of Problem/Comments Heuristic Severity Number Evaluator IPL2 straight-forward and easy to use based on prior experience 2 0 Lisa Romanoski Error message does not provide instructions on how to correct the issue if not no text entered into search box and search executed. Should be clear for the kid audience. Error message text is confusing with its split into two sections. 2 3 Heather Sherman The IPL search engine can sometimes search for information which does not meet the criteria definition and/or purpose; thus user needs to come up with many searches. 2 3 Jackie Ortanez City searches not useful. 2 3 Jackie Ortanez Searching conventions may be unfamiliar to average user. 2 3 Lina Bertinelli Resources are not listed in a logical order 2 3 Lina Bertinelli No section for middle school students who are not “kids” or teenagers. 2 3 Tiffany Chow Resources for kids and teens are not organized in any particular order. 2 3 Tiffany Chow REPORT: IPL HEURISTIC EVALUATION Description of Problem/Comments 8 Heuristic Severity Number Evaluator No way to determine how search results are organized. 2 4 Tiffany Chow Difficulty navigating back to previous pages. 2 4 Tiffany Chow The help librarian and frequently asked questions were helpful for basic questions. 10 0 Jackie Ortanez “Search Help” link clearly visible under the search bar. 10 0 Lina Bertinelli User didn't need help; noticed "Search Help" and "Ask a Librarian." 10 0 Lisa Romanoski The organization of the IPL design appears to not flow well. 10 2 Jackie Ortanez There should be some type of interactive tutorial to train user; especially, since this is information that educators need to access. 10 3 Jackie Ortanez If search is not working well, maybe there should be some type of alert box to inform user to search different criteria. 10 3 Jackie Ortanez There is no link to help the user. That is, if a user is unfamiliar with the site, there is no “help” button. 10 3 Tiffany Chow User can typically find what he or she is looking for. 7 0 Lisa Romanoski Include clear button on search box so when the user clicks on the back browser button the search criteria has been removed. 7 2 Heather Sherman Search strings with multiple words will sometimes yield results with any and not all of those words. 7 3 Lina Bertinelli Resources are only easy to find on straightforward and popular topics. 7 3 Lina Bertinelli On the main search page, unable to specify to search special collections created by ipl2. 7 3 Tiffany Chow Difficulty navigating back to previous pages. 7 4 Tiffany Chow Pages do not load properly onto Internet Explorer or links do not work properly. 7 4 Tiffany Chow User aware of available search options such as the search box. 3 0 Lisa Romanoski There should be a separate help screen for search help? function. 3 1 Heather Sherman REPORT: IPL HEURISTIC EVALUATION Description of Problem/Comments 9 Heuristic Severity Number Evaluator The user has to click on the browser back button to return to previous screen instead of clicking a back arrow link. 3 2 Heather Sherman Upon choosing icons, for example - "For Kids", there is no user friendly button to go back to previous screen. 3 2 Jackie Ortanez User must return to the main page to switch to a different section. 3 2 Lina Bertinelli User must return to the main page to switch to a different section. 6 2 Lina Bertinelli IPL2 search box search drop-down should contain the same list as the home screen. 6 3 Heather Sherman User should be able to access accurate and efficient information from IPL. 6 3 Jackie Ortanez Left links in blue box and center page links confusing. 6 3 Lisa Romanoski 4 0 Lisa Romanoski When a user hovers over a graphic or minor category they should receive a visual cue in a different color. 4 1 Heather Sherman “For Teens” section does not look consistent with “Resources by Subject” and “For Kids” sections. 4 1 Lina Bertinelli Search results should have navigation buttons on both sides of the screen. The numeric listing should include a page navigator. 4 2 Heather Sherman Sub-category mouse click should be disabled since it just refreshes page. 5 0 Heather Sherman 5 2 Lisa Romanoski Search feature relies on searching conventions the average user may not be familiar with. 5 3 Lina Bertinelli The partners listed on the bottom of the website do not need to be listed on every single page. 8 1 Tiffany Chow Search result page displays same source multiple times, with different descriptions. 8 2 Lina Bertinelli Left links and center page links confusing. 8 3 Lisa Romanoski User understands system operations. 1 0 Lisa Romanoski If familiar, site operates similarly to Google. Search box may not yield desired results; no feedback. REPORT: IPL HEURISTIC EVALUATION Description of Problem/Comments 10 Heuristic Severity Number MySpace link to connect with ipl2 on main page is not viewable. User has to deduce certain judgments pending search box results. Search text reappears in search ipl2 box when user clicks on need help? Button. Evaluator 1 2 Tiffany Chow 9 1 Lisa Romanoski 9 3 Heather Sherman Recommendations for Design Our team has identified the following recommendations for ipl2: 1. Visibility of System Status When users are navigating and searching, the user is able to understand what the system is doing. One area that needs to be updated is the set of links for Facebook, Twitter, and MySpace. While the Facebook and Twitter links take the user to the respective websites, the MySpace link connects the user to a page not viewable by the public (Figure 1). This can confuse users because they don’t know what’s going with the website. Figure 1. Visibility and System Status: The MySpace link appears to be inoperable (ipl.org). 2. Match between System and the Real World When users visit ipl2, they may do so with the expectation that the website performs similarly to other websites with which they are familiar, such as Google or Bing. There are several instances where ipl2 could be improved to accommodate such user expectations: REPORT: IPL HEURISTIC EVALUATION • 11 Provide more robust website link results lists that go beyond limiting links to educational, encyclopedic, and government education sites. • Inform the user with an explanation of why a website link results list is limited to only tested, reliable websites. • Recognize user action and show factual information such as city data first and then a website link results list consisting of educational and governmental sites, as compared to only listing just the link results. • Tailor to specific age groups, perhaps by providing options listing ages as opposed to kids and teenager categories, for example (Figure 2). • Present information according to useranticipated conventions, such as alphabetical listing. • Figure 2. Match Between System and the Real World: Are there other options for youth who don't fall into "kids" or "teens" (ipl.org)? Present website link results lists in an organized manner instead of overwhelming users with hundreds of links. • Ensure results lists are in a logical order. Figure 3 shows an example of references for Teen Sports. The references appear to be listed randomly. • Provide a visible “back” button so that Figure 3. Match Between System and the Real World: There does not appear to be any logic behind the order of these references on the page. REPORT: IPL HEURISTIC EVALUATION 12 users don’t have to figure out how to navigate back to previous pages. 3. User Control and Freedom Ipl2 does a good job of providing a user with additional options for searching for information instead of just website exploration, such as the inclusion of the search box. However, ipl2 could be improved by providing a way return to previous screens, as mentioned Figure 4. User Control and Freedom: Ipl2 does not have a navigational aid for returning to previous screens (ipl.org). above. It’s not intuitive to the user how to navigate to other sections from a chosen section other than to return to the ipl2 home page (Figure 4). 4. Consistency and Standards There are several areas in which ipl2 can better adhere to user platform conventions: • Design search tools similarly to Google or Bing so that users aren’t confused as to why their ipl2 results look so different from search results lists generated by competitor sites. • Ensure consistency between font styles, color, underlining, and highlighting when a user’s mouse is moving across the page. • Re-design the teen and kid sections such that they present information the same way, including organization by headings and subheadings. • Ensure easy, consistent transitioning from one page to another within ipl2. 5. Error Prevention In regard to providing good error messages and preventing problems from occurring, ipl2 can inform users with actions they can take to produce better website link results lists if search REPORT: IPL HEURISTIC EVALUATION 13 box terms don’t yield what the user is looking for. Feedback can ease frustration and make for a more enjoyable user experience, ensuring repeat user visits to the site. 6. Recognition Rather than Recall In his book The Design of Everyday Things, Donald Norman shares with readers his findings that people learn better and are more comfortable when knowledge required to perform a task is available externally (2002, p. 189). When considering ipl2, the website can do a better job by making things more visible and easily discernible to users by providing: • Options to switch website sections instead of making a user figure out he or she must navigate back to the homepage. • All subject matter and special collection webpage links in the search box drop-down menu instead of making users rely on their memory of the ipl2 homepage (Figure 5). • Interactive tutorials for users not familiar with the site with the goal of better user experience. • Figure 5. Recognition Rather than Recall: Ipl2 could include all subjects and special collection links in its drop-down menu (ipl.org). Differentiation between the links in the blue box on the left of the screen and the blue-highlighted links in the page center (Figure 6). Figure 6. Recognition Rather than Recall: How are the blue box options different from the blue-highlighted text (ipl.org)? 7. Flexibility and Efficiency of Use According to Reeves et al. (2005), users “want to find the information they desire in the most effective and efficient manner possible” (p. 38). There are several areas in which ipl2 can be redesigned for greater efficiency, including provision of: REPORT: IPL HEURISTIC EVALUATION • 14 A “clear contents” button for the search box. If a user enters a search topic in the box and chooses to return to the previous screen, the search box retains the search text. The user has to click on ipl2 to clear the text (Figure 7). • A search capability that doesn’t list results with some Figure 7. Recovering from Errors: Entering Amerigo Vespucci as a search term did not yield results; the search box retains the search terms (ipl.org). or none of search word terminiology. • Clearly mapped resouces that go beyond listing popular topics. 8. Aesthetic and Minimalist design According to Norman (2002), aesthetics can either help or hinder usability of certain things (p. 79). There is a tradeoff between presenting information and also making it less visible if it’s not needed all at once (Norman, 2002, p. 79). In regard to ipl2, the following items could be redesigned to minimize information overload on the user: • Place the partner list on one webpage, not at the bottom of every single page. • Revise query results so that results don’t appear multiple times with different descriptions. • As metnioned previously, distinguish the purpose of the links in the blue box on the left from the blue high-lighted links in the page center (see Figure 5). 9. Help users Recognize, Diagnose, and Recover from Errors To help users recognize and recover from errors, ipl2 can: REPORT: IPL HEURISTIC EVALUATION • Provide a more effective search box tool with user feedback, such as a pop-up feature that can ask users if they’ve found what they’re looking for and offer suggestions. • Ensure the search box remains clear of text if user navigates back to the previous search page if they don’t find what they’re looking for (see Figure 6). 10. Help and Documentation Although the help librarian, frequently asked questions, and search help link tools are helpful for basic questions, the ipl2 help and documentation functions could be enhanced by: • As mentioned previously, providing feedback if the site detects the user’s search is not yielding useful results. • Also mentioned previously, providing interactive tutorials to educate users. Conclusion The ipl2 website is valued by its users as a source of reliable information, but there is room for improvement in making that information more accessible. All of our interviewees told us that they are familiar with search engines, and several commented that search engines were easier to use and retrieved more results than ipl2. Through our heuristic evaluations, we confirmed the difficulty of navigating ipl2, understanding its organization, using its search feature, and finding help tools. ipl2 will never be able to match the infinite results provided by Google, as each resource needs to be reviewed for accuracy, but they can fix their usability flaws. The recommendations we provided would not change the purpose of ipl2, but simply make the website more attractive, consistent, and easy to use. Our recommendations focus on the way ipl2 displays information, options, and feedback and maintains service integrity. 15 REPORT: IPL HEURISTIC EVALUATION Despite a few design weaknesses, the users of ipl2 recognize its worth. Each of our interviewees stated that they would recommend the website to other students or educators and remarked that the information found on the site was more trustworthy than the information found through search engines. With a few adjustments, we believe ipl2 can be a priceless resource of information users can not only trust, but easily find as well. 16 REPORT: IPL HEURISTIC EVALUATION References Danino, N. (2001, September 3). Heuristic evaluation: A step-by-step guide. Retrieved 03/16/2012 from: http://www.sitepoint.com/heuristic-evaluation-guide/. The ipl2 Consortium. (n.d.a) About ipl2. Retrieved 03/14/2012, from http://www.ipl.org/div/about. The ipl2 Consortium. (n.d.b) Timeline of ipl2 history. ipl2: Information You Can Trust. Retrieved 03/12/2012, from http://www.ipl2.org/div/about/timeline. The ipl2 Consortium. (n.d.c) The Mission and Vision Statements of ipl2. Retrieved 03/15/2012, from http://ipl2.org/div/about/mission_and_vision.html The ipl2 Consortium. (n.d.d) Frequently asked questions. ipl2: Information You Can Trust. Retrieved 03/12/2012, from http://www.ipl2.org/div/about/iplfaq.html. The ipl2 Consortium. (n.d.e) Statement of principles. ipl2: Information You Can Trust. Retrieved 03/12/2012, from http://www.ipl2.org/div/about/mission_and_vision.html. The ipl2 Consortium. (n.d.f). The ipl2 Consortium — Members and Membership Information. Retrieved 03/16/2012 from: http://www.ipl.org/div/about/IPLconsortium/consortiumList.html. The ipl2 Consortium. (n.d.g). Timeline of ipl2/IPL History. Retrieved 03/16/2012 from: http://www.ipl2.org/div/about/timeline. Jeng, J. (2005, June). What is Usability in the Context of the Digital Library and How Can it be Measured? Information Technology and Libraries, 24, (2), 47. May, J. (2002). Human-Computer Interaction. International Encyclopedia of the Social & Behavioral Sciences, Oxford, 2001, 7031-7035. Nielsen, J. (2005). Heuristic Evaluation. Retrieved from: http://www.useit.com/papers/heuristic 17 REPORT: IPL HEURISTIC EVALUATION Nielsen, J (2005). Ten Usability Heuristics. Retrieved from: http://www.useit.com/papers/heuristic/heuristic_list.html. Norman, D.A. 2002. The Design of Everyday Things. New York: Basic Books. Preece, J., Rogers, Y., & Sharp, H. (2011). Interaction Design. (3rd Ed.) New York, NY: Wiley. Reeves, T. C., Apedoe, X.,& Woo, Y. H. (2005, July). Evaluating Digital Libraries: A UserFriendly Guide. Retrieved from: http://drexel.blackboard.com/webapps/portal/frameset.jsp?tab_id=_2_1&url=%2fwebapp s%2fblackboard%2fexecute%2flauncher%3ftype%3dCourse%26id%3d_449400_1%26ur l%3d. 18 REPORT: IPL HEURISTIC EVALUATION Appendix A: Team Interview Instrument 19 REPORT: IPL HEURISTIC EVALUATION Interviewee: Interviewer: 1. Occupation? 2. Age? 3. Location? 4. How comfortable are you with computers? 5. Have you used the ipl2 website before? 6. How did you discover the website? . 7. What devices (computer, iPad, smart phone etc) have you used to access the site? 8. Did you receive any training on ipl2? 9. How much time do you spend (per week? per month?) on ipl2? 10. Have you used other digital library sites? 11. Have you used digital resources on public or school library websites (like databases, reference services, online catalog)? 12. How does ipl2 differ from those services? 13. Do you use search engines? 14. Which one(s)? 15. How does the ipl2 site differ from a search engine? 16. Is ipl2 more or less useful than a search engine? 17. Has the digital library simplified processes or has it made things more difficult? 18. What do you think is the primary use of ipl2? 19. What types of materials have you accessed from the site? (If you have never used it: What types of materials do you think you would access?) 20. How easy is ipl2 to navigate? 21. Do you think students would be able to navigate it? 22. Of what age group? 23. How long does it take you to find the information you need on the ipl2 site? 24. Have you contacted the help desk for assistance in using the site? 25. Have you used the Ask-a-Librarian feature? 26. Is the material organized for specific age groups appropriate for those groups? 27. Have you encouraged your students to use ipl2? 28. Do you think ipl2 could be a helpful classroom tool? How? 29. Would you recommend it to other students/educators? 20 REPORT: IPL HEURISTIC EVALUATION 30. What do you like about ipl2? 31. What don't you like about ipl2? 32. Have you had any problems using ipl2? 33. Can you suggest any improvements for the ipl2 site? 34. Why would you steer school children towards using IPL2 instead of running searches in search engines such as Google? 21 REPORT: IPL HEURISTIC EVALUATION Appendix B: Individual Interview Notes 22 REPORT: IPL HEURISTIC EVALUATION Interviewee: Robert Bertinelli Interviewer: Lina Bertinelli 1) Occupation? Retired special education teacher, tutor at community-center. 2) Age? 65 3) Location? Greenville, South Carolina 4) How comfortable are you with computers? On a scale of one to ten, five. Love using it once I know a program. But takes a while to learn them. 5) Have you used the ipl2 website before? Not before this interview. a) What devices (computer, ipad, smart phone etc) have you used to access the site? Acer laptop on Internet Explorer, then Mozilla Firefox. b) Did you receive any training on ipl2? No c) How much time do you spend (per week? per month?) on ipl2? 6) Have you used other digital library sites? No 7) Have you used digital resources on public or school library websites (like databases, reference services, online catalog)? Yeah a) How does ipl2 differ from those services? Liked the school library website better, access to catalog, access to databases. 8) Do you use search engines? Yes a) Which one(s)? Bing, Yahoo, Google b) How does the ipl2 site differ from a search engine? You get more information faster on a search engine, but ipl2 is probably more reliable. c) Is ipl2 more or less useful than a search engine? Less useful. 9) Has the digital library simplified processes or has it made things more difficult? Both. It’s easier because everything’s right there in one place, but it’s harder because I have to keep up with the technology. 10) What do you think is the primary use of ipl2? Research. 11) What types of materials have you accessed from the site? (If you have never used it: What types of materials do you think you would access?) Items for kids and teens. 12) How easy is ipl2 to navigate? Fairly easy. 13) Do you think students would be able to navigate it? Yes 23 REPORT: IPL HEURISTIC EVALUATION Bertinelli Interview a) Of what age group? Even elementary school students. I’d probably have to help the 1st and 2nd graders. 14) How long does it take you to find the information you need on the ipl2 site? Very fast. 15) Have you contacted the help desk for assistance in using the site? No -How quickly were you able to receive help? 16) Have you used the Ask-a-Librarian feature? No 17) Is the material organized for specific age groups appropriate for those groups? Yes 18) Have you encouraged your students to use ipl2? Not yet a) If not, would you? Yes, definitely 19) Do you think ipl2 could be a helpful classroom tool? Yes a) How? Mostly social studies tools, maybe science fair topics. They have a lot of good activities. 20) Would you recommend it to other students/educators? Yes 21) What do you like about ipl2? Very fast, really easy, got me right to where I wanted, lots of information. Colorful, bright, organized well. A lot of resources for kids. 22) What don't you like about ipl2? Technical issues, sometimes hard to navigate back to previous page. Story time: Wish it said how long it is. 23) Have you had any problems using ipl2? Yes a) Please describe. Pages not loading on Internet Explorer; links not working. 24) Can you suggest any improvements for the ipl2 site? I’d like more information directly on the site, instead of linking away. 24 REPORT: IPL HEURISTIC EVALUATION Interviewee: Lily Cruz Interviewer: Tiffany Chow 1) Occupation? Elementary school. Third grade gifted class from 2001-2009, first grade from 2009-present. 2) Age? 32 3) Location? Hacienda Heights, CA. Works in Los Angeles, CA. 4) How comfortable are you with computers? Is very comfortable using it for basic functions: Microsoft office, internet, I-tunes. 5) Have you used the ipl2 website before? No. a) How did you discover the website? Just found out about it right now. 6) What devices (computer, ipad, smart phone etc) have you used to access the site? Macbook pro a) Did you receive any training on ipl2? No b) How much time do you spend (per week? per month?) on ipl2? Just this one time, about 45 minutes. 7) Have you used other digital library sites? No 8) Have you used digital resources on public or school library websites (like databases, reference services, online catalog)? Yes. Uses digital resources on public library websites – but only for catalog services, used reference service once. a) How does ipl2 differ from those services? Able to actually search for information, it is not an actual library – holds information. Not all services have �ask a librarian’ feature. 9) Do you use search engines? Yes a) Which one(s)? Google, Yahoo b) How does the ipl2 site differ from a search engine? I think ipl2 is definitely more reliable because it doesn’t seem to take you to random sites that can be written by anyone—like blogs. The sites it directs you to are concrete. c) Is ipl2 more or less useful than a search engine? I can’t really say, I’m sure ipl2 is more useful in finding information but I think it took a lot longer for me to find the information I was looking for. I had to use specific key terms to find my information. 10) Has the digital library simplified processes or has it made things more difficult? I don’t think it’s difficult but I can see how it is difficult for teachers who are a lot older and who do not have much experience with computers. 25 REPORT: IPL HEURISTIC EVALUATION Chow Interview 11) What do you think is the primary use of ipl2? Research. I like that its kid-friendly since it has a section “For Kids” and “For Teens.” 12) What types of materials have you accessed from the site? (If you have never used it: What types of materials do you think you would access?) I used it to find some information about space and the distance between the moon and Earth for my solar system lecture. 13) How easy is ipl2 to navigate? It was fairly easy to navigate through the pages but it was a bit tricky finding the information. I kept using the search terms “distance between the moon and Earth” but got zero results. After about 20 minutes, I decided to try a different search term “solar system.” That’s when I started getting results. 14) Do you think students would be able to navigate it? Yes a) Of what age group? Probably kids in middle school and high school. 15) How long does it take you to find the information you need on the ipl2 site? Took me about 30 minutes to find what I was looking for. 16) Have you contacted the help desk for assistance in using the site? No 17) Have you used the Ask-a-Librarian feature? No 18) Is the material organized for specific age groups appropriate for those groups? I think so but under the “For Teens” area, there was a link to “Graphic Novels” and I didn’t like the sound of that even though it probably isn’t sexual. 19) Have you encouraged your students to use ipl2? Not yet. a) If not, would you? I would probably tell the parents about it. I teach first grade so they shouldn’t be using the Internet on their own. 20) Do you think ipl2 could be a helpful classroom tool? Yes a) How? It would show the students what types of materials online are appropriate in searching for information. Not everything found on Google is reliable but it seems like ipl2 has very reliable sources. 21) Would you recommend it to other students/educators? Yes 22) What do you like about ipl2? I like that the sources are reliable and that their motto is “information you can trust.” 23) What don't you like about ipl2? I don’t like that search terms need to be exact with their search terms to look for information. If I had typed in “distance from Earth to moon” on Google, I’m pretty sure hundreds of results would have come up. Since I didn’t use the correct search terms that ipl2 was looking for, I wasted a lot of my own time. 26 REPORT: IPL HEURISTIC EVALUATION Chow Interview 24) Have you had any problems using ipl2? No, I wouldn’t go so far as to say it’s a problem, it may just be my own fault. 25) Can you suggest any improvements for the ipl2 site? I know I have complained about this a lot already, but their search engine needs to be a lot broader. I feel like if you don’t use the correct search terms, then you’re out of luck. Even if it does have the information you’re looking for. I think they can improve on that somehow. 27 REPORT: IPL HEURISTIC EVALUATION Interviewee Name: Jack Liban Interviewed by: Jackie Ortanez 1. Occupation? Junior High Student 2. Age? 15 3. Geographical Location? Daly City, California 4. How comfortable are you with computers? Comfortable. Feels pretty good. 5. Have you used ipl2 website? If yes, how did you discover the website? 6. What is the primary use for the IPL user? Access “For Teens” site to get sports information for a high school class project. For example, foosball report. 7. How does ipl2 differ from other digital library sites? N/A 8. How usable is the site? Very good. It gives you the different categories of different sports that you can choose to give you information. For my foosball report, it gives you detailed information and objectives about the sport. 9. How easy is the site to navigate? Very user friendly. 10. Do you think students would be able to navigate it? Yes, with the proper knowledge of how to search on the site. 11. How interactive is it and how consistent is it? Yes, it interactive and you can go back to the information. 12. Have you used other digital library sites? If yes, please describe? No, this is the first one. 13. Have you used digital resources on public or school library websites (like databases, reference services)? Yes, to access listing of books for books reports. 14. How does the ipl2 site differ from a search engine providing web links? The difference is the type of subject matter and the amount of search information. The ipl2 site is more like an organized encyclopedia/dictionary and reliable and variety of information that you are searching for. 15. What do you like/don't like about the site? This site really has a good purpose for resource information for presentations. 16. Have you been able to get your questions answered? YES 17. What are the biggest changes you've seen from use of hard copy library card catalogs to digital catalogs? Easier to access still need to find more media files for reports for visual presentations such as Powerpoint presentations. 28 REPORT: IPL HEURISTIC EVALUATION Ortanez Interview 18. How long does it take you to find need information on ipl2 site? Fast. Probably less than a few minutes as long as you know what you have in mind. 19. What are the advantages and disadvantages of digital card catalog? Can they be designed better? For a first time user, unable to answer question at this time. 20. Give tasks to complete and rate how easy to use by feature. The feature are great for a first time user. Unable to rate but feel pretty good about it. 21. Have you used the contact librarian feature? No, but I have viewed into the feature for the first time. 22. Has the digital library simplified processes or has it made things more difficult? It has made the process much easier. 23. Can you suggest any improvements for usability on the IPL site? Not as first time user. 24. What devices (computer, iPad, smart phone etc) have you used to access the site? Laptops, iPad, desktop. 25. How useful is ipl2 site compared to a web search engine? Very useful because it gives you more reliable information because it goes directly to the source of the subject matter. 26. Is the material appropriate for the age groups? Yes, because the features allow you to select the age group. 27. How can ipl2 be used for class projects? Mainly for presentations, book reports. 28. What common mistakes would you expect students/people to make when using the site? Probably the subject matter does not relate to the purpose of the search. 29. Have you/would you want to encourage your students to use ipl2? N/A 30. Did you receive any training prior to utilizing ipl2? No 31. For tasks: find some ideas for science fair topics for elementary students? How easy was it to find? Very easy. 32. What types of materials have you accessed from the site? Sports, Sports Figures, Sports Trivia 33. Was there a time when you were not able to access the digital materials? Yes, when there was a minor glitch in the system. 34. Have you contacted the help desk for assistance in using the site? how quickly were you able to receive help? No. 35. How much time do you spend per week, per month on the IPL? When necessary, 3 times per week. 29 REPORT: IPL HEURISTIC EVALUATION Ortanez Interview 36. For what purpose do you/would use ipl? For learning. 37. Would you recommend it to other students/educators? Yes. 30 REPORT: IPL HEURISTIC EVALUATION Interviewee: Marsha Hahn Interviewer: Lisa Romanoski 1) Occupation? Retired school librarian. K-12 experience. Last 18 years as a high school media specialist. Currently adjunct reference librarian at Gloucester County College (NJ) and Rowan University 2) Age? 68 3) Location? Gloucester County NJ 4) How comfortable are you with computers? On a scale of 1-10 about 7-8 5) Have you used the ipl2 website before? Yes a) How did you discover the website? Used it when it was Librarian’s Internet Index. b) What devices (computer, ipad, smart phone etc) have you used to access the site? Computer c) Did you receive any training on ipl2? No d) How much time do you spend (per week? per month?) on ipl2? Maybe 20 minutes per month to check sites that I use on my LibGuide. Other times as needed. 6) Have you used other digital library sites? No 7) Have you used digital resources on public or school library websites (like databases, reference services, online catalog)? Yes a) How does ipl2 differ from those services? I use those (or refer patrons to them) for specific information. I find ipl2 to be a more complete resource. It would be somewhere that I would send a teacher/educator who is looking for teaching resources in a subject area. 8) Do you use search engines? Yes a) Which one(s)? Generally one of the Googles. b) How does the ipl2 site differ from a search engine? I put anything in Google and almost always get the response I am looking for. I use ipl2 when I know what I want but need more complete and authoritative results. c) Is ipl2 more or less useful than a search engine? It depends on what I want at the time. 9) Has the digital library simplified processes or has it made things more difficult? I see it as an additional resource, not one that simplifies or complicates. 10) What do you think is the primary use of ipl2? I see it as an excellent resource for educators and students ….. truly having a digital public library at their fingertips. 31 REPORT: IPL HEURISTIC EVALUATION Romanoski Interview 11) What types of materials have you accessed from the site? (If you have never used it: What types of materials do you think you would access?) I use it on my Children’s Literature LibGuide. 12) How easy is ipl2 to navigate? I find it very user-friendly. 13) Do you think students would be able to navigate it? Yes a) Of what age group? I would guess from age 10 and older. 14) How long does it take you to find the information you need on the ipl2 site? I have never timed my use. 15) Have you contacted the help desk for assistance in using the site? No 16) Have you used the Ask-a-Librarian feature? No 17) Is the material organized for specific age groups appropriate for those groups? I believe it is. 18) Have you encouraged your students to use ipl2? When I was in the high school setting, I encouraged them to use lii. Obviously, if I have it on my LibGuide, I am encouraging college students to use it. 19) Do you think ipl2 could be a helpful classroom tool? Yes a) How? Great resource for the students doing research. 20) Would you recommend it to other students/educators? Yes 21) What do you like about ipl2? Wealth of reliable and in-depth material for student use. 22) What don't you like about ipl2? Haven’t thought about that. 23) Have you had any problems using ipl2? No 24) Can you suggest any improvements for the ipl2 site? No 25) Why would you steer school children towards using IPL2 instead of running searches in search engines such as Google? I generally avoid sending students to Google when I know that I can send them to a more authoritative resource i.e. IPL2 or an online database, etc. Students tend to go to Google without my sending them there. Students, especially the younger ones, often have difficulty distinguishing reliable sources from ones that are less reliable. Also I think the kids IPL2 section is great, and I could see my 10 year old granddaughter using it. 32 REPORT: IPL HEURISTIC EVALUATION Interviewee: Danielle Palmer Interviewer: Heather Sherman 1) Occupation? 5th grade Language Arts teacher 2) Age? 34 3) Location? Ft. Lauderdale, FL 4) How comfortable are you with computers? Very comfortable. I use them daily in my classroom and for my own schoolwork 5) Have you used the ipl2 website before? No a) How did you discover the website? A friend sent it to me. b) What devices (computer, iPad, smart phone etc) have you used to access the site? A laptop and iPhone. c) Did you receive any training on ipl2? No d) How much time do you spend (per week? per month?) on ipl2? 1 hour/week 6) Have you used other digital library sites? Yes a) Please describe. I’ve used www.storyplace.org which is a website for elementary student, and the International Children’s digital library. b) Did you receive any training on these sites? No c) How does ipl2 differ from other digital library sites? It has a lot more information. d) Which do you prefer? Story place because it is much easier to navigate, particularly for students. 7) Have you used digital resources on public or school library websites (like databases, reference services, online catalog)? Yes a) How does ipl2 differ from those services? Ipl2 gives a lot more information and you can search by topic. 8) Do you use search engines? Yes a) Which one(s)? Google. b) How does the ipl2 site differ from a search engine? Google seems easier (just put in a search term and a LOT of information comes up). c) Is ipl2 more or less useful than a search engine? Less useful. 9) Has the digital library simplified processes or has it made things more difficult? More difficult if you’re asking about the search-ability aspect. 33 REPORT: IPL HEURISTIC EVALUATION Sherman Interview 10) What do you think is the primary use of ipl2? To get students to read and listen to books that are of interest to them. 11) What types of materials have you accessed from the site? (If you have never used it: What types of materials do you think you would access?) I would access the lesson plans page, and I would let my students get books to listen to and read, since it is important for students to both hear the reading and have a choice in what they read. I would also have them look at the homework help and writing references. 12) How easy is ipl2 to navigate? It is easy, particularly for students. However, the way the books are listed are a little confusing and there is too much listed. Students become easily distracted/confused and need bigger links or less links in order to find things. 13) Do you think students would be able to navigate it? Yes. a) Of what age group? 4th grade and higher 14) How long does it take you to find the information you need on the ipl2 site? Not that longabout two minutes. 15) Have you contacted the help desk for assistance in using the site? No. 16) Have you used the Ask-a-Librarian feature? No 17) Is the material organized for specific age groups appropriate for those groups? Yes 18) Have you encouraged your students to use ipl2? a) If not, would you? Most definitely. 19) Do you think ipl2 could be a helpful classroom tool? Yes a) How? My students love to use the computer and do research. The ipl2 would allow them to use the computer, read, and research all in one place. 20) Would you recommend it to other students/educators? Yes 21) What do you like about ipl2? Lots of resources available. 22) What don't you like about ipl2? Too much on the screen at times. 23) Have you had any problems using ipl2? No 24) Can you suggest any improvements for the ipl2 site? Use less links (particularly with the listing of books and have more color. Maybe have the students click on a picture of the title instead of the link. 34 REPORT: IPL HEURISTIC EVALUATION Appendix C: Personas and Scenarios 35 Persona Name: Robert Age: 65 Location: Greenville, SC Occupation: Tutor for afterschool program; Retired special education teacher Education: M.Ed in special education Robert recently moved to Greenville, South Carolina from Tucson, Arizona, where he worked as a special education teacher of 6th, 7th, and 8th graders. He now has a part-time position as a tutor for an after-school program at a community center in an underserved area. His duties include helping elementary-school students with homework and providing them with fun and educational activities. Though Robert doesn't feel completely confident in his computer skills, he loves what new technology has added to his teaching experience. He prefers the Elmo document camera to traditional projectors, has helped students navigate the internet, and has encouraged his students to use both digital and physical resources. Robert is not familiar with digital libraries, but has used online services from both school and public libraries. He feels comfortable using online catalogs and databases such as Ebscohost for research. Because Robert currently works for a community-center, rather than a school, he and his students do not have access to a school library. The public library is also not close enough to easily visit from the center. While there are several textbooks and encyclopedias available in the classroom, his most valued tools are the computers. Robert also loves music, and tries to incorporate his guitar into lessons whenever possible. Goals �� To find educational resources for elementary-school students �� To stay knowledgeable about a wide-range of subjects �� To play his guitar often 1 2 Scenario Robert is planning for his next afternoon at the community center. He knows that some of his 4th grade students are working on a report on United States presidents and wants to find some resources that will be easy for the nine year olds to use and understand. He has recently heard of the site ipl.org and wants to check it out using Internet Explorer. He is able to access the main page, but when he tries to view the resource pages, they look blank. Unsure of the problem, he decides to open in the site in Mozilla Firefox instead, and Robert is able to explore the "For Kids" section for materials. Since ipl2 has a sidebar of popular topics, he is able to find the US Presidents section easily. There he finds a chronological list of the presidents, which provides basic facts and links to more in-depth biographies, documents, pictures, and even audio files. Robert also tries looking through the History section to see if there are any additional resources on US Presidents, but only finds material on Abraham Lincoln. He is still happy with the resources he has found and decides to show his students the site in class the next day. While on ipl2, Robert notices the Resources for Parents & Teachers page. Since he loves music, he explores the Art & Music section and finds a great website with musical lesson plans and activities for children. There is often time for fun activities when the students finish their homework, so Robert decides to use one of the lesson plans to teach the children about musical instruments. Plus, he is excited for the excuse to bring his guitar and drums into the classroom. Overall, Robert is pleased that he was able to find a wide variety of resources on ipl2 and that he was able to plan for an entire afternoon on one website. PERSONA Background Information: Lily was born in Tegucigalpa, Nicaragua and grew up in Los Angeles, California. She attended California State University, Los Angeles from 1997-2001 where she received a scholarship to play on their volleyball team. As a student athlete, she also worked part-time at an elementary school as a teacher’s assistant. It was during this time that she decided to become a teacher. In 2001, Lily graduated summa cum laude with a degree in liberal studies. Name: Lily Chow Cruz Age: 32 Gender: Female Occupation: Elementary school teacher. Third grade gifted class from 2001 - 2009, first grade from 2009 – present. Devices: HP computers (School Use), Macbook Pro, iPad 2 (Personal use) Location: Hacienda Heights, California Goals: - To search for new information and new activities that will help foster her student’s intellectual needs - To be a role model to her daughters and her students - When not working, Lily is taking care of her two young daughters. She often takes them on walks at the park or takes them to Disneyland. She also spends a lot of time during the weekends to take her eldest daughter to softball practices. Lily also enjoys time to herself by working out at the gym whenever she can find a free baby-sitter (usually her sister). To be a great Mom while also being able to balance a career - After graduating from school and receiving her teaching credential, Lily was offered a full-time position as a teacher at the school she worked at as an undergraduate. She has been working with this school, Corona Avenue School, for over 10 years. To maintain a healthy life style by being able to work out on her own time As a teacher, Lily fosters a child’s intellectual development. She truly enjoys her job and is often on the Internet searching for new ways to inspire her young students. She also uses the Internet to search for information that she can add to her lesson plans. She has recently discovered the ipl2 website (http://www.ipl2.org) and hopes that she can use it to incorporate information with fun activities for her students. This will be the first digital library that she has worked with and hopes that it will be extremely helpful. Scenario – Searching for Information It is about the time of the year where Lily teaches her first grade class about the solar system. This year, she decides to add more information to her lesson plan so that the children will maybe appreciate science and space even more. Lily decides to use a new digital library website that she has heard about, ipl2. She logs onto the website and is welcomed with the website’s motto, “Information You Can Trust.” She sighs in relief because she knows she will be able to find reliable information. Lily decides to click on the “For Kids” link so that later on she can show her students the website. By having the children see there is a special location for them on the site, they may be more interested in using it. Lily wants to find the distance between Earth and the moon so she types in “distance between Earth and moon.” Eight results pop up but none of these contain the information she is searching for. She begins to wonder why this digital library does not contain the information she needs. However, she quickly decides to use different search terms. She types in “how far is the Earth from the moon.” She decides this may be a better search term because this may be the way a child searches for information when using the site. Still, the same eight results pop up. Finally, Lily decides to try the term “solar system.” Fifteen results are displayed and she is able to find her answer by clicking on the first website that is listed (NASA’s Solar System Exploration: Kids). Although she was unable to search for the information by using search terms a child would use, she is still happy with the results she found and is able to relay this information with her students during her solar system lecture. I certify that this paper/project is entirely my own work. I have not quoted the words of any other person from a printed source or a website without indicating what has been quoted and providing an appropriate citation. I have not submitted this assignment to satisfy the requirements of any other course. Tiffany Chow March 8, 2012. Digital Library ipl2 site By Jackie Ortanez Persona Name Age Gender Location Enhancing my knowledge as a student researching for materials in today’s digital world GOALS Jack Liban - 15 Male Daly City, California Occupation 9th Grade Student Computer Background iPad, Toshiba Laptop - - - To study and learn more about technology through research and utilizing & testing a variety of devices To research famous sports figures to get a better understanding of the evolving history of sports and how the game is played strategically. Also to view media files to get a better understanding of the sport persona. Able to access material in a way to be better able to help other classmates To continue to achieve higher grades through a well rounded education Background Information Jack is in 9th grade attending a high school in Daly City, California. Jack loves playing sports such as baseball, football, and basketball. He is in the baseball team for the Daly City Youth Baseball Organization. His love of sports through reading and research allows him to utilize technology through different channels such as websites. Jack’s favorite subjects in school are physical education, math, art and science. Jack utilizes the library system quite often to access materials for his class assignments. Jack lives close to the ocean and spends his weekends biking and enjoying the scenery. Jack would love to tie sports and technology utilizing a website of some sort such as a site to search for sports history, famous figures and trivia. He wants to create a site which would be both interesting and exciting to his viewers. Jack has found on-line search engines to help him with various creative ideas for building his site, but now he discovers reliable facts utilizing the digital library site. Scenario Jack has been assigned to complete a sports Powerpoint presentation on “foosball’. The requirements of his presentation includes visual aids and instructions on how to play the game. Also, how players interact with one another. On the ipl2 website, Jack uses the feature “For Teens” to research the foosball information. After Jack clicks on the search, he is given detailed information on a webpage of the sport “Foosball Source”. This site gives a comprehensive broad spectrum of information on this topic. Jack feels pretty good at researching information on the Ipl2 site. Jack finds this Ipl2 site to be very user friendly and fast. The ipl2 site reminds Jack of an organized encyclopedia/dictionary with very reliable information versus a search engine such as Google where it gives unlimited and vast information which does not meet his search purpose. As Jack selects “Learn about Foosball” which will access information on official rules, glossary of terms, build your own table, etc. It is a very comprehensive page with key points all relating to foosball. Since the subject matter was very straightforward, this made it very easy to search for this material on the ipl2 site. Unlike other subject matter which may not be very clear, this site might be difficult to find information. Jack was able to research the important information to help him on his sports presentation. The sports rules, glossary of terms and especially the sports foosball video added an enhancement to the Powerpoint presentation. Jack uses the site on an average of about 2-3 times per week. But for this reports, Jack spent about 5 times per week. As far as prior training, Jack had no Ipl2 training. It was very easy to navigate around with no major type of glitches. Jack would definitely recommend it to his classmates. Since Jack loves technology, he would like to assist in helping other students access and navigate through the site. Jack thought his class presentation was great! He did not receive his grade yet but he felt confident with the information he presented because of the reliable research from the ipl2 site. Background Information Marsha Hahn Name 68 Age Occupation School Librarian and Media Specialist, K-12 Education Location Adjunct Reference Librarian, Gloucester County College and Rowan University, NJ Bachelors of Science in Education Gloucester County, NJ Goals: • • Helping students find reliable, trust-worthy information for projects Directing teachers/educators to teaching resources in a specific subject areas Marsha Hahn is an adjunct reference librarian for Gloucester County College and Rowan University in Gloucester County, NJ, approximately 20 minutes southeast of Philadelphia. Marsha is also a life-long educator, working in K-12 schools and devoting the last 18 years of her life to assisting high school students as a media specialist. Marsha’s fairly comfortable working with computers. She spends approximately 20 minutes per month checking sites listed within Internet Public Library 2 (IPL2). She accesses the site from a computer at Gloucester County College, Rowan University, the high school in which she works, or her personal computer at home. She’s never experienced any problems using the site. Marsha’s decision to use either a search engine like Google or IPL2 depends on what she’s looking for. If she knows exactly what she wants, she uses IPL2 for more complete and authoritative results. When Marsha’s helping students conduct research, she typically directs them to IPL2 because she trusts the information provided through the site. She’s found that students, particularly younger students, have trouble distinguishing between reliable and unreliable sites. She finds the IPL2’s children website particularly useful in regard to the homework help section, access to encyclopedias, and book lists. Researching Amerigo Vespucci at the High School Library Marsha is working at her computer at the reference desk in her high school’s library one day when she is approached by a student. The student needs help looking for research information on Amerigo Vespucci for a history class paper. Marsha directs the student, Joe, to a student computer that accesses the library’s card catalog system and the internet. They sit down together at the computer, and Joe tells Marsha that he doesn’t know where to start in his research process. Marsha instructs Joe to type in the web address for the IPL2 website. At the search prompt on the IPL2 home page, Joe enters “Amerigo Vespucci” and clicks “Search IPL2.” Joe becomes discouraged when the search engine returns “no results found.” Marsha reassures him that there is information out there – they just need to think about and try different search strategies for finding it. Marsha directs Joe to the “Resources by Subject” box on the IPL2 home page. Joe navigates to History under Arts & Humanities. There are 998 resources available, and Joe is overwhelmed. Marsha suggests clicking on “History by Region” and then “North American History.” Joe navigates to “United States History.” He finds 493 resources. Marsha says this is MARSHA HAHN: REFERENCE LIBRARIAN one area he can explore for links to websites that might have useful information. She then suggests they try another area of the IPL2 website. When she instructs Joe to navigate back to the home page, he becomes flustered and asks how he can remember the web page they just left. He’s not sure he can remember how to go back to it. There’s no way to tag or mark locations on IPL2, so Marsha shows Joe how to create a bookmark of the page by using the internet browser’s tools. After reassuring Joe that he will be able to get back to the search page, Marsha directs Joe back to the IPL2 home page. She suggests he click on “For Kids.” Joe scoffs and asks her why she’d tell him to look there when he’s not a kid. Marsha says that just because it says “For Kids” doesn’t mean it won’t have valuable information that he can use. She instructs Joe to navigate to the “History” link under the “Our World” heading on the page. Joe starts to scroll down the page and sees a link for “Zoom Explorers.” He gets excited and clicks on the link and starts to explore the web page. Marsha waits patiently for a minute or two and decides he’s on his way to understanding how to search for information. She tells him she’s going to let me work a little while on his own and return to the reference desk. Joe gets nervous at being left alone, but Marsha reassures him that she’s just a few steps away if he has questions. She directs his attention back to the search tools and leaves him to explore on his own once she sees he’s become engrossed in the web page again. PERSONA Digital Libraries Ipl2 C r e a t e d b y: Heather Sherman “To get students to read and listen to books that is of interest to them” - GOALS Ability to locate reference materials for her elementary aged students - Ability to access library materials from her laptop and iPhone, and school-issued iPads - Ability to assign electronic reading materials to her students for their weekly assignments - Ability to search by topic and/or keyword - Ability to offer student homework assistance - Ability to access information in both English and Spanish Name Danielle Sherman Age 34 Gender Female Location Fort Lauderdale, Florida Occupation 5th Grade Language Arts Teacher Education PhD candidate at Florida Atlantic University Devices Toshiba Laptop, iPhone 4S Background Information Danielle has worked in a charter school, teaching elementary-aged students and has provided individual tutoring. She was recruited to this position from Ohio six years ago. The Florida teaching position required a teacher who could write and read in both Spanish and English. As education technology has evolved, blackboards with chalk have become interactive Smartboards. Research assignments are now conducted online and textbooks are available both in print and on e-readers. Danielle and her fellow teachers are searching for digital library websites where students can receive writing assistance and conduct research assignments in an environment that contains materials appropriate for elementary aged students. Danielle was among the first users of the iPhone. She relishes any opportunity to incorporate new technologies into her classroom. Her students are now using the iPad for the reading assignments. Danielle has been using Storyplace and International Children’s digital libraries. Scenario Digital Libraries Danielle has started creating her lesson plans for the next school year. First she opens her previous year’s approved lesson plans on her laptop. Danielle skims over lesson plans and creates a list of areas that she needs to research. She then takes this list and researches them so that the current lesson plans are engaging and based on the English/Language Arts Common Core Standards. Danielle has to submit all her lesson plans to her assistant principal to review to ensure they meet the state and charter school requirements. Frequently, Danielle will search the internet for updated information to enhance her lesson plans. Once a week, she and the other Language Arts teacher will plan lessons together. Her charter school has implemented a conservative firewall to block any websites that contain inappropriate words or content. However, if need be, Danielle can get sites unblocked. After browsing the lesson plan links, Danielle searches for Spanish materials. As an avid Google search engine user, Danielle is used to searching websites by typing in a key word or sentence. Danielle types in Spanish Reading Materials into the search window and clicks Search ipl2. Her results are only focused on the words resource and materials. The subject matter green text has been replaced by URLs. Once again, Danielle attempts to locate Spanish reading materials. This time Danielle only enters Spanish. At last, Danielle has discovered Spanish reading materials websites with information that she can incorporate into her lesson plans. One of Danielle’s colleagues has recommended a new digital library site call ipl.org. She will have the students use this site during center time on their iPads so they can improve their reading comprehension and fluency through digital books. Danielle visits the ipl site to find sample lesson plans and Spanish reading materials. On the main page Danielle clicks on the For Kids button. She scans the web page and locates the resources for parents and teacher link. Danielle clicks on several of the resources in the Kids--Teachers and Parents corner. Next she selects the Lesson Plan link from the left hand blue vertical bar. Until Danielle started clicking on the links she was not sure of the differences between the left hand blue menu and the detail listing on the center white section. I Certify that: This paper is entirely my own work. I have not quoted the words of any other person from a printed source or a website without indicating what has been quoted and providing an appropriate citation. I have not submitted this entry to satisfy the requirements of any other course. Heather Sherman March 7, 2012 REPORT: IPL HEURISTIC EVALUATION Appendix D: Heuristic Evaluations 46 REPORT: IPL HEURISTIC EVALUATION Bertinelli Evaluation Description of Problem 47 Heuristic Number Search result page displays same source multiple times, with different descriptions. 8 Search strings with multiple words will sometimes yield results with any and not all of those words. 7 Search feature relies on searching conventions the average user may not be familiar with. 2,5 “Search Help” link clearly visible under the search bar. 10 “For Teens” section does not look consistent with “Resources by Subject” and “For Kids” sections (not organized by header, subheadings). 4 User must return to the main page to switch to a different section. 3,6 Resources are not listed in a logical order 2 Resources are only easy to find on straightforward and popular topics. 7 Severity 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe REPORT: IPL HEURISTIC EVALUATION Chow Evaluation Description of Problem 48 Heuristic Number Main page: after typing in search terms, user is only able to search all of ipl2, for kids, for teens, or newspapers & magazines. Unable to specify to search special collections created by ipl2 even though it is one of the main icons on the main page. 7 Main page: there are ways to connect with ipl2 (i.e. facebook, twitter), but Myspace link leads to a missing page. 1 Middle school students who are not yet teenagers may click on “For Kids” and feel as though it is catered more to students younger than they are. Middle school students may feel unable to find a place on the ipl2 website that caters to them. 2 There is no link to help the user. That is, if a user is unfamiliar with the site, there is no “help” button. 10 When searching, there is no way to determine how the results are organized – only a list of preferences is provided. When searching for “solar system” 500 links are provided ; unsure which is best. 2 The “For Kids” or “For Teens” the sections provided are not organized in any way, it seems. One would think that it would be listed alphabetically but it just seems as though it is all just listed randomly. 2 Difficulty navigating back to previous pages. 2,7 Pages do not load properly onto Internet Explorer or links do not work properly. 7 The partners listed on the bottom of the website do not need to be listed on every single page. 8 Severity 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe REPORT: IPL HEURISTIC EVALUATION Ortanez Evaluation Description of Problem The IPL search engine can sometimes search for information which does meet the criteria definition and/or purpose. User may have to come up with different searches. Depending on the search criteria, the IPL does not come up with vast links like Google or Bing, it comes up with links from education sites, encyclopedia sites, government education sites, etc. In other words, it narrows or limits your search to reliable sites if search is worded in such a way in order to meet the user's purpose. Upon choosing icons, for example - "For Kids", there is no user friendly button to go back to previous screen unless you select the back arrow at the top of the screen or after hover over the top left IPL picture which does not indicate. Only after you hover all the pictures. When typing a city name, the search selections come up with more educational, governmental sites than the city information first before any links come up with the city. Searching dictionary first than city will provide information on the city itself. And for some smaller cities, the IPL only provided one link which may indicate not so useful. A user should be able to access accurate and efficient information from IPL. It should give reliable information since this is going to be used for educating students. The IPL is fast, but how effective will the information be if the user is not trained appropriately. There should be some type of interactive tutorial. When user clicks onto the links after selecting one of the 5 main icons on the home page, it is a bit confusing when searching for information the user has already in mind. Design sometimes appears that it does not an easy flow. 49 Heuristic Number 2 3 2 6 and 10 10 The help librarian and frequently asked questions were helpful for basic questions. 10 If search is not working well, maybe there should be some type of alert box to inform user to search different criteria. 10 Severity 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe REPORT: IPL HEURISTIC EVALUATION Romanoski Evaluation Description of Problem/Comments 50 Heuristic Number The user has no problem understanding what the system is doing when navigating and searching for Spanish materials. 1 The user finds IPL2 straight-forward and easy to use based on prior experience using something like Google. 2 The user may not find what she needs the first time navigating the site, but there are other available options for searching for information, such as the search box. 3 The user would find the site operates similarly to a search engine like Google if that user is familiar with that type of search engine. 4 If the user doesn't find what she's looking for while navigating, she can try typing a phrase into the search box. Depending on the results list, it may not have the desire results. There was no feedback from the search tool to tell the user that no results matched the search box input. When first navigating to the "Teachers" and "Parents" corner, the user might not understand the difference between the links on the left in the blue box and the blue-highlighted links in the center of the page. While the user can learn that she can click on them to retrieve information, the differences aren't obvious. The user can typically find what he or she is looking for after trying several different search methods, such as clicking on links or using the search box tool. 5 6 7 Severity 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe REPORT: IPL HEURISTIC EVALUATION Sherman Evaluation Description of Problem 51 Heuristic Number User types in Search ipl2 and the result screen does not include navigation to previous screen. The user has to click on the browser back button to return to previous screen. (Appendix A) 3 Search ipl2 box does not have clear button. When user clicks on back browser to return to previous screen search ipl2 box still contains text. User has to click in ipl2 box to clear text. (Appendix B) 7 Mouse is enabled when user hovers over the current page sub-category listing. When user clicks on subcategory to current page refreshes. (Appendix B) 5 On ipl2 search results user has to move mouse to left side of screen or hit back button to return to previous screen. Results contain a numerical listing instead of number of pages. (Appendix C) 4 Ipl2 search box search drop-down does not contain list to resource by subject or special collections. User has to recall these options from the home page and click on the home page to use them. (Appendix D) 6 When mouse is hovering over major category search link font changes color from orange to blue and is underlined. When mouse is hovering over minor categories color changes from one shade of blue to another and is underlined. When move is hovering over graphic no color shading or underlying. (Appendix E) User does not enter text into search ipl2 and clicks search. Error message does not provide instructions on how to correct the issue. Message should be clear for the kid audience. Error message text is confusing with its split into two sections. (Appendix F) In error message box user receive text need help? versus search help? and both link to the same screen. (Appendix F & G) User enters Amerigo Vespucci term into search ipl box, receives no results found message, clicks on back browser, removes text from search box, clicks on search 4 2 Severity 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor 3 major 4 catastrophe 0 no problem 1 cosmetic 2 minor REPORT: IPL HEURISTIC EVALUATION Sherman Evaluation Description of Problem ipl2, clicks on need help? and Amerigo Vespucci text reappears into search box. Text is being held in memory without a clear button. (Appendix F & G) 52 Heuristic Number Severity 3 major 4 catastrophe 115 Sample: Term Paper - EMI in Wireless Networks in Hospitals This sample , the term project, was prepared for Drexel INFO 614, Distributed Computing and Networks. Details for this course are as follows: Description This course provides an overview framework for the student to become familiar with computer network technologies and transport protocols from a systems engineering viewpoint. Topics include networking planning, design principles, network protocols, internetworking, and distributed computing topics. Course Objectives      Layered computer communications models and frameworks The types of computer networks available and how they interoperate Basic knowledge of network protocols with emphasis on Internet related protocols Routing, Bridging, and network address concepts Network security and Internet application based technologies Term Project The term project was intended for an in-depth study of an applied distributed computing problem or network technology. Topic choice was to be an appropriate applied networking problem or technology (some suggestions are listed below). It must have been applied to a specific real-world problem where possible. For the content, the problem and requirements were to be stated clearly, practical and complete designs to address the problem were to be described, and choices were to be justified and explained. The work was to be convincing such that it demonstrated tackling a real problem and have a real solution. EMI IN HOSPITAL SETTINGS 1 Electromagnetic Interference (EMI) in Wireless Networks in Hospitals By Lisa Romanoski Drexel University Author Note This paper has been prepared in accordance with the requirements of INFO 614. EMI IN HOSPITAL SETTINGS 2 Certification I certify that:  This paper is entirely my own work.  I have not quoted the words of any other person from a printed source or a website without indicating what has been quoted and providing an appropriate citation.  I have not submitted this paper/project to satisfy the requirements of any other course. Signature: Lisa Romanoski Date: June 7, 2012 EMI IN HOSPITAL SETTINGS 3 Introduction Wireless local area networks (WLANS) are widely used in e-Health applications (e.g. electronic medical records (EMRs), clinician notifier, etc.) to improve healthcare mobility and service flexibility (Phunchongharn et al., 2010, p. 1247; Wang & Du, 2005, p. 335). However, design of wireless communications for e-Health applications must consider electromagnetic interference (EMI), which can affect EMI-sensitive medical devices and cause automatic shutdown/restart, waveform distortion, and howling. These EMI effects, in turn, can have serious, negative impacts on patient safety for those patients who rely on medical devices (Phunchongharn et al., 2010, p. 1247; Wang & Du, 2005, p. 335) The goal of this paper is to develop an understanding of what causes EMI and discuss solutions to overcome EMI issues in WLANs. This paper does not address a full-scale, site-specific setup of a WLAN in a hospital or security measures needed to comply with federal and state regulations pertaining to patient data. What is EMI and Why is it an Issue? Electromagnetic (EM) radiation is comprised of alternating waves of electric and magnetic fields, and is produced by such things as television, radio, cellular, and other broadcasting equipment (PDAmd.com, 2010). EMI is a naturally occurring phenomena that results when the electromagnetic field of one device disrupts, impedes or degrades the electromagnetic field of another device by coming into proximity with it (Webopedia.com, 2012). Electronic devices are susceptible to EMI because electromagnetic fields are a byproduct of passing electricity through a wire (Webopedia.com, 2012). According to Williams (1995), “the exposure, frequency, location, orientation, and design of a device all influence whether it will experience EMI.” Furthermore, Witters (2009) notes that “the strength of the EM field at EMI IN HOSPITAL SETTINGS any given distance from the source of the radiated signal (transmitter) is directly proportional to the radiated power of the transmitter and inversely proportional to the distance.” Incidents of EMI with medical equipment has been an issue since approximately 1979, at which time the Food and Drug Administration (FDA) began to receive reports of suspected incidents, including but not limited to (Williams, 1995):  Pacemaker failure during an ambulance ride while the two-way radio was in use.  Pulse rate and oxygen level display on a pulse oximeter machine attached to a dead body, occurring when a telemetry receiver that was part of the system was placed too close to the body.  Instead of identifying a baby’s heartbeat, a fetal heartbeat detector played local radio and CB broadcasts.  Interference with electric wheelchair circuits, including an instance where a man in a powered wheelchair, several miles from a radio tower and three blocks from a busy road where mobile radios were likely in use, was seriously injured when his chair rode off a cliff at high speed. Incidents such as these led the FDA to produce strict shielding requirements for medical equipment. Shielding can be applied to electrostatic discharge, EMI, radio frequency interference (RFI), and microwave absorption (Sealscience.com, 2012):  Electrostatic discharge (ESD) shielding: the process of limiting electric current that flows when an excess of electric charge, stored on an electrically insulated object, finds a path to an object at a different electrical potential (such as ground) by separating them with a barrier made of a lightly conductive material. Static dissipative materials have electrical resistance between insulative and conductive materials. There can be electron flow across or through the dissipative material, but it is controlled by the surface resistance or volume resistance of the material. 4 EMI IN HOSPITAL SETTINGS Typical materials for ESD shielding in the semiconductor and medical device industries include carbon-filled silicone and polyurethane blends that shield highly sensitive electronic circuitry.  Electromagnetic interference (EMI) shielding: the process of blocking the induction of electromagnetic radiation, which is emitted by electrical circuits carrying rapidly changing signals, as a by-product of their normal operation to other circuits which causes unwanted signals (interference or noise). This is achieved by separating the circuits with a barrier made of conductive material.  Radio frequency interference (RFI) shielding: the process blocking radiofrequency electromagnetic radiation from one circuit to another by separating them with a barrier made of conductive material. This is achieved by separating the circuits with a barrier made of conductive material. Typical solutions for EMI/RFI shielding in the aerospace and medical device industries include gaskets and custom molded seals made from highly conductive elastomers that bridge uneven seams in electronic packaging. Anything other than a 100% metal to metal contact can provide gaps that allow interference to degrade systematic performance.  Microwave absorption: the process of absorbing microwave/radar energy at discrete and broadband frequencies by converting the microwave/radar energy into heat. This is achieved by magnetizing an elastomeric material by filling it with a magnetic alloy such as carbonyl iron or ferrite. Microwave absorbing materials/ radar absorbing materials (RAM) are frequently used in the military industry for radar cross-section (RCS) 5 EMI IN HOSPITAL SETTINGS 6 reduction. Seals designed from microwave absorbing elastomers are effective in reducing both EMI and RCS. According to Witters (2009), the key to addressing EMI is the recognition that it involves not only the device itself but also the environment in which it is used, and anything that may come into that environment. More than anything else, the concern with EMI must be viewed as a systems problem requiring a systems approach. In this case the solution requires the involvement of the device industry, the EM source industry (e.g., power industry, telecommunications industry), and the clinical user and patient. The public must also play a part in the overall approach to recognizing and dealing with EMI (Witters, 2009). The next section describes regulatory oversight of medical devices. Regulating Agencies In the U.S., the Federal Communications Commission (FCC) and the Food and Drug Administration (FDA) influence medical device regulation (Fish & Richardson, 2012, p. 2)1. A short discussion of these agencies is included here because their regulations influence safety and EMI outcomes in hospitals. Both FCC certification and FDA authorization are required prior to medical device marketing in the U.S. (Fish & Richardson, 2012, p. 2). Every medical device that uses radio technology falls within the FCC’s authority to manage the electromagnetic spectrum. Under FCC rules, wireless devices must be tested for technical standards conformance and authorized before they may be imported, marketed or operated in the U.S. (p.3). The FCC standards specify permissible frequencies, power levels, duty cycle, band sharing and frequency stability requirements, along with detailed test procedures for measuring these parameters (p. 5). 1 The Centers for Medicare and Medicaid Services (CMS) are also influential in regard to medical devices, but only in terms of payment and marketability (Fish & Richardson, 2012, p. 7). As such, CMS is not discussed in this paper. EMI IN HOSPITAL SETTINGS 7 The FDA regulates the marketing of all medical devices sold or imported in the U.S. (Fish & Richardson, 2012, p. 5). Unlike the FCC which focuses on the interference potential of radio frequency devices, the FDA’s role is to ensure that such devices are safe and effective for patient use (p. 5). The range of products that are classified and regulated as “medical devices” is broad and can include medical information networks, cell phones programmed to remind users to take pills, and conventional devices fitted with radio communication features (p. 5). The next section describes medical devices in greater detail and includes frequency operating ranges. Medical Devices As the purpose of this paper is to look at network solutions for overcoming EMI in hospitals, it may be prudent to develop an understanding of what sort of devices can cause or be influenced by EMI, beginning with medical devices. Medical devices may be implanted or worn on the body and serve the purpose of controlling bodily functions and/or measuring physiological parameters (Fish & Richardson, 2012, p. 1). According to Fish & Richardson (2012), p. 1):  Implanted devices can control heart rhythms, monitor hypertension, provide functional electrical stimulation of nerves, operate as glaucoma sensors and monitor bladder and cranial pressure, and  External devices monitor vital signs, assist the movement of artificial limbs and function as miniature “base stations” for the collection and transmission of various physiological parameters. The days of patients being tethered to one spot are gone (Fish & Richardson, 2012, p. 1). Device design has evolved dramatically since the occurrence of the previously mentioned EMI incidents involving medical devices (Fish & Richardson, 2012, p. 1). Wireless medical devices EMI IN HOSPITAL SETTINGS 8 can communicate with nearby receivers connected to landline networks, cellular systems, or broadband facilities that access the Internet (p. 1). The benefits of this are far-reaching, including a more comfortable environment for the patient, the creation of a safer workplace for medical professionals, the ability to remotely monitor patients on a real time basis, and the ability to provide preventative and managed care (p. 1-2). Generally, wireless medical devices fall into one of two informal FCC categories: short or long range (Fish & Richardson, 2012, p. 4). Short range technologies transmit data from the patient to a local receiver or monitor, which may stand alone or connect to a central monitoring station. Long range technologies generally transmit patient data directly to a remote monitoring location (p. 4). Figure 1 shows the Industrial, Scientific, and Medical Bands in which certain devices may operate. Frequency data is presented here because managers of WLAN operations, particularly those that use radio signals, need to be cognizant of the various devices in use and ensure that they operate in way such that they can co-exist in the same area with each other with minimal interference with each other (Harte, 2004). 802.11 WLAN radio systems that use radio channels operate in the unlicensed frequency bands, which can be used by anyone or any product provided the transmission conforms to transmission characteristics (frequency, power, and channel control) defined by the appropriate regulatory agency, such as Figure 7. ISM Bands (Encyclopedia2. hefreedictionary.com, 2012). EMI IN HOSPITAL SETTINGS 9 those defined by the FCC for medical devices (Harte, 2004). 802.11 WLAN systems may operate in 2.4 GHz or 5.7 GHz, , shown in Figure 1 (Harte, 2004). The 2.4 GHz band has 83.5 MHz of bandwidth, and the 5.7 GHz band is actually divided into three 100 MHz frequency bands. Additional frequency data for current medical telemetry is provided in Table 1. Additional short range technologies for patient monitoring are included in Table 2. Table 3. Current Medical Telemetry Band (Fish & Richardson, 2012, p. A17) Standard Frequency Date Rate Range Description Inductive Coupling Devices < 1 MHz 1-30 kpbs <1m Wireless Medical Telemetry (WMTS) 608-614 MHz Medical Device Radiocommunication Service (formerly “MICS”) > 250 kbps 30-60 m Communicates data from body sensors to 1395-1400 MHz remote monitoring 1427-1429.5 MHz locations 401-406 MHz 250 kbps 802.11 a Wi-Fi 5 GHz 54 Mbps 802.11 b Wi-Fi 2.4 GHz 11 Mbps 802.11 g Wi-Fi 2.4 GHz 54 Mbps 802.11 n Wi-Fi 2.4/5 GHz 248 Mbps 2.4 GHz 3 Mbps 100 m 868, 915 MHz, 2.4 GHz 40 kbps 250 kbps 75 m 2.5 GHz 70 Mbps (fixed) 802.15.1 Bluetooth Class I 802.15.4 (Zigbee) World Interoperability for Microwave Access Used to control or monitor cardio activity 2-10 m Allocated in 1999 for licensed communication between body implants and a nearby controller, the FCC added more frequencies to this service in 2009 for use by body-worn monitoring devices 120 m Used with cell phones, hand held devices and 140 m personal computers, 140 m but can also be used for implanted or body250 m worn medical devices Several Provides wireless km transmission using a EMI IN HOSPITAL SETTINGS Standard 10 Frequency Date Rate (WiMAX) Range Description 40 Mbps (mobile) variety of transmission modes, from point-tomultipoint links to portable and fully mobile Internet access. The technology provides up to 70 Mbps broadband at distances over several kilometers. Table 4. Short Range Patient Monitoring Technologies (Fish & Richardson, 2012, p. 4) Technology Operational and Frequency Details Description Ultra-Wideband Very low power in almost any Used in medical telemetry and region of the spectrum at imaging applications. distances up to a few feet Medical Micropower Networks 413-457 MHz band at distances up to a few feet. Implanted microstimulator devices that might lead to the creation of an artificial nervous system that could restore mobility to paralyzed limbs. Medical Body Area Networks 2360-2400 MHz band at distances up to a few feet A wireless personal area network (“PAN”) of multiple body sensors to monitor or control patient functions Electromagnetic Compatibility Standard As mentioned in the previous section, there are numerous standards that apply to wireless medical devices. Of particular note are IEC 60601-1 and 61000-4, which address electromagnetic compatibility (EMC) (Phunchongharn et al., 2010, p.1248). EMC is the opposite of EMI: it means that the device is compatible with (i.e., no interference caused by) its EM EMI IN HOSPITAL SETTINGS 11 environment, and it does not emit levels of EM energy that cause EMI in other devices in the vicinity (Witters, 2009). IEC 60601-1 specifies general requirements for medical equipment safety, while IEC 61000-4 recommends EMC testing and measurement techniques (Phunchongharn et al., 2010, p. 1248). IEC 60601-1-2 defines the immunity standard level, which is the maximum EM disturbance level in which the device can operate without performance degradation, and the compliance level, or the EM disturbance level, which is below or equal to the immunity level (p. 1248). IEC 60601-1-2 specifies that non-life-supporting devices should be able to tolerate the EM field of at least 3 V/m, while life-supporting devices should be able to tolerate the maximum EM field of 3 V/m caused by RF transmission under 80-800 MHz and 10 V/m caused by RF transmission from 800 MHz to 2.5 GHz (Phunchongharn et al., 2010, p. 1248). Non-lifesupporting medical devices include things such as blood pressure monitors and infusion pumps, whereas life-supporting devices include things such as defibrillators (Phunchongharn et al., 2010, p. 1248). To reduce EM fields to those passive medical devices, the wireless transmitter should decrease the transmit power or increase the separation distance between itself and the medical device (Phunchongharn et al., 2010, p. 1248). Other EMI Sources As shown previously in Figure 1, ISM Bands, WLANs are not the only radio devices operating in the unlicensed frequency band (Harte, 2004). Some non-communication electronic devices can leak radio signals in the unlicensed band such as microwave ovens, computers, and mobile telephones. These devices cause interference in a variety of ways, either temporarily (e.g. microwave oven) or continuously (wireless video security camera) (Harte, 2004). EMI IN HOSPITAL SETTINGS 12 Other sources known to cause interference issues include (Dyrda & Khairy, 2008, p. 824; Harte, 2004) :  High-voltage lines  Security systems  Radio and television towers  Intercom systems  Transformers  Cordless telephones  Residential power generators  Cell phones Cell phones do emit EMI and can cause interference with medical devices (IEEE, 2008, p. 38). Usage policies tend to vary by hospital (Fontaine, 2004). A solution to the potential interference problem is to use a distributed in-building cellular repeater or distributed antenna system (DAS) (Fontaine, 2004). According to Laura Fontaine, a spectrum expert, “most cell phones have power control where the transmit power adjusts depending upon the strength of the signal received from the base station. Signal propagation through the building walls tends to weaken the base station signal, causing the cell phone to operate at higher power since it thinks the base station is farther away. A DAS effectively brings the cellular base station signal inside the building and better distributes it. By using a DAS, the phones will typically operate at a lower power, thus reducing the EMI potential” (2004). With EMI sources identified, subsequent sections explore how some of these sources function within a hospital environment. WLAN systems and their operations are discussed, followed by a review of an EMI-aware access scheme. WLAN System As mentioned previously, WLANs are becoming more commonplace in hospitals that use various e-Health applications (Phunchongharn et al., 2010, p. 1247; Wang & Du, 2005, p. 335). WLANs provide wireless network communication over short distances using radio or infrared EMI IN HOSPITAL SETTINGS signals instead of traditional network cabling (http://bmisigcseit.wikispaces.com, 2012). This section explores the setup of a WLAN that uses radio signals and accommodates e-Health applications, beginning with a description of components followed by a discussion on operations and access. WLAN systems are typically composed of the following devices (Harte, 2004): Inventory system:  Gathers information about all electronic medical devices in the hospital (Phunchongharn et al., 2010, p. 1247; Airtightnetworks.com, 2012):  On/off status  Location  Signal-to-interference-plus-noise ratio (SINR) thresholds Stations:  Access Points  Are radio access transceivers (combined transmitter and receiver)  Are considered base stations and connect wireless data devices to a LAN system  Convert and control the sending of data packets to other devices or networks  Perform data transfer functions including bridging (linking networks), retransmitting (repeating), distributing (hubs), directing packets (switching or routing), or adapt formats for other types of networks (gateways)   Can be mounted on walls, ceilings, and to other objects  Have a wired Ethernet data connector (8 pin RJ-45) and a power supply input Clients:  Wireless data devices that include wireless network interface card (NIC) adapters and integrated radio modules (laptops, personal digital assistants (PDAs), IP phones and other smartphones, or fixed devices such as desktops and workstations  May be considered as either low- or high-priority in terms of access  Communicate with the RAC over wireless links  Access one channel at a time by way of a single, dual-channel radio transceiver  Transmit/receive data through the RAC by adaptively tuning the transmit power 13 EMI IN HOSPITAL SETTINGS  14 Are associated, or registered, with a WLAN system (i.e., a specific access point) to allow information transmission/receipt A radio access controller (RAC):  Connected to the inventory system with wired infrastructure  Equipped with two radio transceivers, one for common channel control and another for data, which can be accessed concurrently  Controls and manages the frequency system using inventory system information  Defines safe transmission parameters for avoiding harmful EMI  Performs channel allocation and controls wireless access Interconnection network:  The connection of access nodes through wire or radio redistribution Servers:  Provide resources to other computers and devices on a network  Include network access control (such as RADIUS), network management, and policy (bandwidth control) servers WLAN Operations WLANs operate by coordinating radio channel access and data packet transmissions between wireless access devices (Harte, 2004). Address and control information allows data packets to reach their destination (Harte, 2004). Packets may be sent directly between units (independent mode) or they may travel through a backbone network (distributed mode) (Harte, 2004). Association of devices with APs keeps track of where devices are operating and the addresses assigned to reach them (Harte, 2004). Addressing Addressing in a WLAN system consists of addresses of devices that are part of the WLAN system (Harte, 2004). These are called medium access control (MAC) addresses. Each EMI IN HOSPITAL SETTINGS device in the WLAN system including stations, APs, and routers has its own unique 48 bit medium access control (MAC) address (also known as a link address) (Harte, 2004). Each data packet that is transmitted in the wireless LAN contains multiple MAC addresses, including the source address (SA), destination address (DA), transmitter address (TA), and receiver address (RA) (Harte, 2004). During the installation process for most wireless networks, the network name or Service Set Identity (SSID) and a channel number needs to be entered for an AP (Harte, 2004, Kurose and Ross, 2010, p. 539). The SSID is a 32-character unique identifier attached to the header of packets sent over a WLAN can differentiate one WLAN from another (Harte, 2004). All APs that are part of a specific WLAN must use the same SSID (Harte, 2004). A device cannot join a WLAN unless it can provide the unique SSID assigned to that system (Harte, 2004). Association Association allows users to move seamlessly (roaming) from one AP coverage area to another with no loss in connectivity (Harte, 2004). When a WLAN station first senses an access point, it associates with the AP, or creates a virtual wire between itself and the AP (Harte, 2004; Kurose and Ross, 2010, p. 539). When a station leaves an AP or wants to transfer to a new AP because the signal quality is better, it disassociates with the AP, releasing resources and allowing the system to hold or reroute packets to the new AP that the station associates with next (Harte, 2004). Quality of Service As mentioned previously, WLANs are based on the IEEE 802.11 standard. Most current implementations use the Distributed Coordination Function (DCF) at the Medium Access Control (MAC) layer (Soomro and Cavalcanti, 2007, p. 117). DCF is a random access 15 EMI IN HOSPITAL SETTINGS mechanism in which a wireless station senses the channel before transmitting a packet and, in the case of overlapping transmissions, retries transmissions after randomly selected backoff periods (p. 117). Since DCF doesn’t support quality of service (QoS), an 802.11e extension to 802.11 was developed to provide different service levels for applications with different throughput and delay requirements (p. 117). Two mechanisms of QoS support are defined, including Enhanced Distributed Channel Access (EDCA) and Hybrid coordination function Controlled Channel Access (HCCA). In EDCA, four access categories (voice, video, best-effort, and background traffic) contend for a channel in a distributed manner with different probabilities or priorities of access (Soomro and Cavalcanti, 2007, p. 117). The access priorities are determined by setting different MAC layer parameters for each category (p. 118). In HCCA, QoS is provide in a centralized manner by a hybrid coordinator (HC), co-located with an AP and determines flow admittance based on application requirements (p. 118). The difference between the two mechanisms is that HCCA guarantees QoS whereas EDCA provides differentiation in a probabilistic manner (p. 118). The next section discusses access in greater detail. The access scheme is based on the 802.11 e standard (Phunchongharn et al., 2010, p. 1248). Access For an e-Health application situation, access could work in the following manner according to a scheme presented by Phunchongharn et al. (2010): 1. Connection: Devices can connect to the RAC in the common control channel by using a time-slotted RTS-CTS-based channel access mechanism (Phunchongharn et al., 2010, p. 1248). RTS and CTS, Request to Send (RTS) and Clear to Send (CTS) are control frames 16 EMI IN HOSPITAL SETTINGS that are used to avoid collisions and the hidden terminal problem, caused by an obstruction that prevents devices from sensing one another’s transmissions (Harte, 2004; Kurose and Ross, 2010, p. 545). 2. Carrier Sensing: Prior to data transmission, devices can perform carrier sensing to avoid collisions, which is based on the contentionbased operation DCF, mentioned previously. With carrier sense multiple access with collision avoidance (CSMA/CD), stations sense the channel during a Distributed Inter-frame Space (DFIS) before transmitting and “backs off” (refrains) from transmitting when the channel is busy (Phunchongharn et al., 2010, p. 1248; Kurose and Ross, 2010, p. 541). 3. Common Control Broadcasting: Each device has a maximum transmit power, P, for transmitting either RTS or CTS that takes into account EMI (Phunchongharn et al., 2010, p. 1249) 2. Since status and locations are dynamic, the RAC computes and broadcasts the transmit power as changes occur (p. 1250). Each user waits until a channel is sensed idle before transmitting an RTS message or data packet (p. 1250). If the RAC needs to increase the transmit power, it can broadcast a new message with information after a short interframe space (SIFS) (p. 1248). Since SIFS is shorter than DIFS, all devices can detect the broadcasting and stop their transmissions so that devices can synchronize to the RAC, which can always capture the change in a hospital environment (p. 1250). 4. Uplink Requests: After common control channel broadcasting, a user can transmit its requests by using an EMI-aware RTS-CTS protocol on the control channel (Phunchongharn et al., 2010, p. 1250). A device first transmits an RTS message to the RAC by using P (p. 1250). If a high-priority device suffers a collision, it will wait for a random time 2 The reader is referred to Phunchongharn et al. (2010) for the transmit power formula. 17 EMI IN HOSPITAL SETTINGS based on an exponential backoff window (p. 1250). Information about the user type is included in the request message. Once the RTS message is received by the RAC, it calculates the upper bound of transmit power for the user on the data channel in the same way as P (p. 1250). If the RAC cannot find a feasible transmit power which meets the EMI constraints on the device and satisfies the minimum QoS requirements of the device, the data transmission request is dropped and a negative CTS message is transmitted to the device/user (p. 1251). Otherwise, the RAC will transmit a CTS message with the maximum allowable transmit power (p. 1248). The device/user can adaptively tune its transmit power on the data channel accordingly. Once the CTS message is successfully received by the user, the user will transmit an acknowledge (ACK) message to the RAC within the same time slot, which is composed of the CTS transmission period and the ACK transmission period (p. 1250). If the RAC does not receive the ACK message at the end of the time slot, it will repeat the CTS transmission using automatic repeat request (ARQ) protocol in the next time slot (p. 1251). 5. Downlink Requests: For downlink requests, the RAC retrieves device/user location and calculates the feasible transmit power to avoid EMI (Phunchongharn et al., 2010, p. 1248). If feasible transmit power is not determined, the transmission request is dropped with probabilities Pd1EMI and Pd2EMI for high- and low-priority users, respectively3 (p. 1251). To avoid congestion, the downlink transmission request can also be dropped with probabilities Pd1cong and Pd2cong, respectively. 3 The reader is referred to Phunchongharn et al. (2010) for the probability equations. 18 EMI IN HOSPITAL SETTINGS If the transmit request is granted, the RAC will transmit an RTS message along with the feasible transmit power on the control channel to the user after an SIFS to avoid collision with RTS messages from other users (p. 1251). Upon receiving the RTS message, the device/user will respond with a CTS message after an SFIS period (p. 1251). In the same time slot of the CTS transmission, the RAC will immediately transmit an ACK message to the user. An ARQ mechanism is also used to recover from erroneous transmissions (p. 1251). In practice, RTS and CTS transmission lengths are small, approximately 18 ms each, while the duration of data transmissions of high-priority and low-priority devices/users are several hundred milliseconds (e.g., 250 ms for high-priority and 810 ms for lowpriority) (p. 1251). As such, the overhead caused by the RTS/CTS protocol is negligible. 6. Prioritized Queue Management and Data Transmission: Upon receiving the CTS message for uplink transmission or RTS message for downlink transmission, the device/user will switch its radio from the control to the data channel (Phunchongharn et al., 2010, p. 1251). The user will wait in the data channel until the RAC transmits a message to allow the user to transmit/receive data when the channel is available (p. 1251). The duration of a time slot is assumed to be fixed during which one packet can be transmitted. The time slot is composed of the data transmission period and the ACK transmission period (p. 1251). Two finite-length queues at the RAC are used to store transmission requests (p. 1251). If they are full, the RAC will transmit a negative CTS message to the user (p. 1251). The user will wait and retransmit the request (p. 1251). High-priority users are always allowed to 19 EMI IN HOSPITAL SETTINGS 20 transmit if there is any request in the transmission queue (p. 1251). Low-priority users have to wait in the queue until the high-priority queue is empty (p. 1251). System Analysis The previously discussed access scheme was developed by Phunchongharn et al. (2010), who presented a rather sophisticated model that was tested with several simulations in MATLAB. Attempting to reproduce it is beyond the scope of this paper, but a discussion on methods and results is included herein. Phunchongharn et al. (2010) analyzed their proposed system with a queuing analysis and development of a discrete-time queuing model (p. 1251). For queuing, the authors assume two servers (one for the control channel and a second for the data channel), two orbits, and two buffers (for high- and low-priority users) (p. 1251). A scenario is considered in which an RTS request arrives at the server in the control channel with arrival probabilities for high- and lowpriority users (p. 1252). When a collision occurs, users go to the orbits and will try retransmitting with respective probabilities (p. 1252). The authors next use a Discrete-time Markov Chain Model to that is used to model the queuing behavior. Markov-chains are certain discrete space stochastic processes in which it is assumed that the future evolution of a process is dependent only on the state of the process at time n, and is independent of the past evolution of the process (Zukerman, 2000, p. 67). According to Zukerman (2000), the “amenability” of the model makes it attractive for use in various types of analyses, including modeling of queuing and telecommunications networks and systems (p. 67). Transitions from one state to another in the model are assumed by Phunchongharn et al. (2010) to be a collision, a successful RTS at the RAC on the control EMI IN HOSPITAL SETTINGS 21 channel, a CTS transmission from the RAC on the control channel, and a user finishing its transmission on the data channel (p. 1252). Next, the authors derive two performance metrics: the average transmission delay of high-priority users ̅ ) and the loss probability of low-priority users ( ). The readers is referred to Phunchongharn et al. (2010) for the equations (p. 1252-3; 1256-8). The authors then develop an optimization scheme for the blocking probabilities Pd1 and Pd2 by using performance measures from the queuing analysis. The goal is to select optimal blocking probabilities that allow for maximum system throughput while concurrently satisfying QoS requirements (p. 1253). System parameters used in the two-stage optimization include those shown in Table 3. Table 5. System Parameters for an EMI-Aware Wireless Access Scheme (Phunchongharn et al., 2010, p. 1253) Parameter Description Arrival priorities of high- and low-priority users, respectively Backoff window sizes Maximum backoff stage for low-priority users Probability of user finishing a transmission; pertains to variable size of medical files for e-Health applications Total number of high- and low-priority users The optimization scheme developed by the authors is listed in Table 4. Table 6. Two-stage Optimization (Phunchongharn et al., 2010, p. 1253) Minimize (1) ̅ Subject to ) ) (2) Minimize (3) ) Subject to ) and ) ) (4) are the QoS requirements for e-Health applications in terms of the average transmission delay of high-priority users and the loss probability of low-priority users EMI IN HOSPITAL SETTINGS (Phunchongharn et al., 2010, p. 1253). In the first stage, an optimal Pd1 is selected to maximize the throughput of high-priority users while the average transmission delay of the users is satisfied in equations 1 and 2 in Table 4. In the second stage, an optimal Pd2 is selected to maximize the throughput of low-priority users while maintaining the loss probability of low-priority users as shown in equation 4 in Table 4. The optimal Pd1 obtained in the first stage is used to compute the loss probability of low-priority users as shown in equation 4 in Table 4. Scenario In their performance evaluation, Phunchongharn et al. (2010) considered clinician notifier and EMR e-Health applications (p. 1253). A clinician notifier application is used by staff to retrieve real-time physiological signals of patients when an alarm occurs (p. 1253). EMR applications are used by staff to add, retrieve, and update medical data (p. 1253). In the authors’ scenario, they considered one life-supporting device (a defibrillator), four non-life-supporting devices (two electrocardiogram (ECG) monitors and two blood pressure monitors), one active medical receiver, and five active medical transmitters (p. 1253). It is assumed that the five active medical transmitters transmit ECG signals to the active medical receiver in a round-robin manner (p. 1253). Various assumptions were developed as to number of times operated and duration of operation. For example, it was assumed that the clinician notifier applications were run 40 times an hour and used to retrieve real-time ECG signals of patients. The sampling rate for clinician notifier was 250 Hz with 8-bit resolution (p. 1254). For the EMR, data size ranges were assumed to range from 10 to100 kB, and access was assumed to occur 60 times in an hour (p. 1254). 22 EMI IN HOSPITAL SETTINGS 23 Results To assess their evaluation, Phunchongharn et al. (2010) considered the performance measures of interference probability and outage probability (p. 1254). The interference probability is the probability of causing EMI to medical devices when the transmit power is higher than an acceptable level (p. 1254). The outage probability is the probability that the receive signal strength at the RAC is less than -94 dBm (p. 1254). Model results reveal that the authors’ proposed protocol does not cause EMI, whereas the traditional CSMA/CA protocol does (Phunchongharn et al., 2010, p. 1254). Additional findings include (p. 1254-5):  Higher transmit power is likely to result in greater probability for interference.  Outage probability was found to be greater due to transmit power limits.  Transmission duration of high-priority users decreases as the average transmission delay of high-priority users ̅ decreases .  Average transmission duration of low-priority users was found to have no influence on high-priority user performance.  Chance for collisions was found to increase with an increase in the number of users.  Average transmission delay ̅ and number of high-priority users in the queue decreases when blocking probability Pd1 increases .  Loss probability of low-priority users ( ) decreases as increases (p. 1255). Conclusion WLAN systems provide the opportunity to improve mobility and service flexibility in healthcare services by making real-time data available to busy clinicians operating in a fast- EMI IN HOSPITAL SETTINGS paced, dynamic setting (Phunchongharn et al., 2010, p. 1247; Wang & Du, 2005, p. 335; Soomro & Cavalcanti, 2007, p. 114). While the advantages of “anytime, anywhere” health information access are clear, EMI continues to be problematic in regard to numerous devices operating in environments such as hospitals. As mentioned previously, the key to addressing EMI is the recognition that it involves not only the device itself but also the environment in which it is used, and anything that may come into that environment (Witters, 2009). More than anything else, the concern with EMI must be viewed as a systems problem requiring a systems approach (Witters, 2009, Wang & Du, 2005, p. 347; Bruns & Dimantha, 2006, p. 42). This paper looked at a QoS provisioning approach that takes into account power transmission in order to minimize EMI affects to sensitive medical equipment. Authors Phunchongharn et al. (2010) successfully demonstrated that such provisioning is possible depending on the WLAN access scheme. While each healthcare setting is different, the approach present herein provides a tool network managers can apply in concert with Witters’ systems approach to minimize EMI. 24 EMI IN HOSPITAL SETTINGS 25 References Ahmed, M. H, Yanikomeroglu, H., & Mahmoud, S. (2006, February). Interference Management Using Basestation Coordination in Broadband Wireless Access Networks. Wireless Communications and Mobile Computing, 6(1), 95 – 103. Airtightnetworks.com. (2012). PCI DSS Compliance FAQs. Retrieved from: http://www.airtightnetworks.com/home/solutions/industry-solutions/retail/pci-dss-andwireless-faqs.html Benkert, M., Gudmundsson, J., Haverkort, H., & Wolff, A. (2008). Constructing MinimumInterference Networks. Computational Geometry: Theory and Applications, 40(3), 179 – 194. Bmisigcseit.wikispaces.com. (2012). Difference Between LAN's, WLAN's and WAN's; Identifying Their Main Characteristics. Retrieved from: http://bmisigcseit.wikispaces.com/difference+between+LAN's,+WLAN's+and+WAN's,+i dentifying+their+main+characteristics Bruns, B. & Dimantha, S. (2006, November/December). Evaluating EMI in a Multi-Hospital Facility. Biomedical Instrumentation & Technology, 40(6), 40-42. Calinescu, Gruia, Tongngam, & Sutep. (2011). Interference-aware Broadcast Scheduling in Wireless Networks. Ad Hoc Networks (1570-8705), 9(7), 1069 – 1082. Cisco.com. (2012). Chapter 7 – Controlling Lightweight Access Points. Retrieved from: http://www.cisco.com/en/US/docs/wireless/controller/5.2/configuration/guide/c52lwap.ht ml Cisco.com. (2012). Cisco Clean Air Technology. Retrieved from: http://www.cisco.com/en/US/netsol/ns1070/index.html EMI IN HOSPITAL SETTINGS David, Y., Paperman, W. D., & Storch, J. (1997, August). Nuts and Volts: Searching for ways to Zap EMI Effects. Health Facilities Management, 10(8), 60-64. Encyclopedia2.thefreedictionary.com. (2012). ISM Band. Retrieved from: http://encyclopedia2.thefreedictionary.com/industrial,+scientific+and+medical+band Feng, G., Liew, S. C., & Fan, P. (2008). Minimizing Interferences in Wireless Ad Hoc Networks Through Topology Control. IEEE International Conference on Communications, 2332 – 2336. Fish & Richardson. (2012). Wireless Medical Devices: Navigating Government Regulation in the New Digital Age. Retrieved from: http://www.fr.com/wireless-medical-devices/ Fontaine, L. (2004, April). Wireless Planning in the Health Care Environment. Retrieved from: http://www.24x7mag.com/issues/articles/2004-04_02.asp Garza, V. R. (2011, September 29). Mobile Device Management for Small Business. Retrieved from: http://www.pcworld.com/businesscenter/article/240768/mobile_device_management_for _small_business.html Geier, J. (2002, November 26). 802.11 Medium Access Methods. Retrieved from: http://www.wi-fiplanet.com/tutorials/article.php/1548381 Geier, J. (2003, May 27). Defining Access Point Range Boundaries. Retrieved from: http://www.wi-fiplanet.com/tutorials/article.php/2212591 Hariharan, D. (2009, May). EMI Shielding for Medical Devices. Medical Design News, 9(4), 18. Harte, Lawrence (2004). Introduction to 802.11 Wireless LAN (WLAN). Fuquay Varina, NC: Althos Publishing. 26 EMI IN HOSPITAL SETTINGS Huang, C. (2009, April). Interference Management for Wireless Networks. Electrical Engineering, 109. IEEE. (2008). IEEE Std 11073-00101: Health informatics—PoC Medical Device Communication, Part 00101: Guide—Guidelines for the use of RF Wireless Technology. New York, NY: IEEE. Jensen, P. A. (2004). Discrete Time Markov Chains. Retrieved from: http://www.me.utexas.edu/~jensen/ORMM/models/unit/markchain/index.html Katia, D., & Khairy, P. (2008, July). Implantable Rhythm Devices and Electromagnetic Interference: Myth or Reality? Expert Reviews, Cardiovascular Therapy, 6(6) 823 – 832. Kazemitabar, A. & Seyed, J. (2008, December). Coping with Interference in Wireless Networks. 148. Kurose, J. F. & Ross, K. W. (2010). Computer Networking, 5th Ed. New York, NY: AddisonWesley. Lee, H., Chung, S., Fragouli, C., Mao, Z. (2010, November). Network Coding for Wireless Networks. Journal of Wireless Communications and Networking, 2010(1), 359475. Li, H., Wu, C., Hua, Q., & Lau, F. (2011, December). Latency-minimizing Data Aggregation in Wireless Sensor Networks under Physical Interference Model. Ad Hoc Networks. Mangold, S., Choi, S., Hiertz, G. R., Klein, O. & Walk, B. (2003, December). Analysis of IEEE 802.11E for QoS Support in Wireless LANs. IEEE Wireless Communications, 10(6), 4050. Marcus, M. L., & Biersach, B. R. (2003, December). Regulatory Requirements for Medical Equipment. IEEE Instrumentation & Measurement Magazine, 6(4), 23-29. 27 EMI IN HOSPITAL SETTINGS McNamee, M. (2011, March 9). Wireless Network Design with Proper RF Planning. Retrieved from: http://www.securedgenetworks.com/secure-edge-networksblog/?Tag=Wireless%20LAN%20Site%20Survey Microsoft.com. (2012). Configuring Wireless Network Clients. Retrieved from: http://www.microsoft.com/resources/documentation/windows/xp/all/proddocs/enus/wlan_client_configuring_concept.mspx?mfr=true Mierya, F., and Silva, F. (2010). Mobile Phones Electromagnetic Interference in Medical Environments: A Review. IEEE International Symposium on Electromagnetic Compatibility, 311-316 Morrissey, J. J. (2004, July). Mobile Phones in the Hospital: Improved Mobile Communication and Mitigation of EMI Concerns can Lead to an Overall Benefit to Healthcare. Health Physics, 87(1), 82-88. NI.com. (2012). Spectral Monitoring and Signal Intelligence. Retrieved from: http://www.ni.com/white-paper/8788/en PDAmd.com. (2012). Wireless Devices and Electromagnetic Interference in Hospitals, Urban Myth? Retrieved from: http://www.pdamd.com/features/interference.xml Phunchongharn, P, Niyato, D., Hossain, E., & Camorlinga, S. (2010, September). An EMIAware Prioritized Wireless Access Scheme for e-Health Applications in Hospital Environments. IEEE Transactions on Information Technology in Biomedicine, 14(5), 1247 – 1258. Posey, B. M. (2012, August 26). Server Hardware Explained (Part 1). Retrieved from: http://www.windowsnetworking.com/articles_tutorials/Server-Hardware-ExplainedPart1.html 28 EMI IN HOSPITAL SETTINGS Scansource.edu. (2012). Radio Frequency Site Survey. Retrieved from: http://www.scansource.eu/en/radio-frequency-site-survey-214.htm Sealscience.com. (2012). EMI/ RFI/ ESD Shielding. Retrieved from: http://www.sealscience.com/Conductive_Rubber.aspx Searchhealthit.techtarget.com. (2010, May). Wireless Medical Telemetry Services (WMTS). Retrieved from: http://searchhealthit.techtarget.com/definition/WMTS-wireless-medicaltelemetry-services Sherman, P. (2006, November/December). EMI Education – A Little Knowledge. Biomedical Instrumentation & Technology, 40(6), 488. Sims, B. (2003, April). Deploying Secure, Reliable Wireless LANs in the Healthcare Environment. Health Management Technology, 24(4), 24-29. Soomro, A., & Cavalcanti, D. (2007, February). Opportunities and Challenges in Using WPAN and WLAN Technologies in Medical Environments. IEEE Communications Magazine, 45(2), 114-122. Spiceworks.com. (2012). Spiceworks IT Desktop. Retrieved from: http://www.spiceworks.com/product/ Thomas, J. (2003, June 23). 802.11e Brings QoS to WLANS. Retrieved from: http://www.networkworld.com/news/tech/2003/0623techupdate.html Waharte, S. (2009, April). Interference-aware Routing in Wireless Mesh Networks, 126. Wang, J., & Du, H. (2005). Setting Up a Wireless Local Area Network (WLAN) for a Healthcare System. International Journal of Electronic Healthcare, 1(3), 335-347. Webopedia.com. (2012). EMI. Retrieved from: http://www.webopedia.com/TERM/E/EMI.html 29 EMI IN HOSPITAL SETTINGS Williams, R. D. (1995, May). Keeping Medical Devices Safe From Electromagnetic Interference. Retrieved from: http://findarticles.com/p/articles/mi_m1370/is_n4_v29/ai_16947864/ Witters, D. (2009, June). Medical Devices and EMI: The FDA Perspective. Retrieved from: http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocument s/ucm106367.htm?utm_campaign=Google2&utm_source=fdaSearch&utm_medium=web site&utm_term=EMI%20shielding%20requirements&utm_content=7 Zukerman, M. (2000). Introduction to Queuing Theory and Stochastic Teletraffic Models. Retrieved from: http://www.ee.cityu.edu.hk/~zukerman/classnotes.pdf 30 146 Sample: Final Paper - Significant Influential Factors Affecting Health Information Technology Diffusion and Infusion This sample , the term project, was prepared for Drexel INFO 731, Organizational and Social Issues in Healthcare Informatics. Details for this course are as follows: Description This course provides an overview of sociotechnical issues in healthcare informatics, focusing on patient care and biomedical research settings. It looks at the human, social, and technological aspects of healthcare IT and focuses on the role of information professionals in applied healthcare IT settings. Course Objectives          Discuss the term "sociotechnical" and give examples of its effect on health IT Describe the basic structure of healthcare organizations and how organizational context of affects IT use Project the implications of IT for future health care delivery and research Compare the design, implementation, and system life-cycle of Health IT to similar projects in other sectors Describe how typical clinician attitudes may affect IT applications Through analysis of selected case examples, show how principles of change management can be applied in health care organizations. Select a healthcare leadership model to apply it to IT management. Identify initiatives in health IT at the multi-organizational, regional, state and national levels and describe their interactions. In summary, students should be able to understand and discuss why clinical IT projects are "incredibly complex social endeavors in unforgiving clinical environments that happen to involve computers, as opposed to computer projects that happen to involve doctors." Final Paper The goal of the final paper was to author a paper that demonstrates and enhances a student’s understanding of a topic of current interest in organizational issues in health informatics. SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Significant Influential Factors Affecting Health Information Technology Diffusion and Infusion By Lisa Romanoski Drexel University Author Note This paper has been prepared in accordance with the requirements of INFO731. 1 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Certification I certify that:  This paper is entirely my own work.  I have not quoted the words of any other person from a printed source or a website without indicating what has been quoted and providing an appropriate citation.  I have not submitted this paper/project to satisfy the requirements of any other course. Signature: Lisa Romanoski Date: June 8, 2012 2 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Abstract Understanding significant factors affecting health information technology (HIT) diffusion and infusion is important because getting a new innovation adopted is difficult regardless of the presence of advantages or disadvantages. Factors can influence implementation decisions and strategies and paint a picture of what to expect pre- and post-decision. This paper focuses on significant external and internal factors. Findings reveal that significant influential external factors include healthcare market characteristics (federal mandates, payment policies, and delivery system), competition, and product quality and effectiveness. Significant influential internal factors include size, financial and staffing resources, culture, compatibility/fit, people, communication pathways and structures, relationships, decision-making, and support mechanisms. Identifying and understanding such factors can provide insight to organizational decision-making, reasons why some innovations are more highly sought than others, and the likelihood for business practice integration success or failure. Caution is recommended for comparing and then hypothesizing from studies that use different methodologies. Introduction Understanding significant factors affecting health information technology (HIT) diffusion and infusion is important because getting a new innovation adopted is difficult regardless of the presence of advantages or disadvantages (Rogers, 2003, p.1). Investigations into diffusion and infusion tend to arise from the need to speed up the process (p. 1). Identifying significant factors can influence implementation decisions and strategies and paint a picture of what to expect pre- and post-decision (Ash, 1997, p. 102-3). While the topic of diffusion/infusion is very broad, the goal of this paper is to identify these significant factors and develop an understanding of some of the organizational attributes and dynamics involved. First, main concepts are introduced and defined. Next, factors external to organizations are identified and then linked to organizational structure, communication pathways, and social networks. This paper relies on key findings presented in a variety of research articles, which may be under or overrepresented in literature (Rye and Kimberly, 2007, p. 253). It does not attempt to address systemic problems in research and design theory (p. 253). Definitions and Concepts Before exploring significant factors influencing HIT diffusion and infusion, key terms will be defined and Diffusion of Innovation Theory is introduced. Key terms used in this paper and their definitions include: 3 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION  Innovation: an idea, practice, or object that is perceived as new by an individual or other unit of adoption (Rogers, 2003, p. 475).  Adoption: a decision to make full use of an innovation as the best course of action available (Rogers, 2003, p. 473).  Implementation: an organizational effort to diffuse an appropriate information technology or innovation within an organizational community (Eder & Igbaria, 2001, p. 234)4.  Diffusion: a process by which innovation is communicated through certain channels over time among members of a social system (Rogers, 2003, p. 5; Sevick, 2004, p. 8). The term generally refers to the spread of use of an innovation or technology (Eder & Igbaria, 2001, p. 234).  Infusion: the degree of integration with existing business processes (Eder & Igbaria, 2001, p. 234; Ash, 1997, p. 103). When used in regard to an IT implementation, infusion is considered the final stage (Eder & Igbaria, 2001, p. 234). Diffusion of Innovations (DOI) Theory was developed in the 1930s but was defined by Everett M. Rogers in the 1960s (Ash, 1997, p. 103). Rogers found that innovation adoption begins with early adopters, followed by early and late majorities, and then laggards (Sevick, 2004, p. 8). Critical mass, the most important point in the process, occurs when enough individuals have adopted an innovation and its further adoption becomes selfsustaining (Sevick, 2004, p. 8). At this point, adopters assume everyone else is an adopter, and non-adopters are forced to cope or accept the change (Sevick, 2004, p. 8). Rogers identifies five critical attributes influential to the adoption rate of an innovation (Rogers, 2003, p. 15-16; Sevick, 2004, p. 8):  Relative advantage: comparison to existing products or conditions  Compatibility: consistency with existing values, past experiences, and needs  Complexity: degree to which it is perceived as difficult to understand or use  Trialability: degree to which it can be experimented with on a limited basis  Observability: results are visible to others According to Rogers (2003), innovations that have greater relative advantage, compatibility, trialability, and observability and less complexity will be more rapidly adopted than other innovations (p. 16). 4 This definition by Eder and Igbaria has been slightly modified for the purposes of this paper. 4 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Returning to the diffusion definition presented earlier, Rogers extracts four key elements: the innovation, communication, time, and the social system through which communication occurs (Rogers, 2003, p. 11). According to Romano (1990), time is the most important element in diffusion and includes consideration of the innovationdecision process, which has five main steps (p. 13; Rogers, 2003, p. 20): 1. Knowledge: individuals learn about the innovation and how it functions 2. Persuasion: occurs when an individual develops an opinion about the innovation 3. Decision: an individual engages in activity focusing on innovation adoption or rejection 4. Implementation: an innovation is put to use 5. Confirmation : occurs when seeking reinforcement of a decision that has been made These steps are important in that they result in the decision to adopt or reject an innovation (Romano, 1990, p. 13). In summary, Rogers’ work on diffusion of innovations provides a framework for understanding the processes involved in predicting the success of an innovation. It continues to be applied in many research areas in order to gain insight to the spreading of ideas and actions in social systems (Green et al., 2009, p. 152.). In regard to healthcare, Green et al. (2009) note that the theory has been applied to physicians adopting a new drug or evidencebased medical practice, public health officers adopting a new policy, other health professionals intervening on heart disease risk factors, and organizations adopting new administrative practices (p. 152). In this paper, significant influential factors pertaining to diffusion and infusion are discussed in relation to a healthcare organization, which can include but not be limited to a hospital. An application of Rogers’ five attributes influential to an innovation’s adoption rate are incorporated into a short review of the New South Wales (NSW) information system case study, which is presented at the end of this paper prior to the conclusion. External Factors Looking at the external factors affecting HIT diffusion/infusion first allows for an understanding of why organizations choose the HIT or other products they do. Learning and/or choose HIT or other products falls into knowledge and persuasion steps of Rogers’ innovation-decision process. Significant external factors include:  Healthcare market characteristics: federal mandates, payment policies, and delivery system  Competition  Product quality and effectiveness 5 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Federal mandates continue to be a significant issue for healthcare organizations, with focus centered on achieving Stage One Meaningful Use and a conversion to International Classification of Diseases, 10th Edition Diagnosis and Procedure Codes (ICD-10) in the next two years (Waldman and Chon, 2007, p. 35, Healthcare Information Management Systems Society (HIMSS), 2012, p.4). Federal mandates impose an enforceable duty upon any state government, so healthcare organizations are required to comply with them (Definitions.uslegal.com, 2012). As such, healthcare organizations may be forced to seek out certain technologies over others in order to comply with the mandates. As an example, achieving Stage One Meaningful Use requires eligible professionals, hospitals, and critical access hospitals (CAHs) to demonstrate meaningful use of a certified electronic health record (EHR) technology in order to receive incentive payments up to $44,000 over five years under the Medicare EHR Incentive Program (CMS.gov, 2012). Converting to ICD-10, a diagnostic coding system implemented by the World Health Organization (WHO) in 1993 to replace ICD-9, will require organizations to update core and secondary computer programs to accept ICD-10, reengineer business processes to support ICD-10 documentation standards, and enhance and/or modify EHRs to accommodate new codes (CMS.gov, 2012; EY.com, 2012). Achieving both of these goals will require organizations to concentrate effort on them and adopt and/or modify HIT to assist in the process (MedPAC, 2004, p. 166). Mandates and regulations are one aspect of healthcare market characteristics that can influence HIT diffusion and infusion. Additional characteristics include payment polices that reward volume rather than quality and healthcare’s fragmented delivery system (MedPAC, 2004, p. 167). One aspect of broad IT diffusion is the reward system in place for the IT product (p. 167). In healthcare, fee-for-service payment systems emphasize service volume, which encourages IT adoption to support billable services, an example of a concentrated effort focused on a specific organizational area. (p. 172). The fragmented delivery system of healthcare pertains to a network of public and private financing, healthcare delivery, and quality assurance structures (Brandeis University, 2010). The challenge of such a fragmented system to HIT diffusion/infusion is the difficulty in adopting technology that can communicate across disparate systems (Brandeis University, 2010; MedPAC, 2004, p. 172). Thus, while HIT is often cited as a tool to address system fragmentation, implementation must also occur as practice and care patterns are redesigned and improved (Brandeis University, 2010). 6 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION A driver also linked to system fragmentation and HIT diffusion and infusion is competition, which can be a facilitator or an inhibitor (Rye and Kimberley, 2007, p. 245). Competition occurs between hospitals that vie for physicians and the patients they can bring to their network (Quigley, 2011, p. 35; Pauly, 2005, p. 1525; Devers et al., 2003, p.457). Competition also develops out of the need to create niche services marketed towards consumers and to develop certain specialty areas of the hospital or system as a center of excellence (Devers et al., 2003, p. 460). Adopting certain types of technology can incentivize both physicians and patients (p. 35). One example is a physician portal, which allows for remote patient record access. The portal is used as a competitive strategy to strengthen relationships with physicians (Grossman et al., 2006, p. 1634). Grossman et al. (2006) noted that “active” hospitals develop portals in response to competitive pressure, whereas “laggard” hospitals with little or no portal development are often weaker financially and place a lower priority on clinical IT activities (p. 1634). While competition influences the development of something such as a physician portal, competition can also influence whether the portal becomes linked to other data sources to create regional health information organizations (RHIOs). Grossman et al. (2006) found that competition is viewed as a barrier to (RHIOs), as “competing and adversarial parties would be required to collaborate and share their more valued asset: patients their data” (p. 1634). In this situation, competition both facilitated the technology adoption and also inhibited its wider incorporation into a larger network. Varying rates of competition also influence HIT diffusion and infusion. Burke et al. (2005) found that hospitals in urban and highly competitive markets have higher adoption rates of administrative, clinical, and strategic IT compared to hospitals in rural markets and in areas of low competition (p. 354; Menachemi et al., 2009, p. S83). The above examples show that competition influences HIT diffusion and infusion by establishing need for HIT. Once need is established, the next likely step is identifying quality products, the lack of which can deter HIT diffusion and infusion. In HIMSS’s February 2012 executive leadership survey, vendors’ inability to effectively deliver satisfactory products or services was cited as the third greatest barrier to HIT implementation (p.9). One such example of vendor dissatisfaction occurred in the case of Cerner FirstNet information system deployment in New South Wales, Australia, hospitals (Patrick, n.d.; Wright, 2011). An extensive review of the system by eHealth expert John Patrick of the University of Sydney’s Health Information Technology Research Laboratory revealed several 7 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION issues, including but not limited to poor software design and failure of the vendor to adequately respond to requests (Patrick, n.d.; Wright, 2011). Vendor dissatisfaction was also identified in a 2011 study regarding vendor switching and dropping among hospitals (Lammers & Zheng, 2011, p. 742). Authors Lammers and Zheng (2011) linked vendor switching and dropping to dissatisfaction with earlier IT systems (p. 742). The authors found that 28 percent of 1,579 hospitals reporting a live and operational electronic medical record (EMR) from a named commercial vendor in 2003 switched to another named commercial vendor by 2008, and an additional eighteen percent reported no automated EMR in 2008 (p. 745). The authors also identified hospital characteristics associated with HIT vendor switching and dropping (p. 747-8):  For-profit hospitals and those with larger portions of Medicaid-covered patients are less likely to switch vendors  Not-for-profit hospitals may be more inclined to incur costs of higher quality systems over time  Teaching hospitals, more sophisticated users, were less likely to drop the technology Competition, as discussed earlier, also factors into vendor decisions, as Lammers and Zheng deduced that technology use signaled a competitive advantage in attracting patients and payers (p. 748). Furthermore, the authors surmised that competition may stimulate greater effort during implementation to ensure more effective IT integration into clinical workflow (p. 748). In summary, the external factors of healthcare market characteristics, competition, and product quality and effectiveness significantly influence HIT diffusion and infusion. The importance of recognizing these factors has implications for healthcare organization executives faced with decision-making regarding HIT investment and management and healthcare policy-makers seeking to positively influence HIT diffusion/infusion (Menachemi, 2011, p. 276). The next section explores significant factors internal to healthcare organizations that influence HIT diffusion and infusion and provides insight to how innovation information diffuses from the outside in. Internal Factors The previous section explored external factors influential to HIT diffusion and infusion. For HIT diffusion and infusion to be successful within an organization, its attributes must be in alignment with the prospective 8 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION 9 implementation strategy. Those attributes, which are significant internal factors and are not necessarily independent of one another, include:  Size  People  Financial resources  Communication pathways and structures  Staffing resources  Relationships  Culture  Decision-making  Compatibility/fit  Support mechanisms Organizational size is a factor in HIT diffusion and infusion in that larger healthcare practices tend to be greater users of clinical IT. This suggests that a larger revenue base or more complex practice with greater management capabilities allows larger groups to better support sizeable HIT investments (MedPAC, 2004, p. 170). Kimberly and Evanisko (1981) also found that economies of scale enhance feasibility (p. 697-8). Economies of scale refers to lower average costs achieved from the spreading of fixed costs over units of production, which can be taken to be the number of patients serviced in a given year (Yafchak, 2000, p. 67). The idea is that greater volumes of activity make it easier for organizations to better afford innovations (Kimberly & Evanisko, 1981, p. 699). Even for some larger organizations, available financial resources to spur HIT diffusion and infusion can be difficult to achieve. HIMSS surveys of IT executive leaders tend to be representative of larger organizations – those with an average bed size of 479 (HIMSS, 2012, p. 8; HIMSS, 2006, p. 4). Almost all executive IT leader surveys prior to February 2012 reported that lack of adequate financial support was the predominant barrier to HIT implementation (HIMSS, 2012, p. 8; HIMSS, 2006, p. 6). The 2012 HIMSS survey, the most recent, reveals the resource of concern pertaining to HIT implementation is now adequate staffing (p. 9). The concern over HIT staffing resources is reflected elsewhere, including a February 2011 article by Joseph Goedert for HealthDataManagement.com in which concerns were expressed by both chief information officers and vendors. One CIO says In particular, he's seeing "kids applying right out of school and thinking they can do these jobs without experience” when three to five years of experience is really needed (Goedert, 2011). Additionally, vendors have an equally difficult time, with one commenting on the ease of finding people with skills in 20- to 25-year old technology and the difficulty of finding those with modern IT skills (Goedert, 2011). SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Assuming financial and staffing resources are in place to support HIT adoption, will an organization’s culture and existing work practices be receptive to HIT? Tuan and Venkatesh (2010) find organizational culture influences innovation (and thus possibly HIT) in two ways (p. 145-6): 1. Through socialization processes in organizations, individuals learn what behavior is acceptable and how activities should function. Norms develop. Individuals will make assumptions about whether innovative behavior forms part of the way in which the organization operates. 2. The basic values, assumptions, and beliefs become enacted in established forms of behaviors and activity and are reflected as structures, policy, practices, management practices, and procedures. Individuals in organizations come to perceive what is considered valuable and how they should act in the work place. In short, organizational culture “affects the extent to which innovative solutions are encouraged, supported, and implemented” and significantly influences organizational success (p. 145-6). The extent to which personnel feel empowered while also working with an organization that allows flexibility positively influences innovation (p. 146). If an organization is accepting of innovations, will that innovation be compatible and fit within the organization’s existing structure and work processes? An innovation such as HIT may have greater difficulty becoming integrated into an organization as compared to something more specific such as a tool used for medical imaging because it tends to be disruptive to existing work flow processes (MedPAC, 2004, p. 167). This highlights the importance of recognizing technological “fit” and the work context into which it is introduced (Melville & Ramirez, 2008, p. 250). The NSW case mentioned earlier is one such example of poor HIT fit within an organization in that the organization’s strategy-structure, strategy-structure-management processes, and strategy-structure-role relationships impeded diffusion (Southon et al., 1997, p. 112; Patrick, n.d., p. 20). In summary, it’s important to note the role of an IT endeavor in regard to supporting business processes and operations, management and employee decision-making, and strategic decision-making for competitive advantage and future planning (Melville & Ramirez, 2008, p. 250). The preceding paragraphs have addressed some of the organizational attributes that affect HIT diffusion/infusion: size, resources, culture, and compatibility/fit. The next significant factor affecting HIT diffusion/infusion is people. The people within an organization are important because they can help find and then diffuse information through their relationships and communication pathways. They can also inhibit diffusion/infusion. The following sections explore the roles of individuals in HIT diffusion and infusion. 10 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Before the onset of meaningful use and conversion to ICD-10 made its way into recent headlines and journal articles, prior work existed on the subject of the way in which information makes its way into a healthcare organization from the outside (Ash, 1997; Fitzgerald, 2003). This subject area is still important and relevant because it established the communication foundation upon which organizations still function. Commercial and professional organization channels are important external-to-internal pathways by which information makes into healthcare organizations. When physicians receive information through commercial channels and it’s validated through professional channels, adopting technological innovations is more likely (Ash, 1997, p. 103). Fitzgerald et al. (2003) also noted that networks and communities of knowledge are key to acquiring scientific acceptance (p. 219). In regard to physicians, Fitzgerald et al. (2003) noted that the people to whom they turn to for information and verification are those whom they know personally, including but not limited to consultants at local hospitals, their immediate colleagues, or other doctors whom they had known for a long time (p. 222). In regard to nurses and allied health professionals, Fitzgerald et al. (2003) found these professionals were more likely to consult someone in their own profession for verification of evidence, may receive information “filtered down” from physicians, or receive regular nurse newsletters from facilitators (p. 222, 224). Regardless of the means in which it is accomplished, these findings show that trust is an issue in the establishment of credibility (p. 222). Once an organization’s information-seekers gain knowledge of an innovation and are convinced of its credibility and usefulness, these people can evolve into champions who then actively and enthusiastically promote the innovation, build support, and ensure technological implementation (Ash, 1997, p. 103). These people can then utilize an organization’s internal communication structure to promote discussion, encourage debate, and thus diffuse the knowledge of the technology/innovation (Fitzgerald et al., 2003, p. 222; Rye and Kimberly, 2007, p. 262). In some instances, the champions become project managers and begin to build up teams (Tuan & Venkatesh, 2010, p. 148). As communication of an innovation makes its way around the inner workings of an organization, the relationships between staff become important to the success or failure of diffusion and infusion. Fitzgerald et al. (2003) noted that good relationships between partners, physicians, and the rest of the professional and administrative staff form the foundation for improvement and innovation (p. 224). Diffusion and infusion is less likely when relationships are dysfunctional and conflicts exist (p. 224). 11 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Once awareness of a technological innovation implementation heightens throughout an organization, decision-making both at the organizational and individual levels becomes influential to diffusion and infusion. Organizational decision-making can be either centralized or decentralized. Centralized decision-making is often done by a smaller number of people operating at the upper echelons of an organization, whereas decentralized decision-making delegates authority to all levels of management and in all of the organization (Managementstudyguide.com, 2012; Vitez, 2012). For HIT adoption, decentralized decision-making and top management support can positively impact success (Ash, 1997, p. 103). Tuan and Venkatesh (2010) also looked at promotion and implementation of technological innovation from a management perspective (p. 148). When comparing top down to staff up decision-making, they found that top down decision-making may hinder innovation from within (p. 148). In these types of environments, staff might see technological innovation as top-management’s business and would learn to use new technology when it was implemented in their department (p. 147). In contrast, innovation is more positively influenced by staff working in supportive environments in which they are encouraged to make beneficial changes, minor or major (p. 147). Referred to as “chaos within guidelines,” top management has a set of strategic goals but allows personnel freedom within the context of these goals (p. 147). Says one doctor surveyed in Tuan and Vekatesh’s study, “The director always tells me to search for new technology, whether it is in treatment or management scope, which is beneficial to patients and makes [our organization] distinctive” (p. 147). These examples clearly show how influential an organization’s decision-making processes can be to diffusion and infusion and provide insight to staff activeness or passiveness in regard to their organization’s goals and strategies. Upper level management decision-making may be influential in getting new technology adopted, but actual diffusion and use of a technology could be inhibited by decision-making at the individual level (Ash, 1997, p. 103). Several factors influence an individual’s decision to use a new technology. Recall from the discussion of Rogers’ Diffusion of Innovations (DOI) Theory that the five critical attributes influential to the adoption rate of an innovation include relative advantage, compatibility, complexity, trailability, and observability (2003, p. 15-16). Supporting evidence for these attributes is as follows. Ash (1997) found that when potential users are included in decision-making and communication is accurate and timely, they accept those decisions more readily (p. 108). Rye and Kimberly (2007) note that decisions to use 12 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION technology are influenced by ease of use and compatibility with routines (p. 252). In addition to these factors, Putzer and Park (2010) identified job relevance, belief that the item improves care, ease and efficiency of operational management, and executive management support also contribute to decisions to use an innovation (p. 6-7). In summary, the internal factors of size, financial and staffing resources, culture, compatibility/fit, people, communication pathways and structure, relationships, decision-making, and support mechanisms can significantly influence HIT diffusion and infusion. As mentioned in the previous section on external factors, the importance of recognizing these factors can influence executive management and policy-makers in their decision-making processes. Great sums of money are being invested in HIT implementation projects (Southon et al., 1997, p. 113). Recognizing significant factors influential factors can make or break a project (Sevick, 2004). Putting it all Together: A Short Review of the NSW Case Study The NSW case, mentioned previously in this paper in regard to issues with vendor dissatisfaction and poor IT fit within an organization, was one in which implementation of several information system components into NSW’s Public Health System (PHS) failed. The NSW case has been covered extensively in research efforts, including but not limited to Professor John Patrick of the University of Sydney, Australia (n.d.), and Southon et al. (1997). The review performed by Southon et al. (1997) looked at the implementation of the system into the NSW’s PHS and its diffusion through the organization (p. 112). As noted by Southon et al. (1997), NSW sought to better manage resources with the use of HIT and decided to implement simultaneously three core systems: financial, pathology and patient administration (PAS)/clinicals (p. 113). In general, the project failed over time, and the PAS clinical system was completely withdrawn after being tried in several pilot sites (p. 113). The overall financial loss from this effort is estimated at $12M (p. 113). As mentioned previously, Roger’s five attributes influential to an innovation’s adoption rate include relative advantage, compatibility, complexity, trialability, and observability (2003, p. 15-16). Using Southon and fellow authors’ 1997 research, these attributes have been applied to the NSW case. Findings are as follows (p. 1179):  Relative advantage: comparison to existing products or conditions � A task that used to take twenty seconds took several minutes; “there did not appear to be any significant gain for staff” � Clinicians were losing functionality  Compatibility: consistency with existing values, past experiences, and needs 13 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION � “They found a considerable difference between what the system provided and what they considered they needed”  Complexity: degree to which it is perceived as difficult to understand or use � “The system was considered rather user unfriendly by clinicians"  Trialability: degree to which it can be experimented with on a limited basis � A total of five pilot sites were used  Observability: results are visible to others � Managers saw little cost savings or resolution of problems � A single implementation was not commercially viable Significant external factors influential in this case study include political pressure to curtail costs, the likelihood of future governmental reporting requirements, and product quality and effectiveness (Southon et al., 1997, p. 116). Significant influential internal factors include size, compatibility/fit, decision-making, and communication. While size was discussed previously in the context of economies of scale, size in the NSW case refers to a geographically dispersed individual units ranging in size from 800-bed hospitals to smaller outpatient clinics (p. 119). The compatibility and fit of the HIT system within the existing NSW was an issue (p. 119). While the HIT selection team of central policy makers and IT specialists included doctors and managers, decision-making will still mostly concentrated at the top of the organization (p. 116). The communication pathways were not very effective in diffusing/infusing the technology because most medical staff went untrained and others collectively voiced complaints about user unfriendliness (p. 118). In summary, the principal lesson from the NSW case was the inability of the current organizational environment to accommodate an HIT system (p. 112). This lack of IT-organizational fit makes diffusion difficult to manage (p. 122). Conclusion External and internal factors can significantly impact HIT diffusion and infusion. Understanding influential external factors such as healthcare market characteristics (federal mandates, payment policies, and delivery system), competition, and product quality and effectiveness can provide insight to organizational decision-making and reasons why some innovations are more highly sought than others. Internal factors such as organizational size, financial and staffing resources, compatibility/fit, culture, and people all affect the manner in which HIT gets 14 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION diffused into the organization and the extent to which it becomes integrated into business practices. Identifying and understanding significant influential factors has implications for resource allocation strategies and policy-making. As mentioned previously, this paper relies on key concepts presented in a variety of research articles. Articles tended to vary in terms of study methodology. While extraction of key concepts from these sources may be sufficient for a broad topic such as the one presented herein, comparing and then hypothesizing from studies that use different methodologies can lead to erroneous conclusions (Sale et al., 2002, p. 43; Kimberly & Rye, 2007, p. 253). 15 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION References AAPC.com. (2012). ICD-10 FAQ. Retrieved from: http://www.aapc.com/icd-10/faq.aspx#what Ash, J. (1997, March/April). Organizational Factors that Influence Technology Diffusion in Academic Health Sciences Centers. Journal of the American Medical Informatics Association, 4(2), 102 – 111. Brandeis University. (2010, July 14). Foundations and Healthcare Reform 2010, Policy Brief: Delivery System Redesign. Retrieved from: http://www.niatx.net/PDF/ARC/Delivery_System_Redesign.pdf Burke, D. E., Wang, B. B. L., Wan, T. T. H., & Diana, M. L. (2002, August). Exploring Hospitals’ Adoption of Information Technology. Journal of Medical Systems, 26(4), 349-355. Coyte, P. C., & Holmes, D.(2007). Health Care Technology Adoption and Diffusion in a Social Context. Policy, Politics, & Nursing Practice, 8(1), 47 – 54. CMS.gov (2012, May 1). EHR Incentive Programs. Retrieved from: https://www.cms.gov/Regulations-andGuidance/Legislation/EHRIncentivePrograms/index.html?redirect=/EHRIncentivePrograms/ CMS.gov. (2012, April 9). Fact Sheet: HHS Proposes One-year Delay of ICD-10 Compliance Date. Retrieved from: http://www.cms.gov/apps/media/press/factsheet.asp?Counter=4330&intNumPerPage=10&checkDate=&ch eckKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&i ntPage=&showAll=&pYear=&year=&desc=&cboOrder=date Deffuant, G., Huet, S., & Amblard, F. (2005, January). An Individual-based Model of Innovation Diffusion Mixing Social Value and Individual Benefit. American Journal of Sociology, 110(4), 1041-1069. Definitions.uslegal.com. (2012). Federal Mandate Law & Legal Definition. Retrieved from: http://definitions.uslegal.com/f/federal-mandate/ Devers, K. J., Brewster, L. R., Casalino, L. P. (2003, February). Changes in Hospital Competitive Strategy: A New Medical Arms Race? Health Services Research, 38(1), 447-469. Eder, L. B. & Igbaria, M. (2001). Determinants of Intranet Diffusion and Infusion. Omega: The International Journal of Management Science, 29(3), 233-242. Federal Mandate. (2012).In USLegal.com online. Retrieved from: http://definitions.uslegal.com/f/federal-mandate/ Fitzgerald, L., Ferli, E., & Hawkins, C. (2003). Innovation in Healthcare: How does Credible Evidence Influence Professionals? Health and Social Care in the Community, 11(3), 219–228. 16 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Goedert. J. (2011, February 1). Tackling the Health I.T. Workforce Shortage. Retrieved from: http://www.healthdatamanagement.com/issues/19_2/tackling-the-health-i.t.-workforce-shortage-418041.html?zkPrintable=true Green, L. W., Ottoson, J. M., Garcia, C., & Hiatt, R. A. (2009). Diffusion Theory and Knowledge Dissemination, Utilization, and Integration in Public Health. Annual Review of Public Health, 30(1), 151-174. Grossman, J. M., Bodenheimer, T. S., & McKenzie, K. (2006, November/December). Hospital-Physician Portals: The Role of Competition in Driving Clinical Data Exchange. Health Affairs, 25(6), 1629-1636. Healthcare Information Management Systems Society (HIMSS). (2012, February 21). 2012 HIMSS Leadership Survey: Senior IT Executive Results. Retrieved from: http://www.himss.org/content/files/2012FINAL%20Leadership%20Survey%20with%20Cover.pdf Kimberly, J. R. (1978, December). Hospital Adoption of Innovation: The Role of Integration into External Informational Environments. Journal of Health and Social Behavior, 19(4), 361-373. Kimberly, J. R., & Evanisko, M. J. (1981). Organizational Innovation: The Influence of Individual, Organizational, and Contextual Factors on Hospital Adoption of Technological and Administrative Innovations. Academy of Management Journal, 24(4), 689-713. Lammers, E. J., & Zheng, K. (2011). Characteristics Associated with Hospital Health IT Vendor Switching and Dropping. American Medical Informatics Association (AMIA) Annual Symposium Proceedings, 742-749. Managementstudyguide.com. (2012). Centralization and Decentralization. Retrieved from: http://www.managementstudyguide.com/centralization_decentralization.htm Medicare Payment Advisory Commission (MedPAC). (2004, June). Information Technology in Health Care. Report to the Congress: New Approaches in Medicare, 156-181. Retrieved from: http://www.medpac.gov/document_TOC.cfm?id=315 Melville, N. & Ramirez, R. (2008). Information Technology Innovation Diffusion: an Information Requirements Paradigm. Info Systems, 18(3), 247–273. Menachemi, N., Shin, D. Y., Ford, E. W., & Yu, F. (2011, July/September). Environmental Factors and Health Information Technology Management Strategy. Health Care Management Review, 36(3), 275-285. Menachemi, N., Brooks, R. G., Schwalenstocker, E., & Simposon, L. (2009, January). Use of Health Information Technology by Children’s Hospitals in the United States. Pediatrics, 123(2), S80-S84. 17 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Okafor, M. C., & Thomas, J. (2008, March). Presence of Innovation Adoption-Facilitating Elements in Hospitals, and Relationships to Implementation of Clinical Guidelines. The Annals of Pharmacotherapy, 42, 354-360. Pare, G., & Trudel, M. (2007). Knowledge Barriers to PACS Adoption and Implementation in Hospitals. International Journal of Medical Informatics, 76, 22-33. Patrick, J. (n.d.). A Critical Essay on the Deployment of an ED Clinical Information System – Systemic Failure or Bad Luck? Draft V6.0. Retrieved from: http://sydney.edu.au/engineering/it/~hitru/essays/Pt%201%20%20The%20Story%20of%20the%20Deployment%20of%20an%20ED%20Clinical%20Information%20Sy stem6.0.pdf Pauly, M. V. (2005, November/December). Competition and New Technology. Health Affairs, 24(6), 1523-1535. Quigley, K. (2011, December 12-18). Healthy Competition. San Diego Business Journal, 32(50), 1, 35). Ramono, C. (1990, December). Diffusion of Technology Innovation. Advances in Nursing Science, 13(2), 11 - 21. Rye, C. B. & Kimberly, J. R. (2007, June). The Adoption of Innovations by Provider Organizations in Health Care. Medical Care Research and Review, 64(3), 235-278. Sale, J.E.M., Lohfeld, L.H., & Brazil, K. Revisiting the Quantitative-Qualitative Debate: Implications for MixedMethods Research. Quality & Quantity, 36, 43-53. Sevick, P. (2004, September). Innovation Diffusion. Business Communications Review, 34(9), 8-11. Southon, F. C. G., Sauer, C., Dampney, C. N. G. (1997, April/March). Information Technology in Complex Health Services: Organizational Impediments to Successful Technology Transfer and Diffusion. Journal of the American Medical Informatics Association, 4(2), 112 – 124. Timmons, S. (2003). Nurses Resisting Information Technology. Nursing Inquiry, 10(4), 257-269. Tuan, L. T., & Venkatesh, S. (2010, July). Organizational Culture and Technological Innovation Adoption in Private Hospitals. International Business Research, 3(3), 144-153. Vitez, O. (2012). Centralized vs. Decentralized Organizational Structure. Retrieved from: http://smallbusiness.chron.com/centralized-vs-decentralized-organizational-structure-2785.html Waldman, J.D., & Cohn, K. H. (2007, September 8). Mending the Gap between Physicians and Hospital Executives. Retrieved from: http://healthcarecollaboration.typepad.com/healthcare_collaboration_/files/physhospgap_waldman.pdf 18 SIGNIFICANT FACTORS: HIT DIFFUSION/INFUSION Wright, C. (2011, March 7). Doctors want NSW eHealth System Scrapped. Retrieved from: http://www.ehealthcentral.com.au/2011/03/dcotors-want-nsw-ehealth-system-scrapped/ Yafchak, R. (2000, Fall). A Longitudinal study of Economies of Scale in the Hospital Industry. Journal of Health Care Finance, 27(1), 67-89. 19 166 Sample: PowerPoint Presentation This sample was prepared for Drexel INFO 731. Course description and goals are here. 8/10/2012 Significant Influential Factors Affecting Health Information Technology Diffusion and Infusion By Lisa  Romanoski Drexel University June 8, 2012 Definitions and Concepts • Innovation: an idea, practice, or object that is perceived as new by an individual or other unit of adoption. • Adoption: a decision to make full use of an innovation as the best course of action available. • Implementation: an organizational effort to diffuse an appropriate information technology or innovation within an organizational community. • Diffusion: a process by which innovation is communicated through certain channels over time among members of a social system. The term generally refers to the spread of use of an innovation or technology. • Infusion: the degree of integration with existing business processes. When used in regard to an IT implementation, infusion is considered the final stage. 1 8/10/2012 Diffusion of Innovation Theory • Early adopters ‐> early/late majorities ‐> laggards • 5 critical attributes influential to adoption rate: 1. Relative advantage: comparison to existing products or conditions 2. Compatability: consistency with existing values, past experiences, and needs 3. Complexitiy: degree to which it is perceived as difficult to understand or us 4. Trailability: degree to which it can be experimented with on a limited basis 5. Observability: results are visible to others Knowledge ‐> Persuasion ‐> Decision ‐> Implementation ‐> Confirmation Factors 2 8/10/2012 External Factors • Healthcare Market Characteristics    Federal mandates Meaningful Use ICD‐10 Payment policies Delivery System • Competition  Physicians, patients • Product quality and effectiveness (From Coast, May 2012) Internal Factors: Size and Resources • Size • Financial resources • Staffing resources “Kids [are] applying right out of school and thinking they can do these jobs without experience when three to five years of experience is really needed.” (Goedert, 2011) 3 8/10/2012 Internal Factors: Culture and Fit • Culture • Compatibility/fit “The director always tells me to search for new technology, whether it is in treatment or management scope, which is beneficial to patients and makes [our organization] distinctive.” (Tuan & Venkatesh, 2010, p. 147). Internal Factors: People • People • Communication pathways and structures • Relationships 4 8/10/2012 Internal Factors: Decision‐making • Decision‐making   Centralized Decentralized • Support • People • Recall: 5 critical attributes influential to adoption rate: 1. Relative advantage 2. Compatability 3. Complexitiy 4. Trailability 5. Observability Conclusions • External and internal factors are important • Provides insight to:  Innovation adoption  Resource allocation strategies  Policy‐making  What to expect pre‐ and post‐decision Thank you!  Questions: [email protected] 5 172 Sample: Use Case This sample , the term project, was prepared for Drexel INFO 620, Information Systems Analysis & Design. Details for this course are as follows: Description This course provides an advanced treatment of systems analysis and design with special emphasis on object-oriented analysis and design techniques based on the Unified Modeling Language (UML). It discusses major modeling techniques of UML including use-case modeling, class modeling, object-interaction modeling, dynamic modeling and state diagrams and activity diagrams, subsystems developments, logical design, and physical design. Course Objectives    Develop an understanding of the fundamentals of Object-Oriented Design and its evolution Develop proficiency in the Unified Process and Unified Modeling Language concepts by creating domain models, system sequence diagrams, UML interaction diagrams, and UML class diagrams Apply General Responsibility Assignment Software Patterns or Principles (GRASP) concepts to a given problem domain Use Case Assignment Details This assignment involved developing a fully dressed use case for an urgent care patient registration system, along with a use case diagram. Use Case Name UC1: Register Patients Assumptions The facility has a laboratory and radiology unit, but no pharmacy. Clinical decision support and adverse event detection is not included in application. Scope Patient registration application Level User goal Primary Actor Clerk and clinician (nurse, doctor, radiologist, and/or laboratory assistant). “User” may refer to clerks or clinicians. Stakeholders/ Interests Clerk Wants to enter Patient details (name, address, phone, height, weight, medical insurance number, and short problem description), determine patient priority, know which rooms are available, know which doctor is assigned to which room, and assign patients to a room. Nurse Wants to acquire Patients’ physiological characteristics, including temperature and blood pressure and enter them into the application. Doctor Wants to enter illness and treatment regimen, including prescribed medications. Radiologist Wants to append radiology results and files to Patients’ files. Laboratory Assistant Wants to append lab results to Patients’ files. Staff Wants to access system to know status of treatment rooms: i.e., in use, needs cleaning, or available. Wants to view list of processed patients, including names and problem descriptions, and assigned room and associated doctor’s name. Patient Wants medical attention to assist in overcoming illness and accurate transcription/coding of the visit for insurance purposes. Healthcare Organization Wants to know what services were provided to which patients by whom. Wants to link services to coding information for billing purposes. Payer/ Insurance Wants to know what services were provided to which patients. Wants services to be linked to payer/insurance for billing purposes. Preconditions Clerk, clinicians, staff, and healthcare organization are identified and authenticated. Success Guarantees (Postconditions) Patient data, patient room assignments, doctor room assignments, xrays/imaging, lab results, illness and treatment regimen, services rendered and associated coding information, and treatment room status saved. Priority listing correctly calculated and updated as patients come in, are seen, and go home. Main Success Scenario 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. Extensions Patient arrives at facility. Clerk checks in Patient: acquires data (name, address, phone, height, weight, medical insurance number, and short problem description). System records Patient data. Clerk determines Patient priority based on problem description. Clerk enters Patient priority into system. System records Patient priority listing. Clerk assigns Doctors to certain rooms. Clerk enters Doctor room assignments into system. System records Doctor room assignments. Clerk checks room availability. Clerk assigns a Patient to a room. System records Patient room assignment. System updates Patient room availability list. Patient goes to assigned room. Nurse takes Patient’s temperature and blood pressure. Nurse enters Patient’s physiological data into system. System records Patient’s physiological data. Doctor sees Patient. Doctor may order lab work and/or x-rays. Laboratory performs test(s) if lab work is ordered. Laboratory assistant enters test results into system. System records test results. Radiology takes x-ray(s) if ordered. Radiologist saves x-ray(s) in system. System records x-ray(s). Doctor accesses and reviews lab test results and/or x-ray(s). Doctor makes a diagnosis. Doctor prescribes a treatment regimen and/or medication(s), including dosage. Doctor enters treatment regimen and/or medications, including dosage into computer. System records treatment regimen and/or medication information. Patient leaves facility. Clerk enters information on services rendered into system. System records information on services rendered. System associates rendered services with medical coding for billing. System produces and sends a bill to payer/insurance company and/or patient. System notifies Staff that a treatment room needs cleaning. Staff clean treatment room. Staff access and update the system to acknowledge room availability. *a. During any log in, user enters invalid authentication code. 1. System signals error to User. 2. System requests User re-type authentication code. 3. System acknowledges authentication code. 3a. System recognizes invalid authentication code for second time. 3b. User re-enters authentication code. 1. System recognizes invalid authentication code for third time. 2. User re-enters authentication code. 3. System fails to recognize authentication code. 4. System locks User out. 5. System signals error to user. 6. System indicates User must contact IT. 4. System allows User access. *b. During any data entry, User enters invalid entry at or in on-screen Extensions prompts/boxes. 1. System signals error to User. 2. System indicates numeric or character entry. 3. System indicates required length of entry. 4. System indicates numeric range for numeric entries. 5. User re-enters item. *c. During any data entry, entry length exceeds text box character spacing limits. 1. System signals error to User. 2. System indicates required length of entry. 2a. User enters text. 3. System records entry. *d. At any time, system fails. To support recovery and correct data recording, ensure data can be recovered from any step of the scenario. 1. User restarts system, logs in, and requests recovery of prior state. 2. System reconstructs prior state. 2a. System does not perform recovery: 1. System signals error to User. 2. System enters a clean state. 3. User begins new session. *e. During any data entry, medical insurance number doesn’t match valid patient. 1. System signals error to User. 2. User re-enters medical insurance number. 2a. System fails to identify Patient. 1. System signals error. 2. User calls Clerk to verify medical insurance number for a specific patient. 3. User obtains correct medical insurance number. 3. System finds Patient. 2-3a. Patient says he or she does not have a medical insurance number. 1. Clerk enters “no” for medical insurance into the system. 2. System records patient data. 4a. If patient’s issue is possibly life, limb, or eyesight threatening, his or her condition is an emergency and should be treated at a hospital emergency room, not at an urgent care center. Examples of such conditions include but are not limited to chest pain, difficulty breathing, severe bleeding, overdose, possible stroke, severe trauma, open fractures, and penetrating eye injuries. 1. Clerk immediately calls 911 for ambulance transport. 8a. Clerk enters conflicting Doctor room assignments into system. 1. System retains selected Doctor. 2. System signals error to Clerk. 3. System indicates no two rooms can be assigned to the same Doctor. 4. System provides pop-up box list to Clerk showing available rooms. 5. Clerk selects an available room for the selected Doctor. 6. System records Doctor room assignment. 8b. All 1. 2. 3. 4. rooms are assigned to Doctors. System signals error to Clerk. System indicates to Clerk that all rooms are assigned. System asks Clerk if Doctor is placed on “float” duty. Clerk either checks or unchecks box for “float” duty. 11a. Clerk enters conflicting Patient room assignment into system. Extensions 1. 2. 3. 4. 5. 6. System retains selected Patient. System signals error to Clerk. System indicates no two rooms can be assigned to the same Patient. System provides pop-up box list to Clerk showing available rooms. Clerk selects an available room for the selected patient. System records Patient room assignment. 11b. All treatment rooms are full. 1. System retains selected Patient. 2. System signals error to Clerk. 3. System indicates all patient rooms are full. 4. System asks Clerk if Clerk wants to assign patient to next available patient room. 5. Clerk selects “yes” or “no.” 5a. System acknowledges “yes” response. 1. System assigns selected Patient to next available room. 5b. System acknowledges “no” response. 1. System exits Patient room assignment screen. 19a. Doctor orders lab work: 1. System asks Doctor to select from an on-screen list of available lab tests. 2. Doctor selects from available tests. 2a. Doctor wants a modified version of available lab test or test not listed. 1. System offers Doctor an “other” option from available test list. 2. Doctor selects “other.” 3. System provides free form text box. 4. Doctor types information into text box. 5. Doctor selects “submit.” 3. System records selected lab test(s). 4. System accesses laboratory department’s schedule. 5. System inserts Patient name, ID, and requested test(s) into laboratory department’s schedule in chronological order based on time of request. 5a. System fails to communicate with laboratory department’s schedule. 1. System restarts communication. a. Schedule unavailable. b. System informs user schedule unavailable. c. Doctor calls laboratory department to schedule test(s). 2. System records patient data into schedule. 19b. Doctor orders x-rays: 1. System asks Doctor to select from an on-screen list of available x-rays. 2. Doctor selects from available list. 2a. Doctor has special instructions for x-ray(s). 6. System offers Doctor a “special instructions” option from available x-ray list. 7. Doctor selects “special instructions.” 8. System provides free form text box. 9. Doctor types information into text box. 10. Doctor selects “submit.” 3. System records selected x-ray(s). 4. System accesses radiology department’s schedule. 5. System inserts Patient name, ID, and requested x-ray(s) into radiology department’s schedule in chronological order based on time of request. 5a. System fails to communicate with x-ray department’s schedule. 1. System restarts communication. a. Schedule unavailable. b. System informs user schedule unavailable. c. Doctor calls radiology department to schedule test(s). 2. System records Patient data into schedule. Extensions 26a. Doctor can’t access lab test results and/or x-ray(s). 1. Doctor logs out of system. 2. Doctor restarts computer. 3. Doctor logs back in to system. 3a. Lab test results and/or x-ray(s) not accessible. 1. System informs Doctor lab test results and/or x-rays not available. 2. System instructs Doctor to call laboratory and/or radiology to discuss results. 29a. Doctor wants to include special prescription instructions. 1. Doctor selects “special instructions” on treatment regimen and prescription(s) screen. 2. Doctor enters text into box. 2a. System won’t accept data entry. 1. Doctor exits system. 2. Doctor logs back in to system. 3. Doctor makes second attempt to enter text. 3a. System won’t accept text during second attempt. 1. System instructs Doctor to call IT. 34a. System cannot find medical code for services rendered. 1. System signals error to Clerk. 2. System asks Clerk to re-enter rendered services. 2a. System does not find a medical code for second entry. 1. System signals error to Clerk. 2. System suggests selecting “other” category for entry. 3. Clerk selects “other category. 4. Clerk enters information. 3. System applies medical code for services rendered. 35a. Payer/insurance company’s system unavailable. 1. Clerk logs out of system. 2. Clerk logs back in to system. 3. Clerk tries to resend bill. 3a. System signals that payer/insurance company’s system is unavailable. 1. Clerk prints out bill. 2. Clerk mails hard copy of bill to payer/insurance company. 4. System signals successful transmittal. 38a. Room availability unknown. 1. Clerk contacts staff to check availability of room. 2. Clerk requests staff log in to the system to update room availability list. Special Requirements None at this time. Technology/ Data Variations List All data entry via keyboard and mouse. Frequency of Occurrence Continuous Miscellaneous Does the system need to be designed to include not only existing ICD-9 but also 15-16. In the next few years, nurses may begin using IPads to collect patient physiological information. ICD-10 for medical coding? Can system be linked to interface with payer/insurance provider? Patient Patient Registration Application Requests Treatment Registers Patients Clerk Prioritizes Patients Assigns Doctors to Rooms Assigns Patients to Rooms Updates Room Availability List Nurse Records Patients’ Physiological Data Orders Lab Tests Doctor «actor» Healthcare Organization Orders X-Rays Laboratory Assistant Records Lab Tests Records X-Rays Radiologist Records Treatment Regimen and/or Medication(s) Records Services Rendered Associates Services Rendered with Medical Produces and Sends Bill to Payer/Insurance Staff Manages Treatment Room Status «actor» Payer/ Insurance 180 Sample: UML Class Diagram and Domain Model This sample was prepared for Drexel INFO 620. Course description and goals are here. Physiological_data -patient_ID -temperature -blood_pressure 1 records 1..* Nurse -nurse_ID 1 1..* sees Patient Clerk -patient_ID -date_visit -med_number -ssn -fname -lname records -address -city -state 1 * -postal_code -phone -race -date_of_birth -height -weight -problem System works_on -clerk_ID -id 1..* 1 has 0..* Staff -staff_ID 1..* Room assigned_to 0..1 1 0..* Xray recorded-as -room_ID -assignment -status 1 1..* 1 -xray_ID -patient_ID -xray_date -xray_findings -xray_code 0..* 1 Test -test_ID -patient_ID -test_date -test_findings -test_code Diagnosis Doctor orders 0..* -service_ID -patient_ID -code -test_ID -xray_ID 1 1 1 1 1 -diagnosis_ID -patient_ID -date_of_init_diagnosis requires 1 Bill -bill_ID -patient_ID -bill_issue_date -service_ID -bill_total 1 requires 0..* 0..* Treatment -treatment_ID -trtmnt_date_start -trtmnt_type produces 1 0..* recorded-as makes -doctor_ID 1 orders 0..* has has 1 Service cleans * Prescription -rx_id -rx_date_start -rx_name -rx_dosage Register Patient Scenario :System :Clerk :LabAssistant :Radiologist :Nurse :Doctor :Staff logson(clerkID) authenticates(clerkID) entersPatientData patientID sendsPatient(roomID) roomID assignsDrtoRoom(drID, roomID) drID, roomID enters(physiologicalData) authenticates(dataRecord) schedules(testID) ordersXray(xrayID) schedules(xrayID) gets(testID) testID enters(testResults) authenticates(testResults) gets(xrayID) xrayID enters(xrayResults) authenticates(xrayResults) gets(testResults, xrayResults) testResults, xrayResults prescribes(treatmentID, prescriptionID) gets(roomIDstatus) roomIDstatus updates(roomIDstatus) authenticates(roomIDstatus) createsBill(services, testID, xrayID) billID 184 Sample: Press Release This sample was prepared for San Francisco State University (SFSU) Technical and Professional Writing (TPW) 400, Fundamentals of Technical and Professional Writing. The purpose for including it in my portfolio is to demonstrate competency in writing press releases. Details for this course are as follows: Description This course Introduces forms, methods, standards, and issues central to the work of career writers in the workplace. Students produce technical instructions, promotions, reports, and correspondence. Assignment Details This assignment focused on learning to write a press release for a virtual reality simulator. 5DT, Inc. 15375 Barranca Parkway, G-103 Irvine, CA 92618 CONTACT: Lisa Romanoski Sales Associate Technology Department Phone: 949-450-9044 Fax: 949-450-9045 Email: [email protected] July 7, 2009, 8:00 AM PST 5DT SIMULATOR PUTS THE “DRIVE” BACK IN DRIVERS’ ED Irvine, CA, July 7, 2009 – 5DT drives into the future with students behind the wheel of its news virtual reality simulators, engaging students in photorealistic drive scenarios with motion feedback. More drive time means more safety and fewer accidents, according to 5DT. The National Highway Traffic Safety Administration states that motor vehicle accidents account for at least 35% of all deaths. 5DT simulators complement on-road drivers’ education courses. Instructors can supervise from a separate computer or set pre-determined drive courses for additional after-hours training. Students navigate in and around other cars and objects. If a student turns or accelerates, they feel the steering wheel resist to turns or slip out of control. -- more -- PUTTING THE DRIVE BACK IN DRIVERS’ ED Page 2 The video-game like experience is a big attraction to students. Instructors see more students signing up for drivers’ education. “Sometimes students are either too nervous, their parents won’t let them, or they just aren’t interested in driving,” says Lowell County High School student Maxx Gavrich. “This is a big hook for them. It’s something new.” With only one in four high schools offering drivers’ education, according to the San Francisco Chronicle, 5DT simulators can provide an alternative to courses subject to rising insurance and gasoline costs. State funding of courses stopped in 1990. The initial purchase cost is the only cost. 5DT simulators are easy to program, resulting in minimal instructor training. 5DT develops, produces, and distributes customized virtual reality hardware, software, and systems, with emphasis on simulators and peripherals. With clients around the world, 5DT serves the automotive, defense, aviation, industrial, marine, mining, and medical industries. Additional information is available at http://www.5dt.com. --30-- 187 Sample: Instructions This sample was prepared for SFSU TPW 400. Course description and goals are here. The purpose for including it in my portfolio is to demonstrate competency in writing instructions. Assignment Details This assignment focused on the learning to write instructions. The subject was write instructions for attaching a ramsink to a video card. A ramsink is a device that helps cool the video card. Attach Super RAMsinks to a BFG Video Card Introduction Thank you for your purchase of Super RAMsinks. RAMsinks reduce video card heat, thereby improving performance. Attachment of a RAMsink will take approximately 60 to 90 minutes. Follow these instructions to attach a RAMsink to your video card. Familiarity with computer hardware and terminology is recommended. You should know how to remove and reinstall a video card. CAUTION! Computer Wizardry, Inc., is not responsible for any damage to hardware caused by this installation. Use a well-ventilated space for all tasks. Required Items 1. Verify adhesive and thermal compound mixing and application instructions with manufacturer’s specifications. 2. Do not reinstall the video card in the computer for at least 12 hours after curing. 3. You will need the following items before you begin:  Super RAMsinks  BFG Video Card  600 Grit Sandpaper  Cotton Swabs and Ball  Masking Tape  A toothpick or other mixing tool  Old, clean plastic lid on which to mix the adhesive and compound  Arctic Silver Premium Silver Thermal Adhesive, or equivalent (adhesive)  Arctic Silver Ceramique Premium High Density Thermal Compound, or equivalent (compound) Recommended Items for Oxidation Removal  Brasso Metal Polish, 8 oz., or equivalent; or steel wool  Rubbing Alcohol  Rust-Oleum Crystal Clear Enamel Spray, or equivalent (sealant) I. Oxidation Removal � If you are using tin-plated RAMsinks, please proceed to section II. � If you are using copper RAMsinks, check for oxidation. Oxidation is caused by air exposure, resulting in a greenish tint. We recommend you remove oxidation for optimum performance. Your RAMsink will still work if you choose not to remove oxidation. Remove oxidation as follows: 1. Choose Brasso Metal Polish, steel wool, or 600 Grit Sandpaper for sanding. � If you choose Brasso Metal Polish, soak a cotton ball in solution for sanding. 2. Gently sand all surfaces. 3. Clean all surfaces with a cotton swab tip soaked in rubbing alcohol. 4. Apply a light coat of sealant to all surfaces except the mounting surface (bottom). 5. Allow sealant to dry at room temperature for 30 minutes. II. Prepare Mounting Surface 1. Gently sand the top of the RAMsinks with 600 Grit Sandpaper. 2. Clean all surfaces with a cotton swab soaked in rubbing alcohol. 3. Tape the edges of the chips with masking tape to ensure no adhesive gets on them. CAUTION! Do not allow masking tape to adhere to surface of video card during installation. III. Adhesive Mix (Mix) 1. 2. 3. 4. 5. Using a toothpick, mix equal parts resin Part A and curing agent Part B on a plastic lid. Mix only enough resin and curing agent needed for application. Apply in approximately 3 minutes after thorough stirring. Ensure thorough stirring by scrapping lid as you mix. Immediately add one drop of thermal compound to mix from step 1. IV. Attach RAMsink to Video card 1. 2. 3. 4. 5. 6. Using a toothpick, apply a thin coat of mix to the bottom of the RAMsink. Firmly press the RAMsink to the video card for 1 minute. Allow 1 hour for curing of RAMsink to video card. Remove masking tape from chips after 1 hour. Allow 12 hours for additional curing of RAMsink to the video card. Reinstall the video card. 190 Sample: Feasibility Study This sample was prepared for SFSU TPW 400. Course description and goals are here. The purpose for including it in my portfolio is to demonstrate competency in writing a feasibility study. PrimeCare, Inc. To: From: Subject: Date: Jan Debliss, Personnel Director Lisa Romanoski, Special Assistant to Walter Henocker Corporate Child Care Feasibility Study July 30, 2009 High absenteeism can lower the quality of resident care at PrimeCare’s twelve California nursing facilities. Staff must assist more patients than they are typically assigned in order to cover for absent employees. Existing and former staff cite child care difficulties as the greatest impediment to coming to and remaining at work during the day. In order to ensure quality care, day shift operations must be executed with 96 employees per the company business plan. We currently have seven vacancies among our day shift staff. Using an internet-based literature search and telephone interviews, I’ve determined that these alternatives are most appropriate for our budget and available space at the nursing homes: 1. Onsite child care developed by PrimeCare. 2. Onsite child care through a consortium program for PrimeCare and others. 3. Referral program for offsite child care using a local family day care provider. I identified the resources and licensing we’ll need through conversations with both Judy Krieger and Shelly Meyer. Judy Krieger is a Center Advocate at Bananas Inc., a child care resource and referral service in northern Alameda County. Bananas Inc. provides cost and child care information to parents and caregivers. Shelly Meyer, Client Outreach Manager at Bright Horizons, provided information on feasibility options given our available resources. Bright Horizons provides feasibility studies for the establishment of employer-sponsored child care onsite child care. I used the following criteria to determine if an alternative is feasible: 1. Does the cost fall within the monthly $4,000 PrimeCare budget? 2. Do staff out-of-pocket expenses exceed a $120 weekly child care budget? 3. Can we reduce our absenteeism rates and costs by 75%? Criteria 1: PrimeCare Budget For Criteria 1, the monthly $4,000 budget is a lump sum amount provided by PrimeCare. Criteria 2: Affordability I created Criteria 2, affordability, based on my research. I found that not spending any money on child care is unrealistic. According to internet sources, some people devote 30-40% of their income to child care expenses. To determine if an alternative is affordable to our staff earning, I’ve established a minimum weekly child care budget of $120. This represents 25% of an annual salary for staff working 40-hour work weeks at a rate of $12 an hour. Criteria 3: 75% Reduction in Absenteeism Rate and Cost Criteria 3 is company cost savings from reduced absenteeism. Absenteeism costs PrimeCare money because we continue to pay salaries and benefits to absent staff. If we provide onsite child care, we would expect to see reduced absenteeism and cost savings. An alternative must result in a 75% reduction in absenteeism rate and cost to be a feasible option for us. Using the Washington Employers Association Method, our current monthly absenteeism rate is 0.97%. HR.com cites 2.1 percent as an “all-time high” for most employers. The money we lose to absenteeism is approximately $3,024 a month. To reach a goal of 75% reduction, the absenteeism rate and cost needs to fall to 0.24% and $763, respectively. Assumptions We’re going to need furniture and a first aid kit for the child care center. This one-time startup cost could be as high as $6,030. The list of items we’ll need can be found at the end of this report. I used Amazon.com to obtain price information. I assumed no fees for licensing, advertising, and insurance. You mentioned previously that our insurance already provides coverage for in-house child care service. We won’t need to advertise if the center is only for PrimeCare staff use. We also don’t need to obtain a state license. A loop hole in California law allows some child care centers to operate without a license if parents are onsite, according to Bananas Inc. Monthly operating costs for one child care center could be as high as $14,293. This cost includes supplies, food, and the cost of six caregivers. If we provide onsite care for 30 toddlers, we will need six caregivers to work in the center. California law requires a ratio of six children to one caregiver for this age group. The monthly cost of one caregiver is approximately $1,728, including benefits. I assumed that the caregiver earns a California minimum wage rate of $8 an hour and works 40 hours a week. I assumed benefits are approximately 35% of the monthly salary. This information is listed at the end of this study. Costs are for one San Francisco Bay Area child care facility. Due to the high cost-of-living, I assume costs are an acceptable representation of other areas. Costs will vary, but I expect them to be lower. Salaries are not subject to cost-of-living increases. ALTERNATIVE 1: ONSITE CHILD CARE DEVELOPED BY PRIMECARE PrimeCare can provide free onsite child care for 30 children, including all equipment, furniture, and meals or snacks. Criteria 1: Cost As mentioned previously, startup costs can be as much as $6,030. Monthly costs are approximately $14,293. These costs exceed PrimeCare’s budget. Alternative 1A We can reduce startup costs by seeking donations or requiring staff to provide their own supplies and meals. We will stay within budget if we reduce the number of caregivers. Two caregivers cost $3,456. However, caregiver reduction results in reduced child space availability. State law requires one caregiver be designated to six children. Space would be limited to 12 children. Criteria 2: Affordability Staff can afford Alternative 1. There are no out-of-pocket expenses for staff. Criteria 3: 75% Reduction in Absenteeism Rate and Cost Absenteeism should be reduced by 100% with onsite daycare. This may not be possible because of child care issues. I assume there will be at least five days each month that an employee may miss because of child care issues. At least three employees may be absent. Using these assumptions, the absenteeism rate is reduced to 0.26%. We do not reach a 75% reduction in absenteeism rate (goal: 0.24%). The monthly cost we incur for absent staff under this scenario is $1,360. To save money, we want a 75% reduction in monthly staff costs (goal: $756). We do not reach our goal with onsite child care. Figure 8. Monthly Absenteeism Rate with Onsite Child Care Benefit Days Lost Through Absence per Month 5 Employees on the First Day of the Month 96 Employees on the Last Day of the Month 93 Average Headcount per Month 94.5 Available Workdays per Month 20 Average Number of Workdays per Month 1,890 Rate 0.26% GOAL 0.24% Figure 9. Monthly Absenteeism Cost Savings Hours Lost to Absenteeism Per Month Wage/Salary Per Hour Benefits Per Hour Compensation of Employee Lost per Hour Compensation Lost to Absent Employees Other Costs Incidental to Absenteeism Cost GOAL 40 $12 $4 $16 $640 $720 $1,360 $756 ALTERNATIVE 2: ONSITE CHILD CARE THROUGH A CONSORTIUM PROGRAM PrimeCare can partner with other companies to form a child care consortium. Other companies provide startup costs, meals or snacks, equipment, and furniture in exchange for facility spaces. We can provide staff and healthcare, but we have only one room. Thirty PrimeCare children will need care. Other companies in our consortium program may need care for as many as 60 children. If 90 children need care, we will need more space, equipment, and caregivers. Criteria 1: Cost If we assume other companies provide the startup, architectural, and construction fees, our cost is monthly operation of the facility: $25,920. These costs exceed PrimeCare’s budget. Alternative 2A We can be totally self-supporting after the first year by providing a sliding-scale fee schedule like the one in Figure 4. The fee schedule could generate monthly revenue as high as $95,035. This will cover most, if not all, of our costs. Criteria 2: Affordability Our staff’s hourly rate of $12 may be low enough to qualify for a subsidized rate lower than the rates shown in Figure 4. I assume other users are paid higher hourly rates, which will offset costs for our staff. As such, staff can afford Alternative 2 and 2A. Criteria 3: 75% Reduction in Absenteeism Rate and Cost Absenteeism rates and costs are expected to be reduced in a similar manner to the onsite child care alternative. Figure 10. Monthly Operating Costs for Alternative 2 Item Qty Arts and Crafts Supplies 0 Disposable Changing Pads (36 Count Box) 0 Cleaning Products 0 Diapers (Economy Pack) 0 Meals for 30 Children 0 Caregivers (Salary and Benefits) 15 Figure 11. Fee Schedule Example Age Infants (6 weeks to 18 months) Toddlers - Preschool (19 months to 6 years) School Age (over 6 years) Unit LS EA LS EA LS EA Monthly $1,332 $1,077 $760 Weekly $333 $269 $190 Figure 12. Expected Monthly Revenue Age Number Infants 5 Toddlers - Preschool 75 School Age 10 TOTAL 90 Revenue $6,660 $80,775 $7,600 $95,035 Cost $200 $15 $75 $40 $2,700 $1,728 TOTAL Total $0 $0 $0 $0 $0 $25,920 $25,920 ALTERNATIVE 3: REFERRAL PROGRAM FOR OFFSITE CARE We can develop an internal referral program and find family child care homes for staff. One staff member can operate the program. Providers are state-regulated and may offer:    Services similar to nursery schools Bilingual environments Drop-in service (backup care) Criteria 1: Cost We can offer this service for approximately $2,080 or less. This is the monthly salary of one full time staff member. Operating expenses, including computer and telephone usage, are not expected to increase costs associated with this activity. Criteria 2: Affordability Based on data presented in Figure 6, Oakland area family child care providers charge an average of $48 per day, or $240 per week, including meals. Figure 6 lists the following information:      Provider name Age of the children they care for Number of children they care for during the day Hours of operation Daily cost The costs listed in Figure 6 indicate that staff cannot afford to use family child care providers. Alternative 3A We can issue $120 vouchers to reduce costs. Staff who works on the referral program can be reduced to a 32-hour work week. Savings result in a budget of $3,984 (Figure 7). Criteria 3: 75% Reduction in Absenteeism Rate and Cost Absenteeism may be greater without onsite child care. I assume that at least seven and a half days each month will be missed by an employee. At least four employees may be absent. Absenteeism rate is 0.40% under this scenario. Absenteeism cost is $1,680. We do not reach a 75% reduction in absenteeism rate or cost (goals: 0.24%, $763). Figure 13. Oakland Area Family Child Care Providers: Children in Care, Hours, Cost Number of Provider Age of Children Children Hours Daily Cost Cared For Gwendolyn Friend 1 month - 12 years 6 7:30 AM - 5:30 PM $45 Phuong Le 3 months - 12 years 8 7:30 AM - 5:30 PM $70 Tracy Mooreland 3 months - 12 years 14 6:15 AM - 9:00 PM $40 Guadalupe Herrea 6 months - 12 years 8 7:30 AM - 5:30 PM $36 Figure 14. Budget with a Voucher System Weekly Average rate 30 Children Need Care PrimeCare Covers Half the Cost Staff Hours: $12/hr x 32 hrs/week BUDGET $240 $7,200 $3,600 $384 $3,984 Figure 15. Monthly Absenteeism Rate Days Lost Through Absence per Month Employees on the First Day of the Month Employees on the Last Day of the Month Average Headcount per Month Available Workdays per Month Average Number of Workdays per Month Rate GOAL 7.5 96 92 94 20 1,880 0.40% 0.24% Figure 16. Monthly Absenteeism Cost Savings Total Hours Lost to Absenteeism per Month Average Wage/Salary per Hour per Employee Cost of Benefits per Hour per Employee Compensation of Employee Lost per Hour Total Compensation Lost to Absent Employees Other Costs Incidental to Absenteeism 1 Cost GOAL 60 $12 $4 $16 $960 $720 $1,680 $763 SUMMARY Onsite childcare through a consortium program, with a fee schedule, and an in-house referral program for offsite child care meet all criteria and are feasible (Figure 10). In general, feasibility of this benefit is constrained by cost. Next steps in our feasibility process could include a patient care quality assessment, staff surveys, and a more detailed budget analysis. I recommend we proceed with this effort. Figure 17. Feasibility Summary of Onsite Child Care Alternatives 1 Onsite Care 2 Consortium Program 2A Consortium Program with Fees 3 Referral Program 3A Referral Program with Vouchers X = Does not meet criteria.  = Meets criteria. Budget Affordability x  x    x  x  Absenteeism Reduction      ATTACHMENT ASSUMPTIONS AND METHODS Absenteeism Rate We have at least 18 absent staff per month. We start each month with a full staff of 96. Our average headcount per month is 89. Average head count is the number of staff who start each month, added to the number remaining at the end of the month, divided by two. There are 20 workdays in a month, assuming staff work five days a week and there are four weeks in a month. The average number of workdays per month is the average headcount multiplied by the number of workdays: 1,850. Eighteen lost days divided by the number of available days yields the absenteeism rate: 0.97%. Absenteeism Cost We have at least 18 absent staff per month. Absent staff would typically work eight hour shifts. We lose 144 hours a month to absenteeism. Hourly compensation lost per absent staff is $16. Monthly compensation lost to absent staff is $2,304. Other costs associated with absenteeism can include cost to pay overtime staff. Overtime pay can cost us as much as $720 a month, assuming staff works an extra two hours a day for a five day work week. There are four weeks in a month. Absenteeism costs PrimeCare $3,024 a month. Figure 1. Startup Costs for Onsite Child Care Item Licensing fees Insurance Advertising First aid/CPR Certification First Aid Kit High Chairs Booster Seats Nap mats Bedding Playpens Portable Cribs Toys Books Child-sized Tables and Chairs (Set) Diaper Disposal Containers Step stools Potty Training Chairs Qty 0 0 0 6 15 15 15 30 30 3 3 1 1 7 2 5 5 Unit EA LS LS EA EA EA EA EA EA EA EA LS LS EA EA EA EA Cost $0 $0 $0 $75 $20 $75 $40 $25 $15 $150 $150 $200 $200 $100 $40 $30 $25 TOTAL Total $0 $0 $0 $450 $300 $1,125 $600 $750 $450 $450 $450 $200 $200 $700 $80 $150 $125 $6,030 Figure 2. Monthly Operating Costs for Onsite Child Care Item Qty Arts and Crafts Supplies 1 Disposable Changing Pads (36 Count Box) 50 Cleaning Products 1 Diapers (Economy Pack) 5 Meals for 30 Children 1 Caregivers (Salary and Benefits) 6 Unit LS EA LS EA LS EA Cost $200 $15 $75 $40 $2,700 $1,728 TOTAL Total $200 $750 $75 $200 $2,700 $10,368 $14,293 202 Sample: Process Description This sample was prepared for SFSU TPW 480, Writing Technical Documentation. Details for this course are as follows: Description This course focuses on design and development of standard types of technical documentation, such as project plans, process descriptions, procedures, tutorials, and usability tests. Topics include: audience analysis, writing style, and best practices. Assignment Details This assignment involved writing a process description for how to use my cell phone. San Francisco State University Technical and Professional Writing Program TPW 480 To From Date Dr. Bob Dvorak Lisa Romanoski October 5, 2009 Subject Process Description for How to Use my Cell Phone The target audience is anyone who wants to borrow my cell phone. Abstract This process description describes how to use my cell phone, an LG Venus, and is intended for friends and family familiar with cell phone usage. The LG Venus is a slider phone that has a hidden key pad beneath a touch screen that slides up and down. All functions require the use of both a traditional key pad and function menus accessible only by touching the screen. The phone has many features, including messaging, voice mail, internet access, a music player, and gaming. This process description focuses on how to use the phone to make a call, send a text message, and access the internet. Process Phone Calls: When a user first holds the phone, the screen will be turned off because the phone is trying to save battery power. To activate the phone to place a call, a user presses the upper unlock button on the right side of the phone. This button is also labeled “Music.” Once activated, the phone display shows a two-part screen. The upper half is a display screen, and the lower half is a menu screen used to navigate to various functions. The menu screen displays these touch buttons: “Message,” “Contacts,” “Shortcut,” and “All Calls.” This is the standard default display of the phone before a function is executed. To place a call, a user must slide the screen up to reveal the key pad. The user enters a phone number using the key pad and then must touch “Call” at the bottom left of the screen. The call is ended by touching “End” on the screen or sliding the screen down. Text Messaging: For text messaging, the user must slide the screen up to access the key pad and touch “Message” on the menu screen. The display screen then lists the following options: 1 Text Message, 2 - Picture Message, or 3 - Video Message. The user selects one of these three items by pressing the corresponding number on the key pad. Process Description, Continued Page 2 After selecting the message type, the user enters a phone number with the key pad in one of several lines displayed on the screen. The menu screen shows “123,” “Add,” “Back,” and “Contacts.” An “Ok” button is located in the middle of the menu functions screen with four navigation arrows on all sides: up, down, left, and right. A user presses either the “Ok” button or the down arrow to begin typing in the text box after entering a phone number. The “123” button can be used to add words, lower- and uppercase text, and symbols. “Add” allows a user to add a phone number from the contacts list, a recent phone call, or a previouslydefined group. “Contacts” lists contact information for friends, family, and colleagues. “Back” allows a user to return to the previous screen. Once the user has navigated to the text box area, he or she will type a message using the key pad. There are three letters per key on the key pad. A user presses the key until the letter he or she wants appears on the screen. The user can access symbols and numbers through the “Abc” button in the upper left corner of the menu display screen. When a user presses this button, six options are displayed on the screen: 1 - Word, 2 - Abc, 3 - ABC, 4 - 123, 5 - Symbols, and 6 - Quick Text. The user selects an option by pressing the corresponding number on the key pad. After typing the message, the user touches “Send” in the middle of the screen to send the message. The screen displays “Message Sent” when the message is sent successfully. The phone then displays the initial start screen. Internet Access: To access the internet, a user selects “Menu” from the touch screen. The screen displays “My Music,” “Get It Now,” “ Messaging,” “ Contacts,” “Recent Calls,” and “Settings and Tools.” The user would navigate to “Get It Now” using the up and down arrows in the menu screen and pressing the “Ok” button. From the display, the user would choose “News and Info” by using the navigation arrows and pressing “Ok” or selecting the corresponding number, 4. Upon activation, the phone begins an internet connection. The user may choose from news, email, entertainment, sports, weather, and search functions by using the key pad to select a number corresponding to an item on the display screen. The user may also use the navigation arrows to highlight a selection. The selection is activated by pressing the “Ok” button. To exit an internet session, a user presses the “Clr” button on the key pad. This returns the user to the initial start screen. Conclusion The process description described herein explains how to use my LG Venus cellular phone to make a phone call, send a text message, or browse the internet. With a state-of-the-art touch screen, this cellular phone is easy to use and allows for quick navigation for a variety of features. 205 Sample: Documentation Plan for an SOP This sample was prepared for SFSU TPW 480. Course description and goals are here. Assignment Details This assignment involved writing a documentation plan for a standard operating procedure. San Francisco State University Technical and Professional Writing Program TPW 480 To From Date Dr. Bob Dvorak Lisa Romanoski October 12, 2009 Subject Documentation Plan for Data Management Standard Operating Procedure Purpose I propose to write a standard operating procedure (SOP) for clinical trial data management. The purpose of the SOP is to provide guidance for managing data and ensuring clinical trial data are collected, verified, and analyzed in compliance with the most current United States Department of Human Services, Food and Drug Administration (FDA), standards and guidance. The SOP will include guidance on:  Source documentation and retention  Computer access  Audit trails, date and time stamps  External security safeguards  Data entry, retrieval, and processing  Backup procedures  Data protection The SOP will be written using the template provided on the I-Learn site for Technical and Professional Writing (TPW) 480. The revision history within this template will be used to track SOP drafts. Audience The target audience is clinical trial personnel authorized to enter, process, and/or retrieve clinical trial data. Resources To meet documentation requirements, I need the following:  Internet access for research  General information on overall clinical trial practice  General information on commercial data management software  Most current FDA standards/guidance  Most current International Conference on Harmonisation (ICH) of Good Clinical Practice standards/guidance  My personal computer  Microsoft Word on my personal computer  October 19, 2009, peer review comments  November 2, 2009, instructor review comments L. Romanoski, Memo on SOP Page 2 Budget Budget is not applicable to this particular project. Deliverables Documentation Plan for Procedure on October 12, 2009 Draft I Procedure on October 19, 2009 Draft II Procedure on November 2, 2009 Final Procedure on November 30, 2009 Contingencies Final submission of SOP is contingent on receipt of peer and instructor review comments by November 9, 2009. Anticipated delays in the schedule will be communicated to Dr. Dvorak via email at least two days prior to each deliverable date. 208 Sample: Standard Operating Procedure This sample was prepared for SFSU TPW 480. Course description and goals are here. The purpose for including it in my portfolio is to demonstrate competency in writing standard operating procedures. Assignment Details The purpose of writing this document was to demonstrate ability to write standard operating procedures and work with standardized forms. Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 1 of 12 Standard Operating Procedure for Data Management FD-001, Release 3 SOP Scope: Poe Biotechnology Data Management Standards Functional Group: Data Management Author: Lisa Romanoski Document Supersedes: N/A Approved by: Name Approval Date «approved_by » «approval_date» «approved_by_1 » «approval_date_1» «approved_by_2 » «approval_date_2» «approved_by_3 » «approval_date_3» «approved_by_4 » «approval_date_4» «approved_by_5 » «approval_date_5» «approved_by_6 » «approval_date_6» «approved_by_7 » «approval_date_7» «approved_by_8 » «approval_date_8» «approved_by_9 » «approval_date_9» «approved_by_10 » «approval_date_10» «approved_by_11 » «approval_date_11» Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 2 of 12 I. Purpose This Standard Operating Procedure (SOP) describes the procedure for managing data and ensuring clinical trial data are collected, verified, and analyzed in compliance with the most current United States Department of Human Services, Food and Drug Administration (FDA) standards and guidance. This SOP is needed to ensure that Poe Biotechnology follows proper protocol in recording clinical trial study data in pursuit of FDA drug approval. II. Scope This SOP references the Poe Biotechnology Data Management Standards and the FDA’s guidance and regulations on computerized systems and electronic records and signatures. This SOP covers source documentation and retention; the data management process; databases; external security safeguards; computer access; data entry, processing, and validation; data protection; audit trails, date and time stamps; and electronic record backup and recovery. This procedure is to be read by Principal Investigators, the Data Manager, and data entry clerks. III. responsibility 1.1 1.2 Principal Investigators (PIs) are responsible for: 1.1.1 The conduct of the clinical trial at a trial site. 1.1.2 The team of individuals at the trial site. 1.1.3 Execution of the trial as outlined in the clinical trial contract. 1.1.4 Reporting project progress as outlined in the clinical trial contract. 1.1.5 Informing study subjects of the nature of the trial and risk factors. 1.1.6 Comply with all Poe Biotechnology policies and procedures related to clinical trials and project management. 1.1.7 Comply with all sponsor rules, regulations, and terms and conditions of the clinical trial contract. 1.1.8 Comply with all FDA inquiries, audits, site inspections, and requests for information. The Data Manager (DM) is responsible for: 1.2.1 Overseeing the completeness, accuracy and internal consistency of the data for the trial. 1.2.2 Performing computer database operation system checks. 1.2.3 Training and education for data entry clerks and others who will use the database. 1.2.4 Protection and appropriate use of electronic signatures. 1.2.5 Provision of computer log-in access codes to data entry clerks and other authorized individuals. 1.2.6 Generation of data tabulations, profiles, and listing to support other medical and clinical colleagues with the monitoring and review of the data. 1.2.7 Generation of status reports to inform the study management team of study progress. Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 3 of 12 1.2.8 Keeping the study management team fully and promptly updated on the status of data flow and data quality through the lifecycle of the clinical trial/disease registry. 1.2.9 The creation of the Case Report Form (CRF) and oversight for the user testing of the clinical database which is created from the CRF. 1.2.10 The completeness, accuracy, and internal consistency of all clinical data collected in the trial, including laboratory safety data and data from ancillary data sources such as academic labs, electrocardiograms (ECGs), pharmacokinetic (PK) data, etc. 1.2.11 Ensuring that patient data are clean and complete in preparation for any agreed reporting event. 1.2.12 Ensuring all coded items in the study are promptly and consistently coded. 1.2.13 Locking of the data in the study/registry, finalizing the applicable documentation in accordance with relevant SOPS, and overseeing the archiving of documentation and clinical data. 1.3 Data entry clerks are responsible for: 1.3.1 Ensuring that all study data are processed and validated in accordance with study guidelines. 1.3.2 Entering data from reports and clinical study documents into the electronic tracking system. 1.3.3 Scanning documents and verifying data entry work to ensure accuracy. IV. Associated Forms 1.4 Case Report Form 1.5 Discrepancy Form V. Definitions 1.6 A case report form (CRF) is a printed or electronic document specifically designed to record observations of study participants. 1.7 A discrepancy form is used by the DM in his or her review of CRFs to note missing data, incomplete fields, or data outside the normal ranges. This form may also be used by the DM to note any unauthorized entries into the secure computer work room. Discrepancy forms are submitted to the PI for review and/or resolution. 1.8 Essential documents are documents that fall into three groups according to the stage of the trial during which they are generated: 1.9 1.8.1 Before the clinical phase of the trial commences 1.8.2 During the clinical conduct of the trial 1.8.3 After completion or termination of the trial Before-trial documents include: 1.9.1 Investigator’s brochure 1.9.2 Signed protocol and amendments Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 4 of 12 1.9.3 Informed consent forms, any other written information, and advertisement for subject recruitment 1.9.4 Financial records 1.9.5 Insurance statement 1.9.6 Signed agreements between involved parties 1.9.7 All documentation pertaining to Independent Review Board/Independent Ethics Committee (IRB/IEC) review and approvals 1.9.8 IRB/IEC composition 1.9.9 Regulatory authority(is) authorization/approval/notification of protocol 1.9.10 CVs and other documents evidencing qualifications of investigators and subinvestigators 1.9.11 Normal value(s)/range(s) for medical/laboratory/technical procedure(s) and/or test(s) included in the protocol 1.9.12 Certifications of facilities to perform required test(s) and support reliability of results 1.9.13 Sample of label(s) attached to investigational product(s) and trial-related materials 1.9.14 Certificate(s) of analysis of investigational product(s) shipped 1.9.15 Decoding procedures for blinded trials 1.9.16 Master randomization list 1.9.17 Pretrial monitoring report 1.9.18 Trial initiation monitoring report 1.10 During-trial documents include: 1.10.1 Investigator’s brochure updates 1.10.2 Any revisions to CRFs, informed consent forms, any written information provided to subjects, and advertisements for subject recruitment 1.10.3 Correspondence from IRBs 1.10.4 Regulatory authorizations for protocol amendments 1.10.5 CVs for new investigators or subinvestigators 1.10.6 Updates to normal values/ranges 1.10.7 Updates of procedures/tests 1.10.8 Documentation of shipments 1.10.9 Letters, meeting notes, and telephone call notes 1.10.10 Signed informed consent forms 1.10.11 Source documents 1.10.12 Signed, dated, and completed CRFs 1.10.13 Documentation of CRF corrections Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 5 of 12 1.10.14 Notification by PI to sponsor of serious adverse events and related reports 1.10.15 Notification by sponsor and/or PI to regulatory authority(ies) and IRBs/IECs of serious adverse drug reactions and other safety information 1.10.16 Notification by sponsor to PI of safety information; interim or annual reports to IRC/IEC and authority(ies) 1.10.17 Subject enrollment log(s) 1.10.18 Investigational product(s) accountability at the site 1.10.19 Signature sheet 1.10.20 Record of retained body fluids/tissue samples 1.11 After-trial documents include: 1.11.1 Investigation product accountability at the site 1.11.2 Documentation of investigational product(s) destruction 1.11.3 Completed subject identification code list 1.11.4 Audit certificate 1.11.5 Final trial close-out monitoring report 1.11.6 Treatment allocation and decoding documentation 1.11.7 Final report by PI to IRB/IEC and regulatory authority(ies) 1.11.8 Clinical study report 1.12 Protected Personal Information is any patient identifiable data or any information that can directly or indirectly lead to the identification of a living person, such as an individual's name, address, e-mail, telephone number, license number, medical identification number, photograph, or other identifying characteristic. The identification can occur by reference to one or more factors specific to the individual's physical, physiological, mental, economic, cultural or social identity. Personal information does not include information that has been anonymized, encoded or otherwise stripped of its identifiers, or information that is publicly available, unless combined with other non-public personal information. 1.13 Relevant records are written procedures, membership lists, lists of occupations/affiliations of members, submitted documents, minutes of meetings, and correspondence. 1.14 Source data is all information in original records and certified copies of original records of clinical findings, observations, or other activities in a clinical trial necessary for the reconstruction and evaluation of the trial. 1.15 Source documents are original documents, data, and records, including: 1.15.1 Hospital records 1.15.2 Clinical and office charts 1.15.3 Laboratory notes 1.15.4 Memoranda 1.15.5 Subjects' diaries or evaluation checklists 1.15.6 Pharmacy dispensing records Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 6 of 12 1.15.7 Recorded data from automated instruments 1.15.8 Copies or transcriptions certified after verification as being accurate and complete 1.15.9 Microfiches, photographic negatives, microfilm or magnetic media, and x-rays 1.15.10 Subject files 1.15.11 Records kept at the pharmacy, at the laboratories, and at medico-technical departments involved in the clinical trial VI. references 1.16 FDA, 21 CFR 11, “Electronic Records, Electronic Signatures; Final Rule.” Federal Register Vol. 62, No. 54, 13429, March 20, 1997. 1.17 FDA, Compliance Program Guidance Manual, “Compliance Program 7348.810 – Bioresearch Monitoring – Sponsors, Contract Research Organizations and Monitors,” February 21, 2001. 1.18 FDA, Computerized Systems Used in Clinical Investigations, May 2007. 1.19 FDA, E6 Good Clinical Practice: Consolidated Guidance, ICH, April 1996. 1.20 FDA, General Principles of Software Validation; Final Guidance for Industry and FDA Staff, January 11, 2002. 1.21 FDA, Guideline for the Monitoring of Clinical Investigations, January 1998. 1.22 FDA, Part 11, Electronic Records; Electronic Signatures – Scope and Application, August 2003 (Lists other documents referred to, appropriate regulations, and/or sources of information relevant to the SOP.) VII. Safety These safety measures apply to all personnel who use computers for data management tasks. Working on a computer for long periods of time can cause inflammation of tendons, nerve sheaths and ligaments and damage to soft tissues. Neck and shoulder pain and stiffness can occur from improper placement of the computer monitor, mouse or document you are working from. If these items are not placed correctly, the muscles of your neck and shoulders are constantly working to keep the head and arms in an awkward position. Phone use while keying can also contribute to neck and shoulder pain from cradling the phone to your ear. 1.23 Position of the wrist must be neutral, or straight. In order to achieve a neutral position, the keyboard needs to be placed so the arms bend at approximately a 90-degree angle. 1.24 Avoid resting the wrist or forearm on a hard surface while keying. This is called contact stress and must be avoided. 1.25 Your line of vision should hit the top of the monitor, the mouse should be next to the keyboard at the same height, and a document holder should be used to make sure paperwork is at the same distance, angle and height as the monitor. 1.26 Arrange the computer equipment in a straight line so you are not twisting your back. 1.27 To reduce telephone related muscle stress, use the speaker function or purchase a headset. 1.28 Chairs should be adjusted so the feet can be placed squarely on the ground or a footrest. 1.29 To reduce glare, tilt the screen down slightly so that that overhead lighting does not hit the screen. Place monitors at right angles to windows so glare does not hit the screen or the user’s Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 7 of 12 eyes. Use blinds or curtains for controlling sunlight glare. Reduce room lighting to half-normal office levels and use task lighting for paper work and other tasks. 1.30 Take breaks by looking away from the screen for ten seconds, or do other work and give your eyes a rest. VIII. Data Management 1.31 Process 1.31.1 The data management process involves evaluating data collected using CRFs. CRFs are transferred into electronic format to allow statistical analysis to be conducted. 1.32 Databases 1.32.1 Once the CRF has been designed and approved in accordance with the protocol and has been approved, the PI (or delegated individual(s)) will set up a new trial database using Oracle Clinical. Oracle Clinical will be used to enter clinical data, monitor trial progress, and track source document verification. 1.33 External Security Safeguards 1.33.1 All authorized users and data entry clerks will obtain individual security work badges and key codes from the DM. 1.33.2 Security work badges must be worn at all times and displayed in one of three visible locations: on a chain worn round the neck, attached to a lapel, or attached to a belt loop. Do not cover the badge with clothing. 1.33.3 The key code must be entered to access the room containing the secure computer work stations. The security system will electronically tag each entry and exit with a date and time stamp. 1.33.4 Security cameras in the hallway and within the work room will monitor entry and exit at all times. These cameras will be monitored 24 hours a day and 7 days a week by security personnel, who will be looking for clearly displayed security badges. 1.33.5 Do not allow unauthorized personnel into the work room. Security personnel will retain any individuals caught entering the room without security work badges. 1.33.6 Do not download data onto any portable electronic device, including laptops, cell phones, CDs, or USB portable flash drives. 1.33.7 Data may be downloaded only into secure project folders within the network. Downloads must be consistent with current project tasks, such as statistical analysis. 1.33.8 The DM will download weekly a list of entry and exit date and time stamps for all key codes entered into the key pad. The DM will verify the key codes belong to authorized users and data entry clerks. 1.33.9 The DM will also download weekly a database activity report. This report will show computer login and logout information, date and time stamps, and any downloads that may have taken place during the work week. The DM will check that data downloads are consistent with the project schedule and work tasks. 1.33.10 The DM will note all database activity and any data downloads in a weekly memo to the PI. This memo will be emailed to the PI no later than 9 AM every Monday morning of the subsequent work week. Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 8 of 12 1.34 Computer Access 1.34.1 Obtain computer log-in access codes and passwords from the DM. 1.34.2 Only log in to secure computer work stations. 1.34.3 Only one individual will enter CRF data. 1.34.4 Data entry will be entered as seen on the CRF without interpretation or modification. 1.34.5 Log out immediately after completion of tasks. 1.34.6 Obtain print-out sheet from adjacent printer that shows the data and time of log-in and log-out. 1.35 Data Entry 1.35.1 The CRF is given to the DM, who will date, stamp, and review the form for any missing data, incomplete fields, or data outside normal ranges. 1.35.2 If there is missing data, incomplete fields, or data outside the normal ranges, the DM will submit the original CRF and a data discrepancy form explaining the issue to the PI by the end of that work day. The PI will investigate the matter and provide a data correction sheet to the DM within two weeks from date of submission of memo. The DM will then give the CRF and correction sheet to the data entry clerk for entry into the database. The DM will also record all corrections in the case files. 1.35.3 Upon completion of this process, log in to the database using a designated, secured computer work station. 1.35.4 Enter the data. 1.35.5 Apply coding to patient procedures using the Current Procedure Terminology (CPT) procedure codes. 1.35.6 After entering data, perform a visual check to compare what was recorded on paper CRF and what was entered on the screen. You may go to any screen while still logged in to re-enter data. 1.35.7 Log out of the database immediately following data entry. 1.36 Data Processing 1.36.1 Obtain the data processing assignment from the PI. 1.36.2 Log in to a designated, secure computer work station. 1.36.3 Perform the assignment, keeping data secure and confidential at all times. 1.36.4 Log off the computer work station immediately after processing. 1.37 Data Validation 1.37.1 Data validation ensures the most accurate validated data set is provided for statistical analysis. Data validation will be completed at three stages during the trial: when CRFs are completed by the PI; when data are entered into the database by data clerks; and when data have been entered and are available for the data manager. 1.37.2 When CRFs have been completed by the PI: 1.37.2.1 Independent monitors will perform data validation in this case. Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 9 of 12 1.37.2.2 The independent monitors will obtain the original patient’s records. 1.37.2.3 Compare the records to the data entered into the CRFs. 1.37.2.4 If discrepancies are noted, fill out a discrepancy form. 1.37.2.5 Submit the discrepancy form to the PI and the DM. 1.37.2.6 The PI and DM will both initial and date the change on the CRF. 1.37.2.7 The DM will then assign a data entry clerk to make the change in the database. 1.37.3 When data have been entered in the database by data entry clerks: 1.37.3.1 The automated Check Program will be activated when data clerks are entering data at all times. The Check Program is the database software’s own internal check for invalid data entries. It will provide warnings to the data entry clerks when values are entered outside of the expected range, or if the type of values entered is incorrect, e.g., a numeric value is entered rather than text. Alerts are also set up for missing values. 1.37.3.2 Data clerks will log in to the work station to run the database software’s automated Check Program. 1.37.3.3 Log off the system immediately. 1.37.4 When data have been entered and are available for the DM: 1.37.4.1 At this stage of the trial, post-entry computer tests will be run. 1.37.4.2 A data clerk will log on to a secure work station. 1.37.4.3 The data clerk will print use the database software’s Print Report function to print a hard copy report of the current database entries. 1.37.4.4 The data clerk will confirm that the report lists any missing values or values outside the pre-defined range. If the data has been entered correctly, the report will state “No errors.” 1.37.4.5 Log off the system immediately. 1.37.4.6 Provide the report to the DM. 1.38 Data Protection 1.38.1 The DM will review trial data. If the data meets the definition of Protected Personal Information (PPI), the DM will stamp each data set prior to distributing to the data entry clerks. The stamp mark will be red, read “PPI,” and appear in the upper right corner of the first page of a data set. Paper CRFs are considered PPI and will be marked as such by the DM. 1.38.2 The database management system will be password protected. 1.38.3 Passwords will be generated and provided by the DM. 1.38.4 Only the PI, the DM, and data entry clerks will be assigned passwords. 1.38.5 Each individual assigned a password is responsible for adhering to all ethical codes of conduct and Poe Biotechnology’s requirements described herein for data protection and privacy. Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 10 of 12 1.38.6 PPI will not be accessed via remote access or synchronization facilities which copy the data and store them locally on the machine/device from which it is accessed, unless the machine is fully encrypted to Protect 4.0 standard or the machine/device is kept within Poe Biotechnology’s premises at all times and lock away when not in use, not left unattended whilst in use, and not used in a public access area. 1.38.7 PPI and paper CRFs will be kept in locked filing cabinets in the locked central filing room, which is only accessible to authorized personnel with key code access. 1.38.7.1 The DM will download weekly an entry and exit activity report for the filing room. This report will show the key codes entered with date and time stamps. The DM will check the key codes with a list of authorized users for the file room. The DM will submit this information in his or her weekly memo to the PI. 1.38.7.2 If the DM finds unauthorized key code entries into the room, the DM will contact security personnel immediately with the name of the individual assigned that key code. If the staff member is on site, security personnel will retain the individual for questioning. If the staff member is off site, security personnel will retain the individual when he or she returns to the Poe Biotechnology campus. 1.38.7.3 The DM will also submit a discrepancy form with the unauthorized key code entries to the PI by the end of that work day. The PI will investigate the matter and provide a resolution memo to the DM within one week from receipt of the discrepancy form. The resolution memo will state the problem, the data encountered, and the type of corrective action taken. The discrepancy form and resolution memo will be kept on file in the file room in the “Security Check” files. 1.38.8 If PPI and paper CRFs are required to be transferred to a coordinating center or the sponsor’s center for data entry, they will be sent by courier. 1.38.9 A log will always be maintained of documents sent and received at each center involved. 1.38.10 If electronic data transfer is used, this will be done with a secure work station, password protection, and encryption using the Protect 4.0 software. 1.38.11 If the data is transferred via email, do not include the password in the email. Utilize a courier to send a hard copy letter with the password. 1.38.12 If electronic CRFS or any other PPI data needs to be transferred or stored offsite using removable media such as laptops, smart phones, CDs, or USB drives, the DM will assign a Poe Biotechnology media device to each authorized user. The DM will encrypt the device(s) with Protect 4.0 software. Upon completing the encryption process, the DM will print out a proof of encryption certificate from the device. This certificate will be stored in the employee’s personnel file in the file room. 1.38.13 The transferred material on the removable media must be deleted by the staff member as soon as transfer has occurred successfully. The staff member will print out a deletion receipt using the Protect 4.0 software on the laptop or smart phone and submit the receipt to the DM upon return to the office. The DM will store deletion receipts in the employee’s personnel file in the file room. If a CD or USB drive was used, the staff member must submit those devices to the DM upon return to the office. The DM will use an independent contractor certified in document protection to destroy CDs. The Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 11 of 12 DM will erase the information on a USB drive. The DM will then write and sign a memo certifying that the USB drive information has been erased. This memo will be appended to the weekly memo to the PI. A copy of this memo will also be filed in the employee’s personnel file in the file room. 1.39 Audit Trails, Date and Time Stamps 1.39.1 The computer database software records the date, time, and user id of each transaction completed by data entry clerks and other authorized users. 1.39.2 The DM will schedule monthly audit checks with Poe Biotechnology’s Quality Assurance/Control (QA/QC) Department. 1.39.3 The QA/QC Department will run monthly audit checks using Datawatch’s Monarch Pro Software. 1.39.4 The QA/QC Department will submit the print-outs from the audit checks to the PI after completion of each audit. 1.39.5 The PI and the DM will review the results of each audit. 1.39.6 If discrepancies are found from the audit, including any discrepancies associate with date, time, and user id stamps, the PI and the DM will create a corrective action plan. 1.39.7 The corrective action plan will forwarded to the CEO and the IRB/IEEB. 1.39.8 The DM is responsible for execution of the corrective action plan. 1.39.9 The DM will meet with the PI one week from plan implementation to ensure all corrective actions have been enforced. 1.40 Electronic Record Backup and Recovery 1.40.1 The DM is responsible for electronic data backup and recovery. 1.40.2 The DM will utilize a subcontract with the company Barracuda Networks for data backup and recovery. 1.40.3 The DM will ensure that a Barracuda Backup Server is installed on site. 1.40.4 The DM will ensure that the Barracuda Backup Service sends data to one of two secure data centers via the internet using an encrypted IP tunnel. Before data is transmitted, it will be encrypted and then compressed for transfer and remote storage efficiency. The key to unlock those parts is in turn also encrypted. 1.40.5 The DM will ensure that replication can occur between the two data centers. All data must be mirrored from one to the other and accessed from either. 1.40.6 The DM will recover records, if needed, using Barracuda Networks’ recovery system. This system allows for backup device management through an internet interface, the Barracuda Restore Tool, WebDAV, and FTP. 1.40.7 If the DM cannot use the local backup server due to loss or equipment failure, the DM will contact Barracuda Networks and request a server and/or hard drive replacement with the loaded data via standard shipping methods. 1.40.8 The DM will document all backup and recovery tasks in logs that are maintained in the archive room. Standard Operating Procedure For Data Management SOP FD-001 Release 3 Page 12 of 12 IX. documentation Completed CRFs ready for database entry will be kept in the Poe Biotechnology central filing room. The completed CRFs will be placed in the data entry mailbox slot in this room. As this is a secure room, data entry clerks must obtain authorization and a computerized access code from the PI. All access codes are unique to the individual assigned. X. history Release No. Effective Date 1 2 10/19/09 11/2/09 3 12/7/09 XI. Attachments 1.41 Case Report Form 1.42 Discrepancy Form Reason/Justification for Change New Draft for Peer Review Teacher Review Draft (Changes from Peer and Personal review include adding definitions, adding steps, and re-organizing scope sections.) Final Draft (Changes from Teacher and Personal Review include adding verification for steps in Sections 8.2, 8.3, 8.5, 8.7, and 8.8) 221 Sample: Documentation Plan for Tutorial This sample was prepared for SFSU TPW 480. Course description and goals are here. The purpose for including it in my portfolio is to demonstrate competency in writing documentation plans. Assignment Details The purpose of writing this document was to write a documentation plan. This assignment is part one of a three part project that focused on writing technical documentation. The program featured in this project is SnagIT, a real tool available from Techsmith.com. San Francisco State University Technical and Professional Writing Program TPW 480 To From Date Dr. Bob Dvorak Lisa Romanoski November 16, 2009 Subject Documentation Plan for Snagit 9.1.3 Tutorial Purpose/ Audience I propose to write a tutorial for Snagit 9.1.3, a PC-based screen shot capture tool. The tutorial will be a Microsoft Power Point Presentation. The tutorial will teach new, entry-level technical writers to perform and retain the knowledge of how to perform the following tasks:    Capture, resize, and store several standard window screen shots. File storage instruction will focus on grouping project-related files for ease of retrieval by current and future project team members. Capture and store a series of related scrolling web pages. Create a short “screen cam” video of a series of menu selections and actions. I anticipate writing two drafts and a final version of the tutorial. Only one draft will be submitted for review by the client. Revision history will be noted on the documents submitted for review. Resources To meet documentation requirements, I need the following:        Budget My personal computer Internet access for research Snagit 9.1.3 free trial software, available from CNET internet site Microsoft Word and Power Point on my personal computer A printer Snagit Tutorial Usability Test Plan results December 7, 2009, instructor review comments Budget is not applicable to this particular project. L. Romanoski, Memo on Snagit 9.1.3 Tutorial Page 2 Deliverables Documentation Plan for Tutorial on November 16, 2009 Usability Test Plan for Tutorial on November 30, 2009 Draft I Tutorial on December 7, 2009 Usability Report on Tutorial on December 14, 2009 Final Tutorial on December 14, 2009 Contingencies Final submission of the tutorial is contingent on receipt of peer and instructor review comments by December 14, 2009. Anticipated delays in the schedule will be communicated to Dr. Dvorak via email at least two days prior to each deliverable date. 224 Sample: Usability Test Plan and Results This sample was prepared for SFSU TPW 480. Course description and goals are here. Assignment Details The purpose of writing this document was to write a usability test plan. This assignment is part two of a three part project. San Francisco State University Technical and Professional Writing Program TPW 480 To From Date Dr. Bob Dvorak Lisa Romanoski December 7, 2009 Subject Snagit 9.1.3 Tutorial Usability Test Plan The Snagit 9.1.3 Tutorial will teach entry-level technical writers in the Poe and Associates Publications Department how to capture, resize, crop, and store computer window screen shots. The tutorial will be a Microsoft Power Point presentation with tasks to be completed for each section. The writers will also learn how to capture and store a series of scrolling web pages. The third part of the tutorial will focus on creation of a short “screen cam” video of a series of menu selections and actions. The tutorial goal is retention of the material so that the writers can return to their work and start using the product after completing the tutorial. The following is a usability test plan to test the initial section of the tutorial: completing a standard screen capture. The goal of the usability test is to assess whether the tester can understand and successfully execute a screen capture using the tutorial in less than 20 minutes. User Profile The anticipated user of the Snagit program is an entry-level technical writer who has experience and is comfortable performing a variety of tasks with PCs but has never used Snagit. To simulate the experience of this entry-level writer, a tester will be used who is familiar with PCs but not necessarily advanced or expert at using them. Testing and Evaluation Measures As the author of the tutorial, I will conduct the usability test and evaluate of the tester. I will provide the tester with my laptop, which has the Snagit program installed on it. I will also give the tester an actual draft of the screen capture portion of the tutorial. I will ask the tester to go through the steps using the draft tutorial and the program. As the tester works, I will be noting the following:       How the tester approaches and initially interacts with the tutorial, computer, and program Step repetition, errors, and re-reading of the tutorial or parts of the tutorial Usefulness of the graphics to the tester Length of time needed to execute the task What the subject was actually able to capture Any comments and complaints made by the tester during the process Usability Test Plan, Continued Page 2 Upon completion of the test, I will interview the tester for additional details on the listed items. I will also have the tester write down any comments he or she may have directly on the draft tutorial. Report Contents/Format Test observations, results, and interview responses will be compiled into a test report. The goal of the test report is to summarize the findings and then make recommendations for fixing problem areas, improving the tutorial, and re-designing the layout if necessary. While the test focuses on only one section of the tutorial, I anticipate that the test results can be applied to other sections. The tutorial will need to be re-designed if the tester fails to execute the task within 20 minutes or needs to re-do all the steps after making an error halfway through the task. San Francisco State University Technical and Professional Writing Program TPW 480 To From Date Dr. Bob Dvorak Lisa Romanoski December 7, 2009 Subject Snagit 9.1.3 Tutorial Usability Test Results Usability Test I conducted a usability test on December 1st using my friend Molly as a test subject. The goal of the test was to determine if Molly could execute a standard screen capture in less than 20 minutes. Molly was provided with the first two pages of my first tutorial draft. The first page lists the steps to perform a screen capture and shows the user graphics of the Snagit screen and Capture icon. The second page discusses next steps after executing a screen capture and defines Editor options. Molly executed a screen capture in less than 2 minutes. Molly took about 15 minutes to read through the second page. I then asked her questions about what she found confusing or could be rewritten for clarification. As she was executing the task, I was observing Molly for her initial approach to the tutorial and my PC lap top. Molly is a copy editor and journalist and works primarily on Macs. I was also looking to see if Molly would repeat a step, re-read the section, or make any errors. Findings The test when better than expected, as Molly executed the screen capture almost immediately. She approached the task with enthusiasm and curiosity. Molly pointed out that the last step on the first page was either out of sequence or could possibly be omitted. This step explained how to cancel out of the screen capture execution process after pressing the Capture icon button. She also found my note on arranging the appearance of a file before the screen capture execution confusing. This note appeared at the end of the screen capture task. In general she found the screen capture execution task easy to follow. The second page contained commentary on the Editor and no sequence of steps in an executable task. It did not contain any graphics of the Editor window. It took Molly longer than I anticipated to read the section. She found some of the definitions of the Editor tabs to be confusing or too wordy. She also wanted to follow along in the reading of the definitions by opening the Editor window and clicking on the various tabs. Molly recommended including some graphics and providing more details. We both agreed that the section could benefit from a subheading such as “Becoming Familiar with the Editor.” Usability Test Plan Results, Continued Page 2 Conclusion and Next Steps for Tutorial Draft II I provided Molly with a very rough first draft of the tutorial and was pleased to see that she executed the task successfully in the 20-minute time frame. I wasn’t surprised that she found the second page confusing. As I wrote it, I wasn’t sure exactly what I wanted to say and the order in which I wanted to present the information. I had also intended to include some graphics to aid in understanding the descriptions, but they never made it into the first draft. For my second draft, I intend to revise all areas that she commented on during our conversation. As my first draft is very simplistic, I will continue to write and enhance all sections with additional discussion and graphics. I would like to link the tasks to actual work place scenarios to show how the program is useful and to also develop an enthusiasm among readers. 229 Sample: Tutorial This sample was prepared for SFSU TPW 480. Course description and goals are here. Assignment Details The purpose of writing this document was to write tutorial. This assignment is part three of a three part project. Copyright 2009 Poe and Associates, Inc. All rights reserved. Snagit Screen          Capture profiles           Profile Settings and Capture Button Snagit Profile = Capture Mode + Input + Effects + Output Snagit Tools Snagit Ribbon Search Pane Snagit Editor Tools Quick Access Toolbar Snagit Button: Click here to open, save, or print. Dialogue Box Launcher: Click here to see more options Open Captures Tray: The tray holds your most recent captures. Collapse the Search Pane: Click your mouse here to collapse the search pane or make it visible. Snagit Library: Locate, manage, and view captures and multimedia files.    Snagit Ribbon Draw: Annotate a capture. Image: Add special effects, crop, rotate, and resize. Draw tab with a group of clipboard options: copy, paste, cut. Hotspots: Create interactive spots to link to a web page or display a pop-up text box. Tags: Assign keywords to your captures or use Flag icons to categorize your capture. View: Pan and zoom. Send: Send your capture to email, Word, Excel, or PowerPoint. Image Tab Crop, trim, resize, or rotate you captures. Hotspots Tab Add edge effects to your captures. Select a color for the Shape (Hotspot) and text popup border and background. Drag a Shape onto your capture. Connect that shape to a web address in Link to. Use Tooltip to enter text that appears when you hover over your Shape (Hotspot) with a mouse. Select all Shapes (Hotspots) and/or remove (delete) them. Use Modify for effects: blue, grayscale, watermark, filers, and spotlight and magnify. Tags Tab Use the icons in the Flags group to identify and categorize your captures. Simply click the icon to assign it to your capture. Click it again to remove it from your capture. Assign Keywords to your captures. Your words are then listed in the All Keywords box by selecting the down arrow to launch the dialogue box. When did you take that screen capture? Check the Details box. Find more information like its file size by clicking the More Details icon. View Tab Send Tab Use View to pan, zoom, and change the view of multiple captures. Send your capture to another program. Select Region for Profile You capture is placed in Editor. Capture Icon Resizing an image Selection Tool Working with the Library Select Region for Profile Select Region for Profile If you have assigned flags to your capture or media file, you will see them in the Tray. You will know more flags are assigned if you see an ellipse symbol after the second flag. Capture a Scrolling Web Page Capture a Scrolling Web Page !! The maximum size of an AVI file produced by Snagit is 2 GB. If you pass this size limit, the entire capture is lost. Reviewing a basic screen capture     Snagit Profile = Capture Mode + Input + Effects + Output 248 Sample: Request for Proposal This sample was prepared for a real request for a proposal. (RFP) The purpose for including it in my portfolio is to demonstrate competency in writing RFPs. Description This proposal was prepared for the Bay Area Toll Authority (BATA) for the purpose of conducting a Project Study Report (PSR) for the Gateway Park Area in the San Francisco Bay Area. The Gateway Park Area is located just south of the toll plaza of the San Francisco-Oakland Bay. The main objective of the Gateway Park Area PSR was to advance the planning for the Gateway Park Area by defining and reaching regional and local agreement on a scope, cost and funding plan for a Gateway Park Area project. The goal of the Gateway Park PSR was to examine alternatives in regards to land uses, activities, environmental impacts, and access to define a project scope, schedule, and cost estimate for the development of a Gateway Park Area. April 7, 2009 Request for Proposal For Preparation of a Project Study Report for the Gateway Park Area in the San Francisco Bay Area WEB: www.mtc.ca.gov Poe and Associates, Inc. Engineering and Consulting May 8, 2009 Mr. Rod McMillan Bay Area Toll Authority Joseph P. Bort MetroCenter 101 Eighth Street Oakland, CA 94607-4700 Subject: Request for Proposal for Preparation of a Project Study Report for the Gateway Park Area in the San Francisco Bay Area Dear Mr. McMillan: Poe and Associates, Inc., is pleased to submit a proposal to the Bay Area Toll Authority (BATA) to conduct a Project Study Report (PSR) for the Gateway Park Area in the San Francisco Bay Area. Our team of experienced professionals can provide a modern approach to the identification of cost effective alternatives pertaining to land use development at the project site. Community and stakeholder consensus is absolutely critical to the success of any project, irrespective of size. At Poe and Associates, we seek to reach out to and bring together all stakeholders. We explain all aspects of the project and seek input from all attendees of meetings. No comment is ever insignificant. We look forward to working under the Gateway Park Working Group (GPWG) on the development of the PSR. We also have on our team experienced professionals available for mediation services. Our goal is to transform the input provided to us into alternatives that are compatible with project goals and input, and proceed with preliminary analysis. Our analysis includes but is not limited to:      Land use, Land ownership and acquisitions, Infrastructure needs, Accessibility requirements, and Environmental documentation requirements. Poe and Associates acknowledges that the two primary areas for analysis include the Gateway Park Area and the larger “Area of Influence,” which takes into account current and/or future land development of the City of Oakland, the Port of Oakland, and East Bay Municipal Utility District, etc. Poe and Associates, Inc. 123 Main Street, Suite 500 * Anywhere, CA 94706 * Phone: 1-800-CAN-DOIT Poe and Associates, Inc. Engineering and Consulting At Poe and Associates, our cost estimating services render affordable projects to our clients. We will develop realistic cost estimates for each alternative and also identify additional funding sources to finance the development. Concurrent with our cost estimates, our project scheduling capability yields construction schedules that adhere to all Federal and State regulatory work windows, and other miscellaneous requirements, while also remaining cost effective to our clients. We seek to build the best project possible within a reasonable amount of time. The primary contact person for the project will be Ms. Smith, project manager:  Ms. Jane Smith Poe and Associates, Inc. 123 Main Street, Suite 500 Anywhere, CA 94706 Phone: 1-800-CAN-DOIT Poe and Associates, Inc. understands that the proposal is a binding offer to contract with BATA according to all requirements, in addition to insurance items, set forth in the RFP for a period of 120 days from the due date for submission of this proposal. We’re excited about this project and the future of the Gateway Park Area. We look forward to working with you, the Gateway Park Working Group, and all stakeholders to advance the planning process for this exciting addition to the San Francisco Bay Area. Sincerely, Ms. Eugenie Poe President, Poe and Associates, Inc. Poe and Associates, Inc. 123 Main Street, Suite 500 * Anywhere, CA 94706 * Phone: 1-800-CAN-DOIT Poe and Associates, Inc. Engineering and Consulting Preparation of a Project Study Report For the Gateway Park Area In the San Francisco Bay Area May 8, 2009 Contact: Ms. Jane Smith Poe and Associates, Inc. 123 Main Street, Suite 500 Anywhere, CA 94706 Phone: 1-800-CAN-DOIT Poe and Associates, Inc. 123 Main Street, Suite 500 * Anywhere, CA 94706 * Phone: 1-800-CAN-DOIT Poe and Associates, Inc. Engineering and Consulting Table of Contents I. II. III. IV. V. VI. Summary of Approach ............................................................................................ 6 Detailed Work Plan ................................................................................................. 6 Management Plan.................................................................................................... 6 Qualifications and References ................................................................................ 7 Proposed Budget ..................................................................................................... 7 CA Levine Act Statement ....................................................................................... 7 Poe and Associates, Inc. 123 Main Street, Suite 500 * Anywhere, CA 94706 * Phone: 1-800-CAN-DOIT Poe and Associates, Inc. Engineering and Consulting I. Summary of Approach 1. Discussion of the purpose of the project; 2. A summary of the proposed approach specific to each task; 3. Assumptions made in selecting the approach; and 4. Identification of any difficult issues that may affect the implementation of the project and how those issues will be addressed. II. Detailed Work Plan 1. Discuss how each task will be conducted, identify deliverables, and propose a preliminary schedule. 2. Identify all key personnel and associated tasks for which he or she is responsible. 3. Describe the role of any subconsultants and how they will be supervised. Discuss previous working relationships. 4. Identify potential project challenges, critical path items, and any other issues that may affect completion of the project within the proposed time frame. Detail a plan to overcome these challenges. III. Management Plan 1. Describe project management approach. 2. Include an organizational chart. 3. Describe response mechanisms for addressing challenges and concerns. -6- IV. Qualifications and References 1. Describe experience and expertise in all areas of the scope of work included in the Appendix A of the RFP. 2. Provide a one page summary of three projects similar in subject matter and scope. a. Include client/contact/reference, contract amount, and contact phone number. 3. List any contracts with any of the GPW agencies listed on Page 1 of the Letter of Invitation. V. Proposed Budget 1. Provide a full description and breakdown of the expected expenditures of funds for the proposed project. Present a breakdown of hours and expenses by task, along with key personnel. VI. CA Levine Act Statement 1. Submit a signed Levine Act Statement. 256 Sample: Healthcare Informatics Evaluation Proposal This sample was prepared for Drexel INFO 732. Description The course introduces planning and evaluation of healthcare informatics applications. Through critical reading, students learn the planning and evaluation cycle and become familiar with quantitative and qualitative methods and measures. Through lectures and assignments, students select a healthcare problem, formulate a problem statement, select evaluation methods and measures and write a proposal. Course Objectives      Identify an informatics issue as an evaluation problem Describe the evaluation cycle (plan, do, test, change) Select evaluation measures and methods appropriate to evaluation in healthcare informatics Write a proposal to conduct an evaluation study in an area of interest in healthcare informatics Critique and present relevant evaluation studies from the informatics literature HEALTHCARE PRIORITY SETTING 1 Priority Setting in Healthcare By Lisa Romanoski Drexel University Author Note This paper has been prepared in accordance with INFO 732 requirements. HEALTHCARE PRIORITY SETTING 2 Introduction and Problem Statement As healthcare organizations become increasingly focused on achieving Stage One Meaningful Use and a conversion to International Classification of Diseases, 10th Edition Diagnosis and Procedure Codes (ICD-10) in the next two years, installation rates for key clinical applications such as electronic medical records (EMRs) continues to increase, yielding greater amounts of electronic clinical data (Healthcare Information Management Systems Society (HIMSS, 2010; HIMSS, 2012, p.4). With so much data available to organizations, they will want to consider how best to use the data to improve clinical performance and outcomes. While this data seems like a goldmine of information waiting to be tapped, challenges exist in regard to how best to use the data and availability of resources (e.g., staff, money, etc.). If staff or other resources aren’t available or in short supply, organizations may need to turn to priority setting, which can provide a focus for work and continued progress towards preventative care, illness/injury reduction, and other healthcare goals (Bate & Mitton, 2006, p. 275; CanhamChervak et al., 2010, p. S11; HIMSS, 2010). The present literature reveals that priority setting in healthcare is not a clear cut process and, due to greater demand for accountability and transparency, there exists a need for such processes. The purpose of this evaluation is to help fulfill that need by seeking answers to the questions: (1) How do healthcare organizations set priorities? (2) Are there instructions or templates that can be used in decision making processes? (3) Can introducing a decision making tool better assist healthcare organizations in setting priorities? Organizations in this study are considered to encompass acute care facilities. Conclusions drawn from this research are expected to add to the body of knowledge in priority setting and decision making. HEALTHCARE PRIORITY SETTING 3 Literature Review History According to the 2012 HIMSS Leadership Survey of senior information technology (IT) executives, the most significant barrier to implementing IT is lack of staffing resources, followed by lack of adequate financial support (p. 24). These results are examples of issues that face all healthcare organizations: how best to allocate resources considering all the demands, wants, and needs collectively competing for those scarce resources (Bate & Mitton, 2006, p. 275; Sibbald et al., 2010, p. 1). Because of this scarcity, decision making tends to be based on prioritizing activities in an effort to determine what to provide, how, where, and for whom (p. 275). Despite the fact this issue is a global phenomenon operating at all levels – from the government allocating a budget to clinicians treating patients – priority setting techniques tend to differ from organization to organization (p. 275). Current Priority-setting Practices in Healthcare In general, most healthcare organizations rely on a health service or an economic approach for priority setting (Bate & Mitton, 2006, p. 277). Health service approaches include base allocation decisions on what was previously funded, needs assessments aimed at determining activities to pursue to achieve goals at the individual or population level, or allocation of resources to support provision of core services (p. 277-8). Health service approaches tend to focus on addressing a need and then directing resources to fill a gap in service provision (p. 279). The shortcoming of this approach is that it results in identification of a resource required to meet a need with little regard to where the resource will come from and which need may trump another in terms of importance (p. 279). HEALTHCARE PRIORITY SETTING 4 Economic approaches include cost-effectiveness analysis (CEA), cost-utility analysis (CUA), and cost-benefit analysis (CBA) (p. 277). The strengths of these analyses is that costs and outcomes are considered, and one treatment may be compared with another in terms of incremental gains for incremental resources expended (p. 277). The shortcoming of an economic approach is that results may not be applicable to the decision making context of an organization, whose decisions tend to focus on service expansion or reduction and allocation of resources over technologies and groups of people (p. 279). Furthermore, Friedman & Wyatt (2006) note that they rarely indicate a correct choice (p. 303). Additional supporting information that takes into account political, ethical, and other concerns may be needed to truly determine if an outcome gain is worth the cost (Friedman & Wyatt, 2006, p. 303). Priority Setting Factors As mentioned previously, priority setting techniques vary from organization to organization (Bate & Mitton, 2006, p. 275; Sibbald et al., 2010, p. 2). Regardless, a review of healthcare organization priority setting literature indicates that factors influential to most organizations’ priority setting processes include (Aspen Advisors, 2011; Brooks, 2008, p. 101-4; Gibson et al., 2004, p. 3; Gouri, 2010, p. 1):  Organizational mission, objectives, values, mandates, and directives  A 360-degree organizational view  The environment into which something might be deployed (technology, an application)  A definition of the future  Strategic initiatives  Constraints  Stakeholder communication Priority setting is typically aligned with mission, values, and strategic goals for most organizations (Aspen Advisors, 2011; Bate & Mitton, 2006; Brooks, 2008; Canham-Cherval et HEALTHCARE PRIORITY SETTING 5 al., 2010; Chaiken, 2003; Gibson et al., 2004; Gouri, 2010; Menon et al., 2007; Sibbald et al., 2010; Vogel, 2003; VQC, 2008). These factors, in combination with others listed above, represent common attributes from various disparate priority setting techniques. Extracting these factors from the literature provides information that should be looked for during the proposed evaluation. Priority Setting Tool Availability In reviewing the literature in search of specific, easy to use, step-wise priority setting tools or toolkits, such as a list of instructional steps or a downloadable form, only one tool was identified (Canham-Chervak et al., 2010). The majority of literature was found instead to consist of miscellaneous rhetoric on the subject or general guidelines developed from qualitative interviews or case studies (Bate & Mitton, 2006; Dolan, 2008; Gibson et al., 2004; Sibbald et al., 2010; VQC, 2008). The one readily available tool found in the literature was developed by Canham-Chervak et al. (2010) for military injury prevention activities. The process first looks at whether the issue is consistent with the agency mission and then uses scoring to assess problem importance, preventability, feasibility, timeliness, and evaluation potential (p. S12 – S16). The higher the score obtained from the process, the stronger the indication that the issue was amenable to program and policy implementation (p. S14). The authors note that the strength of the process is its attempt to minimize bias through the use of quantifiable, objective measures (p. S16). Objectivity is built in by requiring a review of available data (p. S16). The attractiveness of this particular tool is its accessibility, simplicity, ability to be used quickly, and its adaptability to prioritization efforts in other healthcare areas. HEALTHCARE PRIORITY SETTING 6 The guidelines are helpful to get healthcare organizations and decision makers focused to the task at hand. If an organization is looking to make modifications to its existing processes or adopt entirely new methodology, the final method chosen may be a combination of methods and guidelines tailored to the uniqueness of an organization and the context in which decisions are being made (Bate & Mitton, 2006, p. 281). Evaluation Design Qualitative Case Study A two-phase qualitative case study focusing on priority setting is proposed. Case studies are considered appropriate for exploring decision making processes (Friedman & Wyatt, 2006, p. 296). Researchers Principal investigator. Bob Smith has over 20 years of experience as a program manager and advisor to healthcare and IT executives. Research associate. Alison Sweeney holds a PhD from Northern University in Health Service and Policy Research and has 10 years of experience in health policy and administration. Initial Requirements This study will require review and approval by the organization’s institutional review board (IBR) and consent from participants (Friedman & Wyatt, 2006, p. 292, 339). Phase 1: Existing Processes Methods. The first phase of this evaluation consists of a review of current priority setting process for the previous five years of budget appropriations for the Health4U organization’s San Francisco Medical Center. Health4U serves 25 million Americans from 40 hospitals and 700 HEALTHCARE PRIORITY SETTING 7 medical buildings in 12 states5. The review will consist of internal company documents and semi-structured interviews (see Appendix A for a list of questions to be answered during analysis). Documents of interest include but are not limited to the strategic plan; priority setting, decision making, and budget allocation processes; and decision support documents. The purpose is to determine what the current process is, if the process is used consistently from year to year, what the process evaluates, and what the outcomes of the process are. Collectively these findings will establish baseline conditions for the study and help define the existing priority setting process. This portion of the evaluation does not seek to evaluate correctness of priority setting and decision making processes. Information analysis from this part of the study is anticipated to be on-going throughout the evaluation. Phase 2: Using a Tool Methods. The second phase of this evaluation aims to introduce a priority setting tool, which is anticipated to be a modified version of a tool developed by Canham-Chervak et al. in 2010 (see Appendix B). The purpose of this part of the study is to determine if the tool aids, hinders, or has no effect on the organization’s priority setting and decision making process. Using information acquired from Phase 1, Canham-Chervak et al.’s tool will need to be revised and tailored to the specific organization. A copy of this tool is available in Appendix B. Semistructured interviews with key decision-makers will be used to assess the tool’s helpfulness. Participants. Participants in both study phases are anticipated to include employees of the medical center who are directly and indirectly involved in a typical priority setting and/or budgeting process. Interviews and Data Analysis. Interviews will require consent from participants and be tape recorded (Friedman & Wyatt, 2006, p. 292). All tapes will be securely stored. Backup 5 Health4U is a fictitious company developed for purposes of this assignment. HEALTHCARE PRIORITY SETTING 8 copies of tapes will be made and securely stored in a separate location from original tapes (p. 83). Preparing recorded data will require transcribing all tapes and typing transcriptions into computer files (p. 83). Transcription of recordings and typing of any field notes will be completed using a common format as soon as possible following collection (p. 83-4). Transcriptions will be coded to identify repeating ideas and larger themes. When themes seem to coalesce, results may be taken back to participants for confirmation (Friedman & Wyatt, 2006, p. 288). An independent consultant will be used to review data and themes as an added confirmation (p. 288). Preliminary survey questions may be found in Appendix C. Reporting Results and findings will be summarized in a report presented to the organization’s executive committee. The report will include standard sections such as introduction, background, methods, findings/results, discussion, and conclusions (Friedman & Wyatt, 2006, p. 290). An oral presentation will also be prepared, allowing opportunity for discussion, questions, and answers. Stakeholders Stakeholders who have an interest in this study’s outcomes include the organization, executive and managerial staff, clinicians, patients, and the local population. Evaluation outcomes may influence the way an organization sets priorities and makes decisions in the future. Executive and managerial staff may decide to retain existing processes and do nothing or consider revising processes and approaches. Clinicians may experience change or no change depending on policies and decisions made be executive staff. For example, if the organization decides to shift away from a historical allocation budget process to a different approach, certain areas may see a relocation of resources to or from the units in which they work. Outcomes of HEALTHCARE PRIORITY SETTING 9 interest to patients and the local population pertain to changes in provision, type, and cost of service, as well as accountability and transparency in decision making. Quality Control It is generally recognized that the criteria for appraising the quality and trustworthiness of qualitative research differs from quantitative research (Friedman & Wyatt, 2006, p. 291; Shenton, 2004, p. 63). To ensure quality, Guba’s constructs for trustworthiness as presented by Shenton (2004) will be adhered to. Credibility. To ensure credibility, a number of techniques will be employed. This evaluation seeks to use well-established research methods: namely interviews and data organization using coding techniques to extract themes. Familiarity with the medical center and its culture will be established early in the process prior to beginning Phase 1. While random sampling is preferred to negate potential for bias, it may be difficult to achieve random sampling in a study of one medical center. Nonetheless, random sampling will be executed to the extent possible. To ensure results and common themes are as useful as can be, triangulation methods of cross checking information with existing documents may be used. Results may be taken back to previously interviewed or different participants for confirmation. Participants are not required to participate and may withdraw from the study at any point. This tactic aims to involve participants who are genuinely willing to participate and offer information freely. Iterative questioning may be used to flush out contradictory information. Frequent debriefing sessions and peer scrutiny will be used to identify flaws in the course of action and offer a fresh perspective on unfolding activities (Shenton, 2004, p. 66-7). It is anticipated that the Hawthorne effect, “the tendency for humans to improve their performance if they know it is being studied,” may impact outcomes from Phase 2 of the HEALTHCARE PRIORITY SETTING 10 evaluation (Friedman & Wyatt, 2006, p. 211). It is assumed that it may be impossible to prevent, so the researchers of this evaluation choose to remain aware of the possibility, will attempt to decipher behavioral differences since existing data will be reviewed and may serve as a baseline for comparison, and, on the recommendation of Leonard and Masatu (2010), may study the effect more closely in an effort to improve understanding of performance and behavior. Transferability. Since this study focuses on a single organization, transferability to other cases may be problematic. Nonetheless, sufficient contextual information will be provided to enable readers of the research to make decisions about application to other situations (Shenton, 2004, p. 69). Dependability. The methods used in this evaluation, including design and data gathering, will be reported in detail to enable future researchers to repeat the work (Shenton, 2004, p. 71). However, as this particular evaluation focuses on one medical center, the results obtained from any future work using these methods may not necessarily yield the same results. Contextual factors may influence future outcomes. Confirmability. Triangulation will be used as described above and to minimize investigator bias. Assumptions pertaining to approaches and decisions will be discussed in the report. Use of diagrams, as recommended by Shenton (2004) will be used to show the “audit trail” for the evaluation, which typically consists of raw data prior to coding, data reduction and analysis products, and data reconstruction and synthesis products (Wolf, 2003, p. 176). Study Limitations Study limitations include both methodological and researcher limitations. Methodological study limitations pertinent to this study could include data availability, data collection measures, and use of self-reported data (USC.edu., 2012). As mentioned previously, this study proposes to HEALTHCARE PRIORITY SETTING 11 look at one medical center. It is assumed that there are existing documents or other artifacts that can be analyzed to complete Phase 1 of the study. In regard to data collection, the possibility exists for inadvertently leaving out an interview question that may have proved useful in the assessment. To the extent possible, questions initially presented in this proposal may be reevaluated throughout the study and modified to account for such possibilities. Reporting will include information as to why data collection measures may have been revised mid-study. In regard to data collected during interviews, the possibility exists that participants may be introduce bias due to factors including but not limited to selective situational recalls or other factors. Evaluators will attempt to minimize biases according to measures specified in Quality Control. Limitations of the researcher may include access to data, such as existing documentation, and individual bias. Attempts to minimize bias are outlined in Quality Control. Conclusion The research team looks forward to working on this project. Priority setting in healthcare is an important area to focus on because resources always seem to be in short supply, forcing decisions to be made about which activities, programs, or services to pursue. This study proposes to evaluate an existing process, introduce a new tool, and determine the effect of the new tool. The significance of this work lies in its relevancy and importance to addressing the issue of prioritizing in light of the current and future data influx from electronic applications, as well as the demand for greater transparency and accountability in decision making. Our work seeks build upon existing work and answer questions that will assist all healthcare organizations in setting priorities, a fundamental fact of life that is global concern. HEALTHCARE PRIORITY SETTING 12 References Aspen Advisors. (2011, December). Answering the question: how to achieve a return on investment for healthcare business intelligence. Retrieved from: http://www.aspenadvisors.net/results/whitepaper/how-achieve-roi-healthcare-bi Bate, A., & Mitton, C. (2006). Application of economic principles in healthcare priority setting. Expert Review of Pharmacoeconomics & Outcomes Research, 6(3), 275 – 284. Battista, R. N., Hodge, M. J. (1995, November). Setting priorities and selecting topics for clinical practice guidelines. Canadian Medical Association, 153(9), 1233-1237. Bauer, J. C. (2003, Fall). Return on investment: going beyond traditional analysis. Journal of Healthcare Information Management, 17(4), 4-5. Brooks, M. (2007, October). Channeling the data stream: how analytics can radically improve clinical performance. Health Management Technology, 28(10), 46. Byer, C. (2011, October). Using health care data analytics to improve information management. Retrieved from: http://searchhealthit.techtarget.com/tutorial/Using-health-care-dataanalytics-to-improve-information-management Canham-Chervak, M., Hooper, T. I., Brennan, F. H., Craig, S. C., Girasek, D. C., Schaefer, R. A., Barbour, G., Yew, K. S., & Jones, B. H. (2010). A systematic process to prioritize prevention activities. American Journal of Preventative Medicine, 38(1S), S11-S18. Chaiken, B. P. (2003, Fall). Clinical ROI: Not just costs versus benefits. Journal of Healthcare Information Management, 17(4), 36-41. CSC. (2012). Transforming healthcare through better use of data. Retrieved from: http://assets1.csc.com/health_services/downloads/CSC_Transforming_Healthcare_Throu gh_Better_Use_of_Data.pdf HEALTHCARE PRIORITY SETTING 13 Dolan, J. G. (2008). Shared decision making – transferring research into practice: the analytic hierarchy process (AHP). Patient Education and Counseling, 73, 418-425. Family Health International. Qualitative research methods: a data collector’s field guide. Module 5: data documentation and management: organizing and storing your data. Retrieved from: http://www.fhi360.org/NR/rdonlyres/eu6v6ddwvgr36i4xh3yu474tc7oko tgm2rmixlofuk dtmmnduwxowxbb4xyenziztyr7zwg3dodgf/datamanagement1.pdf Fitzgerald, J. A. & Dadich, A. (2009, August). Using visual analytics to improve hospital scheduling and patient flow. Journal of Theoretical and Applied Electronic Commerce Research, 4(2), 20-30. Forman, E. H. & Gass, S. I. (2001, July – August). The analytic hierarchy process: an exposition. Operations Research, 49(4), 469-486. Gibson, J. L., Martin, D. K., & Singer, P. A. (2004). Setting priorities in health care organizations: Criteria, processes, and parameters of success. BMC Health Services Research, 4(25), 1-8). Gouri, A. (2010, December 1). Prioritize data in the context of overall objectives. Managed Healthcare Executive. Retrieved from: http://managedhealthcareexecutive.modernmedicine.com/mhe/article/articleDetail.jsp?id =697479 HIMSS. (2010, June 7). Clinical analytics: can organizations maximize clinical data? Retrieved from: http://www.himssanalytics.org/docs/Clinical_Analytics.pdf HIMSS. (2012, February 21). 2012 HIMSS Leadership Survey: Senior IT Executive Results. Retrieved from: HEALTHCARE PRIORITY SETTING 14 http://www.himss.org/content/files/2012FINAL%20Leadership%20Survey%20with%20 Cover.pdf IBM. (2011). Capturing value from patient-centered care. Retrieved from: http://www.ibm.com/smarterplanet/global/files/us__en_us__healthcare__giw03020-usen00_lr.pdf Kolte, P. Boerboom, L, Miscione, G., & Georgiadou, Y. (2012). A proposal for studying decision making and spatial data infrastructures in the public sector in India. Retrieved from: http://www.gsdi.org/gsdiconf/gsdi11/papers/pdf/381.pdf Krohn, R. (2003, Fall). In search of ROI from CPOE. Journal of Healthcare Information Management, 17(4), 6-9. Lang, R. D. (2003, Fall). ROI and IT: Strategic alignment and selection objectivity. Journal of Healthcare Information Management, 17(4), 2-3. Leonard, K. L. & Masatu, M. C. (2010). Using the Hawthorne effect to examine the gap between a doctor’s best possible practice and actual performance. Journal of Development Economics, 93, 226-234. Local Health Integration Network. (2009, June). Priority setting in the LHINs: a practical guide to decision making. Retrieved from: http://www.northwestlhin.on.ca/uploadedFiles/Home_Page/Integrated_Health_Service_P lan/Priority%20Setting%20in%20the%20LHINs%20%20A%20Practical%20Guide%20to%20Decision making%20FINAL.pdf Martin, D. & Singer, P. (2003, March). A strategy to improve priority setting in health care institutions. Health Care Analysis, 11(1), 59-68. HEALTHCARE PRIORITY SETTING 15 Menon, D., Stafinski, T., & Martin, D. (2007). Priority-setting for healthcare: who, how, and is it fair? Health Policy, 84, 220-233. Mitton, C. R. & Donaldson, C. (2003). Setting priorities and allocating resources in health regions: lessons from a project evaluating program budgeting and marginal analysis (PBMA). Health Policy, 64, 335-348. Mitton, C. & Donaldson, C. (2003). Tools of the trade: a comparative analysis of approaches to priority setting in healthcare. Health Services Management Research, 16, 96-105. Morris, H. D. & Hanover, J. (2010, December). Business analytics and the path to better decisions in healthcare. Retrieved from: http://www.techrepublic.com/whitepapers/business-analytics-and-the-path-to-betterdecisions-in-healthcare/2969661 Mullen, P. M. (2004, February). Quantifying priorities in healthcare: transparency or illusion? Health Services Management Research, 17, 47-58. National Health Service (NHS) Confederation. (2007). Priority setting: an overview. London, UK: NHS. Retrieved from: http://www.nhsconfed.org/Publications/Documents/Priority%20setting%20an%20overvie w.pdf Norheim, O. F. (2008, October 18). Moving forward on rationing. BMJ, 337, 903-4. Reeleder, D., Goel, V., Singer, P. A., & Martin, D. K. (2006). Leadership and priority setting: the perspective of hospital CEOs. Health Policy, 79, 24-34. Shenton, A. K. (2004). Strategies for ensuring trustworthiness in qualitative research projects. Education for Information, 22, 63-75. HEALTHCARE PRIORITY SETTING Sibbald, S. L., Gibson, J. L., Siner, P. A., Upshur, R., & Martin, D. K. (2010). Evaluating priority setting success in healthcare: a pilot study. BMC Health Services Research, 10(131), 1-14. USC.edu. (2012). Organizing your social sciences research paper. Retrieved from: http://libguides.usc.edu/content.php?pid=83009&sid=616083 Victorian Quality Council (VQC). (2008, June). A guide to using data for health care quality improvement. Melbourne, Victoria: Victorian Government Department of Human Services. Vogel, L. H. (2003, Fall). Finding value from IT Investments: exploring the elusive ROI in healthcare. Journal of Healthcare Information Management, 17(4), 20-28. Wolf, Z. R. (2003). Exploring the audit trail for qualitative investigations. Nurse Educator, 28(4), 175-8. 16 HEALTHCARE PRIORITY SETTING Appendix A 17 HEALTHCARE PRIORITY SETTING 18 Document Analysis (These questions were developed based on work by Sibbald et al. (2010).) 1. Is there a record of who was involved during each phase of the priority setting process? Are the records consistent? 2. Is there a record of the process by which decisions were made and people were involved? 3. What forms of communication were used? 4. Was there a clear communication plan? 5. Are there any documents pertaining to an appeal process? What does it look like? 6. What does the process evaluate? 7. What are the process outcomes? (i.e., budget allocation, policy setting, purchase of new equipment, etc.) 8. Is the process used consistently from year to year? Analyze Mission, Vision, Values, and Strategic Plan 9. Were the mission, vision, and values considered considering in the strategic plan? Analyze Budget 10. Does the budget reflect a change in resources or priorities given to the programs? 11. Does the budget have similar or different goals/priorities than other organizational documents (e.g., strategic plan, other departmental/program budgets)? HEALTHCARE PRIORITY SETTING Appendix B 19 HEALTHCARE PRIORITY SETTING Figure B-18. This table will be the tool introduced to the organization to assist in priority setting. It will be revised to fit the specific context and situation following review of existing documents. This table was developed by Canham-Chervak et al. (2010, p. S13). 20 HEALTHCARE PRIORITY SETTING Appendix C 21 HEALTHCARE PRIORITY SETTING 22 Preliminary Survey Tool (These questions were developed based on work by Sibbald et al. (2010).) 1. Were you aware that [organization] had a priority setting process? 2. How involved were you in the priority setting? 3. Were you satisfied with your involvement in the priority setting process? Why/why not? Information and Communication 4. Were the following elements communicated to you? a. b. c. d. Purpose and goals Methods Outcomes Revision/appeals 5. Please indicate how well these items were communicated to you. (Rank: they were not, very poorly, adequately, well, very well, and N/A.) a. b. c. d. Purpose and goals Methods Outcomes Revision/appeals 6. Did you understand the purpose and goals of the priority setting process? 7. How could the communication be improved? Information and Communication 8. Was there an explicit and predetermined timeline for the priority setting process? 9. Was a revision or appeals process available (where a decision can be contested or reviewed? 10. During the priority setting process, the following items were considered and to what extent (not at all, minimally, extensively): a. b. c. d. e. Mission, values, vision Strategic plan Context Culture Community values HEALTHCARE PRIORITY SETTING f. Patient values g. Patient needs h. Staff values 11. What other items should have been considered in priority setting? Outcomes 12. Do you understand the outcome of the priority setting? 13. Do you accept the outcomes of priority setting? 14. Are you satisfied with the outcomes of priority setting? 15. To what degree are the following items reflected in the priority setting? a. b. c. d. e. f. g. h. Mission, values, vision Strategic plan Context Culture Community values Patient values Patient needs Staff values 16. In comparison to previous decision making or priority setting, is there consistency in reasoning between the previous and current process? 17. How satisfied were you with the process behind the priority setting? 18. Did you find the tool helpful? 19. How would you improve the process? 23
© Copyright 2026 Paperzz