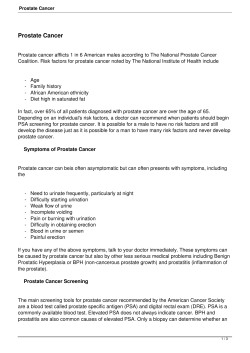
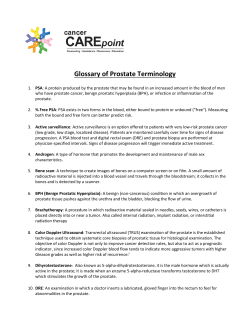
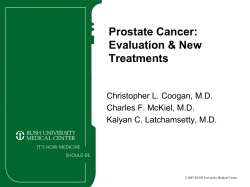
P A A C T, I N C. PROSTATE CANCER COMMUNICATION P ROSTATE CANCER COMMUNICATION NEWSLETTER • VOLUME 21, NUMBER 4 • December 2005 FOUNDER: LLOYD J. NEY, SR. – FOUNDED 1984 President and Chairperson: Janet E. Ney Board of Directors: Edwin Kuberski Treasurer Newton Dilley Helen Mellema Peter Noor Jr. Richard H. Profit Jr. Anthony Staicer Honorary Board Members: Russell Osbun Frank Perry Medical Advisory Board: Richard J. Ablin, Ph.D. V. Elayne Arterbery, M.D. Robert A. Badalament, M.D. Duke K. Bahn, M.D. Israel Barken, M.D. E. Roy Berger, M.D. Michael J. Dattoli, M.D. Fernand Labrie, M.D. Fred Lee Sr. M.D. Robert Leibowitz, M.D. Mark Moyad, M.D., M.P.H. Charles E. Myers Jr. M.D. Gary M. Onik, M.D. Haakon Ragde, M.D. Oliver Sartor, M.D. Stephen B. Strum, M.D., FACP Donald Trump, M.D. Steven J. Tucker, M.D. Ronald E. Wheeler, M.D. Treatment Options for Post-Prostatectomy Incontinence By Gary E Leach, M.D. Director, Tower Urology Institute for Continence Co-Director, Center for Pelvic Health, Cedars-Sinai Medical Center Los Angeles, CA Loss of bladder control (urinary incontinence) after prostate surgery is a devastating complication, which has a significant negative impact on quality of life. The �good news’ is that with appropriate evaluation and treatment, the incontinence problem is usually treatable with significant improvement in quality of life. It is not unusual that lack of bladder control is a problem for the first few months following radical prostatectomy. A biofeedback program may be helpful during this time period to help restore bladder control. When urinary incontinence persists more than 3-6 months after radical prostatectomy, appropriate bladder testing, called urodynamics, is used to evaluate the function of the bladder and sphincter (valve) muscle to determine the exact cause of the post-prostatectomy incontinence (ppi). This urodynamic testing is performed as a 20 minute procedure in the office. The test involves filling the bladder through a special catheter while measuring the pressures in the bladder. During the test, various maneuvers are performed to evaluate the bladder function, demonstrate the urinary incontinence, and thus specifically define the cause of the urine loss. Normally, as the bladder fills to capacity, there is very little change in bladder pressure and the sphincter remains closed allowing the man to stay dry. When incontinence occurs following prostatectomy, this normal balance of bladder and sphincter function is disturbed. Our research1 has defined three main causes of ppi based upon urodynamic findings in men with ppi: 1. High pressure (with �spasms’ of the bladder) developing in the bladder as the bladder fills (50% of men with ppi). These bladder spasms may cause urge incontinence (the need to rush to get to the bathroom), frequent urination, and sometimes loss of urine at night. Let’s Conquer Cancer in OUR Lifetime 2 3 This high pressure bladder dysfunction can also occur following pelvic radiation therapy. Damage to the sphincter muscle (35% of men with ppi). This damage results in stress incontinence with loss of urine during change in position, coughing, straining, or vigorous physical activity. A combination of bladder malfunction and sphincter damage (10% of men with ppi). Men with this combined problem usually experience “mixed incontinence” symptoms with a combination of both urge and stress incontinence. Treatment Options: Biofeedback can be a treatment choice in men who are incontinent and desire treatment early after radical prostatectomy (within the first 3-6 months following surgery). Biofeedback is also a useful treatment option in men who have more minor degrees of incontinence. The treatment program involves weekly visits for about one hour per visit with a trained therapist. A special sensor is inserted into the rectum and attached to the biofeedback computer. During the treatment session, the patient is taught to contract CANCER COMMUNICATON Published Quarterly by: PAACT, Inc. Patient Advocates for Advanced Cancer Treatments 1143 Parmelee NW Grand Rapids, MI 49504 and strengthen the pelvic muscles with this muscular contraction being displayed on the computer screen. Also, an electrical signal can be sent to these pelvic muscles to help strengthen the muscles. Each week, the goal is to make the muscles stronger. Many men experience significant improvement in bladder control with this biofeedback program. With treatment directed by the urodynamic testing, the majority of men are able to experience significant improvement in their urinary control. When the main problem is high bladder pressures, medications to relax the bladder are usually effective. These medicines work by blocking nerve receptors in the bladder. Blocking these receptors results in decreased bladder contractility. Medicines to relax the bladder (generally known as anti-cholinergics) include Enablex, Vesicare, Ditropan XL, Detrol LA, the oxytrol patch, and imipramine. Side effects of these medications may include dry mouth, constipation, and blurry vision. These drugs should not be used in patients with uncontrolled narrow angle glaucoma or in men who do not empty their bladder well. When the oral medications fail to control the high bladder pressures, the Interstim “bladder pacemaker” device can be an excellent treatment option. INDEX Page 1. Treatment Options for Post-Prostatectomy Incontinence (Gary Leach, M.D.) Director…Richard Profit Editor….Richard Profit/Molly Meyers Assistant….Molly Meyers Webmaster….Art Schlefstein 5. When Should You Start Treatment with Ketoconazole? (Mark Scholz, Richard Lam, Brad Guess, Ralph Blum) Postmaster: Send address changes to: Prostate Cancer Communication P.O. Box 141695 Grand Rapids, MI 49514 8. PSA Evaluations in Hormone-Refractory Prostate Cancer (Oliver Sartor, M.D.) Phone: 616/453-1477 Fax: 616/453-1846 E-Mail: [email protected] PAACT Web Page: http://www.paactusa.org Newsletter: http://www.paactusa.org Editor: Articles authored by other than the editor may not fully reflect the views of the corporation but are printed with the understanding that the patient has the right to make his own interpretation of the efficacy of the information provided. In an effort to conserve space and be able to insert as much material as possible in the newsletter, references from various articles are intentionally omitted. If you would like to obtain those references, please contact PAACT, we keep all of the original articles and the references used on file. 10. What The Heck Has Been Going On In My World – Part 9! (Mark A Moyad, M.D., M.P.H.) 14. Everything You Ever Wanted To Know About Chronic Prostatitis: A Critical Update For The “Sons of Survivors – Part II (Ronald E Wheeler, M.D.) 21. Acknowledgements 22. Ask Dr. Barken – Free phone in show. 23. Financial Options for treatment of sphincter damage include biofeedback, injection therapy (which is generally not successful), the artificial urinary sphincter, and the male sling procedure. Those men with “mixed” bladder and sphincter malfunction undergo initial treatment (usually with anti-cholinergic drugs) to improve their bladder function (i.e. lower their bladder pressures) followed by treatment to address the weak sphincter (if necessary). Commonly, follow-up urodynamic studies are performed to evaluate the response to each stage of therapy. Interstim “Bladder Pacemaker” When the usual medical treatments to lower high bladder pressures are not successful, the Interstim “bladder pacemaker” may be an excellent alternative. This treatment involves a “two stage” approach with both stages performed under local anesthesia as an outpatient procedure. The first stage involves placing a special stimulation electrode in the lower back next to the main nerve that controls the bladder (Figure 1a). This stimulation electrode is placed through a special needle under local anesthesia without the need for a large incision. The patient then wears an external stimulation box connected to the stimulation wire for 7-10 days as a “test stimulation” to evaluate the response of the bladder to the electrical stimulation to “relax” the bladder. When a satisfactory response is obtained, we proceed with the second stage of the procedure, which involves implantation of an internal �pacemaker’ generator that is attached to the stimulation electrode and programmed through the skin (Figure 1b). The generator is very similar to a heart pacemaker with a battery that usually lasts 8-10 years. This second stage is also performed under local anesthesia as an outpatient procedure in about 15 minutes. Overall approximately 50-70% of patients respond to the first stage trial of test stimulation. When we proceed with the second stage implant, approximately 85% of patients have an excellent response. Use of the Interstim “bladder pacemaker” is an effective, relatively “non-invasive” treatment option for those patients who have high-pressure bladder dysfunction who do not respond to the usual forms of medical treatment. Surgical treatments of stress incontinence due to sphincter damage following prostatectomy include the Artificial Urinary Sphincter (AUS) and the Male Sling Procedure. In general, injection therapy (i.e. collagen, Durasphere, etc.) has not been successful in men with sphincter weakness. This lack of success is due to the migration of the injected material away from the sphincter area after injection. Figure 1a: Interstim stimulation electrode placed next to nerve that controls the bladder. Figure 1b: Internal Interstim generator attached to stimulation electrode. The Artificial Urinary Sphincter (AUS) Perfected over the last 20 years, the artificial urinary sphincter is a device implanted into the body to correct stress incontinence in men with significant sphincter damage. The AUS has three components: a cuff that helps close the urethra, a pump placed inside the scrotum, and a pressure regulating balloon which is placed in the lower abdomen (see Figure 2). When the man wants to urinate, he squeezes the pump in the scrotum, which opens the cuff around the urethra. Automatically, after 3-5 minutes, the fluid returns into the cuff allowing the cuff to close. After the device is tested during surgery, the cuff is “locked” open, and is only activated when swelling around the pump is gone (usually about 4-6 weeks after surgery). With the current model of the AUS, long-term patient satisfaction has been excellent with less than a 15% mechanical malfunction rate at 7.5 years after implantation of the device.2 Despite these excellent long-term results, however, some men are hesitant to have this prosthetic device placed. For these men, as well as for those with more minor degrees of ppi or for men who do not have the manual dexterity to squeeze the pump in the scrotum, the male sling is a promising alternative. Figure 2: Artificial Urinary Sphincter in place. Male Sling Procedure Over the last few years, the male sling procedure has become a viable treatment alternative for men with ppi due to sphincter damage causing stress incontinence. The “best” candidates for the male sling are men with more minor degrees of stress incontinence (< 2-3 pads/day), men with no previous history of pelvic radiation therapy, and men who have not had a previous AUS inserted. The surgical procedure to implant the sling takes about one hour and can be done either on an outpatient basis or with an overnight hospital stay. The purpose of the “sling” is to compress the urethra and help eliminate loss of urine with coughing, sneezing, or vigorous activity. The sling is placed via an incision between the scrotum and rectum. After exposing the pelvic bone on each side, six titanium bone screws are placed into the pubic bone (three screws on each side). A permanent suture is attached to each bone screw. These sutures are then passed through the material used to create the sling, which will compress the urethra. In the author’s experience, the most effective material used for the sling is a specially prepared synthetic patch which compresses the urethra. Three sutures on one side are passed through one edge of the sling and tightly tied. The three sutures on the other side of the pubic bone are then passed through the sling and tied to create closure of the urethra at a pressure of 60cm water pressure. This pressure is confirmed by running sterile fluid backward into the urethra at 60cm water pressure and confirming that this fluid perfusion stops when the sling is tightened down (see Figure 3). The incision is then closed. A catheter is usually left in place for 24 hours with most men being able to urinate with good control immediately after the catheter is removed. Figure 3: Male sling secured into position. Thus far, the results with the male sling in properly selected patients have been encouraging. In one series of men undergoing the male sling, 40% of men are completely dry, 40% are significantly improved, and 20% are considered failures. Should the male sling not be effective, an artificial urinary sphincter may be considered as a second alternative. Summary Recent advances in the evaluation and treatment of men with incontinence following prostate surgery have allowed many men to regain their urinary control and improve their quality of life. Men with significant incontinence following treatment for prostate cancer should have an appropriate evaluation (i.e. urodynamic testing) to determine the exact cause of their incontinence. Appropriate treatment based upon the results of this testing usually results in significant restoration of bladder control and improvement in quality of life. How to Obtain More Information: Additional information can be obtained on the website: towerincontinence.com. Also, Dr. Leach can be reached by e-mail: [email protected] References: 1. 2. G Leach, B Trockman, and A Wong, et al.: Post-prostatectomy incontinence: urodynamic findings and treatment outcomes. J. Urology 155:1256,1996. F Haab, B Trockman, P Zimmern, and G Leach: Quality of life and continence assessment of the artificial urinary sphincter in men with minimum 3.5 years of follow-up. J. Urology 158:435-439,1997. When Should You Start Treatment With Ketoconazole? Mark Scholz, Richard Lam, Brad Guess, Ralph Blum Ketoconazole, also known as Nizoral is an FDA approved antibiotic that has an additional effect of blocking testosterone production. In the 1980’s, when not used for antibiotic purposes, the drug was primarily administered to men with hormone sensitive prostate cancer, that is cancer responsive to testosterone deprivation. Subsequently it was discovered that high dose Ketoconazole (HDK) is effective against prostate cancer even after the development of hormone resistance. It is HDK’s activity against hormone resistant disease that is of particular interest and the main topic of this article. Prostate cancer is not a single disease but a spectrum of many different illnesses. The more aggressive types of prostate cancer, particularly the hormone resistant variants, need stronger therapy, while lowergrade, hormone sensitive forms can be managed with less toxic agents. Identifying the patients who can benefit from ketoconazole is just as important as knowing the methods for its safe administration. Starting a potentially toxic drug like HDK would be inappropriate in men with low-grade disease. On the other hand delaying the initiation of HDK and allowing the aggressive prostate cancer to proliferate increases the risk of treatment resistance. How delayed treatment results in resistance can be explained by understanding the biology of cancer. Most people don’t realize that there are many different types of prostate cancer. Even less well-known is the fact that several types of prostate cancer can be present in a single individual. When this is the case, these different cancers are called clones. The “clonality” of prostate cancer is illustrated by the Gleason grading system which accounts for the multiplicity of clones by creating a scoring system incorporating two grades, the first and second most common clones. Another important aspect of cancer cell biology is the genetic instability of cancer cells themselves, which can result in mutations. The capacity to mutate means that low grade cancer cells have the potential to transform into more aggressive clones. More aggressive prostate cancer is defined by two basic characteristics: faster growth rates and the development of treatment resistance. Mutations converting cells to more aggressive clones are random events that occur fairly infrequently. However, when cancer cells increase in number, the probability of a mutation increases. This means that treatment-resistant tumor clones become more common as cancer progresses. Gauging the rate of cancer growth has received attention recently as a good way to identify aggressive variants of prostate cancer. Assessing the rate of cancer growth certainly makes sense as we all know that some forms of prostate cancer grow slowly and will never be life threatening. These more benign types of prostate cancer can be safely watched without treatment. However the same cannot be said for faster growing variants. Growth rates are measured by PSA doubling time and PSA velocity. A PSA that doubles in less than 12 months (for men with relapsed disease) or a PSA that increases more than 2 points a year (for men with newly diagnosed disease) are both taken as a reliable indicators for the presence of aggressive prostate cancer. Between these two aspects of aggressive prostate cancer--a fast growth rate or treatment resistance-resistance is the more important. A baseball analogy may convey this concept. Experts in baseball know that the best pitchers dominate and overpower the best hitters. Good hitters have the ability to capitalize on pitching errors when they occur. But skilled pitchers make few errors. In the same way, when an anticancer therapy is working effectively, it stops fastgrowing cancers. The real danger arises when the anticancer treatment stop working. When talking of treatment resistance, what is the type of treatment we are referring to? To most men, prostate cancer treatment usually means surgery. But surgery is not the type of treatment we are referring to. Surgery is not a very effective form of therapy. The New England Journal of Medicine in September of 2002 published a study showing that 20 operations were required to save one life. That means only a 5% improvement in survival at 10 years with surgery. The success or failure of an ineffective treatment like surgery cannot reliably signal the presence of aggressive disease. The type of resistance we are referring to is resistance to testosterone inactivating pharmaceuticals (TIP), otherwise known as androgen deprivation or hormone blockade. The pharmaceuticals we are talking about, just to name a few, are drugs like Lupron, Zoladex, Casodex and Flutamide. TIP is much more effective than surgery. Dr. Messing first reported in The New England Journal of Medicine in 1999 that TIP increases 10 year cancer survival rates 58% to 88% in men with cancer spread to the lymph nodes. This study demonstrates the remarkable effectiveness of TIP in preventing death even in men with more advanced disease. The point is that in men needing treatment because of advancing disease, resistance to TIP is the best way to identify who should quickly be switched to a more effective agent like ketoconazole. Given that TIP resistance creates such a dire situation, what are the signs of its presence? The most obvious sign is a rising PSA despite treatment. Since TIP functions by lowering testosterone in the blood, true resistance must be confirmed by a blood test. A rising PSA with a low testosterone proves that there is TIP resistance. But a rising PSA with a low testosterone is a more advanced sign of resistance. Resistance needs to be spotted early so that effective therapy can be started sooner. An article in the September 2005 issue of the Journal of Clinical Oncology highlighted a better method of identifying resistance. The method, called “PSA nadir” operates by determining how low the PSA drops within 8 months of starting TIP. The authors reported that in men whose PSA failed to drop below 0.2 ng/ml, hormone resistance developed in 75% of cases. We have been emphasizing the importance of PSA nadir as the earliest sign of hormone resistance since 1999 (Journal of Urology). This year we are submitting data to the American Urology Association meeting showing further evidence that nadir is important but also that using an ultra-sensitive assay makes nadir measurements even more accurate. We have found that accuracy increases to 90% using a PSA nadir of 0.05 instead of 0.2. In June of this year we published another study in the Journal of Urology showing that longer remissions occurred in men with hormone resistance who were started on HDK with lower PSA levels. Based on this data we believe the effectiveness of HDK will be even further improved if HDK is started before the PSA starts rising, i.e. as soon as a high PSA nadir is detected. The mechanism by which HDK functions to kill prostate cancer cells has been debated for years. Some have argued that HDK works primarily by fur- ther lowering testosterone levels. But what has been confusing is that HDK can induce remission in men whose testosterone is already low. This capacity suggests that HDK has some form of direct killing effect on prostate cancer cells independent of its testosterone-lowering effect. This belief has been supported by studies showing that HDK suppresses the growth of hormone resistant prostate cancer cells grown in the laboratory. Further light was shed on this question of HDK’s mechanism of action in an article published in the Journal of Clinical Oncology March of 2004 by Eric Small. In this study Dr. Small showed that two testosterone-like hormones coming from the adrenal glands--DHEA and Androstendione (Andro),--were in the blood at higher levels in men with hormone resistant disease that responded to HDK therapy (Andro is the same chemical Mark Maguire is supposed to have taken to hit all those home runs). These same researchers also reported that resistance to HDK in men that were previously responding was signaled by rising levels of DHEA and Andro. This connection between the levels of these hormones and HDK effectiveness appears to confirm a long suspected relationship between HDK’s potent hormone blocking ability and its anti-cancer activity. This connection, established by Dr Small and his collaborators, also fits logically with other research theories that have long suggested that resistance to testosterone blockade is not total but only partial. According to this theory, cancer clones thought to be resistant to testosterone deprivation are not truly hormone resistant. Rather these “hormone resistant clones” are cancer cells with a capacity to grow using the weaker forms of testosterone like DHEA and Andro. Dr. Small’s report indicates that DHEA and Andro production can resume even when adequate levels of HDK in the blood have been documented. This can happen through a process called tachyphylaxis. This is the same bodily process that occurs when morphine addicts require higher and higher doses of morphine to get the same pleasurable results they obtain in times past. What happens is that the body adapts to the morphine, becoming less sensitive to the drug as time goes on, requiring larger and larger doses to achieve the same effect. The hormones we are concerned about--testosterone, DHEA, and Andro-are being produced in two different areas of the body, the adrenal glands and the testicles. How best to manage breakthrough DHEA and Andro production from the adrenals, is not known for sure. Possibilities include restarting HDK after a short holiday period, a trial of a related agent called Cytadren, or perhaps a switch to a completely different class of testosterone blocker, Nilutamide. for what has been termed the “anti-androgen withdrawal response.” It is true that 10-15% of men experience a transient PSA decline lasting an average of 3 months with this maneuver (the Lupron or Zoladex is continued). In our experience these responses are too infrequent and too brief to justify delaying the initiation of a more effective treatment such as HDK. Managing testosterone production from the testicles is a straight forward proposition. Lupron or one of its many alternatives such as Zoladex, Eligard, or Trelstar, is very effective. Since there is a risk of uncontrolled testosterone production from the testicles during HDK treatment, it is our customary practice to continue a drug such as Lupron when using HDK to prevent this from happening. Over the years we have seen mixed results in men who have elected to stop HDK therapy after they achieved a good response and maintained a low, stable PSA. Some of these individuals have responded well when the PSA started rising and the HDK therapy was reinitiated. In some other cases restarting HDK proved ineffective. There is no way to know if a treatment holiday contributes in any way to the onset of HDK resistance. Other explanations besides tachyphylaxis must be considered when it appears that HDK is not working. One possibility is that the ketoconazole is not being absorbed from the stomach into the blood. This possibility is easily evaluated by measuring the amount of HDK via a simple blood test. If the level in the blood is below 1, poor absorption is the most likely explanation. HDK is absorbed best when taken without food and in combination with an acidic agent, like vitamin C (ascorbic acid). The typical dose of ketoconazole is one 200 mg pill every 8 hours increased to two pills every 8 hours if there are no side effects. Once HDK has been started, the PSA should be checked every 2 to 4 weeks to determine whether or not it is effective. A rising PSA after 30 days does not invariably mean that HDK will prove to be ineffective with further treatment. We generally recommend waiting 60 days before concluding that HDK is ineffective. The ultimate goal is a PSA that ends up declining 75% or more from baseline, since it is this threshold that has been associated with longer survival. Such declines, when they occur, usually occur over a number of months. In the study we published in the Journal of Urology, June 2005 in 79 men with varying stages of hormone resistant prostate cancer, a 75% or greater decline in PSA occurred 44% of the time. It has been argued that in men showing early signs of hormone resistance, HDK therapy should be delayed until the results of stopping Casodex or Flutamide can be ascertained. This is accomplished by looking Ketoconazole can have a variety of side effects and drug interactions. The number of potential drug interactions is very extensive and includes most diabetes medications, many allergy medications, blood thinners, as well as some types of sleeping pills and certain antibiotics. Careful review of all potential drug interactions is essential for anyone starting ketoconazole. The most prominent direct side effect of HDK is fatigue. The degree of fatigue varies from individual to individual. The best method to minimize fatigue is to maintain muscle strength with a weight lifting program for at least one hour twice a week. We have also seen some benefit with the use of a medication call Provigil, a drug that is FDA approved for the treatment of narcolepsy. Other common side effects from HDK include stomach and liver problems. Initially, blood tests to check liver function must be done monthly. If any abnormalities are detected the drug must be stopped immediately. Usually HDK must also be stopped if stomach problems like heartburn develop, since taking antacids blocks its absorption into the blood stream making HDK ineffective. An additional hormone besides DHEA and Andro is also produced in the adrenal glands. This hormone, called hydrocortisone, is also blocked by HDK just like DHEA and Andro. Many of us are aware of the undesirable effects of excess cortisone which is sometimes administered in the form of injections or pills by physicians for the treatment of arthritis, asthma, and allergic reactions. Excessively low hy- drocortisone levels can also be dangerous. The first sign of a low level is significant fatigue. The inability of the adrenal glands to release extra hydrocortisone into the blood stream during times of stress is another danger. For this reason hydrocortisone replacement 20 mg with breakfast and 10mg with lunch is routinely administered. Men taking hydrocortisone should wear a bracelet so that if they are knocked unconscious, emergency personal know to administer intramuscular hydrocortisone. The most encouraging aspect of high dose ketoconazole treatment is the possibility of extended remissions lasting for years. If the medication is well tolerated over the first few months it usually continues to be well tolerated throughout the course of treatment. We believe that the best results can be obtained by starting HDK treatment early, before the disease has time to proliferate, mutate, and produce multiple treatment-resistant clones. This means that the best time to start HDK is at the very first sign of hormone resistance, when the PSA nadir on TIP is greater than 0.05 ng/ml. PSA Evaluations in Hormone-Refractory Prostate Cancer Oliver Sartor, M.D. PSA is frequently incorporated into the management of hormone-refractory prostrate cancer (HRPC) patients but is not accepted as an endpoint in clinical trials by the FDA for drugs that are being tested with registrational intent. How is it possible that this commonly used test is not accepted by regulatory authorities and many leaders in the field? First let us examine some of the imperfections in PSA. PSA most directly reflects activity of androgen receptor (AR) activity in prostate cells, and specifically PSA is not a true marker of cell proliferation. Measurements of PSA are more likely to yield estimates of the total volume of PSA producing cells which is not the same as the volume of cancer and is certainly distinct from rate of growth. We know that any drug (leuprolide, gosarelin, bicalutamide, flutamide, dutasteride, finasteride, testosterone, etc.) that affects androgen levels or the androgen receptor influences PSA to a significant degree. We also know that it is folly to over-evaluate changes of PSA when testosterone levels are changing. It is also critical for readers to understand that agents that interact with the androgen receptor (such as the antiandrogens) are conceptually the same as testosterone or dihydrotestosterone (DHT) lowering agents (see Table 1). Table 1. Some Drugs and Hormones Affecting Activity at the Androgen Receptor Hormones AntiLHRH 5-Alpha Androgens Analogues Reductase Inhibitors Testosterone Bicalutamide Leuprolide Dutasteride (Casodex) (Lupron, (Avodart) Eligard) DihydroFlutamide Gosarelin Finasteride testosterone (Eulexin) (Zoladex) (Proscar) DHEA Nilutamide Triptorelin (Nilandron) (Trelstar) Most importantly, PSA declines have not consistently been a surrogate for survival, particularly in HRPC trials. The pivotal TAX327 trial (1) is one case in point. In that trial, the prednisone/dexamethasone/docetaxel every 3 weeks arm and the prednisone/dexamethasone/docetaxel weekly arm had essentially similar PSA >50% decline rates (45% and 48%, respectively) yet only the every 3 week regimen demonstrated a survival advantage compared to prednisone/mitoxantrone. Despite the fact that patients with a PSA response had a 60% reduction in mortality risk compared with PSA nonresponders, a careful analysis indicated that only approximately half the treatment effect on overall survival was accounted for by the PSA response as analyzed in that study (2). The ASCENT trial (3) is another pointed example. In that trial, PSA declines (>50%) were not statistically distinct between arms (calcitriol/dexamethasone/docetaxel versus dexamethasone/docetaxel), but in the multivariable analysis survival was favorably impacted in the experimental arm. It is perhaps relevant to note that the ASCENT trial is still relatively immature with regards to survival, thus the preliminary conclusions and the final conclusions could be distinct. Do these examples mean that PSA is not useful in HRPC? Perhaps not, there are many ways to examine PSA changes other than declines of >50%. Surrogates are typically continuous and not binary (4). Thus simple binary analyses (PSA decline of greater or less than some arbitrary cut-point) may be suboptimal in attempting to establish best predictive values. Any measurement of PSA decline that does not incorporate duration may not capture important information. Better information capture may be accomplished by requiring a minimum duration or decline (for example, 8 or more weeks), by stipulating a “landmark” analysis time point that conveys some duration of the response (i.e. 12 weeks after start of therapy), or by calculating “area under the curves” which combine information regarding the duration and extent of PSA decline. Undetectable PSA nadir is a concept that is increasingly invoked as a critical variable in hormonally treated patients (5,6). HRPC patients rarely have undetectable PSA nadirs due to the relative inactivity of current drugs. Highly effective therapies would potentially advance the field of PSA surrogacy as these agents would potentially permit the role of undetectable PSA to be explored in HRPC (just as viral titer nadirs have been successfully used in HIV infected patients after highly active anti-retroviral therapies). In the presence of highly active therapies, failure to achieve an undetectable nadir will in all probability represent a predictor for survival however we need better therapies in order to test this hypothesis directly. The importance of PSA kinetics (see Figure 1) are widely appreciated in earlier stage disease yet PSA kinetics (such as velocity or doubling time) have yet to be fully explored in HRPC survival studies. Preliminary data reported by Crawford et al (7) indicate that PSA velocity measured during the first 3 months of chemotherapy provides independent prognostic information to treatment. Oudard and colleagues have demonstrated that PSA “half time” (another PSA kinetic measure) during chemotherapy is strongly associated with survival (8). Incorporating time to progression (another variant of PSA kinetics) in HRPC patients is only now beginning to be explored. An analysis from NCI data recently concluded that PSA progression-free survival is an excellent predictor of survival (9). Because time to progression is so critical, it in fact may be a better predictor of survival than PSA declines. This needs more exploration. Though decreases in PSA may be controversial, increases in PSA are not. Most everyone conceptually agrees that a PSA rise is associated with poor prognosis and thus the percentages of patients with PSA rise, and the timing of PSA rises, may be appropriate to carefully examine. It is also important to consider the rate of rise. Every rise is not equivalent. Those patients that rise faster do worse. Taken together, PSA changes, particularly PSA changes over time, represent a fertile field for additional investigation in patients with HRPC. To dismiss the importance of PSA because it has failed to perform perfectly in some well publicized studies may be premature. This potentially important variable is in need of additional and very thorough study in order to maximize its potential. References 1. Tannock IF, de Wit R, Berry WR, Horti J et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004 Oct 7;351(15):1502-12. 2. Roessner M, de Wit R, Tannock IF, et al. Prostate-specific antigen (PSA) response as a surrogate endpoint for overall survival (OS): Analysis of the TAX 327 Study comparing docetaxel plus prednisone with mitoxantrone plus prednisone in advanced prostate cancer. 2005 ASCO Annual Meeting Abstract 4552. 3. Beer TM, Ryan CW, Venner PM, et al. Interim results from ASCENT: A double-blinded randomized study of DN-101 (high-dose calcitriol) plus docetaxel vs. placebo plus docetaxel in androgen-independent prostate cancer (AIPC). 2005 ASCO Annual Meeting Abstract 4516. 4. Johnson K, Stokes B, Anthony D, et al. Modeling oncology surrogate markers. 2005 ASCO Annual Meeting, Abstract 9639. 5. Bianco FJ, Kattan MW, Beekman KW, et al. Prognosis after androgen deprivation therapy in men with a rising PSA after prostatectomy. 2005 ASCO Annual Meeting Abstract 4552. 6. Stewart AJ, Scher H, Chen M, et al. The clinical significance of a PSA nadir > 0.2 to patients with a rising post-operative or post-radiation PSA treated with androgen deprivation. 2005 ASCO Annual Meeting Abstract 4547. 7. Crawford ED, Pauler DK, Tangen CM, et al. Three-month change in PSA as a surrogate endpoint for mortality in advanced hormone-refractory prostate cancer (HRPC): Data from Southwest Oncology Group Study S9916. Journal of Clinical Oncology, 2004 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 22, No 14S (July 15 Supplement), 2004: 4505. 8. Beuzeboc P, Banu E, Goubely Y, et al. Corrected area under prostatespecific antigen (PSA) curve and PSA half-time dynamics during chemotherapy. A new prognostic classification for hormone-refractory prostate cancer (HRPC) patients. 2005 ASCO Annual Meeting. Abstract 4641. 9. D'Amico AV, Chen M, Cox MC, et al. Intermediate end point for survival for patients with hormone refractory metastatic prostate cancer. 2005 ASCO Annual Meeting. Abstract 4553. WHAT THE HECK HAS BEEN GOING ON IN MY WORLD-PART 9!!! By Mark A. Moyad, M.D., M.P.H. I am often asked what the M.P.H. in my name/title stands for and some people think it means “Miles per Hour,” but this is wrong. It stands for “Masters in Public Health.” Okay, now I feel better - that was my brief moment of therapy. Next, by the time you read this article the Michigan and Ohio State football game will be over, and although Michigan has lost half of its team to injuries, I still think Michigan will win. Now, there is little more I can say about this game because it is the greatest football rivalry in sports, and anytime I predict scores or mention other things about Ohio State I seem to get a lot of hate mail. Therefore, since I have no desire to spend the rest of my natural born life in the F.B.I. witness protection program I will only discuss more about this game and really rub it in if we win this year! What if we lose? I will still support the Big Ten (greatest conference in the universe) in all bowl games regardless of the Big Ten team that is there (notice how I capitalized the words Big and Ten). 60) I would like a free booklet on rising PSA while on hormone therapy. Is there such a free booklet? I am glad that you asked this question! Yes, several researchers and patients put together a free color booklet (more than 50 pages) that talks about everything from hormone therapy side effects, diet, secondary hormonal therapies, chemotherapy, clinical trials…. LET ME SAY THIS AGAIN - THIS BOOKLET IS FREE AND ALL YOU HAVE TO DO TO GET IT IS TO LOG ONTO THE WEBSITE www.iche.edu and order the booklet. The booklet is officially entitled “Living with Advanced Prostate Cancer: When PSA rises during hormone therapy.” What is the catch??? There has to be a catch? Yes, there is because you have to get on the internet in or- der to get this booklet. Otherwise, there is no catch!! These dedicated patients and researchers devoted a lot of time in order to make this unique booklet available to anyone that needs it. If you do not have a computer then just go to the local library, but in my opinion everyone needs to just GET THE BOOKLET. Who knows when another booklet or offer will be made to patients?! 61) Do intensive lifestyle changes impact the progression of prostate cancer? (Reference: Ornish D, et al. Journal of Urology, September 2005, volume 174, pages 1065 to 1070.) This was a long awaited clinical study of men that decided not to have conventional therapy done after being diagnosed with prostate cancer. A total of 93 men with a PSA of 4 to 10 and a Gleason score of 6 or less were assigned to an intensive lifestyle change group or control group for 1 year. Keep in mind that these men did NOT have aggressive prostate cancer. The average age of these men was between 65 and 67 years of age. The average starting PSA was approximately 6.3 ng/ml, and the average testosterone level was about 400. The experimental group adhered to the following lifestyle changes: -Vegan diet (no animal products and 10% of calories from fat) -Soy products (1 serving of tofu daily + 58 grams of a fortified soy protein powdered beverage) -Fish oil (3 grams daily) -400 I.U. a day of vitamin E -200 mcg a day of selenium -2 grams/day of vitamin C -moderate exercise (walking 30 minutes/day - 6 days a week) -stress reduction or management (yoga, breathing, meditation, imagery and relaxation for 60 minutes a day) -1-hour support group once weekly None of the lifestyle change men had conventional treatment, but 6 of the control patients had conventional treatment. The average PSA decreased 4% in the lifestyle change group, but increased 6% in the control group. The good news about this study is that it was simply done. You have to give credit to these researchers and patients. The conclusions of the researchers in this study were as follows: “Intensive lifestyle changes may affect the progression of early, low grade prostate cancer in men. Further studies and longer term follow-up are warranted.” However, the editorial comments following the paper were a little different. Paul H. Lange, M.D. from the University of Washington called the differences in PSA from the lifestyle group versus the control group “meager.” I have no desire to comment on this study except to say that many researchers thought the study was great and others thought the results were not so great because despite all the different things these patients had to do during the study there was not a gigantic drop in PSA. Regardless, I think everyone agrees that lifestyle changes before and after a diagnosis of prostate cancer makes sense and should be discussed. This is the common conclusion of this important study. However, the disagreement lies in how much lifestyle change should be done after being diagnosed with prostate cancer? Should the changes be moderate or more extreme? This study suggests that the changes should be more extreme. I am not sure I agree with this, but I do not have the kind of published research that these researchers now have so this is a good study to discuss with your doctor. I do have over a decade of working with prostate cancer patients on dietary changes after being diagnosed with prostate cancer, so again, I believe in a more moderate approach, but stay tuned because there is more research to come from many different groups around the country. In the meantime, you can criticize or not the results of this Ornish study, but in the end you have to give these researchers and patients credit. They are bringing more attention to lifestyle changes after a diagnosis and I believe this is a very, very good thing!!! 62) Aspirin and NSAIDs may reduce the risk of colorectal cancer, but it comes with an apparent increased risk of a bleeding event. (Reference: Nurses Health Study and aspirin JAMA 2005) The Women’s Health Study did NOT find that a baby aspirin taken every other day could reduce the risk of colorectal cancer in healthy middle-aged women over 10 years. However, recent data from the Nurses’ Health Study suggests that it might in larger doses over a longer period of time. This was a prospective study of 82,911 women with a 20-year follow-up period, median age of 46-49 years, and 97% of this cohort consisted of Caucasian women. Women that used regular strength aspirin tablets (325 milligrams) two or more times per week experienced a 23% reduction in risk compared with women that did not use aspirin. However, no significant reduction was found unless women ingested aspirin for more than 10 years. The reduction appeared to be related to the dosage, but so did the risk of gastrointestinal bleeding. A similar dose-response association was found for NSAIDs (ibuprofen, motrin…) users. The researchers of this study concluded that the use of regular aspirin for a long-period of time seems to reduce the risk of colorectal cancer, and NSAIDs have a similar impact. However, these researchers also commented that “These results suggest that optimal chemoprevention for colorectal cancer requires longterm use of aspirin doses substantially higher than those recommended for prevention of cardiovascular disease, but the dose-related risk of gastrointestinal bleeding must also be considered.” The researchers from this study also did a very good job of putting these results in perspective by stating, “…use of aspirin at the highest-dose category compared with no use of aspirin would prevent 1 to 2 cases of colorectal cancer with an excess of 8 episodes of major gastrointestinal bleeding for every 10,000 person-years.” Acetaminophen (Tylenol®…) had no impact on colorectal cancer risk, and this finding has also been supported for years from other major studies. Bottom Line = Regular strength aspirin (325 mg) used for more than a decade may reduce the risk of colorectal cancer, but the risk of a major gastrointestinal bleeding event is also increased to a degree where this side effect risk exceeds the benefit for many women. Therefore, in my opinion no woman or MAN should take aspirin for the prevention or treatment of any cancer without first discussing with their doctor the risk to benefit ratio. 63) Is the Bird Flu coming to get me? I do not believe so, but isn’t it interesting that despite the fact that most infomercials telling the public that researchers today do not have any of the answers it seems that we are completely dependent on these same researchers for giving us an effective medication and vaccine. Have faith in conventional medicine researchers because they are the best hope for preventing and treating this disease if it becomes a problem. ALSO, in order to ensure faith in your average conventional researcher please read the information in #64. 64) I could not sleep last night and I saw several infomercials that told me that conventional medicine is not the answer and that we have made no progress against disease. Is all this stuff true? (Reference: Jemal A, et al. JAMA 2005;294:1255-1259.) (Reference: He J, et al. N Engl J Med 2005;353:1124-1134.) If you happen to believe some of these infomercials then I have some valuable swampland in Michigan that I want to sell you ASAP! Let’s put some things in perspective for the next time that you have difficulty believing in our so-called “conventional” medicine system. Do you know what the average life expectancy of a human born in the year 1900 was….???? It was about 47 years of age! That’s right!!! In about one century we have doubled the average life expectancy!! Now, that is real success. In fact, a baby born in the U.S. right this second will have the longest predicted life expectancy of any previous generation since the beginning of time. Wow, this is real success! In fact, if you look at just the years between 1970 and 2002 a real remarkable trend has been taking place in public health and research in the U.S. The overall age-adjusted death rate from all causes combined has been reduced from 1242 (per 100,000 per year) in 1970 to 845 in 2002. In fact, the death rate from stroke has been reduced by 63%, heart disease death rate has been reduced by 52%, and deaths from accidents have been reduced by 41%. Recently, death rates from all cancers combined have also begun to decrease. So, then why are you hearing that there are more people diagnosed and dying from all major diseases? There is a simple answer to this question. You see, one of the agreed upon risk factors of most major chronic diseases is simply aging. Yes, aging has become one of the biggest risk factors for most major chronic diseases. For example; cancer, heart disease, and even diseases like Alzheimer’s have a common risk factor (aging). The body gets older and most people have to die of something so of course there are more of these diseases than ever before, but the average age of death from these diseases just keeps increasing. So, the infomercials are right in the sense that there are more people than ever before dying from some of these diseases, but what they fail to mention is that the average rate or age of dying from these diseases keeps increasing. So, come on let’s keep these statistics in their proper perspective. Of course we need to do a better job of treating and preventing many diseases, but at the same time the success of conventional medicine has been nothing less than amazing. The latest national report of causes of death also indicated that the death rate from pulmonary disease has increased, that in large part is due to smoking, and the death rate from diabetes has increased, which may also be due in large part to the obesity problem in this country. Regardless, the average age at the time of death just continues to increase, which reflects the success of our system. Some people say, well then why do people in China for example live longer than people in the U.S.??? Is this really the case?! A recent look at the causes of death from China found that cardiovascular disease and cancer are now the leading causes of death in China similar to the U.S. However, when looking at just the middle-age population in this country the death rate from cardiovascular disease and cancer has now surpassed the death rate from these diseases in the U.S. Therefore, although you may hear that in some areas of China people are living longer; overall this is really not the case. I get tired of some infomercials beating up on our medical system and our researchers because the real statistics are not really being mentioned. Researchers in this and other countries are doing a damn good job and they should be getting more credit. In fact, I have more confidence than ever before in these researchers. If they receive even more funding I believe we will continue to see amazing advances in medicine. So, please contact your local congressperson and senators and demand more medical research funding overall. The head of the FDA and National Cancer Institute (NCI) is a prostate cancer survivor; therefore, the time is more than ripe to demand more funding because I think your voice will be heard. We tend to forget that recent advances in AIDS research or advances in breast cancer, or a cervical cancer vaccine are the result of more research. For example, you may have heard about the recent advances in breast cancer with the drug Herceptin®, but this is the result of researchers receiving more funding. The time is now to have more confidence than ever in your researchers, but without serious funding these individuals can never make the advances that will be needed over the next few years. Okay, I will now get off my soap-box!! Just a second!! Before I get off this soap-box, don’t you find it interesting that some of these infomercials pretend that they are actually official interviews rather than an infomercial?! In other words, if they are attempting to be so scientific then why are they pretending to be something that they are not! Who is really getting duped here?! So, come on if you want to see real advances in medicine then support those individuals who are really trying to solve medical problems and not many of the clowns in the circus of infomercials. Of course, I am not implying that we do not have problems in our own conventional medical system, but this is the same system that has helped to extend life expectancy more than any generation that has ever come before us!!! I believe we really sit at a critical moment in medical research. Currently, our system not only has the dedicated individuals, brain power and technology to solve most of our major medical problems, but without the funding of your local researchers it will be hard to continue to build on the current level of success. However, I think that over the next few years as funding increases we will see treatments improve at a pace that was never imaginable just a few years ago!!! 65) I hear that vitamin D is a real amazing vitamin, but where do I get this stuff from food or beverages? (Reference: Consumer reports 2005.) Please keep in mind that ultraviolet B light from the sun is one of the best sources of vitamin D. However, we are a nation on sunscreen and as we get older the body’s ability to make vitamin D becomes less effective. Also, obesity seems to reduce the blood level of vitamin D because most of it gets stored in fatty tissue. So where can you get vitamin D? First of all, if you really want to know about your vitamin D level, please ask your doctor about getting a blood test for vitamin D. A cheap, low-dose multivitamin is a very good source of vitamin D and individual vitamin D supplements and prescription drugs are also very good sources. However, you should also keep in mind that eggs, mushrooms and seafood are the only real natural sources of vitamin D. For example; the average egg contains approximately 25 I.U. of vitamin D. Also, most fish and shellfish contain 100 to 500 I.U. of vitamin D. For example, a serving of catfish contains about 425 I.U. of vitamin D, mackerel about 400 I.U., salmon about 250 I.U., sardines (yummy) about 230 I.U., tuna in a can about 135 I.U., shrimp about 120 I.U., and mushrooms about 50 I.U. What about fortified products like milk? They have added vitamin D, but some of these fortified products have not been entirely reliable sources of vitamin D. I realize that many of these fortified products make certain claims about the amount of vitamin D, but some research suggests that some of these products have less than the amount stated on the label. Regardless, please remember the saying “eggs, fish, mushrooms, and multivitamins” because these are some of the better sources of vitamin D. Regardless, if you are really interested in vitamin D or the vitamin D blood test, please talk to your doctor! Finally, is it true that the darker your skin color the more sunlight you need to produce vitamin D? This is true, because the darker your skin the greater the ability your skin has to protect you from ultraviolet light, but at the same time the more difficult it is to produce vitamin D. 66) I hear that only really colorful fruits and vegetables should be consumed because they contain the most antioxidants and nutrients. Is this true? (Reference: FDA/USDA 2005.) If you believe this, then again, I have some swampland to sell you in Michigan. All fruits and vegetables have something to offer and I will talk about this in a later edition. In the meantime, let’s just look at the poor old piece of celery, which really is not that colorful and is quite boring in appearance. Just 2 medium stalks of celery contain only 20 calories and that is a good thing. It also contains zero fat calories, 350 mg of potassium, 2 grams of dietary fiber, 15% of the daily value of vitamin C, and contains calcium. Regardless, because it contains a good deal of fiber it can help to lower cholesterol and make you feel fuller. The real point here is your diet is supposed to be fun and easy and I get tired of hearing from the so called “experts” that some fruits and veggies that are not that colorful do not have much to offer. This is silly!!! HAVE A NICE HOLIDAY AND MAY YOUR UPCOMING VACATION BE FILLED WITH FAMILY FUN, EGG-NOG, AND CELERY. Finally, Mark I heard you are the new editor of a medical journal by Elsevier called “Seminars in Preventive and Alternative Medicine.” Is this true? Yes, it is and if you go to the web-site of Elsevier publications (www.elsevier.com or call 1-800-654-2452) you can order the same medical journal that the health professionals can use that updates the latest on diet, supplements, and drugs… for cardiac disease, different cancers, and anything else that is happening in preventive and alternative medicine. This is the end of this shameless promotion until the next issue, when I will have exciting new news about another new publication. Everything You Ever Wanted To Know About Chronic Prostatitis: A Critical Update For The “Sons Of Survivors” PART II By Ronald E Wheeler, M.D. THE PROSTATE BIOPSY REVOLVING DOOR: The inability to maintain a normal PSA (less than 1.0 ng/ml ideally) will put you in a unique group of men asked to consider a biopsy of the prostate. Men unique to this group who fail to stabilize the PSA (preferably less than 4.0 ng/ml) will become the hunted. Once the biopsy scheduling (merry-goround) begins, it is difficult to prevent subsequent biopsies, as anxiety is what drives the process in the absence of a cancerous result. As doctors, it is important to find disease, seemingly at any cost, in men who will benefit the most from our therapies. If your PSA is high (≥ 4.0 ng/ml), your prostate will become the target of a biopsy needle with virtually any Urologist you meet. While I might be an exception to the traditional Urologist, there are basic principles that need to be applied when a clinical scenario presents itself as consistent with prostate cancer. In my clinical practice, men with a non-cancerous digital prostate examination can defer the biopsy when prostatitis is identified and the preferred recommended treatment course is followed. Obviously, the Peenuts® prostate nutritional formula is an integral part of the program. The inability to resolve the degree of disease as determined by a normalized PSA will put us back at square one where the biopsy makes most sense. A classic example of a patient’s experience in the traditional doctor’s office involves a 65-year-old man from Lubbock, Texas who had noted a PSA of 18 ng/ml. His Urologist appropriately offered and performed an ultrasound examination and prostate biopsy. The biopsy result noted chronic prostatitis with no evidence of cancer. Antibiotics were ordered despite the lack of a positive culture and sensitivity, with no other therapy considered. Remember that less than 5% of cases of prostatitis are actually caused by bacteria; potentially curable with antibiotics. His PSA was repeated after 6 months and found to be unchanged. The patient underwent a second prostate biopsy, at the doctor’s insistence, which again showed only chronic prostatitis. When the patient asked his doctor what he could do, the urologist offered to repeat the PSA in another 6 months and consider an additional biopsy at that time. This is a clinical scenario that is all too common across the United States whereby men are given no alternative in an attempt to avoid a future biopsy. I believe, as physicians, we must become better educated regarding relevant scientific concepts that may radically change the diagnostic or treatment course of any patient. Far too many men are asked to return to the biopsy arena over and over, without a well thought out, patient-friendly strategy or “masterplan.” In this case, the patient was aware enough to research prostatitis on the Internet. Eventually, he discovered a nutritional product that improved his urinary symptoms substantially and reduced his PSA by almost half, in only 3 months. This was accomplished by merely using an advanced nutritional therapy for the prostate called Peenuts®, which he was able to purchase without a prescription! While this patient’s response was outstanding, not all patients respond identically. The use of the Peenuts® formula is not intended to replace the advice of your doctor but your thoughts (as the patient); will play a role in the physician’s decision. Another equally riveting case involved a 75-year-old male who had experienced five previous biopsies (all negative) associated with a PSA of 22.6 ng/ml. Using only Avodart® (Dutasteride) and the Peenuts® prostate nutritional formula, his PSA dropped to 7.88 ng/ml by the end of 11 months and 5.1 ng/ml at 24 months. Without the presence of prostate cancer, Avodart® would have been expected to cut the PSA in half or to 11.3 ng/ml. The improvement to 5.1 ng/ml is exceptional and validates further the benefit of the Peenuts® nutritional formula related to the resolution of prostatitis. While this approach likely shows the benefit of Avodart® and Peenuts® in combination, the need for additional biopsies is now gone as the patient’s prostate health status has improved markedly. While further studies with this treatment protocol are encouraged, the expectation remains high that similar results will be forthcoming. “NATURAL THERAPIES” FOR PROSTATE DISEASE: THE ROLE OF NUTRITIONAL THERAPIES FOR PROSTATITIS, BPH AND PROSTATE CANCER The 5 Keys to Systemic Health include: Proper Diet, Appropriate Nutrition, Adequate Exercise, Stress Re- duction, and Education. Not surprisingly, these same categories are equally important to prostate health. Regarding the diet, I recommend a modified Mediterranean Cuisine. Specifically, this diet is devoid of saturated fats associated with red meat and dairy products. Nutritionally, I recommend the scientifically validated natural product called Peenuts®, taken at 2-3 capsules per day with meals. Additionally, I recommend Omega-3 fatty acids, based on scientific data that supports the inhibition of known prostate cancer cell lines. This activity takes place with the daily supplement of Eicosapentaenoic acid and Docosahexaenoic acid in an appropriate dose. The need for daily exercise cannot be understated based on enhancement of the immune system and cardiovascular benefit. Stress reduction is critical to the avoidance of many illnesses while assisting a strong immune system. Last, but not least, education will empower the patient to make improved decisions regarding disease prevention and/or treatment. An extended commentary on the diet will be forth-coming in my upcoming book, entitled, “Men at Risk: A Rush to Judgement.” Beyond the 5 Keys to systemic and prostate health, natural remedies for prostate related disease are centuries old. The ancient Chinese, for example, used a combination of Amino Acids, including Glutamic Acid, Alanine and Glycine successfully, for prostate maladies. It is not surprising that various remedies used today contain some combination of these beneficial Amino Acids. Saw Palmetto (Serenoa Repens, Dwarf Palm), indigenous to Florida valued for its Beta-Sitosterol content, has been revered by some and reviled by others. Unfortunately, when the data is reviewed, Saw Palmetto does not demonstrate adequate clinical efficacy, in men with prostate related symptoms. In a randomized, placebo controlled, double-blind study, sponsored by the NIH, Saw Palmetto did not perform clinically any better than a sugar pill (placebo) at one year (N = 225 men). Men were evaluated by the American Urology Association Symptom Index (AUASI), as the primary study outcome. Additionally, maximal urine flow, post void residual, prostate size and other health-related issues were assessed. Take home message: Saw palmetto alone is inadequate to effectively reduce or maintain prostate symptoms and may actually mask prostate disease. To state further, while I personally believe that Saw Palmetto has synergistic benefit when added to other ingredients, it may mask disease recognition, when used alone, by improving slightly the only signal (sign or symptom) a man may have that a problem exists. Specifically, men commonly look to Saw Palmetto when there is any sign of urinary difficulty. As many men “self-treat the symptoms,” any mild improvement (placebo or real) will commonly delay a doctor visit, but more importantly, miss an opportunity to assess prostate health, through a Prostate Specific Antigen (PSA) blood test. The need for a PSA at the time men have urinary symptoms cannot be understated, as prostate disease is the #1 health risk that men face. This should not turn into an opportunity lost. The PSA test will serve as your baseline from which to compare others. An additional reason to get a PSA beginning at age 30-35 is based on the fact that it is not uncommon for men to have prostate disease in an absence of any voiding symptoms. (To order a PSA “Diagnostic Home Kit,” please contact our office (toll free) at 1-866-PSA-CHEK (772-2435). While I endorse natural remedies for prostate disease that can be validated, independent of generic ingredient claims, men should choose a product or formula that works versus prostatitis primarily. While 50% of 50-year-old men will have prostate enlargement, virtually all men, at this age, also have prostatitis as noted through an evaluation of voiding symptoms and EPS (expressed prostatic secretion). Specifically, data presented at the NIH in 1999 showed that 81% of men less than 50 years old, with any level of urinating symptoms, had prostatitis (n = 83), while 88% of men aged 50 or older had prostatitis (n = 152), as judged by the EPS. Take home message: Voiding (Urinary) symptoms represent non-bacterial Prostatitis, until proven otherwise, in men of any age, notwithstanding the possibility that prostate enlargement may also be present. Because prostate enlargement begins in most men by their mid-forties, it would appear likely that multiple disease processes play a role in a male of this age. Despite the controversy, there are few, if any, dependable, disease-altering natural remedies for prostate enlargement. Much of the older historical data suggests a role for Saw Palmetto (Beta-Sitosterol) as a product that blocks the conversion of testosterone to Dihydrotestosterone (DHT). If this were true, the PSA blood test would be altered (cut in half) by using Saw Palmetto. This does not occur, as independent studies performed by Marks & Gerber showed no effect of Saw Palmetto on PSA, at six and twelve months, respectively. If men are interested in shrinking the prostate size, I would refer them to an FDA approved product called Avodart® (Dutasteride). This product blocks the enzyme 5-Alpha Reductase, causing the prostate to shrink in size by 20-30%. Men are encouraged to ask their doctors about this option and should remember to multiply the PSA result by two, to provide an accurate number. Saw palmetto may mask prostate disease and is ineffective in reducing the size of the prostate or PSA, and therefore, does not act clinically as a 5-Alpha Reductase Inhibitor (5-ARI). WHY PEENUTS® QUALIFIES TO BE YOUR PROSTATE NUTRITIONAL FORMULA Peenuts® is a unique formula with a unique name. While the name suggests many things to many people, it is an acronym that stands for “Power to Empty Every Time while Never Urinating Too Soon.” It is also a name you will not likely forget. In effect, the name stands for normal bladder function and expected prostate health. Arguably, this formula is the most studied natural formula in the world. In a randomized, double blind, placebo controlled study performed in 1997, Peenuts® demonstrated improved ability to decrease the signs and symptoms associated with an enlarged prostate or prostatitis. The findings were statistically significant. More importantly, the findings were clinically significant; meaning…the patient was able to recognize the improvement. While all men in the study on Peenuts® improved their voiding symptoms, 69% of men improved either 6 or 7 out of 7 categories measured (Please refer to an IPSS-Index or AUA Symptom Index). In a follow-up to the study, more than 300 men have been evaluated with similar results in the clinic setting. The average improvement in the urinary symptom score was 11 points. The PSA, “the barometer of prostate health,” improved in all patients by an average of 49%, while the EPS, our most sensitive marker for prostatitis, noted a 66% reduction in white blood cells (consistent with a reduction in inflammation). There were no side effects or drug interactions noted during testing or clinical follow up. The Peenuts® patented formula consists of: Vitamin C, Vitamin E, Vitamin B6, Selenium, Zinc, Echinacea, Glycine, Alanine, Glutamic Acid, Saw Palmetto, Pygeum, Pumpkin Seed, Nettle, Garlic and Ginkgo Biloba. Peenuts®, a complex, synergistic blend of natural ingredients, (comprised of antioxidants, antiinflammatories, beta-sitosterols, and immune boosters), is patented to reduce the PSA (associated with inflammation), reduce urinary symptoms and reduce the white blood cell count in the EPS. The mechanism for PSA reduction is based on the formula’s effectiveness versus prostatitis as a cellular oxidative event while validated by a proven reduction in EPS as the diagnostic measure of inflammation. Men should exercise caution when comparing Saw Palmetto and Beta-Sitosterol related products (formulas) that speak to the intention to assist a healthy prostate and a prostatitis formula. Notwithstanding an apparent benefit from Beta-Sitosterol (the active ingredient in Saw Palmetto) on urinary symptoms (real or placebo effect), all prostate formulas are not created equal. In the process of application for European Patent recognition, I was asked by the European Patent Judges to compare the Peenuts® formula to a patented BPH formula. The intent of the study was to judge the benefit of both products regarding prostate inflammation (as judged by white blood cells in the EPS). To state further, the Patent Judges needed to see a difference in clinical outcome unique to the Peenuts® formula that was not seen with the previously patented BPH formula. After four months, of an open label study, a comparison of the EPS noted a 68.2% reduction in white blood cells with the Peenuts® formula while the BPH formula had no effect on the inflammation marker. While this study does not negate the benefit of the BPH formula to prostate health, it is doubtful; there is a benefit versus prostatitis. To reiterate, the only way to accurately assess inflammation of the prostate and the clinical benefit of the nutritional formula you currently use is to evaluate the Expressed Prostatic Secretion (EPS). Failure to do so creates more confusion while questioning the goal of your nutritional supplementation program. Take Home Message: Ten or greater white blood cells in the prostate secretion, obtained at the time of prostate digital examination and massage, evaluated microscopically under 400 power, establishes the diagnosis of prostatitis. In the event a vigorous prostate massage fails to yield an adequate specimen at the tip of the urethra, doctors are encouraged to use the patented dipstick technology on a post-massage urine specimen, to validate the disease process of prostatitis. While this methodology is not as accurate as the EPS, it will serve as an effective diagnostic indicator in the more severe cases of prostatitis. Take Home Message: PEENUTS® is an effective, natural compound guaranteed to lower the PSA in the absence of Prostate Cancer, based on validated studies and a patent. Beyond Saw Palmetto, other sources of sterols (primarily Beta-Sitosterols) include Pygeum Africanum (bark of the African Plum tree), pumpkin seed, sugar cane and nettle. None of these sterolic compounds have been validated to benefit men with prostatitis, as qualified by a numerical reduction in the white blood cell count, associated with the EPS. On the other hand, improvement in urinating symptoms has been reported. Nutritionally, zinc may play a role in the evolution of prostate cancer as most studies show prostate tissue levels of this mineral to be low or absent in prostatitis and prostate cancer. The exact relationship has yet to be scientifically elucidated. Despite the historical data on the potential benefit of these ingredients, the majority of American doctors have shown a decided reluctance to embrace natural remedies for prostate health, without meaningful clinical trials with compelling data. The research of the late William Fair, M.D., Memorial Sloan-Kettering, Katz, Moyad, Lowe, Klotz, and others in the supplement arena continues to set the standard and challenge the industry to provide evidence-based facts. Despite the fact that the FDA has little control over natural products, no one benefits when false claims are made. It is for this reason that all nutritional products or formulas should welcome the constructive criticism of others, but on the other hand, medical journals and the media have an obligation to report on true breakthroughs of academic and clinical thought. In regard to Prostate Cancer, Selenium supplementation, at 200 mcg daily, has been shown to decrease the incidence of Prostate Cancer by 66%, in a 10-year study. Likewise, Vitamin E, at 50 mg daily, was shown to decrease the incidence of Prostate Cancer by 32% (Alpha-Tocopherol/Beta-Carotene Study). It is interesting to note that the Vitamin E findings were demonstrated in a group of smokers. Notwithstanding the data, it is unknown what effect smoking has on the development of Prostate Cancer, independent of Vitamin E. The National Cancer Institute (NCI) intends to answer the questions related to the benefit of Selenium and Vitamin E in the evolution of Prostate Cancer, in a large scale 12-year study (start date in 2002). Dubbed, the SELECT Trial, patients will be randomized to Selenium 200 mcg, Vitamin E 400 mg, Selenium E, and Vitamin E in combination, and placebo taken on a daily basis. Based on recent research, there is some concern for toxicity of Vitamin E in excess of 400 mg daily. How this will affect the outcome of the NCI study, as it is moving forward, is unknown, but individuals should be aware that 400 mg may be toxic to the heart in supplement form. Beyond the potential toxicity of Vitamin E, there is also concern for toxicity of other vitamins and minerals, including, but not limited to, Zinc, Calcium, Vitamin A, Vitamin D, Vitamin C and Vitamin B6. When the dust settles on all the issues of toxicity, the most prevalent thought involves taking nutrients in appropriate doses, but more importantly, in moderation. Regardless of what anyone says, more is not better, when it comes to nutritional supplementation. FINAL THOUGHTS: To declare your prostate healthy, your PSA must be less than 1.0 ng/ml with a complete absence of urinary symptoms; To Check your PSA in the comfort of your home, call today for your PSA “Diagnostic Home Kit” – Toll Free: 1-866-PSA-CHEK (7722435). A PSA of ≥ 1 likely indicates an unhealthy prostate. It’s obvious that the lower the PSA, the lower the risk of prostate cancer. Anything you can do to lower your PSA level will likely reduce your risk of eventually getting prostate cancer. Keep track of your PSA level for your own records. The risk is too high if you do not! If your PSA is between 1.0 – 4.0 ng/ml, there is a 20-30% chance prostate cancer exists. Likewise, if your PSA is between 4.1-10.0 ng/ml, there is a 20-30% chance that prostate cancer is present. Given this data, the healthiest number for your PSA is less than one; remembering that prostate cancer has been reported with a PSA of less than one, as well, but the odds of not having cancer with such a low number are in your favor. Have your PSA and rectal examination performed regularly, usually at least every year for men 30-35 or older. Men at greater than average risk for prostate cancer, such as Blacks and men with a positive family history of prostate cancer should be checked yearly starting at age 30. Men with known elevations in their PSA levels and those with inconclusive or “suspicious” previous biopsies may need to be checked more often. (Figure 5) Don’t be afraid to ask questions of your physician or get a second opinion about your health. A true professional will take the time to answer your questions and be open to suggestions about alternative therapies (after all, chances are the traditional therapies have not worked at this point, if you are reading this article). Research from the American Association of Cancer Research (AACR) and others indicate the link between prostatitis and prostate cancer is real! Practically all men with prostatitis will eventually get prostate cancer (if we live long enough) as the diseases are commonly found together. Remember, understanding prostatitis is your best first step to helping yourself. Learn all you can about prostatitis and treat it as aggressively and effectively as possible. Peenuts® may be your best first opportunity to establish and/or maintain prostate health and may delay or even prevent the development of prostate cancer. Validation will be identified by any combination of biologic disease marker improvement, as determined by a decrease in PSA, a decrease in EPS and/or a decrease in Urinary Symptoms. Be aware that your physician may not be an expert on the treatment of prostatitis. Ask him about the vari- ous diagnostic tests and therapies available and which ones are appropriate for you. For more information on Peenuts® and other nutritional products for the prostate, call Preferred Health Resources at 1-888-733-6887 or log onto the Peenuts® website at www.Peenuts.com Also, check out the National Institutes of Health (NIH) Website (www.nih.gov) for more general information on prostatitis and prostate cancer research. Men Who Should Consider Peenuts® Prostate Nutrition • All Men with a Family History of Prostate Cancer, Regardless of Age, Have a 10% Increased Risk for Prostate Cancer • Men with Known Prostatitis Regardless of Age; Prostatitis is Associated with All Cases of Prostate Cancer • Men with Voiding Symptoms – Voiding Symptoms represent Prostatitis until Proven Otherwise. In a study of 235 Consecutive Men, with Voiding Symptoms, More than 80% had Prostatitis, Regardless of Age. This is a Landmark Finding Not Seen Before in the Literature. • All Men with PSA Elevation ≥ 1 ng/ml; The Normal Range for PSA of 0-4 ng/ml is Incorrect; 0-4 ng/ml Cannot Be Normal when 30% of All Prostate Cancers are in This Range, A True Medical Oxymoron! • All Men Who Have Undergone Prostate Biopsy Noting Negative Evidence of Prostate Cancer and a PSA ≥ 1 ng/ml • All Men Younger than 30 who are Admittedly Proactive; One Capsule a Day May be Appropriate if Negative Symptoms and a PSA of < 1 ng/ml is Identified in Association with a Normal EPS • All Men Who Have Failed to Be Cured by Traditional Antibiotic Therapy Who Note Continued Voiding Symptoms and/or a Rising PSA • Men Who are Presently Taking Proscar (Finasteride) and are Not Comfortable with a Chemical that Works Minimally Versus Urinary Symptoms (PLESS Study), yet Costs Significantly • Men Who Take Alpha-Blockers such as Hytrin, Cardura, and Flomax; These Products Have Side Effects and Do Nothing to Improve the Health of the Prostate (Figure 5) EDITORIAL COMMENT By Stephen W. Leslie, MD FACS (Urologist) The widespread incidence of prostatitis is well known to urologists and other doctors, but its association with prostate cancer has previously been considered incidental. In this article, Dr. Wheeler has suggested that prostatitis may actually cause prostate cancer based on evidence supportive of inflammation leading to cancer consistent with a number of other organ cancers, the research of the American Association of Cancer Research, David Bostwick and others. While the association alone between these two conditions falls short of being considered definitive, it is certainly plausible and deserves more study. Even a limited causative link between prostatitis and prostate cancer would cause a dramatic change in our attitude and approach to prostatitis. Currently, prostatitis therapy consists primarily of antibiotics, alpha blockers and other drugs. The article correctly points out that these remedies are often inadequate. Dr. Wheeler recommends considering nutritional agents in the absence of successful definitive therapy. Although nutritional therapy has been widely used and studied in Europe, it is not routinely recommended by many U.S. physicians for a number of reasons. Nutritional therapy is not taught in most U.S. medical schools and many American physicians are unfamiliar with the available scientific research on the subject. Published studies on nutritional therapy are criticized for using different preparations and dosages, having too small a sample size with limited numbers of participants, being of inadequate duration, and bias in the selection of patients to be tested. Commercially available nutritional therapies are usually not manufactured to a pharmaceutical grade standard, which means each bottle, even from the same company, may have different biological effects. There is no universally accepted dosing schedule for many of these natural remedies and their mechanism of action is often unknown. Further, no specific combination nutritional product for either prostatitis or symptoms of prostate enlargement has ever been properly tested in a well designed, scientific study. Dr. Wheeler describes a study he performed at The Prostatitis & Prostate Cancer Center on a unique combination nutritional therapy called Peenuts®. He reports outstanding objective and clinical results, but the scientific details of his research need to be care- fully reviewed and his finding duplicated by other medical experts. If further research indicates he has indeed found a safe and highly effective therapy for the signs and symptoms of prostatitis and prostate enlargement, this would be a major contribution to the health and well-being of American men while saving the health care system tens of millions of dollars. Further elaboration of the prostatitis to prostate cancer model would qualify as a major medical breakthrough. Minimally, Dr. Wheeler’s research offers a patented formula with little downside with a potentially tremendous upside for motivated men. Benefits of Taking Peenuts® (The Premier Prostate Nutritional Formula) A Nutritional Guide at a Glance • Antioxidants – Benefit in Fighting Free Radicals and are Synergistic to the Formula • Immune Boosters – A Unique Combination is Vital to Allowing the Body to Heal Itself • Vitamin E and Selenium are Synergistic AntiOxidants and Boost the T Cells • Vitamin E – 32% Fewer Prostate Cancers noted in the Finnish Study (ATBC Study), using 50 mg daily • Echinacea – A Mild Immune System Stimulant is Synergistic to the Formula • Zinc – An Immune Booster that is Low to Absent in Men with Prostatitis and Prostate Cancer • Selenium: 66% Fewer Prostate Cancers Versus Placebo (L Clark, PhD) • Natural Antibiotic – Garlic Works to Improve the Host Response to Inflammation, Working in Synergy with All Other Ingredients • Anti-BPH Ingredients – Saw Palmetto, Pygeum, Stinging Nettle (also a Source of Vitamin E) and Pumpkin Seed (also a Source of Zinc) are All Synergistic • Ginkgo Biloba – Nature’s Vascular Stimulant • Amino Acids – Glutamic Acid, Glycine, LAlanine Represent the Chinese Remedy to Prostate Health • B6 – Assists the Metabolism of other Ingredients IPSS – INDEX AUA (BPH) SYMPTOM SCORE Patient:_______________________ Not At All Less than 1 time in 5 Less than half the time About half the time More than half the time 0 1 2 3 4 5 0 1 2 3 4 5 0 1 2 3 4 5 0 1 2 3 4 5 0 1 2 3 4 5 0 1 2 3 4 5 None 1 time 2 times 3 times 4 times 5 or more times 3 4 5 Date:________________________ INCOMPLETE EMPTYING 1. Over the past month, how often have you had a sensation of not emptying your bladder completely after you finished urinating? FREQUENCY 2. Over the past month, how often have you had to urinate again less than 2 hours after you finished urinating? INTERMITTENCY 3. Over the past month, how often have you found you stopped and started again several times when you urinated? URGE TO URINATE 4. Over the past month, how often have you found it difficult to postpone the urination? WEAK STREAM 5. Over the past month, how often have you had a weak urinary stream? STRAINING 6. Over the past month, how often have you had to push or strain to begin urination? URINATING AT NIGHT 0 1 2 7. Over the past month, how many times did you most typically get up to urinate from the time you went to bed at night until the time you got up in the morning? SYMPTOM SCORE: 1-7 Mild, 8-19 Moderate, 20-35 Severe Almost always TOTAL:__________ BOTHER SCORE DUE TO URINARY SYMPTOMS QUALITY OF LIFE DUE TO URINARY SYMPTOMS How would you feel if you had to live with your urinary condition, the way it is now, for the rest of your life? Delighted Pleased 0 1 Mostly Mixed Mostly satisfied dissatisfied 2 3 4 Unhappy Terrible 5 6 Acknowledgments of Contributions August 1, 2005 Through October 31, 2005 (YOUR NAME WILL APPEAR BELOW IF WE RECEIVED YOUR DONATION BETWEEN THE ABOVE DATES) Memorial Contributions In Loving Memory of Lloyd J. Ney, Sr. Founder of PAACT, INC., Grand Rapids, MI Conway Taylor D. Curtis Shaneour, Jr. William Prokous In Loving Memory of Andrew Yurksaitis Donald & Karen Zastawny Robert & Nancy Cichon John & Mary Lou Albanese L.C. Tuttle In Loving Memory of John Farrell Mr. & Mrs. Raymond Bourgoin Joe & Fran Lombardo In Loving Memory of Harry Barton Ewers Dorothy Trenor Ann & Jim Farr In Loving Memory of Joan Vincunas John & Jean Reardon In Loving Memory of Joe Migliaccio Antonio & Sofia Barucco In Loving Memory of Dr. Ray E. Worley Billie A Worley In Loving Memory of Thomas Smoyer Robert Grocott In Loving Memory of Dominic Gallo Rodney & Marjorie di Girolamo In Loving Memory of Kenneth O’Brian Bobbie Stelzer In Loving Memory of Miriam Reese Charlene Sirowitz & Family In Loving Memory of Gunilla V Pintar Harold R Pintar ****************************************************************** Contributions ($1,000 and Above) Anonymous Endocare Estate of Rochelle Pinz Estate of U Sidney Bateman Hoogland, C.R. Contributions ($500 to $999) Barton, John Jones, Russell Preston, Fred Patron Membership ($100 to $499) Anonymous Barry, Thomas Belter, Walter Breslin, John Brown, James E Carl, Samuel Clauser, Ray Coffin, Jerry Cook, Jesse Cuthbert, Kingsley Devries, Mark Edwards, Alan Franz, Marvin Fulmer, Robert Greenberg, Stanley Hagan, Donald Hinckley, Stanley Howe, Richard Irish, A.W. (Bud) Jezek, Ray Joe, Paul Litster, Gordy Lynch, Terence McLaughlin, William Mediplan RX Mirmelstein, Cyril Mulvey, John Niebuhr, Herman Palmer, Joseph Payne, Don Peplau, Harold Peterson, Palmer Popoff, William Ross, Phillip Sanken, Heinz Shimer, Alan Sinder, Ned Snyder, William Stern, Robert Stevens, Len Trueblood, Harry Wahtera, Edward Paact Membership ($50 to $99) Aaronson, David Alderson, Leland Altiere, Elmer Anonymous Aye, Charles Babcock, C.I. Barboo, Samuel Beltrani, John Benn, Donald Berles, Bob Blake, Charles Bonanno, Charles Borys, Richard Boyd, Kenneth Brorein, William Buhaly, Joseph Burroughs, John Butler, Bernard Butters, Robert Campbell, John Cantwell, Alan Chmelka, Marvin Clark, Willard Compton, Joseph Cree, James Cremin, James Crumbine, Peter Derdoy, Jorge Dittmar, Mary Jane Donahue, William Dunsworth, E.E. Edwards, Joseph English, Ross Fialkov, Herman Finnerty, Robert Fleming, Steven Forbes, Charles Genter, John Gerakas, Evans Gibson, Gordon Gordon, George Gouin, Leon Gray, Wayne Grey, Schuyler Grosh, R.L. Hannum, Terry Haynes, Leonard Hazlehurst, Charles Hendrickson, William Holmes, Oliver Hoose, Harry Hossfeld, James Iogha, Donald Irish, Richard Irish, Thomas Irish, William Keeley, Gilbert Kelly, Ronald Kessler, Robert Kieft, Garry Kirk, Cameron Kottich, Charles Kress, Patricia Lacewell, Kenneth Landau, Jacques Leachman, Charles Lee County Lenhardt, Otto Lipschutz, Howard Marinkovic, Zoran Masser, Paul Massey, Joseph McAlister, Frank McCarthy, Dennis McGaan, Dean McGann, Thomas McInerney, Eugene Meetze, Bill Merrill, Gene Mikaeloff, Robert Milton, Edward Misali, Akila J Ike Naughton, Thomas Neumann, Tibor Nibecker, A.F. Nordmo, Rowland Olson, Richard Paradiso, Guy PC Support Group of Pederson, David Poletti, R.L. Popham, J.K. Reed, Alexander Reed, William Rich, Howard Richardson, Richard Ritz, Robert Roche, Bartly Rohn, Dennis Rohrer, Dan Rolka, Arthur Schaffer, Hal Scoville, James Sheldon, Lewis Soifer, Paul Spangrude, George Stella, Angelo Stocker, John Stokes, Joseph Tackaberry, George Templeman, John Thompson, David Travis, John Tremba, Edward Turek, John Unitis, Joseph Vardaro, Christina Verderese, Frank Waller, John Wernick, Paul Wilson, Doug Wilson, William Miscellaneous Contributions (less than $50) Allen, Charles Amendt, Kenneth Anonymous Archibald, Lloyd Banks, James Baylis, John Bothwell, Bruce Brown, Mackintosh Busch, Edward Cali, Vincent Camplin, W Erle Dreier, John Harden, Wayne Harding, Charles Harkness, Robert Hastings, Jack Holt, Melvin Hornbeck, Robert Hummel, Richard Jackewicz, William Jefferson, Gene Kath, Vern Kras, Eugene Kroening, Theodore Lada, Stephen Lamey, Ron Maroney, John Matulonis, Robert Meyers, Bernard Mezhinsky, Victor Morrow, John Oddon, Louis Parsons, Robert Patierno, Frank Pinkard, Dennis Plotkin, Nathan Pollick, Albert Potter, Gerald Rabinowitz, Herman Rasoletti, Wayne Saint, Don Sandberg, Carl Schlidt, Rudolf Scott, Thomas Sedlacek, E.J. Singer, Lloyd Standal, Norman Taub, Elston Tsantles, Penny Von Oppen, Dieter Waldenfels, James Warren, Carl Wicklund, Rodney Widmayer, William Yorko, Edward Cans For Cancer Postal Employees Contributions by State & Province Alabama……… Arizona.......……. California.……. Colorado....….…. Connecticut….…. Florida....…..... Georgia…..….…. Illinois........……. Indiana.......……. Iowa……………. Louisiana………. Maryland...….…. Massachusetts.… Maine…………. Michigan...…… Minnesota..….… Montana………... Nevada…………. New Hampshire.. New Jersey...…... New York....….. N. Carolina….…. Ohio...........……. Oregon........….... Pennsylvania.….. Rhode Island…… S. Carolina..……. Tennessee…….. Texas..........……. Utah……………. Virginia...…..….. Washington……. Wisconsin……… Argentina………. Australia……….. Canada…..…….. France……..…… Pohnpei………… 3 4 37 10 3 30 5 12 2 1 1 2 4 2 23 4 1 3 1 8 15 6 5 4 9 2 1 1 5 2 7 6 2 1 1 5 1 1 FINANCIAL SUMMARY REPORT (January 1, 2005 through September 30, 2005) GENERAL FUND 1,451,350.83 Balance on Hand December 31, 2004 REVENUES RECEIVED Membership Contributions Memorial Income Legacies & Bequests Investment Income Total Revenues 57,927.44 8,473.00 42,818.00 43,241.51 152,459.95 Total Balance on Hand and Revenues EXPENDITURESEmployee Wages Payroll Taxes Medical Insurance Outside Services, Labor Rent Meals, Motel, and Transportation Auto Expense Printing Postage and Delivery Telephone Service Fees Maintenance & Repairs Office and Computer Supplies Miscellaneous Total Expenditures 1,603,810.78 Balance on Hand September 30, 2005 1,468,820.25 Assets: Checking Account Petty Cash Saving Account Certificates of Deposit, Stocks, and Bonds Money Market Funds Equipment 39,131.27 50.00 29.63 1,688,671.30 164,500.61 27,028.55 1,919,411.36 Net Assets: Foundation Fund Balance 56,686.14 6,190.49 18,170.50 2,926.14 9,000.00 2,024.88 1,325.09 17,797.94 16,041.99 1,951.64 1,106.28 135.00 1,246.98 387.46 134,990.53 328,151.40 PATIENT ADVOCATES FOR ADVANCED CANCER TREATMENTS, INC. 1143 Parmelee NW Grand Rapids, MI 49504 P.O. Box 141695 Grand Rapids, MI 49514 Phone: (616) 453-1477 Fax: (616) 453-1846 PROSTATE CANCER COMMUNICATION ADDRESS SERVICE REQUESTED NONPROFIT ORG U.S. POSTAGE PAID GRAND RAPIDS, MI PERMIT NO. 875 PAACT Membership Form Name: Address: City: Telephone HM: Birthdate: St/Province: WK: / / Postal Code: Fax: E-Mail: Other: Annual Membership Classification _____Patient………………….…………...$50 _____Donor………….………………………$500 _____Advocate…………..……………..…$50 _____Sponsor……………..………………..$1000 _____Professional………….…………....$100 _____Corporate…….……...………………$1000 _______Other………..………………………………………………….………...$________ _______Include me as a PAACT member, though I currently cannot contribute Tribute gifts support the daily operations of PAACT, Inc., by furnishing PC patients, doctors and advocates with the latest information available on the methods of detection, diagnostic procedures, evaluation and treatments for prostate cancer. We also participate in matching gift programs and United Way. For more information contact us at( 616) 453-1477. □ Check Enclosed □ Charge to my credit card (below): □ MC □ VISA □ Discover □ American Express Enclosed is $ ________________________________________________, a gift to the Lloyd J. Ney, Sr. Memorial Fund. Enclosed is $ ________________________________________________, for PAACT’s general operation expenses. Enclosed is $ ________________________________________________, I wish to remain anonymous. In Memory of ___________________________________________________________________________________________ Please send acknowledgement card to: Name __________________________________________________________________________________________________ Address_________________________________________________________________________________________________ City_________________________________________________State____________________Zip________________________ Account Number: ________________________________________________ Amount $ _______________________________ Signature: ______________________________________________________Expiration Date: ___________________________
© Copyright 2026 Paperzz