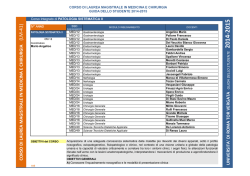
Cop 2014_Layout 1 04/04/14 10:12 Pagina 1 w ess N o cc a. i t A u en w.ai p O w w ISSN 1124-3562 Poste Italiane S.p.A. - Spedizione in abbonamento postale - D.L. 353/2003 (conv. in L. 27/02/2004 n. 46) Art. 1, comma 1 DCB Milano Archivio Italiano di Urologia e Andrologia / Archives of Italian Urology and Andrology - Vol. 86; n. 1, March 2014 Vol. 86; n. 1, March 2014 ANDROLOGICAL SCIENCES Antioxidant cosupplementation therapy with vitamin C, vitamin E, and coenzyme Q10 in patients with oligoasthenozoospermia Yoshitomo Kobori, Shigeyuki Ota, Ryo Sato, et al. Is there any effect of insulin resistance on male reproductive system? Ayhan Verit, Fatma Ferda Verit, Halil Oncel, Halil Ciftci Evaluation of penile cavernosal artery intima-media thickness in patients with erectile dysfunction. A new parameter in the diagnosis of vascular erectile dysfunction. Our experience on 59 cases Domenico Prezioso, Fabrizio Iacono, Umberto Russo, et al. Urinary and sexual functions after surgical treatment of penile fracture concomitant with complete urethral disruption Ali Abdel Raheem, Hassan El-Tatawy, Ahmed Eissa, et al. Testicular microlithiasis and dyspermia: Is there any correlation? Francesco Catanzariti, Ubaldo Cantoro, Vito Lacetera, et al. Treatment of urethral strictures in balanitis xerotica obliterans (BXO) using circular buccal mucosal meatoplasy: Experience of 15 cases Abdulmuttalip Simsek, Sinasi Yavuz Onol, Omer Kurt Present and future association between obesity and hypogonadism in Italian male Valentina Boddi, Valeria Barbaro, Paul Mc Nieven, et al. In vitro effects of PDE5 inhibitor and statin treatment on the contractile responses off experimental MetS rabbit's cavernous smooth muscle Yasin Erden, Esat Korgalı, Gokce Dundar, et al. Penile fracture: Penoscrotal approach with degloving of penis after Magnetic Resonance Imaging (MRI) Gabriele Antonini, Patrizio Vicini, Salvatore Sansalone, et al. First case of bilateral, synchronous anaplastic variant of spermatocytic seminoma treated with radical orchifunicolectomy as single approach: Case report and review of the literature Giorgio Gentile, Francesca Giunchi, Riccardo Schiavina, et al. Penile strangulation: An unusual sexual practice that often presents an urological emergency Lucio Dell’Atti Rare case of intra-testicular adenomatoid tumour Filippo Migliorini, Roberto Baldassarre, Walter Artibani, et al. Use of inflatable penile prostheses AMS CX with momentary squeeze in a patient with Peyronie’s disease after removal of two previously implanted penile prostheses Patrizio Vicini, Ferdinando De Marco, Gabriele Antonini, et al. Surgical repair of the iatrogenic falsepassage in the treatment of trauma-induced posterior urethral injuries Faruk Dog˘an, Ali Feyzullah S¸ahin, Tevfik Sarıkaya, Alper Dırık The impact of non-urologic drugs on sexual function in men Ferdinando Fusco, Marco Franco, Nicola Longo, et al. Practical recommendations for performing ultrasound scanning in the urological and andrological fields Pasquale Martino, Andrea Benedetto Galosi, Marco Bitelli, et al. Sahin CR_Stesura Seveso 26/03/14 10:47 Pagina 48 DOI: 10.4081/aiua.2014.1.48 CASE REPORT Surgical repair of the iatrogenic falsepassage in the treatment of trauma-induced posterior urethral injuries Faruk Dog˘an 1, Ali Feyzullah S¸ahin 1, Tevfik Sarıkaya 2, Alper Dırık 1 1 Department 2 Department of Urology, S¸ifa University Medicine School, I˙zmir, Turkey of Urology, Sivas Public Hospital, Sivas, Turkey Pelvic fracture associated urethral injury (PFAUI) is a rare and challenging sequel of blunt pelvic trauma. Treatment of iatrogenic false urethral passage (FUP) remains as a challenge for urologists. In this case report we reviewed the iatrogenic FUP caused by wrong procedures performed in the treatment of a patient with PFAUI and the treatment of posterior urethral stricture with transperineal bulbo-prostatic anatomic urethroplasty in the management of FUP. A 37-year-old male patient with PFAUI had undergone a laparotomy procedure for pelvic bone fracture, complete urethral rupture, and bladder perforation 8 years ago. After stricture formation, patient had undergone procedures that caused FUP. Following operations, he had a low urinary flow rate, and incontinence and urgency even with small amounts of urine. FUP was diagnosed by voiding cystourethrography and retrograde urethrography. FUP was fixed with open urethroplasty with the guidance of flexible antegrade urethtoscopy. False passage should always be taken into account in the differential diagnosis of patients with persistent symptoms that underwent PFAUI therapy. In addition, we believe that in the evaluation of patients with PFAUI suspected for having a false passage, bladder neck and urethra should be assessed by combining routine voiding cystourethrography and retrograde urethrography with preoperative flexible cystoscopy via suprapubic route. trauma may cause a life-long morbidity unless properly treated. While treatment approach in partial urethral rupture includes watchful waiting after performing a simple cystostomy, complete urethral rupture can be repaired with 3 methods: 1) Realignment of the separated urethral ends over a catheter (urethral realignment), 2) Primary anastomosis of separated urethral ends, and 3) Immediate suprapubic cystostomy and delayed repair of the resulting stricture on an elective basis (3). Emergency treatment of PFAUI has not been standardized in developing countries. On majority of cases wrong procedures cause iatrogenic injuries in addition to trauma itself (4). Sometimes, careless and/or repeated urethral dilatations also lead to false urethral passage (FUP) formation, which results in infections and incontinence. Treatment of iatrogenic FUP remains as a challenge for urologists (5). Furthermore, there is a paucity of data about the urethroplasty procedure performed for urethral stricture formed by FUP. In this case report we reviewed the iatrogenic FUP caused by wrong procedures performed in the treatment of a patient with PFAUI and the treatment of posterior urethral stricture with transperinealbulbo-prostatic anatomic urethroplasty in the management of FUP. Case Report and Figures are posted in Suppementary materials on www.aiua.it. KEY WORDS: False urethral passage; flexible cystoscoby; pelvic fracture; urethral injury. False passage is an abnormal passage between urinary bladder and urethra, which is observed in association with posterior urethral stricture and is caused by a iatrogenic injury resulting from careless and wrong treatment procedures after trauma. If unnoticed, this false passage between urethra and bladder causes very frequent complaints; furthermore, repeated endoscopic procedures (internal urethrotomy), catheterization, or urethral dilatation become necessary. Following dilatation, hesitancy, incontinence, and urgency persist. Furthermore, false passage scar tissue around traumatized tissue causes prolonged and chronic infections and hence leads to stricture formation (6). Summary Submitted 30 July 2013; Accepted 31 December 2013 INTRODUCTION Pelvic fracture associated urethral injury (PFAUI) is a rare and challenging sequel of blunt pelvic trauma. In 425% of male patients with pelvic bone fractures, simultaneous posterior urethral injury is observed (1). Injury to posterior urethra may be a simple contusion, or it may appear as partial or complete rupture (2). Urethral No conflict of interest declared 48 Archivio Italiano di Urologia e Andrologia 2014; 86, 1 DISCUSSION Sahin CR_Stesura Seveso 26/03/14 10:47 Pagina 49 Surgical repair of the iatrogenic falsepassage in the treatment of trauma-induced posterior urethral injuries Methods used for diagnosis of posterior urethral strictures before reconstruction should clearly delineate stricture length and site, determine the anatomy of posterior urethra and bladder neck, and show false passages and fistulas if any. Conventional methods include simultaneous CCUG and dynamic retrograde urethrography. It is necessary to make a pre-treatment assessment via combined radiological and endoscopic methods especially in obliterated cases where prostatic and proximal urethra cannot be visualized. False passage is diagnosed with urethrography. Combined voiding cystourethrography and retrograde urethrography can clearly show the site and path of the passage (7). Cystourethroscopy plays a limited role in diagnosis since normal anatomical structures cannot be localized. This was also the case in our patient because his false passage could not be identified despite multiple endoscopic procedures at other medical facilities. A false passage should be taken into consideration for diagnosis in case normal anatomical markers like veru montanum, bladder trigone, and external sphincter could not be seen during cystourethroscopy. A flexible cystoscope advanced through a suprapubic route is highly useful for the diagnosis of false passage. While normal bladder neck is a funnel-shaped, soft, elastic, and of smooth structure, a false passage is a pale mucosal formation associated with a vertical circular dense scar and a coarse granulation that is located close to bladder neck (6). In conclusion, recurrent urethral strictures develop due to inappropriate and insufficient initial therapies in patients with PFAUI with complete urethral separation; Figure. Preoperative VCUG and RUG shows the location of a false passage and urethral stricture. The black arrow shows normal bladder neck and prostatic urethra, the blue arrow shows the urethral stricture and the beginning of the intraprostatic false passage, while the white arrow shows the false passage located close to bladder neck. as a result, various endoscopic procedures and urethral dilatations become necessary. Even after these therapies, hesitancy, incontinence, and urgency are observed. False passage should always be taken into account in the differential diagnosis of patients with persistent symptoms that underwent PFAUI therapy. In addition, we believe that in the evaluation of patients with PFAUI suspected for having a false passage, bladder neck and urethra should be assessed by combining routine voiding cystourethrography and retrograde urethrography with preoperative flexible cystoscopy via suprapubic route. The guidance of a flexible cystoscope via suprapubic route during the operation is quite helpful. It also guides procedures of curettage and dissection to determine the true anatomical structures and to identify the normal urethral tract, particularly in cases where prostatic urethra is blocked. REFERENCES 1. Koraitim MM, Marzouk ME, Atta MA, et al. Risk of urethral injury in pelvic fractures. Br J Urol. 1996; 77: 876-80. 2. Lupu AN, Forrer JH, Smith RB, Kaufman J. Urethral gap in complete disruption of membraneus urethra. Urology. 1987; 29:378-82. 3. Webstre GD, Mathes GL, Selli C. Prostatomembranous urethral injuries: A review of the literature and a rational approach to their management. I. Urol. 1983; 130:898. 4. Barbagli G. History and evolution of transpubic urethroplasty: a lesson for young urologists in training. Eur Urol. 2007; 52:1290-2. 5. Barbagli G, Palminteri E, Lazzeri M, Guazzoni G. One-stage circumferential buccal mucosa graft urethroplasty for bulbous stricture repair. Urology. 2003; 61:452-5. 6. Qiang Fu, Jiong Zhang, Ying-long Sa, San-bao Jin, Yue-minXu. Transperineal bulbo-prostatic anastomosis for posterior urethral stricture associated with false passage: a single-centre experience. BJU Int. 2011; 108:1352-4. 7. Secrest CL. Staged urethroplasty: indications and techniques. Urol Clin North Am. 2002; 29:467-75. Correspondence Faruk Dog˘an, MD (Corresponding Author) [email protected] Alper Dırık, MD [email protected] Specialist in Urology Department of Urology, S¸ifa University Medicine School, Izmir, Turkey Ali Feyzullah S¸ahin, MD, FEBU [email protected] Asistant Professor in Urology Department of Urology, S¸ifa University Medicine School Sanayi cad. No:7 Bornova, Izmir, Turkey Tevfik Sarıkaya, MD [email protected] Specialist in Urology Department of Urology, Sivas Public Hospital, Sivas, Turkey Archivio Italiano di Urologia e Andrologia 2014; 86, 1 49 Cop 2014_Layout 1 04/04/14 10:12 Pagina 2 9° Congresso Nazionale 2014 22-24 Maggio 2014 Auditorium Pietro d'Abano - Abano Terme (PD) Segreteria Organizzativa MEC Congress Srl Via Gorizia 51 - 95129 Catania Dr.ssa Antonella Barbagallo tel. 334 6527204 - email: [email protected] Società Italiana Chi intende iscriversi alla SIUrO trova le istruzioni ed i moduli necessari sul sito internet www.siuro.it È possibile pagare la quota associativa annuale on-line: con carta di credito collegandosi direttamente al sito www.siuro.it o tramite bonifico bancario intestato alla Società Italiana di Urologia Oncologica, presso Banca Popolare di Milano IBAN: IT08W0558402402000000000539, avendo cura di specificare il nome del socio pagante Per ottenere ulteriori informazioni è possibile contattare la segreteria Via Dante 17 - 40126 Bologna Tel +39 051 349224 Fax +39 051 349224 e-mail: [email protected] www.siuro.it CHI PUÒ FARNE PARTE Possono far parte dell'Associazione con la qualifica di Socio Ordinario gli Urologi Specialisti in Urologia e gli specializOspedalità Gestione Privata zandi in Urologia operanti in strutture assistenziali urologiche dell’Ospedalità a gestione Privata; con la qualifica di Socio Corrispondente gli studiosi italiani o stranieri che abbiano dimostrato un particolare interesse per l'Urologia. ISCRIZIONE Iscriversi è semplice, basta scaricare la scheda di adesione presente sul sito www.urop.it, compilarla in tutte le sue parti prendendo visione dell'informativa sulla privacy ed inviarla via fax al numero 089 771330, allegando la fotocopia di un valido documento di riconoscimento. QUOTA SOCIALE La quota sociale per l'anno 2014 è stabilita in € 100,00 e dà diritto alla ricezione della rivista "Archivio Italiano di Urologia e di Andrologia", organo ufficiale della Associazione. Il pagamento della quota sociale 2014 potrà essere effettuato mediante bonifico bancario come segue: Urop - Banco di Napoli SpA - Ag. 3 - Salerno IBAN IT72 U 01010 15203 100000004420 Inserire nella causale del bonifico bancario il proprio Nome e Cognome seguito dalla dizione QS2014. INFORMAZIONI Per richiedere informazioni contattare il Dr. Stefano Pecoraro all'indirizzo e-mail [email protected] oppure al seguente recapito telefonico 333 7451321 Ed _Cop+Ed+fisse 2006 03/04/14 10:36 Pagina II ll ruolo della SIEUN La SIEUN (Società Italiana di Ecografia Urologica, Andrologica, Nefrologica) riunisce diversi medici specialisti e non che si occupano di tutte quelle metodiche in cui gli ultrasuoni vengono utilizzati a scopo diagnostico ed interventistico in ambito uro-nefro-andrologico. La SIEUN organizza un Congresso Nazionale con cadenza biennale e diverse altre iniziative in genere con cadenza annuale (corsi monotematici, sessioni scientifiche in occasione dei congressi nazionali delle più importanti società scientifiche in ambito UroNefro-Andrologico). Dal 2001 la SIEUN è affiliata all’ESUI (European Society of Urological Imaging); pertanto tutti i soci possono partecipare alla iniziative della Società Europea. L’Archivio Italiano di Urologia e Andrologia è l’organo ufficiale della SIEUN. Questa pagina permette una informazione puntuale sulla attività della nostra Società e consente al Consiglio Direttivo della SIEUN di comunicare non solo ai soci, ma ad una platea più ampia, ogni nuova iniziativa. Notizie dalla SIEUN Linee guida sulla Ecografia Urologica ed Andrologica La versione finale delle linee giuda è online sul sito della Società Italiana di Urologia (www.siu.it). Corso di Perfezionamento in Ecografia Urologica, Andrologica e Nefrologica Università di Bari AA. 2013-2014 Anche quest’anno il corso si tiene presso la Urologia 1° Universitaria del Policlinico di Bari, coordinato dal Prof. a.c. P. Martino. Tra i docenti figurano diversi soci della SIEUN. Sito web: www.uniba.it area formazione post laurea. Informazioni: Prof. Pasquale Martino - e mail: [email protected] - tel. 0805594101 Sig. Giacoma Loverro - e mail: [email protected] - tel. 080.5578719 Società Italiana di Ecografia Urologica Andrologica Nefrologica 19° Congresso SIEUN 19° CONGRESSO S.I.E.U.N. 2014 Società Italiana di Ecografia Urologica, Andrologica, Nefrologica Fermo, 15-17 Maggio 2014 Presidente del Congresso Andrea B. Galosi Sede Congressuale Hotel Royal - Località Casa Bianca - FERMO Presidente Onorario del Congresso Giovanni Muzzonigro Ospedale A. Murri - ASUR Marche AV4 - FERMO Presidente Pasquale Martino Vice Presidenti Paolo Consonni, Vincenzo Scattoni Consiglieri Marco Bitelli, Michele Del Zingaro, Giuseppe D’Eramo, Andrea Galosi, Roberta Gunelli, Amelia Liccardo, Giovanni Liguori Tesoriere Michele Barbera Si terrà a Fermo dal 15 al 17 Maggio 2014. Maggiori informazioni verranno inserite sul sito SIEUN (www.sieun.it). Presidente del Congresso è il dott. Andrea Benedetto Galosi. ECM Evento in procedura di accreditamento ECM Modalità di partecipazione Iscrizioni on line: www.congressare.it sez. Meeting ECM 2014 Segreteria Organizzativa e Provider ECM N.2295 PROMISE GROUP srl Via Ghino Valenti, 2 - 60131 Ancona Tel. 071.202123 - Fax 071.202447 e-mail: [email protected] web: www.congressare.it Segretario Silvano Palazzo www.congressare.it/sieun 2014 I PUNTI SIEUN (una possibilità di incontro tra Soci SIEUN e di contatto con altri specialisti) Presso i punti SIEUN i nostri soci potranno essere continuamente informati su tutte le attività e le iniziative della Società e rinnovare il pagamento della quota associativa. I PROSSIMI APPUNTAMENTI SIEUN La SIEUN nel 2014 sarà presente con relazioni, moderazioni e letture nei congressi delle più prestigiose Società scientifiche di Urologia, Andrologia ed Ecografia: Corso Regionale SIEUN Teorico-pratico di Ecografia Andrologica – Roma, 15 Febbraio 2014 25° Congresso Interregionale della Società Apulo-Lucana di Urologia – Bari, 7-8 Marzo 2014 19° Congresso Nazionale Società Italiana di Ecografia Urologica, Andrologica, Nefrologica (SIEUN) – Fermo (AN), 15-17 Maggio 2014 IX° Congresso Nazionale U.R.O.P. – Abano Terme (PD), 22-24 Maggio 2014 XXX Congresso Nazionale SIA – Maratea (PZ), 28-31 Maggio 2014 XXI Congresso Nazionale AURO.it – Roma, 4-6 Giugno 2014 38° Congresso SIUD – Milano, 19-21 Giugno 2014 XXIV Congresso Nazionale SIUrO – Bologna, 22-24 Giugno 2014 87° Congresso Nazionale SIU – Firenze, 27-30 Settembre 2014 RINNOVO PAGAMENTO QUOTA 2014 La segreteria della Società ELLERRE CENTRE QUOTE ASSOCIATIVE 2014 A partire dal 1 Gennaio 2014 le quote sono: Socio ordinario - Euro 70,00 Socio Junior - Euro 35,00 Via S. Matarrese, 47/G - 70124 BARI Coordinate: Conto Corrente n. 2053691 c/o Monte dei Paschi di Siena Intestato a: Tel. 080.5045353 Fax 080.5045362 "S.I.E.U.N. Soc. It. di Ecografia Urologica Nefrologica" 4 II Archivio Italiano di Urologia e Andrologia 2012, 84,IBAN: www.ellerrecentre.it E-mail: [email protected] IT 72 M 01030 04001 000002053691 - BIC: PASCITM1BA1 è a disposizione per ulteriori informazioni. Inviare copia dell’avvenuto bonifico per e-mail: [email protected] o fax 080.5045362 Cop 2014_Layout 1 04/04/14 10:12 Pagina 2 9° Congresso Nazionale 2014 22-24 Maggio 2014 Auditorium Pietro d'Abano - Abano Terme (PD) Segreteria Organizzativa MEC Congress Srl Via Gorizia 51 - 95129 Catania Dr.ssa Antonella Barbagallo tel. 334 6527204 - email: [email protected] Società Italiana Chi intende iscriversi alla SIUrO trova le istruzioni ed i moduli necessari sul sito internet www.siuro.it È possibile pagare la quota associativa annuale on-line: con carta di credito collegandosi direttamente al sito www.siuro.it o tramite bonifico bancario intestato alla Società Italiana di Urologia Oncologica, presso Banca Popolare di Milano IBAN: IT08W0558402402000000000539, avendo cura di specificare il nome del socio pagante Per ottenere ulteriori informazioni è possibile contattare la segreteria Via Dante 17 - 40126 Bologna Tel +39 051 349224 Fax +39 051 349224 e-mail: [email protected] www.siuro.it CHI PUÒ FARNE PARTE Possono far parte dell'Associazione con la qualifica di Socio Ordinario gli Urologi Specialisti in Urologia e gli specializOspedalità Gestione Privata zandi in Urologia operanti in strutture assistenziali urologiche dell’Ospedalità a gestione Privata; con la qualifica di Socio Corrispondente gli studiosi italiani o stranieri che abbiano dimostrato un particolare interesse per l'Urologia. ISCRIZIONE Iscriversi è semplice, basta scaricare la scheda di adesione presente sul sito www.urop.it, compilarla in tutte le sue parti prendendo visione dell'informativa sulla privacy ed inviarla via fax al numero 089 771330, allegando la fotocopia di un valido documento di riconoscimento. QUOTA SOCIALE La quota sociale per l'anno 2014 è stabilita in € 100,00 e dà diritto alla ricezione della rivista "Archivio Italiano di Urologia e di Andrologia", organo ufficiale della Associazione. Il pagamento della quota sociale 2014 potrà essere effettuato mediante bonifico bancario come segue: Urop - Banco di Napoli SpA - Ag. 3 - Salerno IBAN IT72 U 01010 15203 100000004420 Inserire nella causale del bonifico bancario il proprio Nome e Cognome seguito dalla dizione QS2014. INFORMAZIONI Per richiedere informazioni contattare il Dr. Stefano Pecoraro all'indirizzo e-mail [email protected] oppure al seguente recapito telefonico 333 7451321 Cop 2014_Layout 1 04/04/14 10:12 Pagina 1 w ess N o cc a. i t A u en w.ai p O w w ISSN 1124-3562 Poste Italiane S.p.A. - Spedizione in abbonamento postale - D.L. 353/2003 (conv. in L. 27/02/2004 n. 46) Art. 1, comma 1 DCB Milano Archivio Italiano di Urologia e Andrologia / Archives of Italian Urology and Andrology - Vol. 86; n. 1, March 2014 Vol. 86; n. 1, March 2014 ANDROLOGICAL SCIENCES Antioxidant cosupplementation therapy with vitamin C, vitamin E, and coenzyme Q10 in patients with oligoasthenozoospermia Yoshitomo Kobori, Shigeyuki Ota, Ryo Sato, et al. Is there any effect of insulin resistance on male reproductive system? Ayhan Verit, Fatma Ferda Verit, Halil Oncel, Halil Ciftci Evaluation of penile cavernosal artery intima-media thickness in patients with erectile dysfunction. A new parameter in the diagnosis of vascular erectile dysfunction. Our experience on 59 cases Domenico Prezioso, Fabrizio Iacono, Umberto Russo, et al. Urinary and sexual functions after surgical treatment of penile fracture concomitant with complete urethral disruption Ali Abdel Raheem, Hassan El-Tatawy, Ahmed Eissa, et al. Testicular microlithiasis and dyspermia: Is there any correlation? Francesco Catanzariti, Ubaldo Cantoro, Vito Lacetera, et al. Treatment of urethral strictures in balanitis xerotica obliterans (BXO) using circular buccal mucosal meatoplasy: Experience of 15 cases Abdulmuttalip Simsek, Sinasi Yavuz Onol, Omer Kurt Present and future association between obesity and hypogonadism in Italian male Valentina Boddi, Valeria Barbaro, Paul Mc Nieven, et al. In vitro effects of PDE5 inhibitor and statin treatment on the contractile responses off experimental MetS rabbit's cavernous smooth muscle Yasin Erden, Esat Korgalı, Gokce Dundar, et al. Penile fracture: Penoscrotal approach with degloving of penis after Magnetic Resonance Imaging (MRI) Gabriele Antonini, Patrizio Vicini, Salvatore Sansalone, et al. First case of bilateral, synchronous anaplastic variant of spermatocytic seminoma treated with radical orchifunicolectomy as single approach: Case report and review of the literature Giorgio Gentile, Francesca Giunchi, Riccardo Schiavina, et al. Penile strangulation: An unusual sexual practice that often presents an urological emergency Lucio Dell’Atti Rare case of intra-testicular adenomatoid tumour Filippo Migliorini, Roberto Baldassarre, Walter Artibani, et al. Use of inflatable penile prostheses AMS CX with momentary squeeze in a patient with Peyronie’s disease after removal of two previously implanted penile prostheses Patrizio Vicini, Ferdinando De Marco, Gabriele Antonini, et al. Surgical repair of the iatrogenic falsepassage in the treatment of trauma-induced posterior urethral injuries Faruk Dog˘an, Ali Feyzullah S¸ahin, Tevfik Sarıkaya, Alper Dırık The impact of non-urologic drugs on sexual function in men Ferdinando Fusco, Marco Franco, Nicola Longo, et al. Practical recommendations for performing ultrasound scanning in the urological and andrological fields Pasquale Martino, Andrea Benedetto Galosi, Marco Bitelli, et al. Istr_Stesura Seveso 03/04/14 10:32 Pagina 79 INSTRUCTIONS AUTHORS’ RESPONSIBILITIES Manuscripts are accepted with the understanding that they have not been published or submitted for publication in any other journal. Authors must submit the results of clinical and experimental studies conducted according to the Helsinki Declaration on clinical research and to the Ethical Code on animal research set forth by WHO (WHO Chronicle 1985; 39:51). The Authors must obtain permission to reproduce figures, tables and text from previously published material. Written permission must be obtained from the original copyright holder (generally the Publisher). MANUSCRIPT PRESENTATION Authors must submit the text (MAC and WINDOWS Microsoft Word are accepted) and illustrations by e-mail ([email protected]). Manuscripts must be written in English language in accordance with the “Uniform Requirements for Manuscripts submitted to biomedical journals” defined by The International Committee of Medical Journal Editors (http://www.ICMJE.org). Manuscripts in Italian language can be published after translation (expenses will be charged to the Authors). Manuscripts should be typed double spaced with wide margins. They must be subdivided into the following sections: TITLE PAGE It must contain: a) title; b) a short (no more than 40 characters) running head title; c) first, middle and last name of each Author without abbreviations; d) University or Hospital, and Department of each Author; e) last name, address and e-mail of all the Authors f) corresponding Author g) phone and/or fax number to facilitate communication; h) acknowledgement of financial support; i) list of abbreviations. SUMMARY The Authors must submit a long English summary (300 words, 2000 characters). Subheadings are needed as follows: Objective(s), Material and method(s), Result(s), Conclusion(s). After the summary, three to ten key words must appear, taken from the standard Index Medicus terminology. TEXT For original articles concerning experimental or clinical studies and case reviews, the following standard scheme must be followed: Summary - Key Words - Introduction - Material and Methods - Results Discussion - Conclusions - References - Tables - Legends - Figures. SIZE OF MANUSCRIPTS Literature reviews, Editorials and Original articles concerning experimental or clinical studies should not exceed 20 typewritten pages including figures, tables, and reference list (references are to be limited to 20, additional references may be submitted as supplementary materials for posting on www.aiua.it.). Case reports, Notes on surgical technique, Short Communications and Letters to the editors should not exceed 1000 words (summary included) with only one table or figure, and no more than three references. No more than five authors are permitted. As an accompaniment to Case reports, Notes on surgical technique and Short Communications manuscripts for the print version of Archivio Italiano di Urologia e Andrologia (AIUA), authors may submit supplementary materials for posting on www.aiua.it. The material is subject to the same editorial standards and peer-review procedures as the print publication. FAST-TRACK PEER REVIEW We offer fast-track peer review and publication of controlled trials that we judge of importance to practice or research. If you wish to discuss your proposed submission, please write ([email protected]) or call our editorial office in Milan (+39 02 70608091). REFERENCES References must be sorted in order of quotation and numbered with arabic digits between parentheses. Only the references quoted in the text can be listed. Journal titles must be abbreviated as in the Index Medicus. Only studies published on easily retrieved sources can be quoted. Unpublished studies cannot be quoted, however articles “in press” can be listed with the proper indication of the journal title, year and possibly volume. References must be listed as follows: TO AUTHORS BOOK CHAPTERS Authors of the chapters - Complete chapter title. In: Book Editor, complete Book Title, Edition number. City of publication: Publisher, Publication year: first page of chapter in the book. Example: Sagawa K. The use of central theory and system analysis. In: Bergel DH (Ed), Cardiovascular dynamics. 2nd ed. London: Academic Press Inc., 1964; 115. TABLES Tables must be aimed to make comprehension of the written text easier. They must be numbered in Arabic digits and referred to in the text by progressive numbers. Every table must be accompanied by a brief title. The meaning of any abbreviations must be explained at the bottom of the table itself. (If sent by surface mail tables must be clearly printed with every table typed on a separate sheet). FIGURES (Graphics, algorithms, photographs, drawings). Figures must be numbered and quoted in the text by number. The meaning of all symbols, abbreviations or letters must be indicated. Histology photograph legends must include the enlargement ratio and the staining method. Legends must be collected in one or more separate pages. Please follow these instructions when preparing files: • Do not include any illustrations as part of your text file. • Do not prepare any figures in Word as they are not workable. • Line illustrations must be submitted at 600 DPI. • Halftones and color photos should be submitted at a minimum of 300 DPI. • Power Point files cannot be uploaded. • If at all possible please avoid transmitting electronic files in JPEG format. If this is unavoidable please be sure to save the JPEG at the highest quality available and at the correct resolution for the type of artwork it is • PDF files for individual figures may be uploaded. MANUSCRIPT REVIEW Only manuscript written according to the above mentioned rules will be considered. All submitted manuscripts are evaluated by the Editorial Board and/or by two referees designated by the Editors. The Authors are informed in a time as short as possible on whether the paper has been accepted, rejected or if a revision is deemed necessary. The Editors reserve the right to make editorial and literary corrections with the goal of making the article clearer or more concise, without altering its contents. Submission of a manuscript implies acceptation of all above rules. PROOFS Authors are responsible for ensuring that all manuscripts are accurately typed before final submission. Galley proofs will be sent to the first Author. Proofs should be returned within seven days from receipt. REPRINTS A copy of the issue in which the article appears will be provided free of charge. Reprints are not provided. The PDF file is only for personal use. OPEN ACCESS All papers published in Archivio Italiano di Urologia e Andrologia (AIUA) are peer reviewed and upon acceptance will be immediately and permanently free for everyone to read and download (Open Access). Open Access means making your papers available to anyone, at any time. In order to cover the costs associated with Open Access publication, a fee has to be pay by the author or research funder to cover the costs associated with publication. As of January 1, 2014 the Authors of Case Reports, Notes on Surgical Technique, Short communications and Letters to the Editors published in Archivio Italiano di Urologia e Andrologia (AIUA) will be charged a publication fee of 200 Euros + VAT. Reviews and Original papers will continue to be published free of charge. Authors who will pay a fee for Open Access publication will use an exclusive licensing agreement, where they will retain copyright alongside scholarly usage rights and Edizioni Scripta Manent will be granted publishing and distribution rights. PAYMENT OF ARTICLE PROCESSING CHARGE JOURNAL ARTICLES The submitting authors must confirm, at the time of submission, that they will organize payment should the article be accepted for publication. Following peer review, once a manuscript has received editorial acceptance in principle, the submitting author needs to arrange payment of the article-processing charge. Once formatting checks are completed, and payment of the article-processing charge has been received, the article will be published. BOOKS Payment can be made by any of the following methods: 1) Invoice payment to the bank account Edizioni Scripta Manent s.n.c. Via E. Bassini, 41 - 20133 Milano IBAN: IT 23 K 02008 01749 000100472830 2) PayPal international e-commerce payment connecting to https://www.paypal.com/cgi-bin/webscr?cmd=_s-xclick&hosted_button_id=ZUPFHQWA7WRY2 Name, surname and tax codes (CF and P.IVA for Italy) are to be attached. A receipt will be sent once payment has been processed. All Authors if there are six or fewer, otherwise the first three, followed by “et al.”. Complete names for Work Groups or Committees. Complete title in the original language. Title of the journal following Index Medicus rules. Year of publication; Volume number: First page. Example: Starzl T, Iwatsuki S, Shaw BW, et al. Left hepatic trisegmentectomy Surg Gynecol Obstet. 1982; 155:21. Authors - Complete title in the original language. Edition number (if later than the first). City of publication: Publisher, Year of publication. Example: Bergel DIA. Cardiovascular dynamics. 2nd ed. London: Academic Press Inc., 1974. Istruz_Cop+Ed+fisse 2006 24/06/13 11:14 Pagina 57 NEW WEBSITE: www.aiua.it W! E N Pages 352 - The cost of a printed copy is € 30 plus shipping. Pdf price € 30,00 To purchase go to: http://www.urologyplanet.it/ The stone disease is extremely diverse – from single stone formers with spontaneous stone passage to staghorn stones and stone diseases associated with severe metabolic abnormalities such as renal tubular acidosis and primary hyperoxaluria. It is obvious that these different conditions should be dealt with selectively. In this context sharing knowledge on clinical practices – tips and tricks – between practising stone clinicians becomes especially important, and the most effective way that tips and tricks may be lifted up into an academic sphere is through international knowledge exchange. It is with this respect that this handbook on stone management plays a particular important role by creating a platform for exchange of clinical expertise. The contributors are international renowned stone experts, sharing with us their views of different approaches to the great variety of urinary stone diseases. The handbook offers a unique synthesis of theory and tips-and tricks-technology, bridging basic science and daily clinical practice. Palle Osther, MD, PhD Professor of Urology Chairman, EAU Section of Urolithiasis (eULIS)
© Copyright 2026 Paperzz