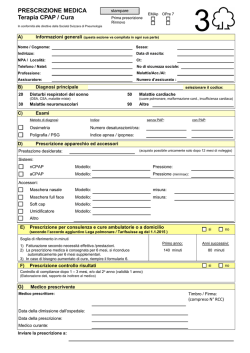
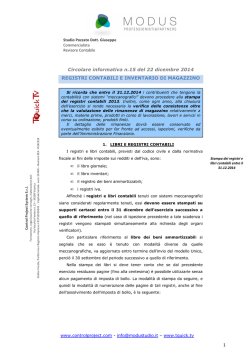
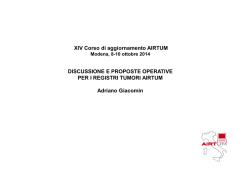
I registri come strumenti per la ricerca indipendente Luigi Naldi USC Dermatologia, Azienda Ospedaliera papa Giovanni XXIII, Bergamo Conflitto di interessi Il dott. Naldi ha svolto, negli ultimi tre anni, consulenza scientifica retribuita per le seguenti aziende: Abbvie, Amgen, Baxter, Boehringer Ingelheim, Celgene, Janssen-Cilag, Lilly, Menarini, Newron, Novartis, Pfitzer, Sanofi-Pasteur, Teofarma • Di cosa parliamo quando parliamo di registri? • Un modo ottimale per valorizzare e mettere in comune l’esperienza clinica • Un antidoto all’auto-referenzialità • registri come nucleo di germinazione di differenti approcci di ricerca • Di cosa parliamo quando parliamo di registri? • Un modo ottimale per valorizzare e mettere in comune l’esperienza clinica • Un antidoto all’auto-referenzialità • registri come nucleo di germinazione di differenti approcci di ricerca What is a registry? A systematic collection of information on all the cases of a particular disease or other health relevant condition. The term applies to the process of collecting data and to the final result of such a process (ie, the file or database containing the information, properly, the ‘‘register’’) • Di cosa parliamo quando parliamo di registri? • Un modo ottimale per valorizzare e mettere in comune l’esperienza clinica • Un antidoto all’auto-referenzialità • registri come nucleo di germinazione di differenti approcci di ricerca Registry requirements 1. Unambiguous case definition 2. Thorough procedures to identify cases 3. Systematic methods for case registration that minimize missing data 4. Standardized procedures for collecting and storing data and ensuring data confidentiality EM majus Stevens-Johnson syndrome Overlap SJS/TEN Atypical target Spot TEN Il professor Keating nel film L’attimo fuggente Treatment registries • Observational (non-experimental) studies that actively enroll subjects • Registration is ideally prospective – Drug exposure at entry – Only treatment newly started (inception cohort) Healthy worker effect Depletion of susceptible Cumulative survival Conventional Biologicals months Research Design Patient Follow-up – Patient follow-up: • Update drug exposure & risk factor information • Collect information on outcome and any new relevant diagnosis of interest • Consistent, similar follow-up for all people to avoid bias • Specify criteria to define subjects that are pending and those lost to follow-up Incidence rate ratio (95% CI) 5.0 Follow-up period of risk estimate 4.0 UK national register US claims data 3.0 RCT meta-analysis Swedish national register German national register 2.0 1.0 1 2 3 0.8 Time period of risk assessment (years) 0.6 Slide Courtesy of Will Dixon • Di cosa parliamo quando parliamo di registri? • Un modo ottimale per valorizzare e mettere in comune l’esperienza clinica • Un antidoto all’auto-referenzialità • registri come nucleo di germinazione di differenti approcci di ricerca REGIONE Abitanti (1.1.2007) Centri Psocare Abruzzo Basilicata Calabria Campania Emilia Romagna Friuli Venezia Giulia Lazio Liguria Lombardia Marche Molise Piemonte Puglia Sardegna Sicilia Toscana Trentino Alto Adige Umbria Valle D'Aosta Veneto 1.309.797,00 591.338,00 1.998.052,00 5.790.187,00 4.223.264,00 1.212.602,00 5.493.308,00 1.607.878,00 9.545.441,00 1.536.098,00 320.074,00 4.352.828,00 4.069.869,00 1.659.443,00 5.016.861,00 3.638.211,00 994.703,00 872.967,00 124.812,00 4.773.554,00 6 1 8 13 11 5 12 7 19 6 1 10 8 5 12 13 5 2 1 9 Totale 59.131.287,00 154 15000 Numero pazienti inseriti per data 380 9 73 173 0 14130 14202 14000 13580 13814 13320 13055 13000 12643 12240 11840 12000 11340 11085 10736 10333 10020 9762 9562 9292 11000 10000 8831 8456 8072 9000 8000 7000 6629 7000 7474 6011 6000 5512 5017 5000 4426 4250 3788 4000 3209 3000 2637 2220 2000 1000 1460 709 t ot 3- t e -s 26 o g -a 29 g -lu 25 u i -g 27 ag -m 30 r p -a 25 ar -m 28 b -fe 29 n e -g 25 c i -d 28 v o -n 30 t t -o 26 t e -s 28 o g -a 31 g -lu 27 u i -g 29 ag -m 25 r p -a 27 ar -m 30 b -fe 7 23 n-0 e -g 26 c i -d 29 v o -n 24 t t -o 27 t e -s 29 o g -a 25 g -lu 28 u i -g 30 ag -m 26 r p -a 28 ar -m 31 b -fe 6 24 n-0 e -g 30 c i -d 27 v o -n 27 t t -o 5 28 t-0 se 28 • Meta-analysis of effect measures • Effect measures are calculated using the same methods and after adjusting for the same confounders. RO OF 01 Evaluation of Patient Education 02 03 04 Luigi Naldi and Fabrizia Sassi 05 06 07 08 09 DP 10 11 12 13 Health Education and Behavioural Changes 14 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 Patient education is the process of enabling individuals to make informed decisions about their personal health-related behaviour. It aims to improve health by encouraging compliance with medical treatment regimens and promoting healthy lifestyles [1]. Patients have a right to receive appropriate education, so they can utilize their knowledge to participate in decision-making process [2]. Professionals in health care have a commitment to provide unbiased and evidence-based information to help educate patients. Virtually every patient encounter should include some element of patient education. The physician who uses a variety of strategies (e.g., verbal messages, printed materials, computerized information) and involves staff in patient education efforts is most likely to be a successful patient educator [3]. Building a partnership with patients over time and understanding the perceptions, values, and beliefs that influence their health behaviours are the underlying principles of clinical practice that provide the foundation for helping patients to change. It is in the context of “continuity of care” that theories of health behaviour are most beneficial [4]. UN CO RR EC TE 15 Behavioural M odels Behavioural change for patients is a complex process and requires more than the simple acquisition of knowledge. In fact, the choices that patients make may be influenced by many factors beyond knowledge, including personal, familial, spiritual, and social issues. Several educational models based on behavioural theories have been developed to explain individuals’ health-related behaviour, including the Stages of Change Model, the Health Belief Model, the Health Promotion Model, the Precede-Proceed Model, the Health Information Model, and many others. These react registro eventi avversi cutanei Obiettivi • Ottenere una precisa caratterizzazione degli eventi avversi gravi dermatologici • Monitorare i tassi di incidenza • Valutare i fattori eziologici con particolare attenzione per farmaci di recente introduzione sul mercato • Valutare mortalità e morbidità associate alle reazioni • Migliorare la gestione clinica attraverso la costituzione di una collaborazione in rete (rete lombarda per la gestione delle reazioni cutanee gravi da farmaco) Centri Partecipanti Responsabile FARMACOVIGILANZA Responsabile DERMATOLOGIA ISTITUTI OSPEDALIERI CREMONA Catia Barosi Enrico Pezzarossa OSP TREVIGLIO - CARAVAGGIO Lavinia Gilberti, Mariella Di Matteo Francesco Accaria OSPEDALE NIGUARDA CA’ GRANDA Giuseppe Vighi Donata Calò, Antonella Citterio, Jan Schroeder OSPEDALI CIVILI BRESCIA Daria Bettoni Andrea Brezzi ISTITUTO DEI TUMORI MILANO Barbara Re Marco Cusini A.O. VALTELLINA VALCHIAVENNA SONDRIO Lucia Canclini Luisa Frattini A.O. S ANTONIO ABATE DI GALLARATE Giovanna Monina Silvia Fossati A.O. BOLOGNINI DI SERIATE Antonio Strippoli Antonio Barcella PRESIDIO OSPEDALIERO A MANZONI LECCO Paolo Corti Domenico Fideli A.O. G. SALVINI GARBAGNATE MILANESE Franca Borin Andrea Bigardi A.O. DELLA PROVINCIA DI LODI Elena Gambarana Claudia De Filippi A.O. OSPEDALE S. ANNA COMO Luisa Clerici Giuseppe Laria IRCCS S MATTEO PAVIA Ester Guarnone Antonio Borroni, Camilla Vassallo A.O. LUIGI SACCO Emilio Clementi, Sonia Radice Gianluca Tadini A.O. OSPEDALE MAGGIORE DI CREMA Luigi Brambilla, Alessandra Ragazzi Serena Percivalle A.O. DI DESIO E VIMERCATE Giuseppina Gilberti Elena Perotta A.O. S CARLO BORROMEO Anna Maria Fiori Pasquale Bruni OSPEDALI RIUNITI DI BERGAMO Monia Lorini Luigi Naldi SAN RAFFAELE Camilla Ferri Massimo Cantori LEGNANO Piercarlo Erpoli Anna.Tosi VARESE Anna Malesci Alberico Motolese HUMANITAS Maria Fazio Marcello Monti Registro regionale di reazioni avverse gravi dermatologiche 2009- M N O A G U ER IG B N R D A TR A EV M O IG M L IL A BR IO N O ES C S C IA A R LO G A PAV LL I A A R AT E C O M O C R E C R MA EM LE ON A G N A SE NO G A R RIA B TE A G VA N LT AT EL E H L U M IN A A N IT A S IL A Notifiche casi TEN, SJS, AGEP,DRESS (aprile 2009-marzo 2013) 20 19 18 17 16 15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 0 • Di cosa parliamo quando parliamo di registri? • Un modo ottimale per valorizzare e mettere in comune l’esperienza clinica • Un antidoto all’auto-referenzialità • registri come nucleo di germinazione di differenti approcci di ricerca Europe-wide observational network on rare skin disease (REDSkin network) Issues • No single centre can collect enough cases to reliably assess risk factors, prognostic variables or disease outcome for rare diseases • An harmonised joined action on rare diseases can rapidly improve knowledge optimizing costs and resources • As documented by a few successful projects (e.g., the RegiSCAR programme, the GeneSkin project) a modular combination of research activities is feasible for motivated people Disease of interest for a piloting phase • • • • • • • Pyoderma gangrenosum Hidrosadenitis suppurativa Sweet syndrome Linear IgA dermatosis Cicatricial pemphigoid Generalized pustular psoriasis Cutaneous small vessel vasculitis In sintesi, i registri all’interno di reti collaborative permettono di ottenere: • Sinergie • Valorizzazione delle competenze • Confronti di esperienze diverse • Un miglioramento della pratica clinica
© Copyright 2026 Paperzz