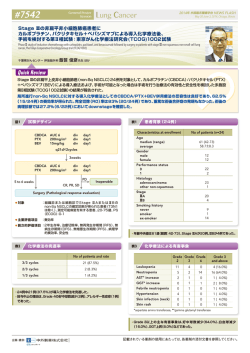
精神・神経疾患研究開発費 23-4 遺伝性神経・筋疾患における患者登録システムの構築と 遺伝子診断システムの確立に関する研究 総括研究報告書 (平成23年度-平成25年度) 平成26年(2014)年 3月 主任研究者 木 村 円 目 次 総括研究報告 木村 主任研究者 円 分担研究報告 Ⅰ. 神経・筋疾患患者登録システム Remudy の運用、データ登録、情報開示/提供 9 1) 遺伝性神経・筋疾患の臨床研究の推進を目的とする疾患レジストリーの構築と有機的運用 独立行政法人国立精神・神経医療研究センター トランスレーショナル・メディカルセンター 木村 円 Ⅱ. Remudy の周知活動 1) 中国・四国地区の筋ジストロフィー患者データベース登録の促進活動 21 ~とくに中国四国政策医療神経筋ネットワーク協議会の活動から~ 独立行政法人国立病院機構 徳島病院 四国神経・筋センター 足立 克仁 25 2) 鹿児島県内の筋ジストロフィー患者のデータベースの構築に関する研究 独立行政法人国立病院機構 南九州病院 園田 至人 29 3) 秋田県における筋ジストロフィー患者登録システムへの登録促進活動 独立行政法人国立病院機構 あきた病院 小林 道雄 Ⅲ. データ解析と疫学研究による情報提供 35 1) 遺伝性神経・筋疾患における臨床試験の課題と患者登録データベースの活用に関する研究 独立行政法人国立精神・神経医療研究センター トランスレーショナル・メディカルセンター 米本 直裕 37 2) 日本のデュシェンヌ型筋ジストロフィー推定患者数 独立行政法人国立病院機構 東埼玉病院 川井 充 Ⅳ. 新規登録システムの開発研究 1) Remudy 登録情報のオンライン管理 43 独立行政法人国立病院機構 下志津病院 1 本吉 慶史 Ⅴ. 遺伝性神経・筋疾患の診断システムの確立 1) 遺伝性神経・筋疾患患者データベースに対する遺伝子診断システムの確立 独立行政法人国立精神・神経医療研究センター 神経研究所 49 西野 一三 2) 遺伝性神経・筋疾患患者データベースに対応する遺伝子診断システムの確立 独立行政法人国立精神・神経医療研究センター 病院 51 南 成祐 3) ジスフェルリン異常症の患者登録システムの構築と遺伝子診断システムの確立に関する研究 独立行政法人国立病院機構 仙台西多賀病院 59 髙橋 俊明 Ⅵ. 新規対象疾患レジストリーへの応用 1) GNE ミオパチー(縁取り空胞を伴う遠位型ミオパチー)患者登録システム確立のための試み 独立行政法人国立精神・神経医療研究センター 病院 森 67 まどか 2) 神経・筋疾患患者データベースの登録促進及び患者登録の研究 一般社団法人 日本筋ジストロフィー協会 71 貝谷 久宣 Ⅶ. 国際協調・難治性希少疾患全体を俯瞰した展開 75 1) 筋ジストロフィーの臨床試験実施体制構築に関する研究 国立保健医療科学院 研究情報支援研究センター 水島 洋 Summary 81 論文 87 Remudy 通 信 115 研究者一覧表 155 2 総 括 研 究 報 告 主任研究者 【研究目的】 木村 円 * 【研究組織】 前研究班(川井班)で構築された Remudy を引き継ぎ 主任研究者 ナショナルレジストリーとしての遺伝性神経・筋疾患患者 木村 円 登録システムを構築・運用し、遺伝性神経・筋疾患の診 (独)国立精神・神経医療研究センター 断に対応できる遺伝子診断システムを確立することが本 トランスレーショナル・メディカルセンター 研究のテーマである。その目的は、1) 神経・筋疾患患者 分担研究者 登録システム Remudy を安定して運用し、臨床試験の実 現可能性を検討するための情報開示、臨床試験の参加 西野 一三(2013 年 8 月〜) 者リクルートに関する情報提供、さらに国際協調を進め 林 由起子(2011 年 4 月〜2013 年 7 月まで) 希少疾患の代表である筋ジストロフィーの臨床開発研究 (独)国立精神・神経医療研究センター を推進すること、2) レジストリーを活用した臨床研究を展 神経研究所 森 まどか 開することで、難治性の希少疾患の克服を目指したオー (独)国立精神・神経医療研究センター 病院 ルジャパン体制の構築と国際協働のためのキーとしてナ 南 成祐 ショナルセンターが担うべき役割のプロトタイプを明確に (独)国立精神・神経医療研究センター 病院 提示すことである。 米本 直裕 1.神経・筋疾患患者登録シスム Remudy の運用 (独)国立精神・神経医療研究センター a)データ収集、情報開示/提供 :木村、森 トランスレーショナル・メディカルセンター b)Remudy の周知活動 川井 充 (独)国立病院機構 東埼玉病院 :足立、園田、小林 足立 克仁(2014 年 4 月〜) c)データ解析と疫学研究による情報提供 :米本、川井 (独)国立病院機構 徳島病院 本吉 慶史 d)新規登録システムの開発研究 :本吉 (独)国立病院機構 下志津病院 水島 洋 2.遺伝性神経・筋疾患の診断システムの確立 :西野、南、高橋 国立保健医療科学院 貝谷 久宣 3.新規対象疾患レジストリーへの応用、難治性の希少 疾患全体を俯瞰した展開 一般社団法人 日本筋ジストロフィー協会 a) 新規の疾患登録整備 園田 至人 :森、貝谷 (独)国立病院機構 南九州病院 b) 国際協調 髙橋 俊明 :水島、木村 (独)国立病院機構 仙台西多賀病院 以上の目的を達成するために、全国から優れた研究戦 小林 道雄 略を持つ研究者を選抜し、総員 13 名の班員構成とした。 (独)国立病院機構 あきた病院 * 独立行政法人国立精神・神経医療研究センター トランスレーショナル・メディカルセンター 3 【研究成果】 1. タと国立病院筋ジストロフィーネットワークのデータベース 神経・筋疾患患者登録シスム Remudy の運用、デー の解析から作成された生命表を用いた研究では、日本 タ登録、情報開示/提供 (木村、森) の現在の DMD 患者数はおよそ 3,500 人と推定された。 H26 年 1 月末現在、dystrophinopathy 登録依頼件数 は 1,243、クリニカルキュレーター及びジェネティックキュ 4. 新規登録システムの開発研究(本吉) レーターによって確認された本登録件数は Duchenne 型 患者自身による登録方法をわかりやすく改良し、これ 874、Becker 型 187、中間型 27、GNE ミオパチー登録 をサポートする医師・医療従事者の負担の軽減を図り、 依頼件数は 148 であった。情報は 1 年毎に更新されてい かつ患者情報登録業務の標準化、登録手順の効率化を る。あわせて患者登録ウェブサイト、筋ジストロフィー臨床 実施した。さらにウェブベースの更新手続きも検討した。 研究班による市民公開講座、日本筋ジストロフィー協会 個人情報に関するセキュリティーを特に重視したウェブ 等の患者支援団体の研修会を通じて登録手順、登録情 登録システムは安定性・汎用性に優れ、臨床研究・治験 報の更新の手順をわかりやすく周知するとともに、最新の を視野においた精神、神経疾患、希少な難治性疾患の 臨床研究・臨床試験に関する情報提供として、郵送の媒 登録システムへの応用を目指している。 体(Remudy 通信:年 3−4 回)、e-mail による情報発信 (Remudy ニュースレター:月 2−3 回)、ホームページ(週 5. に 2−3 回の更新)を継続して実施し、さらに充実中である。 遺伝性神経・筋疾患の診断システムの確立(西野、 南、高橋) アウトプットとして、明確化された開示手順規定のもとに DMD/BMD(西野) 情報開示委員会における承認を含めた手続きを遵守し、 平成 25 年 12 月末までにジストロフィン遺伝子解析依 一部 TREAT-NMD を介し治療研究を推進する研究者・ 頼総数は 342 件で 340 件が解析済みであり、順調に解 製薬企業等に情報開示を実施し(累計 11 件)、さらに臨 析が進められた。MLPA 法で単独エクソン欠失・重複の 床試験のリクルートに関する情報提供を対象となる可能 場合は、当該エクソンとその両側の計 3 エクソンについて 性がある登録者向けに実施した(2 件)。 解析を行い(41%)、MLPA 法で検出できない場合は全 79 エクソンの解析を行った(59%)。 2. GNE ミオパチー (DMRV:縁取り空胞を伴う遠位型ミオパチー) Remudy の周知活動(足立、園田、小林) 日本全国各地に情報を提供するために国立病院機構 (西野) 神経・筋疾患研究ネットワークや、全国の関連する医療 300 名を超える GNE ミオパチー患者の GNE 遺伝子 機関に対して行った郵送によるアンケート調査、および 解析を行い、H25 年 1 月〜H25 年 12 月の解析数は 63 直接の訪問による説明等の方法で広報・周知活動を継 件であった。ホモあるいは複合へテロ接合変異が 41%、 続して行った。特に平成 25 年に園田・足立らによって実 1 変異のみ検出されたもの 3%、変異無しが 51%であっ 施された全国規模の周知状況の調査からは、未だ医療 た。GNE には好発変異が存在するが、新規変異も多く認 機関の約 26%では Remudy 自体が認知されていない状 められた。 況が明らかになり、今後も周知活動が重要であると考えら 眼咽頭型筋ジストロフィー(OPMD)および筋強直性ジス れた。また、中国・四国地域、九州地域、東北地域での トロフィー1 型・2 型(DM1/2)(南) 登録業務の促進や地域データベースの構築・運営に関 PABPN1 遺伝子変異が認められた眼咽頭型筋ジストロ する研究も継続して行った。 フィー(OPMD)99 名/84 家系について、GCN リピート 数・遺伝子型と、発症年令に代表される臨床所見との間 3. データ解析と疫学研究による情報提供(米本、川井) に逆相関があることが確認された。また筋強直性ジストロ 蓄積されたデータベースを有効に活用する方法論を フィー1型・2型の遺伝子解析方法の検討も行われた。 検討し、疫学データの解析を行い、日本における筋ジス ジスファリノパチー(Dysferlinopaty:三好型遠位型筋ジス トロフィーナショナルレジストリーの現状について報告した トロフィー/肢帯型筋ジストロフィー2B 型)(高橋) (1, 2)。特に、ガイドライン作成委員会から派生した情報を PCR-SSCP 法によって 91 家系に 42 種類の dysferlin 元に、本邦においては初めてとなる Duchenne 型筋ジスト 遺伝子変異を確認し、さらに全 55 エクソンのシークエン ロフィーに対するコルチコステロイド・プレドニゾロンの有 スをおこない 45 家系に 31 種類の変異を同定した。また 用性を、世界でも比類のない多数例の比較検討として提 次世代シークエンサーを用いた解析の検討も開始した。 示した。また人口統計による男児の年次別出生数のデー 4 6. 新規対象疾患レジストリーへの応用(森、貝谷) の枠組みの中で本研究が占める役割について検討した。 GNE ミオパチー(DMRV・縁取り空胞を伴う遠位型ミオパチー) また希少疾患・難病に関する連絡会(隔月)、NCNP (森) TMC 主催の疾患レジストリー研究準備会(NCNP 内、 GNE ミオパチー患者情報登録は H24 年 6 月に登録 2013 年 1 月)、疾患レジストリー研究会設立準備会(品川、 をスタートした。H25 年 11 月末現在の臨床・遺伝子変異 2013 年 2 月)では、患者情報登録を計画・推進する研究 に関する情報を解析した。特に呼吸機能検査を受けてい 者・患者支援団体との調整や意見交換を行った。さらに る登録者のうち 33%に%FVC の低下がみられ、若年発症 保健医療科学院と共同で第 1 回 稀少疾患登録/国際ワ 者に%FVC の低下した例が多く、発症年齢と呼吸機能の ークショップを開催し、欧州、米国、中国からキーパーソ 関連が予想された。 ンを招き国際交流・協調を進めると共に、日本国内にお 福山型先天性筋ジストロフィー(貝谷) けるそれぞれの患者情報登録事務局が抱える問題点を 日本筋ジストロフィー協会が主体となり 2011 年 10 月よ 共有し、解決のための意見交換・協力体制を確認できた。 り福山型先天性筋ジストロフィーの登録を開始し、2014 第 34 回日本臨床薬理学会でのシンポジウム「臨床研究 年 1 月 23 日時点で 165 件の登録を受け付けた。年度毎 における疾患レジストリー(患者情報登録)の役割と本邦 にアンケート調査を実施、結果は研究班会議や協会のウ における現状」(2013 年 12 月)では、特に創薬に関わる ェブサイト等で報告され、分科会「ふくやまっこ家族の会」 レジストリーあり方を報告した。一連の活動を通して、希 の活動にも反映された。 少疾患を対象とした臨床研究を進める枠組みには、患 筋強直性ジストロフィーを含むミオトニー症候群(木村) 者・家族、医療者だけでなく、ステークホルダーとなる製 2012 年 2 月、臨床研究の基盤となるレジストリーの準 薬企業担当者、研究者、患者支援団体等との協調体制 備委員会を組織し、キュレーターの育成、登録項目の選 を構築することが重要であることを示した。 定をすすめ、同時に各専門家間の調整を行った。大阪 また国立保健医療科学院 政策技術評価研究部 佐 大学に Remudy 筋強直性ジストロフィー登録事務局を設 藤元部長との共同研究(武田伸一トランスレーショナル・ 置する準備を行い、大阪大学および NCNP の倫理審査 メディカルセンター長が分担研究者)として、臨床研究・ 委員会へ現在申請中である。 治験の情報提供を行うポータルサイトの改良を目指した 「国民・患者への臨床研究・治験に関する情報利用実態 7. 国際協調・難治性希少疾患全体を俯瞰した展開 とニーズ調査」を NCNP 病院職員、通院患者に先駆けて (水島、木村) Remudy 登録者に対し 2013 年 3, 4 月に実施した。登録 神経・筋疾患の臨床試験を前提とした患者登録システ 者を対象とする研究により、登録事務局の機能が活性化 ムと評価システムの構築と標準的ケアのガイドライン作成 し新規の研究や事業に対する柔軟な受け入れ体制が確 を統合した活動を行う国際組織 TREAT-NMD alliance と 立された。 協調し、登録情報を匿名化の上 TREAT-NMD global registry に統合し世界的なデータ解析を実施できた。また 新たにスタートした GNE ミオパチー国際登録との協働を 【今後の研究の進め方】 進め、さらに筋強直性ジストロフィー、ジスファリノパチー 本研究で運営する神経・筋疾患患者登録システム など、順次疾患を拡大する方針とした。 Remudy は、臨床開発研究を見据えた日本初の希少疾 また登録の DMD 患者家族を対象に NCNP 筋疾患セ 病を対象とするナショナルレジストリーである。この成功の ンターと共同で日本語版 CARE-NMD サーベイを実施し 背景は、極めて精度の高い遺伝子解析システム、患者・ た。ヨーロッパを中心に行われている DMD 患者・家族向 家族(患者団体)、診療にあたる全国の医療関係者の理 けの調査であり、これ自体が医療・ケアの標準化を目指 解・協力、国際的協調を含め精密に準備された運営シス した情報提供でもあった。結果はヨーロッパのデータとの テムに拠る。このシステムを継続し、対象疾患を拡大、ま 比較検討を行い、ヨーロッパの報告を待って論文報告す た他の研究グループと協働して精神・神経疾患や難治の る方針とした。 希少性疾患のレジストリーの構築を進める。さらに現在計 画されている難病対策による患者登録の仕組みと相補、 本研究で運営する神経筋疾患患者情報登録 Remudy 特に臨床研究基盤を強化し、我が国の医療行政を含め は、遺伝性神経・筋疾患を含む希少な難治性疾病レジス て全体を俯瞰した公平で効率的に展開される患者情報 トリーのモデルとなることを目指しており、稀少疾患全体 登録システムの構築が重要である。 5 1. 国際的なグローバルレジストリーを展開する TREATNMD alliance や RD connect 等と適宜協調する。具体的 には情報集積性を高め情報開示/提供依頼に対する迅 速化を図る試みに積極的に参加していく。また本邦に多 い疾患では、特に指導的な立場で参画する。 2. 臨床開発を担当する研究者・製薬企業への正確な情 報開示については、筋ジストロフィー臨床試験ネットワー クとも連動し、速やかで正確な情報提供を公平に行う仕 組みを整備し、またこれから実施される医師主導治験、 国際共同試験等のリクルートを含めた登録者への情報 提供が出来るように、実際的な働きかけを続けていく。ま た疾患毎に対応できる臨床研究ネットワークの設立を基 盤としてサポートし、運用面で連携して活動する。 3. 登録患者医療者への公平でタイムリーな情報提供を 継続して実施すると共に、日本全国どこでも公平な形で 情報を共有できる様、登録の少ない地域にも積極的に働 きかけを続けていく。特に筋疾患診療に積極的な医療施 設がない地域に対しても、地域の公的病院・大学病院、 医師会、患者会、保健行政等のネットワークへの働きか けをすすめる。臨床試験に公平に参加できる体制を整備 することが重要である。 4. ウェブ登録システムの導入をすすめる。これは国際協 調の面でも、対象疾患の拡大のためにも重要である。トラ ンスレーショナル・メディカルセンターと共同で、個人情 報保護の面でのセキュリティーに重点を置いたユーザー フレンドリーでかつ登録業務の効率化を実現する汎用性 の高いシステムを構築し、この運用と改良を継続する。 5. 難治性の希少疾病レジストリーへの拡大を指向する。 難病・希少疾病等の研究者による既存のデータベース や現在進められている難病改革の中核となる特定疾患 登録システムの仕組みとの共通点・問題点を比較検討し、 ナショナルレジストリーの成功例として Remudy の役割や 提供できるノウハウを明らかにし、これを提供することで、 我が国の医療行政に貢献することができる臨床研究基 盤を実現させる。 謝辞:ご登録頂いている全国の患者・家族の皆さま、協 力いただいている担当医をはじめ医療従事者の皆さまに 心より感謝申し上げるとともに、臨床開発研究の発展の ために本研究班を組織させて頂いていることに深く感謝 したい。 6 Ⅰ. 神経・筋疾患患者登録システム Remudy の 運用、データ登録、情報開示/提供 遺 伝 性 神 経 ・筋 疾 患 の臨 床 研 究 の推 進 を目 的 とする 疾 患 レジストリーの構 築 と有 機 的 運 用 木 村 円 * 研究協力者 中村 治雅*, 玉浦 明美*, 佐藤 有希子*, 竹内 芙実*, 鷹羽 智子* 小篠 史郎**, 村上 てるみ***, 石崎 雅俊****, 齊藤 利雄***** や遺伝子診断を含む診断方法をわかりやすい形で提供、 【研究の要旨】 周知することが必要である。 遺伝性神経・筋疾患の臨床研究の推進を目的とする 疾患レジストリーの構築、および改良を行いつつ安定し 国際的には、ヨーロッパには、神経・筋疾患の治験を て運営を継続した。設立当初の目的である、1)臨床研究 前提とした患者情報登録システムと評価システムの構築 の計画及び実施の際に対象となる疾患の疫学データを と標準的 ケアのガイ ドライ ン 作成を統合し た TREAT- 供与し、2)参加条件に合致する可能性がある登録者へ NMD alliance(a network of excellence for neuromuscular 可能な限り正確な情報を公平かつ可及的速やかに届け、 diseases)の活動が在る。ここれまでに国内において臨床 迅速かつ効率的なリクルートのフローを構築した。3)さら 試験を前提とした希少疾患の患者情報登録システムは に開発を目的とした臨床研究の計画立案のために有用 なく、日本においても TREAT-NMD との国際的な協調の な情報を提供する基盤的な臨床研究を実施した。 下、ナショナルレジストリーとして Remudy による患者情報 Remudy において現在運用しているジストロフィノパチー 登録システムを構築した。 患者情報登録システムの成功を踏まえ、ナショナルレジ 臨床研究基盤としての患者情報登録システムをジスト ストリーとしての遺伝性神経・筋疾患患者情報登録システ ロフィノパチー以外の疾患へと拡大することで、神経・筋 ムへの発展を目指し、システムの安定性・汎用性の改良 疾患のみならず他の希少疾患におけるナショナルレジス を行い、他疾患、特に希少な難治性疾患(遺伝性神経・ トリー構築のモデルとなる。 筋疾患を含む)疾患レジストリーのモデルケースを提示し た。 【研究の対象および方法】 2009 年 7 月から、神経筋疾患患者情報登録システム 【緒 言】 Remudy を構築し、遺伝解析により診断が確定したデュシ ナショナルレジストリーとしての遺伝性神経・筋疾患患 ェンヌ型筋ジストロフィーおよびベッカー型筋ジストロフィ 者情報登録システムを構築、維持、改良し、システムの ー(DMD/BMD)患者を対象とし登録を行った。本システ 安定性・汎用性の改善を図り、他の希少な難治性疾患の ムの運営は、神経筋疾患患者情報登録システム Remudy 治療法開発を促進するレジストリーのモデルケースとする 運営委員会の監督・管理の下、患者情報登録部門、遺 ことが目的である。 伝子解析部門、登録情報利用及び情報提供審査委員 遺伝性神経・筋疾患の多くは希少な難治性疾患であり、 会を設置し、公正かつ安定した運営を行った。 今後実施の可能性が高い臨床試験において組み入れ 登録の方法 条件を満たす患者は極めて少ないため、短期間で対象 患者情報登録サイト(http://www.remudy.jp)から、説明 患者をリクルートすることが困難であると予想される。研究 用のパンフレット(筋ジストロフィーと開発中の治療法の解 者・製薬企業にとっては、対象となる患者の疫学的デー 説文書)、説明文書および同意文書、遺伝子解析のため タに基づき臨床試験を計画し、実施する臨床試験の情 の書類一式を、簡単にダウンロードできるように設置した。 報を参加する患者にいち早く届けることが重要である。患 ウェブサイト、パンフレット、説明と同意の文書、登録用紙 者側からみて新しい治療の臨床試験に公平に参加でき は、ユーザー(登録希望者・協力医師他)の意見や要望 る体制が望まれる。対象となる可能性がある患者および を反映させてブラッシュアップを続けた。登録情報の正確 担当の医師に、臨床研究や標準的な医療に関する情報 性を担当医が保証し、患者本人が直接登録する手順とし **** 国立病院機構熊本再春荘病院 * 独立行政法人国立精神・神経医療研究センター ***** 国立病院機構刀根山病院 ** 熊本大学医学部附属病院 *** 東京女子医科大学 9 た。情報内容は事務局において誤りがないかチェックを 行い、必要に応じて登録者および協力医師(担当医)に 確認した上で、複数の臨床の専門家(患者情報登録部 門)および複数の遺伝子解析の専門家(遺伝子解析部 門)双方の確認を経て、個人情報と臨床および遺伝情報 を別々にサーバーに登録した。また登録者・協力医療者 からの問い合わせに対しては一定の手順を定めて適切 に実施した実施した(図 1)。 図 2. Remudy 通信の発行 情報提供は患者登録の生命線であり重点的に進 めた。ウェブサイト、e-mail ベースのニュースレター による最新情報の提供とともに、登録者・協力医 療者向けに Remudy 通信を定期的に発行した。 基盤としての臨床研究の実施 さらに開発を目的とした臨床研究の計画立案のために 有用な情報を提供する基盤的な臨床研究として、登録さ れた疫学情報を解析し、特に歩行機能に関する自然歴 とステロイド治療の効果 1)、現在の DMD 患者の体重、心 図 1. 業務手順書 新規登録、情報更新、情報発信、開示、提供の手 機能と心不全に対する治療の現状を示すデータを提示 続き、問い合わせに対する対応等の事務局にお した。二次調査として、ステロイド治療のレジュメの調査を ける標準業務手順書を作成、必要に応じて更新し、 実施している。 業務の標準化、効率化に取り組んだ。 国際協調として、TREAT-NMD Global registry として、 国際的な情報を集約し DMD/BMD の疫学情報の提供を 情報開示および提供、国際協調 行った 2) 3) 。 患者・家族・医療従事者への情報発信として、Remudy このほかに、DMD 患者の医療や療養状況の調査として、 ウェブサイトを通じて最新の医療・臨床研究の情報発信、 筋疾患センター(小牧宏文センター長)と共同で、登録者 e-mail「Remudy ニュースレター」による情報提供、紙媒体 を対象に日本語版 CARE-NMD サーベイを実施した 「Remudy 通信」(図 2)を定期的な発行を継続して行うこ (図 3)。 ととした。患者・家族と研究者・製薬企業との橋渡しとして、 国立保健医療科学院政策技術評価研究部 佐藤元部 研究者・開発企業等からの情報開示依頼、および臨床 長との共同研究(武田伸一トランスレーショナル・メディカ 研究参加者のリクルートに関する登録社への情報提供 ルセンター長が分担研究者)として、「国民・患者への臨 依頼に応じて、登録情報利用及ひ情報提供審査委員会 床研究・治験に関する情報利用実態とニーズ調査」を での審議・承認を経たうえで、個人情報は秘匿した形で Remudy 患者情報登録者に対し、2013 年 3 月~4 月に 登録情報を開示および提供を行うこととした。情報開示、 かけて実施した。 情報提供は TREAT-NMD Global registry の一員として、 TREAT-NMD 事務局を通じて依頼されるケースが主とな ることが想定された。また NCNP、Remudy への直接の依 頼にも対応できるように手順を整備した。 10 ぼ 1〜2 ヶ月の間に解析結果を依頼者に通知できた(分 担研究者 西野一三の項を参照)。診断の内訳は、DMD は 80.3%(873)、BMD は 17.2%(187)、IBM(中間型)は 2.5%(27)であり(図8)、年齢の内訳は、6 歳以上 16 歳未 満が 513 人で(DMD 451, BMD57, IMD 5)全体の 47% であった(図 9)。2013 年 7 月末現在の、診断別の運動 機能、ステロイド使用、歩行可能な患者のステロイド使用 を示した(図 10)。DMD におけるステロイド使用の割合は、 歩行可能な患者に限ってみても 49%(現在使用中:48%、 過去に使用:1%)であった。心機能および使用薬剤、呼 吸機能、遺伝子変異の内訳についても示した(図 11, 12)。 これらのデータはウェブサイトで登録者や医療従事者、 国民(一般の閲覧者)に向けて公開し、療養や医療を受 図 3. 臨床試験へのリクルートに関する情報提供 筋ジストロフィー臨床試験ネットワークと協働した ける際、また診療の情報として利用されると同時に、臨床 情報提供から電話対応、患者紹介、臨床試験へ 研究の計画の参考になる情報として利用された。 の参加者の組み入れまでのフローを示す。 1400 ウェブ登録システムの開発と難治な希少疾患への応用 Remudy で運用中の DMD/BMD 登録システムの改良 1200 月別数 1000 総数 1,226 800 を進め、個人情報の保護を担保しつつ国際標準となって 600 いるウェブ登録のシステムの構築を計画した。これにより、 400 新たな疾患への応用が可能なシステムの維持・運用・汎 200 用性を改善、遺伝性神経・筋疾患を含む難治性の希少 0 疾患レジストリーのモデルケースの提示を行うこととした。 【結 果】 2009 年 7 月〜2014 年 12 月末までで、1,226 名の 図 4. DMD/BMD ナショナルレジストリーの登録依頼者数 DMD/BMD 患者から登録受付を行った(図 4)。 の推移 登録情報は定められた手順(事務局による確認と登録 2009 年 7 月〜2013 年 12 月の間に、1,226 名から 者・協力医師への照会、臨床の専門家(患者情報登録 登録依頼を受けた。 部門)および遺伝子解析の専門家(遺伝子解析部門)に よるキュレーション、個人情報と臨床および遺伝情報を独 立したサーバーに登録する)を遵守して行われた。さらに、 年に一回の情報更新も月毎に登録者に対してお知らせ し、新規登録と同様の手順を踏んで行われた。登録手続 きは後述する情報発信、開示、提供の手続き、問い合わ せに対する対応等とあわせて、標準業務手順書を整備し た(図 1)。全国の医師(298 名、187 施設)の協力を得(図 5)、2013 年 10 月現在の県別の人口 10 万人あたりの登 録依頼者数を示した(図 6)。最も多いのは秋田県で 2.16、 次に多いのは熊本県で 2.10 であった。また最も少ないの は高知県で 0.13、次に少ないのが北海道で 0.18 であっ 図 5. 県別の DMD/BMD ナショナルレジストリー登録の た。 協力医師・施設数 さらに遺伝子解析部門の解析実数は 335 件(2009 年 2009 年 7 月〜2013 年 12 月の期間に、協力医師 7 月〜2014 年 12 月末)であった(図 7)。解析依頼からほ は 298 名、協力施設は 187 施設であった。 11 2.40 2012.1.18 2012.11.9 2013.10.31 2.00 1.60 1.20 0.80 0.40 0.00 図 6. 県別の人口10万人あたりの登録依頼者数。 250 200 デュシェンヌ型 150 ベッカー型 中間型 図 7.遺伝子解析依頼件数の累計(2009 年 7 月〜2013 年 10 月) 100 解析依頼からほぼ1〜2ヶ月の間に解析結果を依 頼者に通知できている。 27 2.5% 50 187 17.2% デュシェンヌ型 873 80.3% ベッカー型 0 中間型 図 8.臨床診断の内訳 図 9. 登録者の年齢の分布 12 図 10. 診断別の運動機能とステロイド使用(ウェブサイトからダウンロード可能) DMD の登録者では歩行可能な割合が 40.7%であり、特に歩行可能な DMD 患者の半数はステロイド治療を 受けていない。 図 11. 心機能および使用薬剤、呼吸機能(ウェブサイトからダウンロード可能) 心機能が低下している割合は、DMD で 34.0%、BMD で 28.0%だった。使用されている薬剤は ACE 阻害剤、 β ブロッカーの順に多かった。DMD の 24%は呼吸器の使用し、内訳は、鼻マスクが 20%、気管切開が 4%で あった。 13 図 12. 遺伝子変異の内訳(ウェブサイトからダウンロード可能) 遺伝子変異の内訳は、DMD で欠失 53.8%、重複 13.5%、微小変異 27.4%、BMD で欠失 73.8%、重複 7.1%、 微小変異 28%であった。欠失ではエクソン 45-55 にホットスポットがみられた。 患者・家族・医療従事者への情報発信として、Remudy ウェブサイトを通じて最新の医療・臨床研究の情報発信 Enquiry Global Enquiry Local Recruit Global Recruit Local (お知らせ欄、週に 2−3 回の更新)、e-mail「Remudy ニュ ースレター」による情報提供(月に 2−3 回)、紙媒体 「Remudy 通信」を定期的な発行(年に 3−4 回)を継続し 2 て行った(図 2)。あわせて、筋ジストロフィー研究班にお ける市民公開講座や日本筋ジストロフィー協会等の患者 支援団体他の講演会においても情報発信と患者情報登 録の周知に努めた。 4 1 研究者・開発企業の依頼を受け、登録情報利用及び 情報提供審査委員会での審議・承認を経たうえで、実施 3 した情報開示は累計で 11 件だった(図 13)。内訳は、 2010 年には 4 件だったが、2011 年は 1 件、2012 年は 0 1 2 件、2013 年は 6 件であった。2013 年には、研究者・開発 企業の依頼を受け、初めて臨床試験へのリクルートに関 する情報提供が実施された(2 件)。情報提供は、登録情 報利用及ひ情報提供審査委員会での審議・承認を経た 図 13. 登録情報の開示および情報提供の内訳 うえで、登録情報を参照し臨床試験の対象となる可能性 TREAT-NMD を介した情報開示依頼が最も多く、 がある登録者向けに郵便で通知した(図 3)。秘密保持契 直接 Remudy に依頼があったものが5件であっ 約が存在するために詳細は公表できないが、約 1 週間で た。2013 年に、リクルートに関する情報提供を実 予定組み入れ数にほぼ到達する問い合わせが、筋ジスト 施した。 14 ロフィー臨床試験ネットワーク事務局に寄せられた。 の地域でも同様な調査が実施されるようになった。 国 際 協 調 と し て 、 TREAT-NMD Global Database また国立保健医療科学院政策技術評価研究部 佐藤 Committee (TGDOC)ミーティングに代表者が参加し日本 元部長との共同研究(武田伸一トランスレーショナル・メ の現状を報告した。キュレーターミーティングにもキュレ ディカルセンター長が分担研究者)として実施された、 ーター候補者のトレーニングを兼ねて日本からの参加を 「国民・患者への臨床研究・治験に関する情報利用実態 促し、毎回異なる臨床・遺伝の専門家が数名ずつ参加し とニーズ調査」は登録者(DMD/BMD, GNE ミオパチー) た。また 2013 年に日本における DMD/BMD レジストリー に対し、2013 年 3 月~4 月にかけて実施した。これは保 の現状を報告 2)、さらに DMD の特に歩行機能に関する 健医療科学院が運用する臨床研究・治験の情報提供を 自然歴とステロイド治療の効果について報告した 。これ 行うポータルサイトの改良を目指したものであり、Remudy は、これまでに公表されている DMD を対象とした臨床研 登録者や登録に協力している医療者にとって、日本語で 究の中で世界最大規模の横断的観察研究であり、ステロ 最新の臨床研究・治験の情報を得ることが出来ることは イド使用群(245 人)は、ステロイド未使用群(315 人)と比 大変有益である。現在、結果は保健医療科学院にて解 較して、歩行可能期間が 11 か月延長していた。また 析中であり、これをまって登録者・協力者に対してもフィ TREAT-NMD Global registry に個人情報を秘匿した形で ードバックを行う予定である。 1) 情報を提供し、これを集約した DMD/BMD の疫学情報 2013 年より、国際的な疾患レジストリーへの対応と幅 の報告に貢献した 3)。ステロイド治療のレジュメに関して 広い様々な疾患への応用と、入力ミスやデータエラーの は、協力医療者からの問い合わせを受けて、Remudy 登 リスクを削減し、効率的な登録手続きを実現するために、 録者に対する二次調査の形で実施している。 最新の技術を導入したウェブ登録システムの開発を行っ 患者の医療や療養状況の調査として、筋疾患センタ た。特に NCNP の大石秀雄情報管理室長および永井秀 ー(小牧宏文センター長)と共同で実施した日本語版 明顧問の指導の下、日立ソリューションズが有する日本 CARE-NMD family survey(図 14)は、ヨーロッパを中心 独自の匿名化技術を応用したシステムを整備しテスト運 に行われている DMD 患者・家族向けの調査を日本語化 用を行った(図 15)。 したものであり、これ自体が医療・ケアの標準化を目指し 国際協調として、2011 年〜2013 年に 3 回の TGDOC た情報提供でもあった。集計された結果の一部は、2013 annual meeting での各国の状況を受け、特に筋強直性ジ 年 4 月 18-19 日(Budapest)と 2013 年 10 月 29 日 ストロフィー、dyferlinopathy、GNE ミオパチーなどのレジ (Newcastle)で行われた CARE-NMD カンファレンスにお ストリーに関する国内の専門家・患者団体間での意見調 いて報告された。現在、ドイツの Dr. Janbernd Kirschner が 整を行った。特に、筋強直性ジストロフィーに関しては、 総括報告を出版準備中である。本邦のデータをヨーロッ 大阪大学神経内科 高橋正紀助教、国立病院機構刀根 パのものと比較検討し、個々の診療・ケアにフィードバッ 山病院神経内科 松村剛部長、国立病院機構青森病院 クされることが期待されている。ヨーロッパ以外の地域で 髙田博仁副院長ら国内のオピニオンリーダーと協調して、 は、日本での調査がはじめてであり、この後に世界の他 臨床研究の一環としてレジストリー構築を準備した。 図 14.日本語版 CARE-NMD family survey ヨーロッパを中心に行われてい る DMD 患者・家族向けの調査 を日本語化したもの、これ自体 が医療・ケアの標準化を目指し た情報提供である。調査はヨー ロッパと同じ内容であり、データ を比較検討できるように設定さ れた。図には、患者さんの暮ら し方、患者年齢別の家族会入 会状況を示した。 15 を取り扱うシステムが整っている、④ 十分なインフォーム ドコンセントが行われる、⑤ すべての患者が公平に臨床 試験の情報を得られる、⑥ すべての研究者・治験依頼 者が公平に利用できる、⑦ 情報の出力に関して明確な 手続きがある、⑧ 検体の研究利用に関して厳格な規則 がある、⑨ グローバルレジストリーと連結可能である、⑩ 継続した運営が保証される、を厳守して運営していること が、3 年間の成功の基本となった(図 16)。特に重点を置 いて進めてきた②、⑤、⑥、⑦、⑨にとどまらず、次期の 研究では⑧ 検体の研究利用、⑩ 継続した運営、につ いて具体的な成果を挙げるための体制作りが重要である。 希少疾患の疫学研究の側面を持つレジストリーでは、対 象疾患の患者数を推定することは極めて重要である。秋 田県・熊本県の人口 10 万人あたりの登録依頼者数のデ 図 15. 現在公開準備中ウェブ登録システムの患者登録 ータ(図 6)および登録された診断の内訳(図 8)から逆算 画面 し、国内の DMD の登録患者数の見込みは約 2,500 人で 日本独自の匿名化技術を応用し、個人情報に ある。比較的年齢が高くまた遺伝子診断を受けていない 対するセキュリティーとユーザー(登録者、協力 DMD 患者は登録の条件を満たさない、もしくは患者登 医師、キュレーター)に対してフレンドリーなシス 録への参加に積極的でないケースが多いと推測されて テムを準備中である。 いる。このことを勘案すると、川井による DMD 患者数の 推定:約 3,500 人(分担 川井充の項を参照)が妥当であ ることを示唆した。さらに周知活動を続け地域差をできる 【考 察】 だけ少なくすることは、疫学研究の面からも重要だと考え 遺伝性神経・筋疾患の臨床研究の推進を目的とする られた。 疾患レジストリーの構築、および改良を行いつつ安定し た運営を継続した。また、設立当初の目的である 1)臨床 日本版 CARE-NMD サーベイ、国民・患者への臨床研 研究の計画及び実施の際に対象となる疾患の疫学デー 究・治験に関する情報利用実態とニーズ調査と、一連の タを供与し、2)参加条件に合致する可能性がある登録者 Remudy 登録者を対象とする研究を受け入れ実施するこ へ可能な限り正確な情報を公平かつ可及的速やかに届 とにより登録事務局の機能が活性化され、新規の研究や け、迅速かつ効率的なリクルートのフローを構築し、実施 事業に対する柔軟な受け入れ体制が徐々に確立されつ することができた。3)さらに開発を目的とした臨床研究の つある点は特筆すべき効果である。これをうけて、ステロ 計画立案のために有用な情報を提供する基盤的な臨床 イド治療のレジュメに関する二次調査は極めて順調に進 研究として成果を提示し、さらに現在も有用なデータを準 行している。 備中である。3 年間の研究としては目標以上に十分な成 Remudy の患者情報登録システムとしての成功を元に、 果を上げることができており成功したと考えている。今後 希少な遺伝性神経・筋疾患のナショナルレジストリーの構 も、この三点は継続して実施することが極めて重要である。 築へつなげていくことが重要である。このために、システ 成功の要因として、研究班全体の協力体制だけでなく日 ムの安定性・汎用性の改良が急務であった。ウェブを用 本全国の患者・家族、協力医療機関の医師、日本筋ジス いた登録システムはほとんどの国で実施されており国際 トロフィー協会の理解と協力は極めて大きく、また筋ジスト 的な標準となっている。その中で、今回の研究の成果の ロフィー臨床試験ネットワーク(NCNP 病院 小牧宏文事 一部として提案する日立ソリューションズが有する日本独 務局長)との協働体制は重要で、特に臨床試験へのリク 自の匿名化技術を応用したシステムは、個人情報部分と ルートに関する情報提供の実現には、不可欠の要素で 臨床情報部分を分けて管理するサーバーシステムと連 あったと考えている。また、前主任研究者である国立病 動させることで、個人情報の保護を担保するセキュリティ 院機構東埼玉病院 川井充院長によるナショナルレジス ーの面で優れた環境を提示することが想定されている。 トリーの 10 箇条:① 正確な遺伝情報と臨床情報が含ま ウェブシステムが提供する環境によって、患者自身による れる、② 臨床情報は常に更新されている、③ 個人情報 登録方法の改良、これをサポートする医師・医療従事者 16 1 正確な遺伝情報と臨床情報が含まれる 5 10 継続した運営が保証される 2 4 臨床情報は常に更新されている 3 9 グローバルレジストリーと連結可能であ 3 2 る 個人情報を取り扱うシステムが整ってい る 1 0 8 検体の研究利用に関して厳格な規則があ 4 十分なインフォームドコンセントが行わ る 7 れる 5 情報の出力に関して明確な手続きがある 6 すべての患者が公平に臨床試験の情報を 得られる すべての研究者・治験依頼者が公平に利 用できる 図 16. Remudy DMD/BMD 患者情報登録の自己評価 日本独自の匿名化技術を応用し、個人情報に対するセキュリティーとユーザー(登録者、協力医師、キュレーター) に対してフレンドリーなシステムを準備中である。 の負担が軽減され、かつ患者情報登録センターの業務 【謝 辞】 の標準化・登録手順の効率化、正確性の向上が期待さ 登録に協力いただいた患者・家族、医療従事者、筋ジ れる。これは他疾患への応用を踏まえた提案であり、希 ストロフィー協会はじめ患者支援団体の方々、臨床・遺伝 少疾患レジストリー構築のモデルを提示することができた。 子キュレーター、登録事務局のメンバーに深謝する。 このレジストリーは、臨床研究の推進を明確な目的として おり、臨床研究への参加を希望する患者が主体的に登 倫理委員会における承認結果等倫理面への配慮 録する仕組みが鍵である。すなわち、現在進められてい 患者情報登録システムの構築と遺伝子検査実施体制に る難病改革の中核となる特定疾患登録システムの仕組 関しては、独立行政法人国立精神・神経医療研究センタ みの中でピットフォールとなりえる軽症者のデータを補完 ー倫理委員会の承認を得て実施した。 する可能性を示しており、将来的には特定疾患登録シス テムの改良に貢献できる方向性を提示するものであると 利益相反自己申告書の提出 有 考えている。さらに、この「患者自身の意志」によって主体 利益相反審査結果 利益相反なし 的に登録するシステムは研究者と患者の間の双方向性 の橋渡しを指向しており、将来臨床研究のアウトカムとな 【研究業績】 る可能性がある”patient oriented outcome”についての基 1) Takeuchi F, Yonemoto N, Nakamura H, Shimizu R, 礎データの収集や、その評価・検討につながっていく可 Komaki H, Mori-Yoshimura M, Hayashi YK, Nishino I, 能性を有している点も重要である。以上のことから、 Kawai M, Kimura E, Takeda S. Prednisolone improves Remudy が提示するモデルは希少な難治性疾患全体を walking in Japanese Duchenne muscular dystrophy カバーするシステムの構築に寄与する可能性を提示する patients. Journal of neurology. 260(12):3023-9, 2013. ことができた。今後、国際的な動向を踏まえつつこれと協 2) Nakamura H, Kimura E, Mori-Yoshimura M, Komaki 調し、希少な難治性疾患全体にこのモデルを拡大するた H, Matsuda Y, Goto K, Hayashi YK, Nishino I, Takeda めに、新しい研究体制を準備し、各疾患の研究グループ、 SI, Kawai M. Characteristics of Japanese Duchenne and これを支援する橋渡し研究を進める研究グループ、患者 Becker muscular dystrophy patients in a novel Japanese 支援団体、製薬業界団体、厚生労働省等に、積極的な national registry of muscular dystrophy (Remudy). 働きかけを行い、新しい臨床研究基盤・臨床研究体制の Orphanet journal of rare diseases. 8(1):60, 2013. 構築の実現を目指したい。 3) Bladen CL, Rafferty K, Straub V, Monges S, Moresco A, Dawkins H, Roy A, Chamova T, Guergueltcheva V, 17 Korngut L, Campbell C, Dai Y, Barisic N, Kos T, Brabec P, Rahbek J, Lahdetie J, Tuffery-Giraud S, Claustres M, Leturcq F, Ben Yaou R, Walter MC, Schreiber O, Karcagi V, Herczegfalvi A, Viswanathan V, Bayat F, de la Caridad Guerrero Sarmiento I, Ambrosini A, Ceradini F, Kimura E, van den Bergen JC, Rodrigues M, Roxburgh R, Lusakowska A, Oliveira J, Santos R, Neagu E, Butoianu N, Artemieva S, Rasic VM, Posada M, Palau F, Lindvall B, Bloetzer C, Karaduman A, Topaloglu H, Inal S, Oflazer P, Stringer A, Shatillo AV, Martin AS, Peay H, Flanigan KM, Salgado D, von Rekowski B, Lynn S, Heslop E, Gainotti S, Taruscio D, Kirschner J, Verschuuren J, Bushby K, Beroud C, Lochmuller H. The TREAT-NMD Duchenne muscular dystrophy registries: conception, design, and utilization by industry and academia. Human mutation. 34(11):1449-57, 2013. 18 Ⅱ. Remudy の周知活動 中 国 ・四 国 地 区 の筋 ジストロフィー患 者 データベース登 録 の促 進 活 動 ~とくに中 国 四 国 政 策 医 療 神 経 筋 ネットワーク協 議 会 の活 動 から ~ 足 立 克 仁 * 研究協力者 柏木 節子*, 齋藤 美穂*, 橋口 修二*, 宮﨑 達志*, 東田 栄子*, 河野 Ⅰ.四国地区の登録促進活動:徳島病院の Duchenne 誠*, 川井 尚臣*, 2. 平成 24 年 10 月 1 日〜25 年 9 月 30 日の 1 年間の /Becker 型患者を中心に 当院入院・外来の各種筋ジストロフィー患者は 158 例 であり、そのうち Duchenne 型患者は 60 例(MLPA 検 【目 的】 索 48 例、Remudy 登録完了例 11 例)で、Becker 型 Duchenne/Becker 型筋ジストロフィー患者の登録システ 患者は 19 例(MLPA 検索 9 例、Remudy 登録完了例 ム(Remudy)の構築は、現在行われている本症治療薬 5 例)であった。 (エクソンスキップ療法)の治験への参加には欠かせない。 当院は、これまで四国で唯一の筋ジストロフィー専門 施設として運営してきた歴史 1) を踏まえ、四国の本症患 者において、待望の本症治療薬の治験参加を推進して いくことが求められている。 【方 法】 当院入院・外来の各種筋ジストロフィー患者を詳細に 調べた。 とくに Duchenne/Becker 型についてはジストロフィン遺 伝子検索(MLPA 法)の施行の有無を調べ、Remudy 登 録完了例を数えた。さらに出身地分布も調査した。 また、Remudy の周知活動についても記載した。 【結 果】 3. 出身地分布は、徳島県、香川県が最も多く、愛媛、高 1. 平成 25 年 5 月現在、当院入院 Duchenne 型患者は 知と続いた。また、四国周辺の広島(6 例)、岡山(5 38 例(18~40 歳、平均 28.5 歳)であった。 例)、兵庫(2 例)、和歌山(2 例)にもみられた。 * 国立病院機構徳島病院 四国神経筋センター 21 4. Remudy 周知活動: は広島西医療センターと松江医療センターである。 1) 研究会等;①徳島神経難病セミナー(徳島県青少 24 年度は広島西医療センターで開催された神経・筋 年センター、平成 25 年 1 月 20 日、全ての医療関 疾患ネットワーク協議会/平成 24 年度中国四国ブロック 係者向け)②平成 25 年度筋ジストロフィー研修会 会議に出席して、各神経内科医・小児科医に Remudy 登 (当院、7 月 26 日、患者家族向け)③徳島神経疾患 録促進をお願いした。 症例研究会(当院、平成 25 年 4 月 25 日、医師会 25 年度は松江医療センターで開催された神経・筋疾 向け)④徳島大学医学部臨床実習(当院、平成 25 患ネットワーク協議会/平成 25 年度中国四国ブロック会 年度、医学生向け)⑤NHO 東徳島 MC 看護学校講 議に出席して、各神経内科医・小児科医に Remudy 登録 義(平成 25 年 10 月 7 日、看護学生向け)⑥徳島県 促進をお願いし、さらに、今回は Remudy についてのア 難病拠点病院報告会(県保健福祉部長室、平成 25 ンケート調査(本研究班園田班員作成)を行った。 年 5 月 13 日、県庁向け) 2) 刊行物;①治療薬、始まる治験(毎日新聞、四国版、 平成 25 年 7 月 26 日)②投句募集(当院俳句集、平 成 25 年 6 月 10 日) 以上、機会あるごとに Remudy についての周知活動を 行った。 【考 察】 当院入院の Duchenne 型患者は高齢化が進んでいた。 当院入院・外来の Duchenne/Becker 型患者について、そ の出身地分布は徳島県、香川県に多いが四国周辺県か らもみられた。 また、ジストロフィン遺伝子検索(MLPA 法)の施行の 有無も調べ、Remudy 登録に役立てた。 【結 果】 今回の Remudy 周知活動のための研究会等では、各 1. 筋ジストロフィー専門施設である松江医療、広島西医 種医療関係者に最新情報を提供した。 療と徳島病院の 3 名の小児科医については、 さらに当院で編集している俳句集(Remudy の記事を Remudy 登録は診療科の方針として推進が2名、主治 掲載)への投句も募り、その作品はその俳句集に掲載し 医の判断が 1 名であった。また、登録の説明は、質問 た。これにより本症患者の社会的活動の活発化ならびに、 があれば説明が 2 名、経過中に説明が 1 名であった。 さらなる Remudy の周知が図れるものと思われた。 2. 8 施設の神経内科医の Remudy 登録の説明は、診療 Remudy 登録完了例はまだまだ少ないが、今後も続け 中の本症患者数が少ないこともあり、少なかった。 て登録活動を行いたい。 【考 察】 筋ジストロフィー専門施設の小児科医は全て Remudy Ⅱ.中国地区の登録促進活動:中国四国神経筋ネットワ 登録の説明を行なっていた。今回のアンケート調査は、 ーク協議会の活動から 医師の Remudy 登録のさらなる認識に貢献したものと思 われた。 【目 的】 今後も機会あるごとに登録促進活動を行い、四国同様 中国四国地区の国立病院機構病院の神経内科・小児 に中国地区においても活発化させたい。 科医師が多数参加する中国四国神経筋ネットワーク協 因みに、平成 26 年度の神経・筋疾患ネットワーク協議 議会 2)に出席し活動することは Remudy 登録数の増加に 会/平成 26 年度中国四国ブロック会議は徳島病院で行う 貢献するものと思われる。 ことが決まっている。更なる登録促進活動を行いたい。 【方 法】 国立病院機構の中国地区の筋ジストロフィー専門施設 22 【全体の結論】 Duchenne/Becker 型筋ジストロフィー患者やその担当 医に Remudy の周知を図り、本症の治験を、早く、スムー スに実施させることは、中国四国の国立病院機構施設が 果たすべき重要な役割であると考えられる。 【参考文献】 1) 足立克仁:徳島病院の筋ジストロフィー患者の病型 について―開棟から 45 年間の推移―.医療 2010; 64: 143-147 2) 足立克仁、井原雄悦:集談会記事.中国四国ブロッ ク神経筋ネットワーク協議会.医療 2011; 65: 238240 23 鹿 児 島 県 内 の筋 ジストロフィー患 者 のデータベースの 構 築 に関 する研 究 園 田 至 人 * 研究協力者 内田 裕一 *, 丸田 恭子 *, 有里 敬代 * 【要 旨】 榜する医療機関及び離島の全医療機関、総数 292 機関 筋ジストロフィーへの治験/臨床試験に関しての情報 に本調査の目的を記した上でアンケートを行い筋ジストロ 発信を広く行うことを可能とする目的で鹿児島県内の医 フィーの診療の有無について一次調査を行い、鹿児島 療機関へのアンケートを行い筋ジストロフィーデータベー 県を 6 地区(、鹿児島市、北薩、薩南、姶良、大隅、離島) スの構築を試み、平成 22 年、24 年に調査、比較検討し に分類し、各地区別の筋ジス患者診療の実態調査を行 た。Duchenne 型では有病率の低下が認められた。また った。また専門医療機関(鹿児島大学病院、南九州病院) 全国調査を行い、全国の Remudy 周知の現状を調査し の受診歴も調査した。さらに筋ジストロフィー診療を行っ た。鹿児島県では Duchenne 型の有病率の低下が見られ ていると回答のあった医療機関に 2 次調査を行い①患者 た。Remudy の周知はほぼ達成されていたが、全国調査 年齢、重症度、遺伝子検査の有無、筋生検の有無、療 では依然、周知不十分の結果であった。今後も Remudy 養形態、患者登録(Remudy)の周知状況、及び参加の有 の情報発信を行い登録への協力を推進していくことが重 無について調査した。また平成 24 年にその結果を基に 要と考えられた。 Duchenne 型、Becker 型の追跡調査、さらに新たなケース を専門医療機関に問い合わせ可能な範囲で最新データ 【目 的】 を得、前回の結果と比較検討を行った。尚、有病率等の 筋ジストロフィー患者へ対する治験/臨床試験は特定 計算には平成 17 年度国勢調査の結果を用いた。 の遺伝子の異常が対象となる。それを踏まえて神経・筋 疾患患者登録(Registry of Muscular Dystrophy: Remudy) Ⅱ全国調査 が開始されている 1)。鹿児島県は,九州の南端にあり, 平成 25 年、全国の小児科・神経内科を有する医療機 総面積は 9,187 平方キロメートルで,薩摩半島,大隅半 関のうち、国立病院機構に属する医療機関 72 施設 112 島の二つの半島と多くの離島を有する。離島の一部には 診療科、大学病院・大学関連病院 138 施設 276 診療科 医師の常駐のない島も存在し、専門的な検査、医療を受 に Remudy に関して周知状況に関してアンケート調査を けることが出来ない患者も存在する。全てのケースで治 行った。 験/臨床試験に公平な参加を可能とする目的で鹿児島 県内の筋ジストロフィー患者データベースの構築を試み 【結 果】 た。平成 22 年、24 年に調査を実施し、その結果を基に Ⅰ.鹿児島県データベースに関して 更に継続性のあるデータベースの構築方法を検討した。 1. 病型別調査結果 Duchenne 型へ平成 22 年 45 例、年齢 21.3±10.9 歳 1)2)3) また平成 25 年には全国の Remudy の周知状況を調査 (Mean±SD)であったが(図 1)、24 年は 39 例、年齢 する目的で全国の医療機関へのアンケート調査を実施し 28.7±11.2 歳であった。人口 10 万人あたりの有病率は 22 た。 年で 2.31 であった。過去の報告より、平成元年 2.75、22 年 2.57 と年々減少する傾向が認められた(図 2)2)。患者 【方 法】 数減少の原因は 6 例ともに死亡であった。死亡時の年齢 Ⅰ.鹿児島県データベースの構築 は 28.7±11.2 歳(Mean±SD)で、最年少 14 歳、最年長 44 平成 22 年、鹿児島県内の「神経内科」「小児科」を標 * 国立病院機構南九州病院 歳であり全例心不全が死因であった。疾患別年齢分布 ≪ Key Words ≫ 鹿児島県 Kagoshima prefecture 筋ジストロフィー muscular dystrophy データベース GNE ミオパチー GNE myopathy 神経筋疾患患者登録 25 data base Registry of Muscular Dystrophy では年齢は, 22 年の 11 例は 24 年も異動はなかった。24 受診歴のない患者数は Duchenne 型、及び先天性筋ジス 年の年齢は 34.4±15.4 歳であり、年齢に伴い、運動機能、 トロフィーでは 1 例も見られなかった。その他のタイプで 呼吸機能、嚥下機能も悪化する傾向にあったが、症例毎 は Becker 型 4 例(36%)、FSH1 例(20%)、LG3 例 で大きな差を認めた。遺伝子検査は 11 例中、7 例で未 (38%)、MyD16 例(70%)、SMA 3 例(19%)であった。 施行であったが、一方筋生検は 7 例で施行済であり、確 Ⅱ.全国調査 定診断のための生検を積極的になされていると考えられ 国立病院機構に属する医療機関 112 診療科、及び大 た 。 そ の 他 の 型 で は 22 年 の 統 計 で 肢 帯 型 (LG) 学病院・大学関連病院 276 診療科、合計 388 診療科通、 55.0±21.3. 顔面肩甲上腕(FSH) 48.0±10.4, 筋強直性ジ 319 診療科よりアンケートを回収した(回収率 84.8%)。そ ストロフィー (MyD) 55±13.7 , 脊髄性筋委縮症(SMA) の内、DMD, BMD, あるいは GNE ミオパチーを診療中 35.8±25.7 先天性筋ジストロフィー22.7±12.5 歳であった。 の慰労機関は国立病院機関に属する医療機関 32 診療 科、大学病院・大学関連病院 73 診療科に上った。それ 診療中の医療機関 73 診療科からのアンケートより以下の 結果を得た。 1. Remudy 登録の方針 Remudy 登録に関して診療科として方針を持っている との回答が約 3 割で大半は主治医の判断に任せている と回答された(図 3)。 図 1. 症例全体(平成 22 年調査) LG :肢帯型筋ジストロフィー、 FSH :顔面肩甲上腕型筋ジストロフィー、 MyD :筋強直性ジストロフィー、 CMD :先天性筋ジストロフィー、 SMA :脊髄性筋萎縮症 図 3. Remudy 登録に関して 多くの施設が主治医の判断に任せている。 2.周知状況・説明時期 Remudy の周知状況は 50%以上、周知されているとの 回答が全体で 57%であり、国立病院機構で周知されてい る割合が高かった。一方、ほぼ 0%であるとの回答が全体 で 35%、大学関連では 38%と依然、Remudy の周知率が 低い現実が見られた(図 4)。 図 2.Duchenne 型年齢分布 2.地区別有病率 地区別の 10 万人当たりの有病率は Duchenne 型は姶 良地区で 4.19 と他の地区(1.14-2.86)と比較すると非常 に高かった。同様に脊髄性筋萎縮症も姶良地区 2.79(他 の地区:0-1.35)も高かった。鹿児島県全体の有病率は Duchenne 型で 2.17 人であった。 図 4. Remudy 周知状況 3. 専門医療機関への受診歴の有無 ほとんど周知されていないとの回答が 3 割以上を占める。 専門医療機関(鹿児島大学あるいは南九州病院)への 26 Remudy の説明時期は約 1 割では初診時、また約半数 挙げられる。鹿児島県内の神経内科、小児科の中核病 は経過中と回答された。一方、積極的に説明しない(質 院に協力を依頼し、新たに筋疾患を有する患者が受診し 問時に説明、特に行わない)との回答も 4 割に上った。説 た際に連絡できる体制を作っていくことが必要と考えられ 明内容は Remudy の存在、遺伝子検査の必要性、登録 る。 の意義、ホームページの存在等がほぼ同じ割合であった 1. 年齢構成及び鹿児島県内の患者分布に関して 現在 Duchenne 型の平均寿命は呼吸管理、心不全へ (図 5)。 の対応によって 30 歳を超えるまでに達した 2)。今回の検 討でも平均年齢 21.3±10.9 歳と過去の鹿児島県の報告と 比較すると高齢化している 3)。福永らは平成元年の統計 として有病率を 10 万人あたり 2.75 と報告し、有病率の低 下を指摘したが 3)、今回さらに 2.17 と低下を見た。年齢 層別では 10 歳未満の患者数が少なく、新たな発症数が 減少していることが明らかである(図 4)。これは出生率の 低下、遺伝カウンセリング等の普及によるところが多いと 考えられるが、その他社会的要因もあろうかと考えられる。 図 5. Remudy 説明の内容 患者分布の特徴は Duchenne 型、脊髄性筋萎縮症が姶 良地区に多いことがあげられるが、南九州病院がその地 区に存在しているためと考えられた。 GNE ミオパチーの登録は全体で 45%(大学関連 48%、 2. 専門医療機関への受診歴に関して NHO で 35%が認知していないとの回答であった(図 6)。 小児科の施設も入っているため低い周知状況と推定され Duchenne 型、先天性筋ジストロフィーは家族も情報を 積極的に得ようとしているため、全例専門医療機関の受 る。 診歴があるものと考えられた。また筋強直性ジストロフィ ーでは受診歴があるケースが少なかったがこれは疾患の 重症度が低い等の要因があると考えた。一方、地方、離 島に居住する患者は専門医療を受ける事が困難である ケースも多い。今後検討すべき課題と考えられた。 3. 療養形態に関して 以前の報告では Duchenne 型は 10 代より入院生活を 送っていたケースが多数を占めていたが、今回の検討で は NIPPV を導入しながらも在宅療養を行っているケース 図 6. GNE ミオパチーの周知状況 も見られた。これは特別支援学校等の対応の変化や、障 害者自立支援等の法的整備、その他、生活環境の変化 が要因となっていると考えた。 【考 察】 Ⅰ.鹿児島県データベースに関して Ⅱ.全国調査に関して データベース構築上の問題点として、①年々変化する 実に 26%の診療科が Remudy の存在を知らないとの ため、データの老朽化が早い。 ②個人情報を含み、取 回答であったが、内容を見ると、ごく少数例(Becker1 例や 扱いに細心の注意が必要。また自由登録であるため、完 Dchenne1 例)を診療している科がその大部分であり、そ 全なデータを得るのは困難である。③疾患タイプによっ の観点では Remudy を全く知らない筋ジス患者数は少な ては専門医療機関を受診しないケースもあり得る。特に いと考えられる。しかし、Remudy が広く平等に治験の機 筋強直性ジストロフィー、Becker の軽症例等。④他県の 会を全患者へ与えるための登録であると考えると 医療機関を受診しているケースは困難。鹿児島県の例で Remudy 周知の努力、情報発信が今後も重要になると考 は、熊本大学発達小児科や神戸大学④拠点病院の人 えられる。 事異動があった場合に継続性が確保できるか。⑤筋ジス トロフィーの専門病院のない県、多数の大病院を有する 【結 語】 首都圏等で漏れなく患者情報を得ることが可能か?等が 1. 27 鹿児島県内の筋ジストロフィー患者の診療状況をア ンケートにより調査した。 1. Duchenne 型では有病率が過去の報告と比較し低下 が見られた。種々の原因が考えられ今後の検討が必 要であった。 2. Remudy への登録は徐々に増加傾向ではあるが、今 回のデータベースを基に、今後情報発信を含め登 録推進の努力が必要である。 4. 治療を念頭に置いた情報発信と共に遺伝子を含め たデータベースの構築が必要と考えられた。 5. 全国的に Remudy の周知は不十分であると考えられ る。今後の周知方法の検討が必要と考えられた。 【参考文献】 1) 中村治雅:筋ジストロフィーの臨床試験実施体制構築 に関する研究 筋ジストロフィー患者登録(Remudy)の 現状報告.厚生労働省精神・神経疾患研究委託費に よる研究報告集 平成 21 年度 (2 年度班・初年度班) 2010:373 2) 多田羅勝義、神野進、藤村春俊:筋ジストロフィーデ ータベース調査-Duchenne 型筋ジストロフィー進行 例の臨床像-.厚生労働省精神・神経疾患研究委 託費 17 指-9 筋ジストロフィーの療養と自立支援のシ ステム構築に関する研究 平成 17~19 年度総括研究 報告書 2009, 322-324 3) 福永秀敏、園田至人、厚地弘子ら:Duchenne 型筋ジ ストロフィー症、その臨床像の変貌-平成元年度鹿児 島県における現況から-.日本医事新報. 1990;3440:29-31 28 秋 田 県 における筋 ジストロフィー患 者 登 録 システムへの 登録促進活動 小 林 道 雄 * 【緒 言 】 全例で Multiplex Ligatioindependent Probe Amplification 本 邦 で は2009 年 7 月 か ら Remudy(Registry of (MLPA)法が施行されていた。デュシェンヌ型 17 人のうち Muscular Dystrophy)が、ジストロフィノパチー患者の登録 複数エクソン欠失が 4 人(24%)に、単独エクソン欠失が 1 を開始している 。登録システムが有効なものになるため 人(6%)に確認され、この患者たちはすべて Remudy への には多くの患者の登録が不可欠である。私達は、平成 20 登録を済ませていた。欠失/重複の検出されなかった 12 年度~22 年度にかけて、「筋ジストロフィーの臨床試験 人のうち 6 人が小児期に筋生検を行われていたが、免疫 実施体制構築に関する研究班」の活動として、秋田県に 染色を行われている症例はなく、検体が残っている症例 おける筋疾患の現状調査や、患者登録システムについ もなかった。残る 6 人は筋生検を施行されておらず、臨床 てのアンケート調査を行いながら、医師や患者に情報発 情報のみからデュシェンヌ型と診断されていた。ベッカー 信をしてきた 型の 3 人は全例複数エクソン欠失が確認されており 2) 1) 。このためか秋田県の登録患者は周囲の 他県より比較的多い 3)。今回の平成 23 年度~25 年度の Remudy への登録も済ませていた。 「遺伝性神経・筋疾患における患者登録システムの構築 【考 察】 と遺伝子診断システムの確立に関する研究」班において MLPA 法で遺伝子変異が確認できなかった成人患者 は、秋田県でさらに登録を増やす余地がないか調査し、 が多かったが、筋生検を行われていないか、或いは行わ また東北 6 県に範囲をひろげての調査も行ったので報告 れていても免疫染色まではやられておらず、検体も残っ する。 ていないため、現在のルールでは登録が難しいようであ った。 平成 23 年度 Ⅰ. 秋田県での調査 2. 小児の登録についての調査 【目 的】 1. 成人の登録についての調査 秋田県での小児登録についてさらに増やす余地がな 【目 的】 いか検討する。 【方 法】 秋田県での成人登録についてさらに増やす余地がな いか検討する。 秋田県内の小児神経専門家が集まる研究会に参加し 【方 法】 て、「秋田県における筋ジストロフィー患者登録システム 前研究班での調査では、成人のジストロフィノパチー への登録促進活動」の演題で発表し、その場でアンケー 患者はすべてあきた病院で診療されていたため、全ジス ト調査を行った。 トロフィノパチー患者の診療録の確認, 病歴の再聴取, 【結 果】 前医への問い合わせなどを行い、遺伝子検査の結果, 医師 9 名より回答が得られた。Remudy について知っ Remudy への登録の有無, 筋生検の施行状況(免疫染色 ていた医師は 4 人(44%), Remudy のホームページをみた が行われているか、検体が残っているかも含めて)につい ことがある医師は 3 人(33%)のみであった。Remudy につ て調査した。 いて知っていた 4 人の医師が計 10 人のジストロフィノパ 【結 果】 チー患者の診療をしており、このうち 5 名の患者はすで 平成 23 年 12 月の調査時点であきた病院では、臨床 に登録され、2 名は登録手続き中で、3 名は登録対象に ならない患者であった。 診断がデュシェンヌ型の患者 17 人, ベッカー型の患者 3 人を診療していた。 * 国立病院機構あきた病院 29 【考 察】 Q3. 神経・筋疾患医学情報登録・管理機構での福山型 小児に関しては、秋田県内で現在登録可能な患者は、 先天性筋ジストロフィー(FCMD)登録をどのくらい知って いますか?という質問では、a.「聞いたことがない」が全体 ほぼ登録が済んでいるか登録手続き中のようであった。 の 69%, b.「話に聞いたことはある」24%, c.「ホームページ 【結 論】 をみたことがある」5%, d.「実際に患者が登録したことがあ 秋田県内で現在のルールで Remudy に登録できる患 る」2%であった。神経内科では a. 72%, b.22%, c. 5%, d. 者は、成人・小児とも概ね登録されていることが明らかに 1%、小児神経では a. 54%, b.33%, c.4%, d. 8%だった。県 なった。 別では、青森が a. 76%, b. 18%, c. 6%, d. 0%、岩手が a. 53%, b. 33%, c. 13%, d. 0%、宮城が a. 73%, b.22%, c. 0%, d.5%、秋田が a. 50%, b. 33%, c. 13%, d. 4%、山形が a. 平成 24 年度 85%, b. 15%, c. 0%, d. 0%、福島が a. 76%, b. 24%, c. 0%, Ⅱ. 東北 6 県での医師を対象にした調査 d. 0%であった。 Q4. この 1 年間で診療している患者数は?という質問の 【目 的】 回答を集計すると、東北 6 県での患者数の総計は DMD 東北 6 県の医師にアンケート調査をすることで、現在 127, BMD 55, DMRV 29, FCMD 32 であった。既登録例, の周知の状況などを知り、情報発信にもつなげる。 遺伝子確定・未登録例, 遺伝子未確定例の割合(%)は、 【方 法】 全症例では 16:35:49 で、疾患別では DMD 18:23:59, 東北 6 県の神経内科専門医 327 人と小児神経専門医 BMD 5:49:45, DMRV 31:41:8, FCMD 16:53:31 であった。 56 人の計 383 人に、平成 24 年 9 月に、郵送によるアン 【考 察】 ケート調査を行った。 Remudy について知らなかった医師は全体の 56%で、 【結 果】 平成 21 年度秋田県調査(93%)2)と比べて、かなり減って 全体で 127 人(神経内科 103 人, 小児神経 24 人)より きていることが明らかになった。特に小児神経専門医で 回答が得られ、回収率は 33.2%(神経内科 31.5%, 小児 は知らない医師が少なかった。県別にみると、登録につ 神経 42.9%)であった。 いての知識には地域差がみられた。 Q1. Remudy についてどのくらい知っていますか? という DMRV の登録については神経内科では DMD/BMD と 質問では、a.「聞いたことがない」が全体の 56%, b.「話に 同程度知られているが、FCMD の登録については、他よ 聞いたことはある」24%, c.「ホームページをみたことがある」 りやや知られていないようであった。 8%, d.「実際に患者が登録したことがある」13%であった。 遺伝子変異が確定していて未登録の例が全体の 35%あ 神経内科では a. 62%, b.22%, c. 6%, d. 10%、小児神経で り、まだ登録を増やす余地があると考えられた。 【結 論】 は a. 29%, b.29%, c.17%, d 25%だった。県別では、青森 が a. 41%, b. 29%, c. 18%, d. 12%、岩手が a. 60%, b. 33%, Remudy について、医師には以前よりだいぶ知られる c. 7%, d. 0%、宮城が a. 73%, b.8%, c. 5%, d.14%、秋田が ようになってきているようであるが、まだ患者登録を増や a. 21%, b. 42%, c. 13%, d. 25%、山形が a. 69%, b. 31%, c. す余地がある。 0%, d. 0%、福島が a. 67%, b. 14%, c. 5%, d. 14%であっ た。 Q2. Remudy の登録対象になると知っていたものは? と 平成 25 年度 いう質問(複数回答可)では、a. デュシェンヌ型筋ジストロ Ⅲ. 東北 6 県での患者を対象にした調査 フ ィ ー (DMD)34%, b. ベ ッ カ ー 型 筋 ジ ス ト ロ フ ィ ー (BMD)29%, c. 縁 取 り 空 胞 を 伴 う 遠 位 型 ミ オ パ チ ー 【目 的】 東北 6 県の患者にアンケート調査をすることで、現在 (DMRV)22.8%であった。神経内科では a. 26%, b.23%, c. の周知の状況などを知り、情報発信にもつなげる。 23%、小児神経では a. 67%, b. 54%, c.8%。県別では、青 森 a. 47%, b. 29%, c. 24%、岩手が a. 27%, b. 27%, c. 20%、 【方 法】 宮城が a. 22%, b.22%, c. 11%、秋田が a. 67%, b. 63%, c. 東北 6 県の DMD, BMD, DMRV, FCMD 患者を対象 46%、山形が a. 15%, b. 15%, c. 23%、福島が a. 24%, b. とした。 アンケートは以下の 3 つの方法で施行した; 1) 14%, c. 19%であった。 平成 24 年度調査で、上記 4 疾患の患者を診ていると回 30 答した東北 6 県の神経内科専門医, 小児神経専門医 40 さらなる努力が必要である。 人に、患者用のアンケートを送付し患者に配っていただ 【学会発表】 くよう依頼(275 通) 2) 日本筋ジストロフィー協会東北ブ 上記のアンケート結果などを、以下の研究会/学会で ロック大会で患者用アンケートを配布(35 通) 3) あきた 発表し、Remudy の周知に努めた。 病院の患者には聞き取り調査を施行(20 通)。 1) 第 47 回秋田県小児神経・発達研究会 【結 果】 平成 23 年 9 月 3 日, 秋田 計 64 人から回答が得られた(回収率 19%)。疾患の内 2) 第 91 回日本神経学会東北地方会 訳は、DMD 36 人(56%), BMD 13 人(20%), DMRV 7 人 平成 25 年 3 月 16 日 (11%), FCMD 8 人(13%)。性別は、男性 58 人(91%), 女 仙台 3) 第 49 回秋田県小児神経・発達研究会 性 6 人(9%)。 平成 25 年 10 月 26 日, 秋田 Q1. Remudy についてどのくらい知っていますか? という 質問では、a.「聞いたことがない」が全体の 22%, b.「話に 4) 第 67 回国立病院総合医学会 聞いたことはある」22%, c.「ホームページをみたことがある」 平成 25 年 11 月 8 日, 金沢 9%, d.「実際に登録した」47%であった。DMD では a. 19%, b.17%, c.11%, d. 53%、BMD では a. 23%, b.23%, c.0%, d. 【参考文献】 54%、DMRV では a. 29%, b. 0%, c. 14%, d. 57%だった。 1) Nakamura H, Kimura E, Mori-Yoshimura M, Komaki H, Q2. 神経・筋疾患医学情報登録・管理機構での福山型 Matsuda Y, Goto K, Hayashi YK, Nishino I, Takeda SI, 筋ジストロフィー登録をどのくらい知っていますか?という Kawai M. Characteristics of Japanese Duchenne and 質問では、a.「聞いたことがない」が全体の 45%, b.「話に Becker muscular dystrophy patients in a novel Japanese 聞いたことはある」33%, c.「ホームページをみたことがある」 national 16%, d.「実際に登録した」6%であった。FCMD では a. 0%, (Remudy).Orphanet J Rare Dis. 2013 Apr 19;8(1):60. registry of muscular dystrophy 2) 小林道雄, 阿部エリカ, 小原講二, 間宮繁夫, 菅原 b.50%, c.0%, d. 50%だった。 Q3. 患者登録についてどのようにして知りましたか?(複 正伯, 和田千鶴, 大西洋英, 豊島至:3 年間の研究 数回答可)という質問では、「医師から」 57%, 「患者会か のまとめ. 平成 20-22 年度 精神・神経疾患研究開発 ら」45%, 「インターネットで」19%, 「他の患者から」9%, 費 筋ジストロフィーの臨床試験実施体制構築に関す 「リハビリの先生から」 2%であった。 る研究 総括研究報告書 42-44, 2011 Q4. まだ登録をしていない患者について、その理由は、 3) 中村治雅, 木村円, 川井充: 治療薬開発のインフラ 「聞いたことがなかった」43%, 「登録の手間が面倒」23%, ス ト ラ ク チ ャ ー - 患 者 登 録 シ ス テ ム . BRAIN and 「自分が登録できると知らなかった」20%, 「遺伝子診断 NERVE 63(11): 1279-1284, 2011 が確定していない」17%, 「登録の必要を感じない」10% であった。 【考 察】 Remudy について知らなかった患者は全体の 22%で、 平成 21 年度秋田県調査(68%)2)と比べて、かなり減って きていることが明らかになった。患者登録についての情 報源は、平成 21 年度調査では医師からが 83%であった が、今回の調査では 57%となっており、患者会など医師 以外から情報が伝わるようになってきている。また、 Remudy のことを知ってはいても登録していない患者が 相当数おり、さらなる努力が必要と感じた。 【結 論】 Remudy について、患者にも以前よりだいぶ知られるよ うになってきている。しかし、単なる周知のみでは、登録 につながらないケースもみられ、より登録数を増やすには 31 Ⅲ. データ解析と疫学研究による情報提供 遺 伝 性 神 経 ・筋 疾 患 における臨 床 試 験 の課 題 と 患 者 登 録 データベースの活 用 に関 する研 究 米 本 直 裕 * 研究協力者 中村 治雅 ** , 竹内 芙実 ** , 鷹羽 智子 ** ンスが発表されたアダプティブデザイン(Adaptive design) 【背 景】 などにおいて適用可能性が考えられ、今後の検討が必 本研究班では遺伝性神経・筋疾患における患者登録 要であることが示唆された。 システムの構築を行っているが、患者登録データベース をより活用することにより、新しい治療薬の開発、臨床試 験のさらなる進展が期待されている。 【結 論】 患者登録データベースを解析・活用することにより、臨 【目 的】 床試験の課題を解決できる可能性がある。今後、具体的 新薬開発の臨床試験のさらなる進展、課題解決のた に疾患の開発事例を通してさらに検討していく必要があ め、患者登録データベースをどのように解析し、活用でき る。 るかを検討する。 平成 24 年度 【方 法】 データベース活用の事例として、ステロイド治療の長 平成 23 年度 期効果に関して検討を行った。Remudy に登録された 【方 法】 791 名のデータを用いて、ステロイド治療例と非治療例の 諸外国の動向を検討するため、臨床試験の学会に参 比較を行った。アウトカムは最終歩行年齢とした。 加し、EU における患者登録システムの拠点を訪問する。 また文献資料等から他の類似領域での課題、活用事例 を検討する。 【結 果】 適格対象の Duchenne Muscular Dystrophy(DMD)は 【結 果】 563 名であった。1 名はステロイド治療の情報がないため 患者登録データベースは、観察研究の 1 種であり、レ 除外し、562 名を解析対象とした。DMD のステロイド治療 ジストリ研究とも呼ばれている。登録システムは臨床試験 割合は 43.8%であった。ステロイド治療群では非治療群 への参加登録の窓口、見込み対象者数算定の資料とし に比べて、歩行可能期間が 11 か月延長していた。 て活用されている。 また、臨床試験を計画するためには、患者さんの実態、 【結 論】 疫学的な情報、治療やリスク要因の影響などに関する情 患者登録データベースは治療実態の解明、有用性の 報が不可欠であり、患者登録データベースを解析するこ 評価についても有用であることが明らかとなった。有用性 とにより、これらの情報を得ることが可能である。ただし、 の評価に関しては、治療情報の詳細(用量、治療開始日、 選択バイアス、情報バイアス、交絡といったバイアスによ 終了日)、安全性に関する情報が必要であるが、これら る結果への影響が存在するため、バイアスの調整が必要 の情報はデータベースになく、その限界も明らかになっ である。 た。今後どのように追加情報を取集すべきかなどについ さらに早期探索試験の実施において、患者登録デー て検討が必要である。 タベースを活用できる可能性がある。近年注目を浴びて おり、2010 年に米国食品医薬品安全局 FDA からガイダ *独立行政法人国立精神・神経医療研究センター トランスレーショナルメディカルセンター **独立行政法人国立精神・神経医療研究センター 35 平成 25 年度 【方 法】 データベース活用の事例として、Duchenne Muscular Dystrophy ( DMD ) 児 の 体 重 に 関 し て 検 討 を 行 う 。 Remudy に登録されたデータを用いて、年齢別の体重を 集計し、健常児の成長曲線との比較をおこなった。 【結 果】 解析対象の DMD 児は 459 名であった。成長曲線の 年齢別の標準体重に対する、DMD 児の体重は、どの年 齢層でも健常児体重の 10 パーセンタイル未満の児が 20%以上みられた。年齢別 6 歳以降では、高低のばらつ きが大きく、年齢が高いほうがよりばらつきが大きかった。 【参考文献】 (図 1) 1. FDA guidance: Adaptive Design Clinical Trials for Drugs and Biologics (http://www.fda.gov/drugs/guidancecomplianceregul atoryinformation/guidances/ucm064981.htm) 2. Takeuchi F, Yonemoto N, Nakamura H, et al. Prednisolone improves walking in Japanese Duchenne muscular dystrophy patients. Journal of neurology. 260(12):3023-9, 2013. 【結 論】 患者登録データベースを用いて、日本における DMD 児の体重の実態を明らかにした。先行研究(図 2)の中で も、本研究は最大規模であり、患者登録データベースの 有益性が示された。栄養管理にさらに役立てるためには、 DMD 児の成長曲線の作成が必要であろう。しかし、実際 の個人の成長を示すためには、同一児による体重の年 齢推移、経時的なデータが必要である。またさらに体重 だけでなく、身長や栄養摂取に関する情報も必要であろ う。これらの情報はデータベースになく、その限界も明ら かになった。近年 WHO が作成した健常児の成長曲線に は 新 し い 統 計 モ デ ル で あ る GAMLSS (http://www.gamlss.org/)が用いられており、そのような統 計分析方法の適用も今後の検討課題であるだろう。 36 日 本 のデュシェンヌ型 筋 ジストロフィー推 定 患 者 数 川 井 充 * 【緒 言】 1987 年にデュシェンヌ型筋ジストロフィーの原因遺伝 子であるジストロフィンが発見されてから 25 年が経過し、 エクソンスキッピング、ストップコドンの読み飛ばしなど発 症機転を標的とする治療法が開発されるようになった。し かし、筋ジストロフィーは希少疾患であるうえに、これらの 治療法の多くはエクソン欠失や点変異など特定のタイプ の遺伝子変異を有する患者を対象とするので、開発の最 終段階である臨床試験においては患者のリクルートに困 難が予想される。Remudy という患者登録システムに期待 がよせられるゆえんである。 しかし、そもそも患者は何人いるか、どのような性別・年 齢分布か、治療を必要とする患者は何人いるのかは治 (1) デュシェンヌ型筋ジストロフィーの生命表の作成 療薬開発には根本的に重要な問いである。デュシェンヌ 型筋ジストロフィー患者は 2000 人台といわれているが根 【目 的】 拠は乏しい。いかに患者登録システムが優れていても、 筋ジストロフィー専門医療施設の入院患者データベー すべての患者が登録されているわけではないので、何ら スを利用してデュシェンヌ型筋ジストロフィー患者の生命 かの方法で患者数とその年齢分布を推定することが強く 表を作成する。 求められている。 筋ジストロフィー専門医療施設の入院患者データベー スには、国立病院機構 26 施設と国立精神・神経医療研 年齢階層別の患者数は年ごとの患者出生数と現在の 究センター病院に入院中の約 2100 人の患者が登録され 年齢に達するまでの生存率によって決定される。年ごと ているが、そのうちデュシェンヌ型筋ジストロフィー患者は の患者出生数は年ごとの男児出生数とこの疾患の発生 950 人前後である。1998 年から毎年 10 月 1 日現在の 率によって規定される。男児の年次別出生数は人口統 全患者が登録されている。登録内容は以下のとおりであ 計から知ることが可能である。デュシェンヌ型筋ジストロフ る。性別、生年月日、居住地、病型、診断根拠、障害度、 ィーの発生率は先進国では減少傾向にあることが知られ 病院、病棟、人工呼吸、気管切開、酸素使用、栄養摂取、 ており、日本のおける年ごとの値はこれまでのいくつかの 死亡、死因等。 報告から推定することができる。 【方 法】 一方、年齢ごとの生存率は最も得難いデータであるが、 2000 年から 2009 年までの 10 年間の年間死亡率から 国立の筋ジストロフィー施設で構築され、10 年以上にわ 生命表を作成した。さらに前半( 2000−2004 年)後半 たって継続されている、患者データベースがあるので、こ (2005-2009 年)2 つの期間に分けて比較した。10 歳未 れを用いて生命表を作成することが可能である。生命表 満のデータがなかったので、10 歳までの死亡率は “0” に表れる生存率をその年齢に達するまでの生存率に代 と仮定した。本来は年ごとに作成すべきであるが、死亡 用することが可能であると考えた。 数が少なかったため、5 年ないし 10 年間にわたって同じ * 国立病院機構東埼玉病院 37 年齢の死亡率を平均した。46 歳以後のデータも乏しかっ 表1 たため、生存率の低下速度は 46 歳以後も同じであると仮 定した。 【結 果】 得られた生命表を標に示す。(表1) また 2000 年代前半と後半の生存率曲線をグラフにし た。5 年の間に生存率曲線のわずかな改善が認められる。 またこのグラフから 50%の患者が死亡する年齢は 34 歳 前後であることが読み取れた。 【考 察】 生命表による生存曲線は現在の医療技術が今後変わ らないと仮定したときの生存曲線と考えることができる。呼 吸管理を行う前(1970 年代)の寿命は 18 歳、呼吸管理が 定着した 2000 年ころは 27 歳であり、2000 年代になって も確実に寿命が延長している。(図1) 図1 38 (2)デュシェンヌ型筋ジストロフィーの発生率の推定 (3)デュシェンヌ型筋ジストロフィー患者数の推定 【目 的】 【目 的】 デュシェンヌ型筋ジストロフィーの発生率はしばしば男 すでに明らかになった、生命表からの年齢別生存率、 子出生 3,000 人に 1 人とされている。しかし、先進国では 年代別発生率を人口統計と組み合わせることによって、 年代が新しくなると発生率は減少することが知られている。 現在のデュシェンヌ型筋ジストロフィー患者の年齢別患 出生年代ごとの出生数を知るために、年代ごとの発生率 者数を推定する。 を推定する。 【方 法】 【方 法】 DMDの患者数は以下の 3 つのデータを使用して推定 日本の DMD の発生率を記した諸報告から 18 組の(発 した。 生率、出生期間)のデータを得た。その中には同じ地域 1. 年あたりの男性出生数 で推移をみた5つの報告が含まれていた。出生期間の中 国立社会保障・人口問題研究所の人口統計資料集 央の時点をそのデータの時間軸の数値とした。このデー (2012)を用いた。得られる最も新しい出生数は 2010 タをグラフにプロットするとともに回帰式をもとめた。 年までであるので、2010 年の推定患者数求めること にした。 【結 果】 2. その年のDMD発生率 デュシェンヌ型筋ジストロフィー患者の発生率(出生 10 日本のDMD発生率を記載した諸報告から 18 組の発 万あたり)は年代が新しくなるに従い低下する傾向がみら 生率、出生期間のデータを得た。これらのデータから れた。回帰式 発生率=-0.34X 西暦年+891.9 が得ら 男子出生 10 万あたりの発生率=-0.34X 西暦年+ れた。 691.9 の回帰式を導いた。 3. 出生から現在までの生存率 出生から現在までの生存率は、国立筋ジストロフィー 専門施設で作成している「筋ジストロフィー患者デー タベース」の 200 年から 2009 年の 10 年間データに 基づいて得られた生命表を代用した。 データが得られない部分については以下の仮定をお いた。 1) DMD患者は 10 歳までは死亡しない。 2) 生命表のデータが存在しない 46 歳以降も同じペ ースで患者数が減少する。 【結 果】 計算の過程も含めた結果を表「出生年別の生存者数 の推定」に示した。またその結果をグラフにしたものが「日 本におけるデュシェンヌ型筋ジストロフィー年齢別推定患 者数」である。 【考 察】 年齢階層別の推定患者数は、0 − 9 歳 570 人、 デュシェンヌ型筋ジストロフィーの発生率が年代ととも 10−19 歳 781 人、20−29 871 人、30−39 歳 771 人、 に減少する理由はこの研究からは明らかではないが、こ 40−49 歳 465 人、50 歳- 100 人、総数 3,559 人となっ れまでの研究から家族にデュシェンヌ型筋ジストロフィー た。 患者がいる女性がデュシェンヌ型筋ジストロフィー患者を 生まなくなったためであると推定されている。 39 ので、根拠不十分な仮定をおかざるをえなかった。しかし、 呼吸筋麻痺が進行するのは 10 歳以後であり、心不全死 があるとしても極めてまれであろう。他の点で 10 歳以前 のはデュシェンヌ型筋ジストロフィー患者の死亡は一般 人口のそれと同じと考えてよいので、ほとんど無視してよ いと考えるのは妥当であろう。高年齢の集団の死亡数は 患者総数が少ないために著しく少なく、死亡率計算には 使えなかった。同じペースで死亡していくという仮定は現 在とりうる判断で最善のものと思われる。 第 2 に、出生年別の生存率が不明であることである。 本来は医療の進歩があるのだから、それぞれの年代に 出生した患者群の生存曲線が必要である。これを生命表 で代用することは、本来は時代とともに変化する生存率 のかわりに、一律に 2000 年代の医療水準による死亡率 をあてはめたことになり、とくに高年齢階層の生存率を過 大に評価する危険があることに留意しなければならない。 第 3 に、入院という医療的管理下にある患者のデータ から年齢別生存率を推定しているので、在宅患者の生存 率を過大に評価している可能性がある。その結果、とくに 高年齢階層に対して患者数を過大に推定していると思わ れる。 第 2、第 3 のポイントを考慮すると、およそ 3,500 人とい う推定患者数は過大に評価されている可能性は捨てき れない。 【結 論】 日本の DMD の推定患者数はおよそ 3,500 人で、し ばしば引用される 2,000 人台より多いと推定される。これ は 30 年間で寿命が大幅に延長しているためである。ま た、20 歳代なかばの患者が最も多い。これは発症率が 減少しつつあるためである。 【考 察】 この研究の価値と限界について論じる。 1) この研究の価値: 根拠をもって現在のDMD患者数を示したはじめての 研究である。デュシェンヌ型筋ジストロフィー患者の実数 把握は極めて狭いコミュニティーは別として事実上不可 能といってよい。医療期間を対象とした調査では患者の 重複は避けられない。死亡の把握も困難である。あくまで も推定の域を出ないが、本研究で採用した方法は考えら れる最善の方法といえる。 2) この研究の限界: 第 1 に、10 歳以前と 46 歳以後の死亡率が不明である 40 Ⅳ. 新規登録システムの開発研究 Remudy 登 録 情 報 のオンライン管 理 本 吉 慶 史 * 治験を目的とした筋ジストロフィー患者登録システム TREAT-NMD の匿名化患者情報から登録項目を抽出。 (Remudy)で構築される患者データベースは NCNP の事 連結可能匿名化を行い、サーバ上に匿名化後の診療情 務局で主として紙ベースで運用されるが、焼失や紛失の 報 DB を作成した。ID とパスワード(PW)により登録情報 危険がある他、データ件数の増加に伴って登録や更新 の一覧ならびに更新ができる Web アプリケーションを開 にあたり不具合を生じる懸念がある。 発した。 筆者は本研究班の前身「筋ジストロフィーの治療と医 サーバでのデータ管理にはオープンソースの RDBMS 学的管理に関する臨床研究」川井班のサーバ上でリレー である PostgreSQL を用いた。Remudy の患者情報入力 ショナル型データベース管理システム(RDBMS)を用い シート、ならびに TREAT-NMD の匿名化患者情報から登 た診療情報データベース(DB)システムを開発し運用し 録項目を抽出し、これらの項目をデータの実体(entity)と てきた。本研究ではこの経験に基づき、リスク対応とデー 実体間の関連(relation)に分けて Entity-Relationship(ER) タの安全な運用管理を目的とする診療情報データベー 図を作成。この ER 図に基づいて正規化を行った。具体 スを構築し、患者や主治医によるオンラインでの閲覧や 的には、診断名や遺伝子診断情報など経時的に変化し 更新が可能な可用性のあるシステムを開発する。 ない項目のテーブル、運動機能や車椅子使用状況、心 機能や呼吸機能、治療内容など経時に推移する繰り返 し項目のテーブルに分け、複数のテーブル(DB スキーマ) を設計した。川井班サーバに DB を実装し、ID と PW に 平成 23 年度 より登録情報の一覧ならびに更新ができる Web アプリケ 川 井 班 の サ ー バ で は Basic 認 証 、 Secure Socket ーションをスクリプト言語 PHP により開発した。 Layer(SSL)技術による通信路の暗号化が行え、スクリプト 言語 PHP とリレーショナル型データベース PostgreSQL が 利用可能であり、これらの機能を用いて診療情報 DB シ 平成 24 年度 ステムを構築した。本システムでは共通鍵方式で通信内 川井班サーバで運用した従来の診療情報 DB は主治 容を暗号化する SSL 技術を用いてインターネット上で安 医のみをユーザとして想定しており、事務局、患者、主治 全に情報交換を行える様にし、さらに個人情報保護と利 医という複数ユーザへの異なるアクセス権の付与を考慮 便性を両立させるため、DB のアクセス制限と利用者の認 していなかった。また単一の公開サーバでの運用では匿 証、セッション管理を実装した。本サーバはホームページ 名化により個人情報が削除されているため、事務局がデ 公開のためにインターネット上の不特定多数のクライアン ータ処理をする際に患者の特定が困難となりがちである。 トからのアクセスを許可しており、オペレーティングシステ そこで事務局からの運用の利便性に配慮して、複数サー ム (OS)や基幹ソフトウェアのバグ等を通じて攻撃を受け バでのレプリケーションを用いたシステム構成とした。 る可能性がある。そこで Remudy に於いては、個人情報 の安全性、機密性を保証するため、インターネットサービ 【方法と結果】 スプロバイダ(ISP)の所有するデータセンタに設置された 本システムでは、患者や主治医に公開する公開サー サーバでの運用を想定した。 バの他に、事務局ならびに公開サーバだけをアクセス対 象とする保護サーバの複数台のサーバ構成とすることに 【方法と結果】 した。 初年度は基本的なデータベース設計と入出力システ 公開サーバ OS として Linux、SSH と VPN 接続のための OpenSSL、 ムを開発した。Remudy の患者情報入力シート、ならびに * 国立病院機構下志津病院 43 WWW サーバとして Apache、RDBMS に PostgreSQL、ス 面では、ユーザ自身による PW、或は E-mail アドレスの クリプト言語として PHP をインストールした、インターネット 変更が可能である。 上の専用サーバに静的情報と動的情報のテーブルを置 運用 き、診療情報 DB システムを実装する。ユーザがアカウン Remudy 登録症例は全て、サーバの DB に登録する。 トと PW によりログインすると、該当する患者情報が表示さ 新規登録の際には、患者や主治医にオンラインでのデ れ、動的情報については新規データの追加ができる。こ ータ参照や更新を希望するかを尋ね、希望する場合に の追加登録は DBMS のレプリケーション機能により保護 はシステム上で一意なアカウントを取得して貰い、通常の サーバに反映される。ユーザ認証は保護サーバに認証 PW を設定するか、OTP のための E-mail アドレスの登録 要求を送ることにより行う。 を求める。 保護サーバ 更新に際しては、患者は体重や運動機能、車椅子使用 ハードウェア・ソフトウェア構成は公開サーバと同様で 状況の変化を随時オンラインで入力し、主治医は外来診 あるが、アクセスは事務局・公開サーバとの間の 察時に心機能や呼吸機能など観察データ、ステロイドや OpenSSL を用いた SSL-VPN 接続に制限する。このサー 心筋症など治療の推移を入力する。 バには、公開サーバに置かれる静的・動的情報テーブル 患者や主治医がオンラインの入力に不慣れな場合を の他に認証テーブルを置き、公開サーバからの認証要 考慮して、入力画面を患者用、主治医用に分け、必要な 求に応える。また病院情報、主治医情報、ならびに患者 項目に限り表示させる。またオンラインだけでなく、画面 個人情報の一部も保護サーバに置かれる。患者情報テ を印刷して該当項目に記入した上で郵送し、事務局が入 ーブルは公開サーバからのレプリケーションにより更新さ 力する手段も可とする。 れ、事務局は保護サーバ上の追加登録データを確認後、 また、これら事務局以外の入力では誤入力が発生する コミットすることで新規データとして確定する。 と考えられるため、公開サーバでは既存データの「修正」 以上の構成にすることにより、事務局は保護サーバに は行わず、動的情報の「追加」登録のみを可能とする。こ アクセスし、公開サーバからレプリケーションされた更新 こで入力された追加データは保護サーバに反映され、事 情報と保護サーバ上に置かれた個人情報を組み合わせ 務局が患者や主治医に電話等で確認した後、コミットし て、Web アプリケーションでデータ管理が出来る様になっ て確定する。 た。 【考 察】 平成 25 年度 Remudy で取り扱われる患者情報はネットワークから切 川井班サーバとは別に、仮想専用サーバ(VPS)をホス り離された PC 上のソフトウェアで管理され、患者や主治 ティングし試験運用を開始した。ユーザ認証に於けるパ 医との情報交換は紙ベースで行われているが、ここには スワードの管理など運用上の課題について対策を講じ、 幾つかの問題がある。 今後の運用方法について検討した。 情報の管理方法として、Word や Excel のファイルの様 に、PC の応用プログラムがデータを保有し管理する形態 をファイル形式と呼ぶが、この方式では多数のデータを 【方法と結果】 インターネット上の VPS に、Linux(CentOS 6)、SSH と 処理する様になると、応用プログラム毎に表現形式が異 VPN 接続のため OpenSSL、WWW サーバに Apache、 なる、複数のファイルの間で同じデータが存在して冗長 RDBMS に PostgreSQL、スクリプト言語として PHP5 をイ になる、一つのデータを修正するために複数のファイル ンストールし、DB システムを構築した。 を更新しなければならず整合性が保ちづらいなどの不具 ユーザ認証 合が生ずる。Access やファイルメーカーなどクライアント 患者や主治医にとつて Remudy 情報の更新は頻繁に 用の RDB ソフトも存在するが、情報処理の専門家ではな 行われるものではなく、通常の PW は失念しやすい。そ い医療関係者が適切なデータベースの設計を行い、 の対策として保護サーバの認証テーブルに、アカウントと TREAT-NMD への登録に必要な XML 形式での出力を 通常の PW の他に、E-mail アドレスのフィールドを置き、 行うことは困難である。 ワンタイムパスワード(OTP)機能を実装した。OTP では公 この様なファイル形式でのデータ管理の不具合を解消 開サーバにアカウントを入力すると、一定時間有効な PW するために 1960 年代に誕生したのが DB 管理システム が登録済のアドレスに E-mail で送られる。ログイン後の画 (DBMS)である。DBMS では一つのデータだけが記憶さ 44 れるのでデータの冗長性を除去でき、更新の際のデータ る。 の一貫性を保つことができる。またアプリケーションは直 この様なサーバ上でのデータ管理手法は、ネットショッ 接データを操作せず、DB の提供する標準的なインター プなど電子商取引が普及した現在では珍しいものではな フェースを介して操作するので、データの安全性を向上 いが、診療情報データベースに限っては筆者の知る限り、 できる。さらに DB システムの提供する標準的なインター 多数のデータが羅列されて視認性に乏しいものが多く、 フェースにより、DB 設計とアプリケーションの開発を独立 また入力必須項目が空欄であったり、以前のデータと齟 して行えるなどの利点がある。DBMS を利用すれば、DB 齬があったり、或は想定外の数値であっても入力時にエ の設計や XML 出力などのソフトウェア開発は情報処理 ラーが発生しないなど完成度の低いものが殆どである。 技術者が行うので、事務局は患者情報の入出力に専念 入力エラーに対して入力時にアラートが発生しなければ、 することが可能になる。 データのチェックをする事務局側で、既登録データと照 また Remudy では遺伝情報など個人情報を含むため 合して誤りを発見し訂正しなくてはならない。これには手 人的、 物理的 、環 境的セ キ ュリ ティが重 要で あるが 、 戻りが生ずるし、エラー自体を発見出来なければデータ NCNP の一部局での管理には焼失や紛失、流出の危険 の正確さを欠き信頼性を損ねることになる。 があるし、ネットワークから隔離された PC ではアンチウイ RDBMS には本来、この様な入力時の誤りを防ぐ空値 ルスソフトのアップデートも出来ず、USB フラッシュメモリ 制約などの入力値制約、参照整合性の担保などの機能 などに潜むマルウェアに対処出来ない。また DBMS をサ があり、不正なデータ入力に即時に対応するトリガー機 ーバ上で運用しネットワーク経由で利用する場合は、サ 能を有するが、これらの機能が発揮できるか否かはデー ーバのシステムやデータのバッ クアップ、ソフトウェアの タ分析とスキーマ設計など論理設計次第である。既存の アップデート、ログ管理など日常のサーバ管理業務が必 診療情報 DB ソフトウェアの不具合は、この論理設計が 要である。この様なハードウェア環境やサーバ管理者を 充分になされていないためであり、見栄えはよくても、蒐 一般の企業やユーザが確保するのは困難であり、ISP の 集したデータの信頼性や一貫性を損なうことになりかね 所有するデータセンタにアウトソーシングするのが一般的 ない。 になっている。さらに災害対策として関東と関西のデータ 筆者は川井班での開発運用経験をもとに、Remudy で センタの両者に同じデータを保存する民間企業も多い。 蒐集する診療情報を分析して ER 図を作成し DB スキー 情報交換については、患者情報の登録ならびに毎年 マを設計した。複数サーバによりシステムを構成し、複数 の更新に際して、患者本人や主治医への確認作業が必 のアクセス権設定と、OTP など認証機能の実装を行った。 要であるが、現状の紙ベースの情報交換には多くの時間 これにより患者や主治医にとっては必要な都度、追加情 と労力を要する。一年毎の更新では車椅子の導入時期 報を登録できる環境が提供でき、作業時間が短縮される や体重について正確を期することはできないし、診療情 とともにデータの正確さが担保される。連結可能な匿名 報については次回の外来受診まで更新を待たねばなら 化データは公開サーバに置かれるが、事務局からは保 ない。主治医に対しても限られた診察時間の中で一年分 護サーバで管理される個人情報を利用してデータ操作 のカルテから観察データや治療内容の推移を纏める作 が出来るため、氏名を含む視認性に優れたデータ管理 業を強いることになる。この様にデータの発生と記録の間 ができる。複数の患者を登録する医療機関に対しても同 にタイムラグがあると、情報が不正確となりやすい。また 様の操作環境を提供することが可能である。また Web 上 Remudy 事務局に蓄積された情報は患者や主治医に還 の一覧画面では患者の経時的な診療記録を閲覧できる 元されることがないため、ユーザに対するインセンティヴ ため、入力元である患者や主治医に対しても有用なフィ にも乏しい。 ードバックとなると考えられる。 これらの不具合を解決するために、筆者はデータセン 東日本大震災に於いては診療録や「お薬手帳」の喪 タにサーバを置き、RDBMS によりデータを管理し、Web 失により診療継続が困難となる事例が多数みられ、リスク アプリケーションを介してデータを利用するシステムを開 管理の観点から、診療録の電子化や、診療録を病院外 発した。RDBMS では情報の独立性を保ち、冗長性を排 のサーバで管理する医療クラウドへの関心が高まってい 除し、その一貫性、整合性、保全性、妥当性、機密性、 る。内閣府 IT 戦略本部は 2010 年、医療分野の情報通 安全性を担保できる。標準の SQL 言語を用いてデータ 信技術戦略として、全国どこでも過去の診療情報に基づ を利用できるので、患者情報の登録だけでなく、XML 形 いた医療が受けられ、健康管理にも取り組める環境を実 式での出力など応用アプリケーションの開発も容易であ 現するための医療・健康情報を電子的に管理・活用する 45 全国レベルの情報提供サービスを創出する「どこでも MY 病院」構想を掲げており、これが実現されれば災害 時支援対策としても有用であるが、各種フォーマットの標 準化も完了していないのが現状で、個人や医療機関の 認証のために電子証明書などの公開鍵暗号基盤(PKI) を必要とするなど実現までに克服すべき点も多い。 本研究で構築した診療情報 DB システムは、個人情報 を保護サーバで管理する多段構成を採用することにより セキュリティに関する種々のコストを省き、誰でもアクセス できる公開サーバと暗号化技術を用いることにより安全 かつリアルタイムに更新作業が行え、患者や主治医に対 しては経時的な診療記録を提供できる「どこでも MY 病 院」のプロトタイプであり、診療情報のバックアップとして も有用なシステムとなると考えられる。 46 Ⅴ. 遺伝性神経・筋疾患の診断システムの確立 遺 伝 性 神 経 ・筋 疾 患 患 者 データベースに対 する 遺 伝 子 診 断 システムの確 立 西 野 一 三 * 【緒 言】 シークエンス対象例は 100 例(54%)であった。3 エクソン 筋ジストロフィーの治験・臨床研究を目的とした遺伝性 の解析例の内訳は、単独エクソン欠失 55 例(66%)、単 神経・筋疾患の患者登録システム Remudy に登録するた 独エクソン重複 15 例(18%)、微小欠失 11 例(13%)、ナ めには、正確な遺伝情報が不可欠である。本研究は、ジ ンセンス変異 2 例(2%)、欠失と重複合併例 1 例(1%) ストロフィノパチー、ならびに今年度より登録を開始した であった。全エクソンシークエンス解析の結果は、ナンセ 遠位型ミオパチーの効率的かつ正確な遺伝子診断シス ンス変異 45 例(45%)、微小欠失/重複 31 例(31%)、 テムの確立を目指すことを目的とする。 イントロン内変異 16 例(16%)、ミスセンス変異 3 例(3%)、 変異の認められなかったもの 5 例(5%)であった。 【方 法】 Remudy 登録を希望するジストロフィノパチー患者で、 平成 24 年度 MLPA 法で“単独”エクソンの欠失あるいは重複が認めら 平成 24 年 12 月末までにジストロフィン遺伝子解析依 れた場合、または MLPA 法で異常が認められないが、筋 頼総数は 289 件で、そのうち平成 24 年 1 月〜平成 24 生検でジストロフィンタンパク質の発現異常が確認された 年 12 月依頼数は 71 件であり、昨年とほぼ同数であった。 場合に、血液から抽出したゲノム DNA を用いてジストロ そのうち解析終了数は 287 件であり、きわめて順調に解 フィン遺伝子の変異解析を行った。単独エクソン欠失・重 析を終了しえた。このうち、3 エクソン解析は 41%、全 79 複の場合は、当該エクソンとその両側の計 3 エクソンにつ エクソン解析が 59%であり、全エクソン解析の割合が増 いて PCR 法を行い、必要に応じて直接シークエンス法を 加した。また、単独エクソンの異常、ナンセンス、ミスセン 併用した。また、MLPA 法で異常のない場合は、ジストロ ス、微小欠失・重複、イントロン内変異などの内訳は昨年 フィン遺伝子全 79 エクソンおよびその近傍イントロン領域 度までの結果とほぼ同様であった。また GNE 変異解析 を PCR 法で増幅し、直接シークエンス法を行った。 はこれまで本邦患者 200 名を超し、平成 24 年 1 月〜平 縁取り空胞をともなう遠位型ミオパチー(GNE ミオパチ 成 24 年 12 月の解析数は 70 件であった。 ー)の確定診断には遺伝子解析を行う必要がある。GNE ミオパチーが臨床(病理学的)に疑われ、かつ Remudy 平成 25 年度 登録を希望する患者に対し、神経研究所疾病研究第一 平成 25 年 12 月末までにジストロフィン遺伝子解析依 部と協力し、ゲノム DNA を用いた直接シークエンス法に 頼総数は 342 件で、そのうち平成 25 年 1 月~平成 25 よって全 12 エクソンおよび近傍イントロン領域の GNE 変 年 12 月依頼数は 58 件であり、昨年の 72 件と比較する 異解析を行った。 と僅かに減少していた。これまでに解析が終了した検体 また、過去の遺伝子解析結果報告で不十分な場合の は 340 件であり、きわめて順調に解析を進めている。こ 再検査も行い、正確な遺伝子診断を目指した。 のうち、3 エクソン解析は 41%、全 79 エクソン解析が 59% であり、全エクソン解析の割合が増加した。また、単独エ 【結 果】 クソンの異常、ナンセンス、ミスセンス、微小欠失・重複、 平成 23 年度 イントロン内変異などの内訳は昨年度までの結果とほぼ 平成 23 年 12 月末日現在、ジストロフィン遺伝子解析 同様であった。 の依頼総数は 210 件(平成 23 年 1 月〜平成 23 年 12 月 GNE 変異解析はこれまで本邦患者 300 名を超し、平 は 68 件)、解析が終了したものは 184 件であった。このう 成 25 年 1 月〜平成 25 年 12 月の解析数は 63 件であっ ち、単独エクソン欠失/重複は 84 例(46%)、全エクソン た。このうち、ホモあるいは複合へテロ接合変異が 41%、 * 独立行政法人国立精神・神経医療研究センター 神経研究所 49 1 変異のみ検出されたもの 3%、変異無しが 51%であっ myopathy with rimmed vacuoles). Neuromuscul た。GNE には好発変異が存在するが、新規変異も多く認 Disord 23,84-88,2013. められた。 【考 察】 MLPA 法で単独エクソンの欠失と判定されても、微小 欠失やナンセンス変異である場合があるので、注意が必 要である。イントロン内変異や変異未同定例については、 今後、骨格筋より抽出した mRNA 解析が必要となる。ま た、ナンセンス変異を有しながら臨床的には Becker 型で あるなど、臨床症状と遺伝子解析の結果が合致しない場 合があり、mRNA 解析を含めた解析が今後必要となるで あろう。 最近、GNE ミオパチーは筋病理診断を行う前に遺伝 子解析を行う場合が増加しており、類縁疾患も存在する ことから、今後、変異同定率は減少していく可能性がある。 遺伝子解析方法はめざましく進歩、改良されており、状 況に応じて臨機応変に対応していく必要がある。今後も 可能な限り、Remudy への登録希望に応えられるよう、工 夫を重ねていく必要がある。 【結 論】 Remudy 遺伝子解析部門として、DMD ならびに GNE 変異解析については、診断方法が確立し、順調に診断 サービスを行っている。今後は、限りある人材と資金の中 で、Remudy の方向性に合わせて、効率的かつ経済的な 解析方法を考慮していく必要がある。 【参考文献】 1) 木村 円,他.日本におけるデュシェンヌ型筋ジスト ロフィー患者登録システムー国際的な希少疾患デー タベースモデルとしての Remudy の取り組み。生体の 科学 63(1); 62-68, 2012. 2) Cho A, et al. Mutation profile of the GNE gene in Japanese patients with distal myopathy with rimmed vacuoles (GNE myopathy). J Neurol Neurosurg Psychiatry, in press 3) Mori-Yoshimura M, et al. Heterozygous UDP-GlcNAc 2-epimerase and N-acetylmannosamine kinase domain mutations in the GNE gene result in a less severe GNE myopathy phenotype compared to homozygous Nacetylmannosamine kinase domain mutations. J Neurol Sci. 318: 100-105, 2012. 4) Mori-Yoshimura M, et al. Respiratory dysfunction in patients severely affected by GNE myopathy (distal 50 遺 伝 性 神 経 ・筋 疾 患 患 者 データベースに対 応 する 遺 伝 子 診 断 システムの確 立 南 成 祐 研究協力者 島田 綾子 *, ** ,*** , 山下 利花 *, 相生 優子 ** 埜中 征哉 *, **, *** , 西野 一三 *, ** , 村山 久美子 *, **, *** , **,*** 平成 23 年度 Ⅰ. センター病院遺伝子検査診断室の現況 【緒 言】 国立精神・神経医療研究センター病院遺伝子検査診 断室(旧 DNA 診断・治療室)では、神経研究所疾病研 究第一部及び疾病研究第二部と共同で、筋病理診断、 生化学的診断、遺伝子診断を組み合わせた、神経・筋 疾患の統合的な診断サービスを提供してきた。また、過 図 1. 遺伝子検査診断室の業務 去 3 年間、Remudy 患者登録の DNA 抽出を担った。遺 伝子検査診断室の現況を報告し、本研究班における役 2. ウェブの活用 割をふまえた課題を検討する。 他院からの検査依頼を可能な限り受け入れており、開 【方法と結果】 設当初から依頼方法をセンターのウェブサイト内で公開 遺伝子検査診断室のデータベースを検索し、活動の してきた。検査項目の紹介にとどまらず、依頼方法を詳 現況を整理し、今後の課題を探る。 細に明示し、必要書類・同意書のダウンロードまでも可能 にしている。このような在り方は、一医療機関としては他 に類を見ないように思われる。 1. 活動の概要 遺伝子検査診断室の活動には大きく3つの柱がある。 3.遺伝子検査 一つめは検体(生検筋、血液等)の受付・登録作業で、 当室でおこなっている遺伝子検査は、保険適用のある 近年は年間に 1,000 件を超えるようになった。二つめは デュシェンヌ型・ベッカー型筋ジストロフィー(平成 22 年 検体からの DNA 抽出と保管であり、本研究班の主たる 度:39 件)、福山型先天性筋ジストロフィー(1 件)、脊髄 活動である Remudy 患者登録のジストロフィン遺伝子シ 性筋萎縮症(10 件)、球脊髄性筋萎縮症(4 件)の他、肢 ークエンスサービスの検体(平成 22 年度:73 件)を含め 帯型筋ジストロフィー2A 型(23 件)、眼咽頭型筋ジストロ て、年間に約 450 件あった。抽出後の DNA は遺伝子検 フィー(11 件)、筋強直性ジストロフィー1 型(11 件)・2 型 査診断室、疾病研究第一部、疾病研究第二部で遺伝子 (4 件)、DRPLA(4 件)であった。 診断や研究に供される。すなわち、三つめは言うまでも 今後の Remudy の対象疾患拡大との関連性を検討す なく遺伝子診断であり、当室では年間に約 150 件おこな るため、いくつかの疾患を取り上げて紹介したい。まず、 っている。 眼咽頭型筋ジストロフィーは、PABPN1 遺伝子の GCN リ ピート数の伸長が原因であり、これまでに 85 名の患者が 見つかっている。リピート回数が長いほど発症が早めで 症状も強い傾向を有意差がないながらも見いだしており、 さらに症例を増やして検討する必要がある。 * 独立行政法人国立精神・神経医療研究センター 病院 ** 独立行政法人国立精神・神経医療研究センター トランスレーショナル・メディカルセンター *** 独立行政法人国立精神・神経医療研究センター 神経研究所 51 TREAT-NMD で治験に向けた患者登録が始まってい つことも指摘している。今回、対象患者数を 99 名/84 家 る筋強直性ジストロフィーでは、repeat-primed PCR 法を 系に増やし、リピート数や遺伝子型と発症年令など臨床 用いて異常伸長アレルの迅速な検索を可能にしている。 所見との関係を再検討した。 この方法は筋強直性ジストロフィー2 型にも応用でき、そ 【方 法】 の検索もまた当室でおこなえる。ただし、この方法は非常 これ ま でに 当 室 にお い て 遺 伝子 診 断 を おこ ない 、 に長く伸長したリピートサイズを求められないため、患者 PABPN1 遺伝子変異が認められた 99 名/84 家系につ 登録を考慮し、サザンブロット法の復活を計画している。 いて、GCN リピート数・遺伝子型と、発症年令に代表され 最後に、脊髄性筋萎縮症である。当室ではこの検査に る臨床所見との関係を検討した。 いち早く MLPA 法を採用している。SMN1、SMN2、NAIP 各遺伝子のコピー数を判定できるため、複合へテロ接合 【結果と考察】 の患者まで見逃すことがまず無く、また、SMN2 遺伝子コ 1. GCN リピート数と病気の発症年令 ピー数が重症度に関係しており、治験のためにも重要な 基礎情報が得られる。この疾患は保険適用であるが、受 病的優性アレルは 12 回から最長 17 回まで 16 回を除 託検査をおこなっている民間の検査センターは未だ存在 いて分布し、最も多いのは 13 回であり約半数の家系 しない。 (46%)を占めた。病気の発症年令は、最小リピート数の 12 回で中央値 63 歳(59 歳〜67 歳、n=3)、最大リピート 【考察と結論】 数の 17 回で中央値 49 歳(42 歳〜53 歳、n=7)に代表さ 以上のような現況をふまえ、次のことが課題となる。 れるように、リピート数が大きいほど下がる傾向があった。 一つめは、遺伝子診断の整備と症例情報の蓄積であ 回数別の発症年令に統計的有意差があるかどうか り、当室が得意とする各種のリピート病や肢帯型筋ジスト Tukey's 多重比較検定を行ったところ、13 回 vs. 15 回で ロフィー2A 型に注力したい。二つめは、有料検査の受託 P<0.001、12 回 vs. 15 回で P<0.01、12 回 vs. 17 回と 13 手続きの整備であり、院内では有料(保険・保険外)でお 回 vs. 17 回で P<0.05 となり、有意差が認められた。眼、 こなっている脊髄性筋萎縮症や、デュシェンヌ型筋ジスト 咽頭、四肢の各症状別の検討では、眼瞼下垂の発症年 ロフィーの保因者診断を他院から利用しやすくする。三 令で有意差が多く得られ、嚥下障害ではオーバーラップ つめは、ウェブページの更新と充実である。当室の情報 が広く有意差は得られなかったが傾向は認められた。四 はもちろん、より広く神経・筋疾患の遺伝子検査に役立 肢筋力低下の発症年令については、15 回以上の大きな つ情報発信をしていきたい。 リピート数で急激に低下するように見えた。 【学会発表】 島田綾子, 村山久美子, 山下利花, 南 成祐: MLPA 法 を用いた脊髄性筋萎縮症の遺伝学的検査. 第 30 回日 本染色体遺伝子検査学会総会・学術集会, 東京, 2012.11.10. 平成 24 年度 Ⅱ. 眼咽頭型筋ジストロフィーの遺伝子診断と表現型 【緒 言】 眼咽頭型筋ジストロフィーは、PABPN1 遺伝子の GCN リピート数の増大が原因であり、野生型で 10 回であるの 図 2. リピート数別の発症年齢 に対して患者では 12 回〜17 回に増加している。我々は これまでに、リピート回数が長いほど発症が早く症状も強 2. 最大リピート数 17 回と遠位筋罹患 い傾向を有意差がないながらも見いだしている。また、最 最頻リピート数である 13 回では、集団全体の傾向とし 大リピート数である 17 回の患者では遠位筋罹患が目立 ては、眼症状→咽頭症状→四肢筋力低下という順で発 52 現していた。それに対し、最大リピート数の 17 回では 50 患者が一部存在する。 歳前後の病初期から筋力低下が顕著に現れていた。し かも、全 7 名中で、3 名は遠位筋優位、2 名はびまん性と 【学会発表】 され、そのため 4 名は眼咽頭遠位型ミオパチーを最も疑 南 成祐, 島田綾子, 相生優子, 埜中征哉, 西野一三: う臨床診断を受けていた。各リピート数別に、臨床診断上 眼咽頭型筋ジストロフィーの表現型と GCN リピート数. 第 の眼咽頭遠位型ミオパチー疑い症例の頻度を調査した 54 回日本神経学会学術大会, 東京, 2013.5.30. ところ、13 回と 14 回で約 5%、17 回で 57%となり、とくに 17 回と遠位筋罹患の結びつきが認められた。 平成 25 年度 Ⅲ. 筋強直性ジストロフィー1 型・2 型の検査法に関する 検討 【緒 言】 筋強直性ジストロフィーには 1 型と 2 型があり、遺伝子 変異はいずれも繰り返し配列の異常伸長である。1 型 (DM1)では CTG が 50 回〜数千回に、2 型(DM2)では CCTG が 75 回〜1 万回以上にまで増大する。 遺伝子診断では、この異常な伸長を判定する。今回、 図 3. 症状別発症年齢の比較:(GCG)13 と(GCN)17 筋強直性ジストロフィー(1 型および 2 型)の遺伝学的診 断について、近年の保険収載や技術的進歩を踏まえた 検査手順を提示することを目的とした。 3. 常染色体劣性型 OPMD 11 回のホモ接合による常染色体劣性型 OPMD 患者 【方 法】 は家系数ベースで約 5%存在した。11 回ホモ接合で発 症する常染色体劣性型 OPMD の発症年令は中央値 65 ① 保険適用の調査 歳(55 歳〜69 歳、n=4)と遅いうえに、眼症状の発現が数 ② 検査会社の受託検査の調査 年以上遅れる可能性が示された。この結果からは、眼症 ③ 推奨されている検査手法の概説、および問題点の整 状に欠ける場合でも、OPMD を鑑別から外すべきではな 理 いと思われる。 ④ 方法の改良や検討 (ア) DM1 の non-RI サザンブロット法における新規標 4. 優性アレルのホモ接合による重症化 識法の検討 12 回のホモ接合患者と 13 回のホモ接合患者を各1名 (イ) DM1 の中断配列の解析法の検証 ずつ経験した。後者は、30 歳台発症で、誤嚥性肺炎を (ウ) DM2 の repeat-primed PCR 法:プローブハイブリ 繰り返し、43 歳から全身に近位筋優位の筋力低下が進 を必要としないフラグメント解析法の検討、およ 行した。17 回の患者よりもさらに顕著に早発・重症であり、 び 3’側解析の開発 ホモ接合は相乗的に作用していることが示唆された。 (エ) DM2 の non-RI サザンブロット法の確立 ⑤ それらを踏まえて診断手順を検討する。 【結 論】 1. リピート数と発症年令の間に逆相関があることにつ 【結果と考察】 いて有意差を持って確認した。 2. 1. 検査の保険適用 遺伝子型による表現型の特徴 遺伝性疾患を対象とする「遺伝学的検査」は平成 18 (GCN)10/12 晩発・軽症(60 歳台発症) 年度から保険導入され、二年ごとに対象疾患や付帯条 (GCN)10/17 初期から四肢の障害、遠位筋罹患 件が見直されてきた。保険点数は当初 2,000 点であった (GCN)11/11 晩発、眼症状の発現が遅れる が、現在は 4,000 点になっている。筋強直性ジストロフィ 3. 優性アレルのホモ接合で相乗的に重症化する ーについては、平成 24 年度に収載され、1 型か 2 型か 4. 臨床的に眼咽頭遠位型ミオパチーと区別しがたい の限定はなく、検査手法についても制約はない。 53 2. DM1 の遺伝学的検査手法の概説 識プローブが使用可能である。定評のある DIG 標識(ロ DM1 の遺伝学的検査では、①サザンブロット法、②通 シュ)はもちろん、今回、アルカリフォスファターゼを酵素 常の PCR 法、③repeat-primed PCR 法の3種類の方法を 反応で標識する新しい方法(日立アロカ)を試し、遜色な 組み合わせて行うことが一般的に推奨されている。サザ い結果が得られた。 ンブロット法は、現在のところ、大きな異常伸長アレルのリ ピート回数が分かる唯一の方法である。しかしながら、手 間と時間がかかるという欠点がある。また、100 回未満の 短い伸長を見逃す恐れがある。一方、通常の PCR 法は、 正常者の大半について簡単かつ迅速に除外診断が可 能で、また、100 回未満の短い伸長を検出できる。しかし、 大きな伸長を検出することができないため、患者を直接 陽性判定できない。また、ホモ接合の正常者も判定でき ない。その後、repeat-primed PCR(RP-PCR)法が開発さ 図 4. DM1 の non-RI サザンブロット解析 れた(原報では triplet repeat-primed PCR を略して TPPCR 法と呼んでいるが、DM2 との汎用性から RP-PCR 法 4. RP-PCR 法では、DM1 リピート中断配列により偽陰性 の名称で統一した)。この方法は、片方のプライマーをリ を生じる ピート内部に置くことで PCR 産物のラダー伸長が得られ、 RP-PCR 法は簡便に陽性・陰性の両方の判定ができる 陽性と陰性のどちらの判定も可能である。唯一の欠点は、 リピート回数が約 100 回以上になると、伸長ラダーから陽 優れた方法であるが、患者の数%において、リピート配 性判定は問題なくできるものの、リピート回数は求められ 列の 5’端側解析では陽性になるのに、同じ患者の 3’端 ない点である。これらの手法の他には Long-PCR 法があ 側解析では伸長ラダーが認められなかったり、不規則で るが、結局はプローブハイブリが必要な手間や、長大な 不十分だったりすることが分かってきた。それらをサザン 伸長に対する不確実性といった面から、日常の臨床検査 ブロット解析すると、リピート領域全体は確かに伸長して においては優越性がさほどない。 いた。ということは、少なくともリピート 3’末端付近に CTG 繰り返しとは異なる何らかの配列があることが推測される。 じつは、2009 年に CCG 中断配列が存在する家系が初 3. DM1 のサザンブロット法を検査会社が受託 検査会社による受託項目を大手三社について調査し めて報告されており、現在までに数件の論文が確認され たところ、各社とも DM1 の遺伝学的検査をサザンブロット た。それらによると以下のようなことが分かってきている。 法で受託していることが分かった。ビー・エム・エルは正 #中断配列の大半が CCG であるが、他には GGC, CTC 式項目としており、三菱化学メディエンスは正式上市で が見つかっている。#その位置は、世代間で変化するこ はないが Web 掲載しており、エスアールエルは Web サイ とがある。#リピート伸長を抑制する傾向がある。#非典 トに掲載はないが特別依頼項目として依頼には応じてい 型的な臨床症状に関与する可能性がある。 ただける。今回、陽性例の見本を取り寄せたが、三社とも、 長大な伸長の検出に向く EcoR I 消化と、Bgl I や BamH I などの短い伸長の検出に向く消化の両方を行うという基 本ルールが守られていた。またスメア-バンド見逃しの主 因であるバックグラウンドの汚れも少なく、見本を見る限り では技術的な問題はとくにないように思われる。スメア-バ ンドのリピート回数の表し方は、エスアールエルが中央値、 ビー・エム・エルと三菱化学メディエンスは何回〜何回と なっていた。以上から、DM1 のサザンブロット解析は、手 図 5. DM1 の RP-PCR 解析で認められる偽陰性 間がかかる手法であるために個々の病院検査室で行うこ 3 症例の 5’端解析と 3’端解析を掲載した。5’端では異 とは困難であるが、検査会社が受託をしており、十分信 頼性のある結果が得られると思われる。 常伸長ラダーが陽性であるが、3’端では陰性ないし不完 全である。数%の患者にこのような 3’端解析の偽陰性が 自前でサザンブロット法を行う場合、現在は non-RI 標 54 見つかる。 6. DM2 の遺伝学的検査手法の概要 つぎに DM2 の遺伝学的検査であるが、DM1 と同様な 5. DM1 リピート中断配列の解析方法の検証 手法が用いられる。ただし、サザンブロット法の信頼性は そこで、臨床遺伝学的な意義を追求するためには、ま DM1 のときのようには高くなく、初期の研究によれば、約 ずは個々の患者の中断配列を同定する必要があると考 20%の患者で偽陰性となるとも言われていた。その理由 え、過去の論文に習い、1 名の患者 DNA を対象として は、平均でも 5000 回=すなわち 20000 塩基対もの長大 RP-PCR 変法による解析を試みた。すなわち、通常用い な伸長がある上にモザイシズムが顕著なため、スメア-バ る(CTG)5プライマーの最後の CTG を各種の中断配列に ンドの検出が DM1 以上に難しいからと考えられている。 置き換えた中断配列解析用リピート内プライマーを用い そのため、DM2 では PCR 法と RP-PCR の役割がむしろ て RP-PCR 変法を行う手法である。すると、CCG 解析用 中心的である。まず、健常者の 90%以上は PCR 法で正 プライマーのときのみ複数のピークを持つ増幅産物が得 常へテロ接合として陰性判定できる。日本人において られた。この増幅産物全体をシークエンス解析したところ、 DM2 は大変まれであることが我々の研究で分かっている ピーク位置にほぼ一致して CCG 中断配列が現れた。さ ため、この除外スクリーニングはとくに効果的である。また、 らに、ピークのない場所にも、CCG 中断配列が連続する RP-PCR 法では、サザンブロット法で見逃してしまうような 領域があることがわかった。これは、中断配列が密に存 患者も含め、99%以上の診断感度があるとされている。よ 在すると逆にプライマーがアニールできないためと説明 って、DM2 では RP-PCR 法による検査が最も重要である。 できる。以上のように、RP-PCR 変法〜シークエンス解析 検査会社では DM2 の遺伝学的検査は行われていな い。 によってリピートの末端付近の中断配列の解析がある程 度は可能なことが確かめられた。今後、患者数を増やし 7. DM2 の RP-PCR 法をさらに確実な方法に改良 て解析し、臨床遺伝学的な意義を追求する計画である。 DM2 において RP-PCR 法は 99%の診断感度を持つ また、リピート深部の解析手法は今後の課題として残った。 図 5 の 3 症例目では、CCG 中断配列解析用プライマ 重要な検査法であるため、簡便性と信頼性の更なる向上 ーを使用したときに増幅産物のピークが現れ、そのシー を狙って改良を行った。第一に、プローブハイブリによる クエンス解析で GCG 配列が多数見つかった。 増感検出を不要とするべく、PCR 条件をチューニングし 図 6. 中断配列の RP-PCR 変法を用いた解析 55 たところ、蛍光シークエンサーを使用したフラグメント解析 によって異常なラダーピークを検出できた。第二に、原法 ではリピート領域の 5’端側しか解析していないが、3’端側 の解析を試みたところ、ラダーパターンがはるかにシンプ ルになり、また PCR 増幅も良好で、確実に異常を証明で きる 75 回以上まで伸長したラダーピークを得ることができ、 陽性判定が容易になった。リピートの両端を解析すること によって、信頼性が格段に向上することが期待できる。 図 8. DM2 non-RI サザンブロット解析 患者 P1、P2 ともに、20-23 kb の伸長、すなわち CCTG 反復にして 5,000〜6,000 回の伸長を認めた。M はサイズ マーカー、N は正常対照。 【結 論】 筋強直性ジストロフィー1 型(DM1) 1) 検査手順: 保険収載されており、検査会社が受託しているサザン ブロット法を中心に考える。 (陰性結果に疑問がある場合は、短い伸長の可能性 を疑い、PCR 法や RP-PCR 法による検証を行う。) 2) 院内で行う場合は、 ① まず、RP-PCR 法+PCR 法を用いて検索 図 7. DM2 RP-PCR 法の改良 ② サイズ決定には non-RI サザンブロット法 注)RP-PCR は両端の解析を行う 3’端側解析は数%の患者で偽陰性(中断配列) 8. DM2 の non-RI サザンブロット法を確立 つづいて、DM2 のサザンブロット法について、non-RI 標識プローブ法を試みた。RI 標識法ですら偽陰性が多 筋強直性ジストロフィー2 型(DM2) いというので困難さを予想していたが、試行錯誤を重ね 1) 国内の主要な検査会社では行っていない た結果、特異プローブを従来のものより長くし、良好な結 2) 検査手順: 果を得ることに成功した。なお、実験的に証明したわけで ① RP-PCR 法+PCR 法で検索 はないが、高分子量 DNA のナイロン膜への転写のため ② Non-RI サザンブロット法で確認とサイズ決定 に、塩酸処理とトランスファー時間を長く念入りに行うこと (重症度や発症年齢との相関はない) もポイントであるように思われた。また、別の方法として、 注)RP-PCR 法は両端の解析を行う Nakamori ら(Neuromuscul Disord. 2009;19:759–762)に (今回、3’端解析法を確立し、可能となった) 習い、Alu I と Hae III という 4 塩基認識の制限酵素による 二重消化によって異常伸長リピート以外のゲノム DNA を 【参考文献】 細かく断片化させ、(CCTG)5 LNA オリゴプローブで増感 Matsuura T, Minami N, Arahata H, Ohno K, Abe K, 検出する方法でも異常伸長バンドを認めることができた。 Hayashi YK, Nishino I.: Myotonic dystrophy type 2 is rare いずれの方法でも、今回の 2 名の患者サンプルでは in the Japanese population. J Hum Genet. 2012;57:219-220. 5000〜6000 回の伸長を認めることができた。今後は、ル ーチン検査で安定的に検出できるよう、ノウハウを積み上 げたい。 56 図 9. 筋強直性ジストロフィーの検査手順 57 ジスフェルリン異 常 症 の患 者 登 録 システムの構 築 と 遺 伝 子 診 断 システムの確 立 に関 する研 究 髙 橋 俊 明 * ジスフェルリンは共同研究者の青木らにより三好型遠 現型を呈していた。変異は遺伝子全体に広く分布し、22 位型筋ジストロフィー(MMD)や肢帯型筋ジストロフィー 種類のナンセンス変異、10 種類のミスセンス変異、10 種 (LGMD)2B 型の原因遺伝子であることが明らかにされた 類 の ス プ ラ イ ス 部 位 の 変 異 だ っ た 。 c.2997G > T 。我々はジスフェルリン遺伝子解析を通じて、日本人 ( p.W999C ) 変 異 が 40 アレ ル ( 22.7% ) 、 c.1566C > G MMD での遺伝子変異の特徴として4種の変異が多いこ (p.Y522X)変異が 23 アレル(13.1%)、c.4497delT 変異 とや G3370T(現 c.2997G>T)変異を伴うと発症年齢が遅 が 15 アレル(8.5%)、c.3373delG 変異が 14 アレル(8.0%) いこと 2) を報告した。 と日本人に多い変異だった。 c.2997G>T 変異は MMD 1) 近年ジストロフィン異常症を中心に遺伝子治療の準備 より LGMD2B に多く見られ、ホモ接合は MMD では 1 人 が急速に進みつつある。一方でジスフェルリン異常症は、 のみだった。一方 c.3373delG 変異は LGMD2B には 1 ア 未だ本邦では患者登録制度も確立していない。しかし将 レルしか認めなかった。 来遺伝子治療が本症をも対象とする日に備え患者登録 制度の基礎となる遺伝子診断システムの確立は重要な 【考 察】 意義がある。 SSCP 法では c.1566C>G 変異の検出率が低かったよ うに、他の見落としの可能性がある。また大きな欠失や重 複も検出できない。イントロン内やプロモーター領域も見 ていない。スプライス異常の確認は RNA の解析も必要で Ⅰ. PCR-SSCP 法による日本人ジスフェルリン遺伝子変 ある。 異のスクリーニング 本研究では我々の行ってきた PCR-SSCP 法により検出 【結 論】 し得た日本人同遺伝子変異の特徴を解析し、本方法の 今後は他の方法を合わせた同遺伝子変異のスクリー ニング法の検討を行っていきたい。 問題点を検討した。 【方 法】 インフォームドコンセントを得た後に、ゲノム DNA を 55 Ⅱ.全エクソンシークエンスによるジスフェルリン遺伝子変 個のエクソンごとに近傍のイントロンを含め PCR-SSCP 法 異のスクリーニング法の検討 にて遺伝子変異をスクリーニングし、直接塩基配列決定 法にて確認した。c.1566C>G 変異は PCR 産物の Mbo I これまではエクソンが 55 個あるため PCR-SSCP 法によ による切断を見て直接塩基配列を確認した。ナンセンス り同遺伝子変異のスクリーニングを行ってきたが、最近は 変異以外は正常 100 染色体に存在しないことを確認した。 全エクソンシークエンスを行っている。これにより検出し得 た日本人同遺伝子変異の特徴を解析した。 【結 果】 91 家系に 42 種類の変異を見出した。54 家系がホモ 【方 法】 接合、31 家系が複合ヘテロ接合だった。6 家系の発端者 インフォームドコンセントを得た後に、ゲノム DNA を 55 では 1 アレルしか変異を見出せなかった。遺伝子変異が 個のエクソンごとに近傍のイントロンを含め PCR し、サイ 確定した 51 人が MMD、40 人が LGMD2B、1 人が distal クルシークエンス法にて変異の検出をした。ナンセンス変 anterior compartment myopathy、7 人が高 CK 血症の表 異以外は正常 100 染色体に存在しないことを確認した。 * 国立病院機構仙台西多賀病院 59 【結 果】 合することで、原因遺伝子の同定を行う。 45 家系に 31 種類の変異を見出した。15 家系がホモ 【結 果】 接合、25 家系が複合ヘテロ接合だった。5 家系の発端者 では 1 アレルしか変異を見出せなかった。遺伝子変異が 連鎖罹患者 5 名、非罹患者 5 名の計 10 名について 確定した 20 人が MMD、20 人が LGMD2B の表現型を 行った結果、LOD score>2 を 5 箇所に同定した。また、 呈していた。変異は遺伝子全体に広く分布し、19 種類の エクソーム解析を罹患者 4 名、非罹患者 3 名の計 7 名に ナンセンス変異、11 種類のミスセンス変異、1 種類のスプ ついて行った結果、罹患者のみに共通する新規の機能 ライス部位の変異だった。c.2997G>T(p.W999C)変異 的変化を起こし得る遺伝子変異は 2 個にまで絞り込まれ、 が 24 アレル(28.2%)、 c.4497delT 変異が 9 アレル(9.4%) その内 1 個が上記の連鎖領域内に存在した。この変異を、 と日本人に多い変異だった。 解析可能な 10 名全てについてサンガーシークエンスし た結果、segregation に矛盾なく、本変異が原因変異であ 【考 察】 ると結論づけた。健常コントロール 191 例では本変異を 45 家系の解析で SSCP によるスクリーニングで見出せ 認めなかった。 ない変異が 15 種類見つかった。また複合ヘテロ接合の 【結 論】 家系の割合が SSCP で行ったときより多かった。本方法で も大きな欠失や重複も検出できないしイントロン内やプロ エクソーム解析と連鎖解析を併用することで、MFM の モーター領域も見ていない。スプライス異常の確認は 大家系で新規の原因変異を同定することに成功した。今 RNA の解析も必要である。 後ジスフェルリン遺伝子変異検出にも次世代シークエン サーを応用していきたい。 【結 論】 労力およびコストの面も考慮する必要があるが、今後も 次世代シークエンサーを含めた他の方法を合わせた同 Ⅳ.エジプトでの最初のジスフェルリン異常症の患者 5) 遺伝子変異検出法の検討を行いたい。 カイロの筋神経研究所の筋ジストロフィー患者筋から 免疫染色とウエスタンブロットで診断されたジスフェルリン Ⅲ.筋原線維性ミオパチーの大家系での次世代シーク 異常症 4 家系 6 人の遺伝子検索を行った。2 家系でホモ エンサーを用いた原因遺伝子の同定 3) 接合の変異、1 家系にヘテロ接合の変異が見出された。 1 家系では変異が見つからなかった。 筋原線維性ミオパチー(MFM)の原因遺伝子およびそ の表現型は現在まで国外を中心として幾つかが報告さ れているが、これらの既知の原因遺伝子に変異を見出す Ⅴ.心障害をともなったジスフェルリン異常症の 1 剖検例 6) ことが出来ない群も多く、依然詳細な病態は明らかとなっ ていない。常染色体優性遺伝形式をとる MFM の本家系 心障害をともなったジスフェルリン異常症の 1 剖検例を では、現在まで 5 世代に渡り約 20 名の罹患者が出てい 報告した。心筋の配列の乱れと高度の横隔膜の変性を る 4)。下垂足を初発症状とし、遠位筋、胸郭、肩甲帯を主 認めた。長期経過例では注意深い心、呼吸機能評価を 体とした慢性進行性の筋委縮と筋力低下を呈するが、比 要する。 較的早期(発症から平均 3.8 年)に呼吸不全を合併する 点に特徴がある。本家系の原因遺伝子は未だ不明であ ることから、本研究に着手した。 Ⅵ.認知症を伴った LGMD2B 型の 1 家系 7) 【方 法】 国立病院機構あきた病院の小林道雄分担研究者らと 次世代シークエンサーによる全エクソンの遺伝子配列 共同で、認知症を伴った LGMD2B 型の 1 家系の遺伝子 解析(エクソーム解析)で罹患者のみに共通した遺伝子 検索を行った。 変異の抽出を行う。また、全ゲノム SNP チップを用いた連 鎖解析によって連鎖領域を明らかとし、これらの結果を照 60 Ⅶ.LGMD2B 型の臨床型と発症の遅い変異 8)9) 【方 法】 インフォームドコンセントを得た後に、ゲノム DNA から 日本の LGMD2B 型の詳細な遺伝子型と臨床型を明 55 個のエクソンごとに PCR-SSCP 法にてジスフェルリン遺 らかにする。 伝子変異をスクリーニングし、直接塩基配列決定法にて 確認した。遺伝子変異の確定した MMD46 家系 49 人の 【方 法】 経過を解析した。 ジスフェルリン遺伝子変異の確定した日本人 【結 果】 LGMD2B 型 36 家系 40 人を対象とした。 c.1566C>G 変異、c.2997G>T 変異、c.3373delG 変異、 【結 果】 c.4497delT の 4 つ の 変 異 が 多 か っ た 。 肢 帯 型 と 比 べ 3 種類の変異(c.1566C>G、c.2997G>T、c.4997delT) c.2997G>T 変異の頻度は低く、c.3373delG 変異の頻度 が多く認められた。c.2997G>T 変異は発症が遅く、より近 が高かった。発症年齢は平均 21.8±7.5 歳で、c.2997G>T 位優位、上肢の筋力低下で発症することも多く、血清 CK 変異を持つと 28.8±9.0 歳、持たないと 21.0±7.0 歳で有意 値が低い。 差がみられた。初発症状はつま先立ち困難を主体とする LGMD2B 型は以下の特徴を示す。 下肢筋力低下がほとんどだったが、踵歩き困難、膝が上 1) 10 歳代後半から若年成人期に発症する。 がらないや握力低下も 1 人ずついた。平均経過ではつま 2) 下肢の筋力低下で発症する。 先立ち困難 0±0 年と手の脱力 9±9 年が肢帯型より早く認 3) 骨格筋 CT で初期から下肢遠位筋の障害がみられ められた。血清 CK 値は肢帯型では c.2997G>T 変異の も の が 最 低 値 だ っ た が 、 MMD で は 他 の 変 異 で も る。 c.2997G>T 変異同様に低値をとるものもあった。 4) 骨格筋 CT で初期から腰椎の傍脊柱筋の障害が みられる。 【考 察】 5) 上肢では近位筋優位の障害である。 6) 後期でも手の機能は保たれる。 MMD で は LGMD よ り 発 症 年 齢 が 早 か っ た が 、 7) 後期でも頸の筋力は保たれる。 c.2997G>T 変異を持つ症例を除くと差がなくなり、両者の 8) 顔面筋や嚥下は保たれる。 差は肢帯型にこの変異が多いためと考えられた。つま先 9) 側彎を呈さない。 立ち困難と手の脱力は、生存曲線での比較で有意に肢 10) 高 CK 血症である。 帯型より早く障害された。 11) 心機能は保たれる。 12) 呼吸機能が低下していく傾向がある。 Ⅸ.ジスフェルリン異常症が疑われる患者の血清 CK 値 11) 【考 察】 ジスフェルリン異常症は呼吸障害をきたすため注意を MMD は下腿屈筋の筋力低下から始まる特徴的な筋 要する。 障害の分布をしめす。常染色体劣性遺伝形式でジスフェ ルリンが原因遺伝子である。本研究では臨床的に MMD 【結 論】 であるが遺伝子変異の確定しなかった患者の検討を行 日本人に多くみられる変異に発症の遅いものが見つ った。 かったことは今後の研究を進めるうえで重要と思われる。 【方 法】 インフォームドコンセントを得た後に、ゲノム DNA から Ⅷ . 日 本 人 MMD の 遺 伝 子 変 異 の 特 徴 と 自 然 歴 55 個のエクソンごとに PCR-SSCP 法にて遺伝子変異をス ―LGMD2B 型との比較―10) クリーニングし、直接塩基配列決定法にて確認した。この 方法でジスフェルリン遺伝子変異の確定しなかったもの MMD の遺伝子変異の特徴と自然歴を同じくジスフェ の、筋障害の分布が MMD のもの 16 人とそれ以外でジ ルリンが原因遺伝子である LGMD2B 型と比較することに スフェルリンの免疫染色が異常なもの 6 人を対象にした。 より明らかにする。 これらの血清 CK 値を遺伝子変異が確定した 78 人の血 61 清 CK 値と罹病期間を考慮し(10 年で 1,000IU/l、27 年 【結 果】 で 800IU/l、37 年で 427IU/l を下限)比較した。 最終検査時の年齢は平均 59.6(38-83)歳。平均罹病 期間は 35.9(5-60)年。最初の検査時の平均罹病期間 は 14.4(2-48)年。血清 CK は初期は 10,000U/l 代から 【結 果】 指数関数的に減少していき発症 40-50 年で正常化した。 筋障害の分布が MMD のものの 5 人で血清 CK 値が 低かった。1 人は免疫染色が陰性ではない異常だった。 ステロイド内服時や体調悪化時に急激に減少した。初期 1 人は c.2997G>T 変異が 1 アレル見つかっていた。 は血清 AST は 100U/l 代、血清 ALT は 200U/l 代でいず MMD 以外は 2 人で血清 CK 値が低かった。2 人とも免 れも指数関数的に減少していき発症 20-40 年で正常化 疫染色が陰性ではない異常だった。 した。血清 LDH は初期は 1,000U/l 代で指数関数的に減 少していき発症 30 年ほどで正常化した。AST、ALT、 【考 察】 LDH は CK よりもばらつきが大きく、体調悪化時に極端 遺伝子変異がみつからない検査方法上の可能性とし なはずれ値を示すことがあった。Cr は初期は正常値で減 て SSCP の感度が低い、プロモーターやイントロンなど未 少していき発症数年から 30 年ほどで正常値以下になっ 検索の部位に変異、大きな欠失や重複の存在などが考 た。ばらつきが大きかった。呼吸機能は%FVC は徐々に えられる。変異が 1 アレル見つかっているものはジスフェ 低下していたが後期まで比較的保たれる群と早期から低 ルリン異常症の可能性が高いと思われるが1人血清 CK 下している群に分かれた。低下している群では非侵襲的 値が低かった。これは血清 CK 値の低くなる c.2997G>T 人工呼吸を行っていた。動脈血ガスはほとんどが、pCO2 変異だったため判断が難しい。免疫染色が陰性のものに は 40mmHg 以上で pO2 は 80mmHg 以下だった。動脈 血清 CK 値が低いものはなかった。これもジスフェルリン 血ガスは人工呼吸や酸素吸入の影響を大きく受けた。 異常症の可能性が高いと思われる。免疫染色が陰性で はない異常の 4 人中 3 人は血清 CK 値が低くジスフェル 【結 論】 リン異常症とするには慎重さを要すると思われた。筋障害 ジスフェルリン異常症の長期の経時的筋原性酵素と呼 の分布が MMD のものでも免疫染色が正常や血清 CK 吸機能の推移を明らかにした。呼吸機能は正常ではなく、 値の低いも のがあ った 。 ジ スフェ ルリ ン 異常症 である 非侵襲的人工呼吸を行う必要もあり注意を要する。 Miyoshi muscular dystrophy (MMD)1 以外に MMD212)や MMD312)13)も知られており他の原因遺伝子も考慮すべき 必要がある。 Ⅺ.LGMD2A 型の1例―2B 型との比較―15) 症例は 65 歳女性.常染色体劣性遺伝形式に矛盾し Ⅹ.ジスフェルリン異常症の長期の経時的筋原性酵素と ない家族歴。27 歳走るのが遅いで発症。50 歳杖歩行。 呼吸機能の推移 14) 56 歳車いす使用。57 歳初診時 CK 651 IU/l。顔以外の 近位優位筋力低下、筋委縮。Calpain-3 遺伝子の intoron ジスフェルリン異常症において長期にわたる筋原性酵 10 に c.1354+1G>T と exon 20 に c.2120A>G 変異が見 素と呼吸機能の推移を明らかにする。 つかり診断された。カルパイン異常症には簡便なスクリー ニング法がなく、本邦で LGMD2A 型は LGMD2B と並ん 【方 法】 で多い。そのため LGMD2A の特徴をより明らかにするた ジスフェルリン遺伝子変異の確定した 15 人のジスフェ め LGMD2B と比較した。本症例は LGMD2B と比べ近 ルリン異常症患者を対象にした。遺伝子診断はインフォ 位筋優位、進行が遅い、血清 CK 値が低い、肺活量が保 ームドコンセントを得た後に、ゲノム DNA の PCR 産物を たれる。多数例の比較により LGMD2A の特徴がより明確 直接塩基配列決定した。患者の診療録を後方視的に観 になるであろう。 察し、筋原性酵素は血清 CK、AST、ALT、LDH を検討 した。血清クレアチニン(Cr)も検討した。呼吸機能は%努 Ⅻ.Poxamer 188 の持続投与がジスフェルリン欠損 SJL 力性肺活量(%FVC)、動脈血ガス分析を観た。 マウスの過負荷による筋委縮を減少させる 16) 62 ジスフェルリンが欠損している SJL マウスはジスフェル involvement. Muscle and Nerve. 2012; 45: 298-299. リン異常症の研究に用いられる。膜修復剤の poloxamer 7) 和田千鶴、小原講二、阿部エリカ他.認知症を伴っ 188 はポンプによる 6 週間の投与で SJL マウスの筋委縮 た肢帯型筋ジストロフィー2B 型の 1 家系.臨床神経 の減少に効果があることを示した。2 週間の投与では変 学.2013; 53: 754. 化が見られなかったことから poloxamer 188 は長期間の 8) Takahashi T, Aoki M, Suzuki N, et al. Clinical features 投与が必要と思われた。また回転ゲージによる and a mutation with late onset of limb girdle muscular poloxamer 188 を投与した SJL マウスの運動持久力も調 dystrophy 2B. Journal of Neurol, Neurosurgery, and べた。poloxamer 188 を投与した SJL でリン酸化 p38 が減 Psychiatry. 2013; 84: 433-440. 少した。マイクロアレイの解析で筋委縮に関与する E3 ユ 9) 髙橋俊明.Dysferlinopathy.内野誠監修,青木正志 ビキチンリガーゼの atrogin-1 の発現が減っていた。SJL 編集,筋疾患診療ハンドブック.東京,中外医学社. マウスへの持続的な poloxamer 188 の投与が筋委縮を減 2013; 145-151. 少させ、腓腹筋の p38 や atrogin-1 に働くことで運動機能 10) 髙橋俊明,青木正志,鈴木直輝他.日本人三好型 を改善させる。これらの結果はジスフェルリンが欠損した 遠位型筋ジストロフィーの遺伝子変異の特徴と自然 筋線維への治療に役立つものと思われる。 歴―肢帯型筋ジストロフィー2B 型との比較―.臨床 神経学.2011; 51: 1301. 11) 髙橋俊明,鈴木直輝,加藤昌昭他.Dysferlinopathy 【Remudy への登録促進活動】 が疑われる患者の血清 CK 値.臨床神経学.2012; 52: 1548. 国立病院機構あきた病院の小林道雄分担研究者らと 12) Linssen WHJP, de Visser M, Notermans NC, et al. 共同で、Remudy の患者対象アンケート調査を行った。 Genetic heterogeneity in Miyoshi-type distal muscular dystrophy. Neuromuscular Disorders. 1998; 8: 317320. 【参考文献】 13) Bolduc V, Marlow G, Boycott KM, et al. Recessive 1) Liu J, Aoki M, Illa I, et al. Dysferlin, a novel skeletal mutations in the putative calcium-activated chloride muscle gene, is mutated in Miyoshi myopathy and channel Anoctamin 5 cause proximal LGMD2L and limb girdle muscular dystrophy. Nature Genetics. distal MMD3 muscular dystrophies. American Journal 1998; 20: 31-36. of Human Genetics. 2010; 86: 213-221. 14) 髙橋俊明,加藤昌昭,竪山真規他.Dysferlinopathy 2) Takahashi T, Aoki M, Tateyama M, et al. Dysfelin mutations in Japanese Miyoshi 患者の長期の経時的筋原性酵素と呼吸機能の推移. myopathy: 臨床神経学.2013; 53: 1580. Relationship to phenotype. Neurology. 2003; 60: 15) 髙橋俊明,田中洋康,吉岡勝他.肢帯型筋ジストロ 1799-1804. 3) 井泉瑠美子,新堀哲也,青木洋子他.Myofibrillar フィー2A 型の 1 例―2B 型との比較―.臨床神経学. myopathy の大家系での次世代シークエンサーを用 2012; 52: 123. いた原因遺伝子の同定. 臨床神経学. 2013; 53: 16) Suzuki N, Akiyama T, Takahashi T, et al. Continuous 2013. administration of poloxamer 188 reduces overload- 4) Abe K, Kobayashi K, Chida K, et al. Dominantly induced muscular atrophy in dysferlin-deficient SJL inherited cytoplasmic body myopathy in a Japanese mice. Neuroscience Research. 2012; 72: 181-186. kindred. Tohoku Journal of Experimental Medicine. 1993; 170: 261-272. 5) Fahmy N, Abd El-Hady A, Abd El-Naser A, et al. First dysferlinopathy pathological patients and in genetic Egypt: Clinical, characteristics. Neuromuscular Disorders. 2011; 21: 677. 6) Suzuki N, Takahashi T, Suzuki Y, et al. An autopsy case of a dysferlinopathy patient with cardiac 63 Ⅵ. 新規対象疾患レジストリーへの応用 GNE ミオパチー(縁 取 り空 胞 を伴 う遠 位 型 ミオパチー) 患 者 登 録 システム確 立 のための試 み 森 ま ど か * 研究センター倫理委員会の承認を得ている。 【緒 言】 目的)縁取り空胞を伴う遠位型ミオパチー(DMRV)は 取り扱う情報は、遺伝子解析の結果を含む個人情報 本邦に多く集積するミオパチーで、シアル酸補充による であり、個人情報管理については十分な配慮を行った。 治療法の有効性が示され、国内外で臨床治験が開始さ 本研究は厚生労働省・文部科学省「疫学研究に関する れて い る。 (ClinicalTrials.gov Identifier: NCT01236898, 倫理指針」を準拠し、行政機関の保有する個人情報の保 NCT01359319)。数年以内に実施されると予想される II, 護に関する法律を遵守した。 III 相国内治験の実施をより効率的に行い、患者・製薬会 【研究結果】 社・研究者へ情報提供するため、筋ジストロフィー患者登 録システム Remudy で GNE ミオパチー患者登録システ 1. 登録項目の選定 71 名の患者アンケートから、発症年齢は約 25 歳(12- ムを構築し、治験促進の試みを開始した。 58 歳)、患者の半数は歩行不能、発症から歩行喪失まで 【研究方法】 17 年であることが判明した。遺伝子変異ごとの表現型の Remudy の dystrophin 異常症のシステムを拡張し、新 相違が疑われた[1]。モデルマウスの表現型から、心筋障 たな疾患登録を開始した。患者自身による登録を行うシ 害と呼吸筋障害の存在が疑われた[2]。後ろ向きカルテ ステムとし、患者には、NCNP ホームページ、Remudy 患 調査から、歩行不能患者の一部に重度の呼吸障害を認 者登録サイト、筋ジストロフィー研究班、患者団体を通じ め、クレアチンキナーゼ(CK)値と相関することが判明し て登録手順を周知、登録に必要な書類等を入手可能と た[3]。前向き自然歴調査から、歩行機能と握力が進行の した。登録患者への情報提供として、ニュースレター、ホ 把握に有用と考えた。これらを総合して、登録項目を身 ームページを通じ、治験情報を患者に提供することを可 長・体重・遺伝子変異・家族歴・発症年齢・歩行の可否と 能とした。登録された患者情報は、開示委員会における 歩行不能時期・CK 値・握力・肺活量・心機能とした(表 1)。 承認を得た後に開示することとした。 データ解析に当たり、ヘテロ接合の患者では筋生検で縁 登録項目の決定のため、病状のより詳細な検討が必 どり空胞を伴い、GNE ミオパチーと臨床的に診断されて 要と考えられ、GNE ミオパチーに関する文献・GNE ミオ いる症例のみを解析した。 パチー患者アンケート、モデルマウスによる検討および 2. 登録後の状況 国立精神・神経医療研究センター病院患者のカルテ後 1) 登録人数:2012 年 6 月より登録を開始し、2013 年 向き研究および前向き自然歴研究の結果を参照した。 10 月末までに 140 名の登録患者を受け付け、121 変異部位の記載は GNE-001 (ENST00000377902)を基 人を本登録した (図 1)。39 都道府県 73 施設医師 準に行うこととした。GNE-003 (ENST00000396594)が発 92 名が調査票に記載した(図 2)。 表されたため、記載する際には混乱のないよう留意する。 2) 登録者の現状:現在の年齢 44.8±13 歳、発症年 国内外の臨床専門家・基礎研究者との議論を経て登 齢 27.7±9.6 歳、歩行不能患者 43 %, 努力肺活 録票を作成した。また Remudy 事務局内における事務手 量低下(%FVC<80%)患者 33%と、いずれも過去 続きを決定した。治験実施可能施設への呼びかけを行 の NCNP 患者を中心とした報告より軽症である傾 い、治験施行の際に利用してもらうよう周知活動を行った。 向が見られた。合併症・既往歴として特異的な疾 (倫理面への配慮)患者登録システムの構築と遺伝子検 患は見いだせなかった。心機能の記載があったの 査実施体制(Remudy)・および GNE ミオパチー患者登録 は 32.8%のみであったが、FS, EF とも低下が診ら システムについては、独立行政法人国立精神・神経医療 れる患者はいなかった。呼吸機能検査は 65%に * 独立行政法人国立精神・神経医療研究センター 病院 67 施行されており、発症年齢が若いほど呼吸機能が 低い傾向が見られた。夜間のみ非侵襲的人工呼 吸器を用いている患者が 121 人中 2 名存在した。 3) 遺伝子変異:遺伝子型ではホモ接合 32%, 複合へ テロ接合 65%, ヘテロ接合 3%であった。家族歴 は 32.2%, 血族婚は 9%の患者に見られた。アリル 頻度は V572L 46.1%, D176V 25.2%, C13S 3.9%と 過去の報告と同様だった。 4) 広報・治験サポート活動: Remudy 通信に疾患情 報、健康維持のためのアドバイス等患者に有用と 思われる記事を毎号配信した。特に呼吸機能低 下について注意喚起し、Remudy 通信で配布した。 図 3. 治験情報提供 また、東北大学で開始される GNE ミオパチー追加 第一相治験の情報を提供し、患者リクルートに貢 【考 察】 献した。(図 3) 5) 国際協調:Treat NMD が 2012 年から開始した GNE ミオパチー患者は国内には 300-400 名程度の患 GNE ミオパチー国際登録事業(NCT01784679)に 者が存在すると考えられる。今後は年度ごとに経時変化 おいて、日本人および日本語利用者を Remudy を追い、概略的な自然歴調査を行うため更新用紙を発 登録で集計し、匿名データとして解析を行う国際 行し、情報を更新する。定期的に書面やホームページ、 共同研究に参加予定であり現在進行している。 ニュースレター、メール等を用いて、治験情報や病態の 啓発を行う。呼吸機能障害については早期に啓発文書 の配布を行ったが、生命に関わることで有るにもかかわら ず周知度が低いため繰り返し情報提供する。 GNE ミオパチーの患者登録制度は世界初である。今 後は TREAT-NMD など国際的な神経・筋疾患の治験を 前提とした患者登録システムとの協調を行うために具体 的な構築を行う。 【結 論】 GNE ミオパチー患者登録制度を開始した。患者登録 制度は病態や自然歴の解明、患者や医師の啓発、治験 図 1. 登録依頼者数 のリクルートに有用であり、今後もさらに発展的な活動を 2013 年 10 月末までに 140 名 継続する。 【健康危険情報】 特になし 【研究発表】 1. 論文発表 [1]Heterozygous UDP-GlcNAc 2-epimerase and Nacetylmannosamine kinase domain mutations in the GNE gene result in a less severe GNE myopathy phenotype compared to homozygous acetylmannosamine kinase domain mutations. 図 2. 都道府県別の登録依頼者数 NJ Neurol Sci.2012 ; 318 : 100-105. Mori-Yoshimura M, 68 Monma K, Suzuki N, Aoki M, Kumamoto T, Tanaka K, Tomimitsu H, Nakano S, Sonoo M, Shimizu J, Sugie K, Nakamura H, Oya Y, Hayashi YK, Malicdan MC, Noguchi S, Murata M, Nishino I. [2]Respiratory dysfunction in patients severely affected by GNE myopathy (distal myopathy with rimmed vacuoles). Neuromuscul Disord. 2013;1:84-88 MoriYoshimura M, Oya Y, Hayashi YK, Noguchi S, Nishino I, Murata M. 2. 学会発表 重症 GNE ミオパチーは呼吸機能低下を生ずる 第 53 回日本神経学会学術大会 東京 2012.05.24 森まど か、大矢寧、西野一三、村田美穂 GNE ミオパチー自然歴研究 第 54 回日本神経学会 学術大会 東京 2013.05.30.森まどか、矢島寛之、米 本直祐、瀬川和彦ほか Respiratory dysfunction of GNE myopathy (Distal myopathy with rimmed vacuoles) The 11th Annual Scientific Meeting of the AsiaOseania Myology Center 京都 2012.06.07 Respiratory dysfunction of GNE myopathy (Distal myopathy with rimmed vacuoles) The17th international meeting of world muscular society Perth, Australia 2012.10.09 【参考文献】 [1] Mori-Yoshimura et al. Heterozygous UDP-GlcNAc 2epimerase and N-acetylmannosamine kinase domain mutations in the GNE gene result in a less severe GNE myopathy phenotype compared to homozygous Nacetylmannosamine kinase domain mutations. J Neurol Sci. 2012 Jul 15;318(1-2):100-105. [2]Malicdan et al. Prophylactic treatment with sialic acid metabolites precludes the development of the myopathic phenotype in the DMRV-hIBM mouse model. Nat Med. 2009 15(6):690-5. [3]Mori-Yoshimura et al. Respiratory dysfunction in patients severely affected by GNE myopathy (distal myopathy with rimmed vacuoles). Neuromuscul Disord. 2013 Jan;23(1):84-8 69 表 1. 登録用紙 70 神 経 ・筋 疾 患 患 者 データベースの登 録 促 進 及 び 患 者 登 録 の研 究 貝 谷 久 宣 * 研究協力者 井原 千琴 *, 大澤 真木子 *, 池上 香織 **, 松木 正道 ** 活動の意義をご理解いただけるよう登録を呼びかけてい 【緒 言】 く予定である。 日本筋ジストロフィー協会(以下、協会)は、一日も早 い治療法開発へ向けた重要な基盤整備活動の一つとし て、2011 年 10 月より、先天性福山型筋ジストロフィーの 医学情報登録活動を行なっている。Remudy や筋ジスト ロフィーに関わる多くの諸先生方のご指導を得ながら、 活動は 3 年目を迎えた。医学情報登録の推進活動を活 動目標の一つとして 2012 年夏に発足した福山型分科会 「ふくやまっこ家族の会」(以下、分科会)の活動も 2 年目 を迎え、会員数(患者数)は 117 名(2014 年 1 月上旬)と なっている。2013 年 7 月より東京女子医大名誉教授の大 澤真木子先生に新機構長へご就任いただき、機構として は新たな段階を迎えつつある。協会が主体となって登録 表 1. 福山型 月別登録数(2013 年 12 月 31 日時点) 活動を開始後、患者家族会活動がどのような展開をみせ ているか、患者登録システムの在り方を考えていく上で 【デュシェンヌ型・ベッカー型の登録通知状況】 重要な記録の一つとなると考える。そうした観点から、登 録状況、登録促進のための活動に加えて、登録者にお 協会会員の Remudy への登録状況把握を目的として、 ける分科会会員数および分科会の最近の活動内容につ ジストロフィノパチーの登録者を対象に、Remudy から案 いてもご報告する。 内を渡していただく方法で、協会へ登録の通知をお願し ている。2014 年 1 月末までに 238 件の登録通知をいた だいた。この数字は Remudy の登録者 1,226 名(2013 年 【福山型の登録状況】 2014 年 1 月 23 日時点で 165 件の登録を受け付けて 12 月末)の約 2 割にあたる。 いる(表 1)。年代別人数は、0~5歳(57 名)、6~10歳 (40 名)、11~15歳(25 名)、16~20歳(27 名)、21~2 【福山型の登録促進のための活動】 5歳(10 名)、26歳以上(6 名)である。当初の目標値であ 2012 年度、登録に関する説明会を開催したが、2013 る“2 年で 200 名(推定国内患者数を 1,000 名とすると約 年度は 2014 年 1 月に、登録の多く見込まれる福岡にお 2 割)”にはやや及ばなかったものの、推定患者数の 2 割 いて、2 月には東京において医学情報登録に関する説 弱のご登録をいただいた。福山型の患者さんやご家族を 明会を開催した。また、韓国にも福山型の患者が報告さ 初め、全国 77 の施設および 97 名の医師にご協力を賜 れていることや、本協会は韓国の筋ジストロフィー協会と っている(2013 年 11 月末)。 交流があることから、今後の国際連携の機会を見据えて、 人口比から登録の多く見込まれる上位 5 ヶ所は、福岡 登録用紙の韓国語版を作成した。 県・神奈川県・東京都・静岡県・北海道、また、全く登録 のない県は 9 県となっている。今後も引き続き、こうした登 【福山型の施設利用状況調査結果のお知らせ】 録の見込まれる県、及び協会会員以外の方々にも登録 2013 年 2 月に、福山型の医療と福祉に関する施設情 * 一般社団法人日本筋ジストロフィー協会 ** 一般社団法人日本筋ジストロフィー協会 分科会ふくやまっこ家族の会 71 報の集約を目的として、調査時点の全登録者 115 名のご 家族を対象とした施設利用状況を尋ねる自記式・無記 名・郵送のアンケート調査を実施した。今年度は本調査 報告書を配布時点の全登録者に郵送し、福山型分科会 のホームページ内の協会員限定閲覧ページに掲載した。 アンケートで寄せられた 140 件を超える疑問・要望に関し ては今後分科会活動に活用し、確認できたものからホー ムページ内の協会員限定閲覧ページにて回答していく 予定である。また、回答いただいた方からは、登録した後 に福山型に関するアンケートに回答するといった活動が あることで、登録のメリットを継続して感じられるという声も 寄せられており、2013 年 3 月以降に登録いただいた方々 についても同じ調査を実施予定である。登録には手間や ご負担もあることから、登録しているご家族にとって、登録 活動に参加していることのメリットを意識できるような取り 組みは必要と考えられ、今後もこのような取り組みを継続 していきたい。 【福山型分科会の活動】 2013 年 12 月より、分科会では HP「ふくやまっこ広場」 の会員限定閲覧ページの「先生教えて」のコーナーで、 福山型によくある症状とその対策について、東京女子医 科大学病院の石垣景子先生にご協力いただいて公開を 開始した。まだ福山型のことをよくご存知ない医療機関も 多くあるという声があり、まずは会員自身が正しい知識を 身につけるべく活動をしている。そして、日常の工夫など の情報を共有する場として「センパイ教えて」のコーナー も公開を開始した。直接的に登録活動と関係はないが、 このような分科会からの情報発信が、登録や登録情報の 更新への動機づけとしても機能していくことが期待される。 また、分科会としては、登録しない意思も尊重しつつ、 登録しやすい環境づくりに努めている。実際、分科会会 員で登録していない方々は 4 割弱という状況で、登録活 動以外の活動も支持を得ていることが伺える。 【登録者における福山型分科会会員数】 登録者数 165 名中 78 名(47%)は分科会会員(協会 会員であることは必須でない)だった(2014 年 1 月時点)。 会員・非会員を問わず、分科会会員と登録者数合わせ て 204 名(重複を除外した分科会会員数と登録者数の総 数)の患者さんに福山型に関する情報を届けることが可 能となった。 72 Ⅶ. 国際協調・難治性希少疾患全体を俯瞰した展開 筋 ジストロフィーの臨 床 試 験 実 施 体 制 構 築 に関 する研 究 水 島 洋 * 研究協力者 田辺 麻衣 **, 金谷 泰宏 ** 【研究要旨】 ーシアム会合に参加して情報収集を行い、さらに関係者 希少疾患・難病は症例数が少ないがゆえに、その対 との面談も行った。 策や薬の開発などにおいてひとつの国では限度があり、 (倫理面への配慮) 国際的な共同研究や連携が重要である。特に疾患登録 については、病気の対策を行う上で、さらに新薬の開発 この研究においては、医療行為や個人の医療情報に を行う上でも重要な機能をはたすものの、なかなか進ん 関する取扱いは行っていないため、倫理面に関する手 でいない。欧州や米国における希少疾患登録に関する 続きは行っていないが、必要になった場合にはすみやか 調査に加え、国際的な取組に関する調査を行い、それぞ な手続きを行う。 れの特徴を比較し、日本における患者登録のあるべく要 【結 果】 件を検討した。 1.患者登録の種類 Abstract 患者登録は実施主体別に、国・地域・学会や大学・製 Rare diseases need to have international collaboration and international research, as it is rare and one country don’t 薬会社・患者会・企業に分けられる。 have enough patient numbers. Patient registry is key for the 国による希少疾患患者の登録を行っているところは、 policy making and drug discovery for rare diseases, すべての疾患について行っている北欧などを除くと日本 however, it is not well organized. This paper reports about とイタリアであり、現在フランスやスペインで準備が行われ the current status of patient registry in US and Eurpean ている。 countries. 日本では特定疾患治療研究事業として 1978 年から開始 され、現在 56 疾患に関して毎年約 70 万人の登録があ る。ただ、法的な根拠はなく、患者の治療費の補助という 福祉目的を併せ持っているためにデータが重症化傾向 【目 的】 筋ジストロフィー臨床試験の基盤を整備する支援を行 で記載される課題があり、紙ベースでの記載を毎年行う うため、特に国際的な登録に関する情報収集を行い、相 ことによる医師および都道府県における入力も課題にな 互連携可能な形での登録を検討する。 っている。そのため、難病対策の抜本的改革が予定され ており、その中では難病指定医が直接ネット上のシステ ムに情報を登録することによって、精度の向上を図ること 【方 法】 を予定している。 欧州に関しては欧州委員会希少疾患専門家委員会、 オーファネット、患者団体連合(EURODIS)等を訪問して 患者登録の多くは学会や研究会、大学の研究プロジ の情報収集をするとともに、インターネット上にある情報 ェクトなどで行われているが、研究費が単年度であるうえ を集めた。患者登録プロジェクト(EPIRARE)については に担当教授の退官など、継続性の課題がある。 最近、患者の声を直接吸い上げる仕組みとして患者会 イタリアにおける会合に参加して情報収集行う。 米国に関しては、国立保健研究所(NIH)にある希少疾 による登録がはじまっている。さくら会が厚労科研ではじ 患研究事務局(ORDR)や医薬食品局(FDA)等の情報 めた「We Are Here」というサイトでは、ライフヒストリーを時 収集をするとともに、インターネット上にある情報を集めた。 系列的に登録でき、Patient Reported Outcome による評価 国際的な取り組みに関しては、国際希少疾患研究コンソ 指標を実現にするとともに、患者同士で知恵や苦労話を * 国立保健医療科学院 研究情報支援研究センター ** 国立保健医療科学院 75 分かち合うサイトなどを行っている。 究室(ORDR)は本年よりトランスレーショナル研究推進セ ンター(NCATS)の所属になり、主に希少疾患研究の推 進のための調整や情報提供を行っている。 2.欧州における希少疾患対策 欧州における希少疾患の定義は、患者数が 1 万人に 患者登録に関しても直接行わず、患者団体による登録を 5 人以下で、有効な治療法が未確立であり、生活に重大 支援し、ORDR として標準的な形式で収集を進める体制 な困難を及ぼす非常に重傷な状態であることとされてい と し て 、 Global Rare Disease Patient Registry and Data る。2009 年の欧州委員会(EU)の決定に基づいて EU 内 Repository (GRDR)という仕組みを 2012 年に開始した。 に欧州委員会希少疾患専門家委員会(European Union 患者の重複を避けるための一意になる GUID を採用し、 Committee of Experts on Rare Diseases: EUCERD)が立ち 患者会主導による患者による登録システムの共通プラッ 上がった。ここで様々な国際協調政策が行われている。 トフォームとしている。患者登録で問題となる医学的な品 その中の 1 つのプロジェクトに、患者登録プロジェクト 質については、医療関係者がバリデーションを行うように (EPIRARE)がある。希少疾患患者の登録に関しての実 指導している。このシステムを共同開発している Patient 態調査を行い、その範囲やデータ項目などの整理を行 Crossroad 社によると、すでに多くの患者会で採用され、 ったうえで、最終的には統一した登録システムの構築を 治験情報や症状に会った生活の工夫など、患者の興味 目指すという、プロジェクトである。欧州には約 500 の登 に従った情報を提供することで患者自身による日常の情 録プロジェクトがあると言われており、同じ疾患でも各国、 報を入力してもらえることや、治験情報の提供やリクルー 各地域で構築されている場合もある。これらを整理するこ トなど創薬への推進にも役立っている。 とで、共通登録項目や、その体系などの標準化を行うこと 一方、米国では民間による登録も進んでいる。Patients は重要である。2012 年 10 月にはローマで Workshop が Like Me(PLM)社では、自分と似た症状を示す患者さん 開催され、現在の調査の進捗や共通項目に関する議論 との情報共有をコンセプトとして、ソーシャルネットワーキ などが行われた。しかし、現状の登録を把握することにと ング型のサイトを立ち上げている。自分の症状や疾患に どまっており、共通登録システムを提言するには至ってい 関する登録を行うことで、会員の中で似た症状に悩む人 ない。 たちの情報を見て共有することで自分に役立てたり、交 欧州における新しいプロジェクトとして、RD-Connect が 流したりすることができる。診断や症状、検査値、服薬記 2012 年秋に 6 年間のプロジェクトとしてスタートした。オミ 録など様々な情報をタイムライン上に表示することができ ックスデータベース、患者登録、バイオバンク、情報ツー るので自分の体調管理にも活用できる。 ルなどに関して加盟組織の横断的検索を可能にするも ので、現在 19 か国、44 機関が参加している。代表は筋 4.国際的な研究協力体制 ジストロフィーの登録を行っていた TREAT-NMD の代表 2011 年 4 月、EU と NIH が中心となって、国際的に研 Hanns Lochmüller 氏であり、この枠組みの中で各国の患 究を推進するために、「国際希少疾患研究コンソーシア 者登録の共通化を図ろうという動きが活発になっている。 ム」(IRDiRC)が設立された。5 年間に約 100 億円以上の イタリアでは地域ごとに登録センターがあり、ここで情報 研究費を配分している機関を参加条件にしている。現在、 が入力された後、匿名化情報が国の保健省の研究所 15 カ国(地域)、34 機関が正式加盟している。定期的な会 (ISS)に集約される形で把握されている。 合と研究情報や研究資源の情報交換が中心で、加盟費 スペインでも希少疾患の登録が 2012 年からのプロジェク 用などの必要もなく、研究資源の提供義務などもない。 トとして SpainRDR が行われており、国(カルロス三世保 EU や 米 国 に お け る 各 種 の プ ロ ジ ェ ク ト で は 、 今 後 健研究所)としての登録に加え、地域ごとの登録や、6 つ IRDiRC で調整される研究方針にしたがって標準化され の学会、4 つの研究ネットワークなどが参加し、様々な面 たデータ項目などでの情報収集や情報連携を行ってい からの登録を支援している。 く方針を示しており、今後、この組織が希少疾患・難病研 フランスでも新しい希少疾患対策の一環としての登録が 究の中心的役割を演じてくる体制作りが進んでいる。 準備されており、現在その項目に関する調整が行われて 参加機関からなる Executive Committee が意思決定組織 いる。 であり、その下に Diagnostics, Interdisciplinary, Therapies の 3 つの Scientific Committee がある。さらに 12 のワー キンググループがあり、それぞれの課題に関する議論を 3.米国における希少疾患対策 米国国立健康研究所(NIH)に設置された希少疾患研 行っている。 76 Genome/Phenome, Model Systems, Sequencing, 希少疾患にとって、国際協調は極めて重要である。これ Biobanks, Data sharing and bioinformatics, Ethics and まで欧州における国際協調や米国における取組などが governance, Registries an natural history, Biomarkers for 行われてきたが、IRDiRC など世界的規模での協調が開 disease progression and therapy response, Biotechnology- 始されたところである。 derived products including cell- & gene-based therapies, アジア各国のこれらの動きに同調する意向を示している Chemically-derived 中、難病研究に関する長年の歴史のある日本に、アジア Ontologies and Disease Prioritization, products including repurposing, Orphan drug-development and regulatory processes であ における中心的な立場を欧米では期待ている。 る。 【研究発表】 2013 年 4 月にはアイルランドのダブリンにおいて第 1 回 のカンファランスが開催された。希少疾患に関する各種 (平成 25 年度分) の課題を網羅する講演発表や会合が開かれた。 1.論文発表 現在、IRDiRC の会長はカナダの Paul Lasko 教授である 1. 原著論文 が、2014 年 1 月に来日し、精神神経医療研究センター 1) Kikuchi A, Ishikawa T, Mogushi K, Ishiguro M, や日本の希少疾患の連絡会で講演し、製薬協などに Iida S, Mizushima H, Uetake H, Tanaka H, IRDiRC に関する説明と加盟に関する打ち合わせを行っ Sugihara K. Identification of NUCKS1 as a た。 colorectal cancer prognostic marker through integrated expression and copy number analysis. 【考 察】 Int J Cancer. 2013 May 15;132(10):2295-302. doi: 国際的な治験がなされようとしているものの、データ項 10.1002/ijc.27911.PubMed PMID: 23065711. 目の統一などはいまだ進んでいない現状がわかった。 2) 水島 洋 電子機器による環境制御:移動体通 希少性がゆえに研究や臨床研究がむずかしい希少性疾 信 端 末 と ク ラ ウ ド の 可 能 性 と 課 題 Journal of 患・難病について、難病として対策や研究の歴史が長い Clinical Rehabilitation 2013.Oct; 日本としては、諸外国との研究協力や情報交換を活発に 22 (10):1043-47 する必要がある。 3) Mizushima H. Ishimine Y. Kanatani Y., A health この意味で、IRDiRC 参加によって研究情報交換による support system of disaster management using the 国際共同研究及び国際共同治験の推進を行うことが重 cloud. World Disaster Report 2013 (Patrick Vinck 要である。 Ed.)pp.81-83 (2013.Nov) 患者情報を国際的に連携させるためには、収集する データ項目を整合させる必要がある。それぞれの特性の 2.学会発表 ためにすべでのデータ項目を合わせることはできないが、 1) 水島 洋 医療情報データベースと希少疾患治療 最低限集めるデータ(最小データセット Minimum Data 薬の開発 希少疾患連絡会 (2013.4.2 東京) Set: MDS )を定義して合わせることは重要である。また、 2) 水島 洋 、田村麻衣、伊藤篤史、金谷 泰宏 難 同じ患者を 1 つの ID に統一するための仕組みも必要で 病・災害ネットワークの可能性-医療用閉域ネットワ ある。現在、米国 GRDR や EpiRARE、フランスの新登録 ークとクラウド型災害時情報共有システム 第 33 システムでは、MDS を定義しているが、すべて一致して 回インターネット技術研究委員会研究発表会 いるわけではない。ただ、いずれも Global User ID(GUID) (2013.5.24 大阪) に必要な項目は収集することにしている。 出生時の姓 3) 水島 洋 金谷泰宏 モバイルを活用した災害時 名、生年月日、性別、出生市である。これらを用いたハッ における情報共有システム IT ヘルスケア学会 シュ関数で定義される GUID で共通化することが可能に (2013.6.29 東京) なるように調整されており、Remudy を含む日本の登録に 4) 水島 洋 患者参加による創薬支援プロジェクト おいても最低限これらの調整はすべきである。 モバイルヘルスシンポジウム(2013.6.29 東京) 5) 田辺麻衣 金谷泰宏 水島 洋 難病登録の現状 と課題 IT ヘルスケア学会(2013.6.29 東京) 【結 論】 6) 水島 洋 国際的な患者登録の現状 難病・希少 患者数が少ないために対策も研究開発も遅れている 疾患患者登録国際ワークショップ(2013.7.26 東京) 77 7) 水島 洋 医療クラウドの要件 クラウド医療・健 康・福祉フォーラム(2013.8.30 東京) 8) 水島 洋、金谷泰宏 H-CRISIS の現状と今後 全 国保健所長会 総会(2013.10.22 津) 9) 水島 洋、田辺麻衣、金谷泰宏 難病登録の課題 と国際的な動向 日本公衆衛生学会(2013.10.24 津) 10) 田辺麻衣、水島 洋、金谷泰宏 わが国における 稀少・難治性疾患登録の現状と課題 難病医療ネ ットワーク学会(2013.11.9 大阪) 11) 水島 洋 飯島久美子 長寿遺伝子・がん関連遺 伝子の mRNA 解析検査の新提案 臨床ゲノム医 療学会(2013.11.23 大阪) 12) 水島 洋 インターネットによる難病・希少疾患情 報の現状と課題 JIMA インターネット医療フォー ラム (2013.12.5 東京) 13) 水島 洋、田辺麻衣、金谷泰宏 難病登録の現 状・課題と国際的な動向 日本臨床薬理学会 (2013.12.6 東京) 14) 水島 洋 田辺麻衣 金谷泰宏 ISO13606 アーキ タイプに基づく難病データベース アーキタイプ研 究会(2014.1.13 東京) 15) 水島 洋 難病・災害のためのクラウド型情報ネット ワーク NORTH イ ン タ ー ネ ッ ト シ ン ポ ジ ウ ム (2014.2.19 札幌) 16) 石峯康浩、水島 洋、金谷泰宏 災害時健康支援 情報共有システムの開発と国立保健医療科学院 の研修における利活用 第 19 回日本集団災害医 学会総会(2014.2.26 東京) 【知的財産権の出願・登録状況】 1.特許取得 なし 2.実用新案登録 なし 3.その他 なし 78 Summary 2 3 -4 Act i vi t y R ep o rt o f a N atio n al Re sea r c h Gro up Orga n ized b y N at io nal Ce nt er o f Ne uro lo g y and P s yc hi atr y ( N CNP ) : Co n str u ct io n o f a p at ie n t re g is tra tio n a nd ge ne ti c d i a g no si s s ys t e m fo r he r ed i tar y ne uro mu s c ula r d i se as e s En Ki mu ra, M.D . P h .D. (P rin cip a l I n v es ti g ato r) Trans la tio n al Med ica l C en ter, N CNP To d eve lo p n e w d r u g f o r th e r ar e d i se a se s, t he p atie n t re gi s tr y h a s b ee n reco g n iz ed as o ne o f t he mo st i mp o r ta n t i n fr as tr u ct ur e to p r o mo te c li n ica l res earc h. D r. K a wa i, a fo r mer p ri n cip le i n v e st i g ato r, la u nc hed R e mu d y: R e gi s tr y o f mu s c ul ar d ys tro p h y a s a n at io nal r e gi s tr y fo r ne uro mu s c ul ar d i so rd ers. To d ev elo p t h is i n fr a str uc t ur e to war d cl i ni cal re sear c h a nd e xp a nd f o r ma n y rar e d is ea se s, we o rga ni zed a Na tio n al r e sea r c h gr o up a nd I b ri efl y s u m mar iz e t he p ro gre s s 2 0 11 /2 0 1 2 /2 0 1 3 /2 0 1 4 p ur s ued b y o ur gr o up . 1 . O pera tio n a nd cu r re nt st a t us o f R e mu d y, a na tio na l pa ti ent reg i stry o f dy st ro p hi no pa t hy, Du ch en ne a n d B e c ker mu s c u la r dy st ro ph ie s ( DM D/B M D) I n 2 0 0 9 , Dr. K a wa i wi t h hi s nat io na l gr o up a nd N CNP h a ve d e ve lo p ed a n atio n al re gi s tr y o f J ap a n ese DMD /B M D p a tie n t s: Re mu d y i n co l lab o r at io n wi th t he J ap a ne se na tio n al mu s c u lar d ys tro p h y re se arc h gr o up s, 2 7 tr ad i tio na l mu s c u lar d ys tr o p h y war d s a nd ho sp i tal s b elo n g in g to t h e N at io na l Ho s p ita l Orga n iz at io n (N HO ) , t h e J ap a ne se M u sc ul ar D ys t ro p h y As so c ia tio n (J MD A) , a nd fi n all y t h e T RE AT NMD al lia n ce. T he d at a b ase i ncl ud e s cl i nic al a n d mo l ec u lar ge ne ti c d at a as we ll a s a ll i te ms req u ired fo r t he T RE AT- NM D gl o b al p a tie n t r e g i str y. As o f J a n ua r y 2 0 1 4 , 1 ,2 4 3 p ati e nt s we re re g i st ere d in th i s d at ab a se. J ap a ne s e Re mu d y D M D/B M D re gi str y s u p p l ied t h e ep id e m io lo gi ca l d ata fo r fe as ib i lit y st ud ie s fo r 11 ti me s , a nd p r o v id ed ti me l y i n fo r ma tio n to r e gi s tra nt s who mi g h t b e el i gib le fo r up co mi n g cl i ni cal tr ia ls in o r d er to ac ce lera te t h e e ffec ti v e r ecr ui t me n t fo r t wo t i me s. T hi s r e gi s tr y d ata i s a l so i nc l ud i n g mo r e d eta il ed k no wl ed ge ab o ut n at ur al hi s to r y, ep id e mio lo g y, a nd cl i nic al c are. A) P ub li c rela t io ns To let p eo p l e k no w ab o ut t h e a ct i vi t y o f R e mu d y, we se n t t he p ap er v ers io n o f “R e mu d y n e ws”, “R e mu d y ne ws le tt er ” b y e - mai l, a nd r e ne wed o ur web si te. We al so to o k t he lo cal le ct ur e mee ti n g s fo r me d ic al p eo p le a nd p ati e nt s, se n t o ut t h e q u es tio n na ire s fo r me d ic al p ro v id er s t hro u g ho u t J a p an in 2 0 1 3 , a nd fo u nd nea r l y 2 6 % o f med i cal p ro vid ers d id no t k no w ab o ut t he R e mu d y a ct i vi t y. B ) E pi de mio lo g i ca l da t a a na ly si s We p ub l is h ed t he c ur r e n t s ta t us o f R e mu d y i n 2 0 1 3 . To take ad va n ta ge o f t he na tio na l d a tab a se , we al so a na l yz ed ep id e mi o l o gi ca l d a ta fr o m t he re gi str y. Fro m a re se arc h q u es tio n r i se n b y t he J ap a n ese DMD g uid eli n e co m mi tt ee me mb er s, we r ep o rte d a lo n g - ter m e ffec t o f c o rtico s tero id t h erap y a m o n g 5 6 0 J ap a ne se DMD p at ie nt s. T h e t i me to lo s s o f a mb u la tio n o f tre at ed gr o up ( n =2 4 5 ) wa s 11 mo n th s lo n g er t ha n t h at o f u n -tr eated gr o up ( n=3 1 5 ) . T his i s a la rge st cro s s - se ct io n al o b j e ct i ve st ud y i n th e wo rld . We al so e st i ma te d th e n u mb er o f DM D p ati e mt s i n J ap a n wa s ab o ut 3 ,5 0 0 , acco rd i n g to th e an n u al n u mb er s o f b o y’s b ir t h d a ta i n J ap a n i n t h e l i fe c har t o f D MD fro m t he N HO ho sp i tal d a tab ase . C) New w eb reg i st ra t io n s y st e m We s t ud ied t h e s a fe a nd e ff ic ie n t wa y o f t he p a tie n t s el f -r e gi str y a nd d ev elo p ed a ne w web b a sed 81 r eg i str at io n s ys te m u nd e r co l lab o r a tio n s wi t h Hit ac hi So l uti o ns, Ltd . T h i s e xce lle n t s ys t e m b e tt er fo r sec u rit y, st ab i li t y, a nd b ett er fo r ap p l yi n g ge ne ral -p urp o se, co uld b e u s efu l fo r o t h er rare d i sea se s in cl ud i n g ma n y p s yc h o - ne ur o lo gi ca l d i so rd er s. D) E sta b li s h me nt o f g e n e a na ly si s sy st e m fo r he redi ta ry ne u ro mu s c ula r di so r de rs Dy st ro p hi no pa t hy ( DM D/B M D) : At t h e e nd o f Dec e mb er 2 0 1 3 , we ha v e we ll a nal yz ed t he d ys t ro p h in g en e i n 3 4 0 o ut o f 3 4 2 c a se s. I n cas e o f si n g le e xo n d el e tio n/d up li ca tio n r ep o r te d b y t he M LPA me t ho d s , t he co rr esp o nd i n g e xo n and th e nei g hb o r e xo n s we r e seq ue nc ed ( 4 1 %) . In c a se o f no d ele tio n /d up l ic atio n rep o rted b y t h e M LPA me t ho d s, wh o le 7 9 e xo n s we r e seq u e nced (5 9 % ) . GNE m yo p at h y ( D is ta l m yo p a t h y wi t h Ri m me d va c uo le s : D M RV): I n mo r e t h a n 3 0 0 G NE m yo p a t h y c a se s, we ha v e a na l yzed t he G NE g en e (6 3 ca se s b et wee n J a n uar y and D ece mb er o f 2 0 1 3 ) , th e n fo u nd 4 1 % o f co n fi r med ho mo z yg o te o r co mp o u nd het ero z yg o te, 3 % o f si n g le mu t at io n o n si n g le al le le, 5 1 % o f no mu tat io n. So me freq ue n t m ut at io n s i n G NE g en e were fo u nd . Oc ulo p h ar yn g ea l mu s c u l ar d ys tr o p h y ( OP MD ) a n d M yo to n ic d ys tro p h y t y p e 1 a nd 2 ( DM1 /2 ): T he PAB P N1 g en e mu t at io n s wer e d e te cted i n 9 9 p atie n t s (8 4 fa mi li e s). T he o p p o s ite co r re lat io n was fo u nd b e t we e n G C N r ep eat n u mb e r s a nd t he a g e o f o ns et. T he ge ne a n al ys i s me t ho d s fo r M yo to ni c d ystro p h y t yp e 1 a nd 2 we r e al so e x a mi n ed . D ys ferl i no p a t h y ( M yo s h i m yo p a t h y, Li mb - g ird le mu sc u lar d ys tro p h y t yp e 2 B , LGMD2 B ) : B y P CR - S S CP met ho d , 4 2 i nd ep e nd e n t mu t at io n s a mo n g a ffect ed 9 1 fa mi l ie s we re d e ter mi n ed , th e n wh o le 5 5 e xo n seq ue n ci n g me t ho d , 3 1 i nd ep e nd en t mu t at io n s a mo n g a ff ected 4 5 fa mi l ie s. We a lso st ud ied t he u se fu l ne s s o f t he n e xt g e ner a tio n s e q ue n ci n g fo r d ys fer l i no p at h y. E) Ap pl ica t io n o f t he reg i st ry f o r o t h er ra re di se a se s G NE my o pa t hy (D ista l my o pa t hy w it h R i mme d v a c uo le s: D M RV): T he n at io nal re g i str y f o r G NE m yo p a t h y la u nc h ed J u ne 2 0 1 2 . T he d a ta se t b et wee n J u ne 2 0 1 2 and No ve mb er 2 0 1 3 wer e a n al yzed . We fo u nd 3 3 % o f re gi s tra n ts to o k re sp i r ato r y fu n ct io n e xa mi n at io n , and s u g g es ted t he co r r e l atio n b et wee n a ge o f o n se t a nd r esp ira to r y d ys f u nc tio n. F u k u ya ma co n ge n it al m u sc u lar d ys t r o p h y (F C M D): T he J ap a ne se M u sc u lar D ys t r o p h y As so cia tio n e st ab l is h ed t he F u k u ya ma co n ge n ita l mu s c u lar d ystro p h y r e gi st r y o n O cto b er 2 0 11 . At J a n uar y 2 3 r d , 2 0 1 4 , 1 6 5 c a nd id at e re gi st ra nt s were acc ep ted . Ev er y year, t h e q ue st io n na ir e s fo r r e g i stra n t s we re se n t o ut, a nd t ho s e res u lt s were r ep o rted at t h e r es earc h gro up me et i n g and J M D A web si te, t h e n we re re flec ted to t he a cti v it y o f t h e b r a nc h me eti n g fo r F CM D p a ti e nt s i n t h e J MD A. M yo to ni c d ys tro p h y a nd o t her m yo to ni a s yn d ro me s : T he arra n ge me nt me et i n g fo r t he M yo to n ic d ys tro p h y r e gi st r y st art ed at F eb r uar y 2 0 1 2 . We h av e p la n ned t he c ur ato r s tr ai ni n g, se t up t he re g is tr y ite ms, a nd co lle cted a nd r e g ula ted t h e e xp e rts ’ o p i nio n s. We p rep ar ed t h e D M r e g i str y o ff ice a t t he d ep ar t me n t o f Ne u r o l o g y, Os a ka U ni v er si t y. N o w, th e ap p l ic at io n o f DM r eg i str y i s u nd er r e vie w b y t he Et h ica l co m mi t te e i n b o t h O sa k a U n i ver s it y and N CNP. F) In ter na t io na l, na t io n - w ide , co lla bo ra t io n fo r r a re di s ea s es B o th i n a nd o ut o f E ur o p e, T RE AT-N MD al li a nc e, a cl i ni ca l re se arc h n et wo r k fo r n e uro mu s c ul ar d iso rd er s, h as d e ve lo p ed a glo b a l d at ab a se fo r D u c he n ne a nd B e ck er mu s c u lar d ys tro p hi e s 82 ( DM D/B M D) p a ti e nt s to p r o mo te cl i nic al tri al s fo r n e w t herap e ut ic st r at eg ie s, as a to o l s to s t ud y t he ep id e mi o lo g y. T h e co l la b o r atio n o f T RE AT-N M D G lo b al re gi s tr y p re se nt ed t h e wo r ld wi d e s tat u s o f DMD /B M D p a ti e nt r e gi s tr ie s i nc l ud i n g g e net ic i n fo r ma t io n. We h a ve a l s o p la n ned to e s tab l i s h o t her t yp e o f mu s c u lar d ys tr o p hi e s a nd m yo p at h ie s, s uc h a s M yo to ni c d ys tro p h y, d ys fer li no p at h y. T he C AR E - NMD f a mi l y s ur ve y i n J ap a n wa s ca rried o ut u nd er co ll ab o r atio n wi t h t he C ARE - N MD in ter n at io na l s ur ve y g r o up a nd t he M u s c ular Di sea s e Ce n ter a t N CNP. T hi s s ur ve y wa s u se fu l fo r gi v i n g t he p a ti e nt i n fo r ma tio n ab o ut t he car e a n d c ure fo r DM D p a ti e nt s . We a l so d is c us s ed t h e r o le o f t h e Re mu d y a m o n g t he r ar e d i s ea se i n fra s tr uc t ur e fo r t he cl i n ica l r es earc h. We to o k e ver y r e gar d i n g me et i n gs, s u ch a s t h e me et i n g fo r r are a nd i nt rac tab le d is e ase s he ld e ver y o t her mo nt h and t h e p r ep ar a tio n mee ti n g s fo r p a tie n t r e gi st ri es i n J a n uar y a nd Feb r u ar y 2 0 1 3 . In t he fir s t i n ter n atio n al wo r ks ho p fo r ra re d i sea se r e gi str ie s i n J ul y 2 0 1 3 , t he i n ter n at i o na l ke y s p ea k er s fro m E u r o p e, t he U n ited St ate s, a nd C hi na were i n v it ed , a nd d o me st ic sp ea k er s wo r k in g fo r t he e ac h p a ti e nt r e g is tr y d i sc u s sed t he co l l ab o rat io n a mo n g t he r ar e d i sea se re gi s trie s. At th e s y mp o si u m i n t he 3 4 t h An n ua l Me et i n g o f T he J ap a n es e So c ie t y o f Cli n ic al P h ar ma co lo g y a nd T herap e u ti cs , we d i sc u s sed t he r o le s a nd t h e rec en t st at u s o f p at ie nt re g i str ie s i n in J ap a n. A mo n g t he se a cti v it ie s, we co n fir med t he har mo n iza tio n o f cl i nic al re sea rch p ati e nt s a nd fa mi l ie s, me d ica l p r o v id er s, a nd o t he r s ta k eho ld er s, s uc h a s p har ma ce ut ica l i nd u s tri es , re se arc her s, p at ie nt ad vo c ac ie s, and t he re g ul ato r y a ge nc y wa s i mp o r t a nt. Pla n fo r n e xt te r m: T he Re mu d y, t h e p at ie n t r e g i str y f o r t he ne uro mu s c u lar d i so rd er s, i s t he fi rs t n at io na l r e gi str y fo r r ar e d is ea se s, wh i c h le ad s to t he cl i ni cal d e ve lo p me nt al s t ud y. We r u n t he R e m u d y s uc ce s s ful l y, b eca u se o f t he ac c ur at e ge n e a nal ys i s s ys te m, co o p erat io n o f p a ti e nt s, fa mi l ie s, ad vo ca c y gro up s, a nd med ic al p ro vid er s, car e f ul l y p la n ned o p er at io n s ys t e m i ncl ud i n g t he s tee ri n g co m mi t te e, as we ll as in ter n at io na l co l lab o r a ti o n. We wi l l co nt i n ue t hi s s ys te m, e xp a nd t he t arg e t d i sea se s, a nd s tep fo r ward to d e ve lo p t he n e w s ys t e m co v er i n g t he wh o l e rar e a nd i n trac tab le d i s ea se s wi t h o t her r es earc h gro up s. T he p a ti e nt re g is tr i e s a r e no w r e co g ni zed a s a us e ful to o l to acc eler a te cl i ni cal re se arc h o f t he var io u s r are d i sea s es. F u r t her, we wi l l p r o mo te t h is i n fr a str uc t ure fo r cl i ni cal re sea rc h to co mp l e m en t th e p i t fa ll o f t h e n at io n al i n tr ac tab le d i se a se re gi s tri es no w b ei n g p la n ned a s o ne o f t he e ffe ct iv e me a s ure s to o v er co me t he m b y t he Mi n i str y o f Hea lt h, Lab o r a nd We l fare, e sp e ci al l y p rep ar ed fo r d ed u ct io n fo r p a ti e nt ’s med ic al e xp e n se s. O ur p ro p o sed ne w r e gi st r y s ys te m wi l l ma k e t he he al t h care ad mi ni s tra tio n o f t he go ver n me nt mo r e sa ti s fact o r y. 83 84 論文 Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 RESEARCH Open Access Characteristics of Japanese Duchenne and Becker muscular dystrophy patients in a novel Japanese national registry of muscular dystrophy (Remudy) Harumasa Nakamura1,3, En Kimura2*, Madoka Mori-Yoshimura3, Hirofumi Komaki4, Yu Matsuda5, Kanako Goto5, Yukiko K Hayashi5, Ichizo Nishino5, Shin‘ichi Takeda6,2 and Mitsuru Kawai7 Abstract Background: Currently, clinical trials for new therapeutic strategies are being planned for Duchenne and Becker muscular dystrophies (DMD/BMD). However, it is difficult to obtain adequate numbers of patients in clinical trials. As solutions to these problems, patient registries are an important resource worldwide, especially in rare diseases such as DMD/BMD. Methods: We developed a national registry of Japanese DMD/BMD patients in collaboration with TREAT-NMD. The registry includes male Japanese DMD/BMD patients whose genetic status has been confirmed by genetic analysis. The registry includes patients throughout Japan. Results: As of February 2012, 583 DMD and 105 BMD patients were registered. Most individuals aged less than 20 years. In terms of genetic mutations of registrants of DMD and BMD, deletion of exons was the most frequent (61.4% and 79.0%) followed by point mutations (24.5% and 14.3%) and duplications (13.6% and 4.8%), respectively. 43.6% of DMD are capable of walking, and 76.2% of BMD registrants are able to walk. 41.1% of DMD registrants in the database were treated using steroids. 29.5% of DMD and 23.8% of BMD registrants were prescribed one cardiac medicine at least. 22% of DMD used ventilator support, and non-invasive support was common. Small numbers of DMD and BMD registrants, only 3.9% and 1.0% of them, have received scoliosis surgery. 57 (9.8%) patients were eligible to clinical trial focused on ‘skipping’ exon 51. Conclusions: The Remudy has already demonstrated utility in clinical researches and standardization of patients care for DMD/BMD. This new DMD/BMD patient registry facilitates the synchronization of clinical drug development in Japan with that in other countries. Keywords: Duchenne and Becker muscular dystrophy, Neuromuscular disorder, National registry, TREAT-NMD, Registry of muscular dystrophy (Remudy), Japan Introduction Duchenne muscular dystrophy (DMD) and Becker muscular dystrophy (BMD) are X-linked recessive forms of muscular dystrophy caused by mutations in the dystrophin gene (DMD) on chromosome Xp21.2 [1]. The DMD gene is the largest gene identified in human and contains 79 exons. Mutations in this gene cause deficiency of normal dystrophin protein [2]. DMD is the most frequently inherited muscular disease, affecting approximately 1 out of 3500 live male new-borns. DMD patients commonly lose their ability to walk before the age of 12 years, coupled with deterioration in respiratory and cardiac functions. DMD is usually fatal in the third decade because of either cardiac or respiratory failure. On the other hand, the course and severity of BMD is more variable [3]. Since the discovery of the dystrophin gene, many efforts have been made to develop effective therapeutic strategies for DMD/BMD. * Correspondence: [email protected] 2 Department of Promoting Clinical Trial and Translational Medicine, Translational Medical Center, National Center of Neurology and Psychiatry, 4-1-1 Ogawa-Higashi, Kodaira, Tokyo 187-8551, Japan Full list of author information is available at the end of the article © 2013 Nakamura et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 87 Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 Page 2 of 7 patients and was made possible by collaboration with the Japan Muscular Dystrophy Association. Clinical trials are now being planned and conducted for DMD/BMD [4-8]; however, many challenges exist with regard to both planning and conducting clinical trials for such rare diseases. Because of limited epidemiological data, the total number of patients, natural history of the disease and clinical outcome measures are unclear. In addition, adequate numbers of patients are needed to achieve significant results in clinical trials. As solutions to these problems, patient registries are an important resource especially in case of rare diseases such as DMD/ BMD. In Europe, Translational Research in Europe–Assessment and Treatment of Neuromuscular Diseases (TREAT-NMD) [9], a research network for neuromuscular disorders, developed a global database for DMD and spinal muscular atrophy (SMA) to obtain epidemiological data; examine the total number of patients; determine the natural history of the disease; determine appropriate clinical outcome measures and collect adequate numbers of patients needed to achieve significant results in clinical trials and inform patients of new drug development as soon as possible. To date, several Japanese DMD/BMD databases have been developed [10-12]; however, these have not been on a broad national scale. For instance, some were on a single-centre basis and others encompassed only a small local area or several hospital sites. Some others were restricted to inpatients only. Despite these early efforts, no national registry has been developed with the purpose of focusing on clinical trials. In 2009, we developed a national registry of Japanese DMD/BMD patients (REgistry of MUscular DYstrophy; Remudy. http://www.remudy. jp/) in collaboration with TREAT-NMD. The purpose of this registry was to effectively recruit eligible patients to new clinical trials and provide timely information to patients about upcoming trials. Registry data also provides more detailed knowledge about the natural history and epidemiology of the disease, as well as information about clinical care. In this paper, we introduce Remudy, the Japanese DMD/BMD registry, and describe the clinical and molecular genetic characteristics of Japanese dystrophinopathy patients. Patients The database includes male Japanese DMD/BMD patients whose genetic status has been confirmed by genetic analysis. The database includes patients throughout Japan. The cost of sequencing analysis of the DMD gene is not covered by the system of the public health insurance in Japan. For patients who intend to register but whose genetic status is not confirmed using multiplex ligationdependent probe amplification (MLPA), Remudy provides free service of sequencing analysis of the DMD gene. Method of registration and data collection Information about the registry was provided to interested individuals and their informed consent was obtained. Provision of all data by patients is voluntary and is not shared with any third party without the permission of the committee responsible for disclosing the information. Inclusion in the database confers no obligation for the patient, and they may be removed from the registry immediately on request. It was stated that refusal to participate would not affect the subsequent medical care of the patient. This study was approved by Institutional Review Board of National Center of Neurology and Psychiatry, Japan. Structure of the registry form Data obtained via the registry form included clinical symptoms, results of biochemistry, muscle biopsy and other laboratory analysis and description of the genetic mutation. Epidemiological information provided includes walking capability, cardiac and respiratory functions, creatine kinase levels, history of scoliosis surgery and steroid therapy status. All these data should be confirmed by molecular and clinical curators in Remudy (three active molecular and three active clinical curators). The structure of the Case Report Form and registry items are shown in Table 1. Information was annually updated by registrant’s self report after their physician’s confirmation following reminder from registration office. To decide whether a patient was classified as DMD or BMD, first, attending physician made a diagnosis whether a patient was DMD or BMD by the clinical and molecular information. Then, when our clinical and genetic curators double-checked their classification by reviewing clinical information, and also data from pathological (including dystrophin immuno-staining, if applicable) and genetic analysis. Materials and methods Institution, organization and leadership Remudy is supported by a Research Grant (20B-12, 23–4) for Nervous and Mental Disorders from the Ministry of Health, Labour and Welfare. The development and management of the registry is led by the principal investigator of the Japanese muscular dystrophy research group. Steering committee members include scientists, clinicians and representatives of patient organizations. The office of the registry of muscular dystrophy was set up within the National Center of Neurology and Psychiatry (NCNP), Tokyo, Japan. This project includes Japanese DMD/BMD Results As of February 2012, 876 Japanese patients across Japan had sought registration, and 583 DMD and 105 BMD patients were registered based on their eligibility as 88 Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 Page 3 of 7 confirmed by clinical and molecular genetic data (Figure 1, Figure 2 and Table 2). Most individuals aged less than 20 years; however, several registered individuals were aged over 35 years. There are five patients between 45 and 49 years old in DMD. The molecular data of four patients are consistent with reading frame rule, and these patients became bedridden with tracheotomy in muscular dystrophy care ward. A molecular data of another patient isn’t consistent with DMD mutation (inframe mutation, del 10–42), however he lost his walking ability in childhood and had a tracheotomy. His attending doctor clinically diagnosed him as DMD. In terms of genetic mutations of registrants of DMD and BMD, deletion of exons was the most frequent (61.4% and 79.0%) followed by point mutations (24.5% and 14.3%) and duplications (13.6% and 4.8%), respectively. Most registered patients lived in cities, namely Tokyo, Osaka and Nagoya (Figure 3). Tables 3 describe the clinical characteristics of Japanese DMD/BMD patients included in the registry. The information collected was similar to that for the core items required for the TREAT-NMD global registry, and thus, we will be able to compare Japanese data with those contained in the global registry. Among the DMD registrants, 43.6% of them are capable of walking. On the other hand, 76.2% of BMD registrants are able to walk. In terms of cardiac and respiratory function, 67.2% of DMD and 72.4% of BMD have normal cardiac function and respiratory functional examination was not performed among half of DMD registrants. It was suggested that many registrants were too young to be tested when they were registered. 41.1% of DMD registrants in the database were treated using steroids. 29.5% of DMD and 23.8% of BMD registrants were prescribed one cardiac medicine at least, and ACE–inhibitor was the most common medicine for cardiac failure. One fifth of DMD used ventilator support, and among the registrants with Table 1 The report form for registry to Remudy Contact Clinical data -Name -Data -ID number -Muscle biopsy -Hospital -Date of birth -Address -Phone •Examed/not examed •Dystrophin immunostain -Walking capability •Ambulant /wheelchair -E-mail -Use steroid therapy -Signed up for other registries -Cardiac function -Attending any clinical trials •LVEF(%) -Registering other database •Medication Diagnosis -DMD/BMD/IMD -Proof of the diagnosis -Respiratory function •FVC •Mechanical support •Genetic confirmed -Scoliosis surgery •Muscle biopsy -CK level •Suspected from family history -Weight •Others Molecular genetic data (certificated report should be attached) -Method •MLPA/Multiplex PCR/southern blot/RTPCR/ Direct sequencing of exons -Type of mutation •Deletion/duplication/others •Details of the mutation DMD, Duchenne muscular dystrophy; BMD, Becker muscular dystrophy; IMD, Intermediate muscular dystrophy; MLPA, Multiplex ligation-dependent probe amplification; LVEF, Left ventricular ejection fraction; FVC, Forced vital capacity; CK, Creatine kinase. Number of patients 180 154 160 162 140 DMD BMD 120 100 80 88 62 56 60 40 20 5 14 28 21 11 7 9 139 126 25 30 0 7 57 03 02 2 0 5 10 15 20 35 40 45 50 55 60 61 Age Figure 1 Ages of registered individuals. Most registrants are under 20 years of age, but those over 35 years with DMD are also registered. 89 Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 Page 4 of 7 160 149 DMD 140 140 119 120 105105 105 100 92 80 74 60 44 40 20 48 46 50 50 52 51 51 48 43 43 45 33 35 47 42 39 37 39 35 33 33 33 33 34 33 33 33 33 31 31 32 29 29 29 29 34 36 28 27 27 27 26 29 18 12 10 12 10 11 11 10 11 12 11 8 10 9 9 10 9 9 9 9 9 9 7 7 7 7 7 0 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 575656 60 BMD 40 33 19 20 0 1 9 9 9 9 9 9 8 8 8 8 8 9 10 9 9 9 9 8 8 8 8 9 8 8 8 8 8 8 8 6 6 5 5 4 7 7 7 4 4 5 5 6 11111010 5 5 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 Figure 2 Frequency of deleted exons observed in registrants with DMD and BMD. Distribution of exon deletion shows common hot spot regions in exons 45–54 in DMD and BMD. been recently conducted in Japan. From the Remudy registry data, 57 (9.8%) patients have mutations theoretically addressable by skipping of exon 51 (Table 4). mechanical ventilation, non-invasive support was common. Small numbers of DMD and BMD registrants, only 3.9% and 1.0% of them, have received scoliosis surgery. The Remudy registry has already demonstrated utility in clinical trials for DMD/BMD. A clinical trial focused on ‘skipping’ exon 51 using antisense oligonucleotides has Discussion The DMD/BMD registry run by Remudy is the one of its kind in Japan specifically targeting neuromuscular diseases. It is the first national registry in Japan to include both clinical and molecular genetic data, and its utility in promoting clinical trials has been demonstrated. Prior to the development of Remudy, some DMD/BMD databases existed in Japan [10-12]; however, they were limited in their coverage and utility. This is the first Japanese DMD/ BMD database aimed at facilitating clinical trials and the first to coordinate with a global database. Since 2011, a worldwide phase III, randomized, doubleblind, placebo-controlled clinical study is being conducted for patients with DMD who have a DMD gene mutation amenable to an exon 51 skip. Partially because of the development of the Remudy database, this trial now includes Japanese sites and is thus the first global clinical trial to become available to Japanese DMD patients. Up until now, clinical trials for DMD under new International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use–Good Table 2 Distribution of mutations in the registrants with DMD and BMD DMD patients BMD patients No. of case % of cases No. of case % of cases Deletion 358 61.4% 83 79.0% Distribution of mutation Duplication 79 13.6% 5 4.8% Deletion and Duplication 1 0.2% 0 0.0% Others * 144 24.7% 15 14.3% No mutation found** 1 0.2% 2 1.9% 583 100.0% 105 100.0% * Others include nonsense mutations, small insertion/deletion mutations, deep intronic mutations, and splice site mutations. ** Their diagnosis was confirmed based on their pathological findings in muscle biopsy including a negative immunohistochemical staining against dystrophin. 90 Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 Page 5 of 7 <5 5 and over 10 and over 20 and over 40 and over Osaka Nagoya Tokyo Figure 3 Prefectural distribution of the registrants. There are 47 prefectures in Japan. Individuals from all rural areas in Japan were registered but most registrants were concentrated in big cities, namely Tokyo, Osaka and Nagoya. has been prolonged [14]. Our findings support this, with the Remudy registry including several individuals over 40 years of age (though most were aged <20 years). 41.1% of DMD patients in the database were treated using steroids. Importantly, this ratio may be relatively low compared to that in western countries, considering that the family guide for the diagnosis and management of DMD became available to download in Japanese in 2011 [15]. Given that this treatment is recommended in the guide, the number of individuals being treated with steroids for DMD may increase in future. Remudy is intended to be used as a public service for the benefit of patients living with neuromuscular diseases. Through participation in the database, patients may be identified as candidates for upcoming clinical trials. In addition, Remudy has provided additional useful resources for patients through a website and newsletter. The information provided via these methods includes the development of new therapeutic compounds, information regarding care standards (known as the Family Guide for the Diagnosis and Management of Duchenne Muscular Dystrophy [15]) and other relevant medical information. In addition, Remudy has facilitated the genetic diagnosis and detailed sequencing analysis of individuals, thereby promoting genetic counseling in family and also providing important information required to determine eligibility for clinical trials. As a result, more dystrophinopathy patients have become aware of the necessity of confirming their diagnosis via analysis of the DMD gene. The development of Remudy is part of a global trend toward database development for neuromuscular disorders. Clinical Practice (ICH-GCP) have not been conducted in Japan. Registry information concerning eligible Japanese individuals was sought by TREAT-NMD and pharmaceutical companies and has been provided with permission. This example demonstrates the usefulness of the registry for facilitating patient access to clinical trials, as well as enhancing recruitment for such trials. Another novel aspect is patient participation in the registration process. Previously, database information was supplied by clinicians. In contrast, the Remudy system enables patients themselves to provide their information to the registry in collaboration with their clinicians. The registry consists of valuable clinical and genetic data, which yields valuable epidemiological information including walking capability, cardiac and respiratory functions, creatine kinase levels, history of scoliosis surgery and steroid therapy status, all of which are needed to plan clinical trials and determine the eligibility of individuals for such trials. This has resulted in Remudy becoming one of the largest and most reliable rare disease registries in Japan. Remudy also reveals the structure of mutations in Japanese DMD/BMD patients. The distribution of mutations and the frequency of individual exon deletion found in our study are consistent with previous reports. In DMD, distribution, duplication and point mutations comprise 61.4%, 13.6% and 24.5%, respectively. Distribution of exon deletions reveals significant region in exons 42–54 (Figure 2). This is similar to the findings of other databases [13] and those of a Japanese study in a single referral centre [11]. Because of improvements in respiratory and cardiac complications, life expectancy of Japanese DMD patients 91 Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 Page 6 of 7 Table 3 Clinical manifestations, medications and intervention characteristics in the registrants with DMD and BMD DMD patients No. of case Table 3 Clinical manifestations, medications and intervention characteristics in the registrants with DMD and BMD (Continued) BMD patients % of No. of cases case Scoliosis surgery % of cases Walking capability Normal walking 254 43.6% 80 76.2% Not able to walk, and sit without support 184 31.6% 19 18.1% Not able to sit without support 145 24.9% 6 5.7% 583 100.0% 392 67.2% 76 72.4% Dysfunction 180 30.9% 28 26.7% 11 1.9% 1 1.0% Normal 65 11.1% 45 42.9% 202 34.6% 18 17.1% Not performed 316 54.2% 42 40.0% 105 100.0% Steroid use Current 171 29.3% 6 5.7% Used to 69 11.8% 6 5.7% 343 58.8% 93 88.6% 583 100.0% 105 100.0% Cardiac medication Prescribed 172 29.5% 25 23.8% Not prescribed 411 70.5% 80 76.2% 583 100.0% 1.0% No 560 96.1% 103 98.1% Not described 0 0.0% 1 1.0% 105 100.0% TREAT-NMD is an excellent network in the field of neuromuscular disorders and has been leading international registry collaboration for many diseases including DMD, spinal muscular atrophy, myotonic dystrophy type 1 and others. Close collaboration with TREAT-NMD has allowed Japan to enhance the management and care of Japanese DMD and BMD patients and facilitated research in neuromuscular disorders. One of the most important outcomes of this collaboration is the development of the Japanese national registry for DMD described in this paper. By collecting common information, the registry data can easily be compared between Japan and other countries. TREAT-NMD has helped to support these efforts by providing an infrastructure that continues to accelerate research, therapy development, and trial readiness in addition to increasing collaboration and improving patient care. Japanese patients, families, physicians and anyone affected by a neuromuscular disorder play a key role in the worldwide neuromuscular community by participating in this collaboration with TREAT-NMD, which is Remudy. The TREAT-NMD global registry has been focused on European countries and the United States; however, it is currently expanding to other countries. Rare disease registries are emerging in Asian countries [16] and Japanese experiences in collaboration with TREAT-NMD and registry development should be able to provide more information about these activities to Asian countries. A global registry 105 100.0% Dysfunction Never 1 *1; The number of registrants who were prescribed with cardiovascular medicines. *2; The number of registrants using ventilator support. Respiratory function 583 100.0% 3.9% 105 100.0% Normal 583 100.0% 23 583 100.0% Cardiac function Not performed Yes 105 100.0% Drug β-blocker 94 54.7% 16 64.0% ACE-inhibitor 140 81.4% 19 76.0% ARB 12 7.0% 5 20.0% Diuretics 43 25.0% 7 28.0% Other 29 16.9% 7 28.0% 172*1 100% 25*1 100% 455 78.0% 103 98.1% 128 22.0% 2 1.9% Mechanical ventilation No Yes 583 100.0% Invasive Non-invasive 20 108 15.6% 84.4% 128*2 100.0% Table 4 Applicable individuals for exon 51 skipping clinical trial 105 100.0% 2 100.0% 0 0.0% 2*2 100.0% No. of individuals % in registrants 45-50 17 2.9% 47-50 0 0.0% 48-50 9 1.5% 49-50 18 3.1% Temporal 71 55.5% 0 Continuous 57 44.5% 2 100.0% 50 6 1.0% 2*2 100.0% 52 7 1.2% 128*2 100.0% 0.0% Deleted exons 92 52-63 0 0.0% total 57 9.8% Nakamura et al. Orphanet Journal of Rare Diseases 2013, 8:60 http://www.ojrd.com/content/8/1/60 Page 7 of 7 for patients with myotonic dystrophy type 1 will be launched in the near future [17]. Several other registries for neuromuscular diseases have been developed worldwide, such as the international congenital muscular dystrophy registry (CMDIR) run by the US patient organization ‘Cure CMD’. Remudy has been developing Japanese registries for other neuromuscular diseases including glucosamine (UDP-N-acetyl)–2-epimerase/Nacetylmannosamine kinase (GNE) myopathy and myotonic dystrophy type 1 (DM1). We have thus demonstrated how this registry can enhance the readiness for clinical trials in Japan, and how this unique form of infrastructure can be used to accelerate international efforts in fighting orphan diseases. 4. Conclusions The Remudy registry has already demonstrated utility in clinical trials and standardization of patients care for DMD/BMD. This new DMD/BMD patient registry will facilitate the synchronization of clinical drug development in Japan with that in other countries. 11. 5. 6. 7. 8. 9. 10. 12. 13. Competing interests The authors declare that they have no competing interests. 14. Authors’ contributions HN and EK participated in planning this study, analysis and interpretation, generation of the tables and figures, in writing of the manuscript. MY and HK participated in curating clinical data and data collection. YM, KG, and YH participating in genetic analysis, curating the molecular data and data collection. IN, ST and MK supervised in planning this study. All authors read and approved of the final manuscript. 15. 16. 17. Acknowledgements Remudy, the Japanese DMD/BMD registry, is supported by a Research Grant (20B-12, 23–4) for Nervous and Mental Disorders from the Ministry of Health, Labor and Welfare. Creation of this registry was made possible by collaboration with TREAT-NMD (EC, 6th FP, proposal #036825; http://www. treat-nmd.eu). We are grateful to the Japan Muscular Dystrophy Association for their collaboration. Van Deutekom JC, Van Ommen GJ: Advances in Duchenne muscular dystrophy gene therapy. Nat Rev Genet 2003, 4:774–783. Guglieri M, Bushby K: Molecular treatments in Duchenne muscular dystrophy. Curr Opin Pharmacol 2010, 10:331–337. Welch EM, Barton ER, Zhuo J, Tomizawa Y, Friesen WJ, Trifillis P, Paushkin S, Patel M, Trotta CR, Hwang S, et al: PTC124 targets genetic disorders caused by nonsense mutations. Nature 2007, 447:87–91. Van Deutekom JC, Janson AA, Ginjaar IB, Frankhuizen WS, Aartsma-Rus A, Bremmer-Bout M, den Dunnen JT, Koop K, van der Kooi AJ, Goemans NM, et al: Local dystrophin restoration with antisense oligonucleotide PRO051. N Engl J Med 2007, 357:2677–2686. Goemans NM, Tulinius M, van den Akker JT, Burm BE, Ekhart PF, Heuvelmans N, Holling T, Janson AA, Platenburg GJ, Sipkens JA, et al: Systemic administration of PRO051 in Duchenne’s muscular dystrophy. N Engl J Med 2011, 364:1513–1522. TREAT-NMD website. Available at: http://www.treat-nmd.eu. Accessed November 26, 2012. Fukunaga H, Ishiduka T, Sato M, Igata A, Nishitani H: [Database for patients with Duchenne muscular dystrophy]. Rinsho Shinkeigaku 1990, 30:1202–1207. Tatara KFH, Kawai M: Clinical survey of muscular dystrophy in hospitals of national hospital organization. Iryo 2006, 60:112–118. Takeshima Y, Yagi M, Okizuka Y, Awano H, Zhang Z, Yamauchi Y, Nishio H, Matsuo M: Mutation spectrum of the dystrophin gene in 442 Duchenne/ Becker muscular dystrophy cases from one Japanese referral center. J Hum Genet 2010, 55:379–388. Aartsma-Rus A, Van Deutekom JC, Fokkema IF, Van Ommen GJ, Den Dunnen JT: Entries in the Leiden Duchenne muscular dystrophy mutation database: an overview of mutation types and paradoxical cases that confirm the reading-frame rule. Muscle Nerve 2006, 34:135–144. Ishikawa Y, Miura T, Aoyagi T, Ogata H, Hamada S, Minami R: Duchenne muscular dystrophy: survival by cardio-respiratory interventions. Neuromuscul Disord 2011, 21:47–51. The family guide for the diagnosis and management of DMD. Available at: http://www.treat-nmd.eu/care/dmd/family-guide/translations/. Accessed November 26, 2012. Zhang YJ, Wang YO, Li L, Guo JJ, Wang JB: China’s first rare-disease registry is under development. Lancet 2011, 378:769–770. Thompson R, Schoser B, Monckton DG, Blonsky K, Lochmuller H: Patient registries and trial readiness in myotonic dystrophy–TREAT-NMD/ marigold international workshop report. Neuromuscul Disord 2009, 19:860–866. doi:10.1186/1750-1172-8-60 Cite this article as: Nakamura et al.: Characteristics of Japanese Duchenne and Becker muscular dystrophy patients in a novel Japanese national registry of muscular dystrophy (Remudy). Orphanet Journal of Rare Diseases 2013 8:60. Author details 1 Institute of Genetic Medicine, Newcastle University, Newcastle upon Tyne, UK. 2Department of Promoting Clinical Trial and Translational Medicine, Translational Medical Center, National Center of Neurology and Psychiatry, 4-1-1 Ogawa-Higashi, Kodaira, Tokyo 187-8551, Japan. 3Department of Neurology, National Center Hospital, National Center of Neurology and Psychiatry, Tokyo, Japan. 4Department of Child Neurology, National Center Hospital, National Center of Neurology and Psychiatry, Tokyo, Japan. 5 Department of Neuromuscular Research, National Institute of Neurosciences, National Center of Neurology and Psychiatry, Tokyo, Japan. 6Department of Molecular Therapy, National Institute of Neuroscience, National Center of Neurology and Psychiatry, Tokyo, Japan. 7Department of Neurology, National Hospital Organization, Higashi-Saitama National Hospital, Saitama, Japan. Submit your next manuscript to BioMed Central and take full advantage of: • Convenient online submission Received: 4 January 2013 Accepted: 11 April 2013 Published: 19 April 2013 • Thorough peer review • No space constraints or color figure charges References 1. Davies KE, Smith TJ, Bundey S, Read AP, Flint T, Bell M, Speer A: Mild and severe muscular dystrophy associated with deletions in Xp21 of the human X chromosome. J Med Genet 1988, 25:9–13. 2. Muntoni F, Torelli S, Ferlini A: Dystrophin and mutations: one gene, several proteins, multiple phenotypes. Lancet Neurol 2003, 2:731–740. 3. Emery AE: The muscular dystrophies. Lancet 2002, 359:687–695. • Immediate publication on acceptance • Inclusion in PubMed, CAS, Scopus and Google Scholar • Research which is freely available for redistribution Submit your manuscript at www.biomedcentral.com/submit 93 DATABASES OFFICIAL JOURNAL The TREAT-NMD Duchenne Muscular Dystrophy Registries: Conception, Design, and Utilization by Industry and Academia www.hgvs.org Catherine L. Bladen,1 Karen Rafferty,1 Volker Straub,1 Soledad Monges,2 Angélica Moresco,2 Hugh Dawkins,3 Anna Roy,4 Teodora Chamova,5 Velina Guergueltcheva,5 Lawrence Korngut,6 Craig Campbell,7 Yi Dai,8 Nina Barišić,9 Tea Kos,9 Petr Brabec,10 Jes Rahbek,11 Jaana Lahdetie,12 Sylvie Tuffery-Giraud,13 Mireille Claustres,13 France Leturcq,14 Rabah Ben Yaou,14 Maggie C. Walter,15 Olivia Schreiber,15 Veronika Karcagi,16 Agnes Herczegfalvi,16 Venkatarman Viswanathan,17 Farhad Bayat,18 Isis de la caridad Guerrero Sarmiento,18 Anna Ambrosini,19 Francesca Ceradini,20 En Kimura,21 Janneke C. van den Bergen,22 Miriam Rodrigues,23 Richard Roxburgh,23 Anna Lusakowska,24 Jorge Oliveira,25 Rosário Santos,25 Elena Neagu,26 Niculina Butoianu,26 Svetlana Artemieva,27 Vedrana Milic Rasic,28 Manuel Posada,29 Francesc Palau,30 Björn Lindvall,31 Clemens Bloetzer,32 Ayşe Karaduman,33 Haluk Topaloğlu,33 Serap Inal,34 Piraye Oflazer,34 Angela Stringer,35 Andriy V. Shatillo,36 Ann S. Martin,37 Holly Peay,37 Kevin M. Flanigan,38 David Salgado,41,42 Brigitta von Rekowski,1 Stephen Lynn,1 Emma Heslop,1 Sabina Gainotti,39 Domenica Taruscio,39 Jan Kirschner,40 Jan Verschuuren,22 Kate Bushby,1 Christophe Béroud,41 and Hanns Lochmüller1 ∗ 1 MRC Centre for Neuromuscular Diseases at Newcastle, Institute of Genetic Medicine, Newcastle upon Tyne, UK; 2 Hospital Pediatrı́a J. P. Garrahan, Argentina; 3 Office of Population Health Genomics, Department of Health, 189 Royal Street, Level 3C Western Australia, Australia; 4 WIV-ISP, Brussels, Belgium; 5 Department of Neurology, Medical University-Sofia, Sofia, Bulgaria; 6 University of Calgary, Health Sciences Centre, NW Calgary, Alberta, Canada; 7 Department of Paediatrics, Clinical Neurological Sciences and Epidemiology, Western University, London, Ontario, Canada; 8 Department of Neurology, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, China; 9 Division of Paediatric Neurology, University Hospital Centre Zagreb (KBC Zagreb), University of Zagreb Medical School, Zagreb, Croatia; 10 Institute for Biostatistics and Analyses, Masaryk University, Brno, Czech Republic; 11 National Danish Rehabilitation Centre for Neuromuscular Diseases, Aarhus, Denmark; 12 Turku University Central Hospital, Turku, Finland; 13 Laboratoire de Génétique de Maladies Rares, Université Montpellier 1 and Inserm U827, Montpellier, France; 14 Laboratoire de Biochimie et Génétique Moléculaire, Hôpital Cochin, Paris, France; 15 Friedrich-Baur-Institute, Department of Neurology, Ludwig-Maximilians-University of Munich, Munich, Germany; 16 NIEH, Molecular Genetic Department, Budapest, Hungary; 17 Kanchi Kamakoti CHILDS Trust Hospital, Nungambakkam, Chennai, India; 18 Pasteur Institute of Iran, Karaj Complex, Tehran, Iran; 19 Fondazione Telethon-Piazza Cavour 1, Milan, Italy; 20 Parent Project Onlus, Via Aurelia 1299 Roma, Italy; 21 Translational Medical Centre, National Centre of Neurology and Psychiatry, 4-1-1 Ogawa-Higashi, Kodaira, Tokyo 187-8551, Japan; 22 Leiden University Medical Center, Department of Neurology, ZA, Leiden, The Netherlands; 23 Neurology, Auckland City Hospital, Auckland, New Zealand; 24 Department of Neurology, Warszawa Banacha 1a, Poland; 25 Centro de Genética Médica Jacinto Magalhães, Porto, Portugal; 26 Pediatric Neurology Department, Hospital Al. Obregia, Bucharest, Romania; 27 Rublevskoe shosse, Moscow, Russia; 28 Clinic for Child Neurology and Psychiatry, Belgrade, Serbia; 29 Institute of Rare Diseases Research, Institute of Health Carlos III, Madrid, Spain; 30 Unit of Genetics, Hospital la Fe, Valencia, Spain; 31 Muskelcentrum, Dep of Neurology, USÖ, Örebro, Sweden; 32 Paediatric Neurology and Neurorehabilitation Unit, Lausanne University Hospital, Lausanne, Switzerland; 33 Hacettepe University Faculty of Health Sciences Department of Physiotherapy and Rehabilitation, Altındağ, Ankara, Turkey; 34 Istanbul University Faculty of Medicine, Neurology Department, PTR Unit, Istanbul, Turkey; 35 Action Duchenne, Epicentre, London, UK; 36 Institute of Neurology, Psychiatry and Narcology of NAMS, Kharkiv, Ukraine; 37 DuchenneConnect, Hackensack, New Jersey; 38 The Ohio State University, and Nationwide Children’s Hospital, Columbus, Ohio; 39 National Centre for Rare Diseases, Istituto Superiore di Sanità, Rome, Italy; 40 University Medical Center, Freiburg, Germany; 41 INSERM UMR_S910, Aix-Marseille UniversitéFaculté de Médecine La Timone, Marseille Cedex, France; 42 Australian Regenerative Medicine Institute, EMBL-Australia, Monash University, Clayton Campus Communicated by Mark H. Paalman Received 8 May 2013; accepted revised manuscript 19 July 2013. Published online 2 August 2013 in Wiley Online Library (www.wiley.com/humanmutation). DOI: 10.1002/humu.22390 dystrophin protein. Although many novel therapies are under development for DMD, there is currently no cure and affected individuals are often confined to a wheelchair by their teens and die in their twenties/thirties. DMD is a rare disease (prevalence <5/10,000). Even the largest countries do not have enough affected patients to rigorously assess novel therapies, unravel genetic complexities, and determine patient outcomes. TREAT-NMD is a worldwide network for neuromuscular diseases that ABSTRACT: Duchenne muscular dystrophy (DMD) is an X-linked genetic disease, caused by the absence of the Additional Supporting Information may be found in the online version of this article. ∗ Correspondence to: Hanns Lochmüller, MRC Centre for Neuromuscular Diseases at Newcastle, Institute of Genetic Medicine, Central Parkway, Newcastle upon Tyne, NE1 3BZ, UK. E-mail: [email protected] Contract grant sponsor: European Commission and TREAT-NMD (FP6 LSHM-CT2006–036825, 20123307 UNEW_FY2013, AFM (Association Francais contre les Myopathies) 16104). 95 C 2013 WILEY PERIODICALS, INC. have therefore opted to share patient information in the form of patient registries to increase the overall patient cohorts on which clinical outcomes and new technologies can be assessed [Sarkozy et al., 2008]. Before 2007, there were a number of independent registries already in existence for DMD (Fig. 1A). These included the French UMD Duchenne database (www.umd.be), the UK Parent Project (later Action Duchenne) Duchenne registry, the Czech National DMD/BMD registry, and the United Dystrophinopathy Project (UDP) in the USA. The total number of patients represented in these original registries was approximately 2,500. The information stored within these registries, while extremely important, was not freely available to the wider scientific community. There were also significant differences in the types of patient data collected and stored in each registry, and not all registries had consent forms, IRB approval, or data protection act approval, and so on. Differences also existed in the number of questions asked in these original registries, with some asking as few as 36, whereas others collected information on as many as 830, data fields. It was widely agreed that improvements could be made to patient registries if a more standardized and harmonized set of registries could be achieved. Discussions amongst patients, patient advocacy groups, and clinicians highlighted the need for a more harmonized approach to patient registries. This was further highlighted by discussions within the European Neuromuscular Centre (ENMC), where clinical and scientific experts outlined a framework for existing and emerging DMD registries [Mercuri et al., 2008]. What followed was the formation of a “charter” for DMD registries lead by TREAT-NMD. TREAT-NMD was initially established as an EU funded ``network of excellence” with the remit of “reshaping the research environment” in the neuromuscular field [http://www.treat-nmd.eu/, ; Bushby et al., 2009]. Initial TREAT-NMD milestones for disease-specific registries included: defining the data content for each disease/gene, defining the regulatory and ethical framework, identifying and analyzing existing national registries, and training curators for quality control of new and existing registries. The primary objective for a harmonized set of registries was to allow feasibility assessment, planning, and recruitment for clinical trials. Secondary objectives included collecting epidemiological data, establishing genotype–phenotype correlations, defining the natural history, and assessing treatment outcomes and standards of care. Ultimately, discussions under the auspices of TREAT-NMD decided upon a series of mandatory and highly encouraged items to be collected by each registry. TREATNMD registries also agreed to adhere to legal/ethical best practices allowing for patient feedback, possibility of data withdrawal from a registry, and encryption of data sets. provides an infrastructure to support the delivery of promising new therapies for patients. The harmonized implementation of national and ultimately global patient registries has been central to the success of TREAT-NMD. For the DMD registries within TREAT-NMD, individual countries have chosen to collect patient information in the form of standardized patient registries to increase the overall patient population on which clinical outcomes and new technologies can be assessed. The registries comprise more than 13,500 patients from 31 different countries. Here, we describe how the TREAT-NMD national patient registries for DMD were established. We look at their continued growth and assess how successful they have been at fostering collaboration between academia, patient organizations, and industry. C 2013 Wiley Periodicals, Inc. Hum Mutat 34:1449–1457, 2013. KEY WORDS: Duchenne muscular dystrophy; DMD; rare disease; disease registries; TREAT-NMD Introduction Duchenne muscular dystrophy (DMD; MIM #310200) is the most frequent pediatric muscle disorder [Ahn and Kunkel, 1993]. It is an X-linked genetic disease with an incidence of one in every 3,500 to 5,000 male births [Dooley et al., 2010; Emery, 1993]. DMD is caused by the absence of the protein dystrophin [Koenig et al., 1987] (DMD; MIM #300377). Affected boys become symptomatic at an early age (2–5 years of age) because of weakness in their proximal muscles, leading to an abnormal gait and frequent falls [Gowers, 1892]. DMD boys who are not steroid treated are in a wheelchair at a mean age of 9.5 years, and with steroids are often wheelchair bound by their teens [Humbertclaude et al., 2012]. Death occurs typically in the second or third decade due in part to respiratory failure though ventilation and other treatments are delaying death in many countries into the fourth or fifth decades [Baxter, 2006; Emery, 2002]. Currently there is no cure for DMD, but several novel treatment strategies are currently under evaluation in clinical trials including cell therapy, gene replacement, exon skipping, and the repurposing of existing drugs. Current care recommendations (such as the use of corticosteroids, cardiac medications, and assisted ventilation) improve outcomes and quality of life but do not modify the underlying progression of the disease [Hoffman et al., 2012; Sejerson et al., 2009]. Examples of more innovative treatment strategies include exon skipping, an RNA-based technology with the potential to target up to 83% of patients with deletions in the DMD gene [Aartsma-Rus et al., 2009; Beroud et al., 2007; van Ommen and Aartsma-Rus, 2013]. This and other DNA- or RNA-directed treatments require a greater understanding of the genetic basis and variability of a particular disease state. For the diagnosis of DMD, it is no longer standard of care to simply state that a patient is missing dystrophin in the muscle biopsy; a precise genetic diagnosis is required [Bushby et al., 2010; Sejerson et al., 2009]. Genetic diagnosis is confirmed by multiplex ligation-dependent probe amplification or associated sequencing of the dystrophin gene, reviewed in White and den Dunnen (2006). At the population level, DMD is a rare disease (prevalence <5/10,000). Individual countries have small pools of affected patients. Often the patient pool is too small for the initiation of clinical trials or for meaningful statistical analysis of current and historical research data [Brabec et al., 2009]. As with other rare diseases, individual groups 1450 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 Methods and Results TREAT-NMD was established in 2007 with the aim of “reshaping the research environment” in the neuromuscular field and to support translational research in NMD. This was achieved in part by the formation of a harmonized set of national DMD patient registries with a common data sharing philosophy, comprising both new registries set up to follow the TREAT-NMD guidelines and existing national registries who agreed to follow them. Information collected follows a mandatory or highly encouraged set of questions agreed on by the TREAT-NMD global database oversight committee. As a result, information can be shared and compared between the different national registries, with the ultimate goal of all national registries eventually linking into a centralized global DMD registry. We present here a systematic review of the content and activities of the DMD registry members in August 2012 collected via a comprehensive questionnaire (Supp. Fig. S1). All countries with active 96 Figure 1. DMD patient registries in 2007 and in 2012. Geographical location of DMD patient registries in 2007, before TREAT-NMD (A) and 2012, post 5 years of TREAT-NMD as European-funded Network of Excellence (B). Dark red, fully active registries; medium red, registries under construction/new registries; lightest red, planned registries. Further countries are joining under the current TREAT-NMD Alliance (not shown). patient registries (31 countries representing 33 registries) replied to the questionnaire however there are still a number of countries (approximately 11) with DMD patient registries either planned or under construction at this time. Purpose of the Registry Registries reported multiple functions ranging from therapeutic intervention and scientific development to strategic planning (Fig. 2). The most prevalent use of registries included clinical research and recruitment of patients to clinical trials (94%), epidemiological research (83%), natural history surveys and disease surveillance (75%), genotype/phenotype analysis (66%), and mutation data collection (65%). Forty-nine percent of registries reported using the registry for social planning and healthcare services planning. Figure 2. Purpose of the registry. The most prevalent use of registries included, clinical research and recruitment of patients to clinical trials (94%), epidemiological research (83%), natural history surveys and disease surveillance (75%), genotype/phenotype analysis and mutation data collection (66% and 65%, respectively). Forty-nine percent of registries reported using the registry for social planning and healthcare services planning. Characteristics of the Registries Geographical patient demographics The registries contained >13,500 patients from 31 different countries. The smallest registry consisted of 18 patients and the largest of 3337 patients (Fig. 3 and Supp. Fig. S2). Seventy-five percent of registries report geographical coverage at the national level, 20% at the regional level (a specific region within a country), and 5% either at the international or EU level. Coverage of the patient population in the different countries varies. For example, the registry from Denmark includes >95% of Danish DMD patients due to the infrastructure (all patients are recruited into a registry), and organization of their healthcare system (where clinicians enter registry data). A smaller percentage of patients are enrolled in those countries where patients or families have to initiate registry enrolment, but further work is needed to determine the completeness of the data sets for each country (i.e., the percentage of DMD patients from each country enrolled in their national registry). Three countries have more than one DMD registry (Spain, Italy, and the United States). A number of registries represent patients from more than one country; for example, the German registry also represents patients from Austria. 97 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 1451 Figure 3. Number of patients in national DMD registries by country. Numbers of patients in each national registry by country. Data are shown on a log10 scale and arranged in order of number of patients (highest to lowest). Australia and New Zealand collaborated, with Australia providing logistic support and data storage for New Zealand’s otherwise independent database [Rodrigues et al., 2012]. Annual funding of the registries was highly variable with 28% of registries reporting no annual funding at all. Twenty-five percent were funded with 50,000€ or less, 19% with 51,000–100,000€, 5% with 101,000–200,000€, and 3% with 501,000–1M€. A further 5% reported their annual funding as coming from donations and benefactors. The total amount of annual funding for all of the registries for 1 year was in excess of 1,610,000€. Funding sources for setting up registries TREAT-NMD made a direct financial contribution to the funding of the registries. Funding from the original FP6 grant was 1,000,000€ in total (200,000€ per year over 5 years). TREAT-NMD partially funded national registries in four countries and contributed to the coordination efforts of the global registry. National registry responses to the TREAT-NMD questionnaire indicated that initial funding provided to set up the registries came from a variety of sources ranging from personal donations to designated national and regional funding (Fig. 4). 30% of registries were set up with funding from more than two sources; for example, Finland received funds from patient organizations (Lihastautiliitto), a university/research institute (The University of Helsinki, Turku University Central Hospital), the EU agency/commission (TREAT-NMD), and other funding sources (private donations). The amount of money used for initial funding of the registries was variable with some registries being set up with ≤3,000€, whereas others had funds in excess of 200,000€. The median amount of money invested to set up a registry was 27,435€. Australia was a slightly different case with its initial funding coming from the Department of Health at the Government of Western Australia, with guaranteed funding up until 2014. Generally, we found that there was a shift from national funding (e.g., local government initiatives) to university/research institute or private funding after the initial funding period expired. An example would be Iran, who had funding from the Molecular Medicine Network 2010–2011 but now are limited to funding acquired by the registry curator. Eight percent of registries had their funding reduced after the initial funding period expired (generally 1–3 years), whereas only 3% of registries saw an increase in funding. 1452 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 Provision and entry of data Most of the registries obtained data directly from the patients and their families (34%) or clinicians (32%) (Fig. 5A). Clinical genetics units provided 22% of the data reported. Patient organizations provided 9% of the data collected, whereas occasionally data were provided by research laboratories (3%). Data entry methods were also variable with the plurality of registries capturing data on paper for later entry by registry staff (46%), whereas 23% of data providers directly uploaded their data online (Fig. 5B). Data are updated annually in 88% of registries (29 of 33 that replied). Mandatory and highly encouraged data requested by TREAT-NMD TREAT-NMD suggested a series of mandatory and highly encouraged items to be collected by each registry including patient demographics; molecular diagnosis; clinical diagnosis (DMD versus Becker muscular dystrophy); motor function; use of steroids; history of scoliosis surgery; cardiac and respiratory function; clinical trial participation; muscle biopsy; and family history. Genetic diagnosis was collected by all registries. Consistent with previously published data and databases [Brabec et al., 2009; Cunniff et al., 2009; Nakamura et al., 2013; Tuffery-Giraud et al., 2009], DMD 98 Figure 4. Initial funding of registries. Funding for the registries was provided by a number of different sources as outlined. Patient organizations are an important source of funding. Note that only 8% of the initial funding was covered by the European Commission’s grant for TREAT-NMD. mutations observed were mainly large deletions and duplications of one or more exons, with a smaller proportion of point mutations or more complex rearrangements. These questions were chosen (after consultation with TREAT-NMD partners) to maximize the versatility and functionality of the registries for clinical, academic, and industrial applications. Thirty-eight percent (12 of 33) of registries collected data on all of the required fields, 78% (26 of 33) reported on more than five of the required fields, whereas 30% (10 of 33) reported less than five of the required fields, focusing on molecular data and family history. Fifty-two percent (17 of 33) of registries included data over and above that required from TREAT-NMD including natural history, CK values for female carrier, medications, vitamins/supplements, gastrointestinal complications, and cognitive status. All of the registries questioned reported that their registry had been established following TREAT-NMD guidelines, either as part of a research project or following autonomous initiatives (clinician or patient driven). Only 11% (four registries) reported a legal obligation to set up a registry or to comply with regulatory requirements. In cases where the registry would be terminated, 28% of registries reported that they would either archive the registry for an undetermined amount of time or reported having no policy in place for termination. Three percent had a policy in place to destroy the registry upon termination, whereas 8% planned to archive for a predetermined amount of time. 14% would make their terminated data available to other registries. Communication activities of the registries occurred through multiple channels. Registries that maintained a Website tended to have it available at all times. The publication of newsletters tended to be monthly or bimonthly. One example is the Canadian Neuromuscular Disease Registry (www.CNDR.org), which produces a bimonthly newsletter, available in English and French, highlighting registry composition, study enquiries, scientific discoveries, and upcoming conferences. Overwhelmingly, registries reported their efforts to publish in scientific journals and communication at scientific meeting as being as “often as possible” with several publications linked directly to TREAT-NMD. Examples of publications that cite TREAT-NMD include [Griggs et al., 2013; Nakamura et al., 2013; Hollingsworth et al., 2012; Nakamura et al., 2011; Scully et al., 2013; Straub et al., 2012]. The numbers of staff employed by registries was variable but the majority of registries reported between one and four administrative staff working directly on the registries. Sixty percent of registry employees were part-time or were not primarily employed by the registry. Many of the registries also employed part-time medical staff. Only 11% (four of 33) of registries reported employing dedicated, full time clinical personnel. Roughly two of three of the registries had a governing board (Fig. 6), with the majority of the board being made up of internal registry staff (33%). External experts and patient organization representatives were also represented on the governing boards (29% and 27%, respectively). Patient representatives were often represented and made up 11% of the governing boards. Overall, the main function of the governing board was to oversee ethical and legal issues and to facilitate data access and use by internal and external researchers (38% and 36%). Financial/administrative 99 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 1453 Figure 5. Types of data providers and data entry method used. The different types of data providers for the registries are shown (A). Patients, their families, and clinicians are the most frequent data providers. Method of data entry to the registries is shown (B). The majority of data are provided on paper highlighting the need for user friendly electronic options. Figure 6. Composition of registry governing body. Registries were governed by representatives of different stakeholder groups including: Internal registry staff, external experts, patient organizations, and patient representatives. issues, and coordination of all parties involved in the registries was also an important function of the governing body (19%). Utilization of the Registries Third party access to the data in the registries is governed by the TREAT-NMD oversight committee (TGDOC). To obtain access 1454 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 to data, a third party approaches the TREAT-NMD global registry with a request for information contained within the registry. The oversight committee reviews the request and votes whether or not the request is in line with the charter and DMD patient interests. A vote of two-third is required to achieve quorum and therefore approval. If approval occurs, then the global registry approaches the national registries and obtains the data requested. The information is then put into a report, which is then given to the third party company (Fig. 7). In order to further facilitate clinical trial development, the TREAT-NMD Network established a Care and Trial Site Registry (CTSR) in December 2007. The TREAT-NMD CTSR is the largest and most comprehensive database of neuromuscular centers in the world. In addition, CARE-NMD was set up as a 3-year EUfunded project to improve access to best-practice care for DMD across seven EU countries—Bulgaria, the Czech Republic, Denmark, Germany, Hungary, Poland, and the UK [http://www.care-nmd.eu/, ]. CARE-NMD has used patient registries in all participating countries as a powerful tool to perform healthcare research in a specific rare disease. In contrast to common diseases, patient registries are often the only resource in rare disease, as ICD coding systems and other traditional health research methods are not applicable to rare diseases. Through the registries with a very high response rate CARE-NMD has collected care and quality of life information from more than 1,000 Duchenne patients in Europe and the findings are due to be published in 2013. Registries were asked a number of specific questions regarding their uses in academia and industry. Information was collected on the number of national and international studies registries had been used for. At the national level, the registries had been used for a total of 115 studies, some registries having only been involved in one or two studies, whereas others were involved in >10. Overall, 52% of 100 Figure 7. (TGDOC) Registry oversight committee. Schematic showing how a third party approaches the registries with an enquiry and how that enquiry is handled by the oversight committee of TREAT-NMD. registries were used for feasibility studies, split between academic (23%), industry (5%), and internal (24%). Forty-eight percent of registries were used for recruitment, split between academic (26%), industry (12%), and internal (10%). At the international level, the registries had been used in at least 10 studies (Table 1). Sixty-four percent had been used for feasibility studies (90% of which were industry enquiries) and 36% had been used for recruitment purposes (93% of which were industrial recruitment). There seemed to be a clear split between the uses of the registries at the national and international levels. Nationally, the registries were used mainly for academic and internal purposes, such as presentations at national conferences or applications for further funding. At the international level, there was a clear trend in the registries being involved in industrial collaborations. Table 1. International Enquiries Made to the DMD Registries from Industry Industrial liaison Year Feasibility enquiry 2009 2010 2011 2012 1 5 Recruitment enquiry Other (including trial site enquiries) 2 1 1 1 Table showing how the registries have been used for a number of industrial enquiries (both feasibility and recruitment) from 2009 to 2012. Table 1 summarizes the enquiries made to the DMD registries from industry (2009–2012). Although each industrial enquiry was unique, there were many similarities seen in the types of information requested by industry. Age, country of residence, and molecular diagnosis were requested 100% of the time. More than 85% of enquiries also requested patient ambulatory, ventilation, and cardiomyopathy status. Fifty percent of enquiries also requested trial site information from the trial site registry (Table 2). To date there have been more feasibility enquiries than recruitment enquiries. 101 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 1455 Table 2. Frequent Questions Asked to Registries in Enquiries from Industry Question asked in enquiry Patient demographics (e.g., age, country) Genetic diagnosis Ambulatory status Ventilation status Cardiomyopathy status Information from trial site registry Percent requested 100 100 ≥85 ≥85 ≥85 50 Table showing the types of information most commonly requested from the registries by industry. Examples of enquiries to the registries from industry include In 2009, a feasibility enquiry was made to the Global DMD Patient Registry for a phase I clinical program looking at exon skipping technology (exon 51). National registries from 18 countries were in a position to provide the requested data. A total of 2307 patients were retrieved from the TREAT-NMD global registry and identified as being appropriate for exon 51 skipping based on their mutation profile. In 2010, three feasibility enquiries were made to the Global DMD Patient Registry by different companies, two studies looking at exon skipping (exon 51 alone or multiple exon skipping 43, 44, 45, 46, 50, 52, 53, and 55), and one study looking at nonsense mutations. National registries from up to 27 countries were in a position to provide the requested data. More than 9,000 patients were identified as being appropriate for these studies. Two further feasibility enquiries were initiated in 2010 looking at randomized, placebo-controlled drug evaluation studies. In 2011, a recruitment enquiry to the Global DMD Patient Registry was initiated for a clinical trial looking at skipping exon 51. National registries representing seven countries were in a position to provide the requested information. A total of 50 DMD patients were identified as being appropriate for this study. A multinational (Germany, Italy, UK, and US) health economics study titled: “Multi-National, Cross Sectional, Observational Study of Patient and Caregiver Burden of DMD” was carried out in 2012. The study aimed to understand and improve the medical care of DMD, identifying the needs of caregivers, and facilitating future studies of DMD, including evaluations of new medicines (publication in preparation). Discussion Patient registries for rare diseases exist to improve feasibility, planning, and recruitment for clinical trials. The overall patient experience is also enhanced. This might be achieved simply by making a newly diagnosed patient feel part of a community, or it might occur through the facilitation and promotion of the latest medical and scientific advances. The common thread in all rare diseases is the small patient population. Such small cohorts have, in the past, meant little or no interest from pharmaceutical companies. Patient registries have allowed us to greatly increase patient populations simply by sharing agreed and harmonized patient data from individual countries around the world. The establishment of harmonized national patient registries and ultimately a global patient registry for DMD has created a centralized access point for information. This in turn has served to increase interest from TREAT-NMD industrial partners. Clinical trial feasibility and recruitment studies have increased dramatically over the last 3–4 years leading to 1456 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 the development of potential treatment strategies for DMD, such as exon skipping [Aartsma-Rus et al., 2009]. The registries have also allowed for critical analysis of current treatment protocols like the use of corticosteroids [Hoffman et al., 2012]. The registries have also led to improvements in patient care. An example is the work of CARE-NMD. CARE-NMD has used patient registries in variety of countries as a tool to perform healthcare research and to influence policy. Successful registries cooperate with appropriate clinical networks, healthcare services, research groups, patient advocacy groups, and industrial partners. National registries cooperate with genetic databases such as Leiden University in the Netherlands (www.dmd.nl) by providing information on genetic variants. This will be further facilitated through new platforms such as RD-Connect (http://rd-connect.eu/). The key to successful industry/patient registry interaction is quality control of the data within the registry. TREAT-NMD has achieved this through an emphasis on the appointment and training of registry curators. Registry curators provide a regulatory “checkpoint” between data being submitted to a registry and it being made available to the wider scientific community. This aims to minimise errors in the data. This is critical when the data submitted to the registries is entered by several different sources (clinicians, patients, patient organizations, genetics units). Registry curators can also be “data recruiters” by soliciting data from other countries. As the global registry for DMD further develops and matures, curation and surveillance will become increasingly important, not only for maintaining quality assurance but also for critical analysis of these large and well-defined data sets allowing for the potential identification and development of novel and emerging technologies (e.g., omics research). Monitoring the latest advances in scientific research and bioinformatics will ensure that the registries remain high-impact and current. The registries have been utilized extensively by industry for clinical trial activities. The number of returning industrial companies serves to further highlight the importance of the registries and the information that they provide. The impact of the national registries will be further enhanced through the continued inclusion in the global DMD registry (http://www.treat-nmd.eu/resources/patient-registries/ overview/). This federated style of registry development will ultimately provide a “one stop shop” for DMD patient information enquiries and clinical trial activities. Many of the national registries have already uploaded their information to the centralized global registry and it will be prudent to encourage emerging and planned national registries to also participate in the global registry. Looking ahead, we foresee a need for setting up and developing surveillance registries. Such registries will provide industry with a system that is able to manage regulatory post-marketing commitments. This, for example, will allow for the monitoring of drug safety and efficacy. Companies who are required to implement and maintain surveillance registries for their own products spend millions of dollars every year [Kaye, 2010]. A centrally managed registry platform will be independent, credible, and cost saving, and will link the TREAT-NMD global registry to individual surveillance modules. These registries will be sustained by the stakeholders of the DMD community and our industrial partners will pay to use the platform. However, issues do exist; currently, not all of the national registries have transferred their data to the global registry. The current mandatory data set is unlikely to be sufficient for all purposes and will need to be reviewed. Currently, the registries have no intellectual property protection and no sustainability assurance. Securing on-going funding for the registries remains critically important. Funding issues do exist and some registries have had to make use 102 of short-term funding while alternative sources of funding were identified. Further collaboration with industry (clinical trial participation) and the continued support of patient advocacy groups remains vital for sustainability. The registries are not legal entities and rely heavily on the supporting framework of academic institutions. These issues will need to be addressed and resolved for the future of the registries to be assured. It is clear that the global and national DMD patient registries provide an unparalleled resource for patient information, clinical and academic research, and best standards of care assurance. Patients, their families, clinical professionals, and the wider scientific and industrial communities all benefit from the existence of patient registries. The conception and development of these registries has brought about increased clinical trial opportunities translating directly to significant improvements in patient care and treatment options. Acknowledgments The authors would like to acknowledge the families of those living with DMD who have been instrumental in the formation of the DMD national registries. We also acknowledge former and current members of the TREAT-NMD office at the Institute of Genetic Medicine in Newcastle specifically Rachel Thompson. We also extend our thanks to the members of the TREAT-NMD executive committee: Hanns Lochmuller, Annemieke Aartsma-Rus, Anna Ambrosini, Filippo Buccella, Kevin Flanigan, Eric Hoffman, Janbernd Kirschner, Eugenio Mercuri, Ichizo Nishino, Kathy North, Jes Rahbek, and Thomas Sejersen. We also acknowledge the members of the current TGDOC: Jan Verschuuren (Chair), Hugh Dawkins (Chair elect), Anna Ambrosini, Svetlana Artemieva, Alexander N. Baranov, Farhad Bayat, Christophe Béroud, Ria Broekgaarden, Filippo Buccella, Craig Campbell, Nick Catlin, Monica Ensini, Pat Furlong, Kevin Flanigan, Ole Gredal, Lauren Hache, Serap _Inal, Jacqueline Jackson, Pierre-Yves Jeannet, Anna Kaminska, A. Ayse Karaduman, Veronika Karcagi, En Kimura, Janbernd Kirschner, Jaana Lähdetie, Hanns Lochmüller, Vitaliy Matyushenko, Vedrana MilicRasic, Violeta Mihaylova, Marie-Christine Ouillade, Ian Murphy, Miriam Rodrigues, Rosario dos Santos, Pascale Saugier-Veber, Inge Schwersenz, Thomas Sejersen, Rasha El Sherif, Eduardo Tizzano, Isabela Tudorache, Sylvie Tuffery-Giraud, Jen Wang, Simon Woods, W. Ludo van der Pol, Peter Van den Bergh, Petr Vondráček. Disclosure statements: Professor Hanns Lochmuller was elected chair of the TREAT-NMD Alliance in April 2012 and is the previous chair of the oversight committee. Professor Lochmuller has a financial interest/arrangement with Pfizer, Ultragenyx, and GlaxoSmithKline (Research grant investigator). References Aartsma-Rus A, Fokkema I, Verschuuren J, Ginjaar I, van Deutekom J, van Ommen GJ, den Dunnen JT. 2009. Theoretic applicability of antisense-mediated exon skipping for Duchenne muscular dystrophy mutations. Hum Mutat 30(3):293–299. Ahn AH, Kunkel LM. 1993. The structural and functional diversity of dystrophin. Nat Genet 3(4):283–291. Baxter P. 2006. Treatment of the heart in Duchenne muscular dystrophy. Dev Med Child Neurol 48(3):163. Beroud C, Tuffery-Giraud S, Matsuo M, Hamroun D, Humbertclaude V, Monnier N, Moizard MP, Voelckel MA, Calemard LM, Boisseau P, Blayau M, Philippe C, et al. 2007. Multiexon skipping leading to an artificial DMD protein lacking amino acids from exons 45 through 55 could rescue up to 63% of patients with Duchenne muscular dystrophy. Hum Mutat 28(2):196–202. Brabec P, Vondracek P, Klimes D, Baumeister S, Lochmuller H, Pavlik T, Gregor J. 2009. Characterization of the DMD/BMD patient population in Czech Republic and Slovakia using an innovative registry approach. Neuromuscul Disord 19(4): 250–254. Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, Cripe L, Kaul A, Kinnett K, McDonald C, Pandya S, Poysky J, Shapiro F, Tomezsko J, Constantin C. 2010. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol 9(1):77–93. Bushby K, Lynn S, Straub T, Network T-N. 2009. Collaborating to bring new therapies to the patient—the TREAT-NMD model. Acta Myol 28(1):12–15. Cunniff C, Andrews J, Meaney FJ, Mathews KD, Matthews D, Ciafaloni E, Miller TM, Bodensteiner JB, Miller LA, James KA, Druschel CM, Romitti PA, et al. 2009. Mutation analysis in a population-based cohort of boys with Duchenne or Becker muscular dystrophy. J Child Neurol 24(4):425–430. Dooley J, Gordon KE, Dodds L, MacSween J. 2010. Duchenne muscular dystrophy: a 30-year population-based incidence study. Clin Pediatr (Phila) 49(2):177–179. Emery AE. 1993. Duchenne muscular dystrophy—Meryon’s disease. Neuromuscul Disord 3(4):263–266. Emery AE. 2002. The muscular dystrophies. Lancet 359(9307):687–695. Gowers W. 1892. A manual of diseases of the nervous system. London: J & A Churchill. Griggs RC, Herr BE, Reha A, Elfring G, Atkinson L, Cwik V, McColl E, Tawil R, Pandya S, McDermott MP, Bushby K. 2013. Corticosteroids in Duchenne muscular dystrophy: major variations in practice. Muscle Nerve 48(1):27–31. Nakamura H, Kimura E, Mori-Yoshimura M, Komaki H, Matsuda Y, Goto K, Hayashi YK, Nishino I, Takeda S, Kawai M. 2013. Characteristics of Japanese Duchenne and Becker muscular dystrophy patients in a novel Japanese national registry of muscular dystrophy (Remudy). Orphanet J Rare Dis 8(60). Hoffman EP, Reeves E, Damsker J, Nagaraju K, McCall JM, Connor EM, Bushby K. 2012. Novel approaches to corticosteroid treatment in Duchenne muscular dystrophy. Phys Med Rehabil Clin N Am 23(4):821–828. Hollingsworth KG, de Sousa PL, Straub V, Carlier PG. 2012. Towards harmonization of protocols for MRI outcome measures in skeletal muscle studies: consensus recommendations from two TREAT-NMD NMR workshops: May 2, 2010, Stockholm, Sweden; October 1–2, 2009, Paris, France. Neuromuscul Disord 22 Suppl 2:S54–S67. Humbertclaude V, Hamroun D, Bezzou K, Berard C, Boespflug-Tanguy O, Bommelaer C, Campana-Salort E, Cances C, Chabrol B, Commare MC, Cuisset JM, de Lattre C, et al. 2012. Motor and respiratory heterogeneity in Duchenne patients: implication for clinical trials. Eur J Paediatr Neurol 16(2):149–160. Kaye E. 2010. Case study on use of registries in long-term surveillance. NIH/FDA Conference on Antisense Oligonucleotide Therapies in Neuromuscular Disease (Washington DC). Koenig M, Hoffman EP, Bertelson CJ, Monaco AP, Feener C, Kunkel LM. 1987. Complete cloning of the Duchenne muscular dystrophy (DMD) cDNA and preliminary genomic organization of the DMD gene in normal and affected individuals. Cell 50(3):509–517. Mercuri E, Mayhew A, Muntoni F, Messina S, Straub V, Van Ommen GJ, Voit T, Bertini E, Bushby K, Network T-NN. 2008. Toward harmonisation of outcome measures for DMD and SMA within TREAT-NMD; report of three expert workshops: TREAT-NMD/ENMC workshop on outcome measures, May 12–13, 2007, Naarden, The Netherlands; TREAT-NMD workshop on outcome measures in experimental trials for DMD, June 30–July 1, 2007, Naarden, The Netherlands; conjoint Institute of Myology TREAT-NMD meeting on physical activity monitoring in neuromuscular disorders, July 11, 2007, Paris, France. Neuromuscul Disord 18(11):894–903. Nakamura H, Kimura E, Kawai M. 2011. Infrastructure for new drug development to treat muscular dystrophy: current status of patient registration (Remudy). Brain Nerve 63(11):1279–1284. Nakamura H, Kimura E, Mori-Yoshimura M, Komaki H, Matsuda Y, Goto K, Hayashi YK, Nishino I, Takeda SI, Kawai M. 2013. Characteristics of Japanese Duchenne and Becker muscular dystrophy patients in a novel Japanese national registry of muscular dystrophy (Remudy). Orphanet J Rare Dis 8(1):60. Rodrigues M, Hammond-Tooke G, Kidd A, Love D, Patel R, Dawkins H, Bellgard M, Roxburgh R. 2012. The New Zealand neuromuscular disease registry. J Clin Neurosci 19(12):1749–1750. Sarkozy A, Bushby K, Beroud C, Lochmuller H. 2008. 157th ENMC International Workshop: patient registries for rare, inherited muscular disorders; January 25–27, 2008, Naarden, The Netherlands. Neuromuscul Disord 18(12):997– 1001. Scully MA, Cwik VA, Marshall BC, Ciafaloni E, Wolff JM, Getchius TS, Griggs RC. 2013. Can outcomes in Duchenne muscular dystrophy be improved by public reporting of data? Neurology 80(6):583–589. Sejerson T, Bushby K, Excellence T-NENo. 2009. Standards of care for Duchenne muscular dystrophy: brief TREAT-NMD recommendations. Adv Exp Med Biol 652:13–21. Straub V, Carlier PG, Mercuri E. 2012. TREAT-NMD workshop: pattern recognition in genetic muscle diseases using muscle MRI; February 25–26, 2011, Rome, Italy. Neuromuscul Disord 22 Suppl 2:S42–S53. Tuffery-Giraud S, Beroud C, Leturcq F, Yaou RB, Hamroun D, Michel-Calemard L, Moizard MP, Bernard R, Cossee M, Boisseau P, et al. 2009. Genotype– phenotype analysis in 2,405 patients with a dystrophinopathy using the UMDDMD database: a model of nationwide knowledgebase. Hum Mutat 30(6):934– 945. van Ommen GJ, Aartsma-Rus A. 2013. Advances in therapeutic RNA-targeting. N Biotechnol 30(3):299–301. White SJ, den Dunnen JT. 2006. Copy number variation in the genome; the human DMD gene as an example. Cytogenet Genome Res 115(3–4):240–246. 103 HUMAN MUTATION, Vol. 34, No. 11, 1449–1457, 2013 1457 J Neurol DOI 10.1007/s00415-013-7104-y ORIGINAL COMMUNICATION Prednisolone improves walking in Japanese Duchenne muscular dystrophy patients Fumi Takeuchi • Naohiro Yonemoto • Harumasa Nakamura • Reiko Shimizu Hirofumi Komaki • Madoka Mori-Yoshimura • Yukiko K. Hayashi • Ichizo Nishino • Mitsuru Kawai • En Kimura • Shin’ichi Takeda • Received: 21 August 2013 / Revised: 5 September 2013 / Accepted: 6 September 2013 Ó The Author(s) 2013. This article is published with open access at Springerlink.com Abstract We evaluated the long-term efficacy of prednisolone (PSL) therapy for prolonging ambulation in Japanese patients with genetically confirmed Duchenne muscular dystrophy (DMD). There were clinical trials have shown a short-term positive effect of high-dose and daily PSL on ambulation, whereas a few study showed a longterm effect. Especially in Japan, ‘‘real-life’’ observation was lacking. We utilized the national registry of muscular dystrophy in Japan for our retrospective study. We compared the age at loss of ambulation (LOA) between patients in PSL group and those in without-PSL group. Out of 791 patients’ in the Remudy DMD/BMD registry from July 2009 to June 2012, 560 were matched with inclusion criteria. Of the 560, all were genetically confirmed DMD patients, 245 (43.8 %) of whom were treated with PSL and 315 (56.2 %) without PSL. There was no difference between the two groups regarding their mutational profile. The age at LOA was significantly greater (11 month on average) in the PSL group than in the without-PSL group (median, 132 vs. 121 months; p = 0.0002). Although strictly controlled clinical trials have shown that corticosteroid therapies achieved a marked improvement in ambulation, discontinuation of the drug due to intolerable side effects led to exclusion of clinical trial participants, which is considered as unavoidable. In our study, patients were not excluded from the PSL group, even if they discontinued the medication shortly after starting it. The results of our study may provide evidence to formulate recommendations and provide a basis for realistic expectations for PSL treatment of DMD patients in Japan, even there are certain limitations due to the retrospectively captured data in the registry. F. Takeuchi H. Komaki Department of Child Neurology, National Centre Hospital, National Centre of Neurology and Psychiatry, 4-1-1 Ogawahigashi, Kodaira, Tokyo 187-8551, Japan N. Yonemoto R. Shimizu H. Komaki Y. K. Hayashi I. Nishino E. Kimura (&) S. Takeda Translational Medical Centre, National Centre of Neurology and Psychiatry, 4-1-1, Ogawa-Higashi, Kodaira, Tokyo 187-8551, Japan e-mail: [email protected] H. Nakamura M. Mori-Yoshimura Department of Neurology, National Centre Hospital, National Centre of Neurology and Psychiatry, 4-1-1 Ogawahigashi, Kodaira, Tokyo 187-8551, Japan Keywords Duchenne muscular dystrophy Prednisolone Walking National registry Natural history R. Shimizu Tokyo Women’s Medical University, 8-1, Kawada-cho, Shinjuku-ku, Tokyo 162-8666, Japan Introduction Present Address: Y. K. Hayashi Department of Neurophysiology, Tokyo Medical University, 6-1-1 Shinjuku, Shinjuku-ku, Tokyo 160-8402, Japan Duchenne muscular dystrophy (DMD) is a rare disease linked to the X-chromosome that affects 1 in 5,000–6,000 newborn males [1]. The disorder follows a progressive course of muscle weakness and also involves cardiac and respiratory muscles. DMD is caused by mutations in the M. Kawai Higashi-Saitama National Hospital, 4147, Kurohama, Hasuda, Saitama 349-0196, Japan 123 105 J Neurol clinical and molecular genetic data as well as all required items for the TREAT-NMD global patient registry. The database includes male Japanese DMD/BMD patients throughout Japan whose genetic status has been confirmed by genetic analysis. The registry data includes age at registration, birth date, area of residence, features of the muscle biopsy, genomic mutations, complicating diseases, PSL use (present use, past use or never), present functional mobility, age at LOA, cardiac function, respiratory function, spinal surgery, serum CK level, family history of DMD etc., but does not includes PSL regimes (dose, age at commencement and duration), side effects of PSL or physiotherapy. All these data were confirmed by three molecular and two clinical curators in Remudy. In this study, we used the registry data compiled from July 2009 to June, 2012 to compare the clinical course of DMD between patients with and without PSL therapy. Patients were excluded for any of the following reasons: (1) dystrophin expression remained on muscle biopsy by immunohistochemistry test; (2) in-frame, missense or unconfirmed mutation of DMD gene by mutation screenings; (3) comorbidities, such as adrenal hypoplasia or nephrotic syndrome; (4) current age B5 years or C40 years (because PSL therapy for DMD was not common before the 1990s) or (5) missing data on PSL use (Fig. 1). We compared the age at LOA between PSL group of patients, which was comprised of both current and past PSL-treated patients, and without-PSL group, which was comprised of patients who had never been treated with PSL (steroid naı̈ve). The primary outcome measure was ‘independent walking’ defined as ‘unsupported walking indoors’ [11], which is one of the standardized items in the TREAT-NMD global registry format. Because LOA was not well defined in several previous studies, there is no clear consensus on the DMD gene, which results in severe reduction or complete elimination of the dystrophin protein. Although the molecular origins of DMD have been known for several years, there is still no curative treatment for the disease. It has been nearly four decades since the potential benefits of glucocorticoids (GCs) for DMD were first reported by Drachman et al. [2]. In the years since, several randomised controlled trials (RCTs) have concluded that GCs increase short-term muscle strength and improve muscle function (from 6 months to 2 years) [3–7] with frequent but not severe adverse effects [6]. In contrast, the long-term benefits and adverse events of GCs have not yet been assessed by an RCT [4], although non-RCTs have suggested functional benefits for over 5 years in some GC-treated patients [8–17]. However, these studies were conducted in small numbers of patients. While PSL has been available for DMD patients since 1990s, there has been very little literature regarding the regimens of PSL for DMD in Japan. Some Japanese experts have a vague idea that the adequate dose could be lower than the one recommended (0.75 mg/kg/day) based on their expert experiences. Deflazacort has not been available yet in Japan [18].We used a large national registry of DMD patients in Japan to conduct a retrospective study on the long-term clinical efficacy of PSL therapy for maintenance of unassisted ambulation in DMD patients. Methods In 2009, we developed a national registry of Japanese DMD/BMD patients (Remudy) in collaboration with the Translational Research in Europe-Assessment and Treatment of Neuromuscular Diseases (TREAT-NMD) Network of Excellence [19, 20]. The Remudy database includes Fig. 1 Selection of DMD patients from the Remudy database for this study. *1: These 46 patients included outof-frame mutations (n = 7) and nonsense mutations (n = 7). *2: Three patients met (2) and (3) of our exclusion criteria. *3: Twenty-three patients met (1) and (2) of our exclusion criteria. DMD Duchenne muscular dystrophy, PSL prednisolone, Remudy Registry of Muscular Dystrophy [1] Dystrophin expression remained (n = 46*1, *3) 791 174 [2] In-frame (n = 131), missense (n = 6) or no confirmed mutations (n = 3)*2, *3 [3] Comorbidities (n = 5*2) 57 [4] Age <5 yrs (n = 49) or >40 yrs (n = 7) [5] No data on PSL use (n = 1) 560 PSL 245 Without PSL 315 123 106 J Neurol definition of LOA [11]. The Kaplan–Meier method was used to analyse the age at LOA, and the log-rank test was used to compare differences between PSL group and without-PSL group. We used age at LOA as a primary outcome because the database did not contain information on the initiation or duration of PSL treatment [21]. We set 5 years as the start time for PSL therapy. We used the Cox regression model to perform univariate and multivariate analyses to assess the effect of PSL. A covariate selected for adjustment was area of residence because the registrants varied in number and frequency of PSL treatment among 6 geographical areas. In addition, we considered family history of DMD as another covariate for adjustment because it might have influenced the patients’ decisions to accept PSL treatment. We calculated hazard ratios (HRs) and their 95 % confidence intervals (CIs). Statistical significance was defined as a two-sided p value \0.05. The software, SAS version 9.2 (SAS Institute Inc., Cary, NC, USA), was used to perform all statistical analyses. We also searched the PubMed database, reviewed related studies on the long-term effect of GCs on preservation of ambulation, and compared these previous results to those reported in the present study. Table 1 Patient characteristics PSL WithoutPSL Total Total n 245 % 100.0 n 315 % 100.0 n 560 Exon del/dup 183 74.7 230 73.0 413 21 8.6 26 8.3 47 Nonsense 29 11.8 41 13.0 70 Others 12 4.9 18 5.7 30 Family history Yes 60 24.9 110 34.9 170 No 185 75.1 205 65.1 390 Region Hokkaido and Tohoku 17 9.6 13 4.1 30 148 60.4 87 27.6 235 Mutation Frame shift or small del/ins Kanto Year of birth Results Chubu and Tokai 33 13.5 73 23.2 106 Kansai 25 10.2 62 19.7 87 Chugoku and Shikoku 14 5.7 23 7.3 37 Kyusyu and Okinawa 8 3.3 57 18.1 65 2001–2010 87 35.5 106 33.7 193 1991–2000 131 53.5 120 38.1 251 1981–1990 24 9.8 60 19.0 84 1971–1980 3 1.2 29 9.2 32 PSL prednisolone, del deletion, dup duplication, ins insertion Demographics group. Mutations included exon deletions or exon duplications (PSL patients: 183/245, 74.7 %; without-PSL patients: 230/315, 73.0 %); small frame shifts, deletions or insertions (PSL: 21/245, 8.6 %; without-PSL: 26/315, 8.3 %) and nonsense mutations (PSL: 29/245, 11.8 %; without-PSL: 41/315, 13.0 %). There was no difference in the mutation type distribution between the 2 groups. On the other hand, the geographic distribution of the 2 groups was significantly different, between 12 and 63 % of patients received PSL. We also presented distribution of the yearof-birth (per decade) in both PSL group and without-PSL group. The patients (PSL group and without-PSL group) were distributed in 2001–2010 (87/245, 35.5 %; 106/315, 33.7 %), 1991–2000 (131/245, 53.5 %; 120/315, 38.1 %), 1981–1990 (24/245, 9.8 %; 60/315, 19.0 %) and 1971–1980 (3/245, 1.2 %; 29/315, 9.2 %) respectively. Of the 791 patients (from 147 hospitals, with 228 doctors’ cooperation) in the Remudy database, 174 were excluded because they met at least 1 of the exclusion criteria, and dystrophin expression remained on muscle biopsy tissue was observed in 46 patients. One hundred and forty patients were excluded by DMD gene mutation screening, 131 had inframe mutations, 6 had missense mutations and 3 did not show mutations detectable with standard methods (MLPA, exonic sequencing). Five had comorbid diseases, such as nephrotic syndrome and adrenodysplasia. We also excluded 57 patients because 49 were\5 years old, 7 were C40 years old and there was missing data on the use or non-use of PSL for 1 patient. After removing patients who fulfilled at least 1 exclusion criterion, the final group for analysis included 560 genetically confirmed DMD patients (Fig. 1). Baseline characteristics are presented in Table 1. The mean current age of the 560 patients was 15.4 years, and the median current age was 14.0 years (interquartile range, 9–20 years). Of the 560 patients included, 245 (43.8 %) were in PSL group, and 315 (56.2 %) were in without-PSL group. The PSL group included 74 patients who had been treated with PSL in the past and 171 patients were currently on PSL (Fig. 1). Table 1 also presents the features of the DMD gene mutations in the PSL group and without-PSL Outcome Of the 560 patients, we excluded three patients from the PSL group and four from the without-PSL group because ambulation status was unknown. Finally, 553 patients, 242 in the PSL group and 311 in without-PSL group were included in the analysis. LOA was reported in 190 of the 311 patients in without-PSL group and 123 of the 242 123 107 Fig. 2 Time to loss of ambulation in the PSL group and without-PSL group determined by the Kaplan– Meier method. *Three patients in the PSL group and. **Four patients in the without-PSL group were excluded because their ambulation status was unknown. The PSL group had 242, 136 and 8 ambulant patients at 60, 120 and 180 months of age, respectively. The without-PSL group had 311, 145 and 10 ambulant patients at 60, 120 and 180 months of age, respectively. PSL prednisolone, HR hazard ratio Percent ambulant J Neurol PSL Without-PSL Age (months) PSL Without-PSL 242* 311** 136 145 8 10 Without-PSL* n = 311 Median age (months) (interquartile 25%–75%) 121 (10.1 yrs) (120–126) PSL** n = 242 132 (11.0 yrs) (126–138) Log-rank test p = 0.0002 HR 0.67 (95% CI 0.53–0.83; p = 0.0004) Adjusted HR 0.64 (95% CI 0.50–0.82; p = 0.0005) able to ambulate 11 months (0.9 years) longer on average than those without PSL, and the extension was relatively modest as compared to previous studies (Table 2). This may be due to one or several of the following factors: differences in ethnic origin of the treated population: small size of some of the previous studies: differences in the clinical definitions of DMD, different definitions of ambulation, variations in PSL regimens, and most importantly duration of treatment. First, previous studies only have been conducted in small numbers of patients (129 patients at most [12]), whereas the sample size in our study was 560 patients. On the other hand, Ricotti et al. [24] performed a prospective observational study in 360 patients, but their study did not compare a GC-treated group to a non-treated group. Second, the genetic and molecular criteria used to define DMD have varied between studies (Table 2). In the Leiden DMD mutation database, 9 % of the mutations did not follow the readingframe rule [25]. A diagnosis based on a purely molecular genetic approach may not accurately distinguish DMD from Becker muscular dystrophy and milder dystrophinopathies, especially in young children with no family history of DMD. In these patients, a muscle biopsy can help verify dystrophin expression to confirm the existence and severity of a functional mutation in the DMD gene [26]. Using DMD gene analysis only, previous studies may have included subjects with a milder phenotype (residual dystrophin expression) with longer prolongation of independent ambulation regardless of GC treatment history. To improve the precision of diagnosis in our study, we patients in PSL group. The median age at LOA was 121 months (10.1 years, interquartile range: 120–126 months) for the patients in without-PSL group and 132 months (11.0 years, interquartile range: 126–138 months) in PSL group (Fig. 2). The HR for without-PSL group versus PSL group was 0.67 (95 %CI: 0.53–0.83, p = 0.0004), and the adjusted HR was 0.64 (95 %CI: 0.50–0.82, p = 0.0005). Discussion To our knowledge, this is one of the largest studies worldwide on the long-term effects of PSL therapy on prolongation of independent walking ability in DMD and also the first study in Japan (Table 2). Historically, most DMD patients lose the ability to walk between 9 and 11 years of age [22], but recent improvements in care may have increased the age at LOA slightly even without the administration of steroids. In our study, the median age at LOA in patients who were never treated with PSL (without-PSL group) was 10.1 years. In a recent natural history study of 371 DMD boys, those on any steroid regimen for [6 months walked significantly longer (median age at LOA 12.0 years) than those on any regimen for\6 months or never on steroid (10.0 years) [23], which is quite similar to those without-PSL in our study. According to previous studies, patients receiving GC treatment were able to ambulate 2–5 years longer than those not treated with GCs [8, 23]. In the current study, patients treated with PSL were 123 108 109 Pro Pro Ret Ret Ret Ret Pro Ret Ret Pro Ricotti [24] Merlini [13] Bach [15] Straathof [11] Houde [10] King [12] Pradhan [14] Biggar [9] Balaban [8] Yilmaz [16] 22 66 (P) 19 30 (P18, D12) Unknown Unknown Include deletions 19 40 (D) 34 Include deletions Exclude BMD-like mutation and phenotype Include deletions Unknown Unknown Out of frame in 3 patients 15 (P) 68 91 (P36 D25) 42 37 (D) 0 35 (Pi) 117 17 (P16, D1) 3 4 (P ? D) – Include DMD mutation not confirmed mutations 360 (Pi191, Pd169) Exclude in-frame, missense, 315 DMD gene analysis Criteria 245 (P) Treated Non-treated Numbers or and or both Unknown Unknown Include consistent with DMD Unknown Unknown Include Dys (-) Unknown Include Dys (-) Include Dys (-) Include Dys (-) Exclude residual Dys Muscle biopsy Loss of independent walking ability Unable to walk 30 feet on a level floor independently Unable to walk Chair-bound stage Functional walking without orthoses or any assistive device Can no longer walk even with help Unable to walk, unsupported indoors Wheelchair dependence 8.6* 10.0* 8.9–9.9* P10.6–12.4*, D10.9–12.9* 9.8* 11.0* –c 14.0* 9.2* 12.5* 9.6* 11.5* – 10.8 9.7* ¯ 10.8* 16–18b – Assessment 10 m and 6 min walk Pi12.0, Pd14.5 10.1 11.0 Treated Control Median age (Years) Loss of ambulation NorthStar Ambulatory Unable to walk, unsupported indoors Definition of loss of ambulation All treated boys could walk 10 m at 10 years of age, 25 (81 %) of 31 at 12 years, 13 (76 %) of 17 at 15 years and two of six boys walked independently at 18 years of age 4 Treated patients (age 16–18) were fully ambulant, able to fast walk 10 m, and to perform the 6MWT; three of them were still able to climb stairs Comparison between Pd and Pi * Mean age, years c b a Pro Prospective study, Ret Retrospective study, D Deflazacort, P Prednisolone (Prednisone); Pi Intermittent Prednisolone, Pd daily prednisolone, Dys dystrophin expression Ret Our study Study design Table 2 Related studies on long-term effect of GC on preservation of ambulation 1.4 – 3–5c 3.0 3.3 1.9 – 1.1 – 2.5a 0.9 Prolonged ambulation, (Years) J Neurol 123 J Neurol hospitals and doctors, suggested that PSL therapy for the DMD patients had not been standardised in Japan [18]. Clinical practice guidelines for DMD in Japan will be published by the end of 2013. (http://www.neurology-jp. org/link/index.html, accessed August 12th, 2013). Finally, our data presents the first large outcome study of DMD patients in an Asian country. Recently, well conducted natural history studies for DMD have been reported from Europe and North American countries [23, 32]. Considering feasibility of global clinical trials for DMD, it appears relevant to obtain natural history data in non-western DMD patient populations. This study could add important information of the ‘‘real life’’ of DMD patients. excluded all patients who had any residual dystrophin expression in muscle tissue. However, 303 patients in our study were diagnosed as having DMD only based on DMD gene analysis. Of the 303 patients, 125 (28 treated in the past, 97 currently being treated) were in PSL group (50.0 % of 250), and 178 were in without-PSL group (56.5 % of 315). Therefore, some patients with milder phenotype may have been included in both groups. Third, PSL regimes (dose, age at commencement and duration) in our study may possibly have differed from those in related studies. A few previous studies only enrolled patients treated with GC for [1 [4] or [2 [8] years before LOA. Strictly controlled clinical trials have shown a more marked improvement in ambulation. However, discontinuation of the drug due to intolerable side effects leads to exclusion of clinical trial participants, while in our study patients were not excluded from PSL group, even if they discontinued the medication shortly after starting it. The American Academy of Neurology [27] and the Cochrane review [6] evaluated all RCTs on the use of GCs in DMD and concluded that PSL administered at 0.75 mg/kg/day was effective. However, a broadly accepted GC dose– response relationship has not been defined [6]. Therefore, a large-scale prospective study using strict criteria has been started very recently to determine the optimal regime in DMD (FOR-DMD) [28]. Our study is limited because all data is retrospectively captured by the registry. The registry items does not include detailed information of PSL regimes (dose, age at commencement and duration), physiotherapy, or other additive treatments such as creatine [29, 30]. Although we adjusted for family history and area of residence in the multivariate analysis, there was still some possibility of residual confounding between the two groups, such as progression of the attitude of ‘‘the standards of DMD care’’ by the decades. There was no item regarding the side effects of long-term PSL administration. Thus, we did not conclude that the benefits of PSL treatment outweigh the risks. The most frequent adverse effect of long-term GC treatment was a reduction in a patient’s height [6]. Weight gain was the second most frequent adverse event and the reason most often cited for discontinuing treatment [17]. However, weight gain in GC-treated DMD patients was a multifactorial effect due to pharmacological effects of GC and patients immobility, because weight gain generally was more pronounced in non-ambulatory patients [31]. However, our observational study showed actual clinical setting of GCs therapy in Japan (‘‘real life’’ data). The result of our study could provide evidence to formulate recommendations and base realistic expectations for steroid treatment of DMD patients in Japan. The residential variation in PSL use, depending on the geographical region of Japan, probably due to differing practices among Acknowledgments We are grateful to the patients, families and muscular dystrophy support groups, especially the Japanese Muscular Dystrophy Association, and clinicians for their cooperation in establishing the national Registry of Duchenne and Becker Muscular Dystrophy (Remudy) in Japan. We also thank Dr. Fujii, Dr. Matsumura and Ms. Sato for useful comments on the manuscript. The authors would like to thank Enago (http://www.enago.jp) for English language editing. Remudy is operated in collaboration with the TREAT-NMD alliance. This study was supported by an Intramural Research Grant for Neurological and Psychiatric Disorders of the NCNP (23-4). Conflicts of interest flicts of interest. The authors declare that they have no con- Ethical standard Approval of the study was given by the National Centre of Neurology and Psychiatry, Ethics Committee involved in the study. Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited. References 1. Mendell JR, Shilling C, Leslie ND, Flanigan KM, al-Dahhak R, Gastier-Foster J, Kneile K, Dunn DM, Duval B, Aoyagi A, Hamil C, Mahmoud M, Roush K, Bird L, Rankin C, Lilly H, Street N, Chandrasekar R, Weiss RB (2012) Evidence-based path to newborn screening for Duchenne muscular dystrophy. Ann Neurol 71:304–313 2. Drachman DBTK, Myer E (1974) Prednisone in Duchenne muscular dystrophy. Lancet 14:1409–1412 3. Mendell JR, Moxley RT, Griggs RC, Brooke MH, Fenichel GM, Miller JP, King W, Signore L, Pandya S, Florence J, Schierbecker J, Robison J, Kaiser K, Mandel S, Arfken C, Gilder B (1989) Randomized, double-blind six-month trial of prednisone in Duchenne’s muscular dystrophy. N Engl J Med 320:1592–1597 4. Angelini C, Pegoraro E, Turella E, Intino MT, Pini A, Costa C (1994) Deflazacort in Duchenne dystrophy: study of long-term effect. Muscle Nerve 17:386–391 5. Rahman MM, Hannan MA, Mondol BA, Bhoumick NB, Haque A (2001) Prednisolone in Duchenne muscular dystrophy. Bangladesh Med Res Counc Bull 27:38–42 123 110 J Neurol 6. Manzur AY, Kuntzer T, Pike M, Swan A (2008) Glucocorticoid corticosteroids for Duchenne muscular dystrophy. Cochrane Database Syst Rev: CD003725 7. Griggs RC, Moxley RT 3rd, Mendell JR, Fenichel GM, Brooke MH, Pestronk A, Miller JP (1991) Prednisone in Duchenne dystrophy. A randomized, controlled trial defining the time course and dose response. Clinical Investigation of Duchenne Dystrophy Group. Arch Neurol 48:383–388 8. Balaban B, Matthews DJ, Clayton GH, Carry T (2005) Corticosteroid treatment and functional improvement in Duchenne muscular dystrophy. Am J Phys Med Rehabil 84:843–850 9. Biggar WD, Harris VA, Eliasoph L, Alman B (2006) Long-term benefits of deflazacort treatment for boys with Duchenne muscular dystrophy in their second decade. Neuromusc Disord 16:249–255 10. Houde S, Filiatrault M, Fournier A, Dube J, D’Arcy S, Berube D, Brousseau Y, Lapierre G, Vanasse M (2008) Deflazacort use in Duchenne muscular dystrophy: an 8-year follow-up. Pediatr Neurol 38:200–206 11. Straathof CS, Overweg-Plandsoen WC, van den Burg GJ, van der Kooi AJ, Verschuuren JJ, de Groot IJ (2009) Prednisone 10 days on/10 days off in patients with Duchenne muscular dystrophy. J Neurol 256:768–773 12. King WM, Ruttencutter R, Nagaraja HN, Matkovic V, Landoll J, Hoyle C, Mendell JR, Kissel JT (2007) Orthopedic outcomes of long-term daily corticosteroid treatment in Duchenne muscular dystrophy. Neurology 68:1607–1613 13. Merlini L, Gennari M, Malaspina E, Cecconi I, Armaroli A, Gnudi S, Talim B, Ferlini A, Cicognani A, Franzoni E (2012) Early corticosteroid treatment in 4 Duchenne muscular dystrophy patients: 14-year follow-up. Muscle Nerve 45:796–802 14. Pradhan S, Ghosh D, Srivastava NK, Kumar A, Mittal B, Pandey CM, Singh U (2006) Prednisolone in Duchenne muscular dystrophy with imminent loss of ambulation. J Neurol 253: 1309–1316 15. John R, Bach DM, Saulat B (2010) Duchenne muscular dystrophy. The effect of glucocorticoids on ventilator use and ambulation. Am J Phys Med Rehabil 89:620–624 16. Yilmaz O, Karaduman A, Topaloglu H (2004) Prednisolone therapy in Duchenne muscular dystrophy prolongs ambulation and prevents scoliosis. Eur J Neurol 11:541–544 17. Moxley RT 3rd, Pandya S, Ciafaloni E, Fox DJ, Campbell K (2010) Change in natural history of Duchenne muscular dystrophy with long-term corticosteroid treatment: implications for management. J Child Neurol 25:1116–1129 18. Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, Cripe L, Kaul A, Kinnett K, McDonald C, Pandya S, Poysky J, Shapiro F, Tomezsko J, Constantin C, Group DMDCCW (2010) Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol 9:77–93 19. Nakamura H, Kimura E, Mori-Yoshimura M, Komaki H, Matsuda Y, Goto K, Hayashi YK, Nishino I, Takeda SI, Kawai M (2013) Characteristics of Japanese Duchenne and Becker muscular dystrophy patients in a novel Japanese national registry of muscular dystrophy (Remudy). Orphanet J Rare Dis 8:60 20. Bladen CL, Rafferty K, Straub V, Monges S, Moresco A, Dawkins H, Roy A, Chamova T, Guergueltcheva V, Korngut L, Campbell C, Dai Y, Barisic N, Kos T, Brabec P, Rahbek J, Lahdetie J, Tuffery-Giraud S, Claustres M, Leturcq F, Ben Yaou R, Walter MC, Schreiber O, Karcagi V, Herczegfalvi A, 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Viswanathan V, Bayat F, de la Caridad Guerrero Sarmiento I, Ambrosini A, Ceradini F, Kimura E, van den Bergen JC, Rodrigues M, Roxburgh R, Lusakowska A, Oliveira J, Santos R, Neagu E, Butoianu N, Artemieva S, Rasic VM, Posada M, Palau F, Lindvall B, Bloetzer C, Karaduman AA, Topaloglu H, Inal HS, Oflazer P, Stringer A, Shatillo AV, Martin AS, Peay H, Flanigan KM, Salgado D, von Rekowski B, Lynn S, Heslop E, Gainotti S, Taruscio D, Kirschner J, Verschuuren J, Bushby K, Beroud C, Lochmuller H (2013) The TREAT-NMD Duchenne muscular dystrophy registries: conception, design and utilisation by industry and academia. Hum Mutat. doi:10.1002/humu.22390 [Epub ahead of print] John P, Klein MLM (2003) Survival analysis: techniques for censored and truncated data (statistics for biology and health). Springer, Berlin Dubowitz V (1995) Muscle disorders in childhood. WB Saunders, London Bushby K, Connor E (2011) Clinical outcome measures for trials in Duchenne muscular dystrophy: report from International Working Group meetings. Clin Investig 1:1217–1235 Ricotti V, Ridout DA, Scott E, Quinlivan R, Robb SA, Manzur AY, Muntoni F, on behalf of the NorthStar Clinical N, Dubowitz Neuromuscular Centre GOSHfCNHSTL (2013) Long-term benefits and adverse effects of intermittent versus daily glucocorticoids in boys with Duchenne muscular dystrophy. J Neurol Neurosurg Psychiatry 84(6):698–705 Aartsma-Rus A, Van Deutekom JC, Fokkema IF, Van Ommen GJ, Den Dunnen JT (2006) Entries in the Leiden Duchenne muscular dystrophy mutation database: an overview of mutation types and paradoxical cases that confirm the reading-frame rule. Muscle Nerve 34:135–144 Muntoni F, Torelli S, Ferlini A (2003) Dystrophin and mutations: one gene, several proteins, multiple phenotypes. Lancet Neurol 2:731–740 Moxley RT 3rd, Ashwal S, Pandya S, Connolly A, Florence J, Mathews K, Baumbach L, McDonald C, Sussman M, Wade C, Quality Standards Subcommittee of the American Academy of N, Practice Committee of the Child Neurology S (2005) Practice parameter: corticosteroid treatment of Duchenne dystrophy: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 64:13–20 Hoffman EP, Reeves E, Damsker J, Nagaraju K, McCall JM, Connor EM, Bushby K (2012) Novel approaches to corticosteroid treatment in Duchenne muscular dystrophy. Phys Med Rehabil Clin N Am 23:821–828 Kley RA, Tarnopolsky MA, Vorgerd M (2011) Creatine for treating muscle disorders. Cochrane Database Syst Rev: CD004760 Davidson ZE, Truby H (2009) A review of nutrition in Duchenne muscular dystrophy. J Hum Nutr Diet Off J Br Diet Assoc 22:383–393 Beytia Mde L, Vry J, Kirschner J (2012) Drug treatment of Duchenne muscular dystrophy: available evidence and perspectives. Acta Myol 31:4–8 McDonald CM, Henricson EK, Abresch RT, Han JJ, Escolar DM, Florence JM, Duong T, Arrieta A, Clemens PR, Hoffman EP, Cnaan A, Cinrg I (2013) The cooperative international neuromuscular research group duchenne natural history study-a longitudinal investigation in the era of glucocorticoid therapy: design of protocol and the methods used. Muscle Nerve 48:32–54 123 111 Remudy 通 信 Remudy通信一覧は下記のサイトをご覧下さい。 http://www.remudy.jp/remudy_paper/index.html 精 神 ・神 経 疾 患 研 究 開 発 費 23-4「遺 伝 性 神 経 ・筋 疾 患 における患 者 登 録 システムの構 築 と 遺 伝 子 診 断 システムの確 立 に関 する研 究 」 平 成 25 年 度 研 究 者 一 覧 表 区分 主任 氏 名 木 村 所属施設・職名 円 所属施設所在地 独立行政法人 〒187-8551 国立精神・神経医療研究センター 東京都小平市小川東町 4-1-1 トランスレーショナル・メディカルセンター 臨床研究支援部 分担 分担 足立 克仁 貝谷 久宣 独立行政法人 国立病院機構 〒776-8585 徳島病院 四国神経・筋センター 徳島県吉野川市鴨島町敷地 内科 1354 一般社団法人 〒170-0005 日本筋ジストロフィー協会 東京都豊島区南大塚 3-43-11 福祉財団ビル 分担 川 井 充 独立行政法人 国立病院機構 〒349-0196 東埼玉病院 埼玉県蓮田市黒浜 4147 神経内科 分担 分担 分担 分担 小林 道雄 独立行政法人 国立病院機構 〒018-1393 あきた病院 秋田県由利本荘市岩城内道川 神経内科 字井戸ノ沢 84-40 独立行政法人 国立病院機構 〒899-5293 南九州病院 鹿児島県姶良市加治木町木田 臨床研究部 1882 独立行政法人 国立病院機構 〒982-8555 仙台西多賀病院 宮城県仙台市太白区鈎取本町 神経内科 2-11-11 西野 一三 独立行政法人 〒187-8502 (2013 年 8 月~) 国立精神・神経医療研究センター 東京都小平市小川東町 4-1-1 園田 至人 髙橋 俊明 神経研究所 疾病研究第一部 分担 林 由起子 独立行政法人 〒187-8502 (2011 年 4 月 国立精神・神経医療研究センター 東京都小平市小川東町 4-1-1 ~2013 年 7 月) 分担 水 島 洋 神経研究所 疾病研究第一部 国立保健医療科学院 〒351-0197 研究情報支援研究センター 埼玉県和光市南 2-3-6 155 区分 分担 氏 名 南 成 祐 所属施設・職名 所属施設所在地 独立行政法人 〒187-8551 国立精神・神経医療研究センター 東京都小平市小川東町 4-1-1 病院 臨床検査部 分担 森 まどか 独立行政法人 〒187-8551 国立精神・神経医療研究センター 東京都小平市小川東町 4-1-1 病院 神経内科 分担 本吉 慶史 独立行政法人 国立病院機構 〒284-0003 下志津病院 千葉県四街道市鹿渡 934-5 神経内科 分担 米本 直裕 独立行政法人 〒187-8551 国立精神・神経医療研究センター 東京都小平市小川東町 4-1-1 トランスレーショナルメディカルセンター 情報管理・解析部 156
© Copyright 2026 Paperzz