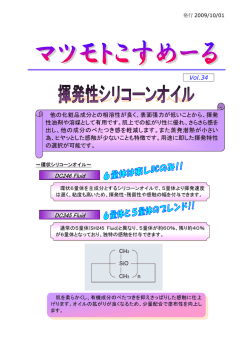
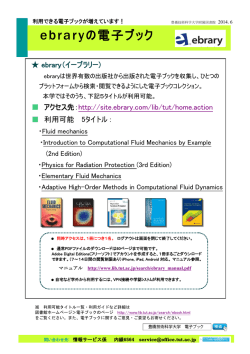
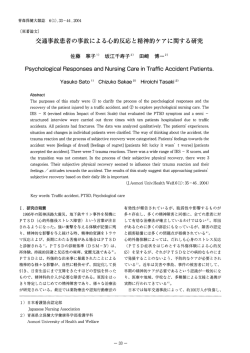
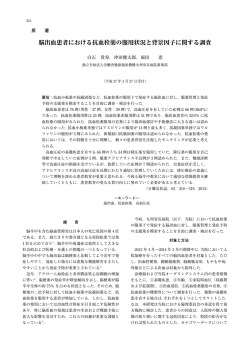
敗血症の輸液について 真剣に考える 2014.7.1 慈恵ICU勉強会 久米村 正輝 敗血症性ショックに対する補液 ✔️ これまで敗血症性ショックの治療において 補液を行うのは当然である、ように思われ る。 ✔ ️ その理由は... Crit Care Med 2013;41:580-‐637 1. a) CVPは8-‐12mmHg b) MAPは65mmHg以上 c) 尿量は0.5ml/kg/hr以上 d) ScvO2もしくはSvO2は70%か65%以上を最初の6時間以内に達成する 2. 乳酸が上昇している場合は正常化するように補液を行う CVP 8-‐12mmHg ✔ ️ 根拠はほぼなし ✔️ 1983年の15例での研究結果のみか MAP ≧ 65mmHg Helsinki University Hospital 9床の混合ICUに1999年から2002年に1419患者が入室 Sepsisと診断され入室から48時間vasopressor supportを要した111症例を後向きに解析 MAP60/65/70/75mmHgを閾値としたときのArea under MAPを算出 30日死亡率との関連性:MAP<65mmHgが最もAUC-‐ROC高い0.853 (95% CI 0.772-‐0.934) • より高いMAPに保つ事の有効性は微妙だが、 少なくとも65mmHg以上は必要であろう • いづれも比較対象となっているのは85mmHgで あり、65mmHgで十分かどうかは微妙 (70mmHg? 75mmHg? 80mmHg?) 尿量 ≧ 0.5ml/kg/hr ✔️ AKIが重症であるほど死亡率が高い ✔️ RIFLE分類やAKIN分類の乏尿の定義は、「尿 量が0.5ml/kg/hr以下が6時間以上継続するこ と」 ✔️ 0.5ml/kg/hr以上の尿量を保つように努める ことでAKIを防ぎ,死亡率を低下させるかもしれ ない 4.敗血症による組織の低還流があると思われる患者に対しては少なく とも30ml/kgの晶質液によるfluid challengeが必要である。患者によっ てはそれ以上の量の補液を必要とすることもある。 5.Fluid challengeは静的および動的パラメータに基づいて循環動態が 改善するまで継続して行われる。 • これまでに示したSSCGで推奨されている項目 についてはすべて推奨度1Cであり、どれも根 拠に乏しい。 • 2001年のRiversらの研究(EGDT)が早期の補 液によるResuscita]onの有効性についての 根拠となっている。 N Engl J Med. 2001 Nov;345(19):-‐1368-‐1377 ✔️ 単施設RCT、263人 ✔️ 従来の治療群 vs. EGDT群 ✔️ CVP,MAP,尿量,ScvO2 or SvO2の4つを指標とした目標値 を6時間以内に達成させる。(resuscita]on bundle) 結果 28日死亡率が46%から30%に減少 • このRiversらの研究ではこれら4つの指標の 根拠となるものは示されていない。 • 根拠を探すとすれば前述のようなものが挙げ られるものの、根拠としては貧弱 • この研究の対象患者に疑問 – 乳酸高値 – CVP,ScvO2低値 • SSCGにおいて4つの指標が用いられ続けた理 由はEGDT群と非EGDT群を比較したRCTが Riversの研究のみであったことが挙げられる。 • それに対して最近3つの大規模RCTが行われ ており,そのうちの1つである,ProCESS trialの 結果が報告された。 ✔️敗血症性ショックの患者に対する初期Resuscitationの検討 ✔️この研究の中でStandard群とusual care群を比較してみる Methods ✔️アメリカの31施設による ✔️大学病院の救急科 乳酸の測定 Resuscitation以外はSSCGに準拠 Resuscitationプロトコールがない 通常ScvO2を測定しない ✔️前向き無作為比較試験 ✔️2008. 3〜 2013. 5 対象患者 • • • • 18歳以上 敗血症の疑われる患者 SIRS ≥2項目 Fluid challengeでもSBP 90 mmHg> or 血管収 縮薬使用 • 乳酸 >4mmol /L 対象患者を3つのグループに割り付け Protocol-based EGDT 群 vs. Protocol-based standard therapy 群 vs. Usual care 群 【1次評価項目】 60日病院死亡率 【2次評価項目】 90日死亡率、90日と1年の積算死亡、血管収縮薬使用 期間、人工呼吸器使用期間、透析使用、入院期間、ICU 滞在期間、退院転帰(disposition)、重大合併症イベント Protocol-‐based EGDT ✔️ScvO2を測定 ✔️補液はCVPで決定 ✔️血圧管理はMAPで決定 ✔️輸血やinotropeはScvO2で決定 ✔️15-30分おきに評価 Protocol-‐based standard therapy ✔️CVは必須ではない ✔️SBPとShock Index(SI)で 輸液の追加を決定 ✔️過剰輸液はJVD,ralesな ど臨床所見で判断 ✔️IAPは必須ではない ✔️低潅流がなく, Baseline の10%以内の低下がなけ ればpass ✔️低灌流:MAP<65, lactate >4,mottled skin, 乏尿,意識の変容 ✔️輸血 Hb <7.5 Usual care ✔️ プロトコールなし ✔️ 担当医師が治療法を決定 医師の質はweb-‐based examで担保 救急医学もしくは集中治療医学の医師 ✔️ 施設の研究リーダーは治療せず Results(1次評価項目と死亡率) standard群とusual群では60日/90日死亡率に差はない Results(2次評価項目) 心臓,肺,腎臓の新規臓器機能不全はstandard群で多い傾向 Results (ResuscitaPon and processes) ✔️輸液量はStandard群(3285 vs. 2279)で多い ✔️Vasopressorの使用はStandard群で多い ✔️Resuscitation以外の治療は同じ Results (ResuscitaPon and processes) ✔️輸液量はStandard群で多い(72hrまでで8193 vs. 6633) ✔️昇圧剤の使用は同じ ✔️ 輸液量はStandard群で多い(有意差があるのは最初の6時間) ✔️最初の6時間ではMAP はStandard群で高いが, 心拍数は差がない ✔️最初の6時間ではpHが Usual群で高い ✔️どちらも時間経過ととも に差が消失している ✔️この研究においてEGDT群は死亡率に差はなく, 特にusual群より勝っている点が指摘できない ため,Standard群とUsual群で比較した ✔️輸液量は最初の6時間でStandard群の方が多 いが,死亡率には寄与していない ✔️pHはUsual群で高い ✔️電解質のうちClはStandard群で有意に高い ✔️酸素化の悪化はないため輸液によって悪化し たとまでは言えないが,新規の臓器不全発生 は増加傾向であり,RRT導入は増加している ✔️ICU入室も多く,コストは増大 ✔️Riversらの研究の時と今回のProCESSでは 支持療法が異なる ✔️敗血症の早期認知,早期の抗菌薬開始,血 糖管理,低1回換気戦略などで予後が改善し ており,死亡率20%前後とこれまでのRCTの中 で最もよい治療成績である 以前と比較して死亡率が低下した分,輸液によ る治療効果が低下し,逆に合併症の発生が明ら かになった可能性がある さらに • 近年EGDTに基づいた治療(補液)に関して否 定的な論文が敗血症だけでなく報告されるよ うになった。 1.外傷 Prehospital Intravenous Fluid Administration Is Associated With Higher Mortality in Trauma Patients: A National Trauma Data Bank Analysis Elliott R. Haut, MD∗ , Brian T. Kalish, BA∗ , Bryan A. Cotton, MD, MPH†, David T. Efron, MD∗ , Adil H. Haider, MD, MPH∗ ‡, Kent A. Stevens, MD, MPH∗ ‡, Alicia N. Kieninger, MD§, Edward E. Cornwell, III, MD¶, and David C. Chang, MBA, MPH, PhD∥ Annals of Surfery, Volume 253, Munber 2, February 2011: 371-377 1 Objective: Prehospital intravenous (IV) fluid administration is common in trauma patients, although little evidence supports this practice. We hypothesized that trauma patients who received prehospital IV fluids have higher mortality than trauma patients who did not receive IV fluids in the prehospital setting. Methods: We performed a retrospective cohort study of patients from the National Trauma Data Bank. Multiple logistic regression was used with mortality as the primary outcome measure. We compared patients with versus without prehospital IV fluid administration, using patient demographics, mechanism, physiologic and anatomic injury severity, and other prehospital procedures as covariates. Subset analysis was performed based on mechanism (blunt/penetrating), hypotension, immediate surgery, severe head injury, and injury severity score. Results: A total of 776,734 patients were studied. Approximately half (49.3%) received prehospital IV. Overall mortality was 4.6%. Unadjusted mortality was significantly higher in patients receiving prehospital IV fluids (4.8% vs. 4.5%, P < 0.001). Multivariable analysis demonstrated that patients receiving IV fluids were significantly more likely to die (odds ratio [OR] 1.11, 95% confidence interval [CI] 1.05–1.17). The association was identified in nearly all subsets of trauma patients. It is especially marked in patients with penetrating mechanism (OR 1.25, 95% CI 1.08–1.45), hypotension (OR 1.44, 95% CI 1.29–1.59), severe head injury (OR 1.34, 95% CI 1.17–1.54), and patients undergoing immediate surgery (OR 1.35, 95% CI 1.22–1.50). Conclusions: The harm associated with prehospital IV fluid administration is significant for victims of trauma. The routine use of prehospital IV fluid vital organ perfusion. Since its inception, the American College of Surgeons Advanced Trauma Life Support course has emphasized immediate treatment of trauma patients with IV fluids, although in the newest eighth edition, the course now emphasizes a more “balanced” approach.2 The routine practice of IV fluid administration in the prehospital arena is touted with great enthusiasm but little data exist to support its use.3,4 An increasing body of evidence has demonstrated that IV fluid administration does not improve survival in trauma and may actually be of harm in certain subsets of trauma patients.5–9 One theory for the possibility of harm is based upon the delay of transport to definitive care. Scene placement of venous access is not only associated with increased scene time but also increased overall time to hospital, in some cases the time to place an IV exceeds that of the actual transport itself.10 In hypotensive patients and those with primary torso injuries, scene placement times exceed that of en route IV line placement.11,12 Many trauma providers believe that the “scoop and run” approach, which minimizes prehospital procedures in favor of rapid transport to definitive care, is preferable to the “stay and play” model of prehospital trauma care.13,14 The second main theory regarding the potential harm of IV fluids is based upon the idea of “popping the clot.” This theory suggests that in patients, who have stopped bleeding temporarily from vasoconstriction and hypotension, IV fluids will raise systolic blood pressure and cause patients to rebleed if their bleeding source is not yet surgically controlled. This theory is supported by one of the few <目的> 外傷患者に対する病院前輸液の有効性について検討 <方法> 米国外傷データバンクに登録された患者で後ろ向きコホート研究 一次アウトカム:死亡率 病院前で輸液を受けた患者とそうでない患者とを比較 居住地区,受傷機転,損傷部位と重症度,その他の処置,外傷が鈍的か 鋭的か,低血圧の有無,手術までの時間, 頭部外傷の有無,外傷重症度 スコアなどについて検討 Annals of Surgery ! Volume 253, Number 2, February 2011 Prehospital IV Fluids in Trauma FIGURE 1. Multiple logistic regression showing odds ratio of death for trauma patients with prehospital IV fluid administration—subset analyses. GSW indicates gunshot wound. worse overall outcomes with IV fluid administration in patients with associated with higher mortality in patients with penetrating trauma in <結果> ✔️対象患者:776,734名 ✔️49.3%が病院前輸液を受け,死亡率は4.6% ✔️病院前輸液を受けた患者の死亡率が有意に高い(4.8%対4.5%) ✔️多変量解析でも病院前輸液を受けた患者の方が有意に死亡率が 高かった(オッズ比1.1、95%信頼区間1.05−1.17)。 ✔️鋭的外傷の患者(オッズ比1.25、95% CI 1.08-1.45) 低血圧(オッズ比1.44、95% CI 1.29-1.59) 重症頭部外傷(オッズ比1.34、95% CI 1.17-1.54) 迅速な手術を受けた患者(OR 1.35, 95% CI 1.22-1.50) 死亡率に有意差あり <結論> ✔️病院前の輸液と関連した不利益は外傷患者で著明である。 ✔️全ての外傷患者にルーチンに行われる病院前の輸液は中止すべ きである。 2.ALI original article Comparison of Two Fluid-Management Strategies in Acute Lung Injury The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network* NEJM 2006;354;24:2564-‐2575 <目的> A bs t r ac t ALIの体液管理に関して水分制限群と大量輸液群の比較 <方法> Background ALI患者 1,000 例を対象にプロトコールに従って、水分制限群と大量輸 ee Optimal fluid management in patients with acute lung injury is unknown. Diuresis d液群を比較する無作為化試験を行った。 or fluid restriction may improve lung function but could jeopardize extrapulmonaryD., endpoint:60 日の時点での死亡 organ perfusion. ltprimary p-secondary endpoint:人工呼吸器を使用しなかった日数、臓器不全が ., Methods s-起らなかった日数、肺の生理機能の測定値 na In a randomized study, we compared a conservative and a liberal strategy of fluid ement str ategies in acute lung injury alances were with associith the cons) than with ) (P = 0.001). ategy group at least one r or less (26 odium value rcent vs. 18 ate value of nt vs. 2 percant differwith at least liter or less Table 3. Main Outcome Variables.* Outcome Conservative Strategy P Value 28.4 0.30 14.6±0.5 12.1±0.5 <0.001 Days 1 to 7 0.9±0.1 0.6±0.1 <0.001 Days 1 to 28 13.4±0.4 11.2±0.4 <0.001 Death at 60 days (%) Ventilator-free days from day 1 to day 28† 25.5 Liberal Strategy The n e w e ng l a n d j o u r na ICU-free days† 1.0 Organ-failure–free days†‡ Days 1 to 7 Cardiovascular failure Alive, liberal strategy 0.9 3.9±0.1 4.2±0.1 0.8 0.04 CNS failure 3.4±0.2 2.9±0.2 0.02 Renal failure 5.5±0.1 5.6±0.1 0.45 Hepatic failure 5.7±0.1 5.5±0.1 0.12 Coagulation abnormalities 5.6±0.1 5.4±0.1 0.23 Cardiovascular failure 19.0±0.5 19.1±0.4 0.85 CNS failure 18.8±0.5 17.2±0.5 0.03 Renal failure 21.5±0.5 21.2±0.5 0.59 Days 1 to 28 Hepatic failure 22.0±0.4 21.2±0.5 0.18 3 and FigCoagulation abnormalities 22.0±0.4 21.5±0.4 0.37 ween the inype of fluid Dialysis to day 60 0.26). TherePatients (%) 10 14 0.06 o the fluidDays 11.0±1.7 10.9±1.4 0.96 catheter asduring the * Plus–minus values are means ±SE. CNS denotes central nervous system. as 25.5±1.9 † This was an a priori secondary outcome. ‡ For this analysis, cardiovascular failure was defined by a systolic blood presgroup and sure of 90 mm Hg or less or the need for a vasopressor (in contrast, shock tegy group was defined by a mean arterial pressure of less than 60 mm Hg or the need for a vasopressor [except a dose of dopamine of 5 µg per kilogram per minute rval for the or less]); a coagulation abnormality was defined by a platelet count of 80,000 onservativeper cubic millimeter or less; hepatic failure was defined by a serum bilirubin e days, days level of at least 2 mg per deciliter (34 µmol per liter); and renal failure was defined by a serum creatinine level of at least 2 mg per deciliter (177 µmol per and ICU-free liter). We calculated the number of days without organ or system failure by were no sigsubtracting the number of days with organ failure from the lesser of 28 days failure-free or the number of days to death. Organs and systems were considered failurefree after patients were discharged from the hospital. rst 28 days, increase in e–free days number of ventilator-free days or ICU-free days Proportion of Patients There were um sodium Alive, conservative strategy Breathing without assistance, conservative strategy 0.7 0.6 0.5 Breathing without assistance, liberal strategy 0.4 0.3 0.2 0.1 0.0 0 10 20 30 40 50 60 Days Figure 3. Probability of Survival to Hospital Discharge and of Breathing without Assistance during the First 60 Days after Randomization. patients in the liberal-strategy group and 23.0 percent of 61 Hispanic patients in the conservative-strategy group) than whites, but this difference did not reach significance (P = 0.10). After adjustment for baseline covariates, the hazard ratio for death among blacks as compared with whites was not significant (hazard ratio, 1.29; 95 percent confidence interval, 0.97 to 1.73), where- apy. T it is u compa of inte ance i was si work s ageme pleme to tho gestin ment practic aspect centra nary-a both w strateg respec Com goal-d are pr cols, p ventio pressu in pat previo gen de <結果> ✔️60 日死亡率:水分制限群 vs. 大量輸液群(25.5% vs. 28.4%) ✔️7 日間体液バランス:水分制限群 vs. 大量輸液群(−136±491 mL vs. 6,992±502 mL) ✔️水分制限群では28 日間における酸素飽和度と肺損傷スコアが改 善し,人工呼吸器を使用しなかった日数と集中治療室に入室しな かった日数(13.4±0.4 vs. 11.2±0.4,P<0.001)が増加した。 ✔️期間中のショックの発生率と有病率および60 日間の透析の使用率 (10% vs. 14%,P=0.06)は増加しなかった。 <結論> ✔️60 日死亡率に有意差なし ✔️水分制限によって肺以外の臓器不全を増加させることなく肺機能 が改善し,人工換気と集中治療の期間が短縮したと思われる。 ✔️ALI患者では大量輸液法より水分制限法が優れている可能性を示 唆する結果となった。 3.AKI RESEARCH Open Access Association between systemic hemodynamics and septic acute kidney injury in critically ill patients: a retrospective observational study Matthieu Legrand1,2*, Claire Dupuis1, Christelle Simon1, Etienne Gayat1,3, Joaquim Mateo1, Anne-Claire Lukaszewicz1,2,4 and Didier Payen1,2,4 Crit Care. 2013 Nov 29;17(6):R278. Abstract <デザイン> Introduction: The role of systemic hemodynamics in the pathogenesis of septic acute kidney injury (AKI) has receivedAKIと血行動態の関連について後方視的観察研究 little attention. The purpose of this study was to investigate the association between systemic Septic hemodynamics and new or persistent of AKI in severe sepsis. Methods: A retrospective study between 2006 and 2010 was performed in a surgical ICU in a teaching hospital. AKI was defined as development (new AKI) or persistent AKI during the five days following admission based on <方法> the Acute Kidney Injury Network (AKIN) criteria. We studied the association between the following hemodynamic targets within 24 hours of admission and AKI: central venous pressure (CVP), cardiac output (CO), mean arterial pressure (MAP), 対象:2006年-2010年に外科系ICU入室した137名の敗血症患者 diastolic arterial pressure (DAP), central venous oxygen saturation (ScvO ) or mixed venous oxygen saturation (SvO ). AKIの定義:AKIN criteriaをもとに入院後5日間で新規発症または持続 Results: This study included 137 ICU septic patients. Of these, 69 had new or persistent AKI. AKI patients had a higher Simplified Acute Physiology Score (SAPS II) (57 (46 to 67) vs. 45 (33 to 52), P < 0.001) and higher mortality (38% vs. 15%, したもの P = 0.003) than those with no AKI or improving AKI. MAP, ScvO and CO were not significantly different between groups. 入院後24時間の血行動態(CVP , COThe,CVP mAP , dAP,ScvO2又はSvO2)と Patients with AKI had lower DAP and higher CVP (P = 0.0003). value was associated with the risk of developing new or persistent AKI even after adjustment for fluid balance and positive end-expiratory pressure (PEEP) level (OR = 1.22 AKIの関係を調べた。 (1.08 to 1.39), P = 0.002). A linear relationship between CVP and the risk of new or persistent AKI was observed. 2 2 2 Conclusions: We observed no association between most systemic hemodynamic parameters and AKI in septic patients. Legrand et al. Critical Care 2013, 17:R278 http://ccforum.com/content/17/6/R278 Figure 2 Statistical model of nonparametric logistic regression showing the relationship between mean central venous pressure during the first 24 hours after admission and the probability of new or persistent acute kidney injury. Note the plateau for the incidence of acute kidney injury (AKI) when the lower limit of central venous pressure (CVP) was between 8 and 12 mmHg. Over this limit, the rise in CVP was associated with a sharp increase in new or persistent AKI incidence. Figure 3 Survival according to the occurrence of new or persistent acute kidney injury in survival according to the occurrence of AKI. AKI, acute kidney injury. patients [6]. Although resuscitation targeting the forward determinants of renal blood flow (MAP and CO) is com(60.9 to 119.6) vs. 100.6 (74.2 to 132.5); P = 0.19) did mon, little is known about backward determinants (renal <結果> ✔️137名のうち69名がAKI,68名がnon-AKI ✔️AKI患者はSAPSⅡスコアが高く、死亡率も高かった(38% vs 15% P=0.003) ✔️MAP,ScvO2とCOは両群で有意差はなかった。 ✔️AKIの患者はDAPが低くCVPが高かった(P=0.0003)。 ✔️CVP値は新規又は持続するAKIの発症に関与 ✔️CVPとAKIの発生率は比例関係であった <結論> ✔️今回CVP値のみがseptic AKIの発生に相関していた ✔️DAPは腎臓にとって潜在的に重要なパラメータである可能性が示 唆された。 補液をするかどうかを 検討した唯一のRCT Design : Setting : Patients : Methods: multicenter, open, randomized, control study 6 clinical centers Kenya(1), Tanzania(1), Uganda(4) 日齢60~12歳 重症熱性疾患に罹患し, 灌流障害を呈した3170名 重症熱性疾患と循環不全を呈する小児を2層に ◎A層(軽症例:3141名) ①5%アルブミン溶液20~40ml/kgボーラス群 ②0.9%生理食塩水20~40ml/kgボーラス群 ③ボーラス無投与(対照群) に無作為に割り付け ◎B層(重症例:29名)では重症低血圧を呈する小児をいず れかのボーラス群に無作為に割り付け Inclusion criteria ① ② ③ 日齢60~12歳 重篤な発熱性疾患 意識障害 呼吸困難 灌流障害 Capillary refill ]me: 3秒以上 末梢冷感 橈骨動脈微弱または頻脈 12カ月以下 >180/min 1~5歳 5歳以上 >160/min >140/min Exclusion criteria ① 重度な栄養失調の患児 ② 胃腸炎の患児 ③ 敗血症性以外のショックの患児 (外傷,熱傷,手術) ④ その他補液が適応外となる状態の患児 B層 A層 B層の基準を満たさない軽度の ショック より重症のB層には control群(no bolus群)を 設定せず アルブミン群 生理食塩水群 対象群 アルブミン群 NS群 control群 モニタリング•治療 ✔️ 医療環境: 小児科医が病棟で管理 ✔️ モニター: SpO2,NIBP(自動測定) ✔️ 維持輸液: 2.5-‐4.0ml/kg/hr ✔️ 感染対策: 抗菌薬,抗マラリア薬,解熱剤,抗痙攣薬 ✔️血糖: BS<45mg/dlの場合に糖負荷 ✔️ Hb: Hb<5g/dlの場合に全血を4時間で輸血 ✔️ 記録: 1/4/8/24/48時間の時点での記録 ①低血圧 ②神経,循環,呼吸 ③肺水腫,頭蓋内圧亢進,アレルギー反応 Primary endpoint ✔️ 48hr後の死亡率 Secondary endpoint ✔️ 4w後の死亡率 ✔️ 4w後の神経学的後遺症 ✔️ 48hrの低血圧ショック ✔️ 肺水腫・頭蓋内圧亢進・重症アレルギー な どfluid resuscita]onに関連した合併症 ✔️年齢中央値: 24か月(13-‐38か月) ✔️平均収縮期血圧93mmHg(85-‐101mmHg) ✔️衰弱:62%,昏睡:15% ✔️呼吸器合併症:83% ✔️52%でショック所見あり ✔️中等度アシドーシス:51% ✔️重症アシドーシス(乳酸>5mmol/l):39% ✔️平均Hb:7.1±3.2g/dl ✔️平均血糖値:124±70mg/dl ✔️マラリア感染率:57% ✔️HIV感染率:4% 各群間に有意差なし Primary endpoint Control群に対してBolus群の方が死亡率,危険度がともに高い Secondary endpoint ✔️ ✔️ ✔️ ✔️ Control群よりBolus群の方が死亡率,危険度が高い アルブミン群とNS群では生存率に差は認めない その他肺水腫,頭蓋内圧亢進,アレルギー反応は3群間で差は認めない 低血圧ショックの発症率は3群間で差を認めない ✔️ 大多数の死亡は24時間以内(87%) ✔️ 1hr以降はbolus群の死亡率が高い傾 向がある ✔️ 対照群では遅発性の死亡も少ない ✔️ 48hr以降の死亡例は少ない A層subgroup解析:48時間死亡 全ての項目においてbolus群の優位はみられない B層 ・平均収縮期血圧: 57mmHg(51~59mmHg) ・死亡率 アルブミンボーラス投与群 : 69% (9/13名) 生理食塩水ボーラス投与群: 56% (9/16名) アルブミン群,NS群どちらも死亡率高く、差は認めない 補液をすると予後が悪くなる? • ショックの状態では末梢血管抵抗が低下 • 血管収縮剤の投与や補液により,主要臓器の 潅流を維持する? • 補液による再潅流障害や肺コンプライアンス, 心筋の機能そして頭蓋内圧への悪影響が benefitを越えたことによって結果としてbolus 群で悪い結果となったのではないか ✔️補液する内容として0.9%NSが問題なのではないか ✔️0.9%NS:hyperchloraemic and acidotic compared with plasma ✔️severe sepsis患者に投与しすぎれば心機能を低下させ、循環を破 綻させる可能性がある ✔️血液のpHや電解質を測定する事ができないような地域では不適切 な輸液によるリスクがよりはっきりと結果に反映するだろう ✔増加した48時間後の死亡率についてはNS群とアルブミン 群はcontrol群に対して死亡率が高かった。NS群とアルブミ ン群との間には死亡率に差はなかった。️ ✔️それはどの年齢層でも,どの施設も,アシドーシスの程度に もショックの定義にもよらずbolus群の害は明らかであった。 ✔️補液によるresuscitationはWHOや国際的なガイドライン によって決められているが、今回の20ml/kgという補液量は そのガイドラインより少ない水準である。 反論と反論の反論 ✔️ NSを補液として使用するとClが高くなり,それによっ て心機能に影響したり,アシドーシスになったりす るが,今回の研究では補液の内容をアルブミンにして も補液をしなかった群と比べると結果が悪い。 ✔️ 患者の状態やbackgroundが異なっても同じように ボーラス群で結果が悪くなる。 ✔️ 現行のガイドラインに比べると輸液量自体も少ない ので入れすぎると悪くなるという議論も微妙。 ここまでのところをまとめると • 敗血症性ショックに対して補液をすることが正 しい治療なのかは不明 • 強く肯定する根拠はなく,EGDTで指標とされて いるものの信頼性も怪しい • さらに最近では補液が他の病態においても疑 問視されている • FEAST studyはlimitaPonはあるものの敗血症 性ショックに対して補液をしない方が死亡率 が低いという結果 では、なぜ補液をするのか 考えられる補液の理由 • • • • 低血圧 循環不全 低心拍出量 乏尿 など、臨床医が「補液をしようかなぁ」と思う時 に頭に浮かぶのはこんな理由 ✔️ 敗血症性ショックでは血管内皮障害が生じ, 末梢血管拡張や血管外漏出により循環血液量 減少が起こる。これを早期に補正するのが EGDTの目的 補液をすることで ✔️ 循環不全を改善することは有益だろう ✔️ 血圧を上昇させることも有益だろう ✔️ 心拍出量を増やす事も有益だろう ✔️ 尿量を増やすことも有益だろう 補液によって起こること – 血管外間質の浮腫や組織浮腫 – 特に脳/心臓/肺/腸管/皮膚/腎臓 – 高Cl血症 ✔️ 脳浮腫/肺水腫/不整脈/吸収不良/腎障害/腹 部コンパートメント症候群/皮膚トラブル/創傷治癒 遅延 ✔️ Clは腎機能だけでなく死亡率にも関与? これまで挙げた研究の結果からも過剰な補液は害にな るのは間違いなさそう ✔️ 輸液量の評価は難しい ✔️ Sta]c parameter(CVP,PAWP)は輸液反応性 の予測に使用するのは疑問 Osman D et al. Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge. Crit Care Med 2007;35:64-‐8 Marik PE et al. Does central venous pressure predict fluid responsiveness? A systema]c review of the literature and the tale of seven mares. Chest 2008;134:172-‐8 ✔️ Dynamic parameter(PPV,SVV)はある一定の 条件下では輸液反応性の指標になりうる Marik PE et al. Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ven]lated pa]ents: a systema]c review of the literature. Crit Care Med 2009;37:2642-‐7 Zhang Z et al. Accuracy of stroke volume varia]on in predic]ng fluid responsiveness: a systema]c review and meta-‐analysis. J Anesth 2011;25:904-‐16 ✔️ 敗血症性ショックへの輸液量に関する多施設前向き観察研究 ✔️ 初期12時間以内と3日目までの総輸液量に関する研究 164人の敗血症性ショック患者を対象 平均輸液量を境目に多い群と少ない群に分けて検証 12時間までの平均が4L,多い群と少ない群で輸液量に有意差あるも,90日死亡率に差なし 3日目までの平均が7.5L,同様に輸液量に有意差があり,90日死亡率では輸液量が多い方 が予後がいいという結果 ✔️ 原因としては多い方の群の輸液が他の研究に比較して多くなく,少ない群の輸液がかなり 少ないために過小輸液になった可能性がある(少なかった群の死亡率62%) ✔️ ✔️ ✔️ ✔️ ✔️ ALIをきたした敗血症性ショック患者212人に対する後ろ向き研究 ✔️ 初期輸液量と7日間の総輸液量を検討 ✔️ AIFR(adequate ini]al fluid resuscita]on):初期輸液によって CVP>8mmHgを達成 ✔️ CLFM(conserva]ve late fluid management):連続した2日間でマイ ナスバランスを達成 77.1% 18.3% 56.6% 41.9% ✔️ 初期輸液がAdequateであり,その後の水分バランス管理がConserva]veであった群が最 も死亡率が低い ✔️ 急性期は輸液を行い,状態が安定したあとはできるだけマイナスバランスに持っていた方 が予後がいいという結果であり,とてもしっくりくる結果? Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality* John H. Boyd, MD, FRCP(C); Jason Forbes, MD; Taka-aki Nakada, MD, PhD; Keith R. Walley, MD, FRCP(C); James A. Russell, MD, FRCP(C) Objective: To determine whether central venous pressure and fluid balance after resuscitation for septic shock are associated with mortality. Design: We conducted a retrospective review of the use of intravenous fluids during the first 4 days of care. Setting: Multicenter randomized controlled trial. Patients: The Vasopressin in Septic Shock Trial (VASST) study enrolled 778 patients who had septic shock and who were receiving a minimum of 5 !g of norepinephrine per minute. Interventions: None. Measurements and Main Results: Based on net fluid balance, we determined whether one’s fluid balance quartile was correlated with 28-day mortality. We also analyzed whether fluid balance was predictive of central venous pressure and furthermore whether a guideline-recommended central venous pressure of 8 –12 mm Hg yielded a mortality advantage. At enrollment, which occurred on average 12 hrs after presentation, the average fluid balance was "4.2 L. By day 4, the cumulative average fluid balance was "11 L. After correcting for age and Acute Physiology and Chronic Health Evaluation II score, a more positive fluid Crit Care Med 2011; 39: 259-‐65 balance at both at 12 hrs and day 4 correlated significantly with increased mortality. Central venous pressure was correlated with fluid balance at 12 hrs, whereas on days 1– 4, there was no significant correlation. At 12 hrs, patients with central venous pressure <8 mm Hg had the lowest mortality rate followed by those with central venous pressure 8 –12 mm Hg. The highest mortality rate was observed in those with central venous pressure >12 mm Hg. Contrary to the overall effect, patients whose central venous pressure was <8 mm Hg had improved survival with a more positive fluid balance. Conclusions: A more positive fluid balance both early in resuscitation and cumulatively over 4 days is associated with an increased risk of mortality in septic shock. Central venous pressure may be used to gauge fluid balance <12 hrs into septic shock but becomes an unreliable marker of fluid balance thereafter. Optimal survival in the VASST study occurred with a positive fluid balance of approximately 3 L at 12 hrs. (Crit Care Med 2011; 39:259 –265) KEY WORDS: sepsis; septic shock; fluid resuscitation ✔️敗血症性ショック患者でのCVP,輸液バランスと死亡率の相関関係 を検討した多施設後ろ向き観察研究 ✔️VASST studyのpost hoc解析で778人のすでに昇圧薬が投与され ている敗血症性ショック患者を対象に年齢と重症度を補正,初期12時 間の輸液バランスとそれに引き続く4日間の輸液バランス,CVP,28日 の死亡率との相関を検討 eptic shock is an extremely some basic treatments remain under- achieving a central venous pressure of 結果 ✔️ 治療開始12時間/第4病日までの輸液バランスは+4.2L/+11L であり、輸液バランスの増加は死亡率を増加させた。 ✔️ 治療開始12時間後および4日目のCVP値と28日死亡率を比較する と,初期12時間後でCVPが12mmHgよりも高い群が最も予後が悪 かった。4日目ではCVPの違いで予後に変化はなかった。 ✔️ 治療開始12時間の輸液バランスがプラス3L程度の場合が最も生存 率が高かった。 現在進行中のRCT • Australasian Resuscita]on In Sepsis Evalua]on Randomised Controlled Trial (ARISE) – 多施設RCT – EGDT vs. standard care – 1600人 – 終了予定 2015.4月 • ProMISe (Protocolised Management In Sepsis) – 多施設RCT、emergency departments (EDs) in the UK – EGDT vs. standard care – 人数不明 – 終了予定 2014.11月 目的:ProCESS/ARISE/ProMISEの3つの研究を比較。 方法:CONSORT guideline(非薬剤性治療に関するRCTの評価方法につ いてのガイドライン)に従って、3つのRCTの各項目を検証。 結果: ✔️ 3つの研究は,すべてEGDTによって敗血症性 ショック患者の予後が改善するという仮説のも とに行われており,デザインや目的など共通す る部分が多い。 ✔ 異なる点はICの取り方とProCESSのみが3群 による比較(EGDT vs. SP vs. UC)を行っている ことである。 ✔️ すべての研究が完了した時点で結果を融合 することで補液をプロトコールに従うことの有効 性(有害性?)を検証することが出来るかもし れない。 結論 ✔️ EGDTを取り入れたSSCGはfluid resuscitaPon の部分の根拠、有効性については疑問 ✔️ EGDTの有効性について検討したProCESS study の結果から身体所見をもとにした輸液で 十分である可能性が示唆された ✔️ 近年他の疾患でも補液が害になるという報 告 が多く見られる ✔️ FEAST studyの結果は臨床医が頭の中で描 いている補液の意味を揺るがす可能性があ り,補液をすること自体の意味を考えなければ ならない。 ✔️ 観察研究のみではあるが,過小輸液も害にな る可能性がある。 ✔️ 「補液をする」ことが患者の予後を改善すると いう根拠はない。 あなたは今日から補液をやめますか?
© Copyright 2026 Paperzz