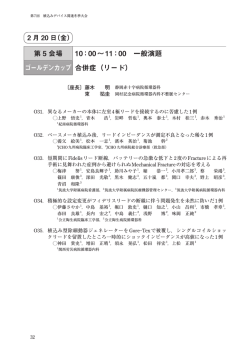
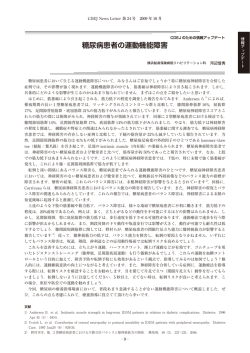
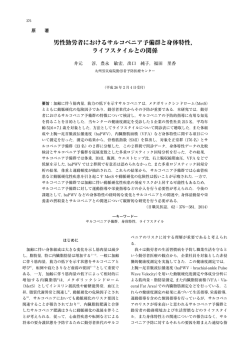
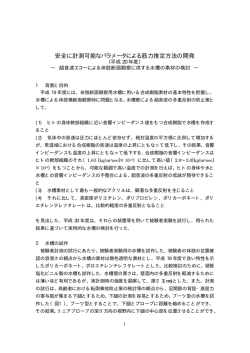
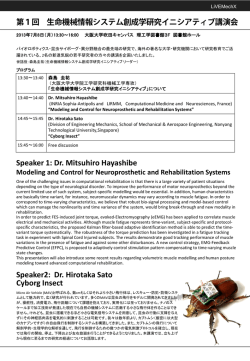
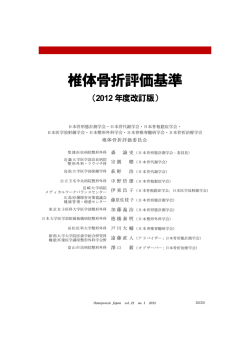
第 27 回健康医科学研究助成論文集 平成 22 年度 pp.128∼137(2012.3) 高齢者の転倒・骨折予防を目的とした、加齢性筋肉減少症 (サルコペニア)の診断法の開発 飛 田 哲 朗* 原 田 敦** 酒 井 義 人** DEVELOPMENT OF DIAGNOSIS METHOD FOR SARCOPENIA TO PREVENT FALLS AND FRACTURES IN FRAIL ELDERLY INDIVIDUALS Tetsuro Hida, Atsushi Harada, and Yoshihito Sakai SUMMARY Background: As populations are aging worldwide, the number of patients with osteoporotic fracture such as hip fracture and osteoporotic vertebral fracture is increasing. Because fractured patients consume much public resources such as hospitalization, medication, surgery and nursing care. The financial burden for osteoporosis is getting more critical. On the other hand, sarcopenia, the attenuation of skeletal muscle due to aging, was known to increase the risk of fall and was indicated for the risk factor of the osteoporotic fracture. But the impact in osteoporotic fracture had rarely been reported. This study was aimed to estimate the prevalence of sarcopenia for in the out-patients from osteoporosis clinic, to investigate character of muscle mass reduction in the patients with osteoporotic fractured, and to establish the diagnostic strategy to find out the patient in high risk for a fracture. Materials and Methods: A total of 2154 patients without fresh fracture from outpatient clinic in the study institute were assigned to the study for estimating the prevalence of sarcopenia. All patients underwent whole-body dual energy X-ray absorptiometry(DXA)for diagnosis of osteoporosis. Bone mineral content, fat mass, and lean soft-tissue mass were measured separately for each part of the body, including the arms and legs. The sum of the lean soft-tissue masses for the arms and the legs were considered to be the appendicular skeletal muscle mass. Since the absolute muscle mass is correlate with height, the appendicular muscle mass index(appendicular SMI) / height2(m2)is commonly used to assess sarcopenia. The appendicular SMI defined as appendicular SMI(kg) ). The criterion values of appendicular is directly analogous to the body mass index(weight(kg)/ height2(m2) SMI for sarcopenia were below 5.46 kg/m2 in female and below 6.87 kg/m2 in male for the study population from previous report. A total of 357 patients with a fresh hip fracture(the hip fracture group)were assigned to the study for estimating arm and leg muscle mass and compared with the patients from osteoporosis clinic(the out-patient group). The muscle of leg and arm was estimated separately by the DXA methods. There were 188 patients with osteoporotic fracture agreed to the various blood tests and psychiatric test such as mini-mental state examination and geriatric depression scale and assigned to the study for clarify the clinical characteristics of sarcopenic patients. * ** 名古屋大学大学院医学系研究科機能構築医学専攻 Department of Orthopedic Surgery, Nagoya University Postgraduate School of Medicine, Nagoya, 運動・形態外科学講座整形外科学 Japan. 国立長寿医療研究センター整形外科 Department of Orthopedic Surgery , National Center for Geriatrics and Gerontology, Aichi, Japan. (129) Results: The prevalence of sarcopenia in the out-patients from osteoporosis clinic was 27.2% in women and 52.8% in men. The arm SMI was not differed significantly between the hip fracture group and the out-patient group. However, the leg SMI was significantly lower in the hip fracture group. The laboratory examination values and the results of psychiatric test did not correlate with ASMI significantly. Conclusion: In conclusion, this study has revealed that high prevalence of sarcopenia in the out-patients and that the attenuated leg muscle mass in the osteoporotic fracture patients. Therefore the combination of sarcopenia and osteoporosis poses the potential risk for osteoporotic fracture. Simultaneous screening for sarcopenia and osteoporosis by DXA serves to determine the patients in risk for osteoporotic fracture. Key words: sarcopenia, fracture, osteoporosis, dual energy X-ray absorptiometry, skeletal muscle mass. る 24,38)。しかしながら、従来のサルコペニアの研 緒 言 究は疫学研究が中心で、実際に骨粗鬆症性骨折患 我が国で年間 18 万人が受傷するとされる大腿 者を対象としてサルコペニアを調査した研究は十 骨頚部骨折は、患者の activity of daily life(ADL) 分になされているとはいえない。 と quality of life(QOL)を 19) 大きく低下させ、 本研究の目的は 2 つある。1 つは骨粗鬆症外来 手 術 を 行 っ て も そ の 機 能 予 後、 生 命 予 後 の 低 通院患者におけるサルコペニア合併の実態を明ら 下 9,19) は避けられず、患者のみならず介護者の かにすること、もう 1 つは骨粗鬆症性骨折患者の QOL も大きく低下することが知られている 筋量減少の特徴とリスク因子を調べ、高齢者の骨 90% 以上の症例で入院加療を要し 。 34) 、再入院 23,37) 折ハイリスク患者の診断法を検討することである。 のリスクも高く 5)、社会における経済的負担は看 方 法 過できない 12)。また、180 万人が受傷するとされ る脊椎骨折 16) は、高齢者の寝たきりの原因の少 なからぬ割合を占め 、保存治療が奏功するこ 18) とも多いが、なかには手術が必要な難治例もあ A.二重エネルギーX線吸光(dual energy Xray absorptiometry; DXA)法を用いた骨粗鬆 症患者におけるサルコペニア有病率調査 。骨粗鬆症性骨折の予防は、世界に類をみ 国立長寿医療研究センターの骨粗鬆症外来で ない超高齢化社会を迎えた我が国の医療政策にお は、整形外科、内分泌内科、婦人科を受診した患 ける喫緊の課題の 1 つである 者の内、基礎疾患の有無にかかわらず、外来担当 る 17) 。 15) 一方、サルコペニア(sarcopenia)とは、加齢 医が骨粗鬆症の可能性が高く精査が必要と判断し による筋肉減少症のことで、ギリシャ語で「肉」 た患者、もしくは検診等で骨粗鬆症の精査が必要 を意味する「sarco」と「減少」を意味する「penia」 とされ初診で受診した患者の、骨粗鬆症の診断お からなり、1989 年に Rosenberg が初めて提唱した よび治療を行っている。骨粗鬆症外来を受診した 概念である 。70 歳以上の高齢者の 40%以上が 患者には、ルーチンで全身骨 DXA 装置(DPX-NT, 罹患していると推定され、20∼80 歳の間に筋量 General Electric Lunar 社 , 米国)により骨粗鬆症 33) は 30%減少するとされる 。この筋量減少は、 の診断を行っている。本研究は 2001 年以降の骨 ロコモティブシンドロームを始めとする身体の 粗鬆症外来を受診し、骨粗鬆症診断目的で全身骨 不安定性や 4) 、ADL の低下や、転倒を引き起こ DXA 検査を施行した新鮮骨折のない患者 2154 人 し 21)、骨粗鬆症性骨折の原因となる 29)。骨盤底 を対象とした。その身体組成を retrospective に解 筋群の筋力低下が高齢者の排尿障害の原因とな 析し骨粗鬆症患者の筋量とサルコペニアの有病率 り 32)、嚥下機能の低下、呼吸筋の筋力低下が誤 を評価した。 嚥性肺炎のリスクになるとする 報告もあり、 DXA 法で計測した上下肢の筋量を、BMI と同 運動器の不安定性や骨折の原因のみならず、高齢 様の手法により、身長の二乗で除して算出した 者の全身的な frailty(脆弱性)の一因であること 「補正四肢筋量」 (appendicular skeletal mass index; が知られ 、近年注目を集めている疾患概念であ ASMI)がサルコペニアの研究において標準的に 8) 28) 30) (130) Limb mass was determined by the image view of DXA. Lean mass ≒ Muscle mass Appendicular muscle mass index(kg/m2) =(arm muscle mass + leg muscle mass)/ height squared Leg muscle mass index(kg/m2) = leg muscle mass/height squared Arm muscle mass index(kg/m2) = arm muscle mass/height squared 図 1 .筋量測定法 : Dual energy X-ray absorptiometry(DXA)法 Fig.1.Measuring method for muscle mass: Dual energy X-ray absorptiometry method. DXA; Dual energy X-ray absorptiometry. 用いられている 8)(図 1) 。サルコペニアの診断基 55 歳以上の新鮮大腿骨頚部骨折患者の内、入院 準としては Baumgartner et al.2)が DXA 法により、 直後に全身骨 DXA 検査を施行し得た 357 人を頚 地域住民の2SD から算出した値を提唱してい 部骨折群(hip fracture group)とした。前述した、 る。この診断基準は白人およびヒスパニックを対 新鮮骨折のない骨粗鬆症外来通院患者 2154 人を 象としたものであり、日本人に関するエビデンス 外 来患 者群(out-patient group) と し た。 上肢 筋 は乏しかった。しかし、2010 年に Sanada et al.35) 量、下肢筋量を身長の二乗で除したものをそれ は本邦で初めてサルコペニアの日本人における基 ぞれ補正上肢筋量(arm skeletal muscle mass index; 準を報告した。この報告では 18∼40 歳の健常な arm SMI) 、補正下肢筋量(leg skeletal muscle mass 日本人男女 529 人の平均値の2SD から算出され index; leg SMI)とした。補正上肢筋量、補正下肢 た値を基に、ASMI が女性で 5.46kg/m2 以下、男 筋量および、補正四肢筋量を頚部骨折群と外来患 性で 6.87kg/m2 以下をサルコペニアありと診断し 者群間で比較することにより、上下肢の筋量の偏 た。Sanada et al. の基準値を用いて、日本人骨粗 在が骨折のリスクとなりうるか検討した。 鬆症患者におけるサルコペニアの有病率を検討し 更に、骨粗鬆症性骨折患者におけるサルコペニ アの現状と、採血検査および精神機能検査と筋量 た。 B.骨粗鬆症性骨折患者におけるサルコペニア の検討 の関連を検討した。 採血検査、精神機能検査による検討は、国立 下肢の筋力低下が身体不安定性を増大させ転倒 長寿医療研究センターに入院した高齢者骨粗鬆 や骨折を増加させることが既に知られており 、 症性骨折患者の内、受傷機転が低エネルギー外 図 1 に示したように、DXA 法では上下肢別々に 傷もしくは脆弱性骨折であり、入院直後に全身 筋量を評価することができる 42)。国立長寿医療 骨 DXA 検査を施行した患者の内、採血検査、精 研究センターで入院加療した転倒を起因とした 神機能検査に同意した 188 人を対象とした。入院 29) (131) 時の採血検査において、栄養状態の評価として血 清アルブミン値 3) を、筋由来酵素の評価として 血清クレアチニンを、骨粗鬆症の評価として、骨 型アルカリフォスファターゼ、Ⅰ型コラーゲン架 橋 N テロペプチドを測定した。血清による内分 泌学的評価として、副腎皮質刺激ホルモン 13)、 インタクト副甲状腺ホルモン、高感度副甲状腺ホ ルモン、遊離トリヨードサイロニン、遊離サイロ キシン、甲状腺刺激ホルモンおよび活性型ビタミ 27) ン D(1,25-hydroxyvitamin D3) の血中濃度を測 定した。精神機能を検討するため、認知機能評価 と し て MMSE(mini-mental state examination:30 点満点,21 点以下認知症あり) 11,25) を、うつ状態 図 2 . 代表症例:80 歳女性、右大腿骨頚部骨折術前 Fig.2.Case: 80 year-old woman with right hip fracture. の 評 価 と し て GDS-15(geriatric depression scale 15 items:15 点満点,0 ∼ 4 点,うつ症状なし; 5 ∼10 点,軽度のうつ病;11 点以上,重度のう つ病)22,40) を入院後早期に臨床心理士により測定 した。これらの検査項目と補正四肢筋量との相関 を検討した。 統計学的解析として、統計ソフト SPSS(version 15.0, SPSS, シカゴ , 米国)を用いた。 患者背景の男女間の比較には、Student の t 検 定を、サルコペニア有病率の男女間の比較には χ2 検定を行った。上下肢筋量の比較には、一般 線形モデルを用い、補正四肢筋量の測定結果を、 図 3-a.大腿骨頚部骨折(矢印)術前レントゲン写真 Fig.3-a.Preoperative X-ray picture of hip fracture(arrow). 筋量に影響する、性別、身長の各因子で調整した うえで比較した。採血検査、精神機能検査結果と 補正四肢筋量との関連は、Pearson の相関係数を 用いて検討した。危険率 5 %未満を有意差ありと した。 本研究にかかわるすべての検査は、国立長寿医 療研究センター倫理委員会の承認(2011 年 2 月 21 日承認,承認番号第 105 号)のもと、患者も しくは患者家族の書面による説明と同意を得て行 われた。 結 果 A.症例提示 図 3-b.人工骨頭置換手術後レントゲン写真 Fig.3-b.Postoperative roentgen image after hemi arthroplasty. 代表症例を提示する。症例は 80 歳女性で、も ともと認知症を合併していた。MMSE13 点。自 者家族の同意を得て掲載) 。 宅で転倒し、右大腿骨頚部骨折を受傷し、当院 身長 149cm、体重 32kg、補正四肢筋量は 4.8 へ救急搬送された(図 2,大腿骨頚部骨折(図 kg/m2 であり、重篤なサルコペニアと診断され 3-a)に対する人工骨頭置換手術直前の患者。患 た。入院 5 日目に人工骨頭置換手術を施行し(図 (132) 3-b)、術後 35 日目につたい歩きの ADL で介護 76.6%に調整した。なお、一般線形モデルを使用 施設へ退院した。 したため、その原理上標準偏差は算出せず、表中 B.二重エネルギーX線吸光法を用いた骨粗鬆 には標準誤差を示している。上肢補正四肢筋量は 症患者におけるサルコペニア有病率調査 外来患者群、頚部骨折群それぞれで 1.50kg/m2、 結果を表 1 に示す。対象となった 2154 人の内、 1.48kg/m2 で有意差を認めなかった。一方補正下 女性は 1699 人(79%) 、男性は 455 人(21%)で 肢筋量は外来患者群、頚部骨折群それぞれ 4.64kg/ あった。平均年齢は女性 70.5 歳、男性 67.5 歳で m2、4.45kg/m2 で有意差を認めた(P<0.001)。補 あった(P<0.001) 。身長、体重、全身骨骨密度 正上肢筋量と補正下肢筋量の和である補正四肢筋 の各基礎データはすべて女性で有意に低かった 量は、外来患者群、頚部骨折群それぞれ 6.13kg/ (P<0.001) 。四肢の筋量を身長の二乗で除した補 m2、5.92kg/m2 で有意差を認めた(P<0.001)。 正四肢筋量は、女性 5.92kg/m 、男性 6.76kg/m で、 骨粗鬆症性骨折患者 188 人の内、女性は 158 人、 男性で有意に多かった(P<0.001) 。サルコペニア 男性は 30 人であった。年齢 82 9.6 歳、身長 148 の有病率は Sanada et al. の基準を用いると、女性 8.5cm、体重 44.3 10.0kg、補正四肢筋量 5.63 2 2 27.2%、男性 52.8%であった(P<0.001) 。骨量と 0.92kg/m2(平均 補正四肢筋量の相関関係を検討した結果、弱いが 有意な相関(R=0.44, P<0.001)を認めた。 症性骨折患者における補正四肢筋量と採血検査結 C.骨粗鬆症性骨折患者におけるサルコペニア の検討 標準偏差)であった。骨粗鬆 果との関連を表 3 に示す。血清アルブミン値、血 清クレアチニン、骨型アルカリフォスファターゼ、 Ⅰ型コラーゲン架橋 N テロペプチド、副腎皮質 転倒に起因する大腿骨頚部骨折群と外来患者 刺激ホルモン、インタクト副甲状腺ホルモン、高 群との補正筋量を表 2 に示す。データはすべて 感度副甲状腺ホルモン、遊離トリヨードサイロニ 一般線形モデルを用い、年齢 71.3 歳、女性比率 ン、遊離サイロキシン、甲状腺刺激ホルモンおよ 表 1 .骨粗鬆症外来患者の背景、筋量およびサルコペニア有病率 Tabel 1.Baseline data , muscle volume, and prevalence of sarcopenia for out patient from the osteoporosis clinic. Number of patients Age(years) Height(cm) weight(kg) Whole body bone mineral density(g/cm2) ASMI(kg/cm2) Prevalence of sarcopenia(%) Female Male 1699 70.5 11.1 150 6.9 50.0 9.8 0.93 0.12 5.92 0.84 27.2 455 67.5 12.9* 160 7.0* 60.3 12.2* 1.09 0.15* 6.76 1.10* 52.8* The values were expressed mean standard deviation. ASMI; appendicular skeletal mass index. *: P<0.001. 表 2 .転倒に起因する大腿骨頚部骨折群と外来患者群との補正筋量の比較 Tabel 2.Muscle mass index of the fracture group and the out-patient group. Number of patients Arm SMI Leg SMI ASMI Out-patient group Hip fracture group P value 2154 1.50 0.07 4.64 0.02 6.13 0.05 357 1.48 0.02 4.45 0.04 5.92 0.02 na P>0.95 P<0.001 P<0.001 The values were expressed mean standard error. All data were controlled by the age of 71.3 years and the female ratio of 76.6%. SMI; skeletal muscle mass index, ASMI; appendicular skeletal mass index, na; not available. (133) 表 3 .骨粗鬆症性骨折患者における補正四肢筋量と採血検査結果の相関 Tabel 3.Correlation between appendicular skeletal muscle mass index and laboratory data of osteoporotic fracture patient with or without sarcopenia. Mean value SD Alb(g/dl) Cre(mg/dl) BAP(U/l) NTx(nmol BCE/l) ACTH(pg/ml) iPTH(pg/ml) PTH-HS(pg/ml) FT3(pg/ml) FT4(ng/dl) TSH(µIU/ml) 1,25(OH)2D3(pg/ml) 3.7 0.74 32.8 20.6 48.4 42.7 453 2.00 1.21 3.08 42.5 Pearson s correlation coefficient 0.45 0.64 17.1 17.1 59.2 23.0 340 0.47 0.21 9.36 18.6 P value 0.43 0.33 0.83 0.35 0.28 0.27 0.90 0.29 0.03 0.60 0.03 0.58 0.66 0.31 0.66 0.70 0.36 0.38 0.82 0.79 0.42 0.83 Data were from Pearson s correlation between appendicular skeletal muscle mass index and each laboratory value. BAP; bone specific alkaline phosphatase, NTx; type I collagen N-terminal telopeptide, ACTH; adrenocorticotropic hormone, iPTH; intact parathyroid hormone, PTH-HS; highly sensitive parathyroid hormone, FT3; free triiodothyronin, FT4; free thyroxin, TSH; thyroid stimulating hormone, 1,25(OH)2D3; 1,25-hydroxyvitamin D3. 表 4 .骨粗鬆症性骨折患者における補正四肢筋量と精神機能検査結果の相関 Tabel 4.Correlation between appendicular skeletal muscle mass index and cognitive examination from osteoporotic fracture patient with or without sarcopenia. Examination value SD Pearson s correlation coefficient P value 16.1 7.8 6.2 3.7 0.02 0.03 0.82 0.87 MMSE GDS-15 Data were from Pearson s correlation between appendicular skeletal muscle mass index and each laboratory value. MMSE; mini-mental state examination, GDS-15; geriatric depression scale 15 items. び活性型ビタミン D の各項目において、補正四 い。一方、1987 年にサルコペニアの概念が提唱 肢筋量と有意な相関を認めた項目はなかった。 されて以来、高齢者の歩行・移動能力低下とそれ 骨粗鬆症性骨折患者における補正四肢筋量と精 に伴う転倒、骨折、変性疾患の罹患にサルコペニ 神機能検査の結果を表 4 に示す。GDS-15 が 5 点 アの存在が多大な影響を与えていることは疑う余 以上の軽度もしくは重度のうつ病ありとされた患 地がなく、近年内科医を中心として注目を集めて 者は 92 人(49%)であった。MMSE で 21 点以 いる分野であるが、いまだにその全貌は明らかで 下の認知症ありとされた患者は 126 人(67%)で はない。諸外国では既に多くの疫学研究、臨床研 あった。GDS-15、MMSE ともに補正四肢筋量と 究が蓄積されつつあり 20)、身体不安定性のみな は有意な相関を示さなかった。 らず、免疫不全やインスリン抵抗性の一因である 考 察 とする報告もある 7)。今後は骨折予防のみならず、 動脈硬化などの生活習慣病治療における新たな切 高齢者の転倒は、骨折や寝たきりなどの直接の り札となる可能性を秘めている 1)。 障害を引き起こすばかりでなく、転倒恐怖による サ ル コ ペ ニ ア の 評 価 法 と し て、 現 在 ま で に 閉じこもり、それによる廃用性萎縮などの悪循環 種々の方法が考案されてきている。そのなかで に陥る主要な原因となっている。代表症例に提示 も DXA 法は、骨密度の計測でも用いられている したように、多くの患者は受傷前よりも ADL が 方法で骨粗鬆症診断に一般応用されており、なじ 低下し、自宅生活が不可能となることも珍しくな み深い方法である。一般に放射線は物質内を通過 (134) •Malnutrition, Vit.D insufficiency Aging •Disuse •Muscle atrophy, denervation Osteoporosis Sarcopenia Prone to fall Loss of bone strength を有するバイアスが存在する可能性が考えられ る。基礎疾患による frailty によりサルコペニアが 引き起こされることが知られており 26,38)、このこ とが高いサルコペニア有病率として表現された可 能性がある。 筋肉量の減少と筋力の低下は、身体の不安定性 Fracture を増大させ、転倒リスクを高めると考えられてい 図 4 . サルコペニアと骨粗鬆症、骨折との関係 Fig.4.Relationship between sarcopenia, osteoporosis, and fracture. る 39)。Baumgartner et al.2) による米国ニューメキ シコ州在住白人およびヒスパニック 883 人におけ る調査では、DXA 法により ASMI を測定した結 果、80 歳以上の女性において、ヒスパニックの する際に減衰するが、その減衰率は組織の体積、 60%、白人の 43.2%がサルコペニアに罹患して 物質を構成する元素の種類、放射線の強さに影響 いるとし、ASMI の低下した人に転倒が多く、身 される。この特徴を生かし、2 種類の強さの X 線 体の不安定性が増すと報告した。また、Sayer et を生体に照射し、それぞれの減衰率から身体組織 al.36)は英国での 2148 人を対象としたコホート研 の組成量を、骨塩量、脂肪量、除脂肪量の 3 種に 究において、転倒歴のある者に有意な筋力低下を 分け計測することができる 31)。DXA 法により測 認めたと報告した。本研究においては、転倒で受 定された組織量と、重量計で測定された重量とは 傷した骨折患者は、骨粗鬆症外来患者と比べ、下 よく一致する。特に内臓重量の影響を受けない上 肢筋量のみの低下が認められ、上肢の筋量の低下 下肢においては、除脂肪量と骨格筋量はほぼ同 は認められなかった。特に下肢の筋力の低下が転 等であるとみなせる。DXA 法は CT や MRI を用 倒を引き起し、骨折の原因となる可能性が示唆さ いた筋肉の断面積にて計測した筋量ともよく相 れ、下肢に限定した筋量のスクリーニング検査が 関し 42)、簡便で、低侵襲、低コストで、正確性 転倒骨折予防に有用である可能性があると考えら の高い方法である 14)。近年サルコペニア診断の れた。 ガイドラインにおいても煩雑な CT、MRI 法に替 これまで、サルコペニアの原因として、ビタミ わる代替的手法として認められた標準的診断法で ン D 不足、低栄養、廃用性萎縮、ホルモン不足 ある 。高齢者におけるサルコペニアの診断に、 などとする種々の報告があるが 6,41,43)、はっきり DXA 法による若年健常者の基準値を用いること とした結論は出ていない。これらのサルコペニア が推奨されており 、本研究において対象が高齢 の原因疾患の候補のなかには、骨粗鬆症の原因と 者であっても、Sanada et al. による日本人の基準 共通するものも多い 10)。本研究では、全身骨骨 値を診断基準に用いた。 密度と補正四肢筋量との間に有意な正の相関関係 8) 8) 本研究では、外来通院患者におけるサルコペニ を認めた。ビタミン D 不足、低栄養、廃用性萎縮、 ア有病率を示した。本研究における平均年齢 70.5 ホルモン不足などの加齢性変化が、サルコペニア 歳の女性の集団では 27.2%であった。従来の地域 と骨粗鬆症を同時に引き起こし、これらの相互作 在住住民らを対象とした報告では、同年代の集 用で骨折を引き起こしている可能性がある (図 4) 。 団で 27.6∼35.1%であり 、矛盾しない結果で サルコペニアの原因の追求のため、本研究で あった。しかし、本研究での平均年齢 67.5 歳の は、さまざまな血液学的検討と精神機能の検討を 男性の集団ではサルコペニアの有病率は 52.8%と 行ったが、筋量減少と関係する検査項目は発見し 高く、従来報告された同年代地域在住住民の 13.5 得なかった。サルコペニアの原因の解明のために ∼20.4%と比しても高率であった 。これは、 は更なる検討が必要であるが、サルコペニアのス 女性と比し男性はもともと骨粗鬆症の有病率が低 クリーニング検査として採血検査、精神機能検査 い 18) にもかかわらず、骨粗鬆症の疑いで外来を を用いることは困難である可能性がある。 受診する男性患者においては、何らかの基礎疾患 本研究の問題点としては、先述した対象患者の 2,43) 2,43) (135) 選別にある。骨粗鬆症外来に通院中の患者を対象 4)Baumgartner RN, Stauber PM, McHugh D, Koehler KM, としたが、このコホートは純粋な一般住民と比べ、 : Cross-sectional age differences in body Garry PJ(1995) 基礎疾患を有する確率が高く、虚弱性が高い可能 composition in persons 60+ years of age. J Gerontol A Biol 性を排除できない。よって、骨粗鬆症患者の下肢 筋量低下を過小評価している可能性がある。今後 は一般住民検診等を対象とし、より質の高い対照 群と骨折患者を比較する必要がある。また、今回 の研究での採血検査、精神機能検査の対象となっ た患者数は限定されており、結論を出すには不十 分であった。今後はより多くの骨粗鬆症性骨折患 Sci Med Sci, 50, M307-M316. 5)Boockvar KS, Halm EA, Litke A, Silberzweig SB, McLaughlin M, Penrod JD, Magaziner J, Koval K, Strauss E, Siu AL(2003): Hospital readmissions after hospital discharge for hip fracture: surgical and nonsurgical causes and effect on outcomes. J Am Geriatr Soc, 51, 399-403. 6)Coin A, Perissinotto E, Enzi G, Zamboni M, Inelmen EM, Frigo AC, Manzato E, Busetto L, Buja A, Sergi G(2008): 者を対象とするべく、データの継続的な蓄積が必 Predictors of low bone mineral density in the elderly: the 要であると考えられた。 role of dietary intake, nutritional status and sarcopenia. Eur 総 括 本研究では、骨粗鬆症患者におけるサルコペニ ア合併の実態を示し、骨粗鬆症性骨折患者の筋量 減少の特徴とリスク因子を検討した。転倒に起因 する骨粗鬆症性骨折患者では、下肢の有意な筋量 低下が認められた。種々の採血検査、精神機能検 査では筋量と相関する項目はなかった。下肢を中 心とした DXA 法による筋量のスクリーニング検 査がサルコペニアの診断に有用である可能性を示 J Clin Nutr, 62, 802-809. 7)Cosqueric G, Sebag A, Ducolombier C, Thomas C, Piette F, Weill-Engerer S(2006): Sarcopenia is predictive of nosocomial infection in care of the elderly. Br J Nutr, 96, 895901. 8)Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinkova E, Vandewoude M, Zamboni M (2010): Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing, 39, 412-423. した。サルコペニア診断により骨折高リスク患者 9)Cummings SR, Melton LJ(2002): Epidemiology and out- を早期に発見し、重点的に、転倒予防を行うこと comes of osteoporotic fractures. Lancet, 359, 1761-1767. が、今後の骨粗鬆症性骨折の予防に有用である可 能性が示された。 謝 辞 本研究を遂行するにあたり、研究助成を賜りました財団 法人明治安田厚生事業団に深く感謝いたします。また、本 研究の実施に快くご協力いただいた関係諸氏に深く感謝い たします。 参 考 文 献 10)Delmas PD(2002): Treatment of postmenopausal osteoporosis. Lancet, 359, 2018-2026. 11)Dick JP, Guiloff RJ, Stewart A, Blackstock J, Bielawska C, Paul EA, Marsden CD(1984): Mini-mental state examination in neurological patients. J Neurol Neurosurg Psychiatry, 47, 496-499. 12)Duclos A, Couray-Targe S, Randrianasolo M, Hedoux S, Couris CM, Colin C, Schott AM(2009): Burden of hip fracture on inpatient care: a before and after populationbased study. Osteoporos Int, 21, 1493-1501. 1)Aubertin-Leheudre M, Lord C, Goulet ED, Khalil A, 13)Emmelot-Vonk MH, Verhaar HJ, Nakhai-Pour HR, Grobbee Dionne IJ(2006): Effect of sarcopenia on cardiovascu- DE, van der Schouw YT(2009): Effect of testosterone lar disease risk factors in obese postmenopausal women. supplementation on sexual functioning in aging men: a Obesity, 14, 2277-2283. 6-month randomized controlled trial. Int J Impot Res, 21, 2)Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, Garry PJ, Lindeman RD(1998): 129-138. 14)Hansen RD, Williamson DA, Finnegan TP, Lloyd BD, Epidemiology of sarcopenia among the elderly in New Grady JN, Diamond TH, Smith EU, Stavrinos TM, Mexico. Am J Epidemiol, 147, 755-763. Thompson MW, Gwinn TH, Allen BJ, Smerdely PI, Diwan 3)Baumgartner RN, Koehler KM, Romero L, Garry PJ AD, Singh NA, Singh MA(2007): Estimation of thigh (1996): Serum albumin is associated with skeletal muscle muscle cross-sectional area by dual-energy X-ray absorp- in elderly men and women. Am J Clin Nutr, 64, 552-558. tiometry in frail elderly patients. Am J Clin Nutr, 86, 952- (136) 958. 15)原田 敦,松井康素,竹村真里枝,伊藤全哉,若尾典充, 太田壽城(2005):骨粗鬆症の医療経済―疫学,費用 Baracos VE, Bain VG, Sawyer MB(2012): Muscle wasting is associated with mortality in patients with cirrhosis. Clin Gastroenterol Hepatol, 10, 166-173. と介入法別費用・効用分析.日老医誌,42,596-608. 27)Montero-Odasso M, Duque G(2005): Vitamin D in the ag- 16)原田 敦,中野哲雄,倉都滋之,出口正男,末吉泰信, ing musculoskeletal system: an authentic strength preserv- 町田正文,伊東 学(2008):骨粗鬆症性脊椎骨折の 病態 高齢者脊椎骨折の入院治療に関する施設特性別 全国調査.臨床整形外科,43,303-308. 17)飛田哲朗(2009):経皮的椎体形成術はどのような骨 粗鬆症患者に適しているか.骨粗鬆症治療薬,7,232239. 18)Johnell O, Kanis JA(2006): An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int, 17, 1726-1733. 19)Kitamura S, Hasegawa Y, Suzuki S, Sasaki R, Iwata H, ing hormone. Mol Aspects Med, 26, 203-219. 28)Nakamura K(2009): Locomotive syndrome: disability-free life expectancy and locomotive organ health in a superaged society. J Orthop Sci, 14, 1-2. 29)Nevitt MC, Cummings SR, Kidd S, Black D(1989): Risk factors for recurrent nonsyncopal falls. A prospective study. JAMA, 261, 2663-2668. 30)Ney DM, Weiss JM, Kind AJ, Robbins J(2009): Senescent swallowing: impact, strategies, and interventions. Nutr Clin Pract, 24, 395-413. Wingstrand H, Thorngren KG(1998): Functional outcome 31)Pacifici R, Rupich R, Vered I, Fischer KC, Griffin M, after hip fracture in Japan. Clin Orthop Relat Res, 348, 29- Susman N, Avioli LV(1988): Dual energy radiography 36. 20)Lang T, Streeper T, Cawthon P, Baldwin K, Taaffe DR, (DER): a preliminary comparative study. Calcif Tissue Int, 43, 189-191. Harris TB(2009): Sarcopenia: etiology, clinical conse- 32)Pfisterer MH, Griffiths DJ, Schaefer W, Resnick NM quences, intervention, and assessment. Osteoporos Int, 21, (2006): The effect of age on lower urinary tract function: a 543-559. 21)Lloyd BD, Williamson DA, Singh NA, Hansen RD, Diamond TH, Finnegan TP, Allen BJ, Grady JN, Stavrinos TM, Smith EU, Diwan AD, Fiatarone Singh MA(2009): study in women. J Am Geriatr Soc, 54, 405-412. 33)Rosenberg I(1989): Summary comments. Am J Clin Nutr, 50, 1231-1233. 34)Saltz C, Zimmerman S, Tompkins C, Harrington D, Recurrent and injurious falls in the year following hip frac- Magaziner J(1998): Stress among caregivers of hip frac- ture: a prospective study of incidence and risk factors from ture patients. J Gerontol Soc Work, 30, 167-181. the Sarcopenia and Hip Fracture study. J Gerontol A Biol Sci Med Sci, 64, 599-609. 35)Sanada K, Miyachi M, Tanimoto M, Yamamoto K, Murakami H, Okumura S, Gando Y, Suzuki K, Tabata I, 22)Lyness JM, Noel TK, Cox C, King DA, Conwell Y, Caine Higuchi M(2010): A cross-sectional study of sarcopenia in ED(1997): Screening for depression in elderly primary Japanese men and women: reference values and association care patients. A comparison of the Center for Epidemiologic Studies - depression scale and the geriatric depression scale. Arch Intern Med, 157, 449-454. with cardiovascular risk factors. Eur J Appl Physiol, 110 (1), 57-65. 36)Sayer AA, Syddall HE, Martin HJ, Dennison EM, Anderson 23)Marottoli RA, Berkman LF, Leo-Summers L, Cooney LM FH, Cooper C(2006): Falls, sarcopenia, and growth in Jr(1994): Predictors of mortality and institutionalization early life: findings from the Hertfordshire cohort study. Am after hip fracture: the New Haven EPESE cohort. Established populations for epidemiologic studies of the elderly. Am J Public Health, 84, 1807-1812. 24)Melton LJ 3rd, Khosla S, Crowson CS, O Connor MK, O Fallon WM, Riggs BL(2000): Epidemiology of sarcopenia. J Am Geriatr Soc, 48, 625-630. 25)Moncada LV, Andersen RE, Franckowiak SC, Christmas C J Epidemiol, 164, 665-671. 37)Takahashi C, Fushimi K, Matsuda S(2011): Factors associated with a protracted hospital stay after hip fracture surgery in Japan. Geriatr Gerontol Int, 11, 474-481. 38)Vanitallie TB(2003): Frailty in the elderly: contributions of sarcopenia and visceral protein depletion. Metabolism, 52, 22-26. (2006): The impact of cognitive impairment on short-term 39)Visser M, Kritchevsky SB, Goodpaster BH, Newman AB, outcomes of hip fracture patients. Arch Gerontol Geriatr, Nevitt M, Stamm E, Harris TB(2002): Leg muscle mass 43, 45-52. and composition in relation to lower extremity performance 26)Montano-Loza AJ, Meza-Junco J, Prado CMM, Lieffers JR, in men and women aged 70 to 79: the health, aging and (137) body composition study. J Am Geriatr Soc, 50, 897-904. Osteoporos Int, 17, 61-67. 40)Wada T, Ishine M, Sakagami T, Okumiya K, Fujisawa M, 42)Wang ZM, Visser M, Ma R, Baumgartner RN, Kotler D, Murakami S, Otsuka K, Yano S, Kita T, Matsubayashi Gallagher D, Heymsfield SB(1996): Skeletal muscle K(2004): Depression in Japanese community-dwelling mass: evaluation of neutron activation and dual-energy X- elderly - prevalence and association with ADL and QOL. ray absorptiometry methods. J Appl Physiol, 80, 824-831. Arch Gerontol Geriatr, 39, 15-23. 41)Walsh MC, Hunter GR, Livingstone MB(2006): Sarco- 43)Waters DL, Hale L, Grant AM, Herbison P, Goulding A (2010): Osteoporosis and gait and balance disturbances in penia in premenopausal and postmenopausal women with older sarcopenic obese New Zealanders. Osteoporos Int, 21, osteopenia, osteoporosis and normal bone mineral density. 351-357.
© Copyright 2026 Paperzz