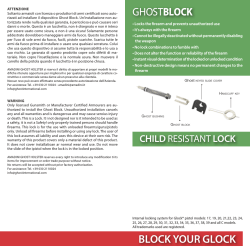
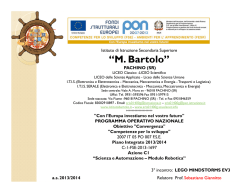
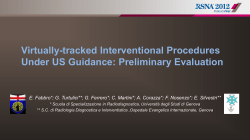
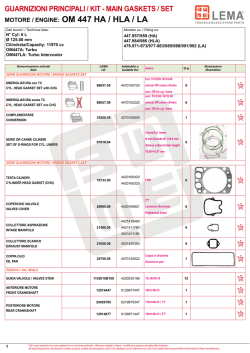
Article ID: WMC004162 ISSN 2046-1690 A Simple Interscalene Block: The Manani's Technique. Some Elements of Distinction from Supraclavicular Perivascular Techniques Corresponding Author: Dr. Gastone Zanette, Senior Lecturer in Anaesthesiology, University of Padua, Department of Neurosciences,Chair of Dental Anaesthesia, via Venezia 90, 35125 - Italy Submitting Author: Dr. Gastone Zanette, Senior Lecturer in Anaesthesiology, University of Padua, Department of Neurosciences,Chair of Dental Anaesthesia, via Venezia 90, 35125 - Italy Article ID: WMC004162 Article Type: Original Articles Submitted on:24-Mar-2013, 07:17:21 PM GMT Published on: 25-Mar-2013, 01:30:08 PM GMT Article URL: http://www.webmedcentral.com/article_view/4162 Subject Categories:ANAESTHESIA Keywords:Interscalene block, Supraclavicular block, Subclavian perivascular block, Anatomical landmarks, Brachial plexus anatomy, Omohyoid muscle How to cite the article:Manani G, Facco E, Zanette G. A Simple Interscalene Block: The Manani's Technique. Some Elements of Distinction from Supraclavicular Perivascular Techniques . WebmedCentral ANAESTHESIA 2013;4(3):WMC004162 Copyright: This is an open-access article distributed under the terms of the Creative Commons Attribution License(CC-BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Source(s) of Funding: Funding or research contracts: None Competing Interests: Conflict of interest: None Additional Files: Comments to this revised manuscript. WebmedCentral > Original Articles Page 1 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM A Simple Interscalene Block: The Manani's Technique. Some Elements of Distinction from Supraclavicular Perivascular Techniques Author(s): Manani G, Facco E, Zanette G Abstract Aim: The aim of this study is an anatomical review regarding the brachial plexus and its relationships with contiguous anatomical structures to better define the Interscalene Brachial Plexus Block Technique already described by Manani (IBPBTM), specifically concerning the point of needle penetration, needle direction and its relationship with OmoClavicular Triangle (OCT) and the inferior belly of omohyoid muscle. Moreover, IBPBTM was compared with other Supraclavicular Perivascular Brachial Plexus Block Techniques (SPBPBT). Materials and methods: The IBPBTM was performed in 80 randomly selected patients scheduled for shoulder surgery. After identification of the OCT and inferior belly of omohyoid muscle, fascial click perception and evocation of adequate muscular contractions, injection of 30 ml of 0.5% bupivacaine in the interscalene space (IS) was performed; the angles delimited by the penetrating needle on the transverse and frontal planes, going across the cutaneous penetration point, were measured and recorded. Moreover, the time of complete anaesthetic block development and failure rate were evaluated by means of an electric stimulation applied on the skin of C3-T1 dermatomes. Results: In almost all patients identification of the OCT, omohyoid inferior belly muscle and fascial click perception were possible. The stimulating needle resulted to be directed with a 14.0±5.2 and -5.1±1.3 degree angle to the frontal and transverse planes going across the cutaneous penetration point, respectively. Deep surgical blocks developed more rapidly on C3, C4 and C5 dermatomes, with respect to the C6, C7, C8-T1 dermatomes. Failure rate was about 8%. Discussion and conclusions: Our results confirm the efficacy of the IBPBTM and provide new insight for a better performance of this block, specifically regarding to the needle penetration angles, the identification of precise anatomical landmarks (OCT and omohyoid inferior belly muscle). The block efficacy was WebmedCentral > Original Articles dependent on a correct performance, including the identification of the IS located medially, behind and above the OCT; on the contrary, in the SPBPBT the needle penetration points are located inside the OCT. From this comparison IBPBTM seems to be superior to SPBPBT in shoulder and peri-shoulder surgery. Introduction Previous studies have shown that interscalene brachial plexus block techniques can be divided into two types of approach depending on whether the local anesthetic solution is injected in the vicinity of the spine or in the thickness of the interscalenic space (IS). In the first case, the area of anesthesia is larger despite lower volumes of local anesthetic; in the second case, the area of anesthesia is more limited, mainly correspondent to the area of innervation of the primary upper trunk of the brachial plexus. Greater extension of the area of anesthesia, using each technique may be achieved using higher volumes of local anesthetic.(1,2) Anesthesia of the brachial plexus innervation area can also be obtained in other ways, among which the supraclavicular and subclavian way.(3) The different ways of approach have generated a multiplicity of techniques, some of which are easy to perform, while others have a more difficult execution and are associated to a higher or lower incidence of success due to the complex anatomy of the region. Anatomical knowledge, acquisition of techniques and their application depending on the surgical requirements, respecting the principles of the techniques used and the skill gained fromfrequent execution of the block, all contribute to excellent results. In this study we want to review our Interscalene Brachial Plexus Block Technique already described by Manani (IBPBTM) (4,5,6,7) along with a comparison of this block with other Supraclavicular Perivascular Brachial Plexus Block Techniques (SPBPBT), in relation to the anatomy of the brachial plexus; moreover, we want to describe more carefully the needle direction, angles and point of penetration. Studying the anatomy of the region we have identified an additional area represented by the inferior belly of the omohyoid muscle that makes the IBPBTM Page 2 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM impossible to compare to the SPBPBT when the omohyoid muscle is easily identified. Anatomy of the brachial plexus in relation to the execution of IBPBTM and SPBPBT.(8) The brachial plexus is located at the base of the neck in the supraclavicular fossa and consists of the anterior branches of C5, C6, C7 and C8 and the anterior branch of T1. (Illustration 1) The plexus is divided into supraclavicular and subclavian portions. The supraclavicular part of the plexus consists of the anterior branches and the primary trunk. Where the supraclavicular part of the plexus joins with the subclavian artery it is referred to as the neurovascular bundle of the subclavian artery (Illustration 2). The neurovascular bundle extends caudally in respect to an imaginary plane between the clavicle and the upper part of the body of the 7th cervical vertebra. The SPBPBT execution area, including the Winnie and Collins(9) and the "classical technique" by Kulenkampff, (10) lies below this plane (Illustration 3). The supraclavicular part of the brachial plexus nerve sheath is surrounded by the IS(8) inside of which, the needle must be inserted in order for the technique to be included among the interscalene block techniques (Illustration 4). The subclavian portion includes the secondary trunk, the origin of the long ramus and it is suitable for the infraclavicular and axillary block techniques. The anterior and middle scalene muscles are important for the anaesthesiologist because the cervical and brachial plexus lie between them. (Illustration 5) The anterior scalene muscle is crossed, in the supraclavicular fossa, by the inferior belly of the omohyoid muscle. (Illustration 6) Between the anterior and middle scalene muscle there is a pyramidal space that contains the brachial plexus and, at the bottom, also the subclavian artery, the so called "inter-scalene triangle" (11) (Illustration 7). The anterior scalene muscles define a depression called inter-scalene groove. The brachial plexus, bonded to the middle scalene muscle through a fibrous lamina, emerges on the lateral margin of the anterior scalene muscle. Emerging between the two scalene muscles, the plexus draws the apex of the inter-scalene triangle located above the upper edge of the omohyoid muscle. The block techniques performed above this landmark are “true interscalene” blocks, like our IBPBTM, because the local anesthetic are introduced through the interscalene sheath in the correspondent groove. The subclavian artery is in relation with the brachial plexus, medially to the scalene muscles, then in between and finally, lateral to the scalene muscles. It WebmedCentral > Original Articles is important to note that the subclavian artery runs in the triangle between the anterior scalene muscle, the omohyoid muscle and the clavicle, also called "the omoclavicular triangle" (Illustration 8).(12) Here, the subclavian artery is in relation to the brachial plexus nerves.(13) The arterial pulsations perceived represent an useful landmark for the performance of SPBPBT and IBPBTM. The omohyoid muscle demarcates the limit between the inferior part of the brachial plexus, organized as neurovascular bundle by the addition of subclavian artery, and the superior part of the brachial plexus which is yet to be formed in the neurovascular subclavian bundle. The brachial plexus is not formed in the neurovascular bundle when, coming out from the anterior and medial scalene muscles, it does not come in relation with the subclavian artery. ( 1 4 ) Approaches below this landmark (omohyoid muscle) must be defined as Supraclavicular Perivascular Brachial Plexus Block Techniques (SPBPBT) while approaches above this landmark must be defined as Interscalene Brachial Plexus Block Technique (IBPBT) as that already described by Manani (IBPBTM).(4) The neurovascular bundle (subclavian artery and brachial plexus) is wrapped by sheaths of thin and dense fibrous lamellar connective tissue connected to the medium and deep cervical fascia.(15,16,17,18) Since this sheath continues with the sheath of the cervical plexus,(19) a single injection of a large volume of local anesthetic in the IS is sufficient to obtain a cervico-brachial plexus block. Bias in performing brachial plexus blocks. These notes about brachial plexus anatomy and relations with contiguous structures, especially with the subclavian artery, suggest that there are some factors that influence the spread of the local anesthetic. Illustration 9 shows the typical distribution of surface anesthesia after IBPBT, SPBPBT, axillary technique and after the combination of IBPBT and axillary technique. Finger pressure was used to impede or facilitate the cephalic progression of the local anesthetic after IBPBT, though Urmey et al.(23) deem there to be no difference in the extension of anesthesia. The search for the "fascial click”, for local anesthetic reflux,(24) for the paresthesias,(25) and for muscle contraction during electric stimulation(26,27) are the prerequisites for the proper execution of the block. These methods seem to be surpassed by the recent ultrasound-guided techniques.(28) The direction of the needle is very important to reach the target. When using IBPBTM, the correct execution requires directing the needle towards the interscalene groove and the IS, although the secondary extensions of connective tissue that wrap the blood vessels and nerves(29) can Page 3 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM be a barrier to the spread of the local anesthetic within the neurovascular space. SPBPBT and IBPBTM: common and different features. The SPBPBT. The SPBPBT has anatomical landmarks which can be used all together or in part. (30,31,32,33) These points are: a) the middle part of the clavicle; b) the outer edge of the clavicular head of the SternoCleidoMastoid muscle (SCM); c) the inner edge of the trapezius muscle at the clavicular insertion; c) the pulsation of the subclavian artery d) Sedillot's triangle which is defined by the two heads of the SCM and the upper margin of the clavicle e) the external jugular vein; f) anterior scalene muscle g) the omoclavicular triangle. SPBPBT occurs when the needle goes through the omoclavicular triangle area involving the primary trunk of the brachial plexus. Kulenkampff's SPBPBT(10) also called "traditional technique", adjusted by Winnie and Collins(9) and the techniques of Alemanno et al.,(34) Vongvises and Panijayanon,(35) Dupre and Danel(34) and the plumb bob technique essentially consist of injecting the local anesthetic in the subclavian perivascular space using a supraclavicular approach. For this reason they are simply called "supraclavicular blocks." The common feature of these techniques is represented by the penetration of the needle in the omoclavicular triangle with many different orientations of the needle, in respect to to the cranio-caudal axis in the techniques of Kulenkamff,(10) Winnie and Collins,(9) Vongvises and Panijayanond (35) and Dupre and Danelàs. (36) The axis of the syringe in Winnie and Collins,(9) Vongvises and Panijayanond(35) and Dupre and Danel(36) techniques is oriented towards the arterial groove of the first rib in the cranio-caudal direction with the risk of an unintentional puncture of the subclavian artery in 20-25% of cases.(37,38) In the plumb-bob and Alemanno's(39-41) techniques, the target is the brachial plexus located in the inferior-medial supraclavicular fossa and the risk is haematoma formation after subclavian artery puncture. The injection of local anesthetic in the subclavian perivascular space, whose section draws a circular surface (Illustration 3A) or ellipsoidal (Illustration 3B) depending on the SPBPBT used, causes a predominant nerve block from C5 to C8. anesthetic injection happens with the piercing of the IS sheath above the inferior belly of omohyoid muscle, the technique, obviously, must be called "INTERSCALENE brachial plexus block technique" (IBPBT). Therefore, IBPBT includes the techniques of Winnie(17), the "double-needle technique" of Pippa et al.(42) and the Manani’s technique(4). The injection of local anesthetic into the IS causes a predominant nerve block from C2 to C5. Complications: SPBPBT and IBPBTM can cause a number of complications which include pneumothorax (incidence of 0.5 to 5.0%), the Claude Bernard-Horner syndrome (incidence of 70-90%), vascular punctures, spinal anesthesia,(43,44), in particular, using Winnie's technique.(17) Finally, there are several neurological complications and unilateral diaphragmatic paralysis even after a low IS block ( 4 5 ) associated with unnoticeable changes in respiratory volumes.(7,46) With SPBPBT, the unilateral diaphragmatic block effect is less frequent, because the different anatomical location of the phrenic nerve on the anterior scalene muscle.(34,46) Methods The patients: The research was carried out on 80 subjects, randomly selected and scheduled for shoulder surgery in the Orthopaedic Department of the University of Padua, after approval of the Ethics Committee of the Department of Medical and Surgical Specialities of Padua University. The IBPBTM. Patients age was between 49 and 80 years, of both gender. The patients physical and anthropological parameters are shown in illustration 10. Patients were informed in detail about the technique of regional anesthesia they would undergo. In particular, they were informed that, on the involved arm, they might experience heat sensation, tingling and loss of sensitivity up to a loss of muscle strength. Furthermore, they had been informed about possible side effects of the regional anesthesia technique. Consent was obtained in accordance with the Hospital of Padua No. 776 of 5 July 2010 through the acquisition of a consent/refusal form for the proposed treatment. Patients with respiratory problems or cognitive impairment and patients scheduled for day surgery were excluded from the study. IBPBTM involves the injection of local anesthetic into the IS space after penetrating the IS sheath, where the brachial plexus has not yet met the subclavian artery to create a neurovascular bundle with ellipsoidal surface section (Illustration 3B). Therefore, if the local The technique: The block technique had been performed in accordance with the procedure already described(4) excluding some modifications proposed in this study. All patients had been placed on the operating table with the chest slightly raised in order to WebmedCentral > Original Articles Page 4 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM optimize diaphragm function, and legs raised in order to avoid sudden hypotension due to Bezold-Jarish reflex. The patients were treated with 0.01 mg fentanyl or midazolam 2 mg intravenously (Illustration 11). Standard monitoring was by ECG, SpO2 and NIBP. After rotation of the patient's head to the other side in respect to the block, the first step was to mark on the skin the subclavian artery pulsation, at the mid-clavicular upper margin (the short red line in illustration 12). From this first landmark, the anesthesiologist drew a vertical line about 2 cm long directed cranially, then, from the apex of this line, another horizontal line about 2 cm long, directed laterally; the outer end of the second, horizontal line corresponds to the needle penetration point. (illustration 13). The inferior belly of the omohyoid muscle was identified by palpating its skin relief with the second and third fingers moving slowly upward from the edge of the clavicle, where the muscle slides forward and up to get to the SCM and then to join the intermediate tendon. The identification of the inferior belly of the omohyoid muscle represents an additional effort to increase safety, allowing the identification of that part of the brachial plexus, situated in a cranial position in respect to the belly muscle, that has not yet formed the neurovascular bundle. To perform the block we used a 50 mm long Uniplex Lanoline Pajunk® 22G needle along with a Multistim Sensor Pajunk® neurostimulator that supplies current from 0 to 60 mA with a stimulation frequency of 1 or 2 Hz. After local anesthesia of the skin, the needle directed in a dorsal, cranial and medial direction, penetrated the interscalenic sheath above the omoclavicular triangle giving the feeling of a “fascial click”. After appropriate muscle response (shoulder abduction, forearm flexion, etc) to appropriate electrical stimulation (0.5 mA), 30 ml of bupivacaine 0.5% were injected within 120 seconds. In many patients it was possible to observe, during the local anesthetic administration, the formation of a typical “sausage swelling” between the anterior and meddle scalene muscles, meaning a correct distribution of the local anesthetic into the IS (illustration 14). The angles formed by the stimulating needle with the transverse and frontal planes, passing through the point of needle penetration, were evaluated after appropriate muscles twitch response. The extension of skin surface anesthesia was assessed by pinprick test, as usual. The evaluations of the skin sensitivity of C3 , C 4 , C 5 , C 6 , C 7 , C 8 -T 1 dermatomes were made every 5 minutes for 30 minutes after the end of the local anesthetic injection. In patients who had not achieved complete analgesia 30 minutes after the local anesthetic injection, the block was evaluated for another 15 minutes. The block WebmedCentral > Original Articles was considered a failure when, after 45 minutes following the local anesthetic injection, the patient continued to perceive the pinprick sensation evoked by the needle. Statistical surveys. The data obtained were expressed as average±SD and, where necessary, the statistical evaluation was performed using χ2 adjusted according to Yates. Results The needle’s angles to perform the block were higher to the frontal plane and lower to the transverse plane. In dorsal needle orientation, angle values ranged between +10 and +20 degrees to the frontal plane; in cranial needle orientation, angles ranged between -2 and -8 degrees to the transverse plane going across the cutaneous penetration point. The average values of the angles to the frontal plane were about 14 degrees and those to the transverse plane were about -5 degrees approximately. Identification of the omohyoid muscle was positive in approximately 75% of patients, indicating that this anatomical landmark is reliable, although not always identifiable; the block failure rate was about 8%. In the first 30 minutes, the Manani’s technique caused a rapid onset of the block in the C3, C4 and C5 cutaneous innervation areas and a slower onset of block in C6, C7, C8-T1 cutaneous innervation areas. Illustration 15 shows the evolution of the block in the C3 and C4 dermatomes of the cervical plexus and in C5, C6, C7, C8-T1 dermatomes of the brachial plexus in the first 30 minutes after the injection of local anesthetic. In the 15 minutes after the local anesthetic injection, the trend towards the complete block was higher in the innervation areas of C3, C4 and C5, with respect to C6, C7, C8-T1. 15 minutes after the onset of anesthesia, the number of patients who had a complete block in C5 was found to be greater than in C3 (χ2 = 4.4, p <0.05), C6 (χ2 = 31 , 4, p <0.01), C7 (χ2 = 29.2, p <0.01) and C8-T1 (χ2 = 34.4, p <0.01). After 30 minutes, the same effect was found to be greater than C7 (χ2 = 7.2, p <0.01) and C8-T1 (χ2 = 37.4, p <0.01). These results indicate that this technique is to be preferred for shoulder and clavicle surgery. Discussion A recent survey carried out to describe brachial plexus anesthesia techniques (28) has shown that IS and cervical paravertebral approaches ensure a higher percentage of success in shoulder and proximal humerus surgery and that the differences between Page 5 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM IBPBT and SPBPBT are related to the local anesthetic injection onto the nervous and neurovascular compartments respectively. Previous studies by Winnie and Collins (9) performed after a careful re-evaluation of the brachial plexus anatomy and by applying the subclavian perivascular space concept developed SPBPBT. At the same time Burnham(47) and Eather(48) confirmed this concept by describing the same technique performed at the axilla and obtained by administering large volumes of local anesthetic into the axillary neurovascular compartment. The IBPBTM causes an extension of anesthesia comparable to that obtained with the IBPBT described by Winnie.(17) Our technique offers a complete anesthesia of the cervical plexus' lowest roots and the highest roots of brachial plexus which are necessary to perform shoulder surgery.(49-52) The high rate of success of this technique comes from having identified a plane were the needle lies in relation to the frontal plane, passing between the anterior and medium scalene muscle and being directed anteriorly and externally according to an average angle of 10-20 degrees. The angle of the needle to the transverse plane, variable from -2 to -10 degrees, allows us to reach the IS cranially at somewhat higher levels, compared to the point of cutaneous penetration. Therefore with our technique, after injection of local anaesthetic through the IS sheath in a point slightly lower than that indicated by Winnie,(17) we obtain a cervico-brachial plexus block (20) useful for shoulder and clavicle surgery. Concluding, in order to obtain a cervico-brachial surgical anesthesia distribution, the important factors include: correct execution of the block, continued use of the technique, good anatomical knowledge.1 References 1. Pippa P, Cuomo P, Panchetti A, Scarchini M, Poggi G, D'Arienzo M. High volume and low concentration of anaesthestic solution in the perivascular interscalene sheat determines quality of the block and incidence of complications. Eur J Anaesthesiol 2006; 10: 855-60. 2. Rucci FS, Barbagli R, Doni L. Quanti sono i blocchi interscalenici? Riflessioni su 109 casi eseguiti con tecniche diverse. Min Anestesiol 1992;58:27-38. 3. Urmey WF. Upper extermity blocks. In Regional Anesthesia and Analgesia. Ed. DL Brown, Saunders. Cap. 16, pp. 254-278, 1996. 4. Manani G, Civran E. Il blocco interscalenico basso: una tecnica innovativa. Acta Anaesth Ital 1998;49:221-230. 5. Manani G, Scorrano Pettine S. Vie di approccio sopraclavicolari ai plessi brachiale e cervicale. Monitor WebmedCentral > Original Articles 2000;2:16-26. 6. Zanette G, Travaglini V, Rinaldi VP, Caputo P, Manani G. Il blocco nervoso nella chirurgia della spalla. Atti del convegno del 6 marzo 1999. Incontri di Anestesia e Rianimazione della riviera del Brenta, p. 30-41. 7. Zanette G, R. Bonato R, A. Marcassa A, Sorbara C, Manani G. Impiego dell’anestesia locoregionale per riduzione di lussazione inveterata di spalla in paziente con cardiopatia invalidante. ALR 2001;10:128-131. 8. Chiarugi G. Istituzioni di anatomia dell’uomo. Soc Ed. Libraria, Milano 1954;5:57-91. 9. Winnie AP, Collins VJ. The subclavian perivascular technique of brachial plexus anesthesia. Anesthesiology 1964;25:353-363. 10. Kulenkampff D. Die Anasthesia des plexus brachialis. Zentrabl Chir 1911;38:1337-1340. 11. Savgaonkar MG, Chimmalgi M, Kulkarni UK. Anatomy of inter-scalene triangle and its role in thoracic outlet compression syndrome. J Anat Soc India 2006;55:52-55. 12. Sobotta J. Atlante di anatomia descrittiva dell’uomo. Vol. III. Ed. Sansoni, 1955, p. 18. 13. Chiarugi G. Istituzioni di anatomia dell’uomo. Soc. Ed. Libraria, Milano 1954;2:414-417. 14. Chiarugi G. Istituzioni di anatomia dell’uomo. Soc. Ed. Libraria, Milano. 1954;2:91-93. 15. De Jong RH. Axillary block of the brachial plexus. Anesthesiology 1961;22:215-225, 1961. 16. Partridge BL, Katz J, Bernirschke K. Functional anatomy of the brachial plexus sheath: implication for anesthesia. Anesthesiology 1987;66:743-747. 17. Winnie AP. Interscalene brachial plexus block. Anesth Analg 1970;49:455-466. 18. Winnie AP. Plexus anestesia; perivascular technique of brachial plexus block, 2nd ed. p. 117, Philadelphia, WB Saunders Co, 1990. 19. Chiarugi G. Istituzioni di anatomia dell’uomo. Soc. Ed. Libraria, Milano. 1954;2:93-101 20. Vester-Andersen T, Christiansen C, Hansen A, Sorensen M, Meisler C. Interscalene brachial plexus block: area of analgesia, complications and blood concentrations of local anesthetics. Acta Anaesth Scand 1981;25:81-84. 21. Brandão RC, Lerner S, Ranger W, Rodrigues I. Bloqueio di plexo braquial. Rev Bras Anesthesiol 1971, ano 21, n 3. 22. Winnie AP, Radonjic R, Akkineni SR, Durrani Z. Factors influencing distribution of local anesthetic injected into the brachial plexus sheath. Anesth Analg 1979;58:225-234. 23. Urmey WF, Gloeggler PJ, Parab S, Sharrock NE. Does a digital pressure technique alter measurable sensory, motor, of diaphragm effects? Anesth Analg Page 6 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM 1992;74:s327. 24. Miranda DR. Identification of the brachial plexus perivascular space. Br J Anaesth 1977;49: 721-722. 25. Bonica JJ. Il dolore. Ed. Vallardi, 1959, pp. 240-241. 26. Fanelli G, Casati A, Chelly JE, Bertini L. Blocchi periferici continui. Ed. Mosby Italia 2001. 27. De QH Tran, Clemente A, Doan J, Finlayson RJ. Brachial plexus blocks: a review of approaches and techniques. Can J Anesth 2007;54:662-674. 28. Marhhofer P, Greher M, Kapral S. Ultrasound guidance in regional anaesthesia. Br J Anaesth 2005;94:7-17 29. Chiarugi G. Istituzioni di anatomia dell’uomo. Soc. Ed. Libraria. Milano 1954;2:99. 30. Gauthier-Lafaye P, Kieny P, Keller B. Precis d’anesthésie loco-régionale. Aette Ed. Paris 1970, pp. 42-48. 31. Moore DC. Regional Block. A handbook for use in the clinical practice of medicine and surgery IV ed, CC Thomas, Springfield 1975, pp. 221-242. 32. Rigal MC, Estève E, Arlan R, Pech C. Blocs du plexus brachial dans la chirurgie du member supérieur. A propos de 139 cas. Anesth Analg Réan 1979;36:231-234. 33. Wasmer JM, Dupeyron JP, Fresnel P, Foucher G, Gauthier-Lafaye IJ. Blocs du plexus brachial per voie supra-clavicolaire. Anesth Analg Réan 1974;31:120-128. 34. Alemanno F, Capezzoli G, Egarter-Vigl E, Gottin L, Bartoloni A. The middle interscalene block: cadaver study and clinical assessment. Reg Anesth Pain Med 2006;31:563-568. 35. Vongvises P. Panijayanond T. A parascalene technique of brachial plexus anesthesia. Anesth Analg 1979;58:267-273. 36. Dupré LJ, Danel V. Nouveoux repères pour le bloc du plexus brachial par voie supra-claviculaire. Avec une sèrie clinique de 44 cas. Anesth Analg Rèan 1980;37:727-729. 37. Hickey R, Garland TA, Ramamurthy S. Subclavian perivascular block: influence of location of paresthesia. Anesth Analg 1989;68:767-771. 38. Hickey R, Hoffman J, Ramamurthy S. Transarterial techniques are not effective for subclavian perivascular block. Reg Anesth 1990;15:245-249. 39. Alemanno F. Tecniche sopraclaveari di blocco del plesso brachiale. Min Anestesiol 2001; 67:50-55. 40. Alemanno F. Un nuovo approccio al plesso brachiale. Min Anestesiol 1992;58:403-406. 41. Hahn MB, McQuillan PM, Sheplock GJ. Anestesia loco-regionale. Mosby Doyma Italia S.r.l. 1997. pp. 105-106. 42. Pippa P, Cominelli E, Marinelli C, Alto S. Nuove WebmedCentral > Original Articles prospettive nel blocco del plesso brachiale per via interscalenica: tecniche del “doppio ago” e del “mandrino gassoso”. XLII Congresso nazionale SIAARTI. Sorrento 20-23 ottobre 1988, pp. 19-22. 43. Gregoretti S. Case of high spinal anesthesia as a complication of an interscalenic brachial plexus block. Min Anestesiol 1980;46:437-439. 44. Caputo F, Ventura R. Brachial plexus block. Effect of low interscalene approach on phrenic nerve paresis. Min Anestesiol 2000;66:195-199. 45. Urmey WF. Interscalene block and pulmonary function. Anesth Analg 1993;76:675-676. 46. Neal JM, Moore JM, Kopacz DJ, Kramer DJ, Plorde JJ. Quantitative analysis of respiratory, motor, and sensory function after supraclavicular block. Anesth Analg 1998;86:1239-1244. 47. Burnham PJ. Regional block of the great nerves of the upper arm. Anesthesiology 1958;19:281-284. 48. Eather KF. Axillary brachial plexus block. Anesthesiology 1958;19:683-684. 49. Heffington CA, Thompson RC. The use of interscalene block anesthesia for manipulative reduction of fractures and dislocations of the upper extremities. J Bone Joint Surg 1973; 55-A:83-86. 50. Wildsmith JAW, Tucker GT, Cooper S, Scott DB, Covino BG. Plasma concentrations of local anaesthetics after interscalene brachial plexus block. Br J Anaesth 1977;49:461-466. 51. Pippa P, Rucci FS. Preferential channelling of anaesthetic solution injected within the perivascular axillary sheath. Eur J Anaesthesiol 1994;11:391-396. 52. Pippa P. Brachial plexus block using a new subclavian perivascular technique: the proximal cranial needle approach. Eur J Anaesthesiol 2000;17:120-125. Page 7 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustrations Illustration 1 Illustration 1. Brachial plexus anatomy. The first, more cranial, transverse line divides the ventral ramus of C5 – T1 (blue colour), located between the scalene muscles, from the brachial trunks (upper, middle, lower), located in the supraclavicular region. Peripherally, each trunk splits forming the anterior and posterior divisions, the cords (lateral, posterior, medial) and finally the terminal branches (radial, ulnar, median, axillary, musculocutaneous nerves). Illustration 2 Illustration 2. Cross-section of the subclavian perivascular space , at level of the 7th cervical vertebra. The 5th and 6th root of the plexus run in between the fascia that wraps the anterior and middle scalene muscles.(9) WebmedCentral > Original Articles Page 8 of 21 WMC004162 WebmedCentral > Original Articles Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Page 9 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 3 Illustration 3. The brachial plexus sheath on the left. Section A represents the needle penetration point according to the subclavian perivascular block techniques. Section B represents the needle penetration point for the subclavian perivascular block by Winnie and Collins.(9) Illustration 4 Illustration 4. Cross section at the level of the 6th cervical vertebra. Notables are the anterior and middle scalene muscles in which space run the ventral rami and the brachial plexus trunks. The local anaesthetic must penetrate into this space to perform IBPBTM and the needle must have passed the superficial cervical fascia and the IS nerve sheath. WebmedCentral > Original Articles Page 10 of 21 WMC004162 WebmedCentral > Original Articles Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Page 11 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 5 Illustration 5. Anterior, middle and posterior scalene muscles. The brachial plexus and the subclavian artery run between the anterior and middle scalene muscles through the IS triangle. Illustration 6 Illustration 6. Omohyoid muscle. The omohyoid muscle crosses the anterior and middle scalene muscles in the supraclavicular fossa. WebmedCentral > Original Articles Page 12 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 7 Illustration 7. Position of the interscalene triangle between the middle and anterior scalene muscles. This pyramidal space contains the brachial plexus and, at the bottom, also the subclavian artery. Illustration 8 Illustration 8. The omoclavicular triangle, the area where the needle enters to perform Supraclavicular Perivascular Brachial Plexus Block Techniques. WebmedCentral > Original Articles Page 13 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 9 Illustration 9. Areas of skin anaesthesia obtained after interscalene block, after supraclavicular perivascular block, after axillary block and after a combined interscalene-axillary technique. WebmedCentral > Original Articles Page 14 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 10 Illustration 10. Patients and surgery features. Illustration 10. Patients and surgery features. Average±SD. Anthropological characteristics / Pathologies Numbers Patients (n) Age (years) Gender (M / F) Weight (kg) Height (cm) ASA (1/2/3) 80 63.2±10.8 24/56 63.6±9.6 162.4±4.9 21/51/8 Pathologies Humeral neck fracture Rotator cuff tear Humeral shaft fracture Clavicle fracture Supraspinous ligament tear 38 21 12 7 2 Surgical procedures Osteosynthesis Arthroscopy Osteosynthesis Osteosynthesis Arthroscopy Legend: ASA = American Society of Anesthesiologists WebmedCentral > Original Articles Page 15 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 11 Illustration 11. Anaesthesia management. Illustration 11. Characteristics of anesthesia management. Average±SD. Patients (n) 80 Posture: semi-recumbent 80 Preanesthesia: fentanyl/midazolam 46/34 Skin wheal (yes/no) 76/4 Omohyoid muscle inferior belly identification (yes/no) 64/16 Fascial click (yes/no) 73/7 Bupivacaine 0.5% 80 Volumes: 30/40 ml 69/11 Injection time (sec) 109±7.6 Needle angle to transverse plane -5.1±1.3 ° Needle angle to frontal plane 14.0±5.2 ° Block failures (yes/no) WebmedCentral > Original Articles 6/74 Page 16 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 12 Illustration 12. Projection on the skin of the interscalene space (black dashed line) and interscalene groove (pink dashed line). SCM = sternocleidomastoid muscle, TR = trapezius muscle; omohy = projection on the skin of the supraclavicular area of the omohyoid muscle; CLAV = clavicle. The red horizontal dotted line and red vertical line (subclavian artery pulse) are important landmarks for the execution of interscalene block. Illustration 13 Figure 13. Needle penetration into an upper-outer point in respect to the subclavian artery pulsation, on the midpoint of the clavicle; the depicted 20G needle is 50 mm long; X = middle of the clavicle, x1 = subclavian pulsation point, x2 = far end of the first line, x3 = far end of the second line . WebmedCentral > Original Articles Page 17 of 21 WMC004162 WebmedCentral > Original Articles Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Page 18 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Illustration 14 Figure 14. The two black lines outline the so called “sausage”, typical sign of interscalene sheath relaxation caused by the spread of the local anaesthetic into the interscalene space. Illustration 15 Figure 15. Indicative curves representing the percentage of patients who experienced complete analgesia from electrical stimulation to the dermatomes examined in the first thirty minutes after the block. The most sensitive dermatomes were C3, C4 and C5 (black dots). The effect of complete analgesia in dermatomes C8-T1, C7 and C6 was relatively minor (white dots). WebmedCentral > Original Articles Page 19 of 21 WMC004162 WebmedCentral > Original Articles Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Page 20 of 21 WMC004162 Downloaded from http://www.webmedcentral.com on 25-Mar-2013, 01:30:09 PM Disclaimer This article has been downloaded from WebmedCentral. With our unique author driven post publication peer review, contents posted on this web portal do not undergo any prepublication peer or editorial review. It is completely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscript but also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions before submitting any information that requires obtaining a consent or approval from a third party. Authors should also ensure not to submit any information which they do not have the copyright of or of which they have transferred the copyrights to a third party. Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater to the needs of an individual patient. The web portal or any content(s) therein is neither designed to support, nor replace, the relationship that exists between a patient/site visitor and his/her physician. Your use of the WebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harm that you may suffer or inflict on a third person by following the contents of this website. WebmedCentral > Original Articles Page 21 of 21
© Copyright 2026 Paperzz