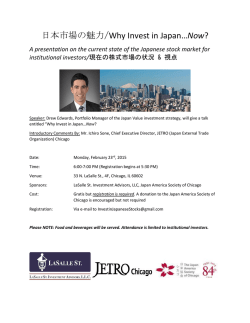
Evaluation of Stridor Cecille G. Sulman, MD Attending Physician, Division of Otolaryngology Children’s Memorial Hospital Objectives • Understand the components of the history and physical exam in the evaluation of stridor • Learn the most common etiologies of stridor • Have a basic understanding on how the most common etiologies of stridor are treated © 2005 Children’s Memorial Hospital, Chicago, Illinois 2 What is stridor? © 2005 Children’s Memorial Hospital, Chicago, Illinois 3 Stridor • High pitched respiratory sound produced by rapid, turbulent flow of air through a narrowed segment of the respiratory tract • Stridor may be inspiratory, expiratory, or biphasic • Site of lesion correlates with stridor © 2005 Children’s Memorial Hospital, Chicago, Illinois 4 Inspiratory stridor • Extrathoracic • Supraglottis/larynx – Laryngomalacia – Supraglottic mass – Glottic lesions – Vocal cord paralysis © 2005 Children’s Memorial Hospital, Chicago, Illinois 5 Biphasic stridor • Bilateral vocal cord paralysis • Laryngeal masses/web • Subglottic – Stenosis – Hemangioma • Respiratory papillomas • Infectious – Epiglottitis – Croup © 2005 Children’s Memorial Hospital, Chicago, Illinois 6 Expiratory stridor • Intrathoracic • Mimics asthma • Trachea or bronchi – Tracheomalacia – Bronchomalacia – Vascular abnormalities – Extrinsic compression © 2005 Children’s Memorial Hospital, Chicago, Illinois 7 Stridor - infants • • • • • • Congenital laryngeal anomalies 60% Congenital tracheal anomalies 16% Congenital bronchial anomalies 5% Infectious conditions 5% Internal laryngeal trauma 5% Other 7% Holinger LD. Ann Otol Rhin 89 (5):397-400,1980 © 2005 Children’s Memorial Hospital, Chicago, Illinois 8 Evaluation - history • Birth history • Age of onset of stridor – Gradual, progressive, or sudden • Quality of stridor – Inspiratory, biphasic, expiratory – Positional – Association with feeds © 2005 Children’s Memorial Hospital, Chicago, Illinois 9 Evaluation - history • Voice quality – Strength, hoarseness • Cyanosis • Previous intubation • Aspiration or reflux © 2005 Children’s Memorial Hospital, Chicago, Illinois 10 Evaluation -SPECS-R History • S: Severity – subjective (parents) • P: Progression • E: Eating – Difficulty feeding, aspiration, failure to thrive • C: Cyanotic - Apparent life threatening events • S: Sleep - Retractions • R: Radiology © 2005 Children’s Memorial Hospital, Chicago, Illinois 11 Evaluation – physical exam • Assess the level of respiratory distress • Signs of respiratory collapse – Tachypnea, fatigue, severe work of breathing • Immediate transfer to a hospital • Secure airway – intubation or tracheotomy © 2005 Children’s Memorial Hospital, Chicago, Illinois 12 Evaluation – physical exam • Observation at rest and after stimulation • Nasal flaring, subcostal or suprasternal retraction, abdominal movement, and cyanosis • Character, quality, and severity of stridor © 2005 Children’s Memorial Hospital, Chicago, Illinois 13 Evaluation – physical exam • Oral cavity, relative size of the mandible and tongue • Level of alertness and muscular tone • Auscultation at mouth, neck, and chest © 2005 Children’s Memorial Hospital, Chicago, Illinois 14 Evaluation – office endoscopy • Flexible Fiberoptic Laryngoscopy (FFL) – – – – – Nasal cavity Choanae Oropharynx Supraglottis Larynx • No sedation • Instant feedback © 2005 Children’s Memorial Hospital, Chicago, Illinois 15 Evaluation - radiographs • Airway films – AP and lateral • Larynx • Subglottis • Tracheal column © 2005 Children’s Memorial Hospital, Chicago, Illinois 16 Airway endoscopy indications • Diagnosis is unclear • Subglottic lesion suspected • Concern for a second airway lesion • Components – Awake FFL – Direct laryngoscopy – Rigid bronchoscopy © 2005 Children’s Memorial Hospital, Chicago, Illinois 17 Airway endoscopy • Pediatric anesthesia • Appropriate sized equipment for age • Team familiar with equipment • Careful preparation • Intensive care unit © 2005 Children’s Memorial Hospital, Chicago, Illinois 18 Airway endoscopy © 2005 Children’s Memorial Hospital, Chicago, Illinois 19 Normal airway Larynx Subglottis Trachea Trachea Bronchus © 2005 Children’s Memorial Hospital, Chicago, Illinois 20 Anatomy • Narrowest portion of infant airway is the subglottis • Normal infant subglottic larynx – 5 mm x 7 mm – 1 mm of edema reduces the crosssectional area to 44% of normal airway © 2005 Children’s Memorial Hospital, Chicago, Illinois 21 Laryngomalacia • Most common congenital laryngeal anomaly • Most frequent cause of stridor • Inspiratory stridor – biphasic if severe • Etiology unknown - delay of maturation • Associated second airway lesion in 27% © 2005 Children’s Memorial Hospital, Chicago, Illinois 22 Laryngomalacia Onset – first few weeks of life Stridor worsens before improving Resolves by 18 – 24 months Exacerbated by crying, agitation, feeding, URI, supine position • Improved in prone position and the neck hyperextended • • • • © 2005 Children’s Memorial Hospital, Chicago, Illinois 23 Laryngomalacia • • • • • Epiglottic collapse Arytenoid collapse Tubular epiglottis Erythema Edema © 2005 Children’s Memorial Hospital, Chicago, Illinois 24 Laryngomalacia • Mild laryngomalacia – Expectant management – Reflux therapy – behavioral precautions • Moderate laryngomalacia – Reflux therapy – medications and behavioral precautions – Close monitoring – Airway films © 2005 Children’s Memorial Hospital, Chicago, Illinois 25 Laryngomalacia • Severe laryngomalacia – Barium swallow – assess for vascular anomalies and aspiration – Airway films – Airway endoscopy Aberrant left subclavian artery © 2005 Children’s Memorial Hospital, Chicago, Illinois 26 Laryngomalacia • Surgical interventions – CO2 laser supraglottoplasty – Laryngoplasty – Tracheostomy © 2005 Children’s Memorial Hospital, Chicago, Illinois 27 Vocal cord paralysis • Second most common congenital anomaly of the larynx • No gender predilection • Unilateral vocal cord paralysis – Quiet, hoarse voice, +/- stridor – Aspiration • Bilateral vocal cord paralysis – Strong voice, biphasic stridor – Respiratory distress © 2005 Children’s Memorial Hospital, Chicago, Illinois 28 Vocal cord paralysis • Congenital – CNS: Arnold Chiari, hydrocephalus, encephalocele – Multiple anomalies – cardiac, pulmonary • Acquired – – – – Idiopathic – most common etiology Iatrogenic – surgical, birth trauma Neoplasia Rare: tetanus, botulism, Guillain-Barre, Myasthenia Gravis © 2005 Children’s Memorial Hospital, Chicago, Illinois 29 Vocal cord paralysis • Labs – CBC, FTA-ABS, Lyme titers, TFT’s, lead screen • Imaging – CT scan - skull base to diaphragm to rule out lesions along the vagus nerve – Modified barium esophagram – aspiration, vascular abnormalities © 2005 Children’s Memorial Hospital, Chicago, Illinois 30 Vocal cord paralysis • Age < 6 months – Observation - vocal cord may recover – Tracheotomy for bilateral paralysis, or for aspiration in unilateral paralysis – Surgery may affect laryngeal growth • Age > 6 months – Observation – vocal cord may recover – Speech therapy – Surgery – no guidelines on duration to wait prior to surgery © 2005 Children’s Memorial Hospital, Chicago, Illinois 31 Vocal cord paralysis • Surgical treatment: – Unilateral - vocal fold injection, medialization thyroplasty – Bilateral - tracheotomy, cordotomy, arytenoidpexy, arytenoidectomy © 2005 Children’s Memorial Hospital, Chicago, Illinois 32 Subglottic stenosis • Third most common congenital anomaly of the larynx • Biphasic stridor • History of recurrent croup • Congenital – Cricoid cartilage deformity • Acquired – Trauma – intubation – GERD © 2005 Children’s Memorial Hospital, Chicago, Illinois 33 Subglottic stenosis © 2005 Children’s Memorial Hospital, Chicago, Illinois 34 Subglottic stenosis © 2005 Children’s Memorial Hospital, Chicago, Illinois 35 Subglottic stenosis • Reflux treatment • Serial dilations • Endoscopic laser excision • Anterior Cricoid Split • Cricotracheal resection • Laryngotracheal Reconstruction (LTR) © 2005 Children’s Memorial Hospital, Chicago, Illinois 36 Subglottic hemangioma • 1.5% of congenital laryngeal anomalies • Females > males • Asymptomatic at birth with progressive respiratory distress • Biphasic stridor - symptoms similar to croup • 50% have a cutaneous hemangioma © 2005 Children’s Memorial Hospital, Chicago, Illinois 37 Subglottic hemangioma © 2005 Children’s Memorial Hospital, Chicago, Illinois 38 Subglottic hemangioma • Steroids - inhibit angiogenesis • Laser ablation - isolated lesions • Alpha-interferon - interferes with endothelial locomotion • All of these modalities are effective in about 60%-80% of cases © 2005 Children’s Memorial Hospital, Chicago, Illinois 39 Respiratory papillomas • Human papilloma virus (HPV) • Incidence < 14 y.o. - 4.3/100,000 • Develop anywhere in the respiratory tract, primarily the larynx • Biphasic or inspiratory stridor • Malignant degeneration in 3-5% • Evaluate for pulmonary involvement with CXR © 2005 Children’s Memorial Hospital, Chicago, Illinois 40 Respiratory papillomas © 2005 Children’s Memorial Hospital, Chicago, Illinois 41 Respiratory papillomas • Surgical debulking – Laser – Microdebrider • Cidofovir – Inhibits DNA polymerization • Alpha interferon – Inhibits translation of viral protein © 2005 Children’s Memorial Hospital, Chicago, Illinois 42 Airway foreign body • National Safety Council - 4300 deaths from choking in 2003 in the US • Children < 3 years are at higher risk • Peanuts most common • History is the key element in diagnosis • Acute onset of stridor accompanied by a choking spell • Airway films and CXR © 2005 Children’s Memorial Hospital, Chicago, Illinois 43 Airway foreign body Electrical wire in larynx © 2005 Children’s Memorial Hospital, Chicago, Illinois 44 Tracheomalacia • Expiratory wheezing, stridor, cough • Primary tracheomalacia – Resolves by 18-24 months – Severe – tracheotomy and positive pressure ventilation • Secondary tracheomalacia – Compression by vascular structures – Associated with tracheoesophageal fistula – Tracheotomy, treat underlying condition © 2005 Children’s Memorial Hospital, Chicago, Illinois 45 Tracheomalacia Tracheomalacia Aberrant innominate artery © 2005 Children’s Memorial Hospital, Chicago, Illinois 46 Bronchomalacia • Expiratory wheezing, stridor • Present before 6 months old • Bronchus lacks rigidity with insufficient cartilage or external compression • Unilateral, bilateral, tracheomalacia • Symptoms decrease as child grows • Severe – tracheotomy, positive pressure ventilation, stent © 2005 Children’s Memorial Hospital, Chicago, Illinois 47 Bronchomalacia Inspiration Expiration © 2005 Children’s Memorial Hospital, Chicago, Illinois 48 GERD • Incidence – 18% of all infants – Up to 70% with co-existing medical conditions • Anatomy Reflux laryngitis – Shorter intra-abdominal esophagus – Immature LES – Swallow less while asleep Normal larynx © 2005 Children’s Memorial Hospital, Chicago, Illinois 49 GERD • Animal models have demonstrated damaging effects of GERD on the larynx • Laryngomalacia patients with FTT or apnea and bradycardia improve with treatment • Treatment of GERD is thought to improve outcomes for laryngotracheal reconstruction McGuirt WF. Ped Clin North Amer 50:487-502, 2003 © 2005 Children’s Memorial Hospital, Chicago, Illinois 50 Conclusions • Stridor is a symptom and not a diagnosis • History and physical are key in diagnosis • Airway endoscopy is an important adjunct • Proper management is possible only after a precise diagnosis has been established © 2005 Children’s Memorial Hospital, Chicago, Illinois 51
© Copyright 2026 Paperzz