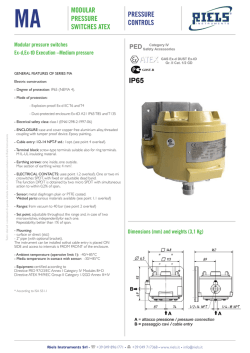
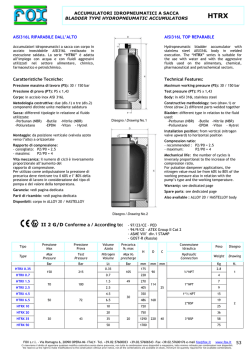
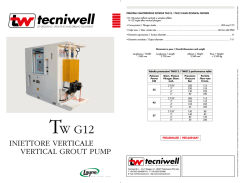
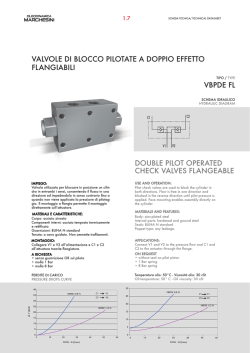
Evaluation monitoring of baroreceptor reflex by blood pressure in unanesthetized cats GIOVANNI BERTINIERI, MARCO DI RIENZO, ANITA CAVALLAZZI, ALBERT0 U. FERRARI, ANTONIO PEDOTTI, AND GIUSEPPE MANCIA Cattedra di Semeiotica Medica and Istituto di Clinica Medica Generale e Terapia Medica, Universitk di Milano, Consiglio Nazionale delle Ricerche and Ospedale Maggiore; Centro di Bioingegneria, Fondazione Pro Juventute e Politecnico di Milano, 20122 Milan, Italy BERTINIERI, LAZZI, ALBERTO SEPPE MANCIA. GIOVANNI, MARCO DI RIENZO, ANITA CAVALU. FERRARI, ANTONIO PEDOTTI, AND GIUEvaluation of baroreceptor reflex by blood pres- sure monitoring in unanesthetized cats. Am. J. Physiol. 254 (Heart Circ. Physiol. 23): H377-H383, 1988.-The arterial baroreceptor control of the sinus node operating in unanesthetized conditions was evaluated in 10 cats in which blood pressure was recorded intra-arterially and scanned by a computer to identify the “spontaneous” sequences of three or more consecutive beats in which systolic blood pressure (SBP) progressively rose and pulse interval (PI) progressively lengthened (type 1 sequences) or SBP progressively fell and PI progressively shortened (type 2 sequences). Many type 1 and 2 threebeat sequences were found; four-, five-, and six-beat sequences of either type were progressively less common, and sequences longer than six beats were almost never identified. The regression coefficient was 30% greater for type 1 than for type 2 sequences. However a prominent feature of either regression coefficient was a wide scattering in each cat (average variation coefficient 50.9 k 5.5%). The regression coefficient values were related to some extent to the PI but not to the SBP existing at the beginning of the sequence. Sinoaortic denervation dramatically reduced the number of sequences of either type. These data validate a method for collecting a large number of observations on the baroreceptor-heart rate reflex in physiological conditions. This method may improve understanding of baroreflex involvement in integrated cardiovascular regulation. baroreflexes; denervation heart rate; joint pattern analysis; sinoaortic CONTROL of the sinus node is commonly evaluated by maneuvers that increase or reduce arterial baroreceptor activity via mechanically or pharmacologically induced rises and falls in blood pressure (10, 16, 21, BARORECEPTOR 24, 26). In unanesthetized animals blood pressure is characterized by spontaneous increases and decreases (22). This results in alterations in baroreceptor activity and raises the possibility that their reflex effects on the heart can be studied without pharmacological or mechanical interventions. In the present study on unanesthetized cats we have tested this possibility by computer analysis of the intra-arterial blood pressure and pulse interval signals. The results demonstrate that spontaneous blood pressure changes can be used to study the baroreceptor-heart rate reflex. II 0363-6135/88 $1.50 Copyright METHODS The study was performed in 10 unanesthetized cats in which blood pressure was recorded twice via a catheter implanted in the abdominal aorta. The implantation was performed aseptically under ether anesthesia 2 days before the first recording session, using the right or left femoral artery. The proximal end of the catheter was guided subcutaneously to an exit near the paravertebral muscles to which it was secured by silk sutures. Once implanted, the catheter was kept patent by periodical flushing with heparinized solution (5 U/ml saline). Each blood pressure recording was obtained with the cat placed in a Plexiglas box large enough to allow activities, such as stretching, standing, eating, drinking, self cleaning, etc., to be attended without restriction. The box was brought to the laboratory l-2 days before the recording to make the cat accustomed to the environment and the people working nearby. During the recording the arterial catheter emerging from the cat’s back was connected to a rigid-walled polyethylene tube that reached a transducer (Statham P23 DC) placed outside the cage at the animal’s heart level. The blood pressure signal was directed to the amplifier of a Grass polygraph and then to a tape recorder (Racall Store 4), to allow its subsequent analysis by a computer (see below). The recording system showed an optimal-response to a square-wave signal (no overshoot and no damping) up to 15 Hz. Furthermore, the equipment gave a linear response from 0 to 200 mmHg and showed no drift of the 0 signal. This ensured the reliability of the recording throughout. Protocol and arterial baroreceptor denervation. After implantation of the aortic catheter, blood pressure was recorded continuously for 2-4 h (mean t SE 3.0 t 0.4). Subsequently, the cat was anesthetized with ketamine (50 mg/kg body wt im). The neck was incised under aseptic conditions to expose the carotid arteries and the vagi (25). All tissues between the external and the internal carotid arteries were enclosed in a double ligature and cut to sever baroreceptor fibers originating from the carotid sinuses. The aortic nerves were divided from the vagi near their connection with the nodose ganglion and cut to sever baroreceptor fibers originating from the aortic arch and the major intrathoracic arteries. The common carotid arteries were isolated to sever aortic baroreceptor fibers possibly traveling outside the aortic 0 1988 the American Physiological Society H377 H378 BEAT-TO-BEAT EVALUATION nerves (13). The completeness of the baroreceptor denervation was verified after surgical intervention by the drastic reduction of the bradycardia induced by an intravenous bolus of phenylephrine hydrochloride as compared with the response observed before the surgical intervention (-26.3 t 7.2 vs. -1.8 t 0.4 beats/min). The cat was allowed to recover for 7-10 days after which a second intra-arterial blood pressure recording of 2-4 h (3.0 t 0.5) was performed. Data analysis. The data stored in the tape recorder were analyzed by a computer (Digital PDP 11/34), which sampled on 12 bit the blood pressure tracing at 600 Hz, i.e., at 1.6-ms intervals. The system of analysis could discriminate minute differences in systolic blood pressure and allowed a maximal error in the estimation of the pulse interval change of 3.2 ms. The results were displayed on a graphic video and examined by an operator who checked and eliminated any grossly distorted pressor waves and stored on a magnetic disk an artifactfree blood pressure signal. This was reanalyzed by the computer to obtain all the systolic blood pressure values OF THE BAROREFLEX occurring throughout the recording period and to derive from them all pulse intervals as well. The computer was also programmed to determine the difference between each two consecutive systolic blood pressure or pulse interval values and to identify the sequences characterized by the fact that 1) systolic blood pressure increased by at least 1 mmHg during each of three or more blood pressure waves, and pulse interval showed a concomitant lengthening of at least 4 ms/beat and 2) systolic blood pressure fell by at least 1 mmHg during each of three or more blood pressure waves, and pulse interval showed a concomitant shortening of at least 4 ms/beat. An example of one sequence as it was identified by the computer is showed in Fig. 1. Finally, the computer analyzed the sequences as linear regressions between the systolic blood pressure values and the subsequent pulse intervals. This phase shift, equal to one, was selected according to the findings of previous studies (24, 28). Because the coefficient of determination (3) of the regression was always sufficiently high (>0.85), the regression coefficient was taken as the 230 FIG. 1. Example of the intra-arterial blood pressure signal as reconstructed by the computer after sampling the original signal at 600 Hz. The signal refers to a sequence during which systolic blood pressure and pulse interval increased progressively for several beats. Absolute pulse interval values are reported at bottom. Vertical axis is in mmHg. i I I 1 I I i / I I I I I I I I 1 1 (576 15941612 162516841 740 1 I i I 1 792. ) 1. Number of sequencescharacterized by progressive increases in systolic blood pressure (SBP) and pulse interval (PI) or by progressive reductions in SBP and PI over three consecutive beats ~-_ -____TABLE +PI/+SBP Cats 1 2 3 4 5 6 7 8 9 10 Means MAP, k SE mmHg 101.1 103.5 127.5 122.3 134.6 128.0 94.3 101.8 115.5 110.3 113.9t4.3 PI, ms 310 319 392 298 386 441 447 238 440 340 361.0t22.5 Total 474 476 1,091 1,445 955 1,179 197 292 153 1,729 799H76 -PI/-SBP No./lO,OOO beats Total No./lO,OOO beats 195 243 494 508 237 520 115 112 77 487 299t58 1,223 608 1,537 1,243 1,013 942 365 254 161 1,619 896k166 502 311 696 437 252 415 212 97 81 456 346261 Data are shown as total number of sequences that occurred during intra-arterial blood pressure recording performed in each intact cat and as number of sequences every 10,000 beats. Sequences reported are only those in which beat-to-beat changes in SBP and PI were ~1 mmHg and 24 ms, respectively, and coefficient of determination of calculated linear regression was >0.85 (see METHODS). Average mean arterial pressure (MAP) and PI of recording period are also shown. BEAT-TO-BEAT EVALUATION OF THE H379 BAROREFLEX measure of the gain or sensitivity of the changes in heart rate induced by the blood pressure changes, as it is done for the baroreceptor-heart rate reflex studied by the vasoactive drug method. A description of this method of data analysis has been made in a preliminary report (3). The regression coefficients derived from each recording were summed to obtain averages t SE for the group as a whole. Statistical comparisons were made by oneway analysis of variance. The level of statistical significance was set at P < 0.05. TABLE 2. Number of sequencescharacterized by progressive increases in systolic blood pressure (SBP) and pulse interval (PI), or by progressive reductions in SBP and PI, over 4, 5, or 6 consecutive beats RESULTS -PI/-SBP, +PI/+SBP, Sequence No./lO,OOO beats 62t22 1lt7 3tl 4 beats 5 beats 6 beats beats No./lO,OOO 68k21 14t9 5t3 Data are shown as averages t SE of mean of Table 1. For other explanations see Table data obtained 1. in each cat Mean Sequences: 3 BEATS r ** 4 f SE BEATS Intact cats. As shown in Table 1 in each cat there were many sequences of three beats characterized by progressive increases in pulse interval and systolic blood pressure (+PI/+SBP) or progressive reductions in pulse interval and systolic blood pressure (-PI/-SBP). On average, the number of three-beat +PI/+SBP sequences was similar to that of the three-beat -PI/-SBP sequences (299 t 58 vs. 346 t 61/10,000 beats). A similar number of +PI/+SBP and -PI/-SBP sequences was also found when sequences lasting four or (n=lO) 5 BEATS 6 BEATS 1 1 T r**i . ,..... ... ... . .. ... . ... .. ... . ... . . .. ..a.. ... . A m +Pl/+SBP m -PI/-SBP * pao.05 **p*O.Ol T ....... ...... ....... ...... ....... ...... -IlkT FIG. 2. Top panels show regression coefficients of sequences characterized by a progressive increase in sysconc blood pressure and pulse interval (+PI/+SBP) and by a progressive reduction in systolic blood pressure and pulse interval (-PI/-SBP). Sequences of 3-, 4-, 5, and 6-beat length are separately shown. Data are expressed as averages &SE of mean regression coefficients obtained in each cat. Averages t SE of standard deviations around the mean separately calculated in each cat, i.e., variability of the baroreflex sensitivity in each animal, are shown in lower panels. *p ** Statistical significance of difference between +PI/+SBP and -PI/-SBP sequences. H380 BEAT-TO-BEAT EVALUATION more beats were considered (Table 2). However, these longer sequences occurred progressively more rarely. On average, the four-beat sequences amounted to 130, the five-beat sequences to 24, and the six-beat sequences to 8/10,000 beats. Sequences of seven- and eight-beat duration occurred only occasionally in some cats, and sequences of > eight beats were never identified in any animal. As shown in Fig. 2, top panel, the average regression coefficients of the three-, four-, five-, and six-beat seauences were greater for the +PI/+SBP than for the A 500 A- 5 BEAT sequences 6 BEAT sequences A : Q) 400 5 Y> ii CI c 0 ; 300 a 200 1 B 5oo 200 100 - 1 1 120 1 Syetolic , 140 Blood I 160 Pro88urs , 1 THE BAROREFLEX -PI/-SBP sequences. For both types, the regression coefficients decreased as the length of the sequences increased. However, in each cat each length showed a wide scattering of the regression coefficients around the mean as shown by the high values of the averaged individual standard deviations (Fig. 2, bottom panel). This scattering is further illustrated by the different slopes of the five- and six-beat sequencesobserved in one cat (Fig. 3) . Information on the factors involved in the scattering of the regression coefficients is reported in Table 3 and Fig. 4. There was little or no correlation between the regression coefficients and the systolic blood pressure observed at the beginning of the sequences. On the other hand, there was a correlation between these coefficients and the pulse interval observed at the beginning of the sequences. This correlation was particularly consistent for the -PI/-SBP sequences. Thus the scattering of the regression coefficient is largely unrelated to base-line blood pressure but depends to some extent on base-line heart rate. Sinoaortic-deneruated cats. Compared with the intact cats, sinoaortic-denervated cats had a similar mean arterial pressure (+4.0 & 4.8 mmHg, P = NS) and a slightly reduced pulse interval (-78 t 18 ms, P < 0.01). The number of the +PI/+SBP and -PI/-SBP sequences was strikingly reduced (Fig. 5). For the three-beat sequences, the reduction was 84.4 t 4.7%, whereas for the four- and five-beat sequences it was 93.6 t 2.7 and 78.3 t 9.9%, respectively. After sinoaortic denervation sequences longer than five beats were never observed. The regression coefficients of the few sequences that remained after sinoaortic denervation were also strikingly less than those observed in the intact condition. For the +PI/+SBP sequences the average regression coefficient after sinoaortic denervation was 6.0 t 1.0 ms/ mmHg, whereas for the -PI/-SBP sequencesit was 3.5 + 0.7 ms/mmHg. This represented a reduction of 72 and 56%, respectively, as compared with control. Baroreceptor influences of a single-beat duration. In the intact cats the three-, four-, five-, and six-beat sequences accounted for -26% of all beats. Less than 1% of beats was organized in sequencesof three or more beats characterized by a “nonbaroreflex” pattern, i.e., -PI/+SBP or +PI/-SBP sequences, whereas -25% of beats were not considered by the computer because there was no change in SBP and/or PI compared with the preceeding value. Thus -48% of beats were characterized by SBP and PI changes of one-cycle duration, which prompted us to examine how often this resulted from short-term I’* 0.85 . 1 OF 100 1 1 200 1 (mmHg) 3. Slopes (or regression coefficients) of linear regressions between progressive increases in systolic blood pressure and pulse interval (&beat sequences, A) and between progressive reductions in systolic blood pressure and pulse interval (6-beat sequences, B). Data refer to all 5- or 6-beat sequences identified in cat 1. Individual pulse interval and systolic blood pressure values are shown for some slopes. FIG. TABLE 3. Correlation coefficients between regression coefficients of 4-beat + SBP/+PI sequencesor of 4-beat pressure (+PI/+SBP) or -PI/-SBP sequencesand SBP or PI values existing at the beginning of the sequences Regression Mean Initial Initial SBP, mmHg PI, ms 0.34-1-0.07 0.40t0.06 Coefficients +PI/+SBP Regression Range P c 0.05 0.10-0.62 0.10-0.65 3 6 Mean Coefficients Range 0.36t0.05 0.14-0.59 0.66t0.04 0.40-0.87 in each of 10 cats of Table 1. Range of individual -PI/-SBP P < 0.05 4 10 Data represent the averages * SE of correlation coefficients obtained correlation coefficients and number of cats in which these values achieved statistical significance are also shown. In 8 cats in which 4-beat sequences were numerous, these were calculated by randomly selecting 70 4beat +PI/+SBP and 70 4-beat -PI/-SBP sequences per cat. In remaining 2 cats, they were calculated by taking all available 4-beat sequences. For other explanations see Tables 1 and 2. BEAT-TO-BEAT 4 Beat 14 1 r= 0.17 Sequences NS EVALUATION OF THE p co.001 . l /t’:=*e. 0’ . . . l . . . ;. . t 1, 140 I r = 0.33 , 160 , 1 180 , 11 200 p<0.01 H381 (n=70) 1 rz0.49 . 20 BAROREFLEX d 11, 240 260 1 . l I I I, 280 300 p* r = 0.82 I,, 320 340 , , 360 , 1 380 0.001 FIG. 4. Relationships between regression coefficients of 4-beat +PI/+SBP sequences (top panels) and the 4-beat -PI/-SBP sequences (bottom pands)and systolic blood pressure or pulse interval values observed at the beginning of sequences. Data refer to 70 sequences of either type randomly selected from cat 5. Symbols as in Fig. 2. . 5ik-l Baseline SBP (mmHg) J,,,,,,,,,,,,,,, 280 300 320 340 Baseline 360 380 PI (msec) 400 420 in blood pressure and pulse interval elicited by pharmacological or mechanical tools (10, 16, 21, 24, 26). Compared with these methods this new approach may 1) provide a larger number of observations and 2) allow the baroreflex sensitivity to be evaluated during the interplay of the multiple factors affecting circulation. This may allow us to study the modulation of the baroreflex by behavioral influences such as exercise (4,7,18,20), stress (6, 27), sleep (2, 5, 28), and possibly by circadian factors (l2), thereby affording a better understanding of how this reflex operates in integrated cardiovascular control. The advantage of evaluating the baroreceptor-heart rate reflex by a large number of observations is emphasized by another result of our study, i.e., that the regression coefficients of the spontaneously occurring pulse interval/blood pressure sequences (i.e., the baroreflex DISCUSSION sensitivity) showed a wide range of values in each cat. Our study demonstrates that, in the unanesthetized This was due in part to the fact that sequences of cat, computer analysis of the intra-arterial blood pressure different duration showed different sensitivities. Howtracing permits identification of a large number of se- ever, different sensitivities also characterized sequences quences characterized by linearly related increases or of the same duration. This indicates that the sensitivity reductions in systolic blood pressure and pulse interval. of this reflex function is not a stable feature of a given More than one-fourth of the total number of beats re- individual but is indeed characterized by a pronounced corded in our intact animals was organized in sequences short-term intraindividual variability. Its evaluation may of this type. Because of their disappearance after sinoaortherefore be better afforded by collection of a large tic denervation, these sequences reflect the ability of number of values rather than by one or few measurearterial baroreceptor stimulation or deactivation to re- ments. Beside validating a new method for studying the barflexly modulate the sinus node. This means that they oreceptor-heart rate reflex, our data prompt some concan provide information on the baroreceptor-heart rate siderations as to the way this reflex operates in normal reflex, complementing the methods based on alterations baroreceptor influences on the sinus node. This was investigated by identifying all the events characterized by 1) a one-beat increase in systolic blood pressure of at least 1 mmHg followed by a one-beat increase in pulse interval of at least 4 ms and 2) a one-beat reduction in systolic blood pressure of at least 1 mmHg followed by a one-beat reduction in pulse interval of at least 4 ms. As shown in Fig. 6 in the intact cats the one-beat +PI/ +SBP and -PI/-SBP changes combined amounted to 55% of the one-cycle events. However, these changes also amounted to -50% of the one-cycle events after sinoaortic denervation. This 50% rate was identical to that obtained in the intact animals by randomly coupling to each other all pulse interval and systolic blood pressure changes of a single-cycle duration. H382 BEAT-TO-BEAT hleans f SE EVALUATION h=lO) OF THE BAROREFLEX % 60 BEAT 4 sequences BEAT 1 sequences 0 Intact m Sinoaortic denervation * p<o.o5 ** p 4 0.01 1 z pti E z 2oa C BEAT sequences f-*1 4 6 1 BEAT n.- u Intact H Random Sinoaortic sequences . coupling denervation FIG. 6. Mean (2 SE) number of events characterized by a l-beat increase or reduction in systolic blood pressure of ~1 mmHg followed by a l-beat increase or reduction in pulse interval of ~4 ms, respectively, before (intact) and after sinoaortic denervation. Data are expressed as percent of all single beat changes after exclusion of beats organized in sequences of 3 or more beats. Sequences in which only SEW or PI changed were also excluded (see text). Number of +PI/ +SBP and -PI/-SBP l-beat events resulting from random coupling of all l-beat changes in systolic blood pressure and pulse interval occurring in the intact animals is shown for comparison. Symbols as in Fig. 2. ditions the baroreceptor-heart rate reflex does not approach threshold or saturation and operates in the linear portion of its stimulus-response curve. It is possible that this reflects the intervention of a rapid resetting mechanism (11, 15, 17). Several studies have demonstrated that the barorecep-PI/‘&BP -PI/-SBP +PI/+SBP *PI/&BP tor-heart rate reflex is characterized by a short latency and that the effects of a baroreceptor stimulation can be FIG. 5. +PI/+SBP or -PI/-SBP sequences of 3-, 4-, 5, and 6-beat seen within one beat (8, 14, 23). In our cats there were length before (intact) and after sinoaortic denervation. Data are shown as means & SE of 10 cats. Symbols as in Fig. 2. many events characterized by a one-beat increase in systolic blood pressure followed by a one-beat lengthenconditions. First, the +PI/+SBP sequences showed a ing in pulse interval, or by a one-beat reduction in baroreflex sensitivity greater than the -PI/-SBP se- systolic blood pressure followed by a one-beat shortening quences. This agrees with the results obtained by the in pulse interval. However, these events were only vasoactive drug method (21, 24) and indicates that, in slightly less after sinoaortic denervation, and their number was only slightly different from that obtained by physiological conditions, the sinus node is more effectively modulated by an increase than by a reduction in randomly coupling all blood-pressure and pulse-interval changes. Thus an overall analysis of the single-beat the ongoing activity of the arterial baroreceptors. changes may be unable to discriminate between baroreSecond, the baroreflex sensitivity showed a positive correlation with the pulse interval at which the pulse flex and nonbaroreflex or casual phenomena. It should be emphasized that the evaluation of the interval began, especially when the sequence was of the baroreflex by analysis of spontaneously occurring PI/ -PI/-SBP type. This confirms on a physiological setting that the effectiveness of the baroreceptor-heart rate re- SBP sequencesalso has limitations. First of all, although flex depends to some extent on the base-line heart rate providing a large number of observations, this method applies to only one-fourth of all beats, which means that value (9). This is particularly the case for the baroreceptor-induced acceleration of the sinus node, which is for a prominent fraction of the recording time the baroreflex function still goes undetected. Furthermore, as the clearly enhanced in presence of a base-line bradycardia traditional methods (10, 16, 21, 24, 26), this method and opposed in presence of a base-line tachycardia. Whether these different base-line values are the cause addresses the baroreceptor influence on the heart and not that on the main baroreceptor target, i.e., blood or the effect of the associated differences in baroreflex pressure (1, 19, 21). In addition, most sequences consist sensitivity remains an unsolved issue (9). Third, the baroreflex sensitivity showed little or no of a small number of beats, which may limit the accuracy relationship with the blood pressure values at which the of the calculated baroreflex sensitivity. On the other hand, it is interesting that in physiological conditions sequence began, the reflex being similarly effective only these relatively short-lived sequences occur; this throughout the range of blood pressures occurring during the recording. This indicates that in physiological con- suggests that the longer sequencesproduced by the vas- BEAT-TO-BEAT EVALUATION oactive drug method (10, 21, 24, 26) do not reflect the pattern of the baroreflex engagement brought about by spontaneous blood pressure fluctuations. In conclusion, our study validates a new approach to the study of the baroreceptor-heart rate reflex which can usefully complement other methods currently in use. By providing a larger amount of information in physiological conditions and by avoiding the intervention of artificially evoked blood pressure changes, this method may be particularly suitable to examine this reflex function during behavior. We thank Paola Boccaccini for typing the manuscript and Riccardo Sarri for technical assistance. This study was supported in part by grants from the Consiglio Nazionale delle Ricerche, Finalized Projects of Degenerative Medicine and from Biomedical Technology. Received 23 March 1987; accepted in final form 29 September 1987. REFERENCES 1. ABBOUD, F. The sympathetic system in hypertension. Hypertension Dallas 4, Suppl. II: 208225, 1982. 2. BACCELLI, G., R. ALBERTINI, G. MANCIA, AND A. ZANCHETTI. Interactions between sino-aortic reflexes and cardiovascular effects of sleep and emotional behaviour in the cat. Circ. Res. 38, Suppl. II: 30-34, 1976. 3. BERTINIERI, G., M. DI RIENZO, A. CAVALLAZZI, A. U. FERRARI, A. PEDOTTI, AND G. MANCIA. A new approach to analysis of the arterial baroreflex. J. Hypertens. 3, Suppl. 3: S79-S81, 1985. 4. BRISTOW, J. D., E. B. BROWN, D. S. C. CUNNINGHAM, H. G. HOWSON, E. STRANGE-PETERSEN, T. G. PICKERING, AND P. SLEIGHT. Effect of bicycling on the baroreflex regulation of pulse interval. Circ. Res. 28: 582-592, 1971. 5. CONWAY, J., N. BONN, J. VANN SONES, AND P. SLEIGHT. Involvement of the baroreflexes in the changes in blood pressure with sleep and mental arousal. Hypertension Dallas 5: 746-748, 1983. 6. DEL Bo, A., G. BACCELLI, G. CELLINA, F. FEA, A. FERRARI, AND A. ZANCHETTI. Carotid sinus reflexes during postural changes, naturally elicited fighting behaviour and phases of sleep in the cat. Cardiovasc. Res. 12: 767-769, 1985. 7. DJOJOSUGITO, A. H., B. FOLKOW, P. H. KYLSTRA, B. LISANDER, AND R. S. TUTTLE. Differentiated interaction between the hypothalamic defence reaction and baroreceptor reflexes. I. Effects on heart rate and regional flow resistance. Acta Physiol. Stand. 78: 376-385, 1970. 8. ECKBERG, D. L. Temporal response patterns of the human sinus node to brief carotid baroreceptor stimuli. J. Physiol. Lond. 258: 769-782,1976. 9. ECKBERG, D. L. Baroreflex inhibition of the human sinus node: importance of stimulus intensity, duration and rate of pressure change. J. Physiol. Lond. 269: 561-577, 1977. 10. GRIBBIN, B., T. G. PICKERING, P. SLEIGHT, AND R. PETO. Effect of age and high blood pressure on baroreflex sensitivity in man. Circ. Res. 79: 424-431, 1971. 11. HEESCH, C. M., M. D. THAMES, AND F. M. ABBOUD. Acute OF THE BAROREFLEX H383 resetting of carotid sinus baroreceptors. Dissociation between discharge and wall strain. Am. J. Physiol. 247 (Heart Circ. Physiol. 16): H824-H832, 1984. 12. HOSSMANN, U., C. T. FITZGERALD, AND C. T. DOLLERY. Circadian rhythm of baroreflex reactivity and adrenergic vascular response. Cardiovasc. Res. 14: 125-129, 1980. fibers from the 13. ITO, C. S., AND D. H. SCHER. Arterial baroreceptor aortic region of the dog in the cervical vagus nerve. Circ. Res. 32: 442-446, 1973. 14- KATONA, P. G., S. W. POITRAS, G. 0. BARNETT, AND B. S. TERRY. --- Cardiac vagal efferent activity and heart rate period in the carotid sinus reflex. Am. J. Physiol. 218: 1030-1037, 1970. 15. KORNER, P. I. Integrative neural cardiovascular control. Physiol. Rev. 51: 312-367,197l. 16. KORNER, P. I., J. SHAW, M. J. WEST, AND J. R. OLIVER. Central nervous system control of baroreceptor reflexes in the rabbit. Circ. Res. 31: 637-652, 1972. 17 KRIEGER, E. M., M. C. SALGADO, AND L. C. MICHELINI. Resetting . of the baroreceptors. In: Cardiovascular Physiology IV, edited by A. C. Guyton and J. E. Hall. Baltimore, MD: University Park, 1982, vol. 26, p. 119-146. (Int. Rev. Physiol. Ser.) 18. LUDBROOK, J., I. B. FARIS, J. IANNOS, G. G. JAMIESON, AND W. S. RUSSEL. Lack of effect of isometric handgrip exercise in the responses of the carotid sinus baroreceptor reflex in man. Clin. Sci. Mol. Med. 55: 189-194, 1978. 19. LUDBROOK, J., G. MANCIA, AND A. ZANCHETTI. Does the baroreceptor heart rate reflex indicate the capacity of the arterial baroreceptors to control blood pressure? Clin. Exp. Pharmacol. Physiol. 7: 499-503,198O. 20. MANCIA, G., J. IANNOS, G. G. JAMIESON, H. H. LAWRENCE, P. R. SHARMAN, AND J. LUDBROOK. The effect of isometric handgrip exercise on the carotid sinus baroreceptor reflex in man. Clin. Sci. Mol. Med. 54: 33-37, 1978. 21. MANCIA, G., AND A. L. MARK. Arterial baroreflexes in humans. In: Handbook of Physiology. The Cardiovascular System. Peripheral Circulation and Organ Blood Flow. Bethesda, MD: Am. Physiol. Sot., 1983, sect. 2, vol. III, part 2, chapt. 20, p. 755-794. 22. MANCIA, G., AND A. ZANCHETTI. Blood pressure variability. In: Handbook of Hypertension. Pathophysiology of Hypertension: Cardiovascular Aspects, edited by A. Zanchetti and R. C. Tarazi. Amsterdam: Elsevier, 1986, vol. 7, p. 125-152. 23. PICKERING, T. G., AND S. DAVIS. Estimation of the conduction time of the baroreceptor-cardiac reflex in man. Cardiovasc Res. 7: 713-719, 1973. 24. PICKERING, T. G., B. GRIBBIN, AND P. SLEIGHT. Comparison of the reflex heart rate response to rising and falling arterial pressure in man. Cardiovasc. Res. 6: 777-783, 1972. 25. RAMIREZ, A., G. BERTINIERI, L. BELLI, A. CAVALLAZZI, M. DI RIENZO, A. PEDOTTI, AND G. MANCIA. Reflex control of blood pressure and heart rate by arterial baroreceptors and by cardiopulmonary receptors in the unanesthetized cat. J. Hypertens. 3: 327335,1985. 26. SLEIGHT, P. Reflex control of the heart. Am. J. Cardiol. 44: 889894,1979. 27. SLEIGHT, P., P. Fox, R. LOPEZ, AND D. E. BROOKS. The effect of mental arithmetic on blood pressure variability and baroreflex sensitivity in man. Clin. Sci. Mol. Med. 55: 381s-382s, 1978. 28. SMITH, H. S., P. SLEIGHT, AND G. W. PICKERING. Reflex regulation of arterial pressure during sleep in man: a quantitative method of assessing baroreflex sensitivity. Circ. Res. 74: 109-121, 1969.
© Copyright 2026 Paperzz