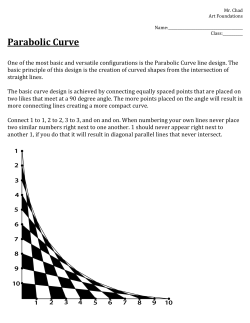
6/11/2013 ExamВ FindingsВ TheВ BloodyВ Masquerader Polypoidal Choroidal Vasculopathy JennyВ Z.В Xu,В O.D. VAВ PaloВ AltoВ HealthВ CareВ System PosteriorВ Segment • VA – ODВ 20/200+В PHNI – OSВ 20/20 • Pupils – ERRL,В noВ APD • Confrontations – EOM:В fullВ OU – VF:В FullВ toВ fingerВ countingВ OS,В completeВ restrictionВ ODВ temp,В infraВ tempВ andВ superiorВ temp • AnteriorВ Segment:В unremarkableВ OU,В noВ rubeosis OU • TONOMETRY:В В 10/12В mmHgВ @В 1417В Polypoidal Choroidal Vasculopathy • Choroidal abnormalityВ characterizedВ byВ branchingВ choroidal vascularВ networkВ andВ vascularВ dilationsВ ofВ terminalВ choroidal vesselsВ inВ shapeВ ofВ polyps • AlsoВ classifiedВ asВ aВ subtypeВ ofВ В occultВ choroidal neovascularization • InitiallyВ describedВ inВ 1982В byВ Yannuzzi “IdiopathicВ polypoidal choroidal vasculopathy”,В alsoВ termed “posteriorВ uveal bleedingВ syndrome” UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 1 6/11/2013 PCVВ Epidemiology • AfricanВ AmericanВ females • MoreВ oftenВ inВ pigmentedВ individualsВ suchВ asВ AfricansВ andВ Asians,В butВ alsoВ foundВ inВ Caucasians • AgeВ ofВ diagnosisВ fromВ 20sВ toВ 80s,В mostВ commonВ betweenВ theВ ageВ ofВ 60В andВ 70В years • 71%В ofВ PCVВ inВ JapaneseВ populationВ maleВ andВ 75%В ofВ PCVВ inВ EuropeanВ populationВ female • PredilectionВ forВ macularВ andВ peripapillary locations • BilateralВ inВ 14%В JapaneseВ populationВ andВ 32%В ofВ EuropeansВ diagnosedВ withВ PCV Diagnosis ClinicalВ Presentation • SmallВ toВ largeВ branchingВ ofВ innerВ choroidal vesselsВ withВ multipleВ polypoidal structures • VariableВ sizedВ serosanguineous detachmentВ ofВ theВ RPEВ andВ neurosensoryВ retina • Subretinal hemorrhages,В lipidВ exudation • Subretinal fibrosisВ mayВ resultВ afterВ resolutionВ ofВ serosanguineous complications • PigmentВ epithelialВ hyperplasiaВ andВ degeneration ICGAВ andВ FAВ ofВ PCV Gomi etВ al.,В ArchВ Clin Exp Ophthalmol,В 2007 EarlyВ phase • ICGAВ isВ theВ goldВ standardВ forВ theВ diagnosisВ ofВ PCV • FAВ notВ helpfulВ dueВ toВ obscurationВ ofВ theВ choroidВ byВ theВ RPE • ICGВ allowsВ forВ higherВ transmittanceВ ofВ lightВ toВ choroidВ andВ betterВ resolutionВ ofВ theВ vasculature • PCVВ definitionВ byВ ICGA:В singleВ orВ multipleВ focalВ areasВ ofВ hyperfluorescence arisingВ fromВ theВ choroidВ withinВ theВ firstВ 6В minutesВ afterВ injectionВ withВ orВ withoutВ associatedВ vascularВ network. – PresenceВ ofВ orange‐redВ subretinal nodulesВ withВ correspondingВ indocyanine greenВ hyperfluoresence isВ pathognomonicВ ofВ PCV UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 MidВ phase ICGA MidВ toВ lateВ phase LateВ phase FAВ 2 6/11/2013 OCTВ PathophysiologyВ KeaneВ PAВ etВ al.В Surv Ophthal,В 2012 DoubleВ layerВ sign:В hyper‐reflective layerВ beneathВ theВ RPE,В inner boundaryВ ofВ Bruch’sВ membrane choriocapillaris complex Pathophysiology – Histology • IncreasedВ hyalinizationВ ofВ choroidal vesselsВ andВ massiveВ exudationВ ofВ fibrinВ andВ bloodВ plasma;В degenerationВ ofВ smallВ vesselsВ withВ thickenedВ basementВ membrane • HyalinizationВ =В extensiveВ replacementВ ofВ smoothВ muscleВ componentВ byВ amorphousВ pseudocollagenous tissueВ ofВ poorlyВ definedВ nature, orВ arteriosclerotic changesВ thatВ areВ found inВ theВ otherВ partsВ ofВ the body • DilatedВ venules andВ arterioles UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 • MechanismВ notВ wellВ understood – agreementВ concerningВ theВ originationВ ofВ theВ polypsВ fromВ theВ innerВ choroid • ConsideredВ toВ beВ aВ subtypeВ ofВ exudativeВ AMDВ (typeВ 1,В sub‐ RPE),В orВ asВ aВ separateВ entityВ dueВ toВ choroidal abnormalities • AMDВ andВ PCVВ shareВ similarВ andВ differingВ geneticВ factorsВ involvingВ theВ complementВ system • AccordingВ toВ Yannuzzi,В PCVВ andВ AMDВ canВ beВ distinguishedВ basedВ onВ age,В peripapillary locationsВ ofВ CNV,В presenceВ ofВ softВ drusen andВ ethnicity • SimilarityВ ofВ PCVВ toВ CSC Pathophysiology – RelationshipВ toВ ARMD • MassiveВ exudationВ ofВ fibrinВ andВ bloodВ plasmaВ raisesВ choroidal tissueВ pressureВ toВ produceВ protrusionВ ofВ choroidal tissuesВ throughВ weakenedВ RPEВ andВ Bruch’s • Choroidal neovascularizationВ alsoВ foundВ aboveВ theВ RPEВ inВ 2В outВ ofВ 5В pathologicalВ specimensВ examined • NeovascularizationВ mayВ ariseВ fromВ RPEВ andВ Bruch’sВ membraneВ breaks • OverexpressionВ ofВ HTRA1В geneВ (responsibleВ forВ extracellularВ matrixВ degradation)В isВ associatedВ withВ bothВ macularВ degenerationВ andВ PCV – OverexpressionВ decreasesВ integrityВ ofВ theВ Bruch’sВ membrane 3 6/11/2013 Pathophysiology – RelationshipВ toВ CSC PCVВ theВ Masquerader • Choroidal vascularВ hyperpermeability:В multifocalВ hyperfluorescence inВ midВ andВ lateВ phasesВ ofВ ICGA • Hyperpermeability inВ patientsВ withВ PCVВ stronglyВ associatedВ withВ aВ historyВ ofВ CSC • EyesВ withВ PCVВ andВ CSCВ hadВ thickerВ choroidВ comparedВ differentВ typesВ ofВ ARMD • IncreasedВ thicknessВ dueВ toВ increasedВ choriopapillary permeabilityВ possiblyВ fromВ increasedВ hydrostaticВ pressure,В leadingВ alsoВ toВ RPEВ leaksВ andВ serousВ retinalВ detachments • CSCВ andВ PCVВ bothВ relatedВ toВ choroidВ congestionВ andВ leakage ratherВ thanВ simplyВ diseasesВ ofВ theВ Bruch’sВ membrane • LargeВ subretinal hemorrhageВ andВ RPEВ atrophyВ mayВ causeВ PCVВ toВ lookВ likeВ wetВ AMD • InВ patientsВ diagnosedВ withВ AMD,В 4.8%В toВ 23%В foundВ toВ haveВ PCVВ instead,В moreВ commonlyВ diagnosedВ inВ JapaneseВ individuals • Yannuzzi alsoВ reportsВ PCVВ masqueradingВ asВ CSCВ dueВ toВ presenceВ ofВ serousВ pigmentВ epithelialВ detachmentsВ andВ neurosensoryВ retinalВ detachment – Re‐diagnosedВ withВ PCVВ basedВ onВ ICGAВ findingsВ thatВ distinguishedВ theВ PEDsВ fromВ choroidal polyps NaturalВ History • HighlyВ variable • RemittingВ andВ relapsingВ courseВ ofВ chronic,В multipleВ recurrentВ serosanguineous detachments • ApproximatelyВ 50%В ofВ patientsВ withВ posteriorВ poleВ lesionsВ haveВ favorableВ visualВ outcomeВ withoutВ treatment • PersistentВ bleedingВ involvingВ theВ maculaВ resultingВ inВ visionВ lossВ inВ others • MacularВ involvementВ rangesВ fromВ 25В toВ 94%В ofВ patients • VisualВ prognosisВ dependsВ onВ theВ locationВ ofВ andВ sizeВ ofВ lesions UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Treatment:В CombinationВ Therapy • EVERESTВ study:В multi‐centered,В doubleВ masked,В ICGAВ guided,В randomizedВ controlledВ trialВ involvingВ 61В patientsВ evaluatingВ bestВ treatmentВ modality • PercentВ ofВ polypВ regression – Visudyne alone:В 71.4%,В VAВ improvedВ byВ 7.5В letters – 3В xВ 0.5В mgВ monthlyВ Lucentis alone:В 28.6%,В VAВ improvedВ byВ 9.2В letters – Visudyne +В Lucentis:В 77.8%,В VAВ improvedВ byВ 10.9В letters,В lowestВ rateВ ofВ PDT – relatedВ hemorrhages • RecommendВ eitherВ combinationВ therapyВ orВ ICGAВ guidedВ PDT • Anti‐VEGF:В effectiveВ forВ reabsorptionВ ofВ subretinal fluid;В monotherapy recommendedВ ifВ PDTВ contraindicatedВ 4 6/11/2013 ManagementВ AlgorithmВ References • • • • • • • • • • • • • • • • • • Koh etВ al,В 2013 • • • Yannuzzi LA.В Idiopathic polypoidal choroidal vasculopathy.В MaculaВ SocietyВ Meeting,В 1982,В Miami,В FL. Yannuzzi LA,В FreundВ KB,В Goldbaum MВ etВ al.В Polypoidal choroidal vasculopathy masqueradingВ asВ centralВ serousВ chorioretinopathy.В Ophthalmology 2000;107(4):767‐77. Lafaut BA,В LeysВ AM,В Snyers B,В etВ al.В Polypoidal choroidal vasculopathy inВ Caucasians.В Graefes ArchВ Clin Exp Ophthalmol 2000;238:752–759. Koh A,В LeeВ WK,В ChenВ LJ,В etВ al.В EVERESTВ study:В efficacyВ andВ safetyВ ofВ verteporfin PDTВ inВ combinationВ withВ ranibizumab orВ aloneВ versusВ ranibizumab monotherapy inВ patientsВ withВ symptomaticВ macularВ polypoidal choroidal vasculopathy.В RetinaВ 2012;32:1453–1464. Ahuja RM,В Stanga PE,В Vingerling JR,В etВ al.В Polypoidal choroidal vasculopathy inВ exudativeВ andВ haemorrhagic pigmentВ epithelialВ detachments.В BrВ JВ Ophthalmol 2000;84:479–484. Gomi F,В Sawa M,В Mitarai K,В etВ al.В AngiographicВ lesionВ ofВ polypoidal choroidal vasculopathy onВ indocyanine greenВ andВ fluoresceinВ angiography.В Graefes ArchВ Clin Exp Ophthalmol 2007;245:1421–1427. Koh A,В ChenВ LJ,В ChenВ SJ,В etВ al.В Polypoidal choroidal vasculopathy:В evidence‐basedВ guidelinesВ forВ clinicalВ diagnosisВ andВ Treatment.В Retina,В JВ RetinalВ andВ VitreousВ DiseasesВ 2013;33(4):686‐716 ImamuraВ Y,В Engelgert M,В IidaВ TВ etВ al.В Polypoidal choroidal vasculopathy:В AВ Review.В Surv Ophthalmol 2010;В 55(6):501‐515 KoizumiВ H,В Yamagashi T,В Yamazai TВ etВ al.В RelationshipВ betweenВ clinicalВ characteristicsВ ofВ polypoidal choroidal vasculopathy andВ choroidal vascularВ hyperpermeability.В AmВ JВ Ophthalmol 2012:1‐9 HayashiВ K,В HasegawaВ YВ andВ Tokoro T.В Indocyanine greenВ angiograophy ofВ centralВ serousВ chorioretinopathy.В Int Ophthalmol 1986;В 9(1):37‐41 Hochman MA,В Seery CMВ andВ Zarbin MA.В PathophysiologyВ andВ managementВ ofВ subretinal hemorrhage.В Surv Ophthalmol 1997;В 42(3):195‐213 Birkholz ES,В JohnsonВ ATВ andВ RussellВ SR.В RetinalВ ArteryВ Macroaneurysm.В EyeRounds.org.В PostedВ JulyВ 7,В 2010;В AvailableВ from:В www.EyeRounds.org/cases/113‐RAMA.htm KimВ SW,В OhВ J,В KwonВ SSВ etВ al.В Comparision ofВ choroidal thicknessВ amongВ patientsВ withВ healthyВ eyes,В earlyВ age‐relatedВ maculopathy,В neovasculra age‐ relatedВ macularВ degeneration,В centralВ serousВ chorioretinopathy,В andВ polypoidal choroidal vasculopathy.В RetinaВ JВ RetinaВ andВ VitreousВ DiseaseВ 2011;В 31(9):В 1904‐1911 SatoВ T,В Kishi S,В WatanabeВ GВ etВ al.В TomographicВ featuresВ ofВ branchingВ vascularВ networksВ inВ polypoidal choroidal vasculopathy.В Retina,В JВ ofВ RetinaВ andВ VitreousВ DiseasesВ 2007;В 27(5)589‐594 MikiВ A,В HondaВ S,В KojimaВ HВ etВ al.В VisualВ outcomeВ ofВ photodynamicВ theraphy forВ typicalВ neovascular age‐relatedВ macularВ degenerationВ andВ polypoidal choroidal vasculopathy overВ 5В yearsВ ofВ followВ up.В Jpn JВ Ophthalmol 2013;В 57:301‐307 GiovanniniВ A,В AmatoВ GP.В DвЂ�AltobrandoВ E,В GiulianiВ M.В OpticalВ coherenceВ tomographyВ (OCT)В inВ idiopathic polypoidal choroidal vasculopathy (IPCV).В DocВ Ophthalmol.1999;97(3‐‐4):367—71 SilvaВ R.В Neovascular Phenotypes:В polypoidal choroidal vasculopathy.В AMDBook.В LastВ revisionВ OctВ 2011;В availableВ from:В http://amdbook.org/content/neovascular‐phenotypes‐polypoidal‐choroidal‐vasculopathy KeaneВ PA,В PatelВ PJ,В Liakopoulos SВ etВ al.В EvaluationВ ofВ Ag‐relatedВ macularВ degenerationВ withВ OpticalВ CoherenceВ Tomography.В Surv Ophthalmol 2012;В 57(5)389‐414 KoizumiВ H,В Yamagishi T,,В YamazakiВ TВ etВ al.В Subfoveal choroidal thicknessВ inВ typicalВ age‐relatedВ macularВ degenerationВ andВ polypoidal choroidal vasculopathy.В Graefes ArchВ Clin Exp Ophthalmol 2011,В 249:1123‐1128 SatoВ T,В Kishi S,В WatanabeВ GВ etВ al.В Tomograhic featuresВ ofВ branchingВ vascularВ networksВ inВ polypoidal choroidal vasculopathy.В RetinaВ 2007,В 27:587‐594 Glaucoma ProgressiveВ OpticВ Neuropathy NormalВ TensionВ Glaucoma TheВ ProblemВ withВ LowВ Pressure KristinВ Symon,В OD UCВ BerkeleyВ SchoolВ ofВ Optometry OcularВ DiseaseВ Resident JuneВ 23,В 2013 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 • DegenerationВ ofВ retinalВ ganglionВ cellsВ andВ axons • LossВ ofВ rimВ tissue • GlaucomatousВ cupping • CorrespondingВ visualВ fieldВ defectsВ thatВ followВ RNFLВ loss 5 6/11/2013 2nd LeadingВ CauseВ ofВ VisionВ LossВ Worldwide • OverВ 40В millionВ peopleВ worldwideВ (12.3%) • OpenВ angleВ glaucomaВ affectsВ moreВ thanВ 2В millionВ individualsВ inВ theВ US • ByВ 2020В thereВ willВ beВ atВ leastВ 3В millionВ affected • 50%В ofВ individualsВ goВ undiagnosed NormalВ tensionВ glaucoma • OpenВ angleВ glaucomaВ withВ untreatedВ IOPВ withinВ theВ normalВ rangeВ (22В mmHg) • 20‐39%В ofВ patientsВ withВ OAGВ inВ theВ USВ andВ Europe • UpВ toВ 30%В ofВ patientsВ areВ underВ ageВ 50 • TheВ CollaborativeВ NormalВ TensionВ GlaucomaВ StudyВ (CNTGS)В showedВ thatВ aВ 30%В decreaseВ inВ IOPВ resultedВ inВ preservationВ ofВ visualВ function (Quigley,В 2004) (MacDonald,В 2012) ExaminationВ Findings PatientВ DY 26В yo KoreanВ Female Examination Findings OD OS BCVA Refraction 20/20‐ ‐5.75 ‐0.50В x 015 20/20‐ ‐4.25 ‐1.50В x 155 Anterior Segment Unremarkable Unremarkable IOPВ (@16:36) 18В mmHg 19В mmHg Gonioscopy Cilliary bodyВ 360 Cilliary bodyВ 360 Pachymetry 580В microns 573В microns PresentedВ toВ clinicВ onВ 9/24/2010 CC:В decreasedВ peripheralВ vision PreviousВ diagnosisВ ofВ Glaucoma ‐ diagnosedВ inВ KoreaВ 8/2010 CurrentВ treatment:В Betoptic 1В gtt OUВ BID Pre‐treatmentВ IOP:В ODВ 19В mmHg,В OSВ 20В mmHg UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 6 6/11/2013 OpticВ NerveВ andВ RetinalВ NerveВ FiberВ LayerВ Analysis вњ• HereditaryВ opticВ neuropathy NormalВ В MRI RuledВ outВ byВ history вњ• вњ•glaucomatousВ Non‐ MassВ lesionВ ofВ orbitВ orВ cranium Trauma cuppingВ andВ visualВ fieldВ defects вњ• HeavyВ metal вњ• HumphreyВ VisualВ FieldВ 30‐2В Threshold NormalВ TensionВ Glaucoma • VisualВ fieldВ defectsВ respectingВ horizontal • NasalВ stepВ andВ arcuate defects • SplinterВ hemorrhageВ atВ opticВ disc IntracranialВ Mass вњ• Infection Auto‐ immune • Neuroretinal rimВ pallorВ exceedsВ cupping • VerticalВ alligned visualВ fieldВ defects • YoungerВ age • ReducedВ visualВ acuity LabВ WorkupВ Normal (GreenfieldВ etВ al,В 1998) UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 7 6/11/2013 DiscВ Hemorrhage • SomeВ studiesВ reportВ increasedВ frequencyВ ofВ discВ hemorrhagesВ inВ normalВ tensionВ glaucoma • ControversialВ supportВ ofВ aВ vascularВ etiologyВ forВ NTG • JonasВ suggestsВ thatВ discВ hemorrhagesВ areВ foundВ inВ mostВ patientsВ withВ glaucoma,В however,В theyВ areВ moreВ apparentВ inВ NTGВ dueВ inВ partВ toВ differentВ pressureВ mechanicsВ atВ theВ opticВ nerveВ head • TheВ CNTGSВ reportedВ thatВ aВ historyВ ofВ migraineВ HAВ andВ presenceВ ofВ DiscВ hemorrhageВ wereВ bothВ relatedВ withВ progressionВ ofВ glaucoma Treatment • PatientВ DYВ wasВ startedВ onВ Xalatan 1В gtt OUВ QHS • Latanoprost (genericВ forВ Xalatan)В isВ moreВ effectiveВ atВ reducingВ IOPВ duringВ sleepingВ hoursВ thanВ Timolol (LiuВ etВ al,В 2003) ProgressionВ ofВ NormalВ TensionВ Glaucoma CNTGS 20% 80% 20%В ofВ patientsВ withВ NormalВ TensionВ GlaucomaВ showedВ progressionВ despiteВ aВ 30%В reductionВ inВ IOP • Progression – VisualВ fieldВ defect – Neuroretinal rimВ thinning – NerveВ fiberВ layerВ defects • AdjunctiveВ topicalВ therapyВ added:В OcularВ Perfusion LowВ ocularВ vascularВ perfusionВ isВ aВ riskВ factorВ forВ glaucoma • NoВ toolВ toВ directlyВ measureВ bloodВ flowВ atВ theВ opticВ nerveВ head • ExtrapolateВ expectedВ perfusionВ throughВ aВ combinationВ ofВ systemicВ bloodВ pressureВ andВ IOP MeanВ ocularВ perfusionВ pressure: MOPPВ =В 2/3В [DBPВ +В 1/3(SBP – DBP)] – IOPВ DiastolicВ ocularВ perfusionВ pressure: DOPPВ =В DBP – IOP – Alphagan 1gttВ OUВ BID DOPPВ lessВ thanВ 55В mmHgВ =В twiceВ theВ relativeВ riskВ ofВ glaucoma DBPВ =В diastolicВ BP SBPВ =В systolicВ BP UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 (Quaranta etВ al,В 2013) 8 6/11/2013 DiastolicВ OcularВ PerfusionВ PressureВ forВ DY 60 55 50 DOPPВ OD 45 40 DOPPВ OS CutВ offВ 55 • UpwardВ trendВ inВ DOPPВ withВ treatment • HoweverВ DOPPВ remainsВ lessВ thanВ 55В mmHg 35 Neuroprotection TheВ searchВ forВ pressureВ independentВ treatmentВ forВ glaucoma • AimВ toВ preventВ orВ delayВ theВ deathВ ofВ neurons PossibleВ Neuroprotective Agents ‐ antioxidants ‐ alpha‐2‐agonists ‐ N‐methyl‐D‐aspartate (NMDA)В receptorВ antagonists ‐ glutamateВ inhibitors ‐ calciumВ channelВ blockers ‐ polyamineВ antagonists ‐ nitricВ oxideВ synthetase inhibitors ‐ GinkgoВ biloba ‐ melatonin ‐ vitaminВ B‐12 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 CerebrospinalВ FluidВ Pressure ExaminingВ theВ darkВ side • Trans‐laminarВ pressureВ differentialВ isВ determinedВ byВ theВ IOPВ andВ theВ orbitalВ CSF‐pressure • Trans‐laminarВ pressureВ isВ likelyВ moreВ importantВ inВ glaucomaВ developmentВ thanВ theВ transcorneal pressureВ measuredВ byВ applanation • LowВ CSF‐pressureВ increasesВ theВ riskВ forВ glaucoma (normalВ CSF‐PВ isВ 5В toВ 15В mmHg) References AGISВ Investigators.В TheВ advancedВ glaucomaВ interventionВ studyВ (AGIS):В 7.В TheВ relationshipВ betweenВ controlВ ofВ intraocularВ pressureВ andВ visualВ fieldВ deterioration.В AmВ JВ Ophthalmology 139,В no.В 4В (2000):В 429‐440. Bengtsson B,В Leske MC,В YangВ Z,В Heijl A,В EMGTВ Group.В DiscВ hemorrhagesВ andВ treatmentВ inВ theВ earlyВ manifestВ glaucomaВ trial.В Ophthalmology 115,В no.В 11В (2008):В 2044‐2048. ChangВ EE,В GoldbergВ JL.В GlaucomaВ 2.0:В Neuroprotection,В neuroregeneration,В neuroenhancement.В Ophthalmology 119В (2012):В 979‐986. Choi J,В Jeong J,В ChoВ H,В KookВ MS.В EffectВ ofВ nocturnalВ bloodВ pressureВ reductionВ onВ circadianВ fluctuationВ ofВ meanВ ocularВ perfusionВ pressure:В a riskВ factorВ forВ normalВ tensionВ glaucoma.В InvestigativeВ OphthalmologyВ &В VisualВ Science 47,В no.В 3В (2006):В 831‐836. ColemanВ AL,В Miglior S.В RiskВ factorsВ forВ glaucomaВ onsetВ andВ progression.В В SurveyВ ofВ Ophthalmology 53В (2008):В S3‐S10. CollaborativeВ Normal‐TensionВ GlaucomaВ StudyВ Group.В TheВ effectivenessВ ofВ intraocularВ prssure reductionВ inВ theВ treatmentВ ofВ normal‐tensionВ glaucoma.В В AmВ JВ Ophthalmology 126,В no.В 4В (1998):В 498‐505. Ernest,В PJ,В SchoutenВ JS,В Beckers HJ,В Hendrikse F,В Prins MH,В Webers CA.В В AnВ evidence‐basedВ reviewВ ofВ prognosticВ factorsВ forВ glaucomatousВ visualВ fieldВ progression.В В Ophthalmology 120В (2013):В 512‐519. GreenfieldВ DS,В Siatkowski RM,В GlaserВ JS,В SchatzВ NJ,В ParrishВ RK.В В TheВ cuppedВ disc:В whoВ needsВ neuroimaging?В В Ophthalmology 105,В no.В 10В (1998):В 1866‐1874. JonasВ JB,В WangВ N.В В AssociationВ betweenВ arterialВ bloodВ pressure,В cerebrospinalВ fluidВ pressureВ andВ intraocularВ pressureВ inВ theВ pathophysiology ofВ opticВ nerveВ headВ diseases.В В ClinicalВ &В ExperimentalВ Ophthalmology 40В (2012):В e233‐e234. Krupin T,В Liebman JM,В GreenfieldВ DS,В Ritch R,В GardinerВ S.В В AВ randomizedВ trialВ ofВ brimonidine versusВ timolol inВ preservingВ visualВ function:В resultsВ fromВ theВ Low‐ pressureВ GlaucomaВ TreatmentВ Study.В В AmВ JВ Ophthalmology 151,В no.В 4В (2010):В 671‐681. LiuВ CJ,В Ko YC,В ChengВ CY,В ChiuВ AW,В ChouВ JC,В HsuВ WM,В LiuВ JH.В В ChangesВ inВ intraocularВ pressureВ andВ ocularВ perfusionВ pressureВ afterВ latanoprost 0.005%В orВ brimonidine tartrate 0.2%В inВ normal‐tensionВ glaucomaВ patients.В В Ophthalmology 109В (2012):В 2241‐2247. LiuВ JHK,В MedeirosВ FA,В SlightВ JR,В Weinreb RN.В В ComparingВ diurnalВ andВ nocturnalВ effectsВ ofВ brinzolamide andВ timolol onВ intraocularВ pressureВ inВ patientsВ receivingВ Latanoprost monotherapy.В В Ophthalmology 116В (2009):В 449‐454. LiuВ JHK,В ZhangВ X,В Kripke DF,В Weinreb RN.В Twenty‐four‐hourВ intraocularВ pressureВ patternВ associatedВ withВ earlyВ glaucomatousВ changes.В В В InvestВ Ophthalmol VisВ Sci.В 44В (2003):В 1586‐90. Macdonald,В D.В В UnderВ pressure:В aВ reviewВ ofВ normal‐tensionВ glaucoma.В В CanadianВ JournalВ ofВ Optometry 74,В no.В 4В (2012):В 33‐44. MedeirosВ FA,В Lisboa R,В Weinreb RN,В Liebmann JM,В Girkin C,В ZangwillВ LM.В В RetinalВ ganglionВ cellВ countВ estimats associatedВ withВ earlyВ developmentВ ofВ visualВ fieldВ defectsВ inВ glaucoma.В В Ophthalmology inВ pressВ (2012):В 1‐9. MorganВ WH,В YuВ DY,В Balaratnasingam C.В В TheВ roleВ ofВ cerebrospinalВ fluidВ pressureВ inВ glaucomaВ pathophysiology:В theВ darkВ sideВ ofВ theВ opticВ disc.В В JВ Glaucoma 17,В no.В 5В (2008):В 408‐413. Quaranta L,В Katsanos A,В RussoВ A,В RivaВ I.В В 24‐hourВ intraocularВ pressureВ andВ ocularВ perfusionВ pressureВ inВ glaucoma.В В SurveyВ ofВ Ophthalmology 58,В no.В 1В (2013):В 26‐ 41. QuigleyВ HA,В BromanВ AT.В В TheВ numberВ ofВ peopleВ withВ glaucomaВ worldwideВ inВ 2010В andВ 2020.В В BrВ JВ Ophthalmology 90В (2006):В 262‐267. Ramli N,В Nurull BS,В Hairi NN,В Mimiwati Z.В В LowВ nocturnalВ ocularВ perfusionВ pressureВ asВ aВ riskВ factorВ forВ normalВ tensionВ glaucoma.В В PreventativeВ Medicine inВ pressВ (2012):В 1‐3. Ren R,В JonasВ JB,В Tian G,В ZhenВ Y,В MaВ K,В LiВ S,В WangВ H,В LiВ B,В ZhangВ X,В WangВ N.В В CerebrospinalВ fluidВ pressureВ inВ glaucoma.В В Ophthalmology 117,В no.В 2В (2010):В 259‐266. Shields,В MB.В В Normal‐tensionВ glaucoma:В isВ itВ differentВ fromВ primaryВ open‐angleВ glaucoma?В В CurrentВ OpinionВ inВ Ophthalmology 19В (2008):В 85‐88. Sung,В K.R.,В S.В Lee,В S.B.В Park,В J.В Choi,В S.T.В Kim,В S.C.В Yun,В S.Y.В Kang,В J.W.В Cho,В M.S.В Kook.В В Twenty‐fourВ hourВ ocularВ perfusionВ pressureВ fluctuationВ andВ riskВ ofВ normal‐ tensionВ glaucoma.В В IntegrativeВ OphthalmologyВ &В VisualВ Science 50,В no.В 11В (NovemberВ 2009):В 5266‐5274. 9 6/11/2013 D.G.В CaseВ Report • 61В yearВ oldВ whiteВ male – RelatesВ suddenВ blurredВ visionВ ODВ forВ 1В month NVG StephenВ Chang,В O.D. OptometryВ Resident SierraВ NevadaВ HCS RenoВ VA JuneВ 23rd,В 2013 • GlaucomaВ suspectВ OU,В pseudophake OU • HistoryВ ofВ poorВ complianceВ withВ followВ upВ visits • UncontrolledВ typeВ 2В diabetes,В hypertension,В hyperlipidemia – FamilyВ historyВ ofВ diabetesВ inВ fatherВ &В grandfather D.G.В ClinicalВ Data • HisВ visionВ wasВ CFВ @В 3В ft OD,В 20/25В OS withВ moderateВ myopicВ andВ astigmaticВ Rx • 2+В RAPDВ OD,В withВ inferiorВ VFВ constrictionВ detectedВ onВ confrontationВ fields • IOPsВ wereВ 42/20 • NVIВ superior/temporally OD • ScatteredВ NVAВ inВ theВ superior/temporalВ quadrant. • HypotensiveВ agentsВ (brimonidine,В cosopt)В decreasedВ theВ IOPВ toВ 25В OD withinВ 2В hrs. UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 10 6/11/2013 3В DaysВ Later • Assessment: – NVGВ secondaryВ toВ CRVOВ OD • Plan: – SameВ dayВ OphthalmologyВ consult/IFVA – Pt startedВ onВ maximumВ hypotensiveВ gtts – hypercoaguable state,В CBC,В LipidВ profile, &В CarotidВ U/S orderedВ Neovascular Glaucoma • LateВ presentationВ ofВ seriousВ underlyingВ systemicВ andВ ocularВ pathology • ArisesВ inВ responseВ toВ profoundВ retinalВ ischemia* • PoorВ prognosis,В highlyВ resistantВ toВ treatment • PRPВ performedВ OD • IOPВ 32/16 • DueВ toВ ACВ cells/flare,В pred forteВ addedВ toВ gtt regimen • ScheduledВ forВ nextВ availableВ anti‐VEGFВ injectionВ OD NVGВ Definitions • WillsВ EyeВ Manual – StageВ 1:В NVI/NVA – StageВ 2:В NVI/NVAВ +В increasedВ IOP – StageВ 3:В 1,В 2В +В partial/completeВ angleВ closure • Moraczewski et.В al – IOPВ >В 21В mmHgВ associatedВ withВ NVI/NVA • EhlersВ et.В al – IOP ≥ 4mmHgВ higherВ inВ eyeВ withВ NV – NVI/NVAВ withВ concurrentВ useВ ofВ hypotensiveВ gtts UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 11 6/11/2013 Signs/Symptoms • • • • • • • • • • • Asymptomatic DecreasedВ vision Pain/photophobia Redness NeovascularizationВ ofВ theВ anteriorВ chamber ElevatedВ intraocularВ pressure AnteriorВ chamberВ cells/flare CornealВ edema Ectropion uveae Synechial angleВ closure CuppingВ ofВ theВ opticВ nerve Treatment • • • • • • • • • • Prevention ReductionВ ofВ theВ IOP Panretinal Photocoagulation ParsВ plana vitrectomy (PPV) Endolaser (EL)В photocoagulationВ Anti‐VEGFВ agents* Trabeculectomy GlaucomaВ DrainageВ ImplantsВ (GDI) Cyclophotocoagulation (CPC) Cryoretinopexy UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 DifferentialВ Diagnosis • AcuteВ angle‐closureВ glaucoma • InflammatoryВ open‐angleВ glaucoma • OcularВ ischemicВ syndrome Pan‐RetinalВ Photocoagulation2 • GoldВ standardВ forВ initialВ treatmentВ ofВ anteriorВ segmentВ neovascularizationВ dueВ toВ retinalВ hypoxia • ReductionВ ofВ ischemicВ driveВ throughВ fragmentationВ ofВ bloodВ columnВ inВ allВ newВ vessels • NoninvasiveВ withВ fewВ complications • EffectsВ areВ long‐lastingВ butВ oftenВ takeВ weeksВ toВ occur • ApplicationВ ofВ burnsВ toВ coverВ aВ majorВ portionВ ofВ theВ retinaВ inВ allВ quadrants • 1200‐1600В burnsВ ofВ 500В micronВ spotВ sizeВ applied* 12 6/11/2013 TheВ roleВ ofВ Antiangiogenic Agents • RegressionВ ofВ neovascularizationВ occursВ quicklyВ butВ isВ temporaryВ andВ recurrenceВ isВ possible* • SmallВ studiesВ (Iliev,В Gheith)В haveВ shownВ thatВ earlyВ treatmentВ withВ intravitreal bevacizumab (IVB)В improvedВ NVGВ outcomes OutcomesВ ofВ TreatmentВ ofВ Neovascular GlaucomaВ withВ Intravitreal Bevacizumab.В В Moraczewski et.В al.В В Br.В JВ Ophthalmol 2009;В 93:589‐593. • BascomВ PalmerВ EyeВ InstituteВ StandardВ ofВ Care – 1.В IVBВ atВ timeВ ofВ diagnosis – 2.В PRPВ shortlyВ thereafter • OrВ Endolaser/PPVВ (ifВ cloudyВ media) – 3.В Medical/surgicalВ interventionВ (ifВ necessary) – IfВ IVBВ isВ administeredВ beforeВ formationВ ofВ PAS,В IOPВ mayВ beВ controlledВ withoutВ surgicalВ procedures9 ProposedВ TreatmentВ AlgorithmВ forВ Neovascular Glaucoma8 FollowВ upВ Schedule • EveryВ 2‐3В weeks1 (Hayreh,В prospectiveВ study) • EveryВ 3‐4В weeksВ forВ theВ firstВ 6В mos,В lessВ frequentlyВ thereafter.1 (Hayreh,В clinically) • NVI/NVAВ mayВ occurВ quicklyВ (daysВ toВ weeks).10 • RateВ atВ whichВ PASВ developsВ isВ remarkablyВ variableВ (daysВ toВ weeks).4 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 13 6/11/2013 OcularВ NeovascularizationВ AssociatedВ withВ CentralВ andВ Hemicentral RetinalВ VeinВ Occlusion.В В Hayreh etВ al.В В RetinaВ 32:1553‐1565,В 2012.В CumulativeВ ProbabilityВ ofВ developmentВ ofВ NVВ fromВ onsetВ ofВ ischemicВ CRVO1 References 1. 2. 3. 4. 5. 6. 7. Iris Angle Glaucoma withinВ 1В month 16% 8% 4% withinВ 2В months 26% 15% 11% withinВ 3В months 33% 28% 20% withinВ 6В months 49% 37% 29% 14. withinВ 9В months 52% 39% 34% 15. withinВ 5В years 63% 49% 39% Posner‐Schlossman SyndromeВ andВ InflammatoryВ Glaucoma 8. 9. 10. 11. 12. 13. 16. 17. OcularВ neovascularizationВ associatedВ withВ centralВ andВ hemicentral retinalВ veinВ occlusion.В В Hayreh etВ al.В В RetinaВ 32:1553‐1565,В 2012.В OphthalmicВ surgery:В PrincipleВ &В Practice.В Spaeth,В George.В 1990.В W.B.В SaundersВ company. NovartisВ PharmaceuticalsВ AustraliaВ PtyВ Limited.В http://www.avastin‐hcp.com/bevacizumab/moa/proposed‐mechanism‐of‐action Glaucoma,В ChandlerВ andВ Grant.В В 4th edition.В В EpsteinВ et.В al.В В 1997.В ChapterВ 225:В Neovascular Glaucoma;В Ophthalmology.В В 04/05/11;В Fanous,В Maher.В В ErythropoietinВ levelsВ inВ aqueousВ humorВ ofВ patientsВ withВ glaucoma.В В Nassiri et.В al.В В MolecularВ VisionВ 2012;В 18:1991‐1995. IntraocularВ PressureВ AbnormalitiesВ AssociatedВ withВ CentralВ andВ Hemicentral RetinalВ VeinВ Occlusion.В В Hayreh et.В al.В В OphthalmologyВ 2004;В 111;В 133‐141 MedicalВ andВ SurgicalВ TreatmentВ ofВ Neovascular Glaucoma.В В Olmos,В Lee.В В InternationalВ OphthalmologyВ Clinics.В В Vol 51,В NoВ 3,В 27‐36. OutcomesВ ofВ TreatmentВ ofВ Neovascular GlaucomaВ withВ Intravitreal Bevacizumab.В В Moraczewski et.В al.В В Br.В JВ Ophthalmol 2009;В 93:589‐593.В В CombinationВ Intravitreal Bevacizumab/panretinal PhotocoagulationВ vs Panretinal PhotocoagulationВ AloneВ inВ theВ TreatmentВ ofВ Neovascular Glaucoma.В В EhlersВ et.В al.В В RetinaВ 28:696‐702,В 2008. SurgicalВ OutcomeВ ofВ Intravitreal Bevacizumab andВ FiltrationВ SurgeryВ inВ Neovascular Glaucoma.В В Kitnarong et.В al.В В Adv.В Ther.В 2008;25(5):438‐443. Panretinal PhotocoagulationВ withВ SimultaneousВ Cryoretinopexy orВ Intravitreal Bevacizumab forВ Neovascular Glaucoma.В В Tatsumi etВ al.В В Graefes ArchВ Clin Exp Ophthalmol.В В 2012.В Mermoud A,В SalmonВ JF,В AlexanderВ P,В etВ al.В Molteno tubeВ implantationВ forВ neovascular glaucoma.В Long‐termВ resultsВ andВ factorsВ influencingВ theВ outcome.В Ophthalmology.В 1993;100:897–902. Krupin T,В KaufmanВ P,В Mandell AI,В etВ al.В Long‐termВ resultsВ ofВ valveВ implantsВ inВ filteringВ surgeryВ forВ eyesВ withВ neovascular glaucoma.В AmВ JВ Ophthalmol.В 1983;95:В 775–82. Anti‐VEGFВ TherapyВ forВ theВ treatmentВ ofВ glaucoma:В aВ focusВ onВ ranibizumab andВ bevacizumab.В В ParkВ et.В al.В В ExpertВ Opin Biol Ther.В 2012В Dec;В 12(12):1641‐7. SurgicalВ resultsВ ofВ AhmedВ ValveВ ImplantationВ withВ Intraoperative Bevacizumab InjectionВ inВ PatientsВ withВ Neovascular Glaucoma.В В Kyoung et.В al.В В JВ GlaucomaВ 2012;21:331‐336. CombinedВ Intravitreal Bevacizumab andВ Trabeculectomy withВ Mitomycin CВ vs Trabeculectomy withВ Mitomycin CВ AloneВ forВ Neovascular Glaucoma.В В Takihara et.В al.В В JВ GlaucomaВ 2011;20:196‐201. 65В yearВ old male • CC: “pressure” inВ eye – ConstantВ pressureВ andВ discomfortВ withinВ OSВ sinceВ thisВ morningВ withВ foggyВ vision,В mildВ dullВ headache,В andВ lightВ sensitivity • MedicalВ History: – HypertensionВ andВ hyperlipidemiaВ medically‐controlled TranВ Nguyen VAВ PaloВ AltoВ HCS PrimaryВ CareВ OptometryВ andВ LowВ VisionВ Rehabilitation UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 • NegativeВ familyВ medicalВ history • FamilyВ ocularВ history:В fatherВ blindВ dueВ toВ glaucoma 14 6/11/2013 HistoryВ Continued: • PatientВ OcularВ History: – “InflammatoryВ glaucomaВ vsВ Posner‐SchlossmanВ SyndromeВ OS” – ResolvedВ BRVOВ OSВ 2009В withoutВ complications – MeibomianВ glandВ dysfunction – MildВ cataractsВ OU – HistoryВ ofВ trauma,В punchedВ inВ ODВ whenВ young IntraocularВ Pressures: 02/26/13: •20/65В В @1438В Brimonidine,В cosopt,В latanoprost,В prednisolone acetateВ 1% •20/61В В @1550В Brimonidine,В cosopt,В latanoprost,В prednisolone acetateВ 1% •20/60В В @1611В Brimonidine,В cosopt,В latanoprost,В prednisolone acetateВ 1% •18/49В В @1650 • ‐‐/55В В В @1850В Diamox 500mgВ po • ‐‐/55В В @2250В В AnteriorВ chamberВ paracentesis OS: •‐‐/13В @2332В В Diamox 250mgВ q6h,В Vigamox qid,В cosopt tid,В brimonidine tid,В В prednislone acetateВ 1%В qid • OcularВ Medications: – CosoptВ bidВ OSВ withВ goodВ compliance • LastВ dose:В twiceВ thisВ morningВ atВ 9:00am DifferentialВ Diagnosis • AcuteВ angleВ closure • NeovascularВ glaucoma • HypertensiveВ uveiticВ syndromes – – – – • • • • • Posner‐SchlossmanВ Syndrome HerpeticВ keratouveitisВ Fuch’sВ heterochromicВ iridocyclitis CytomegalovirusВ iridocyclitis Inflammatory/uveiticВ glaucoma PrimaryВ openВ angleВ glaucoma Non‐arteriticВ ishemicВ opticВ neuropathy OpticВ neuritis MasqueradeВ syndromes UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Posner‐SchlossmanВ Syndrome: Recurrent,В unilateralВ anteriorВ uveitis withВ increasedВ IOP MinimalВ conjunctival injection CornealВ edema FewВ nonpigmented keratic precipitates,В fewВ cellsВ andВ В mildВ flareВ reaction • AnglesВ open • Pupils:В irisВ heterochromia andВ anisocoria • Trabeculitis • • • • – ExactВ mechanismВ unknown 15 6/11/2013 PathogenesisВ ofВ PSS: • SpectrumВ ofВ inflammatoryВ responsesВ toВ membersВ ofВ herpesviridae family – Cytomegalovirus • LocalВ antibodies – HerpesВ simplexВ virus “InflammatoryВ Glaucoma?" • PersistentВ orВ recurrentВ IOPВ elevationВ пѓЁ anatomicalВ andВ physiologicalВ damageВ toВ ONH • HigherВ suspicionВ forВ uveitic etiologyВ withВ unilateralВ glaucomatousВ opticВ neuropathy • AxonalВ andВ secondaryВ retinalВ ganglionВ cellВ lossВ пѓЁ OpticВ rimВ excavationВ &В RNFLВ thinning • Vascular/AutonomicВ imbalance • HLA‐Bw54В positiveВ ElevatedВ IOPВ andВ Non‐glaucomatousВ OpticВ Neuropathy • OpticВ atrophyВ &В PSS • NAIONВ &В PSS Management: • NonsurgicalВ treatment – Corticosteroids – TopicalВ nonsteroidal antiinflammatories – AqueousВ suppressants • FlowВ =В perfusionВ pressure resistanceВ toВ flow • PerfusionВ pressureВ = • SurgicalВ interventionВ withВ medicalВ failureВ orВ highВ riskВ cases – FilteringВ surgery MeanВ bloodВ pressure – IOP • Trabeculectomy withВ antimetabolites • GlaucomaВ drainageВ implants • DiscВ pallorВ inВ 20‐39%В withВ acuteВ angleВ closure • ReducedВ S‐coneВ componentВ ofВ ERGВ inВ PSS • DiagnosticВ labsВ andВ imagingВ whenВ warranted KimВ etВ alВ 2012.В KoreanВ JВ Ophthalmol UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 16 6/11/2013 IntraocularВ Pressures: 02/26/13: •20/65В В @1438В Brimonidine,В cosopt,В latanoprost,В prednisolone acetate •20/61В В @1550В Brimonidine,В cosopt,В latanoprost,В prednisolone acetate •20/60В В @1611В Brimonidine,В cosopt,В latanoprost,В prednisolone acetate •18/49В В @1650 • ‐‐/55В В В @1850В Diamox 500mgВ po • ‐‐/55В В @2250В В AnteriorВ chamberВ paracentesis OS: • ‐‐/13В @2332В В Diamox 250mgВ q6h,В Vigamox qid,В Dorz‐TimВ tid,В Alphagan tid,В PFВ qid 02/27/13 13/40В @1230 02/28/13:  ‐‐/13В @0711В POD#1В s/pВ AhmedВ OS 03/04/13: ‐‐/14В В @1505В POD#5В AtropineВ qd OS,В PFВ qid OS,В Vigamox qis OS 03/18/13: 20/21В @1500В PFВ qid OS 04/04/13: 19/18В @1328В PFВ qid OS,В Timolol 0.25%В bidВ OS 05/14/13: 18/18В @1013В Timolol 0.25%В bidВ OS 05/28/13В Follow‐Up: •VA:В 20/25В OU •1+В leftВ APD •IOP:В 18/23В mmHgВ atВ 0815 C/D:В 0.35H/VВ В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В В C/D:В 0.7H/0.75V UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 17 6/11/2013 Summary:В PosingВ asВ Posner’s? HVFВ OSВ 2006В vs 2013: • PreviouslyВ thoughtВ toВ be “self‐limiting” and “benign” – 26.4%В developВ glaucomatousВ damage – JapВ etВ al • CMVВ andВ HSVВ leadingВ infectiousВ etiologiesВ forВ PSS – StillВ poorlyВ understood • DistinctВ clinicalВ entitiesВ ofВ HSVВ uveiticВ glaucomaВ andВ CMVВ iridocyclitis • MultifactorialВ andВ complicatedВ spectrumВ ofВ conditions • ProphylacticВ treatmentВ inВ considerationВ ofВ NAIONВ associatedВ withВ acuteВ cyclitisВ episodes • ImportantВ toВ monitorВ forВ glaucomatousВ andВ non‐ glaucomatousВ opticВ neuropathy 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. References BeckВ RW,В ServaisВ GE,В HayrehВ SS.В AnteriorВ ischemicВ opticВ neuropathy.В IX.В Cup‐to‐discВ ratioВ andВ itsВ roleВ inВ pathogenesis.В Ophthalmology.В 1987В Nov;94(11):1503‐8. Bloch‐MichelВ E,В DussaixВ E,В CerquetiВ P,В PatarinВ D.В PossibleВ roleВ ofВ cytomegalovirusВ infectionВ inВ theВ etiologyВ ofВ theВ Posner‐SchlossmannВ syndrome.В IntВ Ophthalmol.В 1987В Dec;11(2):95‐6. BodhВ SA,В KumarВ V,В RainaВ UK,В GhoshВ B,В ThakarВ M.В InflammatoryВ glaucoma.В OmanВ JВ Ophthalmol.В 2011В Jan;4(1):3‐9. CeballosВ EM,В ParrishВ RKВ 2nd,В SchiffmanВ JC.В OutcomeВ ofВ BaerveldtВ glaucomaВ drainageВ implantsВ forВ theВ treatmentВ ofВ uveiticВ glaucoma.В Ophthalmology.В 2002В Dec;109(12):2256‐60. CheeВ SP,В JapВ A.В PresumedВ fuchsВ heterochromicВ iridocyclitisВ andВ Posner‐SchlossmanВ syndrome:В comparisonВ ofВ cytomegalovirus‐positiveВ andВ negativeВ eyes.В AmВ JВ Ophthalmol.В 2008В Dec;146(6):883‐9.e1.В CheeВ SP,В BacsalВ K,В JapВ A,В Se‐ThoeВ SY,В ChengВ CL,В TanВ BH.В ClinicalВ featuresВ ofВ cytomegalovirusВ anteriorВ uveitisВ inВ immunocompetent patients.В AmВ JВ Ophthalmol.В 2008В May;145(5):834‐40.В EpubВ 2008В FebВ 6. ContrerasВ I,В RebolledaВ G,В NovalВ S,В MuГ±oz‐NegreteВ FJ.OpticВ discВ evaluationВ byВ opticalВ coherenceВ tomographyВ inВ nonarteriticВ anteriorВ ischemicВ opticВ neuropathy.В InvestВ OphthalmolВ VisВ Sci.В 2007В Sep;48(9):4087‐92. ContrerasВ I,В NovalВ S,В RebolledaВ G,В MuГ±oz‐NegreteВ FJ.В Follow‐upВ ofВ nonarteriticВ anteriorВ ischemicВ opticВ neuropathyВ withВ opticalВ coherenceВ tomography.В Ophthalmology.В 2007В Dec;114(12):2338‐44.В EpubВ 2007В AugВ 27. DarchukВ V,В SampaolesiВ J,В MatoВ L,В NicoliВ C,В SampaolesiВ R.В OpticВ nerveВ headВ behaviorВ inВ Posner‐SchlossmanВ syndrome.В IntВ Ophthalmol.В 2001;23(4‐6):373‐ 9. DaВ MataВ A,В BurkВ SE,В NetlandВ PA,В BaltatzisВ S,В ChristenВ W,В FosterВ CS.В ManagementВ ofВ uveiticВ glaucomaВ withВ AhmedВ glaucomaВ valveВ implantation.В Ophthalmology.В 1999В Nov;106(11):2168‐72. DinakaranВ S,В KayarkarВ V.В TrabeculectomyВ inВ theВ managementВ ofВ Posner‐SchlossmanВ syndrome.В OphthalmicВ SurgВ Lasers.В 2002В Jul‐Aug;33(4):321‐2. FalconВ MG,В WilliamsВ HP.В HerpesВ simplexВ kerato‐uveitisВ andВ glaucoma.В TransВ OphthalmolВ SocВ UВ K.В 1978В Apr;98(1):101‐4. GoldbergВ DE,В FreemanВ WR.В UveiticВ angleВ closureВ glaucomaВ inВ aВ patientВ withВ inactiveВ cytomegalovirusВ retinitisВ andВ immuneВ recovery uveitis.В OphthalmicВ SurgВ Lasers.В 2002В Sep‐Oct;33(5):421‐5. GreenВ RJ.В Posner‐SchlossmanВ syndromeВ (glaucomatocycliticВ crisis).В ClinВ ExpВ Optom.В 2007В Jan;90(1):53‐6. HarringtonВ JR.В Posner‐SchlossmanВ syndrome:В aВ caseВ report.В JВ AmВ OptomВ Assoc.В 1999В Nov;70(11):715‐23. HayrehВ SS.В В AnteriorВ ischemicВ opticВ neuropathy.В ClinВ Neurosci.В 1997;4(5):251‐63. HiroseВ S,В OhnoВ S,В MatsudaВ H.HLA‐Bw54В andВ glaucomatocycliticВ crisis.В ArchВ Ophthalmol.В 1985В Dec;103(12):1837‐9. HongВ C,В SongВ KY.В EffectВ ofВ apraclonidineВ hydrochlorideВ onВ theВ attackВ ofВ Posner‐SchlossmanВ syndrome.В KoreanВ JВ Ophthalmol.В 1993В Jun;7(1):28‐33. HorowitzВ J,В Fishelzon‐ArevВ T,В RathВ EZ,В SegevВ E,В GeyerВ O.В ComparisonВ ofВ opticВ nerveВ headВ topographyВ findingsВ inВ eyesВ withВ non‐arteriticВ anteriorВ ischemicВ opticВ neuropathyВ andВ eyesВ withВ glaucoma.В GraefesВ ArchВ ClinВ ExpВ Ophthalmol.В 2010В Jun;248(6):845‐51.В EpubВ 2010В MarВ 6. IrakВ I,В KatzВ BJ,В ZabriskieВ NA,В ZimmermanВ PL.Posner‐SchlossmanВ syndromeВ andВ nonarteriticВ anteriorВ ischemicВ opticВ neuropathy.В JВ Neuroophthalmol.В 2003В Dec;23(4):264‐7. IwaoВ K,В InataniВ M,В SetoВ T,В TakiharaВ Y,В Ogata‐IwaoВ M,В OkinamiВ S,В TaniharaВ H.Long‐termВ OutcomesВ andВ PrognosticВ FactorsВ forВ TrabeculectomyВ WithВ MitomycinВ CВ inВ EyesВ WithВ UveiticВ Glaucoma:В AВ RetrospectiveВ CohortВ Study.В JВ Glaucoma.В 2012В AugВ 14.В JapВ A,В SivakumarВ M,В CheeВ SP.В IsВ PosnerВ SchlossmanВ syndromeВ benign?В Ophthalmology.В 2001В May;108(5):913‐8. JonesВ RВ 3rd,В PasqualeВ LR,В Pavan‐LangstonВ D.HerpesВ simplexВ virus:В anВ importantВ etiologyВ forВ secondaryВ glaucoma.В IntВ OphthalmolВ Clin.В 2007В Spring;47(2):99‐107 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. KassВ MA,В BeckerВ B,В KolkerВ AE.В GlaucomatocycliticВ crisisВ andВ primaryВ open‐angleВ glaucoma.В AmВ JВ Ophthalmol.В 1973В Apr;75(4):668‐73. KimВ R,В VanВ StavernВ G,В JuzychВ M.В NonarteriticВ anteriorВ ischemicВ opticВ neuropathyВ associatedВ withВ acuteВ glaucomaВ secondaryВ toВ Posner‐SchlossmanВ syndrome.В ArchВ Ophthalmol.В 2003В Jan;121(1):127‐8. KimВ TH,В KimВ JL,В KeeВ C.OpticВ discВ atrophyВ inВ patientВ withВ Posner‐SchlossmanВ syndrome.В KoreanВ JВ Ophthalmol.В 2012В Dec;26(6):473‐7.В EpubВ 2012В NovВ 12. KnoxВ DL.В ClinicalВ featuresВ ofВ cytomegalovirusВ anteriorВ uveitisВ inВ immunocompetentВ patients.В AmВ JВ Ophthalmol.В 2008В Oct;146(4):625;В authorВ replyВ 625‐6. LiВ J,В AngВ M,В CheungВ CM,В VaniaВ M,В ChanВ AS,В WaduthantriВ S,В YangВ H,В CheeВ SP.В AqueousВ cytokineВ changesВ associatedВ withВ Posner‐SchlossmanВ syndromeВ withВ andВ withoutВ humanВ cytomegalovirusВ В 2012;7(9):e44453.В EpubВ 2012В SepВ 13. MaedaВ H,В NakamuraВ M,В NegiВ A.В SelectiveВ reductionВ ofВ theВ S‐coneВ componentВ ofВ theВ electroretinogramВ inВ Posner‐SchlossmanВ syndrome. EyeВ (Lond).В 2001В Apr;15(PtВ 2):163‐7. MietzВ H,В AisenbreyВ S,В UlrichВ Bartz‐SchmidtВ K,В BamborschkeВ S,В KrieglsteinВ GK.GanciclovirВ forВ theВ treatmentВ ofВ anteriorВ uveitis.В GraefesВ ArchВ ClinВ ExpВ Ophthalmol.В 2000В Nov;238(11):905‐9. MohamedВ Q,В ZamirВ E.UpdateВ onВ Fuchs'В uveitisВ syndrome.В CurrВ OpinВ Ophthalmol.В 2005В Dec;16(6):356‐63. MoorthyВ RS,В MermoudВ A,В BaerveldtВ G,В MincklerВ DS,В LeeВ PP,В RaoВ NA.В GlaucomaВ associatedВ withВ uveitis.В SurvВ Ophthalmol.В 1997В Mar‐Apr;41(5):361‐94. OzdalВ PC,В ViannaВ RN,В DeschГЄnesВ J.В AhmedВ valveВ implantationВ inВ glaucomaВ secondaryВ toВ chronicВ uveitis.В EyeВ (Lond).В 2006В Feb;20(2):178‐83. PapadakiВ TG,В ZacharopoulosВ IP,В PasqualeВ LR,В ChristenВ WB,В NetlandВ PA,В FosterВ CS.Long‐termВ resultsВ ofВ AhmedВ glaucomaВ valveВ implantationВ forВ uveiticВ glaucoma.В AmВ JВ Ophthalmol.В 2007В Jul;144(1):62‐69.В EpubВ 2007В MayВ 9. PosnerВ A.,В SchlossmanВ A,В SyndromeВ ofВ unilateralВ recurrentВ attacksВ ofВ glaucomaВ withВ cyclitisВ symptoms.В ArchВ Ophthalmol,В 39В (1948),В pp.В 517–535 RothВ M,В SimmonsВ RJ.В GlaucomaВ associatedВ withВ precipitatesВ onВ theВ trabecularВ meshwork.В Ophthalmology.В 1979В Sep;86(9):1613‐9. SanghaВ SS.В PosnerВ SchlossmanВ syndrome.В Ophthalmology.В 2002В Mar;109(3):409. ShazlyВ TA,В AljajehВ M,В LatinaВ MA.Posner‐SchlossmanВ glaucomatocycliticВ crisis.В SeminВ Ophthalmol.В 2011В Jul‐Sep;26(4‐5):282‐4.В SngВ CC,В SeeВ JS,В NgoВ CS,В SinghВ M,В ChanВ YH,В AquinoВ MC,В TanВ AM,В ShabanaВ N,В ChewВ PT.В ChangesВ inВ retinalВ nerveВ fibreВ layer,В opticВ nerveВ headВ morphology,В andВ visualВ fieldВ afterВ acuteВ primaryВ angleВ closure.В EyeВ (Lond).В 2011В May;25(5):619‐25.В В EpubВ 2011В MarВ 25. SuhВ MH,В KimВ SH,В ParkВ KH,В KimВ SJ,В KimВ TW,В HwangВ SS,В KimВ DM.В ComparisonВ ofВ theВ correlationsВ betweenВ opticВ discВ rimВ areaВ andВ retinalВ nerveВ fiberВ layerВ thicknessВ inВ glaucomaВ andВ nonarteriticВ anteriorВ ischemicВ opticВ neuropathy.В AmВ JВ Ophthalmol.В 2011В Feb;151(2):277‐86.e1.В В EpubВ 2010В DecВ 18. SoodВ GC,В KapoorВ S,В KrishnamurthyВ MS,В ReddyВ S,В SookВ M.В Posner‐SchlossmanВ syndromeВ surgicalВ management.В EyeВ EarВ NoseВ ThroatВ Mon,В 55В (1976),В pp.В 29–32 TakahashiВ T,В OhtaniВ S,В MiyataВ K,В MiyataВ N,В ShiratoВ S,В MochizukiВ M.В AВ clinicalВ evaluationВ ofВ uveitis‐associatedВ secondaryВ glaucoma.В JpnВ JВ Ophthalmol.В 2002В Sep‐Oct;46(5):556‐62. TakusagawaВ HL,В LiuВ Y,В WiggsВ JL.InfectiousВ theoriesВ ofВ Posner‐SchlossmanВ syndrome.В IntВ OphthalmolВ Clin.В 2011В Fall;51(4):105‐15.В TeohВ SB,В TheanВ L,В KoayВ E.В CytomegalovirusВ inВ aetiologyВ ofВ Posner‐SchlossmanВ syndrome:В evidenceВ fromВ quantitativeВ polymeraseВ chainВ reaction.В EyeВ (Lond).В 2005В Dec;19(12):1338‐40. WongВ M,В GoldsteinВ DA,В TesslerВ HH;В PresumedВ FuchsВ heterochromicВ iridocyclitisВ andВ Posner‐SchlossmanВ syndrome:В comparisonВ ofВ cytomegalovirus‐ positiveВ and ‐negativeВ eyesВ authorВ reply.В В AmВ JВ Ophthalmol.В 2009В Jun;147(6):1106‐7 YamamotoВ S,В Pavan‐LangstonВ D,В TadaВ R,В YamamotoВ R,В KinoshitaВ S,В NishidaВ K,В ShimomuraВ Y,В TanoВ Y.В PossibleВ roleВ ofВ herpesВ simplexВ virusВ inВ theВ originВ ofВ Posner‐SchlossmanВ syndrome.В AmВ JВ Ophthalmol.В 1995В Jun;119(6):796‐8. YangВ SY,В ChenВ MJ,В ChenВ KH,В LiВ AF,В ChouВ CK,В LeeВ SM.В CytomegalovirusВ andВ herpesВ simplexВ virusВ asВ causesВ ofВ bilateralВ anteriorВ uveitisВ inВ anВ immunocompetentВ patient.В JВ ChinВ MedВ Assoc.В 2011В Jan;74(1):48‐50.В EpubВ 2011В JanВ 19. 18 6/11/2013 Case Report • 30 year old Caucasian female Lights Out By Baljit Sohal, OD Central California VA Health Care Systems, Fresno CA Case report continued • VA – c/o vision loss in the right eye for past three days – started with some blurriness and felt the “lights went out” in that eye • Medical and ocular history: unremarkable Case continued… • Slit lamp findings – NLP OD, 20/25 OS sc • Entrance testing – Pupils: PERRL 2+APD OD – Extraocular motility testing: • FROM OU with mild pain on down gaze OD – Confrontational visual field testing – Conjunctiva: Temporal pinguecula OU – Cornea: clear OU – Anterior chamber: deep/quiet OU – Lens: 1+ Nuclear sclerotic cataracts OU – IOP: 15mmHg OD, 18mmHg OS by Goldmann • Unable to test OD, full OS UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 19 6/11/2013 Case continued… • 60D undilated fundoscopic view – 0.35V/0.40H OD, 0.50V/0.55H OS – Pink and healthy nerves OU – Macula flat (-)exudates/heme/srf OU – Vessels were normal OU Imaging continued… • MRI of the orbits/brain – Asymmetric enlargement, edema, and enhancement of the right optic nerve anterior to the chiasm involving the intraorbital segment – Brain parenchyma intact, without characteristic white matter lesions of multiple sclerosis UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 What to do? • Assessment – Retrobulbar optic neuritis OD • Plan – CT scan of brain and orbits followed by MRI of brain and orbits with gadolinium – RTC 7-14 days for recheck Optic neuritis and clinical features • Acute demyelinating disease of the optic nerve • Isolated neurological finding or can be associated with MS • Monocular vision loss – 10% in both eyes • simultaneous • rapid succession • Eye pain on eye movements • Visual field defect – central scotoma 20 6/11/2013 Clinical features continued… • Anterior optic neuritis • Retrobulbar optic neuritis – Papillitis • hyperemia • swelling of the disc – Blurry disc margins – Distended veins – APD – Color vision – Normal fundoscopic examination – Disc pallor after few weeks – APD – Color vision – Most common Optic Neuritis Treatment Trial • Results – Patients receiving IV methylprednisolone followed by oral prednisone recovered vision faster than placebo • Final visual outcome was only slightly better at 6 mo – Oral prednisone alone provided no benefit in rate of recovery or final outcome at six months Optic neuritis treatment • Optic Neuritis Treatment Trial – Corticosteroids in the treatment of acute optic neuritis – 457 patients with acute optic neuritis • Oral prednisone x 14 days(1mg per kg of body weight per day) • Intravenous methylprednisolone (1g/day for 3 days) followed by oral prednisone for 11 days • Oral placebo MRI and MS • Typical brain lesion plaques that are seen in patients with MS – Ovoid – Periventricular – white matter lesions – Larger than 3mm • ONTT follow up showed the risk of MS after Optic neuritis • higher rate of new attacks UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 21 6/11/2013 Optic Neuritis Treatment Trial • Cumulative probability of developing MS by 15 year examination was 50% – Strongly related to presence of lesions on the baseline brain MRI – No difference among treatment groups • Risk of developing MS was highest in the first five years overall • In patients w/o lesions, risk was higher for women(16%), or with retrobulbar ON What is MS • Autoimmune • Demyelinating disorder of the nervous system – Commonly manifested with visual involvment • Chronic relapsing and remitting, episodic disease UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 ONTT and MS continued • No baseline MRI lesions – Approx 15% developed MS during 5 years – 25% developed MS during 15 year follow-up • One or more lesions – Approx 42% developed MS during 5 years – 72% developed MS during 15 year follow-up • Low risk of MS – no MRI/brain lesions, – male gender – optic disc edema and atypical optic neuritis Multiple sclerosis symptoms • Numbness or weakness in one or more limbs • Double vision or blurring of vision • Tingling or pain in parts of your body • Electric-shock sensations that occur with certain head movements • Tremor, lack of coordination or unsteady gait • Slurred speech • Fatigue • Dizziness 22 6/11/2013 More ocular involvement • Isolated cranial nerve palsies – Mostly CN 6 • Internuclear Ophthalmoplegia • Defects with Saccades and Pursuits • Nystagmus – INO, vestibular, pendular, gaze-evoked • Retinal periphlebitis (10-39%) – Perivascular exudation, hemorrhage, and retinal venous sheathing “Worst Headache of my life" Treatment and Management of Pituitary Macroadenoma References • • • • • • • • Mathews, Michaela. Nonarteritic anterior ischemic optic neuropathy. Current Opinion in Ophthalmology. Lippincott Williams & Wilkins. 2005 Beck, Roy, M.D, et al. A Randomized, Controlled Trial of Corticosteroids in the Treatment of Acute Optic Neuritis. The New England Journal of Medicine. Massachusetts medical society. 1992 Myelitis Association. The Transverse Myelitis Association, Optic Neuritis. TMA. 2012 Osborne, Benjamin, et al. Optic Neuritis: Pathophysiology, Clinical Feautures, and Diagnosis. Wolters Kluwer Health. Uptodate. 2013 Gal, Robin, et al. Visual Function More Than 10 Years After Optic Neuritis: Experience of the Optic Neuritis Treatment Trial. American Journal of Opthalmology. Elsevier Inc, 2004 Gal, Robin, et al. Multiple Sclerosis Risk after Optic Neuritis: Final Optic Neuritis Treatment Trial Follow up. Arch Neurol. 2008 June; 65(6):727-732 Volpe, Nicholas, et al. Optic Neuritis and risk of MS: Differential diagnosis and management. Cleveland clinic Journal of Medicine. March 2009 vol 76 3 181-190 Chen, Ling, et al. Ocular Manifestations of Multiple Sclerosis. Current Opinion in Ophthalmology 2005. 16:315 -320 D.M п‚ћ 64 yo WM presented to outside Emergency Department п‚ћ “Worse headache of my life” Tresca Truong Optometry Resident VA Sierra Nevada Health Care SystemReno 6/23/13 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 п‚ћ HPI п‚— п‚— п‚— п‚— п‚— Crushing, alleviated by nothing Nausea Vomiting Woke him from sleep No altered mental status, fever or weight loss п‚— No vision loss п‚ћ Systemic medical history п‚— Chronic pain п‚— Colon polyps п‚— Bipolar Disorder п‚— Anxiety п‚ћ Medications: Oxycodone HCL, Morphine п‚ћ Social history п‚— Lives alone п‚— (-) smoking п‚— (+) alcohol: “few times a week” 23 6/11/2013 Differential Diagnosis • • • • • • • Pituitary Gland Migraine Tension headache Cluster headache CVA Intracerebral hemorrhage Intracranial mass Sinusitis Reno VA п‚ћ Right superior visual field loss, losing 11 lbs in one month, confusion, difficulty with memory’ п‚ћ Patient Medical History п‚ћ п‚ћ п‚ћ п‚ћ п‚ћ п‚ћ п‚ћ п‚ћ Anxiety Psychosocial disorder Mood disorder Low back pain Gout Medication seeking behavior Hypercholesteremia Hypogonadism п‚ћ п‚ћ Medications п‚ћ Allopurinol, calcium, docusate, morphine, oxycodine, respiridone, simvastatin, tamulosin Social History п‚— Smoking: quit 40 years ago п‚— EtOH: 3-4x a week, sometimes 6 pack of beer/day, with wine at night п‚— Illicit Drugs: history of cocaine and marijuana use UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 24 6/11/2013 10mm Treatment 1,2,3 • Monitor if <10mm • Endoscopic Transphenoidal Tumor Resection • Radiotherapy only if residual tumor tissue left over after surgery • Labs must be ordered to determine if secreting or non-secreting. – – – – – – – – TSH Thyroxine GH Prolactin Estrogen/Testosterone ACTH LH ADH UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Pituitary Adenoma • Common benign tumors 1,2,3 • 10-12% of adult intracranial neoplasms 2,5,8 • Categorization 6,7,8 – Size (micro vs macro) • Stage 1 <10mm • Stage 2 >10mm • Stage 3 locally invasive • Stage 4 diffusely invasive – Secretions (nonfunctioning vs functioning) • Incidence rates 8,9 – Higher in women in early life – More common with men later in life – Higher in African American and lowest in American Indians/Alaskan Natives 25 6/11/2013 Stage of Improvement 11 Visual Disturbance 1,3,7,10 • Stage One (surgery to one week) – Visual Field Defects 96% • Unilateral 32.9% • Bilateral 67.1% • Rapid recovery, result of recovery of nerve conduction by removal of physiologic conduction block – Visual Acuity 63% – Color vision 38.7-56% – Optic Atrophy 28-49% – Ptosis 6% – Diplopia 10% – Nerve palsy 2% • Stage Two (1 month to 4 months) – Delayed recovery is thought to be the result of remyelination of decompressed optic pathways • Stage Three Positive • • • • • Young age Short duration of symptoms Good acuity Small field loss Normal color vision – Late recovery over months to years. Not well studied Negative • Optic disc pallor • High MD absolute value • Long duration of symptoms • Large Tumor size UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Complete Recovery Partial Recovery Unchanged Visual Field (95%) 48.9% 46.8% 4.3% Visual Acuity 33.35% 33.35% 33.3% Color Vision 30% 52.8% (-) Optic Disc Pallor 16.9% 50% (-) 26 6/11/2013 11/19/2012 Follow-up Follow-up • Biopsy:Non-functioning • Pt reported intermittent left lower VF defect • Given size of mass, will likely need radiation • VA: 20/60 PH 20/30 OD 20/40 PH 20/30-1 OS • Start on testosterone • (-)APD • Ishihara: 14/14 OU • Confrontational fields: left lower quadrant VF constriction • EOMs revealed full ductions and versions Anterior Segment • Unremarkable Posterior Segment • C/Ds: 0.20h/v OU • Macula: normal • Vessels: normal caliber • Periphery: (-)holes and detachments References What can we do? 1. 1. 2. 3. 4. 5. Filters to enhance contrast Low vision exam for devices that may help with magnification Prisms or mirrors to compensate for field loss or diplopia Vision therapy Visual fields important to see if they meet state law requirements for driver’s license. UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Barzaghi et al. Prognostic Factors of Visual Field Improvement after Trans-sphenoidal Approach for Pituitary Macroadenomas: Review of the Literature and Analysis by Quantitative Method. NeuroSurgery Review. 2012. 35:369-379 2. Dhasmana et al. Visual Fields at Presentation and After Trans-Sphenoidal Resection of Pituitary Adenomas. J. Ophthalmic Vis Res. 2011. 6(3):187-191. 3. Schmalisch et al. Predictors for Visual Dysfunction in Nonfunctioning Pituitary Adenomas-Implications for Neurosurgical Management. Clinical Endocrinology. 2012. 77:728-734. 4. Pituitary Macroadenoma Endonasal Endoscopic Removal. St. John’s Health Center. 5. Lee et al. The Volume of Tumor Mass and Visual Field Defect in Patients with Pituitary Macroadenoma. Korean J. Ophthalmology. 2011. 25(1): 37-41. 6. Daly et al. The Epidemiology and Management of Pituitary Incidentalomas. Hrm. Rs. 2007 68(5): 195-198 7. De Aguiar Ribeiro Cury et al. Non-functioning Pituitary Adenomas: Clinical Feature, Laboratorial an Imaging Assessment, Therapeutic Management and Outcome. Arq Bras Endocrinol Metab. 2009. 53 (1): 31-39. 8. Caputo et al. Gender Differences in Presentation and Outcome of Nonfunctioning Pituitary Macroadenomas. Clinical Endocrinology. 2013. 78:564-570. 9. McDowell et al. Demographic Differences in Incidence for Pituitary Adenoma. Pituitary. 2011. 14(10):23-30. 10. Poon et al. Patterns of Visual Loss Associated with Pituitary Macroadenomas. Aus and NZ Journal of Ophth. 1995. 23(2):107-115. 11. Kerrison et al. Stages of Improvement in Visual Fields After Pituitary Tumor Resection. Am. Journal of Ophth. 2000. 130 (6): 813-820. 27 6/11/2013 DifferentialВ DiagnosisВ ofВ anВ EsotropiaВ withВ anВ AbductionВ DeficitВ inВ Infants JillВ Kronberg,В OD JuneВ 23,В 2013 3‐Year‐OldВ Male IncidenceВ ofВ Strabismus • 3‐5%В ofВ childrenВ affectedВ byВ strabismus • EsotropiaВ appearsВ 3‐5В XВ moreВ thanВ exotropia inВ children • 50%В ofВ childhoodВ esotropiaВ hasВ anВ accommodativeВ component • AfterВ ageВ 4В theВ prevalenceВ ofВ exotropia exceedsВ esotropia • IntermittentВ exotropia isВ theВ mostВ commonВ typeВ ofВ exotropia ExamВ Findings • AbductionВ deficit • SecondВ Opinion • • IntolerantВ ofВ spectacleВ wear CurrentВ Rx: • OD: ‐1.25В DS • OS: ‐2.00В DS • PersonalВ MedicalВ History • • • • BornВ past‐term MildВ asthma NICUВ forВ breathingВ difficulty NoВ medications RefractiveВ Findings VisualВ Acuity • CardiffВ @В 100В cm • OD:В 0.6/1.9В MВ ~20/63 • OS:В 0.6/1.2В MВ ~20/40 • OU:В 20/50 Retinoscopy • OD:В plano ‐1.25В x 090 • OS:В plano – 1.50В x 090 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 – OD: ‐2В restriction – OS: ‐4В restriction • CompensatoryВ headВ posture • OcularВ posture:В appearedВ alignedВ inВ primaryВ gaze • ContrastВ sensitivity:В 1.6%В MichelsonВ Contrast • NormalВ colorВ vision • AnteriorВ Segment:В Unremarkable • PosteriorВ Segment:В Unremarkable DifferentialВ Diagnosis • SixthВ CranialВ NerveВ Palsy • TypeВ IВ DuaneВ Syndrome • InfantileВ Esotropia • AccommodativeВ Esotropia • MobiusВ Syndrome 28 6/11/2013 SixthВ CranialВ NerveВ Palsy • SuddenВ onsetВ inwardВ eye‐turn • LimitedВ aBduction • Head‐turnВ towardsВ affectedВ side – EliminatesВ diplopia Etiology • MostВ commonВ cause:В IntracranialВ tumor • Post‐vaccination • Post‐febrileВ infection • Hydrocephalus • Trauma IntracranialВ tumors • WorstВ prognosisВ inВ symptoms – LargeВ restrictionВ ofВ abduction – MostВ likelyВ toВ beВ bilateral • AssociatedВ neurologicВ symptoms – Headache,В ataxia,В andВ otherВ cranialВ nerveВ palsies – OnsetВ withinВ oneВ weekВ ofВ strabismus • TypesВ ofВ tumors – BrainstemВ glioma – CholesterolВ granuloma ofВ petrous bone – Eosinophilic granuloma ofВ petrous bone http://www.meddean.luc.edu/lumen/MedEd/grossanatomy/h_ n/cn/cn1/images/cn‐6.jpg http://avserver.lib.uthsc.edu:8080/Medicine/eye_exam/SixthNervePalsy.jpg Prognosis TypeВ IВ DuaneВ Syndrome • MechanismВ isВ unknown • FullВ recoveryВ expectedВ inВ benignВ palsy • SpontaneouslyВ resolvesВ withinВ 6В months Treatment • • • • ThoroughВ caseВ history AssociatedВ neurologicВ symptoms:В MRI/refer SpontaneousВ resolution NoВ resolutionВ postВ 6В months – Botulinum toxin – Surgery – betterВ outcomeВ closerВ toВ onset • CongenitalВ disorderВ affectingВ ocularВ motility • CharacterizedВ by: – LimitedВ aBduction – NarrowingВ ofВ theВ intrapalpebral fissureВ onВ adduction – RetractionВ ofВ theВ globeВ onВ adduction http://www.mrcophth.com/ocularmotility/duaneb.JPG UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 29 6/11/2013 • • • • Characteristics TypeВ IВ DuaneВ SyndromeВ isВ mostВ commonВ classificationВ ofВ DuaneВ syndrome FemaleВ >В male PossibleВ strabismusВ inВ primaryВ position OSВ moreВ frequentlyВ affectedВ inВ aВ unilateralВ presentation Etiology • AbsenceВ ofВ abducens nucleus • AnomalousВ innervation byВ CNВ IIIВ toВ theВ lateralВ rectusВ muscle – MRВ &В LRВ contractВ simultaneouslyВ causingВ globeВ retraction • NoВ associatedВ degenerationВ associatedВ absenceВ ofВ nucleus Prognosis/Treatment • Prognosis: – Non‐progressive • Treatment – StrabismusВ surgeryВ ifВ strabismusВ inВ primaryВ gaze – BestВ outcomeВ withВ bilateralВ esotropiaВ DuaneВ syndrome Prognosis/Treatment InfantileВ Esotropia • PreviouslyВ knownВ asВ congenitalВ esotropia – NotВ initiallyВ presentВ inВ neonates • PresentsВ beforeВ 6В monthsВ ofВ age • LargeВ angleВ esotropia – (>40В prismВ diopters) • VerticalВ misalignment – DissociatedВ verticalВ deviationВ (DVD) – Over‐actionВ ofВ theВ inferiorВ oblique • AbductionВ obtainable http://health‐ 7.com/Atlas%20of%20Pediatric%20Physical%20Diagnosis/Esodeviations/ 1 AccommodativeВ Esotropia • Over‐convergenceВ associatedВ withВ accommodativeВ system • ThreeВ originsВ ofВ accommodativeВ esotropia • Prognosis – AmblyopiaВ treatment • GoodВ visualВ acuityВ outcomes • UnlikelyВ toВ appreciateВ stereopsis • Treatment – TreatВ amblyopia – Surgery • ContraindicatedВ beforeВ fourВ monthsВ ofВ age • DegreeВ ofВ esotropiaВ mayВ resolveВ beforeВ sixВ monthsВ ofВ age • CorrectВ refractiveВ errorВ beforeВ surgery UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 – Hypermetropia – HighВ ratioВ ofВ accommodativeВ convergenceВ toВ accommodationВ (AC/A) – CombinationВ ofВ hypermetropia andВ AC/AВ ratio TypesВ ofВ AccommodativeВ Esotropia • PartiallyВ accommodative – ResidualВ esotropiaВ withВ fullВ (+)В Rx – Hypothesized:В secondaryВ anatomicalВ contractureВ ofВ medialВ rectus • FullyВ accommodative – CorrectedВ withВ fullВ (+)В Rx 30 6/11/2013 Prognosis/Treatment Mobius Syndrome •UnilateralВ orВ BilateralВ В В В В В В В В В В В В В В В CNВ VIВ Palsy •ImpairmentВ ofВ aBduction • Prognosis:В Excellent – PotentialВ forВ stereopsis – NormalВ visualВ acuity • Treatment – TreatableВ withВ glassesВ /В bifocals • EnsureВ addВ bisectsВ theВ pupil!! – SurgeryВ contraindicated •CNВ VIIВ Palsy •Non‐progressive CharacteristicВ Appearance • • • • Mask‐likeВ facies Drooling Lagophthalmos AssociatedВ limbВ anomalies – ClubВ foot,В fusedВ digits,В absenceВ ofВ portionВ ofВ limb – Poland’sВ anomaly • SyndactylyВ +В malformationВ ofВ unilateralВ pectoralisВ muscle http://bjo.bmj.com/content/86/8/923.full http://www.mastersinhealthcare.net/blog/2010/10‐diseases‐you‐didnt‐know‐existed/ Etiology • Unknown • Hypothesis – TransitoryВ interruptionВ ofВ fetalВ bloodВ supplyВ toВ brainВ stem • SecondaryВ toВ tetratogen exposureВ duringВ theВ firstВ trimester • Tetratogen:В gestationalВ hyperthermia,В electricВ shock,В abuseВ ofВ benzodiazepines,В alcohol,В etc. Prognosis/Treatment DifferentialВ Summary • • • • • Mobius пѓЁ Rare,В allowВ headВ movement VIВ CranialВ NerveВ PalsyВ пѓЁ ReferВ OMD/ConsiderВ MRI InfantileВ EsotropiaВ пѓЁ Co‐managementВ (ProvideВ Rx) AccommodativeВ EsotropiaВ пѓЁ FullВ (+),В don’tВ refer DuaneВ SyndromeВ пѓЁ Relax,В it’sВ stable! • Prognosis:В Good – StableВ condition • Treatment – AllowВ patientВ toВ moveВ headВ intoВ restrictedВ fields UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 31 6/11/2013 TheВ restВ ofВ theВ story… • RemainingВ patientВ history – MildВ leftВ facialВ nerveВ palsy – NoВ limbВ anomalies • PreviouslyВ diagnosedВ withВ Mobius syndromeВ atВ 8В monthsВ ofВ age References • • • Assessment • MobiusВ syndrome – PreviouslyВ diagnosed • RegularВ astigmatism • • • • • • • Plan • DiscontinueВ sphericalВ myopicВ spectacleВ wear • AllowВ ptВ toВ moveВ hisВ head • InformВ pediatrician/physicalВ therapistsВ toВ allowВ headВ movement • SeekВ careВ yearly • • • • • • • • • • Batra,В Noopur N.,В CO.В "ComparisonВ ofВ PrimaryВ PositionВ MeasurementsВ andВ AbductionВ DeficitВ BetweenВ TypeВ IВ DuaneВ SyndromeВ andВ SixthВ CranialВ NerveВ Palsy."В JournalВ ofВ Neuro‐Ophthalmology 31В (2011):В 117‐20.В Print.В Birch,В E.,В D.В Stager,В K.В Wright,В R.В Beck,В andВ Pediatriceyediseaseinvestigator.В "TheВ NaturalВ HistoryВ ofВ InfantileВ EsotropiaВ duringВ theВ FirstВ SixВ MonthsВ ofВ Life1,В 2."В JournalВ ofВ AmericanВ AssociationВ forВ PediatricВ OphthalmologyВ andВ Strabismus 2.6В (1998):В 325‐28.В Print.В Birth,В EileenВ E.В "Stereoacuity OutcomesВ FollowingВ TreatmentВ ofВ InfantileВ andВ AccommodativeВ Esotropia."В OptometryВ &В VisionВ Science 86.6В (2009):В 647‐ 52.В Print.В Briegel,В W.В "NeuropsychiatricВ FindingsВ ofВ Mobius Sequence ‐ aВ Review."В ClinicalВ Genetics 70.2В (2006):В 91‐97.В Print.В Carta,В Arturo,В MD.В "OphthalmologicВ andВ SystemicВ FeaturesВ inВ Mobius Syndrome:В AnВ ItalianВ CaseВ Series."В Ophthalmology 118.8В (2011):В 1518‐523.В Print.В Cheng,В DarylВ R.В "RecurrentВ 6thВ NerveВ PalsyВ inВ aВ ChildВ followingВ DifferentВ LiveВ AttenuatedВ Vaccines:В CaseВ Report."В BMCВ InfectiousВ Diseases 12.105В (2012):В 1‐5.В Print.В Dotan,В Gad.В "TheВ RoleВ ofВ Neuroimaging inВ theВ EvaluationВ ProcessВ ofВ ChildrenВ withВ IsolatedВ SixthВ NerveВ Palsy."В Child'sВ NervousВ System 29В (2013):В 89‐92.В Print.В Hutchinson,В Amy.В "RefractiveВ SurgeryВ forВ AccommodativeВ Esotropia:В Past,В Present,В andВ Future."В EuropeanВ JournalВ ofВ Ophthalmology 22.6В (2012):В 871‐ 77.В Print.В Ing MR. “Long‐termВ follow‐upВ ofВ congenitalВ esotropiaВ inВ aВ populationВ basedВ study.” JournalВ ofВ theВ AmericanВ AssociationВ forВ PediatricВ Opthalmology andВ Strabismus 2009:В 427 Johansson,В Maria,В MD.В "AutisticВ SpectrumВ DisordersВ inВ Mobius Sequence:В AВ ComprehensiveВ StudyВ ofВ 25В Individuals."В DevelopmentalВ MedicineВ &В ChildВ Neurology 43В (2001):В 338‐45.В Print.В Kang,В N.,В andВ J.В Demer.В "ComparisonВ ofВ OrbitalВ MagneticВ ResonanceВ ImagingВ inВ DuaneВ SyndromeВ andВ Abducens Palsy."В AmericanВ JournalВ ofВ Ophthalmology 142.5В (2006):В 827‐34.e2.В Print.В Khan,В A.,В andВ D.В Oystreck.В "ClinicalВ CharacteristicsВ ofВ BilateralВ DuaneВ Syndrome."В JournalВ ofВ AmericanВ AssociationВ forВ PediatricВ OphthalmologyВ andВ Strabismus 10.3В (2006):В 198‐201.В Print.В Kim,В Wook Kyum.В "TheВ AnalysisВ ofВ AC/AВ RatioВ inВ Nonrefractive AccommodativeВ EsotropiaВ TreatedВ withВ BifocalВ Glasses."В KoreanВ JournalВ ofВ Ophthalmology 26.1В (2012):В 39‐44.В Print.В Lee,В Tae‐Eun.В "AccommodativeВ andВ TonicВ ConvergenceВ andВ AnatomicalВ ContractureВ inВ PartiallyВ AccommodativeВ andВ Non‐accommodativeВ Esotropia."В OphthalmicВ &В PhysiologicalВ Optics 32В (2012):В 535‐38.В Print.В Merino,В Pilar,В MD.В "EtiologyВ andВ TreatmentВ ofВ PediatricВ SixthВ NerveВ Palsy."В JournalВ ofВ AmericanВ AssociationВ forВ PediatricВ OphthalmologyВ andВ Strabismus 14.6В (2010):В 502‐05.В Print.В Mohney,В B.В "CommonВ FormsВ ofВ ChildhoodВ StrabismusВ inВ anВ IncidenceВ Cohort."В AmericanВ JournalВ ofВ Ophthalmology 144.3В (2007):В 465‐67.В Print.В Mohney,В BrianВ G.,В Chrystia C.В Lilley,В AmyВ E.В Green‐Simms,В andВ NancyВ N.В Diehl.В "TheВ Long‐termВ Follow‐upВ ofВ AccommodativeВ EsotropiaВ inВ aВ Population‐ basedВ CohortВ ofВ Children."В Ophthalmology 118.3В (2011):В 581‐85.В Print.В Olitsky,В ScottВ E.,В andВ LeonardВ B.В Nelson.В "StrabismusВ Disorders."В PediatricВ ClinicalВ Ophthalmology:В AВ ColorВ Handbook.В London:В Manson,В 2012.В 51‐57.В Print.В Pollard,В ZaneВ F.,В MD.В "AccommodativeВ EsotropiaВ DuringВ theВ FirstВ YearВ ofВ Life."В ArchivesВ ofВ Ophthalmology 94В (1976):В 1912‐913.В Print.В Sachdeva,В Virender,В MS.В "SurgicalВ ManagementВ ofВ BilateralВ Esotropic DuaneВ Syndrome."В JournalВ ofВ AmericanВ AcademyВ ofВ PediatricsВ OphthalmologyВ andВ Strabismus 16.5В (2012):В 445‐48.В Print.В Terzis,В JuliaВ K.,В andВ Katerina Anesti.В "DevelopmentalВ FacialВ Paralysis:В AВ Review."В JournalВ ofВ Plastic,В ReconstructiveВ &В AestheticВ Surgery 64.10В (2011):В 1318‐333.В Print.В В CaseВ Report:В AC • 91В y.o.В HispanicВ male • CC:В SevereВ eyeВ painВ andВ suddenВ visionВ lossВ OS OcularВ IschemicВ Syndrome LavenderВ Orr,В O.D. VACCHCSВ OptometryВ Resident JuneВ 23,2013 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 – BeganВ twoВ daysВ agoВ withoutВ relief – SeenВ byВ outsideВ generalВ ophthalmologist • ElevatedВ IOPВ 60‐70mmHgВ OS • Avastin intraocularВ injection • PrescribedВ topicalВ anti‐hypertensives &В oralВ Diamox • PertinentВ medicalВ Hx – – – – – CongestiveВ heartВ failure COPD TransientВ ischemicВ attack Hypertension Obesity 32 6/11/2013 ExamВ Findings • NormalВ FindingsВ OD • BCVA: – OS:В HM • Pupils: – OS:В mydriatic pupil • Confrontations: – OS:В ConstrictedВ 360 • Biomicroscopy OS – 2‐3+В diffuseВ microcystic edema – FormedВ AC – DefiniteВ 360В irisВ rubeosis • Tonometry: – 16/59mmHgВ @11:11am – OralВ acetazolamide administeredВ w/topicalВ antihypertensives &В Muro 128В ung – ‐‐/52mmHgВ @В 12:23pm – AdditionalВ doseВ ofВ aforementionedВ therapy A&P • Plan: • Assessment: – Neovascular glaucomaВ OS • AcuteВ ocularВ hypertensiveВ crisis – MostВ likelyВ etiologies • OIS • CRAO • oldВ CRVO • Fundus view: – AttenuatedВ arteriesВ OS – NoВ dilated/tortuousВ veins – NoВ obviousВ intraretinal hemorrhaging Neovascular glaucoma • WhatВ isВ NVG? – Chronic,В progressiveВ ocularВ ischemia – RadicalВ IOPВ increase – SevereВ visionВ loss • CommonВ causes: – DM – CRVO – OIS UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 – AcetazolamideВ 250mgВ POВ QID – AntiВ hypertensives w/atropineВ BID – OrderВ carotidВ ultrasound – LabВ testing:В ESR,В CRP,В CBC,В Chem 7 – RTCВ 1В week CRAO • Source: – RetinalВ emboli • Symptoms: – Sudden,В painlessВ lossВ ofВ vision • Signs: – (+)В APD – AttenuatedВ arteries – CherryВ redВ spotВ inВ acuteВ phase – Emboli 33 6/11/2013 IschemicВ CRVO • Source: OcularВ ischemicВ syndrome • Source – ThrombusВ formation – CarotidВ arteryВ occlusion • Symptoms: • Symptoms – Sudden,В painlessВ lossВ ofВ vision – EyeВ painВ &В decreasedВ acuity • Signs • Signs – (+)В APD – WidespreadВ hemorrhaging – Dilated/tortuousВ retinalВ veins – MidВ peripheralВ intraretinal hemorrhages – DilatedВ retinalВ veinsВ withoutВ tortuosity InВ officeВ followВ upВ #1 • GoodВ compliance,В noВ pain • LabВ Testing: – Normal,В mildlyВ elevatedВ ESR • Tonometry: – ‐‐/40mmHg • CarotidВ Ultrasound • SameВ dayВ PRPВ w/В retinalВ specialist • VascularВ consultation – – – – BenefitsВ ofВ CEA MRA 325В mgВ aspirinВ daily Statin medication – GreaterВ thanВ 70%В stenosis toВ nearВ occlusionВ bilaterally UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 OcularВ ischemicВ syndrome • RareВ &В severeВ formВ ofВ ocularВ ischemia – 7.5/1,000,000 • CommonВ symptoms – OcularВ pain – Amaurosis fugax – TIAВ symptoms 34 6/11/2013 DemographicsВ &В Etiology • CommonlyВ seenВ in • Hemodynamically patientsВ overВ theВ ageВ ofВ significantВ ipsilateral 65 internalВ carotidВ arteryВ occlusion • MenВ 2xВ moreВ than – Rare:В occlusionВ ofВ women ophthalmicВ arteryВ or • OtherВ chronicВ illnesses occlusionВ alongВ aortic • 5В yearВ mortalityВ rateВ ofВ arch 40% – GreaterВ thanВ 90% DiagnosisВ &В Treatment • Ophthalmodynamometry – DecreasedВ centralВ retinalВ arteryВ perfusion • FluoresceinВ angiography – DelayedВ &В patchyВ choroidal filling • CarotidВ ultrasound – BenefitВ ofВ MRA – HighВ gradeВ stenosisВ ofВ 70‐ 99% – 92/1,415В =В 6.5% – 2.0% ‐ disablingВ strokeВ orВ death – GoldВ standardВ treatment – SuccessfulВ forВ preventingВ progressionВ ofВ chronicВ ocularВ ischemia – Risky! – ObstructionВ <99% • EarlyВ diagnosisВ isВ critical! Crest:В CEAВ vs CAS NASCET • TheВ NorthВ AmericanВ SymptomaticВ CarotidВ Endarterectomy Trial • CarotidВ Endarterectomy (CEA) • TheВ CarotidВ Resvascularization Endarterectomy vs StentingВ Trial • Overall,В noВ significantВ differenceВ atВ fourВ years – >70В years:В CEA – <70В years:В CAS – Stroke • 2.3%В vs 4.1% – MyocardialВ infarction • 2.3В vs 1.1% – Death • 0.3%В vs 0.7% UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 35 6/11/2013 BEWARE!! • IncreasedВ riskВ ofВ CRAO • ImmediateВ andВ rapidВ changesВ oftenВ affectsВ ocularВ structures – RelativeВ hypotony – RapidВ increaseВ inВ IOP – Pain!! FightingВ ischemia • BestВ toВ manageВ with: • PRP – Anti‐hypertensives thatВ decreaseВ aqueousВ production – TopicalВ cycloplegic – ConstantВ solution • AntiВ VegF – TemporaryВ solution – GoodВ inВ casesВ ofВ mediaВ opacity • PRPВ +В antiВ VegF – IncreasedВ successВ rateВ forВ glaucomaВ surgeryВ References ClinicalВ pearls • • EarlyВ &В promptВ diagnosisВ isВ keyВ toВ preventВ fatalВ effects • WorkВ closelyВ withВ PCP &В otherВ specialists • PatientВ education • • • • • • • • • • • • • • • • • • UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Back,В MartinВ etВ al.В MagneticВ resonanceВ angiographyВ isВ anВ accurateВ imagingВ adjunctВ toВ duplexВ ultrasoundВ scanВ inВ patientВ selectionВ for carotidВ endarterectomy.В JournalВ ofВ VascularВ Surgery 2000;32(3):429‐440.В Barnett,В H.J.M.В etВ al.В NorthВ AmericanВ SymptomaticВ CarotidВ Endarterectomy TrialВ (NASCET).В Stroke:В AВ JournalВ ofВ CerebralВ Circulation 1998;29(6)1270. Brown,В GaryВ CВ etВ al.В TheВ ocularВ ischemicВ syndrome.В CurrentВ OpinionВ inВ OphthalmologyВ 1994;5(3):14‐20. Ciftci,В Suleyman etВ al.В Intravitreal bevacizumab combinedВ withВ panretinal photocoagulationВ inВ theВ treatmentВ ofВ openВ angleВ neovascular glaucoma.В EuropeanВ JournalВ ofВ Ophthalmology 2009;19(6)1028‐1033. Eid,В TE,В etВ al.В TubeВ shuntВ surgeryВ versusneodymium:В YAGВ photocoagulationВ inВ theВ mangement ofВ neovascular glaucoma.В Opthalmology 1997;104(10):1692‐1700. Ferguson,В GaryВ GВ etВ al.В TheВ NorthВ AmericanВ SymptomaticВ CarotidВ Endarterectomy Trial:В SurgicalВ ResultsВ inВ 1415В Patients.В Stroke:В AВ JournalВ ofВ CerebralВ Circulation 1999;30(9)1751‐1758. Gross,В Ronald.В Neovascular glaucomaВ andВ ocularВ ischemicВ syndrome.В JournalВ ofВ Glaucoma 2000;В 9:409‐412.В Haymore,В JonathanВ GВ etВ al.В RetinalВ vascularВ occlusionВ syndromes.В InternationalВ OphthalmologyВ Clinics 2009;49(3):63‐79.В Hazin,В Ribhi etВ al.В OcularВ ischemicВ syndrome:В recentВ trendsВ inВ medicalВ management.В CurrentВ OpinionВ inВ Ophthalmology 2009;20:430‐433.В Kawaguchi,В Shoichiro etВ al.В EffectВ ofВ carotidВ endarterectomy onВ chronicВ ocularВ ischemicВ syndromeВ dueВ toВ internalВ carotidВ arteryВ stenosis.В Neurosurgery 2001;48(2)В 328‐333.В London,В NikolasВ etВ al.В UpdateВ andВ reviewВ ofВ centralВ retinalВ veinВ occlusion.В CurrentВ OpinionВ inВ Ophthalmology 2011;22:159‐165.В Malhotra,В RamanВ etВ al.В ManagementВ ofВ ocularВ ischaemic syndrome.В BritishВ JournalВ ofВ Ophthalmology 2000;84:1428‐1431.В Mantese,В VitoВ A.В MD,В etВ al.В TheВ CarotidВ RevascularizationВ Endarterectomy versusВ StentingВ TrialВ (CREST).В Stroke 2010;41:S31‐34. Olmos,В LisaВ CВ etВ al.В MedicalВ andВ surgicalВ treatmentВ ofВ neovascular glaucoma.В Int OphthalmologyВ Clin 2011;51(3):27‐36.В Raghavan,В Prashant etВ al.В MagneticВ resonanceВ angiographyВ ofВ theВ extracranial carotidВ system.В TopicsВ inВ MagneticВ ResonanceВ Imaging 2008;19(5):241‐ 249.В Saito,В YoshiakiВ etВ al.В BeneficialВ effectsВ ofВ preoperativeВ intravitreal bevacizumab onВ trabeculectomy outcomesВ inВ neovascular glaucoma.В Acta Ophthalmologica 2010;88(1):96‐102. Wakabayashi,В Taku etВ al.В Intravitreal bevacizumab toВ treatВ irisВ neovascularizationВ andВ neovascular glaucomaВ secondaryВ toВ ischemicВ retinalВ diseasesВ inВ 41В consecutiveВ cases.В Ophthalmology 2008;115:1571‐1580.В Winterkorn,В JacquelineВ M.S.В etВ al.В RecoveryВ fromВ ocularВ ischemicВ syndromeВ afterВ treatmentВ withВ verapamil.В JournalВ ofВ Neuro‐Ophthalmology 1995;15(4):209‐211.В Wolintz,В RobynВ J.В CarotidВ endarterectomy forВ ophthalmicВ manifestations:В IsВ itВ everВ indicated?В JournalВ ofВ Neuro‐OphthalmologyВ 2005;25(4):299‐302.В Olmos,В LisaВ CВ MD,В etВ al.В MedicalВ andВ SurgicalВ TreatmentВ ofВ Neovascular glaucoma.В Internation OphthalmologyВ ClinicsВ 2011;51(3):27‐36. 36 6/11/2013 INTRODUCTION • VITREOUS HEMORRHAGE Incidence: 7 cases per 100,000 • Presenting symptoms: floaters, cloudy vision, shadows, cobwebs • Diagnosis: observation • Complete examination: DEVELOPMENT, DIFFERENTIAL DIAGNOSIS, AND MANAGEMENT RECOMMENDATIONS • anterior vitreous at the slit lamp • Indirect ophthalmoscopy with depression scleral • B-scan Marta Banh O.D. • DFE of the contralateral eye San Francisco VAMC Resident • IOP* June 23, 2013 • Gonioscopy* • Management: dictated by underlying etiology POSTERIOR VITREOUS DETACHMENT IN HEALTHY ADULTS LIQUEFACTION OF HUMAN VITREOUS Volume of Gel and Liquid Vitreous Vitreous Syneresis and PVD Posterior Vitreous Detachment (PVD) is the process by which cortical vitreous gel splits away from the internal limiting membrane (ILM) of the retina. • Epidemiology • 53% in those older than age 50 • 65% in those over age 65 • 72-100% in aphakic eyes • May occur up to 10 years early in myopic patients • Higher incidence in women than men Volume of gel vitreous remains stable until about age 40, then it begins to decrease simultaneously with the increase in liquid vitreous. • Subsequent PVD of the fellow eye w/in 2 years of the first eye 65-88%. Balazs EA, Denlinger JL: Aging changes in the vitreous. In: Aging and Human Visual Function, pp 45–57. New York, Alan R. Liss, 1982. UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 37 6/11/2013 POSTERIOR VITREOUS DETACHMENT IN HEALTHY ADULTS PVD development is NOT acute, but rather a slow asymptomatic process until completion. 5 Stages leading from incomplete to complete PVDs: COMMON CAUSES OF VITREOUS HEMORRHAGE 1. Abnormal Vessels Diabetic retinopathy (31–54%) Neovascularization from branch/central retinal vein occlusion (4–16%) Sickle cell retinopathy (0.2–6%) • Stage 0: no PVD, posterior vitreous face firmly attached to the retina. Retinal arteriole macroaneurysm (0.6-7%) • Stage 1: focal perifoveal PVD: incomplete PVD localized in the perifovea, occurring in 1-3 quadrants Retinal tear (11–44%) • Stage 2: incomplete, perifoveal PVD across all quadrants. Posterior vitreous detachment without retinal tear (4–12%) • Stage 3: detached posterior vitreous face from the retina • Stage 4: complete PVD, detached posterior vitreous face with Weiss ring 2. Rupture of Normal Vessels Trauma (12–19%) Retinal detachment (7–10%) Terson’s syndrome (0.5–1%) • • Retinal ischemia leads to VEGF release and induces neovascularization on the anterior retinal surface between the posterior vitreous cortex and ILM. • Normal vitreous traction with eye movement can lead to tractional forces and rupture of these vessels . • Accelerated vitreous liquefaction and syneresis is more common in diabetic eyes even without retinopathy. The vitreous cortex is integrally involved in neovascularization by acting as a surface that is necessary for the cellular proliferation, migration, and organization of neovascularization to occur. Retinal Tear 30% Vein occlusion 11% Proliferative DR 32% Age-related macular degeneration (0.6–4%) Spraul CW, Grossniklaus HE. Major Review: Vitreous Hemorrhage. Surg Ophthalmol 42:3-39, 1997. MECHANISM OF VITREOUS HEMORRHAGE MECHANISM OF VITREOUS HEMORRHAGE Vessels or Abnormal New Blood Vessels Other 13% PVD w/o tear 8% 3. Blood From Adjacent Source Initial Stages of Posterior Vitreous Detachment in Healthy Eyes of Older Persons Evaluated by Optical Coherence Tomography Arch Ophthalmol. 2001;119(10):1475-1479. 1. Bleeding From Diseased Retinal PSR 2% MA 2% AMD 2% Bleeding From Diseased Retinal Vessels or Abnormal New Blood Vessels • Neovascularization may also affect the vitreous. - PVD occur adjacent to neovascularization - region of superotemporal vessels, temporal to the macula, and adjacent to the optic disc. • After partial PVD, blood may layer out - boat shaped hemorrhage Faulborn J, Bowald S: Microproliferations in proliferative diabetic retinopathy and their relation to the vitreous: Corresponding light and electron microscopic studies. Graefes Arch Clin Exp Ophthalmol 223:130, 1985 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 38 6/11/2013 MECHANISM OF VITREOUS HEMORRHAGE 2. Rupture of Normal Retinal Blood Vessels • During a PVD, vitreous traction on the retinal vasculature may compromise a blood vessel especially at firm vitreo-retinal attachments: • Vitreous Base > Posterior Lens > ONH > Macula > Retinal Vessels RESULTS • • Vitreous hemorrhage from a broken retinal blood vessel, with or without a retinal tear, occurs in 6-41% of patients with acute symptomatic PVD. • 24/36 eyes (67%) had at least 1 retinal break • 11/36 eyes (31%) had more than 1 retinal break • 88% of breaks located in the superior retina • 14/39 eyes (39%) had RRD repaired vitrectomy & scleral buckling • Additional 14/39 (39%) had vitrectomy for non-clearing hemorrhage • Vitreous hemorrhages in the setting of an acute symptomatic PVD should alert the doctor that the risk of a retinal breaks is 7095%. • Incidence of RD in eyes w/ a h/o of RD in contralateral eye was 75% CONCLUSION • 1-4 breaks; mean breaks 1.7 Acute, spontaneous, non-traumatic PVD with dense fundus-obscuring vitreous hemorrhage is associated with high incidence of retinal tears and detachments, which require prompt surgical intervention. MECHANISM OF VITREOUS HEMORRHAGE 3. Extension of Hemorrhage Through The Retina From Other Sources • All patients were examined at 6 weeks • Additional risk factors:patients with retinal or vitreal hemorrhage, or pigment in the anterior vitreous (tobacco dust/shaffer’s sign) on the initial exam were re-examined 2 weeks after initial presentation. UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 • Extensive Subretinal hemorrhage precedes the appearance of vitreal blood. • Age-related Macular Degeneration and Choroidal Melanoma are the two most common underlying diseases. • Vitreous hemorrhage in Idiopathic Polypoidal Choroidal Vasculopathy (IPCV) has also been reported. • Ultrasonography shows a highly echogenic subretinal mass without any choroidal shadowing. If the hemorrhage becomes massive, a total hemorrhagic RD should be suspected. 39 6/11/2013 RARE COMPLICATIONS 1. Hemosiderosis Bulbi and Photoreceptor Toxicity • caused by iron toxicity as hemoglobin is broken down 2. Proliferative Vitreo-Retinopathy • 336 eyes with acute spontaneous PVD • 118 (35%) eyes had vitreous hemorrhage • • • • macrophages and chemotactic factors induce fibrovascular proliferation • cell-mediated contraction of these membranes causes tangential retinal traction, fixed retinal folds and subsequent retinal detachment 3. Ghost Cell Glaucoma 43% taking aspirin, clopidogrel, or warfarin 31% not taking these medications Retinal tears occurred in 46% w/ vitreous hemorrhages versus 27% of patients w/o vitreous hemorrhages. • red blood cells degenerate into smaller, khaki-colored, spherical, more-rigid cells and remain for months following the initial hemorrhage. • the ghost cells enter the anterior chamber after disruption of the anterior hyaloid surface: after accidental trauma, cataract extraction, or vitrectomy 4. Hemolytic Glaucoma CONCLUSION: patients taking aspirin, clopidogrel, or warfarin who develop an acute PVD are more likely to present with vitreous hemorrhage. No statistically significant association was found between the use of oral anticoagulants in patients with acute PVD and vitreous hemorrhage and the presence of retinal tears/detachments. MANAGEMENT AND TREATMENT • Free hemoglobin, hemoglobin-laden macrophages and red-blood cell debris can block the trabecular meshwork. • Clinically indistinguishable from ghost cell glaucoma MANAGEMENT AND TREATMENT 1. Establish the etiology and source of the vitreous hemorrhage 1. Observation • Unknown etiology and attached retina on scleral depressed exam and on ultrasonography • Rest with head elevated 30-45 degree angle • Re-evaluate after 3-7 days Observation Referral Referral Timing Acute PVD w/ small VH and w/o retinal tear on scleral depression Acute PVD w/ VH and identified retinal tear Urgent Acute PVD w/ VH and w/o retinal tear on ultrasonography Acute PVD w/ dense fundus obscuring VH Urgent VH secondary to PDR, CRVO/BRVO Non-urgent 2. Referral to retinal specialist VH secondary to RD, open globe injury, AMD, and IPCV UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Urgent 40 6/11/2013 MANAGEMENT AND TREATMENT Timing of Vitrectomy REFERENCES • Balazs EA, Denlinger JL: Aging changes in the vitreous. In: Aging and Human Visual Function, pp 45–57. New York, Alan R. Liss, 1982. • ETDRS report number 7. Ophthalmology 1991;98(5 Suppl):741–756. • Foos RY. Posterior vitreous detachment. Trans Am Acad Ophthalmol Otolaryngol. 1972;76:480-497. Gloor BP. The vitreous. In: Moses RA, Hart MH, editors. Adler's physiology of the eye: clinical applications. St Louis: CV Mosby, 1987:246–67. Retinal Detachment Urgent • Iris or Angle Neovascularization Urgent • Le Goff MM, Bishop PN. Adult vitreous structure and postnasal changes. Eye 2008; 22: 1214-1222 • Sarrafizadeh R, et al. Incidence of retinal detachment and visual outcome in eyes presenting with posterior vitreous separation and dense fundus-obscuring vitreous hemorrhage. Ophthalmology 2001; 108:2273-2278. Type 1 Diabetes One month • Schweitzer KD, et al. Predicting retinal tears in posterior vitreous detachment. Can J Ophthalmol 2011; 46:481-485. • Sebag J, Balazx EA: Morphology and ultrastructure of human vitreous fibers. Invest Ophthalmol Vis Sci 1989;30:1871 • Sebag J. Surgical anatomy of vitreous and the vitreoretinal interface. Duane’s Clinical Ophthalmology. 2006; Vol 6, Ch 51. • Sebag J. Vitreous Pathobiology. Duane’s Clinical Ophthalmology. 2006; Vol 3, Ch 39. • Spraul CW, Grossniklaus HE. Major Review: Vitreous hemorrhage. Surg Ophthalmol 1997 42:3-39. • Ruby AJ, Williams GA, Blumenkranz MS. Vitreous humor. Duane’s Clinical Ophthalmology. 2006; Ch 11. • Uchino E, Uemura A, Ohba N. Initial stages of posterior vitreous detachment in healthy eyes of older persons evaluated by optical coherence tomography. Arch Ophthalmol. 2001; 119:1475-1479 • Witmer MT, Cohen SM. Oral anticoagulation and the risk of vitreous hemorrhage and retinal tears in eyes with acute posterior vitreous detachment. J of Retina and Vitreous Diseases.2013; 33:621-626. Subhyaloid vitreous hemorrhage One month Type 2 Diabetes Two or three months Other Causes Three months or more ETDRS report number 7. Ophthalmology 1991;98(5 Suppl):741–756. Case PT 78 year old female EVALВ ATВ THEВ SOCIETYВ FORВ THEВ BLINDВ (SACRAMENTO)В ONВ 1/2/2013 LV 2’ Bilateral Non-Exudative AMD I SPY WITH MY TELESCOPIC EYE: The Implantable Miniature Telescope for Age-Related Macular Degeneration Caitlin E. Walsh, O.D. University of California, Berkeley Edwin B. Mehr Low Vision Resident June 23, 2013 CC: Implantable Miniature Telescope Evaluation Visual difficulties: Reading books and newspaper, writing POHx: (-) H/o co-existing ocular disease, (-) H/o eye surgery TF refraction OD +1.00 -2.00 x090 OS +0.75 -1.00 x090 20/250-1 20/160+1 Contrast Sensitivity (Pelli-Robson) 5% Weber (2% Weber is normal) Confrontation Visual Fields (transilluminator) Full OD and OS UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 BCVA Anterior Segment L/Ls Blepharitis OU Cornea Clear OU Iris Flat OU Lens Gr 3+ NS OU TA @ 10:45am 11mmHg, OS 12 mmHg Posterior Segment ONH Macula (C/D): 0.25/0.25 OU GA OD>OS, (-)CNV OU 41 6/11/2013 Age-Related Macular Degeneration Functional difficulties FDA approved July 1, 2010 Consequences Reading Recognizing faces Watching television Driving Self-care Social interaction The Implantable Miniature Telescope Increased risk of accidents More dependent on others Decreased quality of life Legal blindness Depression Indication Monocular implant 75 years or older Severe-profound vision loss End-stage macular degeneration 2.7x Fixed Focus Galilean Telescope Works in conjunction with the cornea Optimal focal distance of 3m Goal = Reduce the impact of the central scotoma IMT used for detailed tasks Un-operated eye used for safe travel Projects an enlarged image of the central field onto the retina Field of View OUT = 20-24 degree Field of View IN = 54 degrees 2.7x 54Вє 20Вє http://www.nei.nih.gov/health/maculardegen/armd_facts.asp www.centrasight.com The Implantable Miniature Telescope Visual effects 3.6mm (diameter) x 4.4mm (length), 13.5mm wide including haptics Biocompatible materials Implanted into the posterior chamber following phacoemulsification Protrudes 0.5 mm from the pupillary plane Prohibits binocular vision Modifications from standard phaco with foldable IOL implantation Retrobulbar block 12 mm limbal incision, 7 mm capsulorhexis Prophylactic peripheral iridectomy, 10 nylon sutures Colby et al. 2007. 13.5В mmВ www.centrasight.com Restricts peripheral vision Constricted to diameter of 20 degrees Reduced retinal illuminance Cost = 15,500 (covered by Medicare) 4.4В mm Visual confusion, diplopia or suppression Loss of depth perception Reduced contrast sensitivity 0.5В mm 4.4 mm = 13 IOLS! UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 http://www.ocutech.com/bioptic-driving.aspx 42 6/11/2013 Centrasight TM Treatment Program CentrasightTM Treatment Program A treatment program for End-Stage AMD RetinalВ Specialist Diagnosis, surgical evaluation, pre and postoperative care Utilizes the Implantable Miniature Telescope Created by Isaac Lipshitz, M.D. Manufactured by VisionCare Ophthalmic Technologies (Saratoga, Ca) Requires a multidisciplinary approach Retinal specialist Corneal and Cataract specialist Low Vision Optometrist Occupational Therapist OccupationalВ Therapist Demonstrates the External Telescope Simulator (ETS) Determines the patients preferred retinal locus Determines the eye to receive the prosthetic device Facilitates patching exercises prior to treatment Provides post-operative vision care VISUAL CRITERIA Severe to profound vision loss BCVA (20/160 – 20/800) Improvement in Vision with ETS Determines good surgical candidates Performs the surgery and post-op care DISEASE CRITERIA Geographic Atrophy or Disciform Scar Bilateral foveal involvement Provides eccentric viewing training ANATOMICAL CRITERIA Stable for at least 6 months No active CNV or Tx for CNV Baseline Endothelial Density 75-84 years old 2000 cells/mm2 85+ years old 1800 cells/mm2 Visually Significant Cataract > or = Grade 2 Anterior chamber depth > or = 3.0mm No co-existing ocular disease No anterior segment abnormalities No condition that could compromise the patient’s peripheral vision CentrasightTM Treatment Program LowВ VisionВ Optometrist CorneaВ andВ CataractВ Specialist Initiates appropriate referrals Axial length > 21 mm Myopia < 6.0 D, Hyperopia < 4.0 D Phakic Gr 2+ NS, CS, or PSC Case PT 78 year old female EVALВ ATВ THEВ SOCIETYВ FORВ THEВ BLINDВ ONВ 1/2/2013 TF refraction OD +1.00 -2.00 x090 OS +0.75 -1.00 x090 BCVA 20/250-1 20/160+1 ETS 20/100 20/50 Provides post-operative vision rehabilitation FUNCTIONAL CRITERIA Realistic functional goals IMT will not restore the patient’s natural vision DOES NOT eliminate need for glasses and magnifiers Intraocular: 5 letter improvement Must tolerate loss of peripheral vision and with the ETS depth perception Interocular: 10 letter Must commit to working with the low vision improvement with the ETS optometrist and occupational therapist compared to the other eye following surgery without the ETS UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Reading Acuity using ETS over OS with +5.00D near cap Efficiency was 0.20/2.0M (16 pt font) Threshold was 0.20/1.25M (10 pt font Assessment Both eyes meet visual criteria Target OS for IMT prosthesis Plan Wear eye patch over OS 2-3 hrs/day while performing tasks of daily living Referred to the OT at the UC Davis Med Center 43 6/11/2013 Case GK 84 year old male Case GK 84 year old male EVAL AT THE SOCIETY FOR THE BLIND 1/2/2013 EVAL AT THE SOCIETY FOR THE BLIND 1/2/2013 CC: Glare and Diplopia Pre-op Trial Frame Refraction OD +0.75 -0.50x154 OS pl -0.25 x056 Post-op Trial Frame Refraction OD +3.25 -1.50 x060 OS +0.50 -0.50 x045 BCVA 20/400 20/500 ETS 20/100 BCVA 20/125 20/200 Reading acuity with a +5.00 D Add Efficiency Threshold 0.2/2.5M 0.2/1.6M Contrast Sensitivity (Pelli-Robson) OD 36% Weber and OS 6.3% Weber Assessment Good improvement in visual acuity with IMT OD Light sensitivity Reduced suppression of eye with IMT prosthesis Plan Released SV Distance SRx and SV Near SRx Recommended gray Cocoon fit-overs Recommended continued training with the occupational therapist to work on alternating fixation Confrontation Visual Fields Severely constricted <20 degrees 360 OD No restriction OS Conclusions Conclusions GOOD CANDIDATES FOR THE IMT POOR CANDIDATES FOR THE IMT • Meet anatomical and disease criteria • Previous intraocular surgery • Improvement in visual acuity with the external telescope simulator • Anterior segment abnormalities • Realistic goals and expectations • Constricted peripheral vision in un-operated eye • Willing to work with rehabilitation specialists • Prone to eye rubbing • Good chance of useful improvement in everyday activities • Cognitive impairment • Good chance of adjusting to change in vision UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 44 6/11/2013 Conclusions Acknowledgments Careful patient evaluation, education, and selection are essential for a happy patient following surgery! Society for the Blind Richard Van Buskirk, O.D. Nancy Nguyen, O.D. Penny Riley, Clinic Coordinator IMT will not restore natural vision Glasses and magnifiers will still be necessary following surgery UC Berkeley School of Optometry Robert B. Greer, O.D. Marlena Chu, O.D. Ian Bailey, O.D. Cheyenne Huber, O.D. UC Davis Medical Center Time and effort required for post-surgical visual rehabilitation Jennifer Li, M.D. Mark Mannis, M.D. Terri Hayward, O.T. Colby et. al. 2007. Resources • • • • • • • • • • • • Brown, M. et al. Utility values associated with blindness in an adult population. Br J Ophthalmol2001;85:327-331. CATT Research Group, Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ. N Engl J Med. 2011 May 19; 364(20):1897-908. Colby KA et al. Surgical Placement of an optical prosthetic device for end-stage macular degeneration: the implantable miniature telescope. Arch Ophthalmol. 2007;125:1118-1112. Colucciello, M. The Merits and Limitations of the Implantable Miniature Telescope for AMD. Retinal Physician. 2010. http://www.retinalphysician.com/articleviewer.aspx?articleid=104846. Accessed April 28, 2013. FDA approval letter for Implantable Miniature Telescope. Food & Drug Administration Web Site. http://www.accessdata.fda.gov/cdrh_docs/pdf5/P050034a.pdf. Accessed February 18, 2013. Garfinkel, RA, Berinstein, DM, Frantz, BS. Treatment of Choroidal Neovascularization Through the Implantable Miniature Telescope. Am J Ophthalmol. 2006;141: 766-767. Haddrill, M. FDA-Approved Macular Degeneration Treatment. <Http://www.allaboutvision.com/conditions/amd-treatments.htm>. Haller, JA. A New Option for End-Stage AMD. Review of Ophthalmology. 2010. http://www.revophth.com/content/d/retinal_insider/c/25844/ Harvitt, DM. Lecture 1. Vision Science 203B. Spring 2013. Hudson et al. IMT-002 Study Group. Implantable miniature telescope for the treatment of visual acuity lossresulting from end-stage age-related maculard egeneration: 1 year results. Ophthalmology. 2006;113:1987-2001. Hudson et al. Implantable Telescope for End-stage Macular Degeneration: Long term Visual Acuity and Safety Outcomes. J Ophthalmol 2008;146:664–673. Lane. SS, Kuppermann, BD. The implantable miniature telescope for macular degeneration. Curr Opin Ophthalmol. 2006;17(1):94-98. Resources • • • • • • • • UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Lane, SS et al. A prospective multicenter clinical trial to evaluate the safety and effectiveness of the implantable miniature telescope. Am J Ophthalmol. 2004; 137:9931001. Rein, DB, Wittenborn, JS, Zhang, X, Honeycutt, AA, Lesesne, SB, Saaddine, J,. Forecasting Age-Related Macular Degeneration Through the Year 2050: The Potential Impact of New Treatments. Arch Ophthalmol. 2009;127 (4): 533-540. Rosner, M, Ben-Simon, G, Sachs, D. Feasibility and Safety of Laser Treatments in eyes with an Intraocular Implantable Miniature Telescope. J Cataract and Refractive Surgery.2003; 29:1005-1010. Singer, M et al. Pars plana posterior capsulotomy in a patient with a telescope prothesis for age-related macular degeneration. Arch Ophthalmol. 2010;128(8):1065-1067. VisionCare’s Implantable Miniature Telescope: An intraocular telescope for treating severe to profound vision impairment due to bilateral end-stage age-related macular degeneration. Patient Information Booklet. Saratoga: VisionCare Ophthalmic Technologies, Inc, 2010. Print. VisionCare’s Implantable Miniature Telescope: An intraocular telescope for treating severe to profound vision impairment due to bilateral end-stage age-related macular degeneration. Professional Use Information. Saratoga: VisionCare Ophthalmic Technologies, Inc, 2010. Print. Williams, R, Brody, BL, Thomas, RG, Kaplan, RM, Brown, SI. The Psychosocial Impact of Macular Degeneration. Arch Ophthalmol. 1998;116:514-520. Ying, GS, Maguire, M. Development of a Risk Score for Geographic Atrophy in Complications of the Age-Related Macular Degeneration Prevention Trial. Ophthalmology 2011;118:332–338. 45 6/11/2013 Keratoglobus PKP after KCN: the thick and thin of it Tarah Lee, OD VA Palo Alto Health Care System Primary Care and Low Vision Rehabilitation Resident Cirrus anterior segment OCT PentacamВ images OD http://www.kerasoftic.com/en/eye‐care‐professional/educational/ OS http://benjamineye.com/sites/benjamineye.com/files/i mages/page/pentacam_hr_overview_display.jpg UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 46 6/11/2013 PKP Procedure Indications for PKP • Anterior Cornea – Keratoconus (KCN) – Corneal Dystrophies – Trauma – chemical burns – Infections – scars – Stevens-Johnson Syndrome (SJS) – Ocular cicatricial pemphigoid (OCP) HongВ KongВ MedВ J.В 2012В Dec;18(6):509‐16. Indications for PKP con’t Indications for PK • Posterior Cornea – Fuchs endothelial dystrophy – Bullous Keratopathy • Aphakic (ABK) • Pseudophakic (PBK) – Posterior polymorphous dystrophy (PPMD) – Corneal regraft http://openi.nlm.nih.gov/detailedresult.php?img=2880372_MEAJO‐17‐38‐g002&req=4 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 47 6/11/2013 PKP in KCN Early complications of PKP Suture problems Macular edema Primary graft failure Elevated IOP Wound leaks Persistent epithelial defects Filamentary keratopathy Choroidal hemorrhage Retinal detachment Hyphema Microbial keratitis Endophthalmitis • Immunological rejection rare • • • • • • • • • • • • Late complications of PKP Lamellar Keratoplasty • 10-20% of patients • Good visual outcomes • • • • • • • Late endothelial failure Unstable refractive endpoint Cataracts Glaucoma Graft rejection Epithelial downgrowth Transmission of infectious diseases UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 HostВ Tissue DonorВ Tissue PLK SuperiorВ scleral pocket Posterior stroma,В DMВ andВ endo DLEK Posterior cornealВ disc Posterior stroma,В DMВ andВ endo DSEK EndotheliumВ andВ Descement’s membraneВ strippedВ PosteriorВ stroma, DMВ andВ endo DSAEK EndotheliumВ andВ Descement’s membraneВ stripped PosteriorВ stroma, DMВ andВ endothelium DMEK Descemet’s membrane andВ endotheliumВ stripped DMВ andВ endothelium DALK DMВ andВ endothelium Epithelium to deepВ stroma 48 6/11/2013 Advantages and disadvantages of DALK vs. PKP DALK Advantages Disadvantages Eliminates riskВ ofВ endothelialВ rejection MoreВ technicallyВ demanding ReducedВ endothelialВ cellВ loss ProlongedВ operativeВ time AnticipatedВ improvedВ graftВ survival AstigmatismВ ratesВ similar toВ PKP LargelyВ extraocular procedure RiskВ ofВ conversionВ toВ PKP GreaterВ woundВ strength DoubleВ A/C,В interface haze LessВ dependenceВ onВ topicalВ steroids RecurrenceВ ofВ stromal cornealВ dystrophies EarlierВ sutureВ removal ContraindicatedВ ifВ stroma tooВ thinВ orВ excessiveВ DMВ striae Similar refractiveВ errorВ andВ BCVA http://www.revoptom.com/continuing_education/tabviewtest/lessonid/107933/ Corneal Collagen Cross-linking (CXL) Intracorneal Ring Segments (ICRS) • May slow progression of • PMMA segments KCN • May include epithelial http://www.shinagawa.com.sg/en/lasik-services/lasik-xtra • Flatten and reshape the debridement • Topical riboflavin • Implanted into stroma 370 um http://www.coastalvisionmedical.com/site/intacs.htm cornea • UV-A exposure at 370 um http://www.oocities.org/wallstreet/2124/KERAweb/CornealChange s.html http://www.revophth.com/content/i/1777/c/32329/ UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 49 6/11/2013 Key Points References • • Penetrating keratoplasty (PKP) has been the mainstay of surgical treatment for corneal blindness • Many potential complications, though most are rare • Allograft rejection and late endothelial failure are the most common causes of graft failure • Regrafts are 3x as likely to fail as primary grafts • Increase in lamellar corneal transplants due to improved surgical techniques • Alternative treatments such as intracorneal ring segments and corneal collagen cross-linking are available • • • • • • • • • • • • • • • • Young AL, Kam KW, Jhanji V, Cheng LL, Rao SK. A new era in corneal transplantation: paradigm shift and evolution of techniques. Hong Kong Med J. 2012 Dec;18(6):509-16. Wang J, Hasenfus A, Schirra F, Bohle RM, Seitz B, SzentmГЎry N. Changing indications for penetrating keratoplasty in Homburg/Saar from 2001 to 2010--histopathology of 1,200 corneal buttons. Graefes Arch Clin Exp Ophthalmol. 2013 Mar;251(3):797-802. Stechschulte SU, Azar DT. Complications after penetrating keratoplasty. Int Ophthalmol Clin. 2000 Winter;40(1):27-43. Chan E, Snibson GR. Current status of corneal collagen cross-linking for keratoconus: a review. Clin Exp Optom. 2013 Mar;96(2):155-64 Jhanji V, Sharma N, Vajpayee RB. Management of keratoconus: current scenario. Br J Ophthalmol. 2011 Aug;95(8):104450. Cassidy D, Beltz J, Jhanji V, Loughnan MS. Recent advances in corneal transplantation for keratoconus. Clin Exp Optom. 2013 Mar;96(2):165-72. Reinhart WJ, Musch DC, Jacobs DS, Lee WB, Kaufman SC, Shtein RM. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty a report by the american academy of ophthalmology. Ophthalmology. 2011 Jan;118(1):209-18. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998 Jan-Feb;42(4):297-319 Romero-JimГ©nez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: a review. Cont Lens Anterior Eye. 2010 Aug;33(4):157-66;. Tan DT, Dart JK, Holland EJ, Kinoshita S. Corneal transplantation. Lancet. 2012 May 5;379(9827):1749-61. Borderie VM, Sandali O, Bullet J, Gaujoux T, Touzeau O, Laroche L. Long-term results of deep anterior lamellar versus penetrating keratoplasty. Ophthalmology. 2012 Feb;119(2):249-55. Fares U, Sarhan AR, Dua HS. Management of post-keratoplasty astigmatism. J Cataract Refract Surg. 2012 Nov;38(11):2029-39. Tan DT, Por YM. Current treatment options for corneal ectasia. Curr Opin Ophthalmol. 2007 Jul;18(4):284-9. Claesson M, Armitage WJ. Clinical Outcome of Repeat Penetrating Keratoplasty. Cornea. 2013 Apr 12. Collagen-Crosslinking: asking the tough questions. Retrieved June 1, 2013. http://www.revophth.com/content/i/1777/c/32329/ CXL USA online. Retrieved June 1, 2013. http://www.cxlusa.com/default.aspx Ertan A, Muftuoglu O. Intracorneal ring segments for keratoconus. Expert Rev Ophthalmol. 2008;3(5):585-591. ChiefВ Complaint:В 81В year‐oldВ maleВ withВ painfulВ redВ eyeВ OS Scleritis:В AВ RoyalВ PainВ inВ theВ Eye JenniferВ M.В Tu,В OD SanВ FranciscoВ VAВ MedicalВ Center PrimaryВ Care ExamВ Findings Right Eye VA cc 20/40 20/40 Lids/Lashes Collarettes 2+ Collarettes 2+,В mucousВ 2+В LL Conjunctiva/Sclera Clear InjectionВ 4+,В smallВ elevatedВ noduleВ @sup‐tempВ underВ lid Cornea TraceВ KP TraceВ KP AntВ Chamber DeepВ andВ quiet DeepВ andВ quiet 16В mm Hg IOP 16В mm Hg Lens NSВ 2+ NSВ 2+ Vitreous Syneresis Syneresis OpticВ Nerve:В JuneВ 23,В 2013 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 LeftВ Eye Macula: Periphery: OD:В 0.30 OS:В 0.35 A:В NodularВ anteriorВ scleritis OS ScatteredВ smallВ drusen 1+В OU,В noВ CNV P:В BeginВ ibuprofenВ 400В mgВ QID. NoВ holes/tears/breaksВ OU B‐scan: NegativeВ T‐sign OrderВ labВ testsВ (CBC,В ESR,В PPD,В RPR,В TP‐PA,В ANA,В ACE,В ANCA,В RF)В В 50 6/11/2013 Anatomy DifferentialВ Diagnosis • Conjunctivitis • AcuteВ angleВ closure – DiffuseВ redness – TearyВ eyes,В mucousВ discharge – PapillaryВ vs follicularВ reaction – ElevatedВ IOPВ withВ acuteВ eyeВ pain – Mid‐dilatedВ pupil – CornealВ edemaВ пѓ hazyВ vision Episcleritis • AnteriorВ uveitis* – – – – PainВ withВ photophobia Circumlimbal flush Keratic precipitates AnteriorВ chamberВ reaction Younger Older Onset Acute Insidious VA Unaffected ReducedВ VA Blood Vessels Sectoral superficial injectionВ (brightВ red) Superficial andВ deepВ vesselВ injectionВ (violaceous hue) Vessels blanchВ withВ phenylephrine DeepВ vessels doВ notВ blanchВ withВ phenylephrine No pain Severe,В deep, boring Pain BloodВ Supply • • DerivedВ fromВ theВ anteriorВ ciliary arteriesВ whichВ anastamose withВ theВ posteriorВ ciliary arteries TheВ scleraВ itselfВ isВ anВ avascularВ structure 1. Conjunctival Plexus • MobileВ withВ aВ cottonВ tip 2. SuperficialВ Episcleral Plexus ComposedВ ofВ collagen,В fibroblasts,В andВ GAGs Extraocular musclesВ insertВ intoВ theВ sclera InnervationВ byВ longВ andВ shortВ ciliary nerves BloodВ supplyВ derivedВ fromВ theВ anteriorВ ciliary arteries Scleritis Age *MayВ presentВ withВ scleritis • • • • Conjunctiva Sclera Tenon’s space Episclera PathophysiologyВ ofВ Scleritis • HistologyВ studiesВ showВ granulomatousВ lesionВ consistingВ ofВ plasmaВ cells,В lymphocytes,В andВ mastВ cellsВ clinicallyВ manifestingВ asВ scleralВ inflammation ActiveВ T‐cellВ inflammatoryВ responseВ В incitedВ byВ traumaВ orВ infection EndothelialВ swellingВ ofВ vesselsВ andВ microvascular occlusion SCLERALВ INFLAMMATION • RadialВ orientationВ ofВ vessels 3. DeepВ Episcleral Plexus • DoВ notВ blanchВ withВ phenylephrine UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 CollagenВ fibrilsВ unravelВ dueВ toВ alterationВ ofВ proteoglycans NeutrophilВ infiltrationВ ofВ vesselВ wall 51 6/11/2013 ClinicalВ ExaminationВ Checklist History ExternalВ Exam Pain OnsetВ (acuteВ vs insidious) EvaluateВ inВ naturalВ lighting Violaceous vs brightВ redВ hue Slit LampВ Exam Red freeВ filter CornealВ complications ‐ Marginal orВ interstitial keratitis Anterior chamberВ cellВ Posterior Segment Exudative retinalВ detachment B scanВ forВ fluidВ underВ Tenon’s capsuleВ (T‐sign) ClassificationВ Types Diffuse Nodular Scleromalacia Perforans (NecrotizingВ withoutВ inflammation) NecrotizingВ withВ inflammation Anterior Posterior Scleritis Note:В useВ anВ opticВ sectionВ toВ determineВ extentВ ofВ edemaВ andВ whichВ layersВ areВ involved Diffuse AnteriorВ Scleritis • SeenВ inВ 60%В ofВ cases • RearrangementВ ofВ collagenВ scleralВ fibers – resultingВ inВ blueВ hue • SystemicВ associationВ inВ 45%В ofВ cases – RheumatoidВ arthritisВ mostВ common • CornealВ findings – PeripheralВ infiltrates – CornealВ thinning UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 NodularВ AnteriorВ Scleritis • SeenВ inВ 20%В ofВ cases • MayВ haveВ multipleВ nodulesВ present • SystemicВ associationВ inВ 40 – 50%В ofВ cases – CommonlyВ infectiousВ origin • UnderlyingВ scleraВ mayВ beВ transparentВ howeverВ noВ necrosis Firm,В immobile,В tenderВ nodule typicallyВ foundВ closeВ toВ limbus 52 6/11/2013 Scleromalacia perforans NecrotizingВ withВ inflammation PosteriorВ Scleritis (NecrotizingВ withoutВ inflammation) • • • • LackВ ofВ symptoms SevereВ atrophyВ ofВ theВ episclera Yellow‐whiteВ infarctedВ tissue AssociatedВ withВ longstandingВ RA • WhiteВ scleraВ dueВ toВ capillaryВ dropout • InfarctionВ andВ necrosisВ ofВ underlyingВ sclera • ScleralВ edemaВ extendingВ outwardВ aroundВ theВ globeВ (picturedВ below) • InflammationВ occursВ posteriorВ toВ medialВ andВ lateralВ rectusВ muscleВ insertions • LessВ commonlyВ associatedВ withВ systemicВ disorders • OcularВ complications • Uveitis • RetinalВ detachment • Proptosis andВ diplopia • Subretinal mass • Choroidal effusion OcularВ ComplicationsВ definedВ asВ theВ following: • InterstitialВ keratitis • Cataract • MarginalВ cornealВ ulcer • Vitritis • AnteriorВ uveitis • CystoidВ macularВ edema • IOPВ >В 21В mmВ Hg • ExudativeВ retinalВ detachment DecreasedВ Vision 78%В hadВ pre‐existingВ systemicВ В diagnosis OfВ 243В patients 44%В ofВ patientsВ haveВ anВ associatedВ systemicВ condition PosteriorВ SegmentВ Findings 14%В diagnosedВ afterВ initialВ evaluation • None inВ episcleritis group • 16%В inВ scleritis group InfectiousВ (7%) ConversionВ toВ BilateralВ Disease T‐sign =В thickenedВ scleraВ withВ fluidВ inВ Tenon’s space • Episcleritis: • Scleritis:В RheumaticВ (37%) 8%В diagnosedВ duringВ followВ upВ period 12%В atВ 1В year 24%В atВ 1В year • CommonlyВ seenВ inВ posteriorВ scleritis • InfrequentlyВ associatedВ withВ anteriorВ scleritis UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 HerpesВ zosterВ (4.5%) RheumatoidВ arthritisВ (15.2%) Wegener’sВ GranulomatosisВ (+systemicВ vasculitides) SystemicВ lupusВ erythematosus 53 6/11/2013 LaboratoryВ Testing CompleteВ bloodВ countВ (CBC) CompleteВ metabolicВ panelВ (CMP) Antineutrophil cytoplasmicВ antibodyВ (C‐ANCAВ andВ P‐ANCA) AntinuclearВ antibodyВ (ANA) AngiotensinВ convertingВ enzyme FluorescentВ treponemal antibodyВ absorptionВ (FTA‐Abs) RapidВ plasmaВ reagin (RPR) RheumatoidВ factorВ (RF) PurifiedВ proteinВ derivativeВ (PPD) LymeВ antibody Lysozyme ChestВ x‐ray TakeВ HomeВ Points TreatmentВ Options NSAID OralВ corticosteroids ImmunosuppressiveВ drugs InitialВ drugВ ofВ choiceВ forВ non‐ necrotizingВ anteriorВ scleritis InitialВ drugВ ofВ choiceВ forВ necrotizingВ anteriorВ scleritis andВ posteriorВ scleritis OR FailedВ NSAIDВ therapy NecrotizingВ anteriorВ scleritis OR FailedВ corticosteroidВ therapy OR SteroidВ relatedВ adverseВ events References 1. Akpek EK,В ThorneВ JE,В Qazi FA,В DoВ DV,В JabsВ DA.В EvaluationВ ofВ patientsВ withВ scleritis forВ systemicВ disease.В Ophthalmology.В 2004В Mar;111(3):501‐6.В 2. BeardsleyВ RM,В Suhler EB,В RosenbaumВ JT,В LinВ P.В PharmacotherapyВ ofВ scleritis:В currentВ paradigmsВ andВ futureВ directions.В ExpertВ Opin Pharmacother.В 2013В Mar;14(4):411‐24. • BeВ ableВ toВ recognizeВ theВ clinicalВ featuresВ inВ differentiatingВ episcleritis fromВ scleritis 3. CastellsВ DD.В AnteriorВ scleritis:В threeВ caseВ reportsВ andВ aВ reviewВ ofВ theВ literature.В Optometry.В 2004В Jul;75(7):430‐44.В 4. Galor A,В ThorneВ JE.В Scleritis andВ peripheralВ ulcerativeВ keratitis.В RheumВ DisВ Clin NorthВ Am.В 2007В Nov;33(4):835‐54,В vii. 5. Nizam S,В Johnstone A,В GreenВ M,В GoughВ A.В Necrotising scleritis andВ connectiveВ tissueВ disease‐‐threeВ casesВ andВ aВ review.В Clin Rheumatol.В 2009В Mar;28(3):339‐41. • Scleritis isВ aВ severeВ ocularВ inflammatoryВ disorderВ thatВ mayВ haveВ systemicВ diseaseВ implications 6. JabsВ DA,В Mudun A,В DunnВ JP,В MarshВ MJ.В Episcleritis andВ scleritis:В clinicalВ featuresВ andВ treatmentВ results.В AmВ JВ Ophthalmol.В 2000В Oct;130(4):469‐76. 7. Jachens AW,В ChuВ DS.В RetrospectiveВ reviewВ ofВ methotrexateВ therapyВ inВ theВ treatmentВ ofВ chronic,В noninfectious,В nonnecrotizing scleritis.В AmВ JВ Ophthalmol.В 2008В Mar;145(3):487‐492.В 8. Raiji VR,В PalestineВ AG,В Parver DL.В Scleritis andВ systemicВ diseaseВ associationВ inВ aВ community‐basedВ referralВ practice.В AmВ JВ Ophthalmol.В 2009В Dec;148(6):946‐50. • UrgentВ referralВ isВ warrantedВ toВ initiateВ laboratoryВ testingВ andВ possibleВ systemicВ treatmentВ ofВ theВ underlyingВ condition 9. Sainz deВ laВ Maza M,В MolinaВ N,В Gonzalez‐GonzalezВ LA,В DoctorВ PP,В Tauber J,В FosterВ CS.В ClinicalВ characteristicsВ ofВ aВ largeВ cohortВ ofВ patientsВ withВ scleritis andВ episcleritis.В Ophthalmology.В 2012В Jan;119(1):43‐50.В 10. Sainz deВ laВ Maza M,В MolinaВ N,В Gonzalez‐GonzalezВ LA,В DoctorВ PP,В Tauber J,В FosterВ CS.В Scleritis therapy.В Ophthalmology.В 2012В Jan;119(1):51‐8.В 11. WatsonВ PG,В Hayreh SS.В Scleritis andВ episcleritis.В BrВ JВ Ophthalmol.В 1976В Mar;60(3):163‐91. 12. Wieringa WG,В Wieringa JE,В tenВ Dam‐vanВ LoonВ NH,В LosВ LI.В VisualВ outcome,В treatmentВ results,В andВ prognosticВ factorsВ inВ patientsВ withВ scleritis.В Ophthalmology.В 2013В Feb;120(2):379‐86.В doi:В 10.1016/j.ophtha.2012.08.005.В Epub 2012В NovВ 20.В PubMedВ PMID:В 23177360.В UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 54 6/11/2013 NotВ AlwaysВ onВ Target TICKEDВ OFFВ PATIENTS OcularВ ManifestationsВ ofВ LymeВ Disease SeveralВ countries 43В States CaliforniaВ isВ consideredВ anВ endemicВ area http://www.pbase.com/image/51179027 RyanВ Johnson,В OD Resident,В BinocularВ VisionВ Clinic UniversityВ ofВ California,В Berkeley JuneВ 23,В 2013 Pathognomoic SeenВ inВ 50%В ofВ patients AtВ riskВ afterВ 24В hours http://hardinmd.lib.uiowa.edu/cdc/lymedisease6.html • BetweenВ 3В &В 30В days • NoВ laterВ thanВ 3В months • Erythema Migrans • Borrelial lymphocytoma • 6В months • MigrantВ muscleВ pain • LargeВ jointВ pain • BoneВ pain 100%В transmissionВ byВ 3В days CDCВ DefinitionВ ofВ LymeВ Disease • ExposureВ inВ anВ endemicВ area • Erythema migrans withinВ 30В days Dermatologic Musculoskeletal AВ MultisystemВ Disorder • • • • ExposureВ inВ anВ endemicВ area Erythema migrans absent SignsВ involvingВ oneВ organВ system PositiveВ laboratoryВ test • WithinВ severalВ weeks • 4‐8%В ofВ patients • Atrioventricular blocks • Carditis • HighlyВ variable • MonthsВ toВ yearsВ after • Bannwarth Syndrome • Encephalomyelitis • CranialВ nerveВ palsies • NoВ historyВ ofВ exposure • Erythema migrans present • InvolvementВ ofВ twoВ organВ systems Cardiac Neurologic • NoВ exposureВ inВ anВ endemicВ area • Erythema migrans present • PositiveВ serology UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 55 6/11/2013 DocumentedВ ManifestationsВ ofВ Lyme RoughВ andВ Ready,В California:В 12yo • • • • • • • • • • • • • Blepharospasm Uveitis Panophthalmitis Chorioiditis Optic Disc Edema Macular Edema Pseudotumor Cerebri Optic Neuritis AION Temporal Arteritis Optic Atrophy Horner’s Syndrome Argyll-Robertson Pupil STAGEВ 3:В Late/Immunologic • Conjunctivitis • Periorbital Edema STAGEВ 2:В Dissemination STAGEВ 1:В Infection • DiagnosedВ withВ activeВ neuro‐lyme diseaseВ 2011 • • • • • • Nerve Palsies Stromal Keratitis Episcleritis Scleritis Orbital Myositis Cortical Blindness – ConfirmedВ withВ ELISAВ andВ WesternВ Blot – PresumedВ contractedВ atВ 6yoВ (2007) • Lyme‐associatedВ arthritisВ inВ bothВ knees • PresentingВ Complaints: – – – – Photophobia Floaters MidlineВ Shift TrackingВ Difficulties MechanismsВ ofВ TBIВ andВ VisualВ ConsequencesВ inВ MilitaryВ andВ VeteranВ Populations OptometryВ &В VisionВ Science FebruaryВ 2013 • 65% ‐ ReportedВ visualВ problems • 50% ‐ ReadingВ problems • LightВ Sensitivity – 67%В ofВ blastВ related – 33%В ofВ non‐blastВ related • ConvergenceВ insufficiency • AccommodativeВ dysfunction • Oculomotor anomalies • OcularВ Inflammation – Keratitis – AnteriorВ Uveitis – IntermediateВ Uveitis http://directorsblog.health.azdhs.gov/?p=3493 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 56 6/11/2013 PerceptualВ Difficulties OcularВ Motility SanВ Jose,В California:В 19yo • DiagnosedВ inВ 2011 • SmoothВ PursuitsВ &В Integration • FastВ &В AccurateВ Saccades • NoВ MidlineВ Hesitation – NoВ associatedВ tickВ bite – PresumedВ contractedВ atВ 15yoВ (2010) – StageВ 3 DEM • DifficultiesВ withВ RapidВ AutomaticВ Naming • AdequateВ SpatialВ PlanningВ andВ TrackingВ Skills PMA‐PS • PresentingВ Complaints: – Diplopia;В IntermittentВ atВ distance – “JerkyВ Tracking” – IntermittentВ blurryВ vision • ReducedВ VisualВ ProcessingВ Speed TVAS • SpatialВ PlanningВ Difficulties CranialВ NerveВ Literature CranialВ NerveВ 6В Palsy • Lacomte ‐ 1989 • Esophoria;В DI • IncreasesВ inВ lateralВ gaze • OS:В AbductionВ restriction OcularВ Posture OcularВ Motility п‚— п‚— AbducensВ palsy п‚— ParalyticВ sixthВ nerveВ palsy в—¦ MostВ commonВ causeВ ofВ diplopia п‚— SymptomaticВ forВ 10В years UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 в—¦ Diplopia AbsenceВ ofВ adductionВ restrictionВ 2В weekВ treatmentВ protocolВ в—¦ 200mgВ doxycyclineВ perВ day • DivergenceВ difficulties FacialВ palsyВ mostВ common MRIВ showedВ inflammationВ of: Bilateral:В CNВ 3,7,9,10,11,12 Unilateral:В 4,5,6 Collegium Antropologicum 2005 ‐ Zrinsnak в—¦ RulesВ outВ nuclearВ lesion Vergence • DiplopiaВ duringВ binocularВ facility – – – – ClinicalВ InfectiousВ Disease 2009 ‐ Sauer п‚— Accommodation • VanВ Erp ‐ 2011 – FacialВ palsyВ mostВ common • 2/3В unilateral,В 1/3В bilateral – UsuallyВ duringВ secondВ monthВ ofВ disease – Oculo‐motorВ nerveВ alsoВ described or в—¦ Headaches п‚— StrabismusВ surgery в—¦ InitialВ 40pDВ esotropia в—¦ Post‐Op:В 10pDВ esotropia в—¦ 2gВ ceftriaxoneВ perВ day в—¦ UnableВ toВ abduct п‚— ResolutionВ atВ 2 ‐12В weeks в—¦ DiplopiaВ remained п‚— ResolutionВ throughВ 7В years 57 6/11/2013 Tuolumne,В California:В 29yo DiagnosingВ ConvergenceВ Palsy • DiagnosedВ inВ 2010 • Diplopia • jj – WhenВ watchingВ TVВ orВ reading – Horizontal – 6В months • Arthritis • “BrainВ fog” – ChangesВ inВ memory – Clumsy – ChangesВ inВ cognitiveВ functioning • Versions • Ductions OcularВ Motility OcularВ Posture • R‐AX(T) • Divergence • Convergence • NPC Vergence • Headaches SeeingВ ThroughВ TheВ BrainВ Fog DEM PMA‐PS • DifficultiesВ withВ RapidВ AutomaticВ Naming • AdequateВ SpatialВ PlanningВ andВ TrackingВ Skills • ReducedВ VisualВ ProcessingВ Speed UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Readalyzer • IncreasedВ NumberВ ofВ Fixations • ProlongedВ FixationВ Duration • ReducedВ ReadingВ Rate DenaliВ NationalВ Park,В Alaska:В 37yo • DiagnosedВ withВ LymeВ diseaseВ inВ 2012 • SuspectedВ presentВ forВ moreВ thanВ 10В years • PresentingВ Complaints: – AsthenopiaВ &В fatigueВ withВ reading – AuditoryВ processingВ easierВ thanВ visualВ processingВ 58 6/11/2013 LymeВ DiseaseВ asВ anВ AcquiredВ BrainВ Injury PerceptualВ Difficulties OcularВ Motility DEM VariabilityВ ofВ Presentation LightВ Sensitivity п‚— ConvergenceВ InsufficiencyВ &В Palsy п‚— CranialВ NerveВ Palsies п‚— VisualВ PerceptualВ Difficulties п‚— п‚— • Pursuits:В SaccadicВ Intrusions • Saccades:В Hypometric • DifficultiesВ withВ RapidВ AutomaticВ Naming • AdequateВ SpatialВ PlanningВ andВ TrackingВ Skills References • • • PMA‐PS • ReducedВ VisualВ ProcessingВ Speed • • • • Readalyzer • IncreasedВ NumberВ ofВ Fixations • ProlongedВ FixationВ Duration • ReducedВ ReadingВ Rate • • • • • Biesiada,В Grazyna etВ al. “LymeВ Disease:В Review.” ArchivesВ ofВ MedicalВ Science.В 6В (2012):В 978‐82. Fatterpekar,В Girish etВ al.  “OrbitalВ LymeВ Disease:В MRВ ImagingВ BeforeВ andВ AfterВ Treatment:В CaseВ Report.” AmericanВ JournalВ ofВ Neuroradiology. 23В (2002):В 657‐9. Goodrich,В GLВ etВ al.  “MechanismsВ ofВ TBIВ andВ VisualВ ConsequencesВ inВ MilitaryВ andВ VeteranВ Populations.” OptometryВ &В VisualВ Science.В 90.2В (2013):В 105‐12. Huppertz,В Hans‐Iko etВ al.  “OcularВ ManifestationsВ inВ ChildrenВ andВ AdolescentsВ WithВ LymeВ Arthritis.” BritishВ JournalВ Ophthalmology. 83.11В (1999):В 1149‐52. Lecomte,В FВ etВ al.  “NeurologicalВ Maifestations ofВ LymeВ DiseaseВ andВ Treatments.” BiomedicalВ andВ Pharmacotherapy. 43В (1989):В 409‐413. Mikkila,В HelenaВ etВ al.  “TheВ ExpandingВ ClinicalВ SpectrumВ ofВ OcularВ LymeВ Borreliosis.” Ophthalmology.В 107.3В (2000):В 581‐87. Mora,В PaoloВ andВ Carta,В Arturo.  “OcularВ ManifestationsВ ofВ LymeВ Borreliosis inВ Europe.” InternationalВ JournalВ ofВ MedicalВ Sciences.В 6.3В (2009):В 124‐ 125. Sauer,В Arneud etВ al. “FiveВ CasesВ ofВ ParalyticВ StrabismusВ asВ aВ RareВ FeatureВ ofВ LymeВ Disease.” ClinicalВ InfectiousВ Diseases. 48В (2009):В 756‐9. Sperling,В JВ etВ al.  “EvolvingВ PerspectivesВ onВ LymeВ Borreliosis inВ Canada.” TheВ OpenВ NeurologyВ Journal. 6В (2012):В 94‐103. VanВ Erp,В Willemijn etВ al.  “Opsoclonus andВ MultipleВ CranialВ NeuropathyВ asВ aВ ManifestationВ ofВ Neuroborreliosis.” Neurology. 77В (2011):В 1013‐14. Winterkorn,В Jacqueline.  “LymeВ Disease:В NeurologicВ andВ OphthalmicВ Manifestations.” SurveyВ ofВ Ophthalmology. 35.3В (1990):В 191‐204. Zrinsnak,В Ognjen etВ al.  “ParalyticВ StrabismusВ asВ aВ ManifestationВ ofВ LymeВ Borreliosis.В Coll Anthropology. 29В (2005):В 137‐9. NothingВ butВ Net: ChoroidalВ NeovascularВ MembranesВ forВ theВ PrimaryВ CareВ Optometrist JillianВ F.В Meadows,В OD,В MS SanВ FranciscoВ VAMC JuneВ 23,В 2013 RFV: temporallyВ associatedВ withВ getting “dustВ inВ eye” whileВ drivingВ twoВ daysВ ago OcularВ Hx: VAsc (cPH) MRx Pupils AntВ Seg Health Ta (Tonosafe) ONH UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 CaseВ Presentation 63 y/o HMВ presentedВ withВ decreasedВ visionВ OD,В CE/PCIOL 1999В OU OD OS 20/150‐ (NI) 20/30+ (20/20) NI ‐‐ ERRL,В (‐)APD ERRL,В (‐)APD WNL WNL 16 16 0.35,В fullВ pinkВ rim 0.35,В fullВ pinkВ rim Macula SeeВ photo Flat,В clear Post Seg Health SeeВ photo 1 intraretinal flameВ hemorrhage,В roundВ hypopigmented areaВ nasalВ toВ foveaВ В 59 6/11/2013 CaseВ Presentation CaseВ Presentation PresumedВ idiopathicВ choroidalВ neovascularВ membrane CardinalВ SignsВ ofВ CNV PigmentВ epithelialВ detachment CardinalВ SignsВ ofВ CNV CystoidВ macularВ edema SubretinalВ fluid IrregularВ elevationВ ofВ RPE UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 60 6/11/2013 CardinalВ SignsВ ofВ CNV SubretinalВ andВ intraretinal LipidВ exudation DifferentialВ DiagnosisВ ofВ CNVM hemorrhage Idiopathic ExudativeВ AMD ExcessiveВ photocoagulation ChoroidalВ rupture Polypoidal CNVM ChoroidalВ tumors MacularВ Telangiectasia PathologicВ myopia NormalВ VasculatureВ Development AllВ organsВ exceptВ theВ brainВ andВ kidneyВ areВ vascularizedВ viaВ vasculogenesis. Angioid streaks CSCR POHS EmbryologicВ VasculatureВ Development Vasculogenesis Angiogenesis Vasculogenesis:В LocalВ precursorВ cellsВ differentiate intoВ endothelialВ cells,В whichВ subsequentlyВ joinВ toВ formВ vessels Angiogenesis:В Blood vesselsВ sproutВ fromВ existingВ vesselsВ andВ penetrateВ adjacentВ tissue TheВ retinaВ isВ vascularizedВ byВ bothВ vasculogenesis andВ angiogenesis. HighlyВ coordinatedВ processВ involvingВ VEGF,В itsВ receptors,В andВ otherВ growthВ factors Final “maturation” processВ allowsВ vesselsВ toВ recruitВ pericyte supportВ andВ developВ structuralВ integrity,В facilitatedВ byВ PDGF,В Ang1,В Ang2,В TGF‐β1. Copyright В© 2001, European Society of Cardiology Conway E M et al. Cardiovasc Res 2001;49:507-521 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 AllВ mediatedВ byВ VEGFВ (andВ friends) 61 6/11/2013 VEGFВ andВ Whom? VascularВ EndothelialВ GrowthВ FactorВ Family • Glycoproteins • VEGF‐A, ‐B, ‐C, ‐D, ‐E • PlacentalВ GrowthВ FactorВ (PlGF) PathologicВ VasculatureВ Development UnregulatedВ angiogenesisВ thatВ lacksВ maturationВ intoВ vesselВ competency,В resultingВ inВ leakyВ vesselsВ ofВ poorВ integrity ProducedВ byВ RPE,В MГјllerВ cells,В pericytes,В endothelialВ cells,В andВ ganglionВ cells Normal Functions: • PromotesВ proliferation,В migration,В andВ capillaryВ tubeВ formation…but notВ maturation • IncreasesВ vascularВ permeability Stimuli: • NormalВ physiologyВ (includingВ trophicВ maintenanceВ ofВ choriocapillaris) • Hypoxia • Inflammation? • StructurallyВ sound • TargetedВ direction • VisuallyВ necessary • Bruch’sВ deposits • CNVВ inВ choroiditis • ButВ notВ allВ choroiditides causeВ CNV vs. Hypoxia • DiffuseВ thickeningВ ofВ Bruch’s • ButВ notВ allВ CNVsВ dueВ toВ hypoxia PrevailingВ theories DisruptionВ ofВ Bruch’sВ Membrane AlteredВ RPEВ andВ ECMВ metabolism UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 • Incompetent • Invasive,В lackingВ taxis • VisuallyВ destructive RecentВ paradigmВ shift ProbablyВ not… Inflammation Pathologic VeryВ delicateВ homeostasis… SoВ whatВ tipsВ theВ balance? AreВ allВ CNVMsВ createdВ equal? ChoroidalВ neovascularizationВ isВ poorlyВ characterizedВ andВ poorlyВ understood. V E G F Surgical CNVMВ excision MacularВ translocation Anti‐inflammatory Triamcinolone Ablative LaserВ photocoagulation PhotodynamicВ therapy MolecularВ (Anti‐VEGF) Macugen (pegaptanib) LucentisВ (ranibizumab) AvastinВ (bevacizumab) 62 6/11/2013 LatestВ therapeuticВ agents VEGFВ TrapВ (aflibercept) • FDAВ approvedВ forВ exudativeВ AMD • HighВ affinityВ toВ mostВ membersВ ofВ VEGFВ family,В includingВ PlGF • LessВ frequentВ dosingВ scheduleВ thanВ currentВ anti‐ VEGFВ meds • EfficacyВ comparisonВ toВ LucentisВ stillВ ongoing… PatientВ Update RNAВ Interference • Bevasirinib – InhibitionВ ofВ VEGFВ throughВ RNAВ interference – UpstreamВ mechanismВ causesВ delayedВ onsetВ ofВ activity;В notВ superiorВ toВ currentВ meds • AGN211745В (Sirna‐027) – InhibitionВ ofВ VEGFR‐1В throughВ RNAВ interference – StudiesВ ongoingВ BCVA:В В В 20/150В toВ 20/80В s/pВ AvastinВ xВ 3 ClinicalВ Pearls • KnowВ theВ clinicalВ signsВ thatВ signalВ presenceВ ofВ CNVM: – PED,В RPEВ irregularity,В subretinalВ fluid,В CME,В lipidВ exudation,В andВ subretinalВ hemorrhage • VEGFВ isВ onlyВ oneВ ofВ likelyВ manyВ incitingВ factorsВ thatВ canВ initiateВ CNVM,В andВ notВ allВ CNVMsВ areВ createdВ theВ same. • Long‐termВ blockadeВ ofВ VEGFВ mayВ accelerateВ choriocapillarisВ atrophy.В OtherВ therapeuticВ mechanismsВ needВ toВ beВ discovered. UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 References • • • • • • • • DoВ DV.В DetectionВ ofВ new‐onsetВ choroidalВ neovascularization.В Curr Opin Ophthalmol.В 2013В May;24(3):244‐7.В PubMedВ PMID:В 23518615.В DoВ DV,В GowerВ EW,В Cassard SD,В BoyerВ D,В Bressler NM,В Bressler SB,В Heier JS,В Jefferys JL,В Singerman LJ,В SolomonВ SD.В DetectionВ ofВ new‐onsetВ choroidalВ neovascularizationВ usingВ opticalВ coherenceВ tomography:В theВ AMDВ DOCВ Study.В Ophthalmology.В 2012В Apr;119(4):771‐8.В PubMedВ PMID:В 22297028.В Kinnunen K,В Ylä‐Herttuala S.В VascularВ endothelialВ growthВ factorsВ inВ retinalВ andВ choroidalВ neovascularВ diseases.В AnnВ Med.В 2012В Feb;44(1):1‐17.В PubMedВ PMID:В 21284527.В Qazi Y,В Maddula S,В Ambati BK.В MediatorsВ ofВ ocularВ angiogenesis.В JВ Genet.В 2009В Dec;88(4):495‐515.В PubMedВ PMID:В 20090210;В PubMedВ CentralВ PMCID:В PMC3306772.В Campochiaro PA.В RetinalВ andВ choroidalВ neovascularization.В JВ CellВ Physiol.В 2000В Sep;184(3):301‐10.В PubMedВ PMID:В 10911360.В Spaide RF.В ChoroidalВ neovascularizationВ inВ youngerВ patients.В Curr Opin Ophthalmol.В 1999В Jun;10(3):177‐81.В PubMedВ PMID:В 10537776.В D'Amore PA.В MechanismsВ ofВ retinalВ andВ choroidalВ neovascularization.В InvestВ Ophthalmol VisВ Sci.В 1994В Nov;35(12):3974‐9.В PubMedВ PMID:В 7525506.В Gass JM.В StereoscopicВ AtlasВ ofВ MacularВ Diseases.В 3В ed.В KleinВ EAВ editor.В St.В Louis,В Missouri:В Mosby;В 1987.В 63 6/11/2013 MyopiaВ Prevalence1 Pediatric Myopia Modulation Alex J Smith, OD, FAAO Diplomate, American Board of Optometry UC Berkeley Dr. Michael G Harris Contact Lens Resident IncreasingВ prevalenceВ ofВ myopia RisksВ ofВ highВ myopia • “MyopiaВ hasВ reachedВ epidemicВ proportions.”3 – Ophth Physiol Optics. SeptemberВ 2005 • PublicВ HealthВ Ramifications3,4 • TaiwaneseВ schoolchildren2: – – – – YearВ 2000:В 84% 16‐18В yr oldsВ myopic YearВ 1983:В 74% 16‐18В yr oldsВ myopic YearВ 2000:В 21% HighВ (>6.00D)В myopiaВ atВ 18В yrs old YearВ 1983:В 10.9% HighВ (>6.00D)В myopiaВ atВ 18В yrs old UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 – – – – – – – – – – RetinalВ detachment POAG Maculopathy DiscВ anomalies LacquerВ cracks/CNVM MacularВ hole Staphyloma Cataracts ReducedВ visualВ quality LifetimeВ $В forВ treatment 64 6/11/2013 PeripipheralВ HyperopicВ DefocusВ vs.В LagВ ofВ accommodation • InВ bothВ cases,В lightВ isВ focusedВ behindВ theВ retinalВ plane CLAMPВ STUDY5 • RGPsВ forВ MyopiaВ Control – NotВ effective • PeripheralВ hyperopicВ defocus – WhenВ opticalВ correctionВ isВ inВ place,В centralВ raysВ focusВ centrally – PeripheralВ raysВ focusВ behindВ theВ retina • NoВ plusВ inВ it • LagВ ofВ accommodation – TransientВ centralВ hyperopicВ defocus – HigherВ levelsВ ofВ educationВ associatedВ withВ myopia COMETВ StudyВ 20036 • +2.00В addВ PAL – SmallВ areaВ ofВ plusВ power • OverallВ 0.20В DВ differenceВ (14%)В overВ 3В years 2008В OEPВ NorthwestВ Congress • Aller &В Wildsoet twinВ study7 – AcuvueВ bifocalВ (puttingВ plusВ onВ it) – StatisticallyВ significantВ but “notВ clinicallyВ significant” – OccurredВ inВ firstВ year • HigherВ efficacyВ ifВ highВ lagВ ofВ accommodationВ +В lowerВ baselineВ myopia – 0.48В DВ difference • HighestВ efficacyВ ifВ highВ lagВ ofВ accommodationВ +В eso – 0.64В DВ difference UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 65 6/11/2013 ImageВ shell8 ImageВ shell ‐ Orthokeratology 9 LORICВ STUDYВ 200510 2008В OEPВ NorthwestВ Congress • AtropineВ intervention – ChuaВ 200611 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 66 6/11/2013 COMETВ 2В StudyВ 201112 • 0.28В DВ 3‐yearВ difference CambridgeВ Anti‐MyopiaВ StudyВ 201313,14 • “PeripheralВ RefractiveВ ChangesВ AssociatedВ withВ MyopiaВ Progression” IOVS FebВ 2013 • NoВ differenceВ inВ myopicВ progressionВ betweenВ anyВ arm • NoВ plusВ powerВ (myopicВ defocus)В appliedВ toВ retina Hiraoka etВ alВ 201215 ReducedВ concentrationsВ ofВ Atropine • ChiaВ etВ alВ 201216 UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 67 6/11/2013 WhatВ canВ anyВ ODВ doВ forВ PatientsВ Tomorrow? • AtropineВ 0.1% References • • – BestВ balanceВ ofВ efficacyВ vs.В sideВ effects – 0.01%В minimalВ sideВ effectsВ forВ similarВ efficacyВ toВ O‐K,В MFВ soft • Orthokeratology – TopographerВ needed – OvernightВ lensВ wearВ risks • MultifocalВ softВ contactВ lenses – DistanceВ centerВ hasВ mostВ evidence • ExecutiveВ bifocalВ glassesВ withВ 3^BI • • • • • • • • • • • • • WhenВ inВ doubt... • • 1.В Santodomingo,В J. “ControllingВ MyopiaВ ProgressionВ inВ Children” Menicon Horizons.В 2011В May;В 6. 2.В Lin,В LLKВ etВ al. “PrevalenceВ ofВ MyopiaВ inВ TaiwaneseВ Schoolchildren:В 1983‐2000.” AnnalsВ AcademyВ ofВ Medicine. 2004В Jan;33(1):27‐33. 3.В Saw,В S‐M,В etВ al. “MyopiaВ andВ associatedВ pathologicalВ complications.” Ophthal Phys Optics.В 2005В Sept;22(5):381‐391 4.В Kanski,В JackВ J.В ClinicalВ Ophthalmology. 5th Ed.В Butterworth‐Heinemann.В 2003 5.В Walline,В JeffreyВ JВ etВ al. “AВ RandomizedВ TrialВ ofВ theВ EffectsВ ofВ RigidВ ContactВ LensesВ onВ MyopiaВ Progression.” ArchВ Ophthalmol. 2004;122:1760‐1766. 6.В Gwiazda,В Jane. “TreatmentВ OptionsВ forВ Myopia.” Optom VisВ Sci. 2009В June;86(6):624‐628 7.В Aller,В TA. “MyopiaВ ProgressionВ inВ aВ TwinВ PairВ withВ BifocalВ SoftВ ContactВ Lenses – SecondВ YearВ ResultsВ AfterВ SingleВ Crossover.” <http://www.aaopt.org/Submission/Search/SubmissionViewer.asp?SID=4203&BR=SP> 8.В Smith,В E. “PrenticeВ AwardВ LectureВ 2010:В AВ CaseВ forВ PeripheralВ OpticalВ TreatmentВ StrategiesВ forВ Myopia.” Optom VisВ Sci.В 2011В Sept;88(9):1029‐1044. 9.В Herzberg,В C. “AnВ UpdateВ onВ Orthokeratology.” ContactВ LensВ Spectrum;В 2010В Mar.В http://www.clspectrum.com/articleviewer.aspx?articleid=103967 10.В Cho,В PВ etВ al. “TheВ longitudinalВ orthokeratologyВ researchВ inВ childrenВ (LORIC)В inВ HongВ Kong:В aВ pilotВ studyВ onВ refractiveВ changesВ andВ myopicВ control.” Curr EyeВ Res. 2005В Jan;30(1):71‐80. 11.В Chua,В WHВ etВ al, “AtropineВ forВ theВ treatmentВ ofВ childhoodВ myopia.” Ophthalmology. 2006В Dec;113(12):2285‐91. 12.В PEDIG. “Progressive‐AdditionВ LensesВ vs.В Single‐VisionВ LensesВ forВ SlowingВ ProgressionВ ofВ MyopiaВ inВ ChildrenВ withВ HighВ AccommodativeВ LagВ andВ NearВ Esophoria.” IOVS.В 2011В April;52(5):2749‐2757 13.В Radhakrishnan,В H.В etВ al. “PeripheralВ RefractiveВ ChangesВ AssociatedВ withВ MyopiaВ Progression.” IOVS. 2013В Feb;54(2):1573‐81 14.В Allen,В PM.В EtВ al. “AberrationВ ControlВ andВ VisionВ TrainingВ asВ anВ EffectiveВ MeansВ ofВ ImprovingВ AccommodationВ inВ IndividualsВ withВ Myopia.” IOVS. 2009В Nov;50(11):5120‐5129. 15.В Hiraoka,В T.В etВ al, “Long‐TermВ EffectВ ofВ OvernightВ OrthokeratologyВ onВ AxialВ LengthВ ElongationВ inВ ChildhoodВ Myopia:В AВ 5‐ YearВ Follow‐UpВ Study.” IOVS. 2012В June;53(7):3913‐3919 16.В Chia,В A.В etВ al. “AtropineВ forВ theВ treatmentВ ofВ ChildhoodВ Myopia:В SafetyВ andВ EfficacyВ ofВ 0.5%,В 0.1%В andВ 0.01%В DosesВ (AtropineВ forВ theВ TreatmentВ ofВ MyopiaВ 2).” Ophthalmology.В 2012В Feb;119(2):347‐354. PrimaryВ OcularВ HSV • SubclinicalВ inВ 94%В Re‐thinkingВ HSVВ Keratitis • Bimoidal distribution – AgesВ 1‐5;В AgesВ 13‐25 • LidВ vesiclesВ orВ erosiveВ blepharitisВ (34‐ 44%) AndreaВ DeВ Souza,В O.D. PrimaryВ CareВ andВ ContactВ LensВ Resident UCВ BerkeleyВ SchoolВ ofВ Optometry UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 • EpithelialВ keratitisВ (15‐63%) • FollicularВ orВ pseudomembraneous conjunctivitisВ (54‐84%) 68 6/11/2013 UnilateralВ orВ Bilateral? HSVВ EpithelialВ Keratitis • 50‐80%В ocularВ HSV • Souza:В 98%В unilateral • ThreeВ types: • Wilhelmus:В 97%В unilateral – BilateralВ HSVВ isВ undefined – BilateralВ herpeticВ keratitis:В presenceВ ofВ dendritic orВ geographicВ epithelialВ ulceration – Stellate – Dendritic (9‐15%) – Geographic • Brandt:В 88.2%В unilateral • Rezende:87.8%В unilateral • Darougar:В 81%В unilateral – BilateralВ herpeticВ keratitis:В anyВ formВ ofВ HSVВ keratitis Management:В GoldВ Standard • Orals: – 400mgВ AcyclovirВ 5x/d – 500mgВ Valacyclovir TID – 250mgВ Famciclovir TID • Topicals: – 1%В TrifluridineВ 9x/d – 0.15%В Gancyclovir 5x/d 1%В TrifluridineВ (Viroptic) • Thimerosol preservative – – – – CornealВ toxicityВ (punctateВ keratopathy) BurningВ orВ stingingВ (4.6%) CornealВ edema Conj.В edema,В hyperemia • Compliance? • ConsumerВ availability? • Cost:В ~$100В (7.5mL) UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 69 6/11/2013 0.15%В Gancyclovir GelВ (Zirgan) п‚— BAKВ preservative в—¦ IrritationВ (20%) в—¦ SPKВ (5%) в—¦ HyperemiaВ (5%) п‚— п‚— Compliance? Cost:В ~$170В (1В tube,В 5gm) OralВ and/orВ TopicalВ Acyclovir TopicalВ Steroids? • StromalВ keratitisВ andВ endotheliitis?В Yes. • EpithelialВ keratitis?В NO! • Complications: – EnlargementВ ofВ stellate lesionsВ orВ dendrites – ProgressionВ toВ necrotizingВ stromalВ keratitis – IritisВ orВ hypopyon – SecondaryВ GLC Photo ODВ vs OMDВ Management • HEDSВ 2:В TrifluridineВ andВ 400mgВ acyclovir – noВ benefitВ inВ preventingВ stromalВ keratitisВ orВ iritis • Collum L.:В 3%В acyclovirВ ophthalmicВ ointmentВ vs.В 400mgВ oralВ acyclovir – noВ statisticallyВ significantВ differenceВ inВ theВ medianВ timeВ toВ healing UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 GroupВ 1:В OD GroupВ 2:В OMDВ withoutВ corneaВ fellowship GroupВ 3:В OMDВ withВ corneaВ fellowship 70 6/11/2013 Pros: ‐ ‐ TopicalВ Antivirals ‐ EasierВ toВ administer LowerВ systemicВ penetration Costly ‐ Trifluridine:В $100 ‐ Gancyclovir:В $170 Cons: ‐ ‐ ‐ FrequentВ dosingВ (trifluridine) GreaterВ ocularВ sideВ effects RefrigerationВ (trifluridine) Oral Antivirals Pros: Cons: ‐ ‐ ‐ ‐ ‐ ‐ ‐ LessВ frequentВ dosing FewerВ sideВ effects ‐ MetabolizedВ byВ kidneys NoВ refrigeration Cost ‐ Acyclovir:В $20 ‐ Valacyclovir:В $200 ReducesВ systemicВ viralВ load PenetratesВ multipleВ ocularВ tissues DifficultВ toВ swallow AlternativeВ ManagementВ OralВ Antivirals Pros: Cons: ‐ LessВ frequentВ dosing ‐ FewerВ sideВ effects ‐ DifficultВ toВ swallow ‐ MetabolizedВ byВ kidneys ‐ NoВ refrigeration ‐ Cost ‐ Acyclovir:В $20 ‐ Valacyclovir:В $200 ‐ ReducesВ systemicВ viralВ load ‐ PenetratesВ multipleВ ocularВ tissues FluoroquinolonesВ forВ HSV • PrimaryВ orВ recurrentВ HSV: – 800mgВ AcyclovirВ 5x/dВ (10В days) • FasterВ healingВ time • NoВ increasedВ sideВ effects • DNA‐topoisomerase cleavageВ complexes • StructuralВ similaritiesВ betweenВ topoisomerases ofВ DNAВ virusesВ andВ bacteria • HSVВ 1В andВ 2: – dsDNA virus – usesВ topoisomerase IВ &В II UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 71 6/11/2013 п‚— AfricanВ SwineВ FeverВ Virus:В п‚— п‚— Method: п‚— п‚— NoВ viralВ genomeВ fragmentationВ observed п‚— ProposedВ MOA:В ASFVВ topoisomerase IIВ inhibitor DNAВ encodesВ forВ topoisomerase II injectВ animalВ cellsВ withВ 30В fluoroquinolonesВ atВ varyingВ timesВ afterВ infection interferenceВ withВ ATPase activity torsional/replicative stress п‚— reductionВ inВ viralВ DNAВ replicationВ andВ proteinВ synthesis п‚— п‚— п‚— NoВ viralВ genomeВ fragmentationВ observed п‚— ProposedВ MOA:В ASFVВ topoisomerase IIВ inhibitor interferenceВ withВ ATPase activity torsional/replicative stress п‚— reductionВ inВ viralВ DNAВ replicationВ andВ proteinВ synthesis п‚— п‚— ReviewingВ Differentials CanВ fluoroquinolonesВ haveВ aВ similarВ effectВ onВ HSV? HSV EpithelialВ Keratitis Microbial Keratitis Unilateral orВ bilateral Unilateral Stellate lesions • multiple, elevated Infiltrate/ulcer • single, excavated Greater corneal orВ lidВ edema CanВ fluoroquinolonesВ temporarilyВ reduceВ hostВ cellВ replication? UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 Tx:В antivirals Tx:В antibiotics 72 6/11/2013 ReviewingВ Differentials HSV EpithelialВ Keratitis Infiltrative Keratitis Unilateral orВ bilateral Unilateral orВ bilateral Stellate lesions • multiple, elevated,В irregularВ shape PinpointВ lesions • multiple,В flat,В round References • • • • Greater corneal orВ lidВ edema Tx:В antivirals Tx:В steroids • • • • • • • • • • • • • • UCВ BERKELEYВ RESIDENTВ FORUMВ JUNEВ 2013 NationalВ EyeВ Institute. “HerpeticВ EyeВ DiseaseВ StudyВ (HEDSВ 1/2)”.В U.S.В NationalВ InstitutesВ ofВ Health.В В SeptВ 1999.В В Bernstein,В D.В etВ al. “Epidemiology,В ClinicalВ Presentation,В andВ AntibodyВ ResponseВ toВ PrimaryВ InfectionВ WithВ HerpesВ SimplexВ VirusВ TypeВ 1В andВ TypeВ 2В inВ YoungВ Women”.В В ClinicalВ InfectiousВ Diseases.В FebruaryВ 1,В 2013;В 56(3):344–51 Souza,В P.В etВ al. “BilateralВ HerpeticВ Keratoconjunctivitis”.В AmericanВ AcademyВ ofВ Ophthalmology.В MarchВ 2003.В Vol 110,В Num.В 3,В Pgs.В 493‐496. Remeijer,В L.В etВ al. “HumanВ herpesВ simplexВ virusВ keratitis:В theВ pathogenesisВ revisited”.В OcularВ ImmunologyВ andВ Inflammation – 2004,В Vol.В 12,В No.В 4,В pp.В 255–285 Saini,В J.В andВ Argawala,В R. “ClinicalВ PatternВ ofВ RecurrentВ HerpesВ SimplexВ Keratitis”.В IndianВ JournalВ ofВ Ophthalmology.В 1999.В Vol:В 47,В Issue:1.В PgВ 11‐14.В Wilhelmus,В K. “BilateralВ herpeticВ keratitis”.В BritishВ JournalВ ofВ Ophthalmology,В 1981,В 65,В Pgs.В 385‐387.В Liesegang,В L. “HerpesВ SimplexВ VirusВ EpidemiologyВ andВ OcularВ Importance”.В CorneaВ (2001).В В 20(1):В 1–13,В 2001. Sacks,В S.В etВ al. “ClinicalВ ManagementВ ofВ HerpesВ Virus”.В IOSВ Press.В Netherlands.В 1995.В Pg.В 23 Darougar,В S.В etВ al.   “EpidemiologicalВ andВ clinicalВ featuresВ ofВ primaryВ herpesВ simplexВ virusВ ocularВ infection”.В BritishВ JournalВ ofВ Ophthalmology,В 1985,В 69,В Pgs.В 2‐6. Farooq,В A.В andВ Shukla,В D. “HerpesВ SimplexВ EpithelialВ andВ StromalВ Keratitis:В AnВ EpidemiologicВ Update”.В SurveyВ ofВ Ophthalmology.В OctoberВ 2012.В Vol.В 57,В NumberВ 5,В Pgs.В 448‐461. Potter,В W. “AnВ OverviewВ ofВ OcularВ HerpeticВ Disease”.В ReviewВ ofВ Optometry.В MayВ 2010. Thygeson,В P.В etВ al. “TheВ UnfavorableВ ResponseВ ofВ TopicalВ SteroidВ TherapyВ onВ HerpeticВ Keratitis”.В TransactionsВ ofВ theВ AmericanВ OphthalmologicalВ Society.В 1960;В 58:В 246–256. Kimura,В S.В etВ al. “HerpesВ SimplexВ Keratitis:В AnВ ExperimentalВ Study”.В InvestigativeВ Ophthalmology.В AprilВ 1962.В PgsВ 273‐278. Lee.В S.В andВ Pavan‐Langston,В D. “RoleВ ofВ AcyclovirВ inВ theВ TreatmentВ ofВ HerpesВ SimplexВ VirusВ Keratitis”.В InternationalВ OphthalmologyВ Clinics.В 1994.В VolumeВ 3,В IssueВ 3.В PgsВ 9‐18. Collum,В L.В etВ al. “OralВ AcyclovirВ (Zovirax)В inВ HerpesВ SimplexВ Dendritic CornealВ Ulceration”.В BritishВ JournalВ ofВ Ophthalmology.В 1986;В 70.В PgsВ 435‐438.В Mottola,В C.В etВ al. “InВ VitroВ AntiviralВ ActivityВ ofВ FluoroquinolonesВ AgainstВ AfricanВ SwineВ FeverВ Virus”.В VeterinaryВ Microbiology.В 2013.В PgsВ 1‐9. Bapat,В A.В etВ al. “StudiesВ onВ DNAВ Topoisomerases IВ andВ IIВ inВ HerpesВ SimplexВ VirusВ TypeВ 2‐ infectedВ Cells”.В JournalВ ofВ GeneralВ Virology.1987.В Vol.В 68.В PgsВ 2231‐2237. Ebert,В S.В etВ al. “Topoisomerase IIВ CleavageВ ofВ HerpesВ SimplexВ VirusВ Type1В DNAВ InВ VivoВ IsВ ReplicationВ Dependent”.В JournalВ ofВ Virology.В Sept.В 1990.В Vol.В 64,В No.9.В В PgsВ 4059‐4066 73
© Copyright 2026 Paperzz