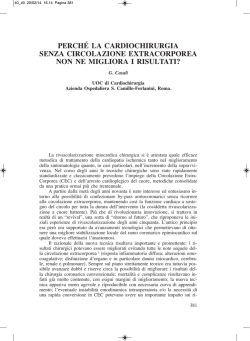
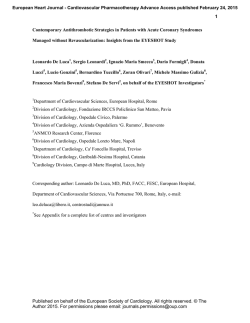
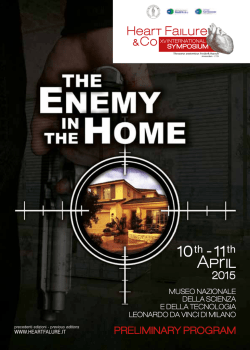
284 La Radiologia Medica - Radiol Med 106: 284-296, 2003 Edizioni Minerva Medica - Torino Non-invasive angiography of the coronary arteries with multislice computed tomography: state of the art and future prospects Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato Stato dell’arte e prospettive future L’angiografia convenzionale ha rappresentato fino ad oggi l’unico strumento per la valutazione delle arterie coronarie. Tentativi sono stati effettuati durante la scorsa decade per validare una tecnologia non invasiva per lo studio delle coronarie. In particolare la Tomografia ad emissione di elettroni e la Risonanza Magnetica sono state utilizzate a questo scopo senza però divenire strumenti clinici. Di recente la tecnologia di tomografia computerizzata (TC) spirale, migliorata dall’utilizzo di sistemi multistrato a 4 linee di detettori e da una velocità di rotazione del tubo radiogeno di 500 ms, ha mostrato un ottimo potenziale senza entrare nella pratica routinaria. L’introduzione della tecnologia multistrato a 16 canali, con tempi di rotazione del tubo radiogeno inferiori a 500 ms, ha reso possibile ottenere risultati di rilievo nella valutazione delle stenosi coronariche significative (>50%), tali da proporne l’utilizzo clinico. In questo lavoro verranno descritti la tecnica di esecuzione dell’esame ed i risultati, allo stato dell’arte, dell’angiografia con TC delle arterie coronarie. Until now conventional angiography has represented the only technique for assessing the coronary arteries. During the last decade, attempts have been made to validate a non-invasive technique for the study of coronary arteries. In particular, Electron-beam Tomography and Magnetic Resonance Imaging have been used for this purpose, even though they have not become clinical tools. More recently, spiral computed tomography (CT) technology, improved by the use of multiple slices and 500ms gantry rotation times, has shown a good potential without entering routine clinical practice. The introduction of multislice technology with 16 rows and rotation times below 500ms has yielded such good results in detecting significant (>50%) coronary artery stenosis that it has been proposed as a clinical tool. This paper describes the examination technique and the results achieved in CT angiography of the coronary arteries. PAROLE CHIAVE: Coronarografia - Imaging non invasivo - Tomografia computerizzata multistrato. KEY WORDS: Coronary angiography - Non-invasive coronary imaging - Multislice Computed Tomography. Filippo CADEMARTIRI1 - Giacomo LUCCICHENTI2 Riccardo MARANO3 - Koen NIEMAN1, 4 - Nico MOLLET1, 4 Pim DE FEYTER1,4 - Gabriel P KRESTIN1 - Lorenzo BONOMO3 A Introduzione Introduction Dalla sua introduzione nella pratica clinica, l’angiografia coronarica convenzionale rappresenta lo strumento più accurato per la valutazione dell’emodinamica delle arterie coronarie [1, 2]. Questa tecnica è soggetta a quegli inconvenienti che sono caratteristici delle metodiche angiografiche convenzionali come la natura proiettiva delle immagini e l’impossibilità di visualizzare la parete del vaso. Inoltre, invasività, rischi e costi impediscono l’impiego di questa tecnica su larga scala se non in pazienti con precise indicazioni cliniche. Nell’ultima decade vi sono stati alcuni tentativi di ovviare a questi inconvenienti. In particolare la risonanza magnetica (RM) e la tomografia computerizzata ad emissione di elettroni (EBT), hanno fornito risultati interessanti ma non sufficienti per estenderne l’utilizzo alla pratica clinica routinaria [1, 3-8]. L’imaging delle arterie coronarie necessita, a causa delle dimensioni delle strutture studiate e del movimento indotto dalle pulsazioni cardiache, di risoluzioni spaziale e tempo- Ever since its introduction, Coronary Angiography (CA) has been considered the gold standard in the hemodynamic evaluation of coronary arteries [1, 2]. Drawbacks of this technique are the inner projective nature of the images, and the inability to directly visualize the vessel walls. The invasive nature, the risks and the costs limit the use of CA strictly to patients with a well-defined clinical indication. In the last decade attempts have been made to overcome these limitations with Magnetic Resonance (MR) and Electron-Beam Computed Tomography (EBCT), with interesting results but not sufficient to extend the use of these diagnostic tools to routine clinical practice [1, 3-8]. Imaging of the coronary arteries requires high spatial and temporal resolution because of the small size of the vessels and of motion due to the heartbeat. Multislice Computed tomography (MSCT) technology provides high spatial and temporal resolution. Four-row MSCT has shown encouraging results although the rate of non-assessable vessels is high [9-13]. The introduction of 16-row MSCT scanners allows the spa- Dipartimento di Radiologia1 - Erasmus Medical Center - Rotterdam, Olanda - Dipartimento di Radiologia2 - Università degli Studi di Parma - Italia Dipartimento di Radiologia3 - Università di Chieti - Italia - Dipartimento di Cardiologia4 - Thoraxcentre - Erasmus Medical Center - Olanda. Pervenuto alla Redazione il 03.04.2003; revisionato il 05.05.2003; restituito corretto il 23.05.2003; accettato per la pubblicazione il 31.05.2003. Indirizzo per la richiesta di estratti: Dott F. Cademartiri, Viale Rustici, 2 - 43100 Parma PR - Italia - Tel. 0521/961833. E-mail:[email protected] F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato rale elevate. Queste ultime sono state ottenute con l’impiego della tecnologia multistrato. Le apparecchiature multistrato a 4 canali hanno fornito risultati incoraggianti ma insufficienti a causa di una elevata percentuale di vasi non valutabili [9-13]. Lo sviluppo di scanner a 16 canali ha permesso un ulteriore miglioramento delle risoluzioni spaziale e temporale. La scansione coronarica può essere, infatti, completata in un tempo inferiore ai 20 s (contro i 35-40s precedentemente necessari), e con una risoluzione spaziale di 0,75mm (contro il valore di 1-1,25 mm delle precedenti generazioni [1417]. Gli ottimi risultati ottenuti con le apparecchiature a 16 strati hanno indotto a proporre l’impiego di questa tecnica nella routine clinica [18, 19]. Lo scopo di questo lavoro è di illustrare il razionale clinico-diagnostico, le basi tecniche, i risultati e le prospettive future della tecnologia multistrato applicata alle arterie coronarie. In particolare verrà focalizzata l’attenzione sul paragone tra apparecchiature a 4 e 16 strati. Materiale e metodi Preparazione del paziente I pazienti con fibrillazione atriale, allergia nota al mezzo di contrasto iodato e insufficienza renale (creatinina sierica >120 mmol/L-1) vengono esclusi [18]. È stato descritto come la frequenza cardiaca elevata influenzi negativamente le prestazioni ed il successo della scansione in termini di qualità diagnostica [8, 13, 20, 21]. Ai pazienti con frequenza cardiaca superiore a 65 battiti per minuto (bpm) viene somministrato, 45-60 minuti prima della scansione, metoprolo-tartrato per os con dosaggio compreso tra 50 e 200 mg a seconda della frequenza cardiaca. La bradicardizzazione è più difficoltosa in pazienti con frequenza >90 bpm. Per uno studio ottimale delle arterie coronarie è necessario ottenere una frequenza cardiaca al di sotto di 65 bpm. Nel caso in cui si stia valutando il muscolo cardiaco, il pericardio, l’anatomia dei grossi vasi o la funzione miocardica è possibile studiare anche pazienti con frequenze cardiache superiori o con fibrillazione atriale a condizione che sia a bassa risposta ventricolare. Al fine di ottenere una traccia elettrocardiografica (ECG), tre elettrodi vengono posizionati per ottenere una sola derivazione ECG corrispondente a D1. Il vettore della derivazione infatti va dalla spalla destra alla spalla sinistra. Gli elettrodi vengono posizionati nel cavo ascellare destro e sinistro (la terra sulla superifice addominale o sul fianco sinistro) in modo che non siano a contatto con i grandi muscoli del torace (grande pettorale e grande dorsale). Questo evita irregolarità della linea basale dell’ECG, dovute a contrattura muscolare, quando le braccia vengono posizionate al di sopra della testa per la scansione. Il mezzo di contrasto iodato viene somministrato per via endovenosa antecubitale mediante un’agocannula da 18-20 G ed un iniettore automatico. Il lato da scegliere quando possibile è il destro. Da questo lato infatti l’anatomia della vena anonima è più favorevole e gli artefatti da indurimento legati alla elevata densità del contrasto a livello venoso non compromettono eccessivamente la visualizzazione dell’arco aor- 285 tial and temporal resolution to be increased. Coronary CT imaging can be performed in less than 20 sec (versus 3540s of 4-row MSCT), with a spatial resolution of 0.75mm (versus 1-1.25mm of 4-row MSCT) [14-17]. Sixteen-row MSCT has already shown good results and it is suggested as a tool for routine clinical practice [18, 19]. The aim of this paper is to illustrate the clinical and diagnostic rationale, the basics of the technique and future prospects of multislice technology applied to coronary artery imaging. Particular focus will be given to the comparison between 4-row and 16-row multislice scanners. Materials and methods Patient preparation Exclusion criteria are atrial fibrillation, previous contrast material (CM) adverse reaction, renal insufficiency (serum creatinine >120mmol/L-1) [18]. High heart rates have been reported to reduce diagnostic quality of MSCT scans [8, 13, 20, 21]. Patients with a heart rate >65bpm are given an oral dose of metoprol-tartrate (50-200mg depending on the heart rate), 45-60 minutes before the start of the scan. It is more difficult to slow down the heart rate when its value is >90bpm. When the heart rate is <65bpm it is usually possible to perform an optimal MSCT of the coronary arteries. For the evaluation of the myocardium, the pericardium, the anatomy of the great intra-thoracic vessels or cardiac function, it is possible to scan patients with higher heart rates or patients with atrial fibrillation and low ventricular response. The patient is positioned in the supine position, and then the three leads are connected to record the patient’s ECG. The leads are positioned on the middle axillary lines and on the left flank, to avoid irregularity of the baseline ECG track due to muscle contraction when both arms are positioned above the head during the scan. Contrast material is administered intravenously (i.v.) with an automatic power injector using a 18-20G cannula; the right arm is preferred because of the favorable anatomy of the right brachio-cephalic vein and because it produces less beam hardening artifacts at the level of the aortic arch. CT scan Angiographic CT is performed with a 4-16 row multislice scanner (Sensation 4-16 – Siemens Medical Solutions, Forchheim, Germany), after i.v. administration of 100-125 ml of non ionic contrast material (300-400 mgI/ml) at a flow rate of 4-5 ml/s with an automatic power injector (EnVision CT – MedRad, Pittsburgh, USA). The administration of a saline bolus-chaser of 40-50ml at the same flow rate, with a double head injector (Stellant - MedRad, Pittsburgh, USA) can be useful to push the contrast medium after the end of its administration while the scan is still underway. The patient’s ECG is recorded at the same time as CT scan is performed. The scan time is 40s for 4-row MSCT scanners and <20s for 16-row scanners. Scan parameters for 4-row MSCT are: detector number 4, detector collimation 1mm, rotation time 500ms, feed/rotation 1.5mm (pitch 0.375), kVp 120, mAs 400-500, field of view 150mm, effec- 286 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato Fig. 1. — Schema del sistema di modulazione del milliamperaggio. Modulazione prospettica della dose somministrata al paziente attraverso la sincronizzazione della corrente del tubo radiogeno con il tracciato ECG. The prospective modulation of the X-ray exposure through the synchronization of the tube current with the ECG. tico e dell’origine dei tronchi sovra-aortici (quando la scansione viene estesa per coprire per esempio l’origine delle arterie mammarie interne). Scansione La scansione angiografica viene effettuata con scanner spirali a 4-16 linee di detettori (Sensation 4-16 - Siemens Medical Solutions, Forchheim, Germania), dopo la somministrazione endovenosa per via antecubitale di un bolo di mezzo di contrasto non ionico (300-400 mgI/ml) di 100-125 ml con una velocità di 4-5 ml/s mediante un iniettore automatico (EnVision CT - MedRad, Pittsburgh, USA). La somministrazione di un bolo da 40-50 ml di soluzione salina alla stessa velocità del bolo principale è di ausilio per sospingere il bolo di mezzo di contrasto dalle vene del braccio. In questo caso è necessario impiegare un iniettore a doppia testa (Stellant - MedRad, Pittsburgh, USA). Contemporaneamente alla scansione viene registrata una traccia elettrocardiografica (ECG). La durata complessiva della scansione è di circa 40 s per i tomografi a 4 linee e inferiore ai 20 s per quelli a 16 linee. I parametri di scansione per la generazione a 4 linee sono: numero di detettori/collimazione 4/1 mm, tempo di rotazione del tubo radiogeno 500 ms, avanzamento/rotazione 1,5 mm (pitch 0,375), kVp 120, mAs 400, campo di vista 150 mm, spessore effettivo dello strato 1,25 mm, incremento di ricostruzione 0,7 mm, filtro di convoluzione per tessuti molli. I parametri di scansione per la generazione a 16 linee sono: numero di detettori/collimazione 16/0,75 mm, tempo di rotazione del tubo radiogeno 420 ms, avanzamento/ rotazione 3,0 mm (pitch 0,25), kVp 120, mAs 400-500, campo di vista 150 mm, spessore effettivo dello strato 0,75 mm, incremento di ricostruzione 0,4 mm, filtro di convoluzione per tessuti molli. Nella tabella I sono riassunti i principali parametri di scansione, irradiazione, ricostruzione e somministrazione del mezzo di contrasto. tive slice width 1.25 mm, reconstruction increment 0.7mm, soft tissue kernel. Scan parameters for 16-row MSCT are: detector number 16, detector collimation 0.75mm, rotation time 420ms, feed/rotation 3.0mm (pitch 0.25), kVp 120, mAs 400-500, field of view 150mm, effective slice width 0.75mm, reconstruction increment 0.4mm, soft tissue kernel. Table I summarises the main scan parameters, radiation dose, reconstruction and contrast medium administration parameters. Dose Radiation exposure La dose somministrata al paziente varia a seconda del sesso, del volume e dei parametri di scansione. Per il maschio Radiation exposure depends on the patient’s sex, the study volume and scan parameters. For males the dose is Fig. 2. — Schema dei metodi di sincronizzazione retrospettiva. Modalità di sincronizzazione retrospettiva della ricostruzione basata sul segnale ECG. La finestra di ricostruzione può essere posizionata utilizzando un metodo con ritardo fisso detto «assoluto inverso» (A), o con ritardo percentuale detto «relativo» (B). Nel primo caso la distanza dall’onda R rimane costante quindi a frequenze elevate (>70bpm) la fase che piu’ favorevolmente sarà definita tele-diatsolica sarà prossima a –350 ms, mentre a frequenze inferiori la finestra a –400 ms è ottimale. Nel secondo caso invece, la posizione delle finestre di ricostruzione varia proporzionalmente alla variazione dell’intervallo RR e, di conseguenza, alla frequenza cardiaca. Retrospective ECG synchronisation of the reconstruction. The reconstruction window can be positioned with a fixed delay so called «absolute reverse method» (A), or with a percentage delay so called «relative method» (B). In the first case, the distance from the R-wave is constant, then at higher heart rates (>70bpm) the most favourable window will be at –350 ms, while at lower heart rates –400 ms is almost always optimal. In the second case, the position of reconstruction window varies proportionally with the variation of RR interval and heart rate. F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato 287 è di circa 6,82 mSv mentre la femmina è di circa 10,12 mSv, senza l’utilizzo di modulazione prospettica del milliamperaggio [22, 23]. Questi valori possono essere ulteriormente ridotti sincronizzando l’emissione di raggi X all’ECG prospetticamente mediante la modulazione della corrente del tubo radiogeno [22]. Con questa tecnica è possibile ridurre la dose fino al 50% in meno a seconda della frequenza cardiaca (fig. 1). Ricostruzione delle immagini Le immagini vengono ricostruite in modo da corrispondere ad una particolare fase del ciclo cardiaco. Ciò viene ottenuto sincronizzando retrospettivamente i dati acquisiti all’ECG registrato durante la scansione. La fase del ciclo cardiaco alla quale appartengono i dati grezzi impiegati per la ricostruzione dell’immagine viene espressa come percentuale dell’intervallo R-R, oppure come distanza temporale dalla successiva onda R espressa in milli-secondi (Fig. 2). Qualunque fase del ciclo cardiaco può essere ricostruita per ottenere informazioni morfologiche delle strutture vascolari o funzionali (frazione d’eiezione, perfusione miocardica e motilità delle pareti miocardiche). Le coronarie possono essere valutate impiegando ad esempio tre finestre di ricostruzione della fase tele-diastolica a -350ms, -400ms, e -450ms dalla successiva onda R. Utilizzando il metodo percentuale relativo le finestre da utilizzare sono 65%, 70% e 75%. La necessità di ricostruire diverse finestre per la visualizzazione delle coronarie deriva dal movimento desincronizzato dei differenti segmenti coronarici. Alcuni tratti dei vasi infatti possono mostrare minore motilità in una fase del ciclo mentre altri in fasi leggermente diverse [8, 24]. Gli strati così ricostruiti possono essere definiti isocardiofasici, poiché appartengono alla stessa fase del ciclo cardiaco. Nel caso in cui la finestra di ricostruzione sia di durata insufficiente per fornire tutti i dati necessari, è possibile ottenere le informazioni da due cicli cardiaci adiacenti con una metodo definito di ricostruzione multi-segmentaria mostrato in figura 3 [25]. Per la ricostruzione di circa 250 immagini sono necessari circa 42s con una velocità di ricostruzione che può arrivare fino a 6 immagini al secondo. Analisi delle immagini La valutazione delle immagini viene effettuata su una stazione di lavoro (PC). Le ridotte dimensioni e l’anatomia complessa delle strutture studiate impediscono la loro valutazione sul solo piano di scansione. È fondamentale l’impiego di algoritmi di riformattazione multiplanare lungo il decorso delle arterie coronarie, e Maximum Intensity Projection (MIP, proiezione di massima intensità) che fornisce immagini di tipo angiografico. Le ricostruzioni tridimensionali con Volume Rendering (VR) permettono di rappresentare in modo sintetico la sede e l’entità della patologia (fig. 4). Esistono degli strumenti (software dedicati) semi-automatici ed automatici per la segmentazione dei vasi (Vessel View - Siemens Medical Solutions, Forchheim, Germania) che hanno lo scopo di velocizzare l’analisi delle immagini. L’asse centrale del vaso viene ottenuto a partire dalle sue due estremità. Da questo asse centrale è possibile ottenere Fig. 3. — Schema della modalita’ di ricostruzione bi-segmentale. Ricostruzione delle immagini nella quale tutte le proiezioni in un arco di 180° sono ottenute durante la stessa diastole (A). All’aumentare della frequenza cardiaca, con la tecnica multisegmentaria, le proiezioni dell’arco di 180° vengono ottenute da due o più fasi diastoliche (B). Image reconstruction in which all the 180° projections are obtained in the same diastole (A). When the heart frequency increases, with the segmented reconstruction technique, projections through 180° are obtained from the two or more diastolic phases (B). 6.82 mSv whereas for females it is 10.12 mSv, without the use of prospective tube current modulation [22, 23]. These values can be reduced by 50% using prospective synchronization between ECG and tube current modulation [22] (fig. 1). Image reconstruction All images are reconstructed in a defined phase of the cardiac cycle, by means of retrospective synchronization with the ECG track. This phase of the cardiac cycle is expressed as a percentage of the R-R interval (Relative Delay) or as temporal distance (ms) before the next R wave (fig. 2). Images can be also reconstructed in other phases of the cardiac cycle to obtain morphological or functional information (ejection fraction, myocardial perfusion and cardiac wall motion). The coronary arteries can be evaluated in the late diastolic phase with three different temporal windows at -350ms, -400ms, and -450ms before the next R wave. When the Relative Delay technique is applied, 65%, 70% and 75% are usually preferred. Several different reconstruction windows are normally required to visualize the coronary arteries because of their non synchronous motion [8, 24]. All the reconstructed images of one dataset can be defined as iso-cardio-phasic, because they belong to the same cardiac phase. When the temporal window is too short to provide all the data, the information can be obtained from two contiguous cardiac cycles with a multi-segmental reconstruction algorithm (fig. 3) [25]. To reconstruct 250 images, 42s are needed, with a maximum reconstruction speed of 6 image/sec. 288 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato Fig. 4. — Esempio di scansione coronarica con apparecchiatura TC multistrato a 16 canali. La ricostruzione tridimensionale VR (A), mostra una panoramica anatomica della regione del cuore e dei grossi vasi. Isolando nel volume tridimensionale il cuore dalle altre strutture toraciche (B, C, e D), si può apprezzare il tipico decorso dei 3 vasi principali. La arteria discendente anteriore (ADA) che decorre nel solco interventricolare anteriore (B e C), il ramo circonflesso dell’ arteria coronaria di sinistra (Cx) che decorre nel solco atrio-ventricolare sinistro (D), e la arteria coronaria destra (CDx) che decorre nel solco atrio-ventricolare destro (B e C). Chiaramente dimostrabile anche la posizione del tronco comune (TC) della coronaria sinistra (D). Una analisi dettagliata del lume vascolare presuppone l’utilizzo di ricostruzione multiplanari e curvate di tipo centro-luminale (E, F, G, e H). È possibile infatti visualizzare l’origine di entrambe le coronarie (TC-ADA e CDx) in un solo piano para-coronale curvato (E). La ADA ricostruita lungo il suo intero decorso è dimostrata in F. Lo stesso tipo di ricostruzione viene applicato alla Cx in G ed alla CDx in H. Nelle immagini sono anche dimostrati due rami diagonali (dalla ADA in B e C), e ben 5 rami marginali (dalla Cx in D). Nel caso presentato si osserva una dominanza sinistra, ossia quando la Cx prevale sulla CDx nella parete postero-inferiore del cuore e dà origine alla arteria discendente posteriore (D, G per la Cx e C, H per mostrare la ridotta estensione di CDx nel solco atrio-ventricolare destro). A livello del tratto distale di Cx si osserva una occlusione totale (freccia in D e G). Non sono presenti calcificazioni lungo il decorso delle coronarie e dei loro rami. CT angiography with 16 row scanner of the coronary arteries. Threedimensional reconstruction with VR (A), shows a panoramic view of the heart and the main vessels. The path of the vessels can be better depicted by separating the heart from adjacent structures (B, C and D). Descending anterior artery ADA courses in the anterior interventricular groove (B and C), the left circumflex coronary artery (Cx) courses in the left atrio-ventricular groove (D), and the right circumflex coronary artery (CDx) in the right atrio-ventricular groove (B and C). The common trunk of the left coronary artery is clearly visible (D). Multiplanar and curved reformatted images through the center-lumen allow detailed analysis of the vessel (E,F,G and H). The origin of both coronary arteries (TC-ADA and CDx) can be displayed in a single curved plane (E). The ADA is displayed along its path (F). The same kind of reconstruction has been performed in for Cx (G) and CDx (H). Two diagonal (from the ADA in D) and 5 marginal (from Cx in D) branches are also visible. In this case there is a left dominance, with Cx dominating over the CDx in the postero-inferior wall and generating the posterior descendent artery (D, G for the Cx, and H to show the limited length of CDx in the right atrio-ventricular sulcus). There is a total occlusion of the Cx in its distal tract (arrow in D and G). No calcifications are visible in the coronary arteries and their branches. immagini riformattate perpendicolari o lungo il decorso di questo asse. Risultati In tabella II sono riassunti i dati della letteratura ove la TC multistrato a 4 e a 16 canali è stata paragonata alla coronarografia convenzionale. Gli studi di coronarografia con TC a 4 strati sono stati effettuati su popolazioni comprese tra i 28 ed i 100 pazienti. La valutazione ha riguardato solo i vasi di diametro uguale o superiore a 2 mm (o 1,5 mm in [26]), e sono stati considerate le riduzioni del lume uguali o superiori al 50%. Con questi criteri di valutazione, sono stati ottenuti valori di sensibilità tra 75% ed 91% e di specificità tra 76% e 99% per la visualizzazione delle stenosi vascolari [9, 11, 12, 21, 26-29]. Nonostante questi valori appaiano Image analysis All images are evaluated at the workstation (PC). The small size of the coronary vessels and their complex anatomy prevent the evaluation on the native axial plane. It is therefore mandatory to use Multiplanar reconstructions (MPR) along the path of coronary arteries and Maximum Intensity Projection (MIP) reconstruction algorithms are normally used to create angiographic images. Three-dimensional (3D) Volume Rendered (VR) reconstructions allow the panoramic visualization of the site and grade of atherosclerotic disease (fig. 4). Dedicated software (Vessel View - Siemens Medical Solutions, Forchheim, Germany) can be used for semi-automatic or automatic segmentation of the vessels to increase the speed of vessel analysis. The extremities of the vessel are manually targeted and then a central lumen line is reconstructed. F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato 289 TABELLA I. — Protocolli di scansione angiografica coronarica con TC multistrato. Scanner Produttore Siemens Siemens Modello Volume zoom Sensation 16 Tipo 4 strati 16 strati Detettori 4 16 Collimazione 1 mm 0.75 mm KiloVolt 120 120 Scansione MilliAmpere/s 400 400-500 Tempo di rotazione 500 ms 420 ms Modulazione mAs Sistolica Sistolica Risoluzione temporale effettiva 250 ms 210 ms Risoluzione temporale massima* 125 ms 105 ms Avanzamento/rotazione 1.5 mm 3.0 mm Avanzamento/secondo 3.0 mm 7.1 mm Pitch del detettore 1.5 4.0 Pitch conico 0.375 0.25 Tempo di scansione (120-140mm) 40-45s 17-20s 5.71 mSv 6.82 mSv Dose Dose effettiva – maschio Dose effettiva – femmina 8.49 mSv 10.12 mSv Dose effettiva – maschio (modulazione) 2.8 mSv 3.41 mSv Dose effettiva – femmina (modulazione) 4.24 mSv 5.06 mSv Ricostruzione Spessore effettivo dello strato 1.25 mm 0.75-1.00mm Intervallo di ricostruzione 0.8 mm 0.5-0.6mm Finestre temporali di ricostruzione -350 ms; -400 ms ; -450 ms -350ms; -400ms ; -450ms Campo di vista - FOV 140-180 mm 140-180 mm Filtro di convoluzione medio medio Finestra (ampiezza/centro) 600/200 600/200 140 ml 100 ml Mezzo di contrasto Volume Velocità di somministrazione 3-4 ml/s 4-5 ml/s Tempo di somministr. Mdc 30-25s 25-20s Concentrazione Iodica 300-400 mgI/ml 300-400 mgI/ml Bolus chaser 40ml @ 4 ml/s 40ml @ 4 ml/s Accesso venoso Antecubitale Antecubitale Tempo totale somministr. 30/42.5 s 25/37.5 s elevati, tra il 5% ed il 32% dei segmenti non erano valutabili [9, 11,12,21,26-29]. Una serie di 102 pazienti si distingue da quelle citate riportando con due osservatori separati, una sensibilità, specificità pari a 86-93% e 9697%, rispettivamente senza esclusione di segmenti [30]. Il valore predittivo positivo, il valore predittivo negativo Results Table II summarises the data from the literature on the comparison between 4-row and 16-row MSCT and conventional coronary angiography in the evaluation of coronary artery stenosis. Four-row MSCT coronary angiography has 290 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato TABLE I.—Scan protocols for coronary angiography with multislice CT. Scanner Manufacturer Siemens Siemens Model Volume zoom Sensation 16 Type 4 slice 16 slice Detectors 4 16 Collimation 1 mm 0.75 mm KiloVolt 120 120 Scan MilliAmpere/s 400 400-500 Rotation time 500 ms 420 ms MAs modulation Systolic Systolic Actual temporal resolution 250 ms 210 ms Maximum termporal resolution* 125 ms 105 ms Feed/rotation 1.5 mm 3.0 mm Feed/second 3.0 mm 7.1 mm Detector pitch 1.5 4.0 Beam-cone pitch 0.375 0.25 Scan time (120-140mm) 40-45s 17-20s 5.71 mSv 6.82 mSv Effective dose – females 8.49 mSv 10.12 mSv Effective dose – males (modulation) 2.8 mSv 3.41 mSv Effective dose – females (modulation) 4.24 mSv 5.06 mSv Dose Effective dose – males Reconstruction Effective slice width 1.25 mm 0.75-1.00mm Reconstruction interval 0.8 mm 0.5-0.6mm Reconstruction time window -350 ms; -400 ms ; -450 ms -350ms; -400ms ; -450ms Field of view – FOV 140-180 mm 140-180 mm Convolution filter medium medium Window (amplitude/center) 600/200 600/200 Volume 140 ml 100 ml Administration speed 3-4 ml/s 4-5 ml/s Administration time (CM) 30-25s 25-20s Contrast medium Iodine concentration 300-400 mgI/ml 300-400 mgI/ml Bolus chaser 40ml @ 4 ml/s 40ml @ 4 ml/s Venous access Antecubital Antecubital Total administration time. 30/42.5 s 25/37.5 s e l’accuratezza diagnostica complessiva, sono rispet-tivamente tra 76-92%, 94-98%, e 79-98% [9, 11, 12, 21, 2629]. Gli studi di coronarografia con TC a 16 strati hanno fornito risultati migliori. In uno studio [18] nessun vaso di diametro superiore a 2 mm è stato escluso dall’analisi, al been performed on populations between 28 and 100 patients (pts), evaluating all vessels with a diameter ≥2 mm (or 1.5 mm in [26]; stenoses ≥50% were considered. In the visualization of coronary artery stenosis, the sensitivity ranged between 75% and 91% with a specificity between 76% and 99% [9, 11, 12, 21, 26-29]. Even though these diagnostic 291 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato TABELLA II. — Letteratura sulle casistiche di angiografia coronarica non invasiva mediante TC multistrato. N° paz. Excl. (%) Se. (%) Sp. (%) VPP (%) VPN (%) Acc. (%) Nieman K(12) Lancet ‘01 31 27 81 97 81 97 95 Achenbach S(9) Circulation ‘01 64 32 85 76 56 94 79 Knez A(38) AJC ‘01 44 6 78 98 84 96 94 Vogl TJ(28) Radiology ‘01 38 19 75 99 92 98 98 Giesler T(29) AJR ‘02 100 29 91 89 66 98 96 Nieman K(27) AJC ‘02 53 30 82 93 66 97 90 Kopp AF(30)* EHJ ‘02 102 0 93 97 81 99 96 Nieman K(21) Heart ‘02 78 32 84 95 67 98 93 Becker CR(26) JCAT ‘02 28 5 81 90 57 97 89 Nieman K(18) Circulation ‘02 58 0 95 86 80 97 97 Ropers D(19) Circulation ‘03 77 12 92 93 79 97 93 4-strati 16-strati Accuratezza diagnostica valutata nella rilevazione di stenosi significative, con riduzione del diametro uguale o superiore al 50%, e comparata con la coronarografia convenzionale come «gold standard». N° paz.: numero di pazienti inclusi nello studio; Excl.: percentuale di segmenti esclusi considerati non valutabili; Se.: sensibilità; Sp.: specificità; VPP: valore predittivo positivo; VPN: valore predittivo negativo; Acc.: accuratezza; AJR: American Journal of Roentgenology; EHJ: European Heart Journal; AJC: American Journal of Cardiology; JCAT: Journal of Computed Assisted Tomography; *Risultati dell’ osservatore con la migliore performance. contrario degli studi precedenti [9, 11, 12, 21, 27-30]. La sensibilità, la specificità, il valore predittivo positivo e negativo sono risultati rispettivamente 95%, 86%, 80%, e 97%. L’accuratezza complessiva nella valutazione del tronco comune della coronaria sinistra, della arteria discendente anteriore, della coronaria destra e della circonflessa, sono risultate 100%, 91%, 86%, e 81%, rispettivamente [18]. In un altro studio, solo il 12% dei segmenti di diametro uguale o superiore a 2 mm è stato escluso. Questo valore, apparentemente basso in senso assoluto, lo è sicuramente per il gruppo da cui proviene che era uso escludere tra il 29% ed il 32% dei vasi esaminati con la precedente generazione di scanner a 4 strati [9, 29]. I valori di sensibilità, specificità, valore predittivo positivo e negativo sono risultati 92%, 93%, 79%, e 97%, rispettivamente [19]. Discussione Le arterie coronarie e quindi le lesioni ad esse riferite sono di piccole dimensioni. Inoltre la pulsazione cardiaca concede una finestra temporale relativamente breve durante la quale il movimento è minimo. Le risoluzioni spaziale e tem- values may appear good, between 5% and 32% of all available segments was considered not assessable [9, 11, 12, 21, 26-29]. One series on 102 patients reports different results, with two readers’ sensitivity and specificity of 86-93% and 96-97%, respectively, without exclusion of any segment [30]. The positive and negative predictive value and the diagnostic accuracy were 76-92%, 94-98%, and 79-98%, respectively [9, 11, 12, 21, 26-29]. Studies performed using 16-row MSCT reported better results. In one study [18] no vessel with a diameter ≥2mm was excluded, differently from most previous studies [9, 11, 12, 21, 27-30]. The sensitivity, the specificity, the positive and negative predictive values were 95%, 86%, 80% and 97%, respectively. The overall accuracy in the evaluation of the left main (LM) artery, left anterior descending artery (LAD), right coronary artery (RCA) and circumflex (CX) were 100%, 91%, 86%, and 81%, respectively [18]. In another study, 12% of the vessels with diameter ≥2mm were excluded; this exclusion rate is low but it is even more important because it comes from the group that excluded 29% to 32% of the available vessels with 4-row MSCT [9, 29]. The sensitivity, specificity, positive and negative predictive values were 92%, 93%, 79%, and 97%, respectively [19]. 292 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato TABLE II.—Literature reports on series of non-invasice coronary angiography with multislice CT. N° paz. Excl. (%) Se. (%) Sp. (%) VPP (%) VPN (%) Acc. (%) Nieman K(12) Lancet ‘01 31 27 81 97 81 97 95 Achenbach S(9) Circulation ‘01 64 32 85 76 56 94 79 Knez A(38) AJC ‘01 44 6 78 98 84 96 94 Vogl TJ(28) Radiology ‘01 38 19 75 99 92 98 98 Giesler T(29) AJR ‘02 100 29 91 89 66 98 96 Nieman K(27) AJC ‘02 53 30 82 93 66 97 90 Kopp AF(30)* EHJ ‘02 102 0 93 97 81 99 96 Nieman K(21) Heart ‘02 78 32 84 95 67 98 93 Becker CR(26) JCAT ‘02 28 5 81 90 57 97 89 Nieman K(18) Circulation ‘02 58 0 95 86 80 97 97 Ropers D(19) Circulation ‘03 77 12 92 93 79 97 93 4-strati 16-strati Diagnostic accuracy for the detection of significant stenosis, with diameter reduction equal or more than 50%, compared with conventional coronary angiography as «gold standard». N° paz.: patient included in the study; Excl.: percentage of excluded segments; Se.: sensitivity; Sp.: specificity; VPP: positive predictive value; VPN: negative predictive value; Acc.: accuracy; AJR: American Journal of Roentgenology; EHJ: European Heart Journal; AJC: American Journal of Cardiology; JCAT: Journal of Computed Assisted Tomography; *Results of the observer with better performance. porale delle apparecchiature rappresentano quindi i principali fattori limitanti nell’imaging non invasivo delle arterie coronarie. Per questo motivo l’angiografia convenzionale ha rappresentato per molti decenni l’unica tecnica disponibile per lo studio di questi vasi. La EBT è dotata di elevata risoluzione temporale (50-100 ms), ma ha scarsa risoluzione spaziale lungo l’asse longitudinale (strati da 3 mm). Inoltre la scansione viene sincronizzata prospetticamente sul segnale ECG. Ciò rende la durata della scansione (e dell’apnea) dipendente dalla frequenza cardiaca. Quando questa è troppo bassa è necessario somministrare atropina per permettere di acquisire l’intero cuore durante una sola apnea. La RM è dotata di elevata risoluzione temporale (~50ms), ma caratterizzata da una risoluzione spaziale insufficiente a dimostrare le porzioni distali dei vasi coronarici. Lo sviluppo della tecnologia multistrato ha reso possibile l’impiego della TC per l’imaging vascolare non invasivo delle arterie coronarie. Ciò è stato possibile aumentando la risoluzione spaziale mediante l’impiego di spessori di strato di 1 mm. La risoluzione temporale è stata aumentata riducendo i tempi di rotazione del gantry al di sotto di 500 ms e con l’introduzione di algoritmi di ricostruzione delle immagini in grado di sfruttare solo 180 gradi della rotazione Discussion The coronary arteries and their lesions are small in size. Moreover, the heartbeat determines a relatively short temporal window during which motion is minimized. Therefore, spatial and temporal resolution represent the main limiting factors in the non-invasive evaluation of coronary artery imaging. For these reasons, conventional coronary angiography has remained for decades the only available technique for the study of the coronary tree. EBT is characterized by a high temporal resolution (50100ms) but with a low spatial resolution in the z-axis (3mm slice). Moreover the scan is performed using prospective ECG-triggering. For this reason, the scan time (and apnea) depends on the heart rate. When the heart rate is too low it may be necessary to administer atropine in order to scan the heart within a single breath-hold. Magnetic Resonance has a high temporal resolution (~50 ms), but it has an inadequate spatial resolution to visualize the distal segment of the coronary vessels. The development of multislice technology has enabled noninvasive coronary artery imaging with spiral CT, with an increased spatial resolution due to thinner collimations (1mm). The improvement of the temporal resolution is obtained with F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato 293 Fig. 5. — Esempio di placca aterosclerotica soft a livello della coronaria sinistra. Ricostruzione 3D con VR delle coronarie (A-D). Le ricostruzioni multiplanari con algoritmo MIP mostrano l’arteria coronaria di sinistra (E), la sua suddivisione nel ramo discendente anteriore (E-G) e circonflesso (H) e la coronaria di destra (I). A livello del tratto prossimale della ADA si osserva un ispessimento omogeneo della parete arteriosa settale, in assenza di lesioni calcifiche, da riferirsi a placca aterosclerotica «soft» (freccia). Example of soft aterosclerotic plaque of the left coronary artery. Threedimensional VR of the coronary arteries (A-D). Multiplanar MIP show the left coronary artery (E), its bifurcation in left anterior descending artery (E-G) and circumflex artery (H), and right coronary artery (I). In proximal ADA there is an homogeneous thickening of the septal wall of the artery, without calcified lesions, to be referred as “soft” atherosclerotic plaque (arrow). del tubo radiogeno. I risultati ottenuti con apparecchiature a 4 canali sono stati incoraggianti [9, 12], ma erano gravati da una elevata percentuale di vasi esclusi dalla valutazione a causa di artefatti. In molti studi la valutazione era limitata alle localizzazioni molto prossimali (LM e segmenti prossimali di ADA, Cx, e CDx) [31-35]. In particolare la visualizzazione delle porzioni intermedie di CDx e di Cx era difficoltosa a causa del movimento presente anche in fase telediastolica (fasi precoci della sistole atriale) e per la loro direzione cranio-caudale [27]. Ciò ha impedito l’impiego di questa tecnica nella routine. Questa tecnica è inoltre soggetta a artefatti da movimento che dipendono dalla frequenza cardiaca, e dagli artefatti legati alla presenza di calcificazioni coronariche [21-27]. Lo sviluppo di apparecchiature a 16 strati ha ovviato a questi inconvenienti proponendo la TC per la valutazione non invasiva delle arterie coronarie su larga scala (fig. 5). I risultati ottenuti indicano che è possibile effettuare una valutazione completa e accurata di tutti i vasi coronarici nella maggior parte dei pazienti [18, 19]. Nei pazienti con fibrillazione atriale o con frequenza cardiaca superiore a 70 bpm sono state introdotte le ricostruzioni multi-segmentarie (già disponibili anche sulle apparecchiature a 4 strati). Con questo algoritmo di ricostruzione, invece di utilizzare tutti i dati dal medesimo ciclo cardiaco, una immagine viene ricostruita impiegando segmenti provenienti da cicli cardiaci contigui. Questa tecnica è tuttavia influenzata da alcuni fattori. In essa si assume che la posizione del cuore sia identica tra due o più cicli cardiaci adiacenti. Questa precisione millimetrica tra un ciclo e l’altro è meno probabile in caso di frequenza cardiaca elevata. Inoltre, la ricostruzione multisegmentaria presuppone l’impiego di dati più distanti tra loro lungo l’asse longitudinale a causa dello spostamento del tavolo tra un ciclo e l’altro. Una interpolazione di scansioni più vicine può essere ottenuta aumentando la collimazione o riducendo la velocità del tavolo con un aumento del tempo di scansione ed in ultima analisi delle radiazioni somministrate al paziente. Un aumento della velocità di rotazione del tubo radiogeno sarebbe la soluzione ideale per ottenere risoluzioni temporali effettive pari o inferiori ai 150 ms (pari ad un tempo di rotazione del tubo radiogeno di 300 ms). Ciò ridurrebbe inoltre la necessità di somministrazione di farmaci beta-bloccanti prima dell’esame. Tra i limiti attuali della tecnica ricordiamo la difficile visu- a faster rotation time (<500ms) and with dedicated reconstruction algorithm, which uses information from half rotation (180°). Promising results have been reported with 4-row MSCT [9, 12], but a high rate of vessel exclusion due to the presence of artifacts was also reported. In many reports, the evaluation was limited to the proximal portion of the coronary arteries [31-35]. In particular, the visualization of mid portion of RCA and CX was difficult because of motion artifacts during 294 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato Fig. 6. – Esempio di follow-up di bypass aorto-coronarico. In A è mostrata la vista anteriore di un bypass coronarico confezionato con arteria mammaria interna sinistra (AMIS) per un ramo diagonale della coronaria discendente anteriore (freccia). Il ramo diagonale appare lievemente stirato verso l’alto dal bypass. Nel medesimo paziente (B e C) è presente anche un graft venoso (VGS) che decorre tra la vena cava superiore e atrio destro, per anastomizzarsi distalmente sulla faccia posteriore del cuore sulla arteria discendente posteriore (ramo della coronaria destra che decorre nel solco interventricolare posteriore. Si nota chiaramente il flusso retrogrado nel tratto distale della CDx (C). Follow-up of a coronary by-pass. A by-pass from the left internal mammary artery (AMIS) to a diagonal branch of the anterior descendent artery (arrow) is shown is A. The diagonal branch is slightly stretched upwards from the by-pass. In the same patient (B and C) a venous graft (VGS) is also present running between the superior vena cava and the right atrium, flowing into the posterior descendent artery in the posterior aspect of the heart. Retrograde flow is visible in the distal tract of the CDx (C). alizzazione degli stent e delle calcificazioni. La valutazione degli stent è soggetta, infatti, ad artefatti derivanti dal materiale e dal diametro dello stent utilizzato. Il materiale impiegato ha generalmente elevato coefficiente di attenuazione. Ciò lo fa apparire più grande di quanto effettivamente non sia, determinando il cosiddetto effetto «blooming». Questo effetto può impedire la visualizzazione di iperplasie intimali o del flusso all’interno di stent di piccolo calibro. L’impiego di adeguati filtri di ricostruzione può attenuare l’effetto «blooming». Un’alternativa definitiva sarebbe quella di impiegare materiali che non provochino artefatti. Per ciò che concerne le calcificazioni, si ha lo stesso problema citato per gli stent. Ossia, quando la calcificazione del vaso è estesa e di dimensioni notevoli, a causa del “blooming”, il lume vascolare non è valutabile in modo appropriato. L’utilizzo di filtri più elevati può mitigare questo effetto soprattutto se abbinato all’utlizzo di collimazioni di spessore inferiore. Le clip chirugiche, rilevate lungo il decorso dei bypass (soprattutto arteriosi) pongono problematiche simili (fig. 6). Le prospettive future di sviluppo sono rappresentate sostanzialmente da un ulteriore miglioramento delle risoluzioni spaziale e temporale. L’aumento del numero di detettori, pur comportando una riduzione del tempo di scansione, non implicherebbe un significativo miglioramento della qualità dell’immagine e introdurrebbe ulteriori sforzi nella correzione del fascio conico. I cosiddetti “flat panel detector” hanno invece dimostrato in studi effettuati in laboratorio di produrre un evidente miglioramento dell’immagine ovviando a tutti gli inconvenienti sopra descritti. Le the late diastolic phase (early phase of atrial systolic contraction) and for their vertical direction [27]. Furthermore, this technique was limited by cardiac motion artifacts and by the presence of consistent coronary artery calcifications [21, 27]. All these reasons have limited its routine use. The introduction of 16-row MSCT overcomes several limitations proposing it as a clinical tool for the non-invasive evaluation of coronary arteries (fig. 5). The reported data show the capability of the 16-row MSCT scanner to evaluate all coronary artery segments in most of the patients [18, 19]. In the case of high heart rate (>70bpm) and atrial fibrillation multi-segmental reconstruction algorithms are available. Unfortunately, multi-segmental reconstructions have some limitations: between contiguous heart beats it is assumed that the heart position is exactly the same, but this is less probable at higher heart rates. Multisegmental reconstruction requires data that are far apart from each other along the z-axis because of table’s motion between two or more contiguous cardiac cycles. Data interpolation can be achieved by increasing collimation or reducing the table feed, but with an increased scan time and exposure radiation of the patient. An increased rotation time should be the right solution in order to obtain an effective temporal resolution of 150 ms (rotation time of 300 ms). Then, it could be possible to reduce the administration of beta-blockers prior to the scan. Stents and calcifications still remain a field where the evaluation capability of MSCT is limited. The evaluation of stents is limited by artifacts due to the F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato dosi elevate, e i tempi di rotazione (~30 s) non permettono ancora il loro impiego clinico. In conclusione, l’angiografia coronarica non invasiva con tomografia computerizzata spirale a 16 detettori si aggiunge alla coronarografia convenzionale nella diagnosi e nel follow-up del paziente con patologia coronarica sospetta o nota. La coronarografia TC può trovare impiego nei pazienti a rischio elevato e/o con sintomatologia aspecifica, nei quali non sia possibile eseguire una angiografia coronarica convenzionale per i rischi eccessivi nei quali incorrerebbero. Un ulteriore impiego di questa tecnica è rappresentato dal follow-up di pazienti sottoposti a procedure invasive come il posiziona-mento di stent o di bypass coronarico. Con tale metodica è inoltre attualmente in corso la valutazione dell’effetto sulla placca delle terapie farmacologiche ipo-lipemizzanti orali, delle cavità cardiache (frazione di eiezione e motilità del ventricolo sinistro) e delle valvole native e protesiche [36, 37]. Infine è comunque fondamentale che questo tipo di esame sia gestito da una equipe dedicata basata sulla collaborazione tra specialisti radiologo e cardiologo. Abbreviazioni nelle figure ADA AD AS AMIS Ao AP CDx Cx Arteria Discendente anteriore Atrio destro Atrio sinistro Arteria mammaria interna sinistra Aorta Arteria Polmonare Arteria Coronaria Destra Arteria circonflessa Bibliografia/References 1) Passariello R, De Santis M: Coronary artery disease. Update and prospects of radiologic imaging with CT and MR. Radiol Med 101: 411-423, 2001. 2) Traversi E, Aldrovandi A, Barazzoni G et al: Non-invasive coronary angiography by multislice computed tomography: a new diagnostic method? Ital Heart J 3: 665-668, 2002. 3) Achenbach S, Kessler W, Moshage WE et al: Visualization of the coronary arteries in three-dimensional reconstructions using respiratory gated magnetic resonance imaging. Coron Artery Dis 8: 441448, 1997. 4) Achenbach S, Moshage W, Bachmann K: Noninvasive coronary angiography by contrast-enhanced electron beam computed tomography. Clin Cardiol 21: 323330, 1998. 5) van Geuns RJ, Wielopolski PA, de Bruin HG et al: MR coronary angiography with breath-hold targeted volumes: preliminary clinical results. Radiology 217: 270-277, 2000. D1 M1 Feg SC TC TEVD VD VGS VS Primo ramo diagonale Primo ramo marginale Fegato Seno coronario Tronco comune Tratto di efflusso del ventricolo destro Ventricolo destro Vena grande safena Ventricolo sinistro 6) Rensing BJ, Bongaerts A, van Geuns RJ et al: Intravenous coronary angiography by electron beam computed tomography: a clinical evaluation. Circulation 98: 2509-2012, 1998. 7) Kim WY, Danias PG, Stuber M et al: Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med 345: 1863-1869, 2001. 8) Romagnoli A, Nisini A, Gandini R et al: Multidetector row CT coronary an-giography: technique and preliminary experience. Radiol Med 103: 443-455, 2002. 9) Achenbach S, Giesler T, Ropers D et al: Detection of coronary artery stenoses by contrast-enhanced, retrospectively electrocardiographically-gated, multislice spiral computed tomography. Circulation 103: 2535-2538, 2001. 10) Achenbach S, Ulzheimer S, Baum U et al: Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation 102: 2823-2828, 2000. 11) Knez A, Becker C, Ohnesorge B et al: Noninvasive detection of coronary artery stenosis by multislice helical com- 295 material of the stent (high density) and to its diameter. Because of the so-called “blooming” artifact the stent walls appear larger than they really are. This artifact can prevent the optimal evaluation of intimal hyperplasia and stent endoluminal flow. The use of dedicated kernel can reduce the blooming artifact. An ideal alternative could be the use of different stent material with lower attenuation values. Calcifications of coronary arteries can also determine blooming artifacts, in particular when they are large, therefore limiting the evaluation of vessel lumen. This problem can be reduced by using a higher reconstruction kernel and thinner collimation. Similarly, surgical clips around the arterial coronary bypass can cause the same artifacts (fig. 6). The future developments of MSCT technology are towards a higher spatial and temporal resolution. In fact, an increased number of detectors allows a shorter scan time but it does not improve image quality (e.g. in-plane temporal resolution), with more problems regarding cone beam correction. The new «flat panel detectors» have shown to improve image quality in laboratory tests, overcoming many previous limitations. The high radiation exposure and slow rotation time (~30s) do not yet allow their clinical use. In conclusion, non-invasive coronary angiography with 16-row MSCT is an alternative diagnostic tool in the evaluation of coronary artery and in the follow-up of patients with known or suspected coronary artery disease. Coronary MSCT angiography can be applied in patients with high risk and/or non-specific symptoms, in which conventional coronary angiography is considered too far because of its inner risk. A further role of this technique could be in the follow-up of patients who have undergone endo-vascular procedures, such as stent implantation and surgical myocardial re-vascularization. The evaluation of oral lipid-lowering drugs on atherosclerotic plaques, of cardiac chambers (ejection fraction and left ventricle motion) and native or graft valves with MSCT is currently in progress [36, 37]. This diagnostic tool requires close co-operation between the radiologist and cardiologist in order to perform appropriately. puted tomography. Circulation 101: E221222, 2000. 12) Nieman K, Oudkerk M, Rensing BJ et al: Coronary angiography with multislice computed tomography. The Lancet 357: 599-603, 2001. 13) Hong C, Becker CR, Huber A et al: ECG-gated reconstructed multi-detector row CT coronary angiography: effect of varying trigger delay on image quality. Radiology 220: 712-717, 2001. 14) Heuschmid M, Kuttner A, Flohr T et al: Visualization of coronary arteries in CT as assessed by a new 16 slice technology and reduced gantry rotation time: first experiences. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 174: 721-724, 2002. 15) Flohr T, Stierstorfer K, Bruder H et al: New technical developments in multislice CT-Part 1: Approaching isotropic resolution with sub-millimeter 16-slice scanning. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 174: 839-845, 2002. 16) Flohr T, Bruder H, Stierstorfer K et al: New Technical Developments in Multislice CT, Part 2: Sub-Millimeter 16Slice Scanning and Increased Gantry Rotation Speed for Cardiac Imaging. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 174: 1022-1027, 2002. 17) Cademartiri F, Nieman K, Raaymakers RH et al: Non-invasive demonstration of coronary artery anomaly performed using 16-slice multidetector spiral computed tomography. Ital Heart J 4: 5659, 2003. 18) Nieman K, Cademartiri F, Lemos PA et al: Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography. Circulation 106: 2051-2054, 2002. 19) Ropers D, Baum U, Pohle K et al: Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstruction. Circulation 107: 664-666, 2003. 20) Kachelriess M, Ulzheimer S, Kalender WA: ECG-correlated image reconstruction from subsecond multi-slice spiral CT scans of the heart. Med Phys 27: 1881-1902, 2000. 296 F. Cademartiri et al: Angiografia coronarica non invasiva con Tomografia Computerizzata spirale multistrato 21) Nieman K, Rensing BJ, van Geuns RJ et al: Non-invasive coronary angiography with multislice spiral computed tomography: impact of heart rate. Heart 88: 470-474, 2002. 22) Jakobs TF, Becker CR, Ohnesorge B et al: Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG-controlled tube current modulation. Eur Radiol 12: 1081-1086, 2002. 23) Flohr T, Kuttner A, Bruder H et al: Performance Evaluation of a Multi-Slice CT System with 16-Slice Detector and Increased Gantry Rotation Speed for Isotropic Submillimeter Imaging of the Heart. Herz 28: 7-19, 2003. 24) Kopp AF, Schroeder S, Kuettner A et al: Coronary arteries: retrospectively ECG-gated multi-detector row CT angiography with selective optimization of the image reconstruction window. Radiology 221: 683-688, 2001. 25) Halliburton SS, Stillman AE, Flohr T et al: Do segmented reconstruction algorithms for cardiac multi-slice computed tomography improve image quality? Herz 28: 20-31, 2003. 26) Becker CR, Knez A, Leber A et al: Detection of coronary artery stenoses with multislice helical CT angiography. J Comput Assist Tomogr 26: 750-755, 2002. 27) Nieman K, Rensing BJ, van Geuns RJ et al: Usefulness of multislice computed tomography for detecting obstructive coronary artery disease. Am J Cardiol 89: 913-918, 2002. 28) Vogl TJ, Abolmaali ND, Diebold T et al: Techniques for the detection of coronary atherosclerosis: multi-detector row CT coronary angiography. Radiology 223: 212-220, 2002. 29) Giesler T, Baum U, Ropers D et al: Noninvasive visualization of coronary arteries using contrast-enhanced multidetector CT: influence of heart rate on image quality and stenosis detection. AJR 179: 911-916, 2002. 30) Kopp AF, Schroeder S, Kuettner A et al: Non-invasive coronary angiography with high resolution multidetectorrow computed tomogra-phy. Results in 102 patients. Eur Heart J 23: 1714-1725, 2002. 31) Schroeder S, Kopp AF, Ohnesorge B et al: Accuracy and reliability of quantitative measurements in coronary arteries by multi-slice computed tomography: experimental and initial clinical results. Clin Radiol 56: 466-474, 2001. 32) Schroeder S, Kopp AF, Baumbach A et al: Noninvasive detection and evaluation of atherosclerotic coronary plaques with multislice computed tomography. J Am Coll Cardiol 37: 1430-1435, 2001. 33) Schroeder S, Flohr T, Kopp AF et al: Accuracy of density measurements within plaques located in artificial coronary arteries by X-ray multislice CT: results of a phantom study. J Comput Assist Tomogr 25: 900-906, 2001. 34) Schroeder S, Kopp AF, Baumbach A et al: Non-invasive characterisation of coronary lesion morphology by multislice computed tomography: a promising new technology for risk stratification of patients with coronary artery disease. Heart 85: 576-578, 2001. 35) Kopp AF, Schroeder S, Baumbach A et al: Non-invasive characterisation of coronary lesion morphology and composition by multislice CT: first results in comparison with intracoronary ultrasound. Eur Radiol 11: 1607-1611, 2001. 36) Willmann JK, Kobza R, Roos JE et al: ECG-gated multi-detector row CT for assessment of mitral valve disease: initial experience. Eur Radiol 12: 2662-2669, 2002. 37) Willmann JK, Weishaupt D, Lachat M et al: Electrocardiographically gated multi-detector row CT for assessment of valvular morphology and calcification in aortic stenosis. Radiology 225: 120-128, 2002. 38) Knez A, Becker CR, Leber A et al: Usefulness of multislice spiral computed tomography angiography for determina-tion of coronary artery stenoses. Am J Cardiol 88: 1191-1194, 2001. Dott. F. Cademartiri Viale Rustici, 2 43100 Parma PR Tel. 0521/961833 E-mail:[email protected]
© Copyright 2026 Paperzz