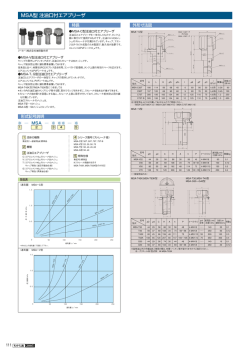
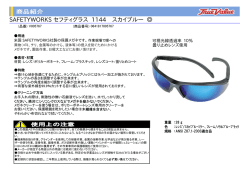
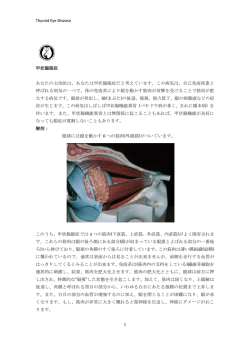
ISSN 1881-901X INCLUDED IN THIS ISSUE Full Articles パーキンソン病患者にみられる中枢神経系以外の病変 多系統萎縮症の診断を目的とした神経画像の基準案 Abstracts 初期パーキンソン病患者に対する 6-[18F]Fluoro-L-dopa 取り込みの 追跡調査で示された被殻における非直線性の進行パターン 他 7 本収載 日本語版 Vol.3 No.2 November 2009 e-mail: [email protected] 日本語版 Vol.3 No.2 November 2009 監修: 水野 美邦 順天堂大学医学部附属 順天堂越谷病院院長 編集委員: 宇川 義一 福島県立医科大学医学部 髙橋 良輔 京都大学医学研究科臨床神経学教授 (五十音順) 神経内科学講座教授 野元 正弘 愛媛大学大学院医学系研究科 病態治療内科教授 梶 龍兒 徳島大学医学部神経内科教授 近藤 智善 公立大学法人和歌山県立医科大学 服部 信孝 順天堂大学医学部脳神経内科教授 神経内科教授 山本 光利 香川県立中央病院神経内科主任部長 Full Articles パーキンソン病患者にみられる中枢神経系以外の病変 2 多系統萎縮症の診断を目的とした神経画像の基準案 10 Abstracts 初期パーキンソン病患者に対する6-[18F]Fluoro-L-dopa パーキンソン病患者の死亡率:20年間の追跡調査研究 34 パーキンソン病患者の嗅上皮生検 36 取り込みの追跡調査で示された被殻における非直線性の 進行パターン 26 パーキンソン病患者のQOLに対する淡蒼球または 視床下部深部脳刺激の長期効果 28 進行期パーキンソン病に対するレボドパの十二指腸内投与: 患者の特徴,適応,有効性,安全性 38 パーキンソン病患者にみられる体重減少と1日の エネルギー消費量および身体活動量との関連性 30 進行期パーキンソン病患者の運動機能および筋電図での サイレントピリオドに対するDBS,前運動野rTMS, レボドパの効果 多系統萎縮症患者の拡散強調画像: 臨床サブタイプ間の比較 40 32 表紙:第13回Movement Disorder Society国際学会の2009年パリ開催記念。 1889年のパリ万博のために新たに建てられた建造物や記念碑がたち並ぶ 1900年当時のパリ市街地図。 (New York Public Library.出典:Garnier Freres, 1900) Selected from Movement Disorders Vol. 24 No. 5-8, 2009 パーキンソン病患者にみられる中枢神経系以外の 病変 Lesions Outside the CNS in Parkinson’s Disease *, ** Ruth Djaldetti, MD, Nirit Lev, MD, and Eldad Melamed, MD * Department of Neurology, Rabin Medical Center, Beilinson Campus, Petah Tiqva, Israel The Norma and Alan Aufzien Chair for Research of Parkinson’s Disease, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel * * パーキンソン病(Parkinson’ s disease; PD)は,黒質 いる。この脳以外の器官には,主に消化管,心臓,腎臓, 緻密部のドパミン作動性ニューロンの消失だけで誘発さ 泌尿生殖器系,皮膚がある。そのほか,PD で障害され れるような単純な運動障害ではない。おそらく,黒質は る CNS 以外の器官として眼や副腎がある。本稿では, PD における唯一の脳損傷領域でもなければ,最初に損 PD で認められる脳以外の所見について,解剖学的・生 傷を受ける領域でもないと考えられる。また,過去およ 理学的・臨床的特徴を見直し,PD の病因および発症機 び最近の研究では,PD の神経変性過程は非常に広範に 序との関連性を報告する。本稿では PD を全身性の わたり,中枢神経系(central nervous system; CNS) CNS・末梢障害と捉え,PD の発症原因と進行に関する だけでなく末梢自律神経系や,末梢自律神経系の支配下 新しい仮説の妥当性を示した。 にある脳以外の器官にも影響が及ぶことが証明されて Movement Disorders, Vol. 24, No. 6, 2009, pp. 793–800 Key Word パーキンソン病,自律神経系,末梢器官 こ の 10 年 の 間 に, パ ー キ ン ソ ン 病(Parkinson’ s 最近の研究では,PD の神経変性過程は非常に広範で, disease; PD)の臨床像と進行に対する解釈は革新的な変 中枢神経系(central nervous system; CNS)だけでなく, 化を遂げた。当初,PD は黒質緻密部(substantia nigra 末梢の自律神経系回路にも影響することが報告されてい pars compacta; SNpc)のドパミン作動性ニューロンの消失 る。PD 患者では自律神経症状が高率にみられることが膨 を特徴とする,単純な運動障害と考えられていた。現在 大な証拠から確認されているが,その理由は広範な神経 では,運動性・非運動性症状を伴う複雑な多巣性神経変 変性によって説明できる。CNS 以外で障害が最も顕著に 性疾患であることが広く認められている。おそらく,黒 認められるのは,末梢の自律神経系(autonomic nervous 質は PD における唯一の脳損傷領域でもなければ,最初 system; ANS)に支配される器官と,カテコールアミン作 に損傷を受ける領域でもないと考えられる。Braak ら は 動性ニューロンを含む器官である。 1 PD 進行過程の病理学的病期を詳細に報告し,重要かつ 本稿では,PD で障害が認められる CNS 以外の器官に 大きな影響力をもつ研究成果をあげた。Braak らは,PD ついて,病変の解剖学的・生理学的・臨床的特徴に焦点 の特徴であるニューロン内のα - シヌクレイン凝集は下 を当て, PD の病因および発症機序との関連性を報告する。 位脳幹,特に迷走神経背側核と嗅球に始まり,徐々に脳 幹上部に広がり,疾患の後期(第 3 期)になってようや く SNpc に至ることを確認した。Saito ら 2 は,PD 患者の α- シヌクレイノパチーが延髄に始まることを確認した。 2 PD における自律神経系の障害 ANS は解剖学的に副交感神経系と交感神経系に分けら R.Djaldetti et al. れる。副交感神経系の中心部分は,迷走神経背側核と仙 特に response fluctuation がみられる患者で胃排出時間の 髄部の側角細胞である。これらの構造から出る節前線維 短縮が報告された 17,18。胃排出時間が延長した場合でも, は,胸壁,腹壁,骨盤内臓器の神経節に到達する。節後 薬物動態学的な影響を伴う。胃が収縮不良になると,レ 線維は心臓,食道,胃,結腸,膀胱,腎臓の平滑筋を活 ボドパ(L—ドパ)の十二指腸への到達が妨げられ,吸収 性化する役割をもつ。交感神経系の中心部分は,脊髄の が遅延し,阻害されることさえある。その結果, 「delayed 中間外側細胞柱に始まる。節前神経は末梢の脊椎傍神経 on」 (L—ドパ投与から臨床効果発現までの時間が長くなる 節に入り,節後線維は心臓,消化管,膀胱などの末梢器 こと)や「no on」 (L—ドパを投与しても患者を「薬効 on」 官まで伸びている。 状 態 に で き な い こ と ) な ど, い く つ か の タ イ プ の PD では一部の末梢器官に広範な障害が認められる。 fluctuation が生じる 19。胃不全麻痺は運動促進剤で治療 これらの器官には,ANS の支配を受ける食道,胃,結腸, できるが,副作用のためにその使用は制限される。この 心臓,膀胱,皮膚のほか,カテコールアミン作動性ニュー ほか,上部消化管での L—ドパ滞留を回避する方法として, ロンを含む眼,副腎がある。 Duodopa の投与(L—ドパの十二指腸内持続投与)20,ア ポモルフィンの皮下注射 21,rotigotine パッチ剤の使用 22 消化管 がある。 消化管の末梢コリン作動性副交感神経支配は,アウエ 結腸 ルバッハ筋層間神経叢とマイスネル粘膜下神経叢の 2 つ PD 患者の結腸の筋層間神経叢および粘膜下神経叢に の神経叢に由来する。これらの神経叢は蠕動波に関与し Lewy 小体が存在することは,1987 年に最初に報告され 23, ており,主な神経伝達物質はアセチルコリンである。 他の研究でも確認されている 4,24。また,筋層間神経叢の ドパミン作動性ニューロンの数が少なく,残存ニューロ 食道 ンには Lewy 小体が存在することも報告されている 24。神 研究初期には,消化管症状のない PD 患者と嚥下障害 経変性疾患のない患者から得た腹部・骨盤部の 100 手術 患者の食道のアウエルバッハ神経叢に Lewy 小体の所見 標本の研究では,9%の標本で腹部・骨盤部神経叢にα - が認められたことで ,PD における自律神経障害の関 シヌクレイン凝集を認めたが,Lewy 小体は検出されな 与が証明された。PD 患者のほぼ 80%に嚥下障害がみら かった。α - シヌクレイン凝集陽性の患者には心臓交感 れる 。バリウム嚥下検査では,口腔期,咽頭期ともに 神経症状が認められ,1 例では線条体の [123I]Ioflupane 取 患者の 79 ~ 95%に異常がみられる。口腔期の嚥下障害 り込みが減少しており,パーキンソニズムであることが は PD に関連する物理的障害の影響を受け,咽頭期には 示された 25。 3–6 7,8 咽頭と食道に運動障害がみられるのが特徴である 9–12。 多数の電気生理学的試験および結腸通過試験では,PD PD 患者の 78%で,嚥下障害が一因と考えられる口腔内 患者の 80%超で結腸通過時間が異常に長いことが明らか の唾液過剰や流涎が報告されている にされている 26,27。この所見と臨床的に相関する症状は便 。唾液分泌量は 13,14 ボツリヌス毒素の耳下腺内注射によって減らすことがで 秘であり,患者の最大 30 ~ 60%で報告されている 14,28–30。 きるが,一方で嚥下障害を悪化させる可能性がある 15。 一部の研究者は,便秘が PD の運動症状に先行する場合 もあることを示唆している。PD 患者 12 名を対象とした 胃 研究では,7 名が PD と診断されるまでの平均 16 年間便 胃に Lewy 小体が存在するという報告は 1 件しかない 5。 秘を訴えていた 31。若年時の便秘も PD の危険因子であ しかし,最近,PD 患者の胃のマイスネル粘膜下神経叢 ると思われる。男性 6,790 名のコホート研究では,重度 のニューロンで,α - シヌクレイン免疫反応陽性封入体 の便秘を呈する者は,平均 12 年間の追跡調査終了後に が検出された 。胃の自律神経障害による主な臨床症状 PD を発症するリスクが 4.5 倍高かった 32。便秘が PD の は,胃排出障害(胃不全麻痺)である。患者は,悪心, 危険因子であるのか,または便秘が PD の基礎にある病 早期満腹感, 腹部不快感, 腹部膨満感を訴えることが多い。 理生理学的プロセスに関連する初期徴候であるのかを判 胃の核吸収試験(nuclear absorption study)では, PD 患者, 断するには,さらなる研究が必要である。 16 3 パーキンソン病患者にみられる中枢神経系以外の病変 便秘はドパミン作動薬にはあまり反応せず,L—ドパ投 末梢 ANS が,MSA では中枢 ANS が障害されることで説 与によって悪化する場合もある。ドパミンアゴニストや 明できる。したがって,心イメージングは PD を早期発 抗コリン薬による悪化はさらに多くみられる。このため, 見し,2 種類のシヌクレイノパチーを鑑別するためのバ 排便回数を減らす作用のある薬剤の投与中止が第一の治 イオマーカーとして有用である。 療戦略となる。このほか,患者の食事・運動習慣の改善や, 浸透圧性緩下剤の投与という選択肢もある。 PD では,副交感神経の心臓活動が障害されても症状 が現れない場合がある。異常を検出できるのは,バルサ ルバ法,深呼吸に対する心拍数変動の検査,head-up tilt 心 臓 試験などの客観的検査だけである。しかし,このような 変化はおそらく心臓副交感神経の機能低下というよりも, PD 患者の心臓解剖標本の研究では,チロシン - ヒドロ 年齢や投薬によるものである 40。交感神経循環不全に伴 キシラーゼ陽性および陰性の神経突起において,Lewy う心臓コリン作動性交感神経支配を評価するために,PD 小体およびα - シヌクレイン陽性の神経突起が認められ 患 者 12 例を 対 象とし て 定 量 的 軸 索 反 射 性 発 汗 試 験 た。この研究結果を受け,PD 患者の心臓における交感神 (quantitative sudomotor axon reflex test; QSART)が行われ 経障害が確認された 。食道や結腸とは対照的に,PD 33,34 たが,全例で異常は認められなかった。この結果から, 患者の心臓では副交感神経系の障害を示す病理学的証拠 PD の交感神経系病変がコリン作動性神経ではなく,節後 は認められていない。 のカテコールアミン作動性神経の消失によるものである PD では心臓交感神経の異常がよくみられる。食後低 ことが示唆された 51。 血圧,運動誘発性低血圧,心拍数変動の障害,不整脈に 加え,患者の 20 ~ 50%には起立性低血圧がみられる。 このような心臓所見は,きわめて初期の PD 患者でも報 告されており 35,36,必ずしも投薬による副作用には関連し ないと考えられる 。 PD の尿路症状は,末梢自律神経ニューロンの損傷によ り説明できると考えられる。健康成人の腹部骨盤部自律 37,38 交感神経の除神経に伴う生化学的特徴として,ノルア 神経叢のα - シヌクレイン凝集を検討した横断的病理学 ドレナリン注入に対する過敏性,head-up tilt 試験※におけ 的研究では,膀胱前立腺標本の 26%が陽性であった 25。 るアルギニンバソプレッシン反応の保持,起立性低血圧 排尿障害は各研究によって 27 ~ 71%と幅があるもの 患者での血中ノルアドレナリン濃度の低下がある 。臨 39,40 の,PD 患者に高率にみられ 52–56,刺激症状が主体である。 床で日常的に利用される自律神経機能検査で異常が検出 尿路症状のうち最も多いのが夜間頻尿で 55,57,尿意切迫 されなかった一方,ノルアドレナリンの生理的アナログ (33 ~ 54%) ,頻尿(16 ~ 36%) ,切迫性尿失禁 53,55,56 と続 である MIBG およびフルオロドパミンを用いた心臓の く。臨床症状は,膀胱充満の初期にみられる不随意性排尿 6-[ F]-PET 試験で,心臓のリガンド取り込みが初期 PD 筋収縮(排尿筋反射亢進)の尿流動態所見と相関する 58。 患者で既に減少していたとの報告がある 41–44。画像所見 PD における尿路症状と運動症状との関係は,まだ明ら 18 は,寡動,発症時年齢,罹病期間と相関したが,性別, かにされていない。尿路症状が PD の進行ではなく年齢 筋強剛,姿勢安定性とは相関しなかった と相関することを示した研究もあるが 55,59,神経学的機能 。以上の結 45,46 果は,自律神経症状が四肢・体幹の寡動の重症度と相関 することを示した臨床試験と合致するが,振戦または硬 直とは合致しない 47,48。 MSA)の患者では,心臓の MIBG および [ F]- ドパミン 18 取り込みに異常はみられない 49,50。この違いは,PD では ※ 障害と PD 病期との相関を報告した研究もある 53,60,61。 PD 患者の尿路機能障害に関してはいくつかの理由が 考えられるが,最も広く受け入れられているのは,大脳 PD と異なり,多系統萎縮症(multisystem atrophy; 4 膀 胱 日本語版注釈:傾けた台の上に立ってもらい,下肢に血液を貯め て心臓への血流を低下させて自律神経調節機構を刺激し,徐脈・ 血圧低下を促すことで失神の要因を調べる検査。 基底核の出力が排尿反射を抑制し,PD における SNpc の 細胞消失が排尿筋を不安定にするというものである 58。 神経性の膀胱症状,特に尿意切迫と頻尿の治療には抗 コリン作動薬が用いられる。膀胱機能に対する L—ドパお よびアポモルフィンの作用を検討した複数の研究では, 相反する結果が得られている 58,62,63。視床下核に対する深 R.Djaldetti et al. 部脳刺激(deep brain stimulation of the subthalamic nucleus; (interplexiform cell)の主要神経伝達物質である 81,82。こ DBS-STN)も,膀胱機能を改善する可能性がある 64–66。 のため,目立った視覚異常は存在しないものの,PD 患者 両側 DBS-STN を施行した患者を対象とした膀胱充満時 の網膜および視覚伝導路については広範な研究が行われ の尿流動態検査では,膀胱充満感の正常化とともに感覚 ている。 障害の改善が認められた PD 患者に最もよくみられる視覚異常は,色の識別能力, 。 67,68 時空間コントラスト感度,色の輪郭知覚の低下である 83–85。 皮 膚 色の識別能力低下と PD の重症度および罹病期間との関 係については,依然として不明なままである。それは, 皮膚の無髄自律神経線維は交感神経節鎖に始まり,末 ほとんどの研究でサンプルサイズが小さく,また試験時 梢神経内を進んで最終標的(血管,汗腺,立毛筋,毛嚢) 点で患者が既に抗 PD 治療薬を投与されていることが結 に到達する。この神経線維はノルアドレナリン作動性で, 果に影響すると考えられるからである。色覚障害と線条 例外として汗腺を支配する神経はコリン作動性である。 体の [123I] β -CIT SPECT 取り込みとの間に相関がなかっ 皮膚はアクセスが容易な組織であるが, これまでのところ, たことから,色覚障害はドパミン作動性黒質線条体変性 PD における皮膚障害を検討した試験はごくわずかであ とは直接関係せず,おそらく黒質以外の病変が関与して る。PD 患者 22 例を対象として,汎神経マーカー PGP 9.5 いると考えられる 86。網膜レベルでは,明所視,暗所視, で免疫染色した皮膚生検検体の試験では,ANS 支配下の パターン刺激網膜電図に変化がみられ,いずれも PD の あらゆる皮膚要素で著明な除神経が認められた。興味深 臨床病期との相関が認められている 87。 いことに,汗腺と血管が最も影響を受けていたが,この所 このような異常は,CNS のドパミン欠乏だけでなく, 見は多汗症や起立性低血圧の訴えとは相関しなかった 。 網膜のドパミン欠乏に起因するものと考えられる。PD 患 別の研究では,PD 患者 16 例の上臀部の皮膚生検検体の 者(8 眼)の網膜を対象とした研究では,対照群に比し 一部でα - シヌクレインが検出されたものの,PD の重症 てドパミン量の有意な減少が認められたが,ドパミン代 度との相関は認められなかった 。 謝 産 物 の ジ ヒ ド ロ キ シ フ ェ ニ ル 酢 酸 69 70 多汗症および体温調節障害は,PD 患者にみられる自律 (dihydroxyphenylacetic acid; DOPAC) ,ホモバリニン酸 神経機能障害の非運動症状に含まれる。発汗異常の発現 (homovanillic acid; HVA)の減少はみられなかった 88。死 頻度は 30 ~ 50%と推定され 71,一部の患者では多量の 後に L—ドパを投与した剖検例 3 例では,対照群と比較し 発汗が最も厄介な症状の 1 つであり,日中や夜間に数回 てドパミン量に差はみられず,L—ドパの全身投与により の着替えが必要となる。多汗症は motor fluctuation を呈す 網膜でドパミン合成が誘導されることが示唆された。網 る患者で報告されており , 「off」時に顕著にみられる 。 膜におけるα - シヌクレイン凝集の有無に関する報告は 好発部位は顔面と体幹部であるが,必ずしもジスキネジ ない。これが明らかになれば,PD 患者の著明な色識別異 ア発現部位とは一致しない。発汗増加と罹病期間および 常や他の視機能障害が,全身性ドパミン欠乏に続発する 71 進行との間に相関性はない 。発汗障害を検討した研究 網膜内ドパミン作動性シナプス活性の変化によるものな では,PD 患者,特に多汗を訴える患者で交感神経性発 のか 88,または PD の神経変性過程の一部であるのかに 汗 皮 膚 反 射 反 応(sympathetic sudomotor skin reflex ついて,新しい情報が得られるであろう。 72 73 response; SSR)が消失または低下していることが報告さ れた 74–78。SSR の異常パターンから,汗腺のコリン作動 性神経支配の減弱が示唆された。PD または MSA の患者 では,障害の強い側で交感神経のコリン作動性機能障害 がより顕著に認められる 。 79,80 副 腎 副腎は進化的に交感神経節と関係があり,その被膜に は自律神経および神経節が含まれる。PD に伴い,副腎の 末梢 ANS に障害がみられるとの証拠が示されている 89–91。 眼 ドパミンは,網膜のアマクリン細胞および網状間細胞 ある研究グループは,一部の患者に副腎髄質封入体(副 腎小体)があることを報告し,これを Lewy 小体に関連 するものと考えた(他の神経疾患とも関連する)92。また, 5 パーキンソン病患者にみられる中枢神経系以外の病変 全身剖検例 783 例のうち 11%では,副腎の交感神経節細 濃 度 が 低 い こと, ス ー パ ー オ キ シ ド ジ ス ム タ ー ゼ 胞および神経束に Lewy 小体関連のα - シヌクレイノパ (superoxide dismutase; SOD)の活性が高いこと 105,脳ミ チーが認められている。ただし,副腎の典型的な封入体 トコンドリアの複合体ⅠおよびⅠV の活性が低いことが挙 である副腎小体の所見は陰性であった 。この PD 患者 げられる 106。神経以外の組織にも同様の変化が認められ 18 名のサンプルでは,全例で副腎に Lewy 小体が認めら ている。ある比較対照試験では,PD 患者で赤血球 SOD れた。副腎の病理学的所見は,起立性低血圧を除き,副 活性 107,ヒドロキシルラジカル(特に早期発症例) ,血漿 腎不全の症状と一致せず,他の部位の交感神経病変にも SOD 活性が有意に高く,赤血球 SOD/SOD1 が有意に低 起因する可能性が考えられる。 値であった(高齢患者)108。ヒドロキシルラジカルの増 93 加は,ミトコンドリアの電子伝達系の損傷によるものと考 末梢血 えられる。実際に,別の研究では PD 患者の骨格筋 109,110, リンパ球 111,112,血小板ミトコンドリア 113 でミトコンドリ PD 患者の SNpc に反応性ミクログリアの所見が認めら ア呼吸酵素の減少が確認されている。PD 患者 18 例の検 れること ,および線条体ドパミン作動性ニューロンに 体による皮膚線維芽細胞培養では,呼吸鎖複合体Ⅰおよ おいて炎症性サイトカインの増加が認められること か びⅠV の欠乏が確認され,全身性のミトコンドリア欠損で ら,免疫反応による炎症が,PD の発症機序の 1 つである あることが示された 114。呼吸鎖欠損はおそらく環境毒素 可能性が示唆される。Kim らが報告した末梢血単核細胞 によるものであり,この毒素は脳選択的ではなく他の組 でのα - シヌクレインの過剰発現は ,CNS と末梢免疫 織にも影響を及ぼす。ただし,PD における酸化ストレス, 系とを結びつける所見と考えられる。さらにマウス骨髄 特に SOD 活性の末梢血マーカーに関する他の諸試験で では,赤芽球,網赤血球,赤血球をはじめとする赤血球 は矛盾する結果が報告されており 115–117,黒質は末梢組織 系細胞にα - シヌクレインの高発現がみられるとの報告 よりも酸化ストレスを受けやすいことが示唆されている。 94 95 96 もある 。しかし,患者群と対照群との間で,α - シヌク 97 レインの量や血小板中の変性型蛋白質の有無に差がない との報告もある 69,98。 結 論 PD に伴い,末梢血のサイトカイン産生にも変化がみら 今は PD を運動症状優位のドパミン介在性大脳基底核 れる。PD 患者 33 名を対象とした末梢血 T リンパ球数に 疾患として捉えることはできない。CNS 以外の器官,特 関する長期試験では,CD4 T 細胞と CD8 T 細胞の比が に広範な自律神経支配を受ける器官も障害を受けること 減 少し,CD5 T 細 胞が 少なく,IFN- γ産 生 T 細 胞と は明白である。本稿の知見に基づき,PD を多系統の運動 IL-4 産生 T 細胞の比が増加していた 。このような免疫 自律神経疾患として捉え,PD に対するアプローチを変更 学的所見は,リンパ球の産生と増殖に影響を及ぼす末梢 していくのは理にかなっている。実際,PD においては黒 ドパミン 質だけが影響を受けるのではなく,初期の PD では黒質 + + + 99 ,または IFN- γ産生 T 細胞数を減少させ 100,101 る L- ドパの連用によって誘発された可能性がある 102 。高 が影響を受けない場合さえある。おそらく PD の神経変 濃度の IL-6 も PD のリスクとなる可能性がある 。異常 性過程は中枢 ANS,場合によっては末梢 ANS に起始す T リンパ球の血液脳関門を越えた脳内への侵入が,PD 患 ると考えられる。興味深いことに,一部の研究者は PD 者の脳にみられる免疫組織化学的変化の一因であると思 が腸神経系に始まり,投射ニューロンを介して迷走神経 われる。 背側核に進み,CNS の他部位に進むという説を提唱して 103 いる 16。もし,実際に自律神経節が最初に影響を受ける その他 6 のであれば,鉄,神経メラニン,ドパミンが神経変性過 程のトリガーであるという病因論や,PD では嗅球が主に PD の発病には,酸化ストレスが関与している可能性が 影響を受けるという病因論は,もはや解決すべき唯一の ある。黒質は,いくつかの原因により酸化障害を受けや 研究課題とは言えないであろう。このような病因論に代 すい(総説 参照) 。PD で酸化ストレスが高いことを示 わる理論として,有毒物質の摂取による PD の発症が考 す証拠として,黒質の鉄濃度が高いこと,グルタチオン えられる。摂取した有毒物質は,自律神経節に損傷を与 104 disorders in Parkinson’s disease. Parkinsonism Relat Disord 2003;9:349–353. 15. Lipp A, Trottenberg T, Schink T, Kupsch A, Arnold G. A randomized trial of botulinum toxin A for treatment of drooling. R.Djaldetti et al. Neurology 2003;61:1279–1281. 16. Braak H, de Vos RA, Bohl J, Del Tredici K. Gastric synuclein immunoreactive inclusions in Meissner’s and Auerbach’s plexuses in cases staged for Parkinson’s disease-related brain えた後,腸内自律神経叢から迷走神経を通って脳に到達 pathology. Neurisci Lett 206;396:67–72. しうる。黒質は酸化ストレスに曝されているため,ドパ 17. Kurlan R, Rothfield KP, Woodward WR Nutt JG, Miller C, 798 R. DJALDETTI ETLichter AL. D, Shoulson I. Erratic gastric emptying of levodopa ミン作動性ニューロンは,脳の他の部位よりもこのよう may cause ‘‘random’’ fluctuations of parkinsonian motility. Neurology 1988;38:419–421. な神経毒性に脆弱であると考えられる。この理論を用い 18. Djaldetti R, Baron J, Ziv I, Melamed E. Gastric emptying in involvement of peripheral organs is exciting not only Parkinson’s disease: patients with and without response fluctuaれば,自律神経症状,特に消化管症状(便秘)が運動症 because it changes our understanding of the disease, tions. Neurology 1996;46:1051–1054. 798 R. DJALDETTI ET AL. but also because peripheral tissues (e.g., における末梢 skin, colon) 19. Djaldetti R, Melamed E. Management of response fluctuations: 状前に現れる理由を説明できる。また,PD Movement Disorders, Vol. 24,Neurology No. 6, 20091998;51:S36–S40. practical guidelines. are more accessible for pathological investigation. This 器官の障害が興味深く感じられるのは,PD 20. Samanta J, Hauser RA. Duodenal levodopa infusion for the could increase the closure of discoveringに対する我々 novel bio18. Djaldetti J, Ziv I,disease. Melamed E. Gastric emptying in treatmentR,ofBaron Parkinson’s Expert Opin Pharmacother involvement of peripheral organs is exciting not only の解釈を変化させたという理由からだけではない。すな markers for early disease detection. Therefore, more Parkinson’s disease: patients with and without response fluctua2007;8:657–664. because it changes our understanding of the disease, 21.tions. KollsNeurology BJ, Stacy 1996;46:1051–1054. M. Apomorphine: a rapid rescue agent for the efforts should be invested to investigate this route. わち,末梢組織(皮膚,結腸など)がアクセスしやすい but also because peripheral tissues (e.g., skin, colon) 19. Djaldetti R, Melamed Management responseParkinson fluctuations: management of motorE.fluctuations in of advanced dispractical guidelines. Neurology 1998;51:S36–S40. ease. Clin Neuropharmacol 2006;29:292–301. are more accessible for pathological investigation. This 部位であり,病理学的検討を行いやすいこともその理由 20. J, Hauser Duodenal levodopa for the 22.Samanta Steiger M. ConstantRA. dopaminergic stimulationinfusion by transdermal could increase the closure of discovering novel biotreatment of dopaminergic Parkinson’s disease. Opin Pharmacother delivery of drugs: a Expert new treatment paradigm in である。これによって PD 早期発見のための新規バイオ REFERENCES markers for early disease detection. Therefore, more 2007;8:657–664. Parkinson’s disease. Eur J Neurol 2008;15:6–15. 21. BJ,WJ, Stacy M. Apomorphine: a rapid rescue for Parthe 23.Kolls Kupsky Grimes MM, Sweeting J, Bertsch R, agent Cote LJ. 1. Braak H, Del K, Rub U, de Vos RA, Jansen Steur EN, マーカー開発を早める可能性がある。したがって,末梢 efforts should beTredici invested to investigate this route. management of motor fluctuations concentric in advanced Parkinson diskinson’s disease and megacolon: hyaline inclusions Braak E. Staging of brain pathology related to sporadic Parkin器官の研究にさらに努力を重ねる必要がある。 ease. Clinbodies) Neuropharmacol (Lewy in enteric 2006;29:292–301. ganglion cells. Neurology 1987;37: son’s disease. Neurobiol Aging 2003;24:197–211. 22. Steiger M. Constant dopaminergic stimulation by transdermal 1253–1255. 2. Saito Y, Kawashima A, Ruberu NN, et al. Accumulation of of C, dopaminergic drugs: a new 24.delivery Singaram Ashraf W, Gaumnitz EA, treatment Torbey C, paradigm Sengupta in A, phosphorylated a-synuclein in aging human brain. J NeuropaREFERENCES REFERENCES Parkinson’s Neurol 2008;15:6–15. Pfeiffer R, disease. Quigley Eur EM.JDopaminergic defect of enteric nervous thol Exp Neurol 2003;62:644–654. 23. Kupsky Grimes MM,disease Sweeting J, Bertsch Cote LJ. Par1.3.Braak H, Del RubYang U, deP,Vos RA, Jansen Steur EN, system WJ, in Parkinson’s patients with R, chronic constipaQualman SJ, Tredici Haupt K, HM, Hamilton SR. Esophageal kinson’s disease and megacolon: concentric hyaline inclusions Braak Staging of brain pathology related sporadic Parkintion. Lancet 1995;346:861–864. Lewy E.bodies associated with ganglion cellto loss in achalasia. bodies) in enteric ganglion cells. 1987;37:F, son’s disease.toNeurobiol Aging 2003;24:197–211. 25.(Lewy Minguez-Castellanos A, Chamorro CE, Neurology Escamilla-Sevilla Similarity Parkinson’s disease. Gastroenterology 1984;87: 1253–1255. 2. Saito Y, Kawashima A, Ruberu NN, et al. Accumulation of et al. Do a-synuclein aggregates in autonomic plexuses predate 848–856. 24. Singaram C, Ashraf W, Gaumnitz Torbey C, Sengupta A, a-synuclein human brain.F. JParkinson’s NeuropaLewy body disorders? A cohortEA, study. Neurology 2007;68: 4.phosphorylated Wakabayashi K, Takahashi inH,aging Ohama E, Ikuta Pfeiffer R, Quigley EM. Dopaminergic defect of enteric nervous thol Exp Neurol 2003;62:644–654. study of Lewy body-contain201:2–8. disease: an immunohistochemical in LL, Parkinson’s patientsRF. withGastrointestinal chronic constipa3. Qualman SJ, in Haupt HM, Yang P, Hamilton SR. Esophageal 26.system Edwards Quigley disease EM, Pfeiffer dysing neurons the enteric nervous system. Acta Neuropathol tion. Lancet Lewy bodies associated with ganglion cell loss in achalasia. function in 1995;346:861–864. Parkinson’s disease: frequency and pathophysiology. 1990;79:581–583. 25. Minguez-Castellanos A, Chamorro CE, Escamilla-Sevilla F, to Parkinson’s Gastroenterology Neurology 1992;42:726–732. 5.Similarity Wakabayashi K, Takahashidisease. H, Ohama E, Takeda S,1984;87: Ikuta F. al. Do a-synuclein aggregatesmotility in autonomic plexuses 848–856. 27.etJost WH. Gastrointestinal problems in predate patients Lewy bodies in the visceral autonomic nervous system in ParLewy body disorders? A Effects cohort of study. Neurology 2007;68: 4. Wakabayashi K, Takahashi H,1993;60:609–612. Ohama E, Ikuta F. Parkinson’s with Parkinson’s disease. antiparkinsonian treatment kinson’s disease. Adv Neurol 201:2–8. an immunohistochemical study ofS,Lewy body-containand guidelines for management. Drugs Aging 1997;10:249– 6.disease: Wakabayashi K, Takahashi H, Takeda Ohama E, Ikuta F. 26. Edwards LL, Quigley EM, Pfeiffer RF. Gastrointestinal dysing neurons in the enteric nervous Acta inNeuropathol 258. Parkinson’s disease: the presence of system. Lewy bodies Auerbach’s Parkinson’s disease: frequency and pathophysiology. 1990;79:581–583. 28.function EdwardsinLL, Pfeiffer RF, Quigley EM, Hofman R, Balluff M. and Meissner’s plexuses. Acta Neuropathol 1988;76:217–221. Neurology 1992;42:726–732. 5.7.Wakabayashi K, Takahashi H, OhamaS, E, Takeda S, IkutacriteF. Gastrointestinal symptoms in Parkinson’s disease. Mov Disord Clarke CE, Gullaksen E, Macdonald Lowe F. Referral 27. Jost WH. Gastrointestinal motility problems in patients Lewy in and the visceral nervous system in Par1991;6:151–156. ria forbodies speech languageautonomic therapy assessment of dysphagia Parkinson’s Effects of antiparkinsonian kinson’s disease. Adv Neurol 1993;60:609–612. 29.with Singer C, Weinerdisease. WJ, Sanchez-Ramos JR. Autonomictreatment dysfunccaused by idiopathic Parkinson’s disease. Acta Neurol Scand and forParkinson’s management. Drugs 6. Wakabayashi K, Takahashi H, Takeda S, Ohama E, Ikuta F. tion guidelines in men with disease. EurAging Neurol1997;10:249– 1992;32:134– 1998;97:27–35. 258. disease: presence of Lewy bodies in Auerbach’s 140. 8.Parkinson’s Leopold NA, KageltheMC. Prepharyngeal dysphagia in Parkin28. Pfeiffer RF, Quigley EM, Rooden HofmanSM, R, Balluff M. and Meissner’s plexuses. Acta Neuropathol 1988;76:217–221. 30.Edwards Verbaan LL, D, Marinus J, Visser M, van Stiggelbout son’s disease. Dysphagia 1996;11:14–22. Gastrointestinal symptoms in Parkinson’s disease. Mov Disordin 7.9.Clarke CE,LL, Gullaksen Macdonald S, Lowe F. Referral criteAM, van Hilten JJ. Patient-reported autonomic symptoms Edwards Quigley E, EM, Harned RK, Hofman R, Pfeiffer RF. 1991;6:151–156. ria for speech andoflanguage therapy of Parkinson’s dysphagia Parkinson disease. Neurology 2007;69:333–341. Characterization swallowing and assessment defecation in 29. WJ, Autonomic caused idiopathic Parkinson’s disease. Acta Neurol Scand 31.Singer AshrafC,W,Weiner Pfeiffer RF,Sanchez-Ramos Park F, Lof J, JR. Quigley EMM. dysfuncConstipadisease.byAm J Gastroenterol 1994;89:15–25. tion with Parkinson’s Neurol 1992;32:134– tionininmen Parkinson’s disease: disease. objectiveEur assessment and response 10.1998;97:27–35. Leopold NA, Kagel MC. Pharyngo-esophageal dysphagia in 140. 8. Leopold NA,disease. Kagel Dysphagia MC. Prepharyngeal dysphagia in Parkinto psyllium. Mov Disord 1997;12:946–951. Parkinson’s 1997;12:11–18. 30. D, Marinus J, Visser M, LR, van et Rooden SM, Stiggelbout disease. Dysphagia 32.Verbaan Abbott RD, Petrovitch H, White al. Frequency of bowel 11.son’s Castell JA, Johnston BT,1996;11:14–22. Colcher A, Li Q, Gideon RM, Castell AM, van Hilten JJ. future Patient-reported autonomicdisease. symptoms in 9. Edwards LL, Quigley EM, HarnedofRK, R, Pfeiffer RF. movements and the risk of Parkinson’s NeurolDO. Manometric abnormalities theHofman oesophagus in patients Parkinson disease. Neurology 2007;69:333–341. Characterization swallowing and defecation in Parkinson’s ogy 2001;57:456–462. with Parkinson’sof disease. Neurogastroenterol Motil 2001;13: 31. ParkY,F, Takahashi Lof J, Quigley EMM. Constipadisease. Am J Gastroenterol 1994;89:15–25. 33.Ashraf AminoW, T, Pfeiffer Orimo RF, S, Itoh A, Uchihara T, Mizu361–364. tion Parkinson’s assessment and occurs responsein 10. Kagel MC.JA,Pharyngo-esophageal dysphagia in sawain H. Profound disease: cardiac objective sympathetic denervation 12.Leopold Blonsky NA, ER, Logemann Boshes B, Fisher HB. Comparison toParkinson psyllium.disease. Mov Disord Parkinson’s Dysphagiafunction 1997;12:11–18. Brain1997;12:946–951. Pathol 2005;15:29–34. of speech disease. and swallowing in patients with tremor 32. RD, H, White LR, et al.M, Frequency of bowel 11. Castell JA, and Johnston BT, Colcher Li Q, Gideon RM, Castell 34.Abbott Iwanaga K,Petrovitch Wakabayashi K, Yoshimoto et al. Lewy bodydisorders in normal geriatricA,patients: a cinefluorographic. movements and theinfuture riskplexus of Parkinson’s disease. DO. Manometric abnormalities of the oesophagus in patients type degeneration cardiac in Parkinson’s and NeurolincidenJ Gerontol 1975;30:299–303 ogy 2001;57:456–462. disease. Neurogastroenterol Motil 2001;13: tal Lewy body diseases. Neurology 1999;52:1269–1271. 13.with EadieParkinson’s MJ, Tyrer JH. Alimentary disorder in parkinsonism. Aust 33. S, Itoh Y, Takahashi A, F, Uchihara 361–364. 35.Amino Orimo T, S, Orimo Takahashi A, Uchihara T, Mori Kakita T, A, MizuWakaAnn Med 1965;14:23–27. sawa H. K, Profound cardiac sympathetic denervation occurs in 12. JA,Królicki Boshes L, B, Spychala Fisher HB.A.Comparison bayashi Takahashi H. Degeneration of cardiac sympathetic 14.Blonsky PotulskaER, A, Logemann Friedman A, Swallowing Parkinson disease. 2005;15:29–34. ofdisorders speech in andParkinson’s swallowingdisease. functionParkinsonism in patients with nerve begins in theBrain earlyPathol disease process of Parkinson’s disease. Relat tremor Disord 34. Iwanaga K, Wakabayashi K, Yoshimoto M, et al. Lewy bodydisorders and in normal geriatric patients: a cinefluorographic. Brain Pathol 2007;17:24–30. 2003;9:349–353. degeneration Parkinson’s and inciden-of Gerontol 1975;30:299–303 36.type Barbic F, PeregoinF,cardiac Canesiplexus M, etinal. Early abnormalities 15.J Lipp A, Trottenberg T, Schink T, Kupsch A, Arnold G. A tal Lewy body diseases.autonomic Neurologycontrol 1999;52:1269–1271. 13. Eadie MJ, Tyrer Alimentarytoxin disorder parkinsonism. Aust vascular and cardiac in Parkinson’s disease randomized trialJH. of botulinum A forintreatment of drooling. 35. Orimo Takahashi A, Uchihara T,Hypertension Mori F, Kakita A, WakaAnn Med 1965;14:23–27. withoutS, orthostatic hypotension. 2007;49:120– Neurology 2003;61:1279–1281. bayashi 14. Królicki Spychala A. Swallowing 126. K, Takahashi H. Degeneration of cardiac sympathetic 16.Potulska Braak H,A,deFriedman Vos RA, A, Bohl J, Del L, Tredici K. Gastric synuclein beginsDS, in the early disease processC, of Pechnik Parkinson’s disorders in Parkinson’s disease. ParkinsonismandRelat Disord 37.nerve Goldstein Eldadah BA, Holmes S, disease. Moak J, immunoreactive inclusions in Meissner’s Auerbach’s Brain Pathol 2007;17:24–30. 2003;9:349–353. Saleem A, Sharabi Y. Neurocirculatory abnormalities in Parkinplexuses in cases staged for Parkinson’s disease-related brain 36. Barbic F, Perego Canesi M, et al. Earlyindependence abnormalitiesfrom of 15. Lipp A, Trottenberg T, 206;396:67–72. Schink T, Kupsch A, Arnold G. A son disease with F,orthostatic hypotension: pathology. Neurisci Lett vascular cardiac Hypertension autonomic control in Parkinson’s disease of botulinum toxin A for treatment of drooling. levodopaand treatment. 2005;46:1333–1339. 17.randomized Kurlan R, trial Rothfield KP, Woodward WR Nutt JG, Miller C, orthostatic hypotension. Hypertension 2007;49:120– Neurology 38.without Goldstein DS, Holmes C, Li ST, Bruce S, Metman LV, Cannon Lichter D,2003;61:1279–1281. Shoulson I. Erratic gastric emptying of levodopa 126. 16. Braak de Vos RA, Bohl J, Del Tredici K. Gastric synuclein RO. Cardiac sympathetic denervation in Parkinson disease. Ann may H, cause ‘‘random’’ fluctuations of parkinsonian motility. 37. Goldstein DS, Eldadah BA, Holmes C, Pechnik S, Moak J, immunoreactive inclusions in Meissner’s and Auerbach’s Intern Med 2000;133:338–347. Neurology 1988;38:419–421. Saleem A, Sharabi Y. Neurocirculatory abnormalities in Parkinplexuses in cases staged for Parkinson’s disease-related brain son disease with orthostatic hypotension: independence from pathology. Neurisci Lett 206;396:67–72. levodopa treatment. Hypertension 2005;46:1333–1339. 17. Kurlan R, Rothfield KP, Woodward WR Nutt JG, Miller C, 38. Goldstein DS, Holmes C, Li ST, Bruce S, Metman LV, Cannon Lichter D, Shoulson I. Erratic gastric emptying of levodopa Movement Vol. 24, No.fluctuations 6, 2009 RO. Cardiac sympathetic denervation in Parkinson disease. Ann may Disorders, cause ‘‘random’’ of parkinsonian motility. Intern Med 2000;133:338–347. Neurology 1988;38:419–421. nerve Brain 36. Barbic vascul withou 126. 37. Goldst Saleem son d levodo 38. Goldst RO. C Intern 7 OUTSIDE kinson’s asegawa istics of ton Res Cardiac ac symrd 2003; awa H. phy in 1999;67: 8 39. Koike Y, Takahashi A. Autonomic dysfunction in Parkinson’s disease. Eur Neurol 1997;38:8–12. 40. Niimi Y, Ieda T, Hirayama M, Koike Y, Sobue G, Hasegawa LESIONS OUTSIDE パーキンソン病患者にみられる中枢神経系以外の病変 Y, Takahashi A. Clinical and physiological characteristics of autonomic failure with Parkinson’s disease. Clin Auton Res 1999;9:139–144. 41.Koike Courbon F, Brefel-Courbon C, Thalamas C, inet Parkinson’s al. Cardiac 39. Y, Takahashi A. Autonomic dysfunction MIBG Eur scintigraphy is a sensitive tool for detecting cardiac symdisease. Neurol 1997;38:8–12. pathetic in Parkinson’s MovG,Disord 2003; 40. Niimi Y, denervation Ieda T, Hirayama M, Koikedisease. Y, Sobue Hasegawa Y,18:890–897. Takahashi A. Clinical and physiological characteristics of 42.autonomic Orimo S, failure Ozawa with E, Nakade S, Sugimoto T, Mizusawa Parkinson’s disease. Clin Auton ResH. [123]I-metaiodobenzylguanidine myocardial scintigraphy in 1999;9:139–144. Parkinson’s disease. J Neurol 1999;67: 41. Courbon F, Brefel-Courbon C, Neurosurg Thalamas Psychiatry C, et al. Cardiac 189–194. MIBG scintigraphy is a sensitive tool for detecting cardiac sym43.pathetic Takatsudenervation H, Nishida in H, Parkinson’s Matsuo H, etdisease. al. Cardiac deMovsympathetic Disord 2003; nervation from the early stage of Parkinson’s disease: clinical 18:890–897. and experimental with S, radiolabeled J Nucl Med 42. Orimo S, Ozawa studies E, Nakade Sugimoto MIBG. T, Mizusawa H. 2000;41:71–77. [123]I-metaiodobenzylguanidine myocardial scintigraphy in 44.Parkinson’s Oka H, Mochio S, Onouchi Morita M,Psychiatry Yoshioka 1999;67: M, Inoue disease. J NeurolK,Neurosurg K. Cardiovascular dysautonomia in de novo Parkinson’s dis189–194. ease. J H, Neurol Sci H, 2006;241:59–65. 43. Takatsu Nishida Matsuo H, et al. Cardiac sympathetic de45.nervation Suzuki M, Urashima M,stage Oka of H, Parkinson’s Hashimoto M, Taira clinical K. Carfrom the early disease: diacexperimental sympatheticstudies denervation in bradykinesia-dominant and with radiolabeled MIBG. J NuclParkinMed son’s disease. Neuroreport 2007;18:1867–1870. 2000;41:71–77. 46.Oka Spiegel J, Hellwig D, Farmakis G, etM,al.Yoshioka Myocardial 44. H, Mochio S, Onouchi K, Morita M, sympaInoue degenerationdysautonomia correlates withinclinical phenotype of ParkinK.thetic Cardiovascular de novo Parkinson’s disson’sJ disease. Mov Disord 2007;22:1004–1008. ease. Neurol Sci 2006;241:59–65. 47.Suzuki Haapaniemi TH, Pursiainen V, Hashimoto KorpelainenM,JT,Taira Huikuri HV, 45. M, Urashima M, Oka H, K. CarSotaniemi KA, Myllylä VV. inAmbulatory ECG and analysis diac sympathetic denervation bradykinesia-dominant Parkin-of heartdisease. rate variability in Parkinson’s disease. J Neurol Neurosurg son’s Neuroreport 2007;18:1867–1870. Psychiatry 2001;70:305–310. 46. Spiegel J, Hellwig D, Farmakis G, et al. Myocardial sympa48.thetic Devos D, Kroumova M, Bordet R, Vodougnon H, ofGuieu JD, degeneration correlates with clinical phenotype ParkinLibersa C, Destee A. Heart rate variability and Parkinson’s disson’s disease. Mov Disord 2007;22:1004–1008. ease severity. J Neural Transm 47. Haapaniemi TH, Pursiainen V, 2003;110:997–1011. Korpelainen JT, Huikuri HV, 49.Sotaniemi Taki J, Nakajima K, Hwang EH, Matsunari I, and Komai K, YoshKA, Myllylä VV. Ambulatory ECG analysis of ita M, K, Tonami N. Peripheral dysfuncheart rateSakajiri variability in Parkinson’s disease. sympathetic J Neurol Neurosurg tion in patients with Parkinson’s disease without autonomic failPsychiatry 2001;70:305–310. ure isD,heart selectiveM,and disease specific. EurH,J Guieu Nucl JD, Med 48. Devos Kroumova Bordet R, Vodougnon 2000;27:566–573. Libersa C, Destee A. Heart rate variability and Parkinson’s dis50.ease Braune S, Reinhardt M, Schnitzer R, Riedel A, Lücking CH. severity. J Neural Transm 2003;110:997–1011. Cardiac uptake of [123I]MIBG separates I,Parkinson’s disease 49. Taki J, Nakajima K, Hwang EH, Matsunari Komai K, Yoshatrophy. Neurology sympathetic 1999;53:1020–1025. itafrom M, multiple Sakajiri system K, Tonami N. Peripheral dysfunc51.tion Sharabi Y, Li with ST, Parkinson’s Dendi R, Holmes Goldstein DS. Neuroin patients diseaseC, without autonomic failtransmitter denervation Parkinson’s ure is heart specificity selective of andsympathetic disease specific. Eur Jin Nucl Med disease. Neurology 2003;60:1036–1039. 2000;27:566–573. 52.Braune Winge S, K, Reinhardt Skau AM, M, Stimpel H, Nielsen KK, A, Werdelin L. CH. Prev50. Schnitzer R, Riedel Lücking alence of bladder Parkinson’s disease. Neurourol Cardiac uptake of dysfunction [123I]MIBGin separates Parkinson’s disease Urodyn 2006;25:116–122. from multiple system atrophy. Neurology 1999;53:1020–1025. 53.Sharabi Araki I,Y,Kuno S. Assessment of voiding dysfunction Parkin51. Li ST, Dendi R, Holmes C, Goldstein DS.inNeuroson’s disease by the Prostate Symptom Score. transmitter specificity of International sympathetic denervation in Parkinson’s J Neurol Neurosurg Psychiatry 2000;68:429–433. disease. Neurology 2003;60:1036–1039. 54.Winge BergerK,Y,Skau Blaivas DeLaRocha ER, Salinas JM. Urodynamic 52. AM,JG, Stimpel H, Nielsen KK, Werdelin L. Prevfindings Parkinson’s disease. Urol 1987;138:836–838. alence of in bladder dysfunction in JParkinson’s disease. Neurourol 55.Urodyn Campos-Sousa RN, Quagliato E, da Silva BB, De Carvalho 2006;25:116–122. RM, I, Jr,Kuno Ribeiro de Carvalho DF. Urinary symptoms in Par53. Araki S. SC, Assessment of voiding dysfunction in Parkinkinson’s disease: and associated Arq Score. Neuroson’s disease by prevalence the International Prostate factors. Symptom 2003;61:359–363. J psiquiatr Neurol Neurosurg Psychiatry 2000;68:429–433. 56.Berger Lemack Dewey RB, Roehrborn CG, O’Suilleabhain PE, 54. Y, GE, Blaivas JG, DeLaRocha ER, Salinas JM. Urodynamic Zimmern PE. Questionnaire-based of bladder dysfindings in Parkinson’s disease. J Urolassessment 1987;138:836–838. function in patients with mild E, to moderate disease. 55. Campos-Sousa RN, Quagliato da Silva Parkinson’s BB, De Carvalho Urology 2000;56:250–254. RM, Jr, Ribeiro SC, de Carvalho DF. Urinary symptoms in Par57.kinson’s Winge disease: K, Fowler CJ. Bladder dysfunction in Parkinsonism: prevalence and associated factors. Arq Neuromechanisms, prevalence, symptoms, and management. Mov psiquiatr 2003;61:359–363. Disord 2006;21:737–745. 56. Lemack GE, Dewey RB, Roehrborn CG, O’Suilleabhain PE, 58.Zimmern Singer C.PE. Urinary dysfunction in Parkinson’s Clin dysNeuQuestionnaire-based assessment disease. of bladder rosci 1998;5:78–86. function in patients with mild to moderate Parkinson’s disease. 59.Urology Gray R,2000;56:250–254. Stern G, Malone-Lee J. Lower urinary tract dysfunction in Parkinson’s disease: changes dysfunction relate to agein and not disease. 57. Winge K, Fowler CJ. Bladder Parkinsonism: Age Ageing 1995;24:499–504. mechanisms, prevalence, symptoms, and management. Mov Disord 2006;21:737–745. 58. Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci 1998;5:78–86. THE CNSR,INStern PDG, Malone-Lee J. Lower urinary tract dysfunction 799 59. Gray in Parkinson’s disease: changes relate to age and not disease. Age Ageing 1995;24:499–504. 60. Araki I, Kitahara M, Oida T, Kuno S. Voiding dysfunction and Parkinson’s disease: urodynamic abnormalities and urinary symptoms. J Urol 2000;164:1640–1643. 61. Sakakibara R, Shinotoh H, Uchiyama T, Yoshiyama M, Hattori T, Yamanishi T. SPECT imaging of the dopamine transporter with [(123)I]-b-CIT reveals marked decline of nigrostriatal dopaminergic function in Parkinson’s disease with urinary dysfunction. J Neurol Sci 2001;187:55–59. 62. Uchiyama T, Sakakibara R, Hattori T, Yamanishi T. Short-term effect of a single levodopa dose on micturition disturbance in Parkinson’s disease patients with the wearing-off phenomenon. Mov Disord 2003;18:573–578. 63. Aranda B, Cramer P. Effects of apomorphine and L-dopa on 60. Araki I, Kitahara M, Oida T, Kuno S. Voiding dysfunction and Parkinson’s disease: urodynamic abnormalities and urinary symptoms. J Urol 2000;164:1640–1643. THE IN PD 799 61.CNS Sakakibara R, Shinotoh H, Uchiyama T, Yoshiyama M, Hattori T, Yamanishi T. SPECT imaging of the dopamine transporter with [(123)I]-b-CIT reveals marked decline of nigrostriatal dopaminergic function in Parkinson’s urinary and dys60. Araki I, Kitahara M, Oida T, Kuno S. disease Voidingwith dysfunction function. J Neurol 2001;187:55–59. Parkinson’s disease:Sciurodynamic abnormalities and urinary 62.symptoms. UchiyamaJT,Urol Sakakibara R, Hattori T, Yamanishi T. Short-term 2000;164:1640–1643. effect of aR,single levodopa dose on T, micturition disturbance 61. Sakakibara Shinotoh H, Uchiyama Yoshiyama M, Hattoriin patients with of thethe wearing-off T,Parkinson’s Yamanishidisease T. SPECT imaging dopaminephenomenon. transporter Mov[(123)I]-b-CIT Disord 2003;18:573–578. with reveals marked decline of nigrostriatal do63.paminergic Aranda B, function Cramer P. of apomorphine L-dopa in Effects Parkinson’s disease withand urinary dys-on the parkinsonian Neurourol Urodyn 1993;12:203–209. function. J Neurol bladder. Sci 2001;187:55–59. 64.Uchiyama Winge K,T,Nielsen KK, R, Stimpel A, Short-term Jensen SR, 62. Sakakibara HattoriH,T,Lokkegaard Yamanishi T. Werdelin Lower urinary dose tract on symptoms and disturbance bladder control effect of a L. single levodopa micturition in in advanceddisease Parkinson’s disease: effects of deep phenomenon. brain stimulaParkinson’s patients with the wearing-off tion Disord in the subthalamic nucleus. Mov Disord 2007;22:220–225. Mov 2003;18:573–578. 65.Aranda Seif C,B, Herzog J, van der HC,ofet apomorphine al. Effect of subthalamic 63. Cramer P. Effects and L-dopa deep on brain stimulation on theNeurourol function Urodyn of the urinary bladder. Ann the parkinsonian bladder. 1993;12:203–209. NeurolK,2004;55:118–120. 64. Winge Nielsen KK, Stimpel H, Lokkegaard A, Jensen SR, 66.Werdelin Finazzi-Agrò E, Peppe D’Amico A, Petta F, Mazzone L. Lower urinaryA,tract symptoms and bladder controlP, Micali F, disease: Caltagirone C. of Effects of subthalamic inStanzione advanced P,Parkinson’s effects deep brain stimulanucleus urodynamic findings in patients with tion in thestimulation subthalamicon nucleus. Mov Disord 2007;22:220–225. Parkinson’s disease. Urol 2003;169:1388–1391. 65. Seif C, Herzog J, van Jder HC, et al. Effect of subthalamic deep 67.brain Herzog J, Weiss on PH,the Assmus A, of et al. stimulation stimulation function theSubthalamic urinary bladder. Ann modulates cortical control of urinary bladder in Parkinson’s disNeurol 2004;55:118–120. ease. Brain 2006;129:3366–3375. 66. Finazzi-Agrò E, Peppe A, D’Amico A, Petta F, Mazzone P, 68.Stanzione Herzog J,P,Weiss PH,F,Assmus A, et C. al. Improved gating Micali Caltagirone Effects ofsensory subthalamic of urinary bladder on afferents in Parkinson’s disease following nucleus stimulation urodynamic findings in patients with subthalamicdisease. stimulation. 2008;131:132–145. Parkinson’s J UrolBrain 2003;169:1388–1391. 69.Herzog Dabby J,R,Weiss Djaldetti R, Shahmurov Treves TA, Gabai B, 67. PH, Assmus A, et al.M, Subthalamic stimulation Melamed cortical E, Sadeh M, Avinoach Skin biopsy for assessment modulates control of urinaryI. bladder in Parkinson’s disof autonomic denervation in Parkinson’s disease. J Neural ease. Brain 2006;129:3366–3375. TransmJ,2006;113:1169–1176. 68. Herzog Weiss PH, Assmus A, et al. Improved sensory gating 70.ofMichell Luheshi LM, Barker RA. Skin disease and platelet a-synurinaryAW, bladder afferents in Parkinson’s following uclein as peripheral biomarkers of Parkinson’s disease. Neurosci subthalamic stimulation. Brain 2008;131:132–145. Lett 2005;381:294–298. 69. Dabby R, Djaldetti R, Shahmurov M, Treves TA, Gabai B, 71.Melamed HirayamaE, M. Sweating dysfunction Parkinson’s disease. Sadeh M, Avinoach I. Skininbiopsy for assessment 2006;253(suppl ofJ Neurol autonomic denervation7):42–47. in Parkinson’s disease. J Neural 72.Transm Sage JI,2006;113:1169–1176. Mark MH. Drenching sweats as an off phenomenon in Parkinson’s andRA. relation to plasma 70. Michell AW, disease: Luheshi treatment LM, Barker Skin and plateletlevodopa a-synprofile. Neurolbiomarkers 1995;37:120–122. uclein as Ann peripheral of Parkinson’s disease. Neurosci 73.Lett Goetz CG, Lutge W, Tanner CM. Autonomic dysfunction in 2005;381:294–298. Parkinson’s Neurology 1986;36:73–75. 71. Hirayama M.disease. Sweating dysfunction in Parkinson’s disease. 74.J Mano Nakamuro T, 7):42–47. Takayanagi T, Mayer RF. Sweat funcNeurolY,2006;253(suppl tion JI, in Parkinson’s disease. J Neurol 72. Sage Mark MH. Drenching sweats 1994;241:573–576. as an off phenomenon in 75.Parkinson’s Bordet R, Benhadjali J, Destee Hurtevent JF, Bourriez JL, disease: treatment andA,relation to plasma levodopa Guieu Ann JD. Sympathetic skin response and R-R interval variabiliprofile. Neurol 1995;37:120–122. ty in CG, multiple atrophyCM. and Autonomic idiopathic Parkinson’s 73. Goetz Lutgesystem W, Tanner dysfunction disin ease. Mov disease. Disord 1996;11:268–272. Parkinson’s Neurology 1986;36:73–75. 76.Mano Braune Korchounov AM, Schipper HI. Autonomic 74. Y, HJ, Nakamuro T, Takayanagi T, Mayer RF. Sweatdysfuncfunctionin in Parkinson’s disease assessed by sympathetic skin tion Parkinson’s disease. J Neurol 1994;241:573–576. response: a prospective clinical A, andHurtevent neurophysiological trialJL,on 75. Bordet R, Benhadjali J, Destee JF, Bourriez 50 patients. Acta Neurol Scand 1997;95:293–297. Guieu JD. Sympathetic skin response and R-R interval variabili77.tySchestatsky Valls-Solé J, Ehlers JA, Rieder CR, Gomes in multipleP,system atrophy and idiopathic Parkinson’s dis-I. Hyperhidrosis Parkinson’s disease. Mov Disord 2006;21: ease. Mov Disordin1996;11:268–272. 41744–1748. 76. Braune HJ, Korchounov AM, Schipper HI. Autonomic dysfunc78.tion Schestatsky P, Ehlersdisease JA, Rieder CR, Gomes I. Evaluation in Parkinson’s assessed by sympathetic skinof sympathetic skin response in Parkinson’s disease. Parkinsonism response: a prospective clinical and neurophysiological trial on Disord 2006;12:486–491. 50Relat patients. Acta Neurol Scand 1997;95:293–297. 79.Schestatsky De Marinis P, M,Valls-Solé Stocchi F, J,Gregori Accornero N. Sympathetic 77. EhlersB,JA, Rieder CR, Gomes I. skin response inandParkinson’s cardiovascular autonomic function2006;21: tests in Hyperhidrosis disease. Mov Disord Parkinson’s disease and multiple system atrophy with auto41744–1748. nomic failure. Mov Disord 2000;15:1215–1220. 78. Schestatsky P, Ehlers JA, Rieder CR, Gomes I. Evaluation of 80.sympathetic Bordet R, Benhadjali J, Destee A, Hurtevent Bourriez JL, skin response in Parkinson’s disease.JF,Parkinsonism 800Relat R.variabiliDJALDETTI ET AL. Guieu JD. Sympathetic skin response and R-R interval Disord 2006;12:486–491. ty Marinis in multiple systemF,atrophy idiopathic N. Parkinson’s dis79. De M, Stocchi Gregoriand B, Accornero Sympathetic ease.response Mov Disord skin and 1996;11:268–272. cardiovascular autonomic function tests in 81.Parkinson’s Kramer SG.disease Dopamine: a retinalsystem neurotransmitter. I. Retinal 100. Bergqu and multiple atrophy with autouptake, storage, and light-stimulated release of H3-dopamine in endoge nomic failure. Mov Disord 2000;15:1215–1220. vivo. Invest Ophthalmol 1971;10:438–452. catech 80. Bordet R, Benhadjali J, Destee A, Hurtevent JF, Bourriez JL, 82.Guieu Brandies R, Yehuda S.skin Theresponse possibleand roleR-R of interval retinal dopaminercrine l JD. Sympathetic variabiliMovement Disorders, 24, No. 6,dis2009 visualatrophy performance. NeurosciVol. Biobehav Rev 101. Cooktygicin system multipleinsystem and idiopathic Parkinson’s 2008;32:611–656. tion of ease. Mov Disord 1996;11:268–272. 83. Bodis-Wollner I. Visual electrophysiology in Parkinson’s disnon-cl ease: PERG, VEP and visual P300. Clin Electroencephalogr 1995;8 1997;28:143–147. 102. Carr L 84. Price MJ, Feldman RG, Adelberg D, Kayne H. Abnormalities of L-d Movement Disorders, Vol. 24, No. 6, 2009 in color vision and contrast sensitivity in Parkinson’s disease. produc Neurology 1992;42:887–890. 103. Chen 85. Buttner T, Kuhn W, Muller T, Patzold T, Heidbrink K, Przuneral in tek H. Distorted color discrimination in ‘de novo’ parkinsonian Am J patients. Neurology 1995;45:386–387. 104. Schapi 86. Muller T, Kuhn W, Buttner T, Eising E, Coenen H, Haas M, thol A Przuntek. Colour vision abnormalities do not correlate with 105. Jenner dopaminergic nigrostriatal degeneration in Parkinson’s disease. disease J Neurol 1998;245:659–664. 106. Schapi 2008;32:611–656. 83. I. Visual electrophysiology in Parkinson’s dis81.Bodis-Wollner Kramer SG. Dopamine: a retinal neurotransmitter. I. Retinal ease: PERG, VEPandand visual P300. release Clin Electroencephalogr uptake, storage, light-stimulated of H3-dopamine in 1997;28:143–147. vivo. Invest Ophthalmol 1971;10:438–452. 84. MJ, R, Feldman Adelberg D, role Kayne Abnormalities 82.Price Brandies YehudaRG, S. The possible of H. retinal dopamineringic color visioninand contrast sensitivity Neurosci in Parkinson’s disease. system visual performance. Biobehav Rev Neurology 1992;42:887–890. 2008;32:611–656. 85. T, Kuhn I.W,Visual Mullerelectrophysiology T, Patzold T, Heidbrink K, Przun83.Buttner Bodis-Wollner in Parkinson’s distek H. Distorted colorand discrimination in Clin ‘de novo’ parkinsonian ease: PERG, VEP visual P300. Electroencephalogr patients. Neurology 1995;45:386–387. 1997;28:143–147. 86. T, Kuhn W, Buttner T, Eising Coenen H, Haas M, 84.Muller Price MJ, Feldman RG, Adelberg D, E, Kayne H. Abnormalities Przuntek. Colour and vision abnormalities correlatedisease. with in color vision contrast sensitivity do in not Parkinson’s dopaminergic nigrostriatal degeneration in Parkinson’s disease. Neurology 1992;42:887–890. Neurol 1998;245:659–664. 85.J Buttner T, Kuhn W, Muller T, Patzold T, Heidbrink K, Przun87. Sartucci F, Orlandicolor G, Lucetti C, Bonuccelli Murri L, Orsini tek H. Distorted discrimination in ‘deU, novo’ parkinsonian C,patients. Porciatti V. Changes in pattern electroretinograms to Neurology 1995;45:386–387. red-green and blue-yellow 86.equiluminant Muller T, Kuhn W, Buttner T, Eising E,gratings Coenen in H, patients Haas M, with early Parkinson’s disease. J Clin Neurophysiol 2003;20: Przuntek. Colour vision abnormalities do not correlate with 375–381. dopaminergic nigrostriatal degeneration in Parkinson’s disease. 88. Harnois Di Paolo T. Decreased dopamine in the retinas of J NeurolC,1998;245:659–664. Parkinson’s disease. Invest Ophthalmol Sci 87.patients Sartucciwith F, Orlandi G, Lucetti C, Bonuccelli U, Murri Vis L, Orsini 1990;31:2473–2475. C, Porciatti V. Changes in pattern electroretinograms to 89. Wakabayashi Takahashi Neuropathology of autonomic equiluminant K,red-green andH.blue-yellow gratings in patients nervous system in Parkinson’s disease. EurNeurophysiol Neurol 1997;38:2–7. with early Parkinson’s disease. J Clin 2003;20: 90. den Jager WA. Histochemistry of adrenal bodies in Parkinson’s 375–381. Neurol 88.disease. HarnoisArch C, Di Paolo1970;23:528–533. T. Decreased dopamine in the retinas of 91. Sugie M, with Goto Parkinson’s J, Kawamuradisease. M, OtaInvest H. Increased norepinephpatients Ophthalmol Vis Sci rine-associated adrenomedullary inclusions in Parkinson’s dis1990;31:2473–2475. Pathol Int K, 2005;55:130–136. 89.ease. Wakabayashi Takahashi H. Neuropathology of autonomic 92. Hart MN, system Cyrus A, Jr. Hyaline globules of the adrenal medulla. nervous in Parkinson’s disease. Eur Neurol 1997;38:2–7. Clin Pathol 1968;49:387–391. 90.Am denJ Jager WA. Histochemistry of adrenal bodies in Parkinson’s 93. Fumimura Y, Ikemura Saito Y, et al. Analysis of the adrenal disease. Arch Neurol M, 1970;23:528–533. useful the peripheral auto91.gland SugieisM, GotoforJ, evaluating Kawamurapathology M, Ota H.ofIncreased norepinephnomic nervous system in Lewy body disease. J Neuropathol rine-associated adrenomedullary inclusions in Parkinson’s disExp Neurol ease. Pathol2007;66:354–362. Int 2005;55:130–136. 94. PL,Cyrus ItagakiA,S,Jr. Boyes BE, McGeer Reactive microglia 92.McGeer Hart MN, Hyaline globulesEG. of the adrenal medulla. are positive HLA-DR in the substantia nigra of Parkinson’s and Am J Clinfor Pathol 1968;49:387–391. disease brains. 93.Alzheimer’s Fumimura Y, Ikemura M,Neurology Saito Y, et1988;38:1285–1291. al. Analysis of the adrenal 95. Mogi HaradaforM,evaluating Narabayashi H, Inagaki Minami autoM, glandM, is useful pathology of theH, peripheral Nagatsu T. Interleukin (IL)-1 b, IL-2, IL-4, IL-6 and transformnomic nervous system in Lewy body disease. J Neuropathol ing levels are elevated in ventricular cerebroExpgrowth Neurolfactor-a 2007;66:354–362. fluid juvenile parkinsonism andEG. Parkinson’s disease. 94.spinal McGeer PL,inItagaki S, Boyes BE, McGeer Reactive microglia Neurosci Lettfor 1996;211:13–16. are positive HLA-DR in the substantia nigra of Parkinson’s and 96. Kim S, Seo JH, Suh UH. a-synuclein Parkinson’s disease, and Alzheimer’s disease brains. Neurology, 1988;38:1285–1291. disease.M, Park Relat Disord 95.Alzheimer’s Mogi M, Harada Narabayashi H,2004;10:S9–S13. Inagaki H, Minami M, 97. Nakai M, T. Fujita M, Waragai al. Expression of alpha-synNagatsu Interleukin (IL)-1M,b,etIL-2, IL-4, IL-6 and transformuclein, a presynaptic implicated ing growth factor-a protein levels are elevatedininParkinson’s ventricular disease, cerebroinspinal erythropoietic lineage.parkinsonism Biochem Biophys Res Commun fluid in juvenile and Parkinson’s disease. 2007;358:104–110. Neurosci Lett 1996;211:13–16. 98. A, Uitti Wszolek , ZK, Yamada disease, T. Altera96.Baba Kim Y, S, Kuroiwa Seo JH, Suh UH. RJ, a-synuclein Parkinson’s and tions of T-lymphocyte populations in Parkinson’s disease. ParAlzheimer’s disease. Park Relat Disord 2004;10:S9–S13. 2005;11:493–498. 97.kinsonism Nakai M,Relat FujitaDisord M, Waragai M, et al. Expression of alpha-syn. DJALDETTI 99. ETLiAL. QX, aCampbell BC,protein McLean CA, etinal.Parkinson’s Platelet aand uclein, presynaptic implicated disease, g-synucleins in Parkinson’s and normal in erythropoietic lineage.disease Biochem Biophyscontrol Res subjects. Commun J 2007;358:104–110. Alzheimer’s Dis 2002;4:309–315. . Retinal 100. J, Tarkowski A, Ekman R, Ewing A. Discovery of 98.Bergquist Baba Y, Kuroiwa A, Uitti RJ, Wszolek ZK, Yamada T. Alteraamine in endogenous catecholamines in lymphocytes and evidence tions of T-lymphocyte populations in Parkinson’s disease. for Parcatecholamine regulation of lymphocyte function via an autokinsonism Relat Disord 2005;11:493–498. opaminerloop. Campbell Proc Natl Acad Sci USA CA, 1994;91:12912–12916. 99.crine Li QX, BC, McLean et al. Platelet a- and hav Rev 101. Cook-Mills JM,in Cohen RL, Perlman Chambers DA. subjects. Inhibig-synucleins Parkinson’s disease RL, and normal control tion of lymphocyte by catecholamines: evidence for a J Alzheimer’s Dis activation 2002;4:309–315. on’s disnon-classical mechanism of catecholamine action. Immunology cephalogr 1995;85:544–549. 102. Carr L, Tucker A, Fernandez-Botran R. In vivo administration ormalities of L-dopa or dopamine decreases the number of splenic IFN gs disease. producing cells. J Neuroimmunol 2003;142:166–169. 103. Chen H, O’Reilly EJ, Schwarzschild MA, Ascherio A. PeriphK, Przuneral inflammatory biomarkers and risk of Parkinson’s disease. Movement Vol.2008;167:90–95. 24, No. 6, 2009 kinsonian Am Disorders, J Epidemiol 104. Schapira AH. Oxidative stress in Parkinson’s disease. NeuropaHaas M, thol Appl Neurobiol 1995;21:3–9. late with 105. Jenner P, Olanow CW. Understanding cell death in Parkinson’s s disease. disease. Ann Neurol 1998;44:72–84. 106. Schapira AH, Cooper JM, Dexter D, Clark JB, Jenner P, MarsMovement Disorders, Vol. 24, No. 6, 2009I deficiency in Parkinson’s disL, Orsini den CD. Mitochondrial complex grams to ease. J Neurochem 1990;54:823–827. patients 107. Younes-Mhenni S, Frih-Ayed M, Kerkeni A, Bost M, Chazot 2003;20: G. Peripheral blood markers of oxidative stress in Parkinson’s disease. Eur Neurol 2007;58:78–83. retinas of 108. Ihara Y, Chuda M, Kuroda S, Hayabara T. Hydroxyl radical Vis Sci and superoxide dismutase in blood of patients with Parkinson’s disease: relationship to clinical data. J Neurol Sci 1999;170:90– utonomic 95. 7;38:2–7. 109. Schapira AH, Mann VM, Cooper JM, et al. Anatomic and disrkinson’s ease specificity of NADH CoQ1 reductase (complex I) deficiency in Parkinson’s disease. J Neurochem 1990;55:2142– repineph2145. on’s dis110. Mizuno Y, Ohta S, Tanaka M, et al. Deficiencies in complex I subunits of the respiratory chain in Parkinson’s disease. Bio- tion of lymphocyte activation by catecholamines: evidence for a action. 100.non-classical Bergquist J, mechanism Tarkowski of A, catecholamine Ekman R, Ewing A. Immunology Discovery of 1995;85:544–549. endogenous catecholamines in lymphocytes and evidence for 102. Carr L, Tucker A, Fernandez-Botran R. Infunction vivo administration catecholamine regulation of lymphocyte via an autoofcrine L-dopa dopamine decreases the number ofR.Djaldetti splenic IFNetg-al. loop.orProc Natl Acad Sci USA 1994;91:12912–12916. cells. Neuroimmunol 2003;142:166–169. 101.producing Cook-Mills JM,J Cohen RL, Perlman RL, Chambers DA. Inhibi103. Chen H, lymphocyte O’Reilly EJ,activation Schwarzschild MA, Ascherio A. Periphtion of by catecholamines: evidence for a eral inflammatory biomarkers and risk of Parkinson’s disease. non-classical mechanism of catecholamine action. Immunology Am J Epidemiol 2008;167:90–95. 1995;85:544–549. 104. Oxidative stress in Parkinson’s disease. Neuropa102.Schapira Carr L, AH. Tucker A, Fernandez-Botran R. In vivo administration thol Appl Neurobiol 1995;21:3–9. of L-dopa or dopamine decreases the number of splenic IFN g105. Jenner P, Olanow Understanding cell death in Parkinson’s producing cells. JCW. Neuroimmunol 2003;142:166–169. Ann Neurol EJ, 1998;44:72–84. 103.disease. Chen H, O’Reilly Schwarzschild MA, Ascherio A. Periph106. Schapira AH, Cooperbiomarkers JM, Dexterand D, risk Clark Jenner P, disease. Marseral inflammatory of JB, Parkinson’s den Mitochondrial complex I deficiency in Parkinson’s disAmCD. J Epidemiol 2008;167:90–95. J Neurochem 1990;54:823–827. 104.ease. Schapira AH. Oxidative stress in Parkinson’s disease. Neuropa107. Younes-Mhenni S, Frih-Ayed M, Kerkeni A, Bost M, Chazot thol Appl Neurobiol 1995;21:3–9. Peripheral bloodCW. markers of oxidative 105.G.Jenner P, Olanow Understanding cellstress deathininParkinson’s Parkinson’s disease. disease.Eur AnnNeurol Neurol2007;58:78–83. 1998;44:72–84. 108. Y, Chuda M, Kuroda S, Hayabara Hydroxyl radical 106.Ihara Schapira AH, Cooper JM, Dexter D, ClarkT.JB, Jenner P, Marsand dismutasecomplex in bloodI of patients in with Parkinson’s densuperoxide CD. Mitochondrial deficiency Parkinson’s disdisease: to clinical data. J Neurol Sci 1999;170:90– ease. J relationship Neurochem 1990;54:823–827. 107.95. Younes-Mhenni S, Frih-Ayed M, Kerkeni A, Bost M, Chazot 109. Schapira AH, Mann Cooper JM, et al. stress Anatomic and disG. Peripheral bloodVM, markers of oxidative in Parkinson’s ease specificity of NADH CoQ1 reductase (complex I) defidisease. Eur Neurol 2007;58:78–83. in Chuda Parkinson’s disease.S, JHayabara Neurochem 1990;55:2142– 108.ciency Ihara Y, M, Kuroda T. Hydroxyl radical 2145. and superoxide dismutase in blood of patients with Parkinson’s 110. Mizuno Ohta S, Tanaka M, etdata. al. Deficiencies complex I disease:Y,relationship to clinical J Neurol Sciin1999;170:90– subunits of the respiratory chain in Parkinson’s disease. Bio95. Biophys Commun 1989;163:1450–1455. 109.chem Schapira AH,Res Mann VM, Cooper JM, et al. Anatomic and dis111. Shinde S, Pasupathy K. Respiratory-chain enzyme activities in ease specificity of NADH CoQ1 reductase (complex I) defiisolated of disease. lymphocytes from patients with Parciency mitochondria in Parkinson’s J Neurochem 1990;55:2142– kinson’s 2145. disease: preliminary study. Neurol India 2006;54:390– 110.393. Mizuno Y, Ohta S, Tanaka M, et al. Deficiencies in complex I 112. Barroso Y, Huertas al. Respiratory subunitsN,of Campos the respiratory chainR,in etParkinson’s disease.chain Bioenzyme activities in Commun lymphocytes from untreated patients with chem Biophys Res 1989;163:1450–1455. disease. Clin 1993;39:667–669. 111.Parkinson’s Shinde S, Pasupathy K. Chem Respiratory-chain enzyme activities in 113. Parker WD, Jr, Boyson SJ, Parks JK. Abnormalities of the isolated mitochondria of lymphocytes from patients withelecPartron transport chainpreliminary in idiopathic Parkinson’s Ann Neukinson’s disease: study. Neurol disease. India 2006;54:390– rol 1989;26:719–723. 393. 114. K, Wiedemann FR, R, Wallesch CW, Kunz WS. 112.Winkler-Stuck Barroso N, Campos Y, Huertas et al. Respiratory chain Effect of coenzyme on the mitochondrial function of skin enzyme activities inQ10 lymphocytes from untreated patients with fibroblasts from Parkinson patients. J Neurol Sci 2004;220:41– Parkinson’s disease. Clin Chem 1993;39:667–669. 113.48. Parker WD, Jr, Boyson SJ, Parks JK. Abnormalities of the elec115. Mann VM, Cooper Krige D,Parkinson’s Daniel SE, Schapira tron transport chain JM, in idiopathic disease. Ann AH, NeuMarsden CD. Brain, skeletal muscle and platelet homogenate rol 1989;26:719–723. in Parkinson’s disease. Brain 114.mitochondrial Winkler-Stuckfunction K, Wiedemann FR, Wallesch CW, 1992;115: Kunz WS. 333–342. Effect of coenzyme Q10 on the mitochondrial function of skin 116. Yoshino H, from Nakagawa-Hattori Y, Kondo T, Mizuno Y. Mitofibroblasts Parkinson patients. J Neurol Sci 2004;220:41– chondrial complex I and II activities of lymphocytes and plate48. in Parkinson’s disease. NeuralD,Transm 115.lets Mann VM, Cooper JM, JKrige Daniel1992;4:27–34. SE, Schapira AH, 117. Ihara Y, Chuda M, Kuroda Hayabara Hydroxyl radical Marsden CD. Brain, skeletalS, muscle andT.platelet homogenate and superoxide function dismutaseininParkinson’s blood of patients Parkinson’s mitochondrial disease.with Brain 1992;115: disease: relationship to clinical data. J Neurol Sci 1999;170:75– 333–342. 116.76. Yoshino H, Nakagawa-Hattori Y, Kondo T, Mizuno Y. Mitochondrial complex I and II activities of lymphocytes and platelets in Parkinson’s disease. J Neural Transm 1992;4:27–34. 117. Ihara Y, Chuda M, Kuroda S, Hayabara T. Hydroxyl radical and superoxide dismutase in blood of patients with Parkinson’s disease: relationship to clinical data. J Neurol Sci 1999;170:75– 76. 9 多系統萎縮症の診断を目的とした神経画像の 基準案 Proposed Neuroimaging Criteria for the Diagnosis of Multiple System Atrophy * David J. Brooks, MD, Dsc, FRCP and Klaus Seppi MD for the Neuroimaging Working Group on MSA * Division of Neuroscience, Faculty of Medicine, Imperial College London, London, United Kingdom 本稿では,多系統萎縮症(multiple system atrophy; 比較・検討する。本研究の結果, 神経画像バイオマーカー MSA)の形態画像と機能画像に関する最新の知見をレ は臨床評価と並んで貴重な裏付けとなるデータを提示 ビューする。また,MSA と他のパーキンソン症候群と するものの,診断のための代替マーカーとしては使用で の鑑別診断における各種画像診断法の有用性について きないとの結論に達した。 Movement Disorders, Vol. 24, No. 7, 2009, pp. 949–964 Key Word 多系統萎縮症,パーキンソン,MRI,PET,SPECT 略 語 本論文中の略語一覧は P25 をご参照下さい。 多系統萎縮症(multiple system atrophy; MSA)の疾患 MSA 患者 10 名以上,対照群 10 名以上を対象としている。 スペクトルには,シャイ ・ ドレーガー症候群,線条体黒 研究を選択する際の要件として,診断の感度および特異 質変性症(striatonigral degeneration; SND または MSA-P) , 度を算出できるよう,患者は確立された診断基準と詳細 孤 発 性 オ リ ー ブ 橋 小 脳 萎 縮 症(sporadic なデータに基づいて診断されていることとした。また, olivopontocerebellar atrophy; sOPCA または MSA-C)が含 試験期間を通じ,同一の磁気共鳴(magnetic resonance; まれる。病理学的には,黒質(substantia nigra; SN) ,線 MR)プロトコルか,少なくとも同一の MR 装置または同 条体, 脳幹・小脳核, 脊髄中間外側柱のグリアおよびニュー 一の磁場強度を用いていることを要件とした。試験期間 ロンに,嗜銀性のα—シヌクレイン陽性封入体が出現する を通じて異なる MR プロトコルまたは磁場強度を用いた ことを特徴とする。MSA の診断に関する現行のコンセン 研究は採用せず,表に記載しなかった。 サス・ガイドラインは画像所見には触れておらず,診断 は純粋に臨床基準に基づいている。本稿では,神経画像 従来型 MRI の潜在的な価値と役割を提示し,考察した。実際に,コ 従来の 1.5T MRI で認められる MSA 患者の異常所見に ン セン サ ス 基 準 の 改 訂 版には, 「MSA の 可 能 性 あり は,萎縮,T2 低信号, 「スリット様」辺縁部高信号などの (possible MSA) 」の診断カテゴリーのために神経画像基 被 殻 異 常 だ け で なく,下 位 脳 幹・中 小 脳 脚(middle 準が追加されている。 cerebellar peduncle; MCP) ・小脳の萎縮のほか,脳橋・ MCP・小脳の高信号も含まれる 1,2,7,12,24–28。MSA とパーキ MSA における形態画像 10 ンソン病(Parkinson’ s disease; PD)は被殻萎縮によって鑑 別できると考えられるが,PD 患者に被殻の T2 低信号や MSA の領域では,過去 20 年間に形態画像検査の診断 被殻の辺縁部高信号が認められる場合もある(Table 1 参 精度に関する研究成果がいくつか報告されている。これ 照)5,7,29–31。実際に,3.0T MRI の T2 強調画像における被 らの研究は Table 1 ~ 4 にまとめたが,いずれの試験も 殻の辺縁部高信号は,非特異的かつ正常な所見である 32。 1 MSA 52/PD 88/HC 29 MSA-P 24/PD 27 MSA-P 10/PD 11/HC 7 MSA-P 36/MSA-C 27/PD 30 MSA-P 14/MSA-C 4/PD 21 MSA-C 30/IDCA-P 11 Righini et al., 20024 Schocke et al., 20025 Lee et al., 20046 Bhattacharya et al., 20027 Burk et al., 20058 MSA-P 15/PD 65/PSP 10 MSA 28/PD 25 Cohort size von Lewinski et al., 20073 Kraft et al., 1999 2 Konagaya et al., 1994 Author/Year Putaminal rim Putaminal rim Putaminal signal changes at T2 Putaminal rim and hypointense putamen Hypointense putamen Putaminal signal changes using T2* GE sequences Signal loss dorsolateral putamen Signal loss dorsolateral putamen and hyperintense putaminal rim SIPUT/CAUD Putaminal signal changes on FSE and CSE FSE CSE (proton density—putaminal hyperintensity) CSE (T2–putaminal hypointensity) Putaminal abnormalities at T2 Putaminal atrophy Putaminal rim 10 supra- and infratentorial MRI findings characteristic for MSA; findings with the highest sensitivity (>70%) are given below; specificity values vs. PD are given Putaminal hypointensity Putaminal atrophy Putaminal rim Dilatation 4th ventricle MCP atrophy Pontine atrophy Cerebellar atrophy Signal increase cerebellum Signal increase MCP Several putaminal and infratentorial abnormalities on MRI; significant MRI findings differentiating MSA-P from PD are given below Putaminal atrophy Putaminal hypointensity (moderate/severe) Putaminal rim (moderate/severe) Midbrain atrophy Pontine atrophy Atrophy medulla oblongata Signal increase MCP Hot cross bun sign Several supra- and infratentorial MRI findings characteristic for MSA; significant MRI findings differentiating MSA-C from IDCA-P are given below MCP atrophy Brainstem atrophy Hypointensity dentate nuclei Hot cross bun sign Hyperintensity MCP Diagnostic predictor 60 80 45 88 83 69 42 65 64 36 61 61 Sensitivity (%) 93 100 57 97 87 43 43 36 36 43 43 21 7 82 82 100 100 100 100 100 95 100 100 100 100 100 70 87 90 87 87 87 90 97 100 100 91 vs. PD/100 vs. HC 100 88 100 91 vs. PD 97 vs. PD 95 vs. PD 100 91 vs. PD/60 vs. PSP 100 100 Specificity (%) 950 90 (MSA-P)/82 (MSA-C) 83 (MSA-P) 72 (MSA-P) 78 (MSA-P)/93 (MSA-C) 75 (MSA-P)/100 (MSA-C) 100 (MSA-C) 96 (MSA-C) 82 (MSA-C) 85 (MSA-C) 1 MSA の診断における従来型 MRI TABLE 1.Table Diagnostic accuracy of conventional MRI forの診断精度 the diagnosis of MSA D.J. Brooks and K. Seppi D.J. BROOKS AND K. SEPPI Movement Disorders, Vol. 24, No. 7, 2009 11 多系統萎縮症の診断を目的とした神経画像の基準案 MSA-P 15/PD 20/HC 11 Seppi et al., 200611 MSA =多系統萎縮症,PD =パーキンソン病,PSP =進行性核上性麻痺,HC =健常対照,GE =グラディエントエコー,SI =背外側被殻の信号強度(signal intensity; PUT/CAUD (SI) SI)/尾状核頭部の dorsolateral MSA, multiple system atrophy; PD, Parkinson’s disease; PSP, progressive supranuclear palsy; HC, healthy controls; GE, gradient echo; SIPUT/CAUD, signal intensity putamen/SI head of caudate =従来型スピンエコー,MCP nucleus; FSE, fast spin echo; CSE, conventional spin = echo; MCP,に一致しない小脳外の症状を伴う孤発性小脳性運動失調症,SCP middle cerebellar peduncle; IDCA-P, idiopathic cerebellar ataxia with extracerebellar presenSI,FSE =高速スピンエコー,CSE =中小脳脚,IDCA-P MSA-C =上小脳脚 tation not corresponding to MSA-C; SCP, superior cerebellar peduncle. 1.0T で実施した 1 件 3 を除き,他の試験はすべて 1.5T で実施。 All but one study3, which was performed at 1.0 T, were performed at 1.5 T. 100 (vs. PD and HC) 100 (vs. PD and HC) 100 (vs. PD and HC) MSA-P 11/PD 12/PSP 20/HC 7 Nicoletti et al., 2006 Paviour et al., 200710 MSA 16 (MSA-P in 13)/PD 26/ HC 14 Putaminal atrophy, putaminal hypointensity, putaminal rim, brainstem atrophy, hyperintensity of the MCP, and cruciform hyperintensity of the pons; significant MRI findings differentiating MSA-P from PD and HC are given below Putaminal hypointensity Putaminal rim Hot cross bun sign Presence of at least one of the abnormal features mentioned earlier Putaminal rim, putaminal hypointensity, signal increases in MCP and pons Putaminal hypointensity Putaminal rim Signal increase pons Signal increase MCP Putaminal abnormalities Putaminal rim (moderate/severe) Putaminal hypointensity (moderate/severe) Putaminal atrophy 27 55 45 36 38 56 50 100 47 47 67 100 96 vs. PD/100 vs. HC 100 96 vs. PD/100 vs. HC Specificity (%) Sensitivity (%) Diagnostic predictor Author/Year 9 Cohort size TABLE 1.(つづき) (Continued) Table 1 100 vs. PD/80 vs. PSP 83 vs. PD/90% vs. PSP 100 vs. all groups 100 vs. all groups NEUROIMAGING CRITERIA FOR THE DIAGNOSIS MSA 951 MSA では, 脳橋およびOF MCP が高信号を呈し 「十字サイン」 が認められる場合がある(Figure 1) 。ただし,この MSA 5,7,29–31 Table 1). In fact, on T2-weighted images at 3.0 の特徴は,他の原因によりパーキンソニズム患者にもみ T, a hyperintense putaminal rim is a nonspecific, normal 33,34 られる場合がある 。 within the pons and finding.32 Signal hyperintensities 全体的にみると,1.5T MRI の場合,MSA MCPs in MSA may occasionally result in theに関連して ‘‘hot-cross bun’’ sign (Fig. 1) and, while a feature of MSA, may 2,5,7,12,24–28 認められる被殻・テント下構造の信号変化と萎縮 occur also in patients with Parkinsonism because of other は,PD または健常対照被験者との比較において特異性 causes.33,34 5–7,26 Overall, the specificity of the MRI signal MSA changes が高い所見である 。しかし,報告されている の and atrophy at 1.5 T associated with MSA in putamen compared with and infratentorial structures その感度は至適レベルには達していない(Figure 2 およ PD or healthy controls is high,5–7,26 but their reported 5,6,28,35,36to sensitivity detect MSA is inconsistent in the び 3) 。実際に,最近の研究では,MSA の罹病期 literature and suboptimal in the early disease stages 間と脳橋・被殻の信号異常との間には明らかに関連性の (Fig. 2 and 3).5,6,28,35,36 A recent study in fact suggests 37 あることが示唆されている 。MSAdisease の検出感度は,スラ a positive association between duration and signal abnormalities in the pons as well as in the putaイス厚などの撮影技術面の変更や,従来型スピンエコー men in MSA.37 Sensitivity can be somewhat improved (conventional spin-echo; CSE) ,または T2* 強調グラディ by modifying technical aspects such as slice thickness エントエコーを用いることで,ある程度向上させること and the use of conventional spin-echo (CSE) or T2*3–5,38 The specificity weighted3–5,38 gradient echo sequences. ができる 。ただし,MSA と他のタイプの非定型パー of conventional MRI for discriminating MSA from キンソン症候群(APS)との鑑別において,従来型 other types of APS is suboptimal27,30 (Table 1). MRI 27,30 Evidence supporting a role for conventional MRI の特異度は至適レベルには達していない (Table 1) 。in the diagnosis of MSA-C is scarce. Burk et al.8 investiMSA-C の診断において,従来型 MRI の有用性を裏付 gated the discriminative validity of conventional MRI 8 ける証拠はごくわずかである。Burk は,MSA-C 患者 (cMRI) at 1.5 T in patients withらsporadic cerebellar ataxia including patients・パーキンソニズム(idiopathic with MSA-C and patients と孤発性小脳性運動失調症 with idiopathic cerebellar ataxia and Parkinsonism cerebellar ataxia and Parkinsonism; IDCA-P)患者を含む散 (IDCA-P). Patients with MSA-C were characterized by a 発性小脳性運動失調症患者を対象に,従来の 1.5T MRI higher frequency and severity of MRI abnormalities (atrophic changes and additional hyperintense signal による鑑別の妥当性を検討した。MSA-C 患者では,MCP changes) of the MCP and pons. The presence of these と脳橋の MRI 異常所見(萎縮性変化とさらなる高信号変 MRI features thus points to the diagnosis of MSA-C and 化)の頻度および重症度が高いという特徴がある。した helps differentiate MSA-C from other types of sporadic cerebellar with extracerebellar が っ て,こataxia の ような MRI 所 見 が 認features め ら れ(Table る 場 合1). は 検出感度は文献間で一致しておらず, 初期の MSA の場合, 2,5,7,12,24–28 MSA-C と診 断され る。また,これ らの MRI 所 見 は, Quantitative Assessment of Regional Cerebral Atrophy Using MRI Planimetry and Volumetry MSA-C と小脳外所見を伴う他のタイプの散発性小脳性運 Using MRI volumetry (MRV) with semiautomatic segmentation techniques with a region-of-interest (ROI) approach at 1.5 T, volume loss of different supratentorial and infratentorial brain structures, includMRI を用いた面積測定および容積測定による局所 ing striatum, brainstem, and cerebellum, has been 的脳萎縮の定量的評価 reported in patients with MSA12,39. On the basis of 関心領域(region-of-interest; ROI)法および半自動領域 individual structure volumetry, differentiation of MSA 12 Applicafrom other parkinsonian disorders is scarce.volumetry; 抽出法を用いた 1.5T MRI 容 積 測定(MRI tion of a stepwise discriminant analysis in patients MRV)に関する研究では,MSA 患者において線条体, with MSA, PSP, PD, and healthy controls allowed dis脳幹,小脳をはじめとする様々なテント上およびテント crimination of all 12 patients with MSA-P and 15 of 17 patients with MSA-C from the 12,39 PD 。個々の脳構 patients and 下脳構造の容積減少が報告されている healthy controls, whereas differentiation of patients 造の容積測定結果に基づいて,MSA と他のパーキンソン 2). with MSA from PSP was poor12 (Table 動失調症との鑑別に役立つ(Table 1) 。 障害とを鑑別することはほとんどできない 12。MSA 患者, 進行性核上性麻痺(progressive supranuclear palsy; PSP) Movement Disorders, Vol. 24, No. 7, 2009 12 952 D.J. Brooks and K. Seppi D.J. BROOKS AND K. SEPPI Table 2 MSA の診断を目的とした MRI による面積測定および容積測定による局所脳萎縮の定量的評価における MRI の TABLE 2. Diagnostic accuracy of MRI methods for the quantitative assessment of regional cerebral atrophy including MR診断精度 planimetry/-volumetry for the diagnosis of MSA Author/Year Cohort size Diagnostic predictor MSA-P 12/MSA-C 17/PD Atrophy of the caudate nucleus, putamen, Schulz 11/PSP 6/HC 16 brainstem, and cerebellum using MRV et al., 199912 Model including volumes of brainstem, caudate nucleus, putamen, cerebellum (using stepwise linear discrimination model)a MSA-C 33/IDCA-P Burk 13/HC 16 et al., 200413 Nicoletti et al., 20069 Atrophy of the caudate nucleus, putamen, brainstem, and cerebellum using MRV. Model including volumes of cerebellum, brainstem, caudate nucleus and putamen, (using stepwise linear discrimination model)b MCP width on T1 MSA 16 (MSA-P in 13)/PD 26/HC 14 MCP with <8 mm Single and combined quantitative imaging measurements of brain structures on T1: midbrain area (M), pontine area (P), MCP width (MCP), SCP width (SCP). Sensitivity and specificity given only compared with PSP. P/M ratio MCP/SCP ratio MR parkinsonism index 5 (P/M)*(MCP/ SCP) MSA-P 19/PD Quattrone 108/PSP 33/HC 50 et al., 200814 Sensitivity (%) 67 (MSA-P)/ 76 (MSA-C) Specificity (%) 100 (MSA-P vs. PD)/ 100 (MSA-P vs. HC)/ 67 (MSA-P vs. PSP/ 100 (MSA-C vs. PD)/ 82 (MSA-C vs. HC)/100 (MSA-C vs. PSP) 82 100 100 100 95 90 100 97 94 100 a No PD patient was classified as having MSA-P or vice-versa; 3 of the PD patients were classified havingまたは MSA-C orに分類された。 PSP; discrimMSA-P に分類された PD 患者または PD に分類された MSA-P however, 患者はいなかったが,PD 患者のうち 3 名は as MSA-C PSP ination of patients with MSA from PSP was poor. b 患者と PSP 患者との鑑別は十分にできなかった。 MSA There was substantial cerebellar atrophy in both cerebellar groups, whereas additional brainstem atrophy was significantly more pronounced in b 小脳疾患の両患者群で実質的な小脳萎縮が認められたが,脳幹萎縮は MSA-C 患者の方が有意に顕著であった。尾状核および被殻の絶対的 MSA-C patients. Absolute caudate and putamen atrophy was found to be restricted to single MSA-C individuals, whereas group comparisons of mean volumes did not yield significant differences from controls. One control subject (6%) and 6 MSA-C patients (18%) were classified as な萎縮が認められたのは MSA-C 患者のみであったが, 平均容積の群間比較では対照群との間に有意差はみられなかった。対照群の 1 名(6%) IDCA-P. および MSA-C 群のsystem 6 名(18%)は IDCA-P に分類された。 MSA, multiple atrophy; PD, Parkinson’s disease; PSP, progressive supranuclear palsy; HC, healthy controls; IDCA-P, idiopathic cereMSAataxia =多系統萎縮症,PD =パーキンソン病,PSP =進行性核上性麻痺,HC = MSA-C bellar with extracerebellar presentation not corresponding to MSA-C; MCP, =健常対照,IDCA-P middle cerebellar peduncle; SCP, に一致しない小脳外の症状を superior cerebellar peduncle. All studies were performed at 1.5 T. 伴う孤発性小脳性運動失調症,MCP =中小脳脚,SCP =上小脳脚 試験はすべて 1.5T 13 で実施。 a Burk et al. used MRV with ROIs to study the atrophy of the cerebellum, brainstem, caudate nucleus, and 患者,PD putamen,患者,健常対照被験者を対象にステップワイ in patients with sporadic cerebellar ataxia (including patients with MSA-C and comズ判別分析を行ったところ,MSA-P 患者IDCA-P) 12 名全ておよ pared with control subjects. By application of stepwise び MSA-C 患者 17 名中 15 名と,PD 患者および健常対照 discriminant analysis, diagnosis could be correctly pre被験者とを鑑別することができたが,MSA PSP 患 dicted in 94% of the controls, 82% of患者と the MSA-C 12 patients (Table 2). patients, and 100% of the IDCA-P 者との十分な鑑別はできなかった (Table 2) 。 More recently, studies using voxel-based morphome13 Burk ら は,ROI 法を用いた により,散発性小 try (VBM) have been performedMRV in patients with MSA confirming previous ROI-based volumetric studies 脳性運動失調症患者(MSA-C 患者および IDCA-P 患者を showing basal ganglia and infratentorial volume loss in 含む)と対照被験者の小脳,脳幹,尾状核,被殻の萎縮 MSA patients40–45 with structural abnormalities in を比較・検討した。ステップワイズ判別分析では,対照 infratentorial brain regions being more pronounced in 44 Furthermore, these MSA-C than in MSA-P patients. 群の 94%, MSA-C 患者の 82%, IDCA-P 患者の 100%で, data also revealed volume loss in several cortical 正確に診断を予測することができた(Table 2) 。 regions in patients with MSA-P and MSA-C. However, つい最近,MSA 患者を対象にボクセル単位形態計測 VBM is not appropriate for routine diagnostic work-up of individual patients. 法(voxel-based morphometry; VBM)を用いた試験が行 As an indirect measure of brain structures known to be atrophic in MSA, groups have applied simple quanROI 法による容積測定試験結果が確認された。さらに, titative measures of diameters and areas of different structures on MSA-C MRI for患者では,いくつかの皮質領域の the differential diagnosis of MSA-P 患者と MSA from other neurodegenerative parkinsonian disor容積が減少していることも明らかになった。しかし, ders. The average MCP width was shown to be signifiVBM cantlyは個々の患者を対象としたルーチンの診断検査には smaller in patients with MSA than in those with PD or control subjects without any overlap between 適していない。 MSA patients and PD patients or healthy subjects.9 MSA において萎縮が確認されている脳構造の間接的 The separation of MSA from PSP patients, however, withと他の神経 the wellwas suboptimal.9,14 (Table 2) Consistent 測定法として,複数の研究グループが MSA known atrophy of the pons in MSA, the area of the 変性パーキンソン障害との鑑別診断を目的に,様々な構 pons measured on midsagittal T1-weighted MR images 造の MRI 画像上の直径と面積を単純に定量してきた。平 has been shown to be significantly smaller in MSA-P patients compared with patients PD and PSP as 均 MCP 幅は MSA 患者の方が PD with 患者または対照被験者 well as healthy controls with overlapping individual よりも有意に小さく,MSA 患者と PD 患者または健常被 values.14,46 On the other hand, midbrain areas meas験者との間に重複はみられないことが明らかにされてい ured on midsagittal T1-weighted MR images are sig9 nificantly smaller 患者と in PSPPSPpatients compared with る 。ただし,MSA 患者との鑑別精度は至適 われ,MSA 患者では大脳基底核およびテント下の容積が レベルには達していない 9,14(Table 2) 。正中矢状断 T1 強 減少し 40–45,MSA-C 患者は MSA-P 患者よりもテント下 調 MRI 画像で測定した脳橋の面積は,MSA でよく知ら 脳領域の構造異常が顕著である れている脳橋の萎縮と一致して,MSA-P 患者の方が健常 Movement Disorders, Vol. 24, No. 7, 2009 44 ことを示した以前の 13 NEUROIMAGING CRITERIA FOR THE DIAGNOSIS OF MSA 953 多系統萎縮症の診断を目的とした神経画像の基準案 TABLE 3. Diagnostic accuracy of quantitative structural MR-based techniques including diffusion-weighted Table 3 MSA の診断における拡散強調画像と磁化移動画像を含む定量的形態 MR and magnetization transfer imaging for the diagnosis of MSA MRI の診断精度 Author/Year Cohort size Schocke et al., 20025 MSA-P 10/PD 11/HC 7 Seppi et al., 200415 MSA-P 15/PD 17/HC 10 including all patients studied by Schocke et al., 2002 MSA-P 11/PD 17/HC 10 Schocke et al., 200416 11 Seppi et al., 2006 Nicoletti et al., 200617 Paviour et al., 200710 Ito et al., 200718 Eckert et al., 200419 MSA-P 15/PD 20/HC 11 including all patients studied by Schocke et al., 2004 MSA-P 16/PD 16/PSP 16/ HC 15 MSA-P 11/PD 12/PSP 20/ HC 7 MSA 20 (MSA-P 10)/PD 21/HC 20 MSA 12/PD 15/PSP 10/HC 20 Diagnostic predictor ADCs in the basal ganglia, pons, white matter; sensitivity and specificity values given for putaminal ADCs (best discriminator) Putaminal ADCs > 0.760 3 103 mm2/s Striatal ADCs Striatal ADCs > 0.795 3 103 mm2/s Putaminal ADC values Putaminal ADC > 0.80 3 103 mm2/s Putaminal ADC values of the whole, anterior and posterior putamen Putaminal ADC > 0.80 3 103 mm2/s Posterior putaminal ADC > 0.80 3 103 mm2/s ADC values in the basal ganglia, pons, white matter; sensitivity and specificity values given for putaminal and MCP diffusivity (best discriminators) MCP ADC > 0.875 3 103 mm2/s Putaminal ADC > 0.953 3 103 mm2/s ADC values in the basal ganglia, pons, MCP, SCP, thalamus; sensitivity and specificity values given for MCP diffusivity (in the article) MCP ADC > 0.733 3 103 mm2/s FA and ADC in the pons, cerebellum and putamen at 3.0T; sensitivity and specificity values given for MSA-P vs. PD ADC pons > 0.98 3 103 mm2/s ADC cerebellum > 0.96 3 103 mm2/s ADC putamen > 0.83 3 103 mm2/s FA pons < 0.38 FA cerebellum < 0.30 FA putamen < 0.35 both low FA and high ADC values in any of the three areas MTR in the globus pallidus, putamen, caudate nucleus, SN, and white mattera Model including MTRs of globus pallidus, putamen and caudate nucleus (using stepwise linear discrimination model) Sensitivity (%) Specificity (%) 100 100 (vs. PD and HC) 93 100 (vs. PD and HC) 100 100 (vs. PD and HC) 93 100 100 (vs. PD and HC) 100 (vs. PD and HC) 100 100 100 (vs. all groups) 100 (vs. PD and HC)/ 81 (vs. PSP) 91 82 (vs. all groups)/ 84 (vs. PSP) 70 60 70 70 70 70 90 70 88 64 100 64 88 100 58 100 (vs. PD and HC)/ 90 (vs. PSP) a The main finding in this study was a change in the MT ratio (MTR) in the globus pallidus, putamen, caudate nucleus, substantia nigra, and a この試験の主な所見は,PD,MSA,PSP 患者の淡蒼球,被殻,尾状核,黒質,白質における MTR の変化であり,基礎疾患の病理学的特徴 white matter in PD, MSA, and PSP patients, matching the pathological features of the underlying disorder. MTRs were significantly reduced in と一致した。MTR は,MSA 患者の被殻では PD 患者や健常対照よりも有意に低下しており,また PSP,MSA,PD 患者の黒質でも有意に低下 the putamen in MSA patients compared with PD patients and healthy controls as well as in the substantia nigra in patients with PSP, MSA, and PD. MSA, multiple system atrophy; PD, Parkinson’s disease; HC, healthy controls; ADC, apparent diffusion coefficient–in the studies by Schocke していた。 etMSA al., 2002 and Seppi et al., =パーキンソン病,HC 2004 measured in z-slice=健常対照,ADC direction only, in =みかけの拡散係数〔Schocke the other studies ADCs were averaged over three orthogonal measure=多系統萎縮症,PD ら(2002)および Seppi ら(2004)の ments, thus representing the trace of the diffusion tensor; PSP, progressive supranuclear palsy; MCP, middle cerebellar peduncle; SCP, superior 試験では z 軸方向のみで測定し,別の試験では ADC を 3 つの直交測定値で平均したため,拡散テンソルのトレースとなっている〕 ,PSP =進 cerebellar peduncle; FA, fractional anisotropy; MTR, magnetization transfer ratio; SN, substantia nigra. which was performed at 3.0 T, were=異方性比率,MTR performed at 1.5 T. =磁化移動比,SN =黒質 All but one study18, =中小脳脚,SCP 行性核上性麻痺,MCP =上小脳脚,FA 3.0T で実施した 1 件 18 を除き,他の試験はすべて 1.5T で実施。 healthy controls and patients with PD and MSA-P.14,46 対照被験者,PD 患者,PSP 患者よりも有意に小さかった Calculation of the ratio between pontine and midbrain areas discriminated completely MSA-P patients from が,個々の数値には重複のあることが明らかにされてい patients with PD and PSP and healthy controls in one 14,46 46 るseries, 。一方,正中矢状断 T1 強調 MRI 画像で測定した though in another individual values overreason, Quattrone proposed an lapped.14 For this 中脳面積は,PSP 患者の方が健常対照被験者,PD 患者, 14 index termed the MR Parkinsonism index (MRPI), このため,Quattrone パーキンソニズム指標(MR which was calculatedはbyMR multiplying the pontine area- midbrain areaindex; ratio MRPI)と呼ばれる指標を提唱した。 (P/M) by the MCP width-SCP Parkinsonism width ratio (MCP/SCP) [(P/M)*(MCP/SCP)]. (Table MRPI 脳橋 面 積was と中 脳 面 積 の higher 比(pontine area2) Theは, MRPI value significantly in patients with PSParea than in patients with PD and MSA-P as well midbrain ratio; P/M)に, MCP 幅と上小脳脚(superior MSA-P 患者よりも有意に小さい 14,46。 ある症例集積研究は, cerebellar peduncle; SCP)幅の比(MCP width-SCP width 脳橋面積と中脳面積の比を求めることで,MSA-P 患者と ratio; MCP/SCP)を乗じて求められる〔(P/M) × (MCP/ PD 患者,PSP 患者,健常対照被験者との完全な鑑別に SCP)〕 (Table 2) 。MRPI 値は,PSP 患者の方が PD 患者, 成功したが 46,別の研究では各数値に重複がみられた 14。 MSA-P 患者,対照被験者よりも有意に高いため,この指 Movement Disorders, Vol. 24, No. 7, 2009 954 D.J. BROOKS AND K. SEPPI D.J. Brooks and K. Seppi Table 4 MSA の診断における経頭蓋超音波の診断精度 TABLE 4. Diagnostic accuracy of transcranial sonography for the diagnosis of MSA Author/Year Cohort size 20 Walter et al., 2003 21 Behnke et al., 2005 Diagnostic predictor MSA 16/PD 25/PSP 9 Hyperechogenicity of the SN and LN (hyperechogenic if it was more intense than the surrounding white matter) SN echogenity (<0.2 cm2) SN echogenity (<0.25 cm2) LN hyperechogenity Hyperechogenity of the SN (>80th percentile of controls) and LN Absent uni-/bilateral SN hyperchogenity MSA-P 32/PD 88/PSP 18 Uni-/bilateral LN hyperechogenity Okawa et al., 200722 23 Walter et al., 2007 MSA 14/PD 98/PSP 17/HC 30 MSA-P 21/PD 138/PSP 22 Combination of absent SN hyperchogenity and uni-/bilateral LN hyperechogenity Combination of unilateral SN hyperchogenity and regular bilateral LN echogenity Hyperechogenity of the SN Absent uni-/bilateral SN hyperchogenity Hyperechogenicity of the SN (greater value of bilateral measurements was considered): normal echogenicity; moderate hyperechogenicity; marked hyperechogenicity; hyperechogenicity of LN (hyperechogenic if it was more intense than the surrounding white matter); 3rd ventricle dilatation–not given here, because it is a characteristic for PSP patientsa Normal SN echogenicity Normal SN echogenicity with hyperechogenic LN Normal/moderate SN hyperechogenicity with hyperechogenic LN Sensitivity (%) Specificity (%) 94 (for MSA)/ 91 (for APS) 100 77 (for APS) 96 (vs. PD) 76 (vs. PD) 77 (vs. PD) 70 (for MSA-P)/ 70 (for APS) 72 (for MSA-P)/ 72 (for APS) 56 (for APS) 89 (vs. PD) 93 (vs. PD) 88 (for APS) 66 (vs. PD) 91 (for MSA), 92 (for APS) 83 (vs. PD) 90 (for MSA-P), 72 (for APS) 65 (for MSA-P), 59 (for APS) 77 for APS 98 (vs. PD) 89 (vs. PD) 100 (vs. PD) 97 (vs. PD) a a Semiquantitative300 grading of のエコー輝度に基づき, the SN hyperechogenicity performed based on SN echogenicity values of 300 0.2 healthy controls: SN 健常対照被験者 名の SN SNwas の高エコー域の半定量的分類を行った。SN の面積が cm2 未満で, HCnormal の 75 パー 2 2 2 echogenicity corresponding to a SN area <0.2 cm , i.e., <75th percentile; moderate SN hyperechogenicity corresponding to a SN area of 0.2 cm2 センタイル未満であれば通常のエコー輝度,SN の面積が 0.2 cm 以上 0.25 cm 未満で,HC の 75 ~ 90 パーセンタイルであれば中等度の高輝 2 2 or larger and <0.25 cm ,2 i.e., 75th–90th percentile; marked SN hyperechogenicity corresponding to a SN area of 0.25 cm or larger, i.e., >90th 度,SN の面積が percentile of HC. 0.25 cm 以上で,HC の 90 パーセンタイル超であれば著明な高輝度とした。 MSA, multiple system atrophy; PD, Parkinson’s disease; PSP, progressive supranuclear palsy; SN, substantia nigra; LN, lentiform nucleus; HC, MSA:多系統萎縮症,PD:パーキンソン病,PSP:進行性核上性麻痺,SN:黒質,LN:レンズ核,HC:健常対照 healthy controls. 標を用いると PSP 患者を誤診することはない。 前部より拡散係数が高かった 11。MSA-P 患者と PSP 患者 as control participants, with no patient with PSP receivMRI ing a の定量的形態画像:拡散強調画像と磁化移動 misdiagnosis when the index was used. fer (MTI) imaging potentially represent useful diagnos5,11,16,17,47 が,1.5T の DWI tic様々な研究グループ tools that can provide additional support forによる被 a diag5,10,11,15–19,47–50 nosis of MSA-P. 殻のみかけの拡散係数(apparent diffusion coefficient; ADC) Different groups5,11,16,17,47 have been reported that と Trace(D) 値から,MSA-P 患者と健常被験者および PD DWI at 1.5 T is able to discriminate patients with 患者とを鑑別できることを報告している。MSA-P 患者で MSA-P and both healthy volunteers and patients with PD on the basis of putaminal ADC and Trace(D) val被殻の拡散係数が高いという結果については,再現性が ues. The finding of increased putaminal diffusivity in 10 patients with MSA-P has been reproduced, although 数は MSA-P 患者の方が PSP 患者よりも高いことが示され, one study10 with methodological limitations regarding 10,17 この 2 つの疾患の鑑別に有用であった acquisition and segmentation of the DWI。別の試験では, images could not confirm this. In line with the known underlying MSA-C 患者の脳橋,MCP,小脳白質,被殻の ADC は, neuropathology in MSA-P, a 49more severe involvement 対照群に比して高値であった 。DWI は,MSA-P と PD of posterior compared with anterior putaminal diffusiv11 5,17,29 とを鑑別する際,MRI でテント上(主に被殻) およ ity was found in patients with MSA-P. Although putaminal diffusivity overlapped in MSA-P and PSP 17 びテント下 の異常の有無を確認するのに優れている。 patients, diffusivity in the MCP has been shown to be 10 Paviourinらpatients は,被殻または SCPcompared の ADC 値について, higher with MSA-P with PSP, allowing a good discrimination these two disMSA 患者と PD 患者または PSP between 患者との間で差がみられ ease entities.10,17 In a further study, an increase of ないことを明らかにした。これは,1.5T において MSA-P ADCs was found in the pons, MCP, cerebellar white 5,6,11,16,17 患者の被殻の拡散係数が有意に高く 患者の matter, and putamen of MSA-C patients,PSP compared 49 50 DWI proved superior to searching for with controls. SCP の ADC 値が有意に低い ことを示した,これまで the presence of supratentorial (mainly putaminal)5,17,29 よび領域抽出に方法論的限界があったため,この知見は および被験者背景の違いが考えられる。Paviour らの報告 確認できなかった。これまでに知られている MSA-P の神 Movement Disorders, Vol. 24, No. 7, 2009 では,これまでの報告に比べ,被験者,特に PD 群の罹 経病理所見と一致して,MSA-P 患者では被殻後部の方が 病期間が長かった。また,スライス厚を 7 mm とする では被殻の拡散係数に重複がみられたが,MCP の拡散係 画像 拡散強調画像(diffusion-weighted imaging; DWI)およ Quantitative Structural MR-Based Techniques: び磁化移動画像(magnetization transfer MTI)は, Diffusion-Weighted Imaging and imaging; Magnetization Transfer Imaging MSA-P の診断をさらに裏付ける有用な診断ツールである Diffusion-weighted (DWI) and magnetization trans5,10,11,15–19,47–50 と考えられる 。 確認されている。ただし,ある試験 では DWI の収集お の報告と明らかに対照的である。その理由として,方法 15 多系統萎縮症の診断を目的とした神経画像の基準案 DWI MR プロトコルは,他の試験で用いられたスライス 厚 3 ~ 5 mm15,17,18,50 に比べると不十分であると思われる。 さらに,領域抽出に誤りがあった可能性もあり,既に公 表されている ROI の図では,被殻の ROI に明らかに淡蒼 球の一部が含まれている。 Ito ら 18 は,3.0T MR 装置を用いて,MSA 患者,PD 患 者,対照被験者間で,脳橋,小脳,被殻の拡散係数と異 方性比率(fractional anisotropy; FA)を比較した。MSA 患者は PD 患者または対照被験者に比して脳橋,小脳, 被殻の拡散係数が有意に高く,FA は低かった。MSA-P と PD との鑑別に FA と拡散係数を用いたところ,脳橋で Figure 2 A:PD 患者(55 歳男性,罹病期間 5 年,HY 病期Ⅰ Ⅰ ) 。 正中矢状断 T1 強調画像(全身用 1.5T MR 装置)では重要な脳幹萎 縮は認められない。B:MSA-P 患者(61 歳女性,罹病期間 3.5 年, HY 病期Ⅰ Ⅰ Ⅰ ) 。正中矢状断 T1 強調画像(全身用 1.5T MR 装置)で テント下萎縮(脳橋および小脳,第四脳室の拡張)が認められる。 は被殻および小脳と比較して感度は同等であったものの MTI を用いた試験では,MSA-P 患者にも大脳基底核の (70%) ,特異度は高かった(100%) 。また,この 3 つの 異常のあることが報告されている 19,48。大脳基底核と SN 各領域で FA が有意に低く拡散係数が高かったのは全例 における磁化移動比(magnetization transfer ratio; MTR) が MSA-P 患者であり,脳橋の FA と拡散係数がともに正 のステップワイズ判別分析では,PD 患者と対照被験者を 常であったのはいずれも PD 患者であった。 MSA 患者と PSP 患者から的確に鑑別することができ, MSA 患者 1 名のみが誤って対照群に分類された。ただし, PD 患者と対照被験者,MSA 患者と PSP 患者との鑑別精 度は至適レベルには達していなかった 19。 経頭蓋超音波 近年,開頭せずに脳実質を描出するため,経頭蓋超音 Figure 1 A:MSA-C 患者〔62 歳女性,罹病期間 3 年,Hoehn and Yahr(HY)病期Ⅰ Ⅰ Ⅰ 〕 。T2 強調画像(全身用 1.5T MR 装置)で十字 サインがみられる。B:MSA-P 患者(66 歳女性,罹病期間 4 年, HY 病期Ⅰ Ⅰ Ⅰ ) 。T2 強調画像(全身用 1.5T MR 装置)で両側の被殻 に変化(辺縁高信号,淡蒼球に比して被殻が低信号,被殻萎縮) が認められる。C:MSA-C 患者(64 歳男性,罹病期間 3.5 年,HY 病期Ⅳ) 。T2 強調画像(全身用 1.5T MR 装置)で被殻の変化(左 側の著明な辺縁高信号,淡蒼球に比較した被殻の低信号,両側の 被殻萎縮)が認められる。D:PD 患者(58 歳女性,罹病期間 5 年, HY 病期Ⅰ Ⅰ ) 。T2 強調画像(全身用 1.5T MR 装置)では大脳基底核 に重要な異常はみられない。 16 Figure 3 A,B:PD 患者(55 歳男性,罹病期間 5 年,HY 病期 Ⅰ Ⅰ ) 。矢状断 T1 強調画像でも軸位断 T2 強調画像(全身用 1.5T MR 装置)でも重要な中小脳脚(矢印)の萎縮は認められない。C,D: MSA-P 患者(61 歳女性,罹病期間 4 年,HY 病期Ⅰ Ⅰ Ⅰ ) 。矢状断 T1 強調画像および軸位断 T2 強調画像(全身用 1.5T MR 装置)で中小 脳脚(矢印)の萎縮が認められる。 D.J. Brooks and K. Seppi 波(transcranial sonography; TCS)が広く用いられるよう を有する。MSA 患者では小脳,脳幹,線条体,前頭皮質 になった。TCS を用いた最近の試験では,PD 患者の 80 の局所脳糖代謝(regional cerebral glucose metabolism; ~ 90%で中脳 SN 領域の高エコー域が報告されたが,同 rCMRglc)の低下を認めたが,PAF 患者では低下はみら 様の所見は健常成人や,MSA および PSP による非定型 れなかった。この研究では,FDG PET で MSA と PAF が パーキンソニズムを呈する患者でも約 10%で報告されて 明確に鑑別されるという結論を下している。 いる 。これとは逆に,レンズ核(lentiform nucleus; Gilman ら 55 は,MSA,sOPCA,優性遺伝性オリーブ LN)の片側または両側の高エコー域は,MSA または 橋小脳萎縮症(dominantly inherited olivopontocerebellar PSP による非定型パーキンソニズムを呈する患者の 70% atrophy; dOPCA)の患者で rCMRglc のパターンを検討し 以上と,PD 患者の 1/4 前後で認められる 20,21,23。高エコー た。MSA 症例と sOPCA 症例では,脳幹,小脳,被殻, を呈するLNと高エコーを認めないSNとの組み合わせは, 視床,大脳皮質の rCMRglc が低下していた。これに対し MSA および PSP の非定型パーキンソニズム患者に特異 て,dOPCA 症例では脳幹と小脳の rCMRglc のみが低下 的にみられる所見であるが,その感度は至適レベルには していた。多くの sOPCA 症例は MSA に移行する可能性 達していない があるが,Gilman らは,以上の所見がこの可能性に矛盾 20–23,51–53 。 21,23 TCS を用いた脳実質超音波検査の利点は,SPECT/PET しないと結論付けた。 または MRI による機能画像などの他の画像診断法に比べ レボドパ不応性の無動・硬直を示し臨床的に SND と考 アクセスしやすく,費用が高くないことである。その一 えられる患者では,FDG PET 試験にて線条体の糖代謝の 方で,TCS には技術的な制約がある。被験者の約 10 ~ 低下が報告されているが,これとは対照的に,PD では線 15%には側頭骨窓がないため,このような被験者に TCS 条体の代謝が維持されている。Eidelberg は,SND と考え を用いることはできない。さらに,脳実質の高エコー輝 られる 10 例中 8 例で線条体の代謝が低下していたが,レ 度を定量化できないため,報告時にはある程度主観的な ボドパに反応する PD 患者では,この代謝が正常な者や 記載にならざるを得ない。 亢進した者もいたことを報告した 56。De Volder らは, SND と考えられる 7 例を検討した。そのうち,自律神経 MSA における機能画像 MSA における FDG PET 試験 不全と小脳性運動失調症も認められた 2 例は完全な MSA 症候群であった 57。この 7 例では被殻と尾状核の平均糖 代謝量が低下していたが,運動失調症の 2 例では小脳の 多数の FDG PET に関する症例集積研究では,様々な 代謝も低下していた。Otsuka ら 58 は,MSA 患者 9 名と 病型の MSA〔SND,OPCA,純粋自律神経失調症(pure 孤発性パーキンソン病(idiopathic Parkinson’ s disease; autonomic failure; PAF) 〕や, 他のパーキンソン症候群〔PD, IPD)患者 15 名の FDG PET 所見を報告した。MSA 患者 PSP,大脳皮質基底核変性症(corticobasal degeneration; のうち 5 名は OPCA,4 名は SND であった。MSA では CBD) 〕 ,小脳性運動失調症にみられる多様な安静時局所 線条体,小脳,脳幹,前頭部,側頭部の rCMRglc が低下 脳糖代謝パターンが検討されてきた。これらの報告は, していたが,MSA 群と正常対照群との間には重複がみら 一般に臨床診断が病理学的に確認されていないものの, れた。PD では線条体の代謝は維持されていた。 疾患が確定した症例の小規模集団を非盲検法で分析して Eckert らは,パーキンソン症候群患者 135 名の鑑別診 おり,フォローアップが行われている場合もある。この 断における FDG PET の有用性を評価した 59。個々の PET ような点を考慮すると,初期症例の MSA 診断や,MSA 画像は,視覚的な評価とともに,rCMRglc の著明な低下 と他のパーキンソン症候群や運動失調症との鑑別におい に 関 す る 統 計 的 パ ラ メト リ ッ ク マ ッ プ(statistical て,FDG PET の真の感度と特異度を評価するのは依然と parametric map; SPM) を用いて評価した。2 年間のフォロー して困難である。 アップでは,最初の PET 所見を知らされていない運動障 Fulham ら は,MSA 患者 30 名と PAF 患者 15 名との 害専門医が独立した形で臨床評価を行い,当初の PET 画 鑑別において,FDG PET の有用性を検討した。MSA 群 像の評価と比較した。盲検下での SPM による評価と臨床 の内訳は,MSA-C 患者 8 名,MSA-P 患者 7 名,MSA 患 診断とが一致したのは全被験者の 92.4%(MSA での一致 者 15 名で,いずれも小脳所見とパーキンソン症状の両方 率 96%)で,視覚的評価と臨床診断とが一致したのは患 54 17 多系統萎縮症の診断を目的とした神経画像の基準案 者の 85.4% (MSA での一致率 76%) であった。患者がパー れている。Davie ら 65 は,当初,臨床的に SND と考えら キンソニズムの疑いで最初に紹介された時点で撮影した れる 7 例中 6 例で LN に由来する PMRS 信号の NAA/ ク FDG PET 画像は,コンピュータ支援画像解析が使用可能 レアチニン(creatine; Cr)比の低下を報告したが,PD と な場合には, 各患者の MSA の臨床診断 (その後のフォロー 考えられる 9 例中 8 例では被殻 NAA レベルの異常を認 アップで確認)を正確に予測することができた。視覚的 めなかった。しかし,Federico らが PD 患者 19 名と MSA 分析による診断の信頼性は低かった。 患者 14 名を検討したところ,MSA 群では全体として LN の NAA/Cr 比の平均値に有意に顕著な低下が認められた 脳血流 SPECT 試験 ものの,この PD および MSA の患者コホートでみると被 Bosman らは,PD と MSA との鑑別を目的に,解剖学 験 者 の 50 % で LN の NAA/Cr 比 が 重 複 し て い た 66。 的標準化と自動分析を用いた脳血流 ECD SPECT の有用 Clarke と Lowry67 は,PMRS の試験 11 件を再検討し,LN 性を評価した 60。PD 患者 81 名,MSA 患者 15 名を含む の NAA/Cr 信号の変化は PD および MSA では一貫して 被験者 140 名を対象に SPECT を行ったところ,MSA と おらず,典型的パーキンソン障害と非定型パーキンソン PD とで違いが認められたのは被殻の血流のみであった。 障害とを確実に鑑別する方法として PMRS を使用するこ この画像によって MSA の正しい分類 (臨床基準に基づく) とはできないと結論付けている。 最近,Watanabe らは,MSA-P の脳橋では LN よりも が可能となり,感度は 73.3%,特異度は 84%,正診率は NAA/Cr 信号の低下が顕著であることを明らかにした 68。 83.6%であった。 Bosman らの研究グループは,次に ECD SPECT と SPM とを組み合わせ,その診断精度を向上させた 。 61 これらの測定値を組み合わせることで,MSA-P 患者 11 名中 8 名と PD 患者 11 名とを鑑別することができた。 MSA とは対照的に,PD 患者では全体的に前頭部および 側頭部の血流が有意に低下していた。 IPD に関連する FDG PET スキャン上の局所代謝の共 シナプス前およびシナプス後ドパミンを指標とし た画像 変動について,再現性のあるパターンを特定するために シナプス前およびシナプス後ドパミン機能は,PET で ネットワーク分析が用いられている 62。この PD 関連パ も SPECT でも調べることができる。ドパミン貯蔵能は, ターン(PD-related pattern; PDRP)の発現は各患者で定 18 F-dopa の取り込みや,11C—ジヒドロテトラベナジン 量化が可能で,PD 患者を健常対照被験者や非定型症例 (dihydrotetrabenazine; DTBZ)結合による小胞モノアミン から鑑別する際に使用されている。Feigin らは,PD 患者 トラン スポーター(vesicular monoamine transporter; と MSA 患者の Tc-ECD SPECT 所見に対し,ネットワー VMAT2)機能,11C-nomifensine,123I- β -CIT,123I-FP- ク分析を適用した 63。しかし,PD 群と MSA 群では被験 CIT,99m Tc-TRODAT-1 の取り込みによるドパミントラン 者の 1/3 の PDRP 値が重複していたため,パーキンソニ スポーター結合によって示される。ドパミン D1 受容体の ズムの鑑別診断における臨床的有用性を疑問視している。 結合は 11C-SCH23390 PET で撮像され,ドパミン D2 受容 Cilia ら 64 は,MSA 患 者 36 名 の 脳 血 流 量 を ECD 体結合は 11C-raclopride PET,123I-IBZM,123I-epidepride, 99m SPECT で測定し,PD 患者 43 名および年齢を一致させた I-IBF SPECT で撮像されている。 123 対照被験者 39 名と比較した。SPM を適用すると,他群 に比べ,MSA 群では線条体,脳幹,小脳に有意に血流の シナプス前ドパミンを指標とした画像 低下した領域が認められた。 臨床的に MSA-P と考えられる患者では,シナプス前ド パミン作動性神経の機能が著しく損なわれている。PD と プロトン MR スペクトロスコピー プロトン MR スペクトロスコピー(proton magnetic 18 同じく,MSA-P の診断確定例では被殻の 18F-dopa 取り込 みが正常レベルの 50%前後まで減少し,各患者の被殻の resonance spectroscopy; PMRS)には,SND と PD とを鑑 18 別できる可能性がある。N —アセチルアスパラギン酸 尾状核の 18F-dopa 取り込みの平均値は,MSA-P 患者の方 (N-acetylaspartate; NAA)はニューロン内に高濃度に存在 が PD 患者よりも有意に低いが,その範囲は患者の 50% し,神経の完全性に関する代謝マーカーであると考えら で重複している。Burn ら 71 は,パーキンソン症候群患者 F-dopa 取り込みレベルは歩行状態と相関している 69,70。 D.J. Brooks and K. Seppi の被殻と尾状核の 18F-dopa 取り込みについて判別分析を いて確実に鑑別することはできなかった。Kim ら 75 は, 行い,患者は同等の頻度で MSA 群,IPD 群,PSP 群に割 123 り振られることを見出した。これに対して,Otsuka らは PSP 患者 6 名を検討し,同じ結論に至っている。 I- β -CIT SPECT で PD 患者 18 名,MSA-P 患者 7 名, MSA 患者 9 名(MSA-C 5 名,MSA-P 4 名)と PD 患者 最近の試験では,99mTc-TRODAT-1 SPECT 画像を用い 15 名の 18F-dopa PET 所見を報告した。この報告では,尾 て,MSA-P 患者 30 名,MSA-C 患者 19 名,PD 患者 36 状核と被殻の F-dopa 取り込みは両群ともに減少してい 名における線条体の DAT 結合が比較されている 76。この たが,尾状核と被殻の取り込みの差を尾状核の取り込み 試験では,99mTc-TRODAT-1 SPECT によって,PD および で除した尾状核 - 被殻指標(caudate-putamen index; CPI) MSA 患者と健常人との鑑別や,MSA-C 患者と MSA-P 患 は MSA 患者が 5.6 ± 4.6,PD 患者が 14.8 ± 5.4 で,MSA 者との鑑別は可能であるが,MSA-P 患者と PD 患者は十 では尾状核の障害が比較的大きいことを示し,18F-dopa に 分には鑑別できないと結論付けている。 18 Scherfler ら 77 および Seppi ら 78 は,SPM および 123I- β よる CPI は MSA と PD との鑑別に有用であると結論した。 Rinne ら 72 は,18F-dopa PET を用いて sOPCA 患者 10 -CIT SPECT を用いて,MSA-P 患者の脳容積全体におけ 名を検討した。被殻の F-dopa 取り込みの平均値は対照 るドパミン作動系の完全性を検討した。その結果,対照 群の平均値である 71%まで有意に減少し,患者別でみる 被験者 13 名に比べると,初期 MSA-P 患者 15 名,PSP 患 と 7 名で有意に取り込みが減少していた。Rinne らは, 者 14 名,PD 患者 17 名では線条体の DAT 活性が低下し MSA の疾患スペクトルの一部であることと一致して, ており,その程度は標準 ROI 法で検出した場合と同様で sOPCA 患者の大半に無症状の黒質線条体機能障害が認 あることを明らかにした。これに加え,対照被験者や PD められるとの結論を下した。Gilman ら 患者に比べると,MSA-P 患者(59%)や PSP 患者(52%) 18 73 は,MSA 患者 4 名と sOPCA 患者 8 名にラセミ体の C-DTBZ を用いた では脳幹に 123I- β -CIT 信号の低下した領域があり,その PET を行い,線条体の VMAT2 結合を検討した。MSA 患 位置を客観的に特定することができた。これは,123I- β 者では,尾状核と被殻の特異的な VMAT2 結合が有意に -CIT SPECT 画像の視覚的評価または ROI 分析では予測 抑制されており,尾状核では平均 61%,被殻では平均 できなかった。中脳の平均 specific-to-nondisplaceable 58%低下していた。sOPCA 患者では低下が小さかった (尾 ※ equilibrium partition coefficient(V3") を 2.3 とすると,PD 状 核 26 %, 被 殻 24 %) 。sOPCA 患 者 で は 線 条 体 の 患者 1 名は非定型パーキンソニズムに分類され,MSA-P VMAT2 結合が抑制されていたことから,無症状の黒質 患者 1 名と PSP 患者 2 名は PD に分類されたが,MSA-P 線条体病変の存在が示唆された。Gilman ら 患者と PSP 患者とを鑑別することはできなかった。 11 73 は,MSA-P 患者 8 名,MSA-C 患者 8 名,sOPCA 患者 6 名を対象と したフォローアップ試験で 11C-DTBZ の活性(+)異性 シナプス後ドパミンを指標とした画像 体を用いた PET を行ったが,やはり VMAT2 結合はすべ ての患者群の被殻で有意に抑制されていた。 Pirker ら 最も広く利用されている 11C-raclopride PET および 123 I-IBZM SPECT による PD 患者のドパミン D2 受容体結 I- β -CIT SPECT を用いて,MSA と考 合の試験では,未治療の早期患者において,障害が大き えられる患者 18 名(MSA-C 3 名,MSA-P 15 名) ,PSP 患 い側と反対側の被殻でドパミン D2 受容体結合が相対的 者 8 名,CBD 患者 4 名,PD 患者 48 名(身体能力障害は に 10 ~ 20%高いことが示された 72,79,80。PD の進行した 同程度)を対象に,ドパミントランスポーター(dopamine 患者やドパミン作動薬投与患者では,11C-raclopride PET transporter; DAT)の結合パターンを検討した。その結果, で被殻のドパミン D2 受容体結合の正常化を示す所見が 線条体の DAT 結合は,MSA,PSP,CBD,PD の患者で 認められ ている 79,81。一 方,123I-IBZM SPECT および そ れ ぞ れ 正 常 平 均 値 の - 51 %, - 60 %, - 35 %, 11 - 58%と有意に抑制されており,対照群の値との重複は パミン D2 受容体結合が正常以下になる可能性があること 74 は 123 C-methylspiperone PET に関する症例集積研究では,ド みられなかった。線条体の I- β -CIT 結合の非対称性は, 123 CBD および PD の患者で有意に亢進しており,MSA およ び PSP 患者ではあまり顕著でなかった。ただし,Pirker らは,これらのパーキンソン症候群を SPECT 所見に基づ ※ 日本語版注釈:標的に特異的に結合したトレーサーと,非特異的 に集積したトレーサーとの比で,平衡状態に達した脳組織で測定 したもの。この係数は,123I- β -CIT SPECT の場合,ドパミントラ ンスポーター結合能を反映する。 19 多系統萎縮症の診断を目的とした神経画像の基準案 SPECT では,すべての PD 症例と MSA-P 症例を健常人 が示唆されている 82–84。 対 照 的 に, 非 定 型 パ ー キ ン ソ ン 症 候 群 で は, と本態性振戦症例から鑑別することができ,線条体の平 I-IBZM SPECT によって,臨 均 DAT 結合の低下は同等であった。MSA 患者 13 名中 7 床症状が発現するとドパミン D2 受容体密度が低下するこ 名 (54%) では線条体のドパミン D2 受容体利用能が低かっ とが示唆されている は,SND と推定さ たが,PD 症例では全例とも 123I-IBZM 取り込みに異常は れるアポモルフィン不応性パーキンソン症候群患者の 2/3 みられなかった。Plotkin らは,123I-IBZM SPECT 所見が で, 線条体の 123I-IBZM 取り込みが減少したことを認めた。 正常である場合,確信を持って MSA を除外することは Kim らは,MSA-P 確定症例の 71%では線条体の できないと結論付けた。 C-raclopride PET および 11 123 。Schwarz ら 85,86 86 123 I-IBF の結合が有意に低下したが,PD 症例では全例ともドパミ Seppi ら 15 は,123I-IBZM SPECT を用いて,初期 MSA ン D2 受容体利用能が正常,または亢進したことを明らか 症例群で客観的かつ長期的に線条体の変性をモニタリン にした 。 グした。18 ヵ月間の試験で線条体のドパミン D2 受容体 75 ドパミン機能のシナプス前画像マーカーとシナプス後 結合は年間 10%低下したことから,Seppi らは,MSA に 画像マーカーとを組み合わせると(DAT およびドパミン 対する神経保護薬と推定される薬剤の有効性を検討する D2 受容体の SPECT 試験) ,PD と MSA との鑑別感度が上 際には,123I-IBZM SPECT が有効なアプローチになりうる 昇することが示唆されている。ただし,Knudsen らがこの と結論付けた。Seppi らは別の試験で,MSA と PD との ようなアプローチを用いたところ,PD 患者 14 名(3 名は 鑑別における DWI と IBZM SPECT の予測精度を比較し 薬剤未投与)と鑑別できたのは,MSA-P 患者 8 名中 2 名 た。線条体の ADC によって MSA 症例の 97%を分類で (全例がドパミン作動薬の投与を受けていた)のみであっ きたのに対し,ドパミン D2 受容体結合で分類できたのは た 。Knudsen らの症例集積研究では,疾患の重症度を考 75%で,MSA-P と PD との鑑別診断においては DWI の 慮しても,PD 症例と MSA 症例との間で線条体の 方が IBZM SPECT よりも正確であると示唆されている。 87 123 I- β -CIT 取り込みの減少に差はみられなかったが,左右の非 SND では,PET によって線条体のドパミン D1 受容体 対称性は PD の方が大きかった。 I-epidepride SPECT で 結合が検討された。被殻の 11C-SCH23390 取り込みの平 測定した線条体のドパミン D2 受容体結合は,MSA-P 患 均値について,軽微であるが有意な減少が報告されてい 者 2 名において PD の範囲を超える亢進が認められた。 るものの,SND 患者,健常人,PD 患者で認められた範 123 Ghaemi ら 39 は, F-dopa,FDG, C-raclopride を用い 18 11 囲には大きな重複があった 89。 たマルチトレーサ PET を行い,PD 患者と MSA-P 患者と の鑑別能を比較した。この試験には健常対照被験者 7 名, オピオイド結合とグリア活性化の画像 MSA-P 診断例 9 名,PD 診断例 24 名が参加した。被殻の 18 F-dopa 集 積 は,ど の 群 で も 同 様 に 減 少 し て い た。 大脳基底核はオピオイドペプチドとその結合部位に富 み,SND と PD で は 受 け る 影 響 が 異 な る。 MSA-P 群では被殻の糖代謝低下とシナプス後ドパミン受 11 容体密度の低下がみられたが,レボドパに反応する PD 結合する非特異的オピオイドアンタゴニストである。尾 群ではこのような所見はみられなかった。被殻の FDG- 状核と被殻の 11C-diprenorphine 取り込みは,ジスキネジ PET と MRV は 個 々 の デ ー タ の 重 複 が 最 も 小 さく, アのない PD 患者では維持されるが,ジスキネジアのあ MSA-PとPD を同等に鑑別できることがわかった。 しかし, る症例では減少し 90,SND と考えられる患者の 50%では MSA-P 患者 2 名では被殻の FDG-PET 値が PD 群の範囲 被殻の取り込みに減少がみられる 91。 内にあり,MSA-P 患者 1 名では MRV での被殻容積が PD 群の範囲内にあった。 Plotkin らは 20 I-FP-CIT および 123 C-diprenorphine は,µ,κ,δ部位に対して等親和性に ミクログリア活 性 化の in vivo マーカーである 11CPK11195 PET を用いて,MSA における神経炎症性変化が I-IBZM SPECT を用い 123 検討されている 92。皮質下での広範囲に及ぶ 11C-PK11195 て,パーキンソニズム症例 72 名を受診順に検討した 88。 取り込みの増加が,特に黒質,被殻,淡蒼球,視床,脳 臨床フォローアップでは,25 名が PD(SPECT の時点で 幹で確認された。同様の変化は PD でも認められたが, 薬剤未投与 12 名) ,13 名が MSA-P(SPECT の時点で薬 そ の 程 度 は 低 か っ た 93。 こ の よ う な こ と か ら, 剤未投与 6 名)ではないかと考えられた。123I-FP-CIT 11 C-diprenorphine と 11C-PK11195 PET は,いずれも MSA D.J. Brooks and K. Seppi Table 5 MSA における形態画像と機能画像 MSA における形態画像 a 1.5T での従来型 MRI MSA 症例は被殻,MCP,脳幹の低信号と萎縮を示し,T2 で辺縁高信号を呈すると考えられるが, このような特徴は(特に PD と比較して)MSA の裏付けとはなるものの,全症例には認められず,他 の非定型パーキンソン病(APD)に比べると特異的ではない。 MRI を用いた面積測定と容 積測定をはじめとする様々 な脳構造の萎縮の定量的評 価 様々な脳構造の萎縮を MRI で定量的に測定すると,MSA を PD(MSA では MCP 幅が縮小し, MSA-P では被殻の容積が減少している)と PSP(PSP 患者では脳橋面積に対する中脳面積の比が減 少している)から鑑別できるが,これらの具体的な試験について再現性は確認されていない。 拡散強調画像(DWI) DWI は, 非定型 PD と, 被殻の拡散係数が高い典型的 PD との鑑別において有望であると考えられる。 しかし,PSP 患者も被殻の拡散係数が高い場合がある。MSA 患者は PSP 患者に比して MCP の拡散 係数が高いという所見が認められているが,他の研究者により再現性が確認される必要がある。 経頭蓋超音波(TCS) 中脳は通常高エコーを呈することはなく,TCS は MSA の診断の裏付けに有用であると考えられる。 PD 症例の 90%では黒質の信号変化がみられる。SN および LN の高エコー輝度による MSA 患者と PSP 患者との鑑別精度は,いずれも至適レベルには達していない。なお,特記すべき点として,この 集団の少なくとも 10%には,脳実質の超音波分析に十分な側頭骨窓が認められない。 MSA における機能画像 シナプス前ドパミンを指標 とした画像 PET または SPECT によるシナプス前ドパミン機能の撮像では,パーキンソン状態と非パーキンソ ン状態とを確実に鑑別できるが,MSA と他のパーキンソン状態との鑑別はできない。 シナプス後ドパミンを指標 とした画像 MSA 症例では被殻のドパミン D2 受容体結合が抑制されているが,PD 症例では変化がないか亢進 している。しかし,PD と MSA で認められる所見の範囲は重複しており,MSA 症例の 1/3 ではドパミ ン D2 受容体利用能は正常である。 FDG PET FDG PET は典型的 PD と非定型 PD との鑑別に有用であり,特にコンピュータを用いた統計的パラ メトリックマッピングを併用した場合,視覚的分析に対して感度は 80%から 95%に上昇する。MSA 症例では線条体,脳幹,小脳の代謝低下が認められるが,PD 症例では被殻の代謝が亢進し,前頭側 頭部の代謝は低下する。 心臓交感神経支配の画像 MIBG SPECT または 18F—ドパミン PET では,PD 症例のほとんどに心筋交感神経支配の低下がみら れるが,MSA または PSP ではみられない。しかし,心臓交感神経支配は初期の PD では正常であり, MSA では低下している場合がある。 a 重要な点として,MSA-C 患者で構造画像はほとんど用いられなかった。MSA-C 患者と,MSA-C に一致しない小脳外の症状を伴う孤発性 小脳性運動失調症患者との鑑別には,1.5T での信号変化,従来型 MRI で認められる様々な脳幹領域(特に MCP と脳橋)の萎縮,MRI を用 いた容積測定での脳幹容積の減少といった所見が有用であると思われる。 と PD とを高感度に鑑別しないと考えられる。 いと考えられる。 MIBG SPECT を用いた研究では,IPD における末梢自 心臓交感神経支配の画像 123 律神経障害に関して重要な情報が得られたが,このモダ I-MIBG は,交感神経終末に取り込まれ,貯蔵される リティにはいくつかの欠点がある。市販の SPECT カメラ ノルエピネフリンアナログである。PD 患者に 123I-MIBG は PET カ メラよりも感 度 および 空 間 分 解 能 が 低く, SPECT を用いた複数の画像試験では,心血管反射に異常 123 がない場合でも心臓の取り込み減少が認められ,心筋の 11 節後交感神経障害が示唆された 94–97。しかし,初期の PD 心筋交感神経支配の程度を直接定量化できる。 患者の場合,MIBG の取り込みは正常であると考えられ I-MIBG の心臓/縦隔集積比に依存して定量化される。 C—メタヒドロキシエフェドリン(11C-MHED)PET は, Berding ら 102 は,MSA 患者 2 名と PD 患者 5 名(うち る 98。ほとんどの MIBG SPECT による MSA の検討では, 3 名は起立性低血圧を合併)の計 7 名に対するパイロッ 心筋交感神経支配は正常であったが ,交感神経支 ト試験の結果を報告した。投与 5 分後,40 分後の MHED 。以上をまとめ 取り込みの心筋/肝臓比を求めたところ,PD 患者 5 名中 配に軽度の低下が報告されている 94,95,98,99 96,100,101 ると,MIBG SPECT は既に確立した PD と MSA-P とを高 4 名はいずれの時点でも取り込み比が MSA よりも低く, い感度で鑑別するものの(PD では心臓の信号が低下し, なかでも起立性低血圧患者の心筋信号が最も低かった。 MSA-P では維持される) ,初期の PD では心臓交感神経 Raffel らは,MSA 患者 5 名,PSP 患者 2 名,健常被験 支配が正常な場合があり,MSA との確実な鑑別はできな 者 10 名の MHED PET 所見を報告した 103。MSA 患者 2 21 多系統萎縮症の診断を目的とした神経画像の基準案 名では心筋の MHED 取り込みが減少していたが,残りの MSA 患者 3 名と PSP 患者 2 名は正常であった。Raffel ら は,ほとんどの MSA 患者は心臓の節後交感神経支配が 正常であるが,重度の脱神経が認められる場合もあると 結論付けた。 Goldstein ら 104 は,自律神経障害のある被験者とない被 験者を対象に,18F—ドパミン PET を用いて心筋交感神経 支配の機能を検討した。Goldstein らが検討した最初の患 者群では,PAF 患者 3 名で心筋の 18F—ドパミン集積が大 幅に減少していた 104。一方,心血管反射障害(シャイ ・ ドレーガー症候群)のある MSA 患者 9 名では心筋交感 神経機能が亢進しており,交感神経循環不全のない MSA 症例では 18F—ドパミン取り込みは正常であった。心血管 反射障害を伴いレボドパに反応するパーキンソニズムの 2 例では,PAF と同じく,心筋の明らかな 18F—ドパミン取 り込みは認められなかった。Goldstein らは,18F—ドパミ ン PET によって自律神経失調症候群を節前,および節後 症候群に分類することができると結論付けた。 Goldstein らはフォローアップ試験を行い,PD 患者 29 work-up of MSA patients presenting requires further prospective studies during early disease stages when the clinical diagnosis remains uncertain. Based on the best current knowledge, the revised consensus criteria include neuroimaging criteria for the diagnostic category of possible MSA.103 Atrophy on conventional しくは小脳の萎縮,または FDG-PET による被殻,脳幹も MRI of putamen, MCP, pons, or cerebellum or hypoしくは小脳の代謝低下が追加されている。また, 「MSA-C metabolism on FDG-PET in putamen, brainstem, or cerebellum were included as additional features for の可能性あり(possible MSA-C) 」の所見としては,従来 possible MSA-P; and atrophy on conventional MRI of 型 MRI による被殻,MCP もしくは脳橋の萎縮,または putamen, MCP, or pons or hypometabolism on FDGFDG-PET による被殻の代謝低下が追加されている。 PET in putamen were included as additional features for possible MSA-C. Acknowledgments: The 謝 辞 second consensus conference on multiple system atrophy (MSA) was supported in part by 第 2from 回の多系統萎縮症(MSA)に関するコンセンサス会 grants the NIH (National Institute of Neurological Disorders and Stroke grant 1 R13 NS055459), Novartis Phar議は,NIH(国立神経疾患・脳卒中研究所の助成金 1 R13 maceuticals, and Chelsea Therapeutics, and the American NS055459) ,Novartis Pharmaceuticals 社,Chelsea Therapeutics 社 Academy of Neurology (AAN) agreed to cosponsor the の支援を一部受けた。また,米国神経学会(American Academy event. This manuscript was prepared for the conference by the Neuroimaging group of the second consensus conferof Neurology; AAN)も協賛に合意している。本稿は,本稿の ence, which included the authors of this manuscript DJB 著者である DJB(議長)および KS が参加する第 2 回コンセ (Chair) and KS. ンサス会議の神経画像検査部会用に作成されたものである。 Contributor Roles: David Brooks: Conception; literature search and writing of the first draft, especially regarding the part of ‘‘Functional imaging役割分担 in MSA’’; review and critique of the whole manuscript. David Brooks:論文の構想,文献検索および論文初稿(特 Klaus Seppi: Conception; literature search and writing of に 「MSA における機能画像」 )の執筆, 論文原稿の査読と批評。 the first draft, especially regarding the part of ‘‘Structural imaging MSA’’; review and critique of the whole manuKlaus in Seppi:論文の構想,文献検索および論文初稿(特に script. 「MSA における形態画像」)の執筆,論文原稿の査読と批評。 名(うち 9 名は心血管反射障害を合併) , MSA 患者 24 名(う ち 17 名は心血管反射障害を合併) ,PAF 患者 7 名を対象に 18 F—ドパミン PET を施行した 105。起立性低血圧を伴う PD の全 9 例と起立性低血圧を伴わない 11 例では,心筋の 18 F—ドパミン取り込みが PAF 患者でみられるような低いレ NEUROIMAGING CRITERIA FOR ベルにまで減少していた。一方,MSA の全 24 例では,心 筋の 18F—ドパミン集積に異常はみられなかった。Goldstein that most cases of PD, but not MSA, are associated らは,再度,PD 症例の大半に心筋節後交感神経の脱神経 with postganglionic sympathetic denervation of the myocardium. がみられるが,MSA ではみられないと結論付けた。 22 結 論CONCLUSIONS To summarize, the characteristic abnormalities shown by MSA cases with the different structural and 以上のように, 臨床診断が確定している患者では, 様々 functional neuroimaging methods have been docuな形態的・機能的神経画像検査によって MSA 症例に特 mented for patients with an established clinical diagnosis (see Table 5). To determine which of these techni徴的な異常が認められている(Table 5 参照) 。今後, ques will emerge as standard investigations in the MSA 患者の精密検査においてどの画像検査法が標準とな work-up of MSA patients presenting requires further prospective studies during early disease stages when るかを判断するには,臨床診断が確定していない MSA the clinical diagnosis remains uncertain. Based on the 初期患者を対象に,さらなる前向き試験を行う必要があ best current knowledge, the revised consensus criteria る。現時点で得られている最善の知見に基づいたコンセ include neuroimaging criteria for the diagnostic cateAtrophy on conventional gory of possible MSA.103 ンサス基準の改訂版には, 「MSA の可能性あり(possible MRI of putamen, MCP, pons, or cerebellum or hypoMSA) 」の診断カテゴリーのために神経画像基準が追加 metabolism on FDG-PET in putamen, brainstem, or 103 されている 。 「MSA-P の可能性あり(possible MSA-P) cerebellum were included as additional features for」 possible MSA-P; and atrophy on conventional MRI of の所見としては,従来型 MRI による被殻,MCP,脳橋も putamen, MCP, or pons or hypometabolism on FDGPET in putamen were included as additional features for possible MSA-C. Acknowledgments: The second consensus conference on REFERENCES REFERENCES 1. Konagaya M, Konagaya Y, Iida M. Clinical and magnetic resonance imaging study of extrapyramidal symptoms in multiple system atrophy. J Neurol Neurosurg Psychiatry 1994;57:1528– 1531. 2. Kraft E, Schwarz J, Trenkwalder C, Vogl T, Pfluger T, Oertel WH. The combination of hypointense and hyperintense signal changes on T2-weighted magnetic resonance imaging sequenTHE DIAGNOSIS OF MSA 961 ces: a specific marker of multiple system atrophy? Arch Neurol 1999;56:225–228. 3. von Lewinski, Werner C, Jorn T, Mohr A, Sixel-Doring F, Trenkwalder C. T2*-weighted MRI in diagnosis of multiple system atrophy. A practical approach for clinicians. J Neurol 2007;254:1184–1188. 4. Righini A, Antonini A, Ferrarini M, et al. Thin section MR study of the basal ganglia in the differential diagnosis between striatonigral degeneration and Parkinson’s disease. J Comput Assist Tomogr 2002;26:266–271. 5. Schocke MF, Seppi K, Esterhammer R, et al. Diffusionweighted MRI differentiates the Parkinson variant of multiple system atrophy from PD. Neurology 2002;58:575–580. 6. Lee EA, Cho HI, Kim SS, Lee WY. Comparison of magnetic resonance imaging in subtypes of multiple system atrophy. Parkinsonism Relat Disord 2004;10:363–368. 7. Bhattacharya K, Saadia D, Eisenkraft B, et al. Brain magnetic resonance imaging in multiple-system atrophy and Parkinson’s disease: a diagnostic algorithm. Arch Neurol 2002;59:835–842. 8. Burk K, Buhring U, Schulz JB, Zuhlke C, Hellenbroich Y, Dichgans J. Clinical and magnetic resonance imaging characteristics of sporadic cerebellar ataxia. Arch Neurol 2005;62: 981–985. 9. Nicoletti G, Fera F, Condino F, et al. MR imaging of middle cerebellar peduncle width: differentiation of multiple system atrophy from Parkinson’s disease. Radiology 2006;239:825–830. 10. Paviour DC, Thornton JS, Lees AJ, Jager HR. Diffusionweighted magnetic resonance imaging differentiates parkinsonian variant of multiple-system atrophy from progressive supranuclear palsy. Mov Disord 2007;22:68–74. 11. Seppi K, Schocke MF, Prennschuetz-Schuetzenau K, et al. Topography of putaminal degeneration in multiple system atrophy: a diffusion magnetic resonance study. Mov Disord 2006; 21:847–852. 12. Schulz JB, Skalej M, Wedekind D, et al. Magnetic resonance imaging-based volumetry differentiates idiopathic Parkinson’s syndrome from multiple system atrophy and progressive supranuclear palsy. Ann Neurol 1999;45:65–74. 8. Burk Dichg teristi 981–9 9. Nicol cerebe rophy 10. Pavio weigh nian v nuclea 11. Seppi pogra phy: 21:84 12. Schul imagi syndr nuclea 13. Burk entiat 175–1 14. Quatt for di kinson atroph 15. Seppi diffus differ system ord 20 16. Schoc tensor atroph 1451. 17. Nicol ficien tiate t progre 2687. 18. Ito M fractio for de rol Ne 19. Ecker pathic sive s tion tr 20. Walte ler D. diseas 60:74 ntional hypom, or es for MRI of FDGeatures nce on part by al Diss Pharmerican or the nce by conferpt DJB erature ing the ique of ting of uctural manu- tic resomultiple 7:1528– , Oertel e signal sequenNeurol study. Neuroimage 2006;31:240–245. cerebellar peduncle width: differentiation of multiple system at30. Yekhlef F, Ballan G, Macia F, Delmer O, Sourgen C, Tison F. rophy from Parkinson’s disease. Radiology 2006;239:825–830. Routine MRI for the differential diagnosis of Parkinson’s dis10. Paviour DC, Thornton JS, Lees AJ, Jager HR. Diffusionease, MSA, PSP, and CBD. J Neural Transm 2003;110:151– weighted magnetic resonance imaging differentiates parkinsoD.J. Brooks and K. Seppi 169. nian variant of multiple-system atrophy from progressive supra31. Ito S, Shirai W, Hattori T. Evaluating posterolateral linearizanuclear palsy. Mov Disord 2007;22:68–74. tion of the putaminal margin with magnetic resonance imaging 11. Seppi K, Schocke MF, Prennschuetz-Schuetzenau K, et al. Toto diagnose the Parkinson variant of multiple system atrophy. pography of putaminal degeneration in multiple system atroMov Disord 2007;22:578–581. phy: a diffusion magnetic resonance study. Mov Disord 2006; 32. Lee WH, Lee CC, Shyu WC, Chong PN, Lin SZ. Hyperintense 21:847–852. putaminal rim sign is not a hallmark of multiple system atro12. Schulz JB, Skalej M, Wedekind D, et al. Magnetic resonance phy at 3T. AJNR Am J Neuroradiol 2005;26:2238–2242. imaging-based volumetry differentiates idiopathic Parkinson’s 33. Muqit MM, Mort D, Miskiel KA, Shakir RA. "Hot cross bun" syndrome from multiple system atrophy and progressive suprasign in a patient with Parkinsonism secondary to presumed vasnuclear palsy. Ann Neurol 1999;45:65–74. culitis. J Neurol Neurosurg Psychiatry 2001;71:565–566. 13. Burk K, Globas C, Wahl T, et al. MRI-based volumetric differ34. Burk K, Skalej M, Dichgans J. Pontine MRI hyperintensities entiation of sporadic cerebellar ataxia. Brain 2004;127(Part 1): (‘‘the cross sign’’) are not pathognomonic for multiple system 175–181. atrophy (MSA). Mov Disord 2001;16:535. 14. Quattrone A, Nicoletti G, Messina D, et al. MR imaging index 35. Watanabe H, Saito Y, Terao S, et al. Progression and prognosis for differentiation of progressive supranuclear palsy from Parin multiple system atrophy: an analysis of 230 Japanese kinson’s disease and the Parkinson variant of multiple system patients. Brain 2002;125(Part 5):1070–1083. atrophy. Radiology 2008;246:214–221. 36. Horimoto Y, Aiba I, Yasuda T, et al. Longitudinal MRI study 15. Seppi K, Schocke MF, Donnemiller E, et al. Comparison of of multiple system atrophy—when do the findings appear, and diffusion-weighted imaging and [123I]IBZM-SPECT for the what is the course? J Neurol 2002;249:847–854. differentiation of patients with the Parkinson variant of multiple 37. Yabe I, Soma H, Takei A, Fujiki N, Yanagihara T, Sasaki H. system atrophy from those with Parkinson’s disease. Mov DisMSA-C is the predominant clinical phenotype of MSA in ord 2004;19:1438–1445. Japan: analysis of 142 patients with probable MSA. J Neurol 16. Schocke MF, Seppi K, Esterhammer R, et al. Trace of diffusion Sci 2006;249:115–121. tensor differentiates the Parkinson variant of multiple system 38. Kraft E, Trenkwalder C, Auer DP. T2*-weighted MRI differenatrophy and Parkinson’s disease. Neuroimage 2004;21:1443– tiates multiple system atrophy from Parkinson’s disease. Neu1451. rology 2002;59:1265–1267. 17. Nicoletti G, Lodi R, Condino F, et al. Apparent diffusion coef39. Ghaemi M, Hilker R, Rudolf J, Sobesky J, Heiss WD. Differficient measurements of the middle cerebellar peduncle differenentiating multiple system atrophy from Parkinson’s disease: tiate the Parkinson variant of MSA from Parkinson’s disease and contribution of striatal and midbrain MRI volumetry and multiprogressive supranuclear palsy. Brain 2006;129(Part 10):2679– tracer PET imaging. J Neurol Neurosurg Psychiatry 2002;73: 2687. 517–523. 18. Ito M, Watanabe H, Kawai Y, et al. Usefulness of combined 40. Brenneis C, Seppi K, Schocke MF, et al. Voxel-based morfractional anisotropy and apparent diffusion coefficient values phometry detects cortical atrophy in the Parkinson variant of for detection of involvement in multiple system atrophy. J Neu962rol Neurosurg Psychiatry 2007;78:722–728. D.J. BROOKS AND K.multiple SEPPIsystem atrophy. Mov Disord 2003;18:1132–1138. 41. Specht K, Minnerop M, Abele M, Reul J, Wullner U, Klock19. Eckert T, Sailer M, Kaufmann J, et al. Differentiation of idiogether T. In vivo voxel-based morphometry in multiple system pathic Parkinson’s disease, multiple system atrophy, progres21.sive Behnke S, Berg palsy, D, Naumann M, Becker G. using Differentiation atrophy of the cerebellar type. Arch Neurol 2003;60:1431– supranuclear and healthy controls magnetiza-of Parkinson’s disease Neuroimage and atypical2004;21:229–235. parkinsonian syndromes by 1435. tion transfer imaging. transcranial ultrasound. J Neurol Neurosurg Psychiatry 2005; 42. Brenneis C, Boesch SM, Egger KE, et al. Cortical atrophy in 20. Walter U, Niehaus L, Probst T, Benecke R, Meyer BU, Dress962 ler76:423–425. D.J.Parkinson’s BROOKS AND K. the SEPPI cerebellar variant of multiple system atrophy: a voxel-based D. Brain parenchyma sonography discriminates Movement Disorders, Vol. 24, Mov No. 7,Disord 2009 2006;21:159–165. 22.disease Okawaand M, atypical Miwa H,parkinsonian Kajimoto Y,syndromes. et al. Transcranial morphometry study. Neurologysonogra2003; phy of the substantia nigra in Japanese patients with Parkin60:74–77. 43. Specht K, Minnerop M, Muller-Hubenthal J, Klockgether T. son’s disease Parkinsonism: clinical potential and Voxel-based of multiple-system atrophy of cerebellar 21. Behnke S, BergorD,atypical Naumann M, Becker G. Differentiation of atrophy of theanalysis cerebellar type. Arch Neurol 2003;60:1431– limitations. disease Intern Med type: complementary results by combining voxel-based morParkinson’s and 2007;46:1527–1531. atypical parkinsonian syndromes by 1435. 23.transcranial Walter U, Dressler D, Probst T, etNeurosurg al. Transcranial brain 2005; sonogphometryC,and voxel-based relaxometry. 2005;25: ultrasound. J Neurol Psychiatry 42. Brenneis Boesch SM, Egger KE, et al.Neuroimage Cortical atrophy in raphy findings in discriminating between Parkinsonism and idi287–293. 76:423–425. the cerebellar variant of multiple system atrophy: a voxel-based Movement Disorders, Vol. 24, No. 7, 2009 opathicM, Parkinson’s Arch 2007;64:1635–1640. 44.morphometry Minnerop M,study. Specht K, Disord Ruhlmann J, et al. Voxel-based mor22. Okawa Miwa H, disease. Kajimoto Y, Neurol et al. Transcranial sonograMov 2006;21:159–165. 24.phy Drayer BP,substantia Olanow W, P, Johnson GA,with Herfkens phometry voxel-based relaxometry in multiple system atroof the nigraBurger in Japanese patients Parkin-R, 43. Specht K, and Minnerop M, Muller-Hubenthal J, Klockgether T. Riederer S. Parkinson plusParkinsonism: syndrome: diagnosis high and field phy—a comparison clinical subtypes son’s disease or atypical clinical using potential Voxel-based analysis between of multiple-system atrophyand of correlations cerebellar MR imaging of brain Radiology 1986;159:493–498. with complementary clinical parameters. Neuroimage 2007;36:1086–1095. limitations. Intern Med iron. 2007;46:1527–1531. type: results by combining voxel-based mor25.Walter Pastakia Polinsky Di CG, JT, Brown Wener 45.phometry Brenneis and C, Egger K, Scherfler C, et al.Neuroimage Progression2005;25: of brain 23. U, B, Dressler D, R, Probst T, etSimmons al. Transcranial brainR,sonogvoxel-based relaxometry. L. Multiple atrophy (Shy-Drager syndrome): MR atrophy in multiple system atrophy. A longitudinal VBM study. raphy findingssystem in discriminating between Parkinsonism andimagidi287–293. ing. Radiology 1986;159:499–502. J Neurol 2007;254:191–196. opathic Parkinson’s disease. Arch Neurol 2007;64:1635–1640. 44. Minnerop M, Specht K, Ruhlmann J, et al. Voxel-based mor26.Drayer SchragBP, A, Kingsley D, Phatouros et al. Clinical usefulness 46.phometry Oba H, Yagishita A, Terada H, et al.inNew and system reliableatroMRI 24. Olanow W, Burger P, C, Johnson GA, Herfkens R, and voxel-based relaxometry multiple of magnetic resonance in diagnosis multiple using systemhigh atrophy. diagnosis for progressive palsy. and Neurology 2005; Riederer S. Parkinson plusimaging syndrome: field phy—a comparison betweensupranuclear clinical subtypes correlations J Neurol Neurosurg 1998;65:65–71. 64: 2050–2055. MR imaging of brain Psychiatry iron. Radiology 1986;159:493–498. with clinical parameters. Neuroimage 2007;36:1086–1095. 27.Pastakia Schrag A, CD,R,Miszkiel et al. Differentiation atypi47.Brenneis Seppi K,C, Schocke Esterhammer R, et al. Diffusion25. B, Good Polinsky Di CG, K, Simmons JT, Brown R,ofWener 45. Egger K, MF, Scherfler C, et al. Progression of brain parkinsonian syndromes with routine MRI. MR Neurology weighted imaging system discriminates progressive supranuclear palsy L.calMultiple system atrophy (Shy-Drager syndrome): imagatrophy in multiple atrophy. A longitudinal VBM study. 2000;54: 697–702. PD,2007;254:191–196. but not from the Parkinson variant of multiple system ing. Radiology 1986;159:499–502. J from Neurol 28.Schrag Savoiardo M. Differential diagnosis and atrophy. Neurology 26. A, Kingsley D, Phatouros C, of et Parkinson’s al. Clinical disease usefulness 46. Oba H, Yagishita A,2003;60:922–927. Terada H, et al. New and reliable MRI parkinsonian imaging. 48.diagnosis Naka H,for Imon Y, Ohshita T, et al.palsy. Magnetization ofatypical magnetic resonancedisorders imagingbyinmagnetic multipleresonance system atrophy. progressive supranuclear Neurology transfer 2005; 2003;24(Suppl 1):S35–S37. measurements J Neurol Neurol Sci Neurosurg Psychiatry 1998;65:65–71. 64: 2050–2055. of brain structures in patients with multiple sys29.Schrag Seppi K, Mair KJ, Progression of putaminal tem atrophy. Neuroimage 2002;17:1572–1578. 27. A, Schocke Good CD,MF, Miszkiel K, et al. Differentiation of atypi47. Seppi K, Schocke MF, Esterhammer R, et al. Diffusiondegeneration in multiple system atrophy: a serial MR 49.weighted Kanazawa M, Shimohata T, Terajima K, supranuclear et al. Quantitative cal parkinsonian syndromes with routine MRI.diffusion Neurology imaging discriminates progressive palsy study. Neuroimage evaluation brainstem in multiple system system atrophy 2000;54: 697–702. 2006;31:240–245. from PD, butofnot from theinvolvement Parkinson variant of multiple 30.Savoiardo Yekhlef F,M.Ballan G, Macia F, Delmer O, Sourgendisease C, Tison by diffusion-weighted MR imaging. J Neurol 2004;251:1121– 28. Differential diagnosis of Parkinson’s andF. atrophy. Neurology 2003;60:922–927. Routineparkinsonian MRI for thedisorders differential diagnosisresonance of Parkinson’s dis1124.H, Imon Y, Ohshita T, et al. Magnetization transfer atypical by magnetic imaging. 48. Naka ease, MSA, PSP, and CBD. J Neural Transm 2003;110:151– 50.measurements Blain CR, Barker GJ, structures Jarosz JM, al. Measuring brain sysstem Neurol Sci 2003;24(Suppl 1):S35–S37. of brain in et patients with multiple 169. K, Schocke MF, Mair KJ, et al. Progression of putaminal andatrophy. cerebellar damage in2002;17:1572–1578. parkinsonian syndromes using diffu29. Seppi tem Neuroimage 31.degeneration Ito S, ShiraiinW, Hattorisystem T. Evaluating linearizasion tensorM, MRI. Neurology multiple atrophy: posterolateral a serial diffusion MR 49. Kanazawa Shimohata T, 2006;67:2199–2205. Terajima K, et al. Quantitative tion of the putaminal margin with magnetic resonance imaging 51.evaluation Berg D, Siefker C, Becker G. Echogenicity the substantia study. Neuroimage 2006;31:240–245. of brainstem involvement in multipleofsystem atrophy to diagnose the Parkinson of multiple system atrophy. nigra in Parkinson’s disease and its relation clinical findings. 30. Yekhlef F, Ballan G, Macia variant F, Delmer O, Sourgen C, Tison F. by diffusion-weighted MR imaging. J Neurolto 2004;251:1121– Mov Disord J Neurol 2001;248:684–689. Routine MRI 2007;22:578–581. for the differential diagnosis of Parkinson’s dis1124. 32.ease, Lee WH, CC,and Shyu WC,J Chong Lin SZ. Hyperintense 52.Blain Stockner SeppiGJ, K, Jarosz Kiechl JM, S, etetal.al.Midbrain transcranial soMSA,Lee PSP, CBD. NeuralPN, Transm 2003;110:151– 50. CR, H, Barker Measuring brain stem putaminal rim sign is not a hallmark of multiple system atronography findings in in a parkinsonian population-based study. using Mov diffuDisord 169. and cerebellar damage syndromes phyS,atShirai 3T. AJNR Am J Neuroradiol 2005;26:2238–2242. 2006;25(Suppl):S634 (Abstract). 31. Ito W, Hattori T. Evaluating posterolateral linearizasion tensor MRI. Neurology 2006;67:2199–2205. 33.tion Muqit MM, Mort D, margin Miskielwith KA,magnetic Shakir RA. "Hot cross bun" 53.Berg Schmidauer C, Sojer M, Seppi K, et al. Transcranial ultrasound of the putaminal resonance imaging 51. D, Siefker C, Becker G. Echogenicity of the substantia in a patient with Parkinsonism to presumed vasshows hypoechogenicity in relation restless to legsclinical syndrome. Ann tosign diagnose the Parkinson variant ofsecondary multiple system atrophy. nigra in nigral Parkinson’s disease and its findings. culitis. J Neurol Neurosurg Psychiatry 2001;71:565–566. Mov Disord 2007;22:578–581. J Neurol Neurol 2005;58:630–634. 2001;248:684–689. 34.Lee Burk K, Lee Skalej Dichgans J. Pontine MRI 54.Stockner Fulham H, MJ,Seppi Dubinsky RM, S,Polinsky RJ, et al. Computedsoto32. WH, CC,M, Shyu WC, Chong PN, Lin SZ.hyperintensities Hyperintense 52. K, Kiechl et al. Midbrain transcranial (‘‘the cross arenot nota pathognomonic for multiple mography,findings magnetic imaging and positron putaminal rimsign’’) sign is hallmark of multiple system system atronography in resonance a population-based study. Mov emission Disord atrophy 2001;16:535. tomography with [18F]fluorodeoxyglucose in multiple system phy at 3T.(MSA). AJNR Mov Am JDisord Neuroradiol 2005;26:2238–2242. 2006;25(Suppl):S634 (Abstract). 35.Muqit Watanabe Saito Terao KA, S, et Shakir al. Progression prognosis atrophy andC, pure Clin Auton ultrasound Res 1991; 33. MM,H, Mort D,Y,Miskiel RA. "Hotand cross bun" 53. Schmidauer Sojer autonomic M, Seppi K,failure. et al. Transcranial in in multiple system atrophy: an secondary analysis to of presumed 230 Japanese 1:27–36. sign a patient with Parkinsonism vasshows nigral hypoechogenicity in restless legs syndrome. Ann 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 23 evalua by dif 1124. Blain and ce sion te Berg D nigra i J Neur Stockn nograp 2006;2 Schmi shows Neuro Fulham mogra tomog atroph 1:27–3 Gilma rent R positro and o 175. Eidelb tabolis son’s d De Vo utiliza nigral Otsuka betwee positro Ann N Eckert ential 26:912 Bosma 99mTc tion b maging atrophy. rintense m atro. ss bun" med vas. tensities system ognosis apanese RI study ear, and saki H. MSA in Neurol ifferene. Neu- Differdisease: d multi002;73: ed morriant of 8. Klocksystem 24 1990;28:547–555. 51. Berg D, Siefker C, Becker G. Echogenicity of the substantia 71. Burn DJ, Sawle GV, Brooks DJ. Differential diagnosis of Parnigra in Parkinson’s disease and its relation to clinical findings. kinson’s disease, multiple system atrophy, and Steele-RichardJ Neurol 2001;248:684–689. son-Olszewski syndrome: discriminant analysis of striatal 18F52. Stockner H, Seppi K, Kiechl S, et al. Midbrain transcranial so多系統萎縮症の診断を目的とした神経画像の基準案 dopa PET data. J Neurol Neurosurg Psychiatry 1994;57:278– nography findings in a population-based study. Mov Disord 284. 2006;25(Suppl):S634 (Abstract). 72. Rinne JO, Burn DJ, Mathias CJ, Quinn NP, Marsden CD, 53. Schmidauer C, Sojer M, Seppi K, et al. Transcranial ultrasound Brooks DJ. Positron emission tomography studies on the dopashows nigral hypoechogenicity in restless legs syndrome. Ann minergic system and striatal opioid binding in the olivopontoNeurol 2005;58:630–634. cerebellar atrophy variant of multiple system atrophy. Ann 54. Fulham MJ, Dubinsky RM, Polinsky RJ, et al. Computed toNeurol 1995;37:568–573. mography, magnetic resonance imaging and positron emission 73. Gilman S, Frey KA, Koeppe RA, et al. Decreased striatal tomography with [18F]fluorodeoxyglucose in multiple system monoaminergic terminals in olivopontocerebellar atrophy and atrophy and pure autonomic failure. Clin Auton Res 1991; multiple system atrophy demonstrated with positron emission 1:27–36. tomography. Ann Neurol 1996;40:885–892. 55. Gilman S, Koeppe RA, Junck L, Kluin KJ, Lohman M, St Lau74. Pirker W, Asenbaum S, Bencsits G, et al. [123I]b-CIT SPECT rent RT. Patterns of cerebral glucose metabolism detected with in multiple system atrophy, progressive supranuclear palsy, positron emission tomography differ in multiple system atrophy and corticobasal degeneration. Mov Disord 2000;15:1158– and olivopontocerebellar atrophy. Ann Neurol 1994;36:166– 1167. 175. 75. Kim YJ, Ichise M, Ballinger JR, et al. Combination of dopamine 56. Eidelberg D, Takikawa S, Moeller JR, et al. Striatal hypometransporter and D2 receptor SPECT in the diagnostic evaluation tabolism distinguishes striatonigral degeneration from Parkinof PD, MSA, and PSP. Mov Disord 2002;17:303–312. son’s disease. Ann Neurol 1993;33:518–527. 76. Lu CS, Weng YH, Chen MC, et al. 99mTc-TRODAT-1 57. De Volder AG, Francart J, Laterre C, et al. Decreased glucose imaging of multiple system atrophy. J Nucl Med 2004;45: utilization in the striatum and frontal lobe in probable striato49–55. nigral degeneration. Ann Neurol 1989;26:239–247. 77. Scherfler C, Seppi K, Donnemiller E, et al. Voxel-wise analysis 58. Otsuka M, Kuwabara Y, Ichiya Y, et al. Differentiating NEUROIMAGING CRITERIA OF MSA 963 of DIAGNOSIS [123I]b-CIT SPECT differentiates the Parkinson variant of between multiple system atrophy and Parkinson’s disease by FOR THE multiple system atrophy from idiopathic Parkinson’s disease. positron emission tomography with 18F-dopa and 18F-FDG. Brain 2005;128(Part 7):1605–1612. Ann Nucl Med 1997;11:251–257. idiopathic Parkinson’s disease. Nucl PET MedinMol 78. Seppi K, Scherfler C, Donnemiller E, et al. Topography of do59. Eckert T, Barnes A, Dhawan V, Eur et al.J FDG the Imaging differ2003;diagnosis 30:16–24.of parkinsonian disorders. Neuroimage 2005; pamine transporter availability in progressive supranuclear ential 61.26:912–921. Van LK, Santens P, Bosman T, De RJ, Mortelmans L, palsy: a voxelwise [123I]b-CIT SPECT analysis. Arch Neurol NEUROIMAGING CRITERIA FOR THE2006;63:1154–1160. DIAGNOSIS OF MSA 963 DierckxT,R. Van Statistical parametric mapping of (99m)Tc-ECD 60. Bosman LK, Santens P. Anatomically standardised SPECT in idiopathic Parkinson’s disease and multiple sys79. Antonini A, Schwarz J, Oertel WH, Beer HF, Madeja UD, 99mTc-ECD brain perfusion SPET allows accurate differentiatembetween atrophy healthy with predominant parkinsonian features: Leenders KL. [11C]raclopride and positron emission tomogration volunteers, multiple system atrophycorreand lation with clinical parameters. Med Mol 2004;45:933– phy in patients Parkinson’s disease: idiopathic Parkinson’s disease. Eur JJ Nucl Med Imaging 78. Seppi K, previously Scherfler C,untreated Donnemiller E, etwith al. Topography of doand lisurideintherapy on striatal dopamine 942. 30:16–24. influence of L-dopa availability 2003; pamine transporter progressive supranuclear D2-receptors. Neurology 1994;44:1325–1329. 62.Van Eidelberg D, Moeller Ishikawa al. Assessment of dis61. LK, Santens P, JR, Bosman T, T,Deet RJ, Mortelmans L, palsy: a voxelwise [123I]b-CIT SPECT analysis. Arch Neurol 80.2006;63:1154–1160. Kaasinen V, Nagren K, Hietala J, et al. Extrastriatal dopamine ease severity in Parkinsonism withmapping fluorine-18-fluorodeoxygluDierckx R. Statistical parametric of (99m)Tc-ECD D2 and A, D3 Schwarz receptors J,inOertel early and discose and J Nucl Parkinson’s Med 1995;36:378–383. SPECT in PET. idiopathic disease and multiple sys79. Antonini WH,advanced Beer HF,Parkinson’s Madeja UD, ease. Neurology 2000;54:1482–1487. 63.tem Feigin A, Antonini A, Fukuda M, et al. Tc-99m ethylene cysatrophy with predominant parkinsonian features: correLeenders KL. [11C]raclopride and positron emission tomogra81.phy Turjanski N, Leesuntreated AJ, Brooks DJ. with In vivo studies on striatal teinatewith dimer SPECTparameters. in the differential of Parkinsonlation clinical J Nucldiagnosis Med 2004;45:933– in previously patients Parkinson’s disease: dopamineofD1 and D2 bindingtherapy in L-dopa-treated ism. Mov Disord 2002;17:1265–1270. L-dopa andsite lisuride on striatal Parkinson’s dopamine 942. influence disease patients with and without dyskinesias. Neurology 1997; 64.Eidelberg Cilia R, D, Marotta G,JR, Benti R, Pezzoli G,Assessment Antonini A. D2-receptors. Neurology 1994;44:1325–1329. 62. Moeller Ishikawa T, et al. of Brain dis49:717–723. SPECT imaging in multiple system atrophy. J Neural Transm 80. Kaasinen V, Nagren K, Hietala J, et al. Extrastriatal dopamine ease severity in Parkinsonism with fluorine-18-fluorodeoxyglu82.D2 Pizzolato Chierichetti F, Rossato A, et al. Alterations 2005;112:1635–1645. and D3G,receptors in early and advanced Parkinson’s dis-of cose and PET. J Nucl Med 1995;36:378–383. striatal dopamine D2 receptors contribute to deteriorated 65.Feigin DavieA,CA, Wenning GK, Barker al. Differentiation ease. Neurology 2000;54:1482–1487. 63. Antonini A, Fukuda M, etGJ, al. etTc-99m ethylene cys-of L-dopa Parkinson’s disease: a [123I]-IBZM response N, to Lees multiple system atrophy idiopathic Parkinson’s disease 81. Turjanski AJ, inBrooks DJ. In vivo studies on striatal teinate dimer SPECT in the from differential diagnosis of ParkinsonSPET study. J Neural Transm Suppl using proton resonance spectroscopy. Ann Neurol -dopa-treated Parkinson’s dopamine D1 and D2 site binding in L1995;45:113–122. ism. Mov Disordmagnetic 2002;17:1265–1270. 83.disease Hwangpatients WJ, Yao WJ,and Wey SP, Shen LH, Ting G. Downregula1995;37:204–210. with without dyskinesias. Neurology 1997; 64. Cilia R, Marotta G, Benti R, Pezzoli G, Antonini A. Brain tion of striatal dopamine D2 receptors in advanced Parkinson’s 66.SPECT Federico F, Simone IL, Lucivero et al. Usefulness proton 49:717–723. imaging in multiple systemV,atrophy. J Neural of Transm disease contributes to the motor fluctuation. magnetic resonance spectroscopy in differentiating parkinsonian 82. Pizzolato G, Chierichetti F, development Rossato A, etof al. Alterations of 2005;112:1635–1645. Eur Neurol 2002;47:113–117. syndromes. Ital J Neurol 1999;20:223–229. striatal dopamine D2 receptors contribute to deteriorated 65. Davie CA, Wenning GK, Sci Barker GJ, et al. Differentiation of 84.response ShinotohtoH,L-dopa Aotsukain A,Parkinson’s Yonezawa disease: H. Striatal dopamine D2 67.multiple Clarke CE, Lowry M. Systematic reviewParkinson’s of proton magnetic a [123I]-IBZM system atrophy from idiopathic disease receptors disease and1995;45:113–122. striato-nigral degeneration resonance of the striatum in parkinsonian synSPET study.inJ Parkinson’s Neural Transm Suppl using protonspectroscopy magnetic resonance spectroscopy. Ann Neurol determined by positron Nagatsu T, dromes. Eur J Neurol 2001;8:573–577. 83. Hwang WJ, Yao WJ, Weyemission SP, Shentomography. LH, Ting G.In: Downregula1995;37:204–210. Fisher A, Yoshida M, editors. Basic,inclinical andParkinson’s therapeutic 68.Federico Watanabe H, Fukatsu H, Katsuno M,al.etUsefulness al. Multiple tion of striatal dopamine D2 receptors advanced 66. F, Simone IL, Lucivero V, et of regional proton advances of Alzheimer’s Parkinson’sofdiseases, Vol. 2. New 1H-MR resonance spectroscopy in multiple system atrophy: NAA/Cr disease contributes to theand development motor fluctuation. magnetic spectroscopy in differentiating parkinsonian York: Plenum Press; 1990. p 107–110. reduction Ital in pontine as a valuable diagnostic marker. Eur Neurol 2002;47:113–117. syndromes. J Neurolbase Sci 1999;20:223–229. 85.Shinotoh van RE, H, Verhoeff NF,A,Speelman JD,H.Wolters Kuiper MA, J Neurol Psychiatry 2004;75:103–109. 84. Aotsuka Yonezawa StriatalEC, dopamine D2 67. Clarke CE,Neurosurg Lowry M. Systematic review of proton magnetic Janssen AG. Multiple system and progressive supranu69.resonance Brooks DJ, Salmon EP, CJ, etin al. The relationship receptors in Parkinson’s diseaseatrophy and striato-nigral degeneration spectroscopy of Mathias the striatum parkinsonian synclear palsybydiminished striatal D2 dopamine In: receptor activity betweenEur locomotor autonomic dysfunction, and the determined positron emission tomography. Nagatsu T, dromes. J Neurol disability, 2001;8:573–577. demonstrated by 123I-IBZM computed integrity H, of the striatal in patients with Fisher A, Yoshida M, editors.single Basic,photon clinicalemission and therapeutic 68. Watanabe Fukatsu H, dopaminergic Katsuno M, etsystem al. Multiple regional tomography. Arch Neurol multiplespectroscopy system atrophy, pure autonomic Parkinadvances of Alzheimer’s and1993;50:513–516. Parkinson’s diseases, Vol. 2. New 1H-MR in multiple system failure, atrophy:and NAA/Cr 86.York: Schwarz J, Tatsch K, Arnold G, et al. 123I-iodobenzamideson’s disease, studiedbase with as PET. Brain 1990;113(Part 5):1539– Plenum Press; 1990. p 107–110. reduction in pontine a valuable diagnostic marker. SPECT predictsNF, dopaminergic in patients 85. van RE, Verhoeff Speelman JD,responsiveness Wolters EC, Kuiper MA, J 1552. Neurol Neurosurg Psychiatry 2004;75:103–109. with de novo Parkinsonism. Neurology 1992;42(3supranuPart 1): 70.Brooks BrooksDJ, DJ, Salmon Ibanez V, GV,CJ, et et al. al. Differing patterns of Janssen AG. Multiple system atrophy and progressive 69. EP,Sawle Mathias The relationship 556–561. striatal 18F-dopa in Parkinson’s multiple clear palsy diminished striatal D2 dopamine receptor activity between locomotoruptake disability, autonomicdisease, dysfunction, andsystem the 87.demonstrated Knudsen GM, M, single Thomsen G, etemission al. Imaging of doatrophy,ofand supranuclear palsy. Ann Neurol byKarlsborg 123I-IBZM photon computed integrity the progressive striatal dopaminergic system in patients with pamine transporters and 1993;50:513–516. D2 receptors in patients with Parkin1990;28:547–555. tomography. Arch Neurol multiple system atrophy, pure autonomic failure, and Parkinson’s disease and K, multiple Eur J Nucl Med 71.son’s Burndisease, DJ, Sawle GV, with Brooks DJ.Brain Differential diagnosis of Par86. Schwarz J, Tatsch Arnoldsystem G, et atrophy. al. 123I-iodobenzamidestudied PET. 1990;113(Part 5):1539– Mol Imaging 2004;31:1631–1638. kinson’s disease, multiple system atrophy, and Steele-RichardSPECT predicts dopaminergic responsiveness in patients 1552. 88.with Plotkin Amthauer H, Klaffke S, et al.1992;42(3 Combined Part 123I-FPson-Olszewski syndrome: discriminant of patterns striatal 18Fde M, novo Parkinsonism. Neurology 1): 70. Brooks DJ, Ibanez V, Sawle GV, et al.analysis Differing of CIT and 123I-IBZM SPECT for the diagnosis of parkinsonian dopa PET data.uptake J Neurol Neurosurg disease, Psychiatry 1994;57:278– 556–561. striatal 18F-dopa in Parkinson’s multiple system syndromes: on 72M,patients. J Neural 2005;112: 284. 87. Knudsen GM,study Karlsborg Thomsen G, et al.Transm Imaging of doatrophy, and progressive supranuclear palsy. Ann Neurol 677–692. 72.1990;28:547–555. Rinne JO, Burn DJ, Mathias CJ, Quinn NP, Marsden CD, pamine transporters and D2 receptors in patients with Parkin89.son’s Shinotoh H, Inoue O, Hirayama et al. Dopamine D1 recepBrooks Positron emissionDJ.tomography on the disease and multiple systemK,atrophy. Eur J Nucl Med 71. Burn DJ, DJ. Sawle GV, Brooks Differentialstudies diagnosis of dopaPartorsImaging in Parkinson’s disease and striatonigral degeneration: a minergicdisease, systemmultiple and striatal opioid binding the olivopontoMol 2004;31:1631–1638. kinson’s system atrophy, andinSteele-Richardpositron tomography Neurosurg Psycerebellar atrophy variant of multiple system Ann 88. Plotkin M,emission Amthauer H, Klaffkestudy. S, et Jal.Neurol Combined 123I-FPson-Olszewski syndrome: discriminant analysis of atrophy. striatal 18Fchiatry Neurol 1995;37:568–573. CIT and 1993;56:467–472. 123I-IBZM SPECT for the diagnosis of parkinsonian dopa PET data. J Neurol Neurosurg Psychiatry 1994;57:278– 90.syndromes: Piccini P, Weeks RA,72Brooks DJ. JAlterations in opioid receptor 73.284. Gilman S, Frey KA, Koeppe RA, et al. Decreased striatal study on patients. Neural Transm 2005;112: binding in Parkinson’s disease patients with levodopa-induced monoaminergic in olivopontocerebellar atrophyCD, and 677–692. 72. Rinne JO, Burn terminals DJ, Mathias CJ, Quinn NP, Marsden dyskinesias. Ann Neurol 1997;42:720–726. multiple atrophy demonstrated positron 89. Shinotoh H, Inoue O, Hirayama K, et al. Dopamine D1 recepBrooks DJ.system Positron emission tomographywith studies on theemission dopa91.tors Burnin DJ, Rinne JO,disease Quinn NP, AJ, Marsden CD, Brooks tomography. Ann Neurol 1996;40:885–892. Parkinson’s and Lees striatonigral degeneration: a minergic system and striatal opioid binding in the olivopontoDJ. Striatal opioid receptor study. bindingJ Neurol in Parkinson’s 74.cerebellar Pirker W,atrophy Asenbaum S, Bencsits G, et al. [123I]b-CIT positron emission tomography Neurosurgdisease, Psyvariant of multiple system atrophy.SPECT Ann striatonigral degeneration and Steele-Richardson-Olszewski in multiple system atrophy, progressive supranuclear palsy, chiatry 1993;56:467–472. Neurol 1995;37:568–573. syndrome, A [11C]diprenorphine PET study. Brain receptor 1995;118 and corticobasal degeneration. Mov Disord 2000;15:1158– 90. Piccini P, Weeks RA, Brooks DJ. Alterations in opioid 73. Gilman S, Frey KA, Koeppe RA, et al. Decreased striatal (Part 4):951–958. 1167. binding in Parkinson’s disease patients with levodopa-induced monoaminergic terminals in olivopontocerebellar atrophy and 92.dyskinesias. Gerhard A,Ann Banati RB,1997;42:720–726. Goerres GB, et al. [11C](R)-PK11195 75.multiple Kim YJ,system Ichise M, Ballinger JR, et al. Combination dopamine Neurol atrophy demonstrated with positronof emission 88. 89. 90. 91. 92. 93. 94. pamin son’s Mol Im Plotkin CIT an syndro 677–6 Shinot tors in positro chiatry Piccin bindin dyskin Burn D DJ. S striato syndro (Part 4 Gerhar PET i phy. N Gerhar microg Parkin Takats kinson cardiac JAMA en CD, e dopaopontoy. Ann striatal phy and mission SPECT r palsy, 5:1158– opamine aluation ODAT-1 004;45: analysis riant of disease. 677–692. kinson’s disease and multiple system atrophy in early disease 89. Shinotoh H, Inoue O, Hirayama K, et al. Dopamine D1 recepstages by means of I-123-MIBG-SPECT. J Neurol Sci 2000;175: tors in Parkinson’s disease and striatonigral degeneration: a 3–12. positron emission tomography study. J Neurol Neurosurg Psy97. Courbon F, Brefel-Courbon C, Thalamas C, et al. Cardiac D.J. for Brooks and K.cardiac Seppi chiatry 1993;56:467–472. MIBG scintigraphy is a sensitive tool detecting 90. Piccini P, Weeks RA, Brooks DJ. Alterations in opioid receptor sympathetic denervation in Parkinson’s disease. Mov Disord 2003; binding in Parkinson’s disease patients with levodopa-induced 18:890–897. dyskinesias. Ann Neurol 1997;42:720–726. 98. Satoh A, Serita T, Seto M, et al. Loss of 123I-MIBG uptake by 91. Burn DJ, Rinne JO, Quinn NP, Lees AJ, Marsden CD, Brooks the heart in Parkinson’s disease: assessment of cardiac sympaDJ. Striatal opioid receptor binding in Parkinson’s disease, thetic denervation and diagnostic value. J Nucl Med 1999;40: striatonigral degeneration and Steele-Richardson-Olszewski 371–375. syndrome, A [11C]diprenorphine PET study. Brain 1995;118 99. Braune S, Reinhardt M, Schnitzer R, Riedel A, Lucking CH. 964(Part 4):951–958. D.J. BROOKS AND K.Cardiac SEPPIuptake of [123I]MIBG separates Parkinson’s disease 92. Gerhard A, Banati RB, Goerres GB, et al. [11C](R)-PK11195 from multiple system atrophy. Neurology 1999;53:1020– PET imaging of microglial activation in multiple system atro1025. phy. Neurology 95. Reinhardt MJ,2003;61:686–689. Jungling FD, Krause TM, Braune S. Scinti100. Yoshita M. Differentiation of idiopathic Parkinson’s disease 93. Gerhard Pavese N, Hotton et forms al. In of vivo imaging of graphicA,differentiation betweenG,two primary dysautofrom striatonigral degeneration and progressive supranuclear nomia early after onset of autonomic dysfunction: of carpalsy using iodine-123 meta-iodobenzylguanidine myocardial microglial activation with [11C](R)-PK11195 PET in value idiopathic diac and pulmonary iodine-123 uptake. Eur J Nucl Med scintigraphy. J Neurol Sci 1998;155:60–67. Parkinson’s disease. Neurobiol Dis MIBG 2006;21:404–412. 2000;27:595–600. 101. Hirayama M, Hakusui S, Koike Y, et al. A scintigraphical qual94. Takatsu H, Nagashima K, Murase M, et al. Differentiating Par96496. D.J. BROOKS kinson’s disease fromMJ,multiple-system atrophy by measuring Druschky A, Hilz Platsch G, et al. Differentiation of Par- AND K. SEPPI itative analysis of peripheral vascular sympathetic function cardiac iodine-123 kinson’s disease andmetaiodobenzylguanidine multiple system atrophy accumulation. in early disease with meta-[123I]iodobenzylguanidine in neurological patients JAMA stages2000;284:44–45. by means of I-123-MIBG-SPECT. J Neurol Sci 2000;175: with autonomic failure. J Auton Nerv Syst 1995;53: 230–234. 3–12. MJ, Jungling FD, Krause TM, Braune S. Scinti95. Reinhardt 102. Berding Brucke T, Odin P, et al. Parkinson’s [[123I]b-CITdisease SPECT 100. Yoshita M.G,Differentiation of idiopathic 97. Courbon F, Brefel-Courbon C, Thalamas C, et al. Cardiac graphic differentiation between two forms of primary dysautoimaging of dopamine and serotonin transporters supranuclear in Parkinson’s from striatonigral degeneration and progressive MIBG scintigraphy sensitive dysfunction: tool for detecting nomia early after onset is of aautonomic value of cardiac cardisease andiodine-123 multiple system atrophy. Nuklearmedizin 2003;42: palsy using meta-iodobenzylguanidine myocardial sympathetic denervation in Parkinson’s disease.Eur Mov DisordMed 2003; diac and pulmonary iodine-123 MIBG uptake. J Nucl 31–38. scintigraphy. J Neurol Sci 1998;155:60–67. Movement Disorders, Vol. 24, No. 7, 2009 2000;27:595–600. 101. Hirayama M, Hakusui Koike Y, et qual- of 18:890–897. 103. Raffel DM, KoeppeS,RA, Little R al. et A al.scintigraphical PET measurement Satoh A,A,Serita Seto M, etG, al.etLoss of 123I-MIBG uptake 96.98. Druschky Hilz T, MJ, Platsch al. Differentiation of Par- by cardiac and nigrostriatal in Parkinsonian synitative analysis of peripheraldenervation vascular sympathetic function the heart in Parkinson’s disease: assessment of early cardiac sympakinson’s disease and multiple system atrophy in disease dromes. J Nucl Med. 2006;47:1769–1777. with meta-[123I]iodobenzylguanidine in neurological patients thetic and diagnostic value. J NuclSciMed 1999;40: stages bydenervation means of I-123-MIBG-SPECT. J Neurol 2000;175: 104. Goldstein DS,failure. HolmesJ C, Cannon Eisenhofer G, Kopin with autonomic Auton NervRO, SystIII, 1995;53: 230–234. 371–375. 3–12. IJ. Sympathetic N Engl J 102. Berding G, Bruckecardioneuropathy T, Odin P, et in al.dysautonomias. [[123I]b-CIT SPECT Braune F, S, Brefel-Courbon Reinhardt M, Schnitzer R, Riedel Lucking CH. 97.99. Courbon C, Thalamas C, etA, al. Cardiac Med 1997;336:696–702. imaging of dopamine and serotonin transporters in Parkinson’s MIBG scintigraphy a sensitive separates tool for Parkinson’s detecting cardiac disease and multiple system atrophy. Nuklearmedizin 2003;42: Cardiac uptake of is[123I]MIBG disease 105. Goldstein DS, Holmes C, Li ST, Bruce S, Metman LV, Cannon sympathetic denervation in Parkinson’s Mov 1999;53:1020– Disord 2003; 31–38. from multiple system atrophy. disease. Neurology RO, III. Cardiac sympathetic denervation in Parkinson’s dis1025. 18:890–897. ease.DM, Ann Koeppe Intern Med 103. Raffel RA,2000;133:338–347. Little R et al. PET measurement of 98. Satoh A, Serita T, Seto M, et al. Loss of 123I-MIBG uptake by cardiac and nigrostriatal denervation in Parkinsonian synthe heart in Parkinson’s disease: assessment of cardiac sympadromes. J Nucl Med. 2006;47:1769–1777. thetic denervation and diagnostic value. J Nucl Med 1999;40: 104. Goldstein DS, Holmes C, Cannon RO, III, Eisenhofer G, Kopin 日本語版略語一覧 371–375. IJ. Sympathetic cardioneuropathy in dysautonomias. N Engl J 99. Braune S, Reinhardt M, Schnitzer R, Riedel A, Lucking CH. Med 1997;336:696–702. Cardiac uptake of [123I]MIBG separates Parkinson’s disease 105. Goldstein DS, Holmes C, Li ST, Bruce S, Metman LV, Cannon 略語 英語(Full Spelling) 和訳 from multiple system atrophy. Neurology 1999;53:1020– RO, III. Cardiac sympathetic denervation in Parkinson’s dis1025. ease. Ann Intern Med 2000;133:338–347. SND striatonigral degeneration 線条体黒質変性症 sporadic olivopontocerebellar atrophy 孤発性オリーブ橋小脳萎縮症 CSE conventional spin-echo 従来型スピンエコー MRV MRI volumetry 1.5T MRI 容積測定 ADC apparent diffusion coefficient 拡散係数 MCP middle cerebellar peduncle 中小脳脚 SCP superior cerebellar peduncle 上小脳脚 MTI magnetization transfer imaging 磁化移動画像 MR Parkinsonism index MR パーキンソニズム指標 fractional anisotropy 異方性比率 transcranial sonography 経頭蓋超音波 LN lentiform nucleus レンズ核 PAF pure autonomic failure CBD corticobasal degeneration sOPCA MRPI FA TCS rCMRglc regional cerebral glucose metabolism 103. 104. 105. Movement Disorders, Vol. 24, No. 7, 2009 純粋自律神経失調症 大脳皮質基底核変性症 前頭皮質の局所脳糖代謝 SPM statistical parametric map 統計的パラメトリックマップ PDRP PD-related pattern PD 関連パターン PMRS proton magnetic resonance spectroscopy プロトン MR スペクトロスコピー DTBZ dihydrotetrabenazine ジヒドロテトラベナジン caudate-putamen index 尾状核 - 被殻指標 CPI 102. 25 Movement Disorders, Vol. 24, No. 7, 2009 with with Berdi imag disea 31–38 Raffe cardi drom Golds IJ. Sy Med Golds RO, ease. 初期パーキンソン病患者に対する 6-[18F]Fluoro-L-dopa 取り込みの追跡調査で示された被殻における非直線性の 進行パターン A Follow-Up Study on 6-[18F]Fluoro-L-dopa Uptake in Early Parkinson’s Disease Shows Nonlinear Progression in the Putamen * Anna Brück, MD, PhD, Sargo Aalto, MSc, Elina Rauhala, MD, PhD, Jörgen Bergman, PhD, Reijo Marttila, MD, PhD, and Juha O. Rinne, MD, PhD * Turku PET Centre, University of Turku, Turku, Finland パーキンソン病(Parkinson’ s disease; PD)を新たに 年間低下量(平均値)は,最初の 2 年間は 0.5,その 発症した患者 16 例を対象に, 5 年間(平均 ± 標準偏差: 後の 3 年間は 0.2 であった(p = 0.002) 。尾状核にお 5.5 ± 0.4 年)の追跡期間中に 6-[ F]fluoro-L-dopa ける Fdopa 取り込みの減少速度は被殻よりも緩徐で, (Fdopa)PET スキャン検査を 3 回行い,線条体におけ 追跡期間中は有意な変化はなく,対側尾状核における年 るドパミン機能低下の進行を検討した。試験期間を通じ 間低下量はベースライン時から 2 年目までが 0.1,2 ~ て Fdopa 取り込みが最も少なかった領域は,運動障害 5 年目が 0.3 であった(p = 0.4) 。以上の結果から, 優位側とは対側の被殻背尾部であった。この対側被殻 PD 患者における被殻のドパミン機能低下は,少なくと における Fdopa 取り込みの低下速度は PD の初期ほど も対側では非直線性の進行パターンを示し,PD の初期 急速で,疾患の進行に伴い緩徐になった。対側被殻に ほど進行が急速であることが示唆される。 18 おける Fdopa 流入定数(Ki,unit × 10 −3 min )の −1 Movement Disorders Vol. 24, No. 7, 2009, pp. 1009–1015 Key Word パーキンソン病,PET,6-[18F]fluoro-L-dopa,進行 BL: Contralateral Ipsilateral Dorsal Caudate Dorsal 82 88 Ventral Rostral 51 33 Caudate 66 46 Putamen Caudal 2 years: Contralateral Ventral 80 36 23 85 61 40 Rostral 78 58 Rostral Putamen Putamen Ventral Caudal 85 52 37 87 71 52 Rostral Putamen Ipsilateral Dorsal 71 35 21 78 51 38 Rostral 26 93 Ventral Caudate Dorsal Ventral 50 Caudal Dorsal 5 years: Contralateral Caudate 65 Ipsilateral Dorsal Caudate 89 Putamen Caudate Ventral Caudal 85 40 25 85 59 35 Rostral Putamen Caudal Figure 1 ベースライン時(BL) , 2 年後,5 年後の PET スキャンに よる PD 患者群の各線条体領域 (運動障害優位側の対側および同 側)の Fdopa 取り込み割合(対 照群の平均値に対する割合)を Caudal 示す略図 Abstract STRIATAL Fdopa UPTAKE IN PARKINSON’S DISEASE 1013 Table 1 PD 患者群〔ベースライン時(BL) ,2 年後,5 年後〕と対照群(BL,5 年後)の Fdopa 流入定数 TABLE 1. The mean Fdopa 6 standard deviations of (Ki 3 1023 min21) in PD patients (baseline (BL), 2 years - 3influx-constants 1 min )の平均 ± 標準偏差 (Ki × 10 after BL and 5 years after BL) and controls (BL and 5 years after BL) BL Caudate Dorsal Contralateral Ipsilateral Ventral Contralateral Ipsilateral Rostral putamen Dorsal Contralateral Ipsilateral Ventral Contralateral Ipsilateral Caudal Putamen Dorsal Contralateral Ipsilateral Ventral Contralateral Ipsilateral Whole putamen Contralateral Ipsilateral * a 2 yr (2.1 yr 6 0.1) 5 yr (5.5 yr 6 0.3) (4.8 yr 6 0.6) Annual change Ki (BL-2 yr) Annual change Ki (2 yr–5 yr) PD NC* PD PD NC* PD PD Mean 6 SD Mean 6 SD Mean 6 SD Mean 6 SD Mean 6 SD Mean 6 SD Mean 6 SD P annual 9.2 6 1.5 10.0 6 1.9 11.2 6 1.5 9.0 6 2.0 9.5 6 2.2 8.0 6 2.2 9.5 6 2.7 11.2 6 0.9 0.1 6 0.6 0.3 6 0.4a 0.3 6 0.6 0.1 6 0.5 0.47 0.36 10.0 6 1.5 10.5 6 2.1 11.3 6 1.3 9.6 6 1.5 9.8 6 1.7 8.7 6 1.4 9.5 6 2.1 11.2 6 1.2 0.2 6 0.5 0.3 6 0.5a 0.3 6 0.4a 0.1 6 0.5 0.58 0.36 5.4 6 1.6 6.9 6 1.9 10.6 6 2.3 4.0 6 2.0 5.8 6 2.3 4.0 6 1.8 4.6 6 2.4 11.4 6 1.6 0.7 6 0.7a 0.6 6 0.5a 0.01 6 0.6 0.4 6 0.5a 0.038 0.21 8.0 6 1.5 9.4 6 1.9 12.1 6 1.5 7.2 6 1.5 8.4 6 1.7 5.9 6 1.5 6.9 6 1.9 11.6 6 11.1 0.4 6 0.4a 0.5 6 0.5a 0.4 6 0.3a 0.4 6 0.4a 0.77 0.70 3.5 6 1.4 5.4 6 2.3 10.5 6 2.0 2.5 6 1.0 4.1 6 2.0 2.3 6 1.1 2.8 6 1.8 11.2 6 1.8 0.5 6 0.3a 0.6 6 0.4a 0.1 6 0.4 0.4 6 0.5a 0.003 0.085 4.9 6 1.3 6.2 6 1.9 10.7 6 2.6 4.0 6 1.1 5.3 6 1.6 3.6 6 1.1 4.0 6 1.5 9.5 6 1.9 0.4 6 0.5a 0.4 6 0.5a 0.1 6 0.3 0.4 6 0.5a 0.019 0.92 5.7 6 1.3 7.2 6 1.8 11.2 6 1.0 4.7 6 1.2 6.1 6 1.7 4.1 6 0.9 4.9 6 1.5 10.9 6 1.0 0.5 6 0.2a 0.5 6 0.3a 0.2 6 0.2a 0.4 6 0.3a 0.002 0.075 *Average of left and right Ki; 左右の Ki の平均 a Change was statistically significant, P < 0.05, Annual changes are shown only for PD subjects. 統計学的に有意な変化(p < 0.05) 。年間変化量は PD 患者のみを示す。 expands this finding by showing a similar pattern of regional dopaminergic hypofunction after a follow-up time of 5 years. Reduced Fdopa uptake is found throughout the striatum but the lowest levels are seen in the dorso-caudal putamen even 6 years after symptom onset. According to post mortem data, the rate of nigral neuronal loss is faster in the beginning of PD. The nigral cell counts decrease with a rate of 45% during the first decade which is 10 times greater than the degeneration in normal aging. It has been estimated that as the disease progresses the nigral cell loss approaches the normal age-related linear decline.2 A PET study reported that recent-onset PD patients showed greater annual decline in Fdopa uptake than more advanced PD patients but the difference failed to reach statistical significance due to wide confidence interval in the rate of progression.11 In a more recent study, 31 PD subjects with various disease durations were scanned with FIG. 2. 95% confidence intervals for PD patients’ annual change in influx constant values (Ki min21) between baseline (BL) and 2 year scans and between 2 year and 5 year scans in caudate and putamen 27 パーキンソン病患者の QOL に対する淡蒼球または視床下部深 部脳刺激の長期効果 Long-Term Effects of Pallidal or Subthalamic Deep Brain Stimulation on Quality of Life in Parkinson’s Disease * Jens Volkmann, MD, Alberto Albanese, MD, Jaime Kulisevsky, MD, Aana-Lena Tornqvist, PhD, Jean-Luc Houeto, MD, Bernard Pidoux, MD, Anne-Marie Bonnet, MD, Alexandre Mendes, MD, Alim-Louis Benabid, MD, Valerie Fraix, PhD, Nadege Van Blercom, PhD, Jing Xie, MD, José Obeso, MD, Maria Cruz Rodriguez-Oroz, MD, Jurge Guridi, MD, Alfons Schnitzler, MD, Lars Timmermann, MD, Alexandre A. Gironell, MD, Juan Molet, MD, Benta Pascual-Sedano, MD, Stig Rehncrona, MD, Elena Moro, MD, Anthony C. Lang, MD, Andres M. Lozano, MD, Anna Rita Bentivoglio, MD, Massimo Scerrati, MD, Maria Fiorella Contarino, MD, Luigi Romito, MD, Marc Janssens, PhD, and Yves Agid, MD * Neurologische Klinik der Christian-Albrechts-Universität, Kiel, Germany 既報の多施設共同臨床試験に参加した進行期パーキン interaction; SI) ,仕事(work; W) 〕のスコアで構成さ ソン病患者を対象に,健康関連 QOL(health-related れている。運動機能の測定には Unified Parkinson’ s quality of life; HrQoL)に対する視床下核深部脳刺激 Disease Rating Scale と日誌を用いた。手術から 6 ヵ (deep brain stimulation of the subthalamic nucleus; 月後には,両群とも「off 時」の運動症状および日常生 STN-DBS)および淡蒼球内節深部脳刺激(deep brain 活動作が有意に改善するとともに,SIP の合計スコア, stimulation of the internal pallidum; GPi-DBS)の効果 身体的領域スコア,心理社会的領域スコアが有意に低下 を評価した。GPi-DBS 施行患者 20 例中 20 例,STN- した。手術から 36 ヵ月後には,STN-DBS 群では身体 DBS 施行患者 49 例中 45 例のサブグループにおいて, 的領域スコア,BCM,E,M,RP に持続的な改善を認め, ベ ースライン 時,6 ヵ月後,36 ヵ月後 に Sickness GPi-DBS 群では M,SI が持続的に改善した。これら以 Impact Profile(SIP)質問票のデータを入手し,分析し 外の SIP のサブスコアはいずれもベースライン値に近 た。SIP は,身体的領域および心理社会的領域の合計ス づいたが,ベースライン値に比べると同等または改善さ コアと,12 のカテゴリー〔注意・集中行動(alertness/ れていた(C を除く) 。一方,運動機能は 36 ヵ月後も intellectual behavior; AIB) ,歩行(ambulation; A) ,整 安定していた。STN-DBS および GPi-DBS により,術 容・動作(body care and movement; BCM) ,コミュ 後早期に HrQoL は有意に改善した。運動機能には持続 ニケーション(communication; C) ,食事(eating; E) , 的な改善が認められたが,初期の効果の多くは 36 ヵ月 情動的行動(emotional behavior; EB) ,家事(home 後にはみられなくなった。この所見は,パーキンソン病 management; HM) , 移動(mobility; M) , レクリエーショ の進行,または良好な健康状態に対する患者の主観的 ン・娯楽(recreation and pastimes; RP) ,睡眠・休息 な捉え方の経時的適応変化によると考えられる。 (sleep and rest; SR) , 社 会 と の 関 わ り(social Movement Disorders Vol. 24, No. 8, 2009, pp. 1154–1161 Key Word QOL,パーキンソン病 / パーキンソニズム,深部脳刺激,視床下核,淡蒼球 28 QUALITY OF LIFE IN PD AFTER DBS 1155 Abstract ned stable after 36 months. STN-DBS and significant early improvements in HrQoL. motor improvements many of these initial after 3 years. This may reflect either prosease or adaptive changes in the subjective perception of health-related wellbeing over time. � 2009 Movement Disorder Society Key words: quality of life; Parkinson’s disease/parkinsonism; deep brain stimulation; subthalamic nucleus; globus pallidus GPi 45 baseline 40 METHODS Patients and Methods who suffered from advanced PD, had n with bilateral DBS in either the GPi ween January 1996 and July 1998, and 30 ns ns 6 months 36 months were followed for 3 to 4 years in a** multicentre proto25 7 ** The aim col.20 ** of the present study was to assess the impact of bilateral DBS on HrQoL in a large group of 15 patients followed for a minimum of 3 years. The par10 ent 5trial, which was designed to blindly assess the effect 0 of neurostimulation at 3 months postoperatively, SIP physical SIP psych SIP had beentotal conducted at 18 centres and included 143 6 patients. A subgroup of patients was included in the STN long-term assessment as outlined elsewhere.7 We con45 fined 40 this supplementary quality of life analysis to the same 35 69 patients reported in the recently published ns * these patients, SIP queslong-term efficacy study.7 Of 30 * 25 tionnaires were available for analysis in a subgroup of ** ** 20 20/20** patients with GPi-DBS and n 5 45/49 n 5 15 patients with STN-DBS at baseline, 6 and 36 months. The10characteristics of the patients are summarized in 5 Table 1. The institutional review board of each partici0 pating centre approved theSIPfollow-up protocol and all total SIP physical psych SIP patients gave written informed consent. The details of Figure 1 ベースライン時と手術から 6 ヵ月後および ヵ月後とを比較し patient selection, surgical procedure, and 36 outcome at 3 た,SIP to 6の合計スコア,身体的領域スコア,心理社会的領域スコアの変化。 months and at 3 to 4 years have been published.6,7 棒グラフは群平均,その上のエラーバーは平均値の標準誤差を示す。 The surgical target (either STN or GPi) was not **p < 0.01, *p < 0.05, =ベースライン値と比較して有意差なし(Wilcoxon randomized butns was left to the discretion of each team の順位和検定,両側) according to their experience and clinical appreciation.6,7 SIP score m medical management of Parkinson’s n complicated by levodopa-induced ns and dyskinesias. Deep brain stimulae internal globus pallidus (GPi) or subs (STN) are effective surgical treatced PD improving all cardinal motor treatment-related motor complicae DBS is a non-curative therapy for a gressive neurodegenerative disorder, it prove, that these symptomatic benefits adverse effects of the procedure and mpact on disability and quality of life. of health-related quality of life (HrQoL) o evaluate the multidimensional, physial, and social aspects of wellbeing in a ements of HrQoL are now widely used ompare the global impact of medical mpairment, disability, and handicap. n PD patients is influenced by several motor aspects of the disease, such as y, depression, sleep problems, pain, ns, and age.4,5 Progression of PD is a decline in quality of life, but the al course and the contributing factors ablished. Although HrQoL assessments ded in a number of clinical trials for ase, little is known about the long-term ents on HrQoL. e multicentre study on DBS in STN or sed on the symptomatic effects of surmonth follow-up6 and in a subset of 4 years,7,8 included the sickness impact widely used generic measure of quality of the present report is to analyze this ssment of HrQoL and to discuss facthe outcome in this group of patients. SIP score 35 ns Outcome Measures In addition to the outcome criteria described in the companion publications,6,7 HrQoL was assessed by the SIP, a 136-item generic measure of HrQoL in 12 cateTable 1 被験者の人口学的データ TABLE 1. Demographical data of the study population Sex* Mean age at implant (y)* Mean duration of follow-up (y)* Mean duration of disease since onset* Mean duration of disease since definite diagnosis* STN-group (n 5 45) GPi-group (n 5 20) 22F/23M 58.5 (9.8) 3.8 (0.6) 15.3 (6.3) 7F/13M 55.8 (9.4) 3.9 (0.7) 15.4 (6.2) 13.9 (6.0) 14.4 (5.7) Values in parentheses are SD. 括弧内の数値は標準偏差 *Fishers Exact-test or Mann-Whitney U-test (two-sided) were used ベースライン時における STN-DBS 群と GPi-DBS 群との比較に to *compare the STN and GPi-group at baseline. No statistical difference between groups was found for these variables. U 検定(両側)を用いた。 は Fisher の直接法または Mann-Whitney 各値について,統計学的に有意な群間差は認められなかった。 Movement Disorders, Vol. 24, No. 8, 2009 29 パーキンソン病患者にみられる体重減少と 1 日のエネルギー 消費量および身体活動量との関連性 Daily Energy Expenditure, Physical Activity, and Weight Loss in Parkinson’s Disease Patients * Evangelia Delikanaki-Skaribas, PhD, Marilyn Trail, MOT, William Wai-Lun Wong, PhD, and Eugene C. Lai, MD, PhD D WL IN PARKINSON’S DISEASE 669 * Parkinson’s Disease Research, Education and Clinical Center, Department of Neurology, Michael E. DeBakey VA Medical Center, Houston, Texas, USA n Total 20 .9 6 7.9 .9 6 16.5 .4 .4 .8 .4 .2 6 6 6 6 6 11.7 9.5 6.9 6.3 7.9 laborater, and s of the s calcukH) and ows: 3 NH Þ he Weir 3 rO2 Þ 7 3 UN 25 (FQ) N is the nd body obtained nts were . Blandpare the method e. ourse of ht from e motor Rating 30 the two As expected, the WL group had a lower body mass (P 5 0.019) and lower fat mass (P 5 0.013) than the WS group. The WL group had a 20% mean body fat whereas the WS group had 28% (P 5 0.029; Table 1). パーキンソン病(Parkinson’ disease; The WS group was about 11s kg heavierPD)患者では with about 3 kg more body fat than the WL group. 体重減少がよく認められるが,これはエネルギー消費量 There was no difference in DEE, REE and fat-free 増加など様々な要因によるものと考えられている。本研 mass between the WS and WL groups. Energy intake 究では,体重が減少した PD 患者は,体重が安定してい (EI) measured from the 3-day food diary was not difる PDbetween 患 者よりも,1 ferent groups.日のエネル However,ギー消費量(daily when EI was expressed per kg of body weight, the WL patients had energy expenditure; DEE)と,その構成要素である安 a higher EI than the WS patients (P < 0.05; Table 2). 静時エネルギー消費量(resting energy expenditure; Figure 1 shows the comparison of DEE and EI in the twoREE)および身体活動エネルギー消費量(physical groups. The WLenergy groupexpenditure; showed higher PA than the WS activity PAEE)が高いという仮説 group (P < 0.042) only when using activity monitors を立てて検証した。体重が減少した PD 患者 10 名と体 placed at the wrist. The PASE and YALE activity 重が安定している 10 名において,二重標識水 questionnaires failedPDto患者 show any differences other than randomlabeled variations between WS and WL patients (doubly water; DLW)を用いてエネルギー消 (Table 2). 費量(DEE)を測定した。身体活動エネルギー消費量 There was a relationship between DEE as well as (PAEE)は,二重標識水(DLW) ,身体活動モニタ,身 PAEE and caloric intake (r 5 0.548; P < 0.05 and 体活動質問票を用いて評価した。安静時エネルギー消 r 5 0.563; P < 0.01, respectively). Patients with a higher DEE tended to have greater PAEE and caloric 費量(REE)は間接熱量測定法により測定した。エネル intake. Additionally, PAEE measured with DLW was ギー摂取量(energy intake; EI)は患者の 3 日間の食 related to activity measured with activity monitors placed both around the waist (r 5 0.471; P < 0.05) and wrist (r 5 0.471; P < 0.05). There was a relationship between the two different accelerometer placements (r 5 0.901; P < 0.05; Table 3). The average 事 日 記 か ら 評 価 し た。 デ ー タ の 評 価 に は,SPSS, Spearman の相関係数,Bland-Altman プロットを用い た。二重標識水(DLW)で測定したエネルギー消費量 (DEE)には体重減少群と体重安定群との間で差はみら れなかった。安静時エネルギー消費量(REE)とエネル ギー摂取量(EI)にも群間差はみられなかった。エネル ギー消費量(DEE) (r = 0.548,p < 0.05)と身体活 p < 0.01)は, 動エネルギー消費量(PAEE) (r = 0.563, カロリー摂取量と相関した。身体活動量は,手首に取り 付けた活動モニタで測定した場合にのみ,体重減少群 。以上 の方が体重安定群よりも高かった(p < 0.042) の結果から,PD 患者にみられる体重減少は,エネルギー 消費量(DEE)の増加だけでは完全には説明できないこ とが示唆される。大規模な縦断的研究を実施して様々な 変数間の関係を検討することで,PD 患者にみられる体 重減少をより深く理解できると考えられる。 Movement Disorders, Vol. 24, No. 5, 2009, pp. 667–671 Key Word パーキンソン病,体重減少,二重標識水,身体活動質問票,身体活動モニタ TABLE 2. DEE, EI, REE, and PAEE estimated with DLW, Table 2 体重安定群および体重減少群で PAMs, and PAQs in both WS and WL groups DLW,PAM,PAQ により測定した DEE,EI,REE,PAEE Variables N DEE (kcal/d) PAEE—DLW (kcal/d) PAEE waist PAM (act. beats) PAEE wrist PAM (act. beats) PAEE sum PAMs (act. beats) PASE PAQ YALE PAQ (kcal/d) REE (kcal/d) EI (kcal/d) EI (kcal/kg/d) WS WL Total 10 2,206 6 560 582 6 420 10 2,267 6 492 622 6 539 20 2,237 6 510 520.9 6 310 49 6 30 63 6 36 101 6 69 167 6 61 79 6 54 110 6 47 57 6 33 a 140 6 71 97 6 51 122 407 1,501 1,909 10.1 6 6 6 6 6 72 229 209 612 3.1 131 372 1,486 2,253 14.4 6 6 6 6 6 72 217 179 409 2.8a 127 388 1,493 2,082 12.4 6 6 6 6 6 70 217 188 544 3.6 Values are mean 6 SD. P < 0.05. DEE 5 daily energy expenditure; EI 5 energy intake; REE 5 resting energy expenditure; PAEE 5 physical activity energy expenditure; DLW 5 doubly labeled water; PAMs 5 physical activity monitors; PAQs 5 physical activity questionnaires; WS 5 weight a 数値は平均値 ± 標準偏差 p < 0.05 DEE = 1 日のエネルギー消費量,EI =エネルギー摂取量,REE =安静時エネルギー消費量,PAEE =身体活動エネルギー消費量, DLW =二重標識水,PAM =身体活動モニタ,PAQ =身体活動質 問票,WS =体重安定,WL =体重減少 a DAILY ENERGY EXPENDITURE- INTAKE (KCAL) Abstract 2000 1000 0 -1000 1- 10 10 WEIGHT STABLE WEIGHT LOSS Figure 1 Bland-Altman 法による 1 日のエネルギー消費量(DEE) とエネルギー摂取量(EI)の群間比較 800 DIFFERENCE (KCAL) 600 400 200 0 -200 -400 WEIGHT LOSS WEIGHT STABLE -600 0 200 400 600 800 1000 AVERAGE (KCAL) Figure 2 二重標識水(DLW)と YALE 身体活動質問票(PAQ) により測定した身体活動エネルギー消費量(PAEE)の差。両測定 値の平均値に対してプロットしている(Bland-Altman プロット) 。 31 多系統萎縮症患者の拡散強調画像:臨床サブタイプ間の比較 Diffusion-Weighted Imaging in Multiple System Atrophy: A Comparison Between Clinical Subtypes * Maria Teresa Pellecchia, MD, PhD, Paolo Barone, MD, PhD, Carmine Mollica, MD, PhD, Elena Salvatore, MD, PhD, Marta Ianniciello, MD, Katia Longo, MD, Andrea Varrone, MD, PhD, Caterina Vicidomini, PhD, Marina Picillo, MD, Giuseppe De Michele, MD, Alessandro Filla, MD, Marco Salvatore, MD, and Sabina Pappatà, MD * Department of Neurological Sciences, University Federico II, Naples, Italy 多系統萎縮症は臨床症状に応じて 2 つのタイプに大別 者の小脳および MCP における Trace (D) 値の上昇は, される。1 つはパーキンソン型(parkinsonian variant 長期の罹病期間と有意に相関していた。MSA-P 患者に of multiple system atrophy; MSA-P) ,もう1つは小脳 おいて,Unified Multiple System Atrophy Rating 型(cerebellar variant of multiple system atrophy; Scale(UMSARS) お よ び Unified Parkinson’ s MSA-C) である。MSA-P 患者 9 例, MSA-C 患者 12 例, Disease Rating Scale(UPDRS)の運動スコアは,被 対照被験者 11 例を対象に,拡散強調 MRI(diffusion- 殻全体および被殻後部の Trace (D) 値と正の相関を示 weighted magnetic resonance imaging; DWI)を施行 した。拡散係数の変化は,MSA-P 患者と MSA-C 患者 し,DWI の変化と罹病期間および重症度との相関性を との間で認められる臨床症状の差および病理学的な差 検討した。被殻全体および被殻前部の Trace (D) 値は, に対応しており,DWI が MSA における神経変性の in MSA-P 患者の方が MSA-C 患者や対照被験者よりも有 vivo での評価に有用なことが示唆される。今回の結果 意 に 高 か っ た が, 小 脳 お よ び 中 小 脳 脚(middle に基づくと,MSA-P 患者の被殻および橋と,MSA-C cerebellar peduncle; MCP) の Trace (D) 値 は, 患者の小脳および MCP における Trace (D) の測定は, MSA-C 患者の方が MSA-P 患者や対照被験者よりも有 疾患過程でみられる微細構造の損傷の定量的マーカー 意に高かった。MSA-P 患者の橋,ならびに MSA-C 患 になるものと考えられる。 Movement Disorders Vol. 24, No. 5, 2009, pp. 689–696 Key Word MRI,MSA のサブタイプ,拡散強調画像 32 A B C D E F Figure 1 対照被験者 (A, D) , M S A - C 患 者( B ,E ), MSA-P 患者(C,F)の被殻 および小脳レベルで撮影し, 平 均 化 し た Trace (D) 画 像 〔Montreal Neurological Institute(MNI)標準脳〕 。対照 被験者に比べ,MSA-P 患者 の被殻および MSA-C 患者の テ ン ト 下 領 域〔 橋,MCP, 小 脳白質(cerebellar white matter; CWM) 〕では Trace (D) 値が明らかに高い。Trace (D) マ ッ プ は, 最 大 値 1.5 × 10 - 3 mm2/sec(赤色)から最 小値 0.4 × 10 - 3 mm2/sec(青 色 ) で 示 し て い る。2 × 10 - 3 mm2/sec を超える Trace (D) 値は表示していない(黒 色) 。 1.0 CWM Trace (D) 1.0 0.9 0.8 0.7 0.6 MSA-C MSA-P 0.9 0.8 0.7 0.6 Controls 1.1 1.1 1.0 MCP Trace (D) 1.2 1.0 0.9 0.8 0.6 MSA-C MSA-P MSA-P Controls MSA-C MSA-P Controls MSA-C MSA-P Controls 0.9 0.8 0.6 Controls 1.0 0.9 0.8 0.7 0.6 MSA-C 0.7 0.7 Pontine Trace (D) Anterior putaminal Trace (D) Posterior putaminal Trace (D) Entire putaminal Trace (D) Abstract 1.2 1.1 1.0 0.9 0.8 0.7 MSA-C MSA-P Controls 0.6 Figure 2 MSA-C 患者,MSA-P 患者,対照被験者の被殻(全体,前部,後部) ,小脳白質(CWM) ,中小脳脚(MCP) ,橋の 692 Trace (D) 値(× 10 - 3 mm2/sec)を示す散布図。MCP に限り, MSA-C 患者群のすべての Trace (D) 値は対照群の最高値よりも高かっ た。 M.T. PELLECCHIA ET AL. -3 2 Table 1 MSA-P 患者,MSA-C 患者,健常対照被験者の局所 Trace (D) 値(10 ± SD TABLE 1. Mean 6 SD regional trace (D) values (1023 mm2/sec) in MSA-P, MSA-C,mm and /sec)の平均 healthy controls Regions Putamen CWM Pons MCP Caudate Posterior putamen Anterior putamen MSA-P (N 5 9) 0.876 0.726 0.784 0.788 0.734 0.952 0.826 6 6 6 6 6 6 6 a,c 0.073 0.056 0.083 0.075 0.098 0.117a 0.063b,c MSA-C (N 5 12) 0.758 0.857 0.910 0.947 0.767 0.794 0.739 6 6 6 6 6 6 6 0.015 0.064a,d 0.104a 0.074a,d 0.011 0.019 0.016 Controls (N 5 11) 0.738 0.678 0.714 0.717 0.722 0.750 0.738 6 6 6 6 6 6 6 0.050 0.034 0.068 0.025 0.107 0.056 0.057 aa P < 0.001 versus controls. p < 0.001 対照群との比較で P < 0.01 versus controls. p < 0.01 P < 0.05 versus MSA-C. cd p < 0.05 MSA-C 群との比較で P < 0.05 versus MSA-P. d CWM, cerebellar white matter; MCP, middle cerebellar peduncle. MSA-P 群との比較で p < 0.05 CWM =小脳白質,MCP =中小脳脚 b b c対照群との比較で patients and controls. Notably, Trace (D) values in the MCP completely separated MSA-C patients from controls (Fig. 2). The analysis of the worse side Trace (D) values showed the same significant differences. with Trace (D) values in the entire putamen (P 5 0.037 and P 5 0.007, respectively) and in the posterior putamen (P 5 0.023 and P 5 0.002, respectively). When we considered age-corrected values, we con- 33 パーキンソン病患者の死亡率:20 年間の追跡調査研究 Mortality in Parkinson’s Disease: A 20-Year Follow-Up Study * Anja Diem-Zangerl, MD, Klaus Seppi, MD, Gregor K. Wenning, MD, PhD, Eugen Trinka, MD, Gerhard Ransmayr, MD, Wilhelm Oberaigner, PhD, and Werner Poewe, MD * Department of Neurology, Innsbruck Medical University, Austria 1974 ~ 1984 年の間にパーキンソン病(Parkinson’ s (95% CI 0.9 ~ 1.4) への SMR の上昇は有意ではなかっ disease; PD)の症状を発症した連続症例 238 名(受 た。発症時に若年ないし高齢であった患者では SMR の 診順)において,死亡率および患者生存の予測因子を決 有意な上昇が認められた。 Cox の比例ハザード分析では, 定した。すべての患者を,2004 年 12 月 31 日または 低生存率の予測因子となる臨床像は,男性であること, 死亡時まで Movement Disorder Clinic(Department 歩行障害があること,振戦がないこと,症状の非対称性 of Neurology, Innsbruck Medical University)にて定 がみられないことであった。本試験では,罹病期間 10 期的に追跡調査した。2004 年 12 月 31 日の時点で 年までの PD 患者では健常対照群との間に生存率の差は 189 名が死亡していた。標準化死亡比(standardized なく,罹病期間が 10 年を超えると一般集団に比して死 mortality ratio; SMR)は経時的に上昇した。SMR は, 亡率がやや上昇することが明らかになった。専門医を定 5 年目が 0.6〔95%信頼区間(CI)0.4 ~ 1.0〕 ,10 年 期的に受診し,現時点で利用可能なあらゆる治療法を駆 目が 0.9(95% CI 0.7 ~ 1.2) ,15 年目が 1.2(95% 使した場合,PD 患者の平均余命は大幅に短縮されるこ CI 1.0 ~ 1.4) , 20 ~ 30 年目が 1.3 (95% CI 1.1~ 1.5) とはない。ただし,患者が男性で,歩行障害があり,受 であった。男性患者では SMR は1.3 (95% CI 1.1~1.6) 診時に静止時振戦がみられなければ長期生存率は低く まで有意に上昇したが,女性患者で認められた 1.2 なる。 Movement Disorders Vol. 24, No. 6, 2009, pp. 819–825 Key Word パーキンソン病,死亡率,SMR,生存の予測因子 822 A. DIEM-ZANGERL ET AL. Table 4 男女別,発症時年齢別にみた 30 年間の追跡調 TABLE 4. Standardized mortality ratios (SMRs) at 30 years 査における標準化死亡比(SMR) of follow-up by gender and age of disease onset Overall Gender Female Male Age at onset <60 yr ‡60 yr SMR 95% CI 1.3 1.1–1.5 1.2 1.3 0.9–1.4 1.1–1.6 1.8 1.1 1.2–2.4 1.0–1.3 Details on statistical significance are explained in the results. CI, 統計学的有意性に関する詳細は,結果の項に記載している。CI confidence interval. =信頼区間 TABLE 5. の比例ハザード回帰モデルによる人口学的 Prediction of survival in Parkinson’s disease ・ Table 5 Cox (n 5 27), and cancer (n and 5 clinical 23). Infeatures contrastusing to other using demographic 臨床的特徴を用いたパーキンソン病患者の生存予測(ハ Cox’s proportional hazards regression studies pneumonia was uncommon (n 5 7)model as a cause ザード比および (hazard ratios 95%信頼区間) and 95% CI) of death in this cohort. Feature present at symptom onset Hazard ratio (95% CIs) P value Age at onset 1.09 (1.07, 1.11) <0.001 PREDICTORS OF SURVIVAL Gendera Men vs. women 1.82 (1.36, 2.44) <0.001 a Univariate analysis revealed a highly significant Tremor Present vs. of absent (0.35,with 0.69) decreased <0.001 association older age at0.49 onset sura Asymmetry vival (P < 0.001). Therefore, Cox’s proportional hazPresent vs. absent 0.59 (0.39, 0.89) 0.01 ard Gaitmodeling disordera of the demographic data and clinical feaPresent vs. absent 1.48 (1.01, 2.18) 0.05 a 34 MORTALITY IN PARKINSON’S a Adjusted for age at onset. 発症時年齢で補正 tures at disease onset was performed by adjusting for age at onset. After adjusting for age at onset, male gender (P < 0.001), gait disorder (P < 0.05) at onset, absence of classical rest tremor (P < 0.001) at onset, and absence of asymmetry (P < 0.01) at onset predicted with ad larly, S PD enro trial co versus i cantly d years (S Altho trials m a likely observe bility, h seen an ment d level of comorb in varia follow-u influenc that ma is likel Abstract 100 100 80 a 60 40 20 Proportion of patients surviving Proportion of patients surviving male female 0 no Tremor Tremor b 80 60 40 20 0 0 5 10 15 20 25 30 0 5 10 Years 15 25 30 no Asymmetry Asymmetry 80 c 60 40 20 0 Proportions of patients surviving no Gait disorder Gait disorder Proportions of patients surviving 20 Years d 80 60 40 20 0 0 5 10 15 Years 20 25 30 0 5 10 15 20 25 30 Years Figure 2 (a ~ d)パーキンソン病患者の生存率に対する性別〔 (a)実線:女性,点線:男性。発症時年齢で補正〕と,古典的 な静止時振戦〔 (b)実線:振戦あり,点線:振戦なし〕 ,歩行障害〔 (c)実線:歩行障害あり,点線:歩行障害なし〕 ,症状の非 対称性〔 (d)実線:非対称性あり,点線:非対称性なし〕等,発症時臨床像(発症時年齢で補正)の影響を示す Kaplan-Meier プ ロット 35 パーキンソン病患者の嗅上皮生検 Biopsies of Olfactory Epithelium in Patients with Parkinson’s Disease *, ** Martin Witt, MD, Katja Bormann, Volker Gudziol, MD, Kerstin Pehlke, Kathrin Barth, PhD, Amir Minovi, MD, Antje Hähner, MD, Heinz Reichmann, MD, and Thomas Hummel, MD * Department of Anatomy, University of Rostock, 18057 Rostock, Germany Department of Otorhinolaryngology, Interdisciplinary Center for Smell and Taste, University of Dresden Medical School, 01307 Dresden, Germany ** パーキンソン病(Parkinson’ s disease; PD)は複数の 9.5(protein gene product 9.5; PGP 9.5) , β - チュー 神経系が関与する神経変性疾患である。嗅覚機能障害 ブリン(beta-tubulin; BT) ,増殖関連抗原(Ki 67) ,幹 は最も初期の PD 症状の 1 つであると考えられる。し 細胞マーカーのネスチン,サイトケラチン,p75NGFr, かし,PD 患者の嗅覚異常に嗅上皮の変化がどの程度関 α- シヌクレインに対する抗体を用いて免疫組織化学的 与しているのか,また,これらの変化が他の嗅覚減退ま 検査を行った。ほとんどの生検標本で,PGP 9.5 また たは嗅覚脱失患者と異なるのかどうか,依然として不明 は BT 陽性であるが OMP 陰性を示す嗅上皮様の不整な である。本研究では,PD 患者の嗅覚障害は PD に特異 領域,異形成上皮が認められた。PD 患者の嗅上皮と対 的な嗅上皮の損傷によるとの仮説を立て,これを検証し 照との間で,これらの蛋白発現または分布に大きな組織 た。PD と診断された患者 7 例から生検標本を採取した。 化学的な差は認められなかった。逆転写 PCR(reverse PD 患者のうち,6 例は嗅覚減退,1 例は嗅覚脱失であっ transcription PCR; RT-PCR)では,嗅覚機能とは無関 た。非 PD 対照として,嗅覚減退患者 9 例,嗅覚脱失 係に,ほぼ全例で OMP mRNA の発現が確認された。 患者 9 例,嗅覚正常者 7 例の生検標本を用いた。さら 以上のデータから,PD 患者の嗅覚障害は,嗅上皮の損 に 死 体 4 例 の 鼻 粘 膜 も 検 討し た。嗅 覚 標 識 蛋 白 質 傷によるのではなく,PD に特有の中枢神経系異常によ (olfactory marker protein; OMP) ,蛋白質遺伝子産物 るとの見解が支持される。 Movement Disorders Vol. 24, No. 6, 2009, pp. 906–914 Key Word 嗅覚脱失,嗅覚減退,嗅覚,嗅上皮,免疫組織化学,RT-PCR 36 Abstract Figure 2 (A)正常嗅覚者の上鼻甲介(ST)レベルでの鼻(死後)の断面図。 OMP(赤色)とネスチン(茶色)を用いた免疫組織化学染色。長方形で囲んだ部 分の拡大図を(B)に示す。EC =篩骨洞細胞,MT =中鼻甲介付着部,NC =鼻腔。 a と b の矢頭は嗅上皮領域の範囲を示している。ヘマトキシリンによる対比染色。 スケールバー:2 mm(A) ,50 µm(B) 。 〔カラーの図は www.interscience.wiley.com のオンライン版で閲覧可能〕 37 進行期パーキンソン病に対するレボドパの十二指腸内投与: 患者の特徴,適応,有効性,安全性 Patient Profile, Indications, Efficacy and Safety of Duodenal Levodopa Infusion in Advanced Parkinson’s Disease * David Devos, MD, PhD for the French DUODOPA Study Group * Department of Neurology, EA2683 IFR114 IMPRT, CHU Lille, France 少人数のパーキンソン症候群患者を対象としたレボド 幻視,50%に認知症が認められた〔Mini Mental State パ(L—ドパ)の十二指腸内投与試験では,運動合併症 Examination(MMSE) :23 点〕 。患者の 98%では,ア に対する治療効果が報告されている。しかし,L—ドパ ポモルフィン注入や脳神経外科治療が無効または禁忌 十二指腸内投与の対象となる患者の特徴や適応につい のため,L—ドパ十二指腸内投与が運動合併症の最後の てはほとんど知られていない。本研究の目的は,日常診 治療選択肢となっていた。患者の 73%は長期間 L- ド 療において L—ドパ十二指腸内投与の対象となる患者集 パ十二指腸内投与を受けており,このうち 90%を超え 団の臨床的特徴と,L—ドパ十二指腸内投与の適応,有 る患者で motor fluctuation,QOL,自立性の改善が報 効性,忍容性を詳細に調べることである。2003 年から 告された。重度の有害事象はほとんどみられなかったが, L—ドパ十二指腸内投与を受けている患者 102 名のうち, 手技的問題は多かった。L—ドパ十二指腸内投与は,パー 91 名を多施設共同レトロスペクティブ試験に登録した。 キンソン病における運動合併症の最後の治療選択肢と 患者の平均年齢は 72.7 歳, 平均罹病期間は 17 年であっ して有効であると考えられる。今後,手技的改善と早期 た。全例が進行期の患者で,91%に歩行障害,65%に 導入を検討する必要がある。 Movement Disorders Vol. 24, No. 7, 2009, pp. 993–1000 Key Word パーキンソン病,レボドパ関連運動合併症,持続性ドパミン刺激,十二指腸内投与,Duodopa 996 D. DEVOS 1 運動症状からみた L —ドパ十二指腸内投与の有効性 TABLETable 1. Efficacy of duodenal levodopa infusion in terms of motor symptoms Patients (n 5 75) Motor fluctuations Dyskinesia Dystonia Pain Gait disorders (freezing, festination, postural instability) Dysphagia Dysarthria Improvement 96% 94.7% 90.7% 74.7% 61.4% 60% 34.7% (n (n (n (n (n (n (n 5 5 5 5 5 5 5 72) 71) 68) 56) 46) 45) 26) No change 2.7% 4% 8% 24% 37.3% 38.7% 64% (n (n (n (n (n (n (n 5 5 5 5 5 5 5 2) 3) 6) 18) 28) 29) 48) Worsening 1.3% 1.3% 1.3% 1.3% 1.3% 1.3% 1.3% (n (n (n (n (n (n (n 5 5 5 5 5 5 5 1) 1) 1) 1) 1) 1) 1) The percentages and the numbers (n) represent the proportion of the population concerned, as assessed by the neurologist on a three-point scale 該当患者の割合および患者数(n)を示す。最終検査時に神経内科医が 3 段階で評価。 at the last examination. 38 DUODENAL LEVODOPA INFUSION IN PARKINSON’S DISEASE 997 classified according to their relationship with (1) levosion (32%), severe cognitive disorders suggestive of dopa treatment, Table (2) 2 gastrostomy, or (3) technical PD dementia (50%), age ‡ 70 years (80%), morphologQOL,自立性,臨床的全般改善度からみた L —ドパ十二指腸内投与の有効性 TABLE 2. Efficacy of duodenal levodopa infusion in terms of quality of life, autonomy and clinical global improvement aspects. Practical, everyday use was also investigated ical (mainly camptocormia and axial deformations) or Patients (n 5 75) the total daily Great improvement Moderate improvement improvement No change and included infused dose of levodopa surgical Slight contraindications (9.5%) or refusalWorsening (9.5%). and the involvement of a nurse, or41.3% the (n 5 31) Duodenal levodopa first-line Quality of life 48% (n a5 caregiver 36) 4% (n 5 3)infusion was 4% (nthe 5 3) 2.7%therapy (n 5 2) Autonomyfor setting up the device 32% 5 24) 42.7% (n 5 32) 16%the (n 5 12) 5.3% (n fulfilled 5 4) 4%indica(n 5 3) patient in(nthe morning, adminin the 2% of population which the Clinical global 61.3%and (n 5shutting 46) (n 5STN 3) 1.3% (n 5and 1) apomorphine 1.3% (n 5 1) istering extraimprovement doses as required down32% the (n 5 24) tion criteria4%for stimulation device in the evening. Solvay Pharma’s role in the pump concerned, therapy. The percentages and the numbers (n) represent the proportion of the population as assessed by the patient him/herself and his/her 該当する患者の割合と患者数(n)を示す。最終検査時に患者自身とその介護者が 5 段階で評価。 caregiver on arestricted five-point scale at the last examination. study was to the provision of logistic support Continuous duodenal infusion of levodopa was per(production, mailing, and recovery of the case report formed during the daytime in 90% of patients and (leading to discontinuation). the transferred final examination, Duodopa in remaining their natural care forms). All received data At were to the round the treatment clock in the 10%. Theenvironment. mean daily the average ‘‘on levodopa’’ Hoehn Yahr stage was 3.3 The very advanced disease stage of our population was authors for analysis. levodopa-equivalent dose was 1388 6 654 mg (range: reflected by the long duration of motor complications, 61.2, the average ‘‘on levodopa’’ UPDRS motor score 500–3300) and was higher (by 199 6 441 mg) than RESULTS Abstract Pre-screening French patients treated with Duodopa® (2005-2007) n = 102 No information on Duodopa® n = 7 Stop n = 4 Screening n = 91 Follow-up analysis n = 91 Long-term Duodopa® treatment continued n = 66 (73%) ∙ Age: 68 y ± 8 [36-87] ∙ Disease duration: 15 y ± 6 [5-35] ∙ Follow-up: 18 months ± 8.4 [12-48] Unrelated deaths n=8 Duodopa® treatment discontinued n = 17 (18%) ∙ Age: 76 y ± 4 [73-80] ∙ Disease duration: 26 y ± 6 [23-28] ∙ Follow-up: 8 months ± 6 [3-10] ∙ Causes: Cardiac arrest (n = 1) Pneumopathy in bedridden patients (n = 7) ∙ Age: 70 y ± 13 [37-88] ∙ Disease duration: 16 y ± 6 [8-21] ∙ Early stop within 3 weeks in 8 patients: Lack of efficacy in nasojejunal test (n = 5) Dopaminergic psychosis (n = 2) Gastrostomy infection: (n = 1) ∙ Late stop (≥ 3 months) in 9 patients: Lack of efficacy (n = 1) Technical/ease of use problems (n = 7) Bedridden patients (n = 2) percentage of patients 100% 87% 97% 91% 86% 48% Motor fluctuations Symptoms duration 8 years ±5 Dystonia 7.7 years ± 4.3 Dyskinesia Gait disorders with falls : 44% Dysarthria Dysphagia 7.5 years ± 4.6 5.5 years ± 3.8 4 years ±2 2 years ±2 Figure 1 L—ドパ関連運動合併症および体幹徴候(axial sign)をは じめとする運動合併症のプロフィール。患者の割合と,L—ドパ十二 指腸内投与前の症状持続期間を示す。数値は平均値および標準偏差。 39 進行期パーキンソン病患者の運動機能および筋電図でのサイ レントピリオドに対する DBS,前運動野 rTMS,レボドパの 効果 Effects of DBS, Premotor rTMS, and Levodopa on Motor Function and Silent Period in Advanced Parkinson’s Disease * Tobias Bäumer, MD, Ute Hidding, MD, Wolfgang Hamel, MD, Carsten Buhmann, MD, Christian K.E. Moll, MD, Christian Gerloff, MD, Michael Orth, MD, PhD, Hartwig Roman Siebner, MD, and Alexander Münchau, MD * Department of Neurology, University Medical Centre Hamburg-Eppendorf, Hamburg, Germany 進行期パーキンソン病患者(Parkinson’ s disease; MEP)の振幅,皮質運動野刺激で誘発される筋電図の PD)では,視床下核(subthalamic nucleus; STN)の 静 止 期(silent period; SP) を, 経 頭 蓋 磁 気 刺 激 深部脳刺激(deep brain stimulation; DBS)が広く行 (transcranial magnetic stimulation; TMS)を用いて測 われ,きわめて高い治療効果が得られている。一次運動 定した。術前は L—ドパおよび PMd に対する 1 Hz の 野や運動関連領野に対する反復経頭蓋磁気刺激 rTMS の効果を測定し,術後は L—ドパ使用時・非使用時 (repetitive transcranial magnetic stimulation; rTMS) の STN 刺激の効果を測定した。L—ドパは臨床症状を有 も PD の症状を改善し,運動野の興奮性を調節すること 意に改善し,SP 持続時間を延長させた。STN 刺激は臨 が明らかにされている。本研究は進行期 PD 患者群を対 床症状を改善したが, SP 持続時間に変化を誘発しなかっ 象に,STN 刺激の臨床的・神経生理学的効果を,背側 た。一方,PMd に対する 1 Hz の rTMS は臨床的には 前運動野(dorsal premotor cortex; PMd)に対する 1 有効でなかったものの, SP 持続時間を正常化させた。L— Hz の rTMS およびレボドパ(L—ドパ)投与での効果と ドパは,PD 患者にみられる様々なレベルの運動回路網 比較した。PD 患者 10 例を術前および術後とも 2 日間 の異常活動に幅広い効果を示した。STN 刺激および 続けて検討した。Unified Parkinson’ s Disease Rating PMd に対する rTMS では,臨床的改善あるいは SP 正 Scale(UPDRS)の運動スコアを用いて臨床効果を評 常化のいずれか一方しか認められず,運動回路網の異 価した。神経生理学的検査としては,運動閾値,軽度随 常活動を部分的に改善しただけであった。 意収縮時の運動誘発電位(motor-evoked potential; Movement Disorders Vol. 24, No. 5, 2009, pp. 672–676 Key Word パーキンソン,深部脳刺激,rTMS,前運動野,L—ドパ 60 200 180 50 160 40 120 100 30 80 20 60 40 10 day 2 prior to implantation of electrodes day 3 LD + DBS baseline DBS + LD DBS baseline rTMS + LD rTMS baseline LD baseline day 1 LD SP UPDRS 20 40 UPDRS score duration of SP (ms) 140 day 4 after implantation of STN electrodes Figure 1 UPDRS スコアおよび静止期(SP)持続時間に対する両 側視床下核(STN)電極留置刺激, L—ドパ(LD) , 背側前運動野(PMd) rTMS の効果。データは平均 ± SEM。DBS =深部脳刺激 e-mail: [email protected] ISSN 1881-901X INCLUDED IN THIS ISSUE Full Articles パーキンソン病患者にみられる中枢神経系以外の病変 多系統萎縮症の診断を目的とした神経画像の基準案 Abstracts 初期パーキンソン病患者に対する 6-[18F]Fluoro-L-dopa 取り込みの 追跡調査で示された被殻における非直線性の進行パターン 他 7 本収載 日本語版 Vol.3 No.2 November 2009
© Copyright 2026 Paperzz
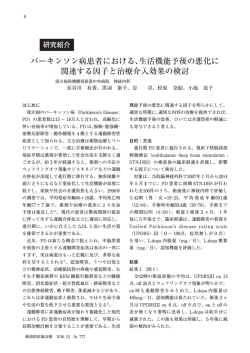

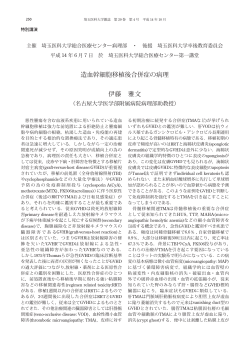
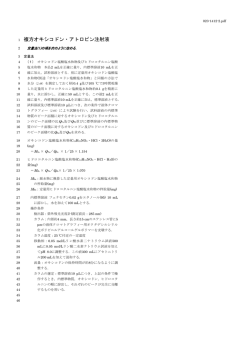
![Microsoft PowerPoint - \217\254\224]\216\270\222\26201302008.ppt](http://s3.paperzz.com/store/data/005626364_1-4cb72c366e12971be31e82be3d00cf94-250x500.png)