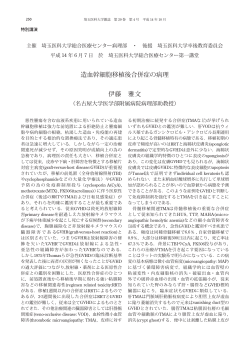
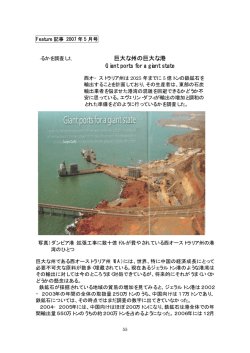
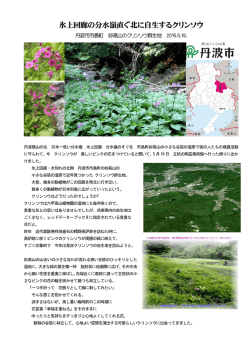
ISSN 1881-901X Highlights from the Official Journal of the Movement Disorder Society 日本語版 Vol.6 No.1 July 2012 INCLUDED IN THIS ISSUE Full Articles 脳内鉄蓄積を伴う神経変性(NBIA) 症候群: 臨床像,組織学的および遺伝学的基礎, 治療に関する最新情報 発行者 ワイリー・パブリッシング・ジャパン株式会社 利き手はパーキンソン病の症状優位側 と相関する: 系統的レビューとメタアナリシス Abstracts 剖検で確認されたパーキンソン病 および多系統萎縮症における ドパミントランスポーター イメージング所見 定価1,470円(本体価格1,400円) 他 11 本収載 Editors-in-Chief International Editorial Board Jose A. Obeso, MD, PhD Department of Neurology University of Navarra Pamplona, Spain E-mail: [email protected] Maren E. Bodden Marburg, Germany Paolo Calabresi Perugia, Italy Richard Camicioli Edmonton, Alberta, Canada Christopher S. Coffey Iowa City, Iowa, USA Ted Dawson Baltimore, Maryland, USA Mark Edwards London, United Kingdom Alfonso Fasano Rome, Italy Susan Fox Toronto, Ontario, Canada Marwan Hariz London, United Kingdom Nobutaka Hattori Tokyo, Japan Robert Hauser Tampa, Florida, USA Christine Klein Luebeck, Germany Paul Krack Grenoble, France Stephane Lehericy Paris, France Andres Lozano Toronto, Ontario, Canada Colum MacKinnon Chicago, Illinois, USA C. Warren Olanow, MD, FRCPC Departments of Neurology and Neuroscience Mount Sinai School of Medicine New York, New York, USA E-mail: [email protected] Associate Editors Erwan Bézard Bordeaux, France Kailash P. Bhatia London, United Kingdom David J. Burn Newcastle, United Kingdom Steven Frucht New York, New York, USA Serge Przedborski New York, New York, USA Andrew D. Siderowf Philadelphia, Pennsylvania, USA Antonio Strafella Toronto, Ontario, Canada Assistant Editors Manuel Alegre Pamplona, Spain Alberto Espay Cincinnati, Ohio, USA CME Editor Kelly Lyons Kansas City, Kansas, USA Editorial Office Julie Nash Managing Editor, Movement Disorders Phone: 919-267-6831; E-mail: [email protected] Pablo Martinez-Martin Madrid, Spain Mike McDermott Rochester, New York, USA Giuseppe Meco Rome, Italy Tetsutaro Ozawa Niigata, Japan Walter Paulus Göttingen, Germany Ron Postuma Montreal, Quebec, Canada Ralf Reilmann Muenster, Germany Maria Rodriguez-Oroz San Sebastian, Spain Webster Ross Honolulu, Hawaii, USA Susanne A. Schneider Luebeck, Germany W.M. Michael Schüpbach Paris, France Andrew Singleton Bethesda, Maryland, USA David G. Standaert Birmingham, Alabama, USA Fabrizio Stocchi Chieti, Italy Josep Valls-Solé Barcelona, Spain Bob van Hilten Leiden, The Netherlands Jens Volkmann Kiel, Germany Daniel Weintraub Philadelphia, Pennsylvania, USA Wiley Publishing Japan K.K. 2012 Wiley Publishing Japan K.K. 2012 2012 Wiley Publishing Japan K.K. e-mail: [email protected] Corporate Sales Associate Director:Kimiyoshi Ishibashi 日本語版 Vol.6 No.1 July 2012 監修: 水野 美邦 北里大学東病院 神経再生医療学講座客員教授 編集委員: 宇川 義一 (五十音順) 福島県立医科大学医学部 髙橋 良輔 京都大学医学研究科臨床神経学教授 神経内科学講座教授 野元 正弘 愛媛大学医学部附属病院 薬物療法・神経内科教授 梶 龍兒 徳島大学医学部神経内科教授 近藤 智善 医療法人社団友志会 服部 信孝 順天堂大学医学部神経学講座教授 リハビリテーション花の舎病院神経内科 山本 光利 高松神経内科クリニック Full Articles 脳内鉄蓄積を伴う神経変性(NBIA)症候群: 臨床像,組織学的および遺伝学的基礎,治療に関する最新情報 2 利き手はパーキンソン病の症状優位側と相関する:系統的レビューとメタアナリシス 15 Abstracts 剖検で確認されたパーキンソン病および多系統萎縮症に おけるドパミントランスポーターイメージング所見 レボドパ誘発性ジスキネジアを伴うパーキンソン病に おける運動課題遂行中の前頭前野fMRI所見の変化 パーキンソン病および進行性核上性麻痺における 脳内鉄蓄積のフィンガープリント パーキンソン病に伴う抑うつにおける セロトニン作動性1A受容体障害の役割 常同症(stereotypy): 批判的評価と臨床的に有用な定義の提案 パーキンソン病における軽度認知障害の診断基準: Movement Disorder Society 作業部会の ガイドライン 32 22 剖検で確認されたLewy小体型認知症における REM睡眠行動障害とサブタイプ 34 24 Parkinson At-Risk Syndrome Studyにおける 嗅覚障害および他の前駆症状の検討 36 26 パーキンソン病の非運動症状に関する MDS-UPDRS Part Iの妥当性の検証 38 27 グルコセレブロシダーゼ遺伝子変異は パーキンソン病の臨床経過中の認知症リスクを高める 40 20 パーキンソン病におけるピサ症候群: 臨床的特徴・筋電図所見・放射線学的所見 28 非運動症状と運動症状の比較: パーキンソン病患者の健康状態への影響はどの程度か? 30 表紙:パルブアルブミンの免疫反応性。対照被験者の青斑核,本態性振戦患者の青斑 核,対照被験者の橋における所見。対照被験者の橋では特異的な染色がみられ,個々 のニューロン(矢印)および線維(矢印)について選択的な免疫反応性が認められる。 (Shill et al, Movement Disorders, 2012, Vol. 27 No. 1, page 113) Selected from Movement Disorders Vol. 27 No. 1-3, 2011 脳内鉄蓄積を伴う神経変性(NBIA)症候群: 臨床像,組織学的および遺伝学的基礎, 治療に関する最新情報 Syndromes of Neurodegeneration with Brain Iron Accumulation (NBIA): an Update on Clinical Presentations, Histological and Genetic Underpinnings, and Treatment Considerations Susanne A. Schneider, PhD, John Hardy, PhD, and Kailash P. Bhatia, FRCP *, **, *** * Schilling Section of Clinical and Molecular Neurogenetics at the Department of Neurology, University of Lübeck, Lübeck, Germany ** Sobell Department of Motor Neuroscience and Movement Disorders, Institute of Neurology, UCL, Queen Square, London, United Kingdom *** Visting Fellow, Department of Neurology, Imperial College, London, United Kingdom 近年,脳内鉄蓄積を伴う神経変性(neurodegeneration 伝子診断で確定された症例の剖検では,一部の下位病 with brain iron accumulation;NBIA)症候群の理解がか 型(サブフォーム)で Lewy 小体および / または神経原 なり進んできた。パントテン酸キナーゼ関連神経変性症 線維変化(tangle)が認められており,比較的一般的な (pantothenate kinase-associated neurodegeneration; 神 経 変 性 疾 患〔 パ ー キ ン ソ ン 病(Parkinson’ s PKAN,1 型 NBIA) や PLA2G6 関 連 神 経 変 性 症 disease;PD)等〕との共通点を示す所見が観察されて (PLA2G6-associated neurodegeneration;PLAN,2 いる。NBIA の原因遺伝子は関連する経路上に位置して 型 NBIA)といった主要症候群のほかにも,いくつかの おり,これらの理解は発症機構に即した治療を進める上 遺伝的原因が特定されている。以前より幅広い臨床スペ で重要である。本レビューでは,NBIA 症候群の歴史的 クトラムが認知されるようになり,年齢依存的な臨床像 な経緯,臨床像,研究の知見,治療成績に加え,遺伝学 も確認されている。また,異なる NBIA 疾患間および他 的および分子的基礎についても概説する。 の疾患との共通点(overlap)も認められつつある。遺 Movement Disorders, Vol. 27, No. 1, 2012, pp. 42–53 Key Word NBIA,PKAN,PLA2G6,鉄 近年の神経遺伝学の進歩により,ある 1 遺伝子の変化 ルフォルデン・スパッツ病と呼ばれた)と PLA2G6 関連 に関連する疾患が,当初の予測よりもはるかに広範囲の 神 経 変 性 症(PLA2G6-associated neurodegeneration; 臨床像(表現型)を呈することが明らかになってきた。 PLAN)がある。しかし,革新的かつ効果的な技術〔同 その一例が脳内鉄蓄積を伴う神経変性(neurodegeneration 祖接合性(autozygosity)マッピングなど〕が開発され, with brain iron accumulation;NBIA)症 候 群 である。 近年, NBIA の他の原因遺伝子も同定されている (Table 1) 。 NBIA 症候群では,進行性錐体外路症状と脳内(特に大 本分野の著しい進歩を受け,我々は今回のレビューを 脳基底核,主に淡蒼球)の過剰な鉄沈着が認められる。 実施した。本稿の目的は,NBIA 症候群の歴史的な経緯, 2 つの主要症候群として神経軸索ジストロフィー,すな 臨床像,研究の知見,治療成績に加え,遺伝学的および わち, パントテン酸キナーゼ関連神経変性症(pantothenate 分子的基礎についても概説することである。特に,これ kinase-associated neurodegeneration;PKAN,以前はハレ らの複雑な疾患群でみられる幅広い臨床スペクトラムに 2 MDs6-1.indb 2 12.7.17 4:36:22 PM Schneider et al. U P D A T E O N N B I A S Y N D R O M E S Table1.1 NBIA の各病型と遺伝子(既知の場合)の概要 TABLE Overview of NBIA conditions and genes (if known) Condition (acronym) PKAN PLAN Kufor–Rakeb disease FAHN Aceruloplasminemia Neuroferritinopathy SENDA syndrome MPAN–NBIA subform identified in a Polish cohorta Idiopathic late-onset cases Synonym Gene Chromosomal position NBIA1 NBIA2, PARK14 NBIA3, PARK9 SPG35 — — — — — PANK2 PLA2G6 ATP13A2 FA2H CP FTL nk (Not yet published) Probably heterogeneous 20p13 22q12 1p36 16q23 3q23 19q13 nk (Not yet published) Probably heterogeneous =セルロプラスミン,FA2H =脂肪酸 2 ヒドロキシラーゼ,FTL =フェリチン軽鎖,MPAN = MIN 関連神経変性症,NBIA =脳内鉄蓄 CP,CP ceruloplasmin; FA2H, fatty acid 2-hydroxylase; FTL, ferritin light chain; MPAN, MIN-associated neurodegeneration; NBIA, neurodegeneration with brain iron accumulation; PANK2 pantothenate kinase 2; PKAN, pantothenate kinase–associated neurodegeneration; PLA2G6, phospholipase A2; PLAN, PLA2G2積を伴う神経変性,PANK2 =パントテン酸キナーゼ 2,PKAN =パントテン酸キナーゼ関連神経変性症,PLA2G6 =ホスホリパーゼ A2, associated neurodegeneration; SENDA, static encephalopathy of childhood with neurodegeneration in adulthood; SPG, spastic paraplegia; nk, not known. a PLAN = PLA2G2 関連神経変性症,SENDA =成人期神経変性を伴う小児期非進行性脳症,SPG =痙性対麻痺,nk =不明 reported by Hartig et al. a Hartig らが報告。 焦点を当てる。ある 1 つの疾患の臨床像は軽症~重症と Historical Review いう範囲に及ぶだけでなく,多くの場合,異なる NBIA 疾患間および他の疾患との共通点(overlap)も認められ Excessive iron is the core feature of NBIA disorders. Perls’ staining forms blue precipitates with iron, るため,臨床症状のみを根拠とする診断は困難である。 known as ferric ferrocyanide or Prussian blue.1 Brain 関連代謝経路が相互に絡み合っていることが,その一因 iron research began in the late 19th century with quantitative analysis of 1 human brain by Zaleski である可能性がある。 (1886).2,3 He correlated iron levels with observations on stained slices and microscopic sections. The first systematic studies of iron in the human brain were 歴史的な経緯 undertaken in the 1920s by Hugo Spatz (1888–1969), who classified brain regions into 4 groups according 4 症候群の中核的な特徴である。ペルル to鉄過剰が staining NBIA intensity. He observed that the globus pallidus and substantia nigra pars reticulata showed the ス染色では鉄により青色沈澱が生じ,これはフェロシア most intense staining, thereby drawing attention to the 1 ン化第二鉄またはプルシアンブルーとして知られる prominent iron concentrations in the nuclei of。脳 the 5 Around the same time, extrapyramidal motor system. 内鉄の研究は,19 世紀後半に Zaleski(1886)がヒト 1例 Julius Hallervorden (1882–1965) encountered a pro2,3 の脳を定量的に分析したことに始まる 。Zaleski は,鉄 gressive neurological disorder predominated by extrap含量を染色切片および顕微鏡用切片の観察所見と関連付 yramidal features. Histology revealed high levels of further brain iron.6 The morphological picture was けた。ヒト脳の鉄に関する最初の系統的研究は 1920 年代 characterized by the presence of ‘‘spheroid bodies,’’ に Hugoare Spatz(1888 ~ 1969)が実施し,彼は脳領域を染 which usually roundish, homogeneous, or faintly 4 to 100 lm in diameter. granular bodies measuring up 色強度により 4 群に分類した 。Spatz の観察では,淡蒼 Occasional spheroids may occur in a variety of condi球と黒質網様部が最も強く染色され,錐体外路運動系の tions, but they predominated in these cases. Interest5 ingly, possible links to Alzheimer’s and 核における高い鉄 濃 度に注目が 集まったdisease 。同じ頃, Parkinson’s disease were discussed in the 49-page origJulius Hallervorden(1882 ~ 1965)は,錐体外路症状を主 inal report.6 Within a few years further cases were 体とする進行性神経疾患の患者に遭遇している。組織学 reported, and variants were recognized. In 1952, Sei6 telberger described the early-onset form, subsequently 的には高レベルの脳内鉄が認められた 。さらに形態像は labeled as ‘‘infantile neuroaxonal dystrophy’’ (INAD) 7 「球状体(spheroid body) 」の存在を特徴とし,これらは who reviewed the literature by Cowen and Olmstead, and described 2 new cases, distinguishing them from 通常,丸みがあり均質またはわずかに粒状の小体で,直 classical Hallervorden–Spatz disease. For ethical rea径は最大 100 µm であった。このような球状体は様々な疾 sons, in view of research during the Nazi regime, the 患で少数生じる場合があるが,これらの症例では多数認 latter is now referred to as PKAN.8 An important milestone in the further workup of められた。興味深いことに,この疾患がアルツハイマー these diseases was the development of high-field MRI 病およびパーキンソン病(Parkinson’ s disease;PD)と関 連する可能性について,Hallervorden の 49 ページに及ぶ 原著報告 6 で論じられている。その後 2 ~ 3 年以内に別 in the 1980s, allowing noninvasive neuroimaging in の症例が報告され,異型の存在も認識されるようになっ vivo with demonstration of decreased T2 relaxation 5,9 time caused by Seitelberger iron deposition. A linear relation た。1952 年には が早期発症型を報告し,そ was found between T2 relaxation rate and iron con7 の後 Cowen と Olmstead が「乳児神経軸索性ジストロ centration in postmortem brains in healthy volunteers, フィー(infantile 」と名付 so that MRI nowneuroaxonal has becomedystrophy;INAD) an important diagnostic tool for the とdiagnosis of iron disorders including けた。Cowen Olmstead は,既報の文献を再検討すると NBIAs. ともに,新規症例 2 例を報告し,これらを古典的なハレ ルフォルデン・スパッツ病と鑑別した。倫理的な理由, NBIA Type 1—PKAN すなわち,ナチス政権時代の研究であることを考慮し, The core syndrome among the NBIA disorders is ハレルフォルデン・スパッツ病は現在,PKAN と呼ばれ PKAN, a result of mutations in the PANK2 gene on ている 8。 chromosome 20p, which accounts for approximately half the cases of NBIA.10 There remains uncertainty その後の研究における重要な画期的出来事は,1980 年 about the diagnosis in cases reported prior to gene 代の強磁場 MRI の開発である。これにより vivo の非 identification, which were based on clinicalinor pathological findings. Identification of the gene allowed a 侵襲的神経画像検査が可能となり,鉄沈着による T2 緩 broad clinical spectrum to be acknowledged with an 5,9 和時間の低下が確認できるようになった 。T2 緩和速度 equally broad genetic gamut. In the classic presentaと鉄濃度との間の直線的関連性が,健常ボランティアの tion age at onset is early. Patients with later onset often show atypical clinical features. 剖検脳で確認された。MRI は現在,NBIA 症候群を含む 鉄関連障害の診断において重要な診断ツールとなってい Classic Presentation of PKAN る。 In the classic variant, onset is around age 3–4 years, occurring before age 6 in almost 90%.11,12 Gait or postural difficulty is usually the presenting symptom.12 1 型 isNBIA:PKAN The phenotype characterized by pyramidal (spasticity, hyperreflexia, extensor toes) and extrapyramidal features dystonia. Prominent NBIA with の 主 prominent 要 症 候 群 とし て PKAN が 挙 げoromanら れ る。 dibular involvement is a characteristic sign.13 PKAN is PKAN は, 染色体 20p の PANK2 遺伝子の変異により生じ, thus one of the main differential diagnoses to consider 10 protrusion dystonia.13 in patients with severe tongue NBIA 症例の約半数を占める 。この遺伝子が同定され Other extrapyramidal features like chorea or parkinる以前に報告された症例は,診断に不確実性が残る。す sonism as well as cognitive features including behavなわち,これらの診断は,臨床所見または病理学的所見 ioral changes14 and dementia may occur. Oculomotor abnormalities suggestive of midbrain degeneration are に基づいている。遺伝子の同定により,幅広い臨床スペ common.15 They include impaired saccadic pursuits クトラムが認識されるようになり,同じように広範囲の遺 伝的変異が確認された。古典的 PKAN は,発症時年齢が Movement Disorders, Vol. 27, No. 1, 2012 43 3 MDs6-1.indb 3 12.7.17 4:36:22 PM NBIA 症候群の最新情報 低い。発症の遅い患者は,非定型的な臨床像を示す場合 外路症状や網膜症が軽度で,認知機能低下および精神症 が多い。 状( 例,同語 反 復 症 )が 最 初に認められる場 合もあ る 12,18-20。全体として,運動症状の重症度は古典型と比較 PKAN の古典的病像 して低い傾向にある 10。 PKAN 患者の睡眠解析では,総睡眠時間の短縮を伴う 古典的病型の場合,発症時年齢は 3 ~ 4 歳頃であり, ほぼ 90%が 6 歳までに発症する 11,12。歩行困難または姿 睡眠構造の変化が認められている。他の神経変性疾患と 勢保持困難が通常の主症状である 12。臨床像は,錐体路 は対照的に,REM 睡眠異常(特に REM 睡眠行動障害) 症 状〔 痙 縮, 反 射 亢 進, 趾 伸 筋 反 応 異 常(extensor や重大な無呼吸 / 呼吸低下は観察されていない。患者 1 toes) 〕 ,および著明なジストニアを伴う錐体外路症状を特 例で睡眠中の軽度の周期性四肢運動が認められている 21。 徴とする。顎口腔領域に顕著な症状がみられ,これが特 症例の大部分では,PKAN に関する詳細検査の結果, 徴的な所見である 。したがって,重度の挺舌ジストニ 淡蒼球での鉄蓄積に対応する特徴的な画像パターンが認 アを伴う患者では,重要な鑑別診断の 1 つとして PKAN められている。特に,T2* 強調 MRI 画像では,中央部に を考慮すべきである 。その他の錐体外路症状(舞踏病 高信号領域,その周囲に低信号領域が存在する「虎の目 13 13 やパーキンソニズムなど)および認知症状(行動変化 14 (eye-of-the-tiger) 」徴候が観察されている(Figure 1A) 。 や認知症など)が発現する場合もある。中脳変性を示唆 これらの低信号・高信号領域を拡散テンソル MRI で比較 する眼球運動異常はよくみられる所見である 。この眼 したところ(臨床的に診断された症例コホートが対象) , 球運動異常には,衝動性追従運動の障害や,垂直衝動性 異方性比率の上昇と平均拡散能の低下が認められた 22。 眼球運動の範囲狭小化や緩徐化がある。核上性垂直注視 重要な点として,MRI 上の変化が臨床的発症に先立って 麻痺も,遺伝子診断で確定された 1 症例で報告されてお 認められる場合がある 23。SPECT によるドパミントラン り,この徴候はニーマン・ピック病や Kufor-Rakeb 病で スポーターイメージング(線条体ドパミン機能の評価尺 も認められる(後述) 。矩形波眼球運動と輻輳不全も 度の 1 つ)所見は,一般に PKAN 患者では正常である 一部で認められる場合がある。垂直視運動反応の異常も が 24,25,遺伝子診断で確定された晩期発症型症例 1 例で 確認されており,前庭動眼反射の抑制不能が報告されて は異常が認められている〔この患者は人格変化,舞踏ア いる 。さらに, 一連の患者 10 例中 8 例で, 扇状虹彩麻痺, テトーゼ運動(choreoathetosis)および振戦を示し,向精 お よ び ア デ ィー 瞳 孔 に 類 似 す る 瞳 孔 縁 乳 頭 状 ひ だ 神 薬(neuroleptics) の 長 期 投 与 を 受 け て い た 〕17。 15 16 15 (papillary ruff)の部分的消失が両眼に認められたとの報 I-MIBG 心筋シンチグラフィーによる評価では,交感神 123 告がある 。類似の瞳孔異常は,他の脳内蓄積症でも観 経系の節後神経機能は PKAN では正常である(PD やそ 察されている 。また,この研究において,色素性網膜 の他の Lewy 小体病では一般に取り込み低下が認められ 症を呈したのは 10 例中 4 例のみであったが,約 70%の る)26。病理学的評価では,淡蒼球に褐色の変色が認め 患者に網膜電図の異常(軽度の錐体異常~重度の桿体 - られる。最近の病理学的研究 27 では,遺伝子診断で確定 錐体障害)が認められた 15。視神経萎縮を示した患者は され た 本 症 の 患 者 6 例 が 検 討 され た。 検 討 の 結 果, いなかった(ただし, 2 型 NBIA ではよくみられる) (後述) 。 PKAN では中枢神経系が侵され,末梢病変(精巣病変を この病態は進行性の経過をたどり,患児は 2 ~ 3 年以 含む)は通常みられないことが明らかになった。顕微鏡 15 15 内に車椅子生活を余儀なくされる。 的変化は主に淡蒼球にみられ,隣接する脳構造(内側被 殻および内包)にも様々な病変が認められるのに対し, 晩期発症型(非定型)PKAN 皮質,脳幹,その他の深部灰白質核には驚くほど病変が 遺伝子診断で確定された成人発症例(20 代および 30 みられない。視神経および小脳も侵されていなかった。 。こうした症例の多く 場合によっては,無傷のニューロンが淡蒼球にみられる は本症として認識されていない可能性が高く,特に臨床 ことから,異常ユビキチン化蛋白質の蓄積が他の神経変 像がやや非定型的であることがその原因と考えられる。 性所見に先行し,変性過程が,核構造やニューロンより 例えば,一側ジストニア性振戦や上肢局所性ジストニア も細胞質に強く影響する可能性が示唆される 27。2 種類 が初発徴候として報告されているが,その一方で,錐体 の球状体(spheroid) ,すなわち,粒状構造を示す大型の 代で発症)が報告されている 12,17,18 4 MDs6-1.indb 4 12.7.17 4:36:23 PM Schneider et al. A B Figure 1 A:NBIA 症例の脳 MRI 画像。パントテン酸キナーゼ関連神経変性症(PKAN) (左) , Kufor-Rakeb 病(ATP13A2 変異による) (中央) , 神経フェリチン症(FTL 変異による) (右)の各 1 例。PKAN では古典的な「虎の目(eye-of-the-tiger) 」徴候がみられる。検討した KuforRakeb 病患者では,鉄蓄積が被殻と尾状核に認められた。遺伝子レベルで証明された神経フェリチン症の本患者では,鉄蓄積が大脳基底核に 認められ,軽度の視床病変も示唆された。B:多系統萎縮症(MSA)患者の脳 MRI 画像。鉄蓄積は,NBIA とは異なり,淡蒼球ではなく後外 側被殻に特徴的に認められる。 もの(変性ニューロンでみられる)と,より好酸性の強 例(遺伝子同定以前に公表されたもの)の一部は,実際 い球状体構造を示す小型のもの(ジストロフィーに陥っ のところ,PKAN ではなく,少なくともその一部は 2 型 たニューロンの基質としてみられる)が識別可能である。 NBIA であった可能性が示唆される。文献から明白なこ 鉄蓄積は淡蒼球にみられ,血管周囲に分布しており,第 とは,過去の報告が,遺伝学的に異質である様々な鉄蓄 二鉄(Fe 積疾患サブタイプをひとまとめに扱い,結果的にハレル ,MRI 低信号との関連が推定される常磁性体 3+ 型)および程度は低いものの第一鉄としても存在した。 フォルデン・スパッツ病 ,NBIA ,PKAN ,その他の用語 神経網のびまん性鉄染色( “iron dust” )も認められた。担 が不正確に使用されていたことである。このように,古 鉄マクロファージおよび鉄を含む星状膠細胞(フェリチ い文献の解釈には問題がある。しかし,現在でもこのよ ンが強く染色される)も存在したが,全体的に炎症反応 うな用語の不正確な使用は続いており,遺伝子レベルで はほとんどみられなかった。また,タウの発現はわずか 確定されていない病型が,包括的用語である NBIA では であった。神経原線維変化(neurofibrillary tangle)やタ なく,PKAN として報告されている場合がある。これら ウ陽性神経炎はなかった 。黒質,赤核,その他の脳幹 の疾患を正しく解析するために,用語の正確な使用は必 領域において神経メラニンの低下はわずかであった(正 要不可欠である。 27 常な加齢変化と一致) 。 数多くの論文で Lewy 小体病変が報告されている 28-33。 変異(大部分がミスセンス変異)は PANK2 遺伝子の 7 つのエクソンすべてに検出されており,欠失,重複, しかし,最近検討され,遺伝子診断で確定された一連の スプライス部位変異に加え,エクソン欠失も報告されて 症例では,Lewy 小体が認められなかった(2 型 NBIA と いる 34。いくつかの変異は,他の変異に比べ,比較的軽 は対照的,後述) 。これは重要な知見であり,Lewy 小体 症の臨床像に関連する可能性がある 12,18。よくみられる 2 病変を伴う過去の「ハレルフォルデン・スパッツ病」症 つの変異(1231G > A および 1253C > T)が症例全体の 5 MDs6-1.indb 5 12.7.17 4:36:23 PM NBIA 症候群の最新情報 約 1/3 を占め,残りの大部分では「家系特異的な変異 床症例 1 例を報告しており,全体的な臨床像は,亜急性 発症型のジストニア・パーキンソニズムとこれに合併す (private mutation) 」がみられる 。 10 PANK2 は,皮質,淡蒼球,マイネルト基底核および橋 る錐体路徴候,眼球運動異常,認知機能低下,精神症状 核のニューロンに最も顕著に存在する。PKAN に関する を特徴とする 47。パーキンソニズム(この病態に関与す 正確な病態生理は未だ不明である。PANK2 遺伝子がコー る遺伝子座は PARK14 )は,安静時の丸薬を丸めるよう ドする関連蛋白質は,コエンザイム A 合成の最初の調節 な動作(pill-rolling)を含む振戦,筋強剛,重度の動作緩 段階を司り,パントテン酸(ビタミン B5)のリン酸化に 慢を特徴とし, レボドパ(L—ドパ)への反応は良好であっ よるホスホパントテン酸の生成を触媒する 。脂質代謝 た(Lewy 小体病変の所見に合致) (後述) 。ただし一方 における役割も示唆されている。PANK2 は主としてミト では,早期のジスキネジアがよくみられている 47。小脳 コンドリアに局在し,代謝障害を引き起こす可能性があ 徴 候 お よ び 感 覚 異 常 は, 早 期 小 児 型 の 病 型(early る 。仮説として,PANK2 を介するフェロポーチン発現 childhood variant)で顕著にみられる場合が多いが,これ の変化が,脳内鉄蓄積に関連すると考えられている 。 らは認められなかった。 35 36 37 NBIA 症候群の治療は依然として対症療法である。淡 こうした臨床像と一致して,神経画像検査では,INAD 蒼球深部脳刺激療法は,ある程度有効である可能性があ の早期に小脳萎縮が認められるが,晩期発症型では認め る られない。その後まもなく,INAD 患者では,T2 強調画像, 。最近のある研究では,深部脳刺激療法の術後 38-41 9 ~ 15 ヵ月時点の追跡調査で,ジストニア重症度の 20% T2* 強調画像およびプロトン密度強調画像上,鉄を反映 以上の改善が患者の 2/3 で認められている 。実験段階 する淡蒼球の低信号領域が認められる。特記すべき点と ではあるが,前運動野に対する 1 Hz 反復経頭蓋磁気刺激 して,この信号強度の異常所見は,PKAN の「虎の目 により,軽度かつ一時的な効果が認められている 43。 (eye-of-the-tiger) 」徴候とは異なり,中央部に高信号領域 PKAN のショウジョウバエ モデルを用いた基礎的病態生 がみられない。黒質の鉄沈着は,一部の非定型症例で認 理に関する研究では,パンテチンの補充投与により CoA められる 48,49。注目すべき点として,鉄沈着を欠く場合も レベルが回復し,ミトコンドリア機能の改善,自発運動 あり(遺伝子診断で確定された晩期発症型の 1 症例で実 の亢進,寿命の延長が認められた 。PANK2 ノックアウ 証されている) ,MRI 所見が完全に正常である場合さえ トマウスは,これまでのところ全般的に PKAN のモデル ある。その他の例として,皮質萎縮または白質変化があ として成功を収めていない 。パントテン酸(ビタミン る程度認められる場合がある。このように,PLA2G6 遺 B5)の神経保護剤としての役割を評価するヒト試験の結 伝子に関連する神経変性症のすべての病型が NBIA 症候 果は,我々の知る限り,まだ得られていない。キレート 群に属するわけではなく, 「神経放射線学的な多様性 42 44 45 療法については下記を参照されたい。 (neuroradiological variability) 」がみられる 47。したがって, ジストニア・パーキンソニズムを伴う患者では,MRI で 2 型 NBIA:PLA2G6 関連神経 変性症(PLAN) 脳内の鉄増加が認められなくても,PLAN を考慮すべき である 47。 PLA2G6 遺伝子は染色体 22q 上に存在し,17 のエクソ NBIA の 2 つ目の主要症候群である PLAN は,PLA2G6 ンを含む。コードされる蛋白質の iPLA2βは VIA 群カル 遺伝子変異を原因とする(2 型 NBIA) 。PKAN 同様,年 シウム非依存性ホスホリパーゼ A2 であり,これはリン脂 齢依存的な臨床像を示すと考えられる。早期発症例は 質の sn-2 アシル鎖を加水分解し,その結果,遊離脂肪酸 INAD を示し,進行性の運動遅滞および精神遅滞,小脳 とリゾリン脂質が生成される。iPLA2βは,膜リン脂質の 性運動失調,著明な体幹筋緊張低下,錐体路徴候,およ リモデリング,シグナル伝達,細胞増殖,アポトーシス び視神経萎縮による早期視覚障害を特徴とする。脳波 に何らかの役割を果たすと考えられる。iPLA2 の機能が (EEG)では速律動(fast rhythm)がしばしばみられ,発 失われた場合には,原形質膜,小胞,エンドソームの脂 作(seizure)が発現する場合もある 。PLA2G6 関連神 10,46 質構成が変化することが示唆されている。このような変 経変性症の発症が比較的遅い場合,臨床像は非定型的と 化は通常,軸索および樹状突起内の膜の挙動(movement) なりうる(非定型神経軸索性ジストロフィー) 。我々は臨 に関与する蛋白質および過程に影響を及ぼし,遠位軸索 6 MDs6-1.indb 6 12.7.17 4:36:23 PM U P D A T E O N N B I A Schneider S Y N D R O MetEal.S TABLE 2. Reported Kufor–Rakeb cases carrying homozygous or compound heterozygous cases to date (adjusted 107 Table 2 既報のホモ接合および複合ヘテロ接合の from Eiberg et Kufor-Rakeb al 2011107) 病症例(Eiberg ら,2011 Country of origin Zygosity Nucleotide change c.1632_1653dup22 c.1306þ5G>A, c.3057delC Brazilian Homozygote Compound heterozygote Homozygote c.1510G>C p.Leu552fs Ex13skipping/fs p.G1019fs p.Gly504Arg Japanese Pakistan Homozygote Homozygote c.546C>A c.1103_1104insGA p.Phe182Leu p.Thr367fs Afghan Homozygote c.2742_2743delTT p.Phe851fs Italian Asian Homozygote Compound heterozygote Homozygote c.2629G>A c.3176T>G (p.L1059R) and c.3253delC c.2473C>AA p.Gly877Arg p.L1059R, p.L1085WfsX1088 p.Leu825fs Jordanian Chilean Inuit Amino acid change を改変) Reference Ramirez et al, Nature. 2006 Ramirez et al, Nature. 2006; Brüggemann et al, Arch Neurol. 2010 Di Fonzo et al., Neurology. 2007; Chien et al., Mov Disord. 2011 Ning et al, Neurology. 2008 Schneider et al., Mov Disord. 2010; Paisán-Ruiz et al., Mov Disord. 2010 Crosiers et al, Parkinsonism Relat Disord. 2010 Santoro et al, Neurogenetics. 2010 Park et al, Hum Mutat. 2011 Eiberg et al., Clin Genet. 2011 the basal ganglia affecting the putamen and caudate is に膜の重積(accumulation)が生じ,最終的には進行性神 present in some (Fig. 1A), including 1 of our cases and 50-52 64,65 経損傷に至ると考えられている 。最近行われた機能 although not the Chilean family mentioned above, 61,62,66 53 all, and classification as NBIA type 3 has been 的表現型 - 遺伝子型研究 では,野生型蛋白質と比較す proposed.64 On transcranial sonography the substantia ると,INAD に関連する変異蛋白質の比活性は 20%未満 nigra was found to be normal,65 in contrast with idioであり pathic(リゾホスホリパーゼおよびホスホリパーゼのアッ PD, where hyperechogenicity can usually be detected. Dopamine transporter imaging showed セイ) ,PLA2G6 リン脂質基質の蓄積が予測された。これ marked bilateral symmetrical reduction of striatal activとは対照的に,ジストニア・パーキンソニズム関連の変 ity, indicative of diminished presynaptic activity.65 Electrophysiological studies suggested pyramidal tract 異は,触媒活性を低下させない。これにより,少なくと damage, in line with clinical findings.67 Motor-evoked も一部の症例について,臨床像が比較的軽症で鉄蓄積を potential latencies were increased in patients. Electro伴わない理由が説明できるものと考えられる。 physiological abnormalities may also be present in asymptomatic heterozygous ATP13A2 mutation PLA2G6 遺伝子に関連する神経変性症の病理学的変化 carriers.67 は Kufor–Rakeb PKAN よりも広範囲に分布し,中枢神経系全体に及 disease is a result of mutations in the 59 54,55 gene, on chromosome 1p.7 は,小脳の萎 The 26-kbATP13A2 ぶ 。病変パターンに関する初期の報告 spanning gene contains 29 exons and encodes a lyso縮と硬化,線条体の脂質蓄積とグリオーシス,視覚経路 somal 5 P-type ATPase. Most patients reported to date have /carried homozygous tract)の一部(錐体路, mutations, but comおよび脳幹 脊髄の長経路(long pound heterozygous cases have also been identified. 脊髄小脳路,脊髄視床路,薄束,楔状束)における変性 To our knowledge, postmortem studies of human に言及している。共に遺伝子レベルで確定されたマウス Kufor–Rakeb disease are so far lacking. Sural nerve bi49,55 axonal degeneration, some opsy68 50has shown acute モデル およびヒト脳 に関する最近の研究では,広 regeneration, and a very mild chronic inflammatory 範囲に及ぶαシヌクレイン陽性 Lewy 病変が特定されて response with endoneurial and epineurial T-cells. In Schwann cells と孤発性 and perineurial and epineurial cells, but おり,PLA2G6 PD とのつながりが明示された。 not in axons, numerous cytoplasmic inclusion bodies 病理学的変化は特に新皮質で高度にみられ,びまん性新 were seen. Electron microscopy revealed the inclusions 皮質型(diffuse neocortical の Braak 病 to be membrane bound,type)の孤発性 irregular, andPDoccasionally folded. Overall, they 49 resembled irregular primary lyso期 6 に一致していた 。小脳病変を示す早期の臨床徴候 somes.68 Recent functional studies have demonstrated および画像検査所見と一致する形で,小脳皮質ニューロ that both truncating and missense ATP13A2 mutations were retained in the endoplasmic reticulum, and ンの様々な喪失(プルキンエ細胞よりも顆粒細胞で顕著) there was premature degradation of mutant ATP13A2 および著明な星状細胞増加(astrocytosis)がみられる場 proteins by the proteasomal, but not the lysosomal, pathways49that may contribute to the etiology.69 合もある 。また,過剰リン酸化タウの蓄積が,細胞質 49 A link to neuronal ceroid-lipofuscinosis (NCL) was 。 として報告されており,Braak 病期 5 に一致していた recently established, when mutations in the ATP13A2 晩期発症型において臨床像が比較的軽度である場合は, gene were identified in animal models of NCL, but 56,57 screening humans with the compatible phenotype of タウ病変も軽度である傾向が認められている 。 70 Kuf’s disease did not reveal mutations. The finding of 10-fold increased ATP13A2 expression in the dopaminergicKufor-Rakeb substantia nigra neurons of patients with iPD 病(PARK9) compared with control samples suggests a possible role of this gene in the etiology of sporadic, clinically Kufor-Rakeb typical iPD.65 病は,まれな常染色体劣性遺伝性の神経 変性疾患であり,Kufor-Rakeb 村出身のヨルダン人の血 さらに別の症例が各国で様々な変異キャリアとして特定 FA2H mutations, previously known to cause leuko71 されている(Table 。Kufor-Rakeb 病の臨床像はパーキ and a 2) form of hereditary spastic parapledystrophy 72,73 were recently identified as another gia (HSP), ンソニズムであり,一部では錐体路徴候がみられる。不 cause of NBIA.56 Like PANK2 and PLA2G6, the met完全な核上性上方注視麻痺を伴う眼球運動異常が,診断 abolic pathway of FA2H involves the lipid and ceramide metabolism. The FA2H-NBIA index cases were の糸口となりうる。垂直方向および水平方向の衝動性眼 3 affected brothers from a consanguineous Italian 球運動ならびに衝動性追従眼球運動の緩徐化も報告され family and 2 affected brothers from an Albanian kin60 ているThe 。また,oculogyric dystonic dred. clinical phenotype wasspasm,顔面‐口蓋‐ characterized by childhood-onset gait impairment, spastic quadripare手指ミオクローヌス(mini-myoclonus) ,自律神経障害も sis, severe ataxia, and dystonia. Divergent strabismus 認められる場合がある。認知症状には幻視と認知症が含 developed. Seizures may be present. Overall, there was 58,59,61-63 to the great similarity of the clinical presentation まれる。発症時期は通常,思春期である 。L—ドパ group of neuroaxonal dystrophies. MRI demonstrated 58 への反応は良好であると指摘されているが ,他の複雑 bilateral globus pallidus T2 hypointensity, consistent な劣性遺伝性ジストニア・パーキンソニズム病型と同様, with iron deposition, prominent pontocerebellar atrophy, mild cortical atrophy, white matter lesions, and L—ドパ誘発性ジスキネジアが早期に発現する傾向にあ corpus callosum thinning. 61,62 るFA2H 。脳 CT および MRI では,びまん性かつ中等度の catalyzes hydroxylation at the 2 position of the N-acyl chain of the ceramide moiety. Glycosphingoli大脳および小脳萎縮がみられる場合がある。大脳基底核 pids, which contain a high proportion of 2-hydroxy (被殻と尾状核) (Figure , 我々 fatty acid, areの鉄沈着は一部にみられ important constituents of 1A) myelin 72 The involvement in lipid and ceramide sheaths. が経験した症例のうちの 1 例や上述のチリ人家系でも認 では糸状物(threads)として,ニューロン周核部では められているが 64,65,全例にみられるわけではなく 61,62,66, pretangle および神経原線維変化(neurofibrillary tangle) 64 3 型 NBIA としての分類が提唱されている Movement Disorders, Vol. 27, No. 1,。経頭蓋的 2012 47 縁家族 58 で最初に報告された。その後,本症に関連する FA2H-Associated 59 遺伝子がチリ人の大規模な血縁集団で同定され ,以後, Neurodegeneration (FAHN)/SPG35 7 MDs6-1.indb 7 12.7.17 4:36:24 PM NBIA 症候群の最新情報 超音波検査の黒質所見は正常であり 65, 孤発性 PD(エコー る種の遺伝性痙性対麻痺(hereditary spastic paraplegia; 輝度上昇が通常検出される)とは対照的であった。ドパ HSP)72,73 の原因となることが知られているが,近年新た ミントランスポーターイメージングでは,両側対称性の に,NBIA の原因としても同定されている 56。PANK2 お 線条体活動の著しい低下が認められ,シナプス前活動の よび PLA2G6 と同様に,FA2H の代謝経路は,脂質およ 低下が示唆された 。電気生理学的検討では,錐体路の び セラミド代 謝に関与する。FA2H 変 異による NBIA 損傷が示唆され,臨床所見との一致が認められている 67。 (FA2H-NBIA)の初発症例(index case)は,イタリア人 運動誘発電位の潜時の延長が患者でみられた。電気生理 血縁家族の兄弟 3 例と,アルバニア人血縁家族の兄弟 2 学的異常は,無症状のヘテロ接合 ATP13A2 変異キャリ 例であった。 臨床像の特徴は, 小児期に発症する歩行障害, アでも認められることがある 。 痙性四肢麻痺,重度の運動失調,ジストニアであった。 65 67 Kufor-Rakeb 病は,染色体 1p 上にある ATP13A2 遺伝 外斜視も認められた。痙攣(seizure)が発現する場合も 子の変異を原因とする。この全長 26 kb の遺伝子は 29 個 ある。全体として,本症の臨床像は神経軸索ジストロ のエクソンを含み,リソソーム 5 型 P 型 ATPase をコード フィーの疾患群とよく似ていた。MRI では,両側淡蒼球 する。これまでに報告された患者の大部分はホモ接合変異 の T2 低信号領域(鉄沈着に一致する所見) ,著明な橋小 キャリアであるが,複合ヘテロ接合症例も同定されている。 脳萎縮,軽度の皮質萎縮,白質病変,脳梁の菲薄化が認 59 我々が知る限り,Kufor-Rakeb 病患者の剖検研究はこ れまで行われていない。腓腹神経の生検 められている。 では,急性軸 FA2H は,セラミド部分の N -acyl 鎖 2 位の水酸化を触 索変性, ある程度の神経再生, ごく軽微な慢性炎症反応 (神 媒する。スフィンゴ糖脂質(高い割合の 2 ヒドロキシ脂 経内膜および神経上膜の T 細胞を伴う)が認められてい 肪酸を含む)は,ミエリン鞘の重要な構成成分である 72。 る。シュワン細胞,神経鞘細胞,神経上膜細胞には多数 脂質およびセラミド代謝への関与により,1 型 NBIA,2 の細胞質内封入体がみられたが,軸索にはみられなかっ 型 NBIA およびその他の神経変性疾患との機能的な関連 た。電子顕微鏡観察では,これらの封入体は膜結合性か が認められる 74。したがって,臨床的および放射線学的 つ不定形で,折りたたまれている場合もあった。全体と 所見に共通点(overlap)が認められることは,それほど して,これら封入体は,不定形の一次リソソームに類似 意外ではない。 68 していた 。最近の機能的研究によると,ATP13A2 の短 68 FA2H 欠損は異常ミエリンを生じ,白質ジストロフィー 縮型変異体とミスセンス変異体は共に小胞体に保持され, および SPG サブフォーム SPG35 といった対立遺伝子疾 そこで変異 ATP13A2 蛋白質の早期変性が生じる。この変 患を引き起こす〔放射線学的所見に共通点(overlap)が 性はリソソームではなく,プロテアソーム経路で生じ, みられる〕 。白質変化が FAHN では認められるが,これ これが病因に寄与している可能性がある 。 は白質ジストロフィーの中核的な要素でもある。FAHN 69 近年,神経セロイドリポフスチン症(neuronal ceroid- でみられる脳梁菲薄化は,一部の SPG の顕著な特徴でも lipofuscinosis;NCL)との関連が確認され,ATP13A2 遺 ある 75。注目すべきことに,SPG とジストニア・パーキ 伝子変異が NCL の動物モデルで同定されている。しかし, ンソニズムとの結びつきが,近年,SPG11,SPG15,およ クッフス病と臨床像が一致した患者のスクリーニングで, び遺伝子レベルで確認されていない SPG 諸型でも明らか 変異は認められなかった 70。黒質ドパミン作動性ニュー にされている 76-79。また,Lewy 小体病変は,ジストニア ロンの ATP13A2 発現が,孤発性 PD 患者では対照群に比 の有無とは無関係に,パーキンソニズムを伴う個々の べて 10 倍上昇していることが確認されており,この遺伝 SPG 症例で認められている 79,80。FA2H のマウスモデルが 子が典型的臨床像を示す散発性孤発性 PD の病因に何ら 最近開発されており 81,このモデルでは,有意な脱髄と かの役割を果たしている可能性が示唆される 65。 高度の軸索消失が中枢神経系において実証された 81。軸 索は異常拡大し,小脳では異常な組織像が認められた。 FA2H 関連神経変性症 (FAHN) / SPG35 FA2H 変異は,以前から,白質ジストロフィー 71 これとは対照的に,末梢神経の構造および機能はほぼ影 響を受けていなかった。FAHN のヒト脳に関する病理学 的研究は今後の課題である。 やあ 8 MDs6-1.indb 8 12.7.17 4:36:24 PM Schneider et al. S C H N E I D E R E T A L . Table 3 無セルロプラスミン血症と神経フェリチン症の比較 TABLE 3. Comparison of aceruloplasminemia and neuroferritinopathy Genetics Ceruloplasmin gene Presentation Defect Pathogenesis Clinical Pathology Aceruloplasminemia Neuroferritinopathy Autosomal recessive loss-of-function mutations Ferritin light-chain gene Third decade—diabetes Fifth decade—neurologic Brain iron recycling Brain iron accumulation Systemic iron accumulation Diabetes, anemia, dementia Dystonia, dysarthria Iron accumulation in astrocytes neuronal loss Autosomal dominant (dominant-negative) mutations Third through sixth decades Brain iron storage Brain iron accumulation Dementia, dystonia, dysarthria Iron accumulation in astrocytes neuronal loss Madsen および Gitlin and から転載。 Reproduced from Madsen Gitlin.105 105 metabolism is a functional link to NBIA1, NBIA2, and other neurodegenerative diseases.74 Thus, the clinical 無セルロプラスミン血症 and radiological overlap is not too surprising. FA2H deficiency results in abnormal myelin, giving 無セルロプラスミン血症は,染色体 3q 上の ceruloplasrise to the allelic disorders leukodystrophy and the HSP遺伝子の変異を原因とする(Table subform SPG35, which show radiological overmin 1 および 3,Figure lap. White matter changes are present in FAHN and 2) 。遺伝形式は常染色体劣性である。臨床像の特徴は, are also a core element of leukodystrophies. The pres成人発症型の運動異常症と認知症である。最近の文献レ ence of a thin corpus callosum seen in FAHN is also a 75 82 hallmark feature in some of the HSPs. Notably, a ビュー によると,診断時年齢は平均 51 歳であり,範囲 link between HSP and dystonia-parkinsonism was は 16 ~ 71 歳である。ホモ接合体症例 28 例の検討にお recently also unraveled for SPG11, SPG15, and geneti76–79 and Lewy body cally 最もよくみられた主症状は認知障害(42%)であり, undetermined HSP forms, いて, pathology has been present in individual HSPs cases 頭蓋顔面ジスキネジア(28%) ,小脳性運動失調(46%) , with parkinsonism, with or without dystonia.79,80 82 網膜変性(75%)の合併がみられた 。糖尿病が合併す Mouse models of FA2H have recently been devel81 In these, significant demyelination and prooped. る場合もある。 found axonal loss could be demonstrated in the 81 Ceruloplasmin 遺伝子がコードする蛋白質は,組織から CNS. Axons were abnormally enlarged, and there was abnormal cerebellar histology. In contrast, strucの鉄動員にきわめて重要な役割を果たし,血漿銅の 95% ture and function of peripheral nerves were largely を運搬する。この蛋白質の機能に異常が生じると,過剰 unaffected. Pathological studies of human FAHN 84 動失調は通常みられない brains are still awaited. 。創始者効果(founder effect) により,症例群(clustering)が英国のカンブリア地方に に鉄が蓄積し,脳(大脳基底核,視床,歯状核,大脳皮質, 認められるが,脳外病変(肝内鉄沈着など)が存在する 小脳皮質)だけでなく, 膵臓や肝臓にも鉄蓄積がみられる。 場合もある 89。最近開発されたマウスモデルでは,ヒト 診断に役立つ所見として,ホモ接合体では,セルロプラ 疾患によく似た脳内鉄蓄積が確認されており,ミトコン スミンは通常,血清中には検出されず,銅および鉄の血 ドリアの重要な役割が示唆されている 90。 みられるが,独立した症例が様々な国々(フランス,イ Aceruloplasminemia ンド,日本など)で報告されている 83,85,86。 Aceruloplasminemia results from mutations in the 無セルロプラスミン血症とは異なり,血清フェリチン ceruloplasmin gene, on chromosome 3q. (Tables 1 and 濃度は低い場合がある。MRI では,大脳基底核の嚢胞性 3, Fig. 2). Inheritance is autosomal recessive. The clinical presentation is characterized by adult-onset move変化と両側淡蒼球の壊死が認められる場合があり,鉄蓄 ment disorders and dementia. A recent literature 82 積が尾状核,淡蒼球,被殻,黒質および赤核にみられ revealed an average age at diagnosis of 51, review with a range from 1688,フェリチン陽性の球状封入体が, to 71 years. For the 28 homozyる 87。病理学的には gous cases, the most common presenting feature was 鉄を多く含む領域に認められ,しばしばミクログリア, cognitive impairment (42%), accompanied by cranioオリゴデンドロサイトおよびニューロンと共に局在して facial dyskinesia (28%), cerebellar ataxia (46%), and retinal degeneration (75%).82 Diabetes mellitus may いた。ユビキチンおよびタウと免疫反応する神経軸索球 be associated. 状体とニューロフィラメントが報告されており,上述の The encoded protein plays a crucial role in the mobilization of iron from tissues and carries 95% of 神経軸索ジストロフィー疾患群とのギャップを埋める所 plasma copper. Protein dysfunction results in excessive 見が観察されている。主要病変は後部被殻および小脳に 清濃度は低下する。一方,フェリチンは 3 ~ 40 倍上昇す る 82。FDG-PET では,大脳基底核と視床の代謝低下が検 出されている。 神経フェリチン症 SENDA 症候群,MIN,遺伝子 レベルで確認されていないその 他の NBIA 病型 遺伝子レベルで未だ確認されていない NBIA 病型が, FIG. 2. Pathways of cellular iron homeostasis and neurological disorders associated with iron accumulation associated with these, adjusted from 神経フェリチン症の原因は,染色体 19q 上の FTL 遺伝 成 人 期 神 経 変 性 を 伴 う小 児 期 非 進 行 性 脳 症(static 錐体外路症状(舞踏病,ジストニア等)がみられ,臨床 精神遅滞からなり,これらの症状は 20 代後半~ 30 代前 像はハンチントン病に類似する 。錐体路障害および運 半までは安定しているが,その後は進行してパーキンソ Madsen and Gitlin.105 Iron uptake can occur via the divalent transporter DMT1 (ferrous iron, Fe21, shown in the lower right) or via endocytosis of the transferrin receptor (ferric 1A) iron,。神経フェリチン症は,本レ Fe31, shown in the upper right). Steap3 isencephalopathy a ferrireductase critical for transferrin-mediated iron release into the 子の変異である(Figure of childhood with neurodegeneration in cell. Ferritin is the predominant storage protein consisting of heavy chains and light chains. Mutations in the gene encoding ferritin light chains are associated with neuroferritinopathy (1). Iron homeostasis is regulated by hepcidin, which binds to ferroportin, the only known cellular iron. Ceruloビューで論じた他の疾患とは異なり,遺伝形式は常染色 adulthood;SENDA) (SENDA 症候群)という名称で近年 plasmin is a ferroxidase-mediating efficient cellular iron release. Mutations in the gene encoding ceruloplasmin cause aceruloplasminemia (2). Iron 91 enters mitochondria via mitoferrin, Frataxin is a mitochondrial protein mediating Fe-S cluster formation and heme biosynthesis. Mutations in frataxin 体優性である。平均発症時年齢は中年期の 40 歳前後で, 報告されている 。臨床像は,早期発症の痙性対麻痺と cause Friedreich ataxia (3). 83 48 Movement Disorders, Vol. 27, No. 1, 2012 9 MDs6-1.indb 9 12.7.17 4:36:24 PM NBIA 症候群の最新情報 Fe3+ Hepcidin Steap3 Fe3+ Ceruloplasmin Transferrin receptor Cu L 2 H Ferroportin S Fe2+ Heme Frataxin 3 S Ferritin H 1 Transferrin L Mitoferrin DMT1 Fe2+ Figure 2 細胞内の鉄ホメオスタシス経路と関連する鉄蓄積を伴う神経疾患(Madsen および Gitlin105 を改変) 。鉄の取り込みは,二価トランス ポーター DMT1(第一鉄,Fe2 +,右下に示す)またはトランスフェリン受容体のエンドサイトーシス(第二鉄,Fe3 +,右上に示す)を介して 生じる。Steap3 は,トランスフェリンを介した鉄の細胞内放出に不可欠な役割を果たす三価鉄還元酵素である。フェリチンは主要貯蔵蛋白質 であり,重鎖および軽鎖よりなる。フェリチン軽鎖をコードする遺伝子の変異は,神経フェリチン症に関連する(1) 。鉄のホメオスタシスは ヘプシジンにより調節され,これはフェロポーチン(既知の唯一の細胞鉄)に結合する。セルロプラスミンは,効率的な細胞鉄放出を仲介す る鉄酸化酵素である。セルロプラスミンをコードする遺伝子の変異は,無セルロプラスミン血症を引き起こす(2) 。鉄はマイトフェリン (mitoferrin)を介してミトコンドリア内に入る。フラタキシンはミトコンドリア蛋白質であり,Fe-S クラスター生成とヘム生合成を仲介する。 Frataxin 遺伝子の変異はフリードライヒ失調症を引き起こす(3) 。 ニズムおよびジストニアに至る。他の症状として,眼球 症(DRPLA) ,マ ン ノシド ー シ ス,表 在 性 鉄 沈 着 症 運動異常,睡眠障害,前頭葉解放徴候(frontal release (superficial siderosis)などが挙げられるが,鉄密度が最も sign) ,自律神経障害などが発現する。画像検査では,淡 高い部位はそれぞれ異なる(私信,文献 94 および 95) 。 蒼球を侵す脳内鉄蓄積,黒質の低信号領域,白質変化が さらに,MRI の鉄沈着所見〔 「虎の目(eye-of-the-tiger) 」 認められている。治療については,L —ドパ投与を試みた 徴候に類似する場合がある〕は,他の神経変性疾患(多 患者で著明な反応が得られている。基礎にある(遺伝子 系統萎縮症など) でも観察される場合がある 96-99。しかし, レベルでの)原因は依然として不明である。 多系統萎縮症において,鉄蓄積は後外側被殻に特徴的に Hartig らは,ポーランド人 NBIA 患者 54 例のコホート について報告した。この患者集団には,痙性対麻痺,ジ みられ,NBIA 疾患のように淡蒼球でみられることはまれ である 100。 ストニア,精神症状,神経障害,視神経萎縮を伴う 1 つ のサブグループが認められた。遺伝子検査により 1 つの 新規 NBIA 遺伝子が同定され,4 つの異なる変異が患者 結 論 21 例で認められた 92。MIN 関連神経変性症を示す頭字語 本稿では NBIA 症候群の原因を要約した。NBIA の主 として MPAN(MIN-associated neurodegeneration)が提案 要症候群に加え,未だに遺伝子レベルで病因が解明され されている。正確なデータの発表が待たれるところであ ていない,臨床的な特徴に基づくサブグループについて る。 も検討した。NBIA 症候群を通じ,我々は,臨床的およ さらに,単一の NBIA 患者に関する症例報告も複数あ び遺伝的多様性について教訓を得ている。例えば,FA2H り,これには PD に似た症状を呈する晩期発症型の症例 の検討から,単一遺伝子の複数の変異により多数の異な が含まれている 。安静時振戦は非対称性であり,再 る臨床像が生じる機序について理解できるであろう。今 出現性の振戦(reemergent component)もみられた。L—ド 後,主要症候群についてさらに幅広い臨床像が発現する パを投与するとジスキネジアが発現したが,深部脳刺激 可能性が高いと考えられる。また,NBIA 症候群の基礎 療法では良好な効果が認められた。 をなす新たな遺伝子も発見されるであろう。しかし,あ 18,93 また,脳内鉄蓄積はその他の病態でも生じ,フリード らゆる遺伝的原因の探索が詳細な臨床的特徴の把握に基 ライヒ失調症(Figure 2) ,歯状核赤核淡蒼球ルイ体萎縮 づいていることには依然として変わりはない。したがっ 10 MDs6-1.indb 10 12.7.17 4:36:25 PM Schneider et al. Acetyl - CoA Palmitoyl - CoA + serine Sphinganine 1 Sphingomyelin Fatty acid Sphingosine Dihydro - Ceramide 10 2 11 Fatty acid Ceramide 6 Galactosylceramide Glucosylceramide 7 4 3 4 8 5 9 Globoside Ganglioside Digalactosylceramide Sulphatide Figure 3 セラミド代謝経路の簡略図。セラミドは 2 つの主要ソースに由来し,それぞれ異なる細胞コンパートメントで反応が生じる。すなわ ち,1 つは膜由来スフィンゴミエリンの加水分解,もう 1 つはパルミトイル CoA およびセリンからの de novo 合成である。これらの経路に関 連する神経疾患を提示する(一部のみ) 。King(2008)106 および http://www.sphingomap.org/ を参照のこと。1:パントテン酸キナーゼ関連神経 変性症(PKAN) ,2:ファーバー病(セラミニダーゼ欠損症) ,3:クラッベ病(βガラクトシダーゼ欠損症) ,4:ファブリー病(αガラクトシダー ゼ A 欠損症) ,5:異染性白質ジストロフィー(セレブロシドスルファターゼ欠損症) ,6:ゴーシェ病(グルコセレブロシダーゼ欠損症) ,7: テイ・サックス病(ヘキソサミニダーゼ A 欠損症) ,8:GM2 ガングリオシドーシス(βガラクトシダーゼ欠損症) ,9:サンドホフ病(ヘキソ サミニダーゼ A + B 欠損症) ,10:PLA2G6 関連神経変性症,11:ニーマン・ピック病(スフィンゴミエリナーゼ欠損症) て,NBIA 症例を経験した医師は,積極的に報告するよ ける鉄の役割が強調されるようになったのは,孤発性 PD うに呼びかけたい。 症例の黒質やβアミロイド斑沈着構造の内部に鉄が見出 注目すべき点として,NBIA 症候群の原因遺伝子の多 されたことに基づいている。また,鉄はこれらの発病機 くは,関連する代謝経路にマッピングされており,未確 序にきわめて重要な役割を果たす可能性があり,鉄の役 定の病型における遺伝子産物も関連生化学経路上に存在 割を理解することで,神経変性過程そのものについての する可能性がある 。また,未だ特徴が明らかにされて 示唆が得られるであろう。 74 いない関連経路に関与する別の遺伝子が,類似する症候 群を引き起こしている可能性もある 。実際のところ, 47,101 現在までのところ,NBIA 症候群に対する治療選択肢 は対症療法に留まり,不満足な成績であることも多い。 セラミド〔スフィンゴ脂質代謝の中心的分子で,N アシ したがって,個々の NBIA 症候群の病態生理,臨床経過, ル化(炭素数 14 ~ 26)されたスフィンゴシン(炭素数 診断基準および予後を理解することが,発症機構に即し 18)からなる〕は,これらの経路において中心的役割を た治療法を探索する上で非常に重要である。鉄が原因と 果たす可能性があり(Figure 3) ,アポトーシスにおける して役割を果たすという仮定に基づき,遊離鉄量を減ら セラミドとミトコンドリアの密接に関連した役割と一致す すキレート剤が検討されている。動物モデルで示された る。セラミドは多くの細胞過程に関与し(レビューは文 有望な結果を受け,ヒトでの試験が開始されており,複 献 数の単独症例で有益な効果が報告されている。ごく最近, 102 および 103 を参照) ,これには Lewy 小体の病態生理 やタウオパチーなどが含まれ,比較的一般的な孤発性疾 PKAN に関する最初の第Ⅱ相予備的オープン試験の結果 患(PD やおそらくアルツハイマー病)との共通点を示す が 公 表 さ れ, こ の 試 験 で は, 経 口 鉄 キ レ ー ト 剤 所見が観察されている deferiprone の臨床的および放射線学的効果が,用量 25 。これらの神経変性過程にお 9,56,74 11 MDs6-1.indb 11 12.7.17 4:36:25 PM NBIA 症候群の最新情報 mg/kg/ 日で 6 ヵ月間評価された 104。試験を完了した患者 9 例のうち 6 例の病型は古典型であり,3 例は非定型の疾 de, which is derived from 2 main sources operating in different cellular compartments: hydrolysis of nthesis from palmitoyl CoA and serine. Neurological diseases along the pathways are demonstrated 患 像 であった。罹 病 期間の中 央 値は 11 年 であった。 ww.sphingomap.org/ (1, pantothenate kinase–associated neurodegeneration [PKAN]; 2, Farber dise [beta galactosidase deficiency]; 4, Fabry disease [alpha galactosidase A deficiency]; 5, metachroDeferiprone の忍容性は全体的に良好であった。副作用と iency]; 6, Gaucher disease [glucocerebroisidase deficiency]; 7, Tay Sachs disease [hexosaminidase osidase deficiency]; 9, Sandhoff disease (hexosaminidase A 1 B deficiency]; 10, PLA2G6-associして悪心および胃痛(44%)等が認められたが,重篤な e [sphingomyelinase deficiency]). 有害事象はみられなかった。報告の著者らは,淡蒼球鉄 ted (14–26 cary play a central e with the interndria in apoptoll processes (for including Lewy ies bridging the iseases including 56,74 The role of sses is strengththic PD cases in tures affected by iron may play a the understandications for neu- NBIA disorders tisfactory. Thus clinical course, he distinct NBIA for mechanistic on plays a causamount of free imal models inies with beneficial ently, the results in PKAN have 含量の有意な低下(中央値:30%,範囲:15 ~ 61%)を been published, assessing the clinical and radiological effects of the oral iron-chelator deferiprone at a dose 観察している。しかし, 臨床的な効果 [Burke-Fahn-Marsden of 25 mg/kg/day over a 6-month period.104 Of 9 dystonia scale(BFMDRS)および medical outcome patients rating who completed the study, 6 had classic disease and 3 had36-item atypical disease. Median disease durastudy short-form health survey(SF-36)で評価]は tion was 11 years. Deferiprone was well tolerated 認められなかった。この結果の原因として,投与期間が overall. Side effects included nausea and gastralgia 比較的短かったこと,罹病期間が既に長期にわたってい (44%), but no serious adverse event occurred. The authors observed a significant (median, 30%) reducたこと,あるいはニューロンの傷害が高度に進行してお tion in globus pallidus iron content, ranging from り機能の回復は不可能であったことが考えられる。さら 15% to 61%. However, there was no clinical benefit, as rated on the BFMDRS and SF-36 scale, which may なる研究が待たれる。 have been a result of the relatively short treatment duration or already long disease duration or neuronal 謝 辞 damage too advanced to allow for a rescue of function. Further studies are awaited. W. Christie と R. Gorenflos の有用な考察,T. Wolf の技術支援, N. Quinn の原稿査読に感謝する。 Acknowledgments: We thank W. Christie and R. Gorenflos for Galvin JE, Gia brain iron accu and gamma-sy 361–368. Hayflick SJ. Neurodegeneration with brain iron accumulation: from genes to pathogenesis. Semin Pediatr Neurol 2006;13: 182–185. 32. Williamson K, in young adul cases. Ann Neu 12. Hayflick SJ, Westaway SK, Levinson B, et al. Genetic, clinical, and radiographic delineation of Hallervorden-Spatz syndrome. N Engl J Med 2003;348:33–40. 33. Eidelberg D, S den-Spatz disea copathological 13. Schneider SA, Aggarwal A, Bhatt M, et al. Severe tongue protrusion dystonia: clinical syndromes and possible treatment. Neurology 2006;67:940–943. 34. 14. Marelli C, Piacentini S, Garavaglia B, et al. Clinical and neuropsychological correlates in two brothers with pantothenate kinase-associated neurodegeneration. Mov Disord 2005;20: 208–212. Hartig MB, Ho notypic spectru generation wit 248–256. 35. Kotzbauer PT, mitochondrial brain iron accu and catalytic a 2005;25:689–6 36. Lin MT, Beal M in neurodegene Gregory A, Hayflick S. Clinical and genetic delineation of neurodegeneration with brain iron accumulation. J Med Genet 2009; 46:73–80. 11. 15. REFERENCES Egan RA, Weleber RG, Hogarth P, et al. Neuro-ophthalmologic and electroretinographic findings in pantothenate kinase-associated neurodegeneration (formerly Hallervorden-Spatz syndrome). Am J Ophthalmol 2005;140:267–274. 16. Bozi M, Matarin M, Theocharis I, et al. A patient with pantothenate kinase-associated neurodegeneration and supranuclear gaze palsy. Clin Neurol Neurosurg 2009;111:688–690. 37. 17. Antonini A, Goldwurm S, Benti R, et al. Genetic, clinical, and imaging characterization of one patient with late-onset, slowly progressive, pantothenate kinase-associated neurodegeneration. Mov Disord 2006;21:417–418. Poli M, Dero (Pank2) silenci portin upregul 39:204–210. 38. 18. Aggarwal A, Schneider SA, Houlden H, et al. Indian-subcontinent NBIA: unusual phenotypes, novel PANK2 mutations, and undetermined genetic forms. Mov Disord 2010;25:1424–1431. Castelnau P, improves panto Neurol 2005;5 39. 19. Yoon WT, Lee WY, Shin HY, et al. Novel PANK2 gene mutations in korean patient with pantothenate kinase-associated neurodegeneration presenting unilateral dystonic tremor. Mov Disord 2010;25:245–247. Mikati MA, Y as a mode of t ated neurodege 40. 20. Chung SJ, Lee JH, Lee MC, et al. Focal hand dystonia in a patient with PANK2 mutation. Mov Disord 2008;23:466–468 Krause M, Fog lidal deep brai pantothenate k 2006;21:2255– 41. 21. Fantini ML, Cossu G, Molari A et al. Sleep in genetically confirmed pantothenate kinase-associated neurodegeneration: a video-polysomnographic study. Parkinsons Dis 2010;2010:342834. Szumowski J, B distribution in ing 2010;31:48 42. 22. Awasthi R, Gupta RK, Trivedi R, et al. Diffusion tensor MR imaging in children with pantothenate kinase-associated neurodegeneration with brain iron accumulation and their siblings. AJNR Am J Neuroradiol 2010;31:442–447. Timmermann L degeneration w pallidal stimula 43. Mylius V, Ger the premotor patient with disease (PKAN 23. Hayflick SJ, Penzien JM, Michl W, et al. Cranial MRI changes may precede symptoms in Hallervorden-Spatz syndrome. Pediatr Neurol 2001;25:166–169. 44. 24. Cossu G, Cella C, Melis M, et al. [123I]FP-CIT SPECT findings in two patients with Hallervorden-Spatz disease with homozygous mutation in PANK2 gene. Neurology 2005;64:167–168. Rana A, Seinen ila model for Proc Natl Acad 45. Wu Z, Li C, L generation: ins 2009;18:3659– 46. Morgan NV, W a phospholipa with high brain useful discussion, T. Wolf for technical support, and N. Quinn for critical review of the manuscript. References 1. Perls M. Nachweis von Eisenoxyd in gewissen Pigmenten [Demonstration of iron oxide in certain pigments]. Virchow’s Arch Pathol Anat Physiol Klin Med 1867;39:48. 25. Hermann W, Barthel H, Reuter M, et al. [Hallervorden-Spatz disease: findings in the nigrostriatal system]. Nervenarzt 2000;71: 660–665. 2. Koeppen AH. Friedreich’s ataxia: pathology, pathogenesis, and molecular genetics. J Neurol Sci 2011;303:1–12. Spatz H.AH, Uber den Eisennachweis im Gehirn, besonders in ZentKoeppen Morral JA, McComb RD, et al. The neuropathology des extrpyramidal-motorischen Systems2011;10:96–103. [On the visualization ofren late-onset Friedreich’s ataxia. Cerebellum of iron in the brain, especially in the centers of the extrapyramiSpatz H. Uber den Eisennachweis im Gehirn, besonders in Zentdal motor system]. Z Ges Neurol Psychiat 1922;77:390. ren des extrpyramidal-motorischen Systems [On the visualization Schenck JF, Zimmerman EA. High-field magnetic resonance imagof iron in the brain, especially in the centers of the extrapyramiingmotor of brain iron: Zbirth a biomarker? NMR Biomed 2004;17: dal system]. Ges of Neurol Psychiat 1922;77:390. 433–445. Schenck JF, Zimmerman EA. High-field magnetic resonance imagHallervorden J, Spatz Erkrankung im extrapyramiing of brain iron: birthH. ofEigenartige a biomarker? NMR Biomed 2004;17: dalen System mit besonderer Beteiligung des Globus pallidus und 433–445. der Substantia nigra.: Ein Beitrag zu den Beziehungen zwischen Hallervorden Spatz H.ZEigenartige im extrapyramidiesen beidenJ,Zentren. Ges NeurolErkrankung Psychiat 1922;254–302. dalen System mit besonderer Beteiligung des Globus pallidus und Cowen D, Olmstead neuroaxonal dystrophy. J Neuder Substantia nigra.: EV. Ein Infantile Beitrag zu den Beziehungen zwischen ropathol ExpZentren. Neurol 1963;22:175–236. diesen beiden Z Ges Neurol Psychiat 1922;254–302. ShevellD,MI, Peiffer EV. J. Julius Hallervorden’s wartime activities: Cowen Olmstead Infantile neuroaxonal dystrophy. J Neuimplications for science under dictatorship. Pediatr Neurol 2001; ropathol Exp Neurol 1963;22:175–236. 25:162–165. Shevell MI, Peiffer J. Julius Hallervorden’s wartime activities: Stankiewicz for J, Panter Neema M et al. Pediatr Iron inNeurol chronic2001; brain implications scienceSS, under dictatorship. disorders: imaging and neurotherapeutic implications. Neurother25:162–165. apeutics 2007;4:371–386. Stankiewicz J, Panter SS, Neema M et al. Iron in chronic brain Gregory A, Hayflick Clinical and genetic delineation of neurodisorders: imaging andS.neurotherapeutic implications. Neurotherdegeneration with brain iron accumulation. J Med Genet 2009; apeutics 2007;4:371–386. 46:73–80. Gregory A, Hayflick S. Clinical and genetic delineation of neuroHayflick SJ. with Neurodegeneration with brainJ iron degeneration brain iron accumulation. Med accumulation: Genet 2009; from genes to pathogenesis. Semin Pediatr Neurol 2006;13: 46:73–80. 182–185. Hayflick SJ. Neurodegeneration with brain iron accumulation: Hayflick SJ, to Westaway SK, Levinson B, et al.Neurol Genetic,2006;13: clinical, from genes pathogenesis. Semin Pediatr and radiographic delineation of Hallervorden-Spatz syndrome. N 182–185. Engl J Med 2003;348:33–40. Hayflick SJ, Westaway SK, Levinson B, et al. Genetic, clinical, Schneider SA, Aggarwal A, Bhatt M, et al. Severe tongue protruand radiographic delineation of Hallervorden-Spatz syndrome. N sion Jdystonia: clinical syndromes and possible treatment. NeurolEngl Med 2003;348:33–40. ogy 2006;67:940–943. Schneider SA, Aggarwal A, Bhatt M, et al. Severe tongue protruMarelli C, Piacentini S, Garavaglia et al. Clinical and neurosion dystonia: clinical syndromes and B, possible treatment. Neurolpsychological correlates in two brothers with pantothenate kiogy 2006;67:940–943. nase-associated neurodegeneration. Mov Disord 2005;20: Marelli C, Piacentini S, Garavaglia B, et al. Clinical and neuro208–212. psychological correlates in two brothers with pantothenate kiEgan RA, Weleber RG, Hogarth P, etMov al. Neuro-ophthalmologic nase-associated neurodegeneration. Disord 2005;20: and electroretinographic findings in pantothenate kinase-associ208–212. ated neurodegeneration (formerly Hallervorden-Spatz syndrome). Egan Weleber 2005;140:267–274. RG, Hogarth P, et al. Neuro-ophthalmologic Am JRA, Ophthalmol and electroretinographic findings in pantothenate kinase-associBozineurodegeneration M, Matarin M, Theocharis et al. A patient with pantotheated (formerly I,Hallervorden-Spatz syndrome). nateJ Ophthalmol kinase-associated neurodegeneration and supranuclear gaze Am 2005;140:267–274. palsy. Clin Neurol Neurosurg 2009;111:688–690. Bozi M, Matarin M, Theocharis I, et al. A patient with pantothe- 26. P D A S, T Miyatake E O N S, N A S Y N D O M E S Doi H,UKoyano et B al. I Siblings with theRadult-onset slowly progressive type of pantothenate kinase-associated neurodegeneration and a novel mutation, Ile346Ser, in PANK2: clinical U P D A T E O N N B I A S Y N D R O M E S features and (99m)Tc-ECD brain perfusion SPECT findings. J Neurol Sci 2010;290:172–176. degeneration and a novel mutation, Ile346Ser, in PANK2: clinical Kruer MC, M, Gregory et al. Novel histopathologic features and Hiken (99m)Tc-ECD brainA,perfusion SPECT findings. J findingsSciin2010;290:172–176. molecularly-confirmed pantothenate kinase-associated Neurol neurodegeneration. Brain 2011;134:947–958. Kruer MC, Hiken M, Gregory A, et al. Novel histopathologic Saito Y,inKawai M, Inoue K, et al. pantothenate Widespread expression of alphafindings molecularly-confirmed kinase-associated synuclein and tau immunoreactivity in Hallervorden-Spatz syndrome neurodegeneration. Brain 2011;134:947–958. with protracted clinical course. J Neurol Sci 2000;177:48–59. Saito Y, Kawai M, Inoue K, et al. Widespread expression of alphaWakabayashi K,immunoreactivity Fukushima T, Koide R, et al. Juvenile-onset gensynuclein and tau in Hallervorden-Spatz syndrome eralized neuroaxonal (Hallervorden-Spatz disease) with with protracted clinical dystrophy course. J Neurol Sci 2000;177:48–59. diffuse neurofibrillary and Lewy body pathology. Acta NeuropaWakabayashi K, Fukushima T, Koide R, et al. Juvenile-onset genthol 2000;99:331–336. eralized neuroaxonal dystrophy (Hallervorden-Spatz disease) with Neumann M, Adler S,and Schluter et al. Alpha-synuclein accumudiffuse neurofibrillary Lewy O, body pathology. Acta Neuropalation in a case of neurodegeneration with brain iron accumulathol 2000;99:331–336. tion type 1 (NBIA-1, formerly Hallervorden-Spatz syndrome) Neumann M, Adlercortical S, Schluter et al. Alpha-synuclein accumuwith widespread and O, brainstem-type Lewy bodies. Acta lation in a case of neurodegeneration with brain iron accumulaNeuropathol 2000;100:568–574. tion type 1 (NBIA-1, formerly Hallervorden-Spatz syndrome) Galvin JE, Giasson B, Hurtig HI, et al. Neurodegeneration with with widespread cortical and brainstem-type Lewy bodies. Acta brain iron accumulation, type 1 is characterized by alpha-, beta-, Neuropathol 2000;100:568–574. and gamma-synuclein neuropathology. Am J Pathol 2000;157: Galvin JE, Giasson B, Hurtig HI, et al. Neurodegeneration with 361–368. brain iron accumulation, type 1 is characterized by alpha-, beta-, Williamson K, Sima AA, Curry B, et al. Neuroaxonal dystrophy and gamma-synuclein neuropathology. Am J Pathol 2000;157: in young adults: a clinicopathological study of two unrelated 361–368. cases. Ann Neurol 1982;11:335–343. Williamson K, Sima AA, Curry B, et al. Neuroaxonal dystrophy D, Sotrel A, Joachim C, et al. Adult HallervorinEidelberg young adults: a clinicopathological study of onset two unrelated den-Spatz disease 1982;11:335–343. with neurofibrillary pathology. A discrete clinicases. Ann Neurol copathological entity. Brain 1987;110:993–1013. Eidelberg D, Sotrel A, Joachim C, et al. Adult onset HallervorHartig MB, Hortnagel K, Garavaglia pathology. B, et al. Genotypic andclinipheden-Spatz disease with neurofibrillary A discrete notypic spectrum of PANK2 mutations in patients with neurodecopathological entity. Brain 1987;110:993–1013. generation with brain iron accumulation. Ann Neurol 2006;59: Hartig MB, Hortnagel K, Garavaglia B, et al. Genotypic and phe248–256. notypic spectrum of PANK2 mutations in patients with neurodeKotzbauer with PT, Truax JQAnn et al.Neurol Altered2006;59: neuronal generation brain AC, iron Trojanowski accumulation. mitochondrial coenzyme A synthesis in neurodegeneration with 248–256. brain iron accumulation caused by abnormal processing, stability, Kotzbauer PT, activity Truax AC, Trojanowski JQ et al. Altered and catalytic of mutant pantothenate kinase 2. Jneuronal Neurosci mitochondrial coenzyme A synthesis in neurodegeneration with 2005;25:689–698. brain iron accumulation caused by abnormal processing, stability, Lin catalytic MT, Bealactivity MF. Mitochondrial dysfunctionkinase and oxidative stress and of mutant pantothenate 2. J Neurosci in neurodegenerative diseases. Nature 2006;443:787–795. 2005;25:689–698. 3.4. 4. 5. 5. 6. 6. 7. 7.8. 8. 9. 9. 10. 10. 11. 11. 12. 12. 13. 13. 14. 14. 12 31. 10. 15. 15. 16. MDs6-1.indb 1216. 27. 27. 28. 28. 29. 29. 30. 30. 31. 31. 32. 32. 33. 33. 34. 34. 35. 35. 36. 37. Lin PoliMT, M,Beal Derosas M, Luscieti S, et al. Pantothenate 36. MF. Mitochondrial dysfunction and oxidativekinase-2 stress silencing causes cell growth reduction, cell-specific ferroin(Pank2) neurodegenerative diseases. Nature 2006;443:787–795. portin upregulation and iron deregulation. Neurobiol Dis 2010; 12.7.17 4:36:26 PM 37. Poli M, Derosas M, Luscieti S, et al. Pantothenate kinase-2 n iron accumulation: atr Neurol 2006;13: 32. Williamson K, Sima AA, Curry B, et al. Neuroaxonal dystrophy in young adults: a clinicopathological study of two unrelated cases. Ann Neurol 1982;11:335–343. al. Genetic, clinical, en-Spatz syndrome. N 33. Eidelberg D, Sotrel A, Joachim C, et al. Adult onset Hallervorden-Spatz disease with neurofibrillary pathology. A discrete clinicopathological entity. Brain 1987;110:993–1013. Severe tongue protruble treatment. Neurol- 34. l. Clinical and neurowith pantothenate kiv Disord 2005;20: Hartig MB, Hortnagel K, Garavaglia B, et al. Genotypic and phenotypic spectrum of PANK2 mutations in patients with neurodegeneration with brain iron accumulation. Ann Neurol 2006;59: 248–256. 35. Kotzbauer PT, Truax AC, Trojanowski JQ et al. Altered neuronal mitochondrial coenzyme A synthesis in neurodegeneration with brain iron accumulation caused by abnormal processing, stability, and catalytic activity of mutant pantothenate kinase 2. J Neurosci 2005;25:689–698. Neuro-ophthalmologic thenate kinase-associden-Spatz syndrome). patient with pantothend supranuclear gaze –690. Genetic, clinical, and ith late-onset, slowly d neurodegeneration. 36. Lin MT, Beal MF. Mitochondrial dysfunction and oxidative stress in neurodegenerative diseases. Nature 2006;443:787–795. 37. Poli M, Derosas M, Luscieti S, et al. Pantothenate kinase-2 (Pank2) silencing causes cell growth reduction, cell-specific ferroportin upregulation and iron deregulation. Neurobiol Dis 2010; 39:204–210. 38. l. Indian-subcontinent mutations, and unde5:1424–1431. 39. l PANK2 gene mutakinase-associated neuc tremor. Mov Disord 40. 76. Kang SY, Lee M ism in heredita Parkinsonism R Gregory A, Westaway SK, Holm IE, et al. Neurodegeneration associated with genetic defects in phospholipase A(2). Neurology 2008;71:1402–1409. 77. Micheli F, Cer plegia associate 2006;21:716–7 56. Kruer MC, Paisan-Ruiz C, Boddaert N et al. Defective FA2H leads to a novel form of neurodegeneration with brain iron accuSchneider et al. mulation (NBIA). Ann Neurol. 2010;68:610–618. 78. Schicks J, Syno parkinsonism d 25(Suppl 2):S5 57. Schneider SA, Bhatia KP. Three faces of the same gene: FA2H links neurodegeneration with brain iron accumulation, leukodystrophies, and hereditary spastic paraplegias. Ann Neurol 2010; 68:575–577. 79. Anheim M, La paraplegia. A n 256:104–108. 58. Najim al-Din AS, Wriekat A, Mubaidin A, et al. Pallido-pyramidal degeneration, supranuclear upgaze paresis and dementia: Kufor-Rakeb syndrome. Acta Neurol Scand 1994;89:347–352. 80. White KD, Ince ings in heredita rology 2000;55 59. Ramirez A, Heimbach A, Grundemann J, et al. Hereditary parkinsonism with dementia is caused by mutations in ATP13A2, encoding a lysosomal type 5 P-type ATPase. Nat Genet 2006;38: 1184–1191. 81. Potter KA, Ker dysfunction in 1009–1021. 82. 60. Machner B, Sprenger A, Behrens MI, et al. Eye movement disorders in ATP13A2 mutation carriers (PARK9). Mov Disord 2010; 25:2687–2689. McNeill A, Pan tion of cerulo 200–205. 83. Chinnery PF, C and natural hi 460InsA mutat 54. Vinters H, Farrell M, Mischel P, et al. Diagnostic Neuropathology. New York: Marcel Dekker Incorporated; 1998:502. 55. Castelnau P, Cif L, Valente EM, et al. Pallidal stimulation improves pantothenate kinase-associated neurodegeneration. Ann Neurol 2005;57:738–741. 61. Mikati MA, Yehya A, Darwish H, et al. Deep brain stimulation as a mode of treatment of early onset pantothenate kinase-associated neurodegeneration. Eur J Paediatr Neurol 2009;13:61–64. Di Fonzo A, Chien HF, Socal M, et al. ATP13A2 missense mutations in juvenile parkinsonism and young onset Parkinson disease. Neurology 2007;68:1557–1562 84. 62. Williams DR, Hadeed A, al Din AS, et al. Kufor Rakeb disease: autosomal recessive, levodopa-responsive parkinsonism with pyramidal degeneration, supranuclear gaze palsy, and dementia. Mov Disord 2005;20:1264–1271. Chinnery PF. N CR, Stephens K versity of Wash 85. Chinnery PF, C French family 2003;40:e69. 86. Kubota A, Hid gene mutation description of c notype correlat Krause M, Fogel W, Tronnier V, et al. Long-term benefit to pallidal deep brain stimulation in a case of dystonia secondary to pantothenate kinase-associated neurodegeneration. Mov Disord 2006;21:2255–2257. 63. Behrens MI, Bruggemann N, Chana P, et al. Clinical spectrum of Kufor-Rakeb syndrome in the Chilean kindred with ATP13A2 mutations. Mov Disord 2010;25:1929–1937. hand dystonia in a 2008;23:466–468 41. n genetically confirmed eration: a video-poly10:342834. Szumowski J, Bas E, Gaarder K, et al. Measurement of brain iron distribution in Hallevorden-Spatz syndrome. J Magn Reson Imaging 2010;31:482–489. 64. 42. 87. Diffusion tensor MR se-associated neuroded their siblings. AJNR Timmermann L, Pauls KA, Wieland K, et al. Dystonia in neurodegeneration with brain iron accumulation: outcome of bilateral pallidal stimulation. Brain 2010;133:701–712. Schneider SA, Paisan-Ruiz C, Quinn NP, et al. ATP13A2 mutations (PARK9) cause neurodegeneration with brain iron accumulation. Mov Disord 2010;25:979–984. 65. McNeill A, Bir tinguishes four accumulation. 88. 43. Mylius V, Gerstner A, Peters M, et al. Low-frequency rTMS of the premotor cortex reduces complex movement patterns in a patient with pantothenate kinase-associated neurodegenerative disease (PKAN). Neurophysiol Clin 2009;39:27–30. Bruggemann N, Hagenah J, Reetz K, et al. Recessively inherited parkinsonism: effect of ATP13A2 mutations on the clinical and neuroimaging phenotype. Arch Neurol 2010;67:1357–1363. 66. Chien HF, Bonifati V, Barbosa ER. ATP13A2-related neurodegeneration (PARK9) without evidence of brain iron accumulation. Mov Disord 2011;26164–1365. Hautot D, Pan tion of elevate ganglia of neu 2007;1772:21– Rana A, Seinen E, Siudeja K, et al. Pantethine rescues a Drosophila model for pantothenate kinase-associated neurodegeneration. Proc Natl Acad Sci U S A 2010;107:6988–6993. 67. Zittel S, Kroeger T, Baeumer T, et al. Abnormal interhemispheric interactions in ATP13A2 mutation carriers: a TMS study. 14th Annual Meeting of the German Society of Neurogenetics, P3, 2008. 89. 44. Mancuso M, D opathy: a nove insights. J Neu Cranial MRI changes atz syndrome. Pediatr P-CIT SPECT findings ease with homozygous 64:167–168. allervorden-Spatz disNervenarzt 2000;71: s with the adult-onset nase-associated neuro- 45. Wu Z, Li C, Lv S, et al. Pantothenate kinase-associated neurodegeneration: insights from a Drosophila model. Hum Mol Genet S C H2009;18:3659–3672. N E I D E R E T A L . 46. Morgan NV, Westaway SK, Morton JE, et al. PLA2G6, encoding KP, A, neurodegenerative et al. Characterization disordersof S 47. C H aPaisan-Ruiz Nphospholipase E I D E RC, A2, EBhatia T is Amutated L . Li in PLA2G6 as a locus Ann Neurol 2009; with high brain iron. for Natdystonia-parkinsonism. Genet 2006;38:752–754. 65:19–23. 47. Paisan-Ruiz C, Bhatia KP, Li A, et al. Characterization of 48. PLA2G6 Gregory as A,aPolster BJ,dystonia-parkinsonism. Hayflick SJ. Clinical and locus for Anngenetic Neuroldelinea2009; tion of neurodegeneration with brain iron accumulation. J Med 65:19–23. Genet 2009;46:73–80.Movement Disorders, Vol. 27, No. 1, 2012 51 48. Gregory A, Polster BJ, Hayflick SJ. Clinical and genetic delinea49. tion Paisan-Ruiz C, Li A, Schneider SA, et iron al. Widespread Lewy body of neurodegeneration with brain accumulation. J Med and tau accumulation in childhood and adult onset dystonia-parGenet 2009;46:73–80. kinsonism cases with PLA2G6 mutations. Neurobiol Aging 2010 49. Paisan-Ruiz C, Li A, Schneider SA, et al. Widespread Lewy body [Epub ahead of print]. and tau accumulation in childhood and adult onset dystonia-par50. kinsonism Malik I, Turk Mancuso DJ, mutations. et al. Disrupted membrane casesJ,with PLA2G6 Neurobiol Aginghomeo2010 [Epub of print]. stasis ahead and accumulation of ubiquitinated proteins in a mouse model of infantile neuroaxonal dystrophy caused by PLA2G6 50. Malik I, Turk J, Mancuso DJ, et al. Disrupted membrane homeomutations. Am J Pathol 2008;172:406–416. stasis and accumulation of ubiquitinated proteins in a mouse 51. model Adibhatla RM, Hatcher JF. Phospholipase oxygen of infantile neuroaxonal dystrophy A(2): causedreactive by PLA2G6 species, and peroxidation in CNS pathologies. BMB Rep mutations. Amlipid J Pathol 2008;172:406–416. 2008;41:560–567. 51. Adibhatla RM, Hatcher JF. Phospholipase A(2): reactive oxygen 52. species, Adibhatla JF. Lipid oxidation and peroxidation andRM, lipidHatcher peroxidation in CNS pathologies. BMB Rep in CNS health and disease: from molecular mechanisms to 2008;41:560–567. therapeutic opportunities. Antioxid Redox Signal 2010;12: 52. Adibhatla RM, Hatcher JF. Lipid oxidation and peroxidation 125–169. in CNS health and disease: from molecular mechanisms to 53. therapeutic Engel LA, opportunities. Jing Z, O’Brien DE et Redox al. Catalytic Antioxid Signal function 2010;12:of 125–169. PLA2G6 is impaired by mutations associated with Infantile Neuroaxonal Dystrophy but not Dystonia-Parkinsonism. PLoS ONE 53. Engel LA, Jing Z, O’Brien DE et al. Catalytic function of 2011;5:e12897. PLA2G6 is impaired by mutations associated with Infantile Neu54. roaxonal Vinters H, Farrell M, P, et al. Diagnostic NeuropatholDystrophy butMischel not Dystonia-Parkinsonism. PLoS ONE ogy. New York: Marcel Dekker Incorporated; 1998:502. 2011;5:e12897. 55. Vinters GregoryH,A,Farrell Westaway SK, Holm et al. Neurodegeneration 54. M, Mischel P, et IE, al. Diagnostic Neuropatholassociated with Marcel genetic Dekker defects Incorporated; in phospholipase A(2). Neurology ogy. New York: 1998:502. 2008;71:1402–1409. 55. Gregory A, Westaway SK, Holm IE, et al. Neurodegeneration 56. associated Kruer MC, Paisan-Ruiz C, Boddaert N et al. A(2). Defective FA2H with genetic defects in phospholipase Neurology leads to a novel form of neurodegeneration with brain iron accu2008;71:1402–1409. mulation (NBIA). Ann Neurol. 2010;68:610–618. 56. Kruer MC, Paisan-Ruiz C, Boddaert N et al. Defective FA2H 57. leads Schneider SA, Bhatia Three faces of the FA2H to a novel form ofKP. neurodegeneration withsame braingene: iron accumulation (NBIA). Ann Neurol. links neurodegeneration with 2010;68:610–618. brain iron accumulation, leukodystrophies, and hereditary spastic paraplegias. Ann Neurol 2010; 57. Schneider SA, Bhatia KP. Three faces of the same gene: FA2H 68:575–577. links neurodegeneration with brain iron accumulation, leukody58. strophies, Najim al-Din Wriekat A, Mubaidin A, etAnn al. Pallido-pyramiand AS, hereditary spastic paraplegias. Neurol 2010; dal degeneration, supranuclear upgaze paresis and dementia: 68:575–577. Kufor-Rakeb syndrome. Acta Neurol Scand 1994;89:347–352. 58. Najim al-Din AS, Wriekat A, Mubaidin A, et al. Pallido-pyrami59. dal Ramirez A, Heimbach A, Grundemann et al. and Hereditary pardegeneration, supranuclear upgaze J, paresis dementia: kinsonism with dementia caused Scand by mutations in ATP13A2, Kufor-Rakeb syndrome. Actais Neurol 1994;89:347–352. encoding a lysosomal type 5 P-type ATPase. Nat Genet 2006;38: 59. Ramirez A, Heimbach A, Grundemann J, et al. Hereditary par1184–1191. kinsonism with dementia is caused by mutations in ATP13A2, 60. encoding MachneraB,lysosomal Sprenger type A, Behrens et al. Eye disor5 P-typeMI, ATPase. Nat movement Genet 2006;38: 1184–1191. ders in ATP13A2 mutation carriers (PARK9). Mov Disord 2010; 25:2687–2689. 60. Machner B, Sprenger A, Behrens MI, et al. Eye movement disorMDs6-1.indb 13 61. ders Di Fonzo A, Chien HF, Socal M, et(PARK9). al. ATP13A2 mutain ATP13A2 mutation carriers Mov missense Disord 2010; 68. 69. 69. 52 70. 70. 71. 71. 72. 72. 73. 73. 74. 74. 75. 75. 76. 76. 77. 77. 78. 78. 79. 79. 80. 80. 81. 81. 82. 82. 83. 90. Deng X, Vida DNA damage Paisan-Ruiz C, Guevara R, Federoff M, et al. Early-onset L-dopatary ferritinopa responsive parkinsonism with pyramidal signs due to ATP13A2, 91. Kruer M, Greg PLA2G6, FBXO7 and spatacsin mutations. Mov Disord 2010;25: athy of childho 1791–1800 Park JS, Mehta P, Cooper AA, et al. Pathogenic effects of novel mutations in the P-type ATPase ATP13A2 (PARK9) causing Kufor-Rakeb syndrome, a form of early-onset Parkinsonism Hum Park JS, Mehta P, Cooper AA, et al. Pathogenic effects of novel Mutat 2011;32:956–964. Movement Vol. 27, ATPase No. 1, 2012ATP13A2 (PARK9) causing mutations inDisorders, the P-type Kufor-Rakeb syndrome, a formGS, of early-onset Parkinsonism Humin Farias FH, Zeng R, Johnson et al. A truncating mutation Mutat 2011;32:956–964. ATP13A2 is responsible for adult-onset neuronal ceroid lipofuscinosis in Tibetan terriers. Neurobiol Dis 2011;42468–474. Farias FH, Zeng R, Johnson GS, et al. A truncating mutation in ATP13A2 responsible adult-onset ceroid lipofusciDick KJ, is Eckhardt M, for Paisan-Ruiz C, neuronal et al. Mutation of FA2H nosis in Tibetan terriers. Neurobiol 2011;42468–474. underlies a complicated form of Dis hereditary spastic paraplegia (SPG35). Hum Mutat 2010;31:E1251–E1260. Dick KJ, Eckhardt M, Paisan-Ruiz C, et al. Mutation of FA2H underlies a S, complicated spastic in paraplegia Edvardson Hama H, form Shaag ofA, hereditary et al. Mutations the fatty (SPG35). Hum Mutatgene 2010;31:E1251–E1260. acid 2-hydroxylase are associated with leukodystrophy with spastic paraparesis and dystonia. Am J Hum Genet 2008;83: Edvardson S, Hama H, Shaag A, et al. Mutations in the fatty 643–648. acid 2-hydroxylase gene are associated with leukodystrophy with spastic dystonia.DM, Am etJ al. Hum Genet 2008;83: Garoneparaparesis C, Pippucciand T, Cordelli FA2H-related disor643–648. ders: a novel c.270þ3A>T splice-site mutation leads to a complex neurodegenerative phenotype. Dev Med Child Neurol 2011; Garone C, Pippucci T, Cordelli DM, et al. FA2H-related disor53:958–961. ders: a novel c.270þ3A>T splice-site mutation leads to a complex phenotype. Child Neurol 2011;in Brasneurodegenerative J, Singleton A, Cookson MR,Dev et Med al. Emerging pathways 53:958–961. genetic Parkinson’s disease: potential role of ceramide metabolism in Lewy body disease. FEBS J 2008;275:5767–5773. Bras J, Singleton A, Cookson MR, et al. Emerging pathways in genetic Parkinson’s potential role ceramide metabolism Hourani R, El-Hajjdisease: T, Barada WH, et al.ofMR imaging findings in inautosomal Lewy bodyrecessive disease. hereditary FEBS J 2008;275:5767–5773. spastic paraplegia. AJNR Am J Neuroradiol 2009;30:936–940. Hourani R, El-Hajj T, Barada WH, et al. MR imaging findings in autosomal recessive hereditary spastic paraplegia. AJNR Am J Kang SY, Lee MH, Lee SK, et al. Levodopa-responsive parkinsonNeuroradiol 2009;30:936–940. ism in hereditary spastic paraplegia with thin corpus callosum. Parkinsonism Relat Disord 2004;10:425–427. Kang SY, Lee MH, Lee SK, et al. Levodopa-responsive parkinsonism in hereditary spastic paraplegia withHereditary thin corpus callosum. Micheli F, Cersosimo MG, Zuniga RC. spastic paraParkinsonism Relatwith Disord 2004;10:425–427. plegia associated dopa-responsive parkinsonism. Mov Disord 2006;21:716–717. Micheli F, Cersosimo MG, Zuniga RC. Hereditary spastic paraplegia associated withM, dopa-responsive Mov Disord Schicks J, Synofzik Petrusson H, parkinsonism. Bauer P, Schöls L. Juvenile 2006;21:716–717. parkinsonism due to a novel SPG15 mutation. Mov Disord 2010; 25(Suppl 2):S524. Schicks J, Synofzik M, Petrusson H, Bauer P, Schöls L. Juvenile parkinsonism due to a novel SPG15 mutation. Mov Anheim M, Lagier-Tourenne C, Stevanin G, et al. Disord SPG11 2010; spastic 25(Suppl 2):S524. paraplegia. A new cause of juvenile parkinsonism. J Neurol 2009; 256:104–108. Anheim M, Lagier-Tourenne C, Stevanin G, et al. SPG11 spastic paraplegia. newPG, cause of juvenile parkinsonism. Neurol 2009; White KD,AInce Lusher M, et al. Clinical and Jpathologic find256:104–108. ings in hereditary spastic paraparesis with spastin mutation. Neurology 2000;55:89–94. White KD, Ince PG, Lusher M, et al. Clinical and pathologic findings in hereditary paraparesis with NeuPotter KA, Kern spastic MJ, Fullbright G, et al. spastin Centralmutation. nervous system rology 2000;55:89–94. dysfunction in a mouse model of Fa2h deficiency. Glia 2011;59: 1009–1021. Potter KA, Kern MJ, Fullbright G, et al. Central nervous system 13 dysfunction a mouse Fa2h deficiency. Glia 2011;59: McNeill A, in Pandolfo M,model Kuhn of J, et al. The neurological presenta1009–1021. tion of ceruloplasmin gene mutations. Eur Neurol 2008;60: 200–205. McNeill A, Pandolfo M, Kuhn J, et al. The neurological presentation of ceruloplasmin Chinnery PF, Cromptongene DE, mutations. Birchall D, Eur et al.Neurol Clinical2008;60: features 200–205. and natural history of neuroferritinopathy caused by the FTL1 12.7.17 4:36:27 PM 460InsA mutation. Brain 2007;130:110–119. l. Neurodegeneration pase A(2). Neurology 77. t al. Defective FA2H with brain iron accu–618. 78. he same gene: FA2H ccumulation, leukodys. Ann Neurol 2010; et al. Pallido-pyramiaresis and dementia: 1994;89:347–352. et al. Hereditary partations in ATP13A2, . Nat Genet 2006;38: Eye movement disor9). Mov Disord 2010; P13A2 missense mutaset Parkinson disease. Kufor Rakeb disease: arkinsonism with pypalsy, and dementia. . Clinical spectrum of ndred with ATP13A2 . t al. ATP13A2 mutah brain iron accumu- Recessively inherited ns on the clinical and ;67:1357–1363. 3A2-related neurodeain iron accumulation. rmal interhemispheric : a TMS study. 14th of Neurogenetics, P3, l. Early-onset L-dopagns due to ATP13A2, Mov Disord 2010;25: U P D A Micheli F, Cersosimo MG, Zuniga RC. Hereditary spastic paraplegia associated with dopa-responsive parkinsonism. Mov Disord 2006;21:716–717. Schicks J, Synofzik M, Petrusson H, Bauer P, Schöls L. Juvenile parkinsonism due to a novel SPG15 mutation. Mov Disord 2010; 25(Suppl 2):S524. 79. Anheim M, Lagier-Tourenne C, Stevanin G, et al. SPG11 spastic paraplegia. A new cause of juvenile parkinsonism. J Neurol 2009; NBIA 症候群の最新情報 256:104–108. 92. Hartig MB, Iuso A, Hempel M, et al. Identification of a second major locus for neurodegeneration with brain iron accumulation. Presented at the American Society of Human Genetics 59th Annual Meeting, Honolulu, 2009. http://www.ashg.org/2009meeting/abstracts/fulltext/f20691.htm. 93. Brueggemann N, Wuerfel JT, Petersen D, et al. Idiopathic NBIA—clinical spectrum and transcranial sonography findings. Eur J Neurol 2011;18:e58–e59. 80. White KD, Ince PG, Lusher M, et al. Clinical and pathologic findings in hereditary spastic paraparesis with spastin mutation. Neurology 2000;55:89–94. 94. 81. Potter KA, Kern MJ, Fullbright G, et al. Central nervous system dysfunction in a mouse model of Fa2h deficiency. Glia 2011;59: 1009–1021. Waldvogel D, van GP, Hallett M. Increased iron in the dentate nucleus of patients with Friedrich’s ataxia. Ann Neurol 1999;46: 123–125. 95. 82. McNeill A, Pandolfo M, Kuhn J, et al. The neurological presentation of ceruloplasmin gene mutations. Eur Neurol 2008;60: 200–205. Levy M, Turtzo C, Llinas RH. Superficial siderosis: a case report and review of the literature. Nat Clin Pract Neurol 2007;3: 54–58. 96. 83. Chinnery PF, Crompton DE, Birchall D, et al. Clinical features and natural history of neuroferritinopathy caused by the FTL1 460InsA mutation. Brain 2007;130:110–119. Chang MH, Hung WL, Liao YC, et al. Eye of the tiger-like MRI in parkinsonian variant of multiple system atrophy. J Neural Transm 2009;116:861–866. 97. 84. Chinnery PF. Neuroferritinopathy. In: Pagon RA, Bird TD, Dolan CR, Stephens K, eds. GeneReviews [Internet]. Seattle, WA: University of Washington, Seattle; 1993–2005. Davie CA, Barker GJ, Machado C, et al. Proton magnetic resonance spectroscopy in Steele-Richardson-Olszewski syndrome. Mov Disord 1997;12:767–771. 98. 85. Chinnery PF, Curtis AR, Fey C, et al. Neuroferritinopathy in a French family with late onset dominant dystonia. J Med Genet 2003;40:e69. Molinuevo JL, Munoz E, Valldeoriola F, et al. The eye of the tiger sign in cortical-basal ganglionic degeneration. Mov Disord 1999;14:169–171. 99. P DSkoglund A T E L,OLindau N N M, B et I Aal. Frontotemporal S Y N D R O demenM E S SantilloU AF, tia-amyotrophic lateral sclerosis complex is simulated by neurodegeneration with brain iron accumulation. Alzheimer Dis Assoc Disord 2009;23:298–300. 100. Schwarz J, Weis S, Kraft E, et al. Signal changes on MRI and increases in reactive microgliosis, astrogliosis, and iron in the putamen of two patients with multiple system atrophy. J Neurol Neurosurg Psychiatry 1996;60:98–101. 101. Schneider SA, Hardy J, Bhatia KP. Iron Accumulation in syndromes of neurodegeneration with brain accumulation—causative or consequential? J Neurol Neurosurg Psychiatry 2009;80: 589–590. 102. Ogretmen B, Hannun YA. Biologically active sphingolipids in cancer pathogenesis and treatment. Nat Rev 2008;4:616. 103. Birbes H, El Bawabb S, Obeid LM, Hannun YA. Mitochondria and ceramide: intertwined roles in regulation of apoptosis. Advan Enzyme Regul 2002;42:113–129. 86. 92. 87. 88. 93. 94. 89. 95. 90. Kubota A, Hida A, Ichikawa Y, et al. A novel ferritin light chain syndrome): a novel iron accumulagene mutation in a neurodegneration Japanese family with with brain neuroferritinopathy: tion (NBIA) [correspondence]. 2009.for Abstract. description ofphenotype clinical features and implications genotype-phenotype Disord Hartigcorrelations. MB, Iuso A,Mov Hempel M,2009;24:441–445. et al. Identification of a second major locus for neurodegeneration ironFSE accumulation. McNeill A, Birchall D, Hayflick SJ, with et al. brain T2* and MRI disPresented four at thesubtypes American of Human Genetics 59thiron Antinguishes of Society neurodegeneration with brain nual Meeting, Honolulu, 2009. http://www.ashg.org/2009meetaccumulation. Neurology 2008;70:1614–1619. ing/abstracts/fulltext/f20691.htm. Hautot D, Pankhurst QA, Morris CM, et al. Preliminary observaBrueggemann Wuerfel JT, Peterseniron D, oxide et al. Idiopathic tion of elevated N, levels of nanocrystalline in the basal NBIA—clinical spectrum and transcranial sonography findings. ganglia of neuroferritinopathy patients. Biochim Biophys Acta Eur J Neurol 2011;18:e58–e59. 2007;1772:21–25. WaldvogelM,D,Davidzon van GP, Hallett M. Increased iron in the dentate nuMancuso G, Kurlan RM, et al. Hereditary ferritincleus ofa novel patients with Friedrich’s Ann and Neurol 1999;46: opathy: mutation, its cellularataxia. pathology, pathogenetic 123–125.J Neuropathol Exp Neurol 2005;64:280–294. insights. Levy M, C, Englander Llinas RH. EW. Superficial siderosis: of a case report Deng X, Turtzo Vidal R, Accumulation oxidative and review Nat in Clin Practmodel Neurol 2007;3: DNA damage ofin the brainliterature. mitochondria mouse of heredi54–58. tary ferritinopathy. Neurosci Lett 2010;479:44–48. 96. Kruer ChangM, MH, Hung A, WL, Liao YC, et al. EyeS.ofStatic the tiger-like MRI 91. Gregory Hogarth P, Hayflick encephalopin parkinsonian of multiple system atrophy. (SENDA J Neural athy of childhood variant with neurodegeneration in adulthood Transm 2009;116:861–866. syndrome): a novel neurodegneration with brain iron accumula(NBIA) 2009. Abstract. 97. tion Davie CA, phenotype Barker GJ,[correspondence]. Machado C, et al. Proton magnetic resonance MB, spectroscopy in Steele-Richardson-Olszewski 92. Hartig Iuso A, Hempel M, et al. Identification of syndrome. a second Mov Disord 1997;12:767–771. major locus for neurodegeneration with brain iron accumulation. at JL, the Munoz American of Human 59thofAn98. Presented Molinuevo E, Society Valldeoriola F, et Genetics al. The eye the nual Honolulu, 2009. http://www.ashg.org/2009meettigerMeeting, sign in cortical-basal ganglionic degeneration. Mov Disord ing/abstracts/fulltext/f20691.htm. 1999;14:169–171. generation wit Disord 2009;23 syndrome): a novel neurodegneration with brain iron accumulation (NBIA) phenotype [correspondence]. 2009. Abstract. 100. Schwarz J, We increases in re putamen of tw Neurosurg Psy 101. Schneider SA, dromes of neur or consequent 589–590. 102. Ogretmen B, cancer pathoge 103. Birbes H, El B and ceramide: Enzyme Regul 104. Zorzi G, Zibor in patients with (PKAN) treated Mov Disord 20 105. Madsen E, Gi Annu Rev Neu 106. King MW. ht lipids. Accessed 107. Eiberg H, Han widens the sp Genet 2011 [E 104. Zorzi G, Zibordi F, Chiapparini L, et al. Iron-related MRI images U P D A T E O N N B I A S Y N D R O M E S in patients with pantothenate kinase-associated neurodegeneration (PKAN) treated with deferiprone: results of a phase II pilot trial. generation with brain iron accumulation. Alzheimer Dis Assoc Mov Disord 2011;26:1755–1759. Disord 2009;23:298–300. 105. Madsen E, Gitlin JD. Copper and iron disorders of the brain. 100. Schwarz J, Neurosci Weis S, Kraft E, et al. Signal changes on MRI and Annu Rev 2007;30:317–337. increases in reactive microgliosis, astrogliosis, and iron in the 106. putamen King MW. http://www.themedicalbiochemistrypage.org/sphingoof two patients with multiple system atrophy. J Neurol lipids. Accessed June 1996;60:98–101. 2011. Neurosurg Psychiatry 93. N, Wuerfel JT, Petersen D, et al. Idiopathic 99. Brueggemann Santillo AF, Skoglund L, Lindau M, et al. Frontotemporal demenNBIA—clinical and transcranial tia-amyotrophicspectrum lateral sclerosis complex is sonography simulated by findings. neurodeEur J Neurol 2011;18:e58–e59. 107. Schneider Eiberg H, SA, Hansen L, Korbo L, etKP. al. Novel mutation in ATP13A2 101. Hardy J, Bhatia Iron Accumulation in synwidens ofthe spectrum of Kufor-Rakeb (PARK9). Clin dromes neurodegeneration with brain syndrome accumulation—causative Genet 2011 [Epub ahead of print] Accessed June 2011. or consequential? J Neurol Neurosurg Psychiatry 2009;80: 589–590. 94. Waldvogel D, van GP, Hallett M. Increased iron in the dentate nucleus of patients with Friedrich’s ataxia. Ann Neurol 1999;46: 123–125. 102. Ogretmen B, Hannun YA. Biologically active sphingolipids in cancer pathogenesis and treatment. Nat Rev 2008;4:616. 95. Levy M, Turtzo C, Llinas RH. Superficial siderosis: a case report and review of the literature. Nat Clin Pract Neurol 2007;3: 54–58. 103. Birbes H, El Bawabb S, Obeid LM, Hannun YA. Mitochondria and ceramide: intertwined roles in regulation of apoptosis. Advan Enzyme Regul 2002;42:113–129. 96. Chang MH, Hung WL, Liao YC, et al. Eye of the tiger-like MRI in parkinsonian variant of multiple system atrophy. J Neural Transm 2009;116:861–866. 104. 97. Davie CA, Barker GJ, Machado C, et al. Proton magnetic resonance spectroscopy in Steele-Richardson-Olszewski syndrome. Mov Disord 1997;12:767–771. Zorzi G, Zibordi F, Chiapparini L, et al. Iron-related MRI images in patients with pantothenate kinase-associated neurodegeneration (PKAN) treated with deferiprone: results of a phase II pilot trial. Mov Disord 2011;26:1755–1759. 105. Madsen E, Gitlin JD. Copper and iron disorders of the brain. Annu Rev Neurosci 2007;30:317–337. 98. Molinuevo JL, Munoz E, Valldeoriola F, et al. The eye of the tiger sign in cortical-basal ganglionic degeneration. Mov Disord 1999;14:169–171. 106. King MW. http://www.themedicalbiochemistrypage.org/sphingolipids. Accessed June 2011. 107. 99. Santillo AF, Skoglund L, Lindau M, et al. Frontotemporal dementia-amyotrophic lateral sclerosis complex is simulated by neurode- Eiberg H, Hansen L, Korbo L, et al. Novel mutation in ATP13A2 widens the spectrum of Kufor-Rakeb syndrome (PARK9). Clin Genet 2011 [Epub ahead of print] Accessed June 2011. 14 MDs6-1.indb 14 12.7.17 4:36:27 PM 利き手はパーキンソン病の症状優位側と相関する: 系統的レビューとメタアナリシス Handedness Correlates with the Dominant Parkinson Side: A Systematic Review and Meta-analysis Anouk van der Hoorn, BSc, Huibert Burger, MD, PhD, Klaus L. Leenders, MD, PhD, and Bauke M. de Jong, MD, PhD * Department of Neurology, University Medical Center Groningen, University of Groningen, The Netherlands * パーキンソン病(Parkinson’ s disease;PD)では特徴 び PD 症状優位側に関するデータを抽出した。両データ 的な症状の非対称性がみられ,より広範な脳病変のあ の記録はあるが,これらの関連性に言及していない研究 る側の対側に症状が出現する。この興味深い非対称性 については,論文著者に連絡して追加情報を入手した。 は,PD 診断上の疾患定義に含まれているにもかかわら オッズ比を固定効果 Mantel-Haenszel モデルで解析し ず,依然として未解明な点の 1 つである。利き手(脳 た。不均質性および公表バイアスを示す所見はわずか の非対称性に関する一般的指標)と症状優位側との関 であった。電子的検索の結果,10 件の研究(4,405 例 連性は,PD における非対称性の症状発現に関する原因 の非対称性 PD 患者を含む)が特定された。右利き患者 因子を探索する際の糸口となる可能性がある。ただし, のうち, 2,413 例(59.5%)は右側, 1,644 例(40.5%) この潜在的な関連性については未だ議論がある。本研 は左側の PD 症状が優位であった。左利き患者ではこの 究の目的は,利き手と PD 症状優位側との間に関連があ 関係が逆転しており,142 例(40.8%)は右側,206 るか否かを明らかにすることである。我々は,横断的研 例(59.2%)は左側の PD 症状が優位であった。全体 究またはコホート研究を検索し,PD 患者の利き手と症 のオッズ比は 2.13〔95%信頼区間:1.71 ~ 2.66〕で 状発症側が記録されている研究を特定した。PubMed, あった。利き手と PD 症状優位側は相互に強く関連し, EMBASE,Web of Science をデータベースの最初から PD 症状は利き手側に出現しやすいことが明らかになっ 2011 年 2 月 14 日までを対象に検索した。利き手およ た。本稿では,潜在的な原因因子についても考察する。 Movement Disorders, Vol. 27, No. 2, 2012, pp. 206–210 Key Word パーキンソン病,疫学,利き手,メタアナリシス パーキンソン病(Parkinson’ s disease;PD)では特徴的 1972 年であった 5。ただし,この関連性については議論 な症状の非対称性がみられ,より広範な脳病変のある側 が続き,結果が再現されることもあれば 6-9,否定される の対側に症状が出現する 1。この興味深い非対称性は, 場合もあった 4,10,11。 PD 診断上の疾患定義に含まれているにもかかわらず,依 依然として議論が続いていることを受け,本研究では, 然として未解明な点の 1 つである 。利き手は,正常な脳 PD 患者の利き手と症状優位側との関連性に関するメタア の非対称性に関する指標として確立されており ,症状優 ナリシスを,コホート研究と横断的研究を対象として実 位側との潜在的な関連性は,PD の発症に寄与する原因 施した。我々は,利き手と PD 症状発症側との間には関 因子を探索する際の糸口となる可能性がある。利き手と 連があり,右利き患者は右側,左利き患者は左側の PD PD 症状優位側との潜在的な関連性は早くも 1971 年に検 症状が優位である場合が多いという仮説を立てた。 2 3 討されており ,この関連性が初めて裏付けられたのは 4 15 MDs6-1.indb 15 12.7.17 4:36:28 PM 利き手はパーキンソン病の症状優位側と相関する 方 法 5692 records identified through database searching 今回の系統的レビューは,Meta-analysis of Observational Studies in Epidemiology(MOOSE)基準 ,Preferred 12 2086 from pubmed 2430 from embase 1176 from web of science Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)基準 13,Assessment of Multiple Systematic Reviews(AMSTAR)指針 14 に従って実施した。これら 3476 records after duplicates removed 以外のレビューに関するプロトコルは使用しなかった。 検索方法と選択基準 横断的研究またはコホート研究を検索し,一般の孤発 3396 records excluded title-based 79 abstracts of records screened 性 PD 患者集団の利き手と PD 症状優位側が記録されて 53 records excluded いる研究を特定した。PubMed,EMBASE および Web of Science の検索は研究者 1 名(A.H.)と神経内科医 / 研究 者 1 名(B.J.)が実施し,両名が別々のセッションにおい 26 full-text records assessed for eligibility て「handedness または hand または handed または handers」 16 excluded および「Parkinson」をキーワードとして検索した。デー 3 data from same study 9 handedness and/or dominant PD side not registered 2 both registered but not reported nor retrieved from the authors 2 experimental study design with irrelevant data タベースは最初から 2011 年 2 月 14 日までを対象に検索 した。言語による制限は行わなかった。解析対象として 組み入れ可能かどうかは,まず文献の標題,次に要約で 判断した。文献の要約で解析対象としての妥当性が示唆 された場合には, 本文全体から適格性を判断した。さらに, 特 定され た 研 究 の 参 考 文 献と学 会 抄 録(conference 1 additional records identified by hand search abstract)についても手作業で検索した。利き手(右利き および左利き) ,PD 症状優位側,PD 罹病期間,PD 発症 時年齢に関するバイナリデータを抽出した。症状発症側 11 studies included in qualitative synthesis および症状の強い側の両者を PD 症状優位側とみなした。 症状発症側では一般に疾患進行中を通じ,より強い症状 が認められることが知られている 。両利きの被験者や左 1 右対称性の症状を呈する PD 患者は登録に含めなかった。 利き手と PD 症状優位側の評価が記載されていても,両 10 studies included in quantitative synthesis (meta-analysis) Figure 1 文献検索のフローチャート 者の関連性に言及していない研究については,論文著者 に問い合わせた。 ルした全体のオッズ比を算出した。不均質性が問題とな る場合には,変量効果モデルも考慮した。統計解析は 統計解析 RevMan 5.1(Cochrane Collaboration)で実施した。有意 公表バイアスの可能性はファンネルプロットで評価し レベルは両側 P < 0.05 に設定した。 た。オッズ比の不均質性は, χ 検定および I 統計量を用 2 2 いて評価した。Cochrane Collaboration のガイドラインに 基づき,不均質性については,I 2 値が 40%未満の場合は おそらく重要でない,75%を超える場合には注目に値す ると判断した。標準的な Mantel-Haenszel 固定効果モデル を用い,利き手と PD 症状優位側との関連に関するプー 結 果 検討した研究の詳細 電子的な検索の結果,計 3,476 件の文献(重複なし) が特定され,うち 10 件の研究 4,6-11,15-17 がメタアナリシス 16 MDs6-1.indb 16 12.7.17 4:36:28 PM van der Hoorn et al. V A N D E R H O O R N E T A L . 1 解析対象研究および除外研究の特徴 TABLE Table 1. Characteristics of included and excluded studies n Study type 166 X-sect Barrett et al.6 (2010) Reynolds and Locke4 (1971) Sarwar and Lai17 (2010) Stewart et al.16 (2009) Štochl et al.10 (2009) Uitti et al.7 (2005) Van der Hoorn et al.8 (2011) Van Rooden et al.11 (2009) 1015 83 245 425 392 1274 287 258 X-sect X-sect X-sect X-sect X-sect Cohort X-sect X-sect Yust-Katz et al.9 (2008) 260 X-sect Onset side, patient recall and right-left difference >4 on UPDRS-III, chart review Excluded studies Klawans5 (1972) Munhoz et al.18 (2010) Torres et al.19 (2010) 46 270 302 X-sect X-sect X-sect Onset side, chart review Onset side, – Onset side, expert exam Included studies Akerman et al.15 (2010) % Male PD onset age (y) PD duration (y) Current handedness, – – – – Handedness, chart review Handedness, chart review Premorbid handedness, chart review Handedness, – Premorbid write-hand, patients recall Handedness, expert exam Premorbid write-hand, chart review Patient recall premorbid AHI scores �–9 left-handed, and �9 right-handed Write-hand, patients recall 61 74 – 64 59 66 58 66 57 – – 58 56 63 57 49 7 – – 8 10 7 9 12 59 30 7 Handedness, – Handedness, – Handedness, expert exam – 53 58 – 53 58 – 12 6 Dominant PD side criteria Onset and dominant side, patient recall Onset side, chart review Onset side, chart review Onset side, chart review Onset side, patient recall Onset side, patient recall Onset side, expert exam Dominant side, chart review Onset side, chart review Handedness criteria =パーキンソン病,X-sect =横断的研究,AHI = Annett Handedness Inventory,UPDRS = UnifiedDisease Parkinson’ s Disease PD,PD Parkinson’s disease; X-sect ¼ cross-sectional; AHI, Annett Handedness Inventory; UPDRS, Unified Parkinson’s Rating Scale. Rating Scale Main Analysis Pooled results from the fixed effect Mantel-Haenszel の対象として適格であった(Figure 1) 。当初 13 件の研究 model showed that PD patients in general have more を対象として組み入れたが,後に 3 件を除外した。この often PD symptoms on their dominant hand-side. Of the right-handed patients, 2413 (59.5%) had right5 うち 1 件は 1972 年の小規模研究であり ,論文著者と連 and 1644 (40.5%) left-dominant PD symptoms. For 18,19 絡がとれなかった。残りの 2件 は,提供を求めた情 the left-handed patients this relation was reversed with 142 (40.8%) rightand 206 (59.2%) left-dominant 報が論文著者から得られなかったために除外した。解析 PD symptoms. The overall OR showed a marked and 対象とした 件および除外した 3 件の研究の特徴を statistically 10significant association (2.13; 95% confidence1 に示す。 interval, 1.71–2.66; P < .0001). Table 対象とした 10 件の研究では,4,405 例の非対称性 PD Publication Bias and Heterogeneity 患者が検討されていた。このうち 2,555 例(58%)の患 The funnel plot did not reveal indications of a publication bias, as no major asymmetry was shown except 者は右側の PD 症状が優位であり,1,850 例(42%)は左 the single outlier constituted by a small negative study4 (Supporting Fig. 1). Neither was a significant 公表バイアスおよび不均質性 heterogeneity present, based upon study characteristics, the forest plot (Fig. 2) and statistical analysis ファンネルプロットで公表バイアスの存在は示されず, by Reynolds (P ¼ 0.12; I2 ¼ 36%). Again, the study 4 1and 件の小規模研究(結果はネガティブ) による単一の外 but the Locke4 showed an opposite relationship CI was large and included 1.00. れ 値 を 除 き, 大 き な 非 対 称 性 は 認 め ら れ な か っ た (Supporting Figure 1) 。研究の特徴,フォレストプロット Discussion (Figure 2) ,統計解析( P = 0.12,I 2 = 36%)に基づき, 有意な不均質性も示されなかった。Reynolds Locke4 の By using the statistical strategy of a とsystematic meta-analysis, we were able to demonstrate a substan研究では,逆方向の関連性が示唆されたが,信頼区間は tial and statistically significant association between the 大きく,1.00 を含んでいた。 dominant side of PD symptoms and hand-dominance. Right-handed patients showed a significant excess of 考 察 側の症状が優位であった。利き手については 4,057 例 (92.1%)が右利き,348 例(7.9%)が左利きであった。 系統的メタアナリシスという統計手法を用いることで, 主要解析 PD 症状優位側と利き手との間に実質的かつ統計学的に Mantel-Haenszel 固定効果モデルで得られたプール結果 有意な関連があることが実証できた。右利き患者の PD から,PD 患者は一般に利き手側に PD 症状を伴う場合が 症状は右側が強い場合が有意に多く,この逆についても 多いことが示された。右利き患者のうち, 2,413 例(59.5%) 同様で,左利き患者の PD 症状は左側が強い場合が有意 は右側, 1,644 例(40.5%)は左側の PD 症状が優位であっ に多かった。以前からこの関連性の存在については議論 た。左利き患者ではこの関係が逆転しており,142 例 されてきた。この関連性の存在を報告する既発表研究は (40.8%)は右側,206 例(59.2%)は左側の PD 症状が優 少なく 5-9,その一方で,この関連性を示せなかった研究 位であった。全体のオッズ比では,著明かつ統計学的に もあった 4,10,11。しかし,逆方向の関連性,すなわち,利 FIG. 2. Forest plot of handedness and dominant PD side. Pooled results of distribution of PD side for right-handed and left-handed patients are shown. PD, Parkinson’s(2.13, disease;95%信頼区間 PD.R, PD with:right-sided symptom dominance; PD.L, PD with left-sided symptom dominance; R-handed, き手と症状の非優位側とが関連することを報告する研究 有意な関連が認められた 1.71 ~ 2.66, right-handed; L-handed, left-handed; M-H, Mantel-Haenszel; CI, confidence interval. P < 0.0001) 。 もなく,この事実そのものが既に非偶然性(nonchance relation)を示していると考えられる。 208 Movement Disorders, Vol. 27, No. 2, 2012 17 MDs6-1.indb 17 12.7.17 4:36:29 PM 利き手はパーキンソン病の症状優位側と相関する Study Akerman (2008) Barrett (2010) Reynolds (1971) Sawar (2010) Stewart (2009) Štochl (2009) Uitti (2005) Van der Hoorn (2011) Van Rooden (2009) Yust-Katz (2008) R-handed PD.R PD.L 70 78 524 403 36 43 69 154 238 153 218 168 739 439 96 158 129 104 132 106 L-handed PD.R PD.L 8 10 51 37 0 4 14 8 23 11 4 2 62 34 18 15 13 12 13 9 Total (95% Cl) Percentage % 2413 1644 59.5 40.5 142 206 40.8 59.2 Odds Ratio Weight M-H, Fixed, 95% Cl 3.3% 0.89 [0.33-2.38] 23.3% 1.79 [1.15-2.79] 0.2% 0.13 [0.01-2.54] 7.8% 3.91 [1.57-9.74] 11.4% 3.25 [1.54-6.86] 2.0% 2.60 [0.47-14.34] 31.8% 3.07 [1.99-4.74] 8.8% 1.98 [0.95-4.10] 5.7% 1.34 [0.59-3.07] 5.8% 1.80 [0.74-4.37] 100% Heterogeneity: Chi2 = 14.06, df = 9 (p = 0.12); I2 = 36% Test for overall effect: Z = 6.66 (p < 0.0001) Odds Ratio M-H, Fixed, 95% Cl 2.13 [1.71-2.66] 0.05 0.02 1 5 20 Figure 2 利き手と PD 症状優位側のフォレストプロット。右利きおよび左利き患者における PD 症状優位側の分布に関するプール結果。PD =パーキンソン病,PD.R =右側症状優位の PD,PD.L =左側症状優位の PD,R-handed =右利き,L-handed =左利き,M-H = MantelHaenszel,CI =信頼区間 今回のメタアナリシスでは方法論的問題(これが研究 議を唱える論拠ともなっている。 間の結果の不一致を引き起こしてきた可能性がある)が このように優位半球は PD の影響を受けやすいと考え 解決されている。既発表研究では左利き患者の数が少な られ,この結果を受け,明確な原因因子の特定が次の課 く,これが利き手と症状優位側は無関係であると報告さ 題となるであろう。PD 症状の左右差は現在のところ未解 れてきた主要原因の 1 つであろう。人口全体では約 10% 明な点の 1 つであるが,本研究で実際に示された利き手 が左利きと推定されるが ,これは今回のメタアナリシ との関連性から,可能性のある因果関係について仮説を スで左利き患者が 8%であったことと矛盾しない。右利き 立てる機運が大きく高まった。この点に関しては,利き 患者と左利き患者のオッズを比べる際,既発表研究のオッ 手に伴う運動コントロールの左右差について次の 2 つの ズ比は,例数が少なく精度に欠ける左利き患者群による 一般的な因果関係を考慮できる。すなわち, (1)左右ど 影響を大きく受けている。このような患者数の少なさが, ちらかの手の優先的な使用は,左右一方の代謝的要求の 統計学的検出力の低下を招いている。今回のメタアナリ 増加を意味し,対応する(対側の)脳半球では酸化的ス シスでは,結果をプールすることにより,これらの問題 トレスによる負の影響が生じている可能性がある 21。また, 20 が解決されている。 (2)基礎にある大脳皮質-大脳基底核-視床回路は優位 試験方法に関連する研究の質は,解析対象研究間で同 様であった。PD 症状優位側および利き手の評価法の違 いにより,小さな差が生じた可能性はある。利き手は, 半球内に広く分布し,言語ネットワークと高度な並列関 係を保ちながら機能している 22-24。 生化学的な特徴に関して言えば,酸化的ストレスの増 PD 発症前(premorbid)の利き手に関する患者の記憶ま 加は,興奮性神経伝達物質 25,26 やドパミン代謝物 21 によ たは診療録の調査により判断された。PD 症状優位側につ る神経毒性に寄与する可能性がある。利き手に関連する いては,初発症状が報告された側に基づく場合が最も多 優位半球の機能には,特に腹側頭頂前運動領域と上側頭 かったが,1 件の研究 では,症状が常により強く報告さ 領域の回路が関与し 27,これらの各領域はさらに線条体 れた側に基づいて推測されていた。PD 症状発症側と症 に投射する 28。この投射により大脳皮質-大脳基底核の 状優位側という 2 つの変数は互いに強く相関する。この 相互作用が維持され,皮質機能の統合が促進される。大 ことは,症状発症側では一般にその後の疾患進行中を通 脳皮質-大脳基底核の相互作用では,大脳基底核を介し じ,より強い症状が認められるという事実から明らかに て分離したチャネルが生じるのに対し 29,緊密に相互接 されている 1。また,この相関性は,患者が,利き手を使 続した皮質野は,より共通性の高い線条体投射を行う 30。 う際の PD 症状により早く気付きやすいという仮説(作業 したがって,優位半球における大脳基底核の活動亢進は, 関連の運動には利き手がより大きく関与するため)に異 理論上,この半球の機能的ネットワークがより拡張して 8 18 MDs6-1.indb 18 12.7.17 4:36:29 PM A N D E D N E S S the reverse was ith a significant existence of this previous studies s others failed to ever, reported an tween dominant symptoms. This hance relation. methodological repancy between nded patients in n a major reason between handednce. In the overated to be left8% left-handed . When compared patients, the fluenced by the handed patients. ack of statistical nt meta-analysis uded studies was isen by differensymptoms and ed either by the ness or by chart D side was most onset, while in 1 istently reported highly correlate own by the fact ains the worst ion.1 Moreover, ative assumption ms earlier when s stronger impli- pears to be more ct causal factors lateralization of of a mystery, the rovides a strong oncerning possie may consider 2 motor control reference implies possible negative he corresponding underlying cortihas an extensive isphere and runs .22–24 characteristics, ribute to neuro- A N D T H E D O M I N A N T P A R K I N S O N S I D E toxicity inflicted by excitatory neurotransmitters25,26 as well as dopamine metabolites.21 Circuitry involved in the referred dominant hemisphere functions comprises particularly ventral parietal-premotor and supeいることに起因すると考えられる。皮質線条体投射は興 rior temporal regions,27 while each of such regions has additional striatum projection.28 Coherent cortical 奮性であり,これは黒質に達する視床下核(subthalamic functioning is facilitated by the cortico-basal ganglia 31,32 nucleus;STN)投射でも維持されている 。これらの結 interactions maintained by these projections. The latter give rise to segregated channels through the basal 果,より広範に拡張した皮質線条体投射に伴う興奮性活 ganglia29 while strongly interconnected cortical fields 動や,場合によっては,黒質に収束するより強力な興奮 have more common striatum projection.30 Enhanced 性負荷により,徐々に興奮毒性作用が生じる可能性があ basal ganglia activity in the dominant hemisphere may thus logically result from the wider extension of funcる。結果として,優位半球では劣位半球に比べて強いド tional networks in this hemisphere. Corticostriatal パミン作動系異常が生じている可能性がある。ただし, projections are excitatory, which also holds for subthalamic nucleus (STN) projections to the substantia STN による黒質の神経支配は特に黒質網様部に関係し, nigra.31,32 As a consequence, the excitatory drive asso線条体への遠心性線維の起始部である黒質緻密部には関 ciated with more widely extended corticostriatal projections and possibly stronger excitatory load 係しない。正常な運動の左右差は,優位半球の黒質線条 converging onto the substantia nigra might lead to 体ドパミンターンオーバーレベル上昇に関連するという excitotoxic effects in the long run of life. This might 33 主要仮説は,ヒトでの PET による in defect vivo イメージング result in a stronger dopaminergic in the dominant compared to the nondominant hemisphere, で支持されている。この点に関連し,ドパミン細胞数に although the STN innervation of the substantia nigra も非対称性があることが推測される。 particularly concerns the pars reticulare and not the pars compacta from which the striatum efferents originate. The primary assumption that normal motor lat結 論 eralization is associated with an increased level nigrostriatal dopamine turnover in the dominant hemiV A N finds D E Rsupport H O O by R Nhuman E T A . sphere inL vivo measurements 結論として,今回の研究により,利き手と PD33症状の One with positron emission tomography (PET). 6. Barrett MJ, Wylie SA, Harrison MB, Wooten GF. Handedness and 左右差との関連性が実証された。このことから,PD might, in this respect, eveninspeculate find J asymmetmotor symptom asymmetry Parkinson’s to disease. Neurolの発 Neurosurg Psychiatry 2011;82:1122–1124. ric dopamine cell count. 症に寄与する原因因子の特定という新たな課題が提示さ V A N D E R H O O R N E T A L . 6. Barrett MJ, Wylie SA, Harrison MB, Wooten GF. Handedness and motor symptom asymmetry in Parkinson’s van disease. NeuroletNeuder JHoorn al. rosurg Psychiatry 2011;82:1122–1124. 19. Torres L, Nunex cal features of a ease. Mov Disor 7. Uitti RJ, Baba Y, Whaley NR, Wszolek ZK, Putzke JD. Parkinson disease—handedness predicts asymmetry. Neurology 2005;64:1925–1930. 20. Perelle IB, Ehrm 343–350. 8. Van der Hoorn A, Bartels AL, Leenders KL, De Jong BM. Handedness and dominant side of symptoms in Parkinson’s disease. Parkinsonism Relat Disord 2011;17:58–60. 21. Jenner P. Oxid 2003;53(Suppl 3 22. 9. Yust-Katz S, Tesler D, Treves TA, Melamed E, Djaldetti R. Handedness as a predictor of side of onset of Parkinson’s disease. Parkinsonism Relat Disord 2008;14:633–635. Johnson-Frey SH Trends Cogn Sc 23. Potgieser AR, d balances in righ premotor cortex 24. Binkofski F, Bu Brain Lang 2004 25. Atlante A, Calis ella S. Glutamat FEBS Lett 2001; 26. Choi DW. Glut system. Neuron 27. Ramayya AG, G ral substrates su 28. Kemp JM, Pow Brain 1970;93:5 29. Alexander GE, C glia circuits: neu rosci 1990;13:26 30. Yeterian EH, V rhesus monkey: tions. Brain Res 31. DeLong MR, W basal ganglia. A 32. Obeso JA, Mari Parkinson’s dise tions. Ann Neur 33. De la Fuente-Fe AJ. Nigrostriata Brain Res 2000; 10. Štochl J, Hagtvet KA, Brozova H, Klempir J, Roth J, Ruzicka E. Handedness does not predict side of onset of motor symptoms in Parkinson’s disease. Mov Disord 2009;24:1836–1839. 11. Van Rooden SM, Visser M, Verbaan D, Marinus J. Handedness associated to side of onset of Parkinson’s disease? Parkinsonism Relat Disord 2009;15:546–547. 12. Stroup DF, Verlin Ja, Moton SC, et al. Meta-analysis of observational studies in epidemiology; a proposal for reporting. JAMA 2000;283:2008–2012. 13. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097. 14. Shea BJ, Hamel C, Wells GA, et al. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol 2009;62:1013–1020. 15. Akerman C, McElwaine T, Gordon C, Roberts HC. Is there a relationship between handedness, side of onset or worst affected side and the use of cueing methods in patients with Parkinson’s disease? Age Aging 2008;37(Suppl 1):i42. [Abstract] 16. Stewart KC, Fernandez HH, Okun MS, Rodriguez RL, Jacobson CE, Hass CJ. Side onset influences motor impairments in Parkinson disease. Parkinsonism Relat Disord 2009;15:781–783. 17. Sarwar AI, Lai EC. Handedness and Parkinson’s disease. Mov Disord 2010;25(Suppl 2):S363. [Abstract] 18. Munhoz R, Espay A, Morgante F, et al. Effect of handedness and side of onset on survival in Parkinson’s disease. Neurology 2010; 74(Suppl 2):A60. [Abstract] 19. Torres L, Nunex Y, Cosentino C. Some clinical and epidemiological features of a Peruvian cohort of patients with Parkinson’s disease. Mov Disord 2010;25(Suppl 2):S254. [Abstract] 20. Perelle IB, Ehrman L. On the other hand. Behav Genet 2005;35(3): 343–350. 21. Jenner P. Oxidative stress in Parkinson’s disease. Ann Neurol 2003;53(Suppl 3):S26–S38. 22. Johnson-Frey SH. The neural bases of complex tool use in humans. Trends Cogn Sci 2004;8:71–78. 23. Potgieser AR, de Jong BM. Different distal-proximal movement balances in right- and left-hand writing may hint at differential premotor cortex involvement. Hum Mov Sci Epub (in press). 24. Binkofski F, Buccino G. Motor functions of the Broca’s region. Brain Lang 2004;89:362–369. additional data oftotheir A. of vanParkinson’s der Hoorn disease? had full access to all associated sidestudies. of onset Parkinsonism 25. data and the accuracy of the data analysis. 12. Stroup DF, Verlin Ja, Moton SC, et al. Meta-analysis of observational studies in epidemiology; a proposal for reporting. JAMA REFERENCES 2000;283:2008–2012. Atlante A, Calissano P, Bobba A, Giannattasio S, Marra E, Passarella S. Glutamate neurotoxicity, oxidative stress and mitochondria. FEBS Lett 2001;497:1–5. 26. Choi DW. Glutamate neurotoxicity and diseases of the nervous system. Neuron 1988;1:623–634. 27. Ramayya AG, Glasser MF, Rilling JK. A DTI investigation of neural substrates supporting tool use. Cereb Cortex 2010;20:507–516. 28. Kemp JM, Powell TPS. The cortico-striate projection in monkey. Brain 1970;93:525–546. 29. Alexander GE, Crutcher MD. Functional architecture of basal ganglia circuits: neural substrates of parallel processing. Trends Neurosci 1990;13:266–271. 30. Yeterian EH, Van Hoesen GW. Cortico-striate projections in the rhesus monkey: the organization of certain cortico-caudate connections. Brain Res 1978;139:43–63. 31. DeLong MR, Wichmann T. Circuits and circuit disorders of the basal ganglia. Arch Neurol 2007;64:20–24. 7. Uitti RJ, Baba Y, Whaley NR, Wszolek ZK, Putzke JD. Parkinson dis- ease—handedness predicts asymmetry. Neurology 2005;64:1925–1930. れている。 8. Conclusions Van der Hoorn A, Bartels AL, Leenders KL, De Jong BM. Handedness and dominant side of symptoms in Parkinson’s disease. ParRelatthe Disord 2011;17:58–60.association between To kinsonism conclude, demonstrated 謝 辞 9. Yust-Katz and S, Tesler D, Treves TA, Melamed Djaldetti R. is Handhandedness lateralization of PD E, symptoms a edness as a predictor of side of onset of Parkinson’s disease. ParProf. Ryanprovides J. Relat Uitti,Prof. Helen C. Roberts,Dr. Stephanie M. fact that a new challenge to identify causal kinsonism Disord 2008;14:633–635. factors contributing to Brozova the onset of PD.J, Roth J, RuzickaA.E. van に対し, 各研究の追加データの提供に感謝する。 10. Rooden Štochl J, Hagtvet KA, H, Klempir Handedness does not predict side of onset of motor symptoms in van derParkinson’s Hoorn は,本研究のすべてのデータを完全に入手して disease. Mov Disordlike 2009;24:1836–1839. Acknowledgments: We would to thank Prof. Ryan J. Uitti, Prof. C. Roberts, Dr. Stephanie M. D, vanMarinus Rooden J. forHandedness providing 11. Helen Van Rooden SM,and Visser M, Verbaan おり,データの完全性およびデータ解析の正確性について責 任を負う。 of the Relat data in the study and takes responsibility for the integrity of the Disord 2009;15:546–547. References 13. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Pre1. Pirker Correlation dopamine transporter with parferredW. reporting itemsoffor systematic reviews imaging and meta-analyses: kinsonian motor handicap: is it? Mov Disord 2003; the PRISMA statement. PLoShow Medclose 2009;6:e1000097. 18(Suppl 7):S43–S51. 14. Shea BJ, Hamel C, Wells GA, et al. AMSTAR is a reliable and 2. Djaldetti R, Ziv I, Melamed E. The of motor asymmetry valid measurement tool to assess the mystery methodological quality of sysintematic Parkinson’s disease. Neurol 2006;5:796–802. reviews. J ClinLancet Epidemiol 2009;62:1013–1020. 3. Liu H, Stufflebeam SM, Sepulcre J, C, Hedden T, HC. Buckner RL.a Evi15. Akerman C, McElwaine T, Gordon Roberts Is there reladence from intrinsichandedness, activity thatside asymmetry human brainside is tionship between of onset of orthe worst affected controlled by multiple factors. Neuroscience 2009;106: and the use of cueing methods in patients with Parkinson’s disease? 20499–20503. Age Aging 2008;37(Suppl 1):i42. [Abstract] 4. Reynolds LM, Fernandez Locke S. Relation between handednessRL, andJacobson side of 16. Stewart KC, HH, Okun MS, Rodriguez onset of Parkinsonism. Lancet 1971;298:714. CE, Hass CJ. Side onset influences motor impairments in Parkinson disease. 2009;15:781–783. HL. HRelation between and side of onset of V5.A NKlawans D E Parkinsonism R O O RRelat N Disord E Thandedness A L . Lancet 1972;299:850. 17. parkinsonism. Sarwar AI, Lai EC. Handedness and Parkinson’s disease. Mov Dis6. 18. 7. ord 2010;25(Suppl 2):S363. [Abstract] Barrett MJ, Wylie SA, Harrison MB, Wooten GF. Handedness and motor symptom asymmetry in Parkinson’s disease. J Neurol NeuMunhoz R, Espay A, Morgante F, et al. Effect of handedness and rosurg Psychiatry 2011;82:1122–1124. side of onset on survival in Parkinson’s disease. Neurology 2010; Movement Disorders, Vol.Putzke 27, No. JD. 2, 2012 74(Suppl 2):A60. [Abstract] Uitti RJ, Baba Y, Whaley NR, Wszolek ZK, Parkinson209 disease—handedness predicts asymmetry. Neurology 2005;64:1925–1930. 8. Van der Hoorn A, Bartels AL, Leenders KL, De Jong BM. Handedness and dominant side of symptoms in Parkinson’s disease. Parkinsonism Relat Disord 2011;17:58–60. 9. Yust-Katz S, Tesler D, Treves TA, Melamed E, Djaldetti R. Handedness as a predictor of side of onset of Parkinson’s disease. Parkinsonism Relat Disord 2008;14:633–635. 10. 11. MDs6-1.indb 19 12. Štochl J, Hagtvet KA, Brozova H, Klempir J, Roth J, Ruzicka E. Handedness does not predict side of onset of motor symptoms in Parkinson’s disease. Mov Disord 2009;24:1836–1839. Van Rooden SM, Visser M, Verbaan D, Marinus J. Handedness associated to side of onset of Parkinson’s disease? Parkinsonism Relat Disord 2009;15:546–547. Stroup DF, Verlin Ja, Moton SC, et al. Meta-analysis of observa- 32. Obeso JA, Marin C, Rodriguez-Oroz C, et al. The basal ganglia in Parkinson’s disease: current concepts and unexplained observations. Ann NeurolY,2008;64(suppl 19. Torres L, Nunex Cosentino C. 2):S30–S46. Some clinical and epidemiological features of a Peruvian cohort of patients with Parkinson’s dis33. De la Fuente-Fernández R, Kishore A, Calne DB, Ruth TJ, Stoessl ease. Mov Disord 2010;25(Suppl 2):S254. [Abstract] AJ. Nigrostriatal dopamine system and motor lateralization. Behav Brain Res 2000;112:63–68. 20. Perelle IB, Ehrman L. On the other hand. Behav Genet 2005;35(3): 210 343–350. Movement Disorders, Vol. 27, No. 2, 2012 21. Jenner P. Oxidative stress in Parkinson’s disease. Ann Neurol 2003;53(Suppl 3):S26–S38. 22. Johnson-Frey SH. The neural bases of complex tool use in humans. Trends Cogn Sci 2004;8:71–78. 23. Potgieser AR, de Jong BM. Different distal-proximal movement balances in right- and left-hand writing may hint at differential premotor cortex involvement. Hum Mov Sci Epub (in press). 24. Binkofski F, Buccino G. Motor functions of the Broca’s region. Brain Lang 2004;89:362–369. 25. Atlante A, Calissano P, Bobba A, Giannattasio S, Marra E, Passarella S. Glutamate neurotoxicity, oxidative stress and mitochondria. FEBS Lett 2001;497:1–5. 19 12.7.17 4:36:30 PM 剖検で確認されたパーキンソン病および多系統萎縮症における ドパミントランスポーターイメージング所見 Dopamine Transporter Imaging in Autopsy-Confirmed Parkinson’s Disease and Multiple System Atrophy *, ** Laura D. Perju-Dumbrava, MD, Gabor G. Kovacs, MD, Susanne Pirker, MD, Kurt Jellinger, MD, Martha Hoffmann, MD, Susanne Asenbaum, MD, and Walter Pirker, MD * Institute of Neurology, Medical University of Vienna, Vienna, Austria Department of Neurology, Medical University of Vienna, Vienna, Austria ** ドパミントランスポーター SPECT では,パーキンソン められた。線条体全体の結合率(平均値)は,多系統 病および多系統萎縮症におけるドパミン作動性神経変 萎縮症患者群で 53%,パーキンソン病患者群で 52% 性の画像化が可能である。いくつかの研究では,ドパミ 低下していた。多系統萎縮症患者群の線条体における ントランスポーターイメージングで両疾患の鑑別が可能 結合の非対称性は,パーキンソン病患者群に比べて顕 であり,線条体のドパミントランスポーターの結合の低 著である傾向がみられ(23 ± 15% 対 10.5 ± 7%, 下は,パーキンソン病患者に比べて多系統萎縮症患者 P = 0.071) ,多系統萎縮症患者 3 例の線条体における においてより広範囲かつ対称的であることが示唆されて 結合の非対称性は,どのパーキンソン病患者よりも顕著 いる。本研究では,線条体のドパミントランスポーター であった。被殻 / 尾状核の結合比に群間差はなかった。 の分布パターンを,剖検で確認されたパーキンソン病お 本研究は,剖検で確認された多系統萎縮症とパーキン よび多系統萎縮症において比較した。剖検で多系統萎 ソン病においてドパミントランスポーターイメージング 縮症(6 例)またはパーキンソン病(8 例)と診断され, 所見を比較した初めてのものである。意外なことに,線 生前ドパミントランスポーターイメージングを受けてい 条体における結合の非対称性は,パーキンソン病患者 た患者を対象とした。イメージング実施時点の平均罹病 よりも多系統萎縮症患者でより顕著である傾向が認めら 期間は,多系統萎縮症患者群 3.6 年,パーキンソン病 れた。本研究の知見から,両疾患の鑑別は,線条体ドパ 患者群 4.1 年であった。画像解析の結果,すべての患 ミントランスポーター結合の亜領域解析では不可能であ 者で両側性のドパミントランスポーター結合の低下が認 ることが明らかになった。 Movement Disorders, Vol. 27, No. 1, 2012, pp. 65–71 Key Word ドパミントランスポーター,SPECT,パーキンソン病,多系統萎縮症,ドパミン作動性神経変性 20 MDs6-1.indb 20 12.7.17 4:36:30 PM Abstract PD 1 2 5 6 3 4 7 8 9 10 11 12 13 14 MSA Figure 1 患者 14 例の 123I-β-CIT を用いたドパミントランスポーター SPECT 所見。線条体レベルの代表的な横断像。 21 MDs6-1.indb 21 12.7.17 4:36:31 PM レボドパ誘発性ジスキネジアを伴うパーキンソン病における 運動課題遂行中の前頭前野 fMRI 所見の変化 Prefrontal Alterations in Parkinson’s Disease with Levodopa-Induced Dyskinesia During fMRI Motor Task * Antonio Cerasa, PhD, Pierfrancesco Pugliese, MD, Demetrio Messina, MD, Maurizio Morelli, MD, Maria Cecilia Gioia, PhD, Maria Salsone, MD, Fabiana Novellino, MD, Giuseppe Nicoletti, MD, Gennarina Arabia, MSc, and Aldo Quattrone, MD * Neuroimaging Research Unit, Institute of Neurological Sciences, National Research Council, Germaneto (CZ), Italy レボドパ(L—ドパ)誘発性ジスキネジアは,パーキンソ 行中に行動の差は認められなかったが,MRI を解析し ン病(Parkinson’ s disease; PD)治療を目的としたド た結果, 標的とした皮質領域に有意な変化が検出された。 パミン作動薬の長期投与による合併症で,患者の日常生 特に,L—ドパ誘発性ジスキネジアを伴う PD 患者では, 活に支障を来たす。最近,我々のグループは,L—ドパ誘 伴わない PD 患者に比べ,補足運動野の有意な活動亢 発性ジスキネジアを伴う PD 患者の特徴として,下前頭 進と右下前頭前回の有意な活動低下が両課題遂行中に 前回に異常な容積変化がみられることを報告した。本研 認められた。さらに,これらの前頭前野の機能変化は, 究では,この構造的異常と機能との関連性を機能的磁気 Abnormal Involuntary Movement Scale のスコアと有 共鳴画像(fMRI)で探索した。ジスキネジアを伴う PD 意に相関した。今回の fMRI 研究は,我々が以前に報告 患者 10 例およびジスキネジアのない PD 患者 10 例の した容積変化の所見とともに,ニューロンレベルのジス 「off 期」に,外的および内的なきっかけによる視覚運動 キネジア発症機序における前頭前皮質の役割を強調す 課題遂行中の fMRI を撮像した。どちらの群でも課題遂 るものである。 Movement Disorders, Vol. 27, No. 3, 2012, pp. 364–371 contrast estimate at [42, 32, 12] Key Word パーキンソン病,レボドパ誘発性ジスキネジア,機能的磁気共鳴画像(fMRI),下前頭前回,補足運動野 1 0 Figure 3 患者群による主要効果の結果。L—ドパ誘発性ジスキ -1 -2 -3 -4 Dyskinetic (EXT) Dyskinetic (INT) Non-Dyskinetic Non-Dyskinetic (EXT) (INT) ネジアを伴う患者では,伴わない患者に比べ,右下前頭前回の 活動亢進が認められる(課題の内容とは無関係) 。各領域につい てコントラスト〔外的なきっかけによる課題(EXT)>安静時, 内的なきっかけによる課題(INT)>安静時〕のパラメータ推定 値を患者群ごとにプロットしている。 22 MDs6-1.indb 22 12.7.17 4:36:31 PM Abstract contrast estimate at [-8, 4, 56] 8 6 4 2 0 -2 -4 Dyskinetic (EXT) Dyskinetic (INT) Non-Dyskinetic Non-Dyskinetic (EXT) (INT) Figure 2 患者群による主要効果の結果。L—ドパ誘発性ジスキネジアを伴う患者では,伴わな い患者に比べ,特に補足運動野に活動亢進が認められる(課題の内容とは無関係) 。各領域に ついてコントラスト〔外的なきっかけによる課題(EXT)>安静時,内的なきっかけによる課 題(INT)>安静時〕のパラメータ推定値を患者群ごとにプロットしている。機能的変化の空 間的位置をより明確に示すため,独自のソフトウェア(BrainShow,MatLab v. 5.3 で作成)32 を 用い,Montreal Neurological Institute(MNI)標準脳(single-subject brain)の明確な解剖学的区 画に基づく解剖学的脳画像に統計学的マップを重ねた 18。緑色の線は補足運動野の解剖学的 位置を,青色の線は前補足運動野を含む内側上前頭回(BA 8)の境界を示す。 [参考文献リストはオンライン版(http://onlinelibrary.wiley.com)で閲覧可能] Response at [40; 37; 11] Response at [-2; 4; 58] 2 1.8 1.6 1.4 1.2 1 0.8 6 7 8 9 AIMS 10 11 12 -0.25 -0.35 -0.45 -0.55 -0.65 -0.75 -0.85 6 7 8 9 AIMS 10 11 12 Figure 4 ジスキネジアを伴う PD 患者群における脳シグナル強度と Abnormal Involuntary Movement Scale(AIMS)スコアとの有意な相関。 下段の散布図は,外的なきっかけによる運動課題(EXT)遂行中の補足運動野(左図)/ 右下前頭前回(右図)における全ボクセルの平 均シグナル変化(y 軸)と AIMS スコア(x 軸)の分布を示す。 23 MDs6-1.indb 23 12.7.17 4:36:32 PM T 2 0 D I F F E R E N T I A T E S P S P F R O M P D Statistical Analyses Data were analyzed using the SPSS software package for windows (version 15.0; SPSS, Inc., Chicago, IL). Measures of interrater reliability of ROI segmentation were calculated using the Pearson correlation coefficient. Based on the segmented ROIs, T20 values were acquired and the mean of T20 was determined for further statistical analysis. For statistical analysis, respective multivariate analyses of variance (ANOVAs) were performed for the baBrain Iron Deposition Fingerprints in Parkinson’s Disease and Progressive Supranuclear sal ganglia, thalamus, and WM ROIs.Palsy In addition, univariate ANOVAs were performed on the T20 meas* Kai Boelmans, MD, PhD, Brigitte Holst, MD, Marc Hackius, Jürgen Finsterbusch, Christian Gerloff, MD, Jens Fiehler, and Alexanures ofPhD, each region. A stepwise linearMD, discriminant der Münchau, MD analysis (LDA) was used to predict the clinical diagno* Department of Neurology, University Medical Center Hamburg-Eppendorf, Hamburg, sis. TheGermany objective of this mathematical model is to generate a discriminant function that is a linear combination of feature variables and calculates a probability score for each case. The coefficients in the function are determined such that the separation between the distributions of the probability scores of the 3 groups 古典的パーキンソン病(Parkinson’ s disease; PD)と 測定した。主要所見として,PSP 患者では,PD 患者お is maximized. The subjects are then classified (pre進行性核上性麻痺(progressive supranuclear palsy; よび対照被験者に比べ,尾状核,淡蒼球および被殻の dicted) to be in the group with the highest probability score. If pathological changes affect multiple brain PSP)との臨床的鑑別は時に困難である。現在のところ, T2’ 値が短縮していた。段階的な線形判別分析により, structures, an LDA can account for more than 1 両疾患を高い信頼性で鑑別できるバイオマーカーは認 PSP 患者を region. ForPD this患者および健常対照被験者から鑑別で analysis, T20 values of the basal ganglia and thalamus were averaged over the left患and められていない。本稿では,異常な脳内鉄蓄積が両疾患 きた。すべての PSP 患者が正しく分類された。PSP FIG. 1. ROI definitions. Placement of basal ganglia ROIs: (A) globus right brain hemisphere for every subject. Differences pallidus and putamen; (B) caudate nucleus and thalamus with 4 subreにおける進行中の神経変性のマーカーであり,鉄蓄積の 者が健常対照被験者として誤分類された例はなく, また, were considered significant if P < .05. Multiple tests gions (AT, anterior thalamus; MotorT, motor thalamus; PT, posterior 解剖学的分布は両者で異なることを報告する。本研究 健常対照被験者が thalamus; MT, medial thalamus). White matter (WM) ROIs: (C) frontal on the same dataPSP pool患者として誤分類された例もな were Bonferroni-corrected. and occipital WM; (D) UMC, underneath motor cortex. では,定量的 T2’ マップを,PD 患者および PSP 患者 かった。PD 患者のうち,PSP 患者として誤分類された パーキンソン病および進行性核上性麻痺における脳内鉄蓄積 のフィンガープリント の局所脳内鉄含量のマーカーとして解析し,年齢をマッ 例は 6.7%にすぎなかった。大脳基底核における T2’ transaxial sectioned nuclei. ROIs for the frontal and チさせた対照被験者と比較した。T2 強調および T2* 強 緩和時間の局所的な短縮(該当する脳領域の鉄負荷の occipital WM were located superior to the gray matter Results 調画像を,PD 患者 30 例,PSP 患者 12 例,対照被験 上昇を反映)は,PSP 患者に特徴的な所見であり,PD ROIs. ROIs were chosen carefully to minimize partial 者 24 effects. 例において で撮像した。各半球内の大 患者では認められない。 Clinical Findings volume The1.5 sizeTesla and shape of ROIs were kept 2 ; identical across subjects: caudate nucleus, 21 mm Demographical and clinical characteristics of 脳基底核,視床および白質の関心領域の平均 T2’ 値を globus pallidus, 42 mm2; putamen, 77 mm2; thalamus, patients and healthy controls are given in Table 1. 69 mm2; anterior, motor, medial, and posterior thalaThere were no significant differences in gender distrimus each 31 mm2; frontal WM, 35 mm2; occipital P butionMovement (P ¼ .211, v2 tests) Disorders, Vol.or 27,age No.(F 3,(2,63) 2012,¼pp.2.420, 421–427 WM, 35 mm2; and UMC, 45 mm2 (Fig. 1). The raters ¼ .097) between PD, PSP, and healthy controls. PD were blind to the clinical diagnoses when placing patients had a longer disease duration (t (40) ¼ 3.148, Key Word 進行性核上性麻痺,パーキンソン病,大脳基底核,脳内鉄,MRI ROIs. To assess the reproducibility of the ROI placeP ¼ .003) compared to PSP patients. The PSP group ments, we performed an interrater reliability test for had a significant higher UPDRS-III score (t (40) ¼ the 2 raters (K.B., M.H.) across all ROIs for each 2.953, P ¼ .005) and Hoehn & Yahr stage (t (40) ¼ subject. 5.570, P < .001) compared to PD patients. Table 1 対照群と患者群の背景因子および臨床的特徴 TABLE 1. Demographical and clinical characteristics of control subjects and patients Group Controls PD PSP n (male/female) Age at examination, y, mean 6 SD (range) Disease duration, y, mean 6 SD (range) UPDRS part III, mean 6 SD (range) Hoehn & Yahr stage, mean 6 SD (range) 24 (13/11) 30 (19/11) 12 (4/8) 62.8 6 9.9 (42–78) 61.5 6 10.5 (41–80) 68.8 6 8.0 (55–80) – 9.7 6 5.2 (0.6–22.7)* 4.5 6 3.7 (0.7–10.3) – 32.5 6 11.2 (12.0–61.0)* 45.9 6 17.6 (15.0–78.0) – 2.2 6 0.8 (1.0–4.0)* 3.7 6 0.8 (2.0–5.0) *PSP との比較で有意差あり( P< 0.005) *Significant differences compared with PSP (P <。 .005). PD, disease; PSP, progressive supranuclear palsy; UPDRS, Unified Parkinson’s SD, standard deviation. PDParkinson’s =パーキンソン病,PSP =進行性核上性麻痺,UPDRS = Unified Parkinson’ sDisease DiseaseRating RatingScale; Scale,SD =標準偏差 Movement Disorders, Vol. 27, No. 3, 2012 423 24 MDs6-1.indb 24 12.7.17 4:36:33 PM Abstract T 2 TABLE 2. Diagnostic classification matrix, based on T20 Table 2 大脳基底核および視床の T2’ 値に基づく診断分類 values in basal ganglia and thalamus 0 D I F F E R E N T I A T E S P S P F fied as having PD. Probability scores for all given in Table 2. Predicted group by T20 , n (%) Clinical classification (n) Controls (24) PD (30) PSP (12) Controls PD PSP 18 (75.0) 9 (30.0) 0 6 (25.0) 19 (63.3) 0 0 2 (6.7) 12 (100.0) 線形判別分析結果の要約。大脳基底核(尾状核,淡蒼球,被殻)お Summary of results of the linear discrimination analysis. The classification of subjects due to their T20 values of basal ganglia (caudate nucleus, よび視床の T2’ 値による被験者の分類を,臨床診断ごとに示す。各行 globus pallidus, and putamen) and thalamus is shown with respect to their は臨床診断,各列は T2’ 値から予測される診断。太字は正しい診断を clinical diagnosis. Rows represent the clinical diagnosis and columns the diagnosis predicted by T20 values. Bold values indicate correct diagnosis. 示す。PD =パーキンソン病,PSP =進行性核上性麻痺 PD, Parkinson’s disease; PSP, progressive supranuclear palsy. corrections were performed on the T20 measures of the WM ROIs to further investigate the main effects. These analyses revealed a significant main effect for the factor disease in frontal WM (F(2,102) ¼ 5.976, P ¼ .004) A and UMC (F(2,102) ¼B9.316, P < .001). Post hoc analysis showed significant differences for the comparison between controls and PDCaudate patients (P < .001) and between controls and PSPnucleus patients (P < Putamen .001) for UMC. In addition, significant main effects were found for AT P ¼ .01), occipiage in frontal WM (F(2,102) ¼ 4.817, Motor T Globus ¼6.067, P ¼PT .003), and UMC tal WM (F(2,102) pallidus Thalamus duration in (F(2,102) ¼ 4.784, P ¼ .01), for disease MT UMC (F(2,102) ¼7.734, P ¼ .001), and for UPDRS-III in frontal WM (F(2,102) ¼ 4.854, P ¼ .01) and occipital WM (F(2,102) ¼ 6.644, P ¼ .002). Significant interactions were observed for age*disease duration in frontal C WM (F(3,102) ¼ 3.234,DP ¼ .025) and in UMC P ¼ .023) and for disease*UPDRS(F(3,102) ¼ 3.324, Frontal WM III in UMC (F(1,102) ¼ 4.279, P ¼ .041). All means, standard deviations, and significance levels are sumUnderneath marized in Figure 2B. motor cortex Discrimination Between PD, PSP, and Control Subjects In our LDA model, only the basal ganglia (caudate Occipital WM nucleus, globus pallidus, and putamen) and thalamus ROIs were considered. WM ROIs were excluded as these variables showed more than 1 main(A)淡蒼 effect in Figure 1 関心領域(ROI)の定義。大脳基底核 ROI: addition to disease in the univariate ANOVAs. 球および被殻, (B)尾状核および 4 つの下位領域(AT:前部視床, The overall classification was 74.2%. No control MotorT:運動性視床,PT:後部視床,MT:内側視床)を含む subject was incorrectly classified as being in the(D) PSP 視床。白質(WM)ROI: (C)前頭葉および後頭葉 WM, group, and no PSP patient was incorrectly classified as UMC:底部運動皮質 being in the PD group. Thus, all 12 PSP patients were correctly classified as having PSP. The LDA model was also good at discriminating between PD and PSP patients. Of 30 PD patients, 19 were correctly classified as having PD, and only 2 PD patients were incorrectly classified having PSP. Of 24 controls, 18 were identified correctly; 6 controls were incorrectly classi- Discussion In the present study, the main finding wa cant shortening of T20 in the caudate nucle pallidus, and putamen in PSP patients co PD patients and healthy controls. In additio LDA, using T20 mean values allowed exc crimination between the PSP group compa PD and healthy control group. The distribution of shortened T20 values i ganglia in this study reflects several previous regional pathology in PSP patients. An incr iron level was found in the striatum (cauda and putamen) in PSP, but not in PD.20 In a proven PSP case, a region-specific decrease i was found, corresponding to increased de ferric iron.21 Disease-specific gray matter PSP compared to PD patients have also b mented by an increased apparent diffusion in the caudate nucleus, globus pallidus, an using diffusion-weighted imaging,22 or by th of N-acetylaspartate in the lentiform nucleus ton magnetic resonance spectroscopy.23 In magnetization transfer ratios were significan in the caudate nucleus, globus pallidus, and PSP, in contrast to PD patients and controls. At first sight, the increased T20 in UM patients in our study is unexpected. This fin be explained by a decrease of oxygen extr to a reduced metabolic state of brain tissue. quent reduced conversion from oxyhemo deoxyhemoglobin would lead to diminishe bility. However, in contrast to basal ganglia mus ROIs, in UMC significant main effects found for age and disease duration, making to interpret T20 values with respect to disea cation. Therefore, we have excluded WM R subsequent LDA and considered only ba and thalamus ROIs. The T20 protocol used in our study has b to be a sensitive method for the estimation gional brain iron content and to be supe imaging in this regard.12,25 For instance, in h trol subjects the pattern of T20 values decreasing gradient from frontal WM to the lidus, which corresponds to the histopatholo ven distribution of brain iron in healthy cont In line with our results, a previous study et al.28 using a T20 MR protocol to investig gional iron content in PD patients also repo nificant decrease of T2 relaxation time in th compared to healthy controls. Using 3 Tesl including ROI measurements of the most af 25 Movement Disorders, Vol. 27, No. 3, MDs6-1.indb 25 12.7.17 4:36:33 PM パーキンソン病に伴う抑うつにおけるセロトニン作動性 1A 受容体障害の役割 Role of Serotonergic 1A Receptor Dysfunction in Depression Associated with Parkinson’s Disease * Benedicte Ballanger, PhD, Helene Klinger, PsyD, Julien Eche, MD, Jérôme Lerond, MD, Anne-Evelyne Vallet, MD, Didier Le Bars, PharmD, PhD, Leon Tremblay, PhD, Véronique Sgambato-Faure, PhD, Emmanuel Broussolle, MD, PhD, and Stéphane Thobois, MD, PhD * CNRS, UMR 5229, Centre de Neurosciences Cognitives, Bron, France 抑うつは,パーキンソン病(Parkinson’ s disease; PD) 〔未補正(uncorrected)P < 0.001〕 。抑うつを伴わな においてよくみられるが,その病態生理は依然として不 い PD 患者と比較した場合,抑うつを伴う患者では,ト 明である。最近の 2 件の研究では,セロトニン作動系 レーサ取り込みの低下が左海馬,右島,左上側頭皮質, のシナプス前レベルでの役割が検討されている。本研 眼窩前頭皮質で認められた。対照群と比較した場合,抑 究の目的は, F-MPPF PET を用い,シナプス後のセ うつを伴わない PD 患者では,18F-MPPF 取り込みの低 ロトニン作動系障害が PD に伴う抑うつの病態生理に及 下が両側の下前頭皮質,右腹側線条体,島で認められた。 ぼす影響を検討することである。抑うつを伴う PD 患者 対照群と比較した場合,抑うつを伴う PD 患者では, 4 例と抑うつを伴わない PD 患者 8 例を本試験に登録 18 した。各患者に対し, F-MPPF(選択的セロトニン 前頭皮質,右海馬領域,側頭皮質で認められた。今回 1A 受容体アンタゴニスト)を用いた PET を実施した。 の画像研究から,辺縁系のセロトニン 1A 受容体神経伝 18 F-MPPF 取り込みを,2 つの PD 患者群および条件を 達の異常が,PD 患者の抑うつの基礎にある神経機構に マッチさせた健常被験者 7 例において,統計的パラメ 関与している可能性が示唆される。 18 18 F-MPPF 取り込みの低下が左背側前帯状皮質,眼窩 トリックマッピングを用いてボクセルごとに比較した Movement Disorders, Vol. 27, No. 1, 2012, pp. 84–89 Key Word パーキンソン,抑うつ,セロトニン,PET,18F-MPPF Orbitofrontal cortex Dorsal ACC Insula Hippocampus Insula Superior temporal cortex 35 30 30 20 15 Uncus T-score Orbitofrontal cortex 25 20 15 Parahippocampal Gyrus 10 Fusiform Gyrus 5 10 0 5 Figure 2 対 照 群と比 較して抑うつを伴う PD 患 者において 18 F-MPPF 結合レベルが低かった領域。これらの領域は,側頭皮質, 眼窩前頭皮質,島皮質,背側前帯状皮質(ACC) ,海馬傍皮質か らなる。SPM 5 で得られた解剖学的な脳 MRI 画像上に重ね合わせ て示す。 T-score 25 0 Figure 3 抑うつを伴わない PD 患者と比較して抑うつを伴う PD 患者において 18F-MPPF 結合レベルが低かった領域。これらの領域 は,島皮質,眼窩前頭皮質,海馬からなる。SPM 5 で得られた解剖 学的な脳 MRI 画像上に重ね合わせて示す。 26 MDs6-1.indb 26 12.7.17 4:36:34 PM Clinical Utility C R I T I C A L A P P R A I S A L movements (such as hand/arm flapping) which are ‘‘looped’’ motor patterns but which occur intermittently, as well as more severe repetitive movements which dominate motor output at the expense of other movements. We believe that this definition will help to reduce the inexorable expansion of causes of stereotypy and may provide the clinician with a concept that is of clinical utility and can aid diagnostic categorization of A Npatients. D C L IIn N Table I C A L1Lwe Y have UC SR EIdivided F IUCL A the F PI P N R I of TA I IsterOS NA L T LD E A causes eotypy into broad headings, and in Table 2 we have TABLE 2. (such Conditions that may be confused with are movements as hand/arm flapping) which given a list of conditions that can be confused with stereotypies ‘‘looped’’ motor patterns but which occur intermitstereotypy which we feel are excluded under our tently, Motor tics as well as more severe repetitive movements definition. Tardive (see Video, Segment 5) at the expense of other whichdyskinesia dominate motor output ‘‘Motor habits’’ occurring as part of preparation for certain voluntary movements. 常同症(stereotypy) :批判的評価と臨床的に有用な定義の 提案 Stereotypies: A Critical Appraisal and Suggestion of a movements Clinically DefinitionUtility of the (eg, Useful in sportspeople) Pathophysiological Restless legs syndrome of Stereotypy Clinical Utility Clinical Utility Automatisms in Concept the context of epileptic seizures Mark J. Edwards, PhD, Anthony E. Lang, MD, and Kailash P. Bhatia, MD * Repetitive behaviors in the context of psychiatric disorders such as * Sobell of Motor Movement Disorders, of Neurology, Queen Square, London, UK schizophrenia obsessive disorder occur to Does the and concept ofcompulsive stereotypy so defined have any We Department believe that thisNeuroscience definitionand will help to reduceUCL Institute We believe that this definition willthat help reduce the inexorable expansion of causes of stereotypy and may provide the clinician with a concept that is of clinical utility and can aid diagnostic categorization of patients. In Table 1 we have divided the causes of stereotypy into broad headings, and in Table 2 we have given a list of conditions that can be confused with 運動異常症の臨床分類は,その障害を表す用語の正確 stereotypy which we feel are excluded under our な 定 義 を 基 礎 に 成 り 立 っ て い る。 我 々は,常 同 症 definition. (stereotypy)という用語が現在,臨床的および学術的 Pathophysiological Utility of the 使用に必要とされる正確さを全く欠いており,臨床的に Concept of Stereotypy 有用な診断カテゴリーが提示されておらず,病態生理学 的に関連する一連の病態の定義付けもなされていない Does the concept of stereotypy so defined have any ことを指摘する。常同症の概念の定義付けが難しいとい pathophysiological utility? There are certainly interestingう状況は今に始まったことではなく,これは我々が検討 questions raised by the observation that certain stereotypies are part of normal development and appear to go through a normal progression, eventually disappearing.22,23 The occurrence of such repetitive rhythmical movements appears to peak at about 24 23 C R are I T Ipresent C A L A P P Rbirth. A I S24A L months of age, but they from Key Word 常同症,チック,定義 movements (such as hand/arm flapping) which are Table 1 常同症の原因 TABLE 1. Causes of Stereotypy ‘‘looped’’ motor patterns but which occur intermittently, as well as more severe repetitive movements Physiological which dominate motormovements output that at the of other Non–goal directed repetitive occurexpense as part of normal development (body rocking, head nodding), which are expected to movements. follow a normal progression and largely disappear over time. (see Video, Segment 2). Primary Patients who have a stereotypy as the only clinical sign without history of developmental delay,this psychiatric disorder,will Tourette’s We believe that definition helpsyndrome, to reduce other secondary or degenerative theorinexorable expansion of cause causes of stereotypy and Secondary may provide the clinician with a concept that is of Developmental delay, autistic spectrum disorder clinical utility and diagnostic categorization of Basal ganglia lesion (seecan Video,aid Segment 4) patients. In Table 1 we have divided the causes of sterTourette’s syndrome Postinfectious Video,headings, Segment 3) and in Table 2 we have eotypy into (see broad Encephalitis lethargica given a list of conditions that can be confused with Paraneoplastic stereotypy which we feel are excluded under our Associated with anti-NMDA antibodies definition. Drug induced Amphetamines and other psychostimulants Confinement or sensory deprivation (eg, deafness, blindness) Heredo-Degenerative Rett’s syndrome (see Video, Segment 1) Neuroacanthocytosis Neuronal brain concept iron accumulation Does the of stereotypy so defined have any Frontotemporal dementia pathophysiological utility? There are certainly interestWilson’s disease ing questions raised by the observation that certain Lesch-Nyhan syndrome Clinical Utility Pathophysiological Utility of the Concept of Stereotypy stereotypies are part of normal development and appear to Ngoメチル through a normal progression, eventually NMDA, N-methyl-D-aspartate. NMDA = -D- アスパラギン酸(N-methyl-D-aspartate) 22,23 disappearing. The occurrence of such repetitive [動画ファイルはオンライン版(http://onlinelibrary.wiley.com)で rhythmical movements appears to peak at about 24 閲覧可能] months of age,23 but they are present from birth.24 TABLE 1. Causes of Stereotypy MDs6-1.indb Physiological Non–goal directed repetitive movements that occur as part of normal development (body rocking, head nodding), which are expected to follow a normal progression and largely disappear over time. (see Video, Segment 2). 27 Primary secondary to a delusional belief or of obsessive thought pathophysiological utility? There are certainly interestthe inexorable expansion causes of stereotypy and Secondary causes of raised head nodding cerebellar disorders,that certain ing questions by (eg, thewith observation may provide the clinician a concept that is of third ventricular cysts, congenital nystagmus, spasmus nutans) stereotypies of diagnostic normal development clinical utilityare andpart can aid categorizationand of appear through normal progression, eventually patients.toIngoTable 1 wea have divided the causes of ster22,23 disappearing. occurrence such2 repetitive Are theseinto movement patterns merely epiphenomena of eotypy broad The headings, and inof Table we have rhythmical movements appears to peak at about 24 normal motor development, or do they serve a purpose given a list of conditions that can be confused with した本用語の歴史的変遷からも明らかである。我々は, 24 months of which age,23 but are system present birth. in the development of athey mature offrom motor constereotypy we feel excluded under our この歴史的背景を総合的にまとめるとともに,臨床医が trol? It is of interest that repetitive movement patterns definition. are typically TABLE replaced in normally developing children 1. Causes of Stereotypy 特定の運動障害について関連カテゴリーのチック(tics) by more complex repetitive behaviors extend ではなく常同症というカテゴリーを使用する必要がある Pathophysiological Utilitywhich of the Physiological beyond movements into an insistence on sameness and Non–goal directed repetitive movements that occur as part of normal と感じた理由を探索する。また,現在の研究および実地 of Stereotypy ritualdevelopment with Concept regard to daily andareordering (body rocking, head activities nodding), which expected to of 25 follow a The normal formation progression andoflargely disappear time. may habits andover rituals objects. 臨床における本用語の多重使用について論じ,これらに Does the concept so defined have any (see Video, Segment 2).of stereotypy allow precious cognitive resources to be diverted else基づいて新たな定義と分類を提案する。 pathophysiological utility? There are certainly interestPrimary where while allowing us to proceed ‘‘on autopilot.’’ who haveraised a stereotypy only clinical sign that withoutcertain history ingPatients questions by as thethe observation The of segregation between goal-directed behavior (medidevelopmental disorder, development Tourette’s syndrome, stereotypies are delay, partpsychiatric of normal and ated or by frontal-associative basal ganglia-thalamic or degenerative cause appearother to secondary go through a normal progression, eventually Secondary loops) and stimulus-response habitual behavior (medi22,23 disappearing. The spectrum occurrence of 2012, suchpp.repetitive Developmental delay, autistic Movement Disorders, Vol. 27,disorder No. 2, 179–185 ated by sensorimotor cortex-sensorimotor basal ganrhythmical movements appears to peak at about 24 Basal ganglia lesion (see Video, Segment 4) glia-thalamic loops) is an increasingly important A N Tourette’s D C L syndrome I C 23 A L L Y U S E F U L D E F I N I T I O 24 months ofI Nage, but they are present from birth. N concept, recently extended to 3)provide a pathophysiologPostinfectious (see Video, Segment 26 TABLE for 2. Conditions that may be confused withthat Stereotypies icalEncephalitis model Parkinson’s disease. lethargica Table 2 常同症と混同されやすい病態 TABLE 1. Causes of Stereotypy stereotypies Paraneoplastic occur as part of normal motor development may reflect Associated withofanti-NMDA development habitualantibodies motor patterns that can subseMotor tics Physiological Drug induced Tardive dyskinesia (see Video, Segment Non–goal repetitive movements that occur as part ofactions, normal quently bedirected incorporated into 5)more complex Amphetamines and psychostimulants ‘‘Motor habits’’ occurring asbe partan of preparation certain development (bodyother rocking, head nodding), for which are voluntary expected to and may therefore important part of normal Confinement or sensory deprivation (eg, deafness, blindness) movements (eg, in progression sportspeople) follow a normal and largely disappear over time. motor physiology. A more precise definition of pathoHeredo-Degenerative Restless syndrome (seelegs Video, Segment 2). Rett’s conditions syndrome Video, Segment 1) logical where stereotypies occur might allow Automatisms in the (see context of epileptic seizures Primary Neuroacanthocytosis us to find outhave what these patterns areasreally Repetitive behaviors ina the contextmovement of the psychiatric disorders Patients who stereotypy as only clinical sign such without history Neuronal ironobsessive accumulation schizophrenia and compulsive disorderTourette’s that of developmental delay, psychiatric syndrome, telling us brain about normal motor disorder, control andoccur the manner Frontotemporal dementia tosecondary a delusional belief or obsessive or otherneurological or degenerative cause in secondary which disorders can thought cause pathological Wilson’s diseaseof head nodding Secondary causes (eg, cerebellar disorders, stereotypies emerge. Lesch-Nyhan to syndrome third ventriculardelay, cysts,autistic congenital nystagmus, spasmus nutans) Developmental spectrum disorder Basal ganglia lesion (see Video, Segment 4) NMDA, N-methyl-D-aspartate. Tourette’s syndrome [動画ファイルはオンライン版(http://onlinelibrary.wiley.com)で Postinfectious (see Video, Segment 3) merely epiphenomena of Are these patterns 閲覧可能] movement Encephalitis lethargica normal motor development, or do they serve a purpose Paraneoplastic we have charted historical of inHere the development of a the mature systemdevelopment of motor conAssociated withofanti-NMDA antibodies the concept stereotypy, and through this hope to trol? is of interest that repetitive movement patterns DrugItinduced have demonstrated the shifting definition of this enigareAmphetamines typically and replaced in normally developing children other psychostimulants matic movement disorder. Our argument has extend been or sensory deprivation (eg, deafness, blindness) byConfinement more complex repetitive behaviors which that the historical difficulty in the precise definition of Heredo-Degenerative beyond movements into an insistence on sameness and Rett’s syndrome (see Video, Segment 1) use of the term that stereotypy has led to a modern ritual with regard to daily activities and ordering of Neuroacanthocytosis neither serves a useful clinical purpose defines a 25 The of habits andnorrituals may objects. Neuronal brain iron formation accumulationentity. clear pathophysiological The main reason for allow precious cognitive resources to be diverted elseFrontotemporal dementia this current unsatisfactory is clear: that once Wilson’s disease where while allowing us situation to proceed ‘‘on autopilot.’’ one steps outside a very rigid definition of stereotypy Lesch-Nyhan syndrome The segregation between goal-directed behavior (medi- Conclusions as a single pattern continuously repeated at ated by movement frontal-associative basal ganglia-thalamic the expense of all other movement, it becomes NMDA, N-methyl-D-aspartate. loops) and stimulus-response habitual behaviordifficult (medi- Restless legs syndrome Automatisms in the co Repetitive behaviors in schizophrenia and o secondary to a delus Secondary causes of h third ventricular cyst A N D C L I N I C Are these movem TABLE 2. Co normal motor de in the developm Motor tics trol? It is of inte Tardive dyskinesia (see are typically rep ‘‘Motor habits’’ occurri bymovements more comple (eg, in s beyond movemen Restless legs syndrome Automatisms co ritual within the regar 25 Repetitive behaviors objects. The inf schizophrenia and o allow precious c secondary to a delus where Secondarywhile causes allo of h The thirdsegregation ventricular cyst ated by fronta loops) and stimu Are these movem ated by sensorim normal motor glia-thalamic de lo in the developm concept, recently trol?model It is offor inte ical P are typically occur as part rep of n by more comple development of h beyond movemen quently be inco ritualmay withtherefo regar and 25 The objects. motor physiologf allow precious logical conditionc where while us to find out allo wh The segregation telling us about ated by neurolo fronta in which loops) and stereotypiesstimu to em ated by sensorim glia-thalamic lo concept, recently ical model for P occur part of n Hereaswe have development the concept of hs quently be inco have demonstrat and may therefo matic movemen motor that thephysiolog historica logical condition stereotypy has le us to find out wh neither serves a tellingpathophysi us about clear in which neurolo this current unsa stereotypies to em one steps outsid as a single move the expense of al Here we have the concept of s have demonstrat matic movemen that the historica stereotypy has l neither serves a clear pathophysi this current unsa one steps outsid as a single move the expense of al ated by sensorimotor cortex-sensorimotor basal ganglia-thalamic loops) is an increasingly important Movement Disorders, Vol. 27, No. 2, 2012 183 concept, recently extended to provide a pathophysiological model for Parkinson’s disease.26 Stereotypies that occur as part of normal motor development may reflect 27 development of habitual motor patterns that can subsequently be incorporated into more complex actions, and may therefore be an important part of normal motor physiology. A more precise definition of patho12.7.17 4:36:35 PM logical conditions where stereotypies occur might allow パーキンソン病におけるピサ症候群:臨床的特徴・筋電図所見・ 放射線学的所見 Pisa Syndrome in Parkinson’s Disease: Clinical, Electromyographic, and Radiological Characterization *, *** Cristina Tassorelli, MD, PhD, Anna Furnari, MD, Simona Buscone, MD, Enrico Alfonsi, MD, Claudio Pacchetti, MD, Roberta Zangaglia, MD, Anna Pichiecchio, MD, Stefano Bastianello, MD, Alessandro Lozza, MD, Marta Allena, MD, Monica Bolla, MD, Giorgio Sandrini, MD, Giuseppe Nappi, MD, and Emilia Martignoni, MD * IRCCS ‘‘National Neurological Institute C. Mondino’’ Foundation, Pavia, Italy Department of Public Health and Neurosciences, University of Pavia, Pavia, Italy *** 体 幹 の 姿 勢 異 常 は パ ー キ ン ソ ン 病(Parkinson’ s に高かった。ピサ症候群を伴う PD 患者群の大部分で, disease;PD)の典型的な症状である。ピサ症候群,す 体幹屈曲は PD 症状発症側の対側に認められた。筋電図 なわち,矢状面での軽度回旋を伴う筋緊張性の体幹側 では,異常な緊張性過活動が屈曲側の胸椎部傍脊柱筋 屈も,そのうちの 1 つである。本研究では,ピサ症候 と腹斜筋に認められた。腰椎部傍脊柱筋の CT 所見とし 群の臨床的特徴,筋電図所見,および放射線学的所見を, て,屈曲側でより著しい筋萎縮がみられ,萎縮の分布に PD 患者 20 例を対象として検討した。体幹屈曲を伴う は頭側と尾側で差(gradient)が認められた。ピサ症候 患者全例が,筋電図検査および放射線学的検査(X 線検 群は,進行期 PD の合併症の 1 つであり,PD 症状の非 査および CT スキャン)を受けた。ピサ症候群を伴う 対称性が高く,症状の弱い側の背部傍脊柱筋に過活動 PD 患者群の臨床的特徴を,体幹屈曲を伴わない PD 患 が検出される患者サブグループに発現すると考えられ 者の対照群と比較した。ピサ症候群を伴う PD 患者群は, る。この姿勢異常は注目に値し,併存症および疼痛を予 PD 症状の非対称性に関するスコアが対照群よりも有意 防するため,適切かつ早期に治療する必要がある。 Movement Disorders, Vol. 27, No. 2, 2012, pp. 227–235 Key Word ジストニア,パーキンソン,神経画像検査,疼痛,脊柱側弯 Abdominal oblique muscle (contralateral side) Abdominal oblique muscle (bending side) Paraspinal thoracic muscles (contralateral side) Paraspinal thoracic muscles (bending side) Figure 2 直立状態で記録した筋電図の代表例。左側に屈曲した ピサ症候群の PD 患者 1 例における腹斜筋および胸椎部傍脊柱筋 (T7 ~ T8 レベル) 。持続性の緊張性活動が左側の胸椎部傍脊柱筋 と腹斜筋に認められた。 28 MDs6-1.indb 28 12.7.17 4:36:35 PM Abstract Bending side Contralateral side Figure 1 右側に屈曲したピサ症候群の PD 患者 1 例(代表例) 。臨床評価時,左側背部の腰椎部傍脊柱 筋に肥厚の所見が認められた一方,右側ではほぼ触知されなかった。T10 レベルの筋電図では屈曲側の 過活動が認められた。 [カラーの図はオンライン版(http://onlinelibrary.wiley.com)で閲覧可能] 。 IP MF a) b) Bending side Bending side Figure 4 a:多裂筋(MF)が腸腰筋(IP)よりも大きく関与することを示す代表例。b:傍脊柱筋萎縮の 非対称性分布を示す代表例。注目点として,萎縮は屈曲側のほうが顕著である。 [カラーの図はオンライン 版(http://onlinelibrary.wiley.com)で閲覧可能] 。 29 MDs6-1.indb 29 12.7.17 4:36:35 PM 非運動症状と運動症状の比較:パーキンソン病患者の健康状 態への影響はどの程度か? Nonmotor Versus Motor Symptoms: How Much Do They Matter to Health Status in Parkinson’s Disease? * Claire Hinnell, MD, Catherine S. Hurt, PhD, Sabine Landau, PhD, Richard G. Brown, PhD, and Michael Samuel, FRCP, on behalf of the PROMS-PD Study Group * Department of Neurology, King’s College Hospital, King’s Health Partners, London, United Kingdom エビデンスから,運動症状および非運動症状の両者が 算用量で説明できた。年齢が低いほど,健康状態が不 パーキンソン病患者の健康状態に影響することが示唆 良であることが予測された。完全回帰モデル(試験開始 されている。依然明らかにされていないのは,これらの 前の変数と症状 5 領域すべてを含む)では,健康状態 臨床的変数が変化した場合に健康状態がどの程度変化 に関する分散の 56%が説明できた。抑うつに関する標 するかということである。また,不安が,抑うつとは独 準化β係数は,運動症状,不安,その他の非運動症状の 立した形で,健康状態の予測因子として検討されたこと それぞれ 2.1 倍,1.6 倍,1.3 倍であった。今回の知見 はほとんどない。本研究では,階層的重回帰分析および から,パーキンソン病患者の健康状態に対する各臨床 標準化β係数を用い,パーキンソン病(Parkinson’ s 的変数の相対的影響をランク付けすることができ,抑う Disease; PD) 患 者 462 例 の 診 断 確 定 コ ホ ー ト つが健康状態に及ぼす影響は運動症状による影響の 2 (prevalent cohort)において,健康状態〔Parkinson’ s 倍以上であることが明らかになった。不安およびその他 Disease Questionnaire(PDQ)で評価〕に対する周知 の非運動症状も,パーキンソン病患者の健康不良状態 のパーキンソン病症状 5 領域(運動症状,抑うつ,不安, に関する重要な独立決定因子である。本研究結果は, 認知障害,その他の非運動症状)の相対的影響を検討 パーキンソン病患者の個別ケアの策定やサービス計画 した。健康状態のスコアに関し,分散(variance)の の立案に役立つであろう。 19.6%は年齢,併存疾患の数,罹病期間,レボドパ換 Movement Disorders , Vol. 27, No. 2, 2012, pp. 236–241 Key Word パーキンソン病,健康状態,抑うつ,非運動症状,相対的影響 30 MDs6-1.indb 30 12.7.17 4:36:35 PM L PDQ-8 score 29.5 (18.5) 0–100 a Median and interquartile range. This very high score represents a patient on continuous subcutaneous apomorphine infusion.LEDD, levodopa-equivalent daily dose; UPDRS, Unified Parkinson’s Disease Rating Scale; NMSS, Non-Motor Symptoms Scale; ONMS, other nonmotor symptoms; HADS, Hospital Anxiety and Depression Scale; ACE-R, Addenbrooke’s Cognitive Examination-Revised; PDQ, Parkinson’s Disease Questionnaire. b Nearly one quarter (23.6%) of patients were on an antidepressant at the time of assessment. One quarter (24.5%) showed significant cognitive impairment. A baseline regression model accounted for 19.6% of variance in PDQ-8 scores, with worse HS predicted by a younger age, greater number of physical comorbidities, living alone, longer disease duration, and higher LEDD. Each symptom domain contributed a significant amount of variance when entered independently after variance in HS, an increase of 36.6% from the baseline model. The unique variance explained by each variable is shown in Table 3; depression explained the largest portion of variance, more than ONMS, anxiety, and motor state. The unique variance contributions obtained from the full model were smaller than those obtained from the individual regression models Abstract because domain scores were positively correlated. In the final model (adjusting for other domain effects), cognition was no longer significantly associated with HS, but the effects of the other 4 domains remained significant (Table 2). The adjusted standardized beta coefficients obtained from the full model are given in Table 2. The adjusted standardized beta coefficient for HADS-D was 2.1, 1.6, and 1.3 times that of UPDRS-III, HADS-A, and ONMS, respectively. Table 2 スコアの最終的重回帰分析の結果(最終モデル) TABLE 2. Results ofPDQ-8 final multiple regression analysis of PDQ-8 scores (final model) Independent variables Standardized regression (beta) coefficients P value Regression coefficients 95% CI 0.006 �0.141 0.047 0.055 0.096 0.074 �0.043 0.148 0.196 0.232 0.308 .857 < .001b .144 .108 .009b .039b .224 < .001b < .001b < .001b < .001b 0.073 �0.081 0.684 0.194 0.095 0.001 �0.025 0.076 0.259 0.053 0.503 �0.718 to 0.864 �0.124 to 0.039 �0.235 to 1.604 �0.043 to 0.431 0.024 to 0.167 0.000 to 0.001 �0.064 to 0.015 0.039 to 0.113 0.152 to 0.366 0.036 to 0.069 0.373 to 0.633 Sex Age Living alone No. of physical of health conditions Duration of PD (y) LEDD ACE-R UPDRS-III HADS-A ONMSc HADS-D Adjusted R2a 0.562 (P < .001)b 補正後RR2, :検討したすべての独立変数を含むモデルで説明可能な の分散の推定割合。 Adjusted estimated proportion of the variance of PDQ-8 explained by the PDQ-8 model including all listed independent variables. Statistically significant results. b c 統計学的に有意。 NMSS minus mood and cognition components. a a 2 b Non-Motor Symptom Scale から気分および認知機能の項目を除いたもの。 c 238 E T Movement Disorders, Vol. 27, No. 2, 2012 A L . Table 3 完全回帰モデルから各変数を除いた算出結果 TABLE 3. Results of subtraction from full regression to LE 1. Patient characteristics (n ¼ 462) Mean (SD) (各変数固有の分散の割合) determine unique variance portion of each variable Range nd social characteristics ) white) rking (% full- or part-time) (%) hysical health cluding PD treatment nset (y) PD since diagnosis (y) ay) al score r stages I/II–III/IV–V (%) score S minus mood n) ssion score y score score 67.5 (10.3) 64.9 96.3 13.4 20.1 32–94 — — — — 2.9 (1.7) 1–11 60.6 (11.9) 5.0 (8.0)a 600.0 (720.0)a 13–92 0–39 0–7365b 25.9 (11.6) 12.6/81.4/5.9 48.0 (52.3)a 37.3 (35.3)a 4–78 — 0–235 0–150 6.1 7.1 86.9 29.5 (3.6) (4.5) (10.3) (18.5) 0–17 0–20 46–100 0–100 terquartile range. h score represents a patient on continuous subcutaneous nfusion.LEDD, levodopa-equivalent daily dose; UPDRS, on’s Disease Rating Scale; NMSS, Non-Motor Symptoms other nonmotor symptoms; HADS, Hospital Anxiety and ale; ACE-R, Addenbrooke’s Cognitive Examination-Revised; MDs6-1.indb 31 n’s Disease Questionnaire. Independent variables HADS-D ONMSa HADS-A UPDRS-III ACE-R Full model standard R2 Standard R2 with variable removed Unique percent variance explained by variable 0.573 0.573 0.573 0.573 0.573 0.517 0.536 0.551 0.560 0.571 5.6% 3.7% 2.2% 1.3% 0.2% a a Non-Motor Symptom Scale から気分および認知機能の項目を除いたも NMSS minus mood and cognition components. の。 the baseline measures: depression (26.7% additional variance), anxiety (19.0%), nonmood and noncognitive NMS (17.7%), motor severity (9.0%), and cognition (2.5%). As each symptom domain significantly predicted HS in its individual regression models and there was no evidence of multicollinearity (all intercorrelations being less than 0.6),24 all planned variables were included in the full regression model. The full model (Table 2) explained 56.2% of the variance in HS, an increase of 36.6% from the baseline model. The unique variance explained by each variable is shown in Table 3; depression explained the largest portion of variance, more than ONMS, anxiety, and motor state. The unique variance contributions obtained from the full model were smaller than those obtained from the individual regression models 31 12.7.17 4:36:36 PM パーキンソン病における軽度認知障害の診断基準: Movement Disorder Society 作業部会のガイドライン Diagnostic Criteria for Mild Cognitive Impairment in Parkinson’s Disease: Movement Disorder Society Task Force Guidelines * Irene Litvan, MD, Jennifer G. Goldman, MD, MS, Alexander I. Tröster, PhD, Ben A. Schmand, PhD, Daniel Weintraub, MD, Ronald C. Petersen, MD, PhD, Brit Mollenhauer, MD, Charles H. Adler, MD, PhD, Karen Marder, MD, Caroline H. Williams-Gray, MRCP, PhD, Dag Aarsland, MD, PhD, Jaime Kulisevsky, MD, PhD, Maria C. Rodriguez-Oroz, MD, PhD, David J. Burn, MD, FRCP, Roger A. Barker, BSc, MBBS, MRCP, PhD, and Murat Emre, MD * Division of Movement Disorders, Department of Neurology, University of Louisville, Louisville, Kentucky, USA; and Movement Disorders Program, Frazier Rehab Neuroscience Institute, Louisville, Kentucky, USA 軽 度 認 知 障 害 は, 非 認 知 症 の パ ー キ ン ソ ン 病 像,神経生物学,評価,長期経過に関する我々の理解が (Parkinson’ s disease;PD)患者に一般的にみられ, 深まるにつれて,本診断基準の妥当性の検証や,場合に 認知症の前兆である可能性もある。その重要性に鑑み, よっては改良版の作成が必要になるであろう。これらの Movement Disorder Society は作業部会に対し,PD に 診断基準は今後の研究の取り組みを推進し,進行性の おける軽度認知障害の診断基準を明示するよう委託し 認知機能低下および認知症のリスクが高く認知症発症 た。提案された診断基準は,文献レビューと専門家の合 前(predementia)段階での臨床的介入が有益となりう 意に基づくものである。本論文ではガイドラインを提示 る PD 患者をごく初期段階で特定するのに役立つものと し,その臨床症状と診断方法を明らかにする。ただし, 考えられる。 今後さらなる研究を通じてこの臨床症候群の疫学,臨床 Movement Disorders, Vol. 27, No. 3, 2012, pp. 349–356 Key Word パーキンソン病,認知,軽度認知障害,診断基準,認知症 Table 1 パーキンソン病における軽度認知障害 (PD-MCI)の診断基準 I.選択基準 ・英国 PD Brain Bank 基準 20 に基づくパーキンソン病の診断。 ・確立した PD を背景に認知能力の段階的低下がみられる(患者 や情報提供者による報告,または 臨床医の観察) 。 ・認知障害が正式な神経心理学的検査または 1 種類の全般的認知 能力評価尺度で認められる(詳細はセクションⅢ参照) 。 ・認知障害の程度は,患者の機能的自立を大きく妨げるほどでは ないが,複雑な機能的タスクの遂行は若干難しい場合がある。 II.除外基準 ・Movement Disorder Society 作業部会提案の基準 18 に基づく,PD における認知症の診断。 ・認知障害に関する他の主要原因がある(例:せん妄,脳卒中, 大うつ病,代謝異常,薬剤の有害作用,頭部外傷) 。 ・他に PD 関連の併存症(例:運動障害,重度の不安,抑うつ, 日中過眠,精神病)があり,臨床医の意見では,認知機能検査 成績に大きく影響している。 III.PD-MCI の具体的なガイドライン(カテゴリー:レベル I およ びレベル II) A.レベル I(簡易評価) ・PD での使用の妥当性が確認された 1 種類の全般的認知能力評 価尺度で障害が認められる a,または ・一連の神経心理学的検査が限定的に実施されており(すなわち, 5 つの認知機能領域それぞれについて実施された検査が 1 種類 以下,または,評価された認知機能領域が 4 つ以下) ,2 種類以 上の検査で障害が認められる。 32 04_Abstract_MD6-1.indd 32 B.レベル II(包括的評価) ・神経心理学的検査として,5 つの認知機能領域(注意・作業記憶, 遂行機能,言語,記憶,視空間認知能力)それぞれについて 2 種類の検査が実施されている b。 ・2 種類以上の神経心理学的検査で障害が認められる。すなわち, 1 つの認知機能領域に関する 2 種類の検査,または,2 つの認知 機能領域に関する各 1 種類の検査で障害が認められる。 ・神経心理学的検査による障害の判定は下記による: ‐検査成績が適切な基準を約 1 ~ 2 標準偏差(SD)下回る,または ‐連続的に実施された認知機能検査で,検査成績が有意に低下, または ‐推定される発症前(premorbid)レベルから検査成績が有意に 低下。 IV.PD-MCI のサブタイプ分類(オプションの評価。5 つの認知機 能領域それぞれについて 2 種類の検査が実施されている必要があ る。研究目的での使用が強く推奨される。 )c ・単一領域型 PD-MCI:1 つの認知機能領域に関する 2 種類の検 査で異常がみられ(該当領域を特定する) ,他の領域に障害はな い,または ・複数領域型 PD-MCI:2 つ以上の認知機能領域において 1 種類 以上の検査で異常がみられる(該当領域を特定する) 。 Table 2(PD での妥当性が確認された全般的認知能力に関する評 価尺度の例)を参照。 b Table 3(5 つの認知機能領域に関する神経心理学的検査の例)を 参照。 c サブタイプ分類が適用できるのは,5 つの認知機能領域のそれぞ れについて2 種類以上の検査が実施されたPD-MCI 患者のみである。 [参考文献リストはオンライン版(http://onlinelibrary.wiley.com) で閲覧可能] a 12.7.18 11:56:44 AM L I T V A N E T A L . L I T V A N E T Abstract A L . TABLE 2. Examples of Neuropsychological Scales for of the clinician, may have significantly influenced cognitive TABLE and 2. Examples of Neuropsychological Scales for Assessing Global Cognitive Abilities Estimating of the clinician, may have significantly influenc testing (see Table 1 for specific examples). Table 2 全般的認知能力の評価および認知症発症前の認知機能(premorbid Premorbid Intelligence* Assessing Global Cognitive Abilities and Estimating intelligence)の testing (see Table 1 for specific examples). 推定を目的とした神経心理学的評価尺度の例 * Premorbid Intelligence* Assessment Global cognition Estimated premorbid intelligence Specific Estimated Time of Test, min Neuropsychological Neuropsychological Tests40 Assessment MoCA22,58 PD-CRS24,59 Global cognition SCOPA-COG59,60 MDRS23,59,61 NART40 WTAR40 10 15 15 20 to 30 5 5 Estimated premorbid intelligence Guidelines for PD-MCI Level I and LevelTime II Categories Specific Guidelines for PD-MCI Lev Estimated Tests40 of Test, min Level II Categories Level I (Abbreviated Assessment, Possible PD-MCI) Level I (Abbreviated MoCA22,58 The level I category 10 allows for the diagnosis of PD-Assessment, Possible 15 PD-CRS24,59 MCI based on an abbreviated cognitive The level assessment, I category allows for the diagn 59,60 15 SCOPA-COG because comprehensive testing may not based always on be practi23,59,61 MCI an abbreviated cognitive 20 to 30 MDRS cal or available. Level I criteria because provide comprehensive less diagnostic testing may not alway NART40 certainty than 5level II. The requirements for level I are cal or available. Level I criteria provide less WTAR40 impairment on5a scale of global cognitive abilities vali- certainty than level II. The requirements for Some of these tests are copyrighted and require permission from the authors dated for use in PD (Table 2; and see cut-offon guidelines to be used. The PD-CRS is a scale owned by the Movement Disorders impairment aが scale of global cognitive ab これらの検査の一部は著作権で保護されており,使用に際して著者の許諾を必要とする。PD-CRS は Movement Disorders Society 21–25 Society (see www.movementdisorders.org/publications/rating_scales/). Some of these tests are copyrighted and require permission from thetests authors ) or impairment on a limfor global cognitive *See also reference no. 57. dated for use in PD (Table 2; and see cut-of to be used. The PD-CRS is a scale owned by the Movement Disorders 所有する評価尺度(www.movementdisorders.org/publications/rating_scales/ 参照) 。 ited battery of neuropsychological tests (e.g., including 21–25 Abbreviations: MoCA, Montreal CognitiveSociety Assessment; PD-CRS, Parkinson’s (see www.movementdisorders.org/publications/rating_scales/). 57 ) or impairmen for global cognitive tests * 文献 (National Institute of *See Neurological Disorders and Disease-Cognitive Rating scale; SCOPA-COG, for no. Outcomes of NINDS common data elements. 2011. alsoScales reference 57. Stroke. only one test per cognitive domain or those assessing Parkinson’s disease–Cognition; MDRS, Mattis Dementia Rating Scale. ited battery of neuropsychological tests (e.g Abbreviations: MoCA, Montreal Cognitive Assessment; PD-CRS, Parkinson’s Available at: www.ninds.nih.gov/research/clinical_research/toolkit/ common_data_elements.htm.)も参照。 fewer than Identical to the MDS Disease-Cognitive Rating scale; SCOPA-COG, Scalesfive for cognitive Outcomes domains). of only one test per cognitive domain or thos 略語:MoCA = Montreal Cognitive Assessment,PD-CRS Parkinson’ sDementia Disease-Cognitive Rating Scale,SCOPA-COG = Scales for Parkinson’s disease–Cognition; = MDRS, Mattis Rating Scale. PDD operational criteria, the relevant cognitive domains fewer than five cognitive domains). Identical t PDD operational criteria, the relevant cogniti Outcomes of Parkinson’ s disease-Cognition,MDRS = Mattis Dementia Rating Scale Table 3 * TABLE 3. Examples of認知機能領域検査の例と検査所要時間 Tests for Cognitive Domains and Estimated Time* Estimated Time of TABLE 3. Examples of Tests for Cognitive Domains and Estimated Time* 40 Cognitive Domain Attention and working memory Neuropsychological Tests WAIS-IVDomain (or earlier version) Letter Number Sequencing Cognitive Test, min Est 5 40 Neuropsychological Tests WAIS-IV Coding (or earlier version) or other substitution task, written or oral 5 5 to 10 Trail Making Testa memory Attention and working WAIS-IV (or earlier version) Letter Number Sequencing Digit span backward or digit ordering 5 task, written or oral WAIS-IV Coding (or earlier version) or other substitution Stroop color-word test 5 to 10 Trail Making Testa Executive function Language Memoryb Visuospatialc function Digit span backwardmodification) or digit ordering Wisconsin Card Sorting Test (CST), or modified CST (Nelson’s 15 Stroop color-word test (CANTAB) Tower of London test–Drexel version, or Stockings of Cambridge 10 to 15 Verbal fluency test, such as letter fluency (COWAT or similar tests), category fluency 5 Executive function Wisconsin Card Sorting Test (CST), or modified CST (Nelson’s modification) (animals, supermarket, or similar), or alternating fluency tasks (if a well-standardized London test–Drexel or Stockings of Cambridge (CANTAB) version is used). Not more than one verbalTower fluencyoftest abnormality shouldversion, be Verbal fluency test, such as letter fluency (COWAT or similar tests), category fluency used to satisfy the MCI criterion of two abnormal test performances because of the strong relationship among these tests;(animals, supermarket, or similar), or alternating fluency tasks (if a well-standardized version is used). Not more than one verbal fluency test abnormality should be 10 points Clock Drawing Test used to satisfy the MCI criterion of two abnormal test performances because WAIS-IV (or earlier version) Similarities 10 to 15 of the strong relationship among these tests; Confrontation naming task, such as Boston Naming Test (or short-form 5 to 15 10 points Clock Drawing Test validated in PD) or Graded Naming Test Language WAIS-IV (or earlier version) Similarities Word list learning test with delayed recall Confrontation and recognitionnaming conditions, 10 to(or 20short-form task, such suchasas Boston Naming Test Rey’s Auditory Verbal Learning Test, California VerbalinLearning Test, Hopkins validated PD) or Graded Naming Test Verbal Learning Test, and Selective Reminding Test as test with delayed recall and recognition 10 to 15 Prosebrecall3 test with a delayed recall condition, Word listsuch learning conditions, such as Memory Wechsler Memory Scale-IV Logical MemoryRey’s subtest (or earlier version) or Test, California Verbal Learning Test, Hopkins Auditory Verbal Learning Rivermead Behavioural Memory Test paragraph subtest Verbalrecall Learning Test, and Selective Reminding Test Brief Visuospatial Memory Test–Revised (BVMT-R) 10 as to 15 Prose recall3 test with a delayed recall condition, such Wechsler Memory Scale-IV Logical Memory subtest (or earlier version) or Benton’s Judgment of Line Orientation 5 to 10 Rivermead Behavioural Memory Test paragraph recall subtest Hooper Visual Organization Test 10 Brief Visuospatial Memory Test–Revised (BVMT-R) 5 Clock copying (e.g., Royall’s CLOX) c Visuospatial function Benton’s Judgment of Line Orientation 5 5 5t 5 5t 15 10 5 10 5t 10 10 10 5t 類似性の高い 種類の検査(例,2 種類のリスト学習検査または 2 種類のストーリー想起検査)により,2 種類の検査スコアの異常という軽 Two highly similar 2tests (e.g., two list learning tests or two story recall tests) shouldHooper not be Visual used toOrganization meet the MCI of two test-score abnormalities. Testcriterion 10 Similarly, highly correlated scores from the same test (e.g., immediate and delayed recall of a word list) should not be used to meet the criterion of two test 度認知障害(MCI)基準に合致していると判断すべきではない。同様に,同一の検査に由来する相関性の高いスコア(例,単語リストの即時 Clock copying (e.g., Royall’s CLOX) 5 abnormalities. Abnormality of two highly correlated scores only increases confidence in the existence of impairment. 想起と遅延想起)により,検査 2 種類の異常という基準に合致していると判断すべきではない。相関性の高い 2 種類のスコアにおける異常は, *See also reference no. 40 for references. a 48 Trail Making Test (TMT) Part A, Stroop color-word and two colorlist naming, beor used this recall purpose. Theshould TMT and subtests are timed Two highlysubtests similar reading tests (e.g., learningmay tests twofor story tests) notStroop be used to meet the MCI criterion of two test-score 障害の存在に関する信頼性を高めるに過ぎない。 and give an estimate of manual and articulatory slowness that can be used to judge the significance of the more demanding conditions (e.g., TMT-B, Stroop Similarly, highly correlated scores from the same test (e.g., immediate and delayed recall of a word list) should not be used to meet the crite 40 interference) or of other tests, such as fluency performance. Oral versions of neuropsychological tests may provide alternatives. * 文献 (Lezak MD, Howieson DB, Loring DW. ,Neuropsychological Assessment, 4th ed. New York. Oxford University Press: Oxford University abnormalities. Abnormality of two highly correlated scores only increases confidence in the existence of impairment. b In general, prose recall tests are relatively unreliable; therefore, one should administer at least two paragraphs. *See also reference no. 40 for references. c Press; Most 2004.)も参照。 visual memory tests are less appropriate for PD-MCI because these tests either require motor responses (e.g., drawing of geometric or other figures) or a 48 Making Test (TMT) Part A, Stroop color-word subtestsbecause readingitand color may be used this purpose. The TMT and Stroop sub a 48of the evaluate recognition memory, which lessTrail sensitive to early memory decline. BVMT-R is an exception allows fornaming, assessment motorfor component Trail Making Test( TMT)Part A is およびストループ検査 color-word 課題 (色名単語の読みと色の命名に関するサブテスト) が本目的で使用可能。 and give an estimate of manual and articulatory slowness that can be used to judge the significance of the more demanding conditions (e.g., via the copy condition. interference) or of マニュアル反応および口頭反応の遅延に関する推定値が示されるため, other tests, such as fluency performance. Oral versions of neuropsychological tests may provide alternatives. TMT とストループ課題サブテストは時間計測を伴い, より難しい課題 (例, b In general, prose recall tests are relatively unreliable; therefore, one should administer at least two paragraphs. TMT Part B,ストループ干渉)や他の検査(例,流暢度)の意義の判定に利用できる。口頭による神経心理学的検査も利用可能である。 c Most visual memory tests are less appropriate for PD-MCI because these tests either require motor responses (e.g., drawing of geometric or o b evaluate recognition memory, which is less sensitive to early memory decline. BVMT-R is an exception because it allows for assessment of the m 一般に,散文想起検査は信頼性が比較的低いため,少なくとも 2 つのパラグラフで検査を実施すべきである。 352 Movement Disorders, Vol. 27, No. 3,via 2012 the copy condition. c 視覚記憶検査の大部分は, パーキンソン病における軽度認知障害(PD-MCI)の評価にはあまり適していない。これらの検査は運動反応(例, 幾何学的図形または他の図形の描画)を必要としたり,認識記憶(初期の記憶低下に対する感度が低い)を評価しているためである。 BVMT-R は例外で,模写の状況により運動コンポーネントを評価できる。 352 Movement Disorders, Vol. 27, No. 3, 2012 [参考文献リストはオンライン版(http://onlinelibrary.wiley.com)で閲覧可能] MDs6-1.indb 33 33 12.7.17 4:36:37 PM 剖検で確認された Lewy 小体型認知症における REM 睡眠行動障害とサブタイプ Rapid Eye Movement Sleep Behavior Disorder and Subtypes in Autopsy-Confirmed Dementia with Lewy Bodies * Brittany N. Dugger, PhD, Bradley F. Boeve, MD, Melissa E. Murray, PhD, Joseph E. Parisi, MD, Hiroshige Fujishiro, MD, PhD, Dennis W. Dickson, MD, and Tanis J. Ferman, PhD * Department of Neuroscience, Mayo Clinic, Jacksonville, Florida, USA 本研究の目的は,Lewy 小体型認知症(dementia with 害を伴う患者群は,神経原線維変化の Braak 病期(病 Lewy bodies;DLB)において,ほぼ確実な(probable) 期 Ⅳ 対 病 期 Ⅵ )および 老 人 斑スコア(出現 頻 度, REM 睡眠行動障害の有無により,臨床像や病理像が異 18% 対 85%)が低かったが,Lewy 小体の分布に差 なるか否かを検討することである。ほぼ確実な REM 睡 はみられなかった。ほぼ確実な REM 睡眠行動障害が早 眠行動障害を伴う DLB 患者(71 例)および伴わない 期(認知症の発症時または発症前)に認められた患者 DLB 患者(19 例)を対象に, 背景因子, 臨床的変数(DLB では,認知症発症後に認められた患者に比べ,パーキン の中核的症状,認知症の期間,認知機能 / 運動機能の変 ソニズムおよび幻覚の発症が早く,神経原線維変化の 化率) ,病理学的指標(Lewy 小体の分布,老人斑スコア, Braak 病期は低かった。剖検で DLB が確認され,睡眠 神経原線維変化の Braak 病期)を比較した。ほぼ確実 障 害〔 睡 眠 中 に お け る 夢 の 内 容 の 行 動 化(dream な REM 睡眠行動障害を伴う患者群では,男性が非常に enactment behavior) 〕の既往のなかった女性では,幻 多く(82% 対 47%) ,認知症の期間が比較的短く(平 覚およびパーキンソニズムの発症が遅く,神経原線維 均値,8 年 対 10 年) ,パーキンソニズム(平均値,2 変化の Braak 病期は高かった。ほぼ確実な REM 睡眠行 年 対 5 年)および幻視(平均値,3 年 対 6 年)の発 動障害に伴い,独特の DLB の臨床的および病理学的特 症時期が早かった。また,ほぼ確実な REM 睡眠行動障 徴が認められる。 Movement Disorders, Vol. 27, No. 1, 2012, pp. 72–78 Key Word パーキンソン病,REM 睡眠行動障害,Lewy 小体型認知症,Lewy 小体病,アルツハイマー病 D I F F E R E N C E S Table 2 ほぼ確実な REM 睡眠行動障害の発症時期 TABLE 2. Clinical and pathologic differences in early (早期 対 後期)による臨床的・病理学的所見の違い versus late probable RBD Number of patients RBD onset relative to dementia (y), mean 6 SD Male (%) Polysomnography conducted (%) Duration of dementia (y), mean 6 SD Visual Hallucinations (%) Onset relative to dementia (y), mean 6 SD Extrapyramidal signs (%) Onset relative to dementia (y), mean 6 SD Baseline Unified Parkinson Disease Rating Scale (mean 6 SD) Braak NFT stage (mean 6 SD) 34 MDs6-1.indb 34 Early pRBD Late pRBD P value 54 8.5 6 12 17 3.1 6 2 — .001 82% 42.6% 7.4 6 2.8 81.5% 52.9% 9.4 6 2.5 .94 .46 .009 94% 2.1 6 2 87% 3.6 6 2 .42 .04 94% 1.1 6 2.9 93% 3.7 6 2 .83 .027 10.2 6 6 .03 6.1 6 6 3.2 6 1.4 4.2 6 1.7 .02 because of cases of limbic Lewy body type plus a high Braak NFT stage (V–VI). There was no difference in frequencies of Lewy body type (limbic and diffuse) between groups. All differences remained significant after adjusting for age at death. I N D L B B A S E D O N R B D TABLE 3. Pathologic characteristics of a confirmed DLB patients LB type, n (%) Limbic Diffuse CDLB assessment, n (%) Low Intermediate High CERAD NP score, n (%) None Sparse Moderate Frequent Braak NFT stage, median (range) pRBD No pR 20 (28%) 51 (71%) 6 (3 13 (6 2 (3%) 20 (28%) 49 (69%) 5 (2 9 (4 5 (2 13 18 22 14 IV (19%) (27%) (32%) (21%) (0–VI) 0 0 4 14 VI (0 (0 (2 (7 (II- CDLB assessment, likelihood that the pathologic findings with a DLB clinical syndrome; CERAD NP, Consortium Registry for Alzheimer’s Disease neuritic plaque score; NF tangle Braak NFT stage and were less likely to ha neuritic plaques. Lewy body type (limbic fuse) was not associated with the presence of pRBD. That is, patients with pRBD w likely to have brain stem and limbic Lew 12.7.17 4:36:37 PM Abstract D I F F E R E N C E S ents tive to mean 6 SD Early pRBD Late pRBD P value 54 8.5 6 12 17 3.1 6 2 — .001 hy conducted (%) mentia (y), 82% 42.6% 7.4 6 2.8 81.5% 52.9% 9.4 6 2.5 .94 .46 .009 ations (%) o dementia (y), 94% 2.1 6 2 87% 3.6 6 2 .42 .04 signs (%) o dementia (y), 94% 1.1 6 2.9 93% 3.7 6 2 .83 .027 10.2 6 6 .03 d Parkinson ng Scale D) e (mean 6 SD) 6.1 6 6 3.2 6 1.4 4.2 6 1.7 .02 cases of limbic Lewy body type plus a high T stage (V–VI). There was no difference in of Lewy body type (limbic and diffuse) roups. All differences remained significant ting for age at death. Discussion LB cohort, patients with a history of cliniable RBD were more likely to be male, had onset of parkinsonism and visual hallucinave to dementia onset, and had a shorter dullness (based on dementia duration). The of the core DLB clinical diagnostic features onism, fluctuations and visual hallucinarate of dementia progression, extrapyramiy, and severity of somnolence did not DLB patients with and without pRBD. ally, DLB patients with pRBD had a lower plots of medians and 25th and 75th percentiles repreof change over time of UPDRS, MMSE, and ESS-c of change were calculated by subtracting the first exre from the last examination before death, then dividing he time in years between examinations. MDs6-1.indb 35 D L B B A S E D O N R B D S T A T U S TABLE 3. Pathologic characteristics of autopsyTable 3 剖検で確認された DLB 患者の病理学的特徴 confirmed DLB patients LB type, n (%) Limbic Diffuse CDLB assessment, n (%) Low Intermediate High CERAD NP score, n (%) None Sparse Moderate Frequent Braak NFT stage, median (range) pRBD No pRBD 20 (28%) 51 (71%) 6 (32%) 13 (69%) 2 (3%) 20 (28%) 49 (69%) 5 (26%) 9 (47%) 5 (26%) 13 18 22 14 IV (19%) (27%) (32%) (21%) (0–VI) 0 0 4 14 VI (0%) (0%) (22%) (78%) (II-VI) P value .99 .004 .100 < .001 .061 .01 .566 < .001 < .001 CDLB assessment =病理学的所見が DLB の臨床症候群と関連する CDLB assessment, likelihood that the pathologic findings are associated with a DLB clinical syndrome; NP,の老人斑スコア Consortium to(Consortium Establish a 可能性を提示, CERAD NP score CERAD = CERAD Registry for Alzheimer’s Disease neuritic plaque score; NFT, neurofibrillary to Establish a Registry for Alzheimer’ s Disease neuritic plaque score) , tangle NFT =神経原線維変化(neurofibrillary tangle) Braak NFT stage and were less likely to have frequent neuritic plaques. Lewy body type (limbic versus diffuse) was not associated with the presence or absence of pRBD. That is, patients with pRBD were just as RBDbrain stem and limbic Lewy bodies as likely 15to have they were towithout have brain stem, limbic, and neocortical RBD 10 Lewy bodies. This is the first autopsy study to show that pRBD may be a clinical marker of a specific sub5 type in DLB. A history of pRBD is associated with the classic 0presentation of DLB, characterized by early visual hallucinations, early parkinsonism, more rapid disease -5 course, and less Alzheimer’s disease (AD) pathology. These -10 results also reveal that women without a history of pRBD who have autopsy-confirmed DLB may -15 differently from men and women with pRBD. present UPDRS with a MMSE ESS-c Specifically, women history of pRBD have an Figureonset 2 Unified Parkinson’ s Disease Rating Scale(UPDRS) , earlier of visual hallucinations and parkinsonism Mini-Mental Stateconcomitant Examination(MMSE) エップワース眠気尺度 and have less AD , pathology, but the〔患 op者を知る情報提供者による評価,ESS-c(Epworth posite is true for women with DLB whoSleepiness do notScalehave collateral) 〕スコアの経時変化率(中央値,第 1 四分位,第 四 pRBD. The later onset of these core clinical DLB3 fea分位)を示す箱ひげ図。変化率は,死亡前最終検査時のスコアか tures suggests women who do not have pRBD may ら初回検査時のスコアを減じ, pose a greater challenge この値を両検査間の経過時間(年) for initial diagnosis of cliniで除算して算出。 cally probable DLB using existing criteria. Further investigation is needed to determine whether women without pRBD have other clinical or perhaps a specific baseline cognitive pattern that may improve our differential diagnosis of this group. It is unclear how the presence of concomitant AD pathology influences the clinical expression of DLB or if the AD pathology somehow takes precedence, at least in the beginning stages of the disease. Furthermore, we divided cases based on early pRBD (before or within the year of estimated onset of dementia) or late pRBD (after the first year of estimated dementia onset) to understand if the temporal Annualized rate of change Clinical and pathologic differences in early versus late probable RBD I N 35 12.7.17 4:36:38 PM Parkinson At-Risk Syndrome Study における嗅覚障害 および他の前駆症状の検討 Impaired Olfaction and Other Prodromal Features in the Parkinson At-Risk Syndrome Study * Andrew Siderowf, MD, MSCE, Danna Jennings, MD, Shirley Eberly, MS, David Oakes, PhD, Keith A. Hawkins, PsyD, Albert Ascherio, MD, PhD, Matthew B. Stern, MD, and Kenneth Marek, MD, the PARS Investigators * Parkinson’s Disease and Movement Disorders Center, Department of Neurology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania, USA 本 研 究 の 目的 は,嗅 覚 障 害 と 他 の パ ー キ ン ソン 病 が返送された。このうち 669 例は, 嗅覚検査スコア(年 (Parkinson’ s disease;PD)での前駆症状との関連に 齢および性別で標準化)が 15 パーセンタイル以下であ ついて,Parkinson At-Risk Syndrome Study で検討す り,嗅覚低下が確認された。嗅覚低下を伴う被験者は, ることである。PD では多くの場合,運動症状に先立っ 非運動症状(不安・抑うつ,便秘,REM 睡眠行動障害 て嗅覚障害が認められるため,嗅覚検査をスクリーニン の症状)の存在を肯定する確率が有意に高く,運動機能 グ検査法として利用できる可能性が示唆される。スク の変化を報告する確率も有意に高かった。4 つ以上の リーニング法の併用,すなわち,嗅覚検査と運動症状以 非運動症状を伴う被験者の 26%で嗅覚低下がみられた 外の他の前駆症状の併用により,嗅覚検査を単独で使 のに対し,非運動症状が 3 つ以下の被験者で嗅覚低下 用した場合に比べ,PD リスクの検出効率が向上すると 。診断未 がみられたのは 12%であった(P < 0.0001) 考えられる。本研究では,神経疾患の診断を受けていな 確定者において,嗅覚低下は PD の他の非運動症状と関 い被験者を対象に,郵便を利用した調査を実施した。調 連することが明らかになった。嗅覚低下を伴う被験者を 査には,40 項目の University of Pennsylvania Smell 対象に,特異性の高い神経変性マーカー(ドパミントラ Identification Test(UPSIT)および PD 前駆症状に関 ンスポーターイメージング等)による追加評価の実施に する質問票を用いた。非運動症状の報告頻度を,嗅覚 より,嗅覚低下および他の非運動症状の併用検査が将 低下を伴う被験者群と伴わない被験者群で比較した。 来の神経変性リスクの判定に有用であるか否かを明ら 計 4,999 例の被験者から調査票および嗅覚検査の回答 かにできると考えられる。 Movement Disorders, Vol. 27, No. 3, 2012, pp. 406–412 Key Word パーキンソン病,嗅覚,早期発見,非運動症状 36 MDs6-1.indb 36 12.7.17 4:36:38 PM Abstract S I D E R O W F E T A L . N = 10139 Returned screening and background forms by 2/26/2010 N = 741 Not eligible N = 9398 Eligible N = 4999 N = 4399 Completed UPSIT Did not complete UPSIT N = 4330 Normosmic N = 669 Hyposmic FIG. 1. Flow diagram of ascertainment of study cohort. Reasons for Figure 1 試験コホートの内訳を示すフローチャート。除外基準 ineligibility are given in the text. は,年齢 50 歳未満(n = 319) ,パーキンソニズム(n = 208) , 他の神経学的疾患(n = 125) ,重症の鼻炎症状の既往(n = 72) , Statistical Analysis その他(n = 17)であった proportion with hyposmia Descriptive statistics, including means, medians, percentages, and standard deviations (SDs), when appropriate, were calculated for the UPSIT, demographic variables, risk factors, and questions on PD symptoms. To confirm the validity of parametric analyses, sample distributions were visually inspected using histograms or scatter plots, and outlying values were checked for 0.30 accuracy. Subjects completing and not completing the UPSIT were0.25compared using chi-square tests or t tests, as appropriate. Univariate associations between hyposmia and 0.20 other prodromal features of PD were tested using chi-square tests for dichotomous and categorical variables.0.15Cochran-Armitage tests for linear trend were used for ordered categorical variables (e.g., bowel movement frequency). Furthermore, t tests were used 0.10 to test differences in mean scores on continuous scales (e.g.,0.05the CES-D). Logistic regression was used to calculate odds ratios (ORs) for association between hyposmia and other prodromal features. Multiple 0.00 1 3 4 2 0 5 logistic regression models were constructed to test for number of prodromal features independent associations between hyposmia and proFigure 2 複数の前駆症状を伴う被験者群における嗅覚低下例の割 dromal features. 合。検討した前駆症状は次の通り。 (1)何らかの REM 睡眠行動障 All P values reported are based on two-tailed statis害の症状が月 1 回以上みられる, (2)PD 症状自己申告質問票の肯 tical tests. All analyses were performed using SAS soft定的回答が 2 項目以上, (3)Center forInc., Epidemiological Studies ware (version 9.2; SAS Institute, Cary, NC). Depression Scale(CES-D)スコア> 15, (4)State-Trait Anxiety Inventory(STAI)Form A または Form B スコア> 39, (5)排便頻 度< 1 回 / 日。前駆症状の数が多い被験者ほど(特に 4 ~ 5 つ) , 嗅覚低下を伴う可能性が高い(P < 0.0001) 。 Results Characteristics of Research Participants A total of 10,139 subjects returned valid screening and background forms by the closing date of February 408 MDs6-1.indb 37 Movement Disorders, Vol. 27, No. 3, 2012 26, 2010 (Fig. 1). Of these responses, 741 were not eligible. The reasons for ineligibilit age under 50 (n ¼ 319), diagnosis of parki ¼ 208), other neurological condition (n ¼ tory of significant sinus condition (n ¼ 72), (n ¼ 17). Of the eligible subjects, 4,999 (53%) completed and returned the UPSIT subjects were more likely than older subjec plete the UPSIT (mean age, 64 versus 0.0001). Females were more likely than m versus 48%; P < 0.0001) and Caucasians m than non-Caucasians (64% versus 33%; P to complete the UPSIT. Sixty-five percent having a family member with PD returned compared with 46% of those who did 0.0001). Subjects who reported that they th had a decreased sense of smell were less return the UPSIT than those who did not (51% versus 54%; P ¼ 0.04). Demographic istics of subjects completing the UPSIT are Table 1, based on hyposmia status. There nificant differences in age or gender, beca percentile scores are standardized for age a However, older age (r2 ¼ 0.33; P < 0. male gender (male ¼ 31.3 versus female ¼ 0.0001) were significantly associated w unstandardized UPSIT scores. Overall UPSIT Performance Among those who completed the UPSIT jects were judged to be hyposmic based on developed for the study. The average raw U was 34.1 (SD, 3.2) for normosmics and 22.6 for hyposmics. Relationship Between Prodromal Fea PD and UPSIT Performance There were significant associations betw smia and prodromal features of PD, includ pation, RBD symptoms, depression/anxiety reported change in motor function (Table 2 items were endorsed significantly more fre TABLE 1. Demographic Characteristics of t Cohort Comparing Hyposmic and Normosmi Who Completed the UPSIT Age (Mean, SD) Male gender (N, %) White/Caucasian (N, %) PD in family (N, %) None 1 >1 Current/former smoker (N, %) Normosmics (N ¼ 4,330) Hyposm (N ¼ 66 63.9 (9.6) 2,200 (51) 3,820 (98) 64.5 (9 355 (5 583 (9 2,393 1,760 177 2,272 378 265 26 359 (55) (41) (4) (53) 37 12.7.17 4:36:39 PM (5 (4 (4 (5 パーキンソン病の非運動症状に関する MDS-UPDRS Part I の妥当性の検証 Validation of the MDS-UPDRS Part I for Nonmotor Symptoms in Parkinson’s Disease * David A. Gallagher, MRCP, Christopher G. Goetz, MD, Glenn Stebbins, PhD, Andrew J. Lees, MD, FRCP, FMedSci, and Anette Schrag, MD, PhD, FRCP * Institute of Neurology, University College London, London, United Kingdom Unified Parkinson’ s Disease Rating Scale(UPDRS) (Cronbach のα係数:0.85) ,床効果および天井効果 はパーキンソン病(Parkinson’ s Disease; PD)研究に が小さく(床効果:2%,天井効果:0%) ,併存的妥当 おける主要な転帰評価尺度である。UPDRS 改訂版の作 性が良好であった(UPDRS Part Ⅰ オリジナル版との相 成を通じ, 本尺度の特性は改善され, 広範な PD 症状(特 。MDS-UPDRS PartⅠ スコ 関:r = 0.81,P < 0.001) に非運動症状)が網羅されるようになった〔国際運動障 アの標準化 z スコアは,各種の非運動症状評価尺度の 害学会(Movement Disorder Society;MDS)が作成 複合 z スコアと高い収束的妥当性を示し(r = 0.89, した UPDRS 改訂版 (MDS-UPDRS) 〕 。本研究の目的は, P < 0.0001) ,PartⅠ に関する当初の因子解析で特定さ MDS-UPDRS Part Ⅰ (日常生活における非運動症状)の れた 2 つのサブスコアも,対応する非運動症状評価尺 妥当性を確認することである。MDS-UPDRS および妥 度の複合 z スコアと高い相関を示した〔抑うつ,不安, 当性が確認された PD の非運動症状の各種評価尺度を 無感情(apathy)因子スコア:r = 0.72,P < 0.0001, 用い,PD 患者 94 例〔Hoehn and Yahr(HY)分類 そ の 他 の 非 運 動 症 状 因 子 ス コ ア:r = 0.87,P < Ⅰ ~ Ⅴ 〕を検討した。MDS-UPDRS の信頼性,床効果 0.0001〕 。今回のデータから,MDS-UPDRS Part Ⅰ の および天井効果,ならびに妥当性が確認された PD の 総スコアが,妥当性が確認された PD の非運動症状の各 非運動症状の評価尺度と本スコアとの相関性を評価し 種評価尺度の複合スコアと強く相関することが明らかに た。MDS-UPDRS Part Ⅰ は, 内 部 整 合 性 が 高 く なった。 Movement Disorders, Vol. 27, No. 1, 2012, pp. 79–83 G A L L A G H E R E T A L . Key Word パーキンソン病,非運動症状,UPDRS TABLE 2. MDS-UPDRS Item Correlations With Individual Corresponding Clinical Scales and With Composite Scores Table 2 MDS-UPDRS 各項目と対応する臨床評価尺度〔個々の尺度および複数尺度の複合スコア(z スコア) 〕との相関 of Corresponding Scales (z-Scores) 38 MDS-UPDRS Item Nonmotor Symptoms Clinical Scale 1.1 Cognitive impairment 1.2 1.3 Hallucinations and psychosis Depressed mood 1.4 1.5 1.7 Anxious mood Apathy Sleep problems 1.8 Daytime sleepiness 1.9 1.10 1.11 1.12 1.13 Pain and other sensations Urinary problems Constipation problems Lightheadedness on standing Fatigue ACE SCOPA-COG FAB PPRS HDRS HADS-D HADS-A LARS PSQI SCOPA-night ESS SCOPA-day VAS SCOPA-AUT-urinary SCOPA-AUT-gastrointestinal SCOPA-AUT-cardiovascular FSS Mean (6 Standard Deviation) 89.0 24.9 15.1 7.6 4.1 5.8 6.0 �23.4 6.9 5.1 8.9 5.4 17.4 5.8 3.9 1.0 4.2 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 10.3 7.0 2.8 2.3 4.1 3.6 4.1 8.4 4.2 4.1 5.2 4.3 16.9 3.7 3.0 1.4 1.7 Correlation of MDS-UPDRS Items With Corresponding Clinical Scale Correlation of MDS-UPDRS Items With Composite of Corresponding Scales 0.32b 0.26c 0.33b 0.86a 0.56a 0.41a 0.53a 0.67a 0.70a 0.78a 0.56a 0.62a 0.64a 0.55a 0.68a 0.84a 0.61a 0.29b 0.86a 0.53a 0.53a 0.67a 0.80a 0.60a 0.64a 0.55a 0.68a 0.84a 0.61a Statistical analysis comprised Spearman’s rank correlations with the following levels: P <0.01, 0.001; c b, P< and c, P ¼ 0.01. All MDS-UPDRS 統計解析には Spearman 順位相関を用い, 次の有意レベルを設定した。 a:Psignificance < 0.001, b:Pa, < :P =0.01; 0.01。 ドパミン調節異常症候群 (dopamine Part I items are represented, except dopamine dysregulation syndrome (item 1.6). dysregulation syndrome) (項目 1.6)を除くすべての MDS-UPDRS Partrevision I 項目を示す。 Abbreviations: MDS-UPDRS, Movement Disorder Society–sponsored of the Unified Parkinson’s Disease Rating Scale (UPDRS); ACE, Addenbrooke’s Cognitive Examination; SCOPA-COG, Scales for Outcome in Parkinson’s disease (SCOPA), cognitive scale; FAB, Frontal Assessment Battery; PPRS, MDS-UPDRS = Movement Disorder Society が作成した UnifiedRating Parkinson’ s Disease Rating Scale(UPDRS)改訂版,ACE = Addenbrooke’ s Parkinson Psychosis Rating Scale; HDRS, Hamilton Depression Scale; HADS-D, Hospital Anxiety Depression Scale (HADS), depression score; HADS-A, HADS anxiety score; LARS, Lille Apathy Rating Scale; PSQI, Pittsburgh Sleep Quality Index; ESS, Epworth Sleepiness Scale; VAS, Visual Analog Scale; Cognitive Examination,SCOPA-COG = Scales for Fatigue Outcome Parkinson’ s disease(SCOPA) (認知機能) ,FAB =前頭葉機能検査(Frontal SCOPA-AUT, SCOPA autonomic scale; FSS, Severityin Scale. Assessment Battery) ,PPRS = Parkinson Psychosis Rating Scale,HDRS =ハミルトンうつ病評価尺度(Hamilton Depression Rating Scale) , HADS-D = Hospital Anxiety Depression Scale(HADS) (抑うつスコア) ,HADS-A = HADS(不安スコア) ,LARS = Lille Apathy Rating Scale, PSQI =ピッツバーグ睡眠質問票(Pittsburgh Sleep Quality Index) ,ESS =エップワース眠気尺度(Epworth Sleepiness Scale) ,VAS =視覚的ア Correlation of MDS-UPDRS Items With Discussion ナログ尺度(Visual Analog Scale) ,SCOPA-AUT SCOPA(自律神経機能) ,FSS = Fatigue Severity Scale Validated Nonmotor = Clinimetric Scales MDs6-1.indb 38 The standardized z-score of MDS-UPDRS Part I had a high correlation with the composite z-score of nonmotor scales (r ¼ 0.89, P < 0.0001; Fig. 1). The two MDS-UPDRS Part I standardized factor scores had high correlations with composite z-scores of corresponding nonmotor features (depression, anxiety, Our data demonstrate that the MDS-UPDRS Part I total score has a strong, highly significant relationship with a composite score of nonmotor aspects of PD, based on validated scales of individual NMS. This observation suggests that the MDS-UPDRS Part I, with an application time of only 10 minutes, 12.7.17 4:36:39 PM Abstract 3.00000 A 3.00000 B 2.00000 Zscore(total_dep_anx_apath) Zscore(total_non_motor) 2.00000 1.00000 0.00000 -1.00000 1.00000 0.00000 -1.00000 r = 0.72 p < 0.0001 r = 0.89 p < 0.0001 -2.00000 -2.00000 -2.00000 -1.00000 0.00000 2.00000 1.00000 3.00000 Zscore(newUPDRS_nmEDL) -2.00000 -1.00000 0.00000 1.00000 2.00000 3.00000 Zscore(UPDRS_dep_anx_apath) 3.00000 C Zscore(total_other) 2.00000 1.00000 0.00000 -1.00000 r = 0.87 p < 0.0001 -2.00000 -2.00000 -1.00000 0.00000 1.00000 2.00000 3.00000 Zscore(UPDRS_other) Figure 1 散布図および Spearman 順位相関係数。 (A) 「MDS-UPDRS Part I(日常生活における非運動症状)全体の標準化 z スコア」 対「各種の非運動症状評価尺度の複合 z スコア」 , (B) 「MDS-UPDRS の抑うつ・不安・無感情(apathy)因子スコアの標準化 z ス コア」対「抑うつ・不安・apathy に関する各種の評価尺度の複合 z スコア」 , (C) 「MDS-UPDRS のその他の非運動機能因子スコア の標準化 z スコア」対「その他の非運動症状の各種評価尺度の複合 z スコア」 。 39 MDs6-1.indb 39 12.7.17 4:36:39 PM グルコセレブロシダーゼ遺伝子変異はパーキンソン病の 臨床経過中の認知症リスクを高める Glucocerebrosidase Mutations Confer a Greater Risk of Dementia during Parkinson’s Disease Course *, **, *** Núria Setó-Salvia, BS, Javier Pagonabarraga, MD, PhD, Henry Houlden, MD, PhD, Berta Pascual-Sedano, MD, PhD, Oriol Dols-Icardo, BS, Arianna Tucci, MD, Coro Paisán-Ruiz, PhD, Antonia Campolongo, BS, Sofía Antón-Aguirre, BS, Inés Martín, BS, Laia Muñoz, BS, Enric Bufill, MD, PhD, Lluïsa Vilageliu, PhD, Daniel Grinberg, PhD, Mónica Cozar, BS, Rafael Blesa, MD, PhD, Alberto Lleó, MD, PhD, John Hardy, PhD, Jaime Kulisevsky, MD, PhD, and Jordi Clarimón, PhD * Neurology Department. Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Spain Àrea de Prehistoria, Universitat Rovira i Virgili, Tarragona, Spain Institut Català de Paleoecologia Humana i Evolució Social (IPHES), Tarragona, Spain ** *** グルコセレブロシダーゼ遺伝子変異はパーキンソン病 N370S および L444P 変異がこれらの遺伝子変異の (Parkinson’ s disease; PD)および Lewy 小体型認知 50 % を 占 め た。2 種 類 の 新 規 変 異(L144V お よ び 症(Lewy body dementia; LBD)と関連する。しかし, S488T)と 7 種類の既報の変異も認められた。グルコ これらの変化が PD の臨床経過に何らかの影響を及ぼす セレブロシダーゼ変異に伴い,PD の臨床経過中に,有 か否かは,なお不明である。本研究では,グルコセレブ 意に高い認知症リスクが認められた(発症時年齢,発症 ロシダーゼコード領域の完全な遺伝子配列を,スペイン 。 後期間,性別で補正したオッズ比:5.8,P = 0.001) 国内の PD 患者 225 例,病理学的に確認された LBD 患 変異キャリアは,非キャリアよりも運動症状が比較的軽 者 17 例,および対照被験者 186 例で明らかにした。 度で,L- ドパへの反応は良好であり,中間型の PD 症 PD 患者 22 例(9.8%)および LBD 患者 2 例(11.8%) 状(表現型)を呈する傾向にあった。本研究の知見から, がグルコセレブロシダーゼ遺伝子変異キャリアであった グルコセレブロシダーゼ遺伝子変異は,PD および LBD が,対照被験者の変異キャリアはわずか 1 例(0.5%) の発症リスクを高めるだけでなく,PD 経過中の認知症 。 で あ っ た(PD:P = 0.016,LBD:P = 0.021) の発症にも強い影響を及ぼすことが示唆される。 Movement Disorders, Vol. 27, No. 3, 2012, pp. 393–399 Key Word パーキンソン病,Lewy 小体病,認知症,グルコセレブロシダーゼ,遺伝 G B A A N D I T S R O L E I N P D , L B D , A N D P D D TableTABLE 3 グルコセレブロシダーゼ遺伝子(GBA)変異キャリアと非キャリアの臨床的比較 3. Clinical comparison between GBA mutation carriers and noncarriers Years of Age at onset, evolution, Female, mean 6 SD mean 6 SD n (%) Years of Type of evolution Parkinson’s: BR\before BR\Tremoric, n (%) Positive family Dementia, dementia, BR\Rigid-akinetic, n (%) history of PD, UPDRS, n (%) BR\mean 6 SD BR\Intermediate, n (%) n (%) mean 6 SD PD patients with 54.2 6 6.6 14.1 6 6.5 16 11 (50%)a a GBA mutations (72.7%) (n ¼ 22) PD patients without 56.5 6 12.7 12.0 6 6.7 88 48 (23.6%) GBA mutations (43.3%) (n ¼ 203) 12.9 6 6.9 11.3 6 7.6 3 7 12 58 91 53 (13.6%) (31.8%) (54.5%)b (28.7%) (45.0%) (26.2%) H&Y mean 6 SD 11 (50%) 28.7 6 13.3 2.5 6 0.82 79 (39%) 30.1 6 14.1 2.67 6 0.98 0.01 PP<< .01; P b < .05. aa b 40 MDs6-1.indb P < 0.05 new mutations suggested a significant impact on the structure and function of the GBA protein. Also, a mutation at residue 488 (S488P) has been previously described in a patient suffering from type 2 Gaucher disease (GD),31 thus making this amino acid exchange a very plausible pathogenic mutation. The T369M allele was the only variant found in the control series. This nonsynonymous change was also encountered in 2 PD patients (P5 and P6). Because of the discrepancies in the literature regarding the pathological consequences of this particular nonsynonymous change, a reevaluation of the data omitting the T369M allele 40 mutation carriers were used in this comparison). Another explanation could be a differential age-related effect of GBA alterations. Yet when PD patients with late onset of disease were selected (older than 50 years, n ¼ 147), those patients carrying mutations in GBA had a younger disease onset compared with noncarriers (58.9 and 63.7 years, respectively; P ¼ .05). There was an overrepresentation of women among PD patients carrying a mutation. This is the opposite of the male-to-female ratio reported in Neumann et al (2009),16 in which they described an excess of men carrying GBA mutations. However, our study agrees12.7.17 7 4:36:40 PM 「効能・効果」、 「 用法・用量」、 「 警告・禁忌を含む使用上の注意」、 「 用法・用量に関連する 使用上の注意」等につきましては、添付文書をご参照ください。 IN Fu 脳 症 臨 治 と 系 A 剖 お ド イ 発行者 ワイリー・パブリッシング・ジャパン株式会社 利 定価1,470円(本体価格1,400円)
© Copyright 2026 Paperzz