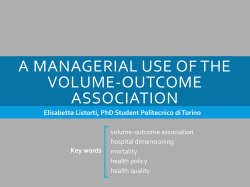
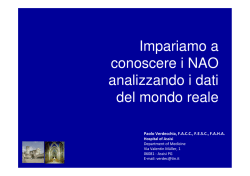
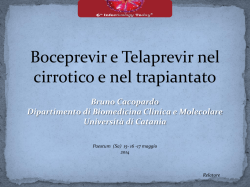
Leukemia (2004) 18, 133–138 & 2004 Nature Publishing Group All rights reserved 0887-6924/04 $25.00 www.nature.com/leu Multiple myeloma: comparison of two dose-intensive melphalan regimens (100 vs 200 mg/m2) A Palumbo1, S Bringhen1, A Bertola1, F Cavallo1, P Falco1, M Massaia1,2, B Bruno1, C Rus3, A Barbui4, T Caravita5, P Musto6, N Pescosta7, F Rossini8, M Vignetti9 and M Boccadoro1 1 Divisione di Ematologia dell’Università di Torino, Azienda Ospedaliera S Giovanni Battista, Torino, Italy; 2Laboratory of Onco-Hematology Research Center on Experimental Medicine, Torino, Italy; 3Ospedale Evangelico Valdese, Torino, Italy; 4 Divisione di Ematologia, Ospedali Riuniti, Bergamo, Italy; 5Cattedra di Ematologia, Policlinico S Eugenio, Roma, Italy; 6 Dipartimento di Onco-Ematologia, IRCCS, Casa Sollievo della Sofferenza, S Giovanni Rotondo, Italy; 7Ospedale Lorenz B:Ohler, Bolzano, Italy; 8Ematologia, HS Gerardo, Monza, Italy; and 9Cattedra di Ematologia, Università Cattolica S Cuore, Roma, Italy Several trials have shown the superior impact of high-dose melphalan (usually 200 mg/m2, MEL200) vs standard therapy in myeloma patients. Intermediate-dose melphalan (100 mg/m2, MEL100) is also superior to the standard dose, but has not been clinically compared with MEL200. A total of 90 patients at diagnosis were treated with two MEL100 courses. Their clinical outcome was compared with that of a control group of 90 pair mates matched for serum b2-microglobulin levels and Durie and Salmon clinical stage. These patients were treated at diagnosis with two MEL200 courses. Patient characteristics were similar in both groups except that the median age of the MEL100 group was significantly higher (Po0.0001). Complete remission was 35% after MEL100 and 48% after MEL200 (P ¼ 0.08). Median event-free survival (EFS) was 32 months in the MEL100 group and 42 months in the MEL200 group (Po0.005), but overall survival (OS) was not different. Transplant-related mortality was not significantly different. Haematological and extra-haematological toxicity was significantly reduced after MEL100. Despite the significant age difference, tandem MEL100 was less toxic than tandem MEL200, and MEL100 was inferior to MEL200 in terms of EFS but not in terms of OS. The intensified nonmyeloablative MEL100 regimen is an effective first-line treatment. Leukemia (2004) 18, 133–138. doi:10.1038/sj.leu.2403196 Published online 30 October 2003 Keywords: myelomatransplantation; dose-intensive; melphalan Introduction By comparison with standard treatment, high-dose melphalan, such as melphalan 200 mg/m2 (MEL200), increases complete remission (CR) rate, and extends event-free survival (EFS) and overall survival (OS) from 3 to 5 years.1–9 All major clinical trials have been conducted on transplanted patients with a median age ranging from 49 to 52 years.1–7,9,10 Unfortunately, older patients constitute more than 50% of the total. In the French randomised trial, transplant exclusions were closely related to age.2 In other analyses, age per se did not significantly affect survival after high-dose melphalan.11 b2-Microglobulin and especially certain cytogenetic abnormalities were the major factors affecting outcome.12–14 We have already evaluated the clinical impact of intermediatedose melphalan: in refractory patients, melphalan 60 mg/m2 was superior to melphalan 30 mg/m2;15 in newly diagnosed patients, melphalan 100 mg/m2 (MEL100) was superior to standard oral melphalan and prednisone.16 In both studies, the median age Correspondence: M Boccadoro, Divisione di Ematologia dell’Università di Torino, Azienda Ospedaliera S Giovanni Battista, Via Genova 3, 10126 Torino, Italy; Fax: þ 39 011 6963737; E-mail: mario.boccadoro @unito.it Received 21 May 2003; accepted 4 September 2003; Published online 30 October 2003 was 63–64 years, and health-care support was similar to that required for intravenous conventional chemotherapy. Both MEL100 and MEL200 are clearly superior to standarddose melphalan. Their comparative toxicities and outcomes, however, were unclear. In this study, patients with similar disease characteristics were treated with tandem MEL100 or tandem MEL200 and their toxicities and outcomes were compared. Materials and methods Patients In all, 90 myeloma patients at diagnosis entered the MEL100 protocol between October 1994 and September 2001. The Southwest Oncology Group (SWOG) diagnostic criteria17 and Durie and Salmon staging system were used.18 Patients aged 55–75 years were eligible. Inclusion criteria were normal cardiac, renal, pulmonary and hepatic function on the basis of routine clinical and laboratory examinations, echocardiography and lung-function tests. Patients serologically positive for HBV, HCV or HIV were excluded. The institutional review board approved the protocol, and written informed consent was obtained from all patients. The clinical outcome of tandem MEL100 was compared with that of 90 previously untreated patients with similar clinical characteristics registered at the Gruppo Italiano Trapianto Midollo Osseo (GITMO) between February 1994 and May 2000 and treated with tandem MEL200. The eligibility criteria were the same as for MEL100. Patient characteristics are listed in Table 1. Selection criteria of match Selection criteria were: (1) patients must have been treated at diagnosis and have received MEL200 as induction regimen, and (2) the conditioning regimen must have been only tandem MEL200. Patients treated with other regimens, such as melphalan 140 mg/m2 þ total body irradiation (MEL140 þ TBI) or similar, were excluded. Patients receiving a single transplant were also excluded. These criteria left 282 patients treated at diagnosis with tandem MEL200. From this group, we selected 90 patients matched for stage (same stage according to Durie and Salmon staging system) and b2-microglobulin levels (within 0.5 mg/l, P ¼ 1.0) with MEL100 patients. Treatment regimens MEL100 regimen: Phase I included two DAV debulking courses (dexamethasone–doxorubicin (adriamycin)–vincristine; Dose-intensive melphalan for myeloma A Palumbo et al 134 Table 1 Patient characteristics MEL100 No. of patients Median age (range) (years) Patients 460 years (%) Male gender (%) Stage at diagnosis (%) IIA IIB IIIA IIIB b2-Microglobulin o3 mg/l b2-Microglobulin 43 mg/l M-protein class (%) IgG IgA Bence Jones protein NS Bone marrow plasma cells 430% MEL200 P 90 90 1 61 (55–73) 52 (28–68) o0.0001 54 (60) 15 (17) o0.0001 48 (53) 44 (49) 0.71 19 3 55 13 40 50 (21) (3) (61) (14) 52 17 18 3 53 (58) (19) (20) (3) (59) 19 3 55 13 38 52 (21) (3) (61) (14) 53 18 17 2 51 (59) (20) (19) (2) (57) 0.98 0.76 0.92 0.88 adriamycin 50 mg/m2 day 1, vincristine 1 mg day 1, dexamethasone 40 mg days 1, 2, 3 and 4, each course repeated every 28 days). Phase II included cyclophosphamide (CY) 4 g/m2 given at day 0. G-CSF was administered at 10 mg/kg from day 3 to the last day of leukapheresis initiated upon recovery of leucocytes to 2 109/l. The percentage of circulating CD34 þ cells was evaluated as previously described.19 Two to four procedures were performed. A Fresenius Cell Separator AS 104 (MTS, Schweinfurt, Germany, EU) was used. Phase III was performed in a regular ward. It started at day 30; MEL100 was infused in 30 min. At day 31, stem cells were reinfused. G-CSF was administered at 5 mg/kg. A second course of MEL100 was given after 2–3 months. MEL200 regimen: Phase I included two or three DAV courses as previously described. Phase II included stem cell mobilisation and harvests performed after CY given at 5–7 g/m2, followed by G-CSF at 5 mg/kg as previously described for MEL100.6,20,21 Phase III was performed in a protected environment. The double-autograft programme was conditioned with MEL200 for both first and second transplant. Response criteria and statistics Partial response (PR) was defined as 50% reduction of serum myeloma protein and 90% decrease of Bence Jones proteinuria. Very good partial response (VGPR) was defined as 90% decrease of serum paraprotein. CR required disappearance of serum or urine myeloma protein analysed by standard electrophoresis and marrow plasmacytosis o5% for at least 6 weeks. All other results were regarded as failures. The proportion of patients with a given clinical characteristic was compared with the w2 test or Fisher’s exact test. Differences in means of continuous variables were assessed with Student’s t-test and checked with the Mann–Whitney U test. All tests were twotailed. Curves for EFS and OS were plotted according to the method of Kaplan–Meier and compared with the log-rank test.22 The Cox proportional hazard regression model was used to estimate the prognostic importance of different variables. The duration of EFS was calculated from the beginning of treatment until relapse, death, progression of disease, or the date the patient was last known to be in remission. The duration of OS was calculated from the beginning of therapy until death. The Leukemia survival curves of patients who relapsed after MEL100 or MEL200 were plotted from the date of relapse or disease progression. Results Response On an intent-to-treat basis, 92% of patients completed the MEL100 programme. All patients received the first course. Seven patients did not receive the second course (one lost during follow-up, two gastrointestinal toxicities, one secondary neoplasm, one renal toxicity, one cardiac toxicity, one inadequate stem cell collection). The second MEL100 was completed within a maximum of 4 months from the first. The median time between the first and second courses was 2.6 months. The frequency of PR, [VGPR], (CR) was 47%, [14%], (19%) after the first MEL100, and 41%, [15%], (35%) after the second MEL100 (Table 2). On an intent-to-treat basis, 88% of patients completed the MEL200 regimen. Three patients stopped treatment after phase II: one due to pneumonia, one cardiac toxicity, one progressive disease. Eight patients stopped during phase III: one due to pneumonia, one mucositis, three inadequate stem cell collection, one gastrointestinal toxicity, one MUD transplant, one sepsis. In all, 79 patients received a double MEL200 and completed the second within a maximum of 9.6 months from the first course. The median time between the first and second courses was 4.3 months. The frequency of PR, [VGPR], (CR) was 36%, [25%], (32%) after the first MEL200, and 17%, [30%], (48%) after the second MEL200 (Table 2). The number of patients who did not respond was similar for both MEL100 and MEL200 groups (P ¼ 0.4). The rates of CR (35 vs 48%, P ¼ 0.08) and VGPR (15 vs 30%, P ¼ 0.01) were slightly increased after two courses of MEL200. The CR rates were also increased by administration of both the second MEL100 (19 vs 35%, P ¼ 0.016) and second MEL200 course (32 vs 48%, P ¼ 0.03). Survival After a median follow-up of 47.7 months for MEL100 survivors, 31% were alive in remission and 69% had relapsed, including 10% who had died from disease progression. After a median follow-up of 36.6 months for MEL200 survivors, 59% were alive in remission and 41% had relapsed; of these, 38% died from disease progression. The median EFS was 31.6 months for MEL100 compared with 42.1 months for MEL200 (Po0.0005) (Figure 1). The median OS was similar for both groups: 67 months for MEL100 and 75 months for MEL200 (P ¼ 0.4) (Figure 2). The actuarial probabilities of EFS (OS) at 5 years after diagnosis were 21% (59%) after MEL100 and 43% (60%) after MEL200. Table 2 Clinical response to MEL100 or MEL200 CR VGPR PR NR Early deaths MEL100 (%) MEL200 (%) P 35 15 41 9 4 48 30 17 5 5 0.08 0.01 0.0003 0.4 1 Dose-intensive melphalan for myeloma A Palumbo et al 135 Figure 1 EFS of myeloma patients treated with melphalan at 100 mg/m2 (MEL100) or at 200 mg/m2 (MEL200). Figure 3 Survival after relapse of myeloma patients treated at diagnosis with melphalan at 100 mg/m2 (MEL100) or at 200 mg/m2 (MEL200). 9 months for patients relapsing after MEL200 (Po0.001) (Figure 3). Treatment at relapse was not standardised: 38% of MEL100 patients received a third MEL100 after relapse, and only 9% of MEL200 patients received a third intensified treatment with stem cell support (P ¼ 0.001). EFS was longer for MEL200, survival from relapse after transplant was superior for MEL100, but OS was identical for both groups. A multiple regression model, including all major clinical prognostic factors affecting outcome, was used to estimate the effect of the type of treatment, adjusted for potential confounders. The choice of treatment (MEL200) was the only factor that retained independent significance on EFS, but not on OS. No other variables modified the results when added to the model (Table 4). Figure 2 OS of myeloma patients treated with melphalan at 100 mg/m2 (MEL100) or at 200 mg/m2 (MEL200). The survival curves of patients who relapsed showed a better outcome for patients treated with MEL100. The median survival after relapse from MEL100 was 28 months compared with Table 3 Toxicity Treatment-related toxicity is illustrated in Table 3. The duration of neutropenia and thrombocytopenia was significantly shorter in the MEL100 group (Po0.0001). Both red cell and platelet transfusion requirements were significantly lower for MEL100 Haematologic and extra-haematologic toxicity MEL100 (n ¼ 173a) Duration of neutropenia (median) (days) Duration of thrombocytopenia (median) (days) No. of platelet transfusion (median) No. of red blood cell transfusion (median) Duration of hospitalisation (median) (days) Duration of intravenous antibiotics (median) (days) Unknown origin fever (%) Mucositis grade 3–4 (%) Viral infections (%) Pneumonia (%) Cardiac toxicity grade 3–4 (%) Pulmonary taxicity grade 3–4 (%) Renal toxicity grade 3–4 (%) Gastrointestinal toxicity grade 3–4 (%) Neurological toxicity grade 3–4 (%) 0–13 (5) 0–8 (2) 0–5 (1) 0–6 (0) 0–31 (7) 0–14 (0) 18 (10) 9 (5) 7 (4) 4 (2) 2 (1) 2(1) 1 (1) 2 (1) 1 (1) MEL200 (n ¼ 169a) 4–12 1–9 0–8 0–5 12–54 0–16 37 23 9 3 1 2 1 1 2 (8) (4) (2) (2) (15) (3) (22) (14) (5) (2) (1) (1) (1) (1) (1) P o0.0001 o0.0001 o0.0001 0.0020 o0.0001 0.05 0.008 0.016 0.97 0.99 0.99 0.99 0.99 0.97 0.97 a Toxicity is related to number of transplants administered. Leukemia Dose-intensive melphalan for myeloma A Palumbo et al 136 Table 4 Multivarite analysis EFS b2-Microglobulin Isotype IgA Stage II III Age Treatment P 0.5 0.78 0.4 0.3 0.04 0.0005 OS P b2-Microglobulin Isotype IgA Stage II III Age Treatment 0.55 0.6 0.58 0.51 0.39 0.34 patients (Po0.002). The median number of infused stem cells was significantly lower after MEL100 (3.7 106/kg) in comparison with MEL200 (5.72 106/kg, Po0.001). Haematologic toxicity was similar after the first and second courses of both MEL100 and MEL200. The differences of haematologic toxicity between MEL100 and MEL200 were mainly related to (i) dose of melphalan; (ii) patient’s age; and (iii) higher number of stem cells infused after MEL200. The median duration of hospitalisation for the MEL100 or MEL200 schedule was significantly shorter for MEL100 (Po0.0001). A substantial proportion of MEL100 patients were discharged 7 days after infusion and haematological recovery occurred at their home. By contrast, all MEL200 patients were hospitalised throughout the entire neutropenic period. The duration of intravenous antibiotics was slightly shorter for patients receiving MEL100 (P ¼ 0.05), and reflected a significantly lower incidence of unknown origin fevers (P ¼ 0.008). The incidence of mucositis (grade 3–4 toxicity, according to World Health Organization scale) was significantly lower for patients receiving MEL100 (P ¼ 0.016). No differences in terms of pulmonary, cardiac, neurologic and renal toxicity were observed. Four toxic deaths occurred in the MEL100 group (pulmonary thromboembolism, acute cardiac infarction, sepsis, pneumonia), and five in the MEL200 group (two pneumonia, one enteritis, one disease progression and one cardiac arrest). Conclusions Several studies have shown that high-dose chemotherapy with autologous transplantation is superior to standard treatment. In the first randomised trial, MEL140 þ TBI was superior to conventional chemotherapy: response rate was 81 vs 57% (Po0.001) and the 5-year OS probability was 52 vs 12% (P ¼ 0.03).2 In a case-matched control analysis, MEL200 was better than standard treatment in terms of PR (85 vs 52%; P ¼ 0.0001), EFS (5-year probability 36 vs 19%, P ¼ 0.0001) and OS (5-year probability 61 vs 39%, P ¼ 0.01).3 In a recent trial, 407 patients were randomly assigned to receive high-dose therapy and autologous transplant or standard conventionaldose combination therapy. CR rate (44 vs 8%, Po0.001), progression-free survival (31 vs 20 months, Po0.0001) and OS (54 vs 42 months, P ¼ 0.04) were again higher after the highdose regimen.23 In newly diagnosed patients, MEL100 was superior to standard oral melphalan for CR (47 vs 5%, Po0.01), EFS (34 vs 17 months, Po0.001) and OS (56 þ vs 48 months, Po0.01).16 These data suggest that both intensified approaches (MEL100) and myeloablative regimens (MEL200, MEL140 þ TBI) are more effective than standard therapy. The conditioning regimen is not standardised. Too many different schemes are used. Which is the less toxic and the Leukemia most effective regimen is still an open question. In a recent randomised study, MEL140 þ TBI was as effective as MEL200 alone (EFS: 21 vs 20 months, P ¼ 0.6; 45-month OS: 45 vs 66%, P ¼ 0.05), but more toxic. The authors conclude that MEL200 is less toxic and at least as effective as MEL140 þ TBI, considering MEL200 as the standard conditioning regimen. The increased toxicity may have been responsible for the borderline shorter OS of patients receiving MEL140 þ TBI. This study suggested that the increased toxicity might reduce survival.24 Here we describe a retrospective case-matched investigation of the clinical relationship between MEL100 and MEL200 in two groups of patients with comparable clinical conditions. Differences in main prognostic factors such as b2-microglobulin and Durie and Salmon clinical stage were eliminated. MEL200 was superior to MEL100 in terms of EFS (Po0.0005), while both regimens were equally effective in terms of CR (P ¼ 0.08) and OS (Po0.1). When oral melphalan was compared with MEL100 and/or MEL200, the CR rate increased from 1–5% to 30–50%. This tremendous increase in response may explain a significant outcome improvement. When we compared MEL100 with MEL200, the CR rate increased from 35 to 48%. This slight increase prolonged EFS but was not enough to induce a significant survival improvement. Caution is naturally required when drawing conclusions from a non randomised trial. Significant differences in outcome would perhaps emerge in a larger series. Even so, it is clear from our results that the response rate, EFS and OS are certainly not halved when MEL100 is used instead of MEL200. Both MEL100 and MEL200 induced a median OS of 5 years with a 40% probability of survival at 7 years. These figures are quite similar to those shown in the majority of international clinical trials on myeloma transplantation2,4,7,24 and significantly different from the median 3 years OS induced by conventional treatment.25 In a randomised Dutch study, patients received either two doses of intensified chemotherapy (melphalan 70 mg/m2) followed by myeloablative therapy (cyclophosphamide, TBI and stem cell reinfusion) or the intensified chemotherapy (melphalan 70 mg/m2) only. For patients receiving myeloablative treatment, CR rate was higher (29 vs 13%, P ¼ 0.002) and time to progression was longer (31 vs 25 months, P ¼ 0.04). By contrast, EFS (22 vs 21 months) and OS (47 vs 50 months) were unchanged. These data are quite similar to our findings. The better CR rate and the longer time to progression did not translate into prolonged survival. Toxicity was significantly higher for patients receiving myeloablative therapy, which might explain why the time to progression was prolonged while the EFS was not. On the other hand, cyclophosphamide and TBI as myeloablative regimen may have an anti-myeloma effect that is inferior to MEL200, which might also shorten the duration of EFS.26 The risk of excessive morbidity and treatment-related mortality has generally restricted MEL200 regimens to patients younger than 60–65 years. Unfortunately, the median age for myeloma patients at presentation is 70 years.27 Our results clearly show a lower toxicity for the nonmyeloablative MEL100 regimen. Severe mucositis, duration of neutropenia and thrombocytopenia, red blood cell and platelet transfusion were drastically reduced. The median duration of hospitalisation dropped from 15 to 7 days with a significant improvement in quality of life and a significant reduction of healthcare expenses. This lower incidence of toxicities occurred despite a significant median age difference (MEL100: median age 61 years; MEL200: median age 52; Po0.001). Dose-intensive melphalan for myeloma A Palumbo et al 137 Dose reduction is safe and prudent in the elderly. When such reduction is required and to what extent is a matter of discussion since the introduction of stem cell transplantation in myeloma. In the French randomised trial, exclusions were 18% for patients younger than 60 years, but 42% for those older than 60 years. After MEL200, the outcome for patients aged 65 years was not significantly different from that of younger patients in a match-pair analysis for prognostic factors.11,28 These data demonstrated that age, per se, does not contraindicate MEL200. Age increases the incidence of poor clinical conditions and concomitant diseases, and these are the major causes of the increase in treatment-related toxicity. Until now, the only alternative was conventional treatment. Here we demonstrate that MEL100 should be used as first choice in this subset. MEL100 should be offered to all patients aged 60–70 years and those who do not meet the inclusion criteria for MEL200. In conclusion, the MEL100 conditioning regimen is less toxic and slightly less effective compared with MEL200. MEL200 offers the possibility of a prolonged EFS, during which no therapy is required, and should be considered the standard for younger myeloma patients in good clinical condition. MEL100 must be the first alternative in elderly patients or in those in poor clinical condition. The end point should be always the best response rate with minimum toxicity. Patients and their physicians must evaluate both options in the light of their expected efficacy, toxicity, age and general condition. In this respect, MEL100 is a new and effective alternative. Acknowledgements This work was supported in part by Associazione Italiana Ricerca Cancro (AIRC), Associazione Italiana Leucemie (AIL), Compagnia di San Paolo and Ministero Università e Ricerca Scientifica e Tecnologica (MURST). We thank Miss Tiziana Marangon for her technical assistance in the preparation of manuscipt. We also thank the many medical and nursing colleagues who have participated in the treatment of patients. References 1 Alegre A, Dı́az-Mediavilla J, San Miguel J, Martinez R, Garcia Larana J, Sureda A et al. Autologous peripheral blood stem cell transplantation for multiple myeloma: a report of 259 cases from the Spanish Registry. Bone Marrow Transplant 1998; 21: 133–140. 2 Attal M, Harousseau JL, Stoppa AM, Sotto JJ, Fuzibet JG, Rossi JF et al. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. New Engl J Med 1996; 335: 91–97. 3 Barlogie B, Jagannath S, Vesole DH, Naucke S, Cheson B, Mattox S et al. Superiority of tandem autologous transplantation over standard therapy for previously untreated multiple myeloma. Blood 1997; 89: 789–793. 4 Barlogie B, Jagannath S, Desikan KR, Mattox S, Vesole D, Siegel D et al. Total therapy with tandem transplants for newly diagnosed multiple myeloma. Blood 1999; 93: 55–65. 5 Bjorkstrand B, Ljungman P, Svensson H, Hermans J, Alegre A, Apperley J et al. Allogeneic bone marrow transplantation versus autologous stem cell transplantation in multiple myeloma: a retrospective case-matched study from the European Group for Blood and Marrow Transplantation. Blood 1996; 88: 4711–4718. 6 Gianni AM, Tarella C, Bregni M, Siena S, Lombardi F, Gandola L et al. High-dose sequential chemoradiotherapy, a widely applicable regimen, confers survival benefit to patients with high-risk multiple myeloma. J Clin Oncol 1994; 12: 503–509. 7 Lenhoff S, Hjorth M, Holmberg E, Turesson I, Westin J, Nielsen JL et al. Impact on survival of high-dose therapy with autologous stem cell support in patients younger than 60 years with newly dignosed multiple myeloma: a population-based study. Blood 2000; 95: 7–11. 8 Moreau P, Misbahi R, Milpied N, Morineau N, Mahe B, Vigier M et al. Long-term results (12 years) of high-dose therapy in 127 patients with de novo multiple myeloma. Leukemia 2002; 16: 1838–1843. 9 Vesole DH, Tricot G, Jagannath S, Desikan KR, Siegel D, Bracy D et al. Autotransplants in multiple myeloma: what have we learned? Blood 1996; 88: 838–847. 10 Imrie K, Esmail R, Meyer RM. The role of high-dose chemotherapy and stem-cell transplantation in patients with multiple myeloma: a practice guideline of the Cancer Care Ontario Practice Guidelines Initiative. Ann Intern Med 2002; 136: 619–629. 11 Siegel D, Desikan KR, Mehta J, Singhal S, Fassas A, Munshi N et al. Age is not a prognostic variable with autotransplants for multiple myeloma. Blood 1999; 93: 51–54. 12 Avet-Loiseau H, Facon T, Grosbois B, Mangrageas F, Rapp MJ, Harousseau JL et al. Oncogenesis of multiple myeloma: 14q32 and 13q chromosomal abnormalities are not randomly distributed, but correlate with natural history, immunological features, and clinical presentation. Blood 2002; 99: 2185–2191. 13 Fassas A, Spencer T, Sawyer J, Zangari M, Lee CK, Anaissie E et al. Both hypodiploidy and deletion of chromosome 13 independently confer poor prognosis in multiple myeloma. Br J Haematol 2002; 118: 1041–1047. 14 Nilsson T, Lenhoff S, Turesson I, Rylander L, Mitelman F, Westin J et al. Cytogenetic features of multiple myeloma: impact of gender, age, disease phase, culture time, and cytokine stimulation. Eur J Haematol 2002; 68: 345–353. 15 Palumbo A, Pileri A, Triolo S, Omede P, Bruno B, Ciravegna G et al. Multicyclic, dose-intensive chemotherapy supported by hemopoietic progenitors in refractory myeloma patients. Bone Marrow Transplant 1997; 19: 23–29. 16 Palumbo A, Triolo S, Argentino C, Bringhen S, Dominietto A, Rus C et al. Dose-intensive melphalan with stem cell support (MEL100) is superior to standard treatment in elderly myeloma patients. Blood 1999; 94: 1248–1253. 17 Durie BGM, Salmon SE. Multiple myeloma, macroglobulinemia and monoclonal gammopathies. In: Hoffbrand AV, Brown MC, Hirsch J (eds). Recent Advances in Haematology. Edinburgh: Churchill Livingstone, 1977, pp 243–261. 18 Durie BGM, Salmon SE. A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment and survival. Cancer 1975; 36: 842–854. 19 Siena S, Bregni M, Brando B, Belli N, Ravagnani F, Gandola L et al. Flow cytometry for clinical estimation of circulating hematopoietic progenitors for autologous transplantation in cancer patients. Blood 1991; 77: 400–409. 20 Corradini P, Voena C, Tarella C, Astolfi M, Ladetto M, Palumbo A et al. Molecular and clinical remission in multiple myeloma: the role of autologous and allogeneic transplantation of hematopoietic cells. J Clin Oncol 1999; 17: 208–215. 21 Tribalto M, Amadori S, Cudillo L, Caravita T, Del Poeta G, Meloni G et al. Autologous peripheral blood stem cell transplantation as first line treatment of multiple myeloma : an Italian Multicenter Study. Haematologica 2000; 85: 52–58. 22 Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53: 457–481. 23 Child JA, Morgan GJ, Davies FE, Owen RG, Bell SE, Phil D et al. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. New Engl J Med 2003; 348: 1875–1883. 24 Moreau P, Facon T, Attal M, Hulin C, Michallet M, Maloisel F, Sotto JJ et al. Comparison of 200 mg/m2 melphalan and 8 Gy total body irradiation plus 140 mg/m2 melphalan as conditioning regimens for peripheral blood stem cell transplantation in patients with newly diagnosed multiple myeloma: final analysis of the Intergroup Francophone du myélome 9502 randomized trial. Blood 2002; 99: 731–735. 25 Gregory WM, Richards MA, Malpas JS. Combination chemotherapy versus melphalan and prednisone in the treatment of multiple myeloma: an overview of published trials. J Clin Oncol 1992; 10: 334–342. Leukemia Dose-intensive melphalan for myeloma A Palumbo et al 138 26 Segeren CM, Sonneveld P, van der Holt B, Vellenga E, Croockewit AJ, Verhoef GEG et al. Overall and event-free survival are not improved by the use of myeloablative therapy following intensified chemotherapy in previously untreated patients with multiple myeloma: a prospective randomized phase 3 study. Blood 2003; 101: 2144–2151. Leukemia 27 Ries L, Hankey BL, Miller BA. Cancer Statistic Review, 1973–1988 (DHHS publ-NIH-n.91-2789). Washington, DC: US Govt Printing Office, 1991. 28 Sirohi B, Powles R, Treleaven J, Mainwaring P, Kulkarni S, Pandha H et al. The role of autologous transplantation in patients with multiple myeloma aged 65 years and over. Blood 2000; 25: 533–539.
© Copyright 2026 Paperzz