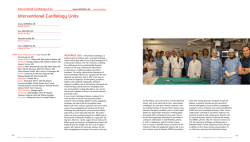
Attualità terapeutiche e diagnostiche delle patologie della retina S.C.Oculistica Direttore Dr.Guido CARAMELLO Enza PIROZZI 21-05-2014 TOMOGRAFIA A COERENZA OTTICA (OCT) La OCT è una tecnica di imaging medico: • non invasiva; • fornisce immagini ad alta risoluzione della retina e della parte anteriore dell’occhio: il potere di risoluzione spaziale è di circa 7-10 µm ; • si basa su una tecnica interferometrica che utilizza luce del vicino infrarosso (λ da 700 nm a 1 µm); • La luce ad alta lunghezza d’onda permette di penetrare a maggiore profondità nel tessuto biologico rispetto ad altre tecniche; • Le prime immagini in vivo della struttura della retina sono state pubblicate nel 1993. 2 UN MODERNO APPARATO DI OCT 3 L'OCT proietta sulla retina un fascio di lunghezza d'onda nel vicino infrarosso (820 nm) generato da un diodo superluminescente; confronta quindi i tempi di propagazione dell'eco della luce riflessa dalla retina con quelli relativi allo stesso fascio di luce riflesso da uno specchio di riferimento posto a distanza nota. Benché la luce riflessa dalla retina sia composta da echi multipli, la distanza percorsa dagli stessi viene determinata tramite la variazione della distanza dallo specchio di riferimento. L'interferometro OCT rileva elettronicamente, raccoglie, elabora e memorizza gli schemi di ritardo dell'eco provenienti dalla retina. I tomogrammi vengono visualizzati in tempo reale utilizzando una scala in falsi colori che rappresenta il grado di riflettività dei tessuti posti a diversa profondità: i colori scuri (blu e nero) rappresentano zone a minima riflettività ottica, mentre i colori chiari come il rosso ed il bianco definiscono zone molto riflettenti. 4 Infine il sistema memorizza le scansioni selezionate, permettendone la successiva elaborazione, tra cui la possibilità di correggere l'effetto dei movimenti oculari longitudinali. L'OCT è quindi un esame semplice, rapido, non invasivo ed altamente riproducibile, ma è limitato dalla presenza di qualsiasi opacità dei mezzi diottrici (edema o leucomi corneali, cataratta, emovitreo) e dalla miosi. Le immagini tomografiche ottenute con l'OCT permettono uno studio sia di tipo qualitativo che quantitativo del tessuto retinico, con la possibilità di dirigere la scansione direttamente verso la zona di interesse grazie alla contemporanea osservazione della retina. Dal punto di vista qualitativo su ogni scansione si può effettuare un'analisi della morfologia e del grado di riflettività degli strati retinici. Per quanto riguarda la valutazione quantitativa lo strumento permette di misurare lo spessore della retina, che può 5 anche essere rappresentato in mappe di spessore. RICOSTRUZIONI: SITUAZIONI FISIOLOGICHE E PATOLOGIE Sezione tomografica della regione maculare in condizioni normali Fibrosi pre-retinica. Si possono osservare aumento dello spessore retinico, scomparsa della depressione foveale e presenza di aree a diminuita reflettività all'interno della retina, indice di edema intraretinico L'OCT è l’esame più indicato per selezionare i casi di foro maculare e di sindrome dell'interfaccia vitreo-retinica potenzialmente suscettibili di trattamento chirurgico 6 (vitrectomia) RICOSTRUZIONI: PATOLOGIE L'OCT consente una semplice e sensibile diagnosi dell'edema maculare secondario a retinopatia diabetica, occlusione della vena centrale della retina, uveite, fibrosi preretinica o post-intervento di cataratta. In questi casi le sezioni tomografiche mostrano un aumento più o meno marcato dello spessore della retina, che può mostrare al suo interno aree tondeggianti a ridotta reflettività, segno di accumulo intraretinico di liquido (edema cistoide). L'ispessimento retinico può essere quantificato e venir rappresentato in mappe di spessore retinico, di evidente utilità nel corso del follow-up del paziente 7 RICOSTRUZIONI: PATOLOGIE Distacco del neuroepitelio maculare. Nella Corioretinopatia Sierosa Centrale di tipo acuto l'OCT permette di valutare in modo oggettivo e quantificabile il distacco del neuroepitelio e l'eventuale presenza di piccoli distacchi dell’epitelio pigmentato associati, con la possibilità di monitorarne l'evoluzione spontanea o successiva a trattamento fotocoagulativo. Anche piccoli sollevamenti del neuroepitelio, non clinicamente identificabili all'esame biomicroscopico, possono essere evidenziati dall’OCT sotto forma di sottili bande a ridotta reflettività comprese tra il complesso EPRcoriocapillare e lo strato dei fotorecettori 8 AMD Age-related maculopathy Malattia degenerativa che colpisce la porzione centrale della retina (macula) con frequenza crescente sopra i 50 anni (oltre 1 su 10 >85 anni) • Circa 20.000 nuovi casi per anno in Italia • 150.000-250.000 casi prevalenti La maculopatia correlata all’età è la prima causa di grave ipovisione nei paesi industrializzati compare compare dopo dopo ii 50 50 aa aa di di eta’ eta’ 10% 10% della della popolazione popolazione tra tra ii 65 65 ee ii 75 75 aa aa 30% 30% della della popolazione popolazione >75 >75 aa aa Destinate Destinate aa crescere crescere di di 33 volte volte nei nei prossimi prossimi 25 25 aa aa Kansky Kansky 2004 2004 Epidemiologia La DMS è la prima causa di cecità legale nei Paesi Industrializzati >50 aa. Dopo i 50 aa, l’incidenza cresce costantemente. Considerando che nel 2020 è previsto un aumento del 107% della popolazione over 65aa la DMS va considerata malattia sociale. Framingham Eye Study Beaver Dam Eye Study Baltimore Eye Study Reticolo di Amsler SINTOMI Calo Calo del del visus visus (( >> >> nella nella DMLE DMLE umida), umida), visione visione offuscata, offuscata, progressiva progressiva perdita perdita visione visione centrale centrale Immagini Immagini distorte, distorte, ondulate, ondulate, interrotte, interrotte, irregolari irregolari Difficoltà Difficoltà alla alla lettura lettura << Visione Visione dei dei colori, colori, << Sensibilità Sensibilità al al contrasto contrasto Fotopsie Fotopsie (( sfarfallii, sfarfallii, lampi lampi luminosi) luminosi) AMD Classificazione AREDS Age-Related Eye Disease Study e Wisconsin Grading System •No DMS: assenza o poche e piccole drusen <64 micron •DMS precoce: combinazione di molte piccole drusen o poche drusen intermedie (63-124 micron) o anomalie EPR •DMS intermedia numerose drusen intermedie,o almeno una large drusen >125 micron o atrofia geografica non coinvolgente la fovea DMS avanzata: “secca” e“umida” Bird, Bressler 1995 DMS Avanzata DMS secca: Atrofia Geografica dell’EPR e della coriocapillare coinvolgente la fovea DMS essudativa: Neovascolarizzazione coroideale (CNV) Distacco sieroso e/o emorragico EPR Essudati lipidici Proliferazione fibrovascolare sottoretinica e subEPR Cicatrice disciforme La diagnosi di DMS Neovascolare e Atrofica viene posta in base alla obiettività clinica, ma è confermata o ampliata dalle tre principali tecniche di “Imaging” della Macula, che hanno scopi diagnostici e terapeutici: FAG, Angiografia al verde indocianina (ICG) OCT ICG FAG OCT FAG fluoresceina sodica, picco di eccitazione tra 465-490 nm(luce blu) e picco di emissione (520-530 nm) iniettata e.v. Permette l’ analisi dettagliata del circolo retinico 80% si lega alle proteine plasmatiche In condizioni normali , non fuoriesce dal circolo retinico, per la presenza delle giunzioni serrate (barriera emato-retinica). La patogenesi della formazione dei neovasi coroideali è meno nota di quella dei neovasi in corso di retinopatia ischemica UP-regulation Angiogenesi Fattori Pro-angiogenesi VEGF Vascular-EndothelialGrow-Factor Downregulation Fattori angiostatici PEDF Pigment-EpithelialDerived-Factor TERAPIA FORME NEOVASCOLARI RAZIONALE Rimuovere Obliterare neovasi Inibire neoangiogenesi neovasi Terapia Terapia Terapia Fisica: laser e PDT medica chirurgica Terapia chirurgica •Rimozione della MNSR •Traslocazione Maculare •Trapianto di EPR Trapianto di Epitelio Pigmentato Razionale ripristinare la funzionalità ridotta o assente dell’epitelio pigmentato retinico Bruch Novel Drugs for Ophthalmic Indications • Ranibizumab has been approved by AIFA: – To treat patients with neovascular AMD – For macular edema following retinal vein occlusion (RVO) – For DME • Aflibercept (VEGF Trap-Eye) is recently approved by the AIFA for treating neovascular AMD. • Intravitreal bevacizumab is widely used off-label for the treatment of these conditions, especially neovascular AMD. Anti-VEGF intravitreali • . • . Ant-VEGF therapy HYPOXIA VEGF Isoforms VEGF A Proteins Anti VEGF VEGF receptors Neovascularization Retina Anterior Segment BEVACIZUMAB (AVASTIN) • Humanized mono-clonal antibody. • Active Against all the isoforms of VEGF’s. • Approved drug for treatment of metastatic colorectal cancer. BEVACIZUMAB RANIBIZUMAB (AVASTIN) (LUCENTIS) • Full Sized Antibody. • Antibody Fragment. • 148 kilodaltons. • 48 kilodaltons. • Half Life 20 days. • Half Life of 3 days. • Clearance is slow. • Clearance 100 folds • Long action & less faster. 140 times higher affinity. dosage. • Cost’s less. • • Costly. BENEFITS OF BEVACIZUMAB • High efficacy. • Longer half life up to 20 days and thus fewer • • • • • • injections. Lack of preservative. Higher safety dose: Normal i/v dose is 1.25mg Retinal toxicity occurs at dosage > 3.5mg. Insignificant systemic absorption and effect. No experimentally proven toxicity. Lower cost. Wide availability. Eylea • Aflibercept è una proteina sintetizzata con la tecnologia del DNA ricombinante. Sulla porzione fissa costante della IGG umana sono stati montati i domini chiave dei recettori umani VEGFR1 e VEGFR2. Si ottiene così un "recettore" potenziato, solubile e iniettabile, in grado di catturare e inattivare VEGFA, VEGFB e PlGF. Eylea • Eylea ha una affinità per i VEGF 150 volte superiore rispetto a quella che essi hanno per i loro recettori naturali. Per questo appena iniettato Eylea sarà in grado di catturarli prima che possano legarsi ai loro siti innescando il danno. Eylea • Lo studio registrativo View ha dimostrato l'equivalenza terapeutica di Aflibercept e Ranibizumab con un numero inferiore di iniezioni: 7 vs 12. ANTI-VEGF COMPLICATION’S • Vitreous Hemorrhage. • Accidental injury to Lens capsule. • Raised IOP. • Retinal detachment. • Central Retinal Artery Occlusion. • Endophthalmitis. Update on Anti-VEGF Therapy in Diabetic Macular Edema, Neovascular AMD, and Retinal Vein Occlusion A New Focus on Ophthalmic Disease • This drug class initially was used to manage neovascular age-related macular degeneration (AMD). • Its value recently was affirmed for treating both branch retinal vein occlusion (BRVO)4 and central retinal vein occlusion (CRVO).5 • Further clinical data support their use in managing diabetic macular edema (DME).6 Clinical Trials of VEGF Inhibitors The READ,3,7 RISE,8 and RIDE8 trials involved the use of ranibizumab in patients with DME. • The DA VINCI trial9 demonstrated the effect of aflibercept therapy in DME patients. • The 2-year results of the CATT trial10 compared use of bevacizumab with ranibizumab therapy in AMD patients. Clinical Trials of VEGF Inhibitors • Investigators involved in the VIEW 1 and VIEW 2 studies11 reported on the use of aflibercept in patients with neovascular AMD. • The management of RVO changed after analysis of the CRUISE and BRAVOstudy results. • Further information has been gathered in the HORIZON study.. Issues Involved in Using VEGF inhibitors • Monthly versus as-needed dosing • The choice of an anti-VEGF agent for treating each condition • Corticosteroid and laser therapy in patients affected by RVO and DME • The safety of intravitreal injections of VEGF inhibitors Diabetic Macular Edema Diabetic Macular Edema: DRCR Trial • In the Diabetic Retinopathy Clinical Research Network • (DRCR) protocol I,6,13 investigators compared sham therapy plus prompt focal laser treatment with: – Ranibizumab plus prompt laser therapy – Ranibizumab plus deferred laser treatment – Triamcinolone plus prompt laser therapy Two-year follow-up data recently showed improved visual acuity and central foveal thickness in both ranibizumab groups as compared with those receiving sham plus laser therapy or triamcinolone plus laser therapy.14 Diabetic Macular Edema: RISE and RIDE Trials • RISE8 and RIDE8 were two parallel studies comparing • • • the use of 0.3 or 0.5 mg of ranibizumab given monthly with sham therapy for DME. In the RIDE trial, patients receiving 0.3 and 0.5 mg of ranibizumab gained 8.6 and 9.7 letters of visual acuity, respectively. Similar results were reported in the RISE trial, with patients given 0.3 mg of ranibizumab gaining 10.0 letters and those given 0.5 mg gaining 9.3 letters. Patients receiving ranibizumab at either dose level showed improvement in visual acuity and retinal thickness and a reduction in diabetic retinopathy. Diabetic Macular Edema: READ 3 Trial • The READ 3 trial7 compared two different ranibizumab • • • doses in patients with DME. Patients were randomized to groups receiving 0.5 or 2.0 mg of ranibizumab monthly for 6 months. At month 6, patients in the 0.5-mg group gained a mean of 8.72 letters, whereas those in the 2.0-mg group gained a mean of 7.35 letters. At month 12, patients in the 0.5-mg group gained 10.88 letters as compared with the 7.39 letters gained by the 2.0-mg group (P = 0.03). Diabetic Macular Edema: BOLT Study • The BOLT study15 compared the use of bevacizumab with focal laser therapy in patients with DME. • Patients in the bevacizumab group gained a mean of 8.6 letters, whereas those in tThe macular laser therapy group lost a mean of 0.5 letters. • Central foveal thickness also was reduced in the bevacizumab group as compared with the laser treatment group. Diabetic Macular Edema: DA VINCI Study Results from the DA VINCI trial9 demonstrated improvement in the eyes of patients with DME who used aflibercept as compared with patients who underwent focal laser therapy. Diabetic Macular Edema: Treatment Considerations The current VIVID-DME (ClinicalTrials.gov NCT01331681) and VISTA DME (ClinicalTrials.gov NCT01363440) trials are examining use of a loading dose of aflibercept every month for 6 months followed by dosing every 6 months. – Data on these phase III trials should be available in the coming years. Diabetic Macular Edema: Corticosteroid Therapy • Corticosteroid therapy continues to be an option for patients with DME. • However, it tends to be used now in individuals who do not respond to antiVEGF treatment. • Increased intraocular pressure and cataracts continue to be the main adverse effects related to the use of corticosteroids. Diabetic Macular Edema: FAME Trial • The FAME trial16 examined the use of a fluocinolone acetonide implant in patients with DME. • At 2 years, a greater than 15-letter improvement in visual acuity was achieved in: Diabetic Macular Edema: Corticosteroid Therapy • The FDA has not approved the use of fluocinolone acetonide implants for treating DME because of insufficient safety data. • Marketing of the implant for this indication is approved in Europe. In selected patients, corticosteroid treatment remains an option. Neovascular AMD Neovascular AMD: Clinical Data and Options • AMD is the leading cause of blindness • During the past few months, data from several large • trials have impacted treatment options. – Use of ranibizumab for neovascular (exudative) AMD was first reported in the MARINA2 and ANCHOR3 studies. – Frequency of ranibizumab dosing has been examined in the PIER,18 PrONTO,19 SUSTAIN,20 EXCITE,21 and HORIZON22 trials. As anti-VEGF treatment alternatives have expanded, ophthalmologists now have 3 options: ranibizumab, aflibercept, and off-label bevacizumab. Neovascular AMD: The CATT Trial • The results also affirmed the effectiveness of • • off-label bevacizumab in treating neovascular AMD. differences in results between groups given monthly or as-needed dosing would increase further after 2 years. Given that many patients with neovascular AMD are treated for longer than 2 years, clinicians are greatly interested in the long-term effects of therapy. Neovascular AMD: The VIEW Trials • Results from the VIEW 1 and VIEW 2 trials, which compared the use of aflibercept with ranibizumab therapy for exudative AMD, were reported recently.11 • These parallel, noninferiority trials randomized a total of 1,217 North American patients – Three monthly 2-mg aflibercept injections given as a loading dose followed by 2 mg of aflibercept every 2 months Neovascular AMD: The VIEW Trials • In 94%–96% of patients, moderate vision loss was prevented. • The three aflibercept groups had results that were noninferior to those observed in the ranibizumab group. • Patients receiving 2.0 mg of aflibercept monthly experienced a 10.9-letter gain as compared with an 8.1-letter gain observed in patients given monthly ranibizumab. Neovascular AMD: The VIEW Trials • The VIEW 2 trial enrolled 1,240 patients in Europe, Asia, and Latin America and had outcomes similar to those of the VIEW 1 trial.11 • Aflibercept may be an option in patients who do not respond well to ranibizumab or bevacizumab. Neovascular AMD: The CATT Trial • Geographic atrophy increased in the monthly dosing groups when compared with the as-needed dosing groups. Retinal Vein Occlusion Retinal Vein Occlusion: FDA-Approved Drugs for Treating RVO • In 2009, the FDA approved the use of a • • • dexamethasone intravitreal implant for the treatment of macular edema following RVO. The following year, it approved the use of intravitreal ranibizumab for the same indication. In the past, RVO initially would have been treated with observation. Now, based on data from the CRUISE and BRAVO studies, prompt treatment of RVO with ranibizumab has become commonplace. Retinal Vein Occlusion: Clinical Trials • Investigators involved in the COPERNICUS study2reported data showing an improvement in macular edema after 6 months of monthly aflibercept therapy in patients with CRVO. • Treatment regimens for RVO now typically start with monthly injections of anti-VEGF agents before patients are switched to asneeded dosing with monthly monitoring. OZURDEX CRVO AV 0,05 AV 0,1….after 3 months without therapy AV 0.4 ….after 3 injections of Avastin AV 0,4 …after 1 months from Ozurdex BRVO+OZURDEX AV 0,1 AV 0,6 …..After 3 months Retinal Vein Occlusion: Clinical Trials • Based on data from the HORIZON trial, in which patients initially enrolled in CRUISE or BRAVO continued therapy with asneeded treatment, fewer injections were required after the initial 12 months of therapy. • Focal laser therapy often is used adjunctively after 5–6 months of initial therapy. Safety of Anti-VEGF Therapy • In recent clinical trials evaluating VEGF inhibition in patients with DME, exudative AMD, or RVO, endophthalmitis occurred in about 1% of patients, about the same frequency as reported in prior studies. • As previously mentioned, increased geographic atrophy has been observed in patients with neovascular AMD receiving monthly injections of ranibizumab or bevacizumab.10 – However, this finding has not been reported in patients who were treated with VEGF inhibitors for DME or RVO. – It is not clear whether this increase in geographic atrophy is directly related to anti-VEGF therapy. • Systemic adverse effects in patients with neovascular AMD previously were evaluated in the SAILOR trial. DISTACCO SIEROSO DEL NEUROEPITELIO Soggetti giovani 20-45 anni M>F Metamorfopsia Sintomi soggettivi Micropsia Scotoma positivo Causa Predisposizione individuale A A volte volte si si associano associano piccoli piccoli distacchi distacchi e/o e/o alterazioni alterazioni cicatriziali cicatriziali dell’epitelio dell’epitelio pigmentato pigmentato CASO CLINICO CRS: SEDE INFEROFOVEALE O TERAPIA TERAPIA FOTODINAMICA FOTODINAMICA VERTEPORFINA -MA) VERTEPORFINA (BPD (BPD-MA) CH2 H2C O H2C O C H H2C NH O C H 2 N Affinità delle metalloporfirine per i tumori descritta nel 1940 NH D H2 O CH2 O I derivati dell’ematoporfirina sono stati usati nel trattamento clinico dei tumori O H O H2C O Si formano ccomplessi omplessi verteporfina -LDL verteporfina-LDL I complessi verteporfina verteporfina-LDL -LDL si accumulano nell nell’endotelio ’endotelio dei neovasi coroideali La verteporfina attivata dalla luce laser produce radicali liber liberii dell ’ossigeno dell’ossigeno I radicali liberi danneggiano ll’endotelio ’endotelio dei neovasi, occludono le membrane neovascolari sottoretiniche, preservando ll’EPR ’EPR e la retina Occlusione Occlusione neovasi neovasi con con trombi trombi ee danno danno ultrastrutturale ultrastrutturale dell’endotelio. dell’endotelio. Numerosi Numerosi neovasi neovasi con con vacuolizzazione vacuolizzazione ee frammentazione frammentazione dell’endotelio. dell’endotelio. Qualche Qualche globulo globulo rosso rosso extravasale. extravasale. Riscontro Riscontro di di neovasi neovasi con con endotelio endotelio normale normale e/o e/o cellule cellule endoteliali endoteliali immature. immature. Possibile Possibile vacuolizzazione vacuolizzazione delle delle cellule cellule dell’epitelio dell’epitelio pigmentato pigmentato Schnurrbusch U.E.K. et al. ‘01 CASO CLINICO PRE POST Enzymatic Vitreolysis with Ocriplasmin for Vitreomacular Traction and Macular Hole Progression of Vitreomacular Traction to Macular Hole Normal OCT Normal vision VMA causing VMT Metamorphop sia VMA causing macular hole Central blindness MH incidence estimated between 8-30 /100 000 3 times more frequent in females in 11%> 80% have VMT OCT, Bilateral optical coherence tomography GO (Oftalmologo Generale) Specialista retina medica. Specialista retina chirurgica percorso diagnostico e terapeutico in fori maculari (MH) Sintomi • visione distorta • minorazione visiva • raramente la cecità ... A Case of Macular Hole Closure After Intravitreal Ocriplasmin Injection, shown by Spectral Domain OCT Stalmans P et al. N Engl J Med 2012;367:606 (supplementary material) Next slide MIVI study • Vitreous manipulation effected through intravitreal injection may occasionally result in a PVD, in which case, the placebo injection of 0.1 mL may have induced some treatment response • The superior therapeutic effects of the ocriplasmin injection would then be indicative of an additional biologic effect of enzymatic vitreolysis over placebo Stalmans P et al. N Engl J Med 2012;367:606 Next slide MIVI study • Enzymatic vitreolysis represents a means to resolve VMT and to close MH • Intravitreal injection of ocriplasmin was superior to injection of placebo in altering the vitreoretinal interface of affected eyes, although it was accompanied by some, mainly transient, ocular adverse events Stalmans P et al. N Engl J Med 2012;367:606 • „ Watchful waiting“ of VMT can lead to • • • irreversible retinal damage, cysts and hole formation Spontaneous separation of VMT occurs rarely Vitreous surgery indicated if VA loss or disease progression but surgical trauma to retina possible as well as complications (f.Ex. hemm, endop, RD) Pharmacologic treatment to vitreous separation may separate the vitreous timely, will cause less manipulation to the retina and improve vision in a considerable number of patients
© Copyright 2026 Paperzz