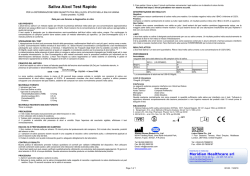
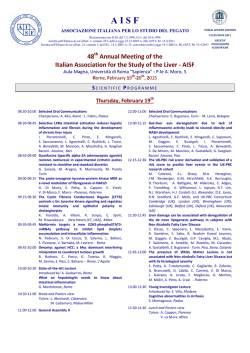
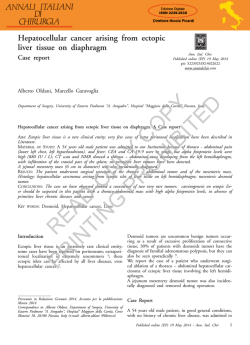
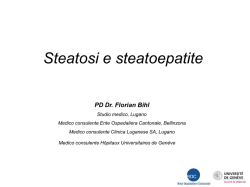
Il danno epatico da alcol Giovanni Addolorato Unità Operativa di Alcologia, UOC di Medicina Interna e Gastroenterologia, Università Cattolica di Roma - Policlinico “Agostino Gemelli” Dipartimento Politiche Antidroga, Presidenza del Consiglio dei Ministri Giovanni Addolorato Unità Operativa di Alcologia, UOC di Medicina Interna e Gastroenterologia, Università Cattolica di Roma - Policlinico “Agostino Gemelli” - Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d’interesse in relazione a questa presentazione - la presentazione contiene discussione di farmaci in studio e ad uso off-label (Baclofen) Alcohol Unit: drink 1 drink = 12-14 g pure alcohol What is light-to-moderate drinking? - Men: Up to 2 drinks per day - Women: Up to 1 drink per day PATOLOGIE ALCOL - RELATE CARDIOPATIA ENCEFALOPATIA MIELOPATIA INFEZIONI ULCERA GASTRICA E DUODENALE EPATOPATIA PANCREATITE IMPOTENZA NEOPLASIE TUBO DIGERENTE MIOPATIA E MALNUTRIZIONE ALCOL E FEGATO RISCHIO DI EPATOPATIA CRONICA 20 Epatopatia cronica alcolica 20 Cirrosi alcolica Maschi Femmine Maschi Femmine 16 Rischio relativo Rischio relativo 16 12 8 12 8 4 4 0 0 <1 1-6 7-13 14-27 28-41 42-69 >/=70 <1 1-6 7-13 14-27 28-41 42-69 >/=70 Becker et al, Hepatology 1996 Relationship between daily alcohol consumption and non-cirrhotic (NCLD) and cirrotic (CLD) alcohol induced liver Damage as derived from the cohort Dionysos population. No Alcohol intake damage (g per day) (%) Teetotaler 99,9 NCLD CLD (%) (%) OR for NCLD OR for CLD 0 0,04 0 0 0 0 < 30 99,3 0,5 0,15 31-60 97,2 1,8 1 61-90 93 4,7 2,3 20,2 25 91-120 91,6 3,5 4,9 15,1 52,9 >120 86,5 7,8 5,7 35,8 63,2 7,5 10,9 Bellentani et al, Gut 1997 ALCOL E FEGATO L’abuso alcolico rimane la più frequente causa di cirrosi epatica nei Paesi Occidentali Tilg & Day, Nat Clin Pract Gastroenterol Hepatol 2007 21% 36% HCV ALCOL HBV CBP HCV+ALCOL HBV + ALCOL EMOCROMATOSI CRIPTOGENETICA Bellentani S et al, Hepatology 1994 HCV HCV+ALCOL ALCOL HBV + ALCOL HBV ALTRO Sagnelli E et al, J Med Virol 2001 ALCOL E FEGATO PATOGENESI DEL DANNO Alcol & Metaboliti ALCOL E FEGATO PATOGENESI DEL DANNO EPATICO ACETALDEIDE ADDOTTI PROTEICI reazioni immunitarie NECROSI EPATOCITI ALCOL stress ossidativo perossidazione lipidica FIBROSI ↑ permeabilità intestinale ENDOTOSSINE cellule di Kuppfer Gramenzi et al, Aliment Pharm Ther 2006 Oxidative damage and alcohol intake caused by free radical intermediates Addolorato et al. Dig Dis Sci, 2001 ALCOL E FEGATO PATOGENESI DEL DANNO Alcol & Metaboliti Genere Razza Modalità Nutrizione Virus Co-fattori ALCOL E FEGATO IL SUBSTRATO GENETICO • GENERE • RAZZA • MODALITA’ DI ASSUNZIONE ↓ volume di distribuzione ↓ ADH gastrica < estrogeni ↑ risposta immunitaria ALCOL E FEGATO IL SUBSTRATO GENETICO • GENERE • RAZZA • MODALITA’ DI ASSUNZIONE < < ALCOL E FEGATO MODALITÀ DI ASSUNZIONE 30.000 morti /anno prevalenza di vino prima causa di morte fino a 24 anni prevalenza di birra prevalenza di superalcolici “BINGE DRINKING” VINO DURANTE IL PASTO ALCOL E FEGATO MODALITÀ DI ASSUNZIONE p < 0.001 Assunzione prolungata di bevande alcoliche > 30 g/die FUORI DEI PASTI p < 0.001 SOLO AI PASTI Bellentani et al, Gut 1997 ALCOL, DANNO METABOLICO E NUTRIZIONE • in pazienti con abuso alcolico: - incrementata REE - ridotta FM - incrementato WHR - incrementata ECW - ridotta ICW Spesa energetica/kg peso corporeo ** 0.18 0.15 g/min Kcal/24 h/Kg * Velocità di ossidazione dei substrati 0.12 0.09 CONTROLLI ALCOLISTI ** 0.06 0.03 0 LIP CHO Addolorato et al, Am J Gastroenterol 2000 Distribuzione del grasso corporeo: WHR WHR 1,1 1 * * P < 0.01 * 0,9 ** P < 0.001 0,8 0,7 0,6 Addolorato et al, J Internal Med 1998 Uomini Donne A) SOCIAL DRINKER BEHAVIOUR ATP SYNTHESIS CH3 -CH2 -OH (ETHANOL) NAD+ ADH CH3 -CHO + NADH + H+ (ACETALDEHYDE) FATTY ACIDS MITOCHONDRIA NADPH + H+ + MEOS B) CHRONIC ALCOHOL ABUSE Hypothalamic pituitary CH3 -CH2 -OH (ETHANOL) O2 CH3 -CHO + NADP+ (ACETALDEHYDE) GLUCOCORTICOIDS adrenal axis activation ADH NAD+ REDUCED FAT MASS AND ALTERATION OF FAT DEPOSITION CH3 -CHO + NADH + H+ (ACETALDEHYDE) stress FR MITOCHONDRIA ADAPTATION/ REARRANGEMENT GIANT MITOCHONDRIA NADPH + H+ + O2 CH3 -CHO + NADP+ (ACETALDEHYDE) HEAT W/H ATP SYNTHESIS Oxidative MEOS INDUCTION H2 O + CO2 FAT OXIDATION FAT OXIDATION FR ACETATE CATECHOLAMINE RELEASE CARDIAC OUTPUT ENERGY EXPENDITURE Addolorato et al. J Int Med 1998 Gasbarrini G et al, Ann Ital Med Int 2003 ALCOL E FEGATO DANNO EPATICO 0 – 30% Fegato normale 60 – 100% Steatosi epatica 20 – 40% Steatoepatite EASL Clinical Practical Guidelines, J Hepatol 2012 10 – 15% Fibrosi/Cirrosi ALCOL E FEGATO COMORBILITÀ HCV Alcol HCV OR 0 + 1 9,2 25 – 50 + + + + 0,9 9,5 4,5 26,1 13,0 133,4 15,0 147,2 S index (g/die) 75 – 100 125 – 150 >175 Rischio di sviluppare cirrosi 1,1 2,2 6,5 6,6 Corrao & Aricò, Hepatology 1998 Moderate Alcohol Consumption and HCV • Investigation of 78 HCV-infected patients with alcohol consumption <40g/d, who underwent two liver biopsies in a mean interval of 6.3 years. Progressive fibrosis with increased: - total alcohol consumption - daily alcohol consumption - frequency of drinking occasions Westin et al., J Viral Hepatol 2002 • Prospective study with 260 HCV-infected patients showed that even moderate alcohol consumption, as low as 31-50 g/day in men and 2150 g/day in women, may aggravate histological lesions. Hezode et al., Aliment Pharmacol Ther, 2006 HCV e alcol: sinergismo Incremento di fibrosi e di rischio di HCC: meccanismi - Aumentata produzione di radicali liberi dell’ossigeno - Accumulo di ferro - Induzione di steatosi - Modulazione della risposta immunitaria e dell’apoptosi - Danno diretto sul DNA As reviewed in: Singal & Anand, J Clin Gastroenterol 2007 Mueller et al., Word J Gastroenterol 2009 McCartney & Beard. World J Gastroenterol 2010 - Effetto sulla viremia: aumentata replicazione virale in presenza di uso/abuso alcolico Addolorato et al, Alcohol Res 2000 Zhang et al, Hepatology 2003 What is light-to-moderate drinking? [1 drink = 12-14 g pure alcohol] - Men: Up to 2 drinks per day - Women: Up to 1 drink per day When is "low-risk" drinking still too much? - taking medications that interact with alcohol - medical condition that can be made worse by drinking e.g. liver disease (such as HCV), bipolar disorder, abnormal heart rhythm, and chronic pain. - underage - planning to drive a vehicle or operate machinery - pregnant or trying to become pregnant Treatment of ALD Nutrition and Antioxidants Steroid (prednisolon) Pentossifillin Anti-TNFα (infliximab, etanercept) Propiltiouracil Colchicin NCB1 agonist/antagonist Total alcohol abstinence • The most effective management strategy for alcoholics with ALD is to achieve total alcohol abstinence Medical and surgical treatments for ALD have limited success when drinking continues Tilg & Day. Nat Clin Pract Gastroenterol Hepatol 2007 • Persistent alcohol intake has been associated with increased mortality in patients with liver cirrhosis Pessione et al. Liver Int 2003 • Effective Anticraving Medications for Alcohol Dependence Medication Mechanism of Action Naltrexone (Nalorex® and Vivitol®); Nalmefene ? Mu opioid receptor inhibitor ?OPRM1 (label) Acamprosate (Campral®) Glutamate receptor modulation (label) Ondansetron (Zofran®) Serotonin- 3 receptor antagonist (off-label) Type B/SERT & 3-UTR Sodium Oxybate (GHB) (Alcover®) GABA-B/ GHB agonist (label in Italy and Austria) Baclofen (Lioresal® and Liofen®) GABA-B antagonist (off-label) Alcohol dependent; Severe liver disease Topiramate (Topamax®) GABA/Glutamate modulator Heavy current drinkers (off-label) Addolorato et al, Nature Neuropsychopharmacol 2012 Baclofen and liver cirrhosis Baclofen showed its safety and efficacy in achieving and maintaining alcohol abstinence in alcohol-dependent patients with liver cirrhosis Trial profile p = 0.0002 CAD: 30.8 ± 5.5 p = 0.001 CAD: 62.8 ± 5.4 Kaplan–Meier survival analysis of proportion of lapse and relapse Number at risk refers to proportion remaining free for lapse and relapse Pilot study at Loma Linda University Medical Center, US • Baclofen used for 5-8 months in 14 patients with severe alcoholic hepatitis • 13/14 patients completely stopped drinking/craving and one patient reported a significant reduction in alcohol consumption • There was a significant reduction in total bilirubin (p=.0057) and AST (p=.0438) and there was a trend for reduced ALT (p=.083). No side effects were reported Yamini & Runyon. Alcohol Alcohol 2014 Pilot study at Royal Alexandria Hospital Paisley, Glasgow, UK • Baclofen used ‘off label’ in > 50 patients • the dose required was lower in those patients with advanced alcoholic liver disease; patients reduce/stop drinking/craving. No side effects were reported Heydtmann. Alcohol Clin Exp Res 2011 Alcoholic liver disease • When abstinence fail to improve liver function or the patient develop a severe liver damage (e.g. acute alcoholic hepatitis), OLT is the most effective therapy Steatosis Steatohepatitis Cirrhosis Liver transplantation in alcohol‐related cirrhosis Management of alcoholic liver disease, Journal of Hepatology, 2012 Management strategies in alcoholic liver disease, Nature, 2007 Alcoholic liver disease, Hepatology 2010 Indicazioni al trapianto in Italia Pazienti adulti Mirante VG et Al. AISF 2000 Liver transplantation in alcohol‐related cirrhosis Primary indications of Liver Transplantation in 297 Cirrhosis in Liver Transplant Centre, Gemelli Hospital, Roma ‐ 1995‐2009 31 % Ethical problems AASLD Practice Guidelines, Hepatology 2010 The 6‐months rule Liver transplantation in alcoholic hepatitis Mathurin et al, NEJM 2011 Results Number of patients, divided by etiologies, who underwent liver transplantation between 1995 and 2009. Trend of transplantation for alcoholic cirrhosis. Results: recidivism and survival ∆ = 0.2 Kaplan‐Meier analysis. Estimated survival probability curves for patients followed and not followed at the AAU, together with p‐ values from log‐rank tests at different times of observation (p<0.0001 at 8yrs). Difference in the estimated survival probability for patients followed and not followed at the AAU, along with the related confidence bands. (95% CI: ‐0.09:‐0.47; p=0.005). Results: pre‐OLT alcohol abstinence time Advanced ALD is a widely accepted indication for OLT and the survival rate after OLT is not different (or better) than other indications Moralistic view (self‐inflicted disease, risk of recidivism, ecc) should not undetermine OLT procedure in these patients Alcoholic patients should be followed before and after liver transplantation by clinicians with expertise in alcohol use disorder management, within LT Unit Abstinence time before transplantation could be shortened in select patients when clinical condition do not allow 6‐ month waiting time A. Ferrulli, A. Mirijello, L. Leggio, G. Vassallo, M. Antonelli, C. D’Angelo, G. Gasbarrini, A. Gasbarini Grazie per l’attenzione
© Copyright 2026 Paperzz