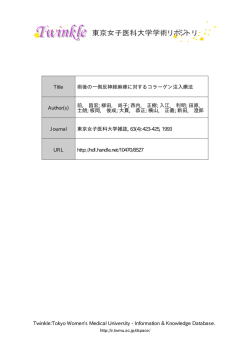
ISSN 1881-901X Highlights from the Official Journal of the Movement Disorder Society 日本語版 Vol.5 No.1 July 2011 INCLUDED IN THIS ISSUE Full Articles パーキンソン病患者の病的賭博には 前頭葉‐線条体間の連携離断が関連 している:パスモデリング解析 無 動‐筋 強 剛 型 お よ び 振 戦 優 位 型 パ ー キ ン ソ ン 病 患 者 で は FP-CIT SPECT 所見が異なる Abstracts 早期パーキンソン病における低用量 プラミペキソールの 1 日 2 回投与: 無作為化プラセボ対照試験 他 11 本収載 書き出し用.indd 3 11.7.14 2:27:09 PM J_ID: za2 Customer A_ID: MDS_25_13_EDBD Date: 16-SEPTEMBER-10 Stage: I Page: 1 J_ID: za2 Customer A_ID: MDS_25_13_EDBD Date: 16-SEPTEMBER-10 Stage: I Page: 1 J_ID: za2 Customer A_ID: MDS_25_13_EDBD Date: 16-SEPTEMBER-10 Jose A. Obeso, MD, PhD University of MD, Navarra Jose A. Obeso, Obeso, MD, PhD PhD Jose A. Pamplona, Spain University of Navarra University of Navarra Pamplona, Spain Jose Pamplona, A. Obeso, Spain MD, PhD University of Navarra Pamplona, Spain Erwan Bézard Erwan Bézard Erwan Bézard Bordeaux, France KarlUniversity Kieburtz of Bordeaux, France Rochester, New York, USA Karl Kieburtz Pamplona, Erwan Bézard Karl Kieburtz Rochester, New York, USA Jose A. Obeso, Bordeaux, France Bordeaux, Rochester, New France York, USA AKarl SSISTANT EDITOR Kieburtz Manuel Rochester, NewAlegre York, USA A SSISTANT E DITOR ASSISTANT EDITOR Pamplona, Spain Manuel Alegre Manuel Pamplona,Alegre Spain Pamplona, E Spain SSISTANT DITOR ErwanABézard Manuel Alegre Bordeaux, France Pamplona, Spain MD, PhD Navarra Spain Stage: I Page: 1 EDITORS-IN-CHIEF E DITORS-IN-CHIEF EDITORS -IN-CHIEFC. Warren Olanow, MD, FRCPC C.Mount Warren Olanow, MD, FRCPC Sinai School MD, of Medicine EDITORS-IN-CHIEFC. Warren Olanow, FRCPC New Sinai York,School New York, USA Mount of Medicine Mount Sinai School of Medicine C. Warren Olanow, MD, USA FRCPC New York, York, New York, York, USA New New Mount Sinai School of Medicine DITORS-EIN -CHIEF New York, New York, USA AE SSOCIATE DITORS Kailash P.EBhatia David J. Burn A SSOCIATE DITORS ASSOCIATE EDITORS Newcastle, Kingdom C. Warren Olanow, MD, FRCPC DavidUnited J. Burn DavidUnited J. Burn Newcastle, Kingdom Kapil Sethi Newcastle, United Kingdom Mount Sinai SchoolAugusta, of Medicine Georgia, USA Serge Przedborski Kapil Sethi Kailash P. Bhatia David J.Sethi Burn New York, New Augusta, York, USA Serge Przedborski Kapil New York, New York, USA Georgia, USA London, United Kingdom Kailash P. Bhatia Kailash P. Bhatia London, United Kingdom Przedborski ASerge SSOCIATE EKingdom DITORS London, United New York, New York, USA London, Kingdom New York,United New York, USA Newcastle, Kingdom Augusta, United Georgia, USA CME EDITOR Serge Przedborski Kelly Lyons New York, New York, USA CME E DITOR CME DITOR USA Kansas City, EKansas, Kelly Lyons ASSOCIATE EDITORS KansasKelly City, Lyons Kansas, USA ASSISTANT EDITOR Kapil Sethi Tagliati Augusta, Georgia, USA AMichelle SSISTANT EDITOR DITOR A SSISTANT New York, NewEYork, USA Michelle Tagliati Tagliati NewMichelle York, New York, USA NewAYork, New E York, USA SSISTANT DITOR Kansas City, E Kansas, CME DITOR USA Kailash P. Bhatia David J. Burn Kelly Lyons Michelle Tagliati Newcastle, United Kingdom London, United Kingdom INTERNATIONAL DITORIAL Kansas City, EKansas, USABOARD IINTERNATIONAL NTERNATIONAL E DITORIAL B OARD Alfonso Fasano Serge Przedborski EDITORIAL BHiroshi OARD Matsuda New York, New York, USA Klaus Seppi Aarsland KarlDag Kieburtz Kapil Sethi Innsbruck, Austria USA Saitama, Japan Rome, ItalyNew York, New York, USA Stavanger, Norway Rochester, New York, USA Augusta, Klaus Georgia, Seppi Hiroshi Matsuda Alfonso Fasano Dag Aarsland Klaus Seppi Hiroshi Matsuda Alfonso Dag Aarsland Innsbruck, Austria Saitama, Japan Rome,Fasano Italy Stavanger, Norway McDermott INTERNATIONAL EDITORIAL BMike OARD Fabrizio Stocchi Victor Angelo Antonini Innsbruck, Austria Saitama, Japan Rome, Fung Italy Stavanger, Norway Rochester, New York, USA Chieti, Italy Westmead, Australia Monza, Italy Mike McDermott Fabrizio Stocchi Victor Fasano Fung Angelo Antonini Klaus Seppi Hiroshi Matsuda Alfonso Dag Aarsland Mike McDermott Fabrizio Stocchi Victor Fung Angelo Antonini ASSISTANT ENorway DITOR A SSISTANT EDITOR Rochester, New Meco York, USA Giuseppe Chieti, Italy Westmead, Australia CME EDITOR Monza, Italy Innsbruck, Austria Saitama, Rome,Halliday Italy Stavanger, Louis Tan Glenda Erwan Bézard Rochester, NewJapan York, USA Chieti, ItalyTagliati Westmead, Australia Monza, Italy Rome, Italy Manuel Alegre Kelly Lyons Michelle Singapore, Singapore Giuseppe Meco Sydney, Australia Bordeaux, France Mike McDermott Louis Stocchi Tan Glenda ErwanAntonini Bézard VictorHalliday Fung Kansas City, Kansas, USA Angelo Giuseppe Meco Pamplona, Spain NewFabrizio York, Louis New Tan York, USA Rome, Italy Janis Miyasaki Glenda Halliday Erwan Bézard Rochester, New York, USA Singapore, Singapore Sydney, Australia Bordeaux, France Chieti,C. Italy Westmead, Australia Monza, Italy Rome, Italy Barbara Tilley Regina Katzenschlager Maren E. Bodden Singapore, Singapore Toronto, Ontario, Canada Sydney, Australia Bordeaux, France Janis Miyasaki Charleston, South Carolina, USA Vienna, Austria Marburg, Germany Giuseppe Meco Janis Miyasaki Barbara C. Tilley Regina Katzenschlager Maren Bodden Louis Tan Glenda Halliday ErwanE.Bézard Toronto, Ontario, Canada Tetsutaro Ozawa Barbara Tilley USA Regina Katzenschlager Maren E. Bodden Rome, Italy Toronto, Ontario, Canada Charleston, SouthC. Carolina, Vienna, Austria Marburg, Singapore, Singapore Sydney, Australia Bordeaux,Germany France Niigata, Japan Karl Kieburtz Mathias Toft Vincenzo Bonifati Charleston, South Carolina, USA Vienna, Austria Marburg, Germany Tetsutaro Ozawa Janis Miyasaki I NTERNATIONAL E DITORIAL B OARD Tetsutaro Ozawa Rochester, New York, USA Oslo, Norway Rotterdam, The Netherlands Niigata, Japan Walter Paulus Karl Kieburtz Barbara C.Toft Tilley Regina Katzenschlager Maren E. Bonifati Bodden Mathias Vincenzo Toronto, Ontario, Canada Niigata, Japan Karl Kieburtz Mathias Toft Vincenzo Bonifati Göttingen, Germany Rochester, New York, USA Charleston, South Carolina, Vienna, Austria Marburg, Germany Oslo, Norway Rotterdam, The Netherlands Christine Klein KlausUSA Seppi Hiroshi Matsuda Alfonso Fasano DagRotterdam, Aarsland Claudia PaoloThe Calabresi Walter Paulus Rochester, New York, USA Oslo,Trenkwalder Norway Netherlands Tetsutaro Ozawa Walter G. Paulus Luebeck, Germany Kassel, Germany Perugia, Italy Stephen Reich Göttingen, Germany Innsbruck, Austria Saitama, Japan Rome, Italy Stavanger,Vincenzo Norway Christine Klein Niigata, Japan Karl Kieburtz Claudia Trenkwalder Paolo Calabresi Mathias Toft Bonifati Göttingen, Germany Christine Klein Claudia Trenkwalder Paolo Calabresi Baltimore, Maryland, Luebeck, Germany Rochester, New York, USA Kassel, Germany Perugia, Italy Stephen G. ReichUSA Oslo,van Norway Rotterdam, The Netherlands Paul Krack Richard Camicioli Walter Paulus Bob Hilten Mike McDermott Luebeck, Germany Kassel, Germany Perugia, Italy Stephen G. Reich Fabrizio Stocchi Victor Fung Angelo Antonini Baltimore, Maryland, Webster Ross USA Grenoble, France Edmonton, Alberta, Canada Göttingen, Germany Leiden, The Netherlands Baltimore, Maryland, USA USA Rochester, New York, Christine Klein Paul Australia Krack Richard Camicioli Claudia Trenkwalder Paolo Chieti, Italy Westmead, Bob van Hilten Monza,Richard Italy Calabresi Honolulu, Hawaii, USA Paul Krack Camicioli Bob van Hilten Webster Ross Luebeck, Germany Grenoble, France Edmonton, Alberta, Canada Kassel, Germany Perugia, Italy Stephen G.Ross Reich Leiden, The Netherlands Webster Andres Lozano Mark R. Cookson JensThe Volkmann Grenoble, France Edmonton, Alberta, Canada Giuseppe Meco Leiden, Netherlands Honolulu, Hawaii, USA Terrance Sanger Baltimore, Maryland, USA Louis Tan Glenda Ontario, Halliday Erwan Bézard Honolulu, Rome, Hawaii, Italy USA Toronto, Canada Bethesda, Maryland, USA Kiel,van Germany Paul Krack Richard Palo Alto, California, USA Andres Lozano Mark R.Camicioli Cookson Bob Hilten Jens Volkmann Terrance Sanger Singapore, Singapore Sydney, Australia Bordeaux, France Andres Lozano Mark R. Cookson Jens Volkmann WebsterSanger Ross Grenoble, France Edmonton, Alberta, Canada Terrance Toronto, Ontario, Canada Bethesda, Maryland, USA Leiden, The Netherlands Kiel, Germany Palo Alto, California, USA Daniel Weintraub W.M. Michael Schüpbach Pablo Martinez-Martin TedMaryland, Dawson USA Toronto, Ontario, Canada Bethesda, Kiel, Germany Miyasaki Honolulu, Hawaii, USA Palo Alto,Janis California, USA Philadelphia, Pennsylvania, USA Madrid, Spain Paris, France Baltimore, Maryland, USA Barbara C. Tilley Regina Katzenschlager Maren E.Mark Bodden Andres Lozano Cookson Toronto, Canada Daniel Weintraub W.M. MichaelOntario, Schüpbach Pablo Martinez-Martin TedR. Dawson Jens Volkmann Daniel Weintraub W.M.Terrance Michael Sanger Schüpbach Pablo Martinez-Martin TedMaryland, Dawson USA Charleston, Carolina, USA Vienna, Austria Marburg, Germany Toronto, Ontario, Canada Bethesda, Philadelphia, Pennsylvania, USA Madrid, Spain Paris, France USA Baltimore, Maryland, USA Kiel, Germany South Palo Alto, California, Philadelphia, Pennsylvania, USA Madrid, Spain Paris, France Ozawa Baltimore, Maryland, USA Tetsutaro Daniel Weintraub W.M. Michael Schüpbach Pablo Martinez-Martin Ted Dawson Niigata, Japan Karl Kieburtz EDITORIAL OFFICE PAST EDITORS-IN-CHIEF Mathias Toft Vincenzo BonifatiFOUNDING EDITORS Philadelphia, Pennsylvania, Madrid, Spain Paris, France Maryland, USA 1986–1995 2004–2009 Oslo, USA Norway Rotterdam,Baltimore, The Netherlands FOUNDING EDITORS Rochester, New York, USA EDITORIAL OFFICE PAST E DITORS-IN-CHIEF Julie Nash Walter Paulus FOUNDING EDITORS EDITORIAL OFFICE PAST EDITORS-IN-CHIEF 1986–1995 2004–2009 Disorders Stanley Fahn Günther Deuschl Göttingen, Germany JulieMovement Nash ChristineManaging Klein Editor, 1986–1995 2004–2009 Claudia Trenkwalder Paolo Calabresi Julie Nash 320 North SalemMovement Street, Suite 205 David Marsden G. Goetz Managing Editor, Disorders Stanley Fahn Günther Deuschl DITORS DITORIAL OFFICE PChristopher AST EDITORS -IN-C HIEF Luebeck, Germany Kassel, Germany Perugia, Italy FC.OUNDING Stephen G. Reich Managing E Editor, Movement Disorders Stanley E Fahn Günther Deuschl Apex, NC 27502 320 North Salem Street, Suite 205 C. David Marsden Christopher G. Goetz 1986–1995 2004–2009 Baltimore, Maryland, USA Julie Street, Nash Suite 320 North Salem 205 C. David Marsden Christopher G. Goetz Phone: 1-919-423-7009; [email protected] Richard Camicioli Wiley Bob van Hilten Apex, E-mail: NC 27502 Publishing Japan Paul K.K.Krack Managing Editor, Movement Stanley Fahn Apex, NC 27502 Disorders Webster Ross Günther Deuschl Grenoble, France Edmonton, Alberta, Canada Leiden, The Netherlands Phone: 1-919-423-7009; E-mail: [email protected] 320 North Salem Street,[email protected] SuiteHonolulu, 205 C. David Marsden Christopher G. Goetz Phone: 1-919-423-7009; E-mail: Hawaii, USA Apex, NC 27502 For R. submission and all Lozano other information, please visit http://www.movementdisorders.org/publications/journal.php. Mark Cooksoninstructions, subscriptions,Andres Jens2010 Volkmann Terrance Sanger Phone: 1-919-423-7009; E-mail: [email protected] For Maryland, submission USA instructions, subscriptions, and all other information, please visit http://www.movementdisorders.org/publications/journal.php. Toronto, Bethesda, Kiel, Germany Wiley Japan K.K. Palo Alto, California, USA For submission instructions, subscriptions, and Ontario, all otherCanada information, please visitPublishing http://www.movementdisorders.org/publications/journal.php. � 2010 Movement Disorder Society. All rights reserved. No part of this publication may be reproduced in any form or by any means, except as permitted under section 107 or 108 of the 1976 United States Copyright Daniel Weintraub W.M. Michael Schüpbach Pablo Martinez-Martin Tedwithout Dawson Act, either the prior written permission of the publisher, or and authorization throughinformation, the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400, fax (978) 750-4470. Such requests For submission instructions, subscriptions, all other please 2010 Movement Disorder Society. All rights reserved. No part of this publication may be reproduced in any form orvisit byStreet, anyhttp://www.movementdisorders.org/publications/journal.php. means, except as permitted under section 107 or 108 of the 1976 United States Copyright � and other permission inquiries shouldAll be addressed to the Permissions Department, c/o John & Sons, 111 River Hoboken, NJas 07030; (201)under 748-6011, fax107 (201) 748-6008, e-mail: [email protected]. Philadelphia, Pennsylvania, USA Madrid, Spain Baltimore, Maryland, USA Paris, France 2010 Movement Disorder Society. rights of reserved. No partorofauthorization this publication may beWiley reproduced in Inc., any form or by222 anyRosewood means, except permitted section or 108 offax the(978) 1976 United States Copyright � Act, without either the prior written permission the publisher, through the Copyright Clearance Center, Drive, Danvers, MA 01923, (978) 750-8400, 750-4470. Such requests Printed in theeither United America by The Sheridan Press. or authorization through the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400, fax (978) 750-4470. Such requests Act, without theStates priorof written permission of the and other permission inquiries should be addressed to publisher, the Permissions Department, c/o John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030; (201) 748-6011, fax (201) 748-6008, e-mail: [email protected]. and other permission inquiries should beby addressed to thePress. Permissions Department, c/o John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030; (201) 748-6011, fax (201) 748-6008, e-mail: [email protected]. Printed in the United States ofSociety. America The Sheridan 2010 Movement Disorder All rights reserved. No part of this publication may be reproduced in any form or by any means, except as permitted under section 107 or 108 of the 1976 United States Copyright � Printed in the United States of America by The Sheridan Press. Act, without either the prior written permission of the publisher, or authorization through the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400, fax (978) 750-4470. Such requests OUNDING DITORS FFICE DITORS IN [email protected]. HIEF and other permission inquiries should be addressed to the Permissions Department, c/o John WileyDITORIAL & Sons, Inc., 111 River Street, Hoboken, NJ 07030; (201) 748-6011,AST fax (201) 748-6008, e-mail: Printed in the United States of America by The Sheridan Press. F E 1986–1995 Stanley Fahn C. David Marsden 2011 E O Julie Nash Managing Editor, Movement Disorders 320 North Salem Street, Suite 205 Apex, NC 27502 Phone: 1-919-423-7009; E-mail: [email protected] P E - -C 2004–2009 Günther Deuschl Christopher G. Goetz 2011 Wiley Publishing Japan K.K. For submission instructions, subscriptions, and all other information, please visit http://www.movementdisorders.org/publications/journal.php. � 2010 Movement Disorder Society. All rights reserved. No part of this publication may be reproduced in any form or by any means, except as permitted under section 107 or 108 of the 1976 United States Copyright Act, without either the prior written permission of the publisher, or authorization through the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400, fax (978) 750-4470. Such requests e-mail: [email protected] and other permission inquiries should be addressed to the Permissions Department, c/o John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030; (201) 748-6011, fax (201) 748-6008, e-mail: [email protected]. Printed in the United States of America by The Sheridan Press. Corporate Sales Associate Director:Kimiyoshi Ishibashi 書き出し用.indd 4 11.7.14 2:27:11 PM 日本語版 Vol.5 No.1 July 2011 監修: 水野 美邦 北里大学東病院 神経再生医療学講座客員教授 編集委員: 宇川 義一 (五十音順) 福島県立医科大学医学部 髙橋 良輔 京都大学医学研究科臨床神経学教授 神経内科学講座教授 野元 正弘 愛媛大学医学部附属病院 薬物療法・神経内科教授 梶 龍兒 徳島大学医学部神経内科教授 近藤 智善 公立大学法人和歌山県立医科大学 服部 信孝 順天堂大学医学部脳神経内科教授 神経内科教授 山本 光利 香川県立中央病院神経内科主任部長 Full Articles パーキンソン病患者の病的賭博には前頭葉‐線条体間の連携離断が関連している:パスモデリング解析 無動‐筋強剛型および振戦優位型パーキンソン病患者ではFP-CIT SPECT所見が異なる 2 11 Abstracts 早期パーキンソン病における低用量プラミペキソールの 1日2回投与:無作為化プラセボ対照試験 20 パーキンソン病患者のニューロン新生に対する 薬物療法の効果 21 AAV2-neurturin遺伝子治療(CERE-120)の生物活性: パーキンソン病患者と非ヒト霊長類の脳における相違点 22 パーキンソン病の臨床サブタイプ 24 パーキンソン病におけるDiphasicおよび Peak-Doseジスキネジアの遺伝的感受性の違い 30 本態性振戦とパーキンソン病との関連についての再考 32 パーキンソン病患者の健康関連の生活の質に対する 非運動症状の影響 34 パーキンソン病の運動症状と発症時年齢との関連 36 薬物未投与のパーキンソン病患者における 衝動性と強迫性 38 認知機能状態別にみるパーキンソン病患者の 皮質萎縮パターン 40 26 リチャードソン症候群(PSP-RS),進行性核上性麻痺-パーキ ンソニズム(PSP-P)およびパーキンソン病(PD)患者の 28 脳幹構造のMRI測定 表紙:ボクセル・ベース・モルフォメトリー解析で前頭葉性行動質問紙(Frontal Behavioral Inventory)スコアとの相関が認められた領域。 (Josephs et al, Movement Disorders, 2011, Vol. 26 No. 3, page 493) 書き出し用.indd 1 振戦に対する視床刺激: 刺激標的部位の同定は改善可能か Selected from Movement Disorders Vol. 26 No. 1-3, 2011 11.7.14 3:06:08 PM パーキンソン病患者の病的賭博には前頭葉‐線条体 間の連携離断が関連している:パスモデリング解析 Pathological Gambling in Patients with Parkinson’s Disease is Associated with FrontoStriatal Disconnection: A Path Modeling Analysis *, **, *** Roberto Cilia, MD, Sang Soo Cho, PhD, Thilo van Eimeren, MD, PhD, Giorgio Marotta, MD, Chiara Siri, PsyD, Ji Hyun Ko, PhD, Giovanna Pellecchia, PhD, Gianni Pezzoli, MD, Angelo Antonini, MD, and and Antonio P. Strafella, MD, PhD, FRCPC * Division of Brain, Imaging and Behaviorur-Systems Neuroscience, Toronto Western Research Institute and Hospital, UHN, University of Toronto, Toronto, Ontario, Canada * * PET Imaging Centre, Centre for Addiction and Mental Health, University of Toronto, Toronto, Ontario, Canada * * * Parkinson Institute, Department of Neurology, Istituti Clinici di Perfezionamento, Milan, Italy 背景 : パーキンソン病 (Parkinson’ s disease; PD) では, effective connectivity 解析を行い,パスモデルを明ら ドパミン補充療法の合併症の 1 つとして病的賭博が生 かにした。 じる場合がある。神経画像研究では報酬系内のドパミン 結果:PD における賭博の重症度は,腹外側前頭前皮質, 伝達異常が示唆されているが,病的賭博のある PD 患者 前帯状皮質,後帯状皮質,内側前頭前皮質,島,線条体 に特徴的な神経回路の変化については,これまで検討さ など,意思決定,リスク処理(プロセシング)および反 れていない。 応抑制に関与する脳内ネットワークの障害と関連してい 方法:PD 患者 30 例(活発な賭博行為がみられる PD た。賭博行為のみられる PD 患者では前帯状皮質‐線 患者 15 例および対応する対照 PD 患者 15 例,いずれ 条体間の連携離断が認められたのに対し,両対照群で も薬物療法中)と健常被験者 15 例を対象に,安静時脳 はこれら 2 領域間の連携はきわめて強固に保たれてい 血流 SPECT を実施した。賭博の重症度は South Oaks た。 Gambling Scale(SOGS)を用いて評価した。共分散 考察:ネガティブな結果を受けた行動転換(shifting 分析を用い,その活動性が賭博の重症度と関連する脳 behavior)の特異的な障害の基礎には,前帯状皮質‐ 領域を同定した。これらの領域を関心体積(VOI)とし 線条体間の連携離断があると考えられる。賭博行為の たボクセル単位の共分散分析により,機能的に相互結 みられる PD 患者が,自滅的な結果を招くにもかかわら 合する脳の部位を同定した。構造方程式モデリング ずリスクテイキング行動を執拗に繰り返す理由は,これ (Structural Equation Modeling)の枠組み内において により説明できる可能性がある。 Movement Disorders, Vol. 26, No. 2, 2011, pp. 225–233 Key Word パーキンソン病,病的賭博,SPECT,effective connectivity,SPM ド パ ミン 補 充 療 法 を 受 け て い る パ ー キ ン ソ ン 病 患者の病的賭博の重症度にみられる個体差の背景にある (Parkinson’ s disease; PD)患者では,病的賭博など,様々 神経相互作用については,現在のところ検討されていな な衝動制御障害が報告されている 。PD 患者に対する い。今回の研究では,脳領域間結合解析(connectivity 慢性的なドパミン刺激は,ネガティブフィードバックか analysis)を用い,病的賭博のある PD 患者と対応する対 らの学習を選択的に障害し,また衝動性と新奇探索傾向 照群とを区別する重要な神経相互作用を同定した。本研 を亢進することが示されている 。最近の知見では,PD 究は,ボクセル単位の共分散分析 8 および構造方程式モ 患者の薬剤誘発性病的賭博が報酬系の明らかな異常に関 デリング(Structural Equation Modeling)9 を適用して様々 連することが示唆されているものの 6,7,薬剤投与中 PD な被験者群の重要な神経相互作用を検討し,さらにこの 1,2 3-5 2 #MD5-1.indb 2 11.7.14 2:24:37 PM R. Cilia et al. C I L I A 手法を SPECT データに用いた初めての画像研究である。 E T A L . Table 1 賭博行為のみられる PD 患者,対照 PD 患者 TABLE 1. Clinical features of PD gamblers, PD controls, および健常被験者の臨床的特徴 and healthy subjects 患者および方法 適格 / 除外基準(詳細は別途記載 6)に基づき,活発な 病的賭博を伴う PD 患者 15 例を本試験に登録した。試験 参加者の背景因子と臨床的特徴の詳細を Table 1 に示す。 病的賭博の診断は,精神疾患の診断・統計マニュアル第 4 版(fourth edition of the Diagnostic and Statistical Manual of Mental Disorders Text Revision; DSM IV TR)の基準 10 に従って確定した。すべての PD 被験者について,経験 のある神経心理学者が Mini Mental State Examination (MMSE) ,Frontal Assessment Battery(FAB) ,Geriatric Depression Scale(GDS)および South Oaks Gambling Screen(SOGS)によるスクリーニングを行った。病的賭 博の重症度評価に用いた SOGS は,DSM-IV 基準(様々 な臨床状況で賭博の有無とその重症度の評価に広く用い られている)との高い相関を示す信頼性の高いツールで ある 。SOGS スコア 3 ~ 5 は問題のある賭博,スコア 11-13 > 5 は病的賭博の存在を示す 11。本試験では,認知障害 のある患者(MMSE < 24) ,過去に神経外科的処置を受 けた患者,PD 発症前に病的賭博の既往がある患者,ド パミン補充療法開始後に病的賭博が発現したものの検査 時に病的賭博症状を認めなかった患者は除外した。また, ドパミン作動性薬剤以外の向精神薬を投与されている患 者も除外した。臨床評価では,薬剤「on」時の Unified Parkinson’ s Disease Rating Scale(UPDRS)Part Ⅲ(運動 機能)スコアと Hoehn and Yahr(HY)分類を検討した。 これらの患者において,レボドパ(L—ドパ)とドパミン アゴニストの総 1 日用量として,L—ドパ換算 1 日用量を 計算した 。対照群として,年齢をマッチさせた健常被 14 験者 15 例と,背景因子(年齢,男女比) ,臨床的特徴(罹 病期間,重症度) ,平均 1 日ドパミン作動性薬剤摂取量を マッチさせた,病的賭博のない非認知症 PD 患者 15 例を 対象とした(Table 1) 。ヘルシンキ宣言に基づき,全被験 者からインフォームド・コンセントを取得した。本試験 は施設内倫理委員会の承認を受けた。 SPECT 画像およびデータ前処理 脳 SPECT 検査には,超高解像度ファンビームコリメー タを装備した専用 3 検出器ガンマカメラ(Prism 3000, Philips, The Netherlands)を使用した。患者には朝の薬剤 「on」時に安静・閉眼状態で SPECT 検査を実施した。照 Age (yr) Male/female Disease duration (yr) UPDRS III Hoehn and Yahr stage Total LEDD (mg/day) DA daily dose (mg/day) SOGS MMSE FAB GDS PD gamblers (n ¼ 15) PD controls (n ¼ 15) Healthy subjects (n ¼ 15) 59.2 (7.6) 14/1 8.7 (3.3) 16.9 (8.8) 2.0 (0.6) 848.1 (253) 296.1 (147.5) 7.5 (2.7) 28.6 (0.9) 15.4 (1.4) 9.7 (5.2) 58.6 (6.9) 14/1 9.1 (2.1) 18.3 (7.9) 2.3 (0.7) 880 (245) 316.7 (115.6) 0.9 (0.5) 28.4 (1.3) 16.2 (1.7) 10.1 (6.3) 57.7 (7.1) 14/1 – – – – – 1.6 (0.4) 29.1 (0.6) – – SPECT Ima Brain SPECT dedicated triple Philips, The Net solution fan bea the morning onclosed. Six SPEC trix size 128 � 1 rotation 12.9 to between 30 and 740 MBq of 9 (ECD) (Neurolit ica, MA) with p and dimly lit ro lipophilic agent t a rapid first-pass uptake is propo (rCBF) at the tim a polar complex (high initial cere from the brain) images were r (OSEM, 20 iter 3D-Butterworth attenuation corr coefficient 0.1 cm performed in Natick, MA) u (SPM5, Wellcom London, UK).16 standard SPECT smoothed using isotropic Gaussi ratio and to acc structures. Varia scans were remo have an arbitrar threshold maskin All 値はすべて平均値(SD) values are given as mean 。SOGS (SD). SOGS scores are significantly higher in スコアは,両対照群に比べ,賭 PD gamblers compared to both control groups (P < 0.05). 博行為のみられる PD 患者群で有意に高い(p < 0.05) UPDRS III, Unified Parkinson’s Disease Rating Scale motor。 score; LEDD, levodopa equivalent daily dose; DA, dopamine agonist; SOGS, South Oaks UPDRS Ⅲ= Unified Parkinson’ s Disease Rating Scale Part Ⅲ(運 Gambling Scale; MMSE, mini mental state examination; FAB, frontal assessment battery; GDS, geriatric depression 1scale. 動機能)スコア,LEDD =レボドパ換算 日用量,DA =ドパミン アゴニスト,SOGS = South Oaks Gambling Scale,MMSE = Mini Mental State Examination,FAB = Frontal Assessment Battery,GDS 6 = Depression Scale in Geriatric detail elsewhere. Demographic and clinical charac- teristics of the study participants are detailed in Table 1. Diagnosis of PG was established according to the 明を落とした静かな部屋で患者を座位・閉眼の状態にし fourth edition of the99mDiagnostic and Statistical Manual of ® Tc-ECD(Neurolite Bristol-Myersて,約 MBq のText Mental740 Disorders Revision (DSM IV, TR) criteria.10 Squibb, North Billerica, MA)の静注後 ~ 60 分時点で, All PD subjects were screened using the30 Mini Mental State Examination (MMSE), Frontal Assessment Battery (FAB), マトリクスサイズ 128 × 128,ピクセルサイズ 2.0 ~ 2.4 the Geriatric Depression Scale (GDS), and the South Oaks mm,回転半径 12.9 ~ 13.9 administered cm,収集時間 分にて 6neuつ Gambling Screen (SOGS), by20 a trained ropsychologist. The severity of PG was assessed using the の SPECT 画像の収集を開始した。ECD は脳血流シンチ SOGS, a reliable tool with a high degree of association グラフィ―用の脂溶性化合物で,血液脳関門を通過し, with the DSM-IV criteria that is commonly used to iden初回通過時に迅速に取り込まれる(受動拡散) 。ECD の tify and measure gambling severity in different clinical 11–13 contexts. from 3 to 5 identify problem 脳 内 取り 込 みSOGS は, 投scores 与時の 局所 脳血 流 量(regional gambling and scores >5 are considered pathological.11 cerebral blood patients flow; rCBF)に比例する。ECD は選択的脳 We excluded with cognitive impairment (MMSE 内滞留(脳への初期取り込みが高く,脳からのクリアラ <24), previous neurosurgical procedures, history of PG prior to PD onset, and those who developed PG after the ンスが非常に遅い)を示す極性複合体へと代謝され,速 initiation of dopaminergic therapy but no longer sympto15 画像はサブセット やかに腎臓から排泄される matic when examined. We。SPECT also excluded all subjects treated with psychoactive drugs 法, other than20, dopaminer化による期待値最大化法(OSEM 反復数 サブセッ gic medication. Clinical assessment included the Unified ト数 15)で再構成し, 3D-Butterworth フィルター(オーダー Parkinson’s Disease Rating Scale (UPDRS) motor score 0.31/ ピクセル)でフィルタリングし, 5, カットオフ周波数 and Hoehn and Yahr stage while on-medication. In these patients, levodopa equivalent daily dose was Chang 法で減弱補正を行った(減弱係数 0.1/cm) 。画像解 calculated as the sum of daily L-dopa and dopamine 析と統計解析は,Statistical Parametric Mapping(SPM5, agonists.14 As control groups, we identified 15 ageWellcome Department of Imaging Neuroscience, London, matched healthy subjects (HC) and 15 non-demented PD patients without PG matched for demographic (age, UK)を用い,MATLAB version 7.1(Mathworks, Natick, male-to-female 16 ratio), clinical features (disease duration に組み込まれた標準 MA)で行った and severity) and。画像は,SPM5 mean daily dopaminergic medication intake (Table 1). Informed consent was obtained from SPECT テンプレートに対して空間補正し,また,信号対 all subjects according to the declaration of Helsinki. 雑音比を大きくして解剖学的構造上のわずかな差異を明 The study was approved by the Ethics Committee of らかにするために,半値全幅 16 mm の等方性ガウシアン local institution. カーネルを用いて平滑化した。デフォルト値 0.8 に対す 226 The level of si changes was as (Ke) and the p using estimation sian fields. A g perform the app SPM5 in whole our analyses in (Fig. 1): we iden gambling severit didate connectio subsequent effec Correlation An and Regional B To identify br SOGS scores, a Movement Disorders, Vol. 26, No. 2, 2011 3 #MD5-1.indb 3 11.7.14 2:24:38 PM パーキンソン病患者の病的賭博には前頭葉‐線条体間の連携離断が関連している:パスモデリング解析 るマスキング閾値を用い,任意レベル 50 mL/100 mL/ 分 想定において,当該領域に影響を与える領域が 1 単位変 となるように各画像をスケーリングする共分散分析によ 化した場合に,当該領域の活動度がどの程度変化すると り,各被験者間および各スキャン間の全体血流量の変動 予測されるかを示す 9,16。Effective connectivity 解析は次の を取り除いた。 2 つの主要段階から成った。まず,構築されたモデルの安 定性を評価するため,適合度を検定した。適合度,ノル データ解析 ム適合度指標,Akaike 情報基準に基づき,モデル候補の rCBF の変化がみられた脳領域の有意レベルは,ラン 中からデータと最も良好に適合するものを決定した 19。次 ダムガウス場理論に基づく推定値を用い,各領域クラス に,比較適合度指標と Tucker-Lewis 指標(相対適合度指 ターのボクセル(Ke)およびピークの高さ(Z スコア) 標)を計算し,値が 0.95 以上であればモデル適合が良好 による空間的拡がりで評価した。一般線形モデルを用い, であるものとみなした 20-23。このモデ ル の構 造には, 全被験者の全脳について,SPM5 で適切なボクセル単位 SOGS スコアとの相関が認められた複数の領域と,シー の統計解析を行った。次の 3 つの連続的手順により解析 ド VOI による相関解析および神経解剖学関連文献 24,25 で を実施した(Figure 1) 。すなわち,まず賭博の重症度と 明らかにされた,これらの領域間の結合を取り入れた。 関連する脳領域を同定後(段階 1) ,これらの領域間の候 ここでは,分散の外的原因を説明しうる誤差項も組み入 補となる結合を同定し(段階 2) ,effective connectivity 解 れた 22。残存影響(residual influence)はすべての脳領域 析を行った(段階 3) 。 について 0.50 に設定し,これにより分散の原因をモデル 内で説明可能とした 9。各パスは,各領域の総代謝活性 賭博の重症度および局所脳活性間の相関解析 の測定値に基づいて別の領域に対するある領域の直接的 rCBF が SOGS スコアと相関する脳領域を同定するた 影響を反映することから,パス係数が負であれば集団的 め,個々の SOGS スコアを関心共変量として SPM5 に組 な阻害(ensemble inhibition) ,正のパスは正味の興奮を示 み入れ,各群の相関解析を実施した。PD 患者を含む解 すものと解釈される 26。次に,このモデルを用い,3 群間 析では,罹病期間(発症後の年数) ,疾患重症度(HY 分 でパスモデルの違いを評価した。群間比較には「stacked- 類) ,総薬剤投与量(L—ドパ換算 1 日用量)を局外変数 model 法」を使用した 9。帰無仮説モデルでは,パス係数 (nuisance variable)として組み入れた。 の推定値は群を通じて同一でなければならず,一方,代 替モデルでは,パス係数の推定値は群間で異なる。オム 共変量解析(functional connectivity) 病的賭博のある PD 患者で SOGS スコアとの相関が認 ニバス検定(帰無仮説モデル 対 代替モデル)を行い, 所定の自由度における適合度のΧ 2(Χ )を比較して 2 diff められた脳領域を関心体積(VOI)とし,ボクセル単位 統計学的有意性を判定した。2 つのモデル間でΧ 2 適合 の共変量解析により相互作用する領域を同定した 8。脳血 度指標に有意差があれば,これらの群は所定モデルに照 流 SPECT データを用いたシード VOI による共分散分析 らして有意に異なると結論できる。モデルの構築とパス は,他の研究でも広く使用されている 。本試験では, 17,18 まず各領域について VOI を設定し,次に全脳ボクセル単 位相関解析を行った。 解析処理には AMOS 7.0(Small-Waters Co.)を用いた。 すべてのボクセル単位の統計解析において,extent threshold を少なくとも 50 の隣接ボクセルに設定してクラ スターレベルで補正し,閾値 p < 0.05 を適用した。ある パス解析(effective connectivity) 構造方程式モデリングの理論的枠組み内においてパス 解析を実施した。構造方程式モデリングは多変量回帰法 の 1 つで,各変数を結合する可能性のあるパスのサブセッ クラスター内の最も有意性の高いボクセルの座標につい て,SPM ソフトウエアを用い,MNI 標準座標に非線形変 換した。 賭博のみられる PD 患者,対照 PD 患者,健常被験者 トに基づき,ある変数集合の共分散構造をモデル化する。 における背景因子と臨床的特徴の比較には,連続変数の 単 純 な シ ー ド VOI に よ る 共 分 散 分 析(functional 場合は対応のない Student t 検定(p < 0.05) ,カテゴリー connectivity)とは異なり,構造方程式モデリングには指向 変数の場合はΧ 2 検定(p < 0.05)を用いた。統計解析 性情報が含まれる。パス係数〔すなわちパスの重み(path は SPSS for Windows Release 10.0(SPSS, Chicago, IL)で weight) ,範囲 0 ~ 1〕は,他の影響領域が変化しないとの 実施した。 4 #MD5-1.indb 4 11.7.14 2:24:40 PM R. Cilia et al. Region selection - Correlation analysis between rCBF and gambling severity Pathway selection - Seed-VOIs covariance analysis (Functional Connectivity) - Neuroanatomical data from primate literature Model construction Network analysis - Effective Connectivity analysis - Model construction - Network analysis 1. Compute path coefficients in each group 2. Assessment of group differences Figure 1 本試験で実施した解析のフローチャート 結 果 でシード部位として使用した。3 つの被験者群で認めら れた脳領域間の有意な相互作用を,Figure 3A に示す。病 試験参加者の背景因子と臨床的特徴の詳細を Table 1 的賭博を伴わない PD 患者とは対照的に,賭博行為のみ に示す。2 つの PD 患者群の年齢,性別,ドパミン作動 られる PD 患者では, 衝動制御, 報酬およびリスク処理(プ 性薬剤の 1 日用量,罹病期間 / 重症度,認知機能はマッ ロセシング)に重要な役割を果たす皮質および皮質下領 チしていた。賭博行為のみられる PD 患者において,全 域において,異なる相関パターンが認められた。最も顕 般的および前頭葉関連の認知障害は認められず,抑うつ 著な所見として,腹外側前頭前皮質および前帯状皮質, もなかった。病的賭博を伴う PD 患者 15 例中 11 例の詳 後帯状皮質間,ならびに前帯状皮質および線条体間には 細は既報の通りである 。 相関が認められなかった。また,賭博行為のみられる PD 6 患者では,病的賭博のない対照 PD 患者では機能的に結 rCBF と賭博重症度の相関解析 Figure 2 に,賭博行為のみられる PD 患者の全脳 rCBF 合していなかった領域間の血流量に,有意な相関が認め られた。こうした機能的結合は,前帯状皮質と島,補足 および SOGS スコア間の相関解析結果,Table 2 にその詳 運動野および小脳間,腹外側前頭前皮質と腹側淡蒼球間, 細を示す(p < 0.05,クラスターレベルで補正) 。SOGS 内側前頭極皮質と後帯状皮質間,海馬傍回と島間で認め スコアと各クラスター内の補正血流量間の相関について, られた。 散布図を Figure 2B に示す。賭博行為のみられる PD 患者 上述の脳領域およびその機能的結合に基づく構築モデ では,右腹外側前頭前皮質,右前帯状皮質,右後帯状皮質, ルの機能的ネットワークは,良好なモデル適合度指標を 右内側前頭極皮質,右吻側補足運動野,両側前島,右海 示し,デ ータを十 分 説明 可 能 であった〔Χ 2(10)= 馬傍回,右前上側頭回,左線条体の rCBF と SOGS スコ 12.175,p = 0.273〕 。すなわち,適合度指標= 0.93,ノル アとの間に,有意な負の相関が認められた。また,左紡 ム適合度指標= 0.96,Akaike 情報基準= 48.175,比較適 錘状回と小脳では正の相関が認められた。 合度指標= 0.992,Tucker-Lewis 指標= 0.983 であった。 群間解析(Figure 3B)では,このモデルにより,賭博行 結合解析 相関解析で同定された皮質および皮質下領域のうち, 為のみられる PD 患者および対照 PD 患者間〔Χ (11) 2 diff = 27.9,p < 0.005〕 ,賭博行為のみられる PD 患者および モデルの安定性と信頼性が最も高い領域をパス解析の対 健常被験者間〔Χ 象とした。これらの領域は,右腹外側前頭前皮質,左線 験者および対照 PD 患者間〔Χ 条体,右島,右海馬傍回,右内側前頭極皮質,右前帯状 で有意差が明らかになった。賭博行為のみられる PD 患 皮質,右後帯状皮質であり,ボクセル単位の共分散分析 者は, 対照 PD 群および健常被験者群のいずれとも異なる, (11)= 28.0,p < 0.001〕 ,健常被 2 diff p < 0.05〕 (11)= 20.5, 2 diff 5 #MD5-1.indb 5 11.7.14 2:24:41 PM パーキンソン病患者の病的賭博には前頭葉‐線条体間の連携離断が関連している:パスモデリング解析 Z= -15 Z= -7 X= 49 Z= 36 Z= 9 X= -35 X= 5 8 Y= 10 4 A 100 VentroLateral PFC p<0.001 95 Normalized rCBF Normalized rCBF 100 90 85 80 4 6 8 10 12 14 16 Anterior Cingulate Cortex p=0.002 95 90 85 80 4 6 8 10 Striatum p=0.025 90 85 80 75 6 8 10 12 14 95 90 85 80 4 16 6 8 Normalized rCBF medial PFC p=0.008 90 Normalized rCBF 10 12 14 16 SOGS score SOGS score 85 80 75 85 Posterior Cingulate Cortex p<0.001 80 75 70 65 70 4 B 16 14 Insula p=0.012 100 Normalized rCBF Normalized rCBF 95 4 12 SOGS score SOGS score 6 8 10 12 14 16 SOGS score 4 6 8 10 12 14 16 SOGS score Figure 2 賭博行為のみられる PD 患者における賭博重症度(SOGS スコアで評価)と相関した脳領域。正の相関は黄色,負の相関は青色で 示す(A) 。個々の SOGS スコアと rCBF との関連を示す線形トレンドライン付き散布図(B) 。各値は,各クラスターのピーク座標の中央に設 定した半径 5 mm の関心体積(VOI)から抽出した。各プロットについて有意性を示す p 値を示す。PFC =前頭前皮質,rCBF =局所脳血流量, SOGS = South Oaks Gambling Scale 独特の effective connectivity パターンを示した。主な所見 として,賭博のある PD 患者では前帯状皮質(BA 32)か 考 察 らの入力が線条体で離断されており,両対照群(病的賭 今回の解析の第 1 段階では,報酬・リスク処理(プロ 博を伴わない PD 患者および健常被験者)では,このパ セシング) ,意思決定,エラー検出・条件学習,欲求抑制, スの相対加重は 0.75 を上回っていた(Figure 3B) 。特に, 衝動制御に関与する複数の脳領域 27-31 の安静時活動度と, 健常被験者および病的賭博を伴わない PD 患者では,こ SOGS スコアとの間に,負の相関が認められた。特に, れらの 2 領域間に血流量の正相関が認められたのに対し, 右腹外側前頭前皮質で最高レベルの有意性を示すクラス 賭博のある PD 患者群ではこの相関が完全に失われてい ターが観察された。右腹外側前頭前皮質は,行動反応抑 た(Figure 4) 。 制に特異的に関与する領域であり 31-38,その活動度は, 6 #MD5-1.indb 6 11.7.14 2:24:42 PM R. Cilia et al. N E U R A L C O R R E L A T E S O F P A T H O L O G I C A L G A M B L I N G I N P D Table 2 SOGSlocations, スコアと相関した脳領域の解剖学的位置,Brodmann 領域(BA) y, z) ,ボクセル数 TABLE 2. 個別 Anatomic Brodmann areas (BA), MNI coordinates (x,y,z), spatial,MNI extent座標(x, of clusters in voxels (Ke), and T score of brain によるクラスターの空間的拡がり(Ke) regions correlating with individual South Gambling Scale scores ,TOaks スコア Correlations between brain perfusion and gambling severity Brain areas Side Negative correlations Ventrolateral prefrontal cortex Parahippocampal gyrus Posterior cingulate cortex Superior temporal gyrus medial superior frontal gyrus Striatum Anterior cingulate cortex Insular cortex Insular cortex Supplementary motor area Positive correlations Fusiform gyrus Cerebellum BA R R R R M L R R L R 47 30 23 21 9/10 L M 37 Cluster size Ke (voxels) MNI coordinates (x, y, z) T value 277 59 88 186 216 209 122 100 53 59 52, 30, 10 24, 36, 10 12, 22, 38 70, 10, 6 0, 68, 18 12, 8, 0 4, 38, 28 34, 14, 2 33, 21, 7 6, 10, 70 13.32 6.78 5.67 5.19 5.07 4.70 4.29 4.24 4.19 4.12 571 175 38, 44, 18 0, 40, 8 8.04 3.85 32 48 48 6 BA,BA Brodmann area; R, right; L,=右,L left; M, medial. = Brodmann 領域,R =左,M =中央 perfusion within each cluster are shownR_mPFC in Figure 2B. In PD gamblers, we found significant negative correlations between SOGS score and rCBF in the right ven- ACC trolateral prefrontal cortex (VLPFC), right anterior cingulate cortex (ACC), right posterior cingulate cortex (PCC), right medial frontopolar cortex (mPFC), PCC R_VLPFC R_Insula L_Striatum A PHG Healthy controls PD controls R_mPFC ACC R_mPFC PD gamblers ACC PCC PCC R_VLPFC R_VLPFC R_Insula L_Striatum R_Insula L_Striatum positive PHG ACC R_mPFC Path weight PCC R_VLPFC R_Insula L_Striatum negative Non significant <0.5 PHG PHG 0.5 – 0.75 B >0.75 Figure 3 Functional connectivity 解析により 2 領域間の結合(A における双方向矢印)を同定できる。構造方程式モデリングには特定方向に 関する情報も組み入れている(B における単方向矢印) 。実線は有意なパス,破線は非有意なパスを示す(p < 0.05) 。 FIG. 3. Functional connectivity analysis allows the identification of a connection between two areas (bidirectional arrows in A). SEqM additionally incorporates the specific directional information (unidirectional arrows in B). Solid lines indicate significant pathways and broken lines indicated nonsignificant 32 pathways (P < 0.05). 衝動性 および葛藤下意思決定時のリスクを伴う選択 れている。腹外側前頭前皮質に損傷があると,報酬関連 の尺度と逆相関することが報告さ 処理(プロセシング)に障害が生じ,具体的には,嫌悪 (risk-taking choice) 39-43 Movement Disorders, Vol. 26, No. 2, 2011 229 7 #MD5-1.indb 7 11.7.14 2:24:44 PM パーキンソン病患者の病的賭博には前頭葉‐線条体間の連携離断が関連している:パスモデリング解析 p=0.019 65 70 75 80 85 95 90 PD gamblers 90 88 86 84 82 80 78 76 74 72 70 Striatum 90 88 86 84 82 80 78 76 74 72 70 PD controls Striatum Striatum Healthy controls p=0.038 65 70 75 80 85 90 95 ACC ACC 90 88 86 84 82 80 78 76 74 72 70 p=0.51 65 70 75 80 85 90 95 ACC Figure 4 健常被験者,対照 PD 患者,賭博行為のみられる PD 患者における前帯状皮質‐線条体間の血流量の相関を示す,線形トレンドラ イン付き散布図(p < 0.05) すべき結果やリスクテイキング行動に対する反応が鈍化 習の障害について,その特異的な神経基質が明らかにな する 。さらに,嫌悪すべき結果に対する右腹外側前頭 る可能性がある。 43 前 皮 質 の 反 応 性 低 下 は,病 的 賭 博 お よ び 物 質 嗜 癖 構造方程式モデリング解析で得られた主な所見として, (substance addiction)のある被験者における高い衝動性と 賭博行為のみられる PD 患者では,健常被験者および対 関連することが報告されている 。全体として,こうした 照 PD 患者とは異なり,前帯状皮質から線条体への入力 知見から,この脳領域は,衝動性リスクテイキング行動 が離断していた(Figure 3B および 4) 。条件学習および逆 とネガティブフィードバックからの学習障害とを結び付 転学習の障害 54,55 ならびに反応抑制を要する状況下での ける神経基質として,重要な役割を果たすことが示唆さ 衝動性行動 56-58 の基礎には,前頭前皮質‐線条体間の連 れる。 携離断が存在することは既報の通りであり,意思決定時 44 賭博の重症度と負の相関が認められた他の領域として, の衝動制御には前帯状皮質統合がきわめて重要な役割を 前帯状皮質と線条体があった。健常被験者では,ネガティ 果たすことが示唆される。実際,前帯状皮質は自己監視 ブな結果が出た後,将来の選択を最適化するために行動修 に活発に関与するとともに,線条体を介して行動出力へ 正が必要な場合〔特に,結果の予測可能性が低く,誤差 の経路に影響を及ぼす 59。サルとヒトの両者は,ギャン (error)率が高い場合〕 ,前帯状皮質が活性化される 45-47。 ブリング課題遂行中に同じ win-stay-lose-shift ヒューリス 具体的には,嫌悪すべき結果をもたらすような行動がう ティックを採用している 60。将来の結果を最適化するた まく抑制されている際には腹外側前頭前皮質と線条体が めの強化学習プロセスにおいて,報酬の獲得は「stay」 働いており,一方,前帯状皮質は,行動抑制の失敗によ の選択を強化するのに対し,ネガティブな結果は「shift」 るエラー検出により活性化される 。すなわち,不適切 48-50 の選択を促進すると考えられる。逆転学習の際,被験者 行動を抑制して意思決定戦略を適応させていく能力は, がネガティブフィードバックシグナルの漸増的な蓄積を 不適切行動の発生を監視して反応選択時の葛藤を評価し 経験すると,前帯状皮質の活動度はある閾値まで徐々に ,衝動性リスクテイキ 上昇し,その閾値を超えた場合,線条体‐腹外側前頭前 ング行動の亢進には前帯状皮質の障害が中心的役割を果 皮質軸に作用して行動適応が起こるとともに,過去に報 たすと考えられる。一方,線条体の活動度と賭博重症度 酬を得ていた反応が抑制される 37,45,59,61,62。線条体と腹外 との間には負の相関が認められ,病的賭博でない賭博者 側前頭前皮質は,前帯状皮質に収束する密接な相互接続 が裏付けられた。中脳腹側被蓋野 ネットワークにおいて内側前頭極皮質とも結合し,解剖 から線条体,前頭前皮質,帯状皮質へのドパミン介在性 学的・機能的ループを形成している。このループは,報 シグナル伝達は,報酬予測誤差や将来の選択に関する結 酬で誘発される状況の変化に伴う,このような行動転換 。賭 の監視に不可欠である 62,63。賭博行為のみられる PD 患者 博の重症度は,反応抑制障害に関連するだけでなく,誤っ では,前帯状皮質と線条体の連携離断によりこのループ た選択で生じたネガティブな結果に対する処理(プロセ が破壊されており,シード VOI 結合解析で認められた前 シング) の障害にも関連すると考えられる。この知見から, 帯状皮質および腹外側前頭前皮質活動度の相関の欠如で 病的賭博を伴う PD 患者のネガティブフィードバック学 も,このことが裏付けられている。このような連携離断 ていく能力に依存することから に関する過去の知見 51 46,47 果予測の算定に関与することが知られている 28,47,52,53 8 #MD5-1.indb 8 11.7.14 2:24:46 PM Both monkeys and humans adopt the same win-staylose-shift heuristic during gambling tasks.60 The delivery of reward would strengthen the ‘‘stay’’ while negative outcomes would encourage a ‘‘shift’’ strategy in a reinforcement learning process leading to the optimization of the future results. When a subject accumulate more and more negative feedback signals during reversals, activity in the ACC gradually increases up to a certain threshold and over that threshold it が基礎となり,賭博行為のある PD 患者は特異的に,報 engages the striatum–VLPFC axis to trigger behavioral 酬が得られない状況が繰り返し続いても行動を修正でき adaptations and suppress previously rewarded responses.37,45,59,61,62 The striatum and VLPFC are ない可能性がある。強迫的な薬剤希求状態に関して既に also linked with the 59 mPFC in a closely interconnected 報告されているように network converging on,この連携離断により,自滅的な the ACC to form an anatomical and functional loop that is essential to monitor リスクテイキング行動を執拗に繰り返す傾向が説明でき this shift in relation with changes of context induced る可能性がある。特筆すべきことに,中脳辺縁系のドパ by the reward.62,63 In PD gamblers, the disconnection ミン作動性伝達に異常のある被験者では,衝動性および between the ACC and the striatum disrupts this loop, as further evidenced by the lack of covariance between 依存性行動の素因を生み出す神経基質の基礎として,線 the activity of ACC and the VLPFC found using seed条 体 と 腹 外 側 前 頭 前 皮 質 による 前 帯 状 皮 質 利 用 性 VOI connectivity analysis. This may underlie their spe61,64,65 。reward (recruitment)の低下が既に指摘されている cific inability to adjust behavior after repeated 6explain the proneness to perseveromissions and thus 我々は以前の研究 で,賭博行為のみられる PD 患者 ate in self-destructive risk-taking behaviors, as already では,対応する対照群と比較して,依存性プロセスに関 described in compulsive drug-seeking states.59 Notably, the reduced ACC recruitment of the striatum and 与する「辺縁系」領域における安静時脳血流量が相対的 the VLPFC has already been described as the underlyに高いことを確認している。一方,今回の群内解析では, 賭博重症度の個体差は,むしろ,トップダウンの「認知」 analyses allowed us to identify a specific disconnection between the ACC and the striatum. It may be speculated that this is associated with the progressive inability of PD gamblers to process negative outcomes and disengage from those reward-seeking behaviors that gained abnormal subjective salience through previous R. Cilia et al. dopamine-mediated positive reinforcements, resulting in plastic changes within the dorsal striatum-based habit learning circuitry.59 謝 辞 Dr. Cilia は,CAMH(Toronto)での Research Fellowship へ の支援に関し, 「Fondazione Grigioni il Morbo Grigioni di Parkinson」 Acknowledgments: Dr. Cilia thank theper ‘Fondazione per il Morbo di Parkinson’ for supporting his Research Fellowship at CAMH, に感謝する。また,データの SPM Toronto, and Benedicte Ballanger for very解析に対するきわめて有 helpful advices during SPM analysis of data. 用な助言に関し,Benedicte Ballanger に感謝する。 REFERENCES Antonini A, Cilia R. Behavioural adverse effects of dopaminergic treatments in Parkinson’s disease: incidence, neurobiological basis, management and prevention. Drug Saf 2009;32:475–488. 2. Voon V, Fernagut PO, Wickens J, et al. Chronic dopaminergic stimulation in Parkinson’s disease: from dyskinesias to impulse control disorders. Lancet Neurol 2009;8:1140–1149. 3. Cools R, Barker RA, Sahakian BJ, Robbins TW. L-Dopa medication remediates cognitive inflexibility, but increases impulsivity in patients with Parkinson’s disease. Neuropsychologia 2003;41: 1431–1441. 4. Frank MJ, Seeberger LC, O’reilly RC. By carrot or by stick: cogni- C I Ltive I A reinforcement E T A L . learning in parkinsonism. Science 2004;306: 1940–1943. 5. 監視と不適切行動の抑制に関与する脳領域の機能障害と 関連していた。 今回の試験には,考慮すべき問題がいくつかある。本 試験では,実際のところ,安静時の脳血流 SPECT を用い 6. 認する必要があると考えられる。また,最近の文献 66,67 8. Lee DS, Kang H, Kim H, et al. Metabolic connectivity by interregional correlation analysis using statistical parametric mapping (SPM) and FDG brain PET; methodological development and patterns of metabolic connectivity in adults. Eur J Nucl Med Mol Imaging 2008;35:1681–1691. 結 論 賭博重症度の上昇は,リスクの推定および不適切な報 酬希求行動の抑制に関与する脳領域の進行性障害と関連 Platt ML, Hue decision making 30. Lerner A, Bagic cingulate cortic Cereb Cortex 20 31. Robbins TW. Sh rochemical mod Soc Lond B Biol American Psychiatric Association.Diagnostic and statistical manual of mental disorders, DSM-IV-TR, Fourth ed.Washington, DC: American Psychiatric Association; 2000. 33. Aron AR, Fletc Stop-signal inhib gyrus in humans 11. Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiatry 1987;144:1184–1188. 34. Aron AR, Robb rior frontal cort 35. 12. Voon V, Thomsen T, Miyasaki JM, et al. Factors associated with dopaminergic medication-related pathological gambling in Parkinson disease. Arch Neurol 2007;64:212–216. Arnsten AF. Fun circuits and path 36. Garavan H, Hes ual differences Brain Res 2006; 37. Windmann S, K sion making: lin vation to choic 1198–1211. 38. Picton TW, Stu lingham S. Effe Cereb Cortex 20 39. Rogers RD, Ow small, likely rew and orbital prefr 40. Matthews SC, S tion of the nucl Neuroreport 200 41. McClure SM, L neural systems Science 2004;30 42. Vorhold V, Gie Fink GR. The n tional magnetic gia 2007;45:324 43. Floden D, Alexa and risk-taking chologia 2008;4 44. de Ruiter MB, Z, van den Brin sensitivity to re and smokers. N 45. Ridderinkhof K role of the me 2004;306:443–4 13. Holtgraves T. Evaluating the problem gambling severity index. J Gambl Stud 2009;25:105–120. 14. Deep-Brain Stimulation for Parkinson’s Disease Study Group.Deepbrain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med 2001; 345:956–963. 15. Walovitch RC, Cheesman EH, Maheu LJ, Hall KM. Studies of the retention mechanism of the brain perfusion imaging agent 99mTcbicisate (99mTc-ECD). J Cereb Blood Flow Metab 1994;14 (Suppl 1):S4–S11. 16. Friston KJ. Functional and effective connectivity in neuroimaging: a synthesis. Hum Brain Mapp 1994;2:56–78. 状皮質および線条体間の連携離断が関連すると推察でき 17. Hirao K, Ohnishi T, Matsuda H, et al. Functional interactions between entorhinal cortex and posterior cingulate cortex at the very early stage of Alzheimer’s disease using brain perfusion singlephoton emission computed tomography. Nucl Med Commun 2006;27:151–156. る。 こうした患者では, それまでのドパミンによるポジティ ブ反応の強化により,結果として背側線条体の習慣学習 18. Pagani M, Salmaso D, Rodriguez G, Nardo D, Nobili F. Principal component analysis in mild and moderate Alzheimer’s disease—a novel approach to clinical diagnosis. Psychiatry Res 2009;173: 8–14. 19. Hu L, Bentler P. Cutoff criteria for fit indices in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling 1999;6:1–55. 20. Jöreskog KG, Sörbom D. LISREL-VI user’s guide, Third ed. Mooresville, IN: Scientific Software; 1984. 21. Akaike H. Factor analysis and AIC. Psychometrika 1987;52: 317–332. 22. Byrne B. Structural equation modeling with AMOS: basic concepts, applications, and programming (multivariate applications series), Lawrence Erlbaum Associates, Inc., Publishers, 10 Industrial Avenue, Mahwah, New Jersey; Second ed. Kindle Edition; 2001. 行動が異常な主観的な顕現性(salience)を獲得している 23. #MD5-1.indb 9 29. 10. からの離脱に進行性の障害がみられるが,これには前帯 と考えられる。 Schultz W. Get 2002;36:241–26 Horn NR, Dola inhibition and 2003;41:1959–1 PD 患者では,ネガティブな結果の処理や報酬希求行動 回路内に可塑性の変化が生じ 59,これによって報酬希求 28. 32. していた。結合解析により,前帯状皮質および線条体間 の特異的な連携離断が同定された。賭博行為のみられる Vorhold V. The contributions of cision making un McIntosh AR, Gonzalez-Lima F. Structural equation modeling and its application to network analysis in functional brain imaging. Hum Brain Mapp 1994;2:2–22. 化するため,PD 対照群および非 PD 対照群で男女比を慎 重に一致させたことも, 潜在的な制限となると考えられる。 27. 9. とは矛盾しないものの,賭博行為のみられる PD 患者群 には男性が多く,画像データに対する性別の影響を最小 Cilia R, Siri C, Marotta G, et al. Functional abnormalities underlying pathological gambling in Parkinson disease. Arch Neurol 2008; 65:1604–1611. Steeves TD, Miyasaki J, Zurowski M, et al. Increased striatal dopamine release in Parkinsonian patients with pathological gambling: a [11C] raclopride PET study. Brain 2009;132 (Part 5): 1376–1385. て,特別にデザインされた脳賦活試験で我々の仮説を確 ensemble inhibi 1996;16:3753–3 Bódi N, Kéri S, Nagy H, et al. Reward-learning and the noveltyseeking personality: a between- and within-subjects study of the effects of dopamine agonists on young Parkinson’s patients. Brain 2009;132 (Part 9):2385–2395. Movement Disorders, Vol. 26, No. 2, 2011 231 7. たため,賭博の重症度の神経学的根拠はギャンブリング 課題ではなく相関解析から得られたものである。したがっ References 1. 9 46. Tanabe J, Thom reduced in gamb Schumacker RE, Lomax RG. A Beginner’s guide to structural equation modeling, second ed.Mahwah, NJ: Lawrence Erlbaum sion-making. Hu Associates, Inc.; 2004. 11.7.14 2:24:47 PM 47. Matsumoto M, ning and the noveltysubjects study of the nson’s patients. Brain abnormalities underlyse. Arch Neurol 2008; Increased striatal doth pathological gamn 2009;132 (Part 5): onnectivity by interreparametric mapping development and patEur J Nucl Med Mol 2006;27:151–156. Neuroreport 2004;15:2123–2127. between entorhinal cortex and posterior cingulate cortex at the Science 2004;306:503–507. early of Alzheimer’s disease using brain perfusion single18. very Pagani M,stage Salmaso D, Rodriguez G, Nardo D, Nobili F. Principal 41. Laibson C,DI,Wiedemann Loewenstein G, Schütz Cohen H, JD.Gauggel SeparateS, 42. McClure Vorhold SM, V, Giessing PM, photon emission computed tomography. Med disease—a Commun component analysis in mild and moderate Nucl Alzheimer’s neural systems andratings: delayed monetary Fink GR. The value neural immediate basis of risk evidence fromrewards. a func2006;27:151–156. novel approach to clinical diagnosis. Psychiatry Res 2009;173: Science 2004;306:503–507. tional magnetic resonance imaging (fMRI) study. Neuropsycholo8–14. 18. Pagani M, Salmaso D, Rodriguez G, Nardo D, Nobili F. Principal gia 2007;45:3242–3250. 42. Vorhold V, Giessing C, Wiedemann PM, Schütz H, Gauggel S, analysis in mild and for moderate Alzheimer’s disease—a 19. component Hu L, Bentler P. Cutoff criteria fit indices in covariance strucGR.D,The neural MP, basis Kubu of risk evidence from a func43. Fink Floden Alexander CS,ratings: Katz D, Stuss DT. Impulsivity novel approach to clinical diagnosis. Psychiatry Res 2009;173: ture analysis: conventional criteria versus new alternatives. Struct tional magnetic resonance imaging (fMRI) lobe study.lesions. Neuropsycholoand risk-taking behavior in focal frontal Neuropsy8–14. Equ Modeling 1999;6:1–55. gia 2007;45:3242–3250. chologia 2008;46:213–223. パーキンソン病患者の病的賭博には前頭葉‐線条体間の連携離断が関連している:パスモデリング解析 19. L, Bentler CutoffD.criteria for fituser’s indices in covariance 20. Hu Jöreskog KG, P. Sörbom LISREL-VI guide, Third ed. strucMoor43. D, Alexander MP, DJ, Kubu CS, Katz AE, D, Stuss DT. Impulsivity 44. Floden de Ruiter MB, Veltman Goudriaan Oosterlaan J, Sjoerds ture analysis: conventional criteria versus new alternatives. Struct esville, IN: Scientific Software; 1984. and risk-taking behavior in focal frontal lobeand lesions. Z, van den Brink W. Response perseveration ventralNeuropsyprefrontal Equ Modeling 1999;6:1–55. chologia 2008;46:213–223. 21. Akaike H. Factor analysis and AIC. Psychometrika 1987;52: sensitivity to reward and punishment in male problem gamblers 20. Jöreskog 317–332.KG, Sörbom D. LISREL-VI user’s guide, Third ed. Moorand smokers. Neuropsychopharmacology 2009;34:1027–1038. 44. de Ruiter MB, Veltman DJ, Goudriaan AE, Oosterlaan J, Sjoerds esville, IN: Scientific Software; 1984. van den Brink W.Ullsperger Response M, perseveration ventral prefrontal 45. Z, Ridderinkhof KR, Crone EA,and Nieuwenhuis S. The 22. Byrne B. Structural equation modeling with AMOS: basic concepts, 21. Akaike H. Factor analysis and (multivariate AIC. Psychometrika 1987;52: sensitivity to reward and punishment male problem gamblers role of the medial frontal cortex inincognitive control. Science applications, and programming applications series), 317–332. and smokers. Neuropsychopharmacology 2009;34:1027–1038. 2004;306:443–447. Lawrence Erlbaum Associates, Inc., Publishers, 10 Industrial Avenue, Mahwah, New Jersey; Second ed. Kindle Edition; 2001. 22. Byrne B. Structural equation modeling with AMOS: basic concepts, 45. KR, Ullsperger EA, Nieuwenhuis S. Theis 46. Ridderinkhof Tanabe J, Thompson L, ClausM, E, Crone et al. Prefrontal cortex activity series), role of the medial frontal cortex in substance cognitive users control. Science reduced in gambling and nongambling during deci23. applications, Schumacker and RE, programming Lomax RG. (multivariate A Beginner’s applications guide to structural Lawrence Inc., Publishers, Industrial Ave2004;306:443–447. sion-making. Hum Brain Mapp 2007;28:1276–1286. equation Erlbaum modeling,Associates, second ed.Mahwah, NJ: 10 Lawrence Erlbaum nue, Mahwah, New Jersey; Second ed. Kindle Edition; 2001. Associates, Inc.; 2004. 46. J, Thompson L, ClausK,E,Abe et al. activity is 47. Tanabe Matsumoto M, Matsumoto H,Prefrontal Tanaka K.cortex Medial prefron23. Lomax RG. Beginner’s to structural reduced gambling and nongambling substance users during tal cell in activity signaling prediction errors of action values.deciNat 24. Schumacker Seminowicz RE, DA, Mayberg HS, A McIntosh AR, guide et al. Limbic-frontal equation modeling, second ed.Mahwah, NJ: Lawrence Erlbaum sion-making. Hum Brain Mapp 2007;28:1276–1286. Neurosci 2007;10:647–656. circuitry in major depression: a path modeling metanalysis. NeuroAssociates, Inc.; 2004. image 2004;22:409–418. 47. M, Matsumoto K, Arce Abe H, K. Medial prefron-of 48. Matsumoto Matthews SC, Simmons AN, E, Tanaka Paulus MP. Dissociation 24. DA,Derro Mayberg HS, McIntosh et al. Limbic-frontal tal cell activity prediction errors of actioninhibitory values. Nat 25. Seminowicz Ottowitz WE, D, Dougherty DD, AR, Lindquist MA, Fischman inhibition from signaling error processing using a parametric task circuitry major depression: a path modeling metanalysis. NeuroNeurosci 2007;10:647–656. AJ, HallinJE. FDG-PET analysis of amygdalar-cortical network coduring functional magnetic resonance imaging. Neuroreport 2005; image 2004;22:409–418. variance during pre- versus post-menopausal estrogen levels: poten16:755–760. 48. Matthews SC, Simmons AN, Arce E, Paulus MP. Dissociation of tial relevance to resting state networks, mood, and cognition. 25. Ottowitz WE, Derro D, Dougherty DD, Lindquist MA, Fischman fromManuck error processing parametric inhibitory taskof 49. inhibition Brown SM, SB, Floryusing JD, aHariri AR. Neural basis Neuro Endocrinol Lett 2008;29:467–474. AJ, Hall JE. FDG-PET analysis of amygdalar-cortical network coduring functional magnetic resonance contributions imaging. Neuroreport 2005; individual differences in impulsivity: of corticolimbic variance during preversus post-menopausal estrogen levels: poten16:755–760. 26. Nyberg L, McIntosh AR, Cabeza R, et al. Network analysis of circuits for behavioral arousal N E and U R control. A L C Emotion O R R E 2006;6: L A T E S tial relevance to resting state regional networks,cerebral mood, blood and cognition. positron emission tomography flow data: 239–245. 49. Brown SM, Manuck SB, Flory JD, Hariri AR. Neural basis of Neuro Endocrinol Lett 2008;29:467–474. 50. individual Chevrier AD, Noseworthy MD, Schachar R. Dissociation of response differences in impulsivity: contributions of corticolimbic inhibition performance monitoring in the stop signal task using 26. Nyberg L, McIntosh AR, Cabeza R, et al. Network analysis of circuits forand behavioral arousal and control. Emotion 2006;6: event-related fMRI. Hum Brain Mapp 2007;28:1347–1358. positron emission tomography regional cerebral blood flow data: 239–245. ensemble inhibition during episodic memory retrieval. J Neurosci 51. Reuter J, Raedler T, Rose M, Hand I, Glascher J, Buchel C. Patholgical gambling is linked to reduced activation of the mesolimbic 232 1996;16:3753–3759. Movement Disorders, Vol. 26, No. 2, 2011 reward system. Nat Neurosci 2005;8:147–148. 27. Vorhold V. The neuronal substrate of risky choice: an insight into the contributions of neuroimaging to the understanding of theories on de52. Doya K. Modulators of decision making. Nat Neurosci 2008;11: making under risk. Ann NY Acad Sci 2008;1128:41–52. 410–416. 232 cisionMovement Disorders, Vol. 26, No. 2, 2011 28. Schultz W. Getting formal with dopamine and reward. Neuron 53. Rushworth MF, Behrens TE. Choice, uncertainty and value in pre2002;36:241–263. frontal and cingulate cortex. Nat Neurosci 2008;11:389–397. 29. Platt ML, Huettel SA. Risky business: the neuroeconomics of 54. Parkinson JA, Willoughby PJ, Robbins TW, Everitt BJ. Disconnecdecision making under uncertainty. Nat Neurosci 2008;11:398–403. tion of the anterior cingulate cortex and nucleus accumbens core impairs Pavlovian approach behavior: further evidence for limbic 30. Lerner A, Bagic A, Hanakawa T, et al. Involvement of insula and cortical ventral striatopallidal systems. Behav Neurosci 2000;114: cingulate cortices in control and suppression of natural urges. 42–63. Cereb Cortex 2009;19:218–223. 55. Horn NR, Dolan M, Elliott R, Deakin JF, Woodruff PW. Response inhibition and impulsivity: an fMRI study. Neuropsychologia 2003;41:1959–1966. Block AE, Dhanji H, Thompson-Tardif SF, Floresco SB. Thalamicprefrontal cortical-ventral striatal circuitry mediates dissociable components of strategy set shifting. Cereb Cortex 2007;17: 1625–1636. 56. 33. Aron AR, Fletcher PC, Bullmore ET, Sahakian BJ, Robbins TW. Stop-signal inhibition disrupted by damage to right inferior frontal gyrus in humans. Nat Neurosci 2003;6:115–116. Potts GF, George MR, Martin LE, Barratt ES. Reduced punishment sensitivity in neural systems of behavior monitoring in impulsive individuals. Neurosci Lett 2006;397:130–134. 57. 34. Aron AR, Robbins TW, Poldrack R. Inhibition and the right inferior frontal cortex. Trends Cogn Sci 2004;8:170–177. Leibenluft E, Rich BA, Vinton DT, et al. Neural circuitry engaged during unsuccessful motor inhibition in pediatric bipolar disorder. Am J Psychiatry 2007;164:52–60. 58. Mobbs D, Eckert MA, Mills D, et al. Frontostriatal dysfunction 35. N E U R A L C O R R disorder: E L A T E S Arnsten AF. Fundamentals of attention-deficit/hyperactivity circuits and pathways. J Clin Psychiatry 2006;67 (Suppl. 8):7–12. Chevrier AD, Noseworthy MD, Schachar R. Dissociation of response Garavan Hester R, Murphy K, Fassbender C, Kelly IndividinhibitionH,and performance monitoring in the stop signalC.task using ual differences in the functional anatomy of inhibitory control. event-related fMRI. Hum Brain Mapp 2007;28:1347–1358. Brain Res 2006;1105:130–142. Reuter J, Raedler T, Rose M, Hand I, Glascher J, Buchel C. PathWindmann S, Kirsch P, Mier et al. activation On framing in deciolgical gambling is linked to D, reduced of effects the mesolimbic sion making: linking lateral versus medial orbitofrontal cortex actireward system. Nat Neurosci 2005;8:147–148. vation to choice outcome processing. J Cogn Neurosci 2006;18: Doya K. Modulators of decision making. Nat Neurosci 2008;11: 1198–1211. 410–416. Picton TW, Stuss DT, Alexander MP, Shallice T, Binns MA, GilRushworth MF, Behrens TE. Choice, uncertainty and value in prelingham S. Effects of focal frontal lesions on response inhibition. frontalCortex and cingulate cortex. Nat Neurosci 2008;11:389–397. Cereb 2007;17:826–838. 31. Robbins TW. Shifting and stopping: fronto-striatal substrates, neurochemical modulation and clinical implications. Philos Trans R Soc Lond B Biol Sci 2007;362:917–932. quation modeling and tional brain imaging. 32. and statistical manual ed.Washington, DC: mbling Screen (SOGS): pathological gamblers. actors associated with l gambling in Parkin- bling severity index. J se Study Group.Deepor the pars interna of N Engl J Med 2001; all KM. Studies of the imaging agent 99mTcMetab 1994;14 (Suppl vity in neuroimaging: unctional interactions ngulate cortex at the brain perfusion singleNucl Med Commun D, Nobili F. Principal Alzheimer’s disease—a hiatry Res 2009;173: es in covariance strucew alternatives. Struct uide, Third ed. Moor- chometrika 1987;52: 50. 36. 51. 37. 52. 38. 53. 54. Rogers Parkinson Willoughby PJ, Robbins Everitt BJ. Disconnec39. RD,JA, Owen AM, Middleton HC,TW, et al. Choosing between tion oflikely the anterior cingulate andrewards nucleusactivates accumbens core small, rewards and large,cortex unlikely inferior impairs Pavlovian approach evidence for limbic and orbital prefrontal cortex. Jbehavior: Neurosci further 1999;19:9029–9038. cortical ventral striatopallidal systems. Behav Neurosci 2000;114: 40. Matthews 42–63. SC, Simmons AN, Lane SD, Paulus MP. Selective activation of the nucleus accumbens during risk-taking decision making. 55. Neuroreport Block AE, Dhanji H, Thompson-Tardif SF, Floresco SB. Thalamic2004;15:2123–2127. prefrontal cortical-ventral striatal circuitry mediates dissociable 41. McClure SM, Laibson DI, set Loewenstein Cohen JD. Separate components of strategy shifting. G, Cereb Cortex 2007;17: neural systems value immediate and delayed monetary rewards. 1625–1636. Science 2004;306:503–507. 56. Potts GF, George MR, Martin LE, Barratt ES. Reduced punish42. Vorhold V, Giessing C, Wiedemann PM, Schütz H, Gauggel S, ment sensitivity in neural systems of behavior monitoring in impulFink GR. The neural basisLett of risk ratings: evidence from a funcsive individuals. Neurosci 2006;397:130–134. tional magnetic resonance imaging (fMRI) study. Neuropsycholo57. gia Leibenluft E, Rich BA, Vinton DT, et al. Neural circuitry engaged 2007;45:3242–3250. during unsuccessful motor inhibition in pediatric bipolar disorder. 43. Floden D, Alexander MP, Kubu CS, Katz D, Stuss DT. Impulsivity Am J Psychiatry 2007;164:52–60. and risk-taking behavior in focal frontal lobe lesions. Neuropsy58. chologia Mobbs D, Eckert MA, Mills D, et al. Frontostriatal dysfunction 2008;46:213–223. during response inhibition in Williams syndrome. Biol Psychiatry 44. de Ruiter MB, Veltman DJ, Goudriaan AE, Oosterlaan J, Sjoerds 2007;62:256–261. Z, van den Brink W. Response perseveration and ventral prefrontal sensitivity to reward and punishment in male problem gamblers and smokers. Neuropsychopharmacology 2009;34:1027–1038. 45. Ridderinkhof KR, Ullsperger M, Crone EA, Nieuwenhuis S. The role of the medial frontal cortex in cognitive control. Science 2004;306:443–447. 46. Tanabe J, Thompson L, Claus E, et al. Prefrontal cortex activity is reduced in gambling and nongambling substance users during decision-making. Hum Brain Mapp 2007;28:1276–1286. 47. Matsumoto M, Matsumoto K, Abe H, Tanaka K. Medial prefrontal cell activity signaling prediction errors of action values. Nat Neurosci 2007;10:647–656. #MD5-1.indb 10 48. Matthews SC, Simmons AN, Arce E, Paulus MP. Dissociation of AMOS: basic concepts, e applications series), rs, 10 Industrial Avee Edition; 2001. s guide to structural10 J: Lawrence Erlbaum , et al. Limbic-frontal g metanalysis. Neuro- inhibition Biol IPsychiatry O F during P A Tresponse H O L O G I C AinL Williams G A Msyndrome. B L I N G N P D 2007;62:256–261. 59. Sinha R. Inhibitory control and emotional stress regulation: neuroimaging evidence for frontal-limbic dysfunction in psycho-stimulant addiction. Neurosci Biobehav Rev 2008;32:581–597. 60. Hayden BY, Platt ML. Gambling for Gatorade: risk-sensitive decision making for fluid rewards in humans. Anim Cogn 2009;12: 201–207. 61. Jocham G, Klein TA, Neumann J, von Cramon DY, Reuter M, Ullsperger M. Dopamine DRD2 polymorphism alters reversal learning and associated neural activity. J Neurosci 2009;29:3695–3704. 62. Pochon JB, Levy R, Fossati P, et al. The neural system that bridges reward and cognition in humans: an fMRI study. Proc Natl Acad Sci USA 2002;99:5669–5674. 63. van Leijenhorst L, Crone EA, Bunge SA. Neural correlates of developmental differences in risk estimation and feedback processing. Neuropsychologia 2006;44:2158–2170. 64. Klein TA, Neumann J, Reuter M, Hennig J, von Cramon DY, Ullsperger M. Genetically determined differences in learning from errors. Science 2007;318:1642–1645. 65. Comings DE, Rosenthal RJ, Lesieur HR, et al. A study of the dopamine D2 receptor gene in pathological gambling. Pharmacogenetics 1996;6:223–234. 66. Gallagher DA, O’Sullivan SS, Evans AH, Lees AJ, Schrag A. Pathological gambling in Parkinson’s disease: risk factors and differences from dopamine dysregulation. An analysis of published case series. Mov Disord 2007;22:1757–1763. 67. Weintraub D. Impulse control disorders in Parkinson’s disease: prevalence and possible risk factors. Parkinsonism Relat Disord 2009;15 (Suppl 3):S110–S113. O F P A T H O L 59. Sinha R. Inhibit maging evidence addiction. Neuro 60. Hayden BY, Pla sion making fo 201–207. 61. Jocham G, Klein sperger M. Dop and associated n 62. Pochon JB, Levy reward and cog Sci USA 2002;99 63. van Leijenhorst velopmental diff Neuropsycholog 64. Klein TA, Neum sperger M. Gen errors. Science 2 65. Comings DE, R pamine D2 rece netics 1996;6:22 66. Gallagher DA, O logical gambling from dopamine Mov Disord 200 67. Weintraub D. prevalence and 2009;15 (Suppl 11.7.14 2:24:48 PM 無動‐筋強剛型および振戦優位型パーキンソン病 患者では FP-CIT SPECT 所見が異なる Akinetic-Rigid and Tremor-Dominant Parkinson’s Disease Patients Show Different Patterns of FP-CIT Single Photon Emission Computed Tomography * Carsten Eggers, MD, Deniz Kahraman, MD, Gereon R. Fink, MD, Matthias Schmidt, MD, and Lars Timmermann, MD * Department of Neurology, University of Cologne, Cologne, Germany 目的:パーキンソン病の各サブタイプにより,神経病理 取り込みに有意差が認められた。患者の年齢,罹病期間, 学的所見の違いを反映して,Iodine-123 fluoropropyl- 疾患重症度(Hoehn & Yahr 分類,Unified Parkinson’ s carbomethoxy-3 β -(FP-CIT) SPECT におけるドパミ Disease Rating Scale スコア) ,レボドパ(L—ドパ)換 ントランスポーターの結合パターンが異なるか否かを検 算用量をマッチさせた場合,これらの所見は両群間(各 討した。 。 23 例) で均衡し, 有意差は認められなかった (p >0.05) 方法:過去 3 年間に FP-CIT SPECT を受けた一連の患 しかし,FP-CIT SPECT 画像の視覚的解析による線条 者のデータベース(190 例)を解析し,孤発性パーキン 体形状とパーキンソン病臨床サブタイプとの間には,明 ソン病と診断された患者 122 例 (女性 50 例, 男性 72 例, 確かつ有意な関連が認められた。 平均年齢 62 ± 11.1 歳)を特定した。患者背景と FP- 結論:これらの結果から,無動‐筋強剛型パーキンソン CIT SPECT 結果を解析し,振戦優位型,無動‐筋強剛型, 病患者では背側被殻に向かうドパミン作動性投射が,ま 混合型(equivalent type)サブタイプ間で比較した。 た,振戦優位型パーキンソン病患者では外側被殻およ 結果:全パーキンソン病患者を対象とした解析では,振 び尾状核に向かうドパミン作動性投射が減少していると 戦優位型および無動‐筋強剛型サブタイプ間で FP-CIT いう in vivo の神経病理学的モデルが裏付けられた。 Movement Disorders, Vol. 26, No. 3, 2011, pp. 416–423 Key Word Iodine-123 fluoropropyl-carbomethoxy-3 β -SPECT,パーキンソン病,視覚的解析,パーキンソン病サ ブタイプ パーキンソン病(Parkinson’ s disease; PD)は,ドパミ Jellinger 6 は,神経病理学的所見に基づき,各 PD サブタ ン作動性黒質線条体投射の喪失により生じる動作緩慢, イプごとに異なる,線条体構造への黒質ドパミン作動性 筋強剛,振戦,姿勢反射障害を特徴とする運動障害を伴 ニューロン投射のモデルを描いた。すなわち,無動‐筋 う進行性の神経変性疾患である。この神経病理学的変化 強剛型では,背側被殻に投射する黒質緻密部の腹外側部 は複雑な大脳基底核ネットワークに影響を及ぼす 。 の細胞がより高度に脱落している。一方,振戦優位型の 1,2 PD サブタイプにより臨床経過が異なることについて 場合,ニューロンの脱落は,黒質緻密部の外側部(尾状 。振戦優位型 核および前部被殻に投射)および赤核後部(背外側線条 PD 患者は疾患の進行がより緩徐で,認知機能障害も比 体および腹内側視床に投射)よりも,内側部でより高度 較的軽度である 。Rajput ら は,臨床病理学的研究に である。Spiegel ら 7 は,このモデルと一致して,振戦優 おいてこのような臨床的証拠を確認している。彼らの報 位型 PD 患者では,臨床的患側の反対側の被殻および尾 告によると,振戦優位型 PD 患者のほうが無動‐筋強剛 状核における Iodine-123 fluoropropyl-carbomethoxy-3 β 型 PD 患者よりも転帰が良好であり,臨床サブタイプに -(FP-CIT) 取り込みが,無動‐筋強剛型 PD 患者よりも有 一 致 し て 脳 の 生 化 学 的 異 常 に 違 い が 認 め ら れ る。 意に高いことを示した。この研究では,対象患者の病期 は,明確な臨床的証拠が得られている 3,5 3,4 3 11 #MD5-1.indb 11 11.7.14 2:24:50 PM 無動‐筋強剛型および振戦優位型パーキンソン病患者では FP-CIT SPECT 所見が異なる が非常に早期であり,障害も軽度に過ぎなかった〔平均 UK Parkinson’ s Disease Society Brain Bank の基準によった 13。 Hoehn and Yahr(HY) 分 類:1,Unified Parkinson’ s 平均 HY 分類は 2.1 ± 0.6(標準偏差)であった 14。疾患重 Disease Rating Scale(UPDRS)Part Ⅲ(運動機能) :12 ポ 15 症度の評価には UPDRS Part Ⅲ (運動機能) を使用した (平 イント〕 。これに対し,他の画像研究〔FP-CIT SPECT, 均 UPDRS スコア 30.3 ± 15.7) 。UPDRS の評価は「off」 3,4- d i h y d r o x y -6- F - f l u o r o - L - p h e n y l a l a n i n e - P E T 期(薬剤を 12 時間投与していない状態)に行った。振戦 ( F-FDOPA-PET) ,{11C}d-threo-methylphenidate PET 優位型または無動‐筋強剛型の臨床サブタイプ判定にお (11C-dMP-PET) 〕8-10 では,PD サブタイプごとの明確な差 いては,第 1 段階として,経験のある運動障害専門医 2 異は認められていない。このように,画像検査結果につ 名が臨床的に判断した。第 2 段階では,Lewis ら 16 と同 いては議論の余地があり,現時点において,線条体のド 様の方法により,各患者の「振戦スコア」と「非振戦ス パミン取り込みと PD サブタイプとの間に明確な関連性 コア」を算出した。すなわち,振戦スコアは,UPDRS 項 は確立されていない。 目 20(安静時振戦)および 21(手の動作時振戦または姿 18 18 [ I]FP-CIT SPECT(DaTSCAN, Amersham Health, 勢時振戦)の合計ポイントを 7〔評価した下位項目数(別々 UK)画像,ドパミントランスポーター,ドパミントラン に評価している場合の各身体領域の数) 〕で割って算出し スポーター喪失の所見は,PD 患者の剖検時に認められ た。非振戦スコアは,UPDRS 項目 18(言語) ,19(顔の る黒質線条体障害と対応することが報告されている 表情) ,22(筋強剛) ,27(椅子からの立ち上がり) ,28(姿 123 。 11,12 したがって,FP-CIT SPECT は,PD 患者の神経変性を実 勢) ,29(歩行) ,30(姿勢の安定性) ,31(身体寡動およ 証する方法として適切である。 び運動減少)の合計ポイントを 12〔評価した下位項目数 我々は,振戦優位型 PD 患者と無動‐筋強剛型 PD 患 (別々に評価している場合の各身体領域の数) 〕で割って 者における既知の臨床転帰の違いを踏まえ,過去 3 年間 算出した。 振戦スコアが非振戦スコアの2 倍以上であれば, に当施設で実施した一連のすべての FP-CIT SPECT を対 振戦優位型に分類した。逆の場合も同様に,非振戦スコ 象とした後向きデータ解析を実施し,PD サブタイプと アが振戦スコアの 2 倍以上であれば,無動‐筋強剛型に FP-CIT SPECT の視覚的所見が Jellinger モデルに一致し 分類した。それ以外の場合,すなわち,振戦スコアと非 た関連性を示すか否かを検討した。上記の知見と我々の 振戦スコアの差が 2 倍未満の患者は,混合型に分類した。 臨床経験に基づき,無動‐筋強剛型 PD サブタイプでは, 罹病期間は発症時期に基づいて決定した。さらに,各患 脳後部におけるドパミン取り込みの低下が振戦優位型 PD 者について振戦優位型, 無動‐筋強剛型, 混合型(equivalent サブタイプよりも著明であるという仮説を立てた。もし type)に分類した。ドパミントランスポーターに関するセ この仮説が正しければ,無動‐筋強剛型サブタイプの レギリン代謝物と FP-CIT の相互作用を避けるため 17,セ FP-CIT SPECT では「卵形(egg-shaped)像」が認められ レギリンによる治療は FP-CIT 投与の少なくとも 18 時間 るであろう。同様に,振戦優位型 PD 患者では,被殻に 前に中止した。それ以外の抗パーキンソン病治療薬は おける FP-CIT 取り込みの低下により, 被殻の狭小化と「鷲 SPECT 検査中も継続した。臨床情報の詳細については の翼(eagle-wing)像」が認められると考えられる。 Table 1 も参照されたい。本研究では後向き解析を採用し たため,施設内倫理委員会による承認はドイツ連邦法お 材料および方法 方法 被験者 2007 年 1 月 1 日~ 2009 年 12 月 31 日に当施設で FP-CIT よび本大学規則(local university regulations)に照らして 必須ではなかった。しかし,施設内倫理委員会は,要請 に応じた検討の結果,本研究手法を公式に承認している。 全患者の中から 2 つのサブグループを設定した。サブ グループ1は,振戦優位型(23 例)および無動‐筋強剛 SPECT を受けたすべての患者(190 例)のデータベースを 型(68 例)のすべての患者を含んだ。サブグループ 2 は, 解析した。孤発性 PD 患者 122 例(女性 50 例,男性 72 例, 年齢,罹病期間,疾患重症度(HY 分類および UPDRS 平均年齢 62 ± 11.1 歳)が特定された。患者はいずれも, スコア) ,レボドパ(L—ドパ)換算用量をマッチさせた, FP-CIT SPECT のため当施設を紹介される以前に,運動障 振戦優位型(23 例)および無動‐筋強剛型(23 例)PD 害専門医による診察を受けていた。孤発性 PD の診断は, 患者のペアで構成した。条件をマッチさせたサブグルー 12 #MD5-1.indb 12 11.7.14 2:24:51 PM C. Eggers et al. E G G E R S E T A L . Table 1 患者背景 TABLE 1. Patient’s characteristics Subgroup 1 N Mean age Male/female Mean Hoehn & Yahr Mean UPDRS Part III Disease duration L-Dopa-equivalent dose Tremor-dominant/akinetic-rigid/equivalent Subgroup 2 All patients Tremor-dominant Akinetic-rigid Tremor-dominant Akinetic-rigid 122 62 6 11.1 72/50 2.1 6 0.6 30.3 6 15.7 5.5 6 4.41 538 6 375 23/68/31 23 60.83 6 11.7 15/8 1.7 6 0.6 25.1 6 13.0 4.52 6 3.5 439 6 343 – 68 62 6 10.6 38/30 2.2 6 0.6 30.7 6 16.2 6.05 6 4.6 602 6 401 – 23 60.83 6 11.7 15/8 1.7 6 0.6 25.1 6 13.0 4.52 6 3.5 439 6 343 – 23 61 6 10.5 16/7 2.0 6 0.6 25.4 6 12.3 4.0 6 2.5 372 6 356 – Subgroup 1, nonmatched tremor-dominant and akinetic-rigid patients. Subgroup 2, matched PD pairs患者。サブグループ of tremor-dominant and akinetic-rigid patients. サブグループ 1:条件をマッチさせていない振戦優位型および無動‐筋強剛型 2:条件をマッチさせた振戦優位 型および無動‐筋強剛型患者のペア。 Data Acquisition and Analysis Data Processing プ 2は, 各項目について5 組ずつ作成した。 このサブグルー Thirty minutes prior injection, all patients received poプは,最も一致度が高い患者ペアを選択してプールした tassium iodide orally to block the thyroid gland before ものである。 intravenous administration of 185 MBq [123I] FP-CIT: [123I] N-x-fluoropropyl-2b-carbomethoxy-3b-(4-iodophenyl) nortropane (GE Healthcare) to prevent accumuデータ収集および解析 lation of free radioactive iodine in the thyroid gland. SPECT image data acquisition was performed 3 データ処理 hour post injection18,19 with a triple-headed rotating 甲状腺への遊離放射性ヨードの蓄積を防止するため, camera (Picker Prism 3000) using low energy, high-re123 約 185 MBq[ I]FP-CIT: [123I]Nω -fluoropropyl-2β solution parallel hole collimator. One hundred twenty in 128 128 projections were acquired over 360 -ca rbomethoxy-3β-(4-iodophenyl) nortaropane(GE Matrix. The unprocessed projection data was conHealthcare)の静注の 30 分前に,甲状腺ブロック用のヨ trolled with a sinogram and sine display on an Odyssey-FX workstation (Phillips Medical Systems) for ウ化カリウムを全患者に経口投与した。 possible patient motion and artifacts. The 18,19 digital SPECT 画像データは,静注後 3 時間の時点で ,低 images were reconstructed by using a low-pass filter エネルギーの高解像度平行孔コリメータを用いて 3 検出 (Cutoff 0.4 Nyquist, order 8) and corrected with the 18 algorithm for attenuation as previously published. 器回転カメラ(Picker Prism 3000)で収集した。マトリク To analyze the dopaminergic deficit, two different スサイズ 128for ×quantification 128 で 360°方向にわたり approaches are available:120 (1)枚の投影 the twodimensional semi-quantitative region of interest (ROI)像を収集した。患者の体動やアーチファクトの可能性を based method and (2) a three-dimensional approach 考慮し,未処理の投影像データに対して ワー that relates the uptake to a normal Odyssey-FX image template (BRASS tool) on a HERMES workstation (Nuclear クステーション(Phillips Medical Systems)でサイノグラ Diagnostics, Stockholm, Sweden). Both methods allow ムおよび正弦波表示(sine display)による調整を行った。 an observer-independent differentiation between PD デジタル画像はローパスフィルター(カットオフ周波数: and essential tremor.18,20 Additionally to these (semi-) quantitative analyses, visual inspection of FP-CIT ナイキスト周波数の 0.4the 倍,オーダー:8)を用いて再構 SPECT scans allows to grade the images (3).8,21 This 18 成し,既報の通り 減弱補正を行った。 observer-independent approach also allows to differentiate between PD and essential tremor. Analyses were ドパミン作動性ニューロンの脱落状況の解析には,次 performed blinded to the clinical data. の 2 つの定量法が利用可能である。すなわち, (1)二次 元の半定量的な関心領域(ROI)を用いる方法と, (2) Manual ROI Technique. For the manual evaluation method, five consecutive slices with the highest striatal HERMES ワ ー ク ス テ ー シ ョン(Nuclear Diagnostics, image count were selected and summed up to a single Stockholm, Sweden)上で正常画像テンプレート(BRASS slice for analysis of striatal [123I]FP-CIT binding (total thickness 10 mm). The ratio of specific to nonspecific ツール) に取り込みを関連付けていく三次元の方法である。 binding was calculated by standardized, two-dimenいずれの方法も,観察者に依存せずに PD と本態性振戦 sional ROIs (derived from an anatomical brain atlas), which were placed bilaterally over the striatum with 8,21 (3)FP-CIT SPECT 画像の視覚的評価も可能である subregions for caudate and putamen. A ROI over the。 occipital cortex was used as the reference region to この観察者に依存しない方法でも,PD と本態性振戦を鑑 assess nonspecific binding. If necessary, each ROI was 別できる。解析は臨床データを伏せた状態で実施した。 adjusted manually. Specific FP-CIT tracer uptake was calculated with both methods 手動による ROIfor 法 caudate and putamen using the formula: [(mean counts of the target ROI/volume-of手動での評価法として,線条体の画像カウントが最も interest (VOI) mean counts of background)/(mean 123 counts of the5 枚のスライスを選択し,線条体[ background)]. 高い,連続 I]FPCIT 結合解析用に 1 枚のスライスにまとめた(トータル Automated Method/BRASS Tool. For the automated semi-quantitative analysis, HERMES BRASS was の厚さは 10 mm) 。非特異的結合に対する特異的結合の used. BRASS automatically fits the patient’s image 比は,標準化された二次元 ROI(解剖学的脳地図に由来) data to a reference template created from healthy conから求め, ROI は, trols. Thisこれらの is followed by尾状核と被殻の亜領域も含め, placing a predefined threedimensional VOI for the quantification of specific to 線条体を覆うように両側で設定した。後頭皮質を覆う nonspecific binding for striatum, caudate, putamen, ROI を,非特異的結合を評価するための基準領域とした。 and occipital cortex.18,20 The automated fitting algorithm includes an adjustment of the VOIs to compen必要に応じて各 ROI を手動で補正した。 sate anatomic variation. 両者の方法について,尾状核と被殻の特異的 FP-CIT Visual Interpretation. For visual interpretation, two トレーサ取り込みを次式により計算した。 [ (標的 ROI の experienced nuclear medicine physicians (DK and MS), 平均カウント / 関心体積(volume-of-interest; VOI)−背 blinded for clinical data, examined the hardcopy images (i.e., the transaxial images) and classified ]the SPECT 景の平均カウント)/(背景の平均カウント) images into five different patterns of striatal FP-CIT uptake. Before evaluation, both examiners were handed 自動法 Tool representative examples for each out an /BRASS atlas including of 自動の半定量的解析には the five predefined patterns, as follows (Fig. 1): grade HERMES BRASS を使用した。 5 (normal) showed a symmetrical uptake bilaterally in BRASS は,健常対照被験者から作成した基準テンプレー putamen and caudate nuclei; grade 4 (eagle wing) shows an almost患者の画像データを自動で調整する機能をもつ。 normal, symmetrical uptake with a discrete トに対し, reduction in one or both putamina; grade 3 (mixed 調整後には,線条体,尾状核,被殻,後頭皮質について, type) shows an asymmetric uptake with normal or 非特異的結合に対する特異的結合を定量するため,あら almost normal uptake in the putamen in one hemisphere but reduced uptake in が設定される the contralateral 18,20 putamen; かじめ定義された三次元 VOI 。この自動 grade 2 (egg shape) was defined as showing a significant 調整アルゴリズムには,解剖学的な変動を相殺するための bilateral reduced uptake in the putamen bilaterally and normal or almost normal uptake in the caudate nuclei; VOI 補正も含まれる。 grade 1 (burst striatum) was defined as showing severe を鑑別可能である 18,20。これらの(半)定量的解析に加え, 418 Movement Disorders, Vol. 26, No. 3, 2011 13 03_Full-2_MD5-1.indd 13 11.7.14 5:35:14 PM 無動‐筋強剛型および振戦優位型パーキンソン病患者では FP-CIT SPECT 所見が異なる 評価に先立ち,あらかじめ定義した 5 パターンの各代表 例を示すアトラスを配布した。詳細は以下の通りである (Figure 1) 。グレード 5(正常)は,被殻および尾状核に 両 側 対 称 性 の 取り込 みを示 す。グレ ード 4〔 鷲 の 翼 (eagle-wing)像〕は,一側または両側被殻における不連 続な低下を伴う,ほぼ正常な対称性取り込みを示す。グ レード 3(混合型)は,非対称性の取り込みを示し,一 側半球の被殻では正常ないしほぼ正常な取り込みがみら Grade 5 : Normal Grade 4 : Eaglewing れるが,対側被殻では取り込みが低下している。グレー ド 2〔卵形(egg-shaped)像〕は,両側被殻に有意な取り 込み低下がみられ,尾状核では正常ないしほぼ正常な取 り込 み を 示 す。 グ レ ード 1〔 線 条 体 バ ー スト(burst striatum)像〕は,被殻と尾状核の両者でほとんど取り込 みを欠いており,両側性の高度の取り込み低下を示す。 統計解析 年齢,UPDRS スコア,HY 分類,罹病期間,L—ドパ換 Grade 3 : Mixed type Grade 2 : Egg shape 算用量,ならびに同側および対側の被殻と尾状核の半定 量的解析および BRASS 解析結果について,平均値と標 準偏差(SD)を算出した。振戦優位型 PD および無動‐ 筋強剛型 PD サブタイプ間のドパミン作動性ニューロン 脱落状況の有意差を検出するため,PASW Statistics 18 (SPSS, Chicago, IL)の独立サンプルに関する Student t 検 定を用い,同側と対側の被殻および尾状核の半定量的解 析および BRASS 解析の結果を比較した。 視覚的解析に由来するデータはノンパラメトリックな 性質を有するため,2 つの PD サブタイプ間および視覚的 Grade 1 : Burst striatum Figure 1 グレード 5(正常) :被殻および尾状核に強くかつ対称性 の取り込みがみられる。グレード 4〔鷲の翼(eagle-wing)像〕 :一 側または両側被殻における不連続な低下を伴う,ほぼ対称性の取り 込みがみられる。グレード 3(混合型) :非対称性の取り込みであり, 一側半球の被殻では正常ないしほぼ正常な取り込み,対側被殻で は高度低下がみられる。グレード 2〔卵形(egg-shaped)像〕 :両側 被殻に有意な取り込み低下がみられ,尾状核では正常ないしほぼ正 常な取り込みがみられる。グレード 1〔線条体バースト(burst striatum)像〕 :被殻と尾状核の両者でほとんど取り込みを欠いてお り,両側性の高度の取り込み低下がみられる。 に評価したそれぞれの線条体 FP-CIT 取り込み間の平均 値の比較には,ブートストラップ法 22 を用いた。ブート ストラップ法では, 被験者 23 例の 1,000 のブートストラッ プサンプルを無動‐筋強剛型 PD 患者から無作為に抽出 し,帰無仮説下で,振戦優位型 PD 患者において視覚的 に評価した平均線条体 FP-CIT 取り込み分布をトレース した。1,000 の抽出サンプルのそれぞれについて,無動‐ 筋強剛型 PD 患者で線条体の卵形(egg-shaped)像が出 現する平均頻度を算出した。検定統計量の棄却限界値と して,反復 1,000 回の 5 パーセンタイルを使用した。例 視覚的評価 視覚的評価では,臨床データを伏せた状態にある 2 名 の経験のある核医学専門医(DK および MS)がハードコ えば,振戦優位型 PD 患者における鷲の翼(eagle-wing) 像の出現頻度がこの棄却限界値を上回る / 下回る場合に は,差は 5%レベルで有意とみなした。 ピー画像(横断像)を検討し,SPECT 画像の線条体 FPCIT 取り込みパターンを 5 つに分類した。両検査者には, 14 #MD5-1.indb 14 11.7.14 2:24:54 PM C. Eggers et al. により,各 PD サブタイプの異なる神経病理学的特徴を 結 果 反映するパターン分類が可能であることを示唆している。 患者群の詳しい臨床データを 2 つのサブグループに分 けて Table 1 にまとめている。視覚的画像解析では,患者 神経病理学的所見 12 例が線条体バースト(burst striatum)像,85 例が卵形 PD の経過(臨床サブタイプは考慮しない)における (egg-shaped)像,10 例が混合型像,15 例が鷲の翼(eagle- FP-CIT 取り込みの変化については, 「コンマからドットに」 wing)像を示した〔振戦優位型 PD 患者:線条体バース という表現がよく使われる。一般に,FP-CIT 取り込みの ト(burst striatum)像 1 例 / 卵形(egg-shaped)像 15 例 / 低下は,ドパミン作動性ニューロンの進行中の脱落を反 混合型像 2 例 / 鷲の翼(eagle-wing)像 5 例,無動‐筋強 映すると考えられている。これまでのところ,PD サブタ 剛型 PD 患者:それぞれ 9 例 /50 例 /3 例 /6 例,混合型 イプが異なればドパミン作動性ニューロンの脱落パター (equivalent type)患者:それぞれ 2 例 /20 例 /5 例 /4 例〕 。 ンも異なるという所見は,神経病理学的モデルでのみ報 振戦優位型サブタイプでは,半定量的解析〔特異的結合 告されており 6,23,ヒトの生体でもこれが観察されるかど の比(specific ratio; SR) 〕および自動三次元解析(BRASS) うかは不明とされてきた。 のいずれにおいても,最大障害側の同側および対側の尾 Jellinger 6 は,神経病理学的所見に基づき,線条体構造 状核・被殻で無動‐筋強剛型サブタイプに比べて有意に への黒質ドパミン作動性ニューロンの投射が PD サブタ 高いドパミン取り込みが観察された(p < 0.05,Figure 2 イプにより異なるというモデルを構築した。無動‐筋強 参照) 。これらのサンプルの年齢,罹病期間,疾患重症度 剛型では,背側被殻に投射する黒質緻密部の腹外側部の (HY 分類と UPDRS スコア) ,L—ドパ換算用量をマッチさ 細胞脱落がより高度である。一方,振戦優位型の場合, せた場合(23/23 例) ,ドパミン取り込みの有意差は観察 ニューロンの脱落は,黒質緻密部の外側部(尾状核およ されなくなった(p > 0.05) 。ただし,取り込み率は依然 び前部被殻に投射)および赤核後部(背外側線条体およ として振戦優位型サブタイプのほうが高かった。 び腹内側視床に投射)よりも,内側部でより高度である。 視覚的解析では,線条体の鷲の翼(eagle-wing)像と振 すなわち,振戦優位型 PD 患者では,尾状核および外側 戦優位型 PD 患者,ならびに卵形(egg-shaped)像と無動 被殻に特有のドパミン消失が認められ,これが線条体の ‐筋強剛型 PD 患者との間に,明らかな関連性が認められ 狭小化として現れて,FP-CIT SPECT では鷲の翼(eagle- た(Figure 3 および 4 参照) 。ブートストラップ法による wing)形のドパミン取り込みが生じると考えられる (Figure 統計解析では,両群間の有意差が認められた(p < 0.05) 。 4a 参照) 。同様に,無動‐筋強剛型 PD 患者では,背側 被殻へのドパミン作動性投射路の変性により,FP-CIT 考 察 SPECT では卵形(egg-shaped)像が生じるはずである (Figure 4b 参照) 。 FP-CIT SPECT を用いれば,PD 患者,健常被験者,本 態性振戦患者を高い精度で鑑別できる。一方,現在まで 半定量的解析を上回る視覚的解析所見の利点 のところ,FP-CIT 取り込みの違いによって PD サブタイ 今回のデータから,ドパミン作動性ニューロンの変性 プを振戦優位型または無動‐筋強剛型に確実に区別でき パターンの違いは視覚的に描出することが可能であるこ るか否かについては,議論の余地がある 。本研究では, とが示唆される。これとは対照的に,現在までのところ, 年齢,罹病期間,疾患重症度,L—ドパ換算用量を一致さ FP-CIT 取り込み解析用の標準ソフトウェアアルゴリズム せた無動‐筋強剛型 PD 患者群と振戦優位型 PD 患者群 では,この異なる FP-CIT 取り込みパターンを描出するこ を検討したところ,FP-CIT SPECT による標準化半定量的 とができない。これは,ROI は尾状核と被殻を覆うよう 解析では,有意差が認められなかった。これに対し,視 に設定されるが,被殻の内側部および / または外側部に 覚的解析では, 振戦優位型 PD 患者〔 (鷲の翼(eagle-wing) 局在する異なる被殻変性をサブ解析できる設定にはなっ 像〕と無動‐筋強剛型 PD 患者〔卵形(egg-shaped)像〕 ていないためである。特異的結合は,尾状核または被殻 において,線条体取り込み形状パターンの有意な違いが のいずれかにおける特異的取り込みを反映し,被殻内部 認められた。このデータは,FP-CIT SPECT の視覚的検査 におけるより軽微なドパミン供給路の喪失を考慮せずに, 7 15 #MD5-1.indb 15 11.7.14 2:24:55 PM 無動‐筋強剛型および振戦優位型パーキンソン病患者では FP-CIT SPECT 所見が異なる Matched group Non-matched group 4,000 4,000 33 33 3,000 SR contralateral Caudate 2,000 2,000 1,000 1,000 0,000 0,000 2,500 2,500 2,000 2,000 BRASS contralateral Caudate BRASS contralateral Caudate SR contralateral Caudate 3,000 1,500 1,000 0,500 1,500 1,000 0,500 0,000 0,000 2,500 2,500 32 32 33 33 2,000 27 38 1,500 1,000 SR contralateral Putamen SR contralateral Putamen 2,000 27 38 1,500 1,000 0,500 0,500 0,000 0,000 2,000 2,000 33 33 38 38 32 BRASS contralateral Putamen BRASS contralateral Putamen 32 1,500 1,000 0,500 1,500 1,000 0,500 0,000 0,000 Tremordominant Akinetic -rigid Tremordominant Akinetic -rigid Figure 2 振戦優位型サブタイプと無動‐筋強剛型サブタイプにおける手動関心領域解析(SR)および自動三次元解析(BRASS)による対側 (臨床的患側に対して)線条体 FP-CIT 取り込みの平均値,標準偏差,外れ値。条件をマッチさせたサンプル(振戦優位型 23 例 / 無動‐筋強 剛型 23 例,右)とマッチさせないサンプル(振戦優位型 23 例 / 無動‐筋強剛型 68 例,左)を検討。* サブタイプ間で有意差あり(p < 0.05) 。 患側と同側の線条体 FP-CIT 取り込みの結果は Supporting Information を参照されたい。 [カラーの図は wileyonlinelibrary.com のオンライン版で 閲覧可能] 。 16 #MD5-1.indb 16 11.7.14 2:24:56 PM C. Eggers et al. Visual type Burst striatum Egg-Shape Mixed Eagle wing Normal Atypic 80,0% は臨床的価値があまりないように思えるかもしれない。 しかし,日常臨床において PD 診断基準は常に満足でき るものとは限らず,例えば FP-CIT SPECT による追加的 な診断情報は,経済的な見地からみても,その後の治療 60,0% Percentage 法を決定する際に有用であろう 25。本研究は,FP-CIT SPECT の視覚的解析により,PD の臨床サブタイプを高 い信頼性で鑑別可能であることを示している。上述のよ 40,0% うに,サブタイプが異なれば疾患経過や予後も異なる(例 えば,振戦優位型 PD 患者は認知症の発現頻度は低いも 20,0% のの,治療はより困難である)3,5。今後の前向き試験で 本結果が確認されれば,画像データの追加情報は,その 後の戦略的な治療計画立案を改善し,各患者に今後の見 0,0% Tremor-dominant Akinetic-rigid PD subtype 通しをより正確に伝えるための一助となると考えられる。 (a) また,今回のデータがもつ別の重要な側面として,疾患 Visual type Burst striatum Egg-Shape Mixed Eagle wing Normal Atypic 80,0% Percentage 60,0% 修飾療法(例えば神経保護療法)の評価を目的とした臨 床試験では,PD サブタイプの適切な区別が可能となるで あろう。 視覚的解析のバイアスとなる経験不足と 主観的分類 本研究では,各患者の臨床診断を伏せた状態で,核医 40,0% 学専門医 2 名がそれぞれ単独で,各データセットから得 られた横断像を検討した。自動解析ではないため,視覚 20,0% 的解析による分類では,過大評価や過小評価によるバイ アスの発生が当然想定される。原則上,視覚的解析を制 0,0% Tremor-dominant Akinetic-rigid PD subtype (b) Figure 3 a:振戦優位型サブタイプ(23 例)と無動‐筋強剛型サ ブタイプ(68 例) (非条件をマッチさせたペア)における視覚的評 価による線条体形状の割合。 * サブタイプ間で有意差あり (p<0.05) 。 b:振戦優位型サブタイプと無動‐筋強剛型サブタイプ(条件をマッ チさせたペア)における視覚的評価による線条体形状の割合。* サ ブタイプ間で有意差あり(p < 0.05) 。 限する要因としては,分類不可能なデータセットや評価 者の経験不足が挙げられる。評価者の数を増やしてその 合意に基づく診断や系統的教育を行ったり,正常所見お よび症例の所見に関する公開(オンライン)アトラスを 使用したりすることで,診断時の不確定要素を軽減でき るであろう。また,より客観的な形状解析を行うには, 例えば Staff ら 21 が報告しているような形状分類の自動ア ルゴリズムが,視覚的診断の客観性を高める上で重要な 手段となるであろう。 主に後部-前部の変性機構を提示する。我々は,局所結 合係数の差を求めるボクセル単位の解析手法も検討した が,ボクセル・ベース・モルフォメトリー(VBM)は古 典的な ROI 法に対して優越性がないため 24,その使用は 断念した。 結 論 本研究の結果から,無動‐筋強剛型および振戦優位型 PD 患者において,FP-CIT SPECT 画像の視覚的解析によ る線条体形状と PD の臨床サブタイプとの間には,明瞭 臨床的意義 一見すると,視覚的解析による PD サブタイプ分類に かつ統計学的に有意な関連があることが示された。これ らの結果は,無動‐筋強剛型患者では背側被殻に向かう 17 #MD5-1.indb 17 11.7.14 2:24:57 PM 無動‐筋強剛型および振戦優位型パーキンソン病患者では FP-CIT SPECT 所見が異なる (a) reduced striatonigral projections (b) A N A L Y S I S O F F P - C I T axial images from each of the data sets. Due to a missreduced striatonigral ing automatized analysis, it is reasonable projections to assume a bias for over- or undergrading in the classification of the visual analysis. In principle, limitations of the visual analysis are nonclassifiable data sets or unexperienced rater. With a larger number of raters and their consensus diagnosis or systematic teaching and published (online) atlases of normals and cases, it would be possible to diminish diagnostic uncertainty. Additionally, for a more objective analysis of shape, an automatic algorithm for the classification of shapes, e.g., as described by Staff et al.,21 would deliver an reduced projections important instrument to objectify the visual diagnosis. of the retrorubral field よび尾状核に向かうドパミン作動性投射がそれぞれ減少 しているという in vivo の神経病理学的モデルと一致する。 これらの後向き評価結果を確認するためには,本分類法 の妥当性を評価する前向き試験が必須である。 統計解析における有益な支援に関しEsther Florin に感謝する。 Acknowledgments: We thank Esther Florin for her valuable support in the statistical analysis. REFERENCES Benamer TS, Pa tion of parkinso of [123I]-FP-CIT Mov Disord 200 9. Breit S, Reimold date PET in pat J Neural Transm 10. Brooks DJ, Play ruption of the PET study. Neu 11. Kaufman MJ, M sites associated eased striatum. 12. Niznik HB, Fog porter is absent date nucleus. J N 13. Hughes AJ, Da diagnosis of idi study of 100 181–184. 14. Hoehn MM, Ya tality. Neurolog 15. Fahn S. Elton R ease Rating Scal mation, 1987; V 16. Lewis SJ, Foltyn son’s disease in approach. J Neu 17. Laruelle M, Bal dopamine and s cological charac Synapse 1993;13 18. Koch W, Radau optimized softw ent evaluation Med 2005;46:11 19. Tatsch K, Asenb of Nuclear Med sion SPET using Eur J Nucl Med 20. Morton RJ, Gu methods of Dat 26:1139–1146. 21. Staff RT, Ahear omega-fluoropr nortropane sing in the assessmen Med Commun 2 22. Efron B, Tibshir Chapman & Ha Young AB, Penney JB. Biochemical and functional organization of the basal ganglia. In: Parkinsons’s disease and movement disorders (4th ed.). Jankovic J and Tolosa E (eds.). Philadelphia, PA: Lippincott Williams and Wilkins. 2002; pp 1–10. 2. Timmermann L, Gross J, Dirks M, et al. The cerebral oscillatory network of parkinsonian resting tremor. Brain 2003;126:199–212. 3. Rajput AH, Voll A, Rajput ML, et al. Course in Parkinson disease subtypes: a 39-year clinicopathologic study. Neurology 2009;73: 206–212. 4. Jankovic J, Kapadia AS. Functional decline in Parkinson disease. Arch Neurol 2001;58:1611–1615. 18 5. #MD5-1.indb 18 References 1. I 8. Conclusions This study demonstrates a clear, statistically significant association of visually analyzed shapes of the striatum in FP-CIT SPECT and clinical PD subtype for akinetic-rigid and tremor-dominant patients. These results are consistent with neuropathological models Figure 4 a,b:線条体における鷲の翼(eagle-wing)像と卵形(egg-shaped)像の例。無動‐筋強剛型 PD の 74 歳男性患者(a)と振戦優位 for a reduced dopaminergic projection to the dorsal 型 PD の 71 歳女性患者(b) 。各画像の隣に,Jellinger らによる神経病理学的モデルも併せて図示した。 putamen in akinetic-rigid patients and the lateral putamen and caudate nucleus in tremor-dominant PD patients in vivo. To confirm these retrospective evaluated results, there is a clear need for a prospective ドパミン作動性投射が,振戦優位型患者では外側被殻お study aimed to validate 謝 辞 this system of classification. S P E C T 23. Rajput AH, Sitt and Parkinson m Marras C, Rochon P, Lang AE. Predicting motor decline and disrelation. Neurol ability in Parkinson disease: a systematic review. Arch Neurol 11.7.14 2:24:59 PM 2002;59:1724–1728. 24. Kas A, Payoux study aimed this system of classification. tionally, fortoa validate more objective analysis of shape, an automatic algorithm for the classification of shapes, Acknowledgments: We thank Esther Florin for her valuable support in the statistical e.g., asanalysis. described by Staff et al.,21 would deliver an important instrument to objectify the visual diagnosis. 1. References Conclusions Young AB, Penney JB. Biochemical and functional organization of the basal ganglia. In: Parkinsons’s disease and movement disorders (4th study ed.). Jankovic J and TolosaaE clear, (eds.). Philadelphia, PA:signifiLippinThis demonstrates statistically cott Williams and Wilkins. 2002; pp 1–10. cant association of visually analyzed shapes of the 2. Timmermann L, Gross J, Dirks M, et al. The cerebral oscillatory striatum inofFP-CIT SPECT clinical PD subtype for network parkinsonian restingand tremor. Brain 2003;126:199–212. akinetic-rigid and tremor-dominant These 3. Rajput AH, Voll A, Rajput ML, et al. Course patients. in Parkinson disease subtypes: aconsistent 39-year clinicopathologic study. Neurology 2009;73: results are with neuropathological models 206–212. for a reduced dopaminergic projection to the dorsal 4. Jankovic J, Kapadia AS. Functional decline in Parkinson disease. putamen in akinetic-rigid patients and the lateral putaArch Neurol 2001;58:1611–1615. men and C,caudate in tremor-dominant PD 5. Marras Rochon P, nucleus Lang AE. Predicting motor decline and disability in in vivo. Parkinson disease: a systematic review. Arch Neurol patients To confirm these retrospective eval2002;59:1724–1728. uated results, there is a clear need for a prospective 6. Jellinger KA. Post mortem studies in Parkinson’s disease—is it posstudy aimed to brain validate system of classification. sible to detect areas this for specific symptoms?J Neural Transm L Y S I S O F Suppl 1999;56:1–29. Acknowledgments: We thank Esther Florin for her valuable support in the 7. Spiegel J, Hellwig D, Samnick S, et al. Striatal FP-CIT uptake difstatistical analysis. F P - C I T fers S PinE the C Tsubtypes I N ofP early A R Parkinson’s K I N S O disease. N ’ S J DNeural I S E Transm A S E 2007;114:331–335. s. Due to a missable to assume a classification of ations of the vissets or unexperraters and their aching and pubd cases, it would ncertainty. Addisis of shape, an ation of shapes, would deliver an visual diagnosis. atistically signifid shapes of the l PD subtype for patients. These hological models on to the dorsal the lateral putaor-dominant PD trospective evalor a prospective classification. 8. 15. Fahn S. Elton RL, motUDC, editors. The Unified Parkinson’s disease Rating Scale. Florham Park (NJ): McMillan Healthcare Information, 1987; Vol. 2. 16. Lewis SJ, Foltynie T, Blackwell AD, et al. Heterogeneity of Parkinson’s disease in the early clinical stages using a data driven approach. J Neurol Neurosurg Psychiatry 2005;76:343–348. 17. Laruelle M, Baldwin RM, Malison RT, et al. SPECT imaging of dopamine and serotonin transporters with [123I]beta-CIT: pharmacological characterization of brain uptake in nonhuman primates. Synapse 1993;13:295–309. 18. Koch W, Radau PE, Hamann C, Tatsch K. Clinical testing of an optimized software solution for an automated, observer-independent evaluation of dopamine transporter SPECT studies. J Nucl Med 2005;46:1109–1118. 19. Tatsch K, Asenbaum S, Bartenstein P, et al. European Association of Nuclear Medicine procedure guidelines for brain neurotransmission SPET using (123)I-labelled dopamine D(2) transporter ligands. Eur J Nucl Med Mol Imaging 2002;29:BP30–BP35. valuable support in the tional organization of d movement disorders ladelphia, PA: Lippin- he cerebral oscillatory n 2003;126:199–212. References Benamer TS, Patterson J, Grosset DG, et al. Accurate differentiaof parkinsonism and essential tremor using visual assessmentof 1. tion Young AB, Penney JB. Biochemical and123 functional organization ofthe[123 I]-FP-CIT imaging: the [ I]-FP-CIT studydisorders group. basal ganglia.SPECT In: Parkinsons’s disease and movement Mov 2000;15:503–510. (4th Disord ed.). Jankovic J and Tolosa E (eds.). Philadelphia, PA: Lippincott Williams andM,Wilkins. 9. Breit S, Reimold Reischl2002; G, et pp al. 1–10. [(11)C]d-threo-methylpheniPET in patients withJ,Parkinson’s andcerebral essential tremor. 2. date Timmermann L, Gross Dirks M, etdisease al. The oscillatory J network Neural Transm 2006;113:187–193. of parkinsonian resting tremor. Brain 2003;126:199–212. 10.3. Brooks Ibanez Isolated tremor and disRajput DJ, AH,Playford Voll A, ED, Rajput ML,V, et et al. al. Course in Parkinson disease ruption of athe nigrostriatal dopaminergic system: an 18F-dopa subtypes: 39-year clinicopathologic study. Neurology 2009;73: PET study. Neurology 1992;42:1554–1560. 206–212. 11.4. Kaufman Madras AS. BK. Functional Severe depletion recognition Jankovic MJ, J, Kapadia declineofincocaine Parkinson disease. sites with the dopamine transporter in Parkinson’s-disArchassociated Neurol 2001;58:1611–1615. eased striatum. Synapse 1991;9:43–49. 5. Marras C, Rochon P, Lang AE. Predicting motor decline and dis12. Niznik Fogel EF, Fassos P. The dopamine transability HB, in Parkinson disease:FF, a Seeman systematic review. Arch Neurol porter is absent in parkinsonian putamen and reduced in the cau2002;59:1724–1728. date nucleus. J Neurochem 1991;56:192–198. 6. Jellinger KA. Post mortem studies in Parkinson’s disease—is it pos13. Hughes Daniel Kilford L, Leessymptoms?J AJ. Accuracy of clinical sible to AJ, detect brainSE, areas for specific Neural Transm diagnosis of idiopathic Parkinson’s disease: a clinico-pathological Suppl 1999;56:1–29. study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55: 7. 181–184. Spiegel J, Hellwig D, Samnick S, et al. Striatal FP-CIT uptake differs in the subtypes of early Parkinson’s disease. J Neural Transm 14. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mor2007;114:331–335. tality. Neurology 1967;17:427–442. 20. Morton RJ, Guy MJ, Clauss R, et al. Comparison of different methods of DatSCAN quantification. Nucl Med Commun 2005; 26:1139–1146. 21. Staff RT, Ahearn TS, Wilson K, et al. Shape analysis of 123I-Nomega-fluoropropyl-2-beta-carbomethoxy-3beta-(4-iodophenyl) nortropane single-photon emission computed tomography images in the assessment of patients with parkinsonian syndromes. Nucl Med Commun 2009;30:194–201. 22. Efron B, Tibshirani RJ. An introduction to the bootstrap. London: Chapman & Hall; 1993. 23. Rajput AH, Sitte HH, Rajput A, et al. Globus pallidus dopamine and Parkinson motor subtypes: clinical and brain biochemical correlation. Neurology 2008;70:1403–1410. 24. Kas A, Payoux P, Habert MO, et al. Validation of a standardized normalization template for statistical parametric mapping analysis of 123I-FP-CIT images. J Nucl Med 2007;48:1459–1467. 25. Van Laere K, Everaert L, Annemans L, et al. The cost effectiveness of 123I-FP-CIT SPECT imaging in patients with an uncertain clinical diagnosis of parkinsonism. Eur J Nucl Med Mol Imaging 2008;35:1367–1376. e in Parkinson disease Neurology 2009;73: in Parkinson disease. motor decline and disreview. Arch Neurol on’s disease—is it posoms?J Neural Transm al FP-CIT uptake difase. J Neural Transm optimized software solution for an automated, observer-independeased striatum. Synapse 1991;9:43–49. ent evaluation of dopamine transporter SPECT studies. J Nucl 12. Med Niznik HB, Fogel EF, Fassos FF, Seeman P. The dopamine trans2005;46:1109–1118. porter is absent in parkinsonian putamen and reduced in the cau19. Tatsch K, Asenbaum S, Bartenstein P, et al. European Association date nucleus. J Neurochem 1991;56:192–198. of Nuclear Medicine procedure guidelines for brain neurotransmis13. sion Hughes AJ, Daniel SE, Kilford L, Lees D(2) AJ. Accuracy clinical SPET using (123)I-labelled dopamine transporterofligands. diagnosis idiopathic Parkinson’s disease: a clinico-pathological Eur J Nucl of Med Mol Imaging 2002;29:BP30–BP35. study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55: 20. Morton RJ, Guy MJ, Clauss R, et al. Comparison of different 181–184. Eggers 2005; et al. methods of DatSCAN quantification. Nucl Med C. Commun 14. 26:1139–1146. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967;17:427–442. 21. Staff RT, Ahearn TS, Wilson K, et al. Shape analysis of 123I-N15. omega-fluoropropyl-2-beta-carbomethoxy-3beta-(4-iodophenyl) Fahn S. Elton RL, motUDC, editors. The Unified Parkinson’s disease Ratingsingle-photon Scale. Florham Park (NJ): McMillan Healthcareimages Infornortropane emission computed tomography 1987; Vol.of2.patients with parkinsonian syndromes. Nucl inmation, the assessment Commun 2009;30:194–201. 16. Med Lewis SJ, Foltynie T, Blackwell AD, et al. Heterogeneity of Parkinson’s B,disease in the clinical stages a data driven 22. Efron Tibshirani RJ. early An introduction to theusing bootstrap. London: approach.&J Neurol Neurosurg Psychiatry 2005;76:343–348. Chapman Hall; 1993. 17. Rajput Laruelle M,Sitte Baldwin Malison RT,Globus et al. pallidus SPECT imaging of 23. AH, HH, RM, Rajput A, et al. dopamine 123 I]beta-CIT: pharmadopamine and motor serotonin transporters and Parkinson subtypes: clinicalwith and [brain biochemical corcologicalNeurology characterization of brain uptake in nonhuman primates. relation. 2008;70:1403–1410. Synapse 1993;13:295–309. 24. Kas A, Payoux P, Habert MO, et al. Validation of a standardized 18. normalization Koch W, Radau PE, Hamann C, Tatsch K. Clinical testing of an template for statistical parametric mapping analysis 123 optimized software solution an2007;48:1459–1467. automated, observer-independI-FP-CIT images. J Nucl for Med of ent evaluation of dopamine transporter SPECT studies. J Nucl 25. Van K, Everaert L, Annemans L, et al. The cost effectiveness MedLaere 2005;46:1109–1118. of 123I-FP-CIT SPECT imaging in patients with an uncertain clini19. cal Tatsch K, Asenbaum S, Bartenstein al. European diagnosis of parkinsonism. Eur P,J etNucl Med MolAssociation Imaging of Nuclear Medicine procedure guidelines for brain neurotransmis2008;35:1367–1376. sion SPET using (123)I-labelled dopamine D(2) transporter ligands. Eur J Nucl Med Mol Imaging 2002;29:BP30–BP35. 20. Morton RJ, Guy MJ, Clauss R, et al. Comparison of different methods of DatSCAN quantification. Nucl Med Commun 2005; 26:1139–1146. 21. Staff RT, Ahearn TS, Wilson K, et al. Shape analysis of 123I-Nomega-fluoropropyl-2-beta-carbomethoxy-3beta-(4-iodophenyl) nortropane single-photon emission computed tomography images in the assessment of patients with parkinsonian syndromes. Nucl Med Commun 2009;30:194–201. 22. Efron B, Tibshirani RJ. An introduction to the bootstrap. London: Chapman & Hall; 1993. 23. Rajput AH, Sitte HH, Rajput A, et al. Globus pallidus dopamine and Parkinson motor subtypes: clinical and brain biochemical correlation. Neurology 2008;70:1403–1410. 24. Kas A, Payoux P, Habert MO, et al. Validation of a standardized normalization template for statistical parametric mapping analysis Disorders, Vol. 26, No. 3, 2011 423 J Nucl Med 2007;48:1459–1467. of 123I-FP-CIT images.Movement 25. Van Laere K, Everaert L, Annemans L, et al. The cost effectiveness of 123I-FP-CIT SPECT imaging in patients with an uncertain clinical diagnosis of parkinsonism. Eur J Nucl Med Mol Imaging 2008;35:1367–1376. Movement Disorders, Vol. 26, No. 3, 2011 423 19 #MD5-1.indb 19 11.7.14 2:25:00 PM 早期パーキンソン病における低用量プラミペキソールの 1 日 2 回投与:無作為化プラセボ対照試験 Twice-Daily, Low-Dose Pramipexole in Early Parkinson’s Disease: A Randomized, Placebo-Controlled Trial * The Parkinson Study Group PramiBID Investigators * University of Rochester Medical Center, Rochester, New York, USA 本研究の目的は,ドパミン作動性薬剤の投与を受けてい 動作) ,Part Ⅲ (運動機能)の合計スコアの試験参加時 ない早期パーキンソン病(Parkinson’ s disease; PD) から 12 週間後時点までの変化とした。すべての実薬投 患者 311 例を対象とした無作為化二重盲検プラセボ対 与群で抗パーキンソン効果はほぼ同じであり,プラセボ 照試験において,早期 PD における低用量プラミペキ 群と比較してそれぞれ UPDRS スコア 4 ~ 5 ポイント ソール 1 日 2 回(bid)投与の安全性および有効性につ 。実薬投与群では, の低下が認められた(p < 0.0001) いて,標準的な 1 日 3 回(tid)投与と比較することで プラセボ群に比べ,傾眠,疲労,悪心,便秘,末梢性浮 ある。被験者をプラミペキソール 0.5 mg bid 群,0.75 腫が多くみられたが,これらの発現率に投与量による差 mg bid 群,0.5 mg tid 群または対応するプラセボ群に は認められなかった。今回の固定用量無作為化試験で 無作為に割り付け,12 週間投与した。盲検性を維持す は,早期 PD 患者への 12 週間の投与において,プラミ るために,すべての被験者に 1 日 3 回の投与を行い, ペ キソール 1 日 2 回投 与( 総 1 日投 与 量 1.0 ~ 1.5 必要に応じてプラセボを投与した。主要評価項目は, mg)の有効性および忍容性は 0.5 mg 1 日 3 回投与と Unified Parkinson’ s Disease Rating Scale(UPDRS) 同等であった。 Part Ⅰ (精神機能,行動および気分) ,Part Ⅱ (日常生活 Movement Disorders, Vol. 26, No. 1, 2011, pp. 37–44 Adjusted Mean Change in Total UPDRS Key Word 臨床試験,パーキンソン病,プラミペキソール 1.0 0.0 -1.0 -2.0 -3.0 -4.0 -5.0 -6.0 -7.0 -1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Week Placebo Pramipexole 0.5 bid Pramipexole 0.5 tid Pramipexole 0.75 bid Figure 2 投与群別に示した UPDRS 合計スコアの経時的な補正後平 均変化。エラーバーは平均値の 1 標準誤差を示す。 20 #MD5-1.indb 20 11.7.14 2:25:02 PM パーキンソン病患者のニューロン新生に対する薬物療法の効果 The Effect of Drug Treatment on Neurogenesis in Parkinson’s Disease *, ** Sean S. O’Sullivan, PhD, MRCPI, Mary Johnson, David R. Williams, PhD, Tamas Revesz, FRCPath, Janice L. Holton, FRCPath, Andrew J. Lees, MD, and Elaine K. Perry, PhD * Reta Lila Weston Institute of Neurological Studies, University College London, London, United Kingdom Queen Square Brain Bank for Neurological Disorders and Institute of Neurology, University College London, London, United Kingdom ** 近年,アルツハイマー病やパーキンソン病(Parkinson’ s ぼす臨床的因子を特定した。罹病期間と脳室下帯の disease; PD)といった神経変性疾患の病気の進行に Musashi 1 染色性との間に,負の相関が認められた。 ニューロン新生の異常が寄与している可能性が指摘さ そ の 一 方 で,生 涯 の レ ボド パ(L—ド パ ) 投 与 量 と れ,関心を集めている。本研究では,認知症のない PD Musashi 1 染色性との間には正の相関が認められた。 患者において,一般に使用される PD 治療法が神経幹細 我々の知見から,L—ドパの慢性使用は,PD 患者の脳室 胞活性に及ぼす効果を検討した。認知症のない PD 患者 下帯における神経幹細胞数に対し,有益な影響を及ぼ 32 例の,脳室下帯および上衣層細胞を含む剖検脳組織 すことが示唆される。この知見は,神経変性疾患患者の を 入 手 し た。 神 経 幹 細 胞 活 性 は,RNA 結 合 蛋 白 神経保護に関する今後の研究に役立つものと考えられ Musashi 1の免疫組織化学染色により評価した。その後, る。 回帰分析を用い,神経幹細胞活性に独立して影響を及 Movement Disorders, Vol. 26, No. 1, 2011, pp. 45–50 Key Word パーキンソン病,ニューロン新生,神経保護,幹細胞 O ’ S U L L I V A N E T A L . Table1.1 患者の臨床および病理データ TABLE Patient clinical and pathologic data Total PD Group Number Gender, M:F Age PD onset (yr) PD duration (yr) Age death (yr) Duration of L-dopa treatment (yr) Maximum L-dopa dose (mg/d) Lifetime L-dopa (g) No. PAM used in life Duration of PAM use (yr) No. any anticholinergic used in life Duration of any anticholinergic use (yr) No. DA used in life Duration of DA use (yr), in 22 PD patients Interval between stopping DA and death (years), in 22 PD patients EL Musashi1 positivity (% area) SVZ Musashi1 positivity (% area) LB score BþB Alzheimer pathology grade Postmortem delay (hr) Figure 1 脳室下帯(SVZ)および上衣層細胞(EL)の Musashi 1 染色切片。 (A)累積生涯 L—ドパ投与量が低い患者, (B)累積生涯 L—ドパ投与量が高い患者。 (A)および(B) :倍率 10 倍,挿入図= 倍率 40 倍,バー= 100 μ m #MD5-1.indb 21 32 17:15 64.0 6 11.2 15.1 6 7.8 79.1 6 7.0 11.6 6 8.2 825.9 6 475 2,806 6 3,279 0.5 6 0.7 3.0 6 7.3 1.3 6 1.5 6.1 6 8.8 1.3 6 1.1 4.0 6 5.3 0.8 6 1.7 49.2 3.6 6.5 1.1 37.1 6 6 6 6 6 15.8 2.7 2.2 0.9 22.8 Values are given as mean 6 SD. 値は平均値± SD。 DA, Dopamine agonist; LB, Lewy Body; BþB, Braak and Braak; EL, DA =ドパミンアゴニスト,LB = Lewy 小体,B+B =with Braak and Ependymal cell layer; SVZ, Subventricular zone; PAM, Drugs primary antimuscarinic effects. Braak,EL =上衣細胞層,SVZ =脳室下帯,PAM =一次性の抗ム ¼ 0.057). A seco accounted for d showed a trend shi1 staining a SVZ ¼ 0.32, P ¼ 0.05). Multip ease duration (P 0.013) independ area of Musash standardized coe ciated with Mu time L-dopa (Bet positively associ fidence intervals lifetime L-dopa that of the PD regression analy that independen positivity. This study inv PD medications cohort of nonde スカリン作用をもつ薬剤 positive associat not correlate with Musashi1 staining in this study or ber of prolifera in previous studies by our group (unpublished data). 21EL. Medication All patients had used L-dopa, and 22 patients (69%) effects did not in used dopamine agonists during their PD course. FourIn rats, dopa teen patients (44%) had used antidepressants at some neural stem cell point, four having been on more than one type of receptors with 11.7.14 2:25:03 PM AAV2-neurturin 遺伝子治療(CERE-120)の生物活性: パーキンソン病患者と非ヒト霊長類の脳における相違点 Bioactivity of AAV2-Neurturin Gene Therapy (CERE-120): Differences Between Parkinson’s Disease and Nonhuman Primate Brains * Raymond T. Bartus, PhD, Christopher D. Herzog, PhD, Yaping Chu, PhD, Alistair Wilson, BS, Lamar Brown, BS, Joao Siffert, MD, Eugene M. Johnson, Jr., PhD, C. Warren Olanow, MD, Elliott J. Mufson, PhD, and Jeffrey H. Kordower, PhD * Ceregene Inc., San Diego, California, USA 背景:AAV2-neurturin(CERE-120)は,パーキンソ 者の線条体では,neurturin の発現に伴い,わずかなチ ン病(Parkinson’ s disease; PD)患者の変性した黒質 ロシン水酸化酵素誘導が散発的に認められたが,黒質 線条体ニューロンの回復・保護を目的に,神経栄養因子 緻密部ではみられなかった。霊長類では,黒質線条体 neurturin を線条体に送達するよう設計されている。一 ニューロン全体にわたり,neurturin により強固なチロ 般的な仮説として,neurturin のような神経栄養因子は シン水酸化酵素誘導が生じていた。 線条体での発現後,変性した神経終末から黒質緻密部 考察:これらのデータから,遺伝子治療により PD 患者 の神経細胞体へと輸送されると考えられている。 の脳深部で神経栄養因子の発現を高めることができる 方法:本研究では免疫組織化学を用い,PD 患者の脳に こと,また,小規模ではあるものの明確な変性ニューロ おける AAV2-neurturin の生物活性を,同様に処置した ンの機能強化が誘導可能であることを示すエビデンス 非ヒト霊長類と比較してこの概念を検証した。 が初めて得られた。また,これらのデータは,進行期 結果:すべての PD 患者において,標的とした線条体に PD 患者の黒質線条体ニューロンの障害についても重要 neurturin の免疫染色が認められた〔被殻の約 15%(平 な知見を提供している。すなわち,軸索輸送の高度な障 均値,体積比)で発現が認められた〕 。これと同様の 害により,神経細胞体に送達される neurturin が制限さ neurturin 発現が若齢サル,高齢サル,PD モデルのサ れることで,AAV2-neurturin の生物活性が低下してい ルで認められた。しかし,黒質緻密部の神経細胞体にお ることが示唆される。これらを踏まえ,今後,神経栄養 いては,PD 患者で neurturin 発現の所見がほとんど認 因子の投与による神経変性疾患の治療においては,最 められなかった一方,サルでは全例で黒質の高度の 大限の効果を得るため,変性ニューロンの終末部および neurturin 発現を示す十分な所見が観察された。PD 患 細胞体の両方を標的とする必要がある。 Movement Disorders, Vol. 26, No. 1, 2011, pp. 27–36 Key Word 神経栄養因子,トランスレーショナル・リサーチ,軸索輸送,神経変性,神経修復 Figure 2 PD 患者の黒質緻密部におけるメラニン陽性ニューロンおよび neurturin 免疫染色所見の例。黒質においてメラニン陽性のドパミン 作動性周核体クラスターは多数観察されたが(A:低倍率,B:高倍率) ,黒質ニューロンにおける neurturin 染色所見はわずかしかみられなかっ た(C:高倍率) 。パネル A および B は,AAV2-neurturin の被殻内送達後,全般的に,黒質線条体ニューロンが neurturin を黒質周核体へ逆行 性輸送できないことを示している。一方,パネル C は,neurturin の逆行性輸送が行われ,黒質に neurturin が認められたまれな例を示している。 スケールバーはパネル A で 220 μ m,パネル B および C で 22 μ m。 22 #MD5-1.indb 22 11.7.14 2:25:04 PM Abstract Figure 3 線条体に低用量の AAV2-neurturin(意図的に線条体体積の 5.6%および 1.8%のみに neurturin を 発現させた)を投与した若齢サルの neurturin 染色所見(それぞれパネル A および B) 。各サルについて neurturin 発現が最大であった冠状断面を示す。線条体の neurturin 発現範囲はそれほど大きくないものの, AAV2-neurturin 投与のわずか 1 ヵ月後,黒質で neurturin が明確に認められた(パネル C および D) 。パネ ル A および B のスケールバーは 2 mm。パネル C および D のスケールバーは低倍率写真で 1 mm,高倍率 写真で 400 μ m。 Striatal Coverage (%): Aged Monkey #0201 4% Aged Monkey #0202 19% Aged Monkey #0204 25% Striatal NRTN Nigral NRTN Figure 4 線条体に AAV2-neurturin(NRTN)を投与した高齢サル 3 匹の neurturin 所見。線条体 の neurturin 発現体積がわずか 4%であった例を含め,線条体での neurturin 発現後(上段パネル) , 3 匹すべての黒質で neurturin 陽性細胞が豊富に認められた(下段パネル) 。スケールバーは上段 パネルで 2.0 mm,下段パネルで 0.2 mm。 23 #MD5-1.indb 23 11.7.14 2:25:05 PM パーキンソン病の臨床サブタイプ Clinical Subtypes of Parkinson’s Disease * Stephanie M. van Rooden, MSc, Fabrice Colas, PhD, Pablo Martínez-Martín, MD, Martine Visser, PhD, Dagmar Verbaan, PhD, Johan Marinus, PhD, Ray K. Chaudhuri, MD, Joost N. Kok, PhD, and Jacobus J. van Hilten, MD * Department of Neurology, Leiden University Medical Centre, Leiden, The Netherlands パーキンソン病(Parkinson’ s disease; PD)は臨床的 らのサブタイプは,非ドパミン系の障害による症状と運 に不均一な疾患であり,複数のサブタイプが存在すると 動合併症の重症度の差によって,主に特徴付けることが 考えられる。各サブタイプは,その基礎にある別々の病 できた。 「サブタイプ 1」では,すべての臨床領域で軽 因を反映すると考えられ,サブタイプの同定により,今 度の臨床症状がみられた。 「サブタイプ 2」は,重度の 後の遺伝学的研究および薬物療法研究が促進されるで 運動合併症を主な特徴とした。 「サブタイプ 3」は,非 あろう。本研究の目的は,PD の様々な運動症状および ドパミン系の障害による症状が主であり,顕著な運動合 非運動症状を対象にデータ主導型分析を行い,サブタ 併症はなかった。 「サブタイプ 4」では,すべての臨床 イプを同定することである。欧州の 2 つの PD 患者コ 領域で重度の臨床症状がみられた。平均罹病期間はお ホート計 802 例において,PD の運動症状および非運 おむねサブタイプ間で同様であったが〔3 つのクラス 動 症 状 の デ ー タ を 収 集し た。 オ ラ ン ダ 人 コ ホ ート ター(サブタイプ)間で有意差なし〕 ,人口統計学的お (PROPARK)の患者 344 例の試験参加時データを用い, よび臨床的変数との関連ではサブタイプ間で有意差が モデルに基づくクラスター解析を行った。この解析結果 認められた。ある程度の PD 罹病期間が認められる患者 の再現性は,同一コホートの 2 回目の年次評価データ において,PD サブタイプは主に,非ドパミン系の障害 において検討し,また,独立したスペイン人コホート による症状および運動合併症の重症度によって特徴付 (ELEP) の患者 357 例で妥当性を検証した。これに続き, けることができる。これらの PD サブタイプは,発症機 臨床的および人口統計学的変数を用いて各サブタイプ 序,治療,加齢および性別の間の複雑な相互作用を反映 の特徴を明らかにした。異なる 2 つの患者集団において, すると考えられる。 類似する 4 種類の PD サブタイプが同定された。これ Movement Disorders, Vol. 26, No. 1, 2011, pp51–58 Key Word パーキンソン病,サブタイプ,クラスター解析,非ドパミン系,運動合併症 24 #MD5-1.indb 24 11.7.14 2:25:06 PM Abstract A tremor bradykinesia / rigidity FOSS PIGD cognitive impairment psychotic symptoms autonomic dysfunction daytime sleepiness depressive symptoms nighttime sleepproblems motor fluctuations dyskinesias 1 B 2 4 3 tremor bradykinesia / rigidity FOSS PIGD cognitive impairment psychotic symptoms autonomic dysfunction daytime sleepiness depressive symptoms nighttime sleepproblems motor fluctuations dyskinesias C 1 2 1 2 3 4 tremor bradykinesia / rigidity FOSS PIGD cognitive impairment psychotic symptoms autonomic dysfunction daytime sleepiness depressive symptoms nighttime sleepproblems motor fluctuations dyskinesias 3 4 Figure 2 EII-4 モ デ ル の ヒ ー ト マ ッ プ。A:PROPARK コ ホ ー ト(1 年 目 ) ,B: PROPARK コホート(2 年目) ,C:ELEP コホート。FOSS(freezing during on, speech, and swallowing)は, 「on 時のすくみ」 , 「嚥下」 , 「発話」で構成される体軸運動症状。 PIGD(postural-instability-gait-difficulty)は, 「立ち上がり動作」 , 「歩行」 , 「姿勢の不安 定性」で構成される体軸運動症状。各カラム(1 ~ 4)は各クラスター(サブタイプ) に相当する。ヒートマップ中の色は,そのクラスター(サブタイプ)の該当症状に関す る平均重症度が, 群全体の平均よりも低いか(青色)または高いか(赤色)を示している。 25 #MD5-1.indb 25 11.7.14 2:25:07 PM パーキンソン病における Diphasic および Peak-Dose ジスキ ネジアの遺伝的感受性の違い Differential Genetic Susceptibility in Diphasic and Peak-Dose Dyskinesias in Parkinson’s Disease * Jee-Young Lee, MD, Jinwhan Cho, MD, PhD, Eun-Kyung Lee, RN, Sung-Sup Park, MD, PhD, and Beom S. Jeon, MD, PhD * Department of Neurology, Seoul National University Boramae Hospital, Seoul, Korea 本 研 究 の 目 的 は, パ ー キ ン ソ ン 病(Parkinson’ s した。L—ドパ誘発性ジスキネジアが認められた患者は disease; PD)患者におけるレボドパ(L—ドパ)誘発性 計 229 例であった(peak-dose ジスキネジア 205 例, ジスキネジア(levodopa-induced dyskinesia)の 2 つ diphasic ジスキネジア 57 例,両ジスキネジア併存例 の型〔diphasic ジスキネジア(diphasic dyskinesia) 33 例) 。性別,PD 発症時年齢,Hoehn & Yahr 分類,L— お よ び peak-dose ジ ス キ ネ ジ ア(peak-dose ドパ投与期間で補正後,diphasic ジスキネジアのみに dyskinesia) 〕について,遺伝的感受性に違いがあるか つ い て DRD3 p.S9G 変 異 と の 関 連 が 認 め ら れ た。 否かを検討することである。本試験コホートは,L—ドパ DRD3 p.S9G の遺伝子型が AA である場合,L—ドパ療 投与を受け,罹病期間が 5 年以上の韓国人 PD 患者 法の継続に伴って diphasic ジスキネジアの発症リスク 503 例(非血縁者)で構成された。L—ドパ誘発性ジス 。peakが優位に上昇すると考えられた(p = 0.02) キネジアの有無は通常の経過観察において特定し,細 dose ジスキネジアについては,検討した 6 種類の遺伝 心 の 注 意 を 払 っ て L— ド パ 誘 発 性 ジ ス キ ネ ジ ア を 的変異との間に有意な関連は認められなかった。慢性 L— diphasic ジスキネジアおよび peak-dose ジスキネジア ドパ療法を受ける PD 患者の diphasic ジスキネジア発 の 2 つの型に分類した。患者 503 例と健常対照被験者 症には遺伝的感受性が関与すると考えられ,diphasic 559 例において遺伝子型分析を行い,DRD3 p.S9G, ジスキネジアの根底にある病態生理学的メカニズムは DRD2 Taq1A ,GRIN2B c.2664C>T,c.366C>G, peak-dose ジスキネジアとは異なる可能性がある。 c.-200T>G,プロモーター領域 SLC6A4 の多型を検索 Movement Disorders, Vol. 26, No. 1, 2011, pp. 73–79 Key Word diphasic ジスキネジア,パーキンソン病,遺伝的感受性,ドパミン受容体 D3 TABLE 1. Clinical characteristics of the included Table 1 対象被験者の臨床的特徴 subjects AA D R D 3 100 Percent without diphasic dyskinesia, % AG or GG 80 p=0.024 60 40 20 0 0 5 10 Figure 1 DRD3 p.S9G AA 遺伝子型の患者と他の患者における diphasic ジスキネジア無発症の累積確率の比較。p 値はログランク 検定で算出。 #MD5-1.indb 26 Patients (n ¼ 503) Controls (n ¼ 559) Gender (m/f), n Age, yr Age at onset, yr Duration of the disease, yr Hoehn and Yahr (HY) stage, 1�5 Duration of levodopa therapy, yr Motor fluctuation, n (%) Dyskinesia, n (%) Diphasic dyskinesia Peak dose dyskinesia Both peak dose and diphasic dyskinesias 255/248 62.9 (9.3), 23�91 53.5 (9.8), 18�85 9.4 (4.4), 5�33 2.6 (0.7), 1�5 259/300 58.4 (10.6), 37�85 NA NA NA 6.9 (4.1), 0.3�29 NA 285 (56.7) 229 (45.5) 57 (11.3) 205 (40.8) 33 (6.6) NA NA NA NA NA D I P tion of levodop 0.001), a higher higher frequenc 23.1%, P < 0.0 compared with LID (total dail 853.9 vs. 682.2 gender difference DDSK was pre the 229 patient DDSK and PDS acteristics betwe were no significa duration of PD, PD onset, and t levodopa treatm 15 Duration of L-dopa therapy, yrs 26 Characteristics A N D Values are shown as mean (standard deviation), with range or number (%) 値は平均値(標準偏差)と範囲,または例数(%)で示す。 as indicated. NA NA, not=該当せず applicable. despite of chronic levodopa therapy for �5 years as a nondyskinetic control group (n ¼ 152, see Tables 3 and 4, and Supporting Information 3 and 5) in the comparative analysis, thus avoiding nondyskinetic 11.7.14 Gene The allele and and controls we and there were n six genetic varia trols (Table 2). As listed in Ta 2:25:08 PM Abstract L E E E T A L . Table 2 PD 患者群と正常対照群におけるアリル頻度と遺伝子型分布 TABLE 2. The allele frequencies and genotype distribution in PD patients and in normal controls No. of subjects (%) Gene Normal controls (n ¼ 559) DRD2 g.32806C > T ¼TaqIA (rs1800497) DRD3 p.S9G (rs6280) GRIN2B c.-200T>G (rs1019385) GRIN2B c.366C>G (rs7301328) GRIN2B c.2664C>T (rs1806201) SLC6A4 (5HTTLPR) Allele Genotype Allele Genotype Allele Genotype Allele Genotype Allele Genotype Allele Genotype C T CC CT TT A G AA AG GG G T GG GT TT C G CC CG GG C T CC CT TT S L SS LS LL 664 (59.4) 454 (40.6) 196 (35.1) 272 (48.7) 91 (16.3) 802 (71.9) 314 (28.1) 288 (51.6) 226 (40.5) 44 (7.9) 508 (45.4) 610 (54.6) 117 (20.9) 274 (49.0) 168 (30.1) 617 (55.2) 501 (44.8) 165 (29.5) 287 (51.3) 107 (19.1) 548 (49.0) 570 (51.0) 125 (22.4) 298 (53.3) 136 (24.3) 865 (77.6) 249 (22.4) 334 (60.0) 197 (35.4) 26 (4.7) Patients with PD (n ¼ 503) 578 422 164 250 86 705 289 260 185 52 440 558 102 236 161 566 430 160 246 92 483 511 110 263 124 760 226 304 152 37 (57.8) (42.2) (32.8) (50.0) (17.2) (70.9) (29.1) (52.3) (37.2) (10.5) (44.1) (55.9) (20.4) (47.3) (32.3) (56.8) (43.2) (32.1) (49.4) (18.5) (48.6) (51.4) (22.1) (52.9) (24.9) (77.1) (22.9) (61.7) (30.8) (7.5) P-value* 0.458 0.731 0.634 0.263 0.533 0.738 0.448 0.656 0.846 0.973 0.756 0.072 *Comparison of allele and genotype distributions between the patients and normal controls. A Bonferroni correction for multiple testing done and the Pp< *PD 患者群と正常対照群におけるアリルおよび遺伝子型分布の比較。多重検定に関する Bonferroni 補正を行い, 0.008isを有意とみなした。 values are considered significant if they are less than 0.008. 略語:DRD2 D2 遺伝子,DRD3 D3gene; 遺伝子,GRIN2B = Nメチル -D- アスパラギン酸型グルタミン酸 D-aspartate receptor 2B gene; SLC6A4, Abbreviations:=ドパミン受容体 DRD2, dopamine receptor D2 gene; DRD3,=ドパミン受容体 dopamine receptor D3 GRIN2B, glutamate N-methylserotonin transporter gene; PD, Parkinson’s disease. 受容体 2B 遺伝子,SLC6A4 =セロトニントランスポーター遺伝子,PD D R =パーキンソン病 D 3 A N D D I P H A S I C D Y S K I N E S I A I N P D TABLE 3. Comparison of genotype distributions between patients with and without any dyskinesias Table 3 ジスキネジアの有無による遺伝子型分布の比較 Unlike DDSK, the expression of PDSK was not associEffect of Genotype on the Onset of the No. of subjects (%) ated with any of the six genetic variants studied. We Dyskinesia With the DRD3 genotype as a factor, dyskinesiaDiphasic free survival curve revealed that the risk of developing Non-dyskinesia* dyskinesia Gene Genotype ¼ 152) ¼ 57) DDSK significantly increased with(n the duration of (n levodopa therapy in patients with the DRD3 p.S9G AA DRD2 CC 47 (31.1) 19 (33.9) genotype (P ¼ 0.024; g.32806C>T CT Fig. 1). We77found (51.0) no significant 30 (53.6) trends for the variants of DRD2,27 the (rs1800497) TT (17.9)three GRIN2B 7 (12.5) DRD3 AA 67 (44.7) 39 (69.6) variants, and 5-HTTLPR in the development of either p.S9G 66 (44.0) 14 (25.0) DDSK or PDSK. AG (rs6280) GG 17 (11.3) 3 (5.4) GRIN2B GG 26 (17.3) 13 (23.2) c.-200T>G GT 72 (48.0) 26 (46.4) (rs1019385) TT 52 (34.7) 17 (30.4) GRIN2B CC 48 (32.0) 18 (32.7) The present study c.366C>G CG revealed that79genetic (52.7) modification 29 (52.7) (rs7301328) GG factor in the23expression (15.3) 8 (14.5) can be an important of DDSK GRIN2B (25.8) 14 (25.5) in PD. The DRD3CCp.S9G variant39 seemed to be indec.2664C>T CT (46.4) (49.1) pendently associated with DDSK70 after adjusting27for (rs1806201) TT 42 (27.8) 14 (25.5) gender, age at PD onset, HY stage,90and levSLC6A4 SS (60.4)duration of 28 (50.0) odopa treatment. ItLS also exerted 49 significant effects23on (5HTTLPR) (32.9) (41.1) LL onset after 10levodopa (6.7) 5 (8.9) the timing of DDSK treatment. Discussion conducted the same analysis in a subgroup of patients Peak dose who had PDSK without concomitant DDSK and found dyskinesia † consistently results (see Supporting InformaP-value‡ P-value§ (n ¼ 205) negativeP-value tion 5). This novel finding supports the hypothesis that 64 (31.4) underlying 0.646 the development 0.627 0.677 is the mechanism of DDSK 111 (54.4) different from that underlying PDSK.4,5,6 29 (14.2) DDSK occurred less frequently 0.120 than PDSK in our 113 (55.7) 0.006 0.062 cohort,73 which is consistent with previous findings.7 (36.0) (8.4) Several17clinical features suggest that the two conditions 38 (18.5) pathophysiological 0.609 0.678 0.666 is have distinct substrates. DDSK 105 (51.2) usually more dystonic than choreic, beginning at the 62 (30.2) distal 65 lower spreading in0.787 an ascending0.823 wave (31.7)limbs and0.988 to the103trunk and the upper limbs. It is more painful (50.2) 37 (18.0) than PDSK, and it is difficult to treat.1,6 and disabling 38 (18.7)PDSK is 0.928 0.096 0.133 It Conversely, choreic rather than dystonic. 117 (57.6) commonly affects the upper part of the body, it is usu48 (23.6) ally not painful, and0.404 it can go unnoticed when0.885 it is 131 (64.5) 0.730 1 In(29.6) addition, PDSK can occur in normal individumild. 60 12 (5.9) als if the dosage of levodopa is sufficiently high.1,6,18 * *Patients レボドパ投与期間が 5 年以上で,ジスキネジアが認められなかった患者。 who had no dyskinesia treated with levodopa � 5 years. † Comparisons between the diphasic dyskinesia and non-dyskinesia groups. Diphasic ジスキネジア群と非ジスキネジア群との比較。 ‡ 76 Movement Disorders, Vol. 26, No. dyskinesia 1, 2011 Comparisons between the peak dose and non-dyskinesia groups. ‡ §Comparisons between the entire dyskinesia and non-dyskinesia groups. Peak-dose ジスキネジア群と非ジスキネジア群との比較。 †,‡,§ A Bonferroni correction for multiple testing is done and the P-values are considered significant if they are less than 0.008. § 全ジスキネジア群と非ジスキネジア群との比較。 Abbreviations as Table 1 and 2. †, ‡ , § 多重検定に関する Bonferroni 補正を行い,p < 0.008 を有意とみなした。 The AA genotype of DRD3 p.S9G is linked to a TheTable role1 および of the2 参照。 D3 receptor in LID has been sug略語は † #MD5-1.indb 27 gested by studies involving 6-hydroxydopaminelesioned rats19 and a nonhuman primate 1-methyl to 4-phenyl to 1,2,3,6-tetrahydropyridine model expressing LID.10 The D3 is overexpressed in the presence of LID compared with non-LID and normal controls. This overexpression is correlated with the severity of 10,11 weak binding affinity to dopamine.23 Interestingly, the DRD3 p.S9G G allele, a higher binding affinity allele, is associated with susceptibility to tardive dyskinesia,24,25 for which dopamine-receptor hypersensitivity is one of the possible mechanisms.26 Thus, the opposing characteristics of the A and G alleles of DRD3 27 11.7.14 2:25:09 PM リチャードソン症候群(PSP-RS) ,進行性核上性麻痺 - パー キンソニズム(PSP-P)およびパーキンソン病(PD)患者の 脳幹構造の MRI 測定 MRI Measurements of Brainstem Structures in Patients with Richardson’s Syndrome, Progressive Supranuclear Palsy-Parkinsonism, and Parkinson’s Disease * Giulia Longoni, MD, Federica Agosta, MD, Vladimir S. Kosti , MD, Tanja Stojkovi , MD, Elisabetta Pagani, MSc, Tatjana Stoši -Opin al, MD, and Massimo Filippi, MD * Neuroimaging Research Unit, Institute of Experimental Neurology, Division of Neuroscience, Scientific Institute and University Ospedale San Raffaele, Milan, Italy 2 種類の進行性核上性麻痺(progressive supranuclear 脳 脚 比 ) ,MR パ ー キ ン ソ ニ ズ ム 指 標〔MR palsy; PSP)患者およびパーキンソン病(Parkinson’ s parkinsonism index, (橋 / 中脳比)*(中小脳脚 / 上小 disease; PD)患者において,脳幹の MRI 測定に基づく 脳脚比) 〕を算出した。橋 / 中脳比および MR パーキン 診断の精度を検討した。3 次元撮像法による T1 強調画 ソニズム指標により,高い感度(90%,100%) ,特異 像 を 用 い, リ チ ャ ー ド ソ ン 症 候 群(progressive 度(96%,92%) ,正確度(94%,97%)で PSP-RS supranuclear palsy-Richardson’ s syndrome; PSP- と PD とを鑑別できた。PSP-P と PD との鑑別は橋 / 中 RS)患者 10 例,進行性核上性麻痺 - パーキンソニズ 脳比でのみ可能であったが,その診断精度は低かった ム(progressive supranuclear palsy-parkinsonism; (感度= 60%,特異度= 96%,正確度= 86%) 。PSP- PSP-P)患者 10 例,PD 患者 25 例,健常対照被験者 RS に比べ,PSP-P のテント下病変は比較的軽度である。 24 例を対象に,中脳面積,橋面積,上小脳脚の幅,中 橋 / 中脳比は,単体としての PSP-P と PD との鑑別に 小脳脚の幅を測定した。橋面積と中脳面積の比(橋 / 中 おいて有望な尺度であると考えられる。 脳比) ,中小脳脚幅と上小脳脚幅の比(中小脳脚 / 上小 Movement Disorders, Vol. 26, No. 2, 2011, pp. 247–255 Key Word 進行性核上性麻痺,パーキンソン病,脳幹,中脳,萎縮 Figure 1 健常対照被験者の 3 次元 T1 強調矢状断像 と冠状断像。 (A) 中脳および橋領域, (B) 上小脳脚 (SCP) の幅, (C)中小脳脚(MCP)の幅を赤色で示す。MRI 測定値は中脳面積= 123.2 mm2,橋面積= 530.0 mm2, 上小脳脚の幅= 3.9 mm, 中小脳脚の幅= 9.6 mm であっ た。 28 #MD5-1.indb 28 11.7.14 2:25:12 PM Abstract B A PSP-P patient PSP-RS patient C PD patient Figure 2 (A)リチャードソン症候群(PSP-RS)患者, (B)PSP- パーキンソニズム(PSP-P)患者, (C)パーキンソン病(PD)患者の 3D T1 強調矢状断像と冠状断像。 (1)橋および中脳領域, (2)上小脳脚(SCP)の幅, (3)中小脳脚(MCP)の幅を赤色で示す。MRI 測定値は(A) 中脳面積= 48.9 mm2,橋面積= 375.3 mm2,上小脳脚の幅= 1.7 mm,中小脳脚の幅= 5.6 mm, (B)中脳面積= 107.6 mm2,橋面積= 461.2 mm2,上小脳脚の幅= 3.1 mm,中小脳脚の幅= 7.9 mm, (C)中脳面積= 139.0 mm2,橋面積= 525.8 mm2,上小脳脚の幅= 3.6 mm,中小脳 脚の幅= 8.9 mm であった。 220 200 12 12 18 11 27 5 29 160 140 27 120 100 SCP width SCP width 10 MCP MCP width M area 180 9 8 52 7 4 3 80 6 60 2 5 40 PSP-RS PSP-P PD Controls PSP-RS PSP-P Controls PD P/M 8 6 4 2 MR parkinsonism index 35 10 PSP-RS PSP-P PD Controls 32 34 30 25 20 15 10 5 PSP-RS PSP-P PSP-RS PSP-P PD Controls Controls PD Figure 3 脳幹 MRI 測定値の箱ひげ図。有意な群間差が認められる。 「箱」は四分位範囲を示し, 各被験者の測定値の 50%を含む。 「ひげ」は, 「箱」から最大値および最小値に伸びる直線であり,外れ値は除外している。 「箱」を横切る直線は中央値を示す。外れ値(丸印)は, 「箱」の 上端または下端から, 「箱」の長さ(すなわち四分位範囲)の 1.5 倍を超えて離れている値である。 29 #MD5-1.indb 29 11.7.14 2:25:13 PM 振戦に対する視床刺激:刺激標的部位の同定は改善可能か Thalamic Stimulation for Tremor: Can Target Determination Be Improved? *, ** Eric Bardinet, PhD, Hayat Belaid, MD, David Grabli, MD, PhD, Marie-Laure Welter, MD, PhD, Sara Fernandez Vidal, PhD, Damien Galanaud, MD, PhD, Stéphane Derrey, MD, Didier Dormont, MD,Philippe Cornu, MD, PhD, Jérôme Yelnik, MD, and Carine Karachi, MD, PhD * Université Pierre et Marie Curie-Paris6, Centre de Recherche de l’Institut du Cerveau et de la Moelle épinière, Paris, France CNRS, Paris, France ** 視床中間腹側核(ventral intermedius nucleus; Vim) 半の患者(24 例)では,それぞれの手法で得られた標 の高周波刺激は,姿勢時振戦に有効な治療法として使用 的間の距離(ピタゴラスの定理による)が 1.5 mm よ さ れ て い る。 刺 激 標 的 部 位 の 座 標 は,統 計 的 手 法 り大きく,このうち 79%の患者では,患者個別的手法 (statistical method)で算出される場合が最も多い。本 で決定した標的部位に電極が埋め込まれた。標的間の 研究では,刺激標的部位の同定において,統計的手法と 距離が 1.5 mm 未満であった残りの患者(11 例)では, 患者個別的手法(individual targeting method)を比較 73%の患者において,統計的手法で算出した標的部位 する。患者個別的手法では,組織学的知見に基づく変形 に電極が埋め込まれた。全体として,86%の患者で, 可能な 3 次元脳アトラスを用い,各患者の脳にこのア 患者個別的手法で決定した刺激標的部位は,統計的手 トラスを適応させることで,各患者の MRI 画像上で 法の刺激標的部位よりも 2 mm 以上内側であった。本 Vim の位置を特定する。一連の患者 29 例が,重度本態 研究の結果から,統計的手法に基づいた Vim 標的部位 性振戦の治療として,一側または両側 Vim に対する電 の決定は正確でない可能性が示唆される。特に,実際 極の埋め込み術を受けた。計 35 の刺激標的部位は,ま よりも外側方向にずれ計算され,最適な臨床成績が得ら ず統計的手法,続いて,変形可能な脳アトラスを用いた れていない可能性が考えられる。これらの知見から,実 患者個別的手法で決定した。それぞれの手法で得られ 地診療では,Vim 手術中に微小電極によって刺激部位を た標的間の距離は,ピタゴラスの定理で算出した。周術 探索する際,統計的手法で算出される刺激標的よりも内 期の刺激効果について二重盲検法で評価し,統計的手 側の軌道(trajectory)を 1 つ以上含めて検討すべきで 法および患者個別的手法による刺激標的を比較した。大 ある。 Movement Disorders, Vol. 26, No. 2, 2011, pp.307-312 Key Word 振戦,深部脳刺激,視床 30 #MD5-1.indb 30 11.7.14 2:25:14 PM Abstract Table 1 臨床データと刺激標的部位の座標 TABLE 1. Clinical and target coordinates data Tremor severity Patients Age Age of onset 70 Childhood 62 53 53 60 60 30 50 70 40 17 41 60 60 60 Childhood 34 34 Childhood 40 40 35 40 40 3 3 2 3 3 3 3 4 3 2 2 3 4 4 4 4 3 4 3 3 3 2 3 4 3 3 3 3 4 2 3 3 4 4 3 0 0 0 1 0 1 0 1 0 1 1 0 1 2 0 2 0 0 0 1 1 0 0 0 1 2 0 2 2 0 0 0 0 1 0 X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ 14.3 16.8 16.8 15.7 15 15.3 15.3 16.7 14 15.3 15.3 16 13 13 14.8 15.3 13.5 14.3 14.5 14.8 14.8 13.7 14.1 13.8 13.8 16 13.11 14 15.25 15.5 14.4 16.65 14.8 13 15.5 Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y ¼ 6.2 ¼ 6.8 ¼7 ¼7 ¼7 ¼ 6.1 ¼ 6.1 ¼ 7.2 ¼ 6.4 ¼ 6.6 ¼ 6.6 ¼ 6.3 ¼ 5.9 ¼6 ¼ 6.4 ¼ 6.4 ¼6 ¼ 6.7 ¼ 6.6 ¼ 6.6 ¼ 6.6 ¼ 6.2 ¼7 ¼ 5.6 ¼ 5.6 ¼7 ¼ 6.37 ¼6 ¼ 7.5 ¼ 7.2 ¼ 6.4 ¼ 6.7 ¼ 6.6 ¼6 ¼ 6.3 X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X ¼ 12.5 ¼ 15.5 ¼ 14.5 ¼13.5 ¼ 13.5 ¼ 14.5 ¼ 15.5 ¼ 14 ¼ 11.5 ¼ 14 ¼ 14.5 ¼ 17 ¼ 13.5 ¼ 12.5 ¼ 15.5 ¼ 14.5 ¼ 13 ¼ 11.5 ¼ 12.5 ¼ 13 ¼ 12.5 ¼ 12.5 ¼ 14 ¼ 11.5 ¼ 11 ¼ 13.5 ¼ 12.5 ¼ 12.5 ¼ 14.5 ¼ 14.5 ¼ 14 ¼ 14 ¼ 13 ¼ 11 ¼ 13.5 Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ ¼ 5 5 7 8.5 7.5 6 6 9 6 6.5 5.5 6.5 5.5 4 5 6 4 8 6.5 6.5 6 5.5 8.5 7.5 5.5 6.5 4.5 6.5 7 7 6 6.5 6.5 4.5 7.5 2.16 2.22 2.3 2.66 1.58 0.81 0.22 3.24 2.53 1.3 1.36 1.02 0.64 2.06 1.57 0.89 2.06 2.4 2 1.8 2.38 1.39 1.5 2.98 2.8 2.55 1.97 1.58 0.9 1.02 0.57 2.66 1.8 2.5 2.33 2 2 2 2 2 1 1 2 2 1 1 1 1 2 1 2 1 2 2 1 1 2 2 2 2 1 2 2 2 1 1 2 2 2 2 T A R G E T I N G 65 Forelimbs, head Forelimbs R>L Forelimbs R>L Forelimbs R>L Forelimbs R>L Forelimbs, head Forelimbs, head Left hemibody Left hemibody Forelimb R, voice Forelimbs, head, voice Forelimb R Forelimbs, hindlimbs, tronk, head Forelimb R Forelimbs, hindlimbs L>R, head, voice Forelimbs, hindlimbs L>R, head, voice Forelimb R Left hemibody Forelimbs, head, voice Forelimbs Forelimbs Forelimbs L>R, tronk, voice, head Left hemibody Forelimbs R>L, head, voice Forelimbs R>L, head, voice Right hemibody Forelimbs, head Forelimb L Left hemibody Forelimbs>hindlimbs, L>R Left hemibody Left hemibody Forelimbs, hindlimbs, tronk, head, voice Forelimbs, hindlimbs, tronk, head, voice Right hemibody T H A L A M I C Essential 77 Essential 70 Essential 70 Essential 59 Essential 59 Essential 70 Essential 70 Post-traumatic 33 Essential 79 Essential 76 Essential 76 Essential 71 Essential 36 MS 45 Essential 71 Essential 71 Essential 62 Essential 75 Essential 77 Essential 44 Essential 44 Essential 51 Essential 62 Essential 70 Essential 70 Essential 60 Essential 52 Myoclonus dystonia 40 Charcot Marie tooth dis 68 Parkinson disease 73 Essential 73 Essential 74 Essential 70 Essential 70 Parkinson disease 73 Preoperative ON stimulation Guiot target 1 Guiot target 1 Atlas target 2 Atlas target 2 Pythagoreen Choosen score (6 mo) X Y X Y distance target I M P R O V E D F O R 309 T R E M O R Movement Disorders, Vol. 26, No. 2, 2011 A B1 B2 B3 R B3 L B4 R B4 L B5 B6 D1 D2 D3 D4 D5 E1 R E1 L E2 F L1 L2 R L2 L L3 L4 M1 R M1 L M2 M3 N1 N2 P1 P2 P3 V1 R V1 L V2 Etiology Localization of tremor Figure 1 上段パネル:術前計画。左:術前の T1 強調 MRI 冠状断像。右:脳アトラスに基づく視床(濃緑色) ,Vim(薄緑色) ,大脳脚(赤 紫色)の輪郭。同一断面像上に重ね合わせている。赤色の線は患者個別的手法による刺激標的を示す。青緑色の縦線は統計的手法による刺激 標的を示す。患者 A のデータ。中段パネル:統計的手法と患者個別的手法による刺激標的の比較(Vim の 3 次元画像) 。左:手術中に探索し た 3 つの軌道(中央:赤色の線,内側:赤紫色の線,後方:緑色の線) 。統計的手法による刺激標的(緑色の球形)と,アトラスを用いた患者 個別的手法による刺激標的(青色の球形) 。白色の球形は,後方軌道上の振戦誘発部位(tremor cell)を示す。右:同一画像上に,最終的な電 極(筒状の暗灰色部分)の軌道とその 4 つの接触子(円柱状の青色部分)を示す。患者 A のデータ。統計的手法で算出した刺激標的は Vim の外側に位置し, 電極は, アトラスを用いた患者個別的手法による刺激標的に留置されている。下段パネル:術後画像と治療用接触子の位置(青 色の円) 。左列:患者 V1 左側(L)のデータ。術後の T1 強調 MRI 冠状断像と横断像。中列:患者 M3 のデータ。術後の CT スキャン矢状断 像(上)と,それに対応する術前の T1 強調 MRI 画像(CT スキャンに登録) 。右列:患者 D5 のデータ。術後の CT スキャン冠状断像(上)と, それに対応する術前の T1 強調 MRI 画像(CT スキャンに登録) 。 31 #MD5-1.indb 31 11.7.14 2:25:17 PM 本態性振戦とパーキンソン病との関連についての再考 Revisiting the Relationship Between Essential Tremor and Parkinson’s Disease * R. Fekete, MD, J. Jankovic, MD * Parkinson’s Disease Center and Movement Disorders Clinic, Department of Neurology, Baylor College of Medicine, Houston, Texas 背景:本態性振戦(essential tremor; ET)とパーキン ビューするとともに,その背景として既発表データを検 ソン病(Parkinson’ s disease; PD)との関連性は総説 討した。 論文のテーマとされ,長年にわたり議論されている。し 考察: 「純粋な」ET を呈する患者の一部は PD に移行す かし,現在では,少なくとも一部の患者集団においてこ るという考え方については,説得力のあるエビデンスが の 2 つの一般的な運動障害性疾患の病因が共通である 存在すると考えられるものの,この関連性の生物学的な ことを示すエビデンスが増えつつある。 機序は十分には解明されていない。また,その後 PD を 方法:PubMed および著者ら所有のファイルを用い, 発症する ET 患者の予測因子や,PD 患者が ET を発症 臨床像,疫学,遺伝,画像所見,病理における両疾患の しやすいか否かについては,なお不明である。このよう 重複に関するキーワードによりデータベースを検索し な ET と PD が混合した臨床型の理解を深めるためには, た。 疫学,臨床像,遺伝,画像所見,病理に関する研究がさ 結果:上記の各カテゴリーにおける新知見を批判的にレ らに必要である。 Movement Disorders, Vol. 26, No. 3, 2011, pp. 391–398 Key Word 小脳,本態性振戦,Lewy 小体,パーキンソン病,振戦 32 #MD5-1.indb 32 11.7.14 2:25:17 PM Abstract F E K E T E A N D J A N K O V I C Table 1 ET と PD との関連についてのエビデンスを提示する研究の概要 TABLE 1. Summary of studies providing evidence for association between ET and PD Clinical and epidemiologic Studies Incident PD is 3.5 times higher in patients with ET compared with controls7 Patients with preexisting ET are more likely to have tremor-dominant PD15,29 Significantly increased risk of ET in patients with PD in a case–control study of 600 patients28 ET-type tremor present 5 yr before the onset in 20/164 (12.2%) of patients with PD, 2/68 (2.9%) of PSP, and none of 31 CBD cases (P < 0.025); family history of ET-type tremor was identified in 18/84 (21.5%) of PD, 4/46 (6.5%) of PSP, and 1/20 (5.0%) of CBD patients (P < 0.025)14 Patients with PD are 3 to 13 times more likely to have diagnoses of ET than patients with Parkinson-plus syndromes15 20% of patients with ET have rest tremor with characteristics of PD24 In a sample of 163 twins with postural or kinetic tremor, 60% had PD32 Series of 13 patients initially presenting with asymmetric postural tremor eventually developed evidence of PD11 In ET-PD combination, side of the greatest initial ET severity corresponded to the side of the greatest PD severity35 Bradykinesia on repetitive finger movements and impairment of visual reaction tasks shown in ET11 Both idiopathic PD and ET have slower motor initiation than controls12 Different response between ET and PD seen on paired association tests23 Genetic Risk of ET significantly increased for relatives of patients with onset of PD at age 66 or younger37 Risk of action tremor higher in relatives of tremor-dominant PD as opposed to PIGD subtype.38 Isolated ET phenotype followed by PD reported in a patient with LRRK2 R1067Q mutation40 Compound heterozygous PARKIN mutations found in family with combination of ET and PD41 LINGO1 and LINGO2 variants may be associated with both ET and PD, although there is conflicting data42,44,45,46,47 Imaging Patients with long-standing rest tremor without other parkinsonian features have evidence of dopaminergic deficit on F-DOPA PET27 Striatal dopamine transporter loss in patients with ET seen in some,50 but not all51,52 SPECT studies Pattern of DAT transporter loss mostly in caudate in both ET and tremor-dominant PD differs from putaminal DAT loss in akinetic—rigid PD DAT loss predominantly in the putamen27,50,56,57 Diffusion tensor imaging found changes in anisotropy and mean diffusivity in dentate nucleus and superior cerebellar peduncle in ET but not PD60 Midbrain sonography shows increased SN hyperechogenicity in ET patients62 Pathological Existence of families with a combination of ET and autopsy proven PD63 Lewy bodies found in locus ceruleus of brains of patients with ET,65 but the importance of this finding has been challenged by Shill et al.64 -Lewy body subtype of ET is distinct from cerebellar ET68 Therapeutic Levodopa may worsen postural and action tremor in PD72,73 Tremor predominant PD may require addition of medication traditionally used for ET74 参考文献リストは wileyonlinelibrary.com のオンライン版で閲覧可能。 F E K E T E A N D J A N K O V I C Table 2 遺伝疫学研究の概要 TABLE 2. Summary of genetic epidemiological studies with adjusted relative risk (RR) of 3.47 (95% confiN (relatives of HR,7 OR, dence interval, 1.82–6.59; P < 0.001). Author PD probands) or RR P Lack of disease-specific diagnostic markers for ET 37 Rocca PD, et al. short follow-up, 1,278 insufficientHRclinical 2.24 0.006 and informapopulation tion, and various methodological problems may lead sample to misdiagnoses and2,684 probably contribute to the disHR 1.92 0.0004 Rocca et al.37 crepancies in reported associations of the two disorreferral 8 ders. sampleIn a study of 71 consecutive patients presenting HR 2.15 of ET, 37 0.0002 to a tertiary referral 2,684 center with a diagnosis % were found to be misdiagnosed as PD or dystonia according to the Movement Disorders Society criteria 9 study involving for ET. OR 13 3.64 patients ini0.0001 Spanaki and In another 1,524 tially presenting with asymmetric postural hand Plaitakis34 tremor and no rest tremor, diagnosed as ET, all 4.48 at least 10 0.04 patients developed evidence of PDORafter years of follow-up.10 Although the authors suggested that the patients had PD and were initially misdiagnosed as ET, it is also 3,005possible that RR the 2.14 patients ini0.0001 Minen and Louis35 tially had ET and later developed symptoms of PD. ET patients have been shown to have cogwheel rigidLouis15 392 210 PD cases, 210 parkinson plus syndrome Movement Disorders, Vol. 26,cases No. 3, 2011 Jankovic et al.33 319 PD, 140 ET, 125 ETþPD, 99 PSP, 104 control cases ity and bradykinesia of repetitive finger taps and impairment on visual reaction tests, typically associEvaluation Description ated with PD.11 Longer reaction times and slower Clinical evaluation by movement Risk of developing ET in movement velocities on a wrist flexion and extension disorders relatives of PD cases task were alsospecialist found after in both ET and PD.12 positive phone survey Because posturalbytremor is frequently encountered in Clinical evaluation 13 movement Risk of developing ET in patients with specialist PD, studies of association ET disorders after relatives ofbetween PD cases with and PDpositive oftenphone insisted be present at survey that the ET had onset to � 57 evaluation by the movement of developing ET in least Clinical 5 years before onset of Risk PD-related symptoms relatives of criteria, tremor using after these rather arbitrary we (Table disorders 1).6 Byspecialist positive phone survey predominant or mixed found that history of ET much more likely preceded form PD the onset of PD than that of other neurodegenerative Direct clinical evaluation by Risk of developing ET in disorders, suchdisorders as progressive movement specialist supranuclear first-degree palsy relatives(PSP) of PD 14 in most cases, chart review cases In a retrospecor corticobasal degeneration (CBD). Direct clinical evaluation by of developingpatients, ET in tive review of medical records ofRisk consecutive movement disorders specialist first degree relatives or we found history of ET-type tremor at least 5 years in most cases, chart review tremor-dominant or before the onset of the parkinsonian in 20/ mixed disorder PD 164 (12.2%) of patients with PD,Risk compared within 2/68 Proband’s report of action tremor tremor dominant (2.9%) of PSP and none of 31 CBDrelative casesof (P < 0.025). PD case compared Furthermore, family history of ET-type tremorto was OR 12.85 0.001 Direct evaluation by movement disorders specialist 5.1 % PD, 23.4% ET, 20.7 % ETþ PD, 2.6% PSP, 2.2% controls <0.005 for PD versus control and PD versus PSP Probands diagnosed by movement disorders specialist, tremor in relatives as per proband’s report control relative Risk of ET diagnosis in patient with PD compared with patient with Parkinson-plus syndrome Presence of tremor in parents and siblings of proband 参考文献リストは wileyonlinelibrary.com のオンライン版で閲覧可能。 #MD5-1.indb 33 diagnostic errors. In some cases, repeat examinations over a period of time are needed to define the tremor phenotype and associated clinical features. Tremor in ET family members is often wrongly attributed to alcohol but, instead, high alcohol consumption may be a marker for underlying ET.36 In a study of a population based sample of 1,278 relatives of 167 PD ent in the relatives of PD patients more often than in those of controls (OR: 3.64, P < 0.0001) and the risk was even greater (OR: 4.48) when the affected proband had tremor-dominant or mixed PD.34 Twelve subjects had both ET and PD phenotypes. The authors concluded that ‘‘in certain families ET and PD are genetically related probably sharing common hereditary 33 11.7.14 2:25:18 PM パーキンソン病患者の健康関連の生活の質に対する 非運動症状の影響 The Impact of Non-Motor Symptoms on Health-Related Quality of Life of Patients with Parkinson’s Disease *, ** Pablo Martinez-Martin, MD, PhD, Carmen Rodriguez-Blazquez, BS, Monica M. Kurtis, MD, and K. Ray Chaudhuri, MD, FRCP, DSC, on Behalf of the NMSS Validation Group * Area of Applied Epidemiology, National Centre of Epidemiology and CIBERNED, Carlos III Institute of Health, Madrid, Spain Scientific Management, Alzheimer Disease Research Unit, CIEN Foundation, Carlos III Institute of Health, Alzheimer Center Reina Sofia Foundation, Madrid, Spain ** 背景:パーキンソン病患者では,非運動症状により,健 結果:患者からの訴えが最も高頻度に認められた非運動 康関連の生活の質(health-related quality of life; 症状は,夜間頻尿(患者集団の 68.4%) ,疲労(65.9%) , HRQoL) が 低 下 す る。 本 研 究 で は,Non-Motor 流涎(56.7%)であった。 (1)NMSS 総スコアと PDQ- Symptoms Scale(NMSS)を用い,パーキンソン病患 39 Summary Index(SI)との相関係数(r s = 0.70)は, 者の HRQoL に対する非運動症状の影響を評価した。 NMSS 総スコアと SCOPA(運動機能)スコアの相関係 方法:パーキンソン病患者 411 例を対象とした国際的 (2)NMSS 総スコアは, 数(r s = 0.58)よりも高かった。 な多施設共同の横断的研究において,臨床評価尺度 PDQ-39 のすべての評価領域と高度~中程度の相関を示 〔Hoehn and Yahr 分類,Scales for Outcomes in 。 (3)NMSS 総スコアは,PDQした(r s=0.60 ~ 0.38) Parkinson’ s Disease(SCOPA) (運動機能) 〕および 39 SIで評価したHRQoLの最も強力な予測因子であった。 HRQoL 評価尺度〔Parkinson’ s Disease Questionnaire-39 NMSS の各評価領域について,症状のある患者は,症状 items(PDQ-39) , EuroQol Five Dimensions(EQ-5D) 〕 のない患者よりも HRQoL スコアが有意に不良であった。 に加え,NMSS を用いて評価を行った。また,非運動 考察:本研究は,我々の知る範囲において,パーキンソ 症状の有症率も NMSS を用いて評価した。ノンパラメ ン病患者の HRQoL に対する非運動症状の影響を総合 トリック統計を用い,NMSS および SCOPA(運動機能) 的に評価した最初の研究である。本研究の結果,非運 M A 評価尺度との相関,また,NMSS R T I N E Z - M A R T I N E T A L . と HRQoL の各評価 R Tは I N全 E 体とし Z - M A Rて T I運 N 動 E症 T 状 A Lよりも . 動M症A 状 顕著な影響を TABLE 3.examination, Percentage ofSCOPA-motor patients reporting each SCOPA-motor examination, SCOP SCOPA-motor complicaHRQoL に及ぼし,また,非運動症状の進行がパーキン non-motor symptom measured by the NMSS tions, and the NMSS total score w tions, and the NMSS total as score were included as inソン病患者における 低下の重要な要因となるこ の HRQoL スコアの差を推定した。HRQoL の予測因子 dependent dependent variables, once interact variables, onceHRQoL interaction and colinearity Patients* Patients* were excluded. The corresponding were excluded. The corresponding models accounted とが明らかになった。 について重回帰分析で検討した。 for 53% (EQ-5D) and 59% (PDQfor 53% (EQ-5D) Items and 59% (PDQ-39) ofNthe variance. % Items N % NMSS score had the strongest influ NMSS score had the strongest influence on HRQoL as 1. Light-headedness 167 40.6 1. Light-headedness 167 40.6 measured by the PDQ-39, where measured by the PDQ-39, whereas considering EQ- 9.2 2. Fainting 38 2. Fainting 38 9.2 5D, both SCOPA-motor examinati 5D, 3.both SCOPA-motor examination and NMSS were Daytime sleepiness 195 47.4 3. Daytime sleepiness 195 47.4 Movement Disorders, Vol. 26, No. 3, 2011, pp. 399–406 the strongest predictors and almos the strongest In the65.9 4. Fatigue predictors and almost equivalent. 271 4. Fatigue 271 65.9 5. Difficulty falling asleepthe NMSS domains207 5. Difficulty falling asleep 207 50.4 models that included the NMSS do models that included as independ-50.4 6. Restless legs 131andScale,Parkinson’ legs 131 31.9 ent variables, mood/apathy, sleep/ Key Word 6. Restless ent variables, mood/apathy, sleep/fatigue, miscel-31.9 非運動症状,健康関連の生活の質,パーキンソン病,評価,Non-Motor Symptoms s surroundings 34.3 M7.ALost Rdomains Tinterest I N E inZ were - M A the R T most I N Esignificant T A L141 . factors for 34.3 M7.ALost R Tinterest I N E inZ surroundings - M A R T I N E T A L141 . laneous domains were the most si laneous Disease items,EQ-5D 8. Lack motivation 179 43.6 8. Lack motivation Questionnaire-39179 43.6 both the PDQ-39 SI and the EQ-5D both9.the PDQ-39 SI and the EQ-5D index, Feel nervous3.examination, 208 accounting 9. Feel nervous3. Percentage of patients reporting 208 TABLE Percentage ofSCOPA-motor patients reporting each 50.6 SCOPA-motor examination, SCOP TABLE each 50.6 SCOPA-motor complicafor 50% and 38% of the variance, Table 3 for 50% and 38% of the variance, respectively. NMSS において各非運動症状を報告した患者の割合 10. Seem sad 204 49.6 10. Seem sad 204 49.6 non-motor symptom measured by the NMSS non-motor symptom as measured by the NMSS tions, and the NMSS total score w tions, and the NMSS total as score were included as in-32.1 11. Flat mood 132 11. Flat mood 132 32.1 dependent variables, once interact dependent variables, once interaction and colinearity 12. Difficulty experiencing pleasure 121 Patients* 29.4 12. Difficulty experiencing pleasure 121 Patients* 29.4 were excluded. TheDiscussion corresponding were corresponding models 13. excluded. Hallucinations TheDiscussion 72 accounted 17.5 13. Hallucinations 72 17.5 Delusions 40 9.7 14. Delusions Items 40 9.7 for 53% (EQ-5D) and 59% (PDQfor 14. 53% (EQ-5D) the variance. % Items and 59% (PDQ-39) ofN N % This multicenter, international This multicenter, efforton aimed as at17.5 15. Double vision 72isHRQoL 15. Double vision 72 17.5 NMSS score had the strongest influ NMSS score had the international strongest influence 16. 222 54.0 1. Concentration Light-headedness 167 40.6 1. Concentration Light-headedness 167 40.6 evaluating the impact of non-moto 16. 222 54.0 evaluating the the impact of non-motor symptoms, considmeasured by the PDQ-39, where measured by PDQ-39, whereas considering EQForget things or events 209 2.as Fainting 38 9.2 2. Forget Faintingthings or events 38 9.2 17. 209 50.9 ered as a whole, on HRQoL in ered17. aSCOPA-motor whole, on HRQoL in Parkinson’s disease50.9 5D, both SCOPA-motor examinati 5D, both examination and 18. Forget tosleepiness do things 172NMSS were47.4 41.8 3. Daytime 195 3. Forget Daytimetosleepiness 195 47.4 18. do things 172 41.8 patients. The strong points of this c patients. The strong points of this cross sectionalIn study the strongest predictors and almos the strongest the65.9 19. 178 56.7 4. Saliva Fatigue predictors and almost equivalent. 271 4. Saliva Fatigue 271 65.9 19. 178 56.7 include the large sample of patients include the large patients from207 several coun-50.4 20. 121 29.4 5. Swallowing Difficulty fallingsample asleepthe of 5. Swallowing Difficulty falling asleep 207 50.4 20. 121 29.4 models that included the NMSS do models that included NMSS domains as independtries, across all ages, and HY stage tries, across all ages, and HY stages, as well as the use 21. Constipation 202 49.1 6. Restless legs 131 31.9 6. Constipation Restless legs 131 31.9 21. 202 49.1 ent variables, mood/apathy, sleep/ ent variables, mood/apathy, sleep/fatigue, and miscelUrgency 224 54.5 Lost interest incomprehensive, surroundings 34.3 7. Urgency Lost interest in surroundings 141 34.3 of a validated, comprehensive, d 22. 224 54.5 of 22. a7. validated, disease141 specific nonlaneous domains were the most si laneous domains were the most significant factors for 13,14 23. 224 54.5 8. Frequency Lack motivationmeasure such as the NMSS. 179 8. Frequency Lack motivation 179 43.6 23. 224 54.5 motor symptoms measure such as t motor symptoms This43.6 both the PDQ-39 SI and the EQ-5D both the PDQ-39 SI and the EQ-5D index, accounting 24. 281 68.4 9. Nocturia Feel nervous 208 50.6 9. Nocturia Feel nervous 208 50.6 24. 281 68.4 scale is appropriate for estimating scale50% is appropriate for estimating the impact of nonfor 50% and 38% of the variance, for and 38%inof 25. Seem Altered interest sexthe variance, respectively. 135 32.8 10. sad 204 49.6 10. 204 49.6 25. Seem Alteredsad interest in sex 135 32.8 motor symptoms on HRQoL becau motor symptoms on HRQoL because each symptom is 26. Flat Problems 115 28.0 11. mood having sex 132 32.1 11. mood having sex 132 32.1 26. Flat Problems 115 28.0 detected and weighed by frequenc detected weighed pleasure by frequency and121 severity, thus29.4 27. Difficulty Painand experiencing 162 39.4 12. 12. experiencing pleasure 121 29.4 27. Difficulty Pain 162 39.4 Discussion Discussion 28. Hallucinations Tastetheir or smell 171 41.6 13. 72 17.5 13. 72 17.5 capturing their global burden for p 28. Hallucinations Taste or smell 171 41.6 capturing global burden for patients. 29. Delusions Weight 122 14. 40of the non- 29.7 9.7 14. 40 9.7 29. Delusions Weight change 122 29.7 First, our results emphasize the First, our change results emphasize the impact This multicenter, international This multicenter, 30. Double Excessive sweating international effort125 15. vision 72is aimed at17.5 15. vision 72 17.5 30. Double Excessive sweating 125 30.4 motor symptoms accumulation on motor symptoms accumulation on the HRQoL show-30.4 16. Concentration 222 16. Concentration 222 54.0 evaluating the impact of non-motor evaluating the impact of non-motor symptoms, consid-54.0 ing a close association between nu ing a close association between number of non-motor Forget things 1ororevents 209 17. Forgetscoring things 1ororevents 50.9 ered as a whole, on HRQoL in ered17. as a scoring whole, on inNMSS. Parkinson’s disease50.9 *Patients moreHRQoL points on the *Patients more points on the NMSS. 209 symptoms and worse HRQoL. Th symptoms and worse HRQoL. Three symptoms such41.8 *NMSS18.でForget 1 ポイント以上のスコアを付けた患者。 18. Forget to do things 172 to do things 172 41.8 patients. The strong points of this c patients. The strong points of this cross sectional study 19. Saliva 178 56.7 19. Saliva 178 56.7 include the large sample of patients include the large sample of patients from121 several coun-29.4 20. Swallowing 20. Swallowing 121 29.4 tries, across all ages, andofHY stageS tries, across allthan ages,for and stages, as(0.70 well as the useP49.1 21. Constipation 202 vs. total score SCOPA-Motor 0.58; ¼ 21. Constipation 202 vs. 0.58; P49.1 total score than for SCOPA-Motor (0.70 ¼ TABLE 4. Correlations NMSS, TABLE 4. Correlations ofHY NMSS, SCOPA-Motor, and UrgencyHigh comprehensive, 22. UrgencyHigh correlation coefficients 224(from 0.51 54.5 of a validated, comprehensive, d of 22. a validated, disease224 specific non-54.5 0.015). correlation coefficients (from 0.51 to HRQL measures 0.015). to HRQL measures 23. Frequency 224 13,14 54.5 23. Frequency 224 54.5 motor symptoms measure such as t motor symptoms measurebetween such as total the NMSS. Thisand 0.61) were observed NMSS scores 0.61) were observed between total NMSS scores and 24. Nocturia 281 68.4 24. Nocturia 281 68.4 PDQ-39 PDQ-39 theEQ-5D EQ-5D scale is appropriate for estimating scale appropriate for estimating impact ADL, of nontheisAltered following domains: Mobility, EmotheAltered following domains: Mobility, ADL, EmoSI 25. interest PDQ-39 in sex 135 32.8 25. interest PDQ-39 in sex 135 32.8 SI Index VAS motor symptoms on HRQoL becau motor symptoms on HRQoL because each symptom isand tional wellbeing, Cognition, Communication, tional wellbeing, Cognition, Communication, and 26. Problems having sex 115 28.0 26. Problems having sex 115 28.0 34 11.7.14 2:25:21 PM NMSS total score 0.70 NMSS total 0.70 NMSS �0.57 �0.37 detected and weighed by frequenc detected and weighed As by expected, frequency and severity, thus 27. Painscore 162 39.4 Bodily discomfort. domain mood/ 27. Pain discomfort. As expected, NMSS 162 domain mood/ 39.4 Bodily TABLE 3. Percentage of patients reporting each 領域について,非運動症状を伴う患者と伴わない患者と non-motor symptom as measured by the NMSS 34 #MD5-1.indb Abstract M A R T I N E Z - M A R T I N E T A L . Table 5 NMSS 各評価領域の症状の有無による 評価尺度スコア TABLE 5. HRQoL scales scores in patients with and withoutHRQoL symptoms in each NMSS domain NMSS domains Cardiovascular Sleep/fatigue Mood/apathy Perceptual problems/hallucinations Attention/memory Gastrointestinal Urinary Sexual dysfunction Miscellaneous Groups of patients (n) PDQ-39 SI EQ-5D index EQ-5D VAS With symptoms (173) No symptoms (238) Pa With symptoms (356) No symptoms (54) Pa With symptoms (310) No symptoms (100) Pa With symptoms (123) No symptoms (288) Pa With symptoms (296) No symptoms (115) Pa With symptoms (302) No symptoms (109) Pa With symptoms (338) No symptoms (73) Pa With symptoms (177) No symptoms (234) Pa With symptoms (99) No symptoms (312) Pa 32.45 6 17.85 24.79 6 15.66 <0.0001 30.11 6 16.80 14.48 6 11.57 <0.0001 31.31 6 16.87 17.64 6 13.01 <0.0001 36.89 6 17.25 24.22 6 15.47 <0.0001 30.65 6 16.93 21.27 6 15.37 <0.0001 31.02 6 17.84 19.76 6 10.92 <0.0001 29.52 6 17.44 21.12 6 12.97 0.0002 29.71 6 15.97 26.75 6 17.71 0.03 30.38 6 17.36 20.61 6 13.54 <0.0001 0.48 6 0.37 0.62 6 0.32 0.0001 0.52 6 0.35 0.79 6 0.20 <0.0001 0.50 6 0.35 0.74 6 0.27 <0.0001 0.38 6 0.39 0.63 6 0.30 <0.0001 0.52 6 0.36 0.66 6 0.30 0.0005 0.49 6 0.36 0.74 6 0.23 <0.0001 0.54 6 0.36 0.66 6 0.28 0.001 0.53 6 0.34 0.58 6 0.35 0.09 0.50 6 0.36 0.73 6 0.25 <0.0001 61.49 6 21.23 65.17 6 23.01 0.05 61.75 6 21.77 75.74 6 22.45 <0.0001 61.66 6 22.01 70.51 6 21.21 0.0002 57.15 6 25.19 66.40 6 20.39 0.0004 61.35 6 22.21 69.52 6 21.58 0.0005 61.00 6 22.48 71.04 6 20.16 <0.0001 62.82 6 22.56 67.38 6 20.87 0.13 63.17 6 21.92 63.94 6 22.65 0.53 61.61 6 22.32 70.02 6 21.20 0.0006 a a Mann-Whitney test. Benajmini-Hochberg adjustment, P << 0.026. Mann-Whitney 検定。Benjamini-Hochberg 補正,p 0.026。 EQ-5D, EuroQol five dimensions; PDQ-39, Parkinson’s disease questionnaire-39 items; NMSS, non-motor symptoms scale; VAS, visual analogue scale. EQ-5D = EuroQoL Five Dimensions,PDQ-39 = Parkinson’ s Disease Questionnaire-39 items,NMSS = Non-Motor Symptoms Scale,VAS =視 覚的アナログ尺度 40 40 20 60 80 symptoms by patients to their Parkinson’s disease11; NMSS (2) lack of attention to non-motor symptoms by health professionals possibly owing to non-awareness and or time constraints in clinics, or the large number of nonmotor symptoms per patient32; (3) non-motor symptoms may be refractory to current treatment; and (4) the differential importance given by the individual patient to each symptom. 20 0 20 40 60 80 TABLE 6. Multiple linear regression models of HRQoL 0 scales 0 50 100 250 t Sig. 5.55 13.64 4.81 4.15 0.000 0.000 0.000 0.000 9.24 9.11 8.74 2.71 0.000 0.000 0.000 0.000 0.59 (23.76) 0.52 0.20 0.17 .5 1 PDQ-39 SI model (Constant) NMSS total SCOPA-motor complications SCOPA-motor examination EQ-5D index model (Constant) SCOPA-motor examination NMSS total SCOPA-motor complications Adjusted Standardized 200 R2 150 beta 0.53 -.5 0 (0.83) 0.38 0.37 0.12 SCOPA, scales for outcomes in Parkinson’s disease; EQ-5D, EuroQol five dimensions; PDQ-39, Parkinson’s disease questionnaire-39 items; NMSS, non-motor symptoms scale; VAS, visual analogue scale. -1 .5 0 -1 -.5 EQ-5D Index 1 0 PDQ-39 SI 60 80 the present and past studies.14 Nonetheless, NMSS does not assess personal SCOPA-MOTOR relationships, social aspects and communication, aspects evaluated by the PDQ-39 that may be influenced by non-motor and motor symptoms. Regarding the SCOPA-Motor, the highest correlation coefficients were reached with the EQ-5D Index, probably related to the fact that mobility and activities of daily living are heavily weighed in this generic HRQoL scale. Parkinson’s disease patients with prevalent symptoms in any of the NMSS domains showed significantly worse PDQ-39 scores than those with no nonmotor symptoms. NMSS total score was the best predictor of HRQoL as measured by PDQ-39, followed 20 60 0 by SCOPA-motor examination and40complications sub- 80 scales, which had considerably weaker (<50%) influence. Most of the patient population in the study was on dopaminergic therapy and, therefore, the impact of the motor manifestations may be neutralized by effective antiparkinsonian effect. This may not be the case with non-motor symptoms as in spite of the fact that dopaminergic therapy is possibly effective against some non-motor symptoms,36 the burden and impact of non-motor symptoms still appears to be very significant. Potential reasons for this are: (1) many nonmotor symptoms go by untreated due to non-declaration, sometimes due to lack of association of these 0 50 100 150 200 250 Figure 評価尺度と臨床評価尺度との相関を示す散布図。SCOPA = Scales for Outcomes in Parkinson’ s Disease,EQ-5D = EuroQol 404 1 HRQoL Movement Disorders, Vol. 26, No. 3, 2011 Five Dimensions,PDQ-39 = Parkinson’ s Disease Questionnaire-39 items,NMSS = Non-Motor Symptoms Scale。 [カラーの図は wileyonlinelibrary. com のオンライン版で閲覧可能] 。 #MD5-1.indb 35 35 11.7.14 2:25:23 PM パーキンソン病の運動症状と発症時年齢との関連 The Motor Phenotype of Parkinson’s Disease in Relation to Age at Onset * Mirdhu M. Wickremaratchi, PhD, MRCP, M. Duleeka W. Knipe, BSc, MPH, B.S. Dwarakanath Sastry, MBBS, FRCPI, FRCP, Elizabeth Morgan, BSc RGN, Anne Jones, RGN, Rachel Salmon, BSc, RGN, Richard Weiser, FRCP, Maralyn Moran, BN, RGN, Debbie Davies, BSc, RGN, Louise Ebenezer, RGN, MSc, Sandip Raha, BSc, MBBS, Neil P. Robertson, MD, FRCP, Christopher C. Butler, FRCGP, MD, Yoav Ben-Shlomo, MD, PhD, and Huw R. Morris, FRCP, PhD * Department of Neurology, School of Medicine, Cardiff University, Cardiff, United Kingdom 背景:パーキンソン病(Parkinson’ s disease; PD)は はジスキネジアの発現に関する強力な予測因子であり, 不均一な疾患であり,発症時年齢が臨床像の違いに重 発症時年齢が低いほどジスキネジアのリスクが高くなっ 要な影響を及ぼす可能性がある。大半の先行研究は, た。潜在的な交絡因子(罹病期間,L—ドパ投与量,L— 臨床診断された一連の患者集団を対象とし,様々な年齢 ドパ投与期間)を考慮した多変量解析では,発症時年齢 カットオフ値を使用している。 が低い場合(55 歳未満)に L—ドパ誘発性ジスキネジア 方法:地域社会ベースの PD 患者および地域中核病院に の発現が予測された(発症時年齢< 45 歳のオッズ比: 紹介された PD 患者で構成される計 358 例を対象に, 2.1,95% CI:1.0 ~ 4.8,発症時年齢< 55 歳のオッ 臨床像と発症時年齢との関連を検討した。 ズ比:3.8,95% CI:1.8 ~ 8.0) 。病因となる parkin 結果:発症時における振戦の所見は,発症時年齢が 45 または PINK1 変異を保有する早期発症型 PD 患者は 70 歳未満の患者(早期発症型 PD)に比べ,発症時年齢が 例中わずか 2 例(2.9%)であり,早期発症型 PD と晩 65 歳以上の患者で 2 倍多くみられ,発症時年齢が高く 期発症型 PD との臨床的な違いをこれらの遺伝子変異の 。ジ なるほど多くみられた(傾向性に関し p ≦ 0.004) 有無で説明することはできなかった。 ストニアは早期発症型 PD 患者の 60%にみられ,また, 考察:本研究では,早期発症型 PD と晩期発症型 PD と 発症時年齢との曲線相関が認められ(三次関数モデル の臨床的な違いが明らかになり,この知見は診断および ,48 歳未満で発症した患者 対 線形モデル,p = 0.01) 治療において重要な意味をもつと考えられる。 のリスクが最も高かった。本研究において,発症時年齢 Movement Disorders, Vol. 26, No. 3, 2011, pp. 457–463 0 20 % 40 60 80 Key Word 運動症状,発症時年齢,若年発症,早期発症,パーキンソン病 <45 45-54 Tremor* Gait* 55-64 >=65 Akinetic Rigid* Figure 1 各 PD 発症時年齢群における発症時症状の有症率 〔* 傾向性および異質性に関して有意な p 値が認められる(各発 症時症状について,傾向性に関し p < 0.005) 〕 。 36 #MD5-1.indb 36 11.7.14 2:25:24 PM common than in later onset PD (at onset, within the with ainsignificant trend for diminution of LID cases the frequency of amotor symptoms or with increasing ageexcept at onset 5). Adystonia linear model LFADLDS scores, for (Table peak dose (P ¼ was the best fit foratthis relationship withalthough no evidence 0.04), and tremor onset (P ¼ 0.045) this that higher order polynomials significantly improved may have been a Type 1 error due to multiple testing this. (Supporting Information Table S4). There was also a significant difference in the proportion of the waking dayofspent in a dyskineticAbstract state Effects Genotype between the onset groups (P ¼ 0.001; Table 4; SupTwo out of 70 (2.9%) of patients with EOPD had porting Information Table S5). Of those patients having compound heterozygous mutations in parkin and none reported LID (n ¼ 80), the median LFADLDS score had pathogenic mutations in PINK1. Excluding these was 8.5 (interquartile range 5–13.5), with no differenpatients did not significantly alter our findings. ces between onset groups. Younger onset patients in this study had both longer disease and L-DOPA FIG. Prevalence presenting symptom in each PD age at onset first 1.two yearsof and exercise induced dystonia—all group [*Significant P-value for trend heterogeneity (P-values < P values <0.025, Table 3). and During treatment with 0.005 trend, each onset symptom)]. L-DOPA, off period (including early morning) and peak dose dystonia were also significantly more common in early onset (P PDvalues (P � 0.01). EarlyThe dystonia treatment duration < 0.001). mean (at Lonset or in the first two years of treatment) strongly DOPA treatment duration and dose was 7.2 years and related onset age group [20% and (<55) (�55)]. 470 mg to in the EOPD 4.5and years4.3% and 418 mg EOPD patients were nearly three times more likely to in the later onset patients. We examined whether the suffer from dystonia compared to could later onset disease greater frequency of LID in EOPD be explained (OR P <0.0001) having adjusted for sex. This by the2.8, confounding effects of disease duration, duration observed risk was even more marked when looking at of treatment with L-DOPA and total L-DOPA dose at disease onset before the age of 55 (OR 5.3, time of assessment. All four factors were independently associated with an increased risk of developing LID Discussion (Table 5). Following multivariable age at onset <45 Table 2 発症時年齢群別に示した PD 患者の発症時症状 TABLE Presentations onset in PD patients by onset groupspecific clinical variation in was still associated with an odds2.ratio of 2 but atthis This study has identified finding is consistent with chance (P ¼ 0.07). However, PD, related to the age at onset. Most of the features P value in our analysis Allofn (%) age at onset age 45–54 at onset showed simple linear (either or Onset group <45 yr n<55, (%) yr n (%) 55–64 yr a n (%) � 65 yr nchange (%) P valueincreasing for trend remained a significant factor in the development of dysdecreasing) with age suggesting no obvious cut-point Presentation kinesia, independent of confounding factors (OR ¼ for the definition of early onset disease, except for dysTremor 175 (49) 21 (31) 41 (40) 53 (61) 66 (62) <0.001 <0.0001 3.8, CI 1.8–8.0) (Table 5). tonia. This feature did appear to show highest risk in Akinetic-rigid 156 (44) 46 (68) 58 (56) 26 (30) 26 (27) <0.001 <0.0001 the(7) possible effects the youngest age group until around0.04 48 years of0.004 age GaitWe evaluated 24 1 (1) of referral4 bias. (4) 8 (9) 11 (11) Our community-based cases were significantly older at at which point older age was associated with a pro2 Chi-squared tests for heterogeneity trend. 異質性および傾向性に関するχ 検定。 time of assessment (72 vs.and 61 years, P < 0.0001), had gressive reduction in risk. In common with the work older age at onset (64 vs. 51, P <0.0001) and had a of Lohmann and coworkers, these differences were shorter disease duration (7 vs. 9 years, P ¼ 0.0009) not due to the presence of pathogenic mutations in 459 Movement Disorders, Vol. 26, No. 3, 2011 Table 3 発症時年齢群別のジストニアの特徴 TABLE 3. Characteristics of dystonia by onset group Onset group All n (%) <45 yr n (%) 45–54 yr n (%) 55–64 yr n (%) � 65 yr n (%) P value P value for trend Presence of Dystonia Dystonia: At Onset In first 2 years Exercise induced Pre-treatment morning Off period dystonia Peak dose dystonia Treatment related Non-dose related 125 (39) 37 (59) 52 (58) 26 (30) 10 (12) <0.001 <0.0001a 13 7 12 1 19 7 13 4 20 (20) 9 (10) 15 (15) 0 21(20) 4 (4) 7 (7) 19 (15) 5 (6) 4 (5) 5 (6) 0 4 (5) 2 (2) 4 (5) 14 (17) <0.001 0.02 <0.001 0.47 <0.001 0.03 <0.001 0.22 <0.0001a 0.0025 <0.0001a 0.87 <0.0001a 0.0118b 0.0001 0.65 41 21 33 2 44 15 26 34 (12) (6) (9) (1) (13) (4) (8) (12) (20) (11) (18) (2) (30) (11) (21) (9) 3 1 1 1 (3) (1) (1) (1) 0 2 (2) 2 (2) 6 (7) 異質性および傾向性に関するχ Chi-squared tests for heterogeneity and検定。 trend. a <55 vs. �55 heterogeneity test P value (Dystonia < 0.001, At Onset < 0.001 Exercise induced < 0.001, Off-period < 0.0001). a p 値(ジストニア:p < 0.001,発症時のジストニア:p < 0.001,運動誘発性ジストニア:p < 0.001, 55 歳未満 対 55 歳以上,異質性検定の b <45 vs. �45 heterogeneity test P value (Peak dose ¼ 0.004) 2 「off」期ジストニア:p < 0.0001) 。 b 45 歳未満 対 45 歳以上,異質性検定の p 値(peak-dose ジストニア:p = 0.004) 。 460 Movement Disorders, Vol. 26, No. 3, 2011 M O T O R P H E N O T Y P E O F E A R L Y O N S E T P D Table 4 TABLE 4.発症時年齢群別に示したジスキネジアの有無と重症度 Presence and severity of dyskinesia by onset group Onset group <45 yr n (%) 45–54 yr n (%) 55–64 yr n (%) ¼ 65 yr n (%) P-value P-value for trend <45 vs. ¼45 P-value <55 vs. ¼55 P-value (23) 28 (42) 32 (31) 13 (15) 7 (7) <0.001 <0.0001 <0.001 <0.001 (56) (30) (6) (8) 10 14 3 1 20 6 2 4 9 (69) 2 (23) 0 1 (8) 6 (86) 1 (14) 0 0 0.12 0.01 0.217 All n (%) Dyskinesia present 80 Presence of Dyskinesia between: 1–25% of waking day 45 26–50% of waking day 24 51–75% of waking day 5 76–100% of waking day 6 (36) (50) (11) (4) (63) (19) (6) (13) 2 trend. Chi-squared tests for heterogeneity and 異質性および傾向性に関するχ 検定。 TABLE 5. The effects of age of onset (for patients with disease onset <45 and <55 years) on LID with and without adjustment for disease and L-dopa treatment duration and L -dopa dose (two models) Univariablea Age at onset < 45 #MD5-1.indb Male Disease duration quartiles (range) 1 (0.5–4.0) 2 (4.0–7.3) 3 (7.4–12.2) 4 (12.3–38.7) 37 p–value for trend Multivariableb Odds ratio 95% CI P-value Odds ratio 95% CI P-value 2.9 0.7 1.6, 5.1 0.4, 1.1 <0.0001 0.13 2.1 0.6 1.0, 4.8 0.3, 1.2 0.07 0.18 1.0 0.8 6.7 3.9 0.1, 4.6 1.3, 33.8 0.7, 21.2 0.76 0.02 0.12 0.00411.7.14 1.0 1.4 19.3 22.6 0.3, 6.3 5.7, 65.9 6.6, 77.0 0.69 <0.0001 <0.0001 <0.0001 37 2:25:26 PM 薬物未投与のパーキンソン病患者における衝動性と強迫性 Impulsivity and Compulsivity in Drug-Naïve Patients with Parkinson’s Disease *, ** Angelo Antonini, MD, Chiara Siri, PsyD, Gabriella Santangelo, PhD, Roberto Cilia, MD, Michele Poletti, PsyD, Margherita Canesi, MD, Alessandra Caporali, PsyD, Francesca Mancini, MD, Gianni Pezzoli, MD, Roberto Ceravolo, MD, Ubaldo Bonuccelli, MD, and Paolo Barone, MD, PhD * Department of Neurology, Parkinson Institute, Istituti Clinici di Perfezionamento, Milan, Italy Department for Parkinson’s Disease, IRCCS San Camillo, Venice and University of Padua, Venice, Italy ** 背景:パーキンソン病(Parkinson’ s disease; PD)患 items(GDS-15)で評価〕と全般的な認知機能状態も 者ではドパミン補充療法中の異常反復行動が報告され 評価した。また,ICD の発現頻度を健常対照群と比較し ており,衝動性など,素因となる個人特性との関連が指 た。 摘されている。しかし,これまでのところ,ドパミン補 結果:スクリーニングの結果,PD 患者の 17.5%は, 充療法開始前の PD 患者においては,衝動性および強迫 MIDI(17/103 例)および SOGS(1/103 例)におい 性症状は検討されていない。我々は以前,イタリア人コ て 1 つ以上の ICD に関して陽性であったが,DSM-IV ホ ート の 20 % に 衝 動 制 御 障 害(impulse control 基準に基づく障害のある者はいなかった。これらの発現 disorder; ICD)があることを報告している。 頻度は健常対照群とほぼ同じであった。ICD を伴う PD 方法:新規に診断され,薬物投与を受けていない一連の 患者は, BIS-11 の注意衝動性サブスケール (15.2 ± 4.8 PD 患者 103 例(平均年齢:60.5 ± 9.2 歳,平均罹病 対 18.7 ± 4.9,p = 0.007)および MOCQ/R の疑惑 期間:15.4 ± 15.3 ヵ月)を対象に,強迫的な性行動, (Doubting)サブスケール(0.67 ± 1.1 対 1.5 ± 1.2, 強 迫 買 い 物 症, 間 欠 性 爆 発 性 障 害〔Minnesota p = 0.007) の ス コ ア が 高 い 傾 向 に あ っ た。 ま た, Impulsive Disorders Interview(MIDI)で評価〕 ,病的 GDS-15 と BIS-11 との間に正の相関が認められた。 賭博〔South Oaks Gambling Screen(SOGS)で評価〕 結論:治療開始前の早期 PD 患者で,我々が過去に行っ の ス ク リ ー ニ ン グ を 行 っ た。 衝 動 性 は Barratt た調査の健常対照群の結果と同様,ICD がかなり高い割 Impulsiveness Scale(BIS-11) ,強迫症状は Maudsley 合で認められた。また,衝動性と抑うつとの関連が認め Obsessional-Compulsive Questionnaire(MOCQ/R) られた。ドパミン補充療法の開始前には,詳細な行動評 で評価した。抑うつ〔Geriatric Depression Scale 15 価を行うことが推奨される。 Movement Disorders, Vol. 26, No. 3, 2011, pp. 464–468 Key Word パーキンソン病,薬物未投与,衝動制御障害,衝動性,強迫性 38 #MD5-1.indb 38 11.7.14 2:25:26 PM mental state examination corrected score; FABc, frontal assessment battery corrected score. Data Analysis H&Y stage; groups did not show any difference in other clinical features such as side of onset and onset symptoms (tremor or rigidity). As shown by t-test pared ICD positive and negative PD. MoreAbstract analysis, no difference was found also in the global ompared PD patients with a cohort of hiscognitive performance, frontal-lobe functions, and thy controls (HC). depression, according to the MMSE, FAB, and GDSscores and normally distributed variables 15 scores, respectively. In detail, after applying correcared by means of t-test. Correlations were N T O N I N I E T A L . tion for age and education, MMSE was found within means of Spearman’sA correlation test. Frethe range ofclinical, normal values (established cut-off of ¼ PD 24)patients with ere compared by means of v2 test orTABLE Fish- 1. Demographic, and general cognitive features in all PD and patients butimpulse one (MMSEc score 23.7; ICD Test, as appropriate with respect Table to the1 衝動制御障害の有無に基づく PD 患者の背景,臨床的特徴と全般的認知機能 without control disorders negative group), while FABc scores below the estabof events. Features Total patients (n ¼ 103)(13.4) was ICD positive (nin ¼ 18) ICD negative (n ¼ 85) P value lished cut-off recorded sixteen patients l Analysis was carried out using SPSS for (mean score 12.2 6 1.3; 20%15in(83%) ICD negative group 52 (61%) Release 10.0 (SPSS, Men, Chicago, n (%) IL). Results 67 (65%) 0.06 vs. 60.5 11% d with significance set Ageat P < 0.006 with (9.2)in ICD positive group). 58.3 (9.7)Mild to moderate 60.9 (9.1) 0.40 Education comparisons. 11.5 (4.6) (GDS-15 score 6–10) 13.4 (4.7) 0.06 depression was found in 25 PD 11.1 (4.5) correction for multiple Disease duration (mm) 15.4 (15.3) 19.3 (16.5) 14.6 (15.0) 0.25 subjects (24%), and severe depression (GDS-15 > 10) th P < 0.05 but not reaching significance UPDRS II 6.9 (4.1) 7.1 (3.5) 6.9 (4.4) 0.89 was16.4 reported in 6 PD (6%), equally ported as trends. UPDRS III (8.7) 16.5 (8.1) distributed in the 16.4 (8.9) 0.95 two 1.5 subgroups. H&Y stage (0.5) 1.4 (0.5) 1.6 (0.5) 0.14 (1.9) 27.4 (1.5) 0.07 We28found a positive significant correlation between 28.3 (1.9) ResultsMMSEc FABc 15.6 (2.1) 15.2 (2.1) 15.7 (2.1) 0.36 GDS-15 scores and BIS 11 total score (r ¼ 0.27; P ¼ GDS-15 4.4 (3.5) 5 (4) 4.3 (3.5) 0.50 0.005) and a trend toward significance for the correlaphic and clinical features of PD patients tion between GDS-15 and lack of planning subscale detailed in Table 1.Values Using the asscreening 値は平均値(SD) 。 (SD). are given mean 2 P ICD values between ICD positive versus pnegative are tcalculated 2-tailed t-test, considering while men prevalence Chi-square (r ¼ 0.28; P ¼ using 0.01). When the using two sub- test. teen PD subjects (17.5%) resulted positive p 値はχ 陽性群と陰性群を比較した 値は両側 検定で算出した。男性の割合に関する 検定で算出した。 MMSEc, mini mental state examination corrected score; FABc, frontal assessment battery corrected score. groups, the same trend between GDS-15 and BIS 11 st one abnormal behavior atMini theMental MIDI MMSEc = State Examination 補正後スコア,FABc = Frontal Assessment Battery 補正後スコア total score was found (ICD positive r ¼ 0.48 P ¼ s) or SOGS (1 patient), with compulsive buy0.04; ICD negative r ¼ 0.28; PH&Y ¼ 0.03). ompulsive sexual behavior most commonly stage; groups did not show any difference in Data Analysis 0.7%). The remaining subjects were classified other clinical features such as side of onset and onset gative (n ¼ 85). However means ofICD clini-positive and negative PD. Moresymptoms (tremor or rigidity). As shown by t-test Webycompared w based on DSM-IVover, criteria, none of the no difference TABLE Numberof(%) patients with ICDs and was found also in the global we compared PD patients with 2. a cohort his-of PD analysis, Table 2 ICDdomain d a clinically significanttorical disorder. のある distribution PD 患者数(%)と分布 cognitive performance, frontal-lobe functions, and healthy controls (HC). ces in gender did notTesting reach scores significance depression, according to the MMSE, FAB, and GDSand normally distributed variables ICDs scales N total 15 scores, respectively. In detail, after applying correc. were compared by means of t-test. Correlations were tion for age and education, MMSE was found within ent explosive disorderassessed showedbyameans trend offorSpearman’s SOGS correlation test. Fre1 (0.9%) the range of normal values (established cut-off ¼ 24) means uency in men (8/67 quencies vs. 0/36,were P ¼compared 0.03). by MIDI tot of v2 test or Fish17 (17.5%) in all PD patients Compulsive 11 but (11%)one (MMSEc score 23.7; ICD er’satExact appropriate withbuying respect to the subjects were positive moreTest, thanasone Compulsive sexual behavior 11 (11%)FABc scores below the estabnegative group), while frequency of events. none of ICDs was more prevalent than the Intermittent explosive disorder 8 (7%) lished cut-off (13.4) was recorded in sixteen patients Statistical Analysis was carried out using SPSS for h PG as the least frequent (Table 2). (mean score 12.2 6 1.3; 20% in ICD negative group Windows Release 10.0 (SPSS, Chicago, IL). Results PD groups had similar age, age at onset MIDI minnesota = Minnesota Impulsivedisorders Disordersinterview; Interview,SOGS = SouthOaks Oaks MIDI, impulsive SOGS, South vs. 11% in ICD positive group). Mild to moderate are reported with significance set at P < 0.006 with e severity, according to UPDRS scores and gambling Screen(病的賭博) screen: pathological gambling. depression (GDS-15 score 6–10) was found in 25 PD Bonferroni correction forGambling multiple comparisons. subjects (24%), and severe depression (GDS-15 > 10) Results with P < 0.05 but not reaching significance was reported in 6 PD (6%), equally distributed in the level are reported as trends. ment Disorders, Vol. 26, No. 3, 2011 two subgroups. I M P U L S I V I T Y A N D C O M P U L S I V I T Y I N D R U G - N A Ï V E P D We found a positive significant correlation between Results TABLE 3. Mean scores of behavioral and psychiatric screening of 11 PD total patients with GDS-15 scores scales and BIS score (r ¼ 0.27; P ¼ Table 3 ICD clinical の有無に基づく and without impulse control 0.005)disorders and a trend toward significance for the correlaDemographic and featuresPD of患者の行動および精神医学的スクリーニングスケールの平均スコア PD patients tion between GDS-15 and lack of planning subscale have been detailed in Table 1. Using the screening Scales Total patients (n ¼ 103) ICD positive (n ¼ 18) ICD negative (n ¼ 85) P value* (r ¼ 0.28; P ¼ 0.01). When considering the two subscales eighteen PD subjects (17.5%) resulted positive the same trend between for at behavior at the MIDI 65.6 groups, BIS-11 totalleast one abnormal 63.7 (9.5) (12.4) 63.3 (8.8) GDS-15 and BIS 0.3411 Attention 15,8 (5.0) (4.9) score was found (ICD 15.2 (4.8) positive r ¼ 0.48 0.007 P ¼ (17 patients) or SOGS (1 patient), with compulsive buy- 18.7 total Motor 25.0 (4.7) 25.4 (5.9) 24.9 (4.4) 0.69 0.04; ICD negative r ¼ 0.28; P ¼ 0.03). ing and compulsive sexual behavior most commonly Lack of planning 26.1 (4.8) 28.1 (4.6) 25.7 (4.8) 0.14 recorded (10.7%). The remaining subjects were classified 6.3 (3.6) MOCQ/R total 4.7 (3.4) 4.4 (3.3) 0.03 as ICDs negative (n ¼ 85). However Checking 2.2 (2.2) by means of clini2.9 (2.4) 2.1 (2.1) 0.12 cal interview based on DSM-IV criteria, none of the 2.3 (1.4) Cleaning 2.0 (1.5) 0.31 TABLE 2. Number (%) of1.9 PD(1.4) patients with ICDs and Doubting 0.8 (1.1) 1.5 (1.2) (1.1) 0.007 patients had a clinically significant disorder. domain 0.7 distribution SOGS (0.7)reach significance 0.50 (1.5) 0.16 (0.7) 0.04 Differences in gender did 0.2not ICDs scales N total (P ¼ 0.06). Values are given as mean 値は平均値(SD) 。 (SD). Intermittent explosive a trend for SOGS 1 (0.9%) *P values after Bonferroni correctiondisorder are set at Pshowed > 0.006. None of the comparisons reaches significance. p 値は *Bonferroni 補正後のin 0.006 に設定。どの比較も有意差には達していない。 higher frequency menp >(8/67 vs. 0/36, P ¼ 0.03). MIDI tot 17 (17.5%) Compulsive buying 11 (11%) Three PD subjects were positive at more than one negative if the overall measures of impulsivOverall PD patients BIS-11 Compulsive ICD sexual even behavior 11 (11%) ICD, and none of ICDs showed was moremean prevalent thantotal the Intermittent explosive disorder 8 eleva(7%) ity and compulsive behaviors did not differ. The scores of 63.7 6 9.5 (range 45–91), below the normaothers, with PG as the least frequent (Table 2). tion of attention impulsiveness scores in PD screening tive mean values in the age-matched healthy populaThe two PD groups had similar age, age at onset MIDI, minnesota impulsive interview; SOGS, South Oaks positive for ICDs maydisorders suggest a subclinical pattern tion (67.8 6severity, 8.6, range 48–84). The ‘‘attentional’’ and disease according to UPDRS scores and gambling screen: pathological gambling. characterized by a relatively reduced ability to focus factor was the one showing the larger difference on the task at hand.9 Relatively high scores in the between the two groups (PD ¼ 15.8 6 5.2, range 8– MOCQ/R doubting subscale have been associated 30 vs. normative values 25.5 6 4.1, range 17–34). In 39 466 Movement Disorders, Vol. 26, No. 3, 2011 with anxiety and/or depressive thoughts,17 and in our the whole PD sample, the MOCQ/R scores were cases may reflect a reduced self-confidence in presence within the normal range either in the total score or in of compulsive behavior. More importantly, we found any of the subscales (4.7 6 3.4, cut-off > 13). in these drug-naı̈ve patients a positive correlation11.7.14 2:25:29 PM As shown in Table 3, the PD subgroups of patients #MD5-1.indb 39 認知機能状態別にみるパーキンソン病患者の 皮質萎縮パターン P A T T E R N O F C O R T I C A L A T R O P H Y I N P A T I E N T S W I T H P D The Pattern of Cortical Atrophy in Patients with Parkinson’s Disease According to Cognitive Status * Sook K. Song, MD, Ji E. Lee, MD, Hae-Jeong Park, PhD, Young H. Sohn, MD, PhD, Jong Doo Lee, MD, PhD, and Phil Hyu Lee, MD, PhD * Department of Neurology, Jeju University College of Medicine, Jeju, Korea 背景:パーキンソン病(Parkinson’ s disease; PD)患 の左後頭葉,PD-MCI 群の両側頭葉,左前頭葉前部,左 者では認知障害がよくみられる。認知症を伴う PD の島,右後頭葉,また PDD 群の広範囲の脳領域で有意 (Parkinson’ s disease with dementia; PDD)に加え, に低かった。PD-IC 群と比較した場合,PD-MCI 群では 軽度認知障害を伴う PD(mild cognitive impairment in 右中前頭葉の灰白質密度が有意に低く,PDD 群では右 Parkinson’ s disease; PD-MCI)という概念が導入され 頭頂葉,右中前頭葉,右の島,右レンズ核の灰白質密度 ている。 が低かった。PDD 群では,PD-MCI 群に比べ,両中側 方法:PD 患者の認知機能状態に対応する脳構造の候補 頭葉,右下側頭葉,左中前頭葉前部,左上前頭葉前部 と な る 部 位 を 特 定 す る た め, 認 知 機 能 正 常 PD の灰白質密度が有意に低かった。認知症を発症するま (Parkinson’ s disease with(GM) intact cognition; PD-IC) での罹病期間が短かった(5 患者では, FIG. 2. Comparison of gray matter density among patients with Parkinson’s disease with intact cognition年未満)PDD (PD-IC), Parkinson’s disease with mild cognitive impairment (PD-MCI), and Parkinson’s disease with dementia (PDD). Compared to the patients with PD-IC, those with PD-MCI had 群(23 例) ,PD-MCI 群(27 例) ,PDD 群(18 同罹病期間が長かった(5 年以上)患者よりも,後部帯 significantly decreased GM density in the right prefrontal area例)を (A). The area of decreased GM density in PDD relative to PD-IC was widespread, involving the bilateral temporal, bilateral prefrontal, left insular, right thalamus, and right parietal areas (B). GM density in PDD relative to PD-MCI 対象に,ボクセル・ベース・モルフォメトリー(VBM) 状回の灰白質萎縮が高度であった。 showed significantly decreased GM densities in the bilateral temporal, bilateral prefrontal, right postcentral, and right fusiform (C). [Color figure can beを用いて灰白質密度を比較した。 viewed in the online issue, which is available at wileyonlinelibrary.com.] 結論:本データから,PD 患者の皮質萎縮の範囲は,認 結果:PDWhen 患者群を通じて背景データはほぼ同じであっ duration. the discrimination threshold was たが,PD-IC 群に比べて PDD 群では reduced (uncorrected P <PD-MCI 0.005),群および decreased GM density in PDD patients with shorter duration relative to 全般的な認知機能障害がより重度であり,罹病期間も長 those with longer duration was observed in the posteかった。灰白質密度は,健常対照群に比べ,PD-IC 群 rior cingulate and occipital areas, whereas more GM atrophy in PDD of longer duration relative to that of shorter duration was observed in the left prefrontal and right parietal areas (Supporting Information Fig. 1). 知障害レベルの悪化に伴って拡大することが示唆され Discussion る。また,様々な解剖学的基質が各認知機能状態に対応 This study demonstrated different patterns of GM するものと考えられる。 atrophy in patients with PD depending on the status of cognitive function. As the levels of cognitive impairments increase, GM atrophy in PD patients relative to controls tended to extend from the occipital area into Movement Disorders, No. 2, 2011, 289–296 the prefrontal, temporal,Vol. and26, parietal areas,pp.where the extent of GM atrophy in PD-MCI was intermediate Key Word パーキンソン病,軽度認知障害,認知症,皮質萎縮 TABLE 2. Anatomic location of areas showing significant difference in gray matter density amongst controls Table 2 認知機能正常パーキンソン病(PD-IC)群,軽度認知障害を伴うパーキンソン病(PD-MCI)群, Parkinson’s disease-intact cognition (PD-IC), Parkinson’s disease-mild cognitive impairment (PD-MCI), and 認知症を伴うパーキンソン病(PDD)群において灰白質密度に有意差が認められた解剖学的部位 Parkinson’s disease dementia (PDD) Talairach Coordinates X Y PD-IC > PD-MCI 24 14 PD-IC > PDD 35 23 33 11 47 9 40 40 36 51 PD-MCI > PDD 54 4 54 16 60 19 46 15 30 59 26 51 Puncorrected Cluster size, mm3 Zmax Middle frontal gyrus <0.0001 78 3.97 Right Right Right Right Right Insula Lentiform nucleus Middle frontal gyrus Inferior parietal lobule superior parietal lobule <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 53 52 62 399 399 3.72 3.66 4.17 4.00 3.68 Right Right Right Left Left Left Inferior temporal gyrus Inferior temporal gyrus Middle temporal gyrus Middle temporal gyrus Middle frontal gyrus Superior frontal gyrus <0.0001 <0.0001 <0.0001 <0.0001 <0.001 <0.0001 55 95 95 82 53 53 3.71 3.43 3.72 4.02 3.29 3.40 Z Side 52 Right 8 0 36 45 48 32 30 23 12 1 6 Anatomical location 40 Movement Disorders, Vol. 26, No. 2, 2011 #MD5-1.indb 40 293 11.7.14 2:25:30 PM 書き出し用.indd 5 11.7.14 2:27:19 PM INC Fu パー 前頭 して 無動 パー SP Ab 早期 プラ 無作 書き出し用.indd 2 11.7.14 2:27:22 PM
© Copyright 2026 Paperzz