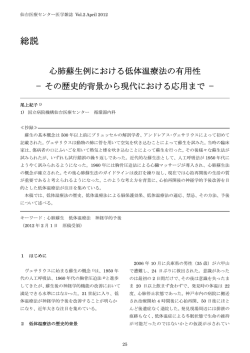
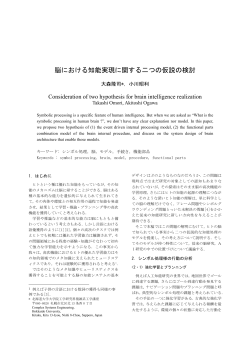
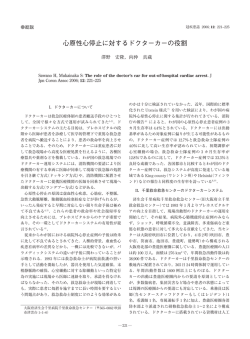
溺水による低体温CPAからの蘇生 国立病院機構 浜田医療センター 秋月 光 沖田泰平 加川隆登 本演題の発表に関して開示すべきCOIはありません 症例 50歳女性 現病歴 自身の運転する車ごと海に入水。車が沈 んでいるのを目撃者により通報された。救 急隊が到着時CPA(Vf)。救急隊にてCPRが 開始され、静脈路確保にアドレナリン1㎎静 注され、除細動1回施行され、当院に搬入し た。 病院到着時はPEA 体温25 瞳孔は6/6mm 対光反射-/2 時間経過 07:54 海中から引き上げ 08:10 CPA 静脈路確保し、アドレナリン1mg静注 モニターVF DC一回でPEAに 08:17 病院到着 08:19 Asys.アドレナリン1㎎静注 08:24 PEA.アドレナリン1㎎静注 08:30 PEA.アドレナリン1㎎静注 約1時間 08:32 モニターはVF DC150J1回 08:36 アミオダロン150㎎投与 モニターはPEAに 08:41 Asys.アドレナリン1㎎静注 08:49 心拍再開確認 3 画像供覧 両肺野に淡い浸潤影 海水の吸引による陰影 4 入院後経過① 入院後、鎮静下で人工呼吸器管理とした。入院 3日目より意識レベルの確認のため短時間の鎮静 解除にて評価を行った。 4日目に鎮静解除( E3VtM6) 5日目に抜管した 7日目に頭部MRIを施行 DWIで大脳皮質下に散在性のスポット状高信号域 5 入院後経過② その後、リハビリを継続し、入院17日目 に独歩で退院となった。 退院後、近医精神科外来に通院となった。 6 今症例のまとめ 今症例では海中から引き揚げ心拍が再開す るまでに約1時間を要している。 1時間の心停止であったにもかかわらず 後遺症を残さず退院できたのは 低体温であったことが考えられる。 7 低体温による脳保護作用 体温が1 低下すると酸素消費量は6~7%低下 する (Drummond JC. et al Cerebral physiology and effects of anesthetics and techniques.) 緩徐におこるグルタミン酸の放出を抑制する (Busto R et al.Effect of mild hypothermia onischemiainduced release of neurotransmitters and free fatty acids in rat brain.Stroke. 1989;20:904910) 8 低体温による心停止の際の 予後良好因子 重度の低体温 低体温に至る原因が窒息や低酸素性脳症で はない 若年者 熟練したチームによる対応 積極的な復温方法 血清カリウム値が高くない 動脈血二酸化炭素分圧が高くない (萩原周一ら 偶発性低体温症:疫学と治 療 ICUとCCU Vol.38 (7) 2014 453-457) 9 低体温による心停止の際の 予後良好因子 重度の低体温 低体温に至る原因が窒息や低酸素性脳症で はない 若年者 熟練したチームによる対応 4項目該当 積極的な復温方法 血清カリウム値が高くない 動脈血二酸化炭素分圧が高くない (萩原周一ら 偶発性低体温症:疫学と治 療 ICUとCCU Vol.38 (7) 2014 453-457) 10 ICU入室後の体温変化 発熱! 入 室 11 低体温からの復温 復温は低体温を維持するよりも高体温を避 けたほうがよい。 (Benjamin M. Sciria. Therapeutic Hypothermia After Cardiac Arrest:Circulation Jannuary 15,2013;127:244-250 ) 12 AHA ガイドライン Hyperthermia After resuscitation, temperature elevation above normal can impair brain recovery. The etiology of fever after cardiac arrest may be related to activation of inflammatory cytokines in a pattern similar to that observed in sepsis.68,69 There are no randomized controlled trials evaluating the effect of treating pyrexia with either frequent use of antipyretics or “controlled normothermia” using cooling techniques compared to no temperature intervention in post– cardiac arrest patients. Case series(70 –74) and studies(75– 80) suggest that there is an association between poor survival outcomes and pyrexia ≧37.6℃. In patients with a cerebrovascular event leading to brain ischemia, studies75– 80 demonstrate worsened short-term outcome and long-term 生存率の低さと37.6℃以上の発熱とは関係がある mortality. By extrapolation this data may be relevant to the global ischemia and reperfusion of the brain that follows cardiac arrest. Patients can develop hyperthermia after rewarming posthypothermia treatment. This late hyperthermia should also be identified and treated. Providers should closely monitor patient core temperature after ROSC and actively intervene to avoid hyperthermia (Class I, LOE C) (2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care) 13 高体温はなぜいけないのか 酸素消費量 増加 低酸素 高体温 グルタミン酸 細胞内Ca流 入 蛋白リン酸化 活性酸素化 イオンチャネ ル活性化 フリーラジカ ル産生 細胞内Ca流 入 細胞膜破壊 細胞アポトーシス 救急・集中治療2005;17:379-381を改変14 結語 低体温によるCPAでは脳保護作用に より神経学的予後に期待できるため 通常であれば蘇生の見込みのないCPA でも積極的に蘇生を行うべきである 15 ご清聴ありがとうございました 16
© Copyright 2026 Paperzz