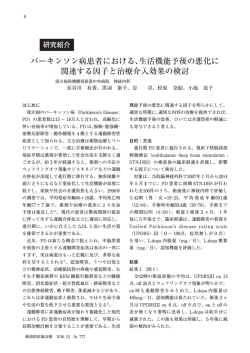
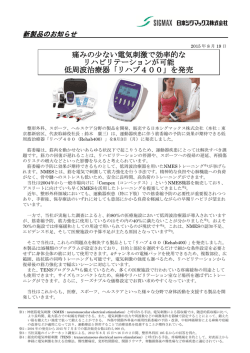
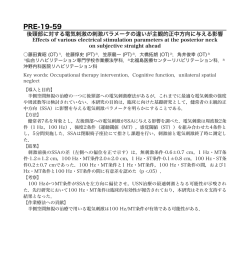
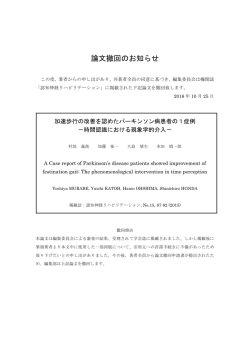
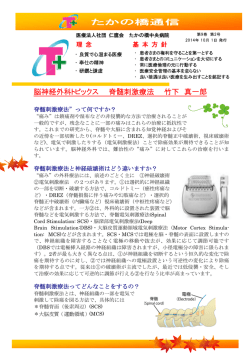
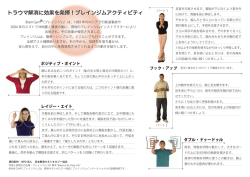
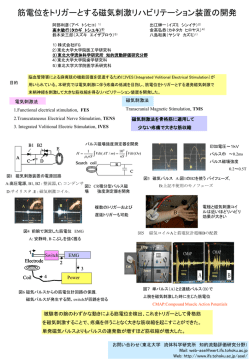
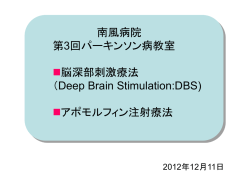
総 説 北里医学 2013; 43: 95-104 パーキンソン病に対する外科治療 佐藤 澄人,隈部 俊宏 北里大学医学部脳神経外科学 パーキンソン病に対する外科治療は長い歴史を持ち,薬物療法と相補的関係にある。外科的治療 のよい適応は,長期間のL-ドパ療法によるwearing offやドパ誘発性ジスキネジアなどの運動合併 症,薬物抵抗性の振戦である。主として淡蒼球や視床下核の脳深部刺激療法 (deep brain stimulation: DBS) が行われ,術前にL-ドパ療法の効果が保たれていることが重要である。術後に運動機能の著 明な改善が認められる一方,認知・精神機能に対する影響も考慮する必要がある。長期経過におい て振戦に対する効果は維持されるが,体軸症状の悪化が問題となる。DBSの作用機序は現在なお明 らかでなく,病態生理の解明とともに今後の研究が待たれる。 Key words: パーキンソン病,視床凝固術,脳深部刺激療法,大脳基底核 はじめに パーキンソン病 (Parkinson's disease) は,1918年に英 国のJames Parkinsonによって報告1されて以来,病因の 解明や治療法の進歩において他の神経変性疾患と比べ 際立っている。黒質緻密部のドパミンニューロンの変 性・脱落 (Trétiakoff,1921年2) に始まり,Lewy小体の 発見 (Lewy,1912年3) やその進展様式 (Braak,2003年4) が明らかにされた。また,MPTP (1-methyl-4-phenyl1,2,3,6-tetrahydropyridine) を用いた実験的パーキンソニ ズムにより病態生理の研究が進み,原因遺伝子も次々 発見されてきている。治療法においても1960年代にLドパ療法が開発され,予後は著しく改善された。さら にドパミンアゴニスト,末梢性カテコラミン分解酵素 阻害薬,モノアミン酸化酵素B阻害薬,アデノシン A2A受容体阻害薬などさまざまな治療薬が開発されつ つある。今後はiPS細胞などの再生医療の分野に期待が 持たれている。 一方,外科的治療に目を転じると,L-ドパ療法に先 立つ1950年代より定位脳手術が行わるようになり,有 効な治療法がなかった暗黒の時代に光明が差し込ん だ5,6。その後,微小電極記録による神経生理学的手法 の導入 (Albe-Fessardら,1963年7) ,MRI誘導による ターゲットの設定,神経科学的知見の蓄積による神経 回路や病態生理の解明,脳深部刺激療法 (deep brain stimulation: DBS) などのエレクトロニクスの進歩によ り,さらに精度の高い理論的な手術が可能となった。 本稿ではパーキンソン病の外科治療における歴史,適 応,手術法,現在考えられているDBSのメカニズムな どについて概説する。 外科的治療の歴史的概観8-11 振戦や筋固縮に対する外科治療の創始期は,まさに 試行錯誤の連続であったと思われる。錐体路の遮断を 目的とした一次運動野の切除 (Bucy,1939年12),固有 感覚入力の遮断のための後外側コルドトミー (Putnam,1933年13),錐体外路系に対する侵襲として大 脳脚切截術 (Walker,1949年14) などが試みられたが, 必然的に重度の運動麻痺を生じる結果となった。 Meyersは尾状核頭部や淡蒼球などの皮質下構造物に目 を向け,レンズ核ワナの遮断が振戦や筋固縮に効果が あることを1942年に報告15した。しかし,定位的方法 ではなく半球間裂および側脳室を経由するアプローチ のため,侵襲の大きな手術法であった。Cooper 11 は Walkerの大脳脚切截術を行う際,意図せず前脈絡叢動 脈を閉塞させてしまった。ところが,術後に筋固縮や 振戦が改善しているのに気づき,前脈絡叢動脈の結紮 術を試みるようになった。その後,ターゲットを淡蒼 球に修正し,1955年にフリーハンドでアルコールを注 入する淡蒼球破壊術 (chemopallidectomy) を報告した。 定位脳手術 (stereotactic surgery) の歴史は,1908年に HorsleyとClarke16によって動物実験用の装置が考案さ れ,1947年にSpiegelとWycis17によって初めて臨床応用 された。定位脳手術とは,皮質下の神経核や神経路に 限局した破壊巣を作成することを目的とし,立体的な 位置と方向を定め,機械的な誘導によって正確にアプ Received 29 November 2013, accepted 3 December 2013 連絡先: 佐藤澄人 (北里大学医学部脳神経外科学) 〒252-0374 神奈川県相模原市南区北里1-15-1 E-mail: [email protected] 95 佐藤 澄人,他 ローチする手法である。最小限の侵襲で最大限の効果 を図る発想で,現在の低侵襲外科 (minimally invasive surgery) に通じるものと言える。この定位的方法により 脳深部の手術は安全なものとなり,レンズ核ワナの凝 固術 (ansotomy) が施行された (SpiegelとWycis,1954 年18)。時を同じくして,本邦でも楢林らが独自の定位 脳手術装置を開発し,1952年にパーキンソン病に対し て淡蒼球手術を行った19。最初は効果を確かめるため に塩酸プロカイン水溶液を注入し,次いで効果を持続 させるために塩酸プロカイン油性懸濁質を注入した。 振戦及び筋固縮は消失し,運動麻痺や感覚障害などは 出現せず,この効果は約40日間持続した。その後振戦 は再燃してきたが,筋固縮の軽減は持続した20。Hassler とRiechertは淡蒼球内節の投射先である視床の破壊も有 効であろうと考え,1952年にventrolateral thalamotomy を行ったところ,筋固縮のみならず振戦に対しても有 効であった。 1960年代より,L-ドパ療法がパーキンソン病治療の 主役となるが,L-ドパを長期間続けることにより様々 な副作用が生じることが次第に明らかとなった。1992 年,LaitinenらはLeksellによる淡蒼球後腹側部の破壊が パーキンソン症状に効果があったとの報告 (Svennilson ら,1960年21) から後腹側淡蒼球破壊術 (posteroventral pallidotomy) の有効性を報告した22。さらに同じ頃, Benabidらが破壊術に代わる安全で効果的な方法とし て,視床23,24や視床下核 (subthalamic nucleus: STN)25の 高頻度刺激療法,すなわちDBSを導入した。これら外 科治療が薬物治療を補う治療戦略として再び注目され るようになった。 い。オフ症状としてのすくみは改善が期待できるが, オン状態のときにみられるすくみはDBSでも治療が困 難である27。オフ状態L-ドパ治療に反応が乏しい場合 には手術の効果は期待できず,多系統萎縮症や進行性 核上性麻痺などのパーキンソン症候群においても手術 適応はない。手術は十分な薬物療法の後に考慮される べきものであるが,年齢としては70歳以下で行うこと が望ましい。手術時の年齢が若い方が良好な経過 2 8 で,後述する認知・精神機能への影響も少ないと考え られる。また,比較的若年で社会的・家庭的に活動度 が高いほど,高い満足度と社会への還元効果が得ら れ,医療経済的にも有利29といえる。最近,比較的早 期のパーキンソン病患者に対するDBSの有用性を検証 するための多施設共同無作為試験 (EARLYSTIM試験) が行われた30。対象は罹患期間4年以上,早期運動合併 症がみられる症例で,STN-DBS + 内科的治療群124例 (平均年齢52.9歳,平均罹病期間7.3年),内科的治療単 独群127例 (52.2歳,7.7年) が割り付けられた。2年間の 評価において,前者が運動症状,ADL,L-ドパ誘発性 運動合併症の改善効果が優れていた。今後はDBSが比 較的早期に治療の選択枝に挙げる必要があるかもしれ ない。 その他,副作用によって十分な薬物療法が行えない 場合31や,薬物療法に抵抗性の振戦症状に対しては, 時期を問わず外科的治療の適応となる。薬物の副作用 によって生じている幻覚はDBS後に減薬することで改 善され得るが,もともと幻覚などの精神疾患を合併し ている場合は悪化する恐れがあるため除外する。Table 1に外科治療の適応32を示す。 手術適応および時期 PDの病態生理とDBSのメカニズム L-ドパ療法を長期間継続すると,薬効が一定せず, 症状の日内変動 (motor fluctuation) や,ドパ誘発性ジス キネジアが生じるようになる。これらを運動合併症 (motor complication) という。運動症状の日内変動に は,L-ドパの薬効時間の短縮するwearing-off現象,突 然効果が切れて動けなり,また再び動けるようになる オン・オフ現象などがある。ドパ誘発性ジスキネジア はオン時,最もL-ドパ濃度が高まっているときに生じ るpeak-doseジスキネジアと,オフからオンあるいはオ ンからオフに切り替わるタイミングで生じるdiphasicジ スキネジアとに大別される。Wearing-offの頻度はさま ざま報告されているが,L-ドパ治療開始後5年で50%程 度26と考えられる。 DBSはこのようなwearing-offとジスキネジアに対し て有効な治療法である。オフ状態がHoehn-Yahr重症度 で3度以上が手術を勧める時期であるが,手術による改 善効果は薬物療法における最良のオン状態を越えるも のではなく,オン状態が3度以下であることが望まし 1989年から1990年にかけて,Albinら33やDeLongら34,35 のグループによって大脳基底核の直接路・間接路モデ ルが提唱され,大脳基底核の神経回路やパーキンソン 病をはじめとする大脳基底核疾患の病態生理の理解は 大きく進歩した36 (Figure 1A,1B)。大脳基底核の出力部 である淡蒼球内節 (internal segment of the globus pallidus: GPi) および黒質網様部 (substantia nigra pars reticulate: Table 1 ・長期L-ドパ療法による運動合併症 (wearing-off現象、ドパ 誘発性ジスキネジアなど) ・薬物抵抗性の重度の振戦 ・副作用 (嘔気,アレルギー,幻覚などの精神症状) により 薬物治療が困難 ・L-ドパ療法の反応性が保たれている (オン状態でHoehnYahr重症度3度以下) ・一般的には70歳以下で重度の合併症がない ・既存の精神疾患がない 96 パーキンソン病に対する外科治療 SNr) はGABA作動性の抑制性ニューロンで,高頻度で 連続して発射しているため,投射先の視床はふだん抑 制された状態にある。大脳皮質からの入力によって線 条体 (striatum) ニューロンが興奮すると,線条体の投 射ニューロンはGABA作動性の抑制性ニューロンなの で,GPi/SNrニューロンが脱抑制され (直接路),投射 先のニューロンが興奮することにより必要な運動が起 こる。一方,淡蒼球外節 (external segment of the globus pallidus: GPe),STNを経由してGPi/SNrニューロンを興 奮させ (間接路),直接路と逆の作用をもたらす。直接 路は意図した運動を脱抑制によって発現させ,間接路 は不要な運動を抑制することにより,運動のSN比を上 げていると考えられている37 (focused selection)。 DBSの臨床応用は,1950年代にHeathら38が精神疾患 の患者に対して実験的に始められた。報酬系について 調べられ,相反する疼痛に対する治療の道を開いた39。 運動障害に対するDBSは,1987年にBenabidら23,24が thalamotomyに代わる治療法としてVim-DBSを試みたの が始まりである。1990年にBergmanら40はMPTPによる パーキンソン病モデルのサルが,一側の視床下核の破 壊によって対側肢の無動,筋固縮,振戦などの運動症 状が改善することを見出した。この知見をもとに Benabidらのグループ25が1995年,パーキンソン病患者 に両側STN-DBSを開始したところ,著明な効果が得ら れ広く普及するに至った。MPTPは自家製麻薬の副産 物として生成され,それを含む麻薬を注射するとパー キンソニズムが発生する (Davisら,1979年41) ことか ら,実験的パーキンソニズムに利用されるようになっ た。MPTPは脳内でモノアミン酸化酵素によって毒性 の強いMPP+に変換され,黒質線条体ニューロンに選 択的に取り込まれる。MPTPを投与されたサルは, パーキンソン病と似た無動や寡動,前屈姿勢,筋固 縮,振戦 (一部の種) が出現する35。 DBSの作用機序については,現在のところまだ明ら かでない。DBSが破壊術と同様の効果を示すことか ら,高頻度連続刺激が局所のニューロン活動をブロッ A B Figure 1. Schematic diagram of the basal ganglia-thalamocortical circuitry under (A) normal and (B) parkinsonian conditions (modified from references 25, 53) Inhibitory connections are shown as black arrows, excitatory connections are gray arrows. Parkinsonism leads to differential changes in the two striatopallidal projetions, which are indicated by the thickness of the connecting arrows. Basal ganglia output to the thalamus is increased. CM, centromedian nucleus; GPe, external segment of the globus pallidus; GPi, internal segment of the globus pallidus; PPN, pedunculopontine nucleus; SNr, substantia nigra, pars reticulate; SNc, substantia nigra, pars compacta; STN, subthalamic nucleus; VA, motor thalamus ventralis anterior; VL, ventrolateral thalamus 97 佐藤 澄人,他 クするという説 (抑制仮説) がある。これには,①脱分 極ブロックによるもの,②抑制性入力線維や抑制性介 在ニューロンが刺激されることによるもの,③入力線 維が逆行性に刺激され,標的ニューロンがブロックさ れたと同じ効果による,などの可能性が挙げられる42。 抑制仮説は,パーキンソン病が黒質緻密部のドパミン ニューロンが変性・脱落することにより,線条体の直 接路のニューロンの活動が減弱,間接路のニューロン の活動が亢進し,結果的にSTNおよびGPiのニューロン 活動の亢進,すなわち平均発射頻度の上昇すること (発 射頻度仮説) と論理が一致している (Figure 1B)。しか し,振戦やドパ誘発性ジスキネジアに対する効果は説 明できない。 一方,高頻度連続刺激は局所のニューロンを興奮さ せる考え方 (興奮仮説) もある。STNからGPiに投射す るニューロンは興奮性 (グルタミン作動性) であり, MPTPによるサルのパーキンソン病モデルにおいて, STNの高頻度刺激によりGPiの発射頻度が増加し,パー キンソン症状が回復したとの報告43がある。興奮仮説 はパーキンソン病の発射頻度仮説では説明できないた め,発射パターンを規則的に変化させることにより病 態を改善させていると考えられている (発射パターン仮 説) 。すなわち,パーキンソン病では大脳基底核の ニューロン活動が発振・共振するために情報処理が阻 害され,そのような発振が視床を介して大脳皮質に伝 達されるため,諸症状が起きると考えられる44-47。これ は,正常では大脳基底核内の情報処理が独立して行わ れているが,ドパミンが不足すると互いに独立性が失 われ情報の混信が起きることを示唆している42,44。高頻 度連続刺激は局所のニューロンを刺激に同期して興奮 させることにより,このような発振や共振を強制的に 脱同期させ,症状を改善すると考えられる42,43。 振戦に対しては視床腹中間核 (ventrointermedius: Vim) が著効を示す (Table 2)。STNとGPiを比較した多数例の 無作為比較試験48-50では,総じて運動機能の改善はほぼ 互角ないしSTNの方が薬剤の減量やDBSの刺激強度が 小さくて済む分優位ととらえられている。しかし, STN-DBS後の減薬はうつやアパシー (apathy) を悪化さ せる51ことが指摘されている。ドパミン補充療法は運 動障害改善に必要な黒質線条体系に作用するだけでな く,中脳辺縁系や中脳皮質系にも作用するため,減薬 によりこれら非運動症状が悪化する可能性がある52。 そのため,われわれはSTN-DBS後の減薬は控えるよう にしている。 STN-DBSによる認知機能の問題は41%に生じたとの 報告53もあり,遂行機能障害 (executive dysfunction)54, 言語流暢性 (verbal fluency) の低下55が指摘されている。 STN-DBSがGPi-DBSと比較して認知・精神機能に影響 を与えやすい原因としては,感覚運動系 (sensorimotor)・ 連合系 (associative)・辺縁系 (limbic) の皮質−大脳基底 核連関において,STNが最もコンパクトに情報が集 まっている56ためと考えられる。体積で比較すると, ターゲットの選択 パーキンソン病に対する定位脳手術のターゲット は,STN,GPi,視床 (特に腹中間核),脚橋被蓋核 (pedunculopontine nucleus: PPN) である (Figure 2)。現在 のところ,主として選ばれるのはSTNとGPiで,いずれ もパーキンソン病の主要運動症状に広く有効である。 Figure 2. Stereotactic targets for Parkinson's disease Thal Vim, thalamic ventrointermedius nucleus; STN, subthalamic nucleus; GPi, internal segment of the globus pallidus; PPN, pedunclopontine nucleus Table 2. Efficacy of each target Thalamus GPi STN Tremor Rigiity Akinesia Gait posture disturbance Wearing off Dyskinesia Drug reduction ○ ○ ○ △ ○ ○ × ○ ○ × ○ ○ × ○ ○ × ○ ○ × ○ × ○: effective, △: partially effective, ×: not effective 98 パーキンソン病に対する外科治療 大脳基底核の入力部である尾状核は4,316 mm3,被殻は 5,625 mm3,介在部である淡蒼球外節は808 mm3,視床 下核は158 mm3,出力部である淡蒼球内節は478 mm3, 黒質網様部は412 mm3である57。すなわち,視床下核は 体積が淡蒼球内節の約1/3で細胞密度も高く,感覚運動 系ループのみならず,連合系や辺縁系ループも近接し ており,DBSによる刺激がそれらに波及しやすいと推 測される。したがって,運動機能への効果と同時に認 知・精神機能への作用も大きいと考えられる。 PPNは橋中脳被蓋尾側に位置しており,大脳基底核 や運動調節に関連する他の脳領域と密接に関連してい る 5 8 。除脳ネコやラットで電気刺激すると歩行動作 (locomotion) が誘発される59,60ため,PPNは中脳歩行動 作領域 (mesencephalon locomotor region,MLR) の一部 と考えられ,S T N やG P i では改善できないすくみ (freezing) や歩行障害などの体軸症状に対しての効果が 期待されるようになった。2005年よりPPN-DBSがPDの 患者に試みられ始め61,年々報告例が増加しているも のの,S T N - D B S との併用効果を述べた論文 6 2 や, UPDRSスコアでは有意な改善が得られなかったとの報 告63など,まだ一定した評価が得られていないのが現 状である64。その背景には,PPNは脳幹網様体に属する 細胞集団で境界が不鮮明であること58,65,解剖学的用語 の混乱66,種による違い67などが考えられる。除脳ネコ やラットのPPNで確認されている歩行制御などの証拠 はサルではまだ確認されておらず65,また四足歩行の 動物と二足歩行であるヒトでは歩行のメカニズムが異 なることが推測される67。現在までのところ,本邦で のPPN-DBSの報告例はみられていない。 まとめると,比較的若年で認知・精神機能に問題が なく,薬物の減量を期待したいときはSTN-DBSを,反 対に高齢で術後の認知機能低下が危惧されるような症 Figure 3. Target selection Figure 4. Number of each surgical procedure in our institute 99 佐藤 澄人,他 例にはGPi-DBSの方が安全といえる。ジスキネジアや ジストニアが目立つ場合はGPi-DBSを,振戦が主症状 であればVimをターゲットに選択する。当施設での術 式の選択基準 (Figure 3) と,これまで行った手術術式 (Figure 4) を示す。2011年よりGPi-DBSがやや増加して いるのが分かるが,DBS療法を開始した当初はSTNDBSのみ行っており,術後に認知機能の低下をきたし た症例を経験した。そこで,STN-DBSを行った場合に 術後の認知機能に悪影響を及ぼすことが懸念される症 例に対し,GPi-DBSを行ったところ良好な結果が得ら れたため,以後積極的にGPi-DBSを取り入れるように なった。Vimをターゲットにする際はDBSではなく凝 固術 (thalamotomy) を行っているが,Vim-DBSとVimthalamotomyは同等に有効であり68,インフォームドコ ンセントにおいて患者がデバイスを留置しない凝固術 を選択したためである。 い。そのため,微小電極記録による神経生理学的な検 証が必要となる。先端が極めて細く,電極のインピー ダンスが数メグオームの微小電極 (microelectrode) と, それに比べて先端がやや太くインピーダンスが数十〜 百キロオーム程の準微小電極 (semi-microelectrode) とが あり,前者は単一ニューロン活動の記録 (single-unit recording),後者は複数のニューロン発射や集合電位の 記録 (multi-unit recording) に用いる。 DBS電極の留置は原則的に局所麻酔下で行う。覚醒 下での脳深部神経活動の記録と臨床所見の観察が可能 で,術中に試験刺激による効果や副作用を確認できる 利点がある。しかし,両側の電極を同じ日に留置する 場合は手術時間が長くなり,患者の身体的・精神的苦 痛が少なくない。不穏をきたした際には,頭部にフ レームを装着している状態での過鎮静は気道確保の点 で危険を伴う。最近,全身麻酔下でも微小電極もしく は準微小電極記録による神経核の同定は可能で,良好 な長期成績が得られたという報告69,70もあり,当施設で も患者の希望に応じて全身麻酔下でのDBS電極留置を 行っている。 DBSシステムは,電極リードと完全埋設型刺激発生 装置 (implantable pulse generator: IPG),両者を接続す るケーブルで構成される (Figure 5A,5B)。電極リード は直径1.27 mmで長さ1.5 mmの電極が1.5 mmもしくは 0.5 mm間隔で4個連なっている。IPGは心臓ペースメー カーと似た装置で,リチウム電池を内蔵し電池の寿命 は通常4〜5年である。一般的には低電圧 (数V以下), 持続時間の短い (数十μs),高頻度 (100 Hz以上) の刺 激が用いられ,1 mA程度の電流が流れるが,電流密度 手術の方法 定位脳手術用フレームを患者の頭部に装着し,フ レームを基準にした位置情報を与えるインジケータを 取り付けてMRIを撮影する。得られた画像データをプ ランニング・ソフトウェアに取り込み,仮標的 (tentative target) を設定する。仮標的とはアトラスや画 像所見から計測する位置で,標準アトラスから求めら れる座標と画像所見に基づく解剖学的な個人差とを すり合わせて決定される。実際の手術では,MRI画 像の歪みや様々な過程で生じる僅かな誤差の積み重ね により,必ずしも意図した結果が得られるとは限らな A B Figure 5. System for deep brain stimulation composed of (A) electrode leads and (B) implanted stimulators. 100 パーキンソン病に対する外科治療 は低い。持続時間が短く電流密度が低いため,ニュー ロンの細胞体よりは軸索,しかも太い軸索が刺激され やすい傾向にあるとされる議論もある42,71。刺激のパラ メータはプログラマーを用いて体外から調整を行うこ とができる。この可逆性,調節性がDBS療法の最大の 利点である。 3. Vim-DBS or thalamotomy ヒトの視床の亜核分類法はHassler75やHiraiとJones79に よるものがあるが,定位脳手術で広く用いられている Schaltenbrandらのアトラス80では前者による用語が記載 されている。Vimは視床腹外側核群で淡蒼球内節から 入力を受ける腹吻側核 (Vo,ventrooralis) の後方,表在 感覚の入力を受ける腹尾側核 (Vc,ventrocaudalis) の前 方に位置し,小脳核からの入力と深部感覚の入力を受 けている81-83。深部感覚の入力を受けるニューロンは Vim核の最外側に存在し,微小電極記録を行うと,四 肢関節の受動運動に対する反応 (kinesthetic response)84 や振戦リズムに一致した群過放電 (tremor-frequency rhythmic discharge) が観察される。それらの位置の凝固 もしくはDBSにより振戦は直ちに抑制される。 1. GPi-DBS Laitinenら22がパーキンソン症状に対する有効性を指 摘したGPi後腹側部は,線条体の運動領域から投射を 受ける淡蒼球尾側の腹側2/3の部位と一致しており,こ れらは淡蒼球の運動領域で体部位局在をもっている。 すなわち,腹側から背側に向かって,口腔顔面,上 肢,下肢の領域が存在する72。これら運動系ループに 属する運動淡蒼球 (motor pallidum) が治療のターゲッ トとなる。サルを使った研究73では,運動淡蒼球の腹 外側部は一次運動野および固有補足運動野の関連領域 で,視床への投射線維はレンズ束 (Forel H2野) となり, STNの背側を内側に向かいForel H野に到達し,視床束 Forel H1野) となり,視床VLo核 (Olszewski74によるサ ルの亜核分類で,Hassler75によるヒトのVoa核に相当) に終止する。一方,運動淡蒼球の背内側部は運動前野 および前補足運動野に関連しており,視床投射線維は 腹側に向かいレンズ核ワナを形成し,視床VApc核 (同74,75,ヒトのLpo核) に終止する。 GPi-DBSにおいて,刺激電極の位置によって臨床効 果が異なることが報告されている。すなわち,GPiの 腹側部刺激では,筋固縮やドパ誘発性ジスキネジアが 改善するが,逆に歩行や無動が増悪し,背側部刺激で はオフ時の無動,歩行障害,筋固縮が改善するが,刺 激強度を上げるにつれてドパ誘発性ジスキネジアが誘 発された76。上記のようなGPiの腹側と背側とで異なっ た投射先であることとの関連が示唆される。 合併症85 定位脳手術における脳内出血合併症の発生率は,諸 報告を総合して0〜5.0%であり,症候性の出血は0〜 2.0%である。脳内出血を起こす危険因子として,高血 圧の既往,高齢であることが指摘されている。また, 微小電極記録の穿刺回数は必要最小限にすべきであろ う。DBSシステムの機器に関連する合併症は,2006年 以降の報告では,4.0〜9.7%で,頭蓋内電極の迷入・脱 落,電極・延長コードの断線,コード・刺激装置埋没 部の皮膚潰瘍,感染,アレルギー性皮膚反応,刺激装 置の故障などが報告されている。 長期効果 STN-DBS,GPi-DBSともに3〜6年にわたり有効性が 維持されていることが報告されている86,87。効果の持続 は症状によって異なり,STN-DBSの8〜10年の経過で は良好な効果が持続されるのは振戦で,すくみや姿勢 反射障害といった体軸症状は効果が低下しやすい傾向 にあった88,89。しかし,これは効果が減弱するという意 味だけではなく,病期の進行に追いつかなくなったと もいえる。DBS療法はパーキンソン病の進行を抑える 効果はないが,DBSをオフにすると症状は増悪するの でDBSの効果自体は持続していると考えられる。ちな みに,淡蒼球内節破壊術 (pallidotomy) はパーキンソン 病の運動症状全般に有効であるが,その効果の持続時 間は2年程度90である。 2. STN-DBS STNはその名の通り視床の下に位置し,外側に内 包,背側にレンズ束 (Forrel H2野),腹側には黒質に囲 まれた158 mm3程の小さな核である。STNの背側部が運 動系ループに属している感覚運動領域で,DBS電極の 留置に適した部位である。このうち,外側部は一次運 動野から体部位局在的な入力を受けており,外側から 内側にかけて口腔顔面,上肢,下肢の領域である。感 覚運動領域の内側部は高次運動野から入力を受けてお り,体部位局在は一次運動野からのものと鏡像関係に なっている72。感覚運動領域の腹側には眼球運動に関 連した領域,さらに腹側には前頭前野系ループに属す る領域,腹内側部には辺縁系ループに属する領域が存 在する56,77,78。 今後の展望 エレクトロニクスの進歩により,デバイスの性能は 向上してきている。刺激条件の設定はこれまで定電圧 式であったが,定電流式も可能になり有効性が示され ている 9 1 。パーキンソン病患者の通常の使用条件で 101 佐藤 澄人,他 は,バッテリーの寿命は4〜5年程度である。その度に IPGの交換が必要となるが,最近は充電式のもの92も利 用できるようになった。現在のところ頻回の充電が必 要であるが,今後の改良が期待される。MRIは原則禁 忌であるが,進行期パーキンソン病の患者は腰痛など 整形外科疾患が併存することも多く,MRI撮影ができ ないことは診療上不利である。この分野で先行する心 臓ペースメーカーではMRI耐性のデバイスが既に開発 されているので,近い将来解決されるものと思われ る。現在のDBSシステムは,設定したパラメータの電 気刺激を脳の局所に一方的に与えるだけであるが,セ ンシング機能を持った心臓ペースメーカーのように, 脳の神経活動を記録しながらそれに合わせて刺激を調 整するclosed-loop DBSシステム93が開発されつつある。 8. Gildenberg PL, Krauss JK. History of Stereotactic Surgery. In: Lozano A, Gildenberg P, Tasker R, editors. Textbook of Stereotactic and Functional Neurosurgery. Berlin Heidelberg: Springer-Verlag; 2009; 1-33. 9. Parrent AG. History of Surgery for Movement Disorders. In: Lozano A, Gildenberg P, Tasker R, editors. Textbook of Stereotactic and Functional Neurosurgery. Berlin Heidelberg: Springer-Verlag; 2009; 1467-85. 10. 横地房子.【視床下核と刺激療法】パーキンソン病外科治療 のOVERVIEW. 脳の科学 2002; 24: 421-5. 11. Cooper IS. Neurosurgical alleviation of parkinsonism. Bull N Y Acad Med 1956; 32: 713-24. 12. Bucy PC, Case TJ. Tremor: Physiologic mechanism and abolition by surgical means. Arch Neurol Psychiatry 1939; 41: 721-46. 13. Putnam TJ. Treatment of athetosis and dystonia by section of extrapyramidal motor tracts. Arch Neurol Psychiatry 1933; 29: 504-21. 14. WALKER AE. Cerebral Pedunculotomy for the Relief of Involuntary Movements. II. Parkinsonian Tremor. TJ Nerv Ment Dis 1952; 116: 766-75. 15. Meyers R. The modification of alternating tremors, rigidity and festination by surgery of the basal ganglia. Res Nerv Ment Dis Proc 1942; 21: 602-65. 16. Horsley V, Clarke RH. The structure and functions of the cerebellum examined by a new method. Brain 1908; 31: 45-124. 17. Spiegel EA, Wycis HT, Marks M, et al. Stereotaxic Apparatus for Operations on the Human Brain. Science 1947; 106: 349-50. 18. Spiegel EA, Wycis HT. ANsotomy in paralysis agitans. AMA Arch Neurol Psychiatry 1954; 71: 598-614. 19. Narabayashi H, Okuma T. Procaine-oil blocking of the globus pallidus for the treatment of rigidity and tremor of parkinsonism (preliminary report). Proceed Jpn Acad 1953; 29: 134-7. 20. Narabayashi H, Okuma T, Shikiba S. Procaine oil blocking of the globus pallidus. AMA Arch Neurol Psychiatry 1956; 75: 36-48. 21. Svennilson E, Torvik A, Lowe R, et al. Treatment of parkinsonism by stereotatic thermolesions in the pallidal region. A clinical evaluation of 81 cases. Acta Psychiatr Scand 1960; 35: 358-77. 22. Laitinen LV, Bergenheim AT, Hariz MI. Leksell's posteroventral pallidotomy in the treatment of Parkinson's disease. J Neurosurg 1992; 76: 53-61. 23. Benabid AL, Pollak P, Louveau A, et al. Combined (thalamotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateral Parkinson disease. Appl Neurophysiol 1987; 50: 3446. 24. Benabid AL, Pollak P, Gervason C, et al. Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet 1991; 337: 403-6. 25. Limousin P, Pollak P, Benazzouz A, et al. Effect of parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet 1995; 345: 91-5. 26. Fahn S. Adverse effects of levodopa. In: Olanow CW, editor. The scientific basis for the treatment of Parkinson's disease. Carnforth, UK: Parthenon Publishing Group; 1992: 89-112. 27. Welter ML, Houeto JL, Tezenas du Montcel S, et al. Clinical predictive factors of subthalamic stimulation in Parkinson's disease. Brain 2002; 125: 575-83. 28. Charles PD, Van Blercom N, Krack P, et al. Predictors of effective bilateral subthalamic nucleus stimulation for PD. Neurology 2002; 59: 932-4. 29. Espay AJ, Vaughan JE, Marras C, et al. Early versus delayed bilateral subthalamic deep brain stimulation for parkinson's disease: a decision analysis. Mov Disord 2010; 25: 1456-63. おわりに 不随意運動疾患に対する定位脳手術などは機能的脳 神経外科 (functional neurosurgery) と呼ばれる,神経組 織自体に手を加えて,その機能を変化させることによ り,目的とする臨床効果を引き出す治療概念である。 最近は,ニューロモデュレーション (neuromodulation) という,神経組織に微弱な電気や薬剤を流すことによ り神経活動を調節する治療法としてとらえられ,医学 と工学技術が融合した最先端治療としてさらなる進歩 が期待されている。また,神経科学の基礎的な研究と も密接に関連しており,基礎医学と臨床医学が連携し て発展させていく必要がある。 文 献 1. ジェイムス・パーキンソンの人と業績. 豊倉康夫編訳,診断 と治療社,東京,2004. 2. Lees AJ, Selikhova M, Andrade LA, et al. The black stuff and Konstantin Nikolaevich Trétiakoff. Movement Disorders 2008; 23: 777-83. 3. Lewy F. Paralysis agitans. I. Pathologische anatomie. Handbuch der neurologie 1912; 3: 920-33. 4. Braak H, Rüb U, Gai WP, et al. Idiopathic Parkinson's disease: possible routes by which vulnerable neuronal types may be subject to neuroinvasion by an unknown pathogen. J Neural Transm 2003; 110: 517-36. 5. 楢林博太郎,金澤一郎. インタビュー ある神経学者の発想 と足跡を辿る─楢林博太郎先生に聞く(1). 神経研究の進歩 2001; 45: 512-22. 6. 楢林博太郎,金澤一郎,大江千廣. インタビュー ある神経 学者の発想と足跡を辿る─楢林博太郎先生に聞く(2). 神経 研究の進歩 2001; 45: 688-700. 7. Albe Fessard D, Arfel G, Guiot G, et al. [CHARACTERISTIC ELECTRIC ACTIVITIES OF SOME CEREBRAL STRUCTURES IN MAN]. Annales de chirurgie 1963; 17: 1185214. 102 パーキンソン病に対する外科治療 30. Schuepbach WM, Rau J, Knudsen K, et al. Neurostimulation for Parkinson's disease with early motor complications. N Engl J Med 2013; 368: 610-22. 31. Katayama Y, Kasai M, Oshima H, et al. Subthalamic nucleus stimulation for Parkinson disease: benefits observed in levodopaintolerant patients. J Neurosurg 2001; 95: 213-21. 32. Sato S, Mochizuki H. Surgical treatment for Parkinson's disease. Advances in Parkinson's Disease Management. Albert Place, London: Future Medicine; 2012: 88-95. 33. Albin RL, Young AB, Penney JB. The functional anatomy of basal ganglia disorders. Trends Neurosci 1989; 12: 366-75. 34. Alexander GE, Crutcher MD. Functional architecture of basal ganglia circuits: neural substrates of parallel processing. Trends Neurosci 1990; 13: 266-71. 35. DeLong MR. Primate models of movement disorders of basal ganglia origin. Trends Neurosci 1990; 13: 281-5. 36. Wichmann T, DeLong MR, Vitek JL. Pathophysiological considerations in basal ganglia surgery: Role of the basal ganglia in hypokinetic and hyperkinetic movement disorders. Mov Disord Surg 2000; 15: 31-57. 37. Mink JW. The basal ganglia: focused selection and inhibition of competing motor programs. Prog Neurobiol 1996; 50: 381-425. 38. Heath RG. Electrical self-stimulation of the brain in man. Am J Psychiatry 1963; 120: 571-7. 39. Richardson D. History of DBS for Pain. In: Lozano A, Gildenberg P, Tasker R, editors. Textbook of Stereotactic and Functional Neurosurgery Berlin Heidelberg: Springer-Verlag; 2009: 204960. 40. Bergman H, Wichmann T, DeLong MR. Reversal of experimental parkinsonism by lesions of the subthalamic nucleus. Science 1990; 249: 1436-8. 41. Davis GC, Williams AC, Markey SP, et al. Chronic Parkinsonism secondary to intravenous injection of meperidine analogues. Psychiatry Res 1979; 1: 249-54. 42. 南部 篤.【脳深部刺激療法】脳深部刺激療法の作用機序. 脳 21 2004; 7: 262-9. 43. Hashimoto T, Elder CM, Okun MS, et al. Stimulation of the subthalamic nucleus changes the firing pattern of pallidal neurons. J Neurosci 2003; 23: 1916-23. 44. Bergman H, Feingold A, Nini A, et al. Physiological aspects of information processing in the basal ganglia of normal and parkinsonian primates. Trends Neurosci 1998; 21: 32-8. 45. Brown P. Oscillatory nature of human basal ganglia activity: relationship to the pathophysiology of Parkinson's disease. Mov Disord 2003; 18: 357-63. 46. Hammond C, Bergman H, Brown P. Pathological synchronization in Parkinson's disease: networks, models and treatments. Trends Neurosci 2007; 30: 357-64. 47. Levy R, Ashby P, Hutchison WD, et al. Dependence of subthalamic nucleus oscillations on movement and dopamine in Parkinson's disease. Brain 2002; 125: 1196-209. 48. Follett KA, Weaver FM, Stern M, et al. Pallidal versus subthalamic deep-brain stimulation for Parkinson's disease. N Engl J Med 2010; 362: 2077-91. 49. Weaver FM, Follett KA, Stern M, et al. Randomized trial of deep brain stimulation for Parkinson disease: thirty-six-month outcomes. Neurology 2012; 79 55-65. 50. Odekerken VJ, van Laar T, Staal MJ, et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson's disease (NSTAPS study): a randomised controlled trial. Lancet Neurol 2013; 12: 37-44. 51. Denheyer M, Kiss ZH, Haffenden AM. Behavioral effects of subthalamic deep brain stimulation in Parkinson's disease. Neuropsychologia 2009; 47: 3203-9. 52. 柏原健一.【脳深部刺激療法】脳深部刺激による認知, 精神機 能への影響. 神経内科 2010; 73: 489-96. 53. Temel Y, Kessels A, Tan S, et al. Behavioural changes after bilateral subthalamic stimulation in advanced Parkinson disease: a systematic review. Parkinsonism Relat Disord 2006; 12: 265-72. 54. Daniels C, Krack P, Volkmann J, et al. Risk factors for executive dysfunction after subthalamic nucleus stimulation in Parkinson's disease. Mov Disord 2010; 25: 1583-9. 55. Parsons TD, Rogers SA, Braaten AJ, et al. Cognitive sequelae of subthalamic nucleus deep brain stimulation in Parkinson's disease: a meta-analysis. Lancet Neurol 2006; 5: 578-88. 56. Mallet L, Schupbach M, N'Diaye K, et al. Stimulation of subterritories of the subthalamic nucleus reveals its role in the integration of the emotional and motor aspects of behavior. Proc Natl Acad Sci U S A 2007; 104: 10661-6. 57. Yelnik J. Functional anatomy of the basal ganglia. Mov Disord 2002; 17 (Suppl 3): S15-21. 58. Jenkinson N, Nandi D, Muthusamy K, et al. Anatomy, physiology, and pathophysiology of the pedunculopontine nucleus. Mov Disord 2009; 24: 319-28. 59. Garcia-Rill E, Skinner RD, Fitzgerald JA. Activity in the mesencephalic locomotor region during locomotion. Exp Neurol 1983; 82: 609-22. 60. Takakusaki K, Habaguchi T, Ohtinata-Sugimoto J, et al. Basal ganglia efferents to the brainstem centers controlling postural muscle tone and locomotion: a new concept for understanding motor disorders in basal ganglia dysfunction. Neuroscience 2003; 119: 293-308. 61. Jenkinson N, Nandi D, Aziz TZ, et al. Pedunculopontine nucleus: a new target for deep brain stimulation for akinesia. Neuroreport 2005; 16: 1875-6. 62. Stefani A, Lozano AM, Peppe A, et al. Bilateral deep brain stimulation of the pedunculopontine and subthalamic nuclei in severe Parkinson's disease. Brain 2007; 130: 1596-607. 63. Moro E, Hamani C, Poon YY, et al. Unilateral pedunculopontine stimulation improves falls in Parkinson's disease. Brain 2010; 133: 215-24. 64. Potter-Nerger M, Volkmann J. Deep brain stimulation for gait and postural symptoms in Parkinson's disease. Mov Disord 2013; 28: 1609-15. 65. 松村 賢.【脳深部刺激】パーキンソン病における脚橋被蓋 核 (PPN) 脳深部刺激術 (DBS) の可能性. 臨床脳波 2010; 52: 187-93. 66. Yelnik J. PPN or PPD, what is the target for deep brain stimulation in Parkinson's disease? Brain 2007; 130: e79; author reply e80. 67. Alam M, Schwabe K, Krauss JK. The pedunculopontine nucleus area: critical evaluation of interspecies differences relevant for its use as a target for deep brain stimulation. Brain 2011; 134: 11-23. 68. Schuurman PR, Bosch DA, Bossuyt PM, et al. A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor. New England J Med 2000; 342: 461-8. 69. Harries AM, Kausar J, Roberts SA, et al. Deep brain stimulation of the subthalamic nucleus for advanced Parkinson disease using general anesthesia: long-term results. J Neurosurg 2012; 116: 107-13. 70. Yamada K, Goto S, Kuratsu J, et al. Stereotactic surgery for subthalamic nucleus stimulation under general anesthesia: a retrospective evaluation of Japanese patients with Parkinson's disease. Parkinsonism Relat Disord 2007; 13: 101-7. 103 佐藤 澄人,他 71. Lozano AM, Dostrovsky J, Chen R, et al. Deep brain stimulation for Parkinson's disease: disrupting the disruption. Lancet Neurol 2002; 1: 225-31. 72. Nambu A. Somatotopic organization of the primate Basal Ganglia. Front Neuroanat 2011; 5: 26. 73. Nakano K. Neural circuits and topographic organization of the basal ganglia and related regions. Brain Dev 2000; 22 (Suppl 1): S5-16. 74. Olszewski J. The thalamus of the Macaca, mulatta. An atlas for use with the stereotaxic instrument. Basle Switzerland: New York, USA: S. Karger; 1952. 75. Hassler R. Architectonic organization of the thalamic nuclei. In: Schaltenbrand G, Walker A, editors. Stereotaxy of the Human Brain. Stuttgart: Georg Thieme Verlag; 1982: 140-80. 76. Krack P, Pollak P, Limousin P, et al. Opposite motor effects of pallidal stimulation in Parkinson's disease. Ann Neurol 1998; 43: 180-92. 77. Karachi C, Yelnik J, Tande D, et al. The pallidosubthalamic projection: an anatomical substrate for nonmotor functions of the subthalamic nucleus in primates. Mov Disord 2005; 20: 172-80. 78. Haynes WI, Haber SN. The organization of prefrontal-subthalamic inputs in primates provides an anatomical substrate for both functional specificity and integration: implications for Basal Ganglia models and deep brain stimulation. J Neurosci 2013; 33: 4804-14. 79. Hirai T, Jones EG. A new parcellation of the human thalamus on the basis of histochemical staining. Brain Res Brain Res Rev 1989; 14: 1-34. 80. Schaltenbrand G, Wahren W, Hassler RG. Atlas for Stereotaxy of the Human Brain: with an accompanying guide. Stuttgart: Thieme; 1977. 81. Ohye C. Thalamus and Thalamic Damage. In: Ramachandran VS, editor. Encyclopedia of the Human Brain. New York: Academic Press; 2002; 575-97. 82. Hamani C, Dostrovsky JO, Lozano AM. The motor thalamus in neurosurgery. Neurosurgery 2006; 58: 146-58; discussion 146-58. 83. Ohye C. Use of selective thalamotomy for various kinds of movement disorder, based on basic studies. Stereotact Funct Neurosurg 2000; 75: 54-65. 84. Ohye C, Shibazaki T, Hirai T, et al. Further physiological observations on the ventralis intermedius neurons in the human thalamus. J Neurophysiol 1989; 61: 488-500. 85. 片山容一,日本定位・機能神経外科学会. 定位・機能神経外 科治療ガイドライン 第2版. 協和企画 (発売); 2013. 86. Volkmann J, Albanese A, Kulisevsky J, et al. Long-term effects of pallidal or subthalamic deep brain stimulation on quality of life in Parkinson's disease. Mov Disord 2009; 24: 1154-61. 87. Moro E, Lozano AM, Pollak P, et al. Long-term results of a multicenter study on subthalamic and pallidal stimulation in Parkinson's disease. Mov Disord 2010; 25: 578-86. 88. Fasano A, Romito LM, Daniele A, et al. Motor and cognitive outcome in patients with Parkinson's disease 8 years after subthalamic implants. Brain 2010; 133: 2664-76. 89. Castrioto A, Lozano AM, Poon YY, et al. Ten-year outcome of subthalamic stimulation in Parkinson disease: a blinded evaluation. Arch Neurol 2011; 68: 1550-6. 90. Baron MS, Vitek JL, Bakay RA, et al. Treatment of advanced Parkinson's disease by unilateral posterior GPi pallidotomy: 4-year results of a pilot study. Mov Disord 2000; 15: 230-7. 91. Okun MS, Gallo BV, Mandybur G, et al. Subthalamic deep brain stimulation with a constant-current device in Parkinson's disease: an open-label randomised controlled trial. Lancet Neurol 2012; 11: 140-9. 92. Waln O, Jimenez-Shahed J. Rechargeable deep brain stimulation implantable pulse generators in movement disorders: patient satisfaction and conversion parameters. Neuromodulation 2013. 93. Rosin B, Slovik M, Mitelman R, et al. Closed-loop deep brain stimulation is superior in ameliorating parkinsonism. Neuron 2011; 72: 370-84. Surgical treatment for Parkinson's disease Sumito Sato, Toshihiro Kumabe Department of Neurosurgery, Kitasato University School of Medicine Surgery is complementary to medical treatment in patients with Parkinson's disease (PD). The chief surgical indications are drug-resistant severe tremor and motor complications such as wearing-off of drug effectiveness and dyskinesia due to the prolonged administration of levodopa. Whether the subthalamic nucleus (STN) or the pallidum should be the main target of deep brain stimulation (DBS) remains controversial. While in patients treated by STN-DBS the administrated dose of antiparkinsonian medications can be reduced, it tends to cause a cognitive decline and/or emotional changes. Patients with tremor-dominant PD may be good candidates for ventrointermedius thalamotomy or DBS. The pedunculopontine nucleus has become a new target for axial symptoms of PD. Although surgical treatment cannot stop the progression of PD, DBS is effective for longer than 6 years. Animal studies have contributed to an understanding of basal ganglia function and the pathophysiology of PD; however, more studies are warranted to clarify the precise mechanism of DBS. Key words: Parkinson's disease, thalamotomy, deep brain stimulation, basal ganglia 104
© Copyright 2026 Paperzz