Clinical Science (1995) 89, 505-510 (Printed in Great Britain)
505
Clinical remission is associated with restoration of
normal high-density lipoprotein cholesterol levels in
children with malignancies
Sandra DESSi. Barbara BATETIA, Ornella SPANO, Francesca SANNA, Mauro TONELLO*,
Mareva GIACCHINO*, Luciana TESSITOREt, Paola COSTELLlt, Francesco M. BACCINOt:\:,
Enrico MADON* and Paolo PANI
Dipartimento di Patologia Sperimentale, Universita di Cagliari, Cagliari, Italy, */stituto di
Discipline Pediatriche, Clinica Pediatrica III, Torino, Italy, tDipartimento di Medicina ed
Oncologia Sperimentale, Sezione di Patologia Generale, Universita di Torino, Torino, Italy,
and tCentro CNR di Immunogenetica ed Oncologia Sperimentale, Torino, Italy
(Received 20 January/5 July 1995; accepted 3 August 1995)
1. Serum lipids and lipoprotein profiles were determined in children affected by different types of
malignancies (Ieukaemias or lymphomas and solid
tumours) both before any treatment and after
remission of the disease following chemical or surgical therapy.
2. At the time of diagnosis, children bearing tumours
showed hypertriglyceridaemia and reduced concentrations of plasma high-density lipoprotein cholesterol
levels, the decrease being particularly prominent in
patients with haematological tumours. Children bearing solid tumours displayed an increase of total
cholesterol, while those with haematological cancer
showed decreased pbospholipid levels; low-density
lipoprotein cholesterol in neoplastic patients was not
significantly different from control values. High
triacylglycerol and low high-density lipoprotein cholesterol levels were also evident in cancer patients
divided according to age into three groups (6-5, 6-10
and 11-15years) when compared with age-matched
control subjects. Similarly, bigh triacylglycerol and
low high-density lipoprotein cbolesterol levels were
also observed in both male and female children when
patients were divided according to sex and compared
with corresponding controls.
3. Clinical remission after therapy was accompanied
by an increase of bigb-density lipoprotein cholesterol
levels compared with values observed at diagnosis. In
contrast, post-treatment levels of triacylglycerol were
higher than those observed before therapy. These
results support the hypothesis that alterations of highdensity lipoprotein cholesterol levels may be related,
at least in part, to the rate of tumour growth, while
modifications of triacylglycerol levels may be
mediated by different mechanisms.
INTRODUCTION
Alterations of cholesterol metabolism, including
increased cholesterol synthesis and accumulation of
cholesterol esters in tumour tissues associated with
a decrease of high-density lipoprotein cholesterol
(HDL-C) in serum, were previously observed in our
laboratories in different experimental models of
neoplastic cell proliferation [1, 2] as well as in
different types of human neoplasms, including haematological malignancies [3, 4]) and solid tumours
[5, 6]. In our studies, changes in other serum lipid
parameters, including total cholesterol (TC), lowdensity lipoprotein cholesterol (LDL-C), triacylglycerols (TAG) and phospholipids (PL), are not
consistent and appear to be species-specific and
dependent on the histological type and/or tumour
grade [1-6]. Therefore, it is possible that modifications of HDL metabolism during tumour growth
may be regulated by different mechanisms from
those involved in the observed changes in other
serum lipid parameters.
Despite the fact that low HDL-C levels seem to
represent a common feature during tumour growth,
the mechanisms involved in this change are currently unclear. Low HDL-C could be a consequence
of alterations in intracellular cholesterol metabolism
that accompany tumour growth. Human HDLs are
involved in maintaining normal cell cholesterol
homoeostasis by promoting the effiux of excess
cholesterol from peripheral tissues to the liver for
reutilization Or excretion into bile [7]. Thus, it
could be supposed that, during tumour growth, the
effiux of cholesterol mediated by HDL is decreased,
presumably to prevent loss of intracellular cholesterol pools which are needed for the assembling of
Key words: cholesterol metabolism, high-density lipoproteins, paediatric tumours.
Abbreviations: HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; PL, phospholipid; TAG, triacylglycerol; TC, total cholesterol.
Correspondence: Prof. Sandra Dessi, Dipartimento di Patologia Sperimentale, Via Porcell, 4, 09124 Cagliari, Italy.
506
S. Dessi et al.
new membranes. However, since precursor particles
of HDL are thought to derive from lipolysis of
TAG-rich lipoproteins, a reduced production of
HDL precursor particles due to decreased lipoprotein lipase activity [7] in tumour host is another
possibility that must be considered. Data in the
literature suggest that low HDL-C concentrations
are indicative of a condition of active cell proliferation, either normal or neoplastic [3, 8, 9]. Alterations of lipid and, particularly, of cholesterol
metabolism, are frequently observed during cancer
growth. Their evaluation as a means to detect the
presence of an early developing tumour has also
been considered [cf. 10]. Moreover, it has been
previously demonstrated that the severity of the
disease is inversely correlated with the HDL-C
levels [3, 6].
The aim of the present work was to evaluate
whether HDL-C levels are also altered in paediatric
cancer patients and whether any correlation exists
with the clinical remission of the disease.
surgical treatment. Patients were not receiving any
chemotherapy at the time of the second sampling.
Blood was collected from all children after an
overnight fasting, then centrifuged within 2 hand
the serum was stored at - 20°C until analysed.
Determination of plasma constituents
Albumin and prealbumin were separated electrophoretically and quantified following standard
laboratory procedures. Circulating insulin was
determined using the insulin radioimmunoassay kit
(Corning, Medfield, MA, U.S.A.).
Determination of serum lipids
PATIENTS AND METHODS
HDL-C was measured in the serum after removal
of very-low-density lipoprotein and LDL by phosphotungstic acid and magnesium chloride [cf. 11].
The concentrations of TC, HDL-C, TAG and PL
were determined enzymically using test kits from
Boehringer (Mannheim, Germany). LDL-C levels
were calculated using the following standard
formula: LDL-C = TC - HDL-C -(TAGj5).
Subjects
Statistical analysis
The study was conducted on 57 children (27
males), aged between 2 and 15 years, affected by
different types of malignancies and admitted to the
Regina Margherita Hospital, Istituto di Discipline
Pediatriche, Clinica Pediatrica III, Torino, Italy.
The study protocol was not submitted to the
Regional Ethical Committee as this was not necessary, according to the Italian rules concerning noninvasive experiments on human beings. There were
32 children affected by haematological neoplasms:
21 with acute lymphoblastic leukaemia (nine males),
four with B-lymphoma (two males), three with acute
non-lymphatic leukaemia (one male), two with Tlymphoma (one male), one with Burkitt's lymphoma
(male) and one with Hodgkin's disease (female). The
other 25 patients were solid-tumour bearers: nine
with osteosarcoma (four males), five with neuroblastoma (four males), three with cerebral tumours
(two males), three with Ewing's sarcoma (one male),
two with medulloblastoma (one male), two with
primary neuroectodermal tumour (one male) and
one with Wilms' tumour (female). A group of 30
children (21 males), aged 0-15 years, admitted to the
hospital with a diagnosis other than cancer or
metabolic disease was used as a control. At the time
of sampling, all children were free of drugs known
to affect lipid metabolism. Since sex and age may
induce modifications in lipid fractions, control subjects and cancer patients were subdivided according
to sex and into three age-groups (0-5 years, 6IOyears and 11--15 years).
Twenty of the 57 cancer patients (13 with haematological malignancies and 7 with solid tumours)
were also examined at the time of clinical remission,
i.e. about 4 or 5 months after chemotherapy or
Statistical significance was calculated by using the
Student's t-test. Paired t-test was applied to compare results in the group of children analysed both
at diagnosis and when the clinical remission of the
disease was obtained.
RESULTS
At the time the study was undertaken, no children
in either cancer or control groups showed any
clinical sign of cachexia nor was undernourished, as
routinely assessed in the hospital. Levels of albumin
and prealbumin were within the normal range
(albumin: 3.5-4.5 gjdl; prealbumin: 13-35 mgjdl).
As shown in Table 1, TC and LDL-C levels were
not different between control subjects and tumour
hosts. When patients were divided according to the
type of tumour (solid or haematological), no differences were observed for LDL-C between cancer
patients and control subjects, while TC was significantly increased in children bearing solid tumours
compared with control subjects.
Serum TAG levels were increased in cancer
patients, the difference being significant for both
children with haematological and solid tumours
compared with control subjects (Table 1). Interestingly, high insulin plasma levels were observed in
these patients (24.2 ± 3.55 fl-unitsjml, normal value
< 15fl-unitsjml). This is suggestive of an increased
peripheral insulin resistance, which could contribute,
at least in part, to the observed hypertriglyceridaemia.
In children with leukaemia or lymphoma, decreased concentrations of PL were also observed
(Table 1).
High-density lipoprotein cholesterol levels in children with tumours
507
Table I. Total cholesterol (TC), LDL-C, HDL-C, TAG and PL plasma levels in cancer-bearing children. Values are
means ± SEM. Statistical significance: *p < 0.05, **p < 0.01 compared with control subjects; tP < 0.05 compared with haematological
tumours.
TC
(mg/dl)
LDL-C
(mg/dl)
HDL-C
(mg/dl)
HDl-C
(% of TC)
Controls
30
138±9
91±6
42±2
30±1
85H
245±7
57
32
25
157±68
150±9
166±8*
103±5
99±8
108±8
28±2**
25 ±2**
33 +3*t
19± 1**
17± 1**
21 +2*
144±13**
158 ± 18**
125+16*
211 ±12
200± 14*
224+20
o
o
o
**
Controls
~Tumours
200
*
l4
l;r
;J;;
I
.:r
~ 100
<3
-,
50
•
-,
-,
;r
,"
0,
'0
20 ~
"
,
0
-,
::I:
-,
o
-,
1)...5
(",,10
-,
o 1)...5
u
...!.
o
10
'-, ,:r -,',1
~
8'
30
*
:::
J'
Controls
Tumours
I
.J
*
oS
PL
(mg/dl)
Tumours
All
Haematological
Solid
250
~ 150
TAG
(mg/dl)
"'"
(",,10 11-15 1)...5 (",,10 11-15 1)...5 (",,10 11-15 1)...5 (",,10 11-15
Age (years)
11-15
o
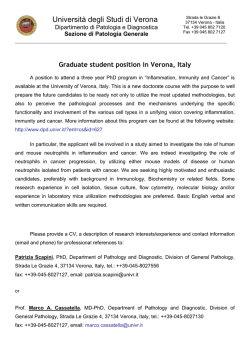
Fig. 2. HDL-C levels in cancer-bearing children divided according to
age. Each value is mean±SEM. Control subjects: 1)...5years (12), (",,1 0years
(10), 11-15 years (8). Patients: 1)...5years (17), (,...IOyears (24), 1I-15years
(16). Statistical significance: *p < 0.0 I compared with age-matched control
subjects.
'-----y----J '-----y----J '-----y----J '-----y----J
TC
LDL-C
TAG
PL
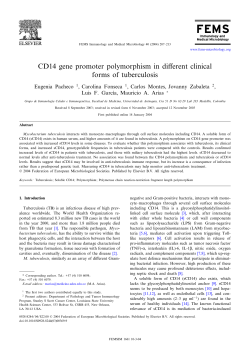
Fig. I. TC, LDL-C, TAG and PL levels in cancer-bearing children
divided according to age. Each value is mean ± SEM. Control subjects:
1)...5years (11), (,...IOyears (10), 11-I5years (8). Patients: 1)...5years (17),
(,...IOyears (24), 1I-15years (16). Statistical significance: *p <0.01 compared
with age-matched control subjects
The HDL-C levels were reduced in cancer
patients and, in addition, were significantly lower in
children with haematological tumours compared
with patients bearing solid tumours. The reduction
in HDL-C was even more evident when values were
expressed as percentages of TC (Table 1).
When control subjects were divided according to
age, no significant differences in plasma lipid parameters were observed between age groups, except
for PL levels which increased significantly in children aged 6-10 years compared with those aged ~5
years. (Fig. 1). These results are in agreement with
those reported for a general age-matched Italian
population of healthy children [11].
A significant increase of TAG and a concomitant
decrease in HDL-C was observed in all age groups
of cancer patients when compared with age-matched
control subjects (Figs 1 and 2). This difference
persisted when patients were analysed according to
sex (Figs. 3 and 4). No significant changes in other
lipid parameters were observed between cancer and
control groups (Fig. 1).
When patients were divided according to sex, no
significant differences were found in any of the lipid
parameters studied in the control group (Fig. 3); this
is in agreement with previously published data [11].
Similarly no alterations in these parameters were
(",,10
11-15
1)...5
Age (years)
250
o
200
!'"
150
5
<3'"
100
Controls
~Tumours
50
0
TC
LDL-C
TG
PL
rc
LDL-C
TG
PL
'----y
v ----)
Male
Female
Fig. 1 TC, LDL-C, TAG and PL levels in cancer-bearing children
divided according to sex. Each value is mean ± SEM. Statistical significance: *p < 0.0 I compared with corresponding control, **p < 0.01 compared with male cancer-bearing children.
detected when female and male cancer patients were
compared, except for a significant decrease in both
TC and LDL-C in female patients (Fig. 3).
Table 2 shows the levels of TC, LDL-C and PL
in 20 children studied both at diagnosis and at the
time of clinical remission of the disease. No changes
in these parameters were observed between the two
time points considered. However, an increase in
both HDL-C levels and in percentage HDL-CjTC,
was evident in children achieving remission from
S. Dessi et al.
508
DCont ros
I
DTumours
lI
40
*
40
*
rl-
30
~
~,
g-
20 ~
~
10
o
I
o
Male
Female
Male
Female
Fig. 4. HDL-C levels in cancer-bearing childrendivided according to
sex. Each value is mean ±SEM. Statistical significance: *P<O.OI compared
with corresponding control.
Table 2. Total cholesterol (TC), LDL-C and PL levels in childrenat
diagnosis and in remission of disease. Values are means ± SEM.
Diagnosis
Remission
20
20
TC (mgjdl)
LDL-C (mgjdl)
PL (mgjdl)
ISHII
164±10
10HI0
91 ± 10
236±17
19S±26
disease (Table 3). In contrast, TAG levels at
remission were higher than those observed before
treatment (Table 3).
DISCUSSION
The results shown in the present study confirm
that, in paediatric neoplastic patients, alterations of
lipid metabolism are already detectable at the time
of diagnosis, as previously demonstrated in adult
cancer hosts [3, 5, 6]. In particular, low HDL-C
levels together with hypertriglyceridaemia were the
most prominent features, being consistently present
in all cancer patients studied, either considered as a
group or divided according to age, sex or type of
neoplasm.
An increase in serum TAG associated with a
reduction of HDL-C has previously been observed
in both leukaemia and lymphoma adult patients
[12, 13]. It has been suggested that low HDL-C
concentrations may be secondary to a decreased
TAG clearance from plasma, a mechanism which
could also contribute to hypertriglyceridaemia [14,
15]. Precursor particles of HDL have in fact been
reported to derive from lipolysis of TAG-rich lipoproteins via lipoprotein lipase activity [7], and a
deficiency of this enzymic activity has been involved
in the development of hypertriglyceridaemia
observed in both experimental and human tumours
[14-16].
However, reduced levels of HDL-C are not constantly accompanied by hypertriglyceridaemia in
cancer patients [3, 5, 6, 17], suggesting that an
impairment of lipolysis of TAG-rich lipoproteins by
lipoprotein lipase is not the only factor responsible
for the altered HDL metabolism in these patients.
Consistent with this hypothesis is the observation
that tumour-bearing rats treated with antibodies
against tumour necrosis factor, a cytokine which
inhibits lipoprotein lipase activity [18], show a
partial normalization of TAG levels and of lipoprotein lipase activity while HDL-C levels remain
low [15, 19].
In the present study we also found that patients
with haematological neoplasms, which are known to
have cell turnover rates relatively higher than solid
tumours, also exhibit lower HDL-C levels. These
observations, together with previous data from our
laboratory [3, 5, 6], support the hypothesis that the
reduced HDL-C concentrations are, at least in part,
related to the rate of cell proliferation.
It is well known that the growth of tissues,
including tumour tissues, imposes the need for additional cholesterol availability to support membrane
biosynthesis. Alterations of intracellular cholesterol
metabolism in tumour tissues include increased
cholesterol synthesis and accumulation of cholesterol esters [1-6, 19]. A major function of HDL is
to remove excess cholesterol from peripheral tissues
[7]. Since in tumour cells, free cholesterol is preferentially diverted to storage as cholesterol esters [2],
it is conceivable that, during rapid tumour growth,
because of the increased demand in the cells, the
efflux of cholesterol is reduced. This fact could well
result in a reduction of the circulating levels of
HDL-C. Many studies in vitro support this conclusion. Exposure to HDL results in a net efflux of
cholesterol from various types of cultured cells [20,
21], this efflux being partially blocked in rapidly
proliferating cells and in transformed cell lines [22,
23]. Furthermore, Oram et al. [24] have demonstrated that HDL binds to cell surface receptors and
promotes selective removal of excess cholesterol
from the intracellular pool. The activity of these
receptors is dependent on both the availability of
exogenous cholesterol and the growth state of cells.
Treatment of quiescent cells with serum growth
factors suppresses both HDL receptor activity and
HDL-mediated efflux [25], while the opposite effect
is observed when cells are treated with growth
inhibitors [26].
Recently, a direct role of HDL levels in the
proliferative response of cells in vitro has also been
proposed [27-29]. Lowering HDL concentrations in
the culture medium was found to result in a stimulatory effect on DNA synthesis in the cells [30].
In this study, the observation that normal levels
of HDL-C are restored when clinical remission of
the disease is achieved further supports the existence
of a relationship between low HDL-C and the
proliferative rate of tissues.
To better clarify the mechanisms responsible for
cholesterol modifications during tumour growth, we
are currently investigating the rate of cholesterol
synthesis, esterification and efflux from the cells as
well as regulation of LDL and HDL receptors and
High-density lipoprotein cholesterol levels in children with tumours
509
Table 3. HDL-C and plasma TAG levels in children at diagnosis and in remission of disease. Abbreviation: ALL, acute
lymphoblastic leukaemia. Statistical significance: *p < 0.01, **p < 0.05 compared with values at diagnosis.
Patient
Diagnosis
Sex and age
in years
I
2
3
4
5
6
7
8
9
10
II
12
13
14
15
16
17
18
19
20
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
Osteosarcoma
Osteosarcoma
Osteosarcoma
Osteosarcoma
Osteosarcoma
Cerebral tumour
Cerebral tumour
M/8
MilS
M/3
FII2
M/12
F/IO
M/7
FI5
F/7
F/5
F/7
M/9
F/3
F/8
F/13
F/9
MilO
MilO
M/6
Mill
Mean ±SEM
HDL-C (mg/dl)
HDL-C (% of TC)
TAG (mg/dl)
Diagnosis
Remission
Diagnosis
Remission
Diagnosis
Remission
25
48
24
9
44
19
14
57
52
37
27
48
24
21
42
24
28
43
27
22
53
72
40
50
II
18
19
II
16
15
9
30
16
16
20
3
16
21
38
41
58
82
77
167
174
124
218
105
102
113
99
44
184
140
81
101
56
76
81
55
50
224
55
183
326
232
113
129
91
140
27
15
26
26
25
26
21
17
30
18
15
28
18
18
30
19
11
23
45
36
30
35
35
25
41 ±3*
IH2
2H2*
107±10
149 ± 15**
23
24
23
21
3
23
37
55
41
48
33
39
40
29±3
3-hydroxy-3-methylglutaryl coenzyme A reductase
gene expression in mononuclear blood cells from
healthy individuals and leukaemic patients.
ACKNOWLEDGMENTS
This work was supported by the Ministero
dell'Universita e della Ricerca Scientifica e Tecnologica, Roma, CNR (Special Project ACRO), Roma,
Associazione Italiana per la Ricerca suI Cancro,
Milano and Regione Autonoma della Sardegna.
REFERENCES
I. Rao KN, Kottapally S, Eskander ED, Shinozuka H, Dessi S, Pani P. Acinar cell
carcinoma of rat pancreas: regulation of cholesterol esterification. Br J Cancer
1986; 25: 305-10.
2. Dessi S, Batetta B, Anchisi C, et al. Cholesterol metabolism during the
growth of a rat ascites hepatoma (Yoshida AH-130). Br J Cancer 1992; 66:
787-93.
3. Dessi S, Batetta B, Pulisci D, Accogli P, Pani P, Broccia G. Total and HDL
cholesterol in human hematologic neoplasms. IntJ Hematol 1991; 54: 483-6.
4. Dessi S, Batetta B, Pulisci D, Broccia G, Pani P. Serum lipids and hematologic
neoplasms: aging and sex. In: Bergamini E, ed. General pathology and
pathophysiology of aging. Milan: Witching, 1993: 187-99.
5. Dessi S, Batetta B, Pulisci D, et al. Altered pattern of lipid metabolism in
patients with lung cancer. Oncology 1992; 8D849: 436-44.
6. Dessi S, Batetta B, Pulisci D, et al. Cholesterol content in tumor tissues is
inversely associated with HDL-cholesterol in serum in patients with
gastrointestinal cancer. Cancer 1994; 73: 253-8.
7. Eisenberg S. High density lipoprotein metabolism. J Lipid Res 1984; 25:
1017-58.
8. Dessi S, Batetta B, Laconi E, Ennas C, Pani P. Hepatic cholesterol in lead
nitrate-induced liver hyperplasia. Chem Bioi Interact 1984; 48: 271-9.
9. Dessi S, Chiodino C, Batetta B, Fadda AM, Anchisi C, Pani P. Hepatic
glucose-6-phosphate dehydrogenase, cholesterogenesis and serum lipoproteins
in liver regeneration after partial hepatectomy. Exp Mol Pathol 1986; 44:
169-76.
46
23
146
158
122
284
117
110
71
96
145
95
144
10. Kritchevsky SB, Wilcosky TC, Morris DL, Truong KN, Tyroler HA. Changes
in plasma lipid and lipoprotein cholesterol and weight prior to the diagnosis of
cancer. Cancer Res 1991; 51: 319S-203.
II. Maglietta V. Esami di laboratorio. In: Valori normali richiami diagnostici e dati
c1inici utili in pediatria. Milano: Casa Editrice Ambrosiana, 1995: 311-37.
12. Barclay M, Skipsi VP, Terebus-Kekish 0, Greene EM, Kaufman J, Stock cc.
Effects of cancer upon high density and other lipoproteins. Cancer Res 1970;
30: 242(}..30.
13. Spiegel RJ, Schaefer EJ, Magrath LT, Edwards BK. Plasma lipid alterations in
leukemia and lymphoma. Am J Med 1982; n: 775-82.
14. Lanza-Jacoby S, Lansey SG, Miller EE, Cleary MP. Sequential changes in the
activities of lipoprotein lipase and lipogenic enzymes during tumour growth in
the rat. Cancer Res 1984; 44: 5062-7.
15. Carbo N, Costelli P, Tessitore L, et al. Anti-tumour necrosis factor-oc
treatment interferes with changes in lipid metabolism in a tumour cachexia
model. Clin Sci 1994; 87: 349-55.
16. Shike M, Russell DM, Detsky AS. Changes in body composition in patients
with small-cell lung cancer. Ann Intern Med 1984; 101: 303-9.
17. Harwood HJ, Alvarez 1M, Noyes WD, Staepoole PW. In vivo regulation of
human leukocyte 3-hydroxy-3-methylglutaryl coenzyme A reductase: increased
enzyme protein concentration and catalytic efficiency in human leukemia and
lymphoma. J Lipid Res 1991; 32: 1237-52.
18. Evans RD, Argiles JM, Williamson DH. Metabolic effects of tumour necrosis
factor-oc (cachectin) and interleukin-1. Clin Sci 1989; Tl: 357-64.
19. Dessi S, Batetta B, Spano 0, et al. Perturbations of triglyceride but not of
cholesterol metabolism are prevented by anti-tumor necrosis factor treatment
in rats bearing an ascites hepatoma (Yoshida AH-130). Br J Cancer 1995 (In
press).
20. Daerr WH, Gianturco SH, Patsch JR, Smith LC, Gotto AM Jr. Stimulation and
suppression of 3-hydroxy-3-methyl-glutaryl coenzyme A reductase in normal
human fibroblasts by high density lipoprotein subclasses. Biochim Biophys Acta
1980; 619: 287-301.
21. Daniels RJ, Guertler LS, Parcher TS, Steinberg D. Studies on the rate of efflux
of cholesterol from cultured human skin fibroblasts. J Bioi Chem 1987; 256:
4978-83.
22. Gebhard RL, Clayman RV, Prigge WF, er al. Abnormal cholesterol metabolism
in renal clear cell carcinoma. J Lipid Res 1987; 28: 1177-84.
23. Pittman RC, Knecht TP, Resenbaum MS, Taylor CA Jr. A non-endocytotic
mechanism for the selective uptake of high density lipoprotein-associated
cholesterol esters. J Bioi Chem 1987; 262: 2443-50.
510
S. Dessi et al.
24. Oram JF. Johnson C, Brown TA. Interaction of high density lipoprotein with
its receptor on cultured fibroblasts and macrophages. J Bioi Chem 1987; 262:
24OS-10.
25. Bierman EL. Oppenheimer M, Oram JF. The regulation of HDL receptor
activity. In: Crepaldi G. Gotto AM, Manzato E, Baggio G. eds. Atherosclerosis
VIII. Amsterdam: Excerpta Medica. 1989: 297-300.
26. Oppenheimer, MJ. Oram JF. Bierman EL. Up-regulation of high density
lipoprotein receptor activity by interferon associated with inhibition of cell
proliferation. J Bioi Chem 1988; 263: 1931S-21
27. Favre G. Blaney J. Tournier F, Soula G. Proliferative effect of high density
lipoprotein (HDL) fraction (HDLI.l' HDL,). Biochim Biophys Acta 1989; 1013:
liS-H.
28. Favre G, Couzi C. Blaney E, Dousset JC. Soula G. Mitogenic effect of high
density lipoproteins (HDL) on Iymphoblastoid cells involved in HMG-CoA
reductase activity. Life Sci 1988; 150: 589-91
29. Cohen DC. Massoglia L. Gospodarowicz D. 3-Hydroxy-3-methylglutaryl
coenzyme A reductase activity of vascular endothelial cells: stimulation by high
density lipoproteins and its role in mitogenesis. J Bioi Chem 1982; 257:
1706-11
30. Favre G, Tazi KA. Le Gaillard F, Bennis F, Hachem H. Soula G. High-density
Iipoprotein,-binding sites are related to DNA biosynthesis in the
adenocarcinoma cell line A549. J Lipid Res 1993; 34: 1093-2106.
© Copyright 2026 Paperzz