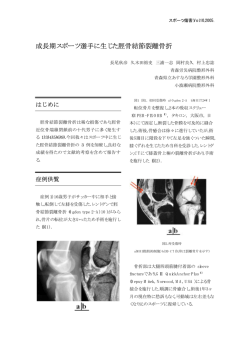
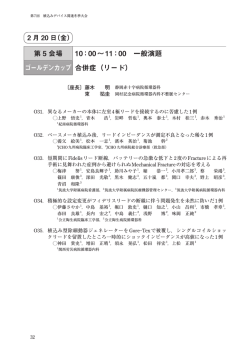
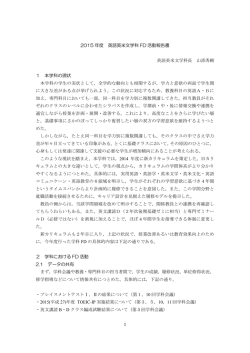
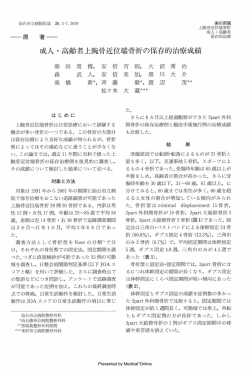
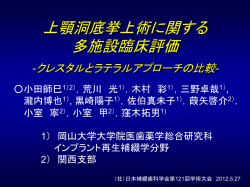
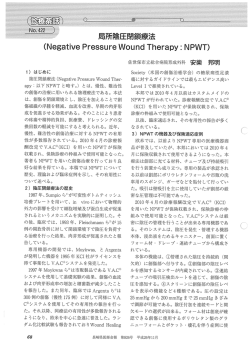
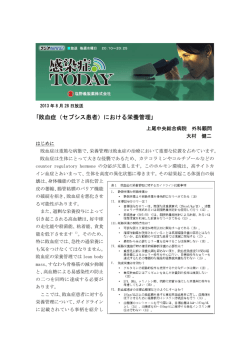
歯・顎・口腔・顔面� 島根大学�医学部�医学科� ��4年次生�チュートリアル講義� ・会話や表情� � ������ ・食事� 歯・顎・口腔・顔面外傷 ��������の診断と治療� 大切な機能と社会生活 ���を担う重要な器官� �� 歯科口腔外科学講座 �(主任:関根浄治教授) � ������� � ���� 講師�管野貴浩 (かんの�たかひろ)� Facial Skeleton 口腔外科領域の外傷治療� Fractures in Maxillo-Facial Area Calvaria Sphenoid Temporal 全身状態精査による合併損傷 (頭蓋内・胸 腔内・腹腔内・四肢損傷など。)� � Nasal B. 可及的速やかなOR-IF�24時間以内が勝負� Ethomoid B. Lacrimal B. � Zyg. Arch 新鮮骨折�VS�陳旧性(変治骨折)� 咬合・咀嚼・嚥下・発語(構音)・開口障害・眼球運動などの 機能障害を避ける 歯の保存� Zygoma Maxilla inf. Choncha 歯・顎・顔面の骨格形態の回復�� Mandible � これらの外傷治療は増加の一方で、口腔顎顔面 外傷治療の専門の医師が救急対応、かつ高度 な診療体制を整備している施設が少ない。� 早期の機能回復 と社会復帰� 救命救急センターと連携した香川県と同 様の顎顔面外傷センター in 島根 ������立ち上げに向けて!� 歯・口腔・顔面は複雑な構造と機能� 治療の開始が少しでも遅れると:� ・上手に噛めない�・口が開かない�・歯を抜く( 抜歯)・治療がより大変で複雑となる�・持続的な 痛みやより大きな傷跡などの後遺症� 機能回復の遅れ!� Japanese Physician Delivery Helicopter 2012年6月26日� 管野貴浩講師 “まめなかクラブ”収録� � 口腔顎顔面外傷治療:早期機能回復 歯・顎・口腔・顔面外傷の終日診療開始� (平成24年4月23日:報道発表記者会見, 山陰NHK番組特集)� � 十分なエビデンスに裏付けされた顎顔面外傷 の診断・治療手段・機材・術式の実践� 顎顔面OR-IF: Shampy technique, AO-CMF technique 治療のゴール� 顔面外傷治療とインプラントを用いた口腔機能再建� 歯/顎口腔機能再建/リハビリテーション� (平成24年6月26日:山陰ケーブルテレビ系列出演)� ,, / � 骨�折� / 早期社会復帰� Facial Skeleton: ! Mid-face + Mandibular fractures 鼻眼窩篩骨骨折 / 外力により骨の生理的連続性 が絶たれた状態� LeFort , , Netter FH. Atlas of Human Anatomy. East Hanover, Novartis,1997 1.顎骨骨折・顔面骨骨折� 1.全身状態の精査(救急部や関連各科と連携)� 2.初期治療からの口腔外科的専門診断と治療 顔面口腔機能障害:咬合、咀嚼、嚥下、発語(構音)、 開閉口、眼球機能 ���1)全身状態の把握と処置 ���2)局所状態の把握と処置 �� 早急な診断と治療 � が予後に直結� 治療のながれ JATEC/JPTEC� F t o o L 診断� full examination of the head, eyes, ears, nose, throat, and neck Examination Extra-oral (e.g. swelling, deformity, Asymmetry, CSF Leaks) Intra-oral (e.g. hematoma, occlusion) Palpation (e.g. irregularities, step deformity, crepitus, cracked pot sound, sensory disturbances) Radiographical investigations Imaging: Plain X-ray, CT (Axial, Coronal, Saggital, 3D) ABC’s: Primary Survey History 問診・・・・受傷状況をきくことにより推定 ��スポーツや喧嘩では1—2箇所の単純骨折。交通事故では ��他部位を含む広範かつ重篤な損傷を受けている可能性が高い 視診・触診・・顔面の変形、左右対称性 骨折による骨片偏位・異常可動性(非生理的可動性) ・軋轢(あつれき)音・malgeigneの圧痛点 軟組織の出血・疼痛・腫脹・知覚異常 運動障害(開閉口障害) 機能障害(咀嚼障害・発音障害・嚥下障害) 歯牙の破損・咬合異常・歯列異常 CT・単純X線写真(PA,LR,Panorama,Waters,Schuller,Grant-Lanting等) ・・骨折線の有無・骨片の偏位 � 研究用(石膏)模型・・歯列の状態から骨折・偏位の有無・程度を把握� CT以外の単純X線写真� 非観血的整復�徒手・各種副子(金属線など)を用いた整復を 行い、骨折骨片の安静を図り、骨癒合を待つ �����おもりやゴムによる牽引整復なども 適応:骨片偏位がない(わずか)、小児、手術拒否、 一部の骨折様態や部位(顎関節突起包内骨折など)� PA ��� Waters LR �� Panorama � ��� Schuller 15 � Grant-Lanting 咬合が基準:顎間固定:通常(2〜)4週間(〜6)� Surgical access Anatomical reduction � �観血的整復��切開により骨折部を露出し,(血餅・軟組織 ��������・仮骨を除去して)整復 近年では非観血的治療・ 保存療法の適応と選択は 非常に少ない。。。。� Internal fixation Functional rehabilitation Wide exposure of the fractured sites through adequate surgical access:手術アプローチ Reduction • T - Manual manipulation - Use of instruments and devices Internal fixation ! The goal is to restore the anatomy in all three dimensions, plating the maxillofacial buttresses wherever necessary. According to the quality and stability of the reduction, the final decision is made regarding the number of plates and screws, and the design of the plates. Forces of mastication Functional rehabilitation 長期間の顎間固定は顎関節の線維性強直と開口障害を引き起こす。 開口練習と食事の経口摂取を行い、3〜4横指 通常40 mm (男性45 mm、女性37 mm)程度の開口量を目指し訓練を行う。� 顎顔面外傷の受傷原因� ①�交通事故(35-56%) ②�転倒・転落 (11-25%) ③�殴打(けんか) (6-22%) Banks P. Fractures of the Facial Skeleton, Oxford, Wright 2001 Rowe NL. Maxillofacial Injuries. Edinburgh, Churchill Livingstone,1985 Skull base Occlusal Unit ! ④�スポーツ (6-14%) ⑤�作業事故 (4-16%) Nasal Fractures: 顎顔面外傷の疫学的特徴� Low-impact Fracture 7〜2 : 1 と圧倒的に男性に多い。 最近は女性の占める割合が、2〜1.5 倍に上昇。 • Most common of all facial fractures. • Injuries may occur to other surrounding bony structures. • Edema and tenderness • Epistaxis • Crepitus and mobility • Nasal deformity: 3 types: – Depressed – Laterally displaced – Nondisplaced 骨折は,10歳代と20歳代に多いが,軟 組織,歯,歯槽骨の損傷は,10歳未満に 多い。� ! ! Zygoma Arch Fractures Zygoma Fractures • The zygoma has 2 major components: – Zygomatic arch – Zygomatic body • Blunt trauma most common cause. • Two types of fractures can occur: – Arch fracture – Tripod fracture: through Zygomatic arch, Zygomaticofrontal suture, Inferior orbital rim and floor • Can fracture 2 to 3 places along the arch • Patients usually present with pain in cheek on opening their mouth. • Limited mandibular movement, Trismus • Palpable bony defect over the arch • Depressed cheek with tenderness ! Zygoma Tripod Fractures ! • Periorbital edema and ecchymosis • Hypoesthesia of the infraorbital nerve • Palpation may reveal step off deformity • Concomitant orbital globe injuries including eye motility are common • Impaired ocular motility. • Diplopia occasionally e PrePost-Ope Ope r , r 上顎骨骨折の特徴� 眼窩底吹き抜け骨折(blowout fracture)� • 上顎骨骨折:下顎骨骨折=1:10 • 歯 槽骨骨折が上顎骨骨折の70%を占め、前歯部 r に多い。 • 鼻骨・頬骨・側頭骨の合併骨折の頻度が高い。 • 顎 口腔領域の他の骨折に比べ、頭蓋損傷の併存 r する可能性が高い。 • 頭 蓋内損傷などにより治療開始までの期間が長 くなることがある(陳旧例として治療開始)。 • 非 観血的整復は困難であり基本的には観血的整 復固定を行う� • 眼窩縁には骨折がないにも関わらず、眼窩壁に骨折が生じ たものを吹き抜け骨折と呼ぶ。 • 正面からの強い外力を受けた結果、脆弱な眼窩下壁に骨 折が生じ眼窩内容物が逸脱する。 • 複視や眼球運動障害(上転障害)が生じる。� 術前CT� 51 顎顔面多発骨折:右側中顔面 (頬骨〜上顎〜眼窩)� �複視、眼球運動障害、右側中顔面陥凹� 術後4カ月� 術前� 術後� 術後6カ月� Maxillary Fractures: 術後機能評価良好� • • • • High energy injuries. Impact of 100G> the force of gravity is required . Patients often have significant multisystem trauma. Classified as LeFort fractures, Rene LeFort 1901 in cadaver skulls morphological study. • Frequently different levels on either side, LeFort I, LeFort II, LeFort III Kanno T, et al: Orbital Floor Reconstruction in ZygomaticOrbital-Maxillary Fracture with a Fractured Maxillary Sinus Wall Segment as Useful Bone Graft Material. Asian Journal of Oral and Maxillofacial Surgery, 2012 � Maxillary Fractures LeFort I – Horizontal fracture of the maxilla at the level of the nasal fossa: Floating maxilla at alar base – Allows motion of the maxilla while the nasal bridge remains stable. Le Fortの分類� Le Fort Ⅰ型 (上顎骨横骨折) 骨折線 梨状口下部 犬歯窩 (上顎洞前壁) 翼口蓋窩蝶形骨翼状 突起 Le Fort Ⅱ型 Le Fort Ⅲ型 (上顎骨錐形骨折) (頭蓋顔面分離骨折) 鼻骨横断 上顎洞前頭突起 眼窩下縁 下眼窩裂 頬骨上顎縫合 上顎前頭縫合 鼻骨前頭縫合 眼窩内側 下眼窩裂 頬骨前頭縫合 – Facial edema – Malocclusion of the teeth, hypoesthesia of teeth – Motion of the maxilla while the nasal bridge remains stable Kanno T, Int J Oral Maxillofac Surg, 2008 Maxillary Fractures LeFort II – Pyramidal fracture: Central midface fracture • Maxilla- Nasal bones : Floating maxilla at Nasion • Medial aspect of the orbits – Facial edema – Dish face, Flat nose, Enophthalmos – Traumatic telecanthus - Epistaxis or CSF rhinorrhea – Movement of the central midface and the nose. – Malocclusion of the teeth, hypesthesia – Impaired ocular motility – lacrimal duct obstruction Maxillary Fractures LeFort III – Fractures through: separation of midface to skull base • Maxilla- Zygoma- Nasal bones- Ethmoid bones • Base of the skull : Floating maxilla at Nasion&Maxilla 36歳�男性�就業上の不慮の事故� 早期からの専門的治療で顎口腔機能と歯をまもる� 顎は動かず全く噛めず、眼も2重に 見える。� 眼を支える骨や、上あご・下あ ごの骨がばらばらで、このまま 治療が遅れてしまっては大変! – Dish faced deformity - Epistaxis and CSF rhinorrhea - Motion of the maxilla, nasal bones and zygoma - Traumatic telecanthus Severe airway obstruction – Malocclusion of the teeth - Impaired ocular motility ・ばらばらの歯と骨を元通りの良いかみ合わせ(咬合)に 戻して、眼の下を補強し、プレートとネジで固定する手術。� 治療後3か月� 下顎骨骨折:Mandibular Fractures� 歯槽骨骨折 骨体部骨折 下顎角部骨折 下顎枝部骨折 関節突起部骨折 筋突起部骨折� 一本の歯も失うことなく綺麗に噛め、骨折後の経過、眼の 機能も元通りに回復し、何でも美味しく食べられます。� 下顎骨骨折の特徴� 下顎骨骨折の部位別頻度� 関節突起部� • 顔面頭蓋骨の骨折では下顎骨が最も頻度が高 い(60%)。 筋突起部� • 関節突起は介達骨折により骨折を起こしやすい。 • 骨片偏位を生じる。 • 下歯槽神経損傷によりおとがい部知覚麻痺が生 下顎枝部� じる。 • 外傷により顎関節円板・靱帯・筋肉などが損傷し た場合には顎関節症が発生することがある。� 骨折による骨片の偏位� 側頭筋� 外側翼突筋� 《外側面》 《内側面》 咬筋� 顎舌骨筋� 内側翼突筋� 顎二腹筋� おとがい舌骨筋� 外側翼突筋� 顎舌骨筋� おとがい舌骨筋� 骨体部 オトガイ部 (前歯部)� (臼歯部)� 下顎角部� 下顎骨骨折症例� 28歳�女性�高所から転落して受傷�� 早期からの専門的治療で顎口腔機能と歯をまもる� ・ばらばらの歯と骨を元通りの良いかみ合わせ(咬合)に 戻して、プレートとネジでしっかりと固定する手術を行う。� 食事はすぐに柔らかいものを食べられます。� 治療後3か月� 一本の歯も失うことなく綺 麗に元通りに回復治癒� 非常に多い顎関節突起骨折治療 � Or �非観血的(保存的)治療 ��観血的治療�� ・骨片の観血的整復� (口内法、口外法)� ・顎内固定� プレートスクリューシステム� � ・骨折受傷部の安静を図る� ・顎間固定� ・早期開閉口リハビリ� ・トレーニングエラスティック� ��������� Controversial� 長期的臨床的予後� :良好な機能回復� �� われわれの治療コンセプト� 何でも美味しく食べられます。� ・早期顎口腔機能回復(翌日から経口摂食)� ・早期社会復帰(早期手術・術後早期退院)� � 顎関節突起骨折のバイオメカニズム 顎関節突起骨折の特徴 ・下顎骨骨折: 全顎顔面骨骨折の65 - 70% ・下顎骨関節突起・顎関節突起骨折: 下顎骨骨折の17.5 - 52%� そのほとんどは下顎骨他部位に加わる外力による� Hunting Bow Concept� Shape, strongest in the symphysis and weakest at the condyles � 介達骨折� Ellis E3rd, et al: Oral Surg Oral Med Oral Pathol, 1985� TMJ:顎関節�functional structures are in harmony with� • Muscle • Occlusion • TMJ Structure Biomechanics for ideal osteosynthesis lines Ideal osteosynthesis lines by Champy according to the tension strain lines � Champy M, 1975, Condyle region Adapted by Meyer� Meyer C, et al: J Craniomaxillofacial Surg, 2007 & 2008� 下顎骨関節突起骨折・顎関節突起骨折の分類� 顎関節突起骨折骨片の骨折様態の分類 解剖学的骨折部位の分類 A. 関節胞内骨折 Intracapsular Fractures B. 頸部骨折 Condylar Neck AO and Ellis E3rd, et al: J Oral Maxillofac Surg, 1999� Fractures C. 基底部骨折 Condylar base (subcond) Fractures A. 変位なしNon-displacement : Normal relationship of the condylar head to the glenoid fossa B. 変位Displacement : Condyle head remains within the glenoid fossa : Size of the joint space has changed C. 脱臼Dislocation : Condyle head is out of glenoid fossa MacLennan WD: Br J Plast Surg, 1952 柴原孝彦: 口腔外科ハンドマニュアル’07� SORG and Loukota RA, et al: Br J Oral Maxillofacial Surg, 2005 & IBRA, 2009� 治療適応 患者年齢: Another critical key factor:重要因子 保存療法 vs 外科療法・手術治療 (OR-IF) Tx.� Strategy for management still remains a source of ongoing controversy� The therapeutic goal in adult patients differs from that in growing patients, since in children and adolescents the condyle is a major growth center for the mandible.� Lindahl L: Int J Oral Maxillofac Surg, 1989 保存療法:Conservative functional (activator) Tx Treatment alternatives: How do you treat? – Non-surgical- soft diet, observation and physical therapy – Closed reduction- utilizes a certain period of IMF and the following a long-term physical therapy – Open reduction- and internal fixation� Conservative (Closed) Tx could be better indicated and adapted frequently for condylar head, diacapitualar fractures � De Riu G, et al: Int J Oral Maxillofac Surg, 2001 Regardless of displacement� Delaire J, et al: Rev Stomatol Chir Maxillofac, 1975 In all circumstances� Assel LA, et al: J Oral Maxillofac Surg, 2001 Time! Effort! Cooperation!� vs� Chrcnovic BR: Oral Maxillofac Surg, 2012 Neff A: Mund Kiefer Gesichtschir, 2000, 2002 6 M follow-up� 6Y Boy� なぜ未だに治療法のコンセンサスがないのか? 手術治療・観血的治療 (OR-IF) Tx� VS� 保存的治療・Conservative Tx� GA, Surgery “invasiveness”� “Acceptable” functional results� Operative scar� Risk of facial nerve � High risk of ・ Chronic TMJ pain ・ Malocclusion ・ Deviation of mouth opening� Restoration functionally and morphologically in shape � Earlier return to normal function� Much longer time of treatment with elastics for occlusal guidance � Modified, Eckelt U, IBRA, Quintessenz, 2009� Internal fixation modalities Operative (Surgical) Treatment Surgical Approaches Biomechanical evaluation of different types of rigid internal fixation techniques � ! Submandibular (Risdon) Approach ! Retromandibular Approach ! Preauricular Approach ! Rhytidectomy Approach ! Postauricular Approach ! Intraoral Approach (Endoscopically-assisted) Tominaga K, et al: J Oral Maxillo fac Surg, 2006 Double adaptation plates fixation technique proved to have superior biomechanical stability in both fracture conditions � 4-times difference in biomechanical strength� Throckmorton GS and Deehow PC: Arch Oral Biol 1994� https://www2.aofoundation.org/ wps/portal/surgery� Randomized clinical trial: two miniplates fixation represented the best solution to obtain functionally more stable osteosysthesis and less complication� Rai A: Ann Maxillofac Surg, 2012 われわれの顎関節突起骨折の治療 � ・早期顎口腔機能回復�・早期社会復帰� � 1 w-MMF at CO Ope-based simplified classification� and rehabilitation� Our clinical strategy� (公社)日本口腔外科学会�外傷ガイドライン 関節突起骨折分類図より抜粋� Extraoral OR-IF via retromandibular approach Intraoral OR-IF� Indication for OR-IF� (Endoscopillary-assited intraoral OR-IF) � All the growing patients < 16 yrs should be treated conservatively first� High-Low - Subcondylar Fx� OR-IF: anatomic reduction and rigid-internal fixation Retromandibular transparotid approach � Double-buttress technique with two-2.0mm locking miniplates A feasible and safe, minimally invasive surgical technique that provides reliable clinical results� AO, Synthes MatrixMandible 2.0� Kanno T, et al: Int J Oral Maxillofac S urg, 2013, accepted 顎関節突起骨折症例� 49歳�男性 自転車にて転倒し受傷� 術後�3カ月� Or� Intraoral OR-IF with angulated screw driver system with endoscopic assistance non-displaced or non-deviated simple linear fractures� 早期機能回復/社会復帰 � 小型内視鏡を併用したより低侵襲な顎関 節突起骨折OR-IF手術� Time consuming on preparation, operation and requiring skills! Low subcondylar- condylar base Fx� Transoral OR-IF with angulated screw driver system without endoscopic assistance� 1. Schmelzeisen R, et al: Patient benefit from endoscopically assisted fixation of condylar neck fractures--a randomized controlled trial. J Oral Maxillofac Surg, 2009. 2. Kanno T, et al: Submandibular approach through the submandibular gland fascia for 2. treating mandibular fractures without identifying the facial nerve, The Journal of Trauma, 2009 古木良彦、管野貴浩、 他:完全口内法での整復固定術を施行した関節突起 基底部骨折の2例�Hosp Dent&Oral-Maxillofac Surg, 2009 Offering reliable clinical results, and safe and minimally invasive surgery� Kanno T, et al: J Oral Maxillofac Surg, 2011 大切なポイント!� 軽傷外傷:�命には別状ありませんので、明 ����今すぐにでも� 日にでも(週明けに)歯科口腔外科に行って 下さい。 重症外傷:命が助かって良かったですね。� 2.歯と歯槽骨の外傷� 歯の脱臼(抜けてしまう)� 可能な限り早期に専門的治療を行うことで より早い回復とより良く綺麗に治せます。� ・外傷性歯脱臼:外力による歯への損傷が強 いと、歯は歯槽窩から脱出する。 ��完全脱臼、不完全脱臼、陥入 ・歯槽骨骨折:歯と同時に周囲歯槽骨の骨折 を伴うことも多い。 顎顔面骨骨折の治療開始が遅くなれば 、それだけ回復が遅れ、機能障害や歯を 守れなくなる可能性が高くなります。� �� � 脱落した歯牙の保存� 顔面外傷の内、歯の損傷及び歯槽骨骨折 の占める割合は約45%である。� 不完全脱臼歯は早期の整復と暫間固定 歯髄壊死には抜髄処置 完全脱臼歯は条件が良ければ再植術� ①歯の外傷� �� 1.破折� 歯冠破折:露髄の有無� 歯根破折:破折位置� 速やかな治療が予後に影響� ①歯槽骨骨折� � 2.完全脱臼� 歯根膜の保存がすべて (30分以内)� 生食、唾液、牛乳、歯牙保存液� 非常に厄介!!:X線評価では困難な場合が多い� 3.不完全脱臼� ・触診にて歯が個別に動揺:歯の脱臼または破折。隣 接歯及び歯周組織が一緒に動揺する場合は最も疑 われる。� 動揺:生理的動揺は0.2mm以内� 挺出:予後良い� 転位:予後比較的良い� ・骨膜、歯肉の付着する歯槽骨は保存する。� 陥入:予後悪い� � 21歳�女性�自転車での交通事故� ・救急隊員が脱臼歯を道路から 拾って生理食塩水中に保存し て持参してくれた。 ・直ぐに口腔外科の専門的治 療が行えた。� 元通りの噛み合わせの位置に戻してから 歯のギプス(暫間固定)� 食事はすぐに柔らかいものを食べられます。� 歯はしっかりと生着も歯の神経は回復せず 神経の処置はかかりつけ歯科にて施行。 事故・治療から4年経過しても経過良好です!� � 16歳�男性�野球部での練習中に受傷� ・保健室の先生が脱臼歯 を拾って歯の保存液に入 れ持参してくれた。 ・直ぐに口腔外科の専門 的治療が行えた。� 元通りの噛み合わせの位置に戻してから�歯 外傷性歯脱臼と歯槽骨骨折: であれば、ぴったりと元通りにもどせます� “�すぐ”�のギプス(暫間固定)� �����これでは全く噛めず、食べられず� すぐに柔らかいものを食べられ 、野球もできます� � 1か月後�歯の神経も回復し骨折も治癒 大切なポイント!� 早期の口腔外科・歯科の専門治療:出来るだ け早く脱落や抜けそうな歯を、もとの位置に戻し 、固定することが大切です。� 完全脱臼した歯でも助けることができます。� 脱落した歯を乾燥させないように保存 液(学校など)、生理食塩水や唾液(だ えき)、牛乳のなかに入れて受傷後すぐ の専門機関の受診・連絡を!� 24歳�女性�前日階段から転落して受傷� ・脱臼歯を探したが見つ からなかった。 ・直ぐに口腔外科の専門 的治療が行えた。� 治療後1年経過しても非常に綺麗です � ただし、非常に高価です。 �����1歯で、約40万円!� どうしても歯がない時には インプラント治療(人口の歯と歯根)も可能です� (自費治療)� 患者様を第一にした親切・丁寧な治療を心掛けて います。���� THANK YOU ! Dr. Takahiro KANNO, DDS, PhD, FIBCSOMS
© Copyright 2026 Paperzz