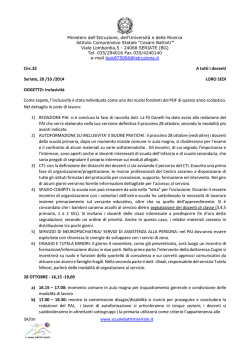
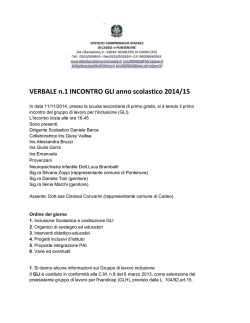
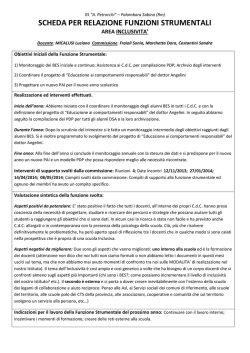
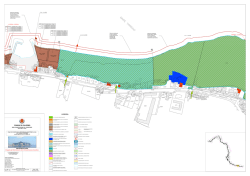
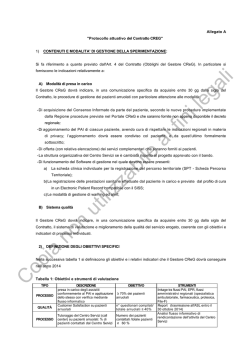
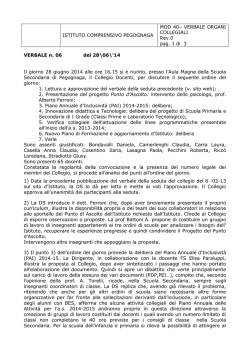
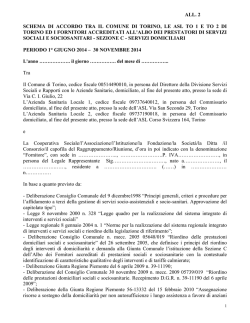
Twin Research (2000) 3, 277–293 © 2000 Macmillan Publishers Ltd All rights reserved 1369–0523/00 $15.00 www.nature.com/tr Categor i es of ∆F508 homozygous cysti c fi br osi s tw i n and si bl i ng pai r s w i th di sti nct phenotypi c char acter i sti cs Frauke M ekus1, M anfred Bal l mann 1, Inez Bronsvel d 2, Jan Bi jman 3, Henk Veeze4 and Burkhard T ümml er 1 1 Clinical Research Group, Department of Pediatrics, Medizinische Hochschule Hannover, Germany Department of Pediatrics, Sophia Children’s Hospital, Rotterdam, The Netherlands 3 Department of Cell Biology 4Department of Clinical Genetics, Erasmus University Rotterdam, The Netherlands 2 Cysti c fi br osi s (CF), the most common sever e autosomal r ecessi ve tr ai t among Caucasi ans, i s caused by mol ecul ar l esi ons i n the cysti c fi br osi s tr ansmembr ane conductance r egul ator gene (CFTR). The cour se of the mul ti -or gan di sease CF i s hi ghl y var i abl e, suggesti ng the i nfl uence of envi r onmental factor s and/or modul ati ng genes other than CFTR on the di sease phenotype. To eval uate the cause of CF di sease var i abi l i ty, the Eur opean CF Tw i n and Si bl i ng Study col l ected data on tw o cl i ni cal par ameter s most sensi ti ve for the cour se and pr ognosi s of CF, i e w ei ght pr edi cted for hei ght (w fh)% (r epr esentati ve for the nutr i ti onal status) and FEVPer c (r epr esentati ve for the pul monar y status) for a cohor t of 277 si bl i ng pai r s, 12 pai r s of di zygous tw i ns and 29 pai r s of monozygous tw i ns. Of these 318 CF tw i n and si b pai r s, 114 w er e r epor ted to be homozygous for the most fr equent CF di sease-causi ng l esi on, ∆F508. I ntr a-pai r di scor dance w as assessed by the i ntr a-pai r di ffer ences w i th w fh% and FEVPer c and by DELTA , a composi te par ameter defi ned by l i near combi nati on of w fh% and FEVPer c i n or der to descr i be di scor dance w i th r espect to the over al l di sease sever i ty. M onozygous tw i ns had a si gni fi cantl y l ow er DELTA than di zygous tw i ns (P = 0.05) i ndi cati ng that CF di sease sever i ty i s modul ated by an i nher i ted component i n addi ti on to the CFTR gene i tsel f. Extr eme phenotypes ar e consi der ed to be mor e i nfor mati ve for the anal ysi s of any quanti tati ve tr ai t. Thus, w e ai med to quanti fy di sease sever i ty and i ntr a-pai r di scor dance i n or der to sel ect pai r s w i th the extr eme phenotypes DI S (di scor dant pati ent pai r s), CON + (concor dant and mi l dy affected pati ent pai r s) and CON – (concor dant and sever el y affected pati ent pai r s). The al gor i thm r el i abl y di scr i mi nated betw een pai r s DI S, CON + and CON – among the cohor t of ∆F508 homozygotes. The sel ected pai r s fr om these categor i es demonstr ated non-over l appi ng pr oper ti es for w fh%, FEVPer c and the i ntr a-pai r di ffer ence of both par ameter s. Twin Research (2000) 3, 277–293. Keyw or ds: cysti c fi brosi s di sease severi ty, affected rel ati ve pai r, tw i n and si bl i ng study, extreme phenotypes, al gori thm based sel ecti on I ntr oducti on Cysti c fi brosi s (CF) i s know n as the most common severe autosomal recessi ve di sease w i thi n the Caucasi an popul ati on, exhi bi ti ng an i nci dence of 1 i n 2500 bi rths.1 The symptoms of the di sorder are caused by an i mpai red functi on of exocri ne gl ands i n many organs, but major mani festati ons i nvol ve the respi ratory and the gastroi ntesti nal tracts.1 The di sease i s caused by mutati ons i n both chromosomal copi es of the cysti c fi brosi s transmembrane conductance regul ator (CFTR) gene.2 The course of CF i s hi ghl y vari abl e w hen compari ng unrel ated pati ents w i th i denti cal CFTR mutati on genotypes,3,4 or even CF si bl i ngs w ho carry the same CFTR al l el es and share several envi ronmental factors, such as soci oCorrespondence: Dr Frauke M ekus, Kl i ni sche Forschergruppe, Department of Pedi atri cs, OE 6711, M edi zi ni sche Hochschul e Hannover, D-30625 Hannover, Germany. Tel : + 49 511 5326722; Fax: + 49 511 5326723; E-mai l : M ekus.Frauke@M H-Hannover.de Recei ved 2 June 2000; accepted 24 Jul y 2000 economi c status, general l i vi ng condi ti ons and therapeuti c measures. Thi s i ndi cates the i mpact of factors other than the CFTR genotype on the CF di sease phenotype. By studyi ng affected pati ent pai rs, the European CF Tw i n and Si bl i ng Study pursues a cl assi c approach to address the rel ati ve i mpact of the CFTR gene, other i nheri ted factors and envi ronmental effects on CF di sease. A pproxi matel y 70% of CF al l el es i n central European popul ati ons bear the same CFTR mutati on ∆F508.5 Consequentl y, hal f of al l CF pati ents are homozygous for the same CFTR l esi on w hi ch enabl es anal ysi s of the di sease severi ty i n a group w i th a homogeneous mutati on genotype i n the major di sease-causi ng gene. Due to the preval ence of one mutati on genotype i n a so-cal l ed monogeni c di sease that fol l ow s an autosomal recessi ve trai t, CF i s the onl y i nheri ted di sorder i n w hi ch a rel ati vel y l arge number of pati ent pai rs can be sel ected w ho carry the same mutati on genotype i n the di sease-causi ng gene. Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y y Categories of CF patient pairs with distinct phenotypes F Mekus et al 278 The search for di sease-modul ati ng factors of CF equal s the assessment of CF di sease severi ty as a quanti tati ve trai t, w hereby the phenotype under i nvesti gati on – the CF di sease severi ty – assumes a conti nuous di stri buti on. Under thi s condi ti on, i ndi vi dual s w i th extreme phenotypes are l i kel y to have a l arge number of functi onal al l el es at most l oci determi ni ng the quanti tati ve trai t, and therefore extreme phenotypes are general l y consi dered to be most i nformati ve.6–9 Based on the phenotype of an i ndi vi dual , three categori es of pati ent pai rs w i th extreme phenotypes can be di sti ngui shed: concordant/ mi l dl y affected pati ent pai rs (CON + ) composed of tw o si bl i ngs w i th mi l d di sease, concordant/ severel y affected pati ent pai rs (CON –) compri sed of tw o severel y di seased si bl i ngs, and di scordant pai rs (DIS) w herei n one si bl i ng i s mi l dl y affected and the other i s severel y affected. Wi th the ai m of i denti fyi ng these most i nformati ve pai rs, w e l ooked for quanti tati ve descri pti on of di sease severi ty and i ntra-pai r di scordance for CF pati ents. The eval uati on w as based on tw o cl i ni cal parameters most sensi ti ve to course and prognosi s of CF di sease, i e w ei ght expressed as w ei ght predi cted for hei ght (w fh% ) – so as to assess the nutri ti onal status of the CF pati ent – and val ues of forced expi ratory vol ume i n 1 s (FEV1) expressed as age and gender normal i sed parameter, so as to assess the pul monary status of the CF pati ent.10 A s a resul t, the CF di sease phenotype w as rated accounti ng for both major affl i cted organs, i e the respi ratory and the gastro-i ntesti nal tracts. M ethods Patients and clinical parameters CF pati ent pai rs w ere enrol l ed from 158 CF cl i ni cs i n 14 European countri es. Usi ng a one-page eval uati on form, i nformati on on gender, CFTR genotype, actual w ei ght, hei ght and forced expi ratory vol ume i n 1 s (FEV1) and the zygosi ty status of tw i n pai rs w as requested. From these data, tw o cl i ni cal parameters most sensi ti ve to course and prognosi s10 w ere cal cul ated: nutri ti onal status w as assessed by w fh% on the basi s of age and gender corrected centi l es for w ei ght and hei ght by Prader et al.11 Pul monary status w as assessed by FEV1% pred w hi ch are predi cted val ues referri ng to the non-CF popul ati on based on the data by Knudson et al.12 A mong CF pati ents, FEV1% pred decl i nes w i th age13 (Fi gure 1b) as expected for thi s progressi ve l ung di sease. To correct for the CF-speci fi c age decl i ne of FEV1% pred, age-corrected centi l es for the CF popul ati on for FEV1% pred, cal l ed FEVPerc, w ere cal cul ated based on the European CF regi stry Fi gur e 1 A ge dependence of w fh% (a), FEV1% pred (b) and FEVPerc (c). The sol i d l i ne i ndi cates the medi an, the dotted l i nes the i nner quarti l es. The number of pati ents w i thi n each age group are: < 7 y: 36, 7–10 y: 75, 10–12.5 y: 66, 12.5–15 y: 75, 15–17.5 y; 84, 17.5–20 y: 76, 20–22.5 y: 48, 22.5–25 y: 50, 25–30 y: 58, > 30 y: 68 (ERCF) report of 199614 w hi ch compi l es l ung functi on data of FEV1% pred from 25 667 CF pati ents from A ustri a, Canada, Denmark, France, Germany, Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 279 Irel and, The Netherl ands, Sw eden, the Uni ted Ki ngdom and USA . Consi stent w i th data from other cross-secti onal studi es, the centi l es w ere age-i ndependent for w fh% 15 (Fi gure 1a) and for FEVPerc (Fi gure 1c) i n the cohort of CF tw i n and si bl i ng pai rs. Evaluation of mono and dizygosity status of CF twins combi nati ons of tw o i ndi vi dual s resul t i n an IRND of 1, but there i s onl y one possi bi l i ty to obtai n the maxi mal IRND of m = (n – 1), by occupyi ng rank numbers 1 and n, respecti vel y. In general , the probabi l i ty f m for any IRND m i n a cohort of n i ndi vi dual s i s gi ven by the normal i sed expressi on fm = Where DNA w as avai l abl e, the zygosi ty status of tw i n pai rs w as assessed to confi rm the i nformati on provi ded by the CF centre usi ng the A mpFLSTR Profi l er Pl us™ typi ng ki t on an A BI Pri sm 377 (Perki n El mer A ppl i ed Bi osystems, Foster Ci ty, CA , USA )16 or by ol i gonucl eoti de fi ngerpri nti ng of si mpl e repeats appl yi ng in situ gel hybri di sati on of MboI or HinfI genomi c di gests.17 n –m = 2 n –m n n –1 ; n – m Σ ( n –1 n –1 ) Σf m =1 (3) m =1 m =1 To test w hether the IRND di stri buti on observed among the CF tw i ns and si bl i ngs di ffered from a j random IRND di stri buti on, cl asses of IRNDs Σ ƒm m=i w ere defi ned w hereby the boundari es w ere chosen such that each cl ass w as occupi ed w i th the same j probabi l i ty i n a random IRND di stri buti on: Σ ƒm = m=i Defi nition of composite parameters const. The si ze of the cl asses w as set to an expec- To assess the overal l CF di sease severi ty and the i ntra-pai r di scordance, the tw o cl i ni cal parameters descri bi ng a pati ent’s nutri ti onal and pul monary status, i e w fh% and FEVPerc, w ere combi ned. Rank numbers x i for w fh% and y i for FEVPerc w ere assi gned to the compl ete pati ent cohort, w hereby a rank number of 1 i ndi cated the most severel y affected state. The di sease severi ty of pati ent i w as characteri sed by the di stance form ori gi n (DfO) i n the pl ot of x i versus yi (Fi gure 2). The i ntra-pai r di scordance w as quanti fi ed by the di stance betw een tw o data poi nts representi ng tw o pati ents i and j of a pai r w i thi n the same di agram (DELTA ). Thus di sease severi ty and i ntra-pai r di scordance w ere defi ned by: tancy val ue E = n ( Σ ƒm ), w here E = 20, 30 or j DfO = 冪x i + yi 2 2 (1) DELTA = 冪(x i – x j ) + (yi – yj ) 2 m=i 50 coupl es per cl ass. For the anal ysi s of the cohort of al l CF tw i ns and si bs, rank numbers w ere assi gned to w fh% for 467 pai rs (n = 934, correspondi ng to 24 (E = 20), 16 (E = 30) and 9 (E = 50) IRND cl asses) and to FEVPerc 2 (2) Analysis of intra-pair rank number difference (IRND) distributions Intra-pai r si mi l ari ty of CF tw i ns and si bl i ngs w as characteri sed by compari son of the pati ent pai r cohort w i th a set of unrel ated coupl es. To assess the i ntra-pai r si mi l ari ty of the compl ete cohort, the di stri buti on of i ntra-pai r rank number di fferences (IRND) w as anal ysed. The IRND di stri buti on expected for unrel ated coupl es w as deri ved as fol l ow s. For a cohort of n i ndi vi dual s, or n/ 2 pai rs, IRNDs betw een 1 and (n – 1) are possi bl e. The mi ni mal IRND of m = 1 i s obtai ned i f tw o i ndi vi dual s from a coupl e occupy rank numbers (n – 1) and n. (n – 1) rank number Fi gur e 2 Defi ni ti on of composi te parameters. The tw o cl i ni cal parameters, w fh% and FEVPerc, descri bi ng the pati ent’s nutri ti onal and pul monary status, w ere combi ned as a measure of the pati ent’s overal l di sease severi ty. Rank numbers for w fh% and for FEVPerc w ere assi gned to al l pati ents. The di sease severi ty of a pati ent w as characteri sed as di stance form ori gi n (DfO) i n the pl ot of the pati ent’s rank number for FEVPerc vs the rank number for w fh% . The i ntra-pai r di scordance w as quanti fi ed through the di stance betw een tw o data poi nts representi ng tw o pati ents i and j of a pai r w i thi n the same di agram (DELTA ). For the set of 318 pai rs, maxi mal val ues of DfO and DELTA as defi ned by equati ons (1) and (2) are 899 and 898, respecti vel y Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 280 for 318 pai rs (n = 648, correspondi ng to 16 (E = 20), 11 (E = 30) and 7 (E = 50) IRND cl asses). Wi thi n the cohort of ∆F508 homozygous tw i ns and si bl i ngs, rank numbers for w fh% and FEVPerc w ere assi gned to 114 pai rs (n = 228, correspondi ng to 6 (E = 20), 4 (E = 30) and 2 (E = 50) IRND cl asses). Observed occupancy of IRND cl asses w as compared w i th expectancy val ues by χ2 stati sti cs.18 at the CF cl i ni c i n Hannover (646 entri es). The EUCFR regi stry recorded the best FEV1% pred w i thi n a 2 year peri od, w hereas i n our study the questi onnai re asked for the most recent l ung functi on data. Comparison of disease severity and intra-pair discordance Zygosi ty status w as determi ned or rel i abl y reported by the CF centre for 41 tw i n pai rs w i th w fh% and FEVPerc avai l abl e (Tabl es 1, 2, 4), ∆F508 al l el e frequency w as 0.67, consi stent w i th popul ati on geneti c data for central Europe.5 The average age of DZ tw i ns w as sl i ghtl y l ow er than that of M Z tw i n pai rs, and ∆F508 homozygous tw i ns w ere younger on the day of eval uati on compared w i th ∆F508 heterozygous tw i ns, but the di fferences i n age w ere not si gni fi cant (Tabl e 2). There w as no bi as betw een M Z and DZ tw i ns i n respect of country of ori gi n (Tabl e 3). How ever, w hereas ∆F508 homozygous tw i ns w ere recrui ted from several European countri es, pai rs from Ital y w ere over-represented among ∆F508 heterozygous pai rs, refl ecti ng the l ow er ∆F508 frequency i n southern European countri es5 (Tabl e 3). Compari ng M Z and DZ tw i ns, the groups w ere i ndi sti ngui shabl e i n w fh% but FEVPerc w as si gni fi cantl y l ow er for DZ tw i ns than for M Z tw i ns (P = 0.02; Tabl e 4). Intra-pai r di scordance w as assessed by the i ntrapai r di fference i n w fh% (representati ve of nutri ti onal status), the i ntra-pai r di fference i n FEVPerc (representati ve of pul monary status) and DELTA (composi te parameter descri bi ng di scordance i n Unl ess stated otherw i se i n the resul ts secti on, al l compari sons w ere carri ed out usi ng the non-parametri c M ann-Whi tney rank test.19 Resul ts Clinical data on 318 CF twin and sibling pairs Data on w fh% w ere obtai ned for both pati ents i n 467 pai rs. Compl ete cl i ni cal data, i e w fh% and FEVPerc, coul d be cal cul ated for 318 CF pati ent pai rs (Tabl es 1, 2, 5), of w hi ch 114 pai rs w ere reported to be ∆F508 homozygous. FEVPerc w as l ow er i n our pati ent pai r cohort than expected from the ERCF report (Tabl e 5a, Fi gure 1c). Thi s systemati c shi ft refl ects di fferent modes of data col l ecti on and coi nci des w i th the w el l know n di fference betw een best and average annual val ues of FEV1% pred w hi ch w as al so demonstrated by the average 8.2% di fference betw een best and mean annual FEV1% pred val ue for the pati ent popul ati on Clinical data on monozygous and dizygous CF twin pairs Tabl e 2 Tabl e 1 Sib pairs mm ff mf Non-6F508/ non-6F508 Non-6F508/ 6F508 6F508/ 6F508 Total Median Twins DZ MZ 75 72 130 3 2 7 14 15 0 88 94 95 3 5 4 2 12 15 277 12 29 Non-6F508: al l CFTR al l el es other than 6F508, i ncl udi ng CFTR al l el es w i th unknow n mutati on; m: mal e; f: femal e. Tabl e 3 Di stri buti on of age at day of eval uati on of CF Genotype and gender of 318 CF tw i n and si bl i ng pai rs Tw i n pai rs M onozygous (29 pai rs) Di zygous (12 pai rs) n.s. Non-6F508/non-6F508 (17 pairs) 6F508/ 6F508 (19 pai rs) n.s. Si bl i ng pai rs A l l si bl i ngs (277 pai rs) 6F508/ 6F508 (95 pai rs) P=0.005 Inner quartiles Range 14.9 years 8.8–21.8 6.8–37.2 14.6 years 11.0–17.9 6.1–31.3 15.1 years 12.2–22.9 6.8–37.2 12.7 years 8.8–17.3 6.1–30.3 17.2 years 12.1–23.5 5.9–59.1 16.9 years 11.2–20.3 6.0–38.1 Country of ori gi n of CF tw i n pai rs M onozygous Di zygous Non-6F508/ 6F508 6F508/ 6F508 France Number of pairs (% ) recruited from: UK & Eire Germany Italy Other a 4 (14% ) 2 (17% ) 3 (18% ) 3 (16% ) 5 (17% ) 2 (17% ) 4 (24% ) 3 (16% ) 6 (17% ) 2 (17% ) 2 (12% ) 6 (32% ) 7 (24% ) 3 (25% ) 2 (12% ) 5 (26% ) 7 (24% ) 3 (25% ) 6 (35% ) 2 (11% ) a Total number of pai rs recrui ted from The Netherl ands, Sw eden, Pol and, A ustri a and Sw i tzerl and. Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 281 respect of overal l di sease severi ty, Fi gure 2). Regardi ng CF tw i n pai rs w i th al l CFTR genotypes, M Z pati ent pai rs had a si gni fi cantl y l ow er DELTA than DZ tw i n pai rs, but i ntra-pai r di fferences i n w fh% and FEVPerc w ere comparabl e for M Z and DZ tw i ns (Tabl e 4). zygous tw i ns and si b pai rs w as si gni fi cantl y more concordant i n IRND di stri buti on of the nutri ti onal parameter w fh% (Tabl e 6 and Fi gure 3). In contrast, the IRND di stri buti on of FEVPerc i n the ∆F508 homozygous pai rs w as i ndi sti ngui shabl e from that of randoml y assi gned coupl es. The range of i ntra-pai r di fferences i n w fh% or FEVPerc w as si mi l ar i n the w hol e cohort of CF pati ent pai rs and i n the ∆F508 homozygous sub-group (Tabl e 5). Intra-pair rank number difference distribution in a cohort of CF twins and siblings To characteri se the cohort of CF tw i ns and si bs i n terms of i ntra-pai r si mi l ari ty, the di stri buti on of i ntra-pai r rank number di fferences (IRND) of the pati ent pai r cohort for w fh% and FEVPerc w as compared w i th the IRND di stri buti on of a set of randoml y assi gned coupl es (see eqn 3). The IRND di stri buti on of the CF pati ent pai rs di ffered si gni fi cantl y from a random IRND di stri buti on (Tabl e 6 and Fi gure 3), i e the average IRND w as si gni fi cantl y l ow er i n CF tw i n and si b pai rs than i n unrel ated coupl es. Li kew i se, the sub-group of ∆F508 homoTabl e 4 Properties of discordant CF patient pairs The age-i ndependent cl i ni cal parameters w fh% and FEVPerc w ere l i nearl y combi ned to defi ne the composi te parameters DfO (eqn 1 and Fi gure 2), as a measure of the overal l di sease severi ty based on equal w ei ght of both anthropometri c and l ung functi on parameters. The parameter DELTA , defi ned as the absol ute di stance betw een the DfO val ues of a tw i n or si b pai r (eqn 2)w as taken as the i ndi cator of i ntra-pai r di fferences of di sease severi ty (Fi gure 2). Di sease mani festati on and i ntra-pai r di scordance of CF tw i ns Median Monozygous (58 patients) Inner quartiles Range Median Dizygous (24 patients) Inner quartiles Range P Di sease mani festati on w fh% FEVPerc 98.9 49.6 91.9–109.4 30.6– 74.6 72.0–136.7 0.5–111 98.7 28.4 92.6–109.6 16.0– 55.0 84.2–125.7 0.1–114 0.43 0.02 Intrapai r di scordance w fh% FEVPerc 5.8 13.8 3.0– 9.3 6.0– 23.9 0.4– 23.9 0.0– 69.8 6.6 27.8 3.8– 11.7 5.6– 49.8 0.7– 21.0 1.7– 92.6 0.48 0.14 Composi te parameter DELTA 145.1 78.2–213.6 17.1–366.0 179.1 135.6–215.3 70.4–510.1 0.04 Tabl e 5 Di sease mani festati on and i ntra-pai r di scordance i n CF si bl i ngs All CF siblings (277 pairs) Median Inner quartiles Range Median 6F508/ 6F508 (95 pairs) Inner quartiles Range P Di sease mani festati on w fh% FEVPerc 100.1 43.8 91.0–109.2 21.2– 74.7 54.5–175.8 –3.0–120 98.7 34.6 89.5–105.5 16.5– 60.6 54.5–145.2 –3.1–115 0.002 <0.0001 Intrapai r di scordance w fh% FEVPerc 11.3 23.4 5.7– 18.5 11.8– 41.7 0.1– 61.4 0.0– 96.9 10.2 24.1 6.1– 15.6 11.9– 42.7 0.3– 53.4 0.0– 96.9 0.21 0.41 Composi te parameter DELTA 244.8 145.0–349.1 8.1–771.6 253.3 179.0–347.9 46.1–694.8 0.13 Tabl e 6 P val ues of r2 test compari sons of IRND di stri buti ons of CF tw i n and si bl i ng pai r cohorts w i th expected IRND di stri buti ons for a cohort of random coupl es A l l pai rs w fh FEVPerc 6F508 homozygotes w fh FEVPerc E=20 E=30 E=50 (647 pai rs) (318 pai rs) P<0.001 P<0.001 P<0.001 P<0.001 P<0.001 P<0.001 (114 pai rs) (114 pai rs) 0.025<P<0.05 0.9 <P<0.95 0.025<P<0.05 0.7 <P<0.9 0.025<P<0.05 0.9 <P<0.95 E: number of pai rs expected w i thi n each IRND cl ass, see M ethods for detai l s. Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 282 Fi gur e 3 Di fferences of i ntra-pai r rank number di fference (IRND) di stri buti ons compari ng a cohort of CF tw i ns and si bl i ngs w i th a cohort of random coupl es of si mi l ar si ze. (a) for w fh% for pati ent pai rs w i th vari ous CFTR genotypes (467 pai rs, 9 IRND cl asses, 50 pai rs expected w i thi n each IRND cl ass; E = 50); (b) for FEVPerc and pati ent pai rs w i th vari ous other CFTR genotypes (318 pai rs, 7 IRND cl asses, 50 pai rs expected w i thi n each IRND cl ass; E = 50); (c) for w fh% and (d) FEVPerc of ∆F508 homozygous pai rs (114 pai rs, 4 IRND cl asses, 30 pai rs expected w i thi n each IRND cl ass; E = 30). Bars representi ng the 9, 7, 4 and 4 IRND cl asses i n (a)–(d) are ordered accordi ng to the magni tude of the IRNDs from l ow IRND to hi gh IRND. To al l ow compari son of data, the scal e w i thi n pl ots (a)–(d) i s normal i sed so as to di spl ay a 75% devi ati on from the expectancy val ue E w i th E = 50 (a) and (b) and E = 30 (c) and (d). In pl ots (a) and (b), + 75 corresponds to an occupati on of an IRND cl ass by 88 pai rs and –75 corresponds to an occupati on of an IRND cl ass by 13 pai rs i n contrast to the expected 50 pai rs. By anal ogy, i n pl ots (c) and (d) + 75 corresponds to an occupati on of an IRND cl ass w i th 52 pai rs and –75 corresponds to an occupati on of an IRND cl ass w i th 8 pai rs i n contrast to the expected 30 pai rs A s show n i n Fi gure 4, the val ue of DELTA di d not correl ate w i th the i ntra-pai r age di fference of si b pai rs. Di scordant pai rs, i ndi cated by hi gh val ues of DELTA , w ere observed at a si mi l ar frequency i n si bpai rs w i th hi gh and l ow age di fferences. For 318 pati ent pai rs carryi ng vari ous CFTR genotypes, the maxi mum rank number that can be assi gned to w fh% or FEVPerc val ues i s, by defi ni ti on, 636. There w as no correl ati on betw een the i ntra-pai r rank number di fferences for w fh% and FEVPerc (data not show n): pati ent pai rs w ere Fi gur e 4 Composi te parameter DELTA and i ntra-pai r age di fference. DELTA w as defi ned as i ndi cated i n Fi gure 2 based on rank numbers for w fh% and FEVPerc to quanti fy i ntra-pai r di scordance. Cl osed ci rcl es: di zygous CF pati ent pai rs. Open ci rcl es: monozygous CF tw i n pai rs observed to be di scordant for both parameters, or onl y di scordant for w fh% , but concordant for FEVPerc and vi ce versa. A mong monozygous tw i ns, the hi ghest val ue for the composi te parameter DELTA w as 366; 64 di zygous pati ent pai rs had val ues for DELTA > 366. These extremel y di scordant pai rs coul d be grouped i n three cohorts as i ndi cated i n Fi gure 5: 15 pai rs w ere concordant i n w fh% but di scordant i n FEVPerc (cohort I), 25 pai rs w ere concordant i n FEVPerc but di scordant i n w fh% (cohort II) and 24 pai rs w ere di scordant for both parameters (cohort III). These three phenotypes w ere di sti ngui shed nei ther by the pati ent’s absol ute val ues for age, w fh% or FEVPerc, nor by the i ntra-pai r age di fference (see l egend and tabl e to Fi gure 5. There w as a trend tow ards over-representati on of ∆F508 homozygotes i n cohort I compared w i th cohorts II and III (P = 0.15; Fi sher’s exact test).20 The average val ue for DELTA w as hi ghest i n cohort III and average val ues for i ntra-pai r di fferences i n DfO w ere l ow er for cohort I (Fi gure 5) than for cohort II and III. The i ntra-pai r di fference i n DfO (Di ffDfO) di fferenti ated betw een pai rs w ho are di scordant (II, III) and not di scordant (I) i n w fh% . By defi ni ng a di scordant pai r (category DIS) as one composed of a si bl i ng w i th l ow DfO and a si bl i ng w i th hi gh DfO, pai rs from cohort I coul d be di sti ngui shed from pai rs bel ongi ng to the category DIS by taki ng i nto account the i ntra-pai r di fference i n DfO (Di ffDfO). Tabl e 7 show s cl i ni cal data from tw o Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 283 the i ntra-pai r sum of DfO (ΣDfO) i s a measure of di sease severi ty: mi l d: hi gh ΣDfO w i th both si bl i ngs di spl ayi ng w fh% and FEVPerc val ues above the 75th centi l e (exampl e III), moderate: i ntermedi ate ΣDfO w i th both si bl i ngs di spl ayi ng w fh% and FEVPerc val ues cl ose to the 50th centi l e (exampl e IV) and severe: l ow ΣDfO w i th both si bl i ngs di spl ayi ng w fh% and FEVPerc val ues bel ow the 25th centi l e (exampl e V). Defi nition of rank numbers ∆F508 homozygous pati ent pai rs (Exampl es I and II) w i th si mi l ar hi gh DELTA but di fferent Di ffDfO to i l l ustrate thei r phenotypi c di fferences. Properties of concordant CF patient pairs To i denti fy concordant pai rs, tw o characteri sti cs, i e concordance and di sease severi ty, had to be combi ned to di sti ngui sh betw een concordant pai rs w i th mi l d phenotype and concordant pai rs w i th severe phenotype. In Tabl e 7, data from three ∆F508 homozygous pati ent pai rs (Exampl es III, IV, and V) representati ve of the phenotypes ‘concordant/ mi l dl y affected’ (category CON + , exampl e III), ‘concordant/ moderatel y affected’ (exampl e IV) and ‘concordant/ severel y affected’ (category CON – exampl e V) are show n. These three pai rs al l have si mi l ar l ow val ues of DELTA and i ntra-pai r di fference i n DfO (Di ffDfO), i ndi cati ng thei r concordance. In concordant pai rs, Based on DELTA , the i ntra-pai r sum of DfO and the i ntra-pai r di fference i n DfO (Di ffDfO), 5 rank numbers w ere cal cul ated (Tabl e 8): DISCDELTA defi ned the pai r’s posi ti on i n the sequence of di scordant pai rs, w hereby the di scordance w as quanti fi ed sol el y on the basi s of DELTA . The most di scordant pai rs w ere recogni sed by l ow DISCDELTA . Rank numbers w i thi n the sequence of concordant pai rs w ere assi gned by l i nearl y combi ni ng a parameter descri bi ng the di sease severi ty of a pai r w i th a parameter descri bi ng the pai r’s di scordance. For i nstance, i n a di agram w here the rank number for DELTA w as assi gned to the x axi s (w hereby rank number 1 corresponded to the l ow est DELTA , i e the most concordant pai r) and the rank number for ΣDfO w as assi gned to the y axi s (w hereby rank number 1 corresponded to the hi ghest val ue for ΣDfO, i e the most mi l dl y affected pai r), the data set cl osest to the ori gi n defi ned the most concordant/ mi l dl y di seased pai r, under these cri teri a. A ccordi ngl y, the rank number for the di stance from ori gi n i n thi s di agram w as used to defi ne + + . By anal ogy, CON –DELTA , CON Di CON DELTA ffDfO and – CON Di ffDfo, w ere defi ned as i n Tabl e 8. Thus the four + + , CON –DELTA , CON Di rank numbers for CON DELTA ffDfO – and CON Di ffDfO defi ned a pai r’s posi ti on i n the sequences CON + and CON –, w herei n di scordance w as defi ned vi a the composi te parameter DELTA and the pai r’s posi ti on i n the sequence CON + and CON – w hen di scordance w as defi ned vi a Di ffDfO. In Fi gure 6, rank numbers DISCDELTA (Fi gure 6e), + (Fi gure 6f), CON –DELTA (Fi gure 6g), CONCON DELTA + – Di ffDfO (Fi gure 6h) and CON Di ffDfO (Fi gure 6i ) are graphi cal l y di spl ayed for monozygous tw i ns. Intrapai r di fferences of rank numbers for w fh% and FEVPerc w ere l ow er for ∆F508 homozygous tw i ns (Fi gure 6a, b) and monozygous tw i ns w i th other genotypes (Fi gure 6c, d) (P = 0.0005 for w fh% and P = 0.01 for FEVPerc). Rank numbers for DISCDELTA w ere si gni fi cantl y l ow er for ∆F508 homozygous monozygous tw i ns than for di zygous ∆F508 homozygotes (Fi gure 6e, P = 0.05, M ann-Whi tney rank + , CONtest). In contrast, rank numbers for CON DELTA – + – DELTA , CON Di ffDfO and CON Di ffDfO w hi ch w ere defi ned by a l i near combi nati on of a parameter descri bi ng the di sease severi ty and a parameter descri bi ng the Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 284 Tabl e 7 Exampl es of CF pati ent pai rs age (years) Sibling A wfh% FEVPerc Si mi l ar hi gh DELTA , di fferent i ntra-pai r di fferences i n DfO Exampl e I 25 119.5 [578] 1 [12] DELTA = 514 Di ffDfDO = 206 Exampl e II 20 103.1 [389] 75 [490] DELTA = 497 Di ffDfO = 418 Si mi l ar DELTA , di fferent i ntra-pai r sum of DfO Exampl e III 8 134.3 [618] 100 [624] DELTA = 105 Di ffDfDO = 106 YDfO = 1650 Exampl e IV 18 94.9 [222] 66 [446] DELTA = 92 Di ffDfDO = 90 YDfO = 1086 Exampl e V 14 92.2 [176] 14 [121] DELTA = 90 Di ffDfDO = 14 YDfO = 412 DfO age (years) Sibling B wfh% FEVPerc DfO 578 [502] 21 120.0 [582] 82 [526] 784 [588] 625 [432] 16 878 [634] 94.2 [206] 1 [27] 207 [115] 9 115.9 [550] 87 [543] 772 [574] 498 [273] 12 98.4 [284] 79 [515] 588 [360] 281 [107] 6 93.9 [197] 199 [112] 2 [33] Graphi c representati on of di sease severi ty and i ntra-pai r di scordance of these pai rs appears i n Fi gure 9. Exampl e I; 9l , pai r 1; exampl e II: 9h, pai r 7; exampl e III: 9d, pai r 1; exampl e IV: 9m, pai r 3; exampl e V: 9a, pai r 5. DELTA and DfO: composi te parameters as defi ned i n Fi gure 2; Di ffDfO: i ntra-pai r di fference i n DfO; YDfO: i ntra-pai r sum of DfO. * Fi gures i n brackets represent Rank numbers assi gned to w fh% , FEVPerc and DfO i n the cohort of 318 pati ent pai rs. Tabl e 8 Defi ni ti on of rank numbers DISCDELTA , CON + DELTA , CON + Di ffDfO , CON – DELTA and CON – Di ffDfO Sequence of di scordant pai rs: rank number deri ved from one parameter: DISCDELTA rank number for DELTA rank number for DISCDELTA = 1: hi ghest DELTA > most di scordant pai r Sequence of concordant pai rs: rank number deri ved from combi nati on of tw o parameters: al l rank numbers are defi ned as di stance from ori gi n i n a pl ot w hereby the fol l ow i ng parameters are assi gned to: CON CON CON CON + DELTA + Di ffDfO – DELTA – Di ffDfO x axis y axis rank number for DELTA rank number for DELTA = 1 > l ow est DELTA most concordant pai r cl osest to ori gi n rank number for YDfO rank number for YDfO =1: hi ghest YDfO mi l dest affected pai r cl osest to ori gi n rank number for Di ffDfO rank number for Di ffDfO = 1 > l ow est Di ffDfO most concordant pai r cl osest to ori gi n rank number for YDfO rank number for YDfO =1: hi ghest YDfO mi l dest affected pai r cl osest to ori gi n rank number for DELTA rank number for DELTA = 1 > l ow est DELTA most concordant pai r cl osest to ori gi n rank number for YDfO rank number for YDfO =1: hi ghest YDfO most severel y affected pai r cl osest to ori gi n rank number for Di ffDfO rank number for Di ffDfO = 1 > l ow est Di ffDfO most concordant pai r cl osest to ori gi n rank number for YDfO rank number for YDfO =1: l ow est YDfO most severel y affected pai r cl osest to ori gi n DELTA and DfO: composi te parameters as defi ned i n Fi gure 2; Di ffDfO: i ntra-pai r di fference i n DfO; YDfO: i ntra-pai r sum of DfO. Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 285 Fi gur e 6 Intra-pai r di scordance (a)–(d) and rank numbers (e)–(i ) for monozygous tw i n pai rs. Intra-pai r di fferences of rank numbers are show n for w fh% (a), (c) and FEVPerc (b), (d) for monozygous ∆F508 homozygous tw i ns (open ci rcl es i n (a), (b) and monozygous tw i ns w i th other CFTR genotypes (open squares i n (c), (d)). The maxi mal i ntra-pai r rank number di fference of 636 i s di spl ayed for a total of 318 pati ent pai rs. Rank numbers (Tabl e 8) for ∆F508 homozygous monozygous tw i ns obtai ned from the cohort of 114 ∆F508 homozygous + + – ; (g) rank CON –DELTA ; (h) rank CON Di pati ent pai rs are di spl ayed i n (e)–(i ): (e) rank DISCDELTA ; (f) rank CON DELTA ffDfO; (i ) rank CON Di ffDfo. Except for rank DISCDELTA , no si gni fi cant di fferences w ere found compari ng the rank numbers betw een the 15 monozygous and the + 99 di zygous ∆F508 homozygous pati ent pai rs: (e) rank DISCDELTA , P = 0.05; (f) rank CON DELTA , P = 0.17; (g) rank CON –DELTA , P = 0.07; (h) + – , P = 0.29; (i ) rank CON , P = 0.17 rank CON Di ffDfO Di ffDfO Tabl e 9 – Defi ni ti on of pati ent pai r categori es DIS, CON +, CON , ND, DC(1) and DC(2) by rank number characteri sti cs DISCDELTA CON +DELTA CON CON CON + ND hi gh hi gh hi gh hi gh l ow l ow DIS DC (1) DC (2) l ow l ow l ow hi gh hi gh hi gh Category – – – CON +Di ffDfO CON l ow hi gh l ow hi gh l ow l ow l ow hi gh l ow (a), (b), (c) (d), (e), (f) (m), (n) hi gh hi gh hi gh hi gh l ow hi gh hi gh hi gh l ow (g), (h), (i ), (j) (l ) (k) DELTA Di ffDfO See Fi gure 9 – CON +: concordant/ mi l dl y affected; CON : concordant/ severel y affected; ND: non-di scordant (concordant/ moderatel y affected); DIS: di scordant pai r; DC(1): di scordant and concordant/ mi l dl y affected; DC(2): di scordant and concordant/ severel y affected. i ntra-pai r concordance, di d not vary si gni fi cantl y betw een monozygous and di zygous ∆F508 homozygotes (Fi gure 6f–i ). Thi s observati on i ndi cates that monozygous ∆F508 homozygous tw i ns express mi l dl y, moderatel y, and severel y concordant affected phenotypes, and consequentl y rank num+ bers for CON DELTA and the three si mi l arl y deri ved rank numbers di d not segregate w i th the zygosi ty status of the pati ent pai r. Categorisation of CF patient pairs The i nter-rel ati on of al l fi ve rank numbers DISCDELTA , + + – CON DELTA , CON –DELTA , CON Di ffDfO and CON Di ffDfO al l ow ed si x di fferent categori es of pati ent pai rs to be di sti ngui shed (Tabl e 9). For a di scordant pati ent pai r (category DIS, exampl e I i n Tabl e 7), a l ow rank number for DISCDELTA , but hi gh val ues for the other four rank numbers w ere expected. Pai rs ranki ng l ow Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 286 + – i n DISCDELTA and i n CON Di ffDfO or CON Di ffDfO w ere di sti ngui shabl e from category DIS. These pai rs w ere summari sed respecti vel y as di scordant/ concordant mi l d di sease (DC(1); exampl e II i n Tabl e 7) and di scordant/ concordant severe di sease (DC(2)). Concordant/ mi l dy affected pati ent pai rs (category CON + , exampl e III i n Tabl e 7) had l ow rank numbers + + for CON DELTA and CON Di ffDfO, but hi gh val ues for the other three rank numbers. By anal ogy, concordant/ severel y affected pati ent pai rs (category CON –, exampl e V i n Tabl e 7) w ere expected to have l ow val ues for CON –DELTA and CON –Di ffDfO, but hi gh val ues for the other three rank numbers. Concordant/ moderatel y affected pai rs w ere summari sed as nondi scordant (ND, exampl e IV i n Tabl e 7). ND pai rs are expected to have si mi l arl y l ow rank numbers for + + – CON DELTA , CON –DELTA , CON Di ffDfO and CON Di ffDfO si nce, by defi ni ti on, i ntra-pai r concordance and di sease severi ty w as w ei ghted equal l y for each of these rank numbers. Consequentl y, pai rs characteri sed by defi ni te i ntra-pai r concordance but average di sease severi ty w ere ranked rel ati vel y l ow i n each of these sequences. Thus, the ND pai rs w ere di sti ngui shed from pai rs categori sed as CON + and CON – by the l ow di fference betw een thei r corre+ spondi ng rank numbers (CON DELTA –CON –DELTA ) and/ + – or (CON DELTA –CON Di ffDfO). To determi ne unambi guousl y the sequence of pai rs w i thi n each of the categori es, a pai r’s posi ti on i n any of the sequences had to be descri bed by the same al gori thm for al l CF pati ent pai rs (Fi gure 7). Categories of ∆F508 homozygous CF twin and sibling pairs The ranki ng al gori thm (Fi gure 7) w as appl i ed to 114 ∆F508 homozygous CF tw i n and si bl i ng pai rs. The outcome i s show n i n Fi gures 8 and 9. A s i ndi cated i n Fi gure 8b, 59% of the ∆F508 homozygous pai rs w ere pl aced i n categori es DIS, CON + and CON – w hi l e the remai ni ng 41% w ere pl aced i n categori es w i th i ntermedi ate phenotypes ND, DC(1) and DC(2). To i denti fy pai rs from the three categori es DIS (di scordant pai rs), CON + (concordant/ mi l dl y di seased pai rs) and CON – (concordant/ severel y di seased pai rs), w e sorted the cohort of pati ent pai rs so that subsequentl y ranked pai rs possessed the qual i ti es of the respecti ve category i n di mi ni shi ng order: the most di scordant pai r (defi ned by rank 1 i n category DIS) i s fol l ow ed by the second most di scordant pai r (defi ned by rank 2 i n category DIS) and so forth. Li kew i se, pai rs w ere ranked i n categori es CON + and CON –. Thi s ranki ng i s apparent from the cl i ni cal data for the pati ent pai r cohorts show n i n Fi gure 8c. Di scordance decreased w i th i ncreasi ng rank i n the category DIS. Thi s w as true of DELTA as of i ntra-pai r di fferences i n w fh% and Fi gur e 7 Fl ow chart for the assi gnment of 114 ∆F508 homozygous tw i n and si bl i ng pai rs to the categori es DIS, CON + , CON –, ND, DC(1) and DC(2) based on fi ve rank numbers deri ved from composi te parameters (see Tabl e 8 for defi ni ti on and text for detai l s) Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 287 Fi gur e 8 Di sease severi ty and i ntra-pai r di scordance of 114 ∆F508 homozygous tw i n and si bl i ng pai rs assi gned to the categori es DIS, CON + , CON –, ND, DC(1) and DC(2). (a) Layout for (b)–(i ) and proposed rel ati on of the three extreme phenotypes DIS, CON + and CON – to the i ntermedi ate phenotypes ND, DC(1) and DC(2). (b) Occupancy of the categori es w hereby 100% represents the total number of 114 ∆F508 homozygous CF tw i n and si bl i ng pai rs. (c) Defi ni ti on of cohorts w i th decreasi ng rank numbers i n the category and number of pai rs per cohort. * M onozygous tw i ns. (d)–(f) Intra-pai r di scordance as defi ned by average val ues w i thi n the cohorts for DELTA (d), i ntra-pai r di fference of w fh% (e) and i ntra-pai r di fference of FEVPerc (f). (g)–(i ) Di sease severi ty as defi ned by average val ues w i thi n the cohorts for the i ntra-pai r sum of DfO (g), w fh% (h) and FEVPerc (i ) FEVPerc (Fi gure 8d, e and f). In the categori es CON + and CON –, DELTA and the i ntra-pai r di fference i n FVEPerc rai sed w i th i ncreasi ng rank number (Fi gure 8d and f). Intra-pai r di fferences for w fh% w ere l ow er i n categori es CON + and CON – than i n category DIS. The average di sease severi ty of pai rs i n category DIS w ere approxi matel y hal f that of pati ent pai rs ranked CON + or CON – (Fi gure 8g, h and i ). The di ssi mi l ar, non-overl appi ng character of pati ent pai rs i n categori es CON + and CON – i s evi dent from the di ssi mi l ar val ues of the average i ntra-pai r sum i n DfO, w fh% and FEVPerc (Fi g- ure 8g, h and i ). Si mi l arl y, these observati ons are vi si bl e i n Fi gure 9 w here rank numbers for w fh% and FEVPerc for al l 114 ∆F508 homozygous tw i n and si bl i ng pai rs are pl otted agai nst the same axes as the composi te parameters DELTA and DfO (Fi gure 2). CON – pai rs are found i n the l eft area of the di agram due to thei r l ow DfO (Fi gure 9a, b, c), w hi l st CON + pai rs are l ocated i n the upper ri ght area of the di agram i ndi cati ng thei r hi gh DfO (Fi gure 9d, e, f). Both cohorts of concordant pai rs occupy di sti nct, non-overl appi ng areas w i thi n the di agram so that pati ents from pai rs summari sed as ND are l ocated Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 Fi gur e 9 Graphi cal representati on of rank numbers for w fh% and FEVPerc for 114 ∆F508 homozygous categori sed pati ent pai rs. Each pati ent pai r i s depi cted as a set of bl ack and w hi te numbered data poi nts w i thi n a di agram of the rank number FEVPerc (y axi s) pl otted agai nst the rank number for w fh% (x axi s) as defi ned i n Fi gure 2. Both axes of al l di agrams w i thi n thi s fi gure are set to the maxi mal rank number of 636 that can be obtai ned for 318 pai rs. For each pai r, the data poi nt cl oser to the ori gi n i ndi cated by the bl ack col our correspondi ng to the more severel y affected pati ent. The l i ne connecti ng both data poi nts of a pai r represents the composi te parameter DELTA descri bi ng the i ntra-pai r di scordance. The pai rs show n i n fi gures (a) to (n) correspond to the cohorts defi ned i n Fi gure 8c as i s expl ai ned i n the tw o tri angul ar di agrams at the bottom of thi s fi gure. (a)–(c) 19 pai rs categori sed as CON – ordered by i ncreasi ng rank number for CON –DELTA ; (d)–(f) 20 pai rs categori sed as CON + ordered by i ncreasi ng rank number + for CON DELTA ; (g)–(j) 28 pai rs categori sed as DIS ordered by i ncreasi ng rank number for DISCDELTA ; (k) 11 pai rs summari sed as DC(2); (l ) 8 pai rs summari sed as DC(1) ordered i n a sequence w i th decreasi ng DELTA ; (m), (n): 28 pai rs summari sed as ND ordered i n a sequence w i th i ncreasi ng DELTA y Categories of CF patient pairs with distinct phenotypes F Mekus et al 288 Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 289 betw een the tw o extreme concordant phenotypes (Fi gure 9m, n). A djacent to the cohorts CON + (III) (Fi gure 9f) and CON –(III) (Fi gure 9c), more di scordant pai rs w i th hi gh or l ow DfO are summari sed as DC(1) (Fi gure 9l ) and DC(2) (Fi gure 9k). In most of the pai rs i n category DIS (Fi gure 9g, h, i and j), the si bl i ng w i th the better phenotype i s characteri sed by hi gher w fh% and FEVPerc, i ndi cated by the posi ti ve l i ne connecti ng both data poi nts of a di scordant pai r. In contrast, pai rs summari sed as DC(1) or DC(2) are concordant i n w fh% but di scordant i n FEVPerc, or di scordant i n w fh% and concordant i n FEVPerc, or the si bl i ng w i th the better w fh% exhi bi ts the l ow er FEVPerc. Thus, most data poi nts from DC(1) and DC(2) pai rs are l i nked by a l i ne paral l el to the y axi s, or paral l el to the x axi s, or w i th a negati ve sl ope. Di scussi on The cl i ni cal phenotype of the monogeni c di sease CF i s characteri sed by a broad spectrum of di sease severi ty and vari ati on of cl i ni cal course among pati ents w i th the same mutati on genotype i n the di sease-causi ng gene, CFTR.3,4 In recent years, modul ati on of CF di sease by genes other than CFTR has been reported for the anti protease al pha1-anti trypsi n,21 HLA DQB1 al l el es,22 i mmunogl obul i n G al l otypes23 and the mannan-bi ndi ng l ecti n.24 A part from these cl earl y i denti fi ed geneti c enti ti es, the effect of resi dual chl ori de secreti on on CF di sease severi ty has been show n i n i ntesti nal ti ssue (modul ati on of basi c defect)25 and the chromosomal regi on 19q13 has been show n to contai n a modi fi er for meconi um i l eus.26 In summary, geneti c modi fi ers for i sol ated aspects of the CF phenotype have been descri bed, but thei r i mpact on the overal l di sease severi ty of CF remai ns to be eval uated. For the mul ti -organ di sease CF, the anthropometri c parameter w fh% and the l ung functi on parameter FEV1 are i nstrumental i n the fol l ow -up of CF pati ents for moni tori ng grow th, devel opment, gastroi ntesti nal and pul monary di sease.10 By studyi ng affected pati ent pai rs, i e CF tw i ns and si bl i ngs, w e have taken a cl assi c approach to assess the effect of i nheri ted vs envi ronmental factors on the cl i ni cal parameters w fh% and the FEV1 deri ved FEVPerc. The promi nent rol e of the CFTR gene i n CF i s evi dent from the mode of i nheri tance of thi s autosomal recessi vel y transmi tted di sease.1 M ore than 800 reported CF associ ated CFTR mutati ons have been rel i abl y cl assi fi ed as conferri ng exocri ne pancreati c suffi ci ency or i nsuffi ci ency,27,28 but the associ ati on of CFTR mutati on genotype w i th CF di sease mani festati on i s l ess strai ghtforw ard w hen descri bi ng nutri ti onal status or CF pul monary di sease. The same range of di sease mani festati on i s observed i n w fh% and FEVPerc among ∆F508 homozygotes, ∆F508 compound heterozygotes and pati ents w i th non-∆F508/ non-∆F508 genotypes (Tabl e 5), so that the CFTR genotype–CF phenotype associ ati on i s ambi guous. To fi nd the effect of the CFTR mutati on genotype on i ntra-pai r di sease vari abi l i ty, w e eval uated the i ntra-pai r rank number di fference (IRND) di stri buti on among CF pati ent pai r cohorts. When the w hol e cohort w i th vari ous CFTR genotypes w as anal ysed, the tw o members of a tw i n or si b pai r w ere on average si gni fi cantl y more si mi l ar i n both w fh% and FEVPerc than unrel ated pati ents (Tabl e 6 and Fi gure 3), demonstrati ng the i mpact of shared CFTR genotype on the CF di sease phenotype. How ever, among ∆F508 homozygous pai rs representi ng a cohort normal i sed for the genotype i n the major di sease-causi ng gene, any devi ati on of the observed IRND di stri buti on from the di stri buti on expected for unrel ated coupl es cannot be based on the CFTR genotype. ∆F508 homozygotes di ffered i n thei r IRND di stri buti on from random coupl es i n w fh% , but not i n FEVPerc (Tabl e 6 and Fi gure 3). A l though more subtl e effects not evi dent i n 100 pai rs w oul d probabl y show up w i th i ncreasi ng sampl e si ze, the gl obal pi cture i s cl ear. The IRNDs w ere apparentl y randoml y di stri buted for FEVPerc, but si gni fi cantl y skew ed to l ow numbers for w fh% . Thi s can onl y be seen i f the shared factors si gni fi cantl y outw ei gh the i ndi vi dual geneti c and epi geneti c factors. Over-representati on of shared al l el es i n si bs compared w i th unrel ated subjects shoul d account for thei r more si mi l ar w fh% val ues, because anthropometry has a strong i nheri ted component.29–31 How ever, predi cted w ei ght for hei ght i n CF i s affected by eati ng habi ts and l i festyl e,32–34 type of and adherence to hi gh-cal ori e di et,32–34 admi ni strati on of pancreati c enzymes and fat-sol ubl e vi tami ns to treat exocri ne pancreati c i nsuffi ci ency and mal di gesti on of nutri ents35 and frequency and severi ty of respi ratory i nfecti ons.36 A l l i nvesti gated pati ent pai rs, w i th the excepti on of a few adul ts, shared homes, fami l y l i fe and CF physi ci an, and w ere thus exposed to the same nutri ti on and medi cal experti se. Common medi cal treatment and l i vi ng condi ti ons certai nl y contri buted to the si gni fi cantl y l ow er i ntrapai r vari ance i n w fh% than i nter-pai r. A regi me ai med at mai ntenance of normal w ei ght i s refl ected by average val ues for w fh% cl ose to 100% among CF pati ents15 (see Tabl es 4 and 5). A s outl i ned above, i n contrast to nutri ti onal status, i ndi vi dual rather than shared factors determi ned l ung functi on of si bs. Pul monary di sease i n CF i s characteri sed by a vi ci ous cycl e of i nfecti on,37,38 i nappropri ate host defence,37,38 ti ssue di si ntegrati on Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 290 and remodel l i ng39 and i rreversi bl e l oss of pul monary functi on.13,40,41 A l though the ai rw ays of si b pai rs w ere typi cal l y i nfected w i th the same bacteri al strai n (data not show n), di fferi ng host response seems to be more i mportant for progressi on of pul monary di sease than shared envi ronment and geneti cs. Generati on of i mmune response by gene rearrangements and somati c mutati on 42–44 and a hi gh degree of pol ymorphi sm i n i mmunorel evant l oci such as the HLA 45–47 are major reasons w hy si bl i ngs di ffer more i n host defence genotypes than i n any other category of expressed genotypes. The i nterrel ati on betw een genes determi ni ng the i ndi vi dual ’s host defence and the chal l enge by i mmunogeni c, i e envi ronmental , factors appears to have a substanti al i mpact on the pul monary status of CF as demonstrated by di zygous tw i ns havi ng a si gni fi cantl y l ow er FEVPerc compared w i th monozygous tw i ns (Tabl e 4). There i s i ncreased suscepti bi l i ty to i nfecti on i n CF48 and nosocomi al transmi ssi on of bacteri al pathogens i s a know n ri sk 49,50 w hi ch shoul d appl y to al l tw i n pai rs i rrespecti ve of zygosi ty status. How ever, tw o monozygous tw i ns are l i kel y to possess equal host defence capabi l i ti es, w hi l st i n di zygous tw i n pai rs, pathogens confront suscepti bl e i ndi vi dual s w i th a di fferent geneti c repertoi re of host defences. Taken together, these fi ndi ngs i ndi cate that nutri ti onal status i n CF i s modul ated by few factors sti l l detectabl e i n the cohort of 114 ∆F508 homozygous pai rs, w hi l st pul monary di sease i n CF i s modul ated by numerous factors. It i s therefore not surpri si ng that the four most di scordant monozygous tw i n pai rs (Fi gure 6e) demonstrate i ntra-pai r di fferences i n FEVPerc (Fi gure 6b), but w i th w fh% i ntra-pai r di fferences are i nconspi cuous. On the day of eval uati on, these pai rs w ere 30, 16, 9 and 9 years ol d. Tw o pai rs of tw i ns w ere mal e and tw o femal e. It remai ns the subject of specul ati on as to w hether the di scordance i n these pai rs mi ght refl ect the i nfl uence of subtl e geneti c di fferences betw een monozygous tw i ns51 such as vari ati on i n the DNA methyl ati on pattern, the resul t of somati c mutati ons, eg at M HC l oci , or di fferenti al X-i nacti vati on i n the femal e pai rs. Wi th equal probabi l i ty, tw i n di scordance i n bi rth w ei ght w hi ch has been documented among monozygous, parti cul arl y monochori oni c, tw i n pai rs52 mi ght gi ve ri se to di fferences i n the tw i ns’ pul monary status. The compari son of i ntra-pai r di scordance i n monozygous (M Z) and di zygous (DZ) tw i n pai rs i s w i del y accepted to separate the effect of geneti c from epi geneti c factors on the i ndi vi dual ’s phenotype.53,54 The hypothesi s ‘a phenotypi c trai t i s determi ned by i nheri ted factors’ i s sustai ned but not proved by the observati on that monozygous tw i n pai rs are more concordant i n the anal ysed trai t than di zygous tw i n pai rs. Thi s appl i es to the parameter DELTA i n the cohort of 41 CF tw i ns w i th know n zygosi ty status. The composi te parameter descri bi ng i ntra-pai r di scordance based on w fh% and FEVPerc (Fi gure 2) w as si gni fi cantl y l ow er for monozygous than for di zygous tw i ns, i ndi cati ng that monozygous CF tw i ns are more concordant than di zygous CF tw i ns (Tabl e 4). How ever, i ntra-pai r di fferences for both w fh% and FEVPerc w ere si mi l ar betw een monozygous and di zygous CF tw i ns (Tabl e 4). Si nce pul monary functi on and nutri ti onal status are cl i ni cal l y rel ated 55,56 the i ntra-pai r di scordance of ei ther parameter mi ght be enhanced by the other. Consequentl y, DELTA shoul d be more sensi ti ve i n respect of i ntra-pai r di fferences than i s each of the i ndi vi dual parameters. A s a resul t, the concordance of monozygous tw i ns detected by DELTA but not by w fh% and FEVPerc i ndi cates the i nheri ted component besi de the CFTR mutati on genotype that i nfl uences CF di sease severi ty. The i mpact of i nheri ted factors on CF di sease i s supported by the observati on that DELTA i s i ndependent of i ntra-pai r age di fference i n CF si bl i ngs (Fi gure 4): The l esser the age di fference, the more have si bl i ngs shared envi ronmental l i vi ng condi ti ons. Independence of DELTA from i ntra-pai r age di fference suggests a stronger i mpact of shared geneti cs than shared envi ronmental factors on di sease mani festati on i n CF. In other w ords, the shared ti me of exposure to envi ronmental factors and the acti on of the envi ronmental factors on si bs at a comparabl e stage of devel opment, i e the extent of shari ng a pati ent’s hi story and state of devel opment, i s l ess i mportant than age-i ndependent factors. Gi ven the hypothesi s that CF di sease mani festati on i s substanti al l y i nfl uenced by genes other than CFTR, methods of reverse geneti cs may be appl i ed to i denti fy the l oci i nvol ved. How ever, the success of such an approach w i l l be determi ned by the sel ecti on of appropri ate candi dates for such a study. For the anal ysi s of a quanti tati ve trai t extreme phenotypes are general l y consi dered to be more i nformati ve.6–9 Consequentl y a strategy to i denti fy these most i nformati ve pati ent pai rs w as devel oped. A s the di sease phenotype had to be descri bed quanti tati vel y metri c data w as empl oyed to eval uate the compl ex mul ti -organ di sease CF. Usi ng w fh% and FEVPerc, tw o cl i ni cal parameters most sensi ti ve to the course and prognosi s of CF10 w ere combi ned i n order to descri be the overal l di sease severi ty i n the tw o major organs affl i cted, i e the respi ratory and gastroi ntesti nal tracts. Furthermore the composi te parameter DELTA descri bi ng the i ntra-pai r di scordance w as empl oyed i n the sel ecti on procedure. A s has been descri bed i n detai l above, DELTA w as more sensi ti ve to the i nfl uence of geneti c background on CF di sease severi ty and therefore the empl oyment of thi s parameter for pati ent pai r sel ecti on shoul d Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 291 faci l i tate the i denti fi cati on of subjects i nformati ve i n a geneti c study. To avoi d ambi guous scores, a computer-assi sted method w as used to rank pati ent pai rs i n those categori es of pati ent pai rs exhi bi ti ng the phenotypes’ concordant mi l d di sease (CON + ), concordant/ severe di sease (CON –) and di scordant (DIS). To ensure that the sel ected pai rs represented the extremes of a conti nuous spectrum of phenotypes, there had to be no overl ap of cl i ni cal characteri sti cs i n the compari son of pai rs from the cohorts DIS, CON + and CON –. A s demonstrated i n Fi gure 8, the al gori thm empl oyed for ranki ng the 114 ∆F508 homozygous pai rs resul ted i n the i denti fi cati on of CON + and CON – pati ent pai rs w i th non-overl appi ng w fh% and FEVPerc val ues. Li kew i se, di scordance i n both cl i ni cal parameters w as di sti nct among pai rs ranked DIS compared w i th pai rs ranked CON + or CON –. In concl usi on, the ∆F508 homozygous tw i n and si bl i ng pai rs expressed vari ous phenotypes. Three categori es of extreme phenotypes – DIS, CON + and CON – and three categori es w i th i ntermedi ate and/ or uncommon phenotypes coul d be di sti ngui shed and w ere characteri sed as phenotypi cal l y di sti nct enti ti es i n respect of pul monary functi on and the nutri ti onal state of the CF pati ents. A ck now l edgements Thi s w ork w as executed as part of the European Cysti c Fi brosi s Tw i n and Si bl i ng Study and supported by the BIOM ED II programme of the EU, the Deutsche Forschungsgemei nschaft, the Deutsche Fördergesel l schaft f ür di e M ukovi szi doseforschung eV, and the M ukovi szi dose eV. The authors thank J Hundri eser (Hannover) and H Otten, R Saml al -Soedhoe and DJJ Hal l ey (Rotterdam) for tw i n typi ng, and J Zeyßi g for her hel p i n prepari ng the manuscri pt. The core teams from Hannover and Rotterdam w oul d l i ke to take thi s opportuni ty to w arml y thank al l pati ents and thei r fami l i es, the physi ci ans, CF centres and thei r staff for thei r ti me, co-operati on and assi stance, w i thout w hi ch thi s study w oul d not have been possi bl e. In parti cul ar w e w oul d l i ke to thank the fol l ow i ng physi ci ans and thei r staff for thei r hel p and support: Professor M A l berti ni , Centre Hospi tal i er Uni versi tai re de Ni ce, Pédi atri e, Ni ce, France; Dr F d Baets, UZ-Gent, Gent, Bel gi um; Dr D Baran, H ôpi tal Erasme, Brussel s, Bel gi um; Professor G Bel l on, Centre Hospi tal i er Lyon Sud, Pi erre Béni te, France; Dr Bertrand, Cl i ni que St-Vi ncent, Rocourt, Bel gi um; Dr Franz, Techni sche Uni versi t ät M ünchen, Germany; Dr P Bi ttner-Dersch, Uni vKi nderkl i ni k, Gi eßen, Germany; Dr C de Boeck, UZ Gasthui sberg, Leuven, Bel gi um; Dr S Borsti ng, Levanger, Norw ay; Dr S Bourke, Dr R Brew i s, Royal Vi ctori a Infi rmary, New castl e upon Tyne, UK; Dr D Bozon, Hospi tal Debrousse, Lyon, France; Dr C Bredi n, Cork Uni versi ty Hospi tal , Cork, Irel and; Dr K Breuel , Uni versi t ät Rostock M edi cal School , Rostock, Germany; Dr S Br ömme, M edi cal School , M arti n-LutherUni versi t ät, Hal l e, Germany; Dr J Brouard, CHU de Caen, Caen, France; Dr R Burger, Ki nderspi tal Z üri ch, Z üri ch, Sw i tzerl and; Dr Bärmei er, Uni v Kl i ni k f ür Ki nder und Jugendl i che, Erl angen, Germany; Dr von Buttl er, Ki nderkl i ni k Essl i ngen, Essl i ngen, Germany; Dr I Campbel l , Ll andough Hospi tal , Penarth, Wal es, UK; Professor A Carbonara, Serv Uni v di Geneti ca M edi ca, Tori no, Ital y; Dr F Carsw el l , Bri stol Chi l dren’s Hospi tal , Bri stol , UK; Professor I Caudarr ère, CM C Foch, Suresnes, France; Dr J-P Chazal ette, H ôpi tal R Sabran, Gi ens, France; Dr A Cl aaß, Uni v-Ki nderkl i ni k, Ki el , Germany; Dr M Cl aßen, ZKH ‘Li nks der Weser’, Bremen, Germany; Professor M Cl austres, Insti tut de Bi ol ogi e, M ontpel l i er, France; Dr G Connett, Southampton General Hospi tal , Southampton, UK; Dr Conw ay, Seacroft Hospi tal , Leeds, UK; Dr H Cuppens, Center for Human Geneti cs, Leuven, Bel gi um; Professor I Dab, Prof Li ebaers, Dr Legei n, A ZK-VUB, Brussel s, Bel gi um; Dr J Dankert-Roel se, Free Uni versi ty, A msterdam, Netherl ands; Dr J Dapena, Hospi tal Infanti l Uni versi tari o, Sevi l l a, Spai n; Professor T Davi d, Booth Hal l Chi l dren’s Hospi tal , M anchester, UK; Dr R Di nw i ddi e, Gt Ormond St Hospi tal , London, UK; Dr H Döhmen, Dr F Fri edri chs, A achen-Laurensberg, Germany; Dr J Domagk, Uni v-Ki nderkl i ni k, Götti ngen, Germany; Professor H Domi ni ck, Ki nderkl i ni k St A nnasti ft, Ludw i gshafen, Germany; Department of Chi l d Heal th, Dundee Ni new el l s Hospi tal , Dundee, Scotl and, UK; Dr F Ei tel berger, A KH, Wel s, A ustri a; Dr I Ei chl er, Uni v-Ki nderkl i ni k, Vi enna, A ustri a; Dr H El l emunter, Uni v-Ki nderkl i ni k, Innsbruck, A ustri a; Dr B Fauroux, H ôpi tal d’Enfants A rmand-Trousseau, Pari s, France; Dr J Ferrer-Cal vette, Hospi tal , ‘La Fe’, Val enci a, Spai n; Professor M Fi tzgeral d, St Vi ncent’s Hospi tal , Dubl i n, Irel and; Dr J Fei gel son, Pari s, France; Dr Foucard, Centre Hospi tal i er de Versai l l es, Versai l l es, France; Dr O Fovet, Centre Hospi tal i er Secl i n, France; Dr J Fri end, Ci ty Hospi tal , A berdeen, Scotl and, UK; Fri ml ey Park Hospi tal , Camberl ey, Surrey, UK; Dr Gei er, St ädt, Krankenhaus Hei l bronn, Hei l bronn, Germany; Dr Generl i ch, Ki nderkl i ni k Li ndenhof, KH Li chtenberg, Berl i n, Germany; Dr M Goodchi l d, Uni versi ty Hospi tal of Wal es, Cardi ff, Wal es, UK; Professor M Götz, Wi l hel mi nenspi tal , Vi enna, A ustri a; Dr I Graupner, Pol i kl i ni k am Kl i ni kum Buch, Berl i n, Germany; Dr J Günther, Chemni tz, Germany; Professor Gui l l ard, H ôpi tal d’Enfants, Bordeaux, France; Dr G Hambl eton, Royal M anchester Chi l dren’s Hospi tal , M anchester, UK; Dr J Hautz, Krei skrankenhaus, Offenburg, Germany; Dr L Heaf, A l der Hey Chi l dren’s Hospi tal , Li verpool , UK; Professor P Hel ms, Dr G Russel l , Uni versi ty of A berdeen M edi cal School , A berdeen, Scotl and, UK; Dr D Hubert, H ôpi tal Cochi n, Pari s, France; Dr L Huel te, Huddi nge Hospi tal , Stockhol m, Sw eden; Dr A Innes, Western General Hospi tal , Edi nburgh, Scotl and, UK; Dr D Journel , Centre Hospi tal i er, Vannes, France; Dr M Kal z, Ruppi ner Kl i ni kum GmbH, Neuruppi n, Germany; Dr K Kel l er, Uni vKi nderkl i ni k, Bonn, Germany; Dr U Kl aer, Otto-von-Gueri cke-Uni versi t ät, M agdeburg, Germany; Dr C Koch, Dr N Høi by, Uni versi ty Hospi tal , Copenhagen, Denmark; Dr H Koch, St M ari enhospi tal Vechta, Germany; Dr R Kornfal t, Uni versi ty Hospi tal , Lund, Sw eden; Dr E Kr üger, St ädti sches Kl i ni kum, Brandenburg, Germany; Dr P K üster, Cl emenshospi tal , M ünster, Germany; Dr J van der Laag, Wi l hel mi na Chi l dren’s Hospi tal , Utrecht, Netherl ands; Dr G Leen, Nati onal Chi l dren’s Hospi tal , Dubl i n, Irel and; Professor Lemarec, Rennes, France; Dr C Lenaerts, CHU, A mi ens, France; Professor G Lenoi r, H ôpi tal des Enfants M al ades, Pari s, France; Dr V Leucht, Fachkl i ni k f ür Lungenkrankhei ten, Cosw i g, Germany; Dr S Wal ter, Uni versi t ätski nderkl i ni k Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 292 Lei pzi g, Lei pzi g, Germany; Dr J Li ttl ew ood, St James’s Hospi tal , Leeds, Engl and, UK; Prof B Loftus, Uni versi ty Col l ege Gal w ay, Gal w ay, Irel and; Dr U Ludw i g, Uni vKi nderkl i ni k, Fri edri ch-Schi l l er-Uni versi t ät Jena, Jena, Germany; Professor G M astel l a, Ospedal e M aggi ore, Verona, Ital y; Dr M Donagh, Sl i go General Hospi tal , Sl i go, Irel and; Dr S M cGui re, Royal Gw ent Hospi tal , New port, Gw ent, UK; Dr E M eyer, Rei nhard-Nei ter-Krankenhaus, Wi l hel mshaven, Germany; Dr O M outerde, Professor E M al l et, H ôpi tal Charl es Ni col l e, Rouen, France; Dr R Nel son, Royal Vi ctori a Infi rmary, New castl e upon Tyne, UK; Dr R Oosterkamp, ZCA , A pel doorn, Netherl ands; Dr J Opi tz, Ki nderkl i ni k, Kl i ni kum E v Bergmann, Potsdam, Germany; Dr R Padoan, Isti tuti Cl i ni ci di Perfezi onamento, M i l an, Ital y; Dr Panti n, Dr Campbel l , North Staffordshi re Hospi tal , Stoke-on-Trent, UK; Dr Paul , Uni v-Ki nderkl i ni k, Dresden, Germany; Professor F Pennaforte, A meri can M emori al Hospi tal , Rei ms, France; Dr G Pi cherot, Centre Hospi tal i er de St-Nazai re, France; Dr F Ratjen, Uni versi t ätskl i ni kum Essen, Essen, Germany; Dr A Redmond, Royal Bel fast Hospi tal for Si ck Chi l dren, Bel fast, N Irel and, UK; Dr E Ri etschel , Ki nderkl i ni kum K öl n, K öl n, Germany; Professor L Romano, Gasl i ni Insti tute, Genova, Ital y; Dr H Röni tz, Kl i ni kum Frankfurt (Oder), Frankfurt/ O, Germany; Dr M Rosenthal , Carshal ton, Surrey, UK; Dr I Rappay, Dr M Roul et, CHUV, Lausanne, Sw i tzerl and; Dr G Russel l , Royal A berdeen Chi l dren’s Hospi tal , A berdeen, Scotl and, UK; Professor M Ruti shauser, Uni versi t ätski nderkl i ni k, Basal , Sw i tzerl and; Dr B Sabl ayrol l es, Toul ouse, France; Dr J Sarl es, H ôpi tal d’Enfants, M arsei l l e, France; Professor O Schi øtz, A arhus Communi ty Hospi tal , A arhus, Denmark; Dr J Schri ever, A kadem Lehrkrankenhaus der Uni versi t ät Bonn, M echerni ch, Germany; Dr Schul ze-Everdi ng, Uni -Ki nderkl i ni k, M ünster, Germany; Dr J Sei denberg, El i sabeth-Ki nderkrankenhaus, Ol denburg, Germany; Dr F Sennhauser, Ki nderspi tal St Gal l en, Ki nderkl i ni k Z üri ch, Sw i tzerl and; Dr C Shel don, Royal Devon and Exeter Hospi tal , Exeter, UK; Dr E Sol yom, Chi l dren’s Hospi tal , M i skol c, Hungary; Dr D Stabl eforth, Bi rmi ngham Heartl ands Hospi tal , Bi rmi ngham, UK; Dr B Stei nbrugger, Uni v-Ki nderkl i ni k, Graz, A ustri a; Dr Stei nschnei der, Centre Hospi tal i er, M eaux, France; Professor M Stern, Uni versi t äts-Ki nderkl i ni k, T übi ngen, Germany; Dr K-D Stettni sch, Krei skrankenhaus Nauen, Berl i n, Germany; Dr O St öl l i nger, A l l gem Öffentl Krankenhaus, Li nz, A ustri a; Professor S Suter, H ôpi tal des Enfants, Gén ève, Sw i tzerl and; Dr R Szczepanski , Ki nderhospi tal Iburger Str, Osnabr ück, Germany; Dr C Tayl or, The Chi l dren’s Hospi tal , Sheffi el d, UK; Dr L Tempany, Cl i ath, Ei re; Dr D Theveni eau, Centre Hospi tal i er Gén éral , A i x-en-Provence, France; Dr K Thoß, Ki nderkl i ni k, Vogtl and-Kl i ni kum Pl auen, Pl auen, Germany; Dr Traw i nska-Bartni cka, Spi tal Dzi ecLi em, Gdansk, Pol and; Dr J Vai zey, Pi l gri m Hospi tal , Boston, UK; Dr Van Schi l , St Vi ncenti us Hospi tal , A ntw erp, Bel gi um; Dr C Vazquez, Hospi tal de Cruces, Cruces-Bi l bao, Spai n; Dr B Watson, Cork Uni versi ty Hospi tal , Cork, Ei re; Professor H Wehi nger, St ädt Ki nderkl i ni k, Kassel , Germany; Dr G Wei nmann, Kl i ni kum Efurt, Efurt, Germany; Dr P Wel l er, Chi l dren’s Hospi tal , Ladyw ood, Bi rmi ngham, UK; Dr A Wel l s, Bradbury CF Uni t, South M anchester, UK; Dr W Wi ebi cke, Zentral krankenhaus St-Jürgen-Str, Bremen, Germany; Professor S Wi ersbi tzky, Kl i ni k und Pol i kl i ni k f ür Ki ndermedi zi n, Grei fsw al d, Germany; Dr M Wi tt, Insti tute of Human Geneti cs, Pozn án, Pol and; Dr A Wol f, Uni versi t ätsKi nderkl i ni k, Ul m, Germany; Dr J W öl fe, Ki nderkrankenhaus, Ravensburg, Germany. Refer ences 1 Wel sh M J, Tsui LC, Boat TF, Beaudet A L. Cysti c fi brosi s. In: Scri ver CR, Beaudet A L, Sl y WS, Val l e D (eds). The Metabolic and Molecular Basis of Inherited Disease. M cGraw -Hi l l , New York: 1995; pp 3799–3876. 2 Kerem BS, Rommens JM , Buchanan JA , M arki ew i cz D, Cox RTK, Chakravarti A , Buchw al d M , Tsui LC. Identi fi cati on of the cysti c fi brosi s gene: geneti c anal ysi s. Science 1989; 245: 1073–1080. 3 Johannsen HK, Ni r M , Hoi by N, Koch C, Schw artz M . Severi ty of cysti c fi brosi s i n pati ents homozygous and heterozygous for the ∆F508 mutati on. Lancet 1991; 337: 631–634. 4 Kerem E, Corey M , Kerem BS, Rommens J, M arki ew i cz D, Levi son H, Tsui LC, Duri e P. The rel ati onshi p betw een genotype and phenotype i n cysti c fi brosi s – anal ysi s of the most common mutati on (∆F508). N Engl J Med 1990; 323: 1517–1522. 5 European Worki ng Group on Cysti c Fi brosi s Geneti cs. Gradi ent of di stri buti on i n Europe of the major CF mutati on and of i ts associ ated hapl otype. Hum Genet 1990; 85: 436–445. 6 Dol an CV, Boomsma DI. Opti mal sel ecti on of si b pai rs from random sampl es for l i nkage anal ysi s of a QTL usi ng the EDA C test. Behav Genet 1998; 28: 197–206. 7 Ri sch N, Zhang H. Extreme di scordant si b pai rs for mappi ng quanti tati ve trai t l oci i n humans. Science 1995; 16: 268: 1584–1589. 8 Ri sch NJ, Zhang H. M appi ng quanti tati ve trai t l oci w i th extreme di scordant si b pai rs: sampl i ng consi derati ons. Am J Hum Genet 1996; 58: 836–843. 9 Eaves L, M eyer J. Locati ng human quanti tati ve trai t l oci : gui del i nes for the sel ecti on of si bl i ng pai rs for genotypi ng. Behav Genet 1994; 24: 443–455. 10 Corey M , M cLaughl i n FJ, Wi l l i ams M , Levi nson H. A compari son of survi val , grow th, and pul monary functi on i n pati ents w i th cysti c fi brosi s i n Boston and Toronto. J Clin Epidemiol 1998; 41: 583–591. 11 Prader A , Largo RH, M ol i nari L, Issl er C. Physi cal grow th of Sw i ss chi l dren from bi rth to 20 years of age. Fi rst Zuri ch l ongi tudi nal study of grow th and devel opment. Helv Pediatr Acta Suppl 1989; 52: 1–125. 12 Knudson RJ, Lebow i tz M D, Hol berg CJ, Burrow s B. Changes i n the normal maxi mal expi ratory fl ow vol ume curve w i th grow th and agei ng. Am Rev Respir Dis 1983; 127: 725–734. 13 Corey M , Edw ards L, Levi nson H, Know l es M . Longi tudi nal anal ysi s of pul monary functi on decl i ne i n pati ents w i th cysti c fi brosi s. J Pediatr 1997; 131: 809–814. 14 Avai l abl e from URL: http:/ / w w w.ERCF.org 15 Lai HC, Corey M , Fi tzSi mmons S, Korosok M R, Farrel l PM . Compari son of grow th status of pati ents w i th cysti c fi brosi s betw een the Uni ted States and Canada. Am J Clin Nutr 1999; 69: 531–538. 16 Sachetti L, Cal cagno G, Coto I, Ti nto N, Vuttari el l o E, Sal vatore F. Effi ci ency of tw o di fferent ni ne-l oci short tandem repeat systems for DNA typi ng purposes. Clin Chem 1999; 45: 178–183. 17 Eppl en JT, M el mer G, Schmi dt P, Roew er L, Hundri eser J, Eppl en C, Bui tkamp J. On the potenti al of si mpl e repeti ti ve DNA for fi ngerpri nti ng i n cl i ni cal , forensi c, and evol uti onary dynami c studi es. Clin Invest 1992; 70: 1043–1051. 18 Weber E. Grundriss der biologischen Statistik. Gustav Fi scher Verl ag, Stuttgart: 1980; 190–191. 19 Weber E. Grundriss der biologischen Statistik. Gustav Fi scher Verl ag, Stuttgart: 1980; 184–190. 20 Weber E. Grundriss der biologischen Statistik. Gustav Fi scher Verl ag, Stuttgart: 1980; 204–207. Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277 y Categories of CF patient pairs with distinct phenotypes F Mekus et al 293 21 Döri ng G, Krogh-Johansen H, Wei di nger S, Hoi by N. A l l otypes of al pha-1-anti trypsi n i n pati ents w i th cysti c fi brosi s, homozygous and heterozygous for del taF508. Pediatr Pulmonol 1994; 18: 3–7. 22 Carri ngton M , Krueger LJ, Hol scl aw DS Jr, Iannuzzi M C, Dean M , M ann D. Cysti c fi brosi s-rel ated di abetes i s associ ated w i th HLA DQB1 al l el es encodi ng A sp-57-mol ecul es. J Clin Immunol 1994; 14: 353–358. 23 Ci ofu O, Pressl er T, Pandey JP, Hoi by N. The i nfl uence of al l otypes on the IgG subcl ass response to chromosomal betal actamase of Pseudomonas aeruginosa i n cysti c fi brosi s pati ents. Clin Exp Immunol 1997; 108: 88–94. 24 Garred P, Pressl er T, M adesen HO, Fredri ksen B, Svejgaard A , Høi by N, Schw artz M , Koch C. A ssoci ati on of mannosebi ndi ng l ecti n gene heterogenei ty w i th severi ty of l ung di sease and survi val i n cysti c fi brosi s. J Clin Invest 1999; 104: 431–437. 25 Veeze HJ, Hal l ey DJ, Bi jman J, de Jongste JC, de Jonge HR, Si naasappel M . Determi nants of mi l d cl i ni cal symptoms i n cysti c fi brosi s pati ents. Resi dual chl ori de secreti on measured i n rectal bi opsi es i n rel ati on to the genotype. J Clin Invest 1994; 93: 461–466. 26 Zi el enski J, Corey M , Rozmahel R, M arki ew i cz D, A znarez I, Casal s T, Larri ba S, M erci er B, Cutti ng GR, Krebsova A , M acek M Jr, Langefel der-Schw i nd E, M arshal l BC, DeCel i e-Germana J, Cl austres M , Pal aci o A , Bal J, Now akow ska A , Ferec C, Esti vi l l X, Duri e P, Tsui LC. Detecti on of a cysti c fi brosi s modi fi er l ocus for meconi um i l eus on human chromosome 19q13. Nat Genet 1999; 22: 128–129. 27 Santi s G, Osborne L, Kni ght RA , Hodson M E. Independent geneti c determi nants of pancreati c and pul monary status i n cysti c fi brosi s. Lancet 1990; 336: 1081–1084. 28 Kri sti di s P, Bozon D, Corey M , M arki ew i cz D, Rommens J, Tsui LC. Geneti c determi nants of exocri ne pancreati c functi on i n cysti c fi brosi s. Am J Hum Genet 1992; 50: 1178–1184. 29 Katzmarzyk PT, M ahaney M C, Bl angero J, Quek JJ, M al i na RM . Potenti al effects of ethni ci ty i n geneti c and envi ronmental sources of vari abi l i ty i n the stature, mass, and body mass i ndex of chi l dren. Hum Biol 1999; 71: 977–987. 30 Pi eti l ai nen KH, Kapri o J, Ri ssanen A , Wi nter T, Ri mpel a A , Vi ken RJ, Rose RJ. Di stri buti on and heri tabi l i ty of BM I i n Fi nni sh adol escents aged 16 y and 17 y: a study of 4884 tw i ns and 2509 si ngl etons. Int J Obes Relat Metab Disord 1999; 23: 107–115. 31 Gi nsburg E, Li vshi ts G, Yakovenko K, Kobyl i anski E. M ajor gene control of human body w ei ght and BM I i n fi ve ethni cal l y di fferent popul ati ons. Ann Hum Genet 1998; 62: 307–322. 32 Dani el s LA , Davi dson GP. Current i ssues i n the nutri ti onal management of chi l dren w i th cysti c fi brosi s. Aust Pediatr J 1989; 25: 261–266. 33 Crevel i ng S, Li ght M , Gardner P, Greene L. Cysti c Fi brosi s, nutri ti on, and the heal th care team. J Am Diet Assoc 1997; 97: S186–S191. 34 Stark LJ, M ul vi hi l l M M , Pow ers SW, Jel al i an E, Keati ng K, Crevel i ng S, Byrnes-Col l i ns B, Harw ood I, Passero M A , Li ght M , M i l l er DL, Hovel l M F. Behavi oral i nterventi on to i mprove cal ori e i ntake of chi l dren w i th cysti c fi brosi s: treatment versus w ai t l i st control . J Pediatr Gastroenterol Nutr 1996; 22: 240–253. 35 A nthony H, Col l i ns CE, Davi dson G, M ew s C, Robi nson P, Shepherd R, Stapl eton D. Pancreati c enzyme repl acement therapy i n cysti c fi brosi s: A ustral i an gui del i nes. Pedi atri c Gastroenterol ogi cal Soci ety and the Di eti ans A ssoci ati on of A ustral i a. J Pediatr Child Health 1999; 35: 125–129. 36 Rei l l y JJ, Ral ston JM , Paton JY, Edw ards CA , Weaver LT, Wi l ki nson J, Evans TJ. Energy bal ance duri ng acute respi ratory exacerbati ons i n chi l dren w i th cysti c fi brosi s. Eur Respir J 1999; 13: 804–809. 37 Döri ng G. Cysti c fi brosi s respi ratory i nfecti ons: i nteracti ons betw een bacteri a and host defence. Monaldi Arch Chest Dis 1997; 52: 363–366. 38 Koch C, Høi by N. Pathogenesi s of cysti c fi brosi s. Lancet 1993; 341: 1065–1069. 39 Tomashefski JF Jr, Bruce M , Gol dberg HI, Dearborn DG. Regi onal di stri buti on of macroscopi c l ung di sease i n cysti c fi brosi s. Am Rev Respir Dis 1986; 133: 535–540. 40 Bal ti more RS, Chri sti e CD, Smi th GJ. Immunohi stopathol ogi c l ocal i zati on of Pseudomonas aeruginosa i n l ungs from pati ents w i th cysti c fi brosi s. Impl i cati ons for the pathogenesi s of progressi ve l ung deteri orati on. Am Rev Respir Dis 1989; 140: 1650–1661. 41 Corey M , Farew el l V. Determi nants of mortal i ty from cysti c fi brosi s i n Canada, 1970–1989. Am J Epidemiol 1996; 143: 1007–1017. 42 Storb U. Progress i n understandi ng the mechani sm and consequences of somati c hypermutati on. Immunol Rev 1998; 162: 5–11. 43 Rajew ski K. Cl onal sel ecti on and l earni ng i n the anti body system. Nature 1996; 381: 751–758. 44 Wei l l JC, Reynaud CA . Rearrangement/ hypermutati on/ gene conversi on; w hen, w here and w hy? Immunol Today 1996; 17: 92–97. 45 Daw ki ns R, Leel ayuw at C, Gaudi eri S, Tay G, Hui J, Cattl ey S, M arti nez P, Kul uski J. Genomi cs of the major hi stocompati bi l i ty compl ex: hapl otypes, dupl i cati on, retrovi ruses and di sease. Immunol Rev 1999; 167: 275–304. 46 Hughes A L, Yeager M . Natural sel ecti on at major hi stocompati bi l i ty compl ex l oci of vertebrates. Annu Rev Genet 1998; 32: 415–435. 47 Hi l l AV. The i mmunogeneti cs of human i nfecti ous di seases. Annu Rev Immunol 1998; 16: 593–617. 48 T ümml er B, Ki ew i tz C. Cysti c fi brosi s: an i nheri ted suscepti bi l i ty to bacteri al respi ratory i nfecti ons. Mol Med Today 1999; 5: 351–358. 49 T ümml er B, Koopmann U, Grothues D, Wei ssbrodt H, Stei nkamp G, von der Hardt H. Nosocomi al acqui si ti on of Pseudomonas aeruginosa by cysti c fi brosi s pati ents. J Clin Microbiol 1991; 29: 1265–1267. 50 Grothues D, Koopmann U, von der Hardt H, T ümml er B. Genome fi ngerpri nti ng of Pseudomonas aeruginosa i ndi cates col oni zati on of cysti c fi brosi s si bl i ngs w i th cl osel y rel ated strai ns. J Clin Microbiol 1988; 26: 1973–1977. 51 Corey LA , Nance WE, Kang KW, Chri sti an JC. Effects of type and pl acentati on on bi rthw ei ght and i ts vari abi l i ty i n monozygoti c and di zygoti c tw i ns. Acta Genet Med Gemellol Croma 1988; 37: 229–238. 52 M achi n G. Some causes of genotypi c and phenotypi c di scordance i n monozygoti c tw i n pai rs. Am J Med Genet 1996; 61: 216–228. 53 M arti n N, Boomsma D, M achi n G. A tw i n-pronged attack on compl ex trai ts. Nat Genet 1997; 17: 387–392. 54 Phi l l i ps DIW. Tw i n studi es i n medi cal research: can they tel l us w hether di seases are geneti cal l y determi ned? Lancet 1993; 341: 1008–1009. 55 Stei nkamp G, von der Hardt H. Improvement of nutri ti onal status and l ung functi on after l ong-term nocturnal gastrostomy feedi ngs i n cysti c fi brosi s. J Pediatr 1994; 124: 244–249. 56 Stei nkamp G, Drommer A , von der Hardt H. Resti ng energy expendi ture before and after treatment for Pseudomonas aeruginosa i nfecti on i n pati ents w i th cysti c fi brosi s. Am J Clin Nutr 1993; 57: 685–689. Twin Research Downloaded from https:/www.cambridge.org/core. IP address: 88.99.165.207, on 17 Jun 2017 at 07:45:32, subject to the Cambridge Core terms of use, available at https:/www.cambridge.org/core/terms. https://doi.org/10.1375/twin.3.4.277
© Copyright 2026 Paperzz